
Submitted:
20 December 2024
Posted:
25 December 2024
You are already at the latest version
Abstract
Integrated serological surveillance involves testing for antibodies to multiple pathogens (or species) simultaneously and can be achieved using multiplex bead assays (MBA). This systematic review aims to describe: pathogens studied using MBA; the operational implementation of MBA, and how data generated was synthesised. In November and December 2023, four databases were searched for studies utilising MBA for integrated surveillance of infectious diseases. Two reviewers independently screened and extracted data regarding study settings and population, methodology, seroprevalence results, and operational implementation elements. Overall, 4,765 studies were identified; 47 were eligible for inclusion, of which 43% investigated multiple malaria species, and 17% for concurrent surveillance of malaria and other infectious diseases (including lymphatic filariasis and tetanus). Only seven studies were found where integrated serosurveillance was the primary objective. Synthesis of data varied and included investigation of age-specific seroprevalence (n=25), risk factor analysis (n=15), and spatial analysis of disease prevalence (n=8). This review demonstrated that the use of MBA for integrated surveillance of multiple pathogens is gaining traction; however, more research and capabilities in lower- and middle-income countries are needed to optimise and standardise sample collection, survey implementation, and analysis and interpretation of results.
Keywords:
public health
; malaria
; neglected tropical diseases
; vaccine preventable diseases
; vector-bourne diseases
; serological surveillance
; IgG
; antibody
; seropositive
Introduction and Background
To monitor progress towards the prevention, control, elimination, and eradication of infectious diseases, accurate and timely surveillance is required [1]. To support the development of targeted public health interventions, population-level serological surveys can provide rich data regarding immunity to infectious diseases from past infection or vaccination, and current burden of chronic infections [2]. However, in low resource settings, disease surveillance is challenged by issues surrounding the time and cost involved in this process and often, diseases are monitored in isolation [3,4]. Furthermore, as disease prevalence within populations decreases, it becomes increasingly difficult to identify remaining individuals, leading to more heterogenous and sparse patterns of disease [3]. One effective method to address these challenges is integrated serological surveillance (serosurveillance), whereby surveys test for multiple pathogens or species of pathogens using a single specimen [4]. Integrated serosurveillance offers many advantages compared to a siloed single disease approach whereby importantly, the time required for sample collection and analysis is significantly reduced when examining multiple pathogens simultaneously.
A commonly employed method for conducting serological analysis of samples for multiple pathogens simultaneously is through multiplex bead assays (MBA), which utilise microscopic beads containing fluorescent dye and target molecules to allow for quantitative analysis of multiple targets simultaneously [5]. For measuring immunoglobulin-G (IgG) antibodies, median fluorescence intensity (MFI) is considered proportional to levels of antigen-specific antibodies in the blood, and a proxy for antibody titers [6]. This can be transformed quantitatively into estimates of seroprevalence to provide information regarding population-level infection, or vaccination coverage for specific pathogens [6]. This technique is less labour intensive compared to traditional single-pathogen analysis such as ELISAs [7] and by analysing samples concurrently, measurement error and bias are minimised since all samples are subjected to the same conditions [8].
Following infection, pathogen-specific antibodies are produced and act as biomarkers that can last from month to years, depending on the pathogen [4]. The use of serology-based epidemiology (sero-epidemiology) as a surveillance method has been shown to be a highly sensitive and specific tool that can detect both high and low prevalence of infection [9], and improve our understanding of the epidemiology of infectious diseases. When combined with geospatial and statistical modelling, serosurveillance data can also be used to produce important insights, such as identifying hotspots of disease occurrence or cold spots of low prevalence of immunity to vaccination-preventable diseases (VPD).
This review aimed to determine how MBA has been used for integrated serosurveillance of infectious diseases and discuss the public health implications of utilising MBA for integrated serosurveillance.
Objectives:
- i)
- To describe the pathogens studied using MBA for serosurveillance.
- ii)
-
To describe the operational implementation of using MBA for serosurveillance:
- Sampling design to determine target population,
- How the samples were collected,
- MBA antibody targets, and
- Laboratories where MBA was conducted.
- iii)
-
To describe the geographical distribution of studies and types of applications of MBA for serosurveillance:
- Synthesis of data,
- Seroprevalence findings, and
- Public health implications.
Methods
Protocol and registration: This systematic review protocol was registered with the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY) in April 2024 [10].
Literature Search: A systematic literature review was performed between November and December 2023 using the following databases: PubMed, MEDLINE, Scopus, Embase and Cochrane Library. Full Boolean and search optimisation and refinement strategies used for each search can be found in Supplementary Material 1. Article screening and data extraction were completed using Covidence (Melbourne, Australia) [11] by two independent reviewers (SW and HL) and any discrepancies were resolved by a third reviewer (BS). This review was completed in accordance with the PRISMA checklist for systematic reviews [12], which is included in Supplementary Material 6.
Inclusion and exclusion criteria: All observational and intervention studies utilising MBA for concurrent serosurveillance of more than one infectious disease were included. There was no limit to the time of publication of studies. To expand the scope of this review, articles reporting multiple species of a single pathogen were also included. As the focus for this review was on the applied use of MBA, we excluded studies that did not report any research data (commentaries, letters, editorials, viewpoints, reviews) and those with a limited focus (case reports, case series, outbreak reports). Studies not published in English or reporting indirect measures of seroprevalence (such as odds ratios for disease prevalence in certain areas compared to others) were excluded. Lastly, studies were excluded if they were conducted only for validation or calibration of laboratory methods, without reporting prevalence.
Data collection: Data were extracted using Covidence and collated into a tabular format to capture the following information: author (year), study design, World Health Organization (WHO) region, country where study was conduct, operational details of sample collection, integrated surveillance type (multiple species of one pathogen or multiple pathogens), diseases studied, antigens and/or antibodies used, collection of repeated samples over time, sampling design of studies, participant demographics (target population), blood collection method, year of sample collection, year of sample testing, total number of participants (sample size), country/laboratory of sample analysis, disease prevalence findings, practical implications, and additional diagnostics used. A narrative summary of the data extracted from the studies is provided. Some studies examined pathogens other than neglected tropical diseases (NTDs), vaccine preventable diseases (VPDs), and malaria, and were grouped as “other”. Studies were placed into categories based on the pathogens studied:
- i)
- Malaria (two or more species)
- ii)
- VPDs (two or more pathogens)
- iii)
- Combination of NTDs/VPDs/Other
- iv)
- Malaria plus combination of NTDs/VPDs/Other
Results
A total of 4,765 records were identified, of which 956 were automatically detected as duplicates through the Covidence application (Melbourne, Australia) [11] . Following title and abstract screening, 354 remained for full text screening. Finally, 47 studies (Table 1) fulfilled inclusion criteria (Figure 1).
Location of studies and time from sample collection to publication: Studies were identified from 30 countries, of which 20 (66%) were conducted in the African region, 12 in the Americas region (25%), eight in the Western Pacific region (17%), four studies in the European region (8%), and three in the South-East Asian region (6%). Haiti (n=8) was the most studied country, followed by Ethiopia (n=6), Bangladesh (n=3), Kenya (n=3), and Tanzania (n=3). The median time between collection of samples and publication of studies was four years (range: 1-14 years). The earliest study was published in 2011, with peak number of studies (n=13) published in 2022, decreasing to only five studies in 2023. (Figure 3). This shows an increasing trend in publications; however, there may be an underestimation of current studies due to the delay between data collection and study publication. Most studies (n=19) focused on malaria (two or more species), followed by NTDs/VPDs/Other (n=14), and malaria plus combination of NTDs/VPDs/Other (n=7). Seven studies focused on VPDs (two or more pathogens).
Pathogens and antigens examined: A full list of pathogens examined, and the antigens used in each study can be found in Supplementary Material 2 and 3. Overall, the most studied pathogens were Plasmodium falciparum (n=26), followed by Plasmodium vivax (n=19) and Plasmodium malariae (n=15). Regarding NTDs, the most studied were Wuchereria bancrofti (n=9), Brugia malayi (n=9), Strongyloides stercoralis (n=7), and Chlamydia trachomatis (n=6). Cryptosporidium parvum (n=7), enterotoxigenic Escherichia coli (n=5), Entamoeba histolytica (n=5) and Toxoplasma gondii (n=5) were the most studied within the ‘other’ category.
Sampling methods: One study included females of child-bearing age only, while all other studies included both genders. Approximately one third of studies targeted only children under 18 years (n=15; 31%). One study did not define the target population of the samples used within the study. Further details regarding sampling methods and the rationale behind this are detailed in Table 2. For 16 studies, the target pathogen for the primary study was the same as the pathogen(s) examined using MBA; however, this was mostly utilised by studies examining malaria (n=13) [16,19,20,31,32,34,36,37,39,40,44,49,56], LF [22,60], and VPDs [17].
How samples were collected: Only seven studies (15%) were undertaken where integrated surveillance was the primary objective of the study, rather than a secondary analysis of data from another study (Table 2). Most studies were performed using samples collected from a previously published study (n=25; 54%). Many studies were also performed using samples collected from public health surveys for lymphatic filariasis (LF) (n=3), malaria (n=4), HIV/AIDS (n=2), trachoma (n=1), onchocerciasis (n=1), or undertaken in conjunction with an emergency nutrition assessment survey (n=3). Regarding the study setting, most were household-based recruitment (n=23), followed by clinic-based (n=8), and school-based recruitment (n=6).
Determining cut-offs for seropositivity and MBA antigens used: Multiple methods were used to determine seropositivity (Supplementary Material 4). The most common method was the presumed unexposed method (n=28), followed by mixture models (n=13), received operating curve (ROC) (n=10), and standard units (n=8). Under the presumed unexposed method, seropositivity cut-off values are generally calculated based on median fluorescence intensity (MFI) levels measured from non-endemic regions of the pathogen of interest [61], whereas mixture models are a form of probabilistic statistical modelling that assume the presence of two or more distinct groups, generally seronegative and seropositive within the sample population [61].
Laboratories where MBA occurred: Most samples were analysed at the US Centers for Disease Prevention and Control (CDC) (n=29) (Table 2). Other laboratories included the Kenya Medical Research Institute in Nairobi [29,47], the CDC in Nigeria [30], the University of Philippines [39], the University of São Paulo, Brazil [44], the National Laboratory of Haiti [56], Institut Pasteur in France [58], the Scientific Institute of Belgium [17,21], the London School of Hygiene and Tropical Medicine [19,20] and the University of Oxford in the UK [41].

Table 2.
Summary of studies included.
| ID | WHO Region (Countries) | Operational details of sample collection with sampling method/s (references) – Data source | Location of lab analysis (Sample type) |
| Malaria (two or more species) | |||
| 4 | Africa (Ethiopia) | Malaria Indicator Survey (2015) – A nationally representative cross-sectional survey using a two-stage cluster approach for selection of enumeration areas and random sampling for household selection targeting individuals of all ages. [62] | CDC, USA (DBS) |
| 7 | Western Pacific (Lao) | Cross-sectional household (conducted in 2016) survey targeting four districts Northern Lao with known malaria hotspots. A stratified two-stage cluster sampling design chose 25 survey clusters based on proportional-to-population size then households were selected randomly. People aged over 18 months within each household were invited to participate. [63] | LSHTM, UK (DBS) |
| 8 | Western Pacific (Malaysian Borneo) | Environmentally stratified, population based cross-sectional study (conducted in 2015) aimed to understand the transmission of malaria in people aged over 3 years, in northern Sabah as part of the MONKEYBAR project. A non-self-weighting two-stage sampling design whereby villages were selected based on proportion of forest cover and 20 households with each village were randomly selected. [64] | LSHTM, UK (Both) |
| 15 | Africa (Ethiopia) | Convenience sampling of individuals (5+ years) within a community-based onchocerciasis survey in three villages (Arengama 1, Arangama 2 and Konche) of southwest Addis Ababa. Participants were selected through convenience sampling in 2016. | CDC, USA (DBS) |
| 18 | Africa (Nigeria) | Nigeria HIV/AIDS Indicator and Impact Survey (NAIIS) - Conducted in 2018, this was a nationally representative cross-sectional survey using a two-stage cluster approach for selection of enumeration areas and random sampling for household selection targeting individuals of all ages. [65] | CDC, Nigeria (DBS) |
| 19 | Africa (Ethiopia) | Primary study: Cross-sectional serosurvey conducted in 2018 in two areas of southwestern Ethiopia (Arjo-Didessa and Gambella) with contrasting malaria transmission intensities. Using household clustering, individuals aged over 15 years were invited to participate. | Not reported (DBS) |
| 20 | Africa (Republic of Djibouti) | Primary study: Cross-sectional household-based serosurvey conducted in 2002 investigating the prevalence of malaria infections in adults aged 15-54 years in the Republic of Djibouti. Cluster sampling was used to select households whereby anonymized samples were collected from adults aged 15 - 54 years. | Not reported (Serum) |
| 22 | Africa (Cote d’Ivoire) | In 2010, 2012 and 2013, patients presenting to Abobo healthcare facility with symptomatic malaria were invited to join the study. In 2011, due to the Civil War, young asymptomatic school children (6 - 15 years) were recruited in a transversal survey (n=207) in addition to 175 symptomatic patients presenting to healthcare. [66] | Not reported (Serum) |
| 24 | Americas (Suriname) | Primary study: A cross-sectional study of adults (>18 years) conducted in three regions of Suriname (Stoelmanseiland and surroundings (Gakaba, Apoema and Jamaica), Benzdorp) between 2017 – 2018. Stoelmanseiland: All villagers who could be reached within a 4-day enrolment period. Benzdorp: Participants were recruited during active case detection conducted by the National Malaria Programme. | CDC, USA (DBS) |
| 25 | Africa (Ethiopia) | Malaria Indicator Survey (2015) – A nationally representative cross-sectional survey using a two-stage cluster approach for selection of enumeration areas and random sampling for household selection targeting individuals of all ages. [62] | CDC, USA (DBS) |
| 26 | South-East Asia (Bangladesh) | Conducted in 2018, this vaccine coverage and vaccine serosurvey was conducted in two areas of Cox’s Bazar, Bangladesh (Nayapara and makeshift settlement camps (MSs)) alongside an Emergency Nutrition Assessment that was concurrently conducted by the Nutrition Sector (led by Action Against Hunger). This assessment uses the Standardized Monitoring and Assessment for Relief and Transitions (SMART) Methodology. In Nayapara, households were selected using simple random sampling whereby in MSs, a cluster sampling design was used.[67] | CDC, USA (DBS) |
| 27 | Western Pacific (Philippines) | A rolling cross-sectional survey was conducted in three municipalities in three provinces in the Philippines. Sites were selected based on the 2014 Philippines’ National Malaria Program operational definition of malaria-endemic provinces (high endemicity - Rizal, Palawan; sporadic local cases - Abra de Ilog, Occidental Mindoro; malaria-free Morong, Bataan). Participants were recruited from health-care facilities between 2016 – 2018. [68] | University of Philippines(DBS) |
| 28 | Africa (Ethiopia and Costa Rica) | Ethiopia: Ethiopia Malaria Indicator Survey 2015 [62] Costa Rica: A household based serosurvey conducted 2015 in the Costa Rican canton of Matina (2015). This location was selected as one of the last locations in the country where malaria cases were present. Ethiopia (n= 7,077) was selected as the country is co-endemic for both P. falciparum and P. vivax, and Costa Rica (n=851) was selected as a representative low, mono-species Plasmodium endemic region. | CDC – USA (DBS) |
| 32 | Americas (Brazil) | Biorepository at the Institute of Biomedical Sciences of the University of São Paulo containing samples from three studies: Curado, et al. (1997): Cross-sectional household-based study of adults (15+ years) in an area 5-10km of a malaria case in two areas in Brazil with few sporadic cases of malaria between 1992-1994. Silva-Nunes, et al. (2006): Cross-sectional study describing baseline malaria and arbovirus prevalence in rural Amazonia in 2004. All households within the study area were invited to participate. Medeiros, et al. (2013): Cross-sectional study examining symptomatic and asymptomatic malaria cases in four localities on the riverbanks of the Madeira River. People aged over 1 year were eligible to participate. [69,70,71] | University of São Paulo, Brazil (Both) |
| 36 | Americas (Haiti) | Transmission assessment survey (TAS) for LF: Conducted yearly between 2014 – 2016, implementation units are chosen if they have completed at least five rounds of annual MDA with a coverage rate ≥ 65% of the entire population of the implementation unit. The target population for TAS are children aged 6 – 7 years and can be conducted as a school-based or community-based design. [72,73] | CDC, USA (DBS) |
| 37 | Africa (Senegal) | Yearly cross-sectional sampling (between 2002-2013) of febrile individuals (all ages) presenting to free medical clinics in two rural villages (Dielmo and Ndiop) in Senegal. [74,75] | Not reported (Serum) |
| 41 | Africa (Mali) | The primary study was a matched-control trial to assess the effectiveness of a school-based WASH program (2014) in southern Mali. Serology samples were collected from school children (4 - 17 years) as part of a cross-sectional study nestled within the longitudinal impact evaluation (NCT01787058). [76] | CDC, USA (DBS) |
| 42 | Americas (Haiti) | A 2017 serosurvey (ages >6 years) for malaria conducted in Haiti. Sampling method not defined. | CDC, USA (Both) |
| 44 | Americas (Haiti) | Based in Grand’Anse, in the southwest of Haiti, a prospective healthcare facility-based case-control study was conducted in 2018. Cases (>6 months) were defined as a febrile individual with positive RDT results for malaria. Controls were RDT negative individuals matched via age and gender. Follow up was conducted as a household visit to collect further information. [77] | National Laboratory, Port-au-Prince (DBS) |
| VPDs (two or more pathogens) | |||
| 5 | Europe (Belgium) | Primary study: A cross-sectional study examining vaccination and immunity to vaccine preventable diseases in adult (>18 years) at-risk patients (current diagnosis of diabetes mellitus, heart failure, chronic pulmonary obstructive disease, chronic kidney disease, HIV or solid organ transplant) attending outpatient clinics at the University Hospitals of Leuven. Active recruitment to the study was conducted between 2014 and 2016. | Scientific Institute, Belgium (Not stated) |
| 6 | Western Pacific (Solomon Islands) | Primary study: Conducted in 2016, a national cross-sectional school-based survey cluster survey of children (6 - 7 years) in the Solomon Islands. Schools (n=80) were systematically chosen proportional to estimated population size and all children eligible were invited to participate. | CDC, USA (DBS) |
| 9 | Europe (Belgium) | Randomly selected left-over serum samples (n=670) collected in 2012 by six laboratories in three regions of Belgium (Flanders, Wallonia and Brussels Capital Region). Samples collected were originally tested (n=1500) for pertussis prior to use within this study. All samples were collected from “healthy” asymptomatic (for pertussis) adults aged 20 – 30 years. [78] | Scientific Institute, Belgium (Serum) |
| 14 | South-East Asia (Bangladesh) | Emergency Nutrition Assessment (2018) - This survey used data and samples from the study described by Lu, et al. (2020). In brief, a survey was conducted in two areas of Cox’s Bazar, Bangladesh (Nayapara and makeshift settlement camps (MSs)) alongside an Emergency Nutrition Assessment. In Nayapara, households were selected using simple random sampling whereby in MSs, a cluster sampling design was used. [67] | CDC, USA (DBS) |
| 21 | Europe (Ukraine) | Conducted in 2017, this cross-sectional serosurvey aimed to investigate immunity to polioviruses following an outbreak of cVDPV1. This survey targeted four areas (Zakarpattya province in the west, Sumy province in the east, Odessa province in the south, and the capital, Kyiv City) with problems related to cVDPVs and/or challenges with routine immunizations. Children (2 - 10 years) were chosen using one-stage cluster sampling in the three provinces and stratified simple random sampling based on registration with healthcare facilities. [79,80,81] | CDC, USA (Serum) |
| 31 | Americas (Haiti) | Nationally representative household-based survey (conducted in 2017) designed to estimate chronic hepatitis B virus infection and immunity to diphtheria, tetanus, measles, and rubella in children aged 5-7 years. Sampling was done by a two-stage cluster sampling method whereby enumeration areas were selected proportional to size and household were selected at random. [82] | CDC, USA (DBS) |
| 42 | Africa (Nigeria) | 2018 Nigeria HIV/AIDS Indicator and Impact Survey - A nationally representative cross-sectional survey using a two-stage cluster approach for selection of enumeration areas and random sampling for household selection targeting individuals of all ages. [65] | Not reported (DBS) |
| Combination of NTDs/VPDs/Other | |||
| 1 | Africa (Ethiopia) | A cluster-randomized trial (conducted in 2015) designed to determine the effectiveness of a comprehensive WASH package for ocular C. trachomatis infection (NEI U10 EY016214) in children (0 - 9 years) in three districts of the Wag Hemra zone of Amhara, Ethiopia. Prior to this trial, door-to-door census was performed to collect demographic information and from this, a random sample of 60 children in each cluster were chosen for inclusion. [83] | CDC, USA (DBS) |
| 2 | Africa (Haiti, Tanzania, and Kenya) | Samples from previous studies (1990 – 1999; 2012 – 2015) Haiti: Household-based cohort study examining LF prevalence in young children (0-4 years) at 6 - 9 monthly intervals in the coastal town of Leogane, Haiti between 1990-1999. Households were selected based on the high prevalence of LF in previous surveys (1990 and 1991). Kenya: A household-based randomized-controlled intervention trial to assess the impact of ceramic water filters on prevention of diarrhea and cryptosporidiosis in young children (4 - 10 months) in the Siaya county of western Kenya. The sampling frame was provided by the health and demographic surveillance system for the region with random sampling of households. Tanzania: House-hold-based, randomized control trial of children (1 - 9 years) examining the effects of annual azithromycin distribution on trachoma infection in 96 independent clusters from the Kongwa district of Tanzania. Clusters were chosen if not previously treated followed by random selection of households. [84,85,86] | CDC, USA (DBS) |
| 10 | Western Pacific (American Samoa) | Transmission assessment survey (TAS) for LF: Data were obtained from three TASs conducted across elementary schools (children aged 6 - 7 years) in American Samoa (all schools on the main island of Tutuila and the adjacent island of Aunu’u) in 2011, 2015, and 2016. Surveys were carried out at 25, 30, and 29 schools for each survey year, respectively. [72] | CDC, USA (DBS) |
| 11 | Western Pacific (Malaysia) | Environmentally stratified, population based cross-sectional study (2015) aimed to understand the transmission of malaria in people aged over 3 years, in northern Sabah as part of the MONKEYBAR project. A non-self-weighting two-stage sampling design whereby villages were selected based on proportion of forest cover and 20 household within each village were randomly selected. [64] | CDC, USA (DBS) |
| 13 | South-East Asia (Bangladesh) | Emergency Nutrition Assessment (2018) - This survey used data and samples from the study described by Lu, et al. (2020). In brief, a survey was conducted in two areas of Cox’s Bazar, Bangladesh (Nayapara and makeshift settlement camps (MSs)) alongside an Emergency Nutrition Assessment. In Nayapara, households were selected using simple random sampling whereby in MSs, a cluster sampling design was used. [67] | CDC, USA (DBS) |
| 16 | Africa (Ghana) | Trachoma pre-validation: A population-based survey conducted in the Northern, Northeast, Savanna and Upper West regions of Ghana between 2015 - 2016 using a two-stage cluster-sampled approach. This survey targeted children (1 - 9 years) as this age group have the highest risk of active trachoma. Villages were chosen proportional to population size and households were selected using compact segment sampling. [87,88] | CDC, USA (DBS) |
| 17 | Africa (Kenya) | Primary study: Random selection (based on site, sex, and age group) of participants (all ages) based off the Health and Demographic Surveillance System database of two Kenyan towns, Kwale and Mbita. Prior to recruitment, individuals were visited at their household and invited to participate by attending a blood sampling location the following day. This was conducted in 2011. | Nairobi laboratory, Kenya (Serum) |
| 23 | Africa (Tanzania) | Sample were leftover serum samples from the Mother-Offspring Malaria Study Project, a large cohort study conducted from 2002 - 2006 in Muheza, northeastern Tanzania, an area of intense malaria transmission. Pregnant mothers (18 - 45 years) were recruited prior to giving birth at the Muheza Designated District Hospital. Infants were seen at birth and at 2-week intervals for full clinical examination and blood sampling for the first year of life. [89] | Not reported (Serum) |
| 29 | Europe (United Kingdom) | The UK Biobank is a large prospective study with over 500,000 participants aged 40 – 69 years, recruited between 2006–2010. Participants were recruited from 22 assessment centers throughout the UK, covering a variety of different settings to provide socioeconomic and ethnic heterogeneity and urban–rural mix. [90] | Oxford University, UK (Serum) |
| 30 | Americas (Alaska) | A cross-sectional survey investigating exposure to highly pathogenic avian influenza virus H5N1 in individuals and their families (>5 years) in Anchorage and western Alaska between 2007 – 2008. Target participants were grouped into four groups that had regular contact with wild birds: (i) rural subsistence bird hunters and (ii) their family members, (iii) urban sport hunters, and (iv) wildlife biologists. [91] | CDC, USA (Serum) |
| 33 | Americas (Alaska) | A cross-sectional survey investigating exposure to highly pathogenic avian influenza virus H5N1 in individuals and their families (>5 years) in Anchorage and western Alaska between 2007 – 2008. Target participants were grouped into four groups that had regular contact with wild birds: (i) rural subsistence bird hunters and (ii) their family members, (iii) urban sport hunters, and (iv) wildlife biologists. [91] | CDC, USA (Serum) |
| 45 | Western Pacific (American Samoa) | Transmission assessment survey (TAS) for LF: Data were obtained from 3 TASs conducted across elementary schools (children aged 6 - 7 years) in American Samoa (all schools on the main island of Tutuila and the adjacent island of Aunu’u) in 2011 and 2015. Target sample sizes in 2011 and 2015 were 1,042 and 1,014, respectively. [72] | CDC, USA (Serum) |
| 46 | Europe (France) | A mix of samples from routine hospital medical care (94.4%) of individuals of all ages (0 - 100 years) or samples collected in the INCOVPED (NCT04336761) study; an observational study examining COVID-19 prevalence in children presenting to emergency departments in north-eastern France. (COVID-19 and seasonal HCoV). Samples collected between 2002 – 2020. | Institut Pasteur, France (Serum) |
| 47 | Africa (Rwanda) | A nested village-level study (10 households with at least one child under 4 years) within a cluster-randomized trial. The larger cluster-randomized trial consisted of 96 sectors (each with approximately 40 villages) in western region of Rwanda whereby 72 sectors received the intervention (improved cookstoves and household water filters) and 24 sectors acted as controls. Selection for inclusion within the nested-study was determined using a stratified, two-stage design - purposive sampling of study areas then random sampling of households. Conducted between 2014 and 2016. [92] | CDC, USA (DBS) |
| Malaria plus combination of NTDs/VPDs/Other | |||
| 3 | Africa (Niger, Malawi, and Tanzania) | Pre-specified, secondary analysis of the MORDOR Niger trial (CT02048007) where 30 rural communities were randomized 1:1 to biannual mass azithromycin distribution or placebo offered to all children 1 - 59 months (0 - 4 years). Communities were chosen for the trial if the population was between 200 and 2000 inhabitants. A sub-study examining morbidity randomly selected 30 communities from the trial and all households in each community were visited and invited to participate in this component. From this, 50 children within each community were asked to provide samples. This study was conducted between 2014 and 2020. [93,94] | CDC, USA (DBS) |
| 12 | Americas (Haiti) | Under the Global Fund grant against malaria, enumeration areas (117 communities) throughout Haiti were selected based on high risk of malaria. Households (20 per enumeration area) were chosen at random, and people of all ages were invited to participate. This study was conducted between 2014 and 2015. | CDC, USA (DBS |
| 34 | Americas (Haiti) | A randomized, placebo-controlled trial conducted between 1998 and 1999 investigating the tolerance, efficacy, and nutritional benefit of combining chemotherapeutic treatment of intestinal helminths and lymphatic filariasis in the coastal town of Leogane, Haiti. Twelve selected primary schools were chosen, and all children aged 5 - 11 years were eligible to participate. Allocation to treatment groups was randomized. [95] | CDC, USA (Serum) |
| 35 | Africa (Kenya) | Cross-sectional study conducted in Eastern and Southern Africa Centre of International Parasitic Control (ESACIPAC), to provide a comprehensive epidemiological assessment of LF infection in people aged over 2 years (as recommended by WHO LF guidelines) before restarting MDA. 10 sentinel sites in costal Kenya were selected and from this, five were selected based on LF risk. Household sampling was conducted door-to-door to achieve a sample size of 300 per sentinel site. This study was conducted in 2015. [72,96] | Nairobi, Kenya (DBS) |
| 38 | Africa (Mozambique) | Primary study: Two consecutive cross-sectional household surveys before and after the LLIN campaign in six rural districts of the northern province of Nampula. From each district, 20 survey clusters were chosen randomly, with random selection of households within each cluster. Individuals of all ages were invited to participate. This study was conducted in 2013 and 2014. | CDC, USA (DBS) |
| 39 | Americas (Haiti) | Household-based longitudinal cohort study (n=61) based on the coastal town of Ca Ira examining the effect of DEC fortified salt on transmission of LF in children (2-10 years) at time points of 2011, 2013, and 2014. Additional samples (n=127) were collected from the above cohort in 2014 as well as samples from additional children (2 - 10 years) in Ca Ira that had not been previously sampled. This study was conducted in 2011, 2013 and 2014. | CDC, USA (DBS) |
| 40 | Western Pacific (Cambodia) | Nationally representative survey (conducted in 2012) designed to estimate serological evidence to vaccine preventable diseases in women of childbearing age (15 - 39 years). Based on the 2009 Cambodian neonatal tetanus risk assessment, multi-stage cluster sampling was performed with oversampling of areas with higher risk of tetanus. [97,98] | CDC, USA (Serum) |
Acronyms: CDC, USA – Centers for Disease Prevention and Control, United States of America. WHO – World Health Organization. DBS – Dried blood spot. LF – Lymphatic filariasis. DEC – Diethylcarbamazine. MDA – Mass drug administration. TAS – Transmission assessment survey. UK – United Kingdom. SMART Methodology - Standardized Monitoring and Assessment for Relief and Transitions Methodology. MSC – Makeshift settlement camps. HCoV – Human coronaviruses. RDT – Rapid diagnostic test.
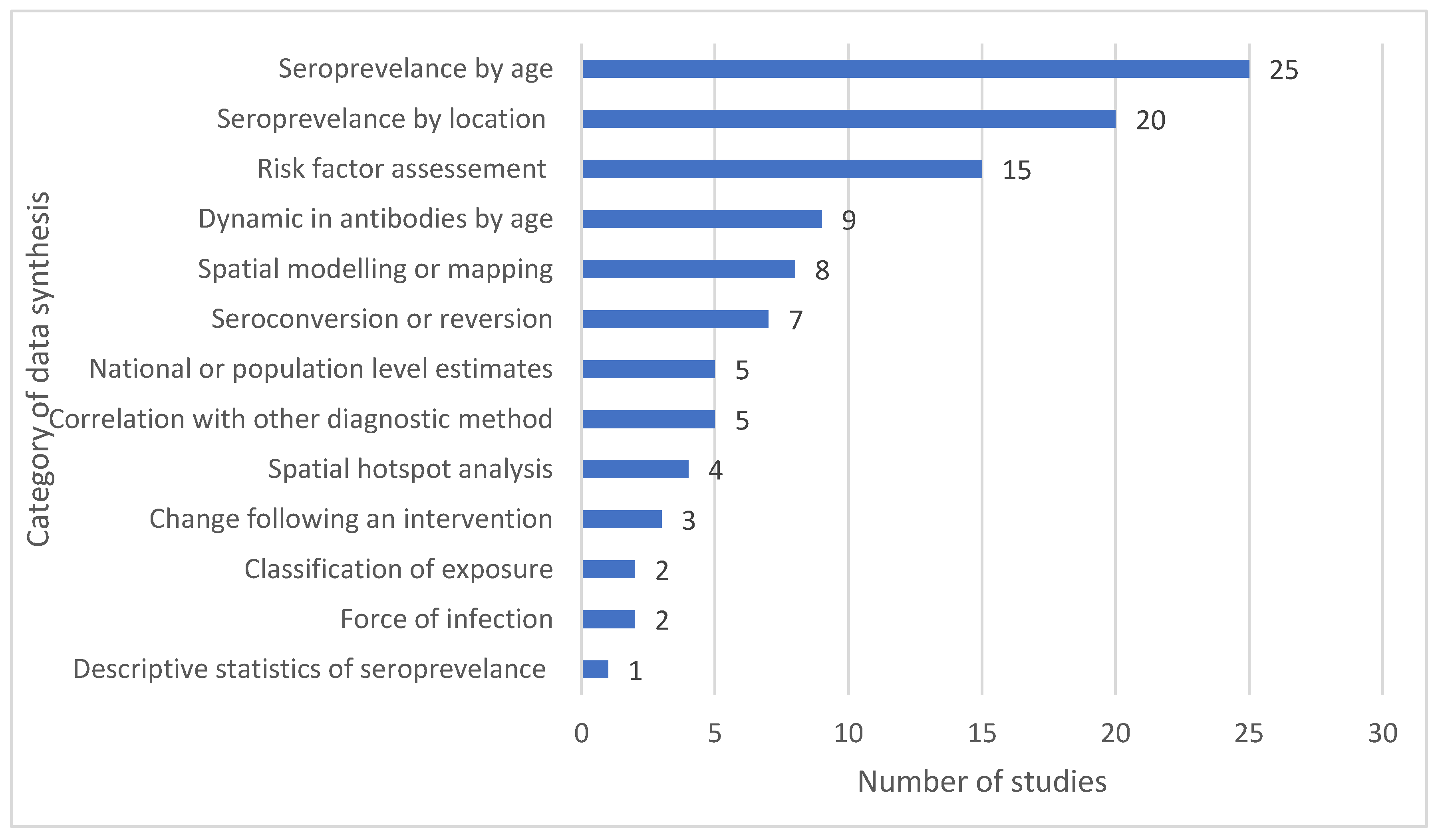
Synthesis of data: Several methods of data synthesis were performed, including age-specific seroprevalence (n=17) or risk factor analysis (n=10). Seven studies estimated seroprevalence by geographic region, two studies provided maps of seroprevalence, and nine studies used spatial analysis methods, of which one was for identification of hotspots. Four studies were used to assess the impact of an intervention. Five studies described correlation of antibody seropositivity with another diagnostic method (polymerase chain reaction (PCR), parasitemia, and vaccine history). Figure 3 summarizes the number of studies using the different types of data synthesis methods and further information on this can be found in Supplementary Material 5.
Prevalence findings: Most studies reported seroprevalence by antigen (Supplementary Material 4). Some studies focused on high prevalence of disease, often in known endemic areas, the most common example being malaria [31,36,46,99,100], while other studies focused on low prevalence of diseases that have been targeted for elimination, such as yaws or trachoma [25,28]. An example of this is the low serological prevalence of yaws among refugee populations in Cox Bazar, where seropositivity to both Rp17 and TmpA antigens were found to be 0% (95% CI: 0 - 1.7) in Nayapara and 0% (95% CI: 0 - 1.1) in makeshift settlements [25].
Potential public implications: Two studies used the data generated to provide national level estimates of disease seroprevalence, while two other studies used the data to provide vaccination coverage estimates. Most study findings have public health implications regarding age-specific immunity or seroprevalence of pathogen (n=27), location-specific immunity or disease prevalence (n=26), or data regarding risk factor analysis (n=16) (Figure 4). Among studies evaluating public health interventions or programs (n=5), two focused on the efficacy of WASH programs, two on the effectiveness of water filters, and one on the impact of long-lasting insecticide-treated bed nets.
Figure 3.
Categories of data synthesis of included studies. Some studies belong to more than one category; thus, the total exceeds the number of included studies.
Figure 3.
Categories of data synthesis of included studies. Some studies belong to more than one category; thus, the total exceeds the number of included studies.
Discussion
In this review we have shown that to date, MBA has mostly been used for integrated serosurveillance of malaria (55%) with less emphasis on other infectious pathogens. Most studies used data from existing or previously published studies as opposed to being conducted as standalone integrated serological surveys. Data synthesis ranged from estimating age-specific seroprevalence and risk factor analysis to spatial analysis and/or hotspot identification. Given the growing utilisation of MBA for serosurveillance, further research is needed to optimise operational components and laboratory analysis. Additionally, expanding the network of laboratories capable of conducting MBA is crucial, as most studies to date have relied on laboratory analysis conducted at the US CDC. Further a deeper understanding of geographical variation in prevalence and associated contextually relevant risk factors for infection can help inform populations that may be eligible for future vaccination and targeted public health interventions, highlighting the importance of integrated serological surveillance as a public health tool and early warning system to aid decision making.
This review found a plethora of antigens used to examine seroprevalence to malaria that target different species (e.g. species specific MSP1-19), and different life stages of the parasite (e.g. AMA targeting the schizont stage, or CSP targeting the sporozoites stage). This may potentially be due to the greater morbidity and mortality burden associated with malaria and the large funding support for malaria research compared to other infectious pathogens [101,102,103]. In 2019 alone, there were an estimated 608,000 deaths caused by malaria globally [104], compared to 36,055 deaths from dengue [105], and 35,000 from tetanus [106]. This relates back to the basics of disease surveillance, as stated by Foege, Hogan, and Newton in 1976, “the reason for collecting, analysing, and disseminating information on a disease is to control that disease” [107]. To extrapolate, infectious pathogens that are harder to control, such as dengue [108], may be less prioritised than other infectious pathogens that have the potential to be controlled through readily expendable public health programs such as chemoprophylaxis and bed-net distribution programs.
For the study of VPDs (15%), the most common form of data synthesis was estimation of seroprevalence by age and region. This is an informative way of conveying immunisation coverage and herd immunity to relevant stakeholders. The use of serology for monitoring population dynamics has been shown to provide information regarding age and population-group specific waning of immunity [4,109], which is especially important when considering the impact of waning immunity on the risk of future outbreaks. Furthermore, many studies have shown that serological surveillance for vaccine coverage provides higher accuracy than historical records [110], especially in low- and middle-income countries (LMICs) [111] where data may be limited, incomplete or hard to access. Information regarding population-level serological immunity is useful, in combination with further vaccination research, for influencing and changing vaccination schedules or promoting vaccination top-up campaigns to areas where this is most needed. Another example of this may include providing targeted education to health care workers regarding risk factors associated with infection, thereby facilitating easier and earlier diagnosis [112].
The WHO Toolkit for Integrated Serosurveillance of Communicable Diseases in the Americas [113] has emphasized the importance of integrated serological surveillance; however, in our review only seven studies (15%) were conducted in which integrated serosurveillance was the primary objective, rather than a secondary analysis of samples collected from another study. Most of the studies examined in this review utilised samples collected from previous studies or public health interventions. While not explicit, this has the potential to introduce sampling bias, for example, if assessing a public health intervention that was targeted to higher risk individuals for the disease(s) of focus. Comparatively, when using a single disease focus, there is much greater risk of introducing bias through targeted sampling methods that may potentially lead to overestimation of true disease prevalence [113]. A recent systematic review examining bias in population-level measles serosurveys found that the majority of studies introduced moderate level sampling bias by utilising a restricted, non-representative sample, such as convenience sampling [114]. While this may not be the case for studies included in this review, it does bring about important considerations when using samples from previously published studies or samples utilised from an established repository or biobank to make more generalized population level inferences. Nonetheless, the advantages of incorporating serological-based surveillance into pre-established surveys, such as health and demographic surveys, likely outweigh the disadvantages that may be introduced through bias.
Another important operational consideration is the physical method of sample collection. Obtaining venous blood samples requires training in phlebotomy, often by nurses, doctors, or laboratory technicians, that may be limited in rural and remote settings or in LMICs. In contrast, many of the samples examined within this review were dried blood spots (DBS) prepared using samples collected by fingerpick blood collection that can be collected by a person without formal training. For MBAs, the performance of DBS have been compared with serum samples, and showed comparable high sensitivity and specificity [115]. For example, a study comparing DBS to serum samples for SARS-CoV-2 testing using MBA found a specificity of 99.5% for both the N and S1 antigen [116]. In the same study, specificity ranged from 83% for samples collected 0-20 days post-symptomatic infection onset to 95% for samples collected 61-90 days post-infection onset [116]. Another example of this pertains to a study examining the use of MBA testing precision between DBS and serum samples for HIV-1 which found that DBS antibody correlation ranged from 0.87 to 0.98 and serum samples raged between 0.90 to 0.97 [117]. In addition to ease of collection and performance of specimens, when kept under ideal conditions between -20ºC and -80ºC, DBS have the potential to remain viable for up to 20 years [118], making integrated serosurveillance a feasible and attractive option.
It is important that national capacity is improved to enable sample analysis at a regional or country level to avoid bottlenecks in data analysis and results dissemination. While most studies utilised laboratory facilities at the US CDC, it is encouraging that some studies undertook sample analysis at in-country laboratories. Of note are those located in lower-middle-income countries such as the CDC in Nigeria [30], Nairobi University in Kenya [47], and the University of Philippines [39]. This aligns well with the WHO toolkit for integrated serological surveillance [113], and the 2030 NTD elimination framework [119,120,121] which, as outlined in the Ending the neglect to attain the Sustainable Development Goals: A road map for neglected tropical diseases 2021–2030, aims for 90% of endemic countries to utilie an integrated approach for NTD surveillance and integrated control by the year 2030 [121]. For this to be achieved, high levels of cross-collaboration and donor support are required to facilitate upskilling and capacity building of local researchers and clinicians. However, moving forward, it would be beneficial to increase capacity for laboratory analysis to be undertaken in more locations, within or closer to the countries in which the studies are being conducted. Furthermore, the median time between sample collection and publication was four years. By increasing the regional and national capacity for sample collection and analysis, this could decrease the time taken for findings to be implemented by public health authorities and for results to be shared. This is particularly important for infectious diseases near elimination or outbreak-prone diseases that require a timely response.
This systematic review has several limitations. Firstly, to expand the scope of this search, we included studies that examined different species of a single pathogen, whereas integrated surveillance is often considered as the concurrent surveillance of many different pathogens. However, this review has demonstrated that as time progresses, the number and range of pathogens studied has steadily increased. This also highlights the potential publication bias as the large range in time between sample collection and study publication may have impacted the number of studies retrieved within this review. Furthermore, another limitation of this study is the inconsistent reporting of sample collection within each study. While many clearly detailed the process by which samples were collected, others referred to previously published studies.
Conclusions
In conclusion, this review has shown that MBA usage for integrated surveillance of pathogens is gaining traction. Given the growing utilisation of MBA for serosurveillance, further research is needed to optimise operational components and laboratory analysis. Additionally, expanding the network of laboratories capable of conducting MBA is crucial, as most studies to date have relied on laboratory analysis conducted at the US CDC. Furthermore, a deeper understanding of geographical variation in prevalence and associated contextually relevant risk factors for infection can help inform populations that may be eligible for future vaccination and targeted public health interventions, highlighting the importance of integrated serological surveillance as a public health tool and early warning system to aid decision making. Lastly, it is important to note that integrated serological surveillance can be used as a complementary method for epidemiological monitoring and cannot replace other methods such as active or passive case detection.
Author Contributions
Conceptualisation: SW, HL, BS, CL. Methodology: SW, HL, BS, CL. Article screening: SW, HL. Data extraction: SW, HL. Writing – original draft preparation: SW. Writing – review and editing: SW, HL, BS, CL. All authors have read and agreed to the published version of the manuscript.
Funding
SW is supported by a Research Training Program (RTP) stipend through the University of Queensland. CLL was supported by an Australian National Health and Medical Research Council Fellowship (Grant number 1193826). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflicts of interest
The authors have no conflicts of interest to declare.
References
- Arnold, B.F., et al., Measuring changes in transmission of neglected tropical diseases, malaria, and enteric pathogens from quantitative antibody levels. PLoS Neglected Tropical Diseases, 2017. 11(5). [CrossRef]
- Haselbeck, A.H., et al., Serology as a Tool to Assess Infectious Disease Landscapes and Guide Public Health Policy. Pathogens, 2022. 11(7). [CrossRef]
- Hatherell, H.-A., et al., Sustainable surveillance of neglected tropical diseases for the post-elimination era. Clinical Infectious Diseases, 2021. 72(Supplement_3): p. S210-S216. [CrossRef]
- Arnold, B.F., H.M. Scobie, J.W. Priest, and P.J. Lammie, Integrated serologic surveillance of population immunity and disease transmission. Emerging Infectious Diseases, 2018. 24(7): p. 1188-1194. [CrossRef]
- Elshal, M.F. and J.P. McCoy, Multiplex bead array assays: performance evaluation and comparison of sensitivity to ELISA. Methods, 2006. 38(4): p. 317-323. [CrossRef]
- Chan, Y.Y., et al., Determining seropositivity-a review of approaches to define seroprevalence when using multiplex bead assays to assess burden of tropical diseases. American Journal of Tropical Medicine and Hygiene, 2020. 103(5 SUPPL): p. 123-124. [CrossRef]
- Ahsan, H., Monoplex and multiplex immunoassays: approval, advancements, and alternatives. Comparative clinical pathology, 2022. 31(2): p. 333-345. [CrossRef]
- Benedicto-Matambo, P., et al. Exploring natural immune responses to Shigella exposure using multiplex bead assays on dried blood spots in high-burden countries: protocol from a multisite diarrhea surveillance study. in Open Forum Infectious Diseases. 2024. Oxford University Press US. [CrossRef]
- Simonsen, J., et al., Sero-epidemiology as a tool to study the incidence of Salmonella infections in humans. Epidemiology & Infection, 2008. 136(7): p. 895-902. [CrossRef]
- Ward, S., H. Lawford, B. Sartorius, and C. Lau, Integrated serosurveillance of infectious diseases using multiplex bead assays: A systematic review. 2024. [CrossRef]
- Veritas Health Innovation, Covidence systematic review software. 2023: Melbourne, Australia,.
- Page, M.J., et al., The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. International journal of surgery, 2021. 88: p. 105906. [CrossRef]
- Aiemjoy, K., et al., Seroprevalence of antibodies against Chlamydia trachomatis and enteropathogens and distance to the nearest water source among young children in the Amhara Region of Ethiopia. PLoS Negl Trop Dis, 2020. 14(9): p. e0008647. [CrossRef]
- Arnold, B.F., et al., Enteropathogen antibody dynamics and force of infection among children in low-resource settings. eLife, 2019. 8. [CrossRef]
- Arzika, A.M., et al., Effect of biannual azithromycin distribution on antibody responses to malaria, bacterial, and protozoan pathogens in Niger. Nature communications, 2022. 13(1): p. 976. [CrossRef]
- Assefa, A., et al., Multiplex serology demonstrate cumulative prevalence and spatial distribution of malaria in Ethiopia. Malar J, 2019. 18(1): p. 246. [CrossRef]
- Boey, L., et al., Seroprevalence of Antibodies against Diphtheria, Tetanus and Pertussis in Adult At-Risk Patients. Vaccines (Basel), 2021. 9(1). [CrossRef]
- Breakwell, L., et al., Seroprevalence of chronic hepatitis B virus infection and immunity to measles, rubella, tetanus and diphtheria among schoolchildren aged 6-7 years old in the Solomon Islands, 2016. Vaccine, 2020. 38(30): p. 4679-4686. [CrossRef]
- Byrne, I., et al., Characterizing the spatial distribution of multiple malaria diagnostic endpoints in a low-transmission setting in Lao PDR. Front Med (Lausanne), 2022. 9: p. 929366. [CrossRef]
- Byrne, I., et al., Serological evaluation of risk factors for exposure to malaria in a pre-elimination setting in Malaysian Borneo. Sci Rep, 2023. 13(1): p. 12998. [CrossRef]
- Caboré, R.N., D. Piérard, and K. Huygen, A Belgian serosurveillance/seroprevalence study of diphtheria, tetanus and pertussis using a luminex xMAP technology-based pentaplex. Vaccines, 2016. 4(2). [CrossRef]
- Cadavid Restrepo, A.M., et al., Potential use of antibodies to provide an earlier indication of lymphatic filariasis resurgence in post–mass drug ad ministration surveillance in American Samoa. International Journal of Infectious Diseases, 2022. 117: p. 378-386. [CrossRef]
- Chan, Y.L., et al., Assessing seroprevalence and associated risk factors for multiple infectious diseases in Sabah, Malaysia using serological multiplex bead assays. Front Public Health, 2022. 10: p. 924316. [CrossRef]
- Chan, Y., et al., Multiplex Serology for Measurement of IgG Antibodies Against Eleven Infectious Diseases in a National Serosurvey: Haiti 2014-2015. Front Public Health, 2022. 10: p. 897013. [CrossRef]
- Cooley, G.M., et al., No Serological Evidence of Trachoma or Yaws Among Residents of Registered Camps and Makeshift Settlements in Cox's Bazar, Bangladesh. Am J Trop Med Hyg, 2021. 104(6): p. 2031-2037. [CrossRef]
- Feldstein, L.R., et al., Vaccination coverage survey and seroprevalence among forcibly displaced Rohingya children, Cox's Bazar, Bangladesh, 2018: A cross-sectional study. PLoS Med, 2020. 17(3): p. e1003071. [CrossRef]
- Feleke, S.M., et al., Sero-identification of the aetiologies of human malaria exposure (Plasmodium spp.) in the Limu Kossa District of Jimma Zone, South western Ethiopia. Malar J, 2019. 18(1): p. 292. [CrossRef]
- Fornace, K.M., et al., Characterising spatial patterns of neglected tropical disease transmission using integrated sero-surveillance in Northern Ghana. PLoS Neglected Tropical Diseases, 2022. 16(3). [CrossRef]
- Fujii, Y., et al., Serological Surveillance Development for Tropical Infectious Diseases Using Simultaneous Microsphere-Based Multiplex Assays and Finite Mixture Models. PLoS Neglected Tropical Diseases, 2014. 8(7). [CrossRef]
- Herman, C., et al., Non-falciparum malaria infection and IgG seroprevalence among children under 15 years in Nigeria, 2018. Nat Commun, 2023. 14(1): p. 1360. [CrossRef]
- Jeang, B., et al., Serological Markers of Exposure to Plasmodium falciparum and Plasmodium vivax Infection in Southwestern Ethiopia. American Journal of Tropical Medicine and Hygiene, 2023. 108(5): p. 871-881. [CrossRef]
- Khaireh, B.A., et al., Plasmodium vivax and Plasmodium falciparum infections in the Republic of Djibouti: Evaluation of their prevalence and potential determinants. Malaria Journal, 2012. 11. [CrossRef]
- Khetsuriani, N., et al., Diphtheria and tetanus seroepidemiology among children in Ukraine, 2017. Vaccine, 2022. 40(12): p. 1810-1820. [CrossRef]
- Koffi, D., et al., Longitudinal analysis of antibody responses in symptomatic malaria cases do not mirror parasite transmission in peri-urban area of Cote d'Ivoire between 2010 and 2013. PLoS One, 2017. 12(2): p. e0172899. [CrossRef]
- Kwan, J.L., et al., Seroepidemiology of helminths and the association with severe malaria among infants and young children in Tanzania. PLoS Neglected Tropical Diseases, 2018. 12(3). [CrossRef]
- Labadie-Bracho, M.Y., F.T. van Genderen, and M.R. Adhin, Malaria serology data from the Guiana shield: first insight in IgG antibody responses to Plasmodium falciparum, Plasmodium vivax and Plasmodium malariae antigens in Suriname. Malar J, 2020. 19(1): p. 360. [CrossRef]
- Leonard, C.M., et al., Spatial Distribution of Plasmodium falciparum and Plasmodium vivax in Northern Ethiopia by Microscopic, Rapid Diagnostic Test, Laboratory Antibody, and Antigen Data. J Infect Dis, 2022. 225(5): p. 881-890. [CrossRef]
- Lu, A., et al., Screening for malaria antigen and anti-malarial IgG antibody in forcibly-displaced Myanmar nationals: Cox's Bazar district, Bangladesh, 2018. Malar J, 2020. 19(1): p. 130. [CrossRef]
- Macalinao, M.L.M., et al., Analytical approaches for antimalarial antibody responses to confirm historical and recent malaria transmission: an example from the Philippines. The Lancet Regional Health - Western Pacific, 2023. 37. [CrossRef]
- McCaffery, J.N., et al., The use of a chimeric antigen for Plasmodium falciparum and P. vivax seroprevalence estimates from community surveys in Ethiopia and Costa Rica. PLoS ONE, 2022. 17(5 5). [CrossRef]
- Mentzer, A.J., et al., Identification of host–pathogen-disease relationships using a scalable multiplex serology platform in UK Biobank. Nature Communications, 2022. 13(1). [CrossRef]
- Miernyk, K.M., et al., Human Seroprevalence to 11 Zoonotic Pathogens in the U.S. Arctic, Alaska. Vector-Borne and Zoonotic Diseases, 2019. 19(8): p. 563-575. [CrossRef]
- Minta, A.A., et al., Seroprevalence of Measles, Rubella, Tetanus, and Diphtheria Antibodies among Children in Haiti, 2017. Am J Trop Med Hyg, 2020. 103(4): p. 1717-1725. [CrossRef]
- Monteiro, E.F., et al., Antibody Profile Comparison against MSP1 Antigens of Multiple Plasmodium Species in Human Serum Samples from Two Different Brazilian Populations Using a Multiplex Serological Assay. Pathogens, 2021. 10(9). [CrossRef]
- Mosites, E., et al., Giardia and Cryptosporidium antibody prevalence and correlates of exposure among Alaska residents, 2007-2008. Epidemiol Infect, 2018. 146(7): p. 888-894. [CrossRef]
- Moss, D.M., et al., Multiplex bead assay for serum samples from children in Haiti enrolled in a drug study for the treatment of lymphatic filariasis. Am J Trop Med Hyg, 2011. 85(2): p. 229-37. [CrossRef]
- Njenga, S.M., et al., Integrated Cross-Sectional Multiplex Serosurveillance of IgG Antibody Responses to Parasitic Diseases and Vaccines in Coastal Kenya. Am J Trop Med Hyg, 2020. 102(1): p. 164-176. [CrossRef]
- Oviedo, A., et al., Spatial cluster analysis of Plasmodium vivax and P. malariae exposure using serological data among Haitian school children sampled between 2014 and 2016. PLoS Negl Trop Dis, 2022. 16(1): p. e0010049. [CrossRef]
- Perraut, R., et al., Serological signatures of declining exposure following intensification of integrated malaria control in two rural Senegalese communities. PLoS ONE, 2017. 12(6). [CrossRef]
- Plucinski, M.M., et al., Multiplex serology for impact evaluation of bed net distribution on burden of lymphatic filariasis and four species of human malaria in northern Mozambique. PLoS Neglected Tropical Diseases, 2018. 12(2). [CrossRef]
- Poirier, M.J., et al., Measuring Haitian children's exposure to chikungunya, dengue and malaria. Bulletin of the World Health Organization, 2016. 94(11): p. 817-825A. [CrossRef]
- Priest, J.W., et al., Integration of Multiplex Bead Assays for Parasitic Diseases into a National, Population-Based Serosurvey of Women 15-39 Years of Age in Cambodia. PLoS Negl Trop Dis, 2016. 10(5): p. e0004699. [CrossRef]
- Rogier, E., et al., Evaluation of Immunoglobulin G Responses to Plasmodium falciparum and Plasmodium vivax in Malian School Children Using Multiplex Bead Assay. Am J Trop Med Hyg, 2017. 96(2): p. 312-318. [CrossRef]
- Rogier, E., et al., High-throughput malaria serosurveillance using a one-step multiplex bead assay. Malar J, 2019. 18(1): p. 402. [CrossRef]
- Tohme, R.A., et al., Tetanus and Diphtheria Seroprotection among Children Younger Than 15 Years in Nigeria, 2018: Who Are the Unprotected Children? Vaccines (Basel), 2023. 11(3). [CrossRef]
- van den Hoogen, L.L., et al., Rapid Screening for Non-falciparum Malaria in Elimination Settings Using Multiplex Antigen and Antibody Detection: Post Hoc Identification of Plasmodium malariae in an Infant in Haiti. Am J Trop Med Hyg, 2021. 104(6): p. 2139-2145. [CrossRef]
- Won, K.Y., et al., Comparison of antigen and antibody responses in repeat lymphatic filariasis transmission assessment surveys in American Samoa. PLoS Negl Trop Dis, 2018. 12(3): p. e0006347. [CrossRef]
- Woudenberg, T., et al., Humoral immunity to SARS-CoV-2 and seasonal coronaviruses in children and adults in north-eastern France. EBioMedicine, 2021. 70: p. 103495. [CrossRef]
- Zambrano, L.D., et al., Use of serologic responses against enteropathogens to assess the impact of a point-of-use water filter: A randomized controlled trial in western province, Rwanda. American Journal of Tropical Medicine and Hygiene, 2017. 97(3): p. 876-887. [CrossRef]
- Won, K.Y., et al., Use of antibody tools to provide serologic evidence of elimination of lymphatic filariasis in the Gambia. American Journal of Tropical Medicine and Hygiene, 2018. 98(1): p. 15-20. [CrossRef]
- Chan, Y., et al., Determining seropositivity—a review of approaches to define population seroprevalence when using multiplex bead assays to assess burden of tropical diseases. PLoS Neglected Tropical Diseases, 2021. 15(6). [CrossRef]
- Institute, E.P.H., Ethiopia National Malaria Indicator Survey 2015. 2016: Ethiopia.
- Lover, A.A., et al., Prevalence and risk factors for asymptomatic malaria and genotyping of glucose 6-phosphate (G6PD) deficiencies in a vivax-predominant setting, Lao PDR: implications for sub-national elimination goals. Malaria journal, 2018. 17: p. 1-12. [CrossRef]
- Fornace, K.M., et al., Environmental risk factors and exposure to the zoonotic malaria parasite Plasmodium knowlesi across northern Sabah, Malaysia: a population-based cross-sectional survey. The Lancet Planetary Health, 2019. 3(4): p. e179-e186. [CrossRef]
- Health, F.M.o., Nigeria HIV/AIDS Indicator and Impact Survey (NAIIS) 2018: Technical Report. 2019: Abuja, Nigeria.
- Koffi, D., et al., Analysis of antibody profiles in symptomatic malaria in three sentinel sites of Ivory Coast by using multiplex, fluorescent, magnetic, bead-based serological assay (MAGPIX™). Malar J, 2015. 14: p. 509. [CrossRef]
- Group, A.A.H.C.a.t.T.A., Standardized Monitoring and Assessment for Relief and Transitions Methodology Manual 2.0. 2017.
- Reyes, R.A., et al., Enhanced health facility surveys to support malaria control and elimination across different transmission settings in the Philippines. The American journal of tropical medicine and hygiene, 2021. 104(3): p. 968. [CrossRef]
- Curado, I., et al., Antibodies anti bloodstream and circumsporozoite antigens (Plasmodium vivax and Plasmodium malariae/P. brasilianum) in areas of very low malaria endemicity in Brazil. Memórias do Instituto Oswaldo Cruz, 1997. 92: p. 235-243. [CrossRef]
- Silva-Nunes, M.d., et al., The Acre Project: the epidemiology of malaria and arthropod-borne virus infections in a rural Amazonian population. Cadernos de Saude Publica, 2006. 22: p. 1325-1334.
- Medeiros, M.M., et al., Natural antibody response to Plasmodium falciparum merozoite antigens MSP5, MSP9 and EBA175 is associated to clinical protection in the Brazilian Amazon. BMC Infectious Diseases, 2013. 13: p. 1-19. [CrossRef]
- World Health Organization, Monitoring and epidemiological assessment of mass drug administration in the global programme to eliminate lymphatic filariasis: a manual for national elimination programmes. 2011.
- Organization, W.H., Assessing the epidemiology of soil-transmitted helminths during a transmission assessment survey in the global programme for the elimination of lymphatic filariasis. 2015.
- Diene Sarr, F., et al., Acute febrile illness and influenza disease burden in a rural cohort dedicated to malaria in senegal, 2012–2013. PLoS One, 2015. 10(12): p. e0143999. [CrossRef]
- Trape, J.-F., et al., The rise and fall of malaria in a west African rural community, Dielmo, Senegal, from 1990 to 2012: a 22 year longitudinal study. The Lancet infectious diseases, 2014. 14(6): p. 476-488. [CrossRef]
- Trinies, V., J.V. Garn, H.H. Chang, and M.C. Freeman, The impact of a school-based water, sanitation, and hygiene program on absenteeism, diarrhea, and respiratory infection: a matched–control trial in Mali. The American journal of tropical medicine and hygiene, 2016. 94(6): p. 1418. [CrossRef]
- Ashton, R.A., et al., Risk Factors for Malaria Infection and Seropositivity in the Elimination Area of Grand'Anse, Haiti: A Case-Control Study among Febrile Individuals Seeking Treatment at Public Health Facilities. Am J Trop Med Hyg, 2020. 103(2): p. 767-777. [CrossRef]
- Huygen, K., et al., Bordetella pertussis seroprevalence in Belgian adults aged 20–39 years, 2012. Epidemiology & Infection, 2014. 142(4): p. 724-728. [CrossRef]
- Huseynov, S., N. Khetsuriani, N. Chitadze, and L. Slobodianyk, Poliomyelitis, measles, rubella, diphtheria, tetanus, and hepatitis B seroepidemiology among children born in 2006–2015 in four regions on Ukraine, 2017. 2021.
- Khetsuriani, N., et al., Seroprevalence of hepatitis B virus infection markers among children in Ukraine, 2017. Vaccine, 2021. 39(10): p. 1485-1492. [CrossRef]
- Khetsuriani, N., et al., Responding to a cVDPV1 outbreak in Ukraine: Implications, challenges and opportunities. Vaccine, 2017. 35(36): p. 4769-4776. [CrossRef]
- Childs, L., et al., Prevalence of chronic hepatitis B virus infection among children in Haiti, 2017. The American Journal of Tropical Medicine and Hygiene, 2019. 101(1): p. 214. [CrossRef]
- Stoller, N.E., et al., Efficacy of latrine promotion on emergence of infection with ocular Chlamydia trachomatis after mass antibiotic treatment: a cluster-randomized trial. International health, 2011. 3(2): p. 75-84. [CrossRef]
- Lammie, P.J., et al., Longitudinal analysis of the development of filarial infection and antifilarial immunity in a cohort of Haitian children. The American journal of tropical medicine and hygiene, 1998. 59(2): p. 217-221. [CrossRef]
- Morris, J.F., et al., A randomized controlled trial to assess the impact of ceramic water filters on prevention of diarrhea and cryptosporidiosis in infants and young children—western Kenya, 2013. American Journal of Tropical Medicine and Hygiene, 2018. 98(5): p. 1260-1268. [CrossRef]
- Wilson, N., et al., Evaluation of a single dose of azithromycin for trachoma in low-prevalence communities. Ophthalmic epidemiology, 2019. 26(1): p. 1-6. [CrossRef]
- World Health Organization, Validation of elimination of trachoma as a public health problem. 2016.
- Debrah, O., et al., Elimination of trachoma as a public health problem in Ghana: Providing evidence through a pre-validation survey. PLoS neglected tropical diseases, 2017. 11(12): p. e0006099. [CrossRef]
- Mutabingwa, T.K., et al., Maternal malaria and gravidity interact to modify infant susceptibility to malaria. PLoS medicine, 2005. 2(12): p. e407. [CrossRef]
- Sudlow, C., et al., UK biobank: an open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS medicine, 2015. 12(3): p. e1001779. [CrossRef]
- Reed, C., et al., Characterizing wild bird contact and seropositivity to highly pathogenic avian influenza A (H5N1) virus in Alaskan residents. Influenza and Other Respiratory Viruses, 2014. 8(5): p. 516-523. [CrossRef]
- Nagel, C.L., et al., Study design of a cluster-randomized controlled trial to evaluate a large-scale distribution of cook stoves and water filters in Western Province, Rwanda. Contemporary clinical trials communications, 2016. 4: p. 124-135. [CrossRef]
- Oldenburg, C., et al., Annual versus biannual mass azithromycin distribution and serologic markers of trachoma among children in Niger: a community randomized trial. American journal of tropical medicine and hygiene, 2018. 99(4): p. 436.
- Keenan, J.D., et al., Azithromycin to reduce childhood mortality in sub-Saharan Africa. New England Journal of Medicine, 2018. 378(17): p. 1583-1592. [CrossRef]
- Fox, L.M., et al., Tolerance and efficacy of combined diethylcarbamazine and albendazole for treatment of Wuchereria bancrofti and intestinal helminth infections in Haitian children. The American journal of tropical medicine and hygiene, 2005. 73(1): p. 115-121. [CrossRef]
- Njenga, S.M., et al., Assessment of lymphatic filariasis prior to re-starting mass drug administration campaigns in coastal Kenya. Parasites & vectors, 2017. 10: p. 1-9. [CrossRef]
- Scobie, H.M., et al., Tetanus immunity among women aged 15 to 39 years in Cambodia: a national population-based serosurvey, 2012. Clinical and Vaccine Immunology, 2016. 23(7): p. 546-554. [CrossRef]
- Mao, B., et al., Immunity to polio, measles and rubella in women of child-bearing age and estimated congenital rubella syndrome incidence, Cambodia, 2012. Epidemiology & Infection, 2015. 143(9): p. 1858-1867. [CrossRef]
- Plucinski, M.M., et al., Screening for Pfhrp2/3-Deleted Plasmodium falciparum, Non-falciparum, and Low-Density Malaria Infections by a Multiplex Antigen Assay. Journal of Infectious Diseases, 2019. 219(3): p. 437-447. [CrossRef]
- Rogier, E., et al., Bead-based immunoassay allows subpicogram detection of histidine-rich protein 2 from Plasmodium falciparum & estimates reliability of malaria rapid diagnostic tests. PLoS ONE, 2017. 12(2). [CrossRef]
- Gelband, H., et al., Is malaria an important cause of death among adults? The American Journal of Tropical Medicine and Hygiene, 2020. 103(1): p. 41. [CrossRef]
- Roser, M., Malaria: One of the leading causes of child deaths, but progress is possible and you can contribute to it, in Our World in Data. 2024.
- Talapko, J., et al., Malaria: the past and the present. Microorganisms, 2019. 7(6): p. 179. [CrossRef]
- Organization, W.H., World malaria report 2023. 2023: World Health Organization.
- Yang, X., M.B. Quam, T. Zhang, and S. Sang, Global burden for dengue and the evolving pattern in the past 30 years. Journal of travel medicine, 2021. 28(8): p. taab146. [CrossRef]
- Li, J., et al., Global epidemiology and burden of tetanus from 1990 to 2019: A systematic analysis for the Global Burden of Disease Study 2019. International Journal of Infectious Diseases, 2023. 132: p. 118-126. [CrossRef]
- Nsubuga, P., et al., Public health surveillance: a tool for targeting and monitoring interventions. 2011.
- Jain, S. and S.K. Sharma, Challenges & options in dengue prevention & control: A perspective from the 2015 outbreak. Indian Journal of Medical Research, 2017. 145(6): p. 718-721. [CrossRef]
- den Hartog, G., et al., Immune surveillance for vaccine-preventable diseases. Expert review of vaccines, 2020. 19(4): p. 327-339. [CrossRef]
- MacNeil, A., C.-w. Lee, and V. Dietz, Issues and considerations in the use of serologic biomarkers for classifying vaccination history in household surveys. Vaccine, 2014. 32(39): p. 4893-4900. [CrossRef]
- Cutts, F.T. and M. Hanson, Seroepidemiology: an underused tool for designing and monitoring vaccination programmes in low-and middle-income countries. Tropical Medicine & International Health, 2016. 21(9): p. 1086-1098. [CrossRef]
- Azizi, H., et al., Health workers readiness and practice in malaria case detection and appropriate treatment: a meta-analysis and meta-regression. Malaria Journal, 2021. 20: p. 1-12. [CrossRef]
- Pan American Health Organization (PAHO), Toolkit for Integrated Serosurveillance of Communicable Diseases in the Americas. 2022: Washington, D.C.
- Sbarra, A.N., et al., Evaluating Scope and Bias of Population-Level Measles Serosurveys: A Systematized Review and Bias Assessment. Vaccines, 2024. 12(6): p. 585. [CrossRef]
- Daag, J.V., et al., Performance of dried blood spots compared with serum samples for measuring dengue seroprevalence in a cohort of children in Cebu, Philippines. The American journal of tropical medicine and hygiene, 2021. 104(1): p. 130. [CrossRef]
- Styer, L.M., et al., High-throughput multiplex SARS-CoV-2 IgG microsphere immunoassay for dried blood spots: a public health strategy for enhanced serosurvey capacity. Microbiology spectrum, 2021. 9(1): . [CrossRef]
- Curtis, K.A., K.M. Ambrose, M. Susan Kennedy, and S. Michele Owen, Evaluation of dried blood spots with a multiplex assay for measuring recent HIV-1 Infection. PLoS ONE, 2014. 9(9). [CrossRef]
- Amini, F., et al., Reliability of dried blood spot (DBS) cards in antibody measurement: A systematic review. PLoS One, 2021. 16(3): p. e0248218. [CrossRef]
- Organization, W.H., Generic framework for control, elimination and eradication of neglected tropical diseases. 2016, World Health Organization.
- Organization, W.H., Validation of elimination of lymphatic filariasis as a public health problem. 2017.
- World Health Organization, Ending the neglect to attain the Sustainable Development Goals: a road map for neglected tropical diseases 2021–2030. 2020.
Figure 1.
PRISMA Flow Diagram of studies included in this review.
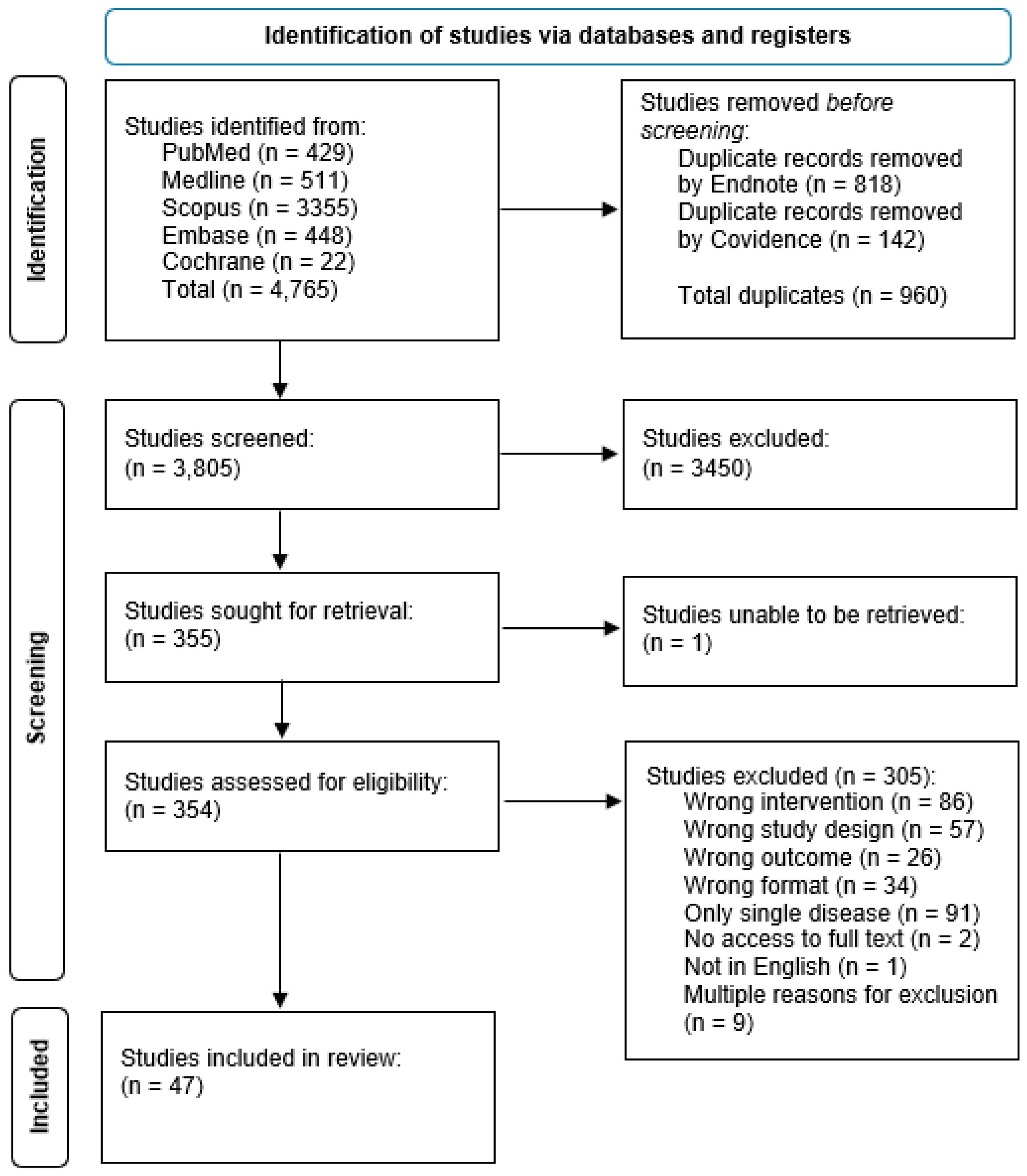
Figure 2.
Number of included studies published each year by disease category Malaria (two or more species); VPDs (two or more pathogens); Combination of NTDs/VPDs/Other; Malaria plus combination of NTDs/VPDs/Other.
Figure 2.
Number of included studies published each year by disease category Malaria (two or more species); VPDs (two or more pathogens); Combination of NTDs/VPDs/Other; Malaria plus combination of NTDs/VPDs/Other.
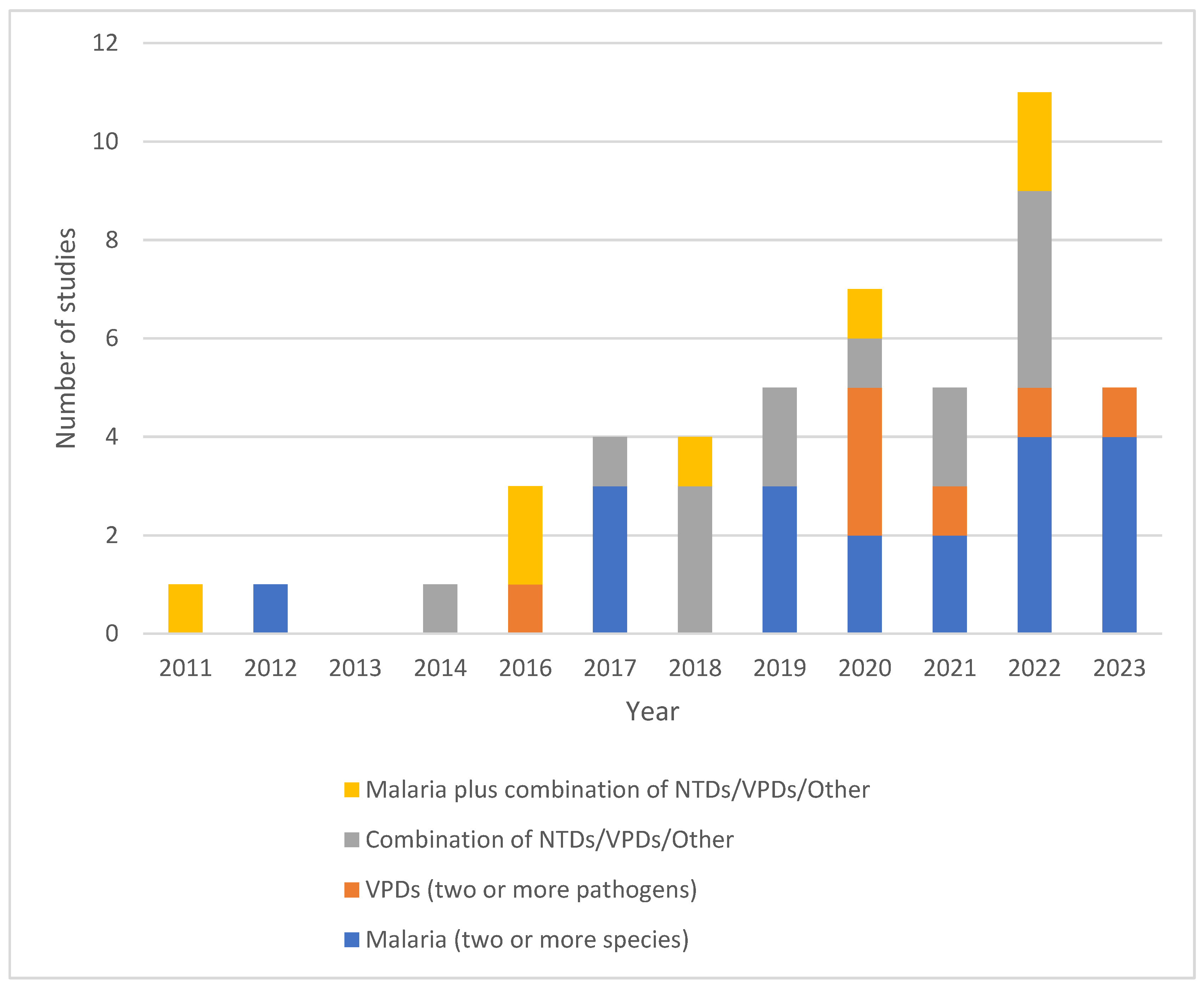
Figure 4.
Potential or reported public health implications of included studies. Some studies belong to more than one category; thus, the total exceeds the number of included studies.
Figure 4.
Potential or reported public health implications of included studies. Some studies belong to more than one category; thus, the total exceeds the number of included studies.
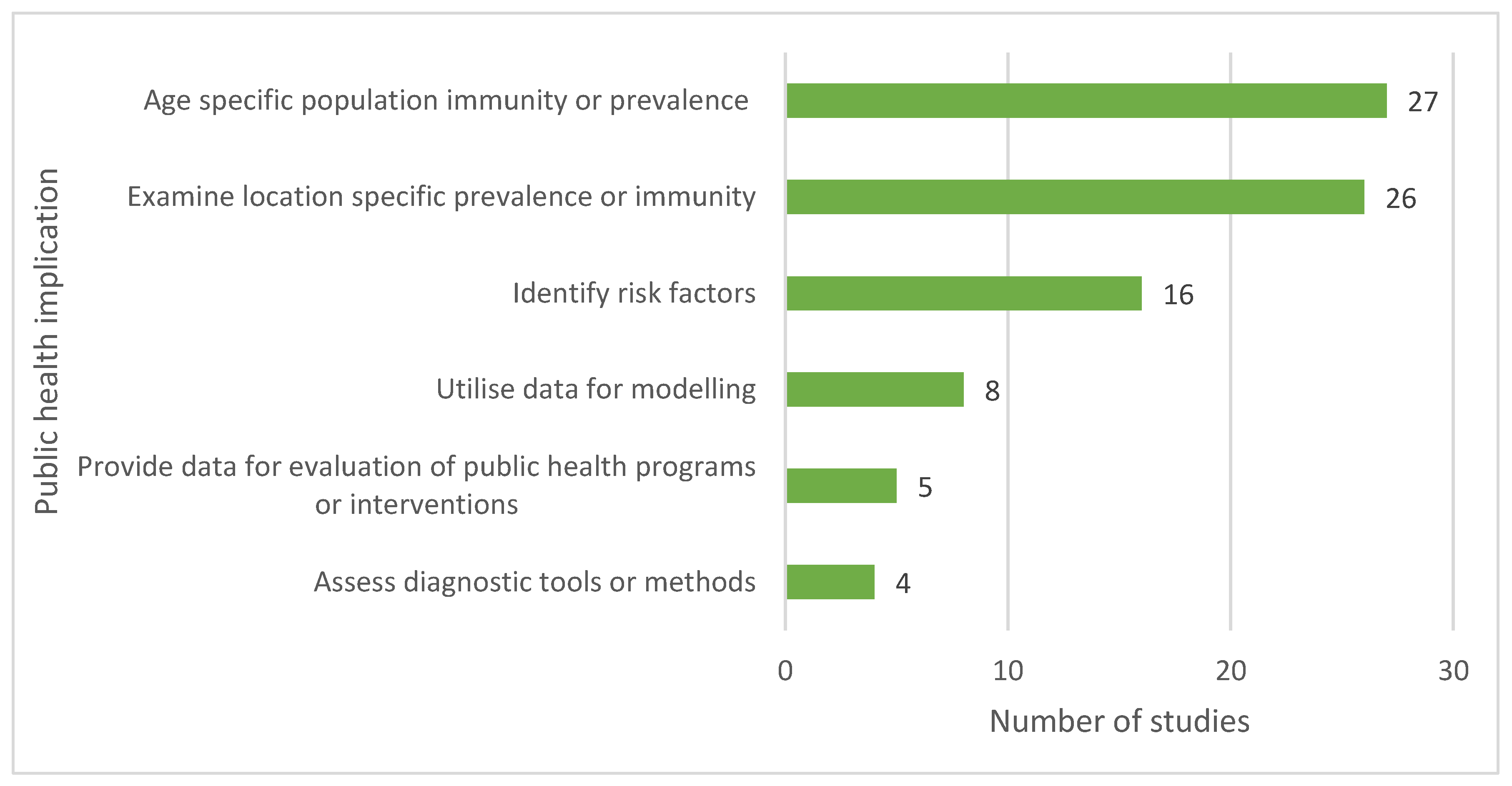
Table 1.
List of studies included in this review.
| ID | First author, year, [reference] | Title |
| 1 | Aiemjoy 2020 [13] | Seroprevalence of antibodies against Chlamydia trachomatis and enteropathogens and distance to the nearest water source among young children in the Amhara Region of Ethiopia |
| 2 | Arnold 2019 [14] | Enteropathogen antibody dynamics and force of infection among children in low-resource settings |
| 3 | Arzika 2022 [15] | Effect of biannual azithromycin distribution on antibody responses to malaria, bacterial, and protozoan pathogens in Niger |
| 4 | Assefa 2019 [16] | Multiplex serology demonstrate cumulative prevalence and spatial distribution of malaria in Ethiopia |
| 5 | Boey 2021 [17] | Seroprevalence of antibodies against diphtheria, tetanus and pertussis in adult at-risk patients |
| 6 | Breakwell 2020 [18] | Seroprevalence of chronic hepatitis B virus infection and immunity to measles, rubella, tetanus and diphtheria among schoolchildren aged 6-7 years old in the Solomon Islands, 2016 |
| 7 | Byrne 2022 [19] | Characterizing the spatial distribution of multiple malaria diagnostic endpoints in a low-transmission setting in Lao PDR |
| 8 | Byrne 2023 [20] | Serological evaluation of risk factors for exposure to malaria in a pre-elimination setting in Malaysian Borneo |
| 9 | Cabora 2016 [21] | A Belgian serosurveillance/seroprevalence study of diphtheria, tetanus and pertussis using a luminex xMAP technology-based pentaplex |
| 10 | Cadavid Restrepo 2022 [22] | Potential use of antibodies to provide an earlier indication of lymphatic filariasis resurgence in post mass drug administration surveillance in American Samoa |
| 11 | Chan 2022 [23] | Assessing seroprevalence and associated risk factors for multiple infectious diseases in Sabah, Malaysia using serological multiplex bead assays |
| 12 | Chan 2022 [24] | Multiplex serology for measurement of IgG antibodies against eleven infectious diseases in a national serosurvey: Haiti 2014-2015 |
| 13 | Cooley 2021 [25] | No serological evidence of trachoma or yaws among residents of registered camps and makeshift settlements in Cox's Bazar, Bangladesh |
| 14 | Feldstein 2020 [26] | Vaccination coverage survey and seroprevalence among forcibly displaced Rohingya children, Cox's Bazar, Bangladesh, 2018: A cross-sectional study |
| 15 | Feleke 2019 [27] | Sero-identification of the aetiologies of human malaria exposure (Plasmodium spp.) in the Limu Kossa District of Jimma Zone, Southwestern Ethiopia |
| 16 | Fornace 2022 [28] | Characterising spatial patterns of neglected tropical disease transmission using integrated sero-surveillance in Northern Ghana |
| 17 | Fujii 2014 [29] | Serological Surveillance Development for Tropical Infectious Diseases Using Simultaneous Microsphere-Based Multiplex Assays and Finite Mixture Models |
| 18 | Herman 2023 [30] | Non-falciparum malaria infection and IgG seroprevalence among children under 15 years in Nigeria, 2018 |
| 19 | Jeang 2023 [31] | Serological Markers of Exposure to Plasmodium falciparum and Plasmodium vivax Infection in Southwestern Ethiopia |
| 20 | Khaireh 2012 [32] | Plasmodium vivax and Plasmodium falciparum infections in the Republic of Djibouti: Evaluation of their prevalence and potential determinants |
| 21 | Khetsuriani 2022 [33] | Diphtheria and tetanus seroepidemiology among children in Ukraine, 2017 |
| 22 | Koffi 2017 [34] | Longitudinal analysis of antibody responses in symptomatic malaria cases do not mirror parasite transmission in peri-urban area of Cote d'Ivoire between 2010 and 2013 |
| 23 | Kwan 2018 [35] | Seroepidemiology of helminths and the association with severe malaria among infants and young children in Tanzania |
| 24 | Labadie-Bracho 2020 [36] | Malaria serology data from the Guiana shield: first insight in IgG antibody responses to Plasmodium falciparum, Plasmodium vivax and Plasmodium malariae antigens in Suriname |
| 25 | Leonard 2022 [37] | Spatial Distribution of Plasmodium falciparum and Plasmodium vivax in Northern Ethiopia by Microscopic, Rapid Diagnostic Test, Laboratory Antibody, and Antigen Data |
| 26 | Lu 2020 [38] | Screening for malaria antigen and anti-malarial IgG antibody in forcibly-displaced Myanmar nationals: Cox's Bazar district, Bangladesh, 2018 |
| 27 | Macalinao 2023 [39] | Analytical approaches for antimalarial antibody responses to confirm historical and recent malaria transmission: an example from the Philippines |
| 28 | McCaffery 2022 [40] | The use of a chimeric antigen for Plasmodium falciparum and Plasmodium vivax seroprevalence estimates from community surveys in Ethiopia and Costa Rica |
| 29 | Mentzer 2022 [41] | Identification of host-pathogen-disease relationships using a scalable multiplex serology platform in UK Biobank |
| 30 | Miernyk 2019 [42] | Human seroprevalence to 11 zoonotic pathogens in the U.S. Arctic, Alaska |
| 31 | Minta 2020 [43] | Seroprevalence of measles, rubella, tetanus, and diphtheria antibodies among children in Haiti, 2017 |
| 32 | Monteiro 2021 [44] | Antibody profile comparison against msp1 antigens of multiple plasmodium species in human serum samples from two different Brazilian populations using a multiplex serological assay |
| 33 | Mosites 2018 [45] | Giardia and cryptosporidium antibody prevalence and correlates of exposure among Alaska residents, 2007-2008 |
| 34 | Moss 2011 [46] | Multiplex bead assay for serum samples from children in Haiti enrolled in a drug study for the treatment of lymphatic filariasis |
| 35 | Njenga 2020 [47] | Integrated cross-sectional multiplex serosurveillance of IgG antibody responses to parasitic diseases and vaccines in coastal Kenya |
| 36 | Oviedo 2022 [48] | Spatial cluster analysis of Plasmodium vivax and Plsmodium malariae exposure using serological data among Haitian school children sampled between 2014 and 2016 |
| 37 | Perraut 2017 [49] | Serological signatures of declining exposure following intensification of integrated malaria control in two rural Senegalese communities |
| 38 | Plucinski 2018 [50] | Multiplex serology for impact evaluation of bed net distribution on burden of lymphatic filariasis and four species of human malaria in northern Mozambique |
| 39 | Poirier 2016 [51] | Measuring Haitian children's exposure to chikungunya, dengue and malaria |
| 40 | Priest 2016 [52] | Integration of multiplex bead assays for parasitic diseases into a national, population-based serosurvey of women 15-39 years of age in Cambodia |
| 41 | Rogier 2017 [53] | Evaluation of immunoglobulin G responses to plasmodium falciparum and plasmodium vivax in Malian school children using multiplex bead assay |
| 42 | Rogier 2019 [54] | High-throughput malaria serosurveillance using a one-step multiplex bead assay |
| 43 | Tohme 2023 [55] | Tetanus and diphtheria seroprotection among children younger than 15 years in Nigeria, 2018: Who are the unprotected children? |
| 44 | vandenHoogen 2021 [56] | Rapid screening for non-falciparum malaria in elimination settings using multiplex antigen and antibody detection: Post hoc identification of plasmodium malariae in an infant in Haiti |
| 45 | Won 2018 [57] | Comparison of antigen and antibody responses in repeat lymphatic filariasis transmission assessment surveys in American Samoa |
| 46 | Woudenberg 2021 [58] | Humoral immunity to SARS-CoV-2 and seasonal coronaviruses in children and adults in north-eastern France |
| 47 | Zambrano 2017 [59] | Use of serologic responses against enteropathogens to assess the impact of a point-of-use water filter: A randomized controlled trial in western province, Rwanda |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



