
Submitted:
20 December 2024
Posted:
23 December 2024
You are already at the latest version
Abstract
High-risk Human Papillomavirus (hrHPV) persistent infection is acknowledged as the primary cause of cervical cancer. Coinfection with other sexually transmitted infections (STIs) may be associated with a higher risk of cervical lesion progression. This study investigated the detection of hrHPV and 7 other STIs in matched clinician-collected cervical samples and self-taken vaginal and urine specimens of 345 asymptomatic women referred to colposcopy for abnormal cervical cytology. The association of sexually transmitted coinfections with cervical dysplasia was evaluated. Detection of hrHPV and 7 other sexually transmitted pathogens was carried out using Anyplex™II HR and Anyplex™II STI-7e, respectively. The positivity of hrHPV infections in cervical, vaginal and urine samples were respectively 67.0%, 71.3% and 68.1%, while STIs were detected in 47.9%, 57.9% and 56.4%. A good analytical agreement was observed between cervical and self-taken samples for hrHPV and STIs detection. STIs positivity rate was found to be higher in hrHPV-positive compared to hrHPV-negative women, but no association was found between STIs coinfections and the grade of cervical lesions. In conclusion, self-collected specimens proved to be a valid non-invasive alternative to cervical samples to detect hrHPV and STIs. Longitudinal studies are required to evaluate the role of STIs coinfections in lesions progression.
Keywords:
High-risk Human Papillomavirus (hrHPV)
; Sexually transmitted infections (STIs)
; Self-sampling
1. Introduction
Cervical cancer represents a serious threat to women’s health globally, with an age-standardized incidence rate of 14.1 per 100,000 women. It is the fourth most common cancer among women, with 661,000 new cases and 348,000 deaths reported in 2022, according to GLOBOCAN data [1]. Persistent infection with high-risk Human Papillomavirus (hrHPV) is widely acknowledged as the primary cause of cervical cancer.
To date, nearly 200 different HPV types have been identified, including twelve classified by the International Agency for Research on Cancer (IARC) as oncogenic or “high-risk” HPV types belonging to the Group 1 (HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58 and 59), with HPV 16 and HPV 18 being the two most common genotypes associated with cervical cancer development [2]. Although HPV infections are widespread among the female population, most of them are transient and spontaneously cleared by the host. Persistent infection with one of the carcinogenic hrHPV types is responsible for the onset of cervical precancer and cancer [3]. Several factors, such as sexual habits, smoking, high parity, long-term use of oral contraceptives and the presence of other sexually transmitted infections (STIs), may increase the risk of cervical dysplasia progression in HPV-positive women.
Coinfections of hrHPV with other sexually transmitted pathogens has been proposed as a risk factor for the development of cervical cancer in HPV-positive women but thier role is controversial and requires to be further investigated [4,5]. Interactions between HPV and other sexually transmitted pathogens that share similar anatomical sites could accelerate cervical lesions progression, enhancing HPV replication and persistence of infection [6].
Although STIs affect both sexes, women are at greater risk due to the anatomy of their reproductive system [7]. While the treatment of symptomatic STIs is effective, many asymptomatic infections are overlooked [8]. The failure to diagnose and treat asymptomatic STIs is responsible for persistence and/or dissemination of infections to sexual contacts. The diagnosis of STIs usually requires screening and/or diagnostic procedures, which may be difficult due to the social stigma associated with this kind of infections, to the limited access to healthcare, particularly in low-middle income countries, and to the invasive nature of the diagnostic procedures [9,10]. The delayed diagnosis and treatment of STIs often increases the risk of long-term health complications, including pelvic inflammatory disease (PID) and infertility in women [11].
Self-samples are currently being used in cervical cancer screening programs worldwide [12]. The accuracy of PCR-based HPV assays on self-collected samples has been demonstrated to be similar to that of clinician-collected cervical specimens [13,14]. Recently, the VALHUDES (Validation of Human Papillomavirus Assays and Collection Devices for Self-samples and Urine Samples) protocol has been developed to evaluate the clinical accuracy of HPV tests in combination with collection devices for HPV testing on self-collected vaginal and urine samples in women referred to colposcopy following cervical cancer screening, in whom higher HPV positivity rates are expected [15].
Self-sampling, as non-invasive and easy-to-perform procedure, could also be applied to the diagnosis and management of other STIs, allowing women who feel uncomfortable with conventional clinical practices to access treatment [9]. Moreover, the use of self-collected samples may represent a more convenient way to screen women for both hrHPV and other STIs from a single clinical sample. A recent review found that self-sampling increased the uptake of STIs testing services compared to samples collected by healthcare professionals [11].
The aim of the present study is to investigate the prevalence and the rates of coinfections of hrHPV genotypes and 7 other sexually transmitted pathogens (Ureaplasma parvum (UP), Ureaplasma urealyticum (UU), Mycoplasma genitalium (MG), Mycoplasma hominis (MH), Chlamydia trachomatis (CT), Neisseria gonorrhoeae (NG), Trichomonas vaginalis (TV)) in clinician-collected cervical samples, self-collected vaginal and urine specimens in women referred to colposcopy. In addition, we evaluated the distribution of STIs among hrHPV-positive and hrHPV-negative women and investigated the association of coinfections between hrHPV and other sexually transmitted pathogens with the severity of cervical dysplasia.
2. Results
2.1. Study Population
Three hundred and forty-five women with a prior abnormal Pap smear were recruited at the first colposcopy referral visit. Their median (interquartile range, IQR) age was 37 (29–46) years. Supplementary Table S1 shows the age distribution of the study population, most of the women (31.3%) were aged 30-40.
Cytology results show that 47.5% of women had low-grade squamous intraepithelial lesions (LSIL), followed by those with atypical squamous cells of undetermined significance (ASCUS) (24.9%) and high-grade squamous intraepithelial lesion (HSIL) (13.6%). 127 women were positive on colposcopic examination, while 218 patients tested negative. Patients underwent cervical biopsy and/or treatment with conization according to clinical judgement and to local clinical protocols. Histological results showed 4 cases of cervical cancer: 2 cases of squamous cell carcinomas, one of adenocarcinoma “in situ” and one cervical carcinoma with dual histological components (Table 1).
2.2. HPV Detection and Genotyping
Among the study population (n = 345), three women were excluded from the analysis because one of their matched samples tested invalid twice. As a result, 342 women were included in the following analysis.
The prevalence of hrHPV, in this cohort of women referred to colposcopy for abnormal cervical cytology, was 67.0% (229/342), 71.3% (244/342), and 68.1% (233/342) in cervical, vaginal, and urine samples, respectively, with HPV16 and HPV31 being the most common types, followed by HPV58 and HPV66 (Figure 1).
In total, 56.3% (129/229), 49.2% (120/244) and 51.1% (119/233) of the women showed single infection with one hrHPV type in cervical swab, vaginal self-sample and urine, respectively, whereas multiple hrHPV infections were detected in 43.7% (100/229), 50.8% (124/244) and 48.9% (114/233) of patients in cervical sample, vaginal swab and urine, respectively (Table 2).
2.3. STIs Prevalence
47.9% (164/342), 57.9% (198/342), and 56.4% (193/342) of investigated women resulted positive for at least one of the seven STIs under investigation in their cervical, vaginal and urine samples, respectively.
UP was the most prevalent pathogen in all samples, followed by UU and MH. No women showed infection with NG. In general, for most of the sexually transmitted pathogens, the detection rate was lower in cervical swabs (Table 5 and Supplementary Figure S1), but statistically significant differences were found only for UP positivity rates in vaginal (p< 0.01) and urine (p< 0.05) specimens compared to cervical samples (Supplementary Tables S2 and S3).
The majority of women with positivity for the STIs panel were infected by a single pathogen in all sample types (Table 6).
2.4. hrHPV and STIs Prevalence in the Different Age Groups
Figure 2 shows the comparison between hrHPV and STIs prevalence in cervical, vaginal and urine samples across the different age groups of women referred to colposcopy for abnormal cervical cytology. hrHPV prevalence was higher in the younger age groups in all sample types. In cervical samples, the highest hrHPV prevalence (75.5%) was observed in the 30-40 age group of women.
Younger women had also higher prevalence of STIs. In the <30 years of age group 55.2% of cervical samples, 71.3% of vaginal self-samples and 69.0% of urine were STIs-positive. The STI rates decreased with age, with the lowest prevalence in the >60 years of group, where all sample types showed a prevalence of 25%.
2.5. hrHPV and STI Co-Infections
Table 9 shows the comparison between STIs prevalence in hrHPV-positive and hrHPV-negative women. For almost all the STIs investigated, the positivity rate among hrHPV-positive women was higher as compared to the hrHPV-negative group in all sample types. The difference was statistically significant for UP, MH in all sample types and for MG in vaginal swabs (Supplementary Table S4).
Table 10 shows the distribution of hrHPV infections in cervical samples according to the clinical data, while Table 11 reports the distribution of hrHPV and STIs infections in the same groups of women.
hrHPV infections showed a high prevalence among young women (<30 years: 71.3%; 30-40 years: 75.5%), women with positive colposcopy outcome (82.4%), and high-grade cytologycal lesions (HSIL: 80.9%; ASCH: 80.8%). In women with histologically confirmed high-grade cervical lesions (≥CIN 2), 96.7% of them showed hrHPV infection (Table 10).
The highest prevalence of co-infections with hrHPV and other sexually transmitted pathogens was found in women under 30 years (46.0%), the lowest in women over 60 years (25.0%). Among women with positive and negative colposcopy outcomes, 45.6% and 33.6% of women showed co-infections with hrHPV and STIs pathogens, respectively. Rates of co-infections with hrHPV and sexually transmitted pathogens among women with low-grade cervical lesions ranged from 21.4% to 43.8%, while among those with high-grade cervical lesions from 34.0% to 50.0%. In the group of women with histologically confirmed ≥CIN 2 lesions, 96.6% of women were hrHPV-positive however no difference was observed between those with or without concomitant coinfections with other sexually transmitted pathogens (48.3% vs 48.3%), as illustrated in Table 11.
3. Discussion
In this cross-sectional study, we evaluated the detection of hrHPV and 7 other sexually transmitted pathogens in self-collected vaginal and urine samples compared to cervical swabs of women referred to colposcopy. A high prevalence of STIs was detected in hrHPV-positive women, but no association was found between women with the high-grade cervical dysplasia and concomitant coinfections with hrHPV and one or more of the other investigated sexually transmitted pathogens.
The VALHUDES study protocol is currently being used for the evaluation of the clinical accuracy of HPV tests in self-collected vaginal and first-void urine samples [16]. However, there are no guidelines for the correct assessment of other STIs in self-collected samples. In the present study, we observed a good analytical agreement between cervical samples and self-collected vaginal and urine samples for the detection of hrHPV. The concordance rate of cervical and vaginal specimens was higher than that of cervical and urine samples, consistent with what was reported in previous studies [17,18]. HPV16 and HPV31 were the most frequently detected genotypes in all sample types. Cervical samples showed a higher prevalence of single hrHPV infections as compared to self-collected samples, as previously reported by our group [18]. The results of this study suggest that self-collected specimens can be considered as a valid non-invasive alternative to cervical samples for the detection of hrHPV, contributing to improving women’s participation to HPV screening. There has recently been a strong emphasis focusing on self-sampling as a key strategy to accelerate the global fight against cervical cancer [19]. Furthermore, self-collection has shown good acceptability in low resource settings, improving success in cervical cancer elimination [20,21] by reducing public health costs and alleviating feelings of shame and discomfort offering women privacy [20]. Acceptability, however, depends on socio-cultural aspects and women’s perceptions. Currently, countries such as New Zealand, Australia, the Netherlands, France and Sweden have included self-sampling in their national cervical cancer screening programs [12,14].
Furthermore the present work has demonstrated a substantial agreement between self-collected samples and cervical specimens for the detection of other STIs in asymptomatic women referred to colposcopy. Vaginal swabs showed the highest STI detection rate, followed by urine specimens. The difference in positivity rates between cervical and self-collected samples was statistically significant for UP. These results are in alignment with other studies reporting that vaginal swabs are more sensitive than urine in detecting these pathogens [22,23]. For the screening of STIs in women, the CDC’s recommendations, published in 2014, have indicated vaginal swabs as the optimal sample type for the laboratory-based detection of both CT and NG [24]. The result of the present study further confirm the accuracy in the use of vaginal swabs for the detection of STIs.
The present study has also reported higher rates of multiple STI infections among self-collected specimens as compared to cervical samples, suggesting that some of the investigated pathogens may be responsible for infections of the lower genital tract. Bacteria belonging to Mycoplasmataceae family, including the two genera Mycoplasma spp. and Ureaplasma spp., are the most common STI pathogens. They are important opportunistic pathogens of the female lower genital tract [25] and they can be isolated in the urogenital system of many healthy individuals as commensals [26]. This may explain the lower detection rates in cervical swabs for most of the investigated sexually transmitted pathogens. Analyzing the distribution of each potential STIs pathogen across the different samples, UP was the most prevalent Mycoplasmataceae detected, followed by UU and MH. This is in line with findings from previous studies conducted in Greece [27], in Australia [28], in China [29] and by our group [6] where UP was found to be the most prevalent microorganism among healthy women. In our study MG, CT, NG and TV were detected at lower rates, probably due to the fact that our participants were asymptomatic and recruited when referred to colposcopy for an abnormal Pap smear.
In the present study, STIs infections were more frequently detected among hrHPV-positive than hrHPV-negative women, but no association was found between the grade of the cervical lesion and the frequency of STIs coinfections detected. While persistent hrHPV infections have been demonstrated to be the necessary cause of the onset of cervical precancer and cancer, the potential role of other STIs as cofactors in the development of cervical lesions is still controversial. While some studies have suggested an association between the presence of STIs and a higher risk of occurrence of high-grade cervical lesions [4,5,30,31,32], others have reported no association [33,34] as also indicated by the results of the present cross-sectional study. Even if the role of STIs other than hrHPV and cervical lesions development remains to be clarified, changes in local microbiota and infections with other sexually transmitted pathogens have been proposed to act as cofactors with HPV infection, potentially facilitating its entry and persistence through chronic cervical inflammation and ulceration of the cervical epithelium as well as through a reduction in host cell–mediated immunity [25]. Persistent cervicitis might also enhance the progress of undetected precancerous cervical lesions [35,36]. In fact, previous published reports indicate that cervical carcinogenesis is associated with inflammation [35,36], driven by the hormonal milieu, regulatory cytokines and chemokines, as well as multiple cervicovaginal microorganisms [37]. The chronic inflammation caused by Ureaplasma spp. infections might favor the entry of other microorganisms or induce chromosomal alterations that might lead to carcinogenesis of epithelial cells [38]. In an early study, Lukic et al. postulated that UU is related to the persistence of HPV infection and early cervical cytological changes [39] through several inflammatory responses, involving the production of reactive oxidative metabolites, increased expression of cytokines, chemokines and angiogenic factors, decreased cell-mediated immunity and the generation of free radicals [32,40]. Moreover, it is well known that the immunological status of a patient may influence HPV infection persistence. Surprisingly however the present study showed no association between hrHPV and STIs coinfections and the underlying severity of cervical lesions.
In this study, statistically significant differences were found in the distribution of UP between hrHPV-positive and hrHPV-negative women in the cervical, vaginal swab and urine samples. Similar results have been previously reported in cervical samples with a significantly higher UP6 infection rate in the HPV-positive group than in the HPV-negative group [41]. In a previous study, Parthenis et al. recruited 345 asymptomatic patients attending a gynecology clinic for routine cervical screening, and Ureaplasma spp., detected in 30.2% of hrHPV-positive women, was the most frequently isolated pathogen [42]. Verteramo et al. showed an increased infection rate of UU in HPV-positive women, with a significant association found in the presence of high colonization rate of UU at cervical level [25]. Surprisingly, the present study showed statistically significant differences in the MH positivity rate for hrHPV-positive women compared to hrHPV-negative women in all sample types, as well as MG positivity in vaginal swabs. Mycoplasma infections have been linked to “in vitro” chromosomal changes and cell transformation [43,44]. No significant difference was found for the other investigated STI pathogens which were rarely detected in our population.
The association between CT and cervical cancer has been widely investigated [25,31,40,45,46]. CT might increase susceptibility to HPV causing micro-abrasions or cervical epithelial cells and molecular alterations, facilitating the entry of virions [25,31]. However, in this study, there wasn’t a significant difference between CT distribution in hrHPV-positive women and hrHPV-negative women, probably because of the low frequency of CT infections in our population.
The results of the present study further confirm the high prevalence of STIs in young women, as previously described in the literature [47,48]. The risk of acquiring sexually transmitted infections decreases with age, as well as the probability of clearing the infection. Since this study is conducted in a colposcopy setting, as expected the prevalence of hrHPV infections was found to be very high. For this reason, the high hrHPV positivity rate found in older women may not reflect the trend of hrHPV infections distribution in the different age groups in the general population.
In our cross-sectional study we found a higher STI rate infection in hrHPV-positive women compared to hrHPV-negative women, but this result was not correlated with the clinical outcome underlying severity of cervical lesions, underlining the controversial role of HPV and STIs coinfections in the development of cervical dysplasia. Further longitudinal studies including a larger number of women will allow in the future to better investigate the possible role of hrHPV-STIs coinfections in cervical lesion development.
In conclusion, the present study demonstrated that self-taken specimens may be a good alternative for screening of both hrHPV and other STIs. Due to the increasing prevalence according to ECDC data [49], it may be important in the future to implement laboratory-based detection of STIs on self-collected samples among women who participate to cervical cancer screening programs or during subsequent visits for the treatment of cervical lesions.
4. Materials and Methods
4.1. Study Design and Sample Collection
From May 2017 to September 2024, 345 women have been enrolled at the Colposcopy Clinics of Fondazione IRCCS San Gerardo dei Tintori (Monza, Italy) following the signing of an informed consent. Women were referred to colposcopy because of a recent abnormal cervical cytology result.
Prior to gynaecological examination, all women were asked to autonomously collect a first-void urine sample using a Colli-Pee® device (Novosanis, Belgium) and a vaginal swab using FLOQSwab® 552.80 (Copan Italia Spa, Brescia, Italy).
Before performing the colposcopy, the physician collected a cervical specimen from each woman using an L-shaped Endo/Esocervical FLOQSwab® (Copan Italia Spa, Brescia, Italy) that was immediately resuspended into 20 ml of ThinPrep® PreservCyt® Solution (HOLOGIC™, Marlborough, MA, USA).
Based on the colposcopy findings and clinical judgment, women underwent biopsy and/or treatment with conisation.
The classification of cytological lesions was conducted according to the Bethesda system [50], whilst the histological outcomes were classified according to World Health Organization (WHO) histological classification of tumors [51]. Histological lesions worse than cervical intraepithelial neoplasia grade 2 (≥CIN2) were considered as high-grade lesions.
The study was conducted following the approval of the Ethics Committee of the University of Milano-Bicocca (Protocol n. 0037320/2017 and update n. 0086409/2018).
4.2. Pre-Analytical Samples Processing and Nucleic Acids Extraction
All samples were processed at the Laboratory of Clinical Microbiology of the University of Milano-Bicocca, Monza, Italy. On their arrival at the laboratory, cervical samples were vortexed for 30 seconds, aliquots of 1.5 mL were dispensed into sterile cryotubes and stored at -20°C until testing.
First-void urine collected using Colli-Pee® was also shaken on the vortex for 30 seconds and aliquots of 1.5 mL were stored at -20°C in sterile cryotubes until testing.
Vaginal self-samples were transported dry at the laboratory where they were suspended in 5.5 mL of ThinPrep® PreservCyt® Solution. 1 ml was then dispensed into sterile cryotubes and stored at -20°C until testing.
200 μl of all sample types were used to perform nucleic acid extraction using STARMag 96x4 Universal Cartridge Kit (Seegene, Seoul, Republic of Korea) on the MicroLab Nimbus workstation (Hamilton) with a final elution volume of 100 μl.
4.3. HPV and STIs Detection
Nimbus platform allows real-time PCR plate preparation of Anyplex™ II HR HPV (Seegene, Seoul, Republic of Korea) and Anyplex™ II STI-7e (Seegene, Seoul, Republic of Korea) assays.
Anyplex™ II HR HPV is a full genotyping HR-HPV assay that individually detects 14 different genotypes of hrHPV (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68) and a cellular gene target by melting curves analysis. The analysis is performed on the CFX96 (Bio-Rad, Hercules, USA) with 5 μl of template DNA in a total volume of 20 μl.
Anyplex™ II STI-7e allows the detection of 7 sexually transmitted pathogens, Chlamydia trachomatis, Neisseria gonorrhoeae, Trichomonas vaginalis, Mycoplasma hominis, Mycoplasma genitalium, Ureaplasma urealyticum and Ureaplasma parvum. According to the manufacturer’s instructions, the real-time PCR analysis is performed on the CFX96 using 5 μl of template DNA in a total volume of 20 μl.
Data interpretation of the results obtained with both assays was done using the Seegene Viewer software according to the manufacturer’s instructions.
Samples that were invalid according to the software interpretation were retested. After two invalid results, samples were excluded from the analysis.
4.4. Statistical Analysis
Qualitative and quantitative variables were summarized using absolute and relative (percentage) frequencies and medians (interquartile ranges, IQR), respectively. Concordance between the results of cervical and self-collected specimens with the two assays was evaluated using Cohen’s kappa (κ) statistics and defined as follows: slight (0.00 < κ < 0.20), fair (0.21 < κ < 0.40), moderate (0.41 < κ < 0.60), substantial (0.61 < κ < 0.80) and almost perfect (0.81 < κ < 1.00). Statistical analyses were performed with R software (R Core Team 2021). Statistical significance between positivity rates was calculated using Pearson’s Chi-squared (X2) test with Yates correction or Fisher’s exact test, as appropriate (Tables S2–S4).
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, Figure S1: Prevalence of STI pathogens in different samples; Table S1: Age distribution of the study population; Table S2: Tests used to calculate statistical significance differences between positivity rates of UP, UU, MH and MG in the three sample types; Table S3: Tests used to calculate statistical significance differences between positivity rates of CT, NG and TV in the three sample types; Table S4: Tests used to calculate statistical significance differences between positivity rates of STI pathogens in hrHPV-positive and negative women in the three sample types.
Author Contributions
Conceptualization, C.E.C. and F.L.; methodology, C.G., M.M., M.R., R.C.N., F.P. and R.M.; formal analysis, C.G., M.M. M.R. and G.M.; investigation, C.E.C.; data curation, C.G, M.M, M.R. and M.L.D.M.; writing—original draft preparation, C.G., M.M. and M.R.; writing—review and editing, C.G., M.M., M.R., M.L.D.M., R.C.N., F.P., G.M., R.F., F.L. and C.E.C.; supervision, C.E.C.; project administration, C.E.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of University of Milano-Bicocca (protocol numbers 0037320/2017 and 0086409/2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Final study datasets generated by the study are stored locally and securely at the University of Milano-Bicocca. Anonymized data will be available by request to the corresponding author on a case-by-case basis pending approval by the University of Milano-Bicocca.
Acknowledgments
The Clinical Microbiology Research Group of the University of Milano-Bicocca received free cervical and vaginal self-sample collection devices from Copan Italia Spa (Brescia, Italy), free Colli-pee® (20 mL) from Novosanis (Belgium), and STARMag 96x4 Universal Cartridge Kit, Anyplex™ II HR HPV and Anyplex™ II STI-7e from Arrows Diagnostics. The University of Milano-Bicocca also received research grants from BD Diagnostics, Seegene, Arrows Diagnostics, Copan, GeneFirst, Hiantis and VITRO.
Conflicts of Interest
C.E.C. is a minority share-holder of Hiantis. C. G., M. M., M. R., M. L. D. M., R. C. N., F. P., G. M., R. M., R. F., F. L. declare no conflicts of interest.
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R. L.; Soerjomataram, I.; Jemal, A. Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA. Cancer J. Clin. 2024, 74 (3), 229–263. [CrossRef]
- Burd, E. M. Human Papillomavirus and Cervical Cancer. Clin. Microbiol. Rev. 2003, 16 (1), 1–17. [CrossRef]
- Walboomers, J. M. M.; Jacobs, M. V.; Manos, M. M.; Bosch, F. X.; Kummer, J. A.; Shah, K. V.; Snijders, P. J. F.; Peto, J.; Meijer, C. J. L. M.; Muñoz, N. Human Papillomavirus Is a Necessary Cause of Invasive Cervical Cancer Worldwide. J. Pathol. 1999, 189 (1), 12–19. [CrossRef]
- Zhu, H.; Shen, Z.; Luo, H.; Zhang, W.; Zhu, X. Chlamydia Trachomatis Infection-Associated Risk of Cervical Cancer: A Meta-Analysis. Medicine (Baltimore) 2016, 95 (13), e3077. [CrossRef]
- Wang, L.; Zhu, L.; Li, H.; Ma, N.; Huang, H.; Zhang, X.; Li, Y.; Fang, J. Association between Asymptomatic Sexually Transmitted Infections and High-Risk Human Papillomavirus in Cervical Lesions. J. Int. Med. Res. 2019, 47 (11), 5548–5559. [CrossRef]
- Martinelli, M.; Musumeci, R.; Sechi, I.; Sotgiu, G.; Piana, A.; Perdoni, F.; Sina, F.; Fruscio, R.; Landoni, F.; Cocuzza, C. E. Prevalence of Human Papillomavirus (HPV) and Other Sexually Transmitted Infections (STIs) among Italian Women Referred for a Colposcopy. Int. J. Environ. Res. Public. Health 2019, 16 (24), 5000. [CrossRef]
- Panchanadeswaran, S.; Johnson, S. C.; Mayer, K. H.; Srikrishnan, A. K.; Sivaran, S.; Zelaya, C. E.; Go, V. F.; Solomon, S.; Bentley, M. E.; Celentano, D. D. Gender Differences in the Prevalence of Sexually Transmitted Infections and Genital Symptoms in an Urban Setting in Southern India. Sex. Transm. Infect. 2006, 82 (6), 491–495. [CrossRef]
- Otieno, F. O.; Ndivo, R.; Oswago, S.; Ondiek, J.; Pals, S.; McLellan-Lemal, E.; Chen, R. T.; Chege, W.; Gray, K. M. Evaluation of Syndromic Management of Sexually Transmitted Infections within the Kisumu Incidence Cohort Study. Int. J. STD AIDS 2014, 25 (12), 851–859. [CrossRef]
- Paudyal, P.; Llewellyn, C.; Lau, J.; Mahmud, M.; Smith, H. Obtaining Self-Samples to Diagnose Curable Sexually Transmitted Infections: A Systematic Review of Patients’ Experiences. PLOS ONE 2015, 10 (4), e0124310. [CrossRef]
- Nodjikouambaye, Z. A.; Compain, F.; Sadjoli, D.; Mboumba Bouassa, R.-S.; Péré, H.; Veyer, D.; Robin, L.; Adawaye, C.; Tonen-Wolyec, S.; Moussa, A. M.; Koyalta, D.; Belec, L. Accuracy of Curable Sexually Transmitted Infections and Genital Mycoplasmas Screening by Multiplex Real-Time PCR Using a Self-Collected Veil among Adult Women in Sub-Saharan Africa. Infect. Dis. Obstet. Gynecol. 2019, 2019, 1–15. [CrossRef]
- Ogale, Y.; Yeh, P. T.; Kennedy, C. E.; Toskin, I.; Narasimhan, M. Self-Collection of Samples as an Additional Approach to Deliver Testing Services for Sexually Transmitted Infections: A Systematic Review and Meta-Analysis. BMJ Glob. Health 2019, 4 (2), e001349. [CrossRef]
- Serrano, B.; Ibáñez, R.; Robles, C.; Peremiquel-Trillas, P.; De Sanjosé, S.; Bruni, L. Worldwide Use of HPV Self-Sampling for Cervical Cancer Screening. Prev. Med. 2022, 154, 106900. [CrossRef]
- Arbyn, M.; Verdoodt, F.; Snijders, P. J. F.; Verhoef, V. M. J.; Suonio, E.; Dillner, L.; Minozzi, S.; Bellisario, C.; Banzi, R.; Zhao, F.-H.; Hillemanns, P.; Anttila, A. Accuracy of Human Papillomavirus Testing on Self-Collected versus Clinician-Collected Samples: A Meta-Analysis. Lancet Oncol. 2014, 15 (2), 172–183. [CrossRef]
- Arbyn, M.; Smith, S. B.; Temin, S.; Sultana, F.; Castle, P. Detecting Cervical Precancer and Reaching Underscreened Women by Using HPV Testing on Self Samples: Updated Meta-Analyses. BMJ 2018, k4823. [CrossRef]
- Arbyn, M.; Peeters, E.; Benoy, I.; Vanden Broeck, D.; Bogers, J.; De Sutter, P.; Donders, G.; Tjalma, W.; Weyers, S.; Cuschieri, K.; Poljak, M.; Bonde, J.; Cocuzza, C.; Zhao, F. H.; Van Keer, S.; Vorsters, A. VALHUDES: A Protocol for Validation of Human Papillomavirus Assays and Collection Devices for HPV Testing on Self-Samples and Urine Samples. J. Clin. Virol. 2018, 107, 52–56. [CrossRef]
- Latsuzbaia, A.; Van Keer, S.; Vanden Broeck, D.; Weyers, S.; Donders, G.; De Sutter, P.; Tjalma, W.; Doyen, J.; Vorsters, A.; Arbyn, M. Clinical Accuracy of Alinity m HR HPV Assay on Self- versus Clinician-Taken Samples Using the VALHUDES Protocol. J. Mol. Diagn. 2023, 25 (12), 957–966. [CrossRef]
- Cho, H.-W.; Ouh, Y.-T.; Hong, J. H.; Min, K. J.; So, K. A.; Kim, T. J.; Paik, E. S.; Lee, J.; Moon, J. H.; Lee, J. K. Comparison of Urine, Self-Collected Vaginal Swab, and Cervical Swab Samples for Detecting Human Papillomavirus (HPV) with Roche Cobas HPV, Anyplex II HPV, and RealTime HR-S HPV Assay. J. Virol. Methods 2019, 269, 77–82. [CrossRef]
- Martinelli, M.; Giubbi, C.; Di Meo, M. L.; Perdoni, F.; Musumeci, R.; Leone, B. E.; Fruscio, R.; Landoni, F.; Cocuzza, C. E. Accuracy of Human Papillomavirus (HPV) Testing on Urine and Vaginal Self-Samples Compared to Clinician-Collected Cervical Sample in Women Referred to Colposcopy. Viruses 2023, 15 (9), 1889. [CrossRef]
- World Health Organisation. WHO Guideline for Screening and Treatment of Cervical Pre-Cancer Lesions for Cervical Cancer Prevention, 2nd ed.; Geneva, 2021.
- Brandt, T.; Wubneh, S. B.; Handebo, S.; Debalkie, G.; Ayanaw, Y.; Alemu, K.; Jede, F.; Von Knebel Doeberitz, M.; Bussmann, H. Genital Self-Sampling for HPV-Based Cervical Cancer Screening: A Qualitative Study of Preferences and Barriers in Rural Ethiopia. BMC Public Health 2019, 19 (1), 1026. [CrossRef]
- Bansil, P.; Wittet, S.; Lim, J. L.; Winkler, J. L.; Paul, P.; Jeronimo, J. Acceptability of Self-Collection Sampling for HPV-DNA Testing in Low-Resource Settings: A Mixed Methods Approach. BMC Public Health 2014, 14 (1), 596. [CrossRef]
- Shafer, M.-A.; Moncada, J.; Boyer, C. B.; Betsinger, K.; Flinn, S. D.; Schachter, J. Comparing First-Void Urine Specimens, Self-Collected Vaginal Swabs, and Endocervical Specimens To Detect Chlamydia Trachomatis and Neisseria Gonorrhoeae by a Nucleic Acid Amplification Test. J. Clin. Microbiol. 2003, 41 (9), 4395–4399. [CrossRef]
- Davis, A.; Gaynor, A. Testing for Sexually Transmitted Diseases in US Public Health Laboratories, 2016. Sex. Transm. Dis. 2020, 47 (2), 122–127. [CrossRef]
- Centers for Disease Control and Prevention. Recommendations for the Laboratory-Based Detection of Chlamydia Trachomatis and Neisseria Gonorrhoeae--2014. MMWR Recomm. Rep. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2014, 63 (RR-02), 1–19.
- Verteramo, R.; Pierangeli, A.; Mancini, E.; Calzolari, E.; Bucci, M.; Osborn, J.; Nicosia, R.; Chiarini, F.; Antonelli, G.; Degener, A. M. Human Papillomaviruses and Genital Co-Infections in Gynaecological Outpatients. BMC Infect. Dis. 2009, 9 (1), 16. [CrossRef]
- Friberg, J.; Gnarpe, H. Mycoplasmas in Semen from Fertile And-Infertile Men. Andrologia 2009, 6 (1), 45–52. [CrossRef]
- Valasoulis, G.; Pouliakis, A.; Michail, G.; Magaliou, I.; Parthenis, C.; Margari, N.; Kottaridi, C.; Spathis, A.; Leventakou, D.; Ieronimaki, A.-I.; Androutsopoulos, G.; Panagopoulos, P.; Daponte, A.; Tsiodras, S.; Panayiotides, I. G. Cervical HPV Infections, Sexually Transmitted Bacterial Pathogens and Cytology Findings—A Molecular Epidemiology Study. Pathogens 2023, 12 (11), 1347. [CrossRef]
- Kong, F.; Ma, Z.; James, G.; Gordon, S.; Gilbert, G. L. Species Identification and Subtyping of Ureaplasma Parvum and Ureaplasma Urealyticum Using PCR-Based Assays. J. Clin. Microbiol. 2000, 38 (3), 1175–1179. [CrossRef]
- Zhang, D.; Li, T.; Chen, L.; Zhang, X.; Zhao, G.; Liu, Z. Epidemiological Investigation of the Relationship between Common Lower Genital Tract Infections and High-Risk Human Papillomavirus Infections among Women in Beijing, China. PLOS ONE 2017, 12 (5), e0178033. [CrossRef]
- Koskela, P.; Anttila, T.; Bjørge, T.; Brunsvig, A.; Dillner, J.; Hakama, M.; Hakulinen, T.; Jellum, E.; Lehtinen, M.; Lenner, P.; Luostarinen, T.; Pukkala, E.; Saikku, P.; Thoresen, S.; Youngman, L.; Paavonen, J. Chlamydia Trachomatis Infection as a Risk Factor for Invasive Cervical Cancer. Int. J. Cancer 2000, 85 (1), 35–39. [CrossRef]
- Smith, J. S.; Bosetti, C.; Muñoz, N.; Herrero, R.; Bosch, F. X.; Eluf-Neto, J.; Meijer, C. J. L. M.; Van Den Brule, A. J. C.; Franceschi, S.; Peeling, R. W. Chlamydia Trachomatis and Invasive Cervical Cancer: A Pooled Analysis of the IARC Multicentric Case-control Study. Int. J. Cancer 2004, 111 (3), 431–439. [CrossRef]
- Biernat-Sudolska, M.; Szostek, S.; Rojek-Zakrzewska, D.; Klimek, M.; Kosz-Vnenchak, M. Concomitant Infections with Human Papillomavirus and Various Mycoplasma and Ureaplsasma Species in Women with Abnormal Cervical Cytology. Adv. Med. Sci. 2011, 56 (2), 299–303. [CrossRef]
- Robial, R.; Longatto-Filho, A.; Roteli-Martins, C. M.; Silveira, M. F.; Stauffert, D.; Ribeiro, G. G.; Linhares, I. M.; Tacla, M.; Zonta, M. A.; Baracat, E. C. Frequency of Chlamydia Trachomatis Infection in Cervical Intraepithelial Lesions and the Status of Cytological P16/Ki-67 Dual-Staining. Infect. Agent. Cancer 2017, 12 (1), 3. [CrossRef]
- Castle, P. E.; Escoffery, C.; Schachter, J.; Rattray, C.; Schiffman, M.; Moncada, J.; Sugai, K.; Brown, C.; Cranston, B.; Hanchard, B.; Palefsky, J. M.; Burk, R. D.; Hutchinson, M. L.; Strickler, H. D. Chlamydia Trachomatis, Herpes Simplex Virus 2, and Human T-Cell Lymphotrophic Virus Type 1 Are Not Associated With Grade of Cervical Neoplasia in Jamaican Colposcopy Patients: Sex. Transm. Dis. 2003, 30 (7), 575–580. [CrossRef]
- Castle, P. E.; Giuliano, A. R. Chapter 4: Genital Tract Infections, Cervical Inflammation, and Antioxidant Nutrients--Assessing Their Roles as Human Papillomavirus Cofactors. JNCI Monogr. 2003, 2003 (31), 29–34. [CrossRef]
- Rokos, T.; Holubekova, V.; Kolkova, Z.; Hornakova, A.; Pribulova, T.; Kozubik, E.; Biringer, K.; Kudela, E. Is the Physiological Composition of the Vaginal Microbiome Altered in High-Risk HPV Infection of the Uterine Cervix? Viruses 2022, 14 (10), 2130. [CrossRef]
- Silva, J.; Cerqueira, F.; Medeiros, R. Chlamydia Trachomatis Infection: Implications for HPV Status and Cervical Cancer. Arch. Gynecol. Obstet. 2014, 289 (4), 715–723. [CrossRef]
- Lv, P.; Zhao, F.; Xu, X.; Xu, J.; Wang, Q.; Zhao, Z. Correlation between Common Lower Genital Tract Microbes and High-Risk Human Papillomavirus Infection. Can. J. Infect. Dis. Med. Microbiol. 2019, 2019, 1–6. [CrossRef]
- Lukic, A.; Canzio, C.; Patella, A.; Giovagnoli, M.; Cipriani, P.; Frega, A.; Moscarini, M. Determination of Cervicovaginal Microorganisms in Women with Abnormal Cervical Cytology: The Role of Ureaplasma Urealyticum. Anticancer Res. 2006, 26 (6C), 4843–4849.
- Liang, Y.; Chen, M.; Qin, L.; Wan, B.; Wang, H. A Meta-Analysis of the Relationship between Vaginal Microecology, Human Papillomavirus Infection and Cervical Intraepithelial Neoplasia. Infect. Agent. Cancer 2019, 14 (1), 29. [CrossRef]
- A, D.; Bi, H.; Zhang, D.; Xiao, B. Association between Human Papillomavirus Infection and Common Sexually Transmitted Infections, and the Clinical Significance of Different Mycoplasma Subtypes. Front. Cell. Infect. Microbiol. 2023, 13, 1145215. [CrossRef]
- Parthenis, C.; Panagopoulos, P.; Margari, N.; Kottaridi, C.; Spathis, A.; Pouliakis, A.; Konstantoudakis, S.; Chrelias, G.; Chrelias, C.; Papantoniou, N.; Panayiotides, I. G.; Tsiodras, S. The Association between Sexually Transmitted Infections, Human Papillomavirus, and Cervical Cytology Abnormalities among Women in Greece. Int. J. Infect. Dis. 2018, 73, 72–77. [CrossRef]
- Macpherson, I.; Russell, W. Transformations in Hamster Cells Mediated by Mycoplasmas. Nature 1966, 210 (5043), 1343–1345. [CrossRef]
- Tsai, S.; Wear, D. J.; Shih, J. W.; Lo, S. C. Mycoplasmas and Oncogenesis: Persistent Infection and Multistage Malignant Transformation. Proc. Natl. Acad. Sci. 1995, 92 (22), 10197–10201. [CrossRef]
- Ssedyabane, F.; Amnia, D. A.; Mayanja, R.; Omonigho, A.; Ssuuna, C.; Najjuma, J. N.; Freddie, B. HPV-Chlamydial Coinfection, Prevalence, and Association with Cervical Intraepithelial Lesions: A Pilot Study at Mbarara Regional Referral Hospital. J. Cancer Epidemiol. 2019, 2019, 1–7. [CrossRef]
- Naldini, G.; Grisci, C.; Chiavarini, M.; Fabiani, R. Association between Human Papillomavirus and Chlamydia Trachomatis Infection Risk in Women: A Systematic Review and Meta-Analysis. Int. J. Public Health 2019, 64 (6), 943–955. [CrossRef]
- Arévalos, A.; Valenzuela, A.; Mongelós, P.; Barrios, H.; Rodríguez, M. I.; Báez, R.; Centurión, C.; Vester, J.; Soilán, A.; Ortega, M.; Meza, L.; Páez, M.; Castro, A.; Cristaldo, C.; Soskin, A.; Deluca, G.; Baena, A.; Herrero, R.; Almonte, M.; Kasamatsu, E.; Mendoza, L.; ESTAMPA Paraguayan Study Group. Genital Infections in High-Risk Human Papillomavirus Positive Paraguayan Women Aged 30–64 with and without Cervical Lesions. PLOS ONE 2024, 19 (10), e0312947. [CrossRef]
- Ginindza, T. G.; Dlamini, X.; Almonte, M.; Herrero, R.; Jolly, P. E.; Tsoka-Gwegweni, J. M.; Weiderpass, E.; Broutet, N.; Sartorius, B. Prevalence of and Associated Risk Factors for High Risk Human Papillomavirus among Sexually Active Women, Swaziland. PLOS ONE 2017, 12 (1), e0170189. [CrossRef]
- ECDC. STI Cases on the Rise across Europe. https://www.ecdc.europa.eu/en/news-events/sti-cases-rise-across-europe.
- Smith, J. H. F. Bethesda 2001. Cytopathology 2002, 13 (1), 4–10. [CrossRef]
- WHO Classification of Tumours. Female Genital Tumours, 5th ed.; IARC: Lyon, 2020; Vol. 4.
Figure 1.
Prevalence of hrHPV genotypes in different samples.
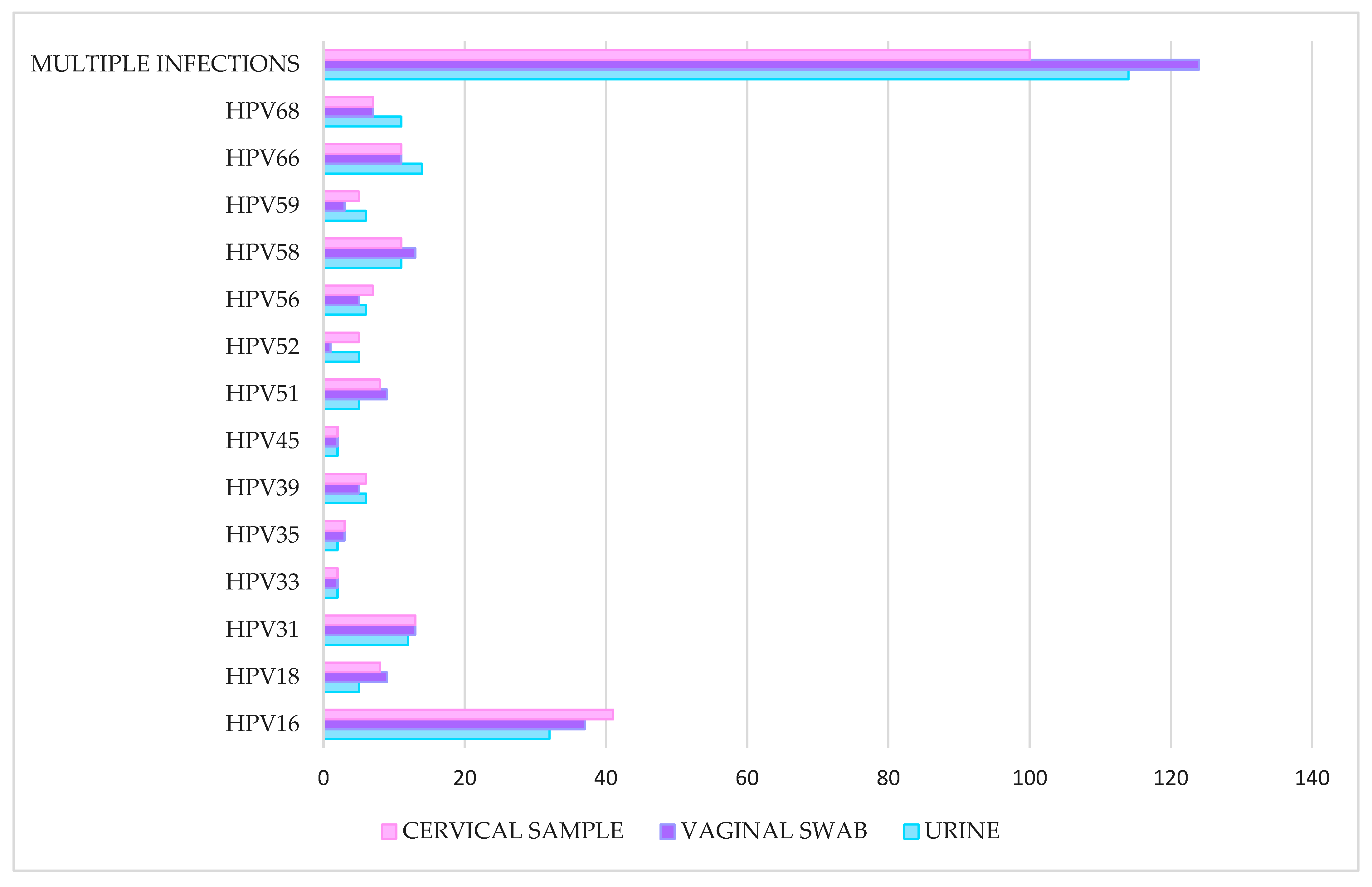
Figure 2.
Comparison of hrHPV (a) and STI (b) prevalence by age group.
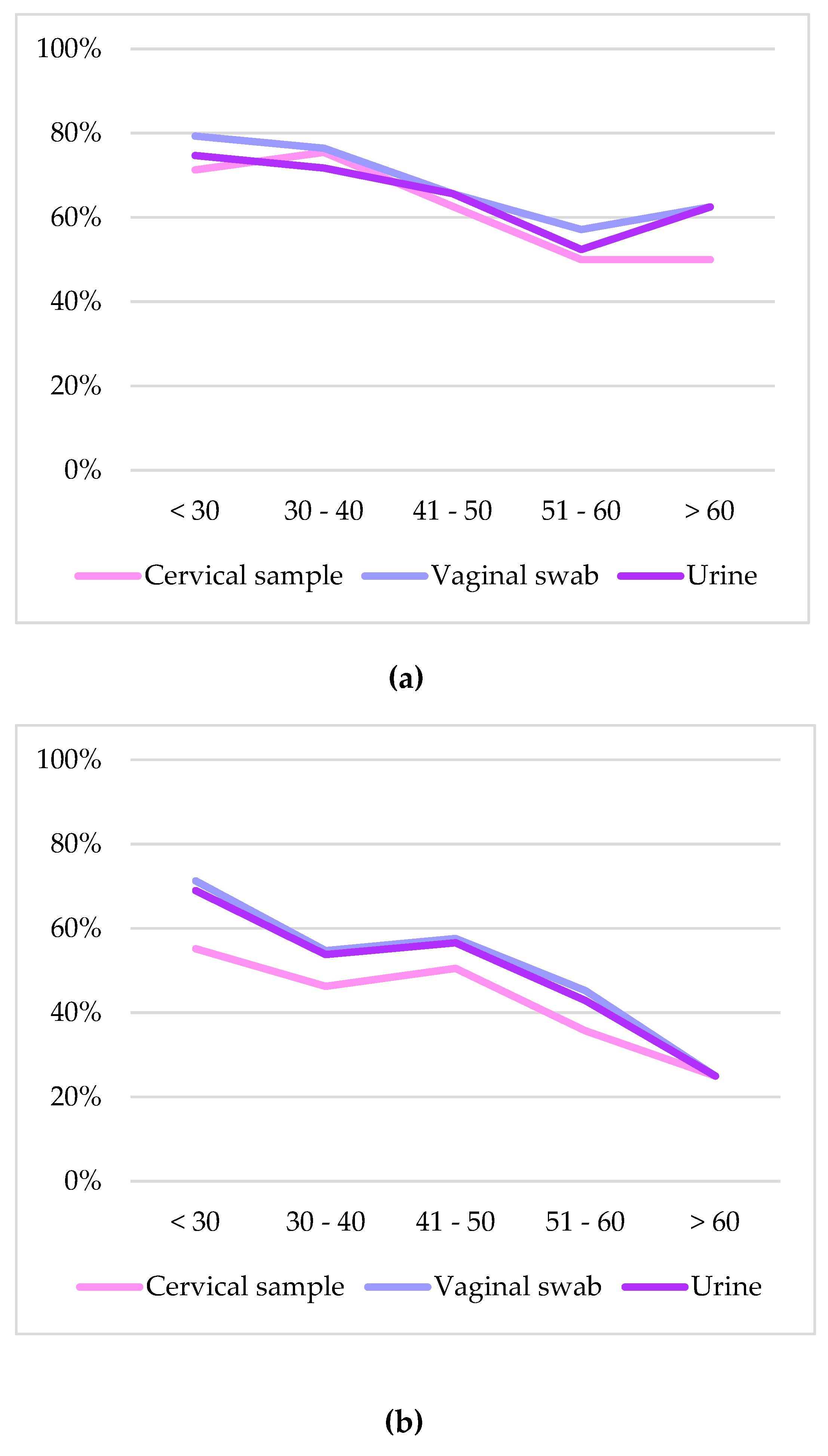

Table 1.
Clinical data of the study group.
| Cytology (n = 345) | N | % |
| HSIL | 47 | 13.6% |
| ASCH | 26 | 7.5% |
| LSIL | 164 | 47.5% |
| ASCUS | 86 | 24.9% |
| AGC | 14 | 4.1% |
| NILM | 8 | 2.3% |
| Colposcopy (n = 345) | ||
| POS | 127 | 36.8% |
| NEG | 218 | 63.2% |
| Histological outcome (n = 84) | ||
| Negative | 11 | 13.1% |
| CIN 1 | 13 | 15.5% |
| CIN 2 | 12 | 14.3% |
| CIN 3 | 44 | 52.4% |
| Cervical cancer | 4 | 4.8% |
HSIL (High-grade squamous intraepithelial lesion); ASCH (Atypical squamous cells—cannot exclude HSIL); LSIL (Low-grade squamous intraepithelial lesion); ASCUS (Atypical squamous cells of undetermined significance); AGC (Atypical glandular cells); NILM (Negative for intraepithelial lesion or malignancy); POS (Positive); NEG (Negative); CIN 1 (Cervical intraepithelial neoplasia grade 1); CIN 2 (Cervical intraepithelial neoplasia grade 2); CIN 3 (Cervical intraepithelial neoplasia grade 3).
Table 2.
Single and multiple infections caused by hrHPV.
|
Cervical sample n. (%) n = 229 |
Vaginal swab n. (%) n = 244 |
Urine n. (%) n = 233 |
|
| Single hrHPV | 129 (56.3%) | 120 (49.2%) | 119 (51.1%) |
| 2 hrHPV | 58 (25.3%) | 77 (31.6%) | 65 (27.9%) |
| 3 hrHPV | 30 (13.1%) | 24 (9.8%) | 27 (11.6%) |
| More than 3 hrHPV | 12 (5.2%) | 23 (9.4%) | 22 (9.4%) |
Table 3.
Type-specific agreement and test concordance between cervical and vaginal self-samples.
| HPV type | +/+¹ | +/- | -/+ | -/- | Agreement [%] | Kappa² [95% CI] | |
| hrHPV | 227 | 2 | 17 | 96 | 94.4 | 0.870 (0.814 - 0.927) | |
| HPV16 | 79 | 1 | 7 | 255 | 97.7 | 0.936 (0.893 - 0.980) | |
| HPV18 | 18 | 0 | 4 | 320 | 98.8 | 0.894 (0.791 - 0.997) | |
| HPV31 | 44 | 2 | 9 | 287 | 96.8 | 0.870 (0.795 - 0.945) | |
| HPV33 | 10 | 5 | 3 | 324 | 97.7 | 0.702 (0.506 - 0.898) | |
| HPV35 | 7 | 0 | 4 | 331 | 98.8 | 0.772 (0.556 - 0.988) | |
| Total | HPV39 | 19 | 1 | 2 | 320 | 99.1 | 0.922 (0.835 - 1.000) |
| population | HPV45 | 10 | 2 | 5 | 325 | 98.0 | 0.730 (0.539 - 0.922) |
| (n = 342) | HPV51 | 26 | 0 | 10 | 306 | 97.1 | 0.823 (0.717 - 0.929) |
| HPV52 | 27 | 3 | 3 | 309 | 98.2 | 0.890 (0.804 - 0.977) | |
| HPV56 | 25 | 0 | 4 | 313 | 98.8 | 0.920 (0.842 - 0.998) | |
| HPV58 | 24 | 2 | 8 | 308 | 97.1 | 0.812 (0.699 - 0.925) | |
| HPV59 | 19 | 0 | 4 | 319 | 98.8 | 0.899 (0.800 - 0.997) | |
| HPV66 | 33 | 1 | 8 | 300 | 97.4 | 0.865 (0.779 - 0.951) | |
| HPV68 | 27 | 2 | 8 | 305 | 97.1 | 0.828 (0.724 - 0.932) |
Table 4.
Type-specific agreement and test concordance between cervical and urine self-samples.
| HPV type | +/+¹ | +/- | -/+ | -/- | Agreement [%] | Kappa² [95% CI] | |
| hrHPV | 214 | 15 | 19 | 94 | 90.06 | 0.773 (0.701 - 0.845) | |
| HPV16 | 68 | 12 | 11 | 251 | 93.3 | 0.812 (0.738 - 0.886) | |
| HPV18 | 14 | 4 | 3 | 321 | 98.0 | 0.789 (0.638 - 0.941) | |
| HPV31 | 43 | 2 | 6 | 291 | 97.7 | 0.901 (0.834 - 0.969) | |
| HPV33 | 10 | 5 | 3 | 324 | 97.7 | 0.702 (0.506 - 0.898) | |
| HPV35 | 7 | 0 | 6 | 329 | 98.2 | 0.692 (0.459 - 0.924) | |
| Total | HPV39 | 16 | 4 | 4 | 318 | 97.7 | 0.788 (0.645 - 0.930) |
| population | HPV45 | 9 | 3 | 2 | 328 | 98.5 | 0.775 (0.584 - 0.966) |
| (n = 342) | HPV51 | 23 | 3 | 11 | 305 | 95.9 | 0.745 (0.617 - 0.872) |
| HPV52 | 24 | 6 | 2 | 310 | 97.7 | 0.775 (0.584 - 0.966) | |
| HPV56 | 25 | 0 | 5 | 312 | 98.5 | 0.901 (0.816 - 0.987) | |
| HPV58 | 21 | 5 | 8 | 308 | 96.2 | 0.743 (0.609 - 0.877) | |
| HPV59 | 18 | 1 | 4 | 319 | 98.5 | 0.870 (0.758 - 0.982) | |
| HPV66 | 31 | 3 | 11 | 297 | 95.9 | 0.793 (0.689 - 0.897) | |
| HPV68 | 23 | 6 | 17 | 296 | 93.3 | 0.630 (0.492 - 0.769) |
hr (high-risk); HPV (Human Papillomavirus); CI (confidence interval); n (number). ¹ +/+ positive on self- and cervical samples, +/- positive only on cervical samples, -/+ positive only on self-samples, -/- negative on both sample types. ² Kappa concordance between the self- and clinician-collected cervical samples is presented as follows: slight (0.00 < κ < 0.20), fair (0.21 < κ < 0.40), moderate (0.41 < κ < 0.60), substantial (0.61 < κ < 0.80) and almost perfect (0.81 < κ < 1.00).
Table 5.
Distribution of STI pathogens in the three sample types.
| UP n (%) | UU n (%) | MH n (%) | MG n (%) | CT n (%) | NG n (%) | TV n (%) | |
| Cervical sample (n = 342) | 129 (37.7%) | 34 (9.9%) | 31 (9.1%) | 8 (2.3%) | 11 (3.2%) | 0 (0%) | 4 (1.2%) |
| Vaginal swab (n = 342) | 165 (48.2%) | 40 (11.7%) | 40 (11.7%) | 11 (3.2%) | 13 (3.8%) | 0 (0%) | 3 (0.9%) |
| Urine (n = 342) | 158 (46.2%) | 38 (11.1%) | 39 (11.4%) | 10 (2.9%) | 11 (3.2%) | 0 (0%) | 3 (0.9%) |
Table 6.
Single and multiple STI infections.
|
Cervical sample n. (%) n = 164 |
Vaginal swab n. (%) n = 198 |
Urine n. (%) n = 193 |
|
| Single STI | 122 (74.4%) | 143 (72.2%) | 141 (73.1%) |
| 2 STIs | 32 (19.5%) | 38 (19.2%) | 39 (20.2%) |
| More than 2 STIs | 10 (6.1%) | 17 (8.6%) | 13 (6.7%) |
Table 7.
Type-specific agreement and test concordance between cervical and vaginal self-samples.
| STI | +/+¹ | +/- | -/+ | -/- | Agreement [%] | Kappa² [95% CI] | |
|
Total Population (n = 342) |
STI | 162 | 2 | 36 | 142 | 88.9 | 0.779 (0.714 - 0.844) |
| UP | 127 | 2 | 38 | 175 | 88.3 | 0.764 (0.697 - 0.831) | |
| UU | 30 | 4 | 10 | 298 | 95.9 | 0.788 (0.681 - 0.895) | |
| MH | 31 | 0 | 9 | 302 | 97.4 | 0.859 (0.769 - 0.949) | |
| MG | 8 | 0 | 3 | 331 | 99.1 | 0.838 (0.657 - 1.000) | |
| CT | 11 | 0 | 2 | 329 | 99.4 | 0.914 (0.795 - 1.000) | |
| NG | 0 | 0 | 0 | 342 | 100 | Not Applicable | |
| TV | 3 | 1 | 0 | 338 | 99.7 | 0.856 (0.576 - 1.000) |
Table 8.
Type-specific agreement and test concordance between cervical and urine self-samples.
| STI | +/+¹ | +/- | -/+ | -/- | Agreement [%] | Kappa² [95% CI] | |
| STI | 156 | 8 | 37 | 141 | 86.8 | 0.738 (0.668 - 0.808) | |
| UP | 121 | 8 | 37 | 176 | 86.8 | 0.732 (0.660 - 0.804) | |
| UU | 26 | 8 | 12 | 296 | 94.1 | 0.690 (0.562 - 0.817) | |
| Total | MH | 27 | 4 | 12 | 299 | 95.3 | 0.746 (0.627 - 0.864) |
| population | MG | 8 | 0 | 2 | 332 | 99.4 | 0.886 (0.729 - 1.000) |
| (n = 342) | CT | 9 | 2 | 2 | 329 | 98.8 | 0.812 (0.632 - 0.992) |
| NG | 0 | 0 | 0 | 342 | 100 | Not Applicable | |
| TV | 3 | 1 | 0 | 338 | 99.7 | 0.856 (0.576 - 1.000) |
STI (sexually transmitted infection); CT (Chlamydia trachomatis), NG (Neisseria gonorrhoeae), TV (Trichomonas vaginalis), MH (Mycoplasma hominis), MG (Mycoplasma genitalium), UU (Ureaplasma urealyticum) and UP (Ureaplasma parvum); CI (confidence interval); n (number). ¹ +/+ positive on self- and cervical samples, +/- positive only on cervical samples, -/+ positive only on self-samples, -/- negative on both sample types. ² Kappa concordance between the self- and clinician-collected cervical samples is presented as follows: slight (0.00 < κ < 0.20), fair (0.21 < κ < 0.40), moderate (0.41 < κ < 0.60), substantial (0.61 < κ < 0.80) and almost perfect (0.81 < κ < 1.00).
Table 9.
Distribution of STI pathogens in hrHPV-positive and negative women in the three sample types. *p < 0.05; **p < 0.01; ***p < 0.001.
Table 9.
Distribution of STI pathogens in hrHPV-positive and negative women in the three sample types. *p < 0.05; **p < 0.01; ***p < 0.001.
| UP | UU | MH | MG | CT | NG | TV | |||||||||
| n (%) | p | n (%) | p | n (%) | p | n (%) | p | n (%) | p | n (%) | p | n (%) | p | ||
| Cervical samples |
hrHPV-positive (n = 229) |
102 (44.5%) | *** | 27 (11.8%) | 0.15 | 29 (12.7%) | *** | 8 (3.5%) | 0.06 | 10 (4.4%) | 0.11 | 0 (0%) | 1 | 3 (1.3%) | 1 |
| hrHPV-negative (n = 113) |
27 (23.9%) | 7 (6.2%) | 2 (1.8%) | 0 (0%) | 1 (0.9%) | 0 (0%) | 1 (0.9%) | ||||||||
| Vaginal swabs |
hrHPV-positive (n = 244) |
137 (56.1%) | *** | 32 (13.1%) | 0.27 | 37 (15.2%) | ** | 11 (4.5%) | 0.04* | 12 (4.9%) | 0.12 | 0 (0%) | 1 | 2 (0.8%) | 1 |
| hrHPV-negative (n = 98) |
28 (28.6%) | 8 (8.2%) | 3 (3.1%) | 0 (0%) | 1 (1.0%) | 0 (0%) | 1 (1.0%) | ||||||||
| Urine | hrHPV-positive (n = 233) |
125 (53.6%) | *** | 30 (12.9%) | 0.18 | 34 (14.6%) | ** | 9 (3.9%) | 0.18 | 10 (4.3%) | 0.18 | 0 (0%) | 1 | 2 (0.9%) | 1 |
| hrHPV-negative (n = 109) |
33 (30.3%) | 8 (7.3%) | 5 (4.6%) | 1 (0.9%) | 1 (0.9%) | 0 (0%) | 1 (0.9%) | ||||||||
Table 10.
Distribution of hrHPV-positive cervical samples according to clinical data.
| hrHPV positivity on cervical sample n (%) | |
| Age in years (n = 342) | |
| <30 | 62/87 (71.3%) |
| 30-40 | 80/106 (75.5%) |
| 41-50 | 61/99 (61.6%) |
| 51-60 | 21/42 (50.0%) |
| >60 | 4/8 (50.0%) |
| Cytology (n = 342) | |
| NILM | 1/8 (12.5%) |
| ASCUS | 52/85 (61.2%) |
| AGC | 5/14 (35.7%) |
| LSIL | 112/162 (69.1%) |
| ASCH | 21/26 (80.8%) |
| HSIL | 38/47 (80.9%) |
| Colposcopy (n = 342) | |
| Negative | 126/217 (58.0%) |
| Positive | 103/125 (82.4%) |
| Histology (n = 84) | |
| < CIN 2 | 16/24 (66.7%) |
| ≥ CIN 2 | 58/60 (96.7%) |
Table 11.
Distribution of hrHPV and STI co-infection in cervical samples.
| hrHPV+ / STI+ | hrHPV+ / STI- | hrHPV- / STI+ | hrHPV- / STI- | Total | |
| Total population | 130 (38.0%) | 99 (28.9%) | 34 (9.9%) | 79 (23.1%) | 342 |
| Age in years (n = 342) | |||||
| <30 | 40 (46.0%) | 22 (25.3%) | 8 (9.2%) | 17 (19.5%) | 87 |
| 30-40 | 40 (37.7%) | 40 (37.7%) | 9 (8.5%) | 17 (16.1%) | 106 |
| 41-50 | 34 (34.3%) | 27 (27.3%) | 16 (16.2%) | 22 (22.2%) | 99 |
| 51-60 | 13 (31.0%) | 8 (19.0%) | 2 (4.8%) | 19 (45.2%) | 42 |
| >60 | 2 (25.0%) | 2 (25.0%) | 0 (0%) | 4 (50.0%) | 8 |
| Cytology (n = 342) | |||||
| NILM | 0 (0%) | 1 (12.5%) | 1 (12.5%) | 6 (75.0%) | 8 |
| ASCUS | 26 (30.6%) | 26 (30.6%) | 10 (11.8%) | 23 (27.0%) | 85 |
| AGC | 3 (21.4%) | 2 (14.3%) | 1 (7.1%) | 8 (57.1%) | 14 |
| LSIL | 71 (43.8%) | 41 (25.3%) | 15 (9.3%) | 35 (21.6%) | 162 |
| ASCH | 13 (50.0%) | 8 (30.8%) | 0 (0%) | 5 (19.2%) | 26 |
| HSIL | 16 (34.0%) | 22 (46.8%) | 7 (14.9%) | 2 (4.3%) | 47 |
| Colposcopy (n = 342) | |||||
| Negative | 73 (33.6%) | 53 (24.4%) | 28 (12.9%) | 63 (29.1%) | 217 |
| Positive | 57 (45.6%) | 46 (36.8%) | 6 (4.8%) | 16 (12.8%) | 125 |
| Histology (n = 84) | |||||
| < CIN 2 | 10 (41.7%) | 6 (25.0%) | 2 (8.3%) | 6 (25.0%) | 24 |
| ≥ CIN 2 | 29 (48.3%) | 29 (48.3%) | 2 (3.4%) | 0 (0%) | 60 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



