Submitted:
19 December 2024
Posted:
21 December 2024
Read the latest preprint version here
Abstract
The role of oxidants and antioxidants in inflammatory bowel disease (IBD) have been actively explored since the early 198Os, starting with the role of the respiratory burst of neutrophils and ischemia in bowel pathology. Since that time the enzymatic components contributing to the pool of reactive oxygen species including , superoxide, H2O2 and lipid hydroperoxides and the counteracting antioxidants, catalase, glutathione peroxidases (GPX), peroxiredoxins (PRDX), superoxide dismutases and others have been fleshed out. My perspective on IBD is from the role of the balance or imbalance of enzymatic oxidant sources and enzymatic antioxidants in the inflammatory process. I will present evidence on the involvement of oxidant and antioxidant processes in IBD, based as much as possible, on my experiences with GPXs. This will be about both the immune system and local bowel oxidant and antioxidant systems. As GPXs are generally selenium-dependent, possible deficiencies in selenium uptake in active IBD and the impact on GPX expression is explored. The more recently introduced ferroptosis, an iron-dependent lipid peroxidation based pathological process, will be reviewed for its possible involvement in IBD.
Keywords:
Inflammatory bowel disease
; GPX1-4
; PRDX
; NOX1
; DUOX2
; ileum
; colon
; immune system
1. Introduction
This discussion is not intended as an exhaustive foray into the area of oxidants, antioxidants, and inflammatory bowel diseases (IBD). With the exception of ferroptosis I am limiting it as much as possible to my experiences, which are largely constrained to studies of rodent tissues and human cancer-derived cell lines (GPX4 for this discussion), the consequences of eliminating oxidant and antioxidant enzyme expression, involving selenium-dependent glutathione peroxidases 1-4 (GPX), NADPH oxidases, NOX1 and DUOX2, and some limited work with superoxide dismutases (SOD)1 and 2 and catalase. Use of drug interventions in mice were intended to broaden the scope of our work to include lipoxygenases (ALOX), mitochondria, and xanthine oxidase (XO) as oxidant sources [1,2]. I will be not commenting on antioxidant supplements (selenium as an exception; trace elements copper, zinc and manganese will be briefly mentioned as components of superoxide dismutases), as these have consistently disappointed in large epidemiological and controlled studies and in some work, I have performed [1,2,3,4,5]. I am not a clinician nor an MD, so my knowledge of IBD comes from contact with co-workers who had IBD, what I have picked up from meetings where clinicians were present and from my reading. Briefly, Crohn’s disease (CD) and ulcerative colitis (UC) are chronic idiopathic inflammatory bowel disorders with periods of active illness followed by periods of remission. UC is confined to the large intestine, generally limited to the mucosa, while CD can impact any region of the alimentary tract with involvement of all layers and occasionally manifesting as inflammation of skin, eyes and joints, liver, or bile ducts. I refer the readers to the following papers for a superior discussion of the clinical features of IBD then I can supply [6,7]. IBD is referred to as an autoimmune disorder and there is a demonstrable genetic predisposition leading to active disease (NOD2 in CD as a notable genetic component) with stressors found to contribute such as infections or diet [8,9,10,11]. Gut microbe dysbiosis is thought to be a major component of IBD [12]. IBD cannot be cured, only managed, and the life span of sufferers may be slightly less than non-sufferers, with an increased risk for colon cancer due to the chronic inflammation [13,14]. In my limited contact with people who had IBD, I observed that they functioned productively, however, the condition could severely impact daily life, consistent with more general findings [15]. The enigma of IBD and a major concern is its increasing incidence in countries with lower socio-demographic indexes, where once it was negligible [16,17].
2. Enzymatic Oxidants, Antioxidants, and Inflammatory Bowel Disease
Suggestions for the involvement of oxidant and antioxidant enzymes in IBD and the use of antioxidant enzymes as therapy lagged 1-2 decades behind discovery of superoxide dismutase (SOD) and selenium-dependent glutathione peroxidase (GPX), gaining ground in the 1980’s (catalase by 80 years; named in 1900) [18,19,20,21,22,23,24,25,26]. The first mention of GPX in reference to IBD involves selenium deficiency in CD subjects in 1984, following 12 years behind the discovery that GPX1 is a selenoprotein [27,28]. Selenium deficiency in CD was noted 1 year earlier (3 years, anecdotally), without relating it to GPX [29]. Likewise, trace elements involved in SOD function, copper and zinc, components of SOD1,and manganese, component of SOD2, have altered levels in IBD, zinc and manganese less, copper possibly elevated. This impact on trace element levels has been suggested to link IBD to antioxidant enzyme malfunction [19,27,30,31,32,33,34,35,36,37]. Iron deficiency is also part of this pattern and actions to treat this have been suggested to occasionally backfire, although most evidence for adverse effects come from animal studies with chemically induced colon pathology [38].
3. The Main Players
There seems to be a large gap until the roles of another major antioxidant family, peroxiredoxins (PRDX), are discussed for in IBD, possibly 2010 [39]. PRDXs are thioredoxin-dependent peroxidases (PRDX6 exception, GSH-dependent). The gap may be due to the strong pathology found in Prdx1-knockout (KO) mice, that “produced pathology of hemolytic anemia and several malignant cancers, including lymphomas, sarcomas, and carcinomas”, but no ileocolitis, and in Prdx2-KO mice yielded “hemolytic anemia, splenomegaly, Heinz body formation, and morphologically abnormal red blood cells”, but no ileocolitis [40]. At the cellular level, loss of either PRDX1 or PRDX2 is not consistently impactful, although simultaneous loss does yield a noticeable effect on cell line oxidant levels [41,42,43,44]. The lack of IBD in the single KOs is not conclusive for lack of a role and possible counter-balancing roles in the immune system, shared with Gpx1, seems to offset any deficiency in local antioxidant protection in the ileum and colon [45]. Single KOs of none of the named antioxidant enzyme families produces spontaneous IBD in rodents. Sod2-KO is a neonatal lethal condition in mice. We looked at intestine samples from long-lived Sod2-KO mice (mitochondrial isoenzyme; on some strain backgrounds mice lived to 19 days) and observed nothing [46]. There are no reports of IBD like issues by use of heterozygous mice or an intestine specific Sod2-KO [47,48]. By way of introduction, superoxide is a radical species, the one electron addition product of oxygen, generated in several processes, but largely by electron leakage from the electron transport system of mitochondria [49]. As such, there is a dedicated mitochondrial SOD, SOD2 with manganese in the active site [50,51]. SOD1 is the cytosolic, zinc/copper active site, version. Superoxide can be damaging, largely by reactions with iron [52]. Superoxide is converted into H2O2, which can act as an antimicrobial agent as is (a pathway usually downstream of NADPH oxidase, NOX2), based on its damaging properties, or after additional reactions with hypohalous acids or thiocyanate that yield more potent antimicrobial species [53]. It is also a signaling agent, able to react with free cysteine residues of proteins to induce activation, inactivation, or structural changes [54]. PRDXs are a family of widely expressed, generally abundant peroxidases, collectively found in all cell compartments and proposed to consume the bulk (90%+) of hydroperoxides generated in cells. This is based on high rate constants and abundance [55]. While all are expressed in the ileum and colon, reports on KOs or rodents subject to knock-down of expression and chemically induced colitis largely showed less pathology, an effect often attributed to effects on the immune system (summarized in ref. 45) [45]. This greater impact on the immune system with chemically induced colitis was also found with a Gpx1-KO (and catalase-KO) mouse line and was also revealed (Gpx1-KO only) in a study of different responses of Gpx1-/-Gpx2+/+ and Gpx1+/+Gpx2-/- mice to allergen-induced airway inflammation (OVA and aluminum hydroxide asthma) [56,57,58]. GPX2 protects the lung from this condition, with Gpx2-KO mice having worse asthma, while lack of GPX1 mitigated the allergic response by suppressing Th2 and Th17 cell developmen . Gpx2 is not expressed in the immune system at significant levels.
One of the common suggestions dating back to 1984 is that impaired selenium uptake, associated with IBD, could constrain the levels of GPX1 and later GPX2, GPX3 and GPX4, all expressed in the ileum and colon [59]. The selenium-dependency of GPX1-4 and GPX6 is based on the co-translational incorporation of selenocysteine into the active site, giving the enzymes the capacity to operate efficiently at physiological pH (pKa ~5.2), although there are workarounds for cysteine (pKa> 8.4, thiolate anion is active form) centered peroxidases (PRDXs) that allow comparatively high ROOH rate constants (ROOH; H202, tert-butyl hydroperoxide, cumene hydroperoxide, linoleic acid hydroperoxide, etc.) [60]. Selenoprotein levels can reflect selenium intake when it is restricted, GPX1 more notably, but all are ultimately vulnerable [61,62,63]. This is noteworthy since the standard use of 10% serum in cell culture places most cell lines in the range of at least marginal selenium-depletion relative to tissues of selenium-sufficient subjects [61,63]. GPX4, the isoenzyme involved in iron, cystine, glutamine and lipid peroxidation-related cell death, ferroptosis, is as vulnerable and this might be factor in studies using cell lines [64]. Gpx2 is highly expressed in the epithelium of the mid-lower GI tract, and this is where we found its greatest impact in mice [46,65,66,67]. The study of Connie Eaves suggested that basal cell compartments, which would include the crypt/gland regions of the mid-to lower GI tract, reverse the standard PRDX dominance (90+% of ROOH reduction) in favor of GPX2 prominence for ROOH metabolism [55,68]. We found high levels of GPX2 more concentrated in the crypt/gland regions in rats [69]. GPXs1-4 are all expressed in the GI tract, with GPX2 confined to the epithelium, GPX1 and GPX4 in all layers and GPX3 in the mature absorptive cells and adherent to the basal lateral membrane [70,71].
3. Finding Overlapping Roles of GPX1 and GPX2 in the Intestine by Peeling Back the Layers of Antioxidants
Single KOs of Gpx1 and Gpx2 did not reveal obvious GI pathology. Our initial attempts to find a function for GPX2 using chemically induced colitis in wild type and Gpx2-KO mice did not turn up anything dramatic, so we turned to gamma-irradiation as a stress based on old, proposed links between GPX activity and prostaglandin levels and, at that time, a recent study showing the impact of Cox1 post-irradiation expression [72]. Whole body gamma-irradiation of mice resulted in an increase in the ileum epithelium GPX activity in wild-type mice, and GPX2 activity in Gpx1-/-Gpx2+/+ mice, but not GPX1 activity (Gpx1+/+Gpx2-/- mice), and not in the jejunum [66]. The magnitude of the increase in the mRNA and the timing, post-irradiation, mimicked cyclooxygenase 1 (COX1; PTGS1 gene) expression and PGE2 production in a prior study, upon which our study was modeled [72]. We were unable to tie PGE2 levels in the irradiated ileum epithelium to GPX activity levels with statistical significance, possibly by looking at Gpx1-/-Gpx2+/+ vs. wild-type instead of Gpx1+/+Gpx2-/- mice. Later work would link GPX2 to expression with suppression of COX2 expression and older literature consistently associated COX activity with low GPX activity [73,74,75,76]. Finally, we did not identify any protective effect of GPX2.
Given the co-expression of Gpx1 and Gpx2 in the gut, it was natural to test the impact of combining the Gpx1-KO and Gpx2-KO constructs to look for effects. We were aware of PRDXs and their suggested roles, although at that time the rate constants were estimated to be fractional of GPXs and inactivation of PRDXs under ROS stress, actively built into eukaryotic PRDX structure, was still widely discussed [77,78]. We included Prdx6 (Aop2) in our irradiation study. This knowledge and the still live debate over GPX and catalase for a greater role in protection of hemoglobin from oxidation meant that our estimation of the odds of finding an impact by combining the Gpx-KOs was 1 in 3 to 1 in 4 [79]. My experience with the main topic is largely limited to studies with mice lacking Gpx1 and Gpx2, in various combinations, Gpx1+/+Gpx2-/-, Gpx1-/-Gpx2+/+, Gpx1+/-Gpx2-/-, Gpx1-/- Gpx2+/- and Gpx1-/-Gpx2-/- [46]. The final combination, Gpx1/2-double knockout mice (Gpx1/2-DKO; mixed B6, 129 strain mice), resulted in spontaneous ileocolitis with high penetrance, the colitis onset prior to weaning and the ileitis peri- and post-weaning (21 days). This was also found at moderate penetrance in GPX1+/-Gpx2-/- mice and was largely suppressed in GPX1-/-Gpx2+/- mice. The spontaneous inflammation in Gpx1/2-DKO mice arises pretty much where Gpx2 expression is detected at appreciable levels, beginning at the junction of the jejunum and ileum and continuing to the rectum, and later tumors arise in the ileum and colon from the chronic inflammation (microadenoma onset at 3 months, resulting in distress to some mice by 6 months) [46,80]. The shift in the handling of the oxidant load from peroxiredoxins to GPX2 must occur at this point in the small intestine and continue into the colon. While we have conjectured this might be related to levels and types of microbes, it could also represent something related to the function of the ileum.
The condition is unique in that the pathology manifested as excess crypt/gland base (ileum/colon) apoptosis and the likely source of inflammatory pathology, crypt/gland base anoikis [1]. The apparent initiation of the pathology from within the crypt/gland epithelial cells coupled with lack of strong inflammatory infiltration in the mice confounded some pathologists we worked with, one of whom suggested on first examination of the histology that the pathology represented graft-versus-host disease. The scale of the apoptosis and the mixed nature of the abscesses (many exfoliated epithelial cells only, some mixed, few neutrophils only; IBD is dominated by neutrophils only and mixed) contributed to this impression. We eventually performed an MPO/cleaved caspase-3 differential analysis to confirm the epithelial cell only, mixed and neutrophil only calls from H&E, as recommended [81,82]. Anoikis or exfoliation/extrusion/shedding of intestinal cells occurs at the lumen as the terminal phase of enterocyte life [83]. It is a protracted process that is leaky to lumen components and excess anoikis has been linked to recurrence of Crohn’s disease [84,85]. While we provided no formal evidence of this, the correlation of ileitis timing and severity with crypt anoikis was very strong. Apoptosis, in the absence of anoikis, as found in Gpx1/2-Duoxa-triple knockout mice, did not result promote formation of neutrophil only and mixed crypt abscesses, a characteristic inflammatory pathology of the Gpx1/2-DKO mice [1,46].
4. Any application to IBD?
In a phrase, the outcome with Gpx1/2-DKO mice has little to do with IBD, although some suggestions do arise from the findings. Gpx1/2-DKO mice are not a model of anything based on the classical definition. They represent the fact of GPX1/2 loss in the GI tract of mice and the simultaneous loss of GPX1 activity in the immune system, which is not enough to turn the tide away from ileocolitis; loss of local protection trumps impact on immune function. As artificial as it was, this peeling back of multiple layers of antioxidant protection allowed unveiling of major sources of oxidants in the ileum and colon, showed that PRDXs do not dominate ROOH metabolism in all tissue compartments and allowed some estimation of the relative impact of GPX1 and GPX2. Since this was eventually connected to the functioning of NOX1 and DUOX2 in the intestine, it would be a real demonstration of oxidant and antioxidant balance in the ileum and colon and an extreme example of the result of loss of that balance required for homeostasis. The one possible connection to IBD is the dramatically increased DUOX2 expression levels [1]. However, use of other KOs results in uncovering other oxidant sources and other pathways to IBD [19,45,58]. The problem with Gpx1/2-DKO mice is that GPX1 and GPX2 levels are suppressed too much to be model of the impact of low selenium intake in IBD subjects and at the same time do not account for the simultaneous suppression of the other 23 (mice) or 24 (human) selenoproteins, GPX4 in particular, with its link to ferroptosis [62]. The better model for this is dextran sodium sulfate (DSS) induced colitis after selenium deprivation of mice, although this yielded mixed outcomes in practice [30,31].
5. Low Selenium Levels in IBD
The low selenium link in IBD remains a suggestion to me, as the degree to which impairment of selenium uptake would have to occur to approximate the GPX levels of Gpx1/2-KO mice and even Gpx1-/-Gpx2+/- mice with ¼ the activity of wildtype and still completely protective, would be unapproachable. More telling, we selenium-depleted young Gpx1+/-Gpx2-/- and Gpx1-/-Gpx2+/- mice, so that the ileum epithelial GPX activity was 6-12% of the selenium sufficient controls, also Gpx1+/-Gpx2-/- and Gpx1-/-Gpx2+/- mice, finding the Gpx1+/-Gpx2-/- mice developed pathology while the Gpx1-/-Gpx2+/- mice did not [86]. One study shows GPX activity (upper colon?) in CD subjects to be about ½ the levels relative to healthy controls [87]. In line with this, plasma selenium levels in an IBD cohort were down to 75 ng/ml in one study and 60 ng/ml in two others, with a small number (3 of 54 subjects in one study and 1 subject of 30 in another) in the 40-50 ng/ml range after stratification into the worst clinical disease index category, relative to ~95 ng/ml as adequate [88,89,90]. Meta analysis found IBD subjects had between 61% and 100% the plasma selenium levels of controls [91]. Even the worst subjects had levels above that reported for the populations of China that experienced Keshan disease, an endemic cardiomyopathy (~20 ng/ml, resulting in blood plasma GPX activity 33- 43% of sufficient subjects [92,93]. IBD was not reported as a symptom of Keshan disease, recognizing that low selenium would not be a root cause of IBD only a potentially aggravating factor. In Keshan disease coxsackie virus is thought to be involved as a co-factor [94,95]. Anecdotal evidence for 5 pediatric subjects on parenteral nutrition for intestinal pathology during a shortage of selenious acid for 3 months showed no increased signs of pathology, although serum selenium levels dropped down to Keshan disease levels [96].
Notwithstanding, there is evidence from mouse models of DSS-induced colon injury that selenium supra-supplementation might be beneficial, 30 papers found using search terms, selenium, DSS, and mice, although lately the focus has shifted to GPX4 and ferroptosis. There is a study with DSS treated mice showing that selenium deficiency (0.01 ppm vs 0.1 adequate; torula yeast base; ref. AIN-76a, 0.11 ppm; AIN-93, 0.15 ppm) did not significantly worsen the pathology while supra-selenium supplementation (0.5 ppm) augmented colon GPX1/2 protein levels, and this possibly contributed to reduced pathology [97,98]. This study also found that COX2 was repressed and COX1 was elevated. A second study on selenium deprivation in mice with DSS (basal diet contained less than 0.01 mg Se per kg; Se-deficient; torula yeast base; the Se-sufficient diet was the same diet supplemented with 0.25 mg Se as sodium selenite per kg) did find a major worsening in pathology [30]. The discrepancy might be due to the second paper using a selenium level greater than standard for the selenium sufficient group. The blood plasma GPX activity levels were 10-fold lower in the selenium deficient group, more than difference in levels between selenium sufficient and deficient human subjects in Keshan disease studies. Another paper found that high selenium (oral gavage, daily) impacted T cells, fewer Th1/Th17 cells more Tregs, and lowered pathology levels [31]. Similar impact of selenium supplementation lessening DSS pathology levels is found in other papers [99,100].
As a rule, selenium supplementation is most effective when the subjects are initially selenium-deficient, and risks may outweigh benefits by trying to increase levels in selenium adequate subjects [102]. The results from rodent studies indicate that supra-supplementation might be effective in IBD subjects balancing out the poor selenium uptake and even possibly yielding higher expression of GPXs than in the selenium adequate condition. Clinical trials are lacking or so limited in covering disease signs as to provide little useful information [103,104,105].
6. NADPH Oxidases and Pathology in Gpx1/2-DKO Mice and Normal Function in Wild Type Mice
The ileocolitis in Gpx1/2-DKO mice was linked to expression of both Nox1 and Duox2, demonstrated in triple KO mice, Gpx1/2-Nox1-TKO, and Gpx1/2-Duoxa-TKO, where complete absence of disease was found in the former and the inflammation and anoikis were absent and the apoptosis was retained in the latter [1,82]. The NOX1 connection makes sense, as it is expressed in the crypt region and in human tissues shares high expression in colon tissues with GPX2 [106,107,108,109]. DUOX2 is normally found in the lumen region and this localization may be preserved in the Gpx1/2-DKO mice, no change in expression levels with pathology progression. Our examination of human IBD tissue showed that the range of DUOX2 protein expression was expanded into the gland base region [1]. This could explain part of the generally reported up-regulation of DUOX2 mRNA expression in IBD samples [110,111]. A recent paper describes expansion of a LCN2, NOS2, and DUOX2 expressing cell type (LND) in Crohn’s disease (CD) that interacts with inflammatory cells [112]. Rare in non-IBD tissues, they are detected as almost 20% of total epithelial cells in active CD; this may be a partial replication our finding. The LCN2 component is linked to ferroptosis by involvement with iron levels [113]. In mice, lumen constrained DUOX2 could transmit oxidant signals to the crypt by way of a proposed cell-to-cell transmission mechanism; direct diffusion of H2O2 from the lumen to the crypt/glands is considered unlikely [114]. The ability of GPX1 to limit ileocolitis in mice of the Gpx1+/-Gpx2-/- and more so in the Gpx1+/+Gpx2-/- genotypes, suggests some damping of the DUOX2 oxidant signaling could occur via this proposed cell-to-cell transmission mechanism with Gpx1 expression.
My take on this is very one sided, limited to what occurs when DUOX2 and NOX1 operate in the absence of the required antioxidant protection; there are enough oxidants generated to initiate apoptosis and the related anoikis. While overactive oxidant generation by NOXs, including NOX2, respiratory burst NOX, has been discussed as a factor in IBD, the flip side has gained traction, with chronic granulomatous disease and an associated IBD, caused by NOX2 deficiency, the classic example [115,116]. The absence of a detected role for NOX2 in Gpx1/2-DKO mice pathology (indicated by absence of pathology progression beyond excess apoptosis in Gpx1/2-Duoxa-TKO mice and general absence of pathology in Gpx1/2-Nox1-TKO mice) may be due to the timeframe over which we generally examined the pathology (birth- (colon) or ileum 21 days to 35-40 days of age) and milder early onset colon pathology in mixed strain and B6 mice. Here only NADPH oxidases operating in the pre-onset and peri-onset ileum pathology would be influencing the processes. Infiltration of possible Nox2 expressing cells was not detected until 27-28 days of age in B6 mice (where we have an extensive timeline of events), rare neutrophil bearing abscesses observed at 28 days and higher levels of infiltration in the mucosa and crypt abscesses occurring at and after 30 days of age [1,2]. Neutrophil bearing abscesses, while a consistent feature, were never abundant in the B6 strain ileum. Direct testing in Nox2-KO mice showed mixed outcomes with DSS, worse outcomes in four studies vs. one no change and one less pathology [117,118]. A currently promoted view is that impairment of NOX1 and DUOX2 by congenital mutations are involved in very-early onset IBD and defects in NOX2 mimicking CD [119,120]. Although, strong support for very-early onset IBD and NOX1 was not backed up by another study [121]. DUOX2 mutations are linked to congenital hypothyroidism. While the condition is rare (1/2000-4000), up to 40% of cases show mutation in the DUOX2 gene [122]. The over-expression of DUOX2 observed with later onset IBD would represent a possible opposing side of the impact [110,111]. However, with the association to the LND cell type, the impact in IBD is not clear. NOX1 levels do not increase to the same degree as DUOX2 in later onset IBD and the differences often do not approach statistical significance. The reverse pattern was found in Gpx1/2-DKO mice.
NOX1 function in the lower GI may be related to induction of active cycling of quiescent stem cells and distribution of cells between the secretory and proliferative roles [123,124,125]. Under-expression seems to limit the ability to repopulated damaged areas of the mid-to -upper crypt or even higher areas [126,127]. This is somewhat at variance with our experience of mitigation of pathology and return to normalcy in the triple knockout, suggesting a more subtle role for NOX1 that can almost escape notice or is somehow compensated by the Gpx2-KO condition. In Gpx2-KO mice, a similar subtle redistribution of proliferating cells seems to occur, observed as reduced levels of Lgr5 [128]. Two studies, one very recent and both focusing on the ileum, suggest that lack of NOX1 activity may limit the generation of peroxynitrite, the product of superoxide and nitric oxide from nitric oxide synthase (NOS) [129,130]. Knaus et al note that the lack of peroxynitrite seems to increase the exposure of the epithelium to bacterial antigens [130]. GPXs could protect from the direct tissue damage of this process by reacting with peroxynitrite [131]. Absence of NOX1 in the antimicrobial role in C57B6 strain mice may be unnoted due to the functioning Paneth cells and for animal resource centers housed mice, absence of pathogens. We received Nox1-KO mouse colon tissue slides (H&E stained) from another facility and noted some scattered focal epithelial cell loss and subsequent restitution (Fig. 1). Our animal facility would not accept the mice for presence of pathogens.
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
On the negative side, Dixon et al, suggest that NOX1 would participate in ferroptosis by reacting with Fe+++ to yield Fe++ that would be freed from storage to participate in lipid peroxidation [132]. It was clear from the study of Gpx1/2-Duoxa-TKO mice that cells were undergoing apoptosis under the stress of NOX1 function, by absence of crypt abscesses and absence of excess monocyte infiltration. Ferroptosis is inherently inflammatory. Another suggestion for the role of NOX1 is depletion of GSH by consuming NADPH [133]. While evidence of increased iron is shown in human IBD samples and DSS-colitis samples, the demonstration of GSH depletion was found in CACO2 cells with TNF-α and IL1-β treatment. TNF-α and IL1-β levels were substantially elevated in the colon of DSS treated mice. This markedly increases the level of NOX1 protein in the cells, which are at moderate to high levels to begin with in CACO2 relative to most COAD-derived cell lines [109]. The reduction in GSH levels was about 30%. While significant, it is not clear that this would compromise GPX4 and PRDX6 activity. Loss of viability in CACO2 cells seemed to require the added stimulation of hepcidin, which in the presence of TNF-α and IL1-β, increased cellular iron stores and lipid peroxidation. Some controls are not presented so the actual impact of hepcidin cannot be fully evaluated. The link between NOX1 and GSH has been examined before, with the opposite outcome [134].
DUOX2’s role would seem to be at least a moderate interaction with the microbiota. While H2O2 alone could have some impact on the microbiotia, it would be a substrate for lactoperoxidase, generating the more potent hypothiocyanite and other hypohalous acids [53]. Based on our take on the impact of knocking out Duox2 expression in Gpx1/2-DKO mice, we were more interested in the up to 25 or more-fold increase in DUOX2/DUOXA2 levels in IBD and the possible damaging impact on the tissue. The finding of an expanded population of LND cells as at least one reason for the indicated increase in DUOX2 expression in IBD complicates our simple notion, suggesting that the increased expression is linked to a package of alterations to enterocytes (one proposed source of LND cells) which have an augmented interaction with immune cells. The specific role of DUOX2, if any, is unclear, and the authors of the LND paper make no comments about this other than to point out that under stress, ileum and colon cells tend to express genes of other lineages [111,112,135]. Grasberger and associates suggested that up-regulation of Duox2 in mice germ-free mice exposed to bacteria was a response to dysbiosis and expression did not sustainably alter the redox status of the mouse epithelium defined as no changes in antioxidant enzyme levels [136]. Thus, the normal presence of GPXs and PRDXs are adequate to buffer the H2O2 released in dysbiosis. The intermediary between the microflora and DUOX2 was shown to be NOD2 with a strong history of linkage to Crohn’s disease by way of GWAS studies and a sensor of muramyldipeptide, derived from bacterial cell walls [137,138]. As dysbiosis is one factor in IBD, there is the possibility of a viscous cycle of pathology driven by alterations in the microbiota that feed back to perpetuate the condition [139,140]. From the evidence presented, NOX1 and DUOX2 would be factors to prevent initiation of disease by limiting the exposure of the epithelium to the microbiota. Their proper function dependent on the fairly reliable presence of antioxidant enzymes.
7. Other Sources of Oxidants
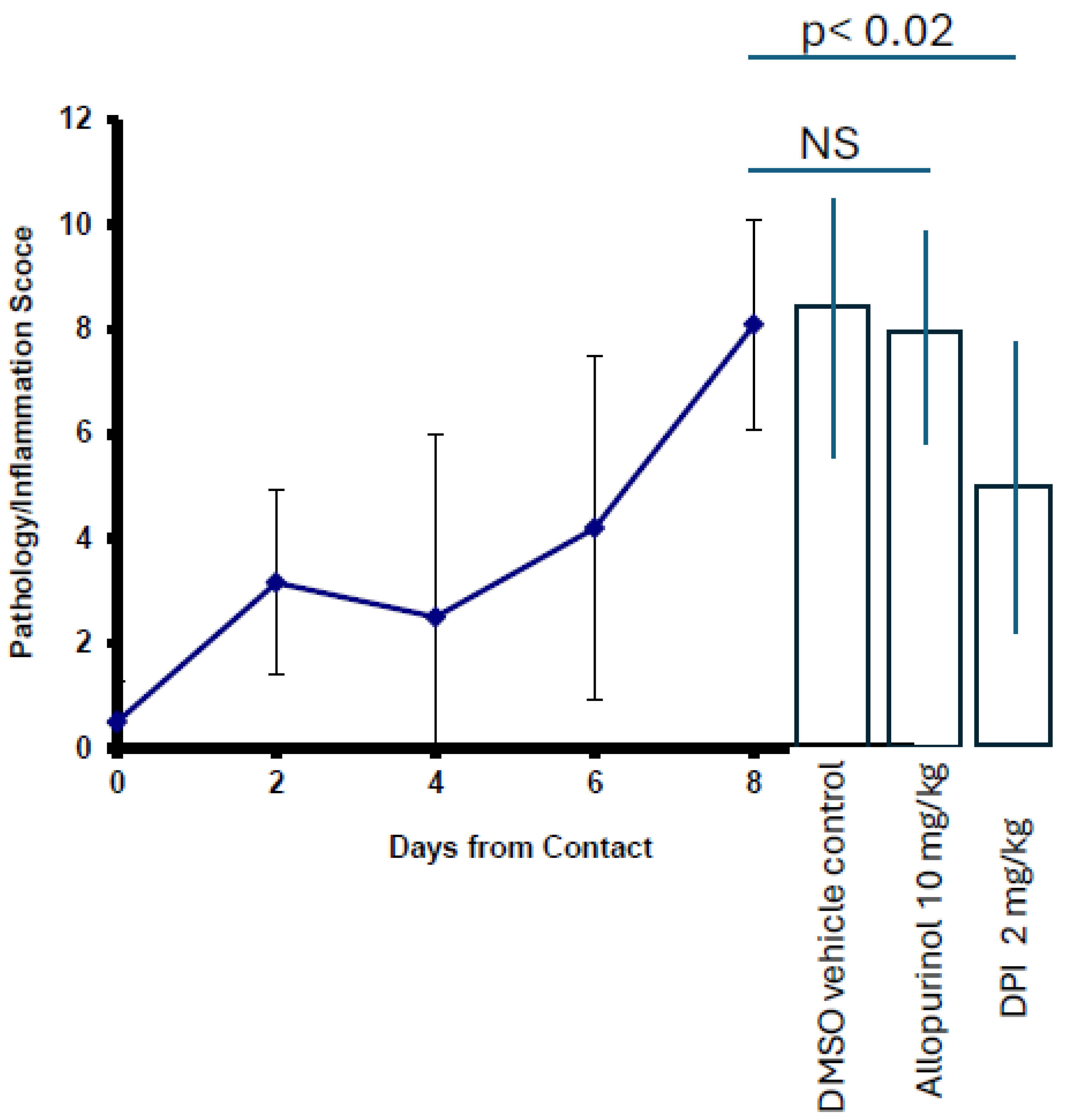
As to other sources of oxidants, xanthine oxidase (XO) , lipoxygenases (AlOX ), and mitochondria have been considered and as later discussed, monooxygenases of the P450 system. Gashler et al ruled mitochondria out as required for ferroptosis, a form of oxidant driven pathology that seems to be operative, at least, in experimental colitis [141]. Our own effort to examine this using MitoQ® (Coenzyme Q10 conjugated to the lipophilic triphenylphosphonium cation to accumulate in mitochondria), revealed a moderate impact that rivaled DTI (pan-NADPH oxidase inhibitor) but did not rise to the level of the Gpx1/2-Duoxa-TKO mice [1,142]. Kruidiner et al and Reynolds et al did not find increased XO protein in UC and CD subjects [143,144]. However, the XO inhibitor, allopurinol has been found to be somewhat effective in humans and more consistently effective in the DSS model of colitis with one dissenting outcome from 4 studies [145,146,147,148,149,150,151]. The minority finding suggests the other action of XO inhibition by allopurinol, purine salvage, was the cause of increased pathology [151]. Allopurinol has been a part of IBD therapy since 2005 when it was found to reduce toxicity related to the use of thiopurines, a cheaper means of therapy used in less developed countries [152]. While the work on XO does not address ferroptosis directly, the implication that DSS induced colitis involves ferroptosis is suggestive for such a role. Given the strong role of NOX1 and DUOX2 in the pathology of Gpx1/2-DKO mice, it is not surprising that allopurinol did not suppress pathology. We studied this in the context of exposing six to seven months-old Gpx1/2-DKO SPF mice (specific pathogen free; derived from a germ-free colony) to bedding from our original colony. We reported that young SPF exposed to the bedding tolerated the exposure with ramifications of cancer at 8 months of age [80]. At six-eight months ileum pathology was nearly completely resolved in the Gpx1/2-DKO SPF cohort [80]. Over the course of 8 days after exposure, the SPF mice showed a violent reaction often requiring euthanasia, with a commensurate increase in the ileum pathology score (N=11 at 8 days). Daily IP injection of allopurinol (10mg/kg, IP; standard dose for mice; n= 6) failed to prevent the increased pathology, while diphenyleneiodonium (DPI, 2mg/kg; n=11), a pan-NOX and DUOX inhibitor, provided some protection in this model and as reported in our later work using the less toxic derivative, di-2-thienyliodnium (6 mg/kg; DTI), on young DKO mice [1,80,153,154,155
[80].
Figure 2.
Effect of allopurinol and DPI in mitigation of pathology in ileum of SPF Gpx1/2-DKO mice over 8 days following exposure to soiled bedding from mice of the original colony. Day zero mice, n=8. DMSO control, n=4. Using DPI as model, N=6 statistical power is 0.85, p≤ 0.05.
Figure 2.
Effect of allopurinol and DPI in mitigation of pathology in ileum of SPF Gpx1/2-DKO mice over 8 days following exposure to soiled bedding from mice of the original colony. Day zero mice, n=8. DMSO control, n=4. Using DPI as model, N=6 statistical power is 0.85, p≤ 0.05.
Similar results were found in the ileum treating mixed strain Gpx1/2-DKO mice with DTI from weaning to 40 days of age (untreated and mock PBS treated ileum pathology score, 7.2±1.9 (Std), n=19), with the toxic effect of DPI (obstruction at the gastroduodenal junction) as much a factor as its healing impact (N=7, with 5 others withdrawn for morbidity; ileum pathology score of 5.6 ±2.7, p=0.12; statistical power of 0.9, p ≤0.05, using a semi-purified AIN-76A diet impact on mixed strain mice as the model positive effect, ileum pathology score 4±3.5, p=0.002, n=26) [156]. The goal was to uncover pathways causing pathology in the mice by looking at broad spectrum of drugs in small groups of mice, effectively looking for miraculous impact. In this quick and dirty drug screen, we found that Trolox (12mg/kg, IP, to 40 days of age; 25mg/kg was not tolerated by the weanling mice; 7 mice, ileum pathology score 7±1.7, p=0.9), a water-soluble form of vitamin E, did not impact pathology, unlike in DSS pathology with induction to promote cell death by hepcidin to tie the impact to ferroptosis (Trolox; 30mg/kg, adult mice, 3 days) [133,156,157]. Caffeic acid (20mg/kg IP; 9 mice, ileum score 5.2±2.2, p=0.028) and DPI, and not allopurinol, seemed marginally effective with deferoxamine (n=5, ileum score 6±1.6, p=0.18; statistical power= 0.75) coming in third as compounds not yielding miracles, but at least worth follow-up. A later follow up showed caffeic acid was ineffective in B6 Gpx1/2-DKO mice at dose of 60mg/kg (daily oral gavage) [1]. This could be due to the difference in the genetic background or route of delivery [156,158]. We generally lost interest in searching for effective drugs beyond NOX and DUOX inhibitors (DPI, DTI and others) when we found that semi-purified AIN diets produced the strongest and most consistent moderation of pathology across all mouse backgrounds and sites and this appeared to involve alterations in the microflora [156,158].
Lipoxygenases (ALOXs) seem to have a role in ferroptosis, seemly discovered before the term was coined, with some of the hallmark features of the phenomenon fleshed out in a 2008 paper [159]. This was found in the context of GPX4 suppression, a theme that is continued when discussing the roles of ALOXs and other factors contributing to ferroptosis. Lipoxygenases can peroxidize non-esterified polyunsaturated fatty acids (PUFA) downstream from the action of PLA2s and have a requirement for activation by ROOH to yield Fe+++ in the active site [160]. As discussed below, the action of PLA2 may be anti-ferroptopic with later binding to fatty acid binding proteins producing ambiguous outcomes. This suggests that the most efficient way to the excess lipid peroxidation state of ferroptosis is within the cell membrane. The role of ALOXs was unclear, seemingly able to contribute, but not necessary; in some papers it is suggested is that ALOXs are initiators of the peroxidation [161]. Part of the problem might have stemmed from multiple mechanisms of suppression of ferroptosis by presumed ALOX inhibitors, with some action by direct lipid radical trapping [162]. For ALOX15 there is an apparent modification of its peroxidation potential in the presence of PEBP1, “scaffold protein inhibitor of protein kinase cascades” [163]. This allows ALOX15 to peroxidize esterified PUFAs, giving it a role in the more efficient membrane route of peroxidization. We looked at NDGA, a pan ALOX inhibitor, mentioned in the PEBP1 study, as part of our quick and dirty drug screen (N=5, 10mg/kg IP, ileum score 6.3±1.3, p=0.44, statistical power 0.75) [164]. Use of the drug yielded the marginal results generally found in this screen and it was not pursued. This mention of ALOXs leads into the final topic, ferroptosis.
8. Ferroptosis, the 800-Pound Gorilla in the Room
To my detriment, I basically ignored ferroptosis except to note the role of GPX4 and now the explosion of studies makes it difficult to perform more than a rudimentary summation (15,000 papers) [64]. I did not find ferroptosis to be novel. Lipid peroxidation initiation by Fenton chemistry was well documented by the time I entered the free radical research field as it was self-titled in 1987 (Society of Free Radical Biology and Medicine), and the initial work on lipid peroxidation can be dated to 1963 [165,166]. The essential role of cystine for cell culture and association with GSH and vitamin E was reported in 1977 [166]. My time spent collaborating with Ursini and Maiorino on the characterization of GPX4 in human cell lines and reading up on their discovery of the enzyme activity reinforced my knowledge this process and the roles of iron, GSH (cystine), GPX4 and PUFAs [168,169]. The ferroptosis inhibiting iron chelator, deferoxamine, was always stocked in the lab and was used in two studies of Gpx1/2-DKO mice (negative results mentioned but not shown in the final paper; B6 background), finding marginal impact on over all ileum pathology (250mg/kg, IP, daily; ileum pathology score=5.8±1.6, p=0.18, N=5 in the fast drug screen, statistical power 0.7, p≤0.05) as opposed to findings in the rodent colitis models, although the levels of apoptosis and anoikis were subdued but not eliminated in the samples (Fig. 3) [1,170,171,172,173].
Deferoxamine failed to sustain Paneth cell numbers, which we showed were depleted by both the apoptosis and anoikis routes by direct evidence and inferred from the outcomes in Gpx1/2-Duoxa-TKO mice vs. DKO mice. In sets where exfoliation was found so were neutrophil only and mixed crypt abscesses; 10 of 21 mice in the DKO set, 2 of 7 mice in the deferoxamine set, 10 of 25 mice in the DTI set, 1 of 19 mice in the Gpx1/2-Duoxa-TKO set. The ileum and colon lengths were not restored with deferoxamine (ileum-30.74 cm deferoxamine (D) vs. 29.74 cm DKO and ~37.5 cm for non-DKO and both TKO sets; colon-8.14 cm D vs. 8.9 cm DKO, and ~10.5 cm for non-DKO and both TKO sets), nor with DTI (ileum-30.1 cm; colon 7.7 cm) [1]. This is contrary to results with the DSS model [174]. A role for labile iron is noted in apoptosis, so that some suppression of intrinsic apoptosis might be expected with chelation [175,176]. Unleashing my cynical side, if I were convinced that ferroptosis can be found almost everywhere (an impression from the literature), the apparent depression of some marker levels in the Gpx1/2-KO mice by deferoxamine could be pushed as evidence.
My first impression of ferroptosis was that it is a manufactured mode of cell death. That is, you had to add multiple unnatural stresses to cells to observe it, deplete GPX4 (possible with low selenium levels in IBD and which might the standard condition of cell lines in culture), starve cells of cystine, overdose them with glutamine and iron, etc., so that was unlikely to be found naturally [180,181]. The value of the revelation was by way of providing more pharmacological (Stockwell, team lead for introduction of ferroptosis, and team members goal) and genetic interventions to reduce pathologies or attack cancers. The only original observation suggesting it might arise in a useful setting was RAS mutations were linked to increased free iron content in cancer-derived cells in the initial papers on erastin [180,181]. As related by Stockwell, the RAS mutated Bej cell line (skin derived fibroblast line) was engineered to be tumorigenic and follow up analysis on tumor-derived lines bearing RAS mutation did not find consistent ferroptosis sensitivity, reinforcing my impression of the contrived nature of ferroptosis [182].
My point of contact is the isolation of the cDNA for human GPX4 and finding the mitochondrial insertion sequence [183]. I worked on the initial characterization of GPX4 in human cancer-derived cell lines with Ursini and Maiorino, and collaborated with A.W. Girotti, who has extensive experience with GPX4 and was a co-author on the 2014 paper that suggested GPX4 was a key factor in ferroptosis [169,184,185]. The 2014 paper also used a cell line, COHBR-1, that I helped characterize for GPX protein expression, showing COHBR-1 cells and 2 other cell lines did not express GPX4 [64,186]. The latter findings, lack of any need to invoke ferroptosis as a source of pathology in Gpx1/2-DKO mice (Fig. 3) and a lack of impact of silencing GPX1 (GPX2 surrogate; GPX2 not expressed) on BJeLR cells, while silencing GPX4 was lethal, are the reasons I generally ignored ferroptosis [64]. One side note is that silencing GPX7 and GPX8 did have some impact on viability of BJeLR cells. These are not selenoproteins; they are ER residents and thought to be involved in protein folding [187]. The absence of an impact by silencing of GPX1, in hindsight, is not as convincing now as then. PRDXs tend to dominate for ROOH metabolism, as indicated. I did not hear of Winterbourn’s upward revised estimates of PRDX rate constants (PRDX1/2, comparable to GPX1; PRDXs more abundant) indicating PRDX dominance until 2012-2013 (Society for FRBM meeting), and probably resisted the implication that my work to date had been with enzymes that generally seem to have a minor role [41,55]. Inactivation of PRDXs under ROS stress, actively built into eukaryotic PRDX structure, was still widely discussed leaving a way GPX1/2 could be important as we found in Gpx1/2-DKO mice [77,188].
There is now a small body of literature suggesting that ferroptosis is a factor in IBD, publications starting in 2020-2021 (10, excluding reviews and mouse models; 85 including rodent models, with some of these mixing human sample derived information, and many using only bioinformatics) and the finding that sulfasalazine, a mainstay of IBD therapy inhibits ferroptosis (from the 2012 ferroptosis paper), which I missed [189]. I still regard ferroptosis, in most instances, as one of the branching end points of severe pathology, a variant of necrosis (essentially failed apoptosis), and dependent on too many processes failing [190]. Alternatively, it could be viewed as an outcome of autophagy responding to cystine deprivation and consequently degrading ferritin [191]. Most refer to ferroptosis as a form of regulated cell death, which is true from the standpoint that the genes involved are, of course, subject to regulation and importantly pharmacological or genetic inhibition or augmentation. A few persist in calling it program cell death, which I reject. For me to be convinced of that ferroptosis has that status in IBD, I would have to see evidence of advanced priming of some cell types for a ferrotopic response or the opposite, enhanced resistance (strong expression bias of genes involved), followed with experimental evidence to show how this would function in a natural setting or logically as a response to stress. As shown below, there is possibly some evidence of this, while there are more signs not of advanced priming to specially promote cell death or resistance but of predilections in metabolism and/or mutations rendering a few cell types susceptible, some by input of common environmental stresses, such as a high fat diet, iron supplementation for IBD subjects or glutamate usage as found in the nervous system [192,193,194]. The metabolic predilections seem to serve positive functions of the cells rather than being intentional precursors for ferroptosis activation [195,196]. The two more studied environmental factors both in humans and rodent models are high fat or western diets and iron supplementation, the latter used as IBD subjects are often depleted of iron as with selenium. Searching for DSS and high fat diets turned up 31 papers, only 2 on ferroptosis, one of the two using DSS/AOM [197,198]. Of these 27 suggest a negative impact while 4 claim a beneficial impact. Impact on the microbiota is the most reported finding with the immune system second and two mentions of impact on epithelial cells. Searching for iron supplementation or dietary iron (to weed out papers only mentioning iron or only measuring tissue iron levels) and DSS yielded 19 papers, four on ferroptosis. The outcomes are mixed, with two finding that both low and excess iron are bad in this model and one finding both an initially damaging effect of iron and a subsequent healing regenerative effect by way of stimulating stem cells [199,200,201]. The impact of iron in these studies is attributed to the epithelium, neutrophils and largely to the microbiota composition [202,203,204,205,206,207,208].
My second issue with ferroptosis is the fact that went from being almost nowhere in 2012 to being almost everywhere in a few years (PubMed; 2015 being arguably the real launching point). It seems too easy to demonstrate and this flies in the face of redundant controls on oxidative stress, iron, and cell membrane lipid metabolism [208,209,210]. Dating back to my attendance of Gorden conferences in the early 1990s, the question was, where was the labile iron? [211]. The ease of inducing ferroptosis in cell lines may involve use of the common protocol of applying ferroptosis inducing agents on unintentionally GPX4 depleted cell Iines (10% serum) in a high oxygen environment to detect influences on the process [212]. While I entertained the notion that low selenium levels in cell culture would render many cell lines vulnerable to ferroptosis in my Linkedin account posts, a recent paper found this to be factual [63]. Also, a newly published pre-print finds that standard adherent 2D cell culture primes cell lines for ferroptosis with low levels of stearoyl-CoA desaturase (SCD) resulting in high levels of cell membrane PUFAs relative to 3D culture [213]. SCD was also indicated to be an activity that could compensate for GPX4 and PRDX6 by in silico analysis [214]. This paper also suggests that PRDX6 might augment GPX4 levels by simulating the supply of selenocysteine, found in other work. The effects of ferroptosis markers, indicated from human samples, may be amplified to the level of apparent significant effects in cell lines under these conditions, regardless of their impact in tissues. None the less, Stockwell recently reviewed evidence that ferroptosis has been detected in natural processes like red blood cell maturation and the pathophysiology of anti-viral immunity and tumor suppression [215,216,217].
As shown below, experiments largely based on the DSS mouse model, likened to ulcerative colitis (UC), suggest ferroptosis is directly involved in death of epithelial cells and strongly influenced by death or resistance to death in several immune cell types, although adaptive immune cell action in the DSS model is not absolutely required and the microbiota can be depleted [218,219,220,221,222]. The involvement of oxidative stress in IBD through the immune system is strongly suggested in the Prdx- and Gpx1-KOs as shown above. This could be linked to ferroptosis both in the immune cells and epithelial cells of the gut by control of non-esterified lipid peroxides.
GPX4 has its impact on esterified lipid hydroperoxides, showing propagation of lipid peroxidation in cell membranes is a unifying feature of ferroptosis [223]. Several studies using different methods suggest that action on non-esterified lipid hydroperoxides is important and allow for an effect of ROOH metabolizing enzymes, like GPX1/2 and PRDX1-5, with PRDX6 in a crossover role [224,225,226,227,228,229,230,231]. The intermediaries for generation of non-esterified lipid hydroperoxides are phospholipase A2 activities (PLA2). The PLA2 activities could suppress ferroptosis by two means: first cleavage of esterified lipid hydroperoxides and release from the membrane for reduction by GPXs or PRDXs with less membrane distortion consequently and, second, upon activation by the presence of lipid hydroperoxides and protein kinase C, exhibiting a somewhat selective removal of arachidonic acid (AA), the main peroxidizable fatty acid constituent of cell membranes from the sites of lipid peroxidation propagation [232,233,234]. PLA2s have been shown to confer resistance to ferroptosis [235,236]. However, in the CNS PLA2 activities are noted for increasing lipid peroxidation [237].
A combination of PLA2 activity and reduction of non-esterified lipid peroxides is found with PRDX6. PRDX6 has a standard hydroperoxidase activity and GPX4 activity, which might be comparably high, and a PLA2 activity at acid pH [238,239]. The relative roles of GPX4 and PRDX6 would depend on expression levels and the importance of the independent PLA2 activity of PRDX6. PRDX6 overexpression could not compensate for GPX4 loss in Pfa1 cells (fibroblasts), while FSP1 did (FSP1 catalyzes the regeneration of CoQ10 using NADPH) [240,241,242]. PRDX6 did inhibit ferroptosis in GPX4 intact cells by increasing the supply of selenium delivery in cells and therefore GPX4 levels [243,244]. A study in lung presents a different story, with the 5-fold higher protein levels of PRDX6 over GPX4 conferring the major resistance to ferroptosis, induced in vitro. This involves action of both the ROOH/GPX4 activity domain and the PLA2 activity domain. The peroxidase and PLA2 activities are in separate protein domains and can be individually impaired by mutation and were studied, independently [245]. PRDX6 also has a lysophosphatidylcholine acyl transferase activity that may also explain its ability to remodel cell membrane composition and impact ferroptosis susceptibility [246,247].
After release, the fatty acids and oxidized derivatives are subject to binding by fatty acid binding proteins (FABP). I was curious about how this would impact reduction of lipid peroxides by GPX3, using defatted serum albumin, the major fatty acid binding protein in blood plasma and linoleic acid hydroperoxide as a model lipid ROOH. Serum albumin inhibited the action of GPX3, presumably through steric hindrance and/or less diffusion and I cautioned against using high levels of serum albumin as stabilizing agent in the GPX assay with substrates like linoleic acid [248]. The action of FABPs could simplistically have a dual impact, beneficially sequestering membrane distorting fatty acid hydroperoxides and peroxidable AA and detrimentally hindering reduction of non-esterified lipid hydroperoxides by GPX1/2 and PRDXs, limiting this route of lipid hydroperoxide detoxification. Serum albumin is not a good model for the action of cytosolic FABPs due to its high Kd (10-6M) while cytosolic FABPs have a Kd ranging from 3 nM to 1000 nM [249,250,251]. On the flip side, lipid peroxidation can be either promoted or inhibited by FABPs with variety of mechanisms proposed for each, some of which stray far beyond simple sequestration and steric processes [249,250,251,252,253,254,255]. Generation of non-esterified free fatty acids by the action of PLA2 activity may result in an overall protective effect based on reduction of membrane distortion that might favor less membrane peroxidation and loss of peroxidable AA. The ambiguous actions of FABPs provide no clear role in reducing ferroptosis vulnerability by binding the non-esterified products generated by PLA2 action. While indicated in some work, the actions of GPX1/2 and PRDX1-5 on non-esterified fatty acid hydroperoxides could be minor relative to GPX4 with PRDX6 being a sole exception, perhaps by its tripartite capacity as a PLA2, with action both on non-esterified fatty acid hydroperoxides and esterified fatty acid hydroperoxides. More papers suggest inhibition of ferroptosis by PRDX6 than the opposite, with a split over whether this action is more reliant on the peroxidase activity or the PLA2 activity with one paper suggesting both contribute, equally (search terms: PRDX6 and ferroptosis and not filtering for IBD; 16 papers) [245].
Ferroptosis could have three major points of impact in IBD, directly in the epithelial cells, the immune system and by influence on the microbiota or feedback from the microbiota. Claims for all have been made in the limited number of studies available. The study closest to my experience suggested that Western diets (fish oils added to mouse diet to increase peroxidizable arachidonic acid content) might increase the oxidizable lipid content of the epithelium and render it susceptible to ferroptosis [256]. This parallels findings in a paper to be discussed later, where this effect is assigned to Treg cells [257]. First, they show that the GPX4 protein levels in CD ileum samples and not colon samples were down by 50%, a possible consequence of low selenium levels, as discussed, although odd for the specific impact in ileum. Another paper does find colon GPX4 mRNA to be down by almost 2-fold in IBD colon (this second paper seems to be the first linking ferroptosis and IBD)[258]. Second, they assayed GPX activity, calling it a GPX4 assay. However, the substrate was cumene hydroperoxide. GPXs1-4 are all active with this substrate, GPX4 with a low rate constant relative to the rest [248]. So, this has little meaning for GPX4 and suggests a general reduction in GPX1/2 activity. GPX assays present a problem in the Yang et al (2014) paper as well [64]. As far as I can tell, the assay shown in figure 2F, suggesting inhibition of GPXs by erastin, omitted GSH (tert-butyl hydroperoxide; later it was included for the Phosphatidyl choline hydroperoxide and cholesterol hydroperoxide assays), and so is another assay of the GSH content of the samples and not GPX activity. Modern literature measuring tissue GPX activities is full of such errors [248]. An examination of mice heterozygous for GPX4 expression showed iron or arachidonic acid feeding produced pathology in the ileum, marked by neutrophil infiltration. Vitamin E protected against the arachidonic acid effect. Vitamin E is a chain-breaking antioxidant for lipid peroxidation and known for its interaction with selenium in pathology [259]. One major function would be to convert lipid hydroperoxyl radicals to hydroperoxides allowing GPX4 and PRDX6 to act. We found that feeding Gpx1/2-DKO mice a chologenic/lithogenic diet with high cholesterol, high fat and cholate (AIN-76A base) induced colitis beginning 4 weeks after introduction of the diet, however, cholate seemed to be the active agent, yielding high levels of deoxycholate in fecal pellets of Gpx1/2-DKO mice and the wild-type control; omission significantly reduced the morbidity [260]. These diets mark the single exception to the AIN base being preventative for Gpx1/2-DKO mouse colitis. We attributed the colitis to a disturbance of the unfold protein response, not looking for ferroptosis (this was 2010), reminiscent of the modest impact of silencing GPX7 and GPX8 in the Yang et al study, thought to be a factor in IBD from GWAS and other studies and, linked to autophagy, another factor in IBD [64,261,262,263]. The original colitis/ferroptosis paper mentioned above actually linked ferroptosis to ER stress [258]. That paper presents a limited marker analysis of human IBD samples, pointing to signs of ferroptosis sensitivity. Mice were subjected to DSS treatment. One important finding was that FER1, a ferroptosis inhibitor, reduced the levels of pathology in the mice, suggesting ferroptosis involvement [264]. Second, they showed signs of an ER stress response along the lines we did in the atherogenic diet study and showed that the PERK inhibitor, GSK2606414, lowered the pathology levels and Fe++ content of epithelial cells. Another paper using wild-type mice and DSS to induce colon pathology found that deoxycholate enemas produced conditions favoring ferroptosis in enterocytes, elevated Fe++, and ACSL4 protein and mRNA, lowered levels of GSH and GPX4 protein and mRNA, associated with increased pathology [265]. While not showing direct signs of ferroptosis, they found that apoptosis (TUNEL) and pyroptosis (marker analysis) were not elevated leaving, in their opinion, only ferroptosis as the factor producing the increased pathology. Preceding this demonstration, they showed that high fat diets (60% fat vs. 16% fat) aggravated DSS-induced pathology and found high levels of deoxycholate in the mouse sera. Finally, they linked Western-style, high fat content diet intake levels by correlation to ulcerative colitis severity in human subjects and to ferroptosis by measure of the markers, GPX4 (IHC, mRNA), DMT1(IHC) and HIF-2alpha (IHC), all showing modest but significant alterations favoring ferroptosis [266,267]. While not looking at ferroptosis, another group found that a deoxycholate enema following DSS administration increased IL-1β production in macrophages [268]. The Western-styled, and so-called pro-hyperplasia inducing Newmark diet (20% corn oil; AIN-76A; WD and WDCaD are Newmark diet with low vitamin D and calcium and with vit. D and Ca at AIN-76a levels) being a derivative of AIN-76A and lacking yeast, other components of LabDiet® mouse chows and cholate, nearly cured the ileum of Gpx1/2-DKO B6 strain mice shown as by the impact on apoptosis in the ileum and colon ( Fig. 4a) and reduced the morbidity of the Gpx1/2-DKO 129 strain mice (N10) (Fig. 4b) [156,260,269].
The apparent vitamin D/Ca effect was attributed to vitamin D3 inducing NOX1, based on the literature, and we did not confirm that [270]. Note, the 129 N10 Gpx1/2-DKO cohort (B6, 129 mixed strain mice backcrossed to 129) was difficult to manage due to extreme morbidity. The preventative impact of AIN diets made it possible to maintain and study this cohort. This differed from the N5 cohort, with moderate morbidity [156,158]. The difference was mapped to a locus on chromosome 2 containing the Duox2 gene, the sequence of which differs between B6 and 129, yielding alter enzyme activity [1,158]. Although we had indications from the use of DPI, it was that finding this led us to explore the roles of DUOX2 and NOX1 in Gpx1/2-DKO mouse pathology, over and above NOX2. The 2012 Dixon et al paper indicates that NOXs play some role in ferroptosis as a source of superoxide, however the specific suggestion that NOX1 is a prime candidate is not supported by the expression profile in the studied Calu-1 cells due to the similarly high expression of NOX2 which is a more potent source of superoxide [132]. Use of the NOX1/NOX4 inhibitor, GKT137831, provides some support for the claim [271]. In colon tissues, NOX1 could be a major source of superoxide before the onset of inflammation [109]. There is one paper suggesting high-fats diets reduce ferroptosis levels in DSS stressed mouse colon by increase uptake of cystine through the SLC7A11transporter (xCT) [272]. This group also reported that high fat diet increased pathology with DSS/AOM and ferroptosis marker levels, while showing, invitro in cancer-derived cells that high lipid exposure lowered ferroptosis by reducing CHAC1 levels, linked to less GSH degradation and less ER stress [273,274,275]. Chac1 was identified by us as one of ten top candidates, alongside Duox2, as an expression level variant with SNPs of unknown effect impacting pathology levels in the Gpx1/2-DKO mouse N5 vs. N10 study [276]. An additional paper on ferroptosis in human samples and DSS-induced colitis also reported the ER stress in the epithelial cells involving the PERK pathway was a major factor [258]. This study does not examine dietary fat. FER1 and deferoxamine were found to demonstrate an impact on the pathology level related to ferroptosis and the PERK inhibitor, GSK2606414, to show the effect of ER stress in epithelial cells in the DSS model. The study jumps to use of cell lines to examine this in detail [258]. Finally, the role NF-κBp65 was examined as an intermediary between ER stress and ferroptosis, finding that an IEC specific NF-κBp65-KO (floxed gene driven by Villin-cre) resulted in increased colon damage in the DSS model. The final assessment was that phosphorylated NF-κBp65 suppressed ER stress by interacting with eIF2α, component of the integrated stress response, which is linked to autophagy [275].
The remaining papers on ferroptosis in the epithelium largely nominate other factors for impact on GPX4 expression, iron uptake, cystine, glutamine, and lipid levels, suggest possible alternative therapies (the bulk promoting traditional medicines) or prognosis based on ferroptosis marker signature sets, a few of the latter mentioning GPX2. A limited number of the roughly 50 mouse/DSS studies (some with AOM) on ferroptosis employ inhibitors or inducing agent in the animals to advance the claim of a role in IBD [277,278,279,280,281]. The use of ferroptosis inhibitors is often limited to parallel studies on cell lines, with CACO2 being the most used. In many, the association is based on marker analysis with the assumption that ferroptosis is a fact in DSS-induced pathology and trusting that the change in marker levels indicate significant effects of the agents or pathways under study show an effect through ferroptosis. In summary, there is some evidence of ferroptosis in IBD, possibly confined to the active stages, where marginal to severe selenium deficiency might be present to impair GPX expression and possibly PRDXs by way of thioredoxin reductase (selenoprotein), the epithelium is under stress, ER stress and autophagy being candidates, and of course the effect of the immune infiltrate. High fat in diets and iron supplementation may be environmental factors that would push the stressed colon toward ferroptosis. Activation of NOXs and presence of DUOX2 outside of its usual boundaries could supply oxidants to fuel the lipid peroxidation.
Ferroptosis could impact the immune system with as great or greater effects on IBD outcome as anything in the epithelium. Limiting search terms to ferroptosis, immune system and inflammatory bowel disease, 9 papers emerged, with 4 being reviews; a few of the mouse studies look at immune function. The fact that the impact of some knockouts of PRDXs and GPX1 seem to operate largely on the immune response (exceptions will be noted below), despite expression in the colon, further suggests their minor contribution to crypt/gland base antioxidant protection, relative to the colon gland based confined GPX2, particularly in the context of lack of GPX1 [282]. There are opposing papers for PRDX4. One paper on PRDX4 shows a local colon effect with DSS treatment of PRDX4-/y mice and linked the pathology to ER stress, the ER being one of the sites for PRDX4 localization (recall GPX7 and GPX8). GPX1 and GPX2 levels were low with DSS in both wild-type and PRDX4-/y mice, attributed to iNOS expression, inactivation of GPXs by nitrosylation and possible destruction [283,284]. One difference from the PRDX4-KO/DSS/AOM cancer paper in addition to use of AOM is the background strain, FVB/N for the immune system DSS/AOM cancer effect and B6 for the local DSS colitis effect. A PRDX6-KO was also found to be protective from DSS-induced pathology; the effect suggested to be based on compensatory up-regulation of other antioxidants in epithelial cells of the gut by activation of NRF2 signaling [285]. Another study found an opposite effect of PRDX6 in association with ferroptosis [286]. Neither study examined possible immune involvement.
As indicated, ferroptosis in the immune compartments could impact IBD and this seems to be the case in DSS- and other mouse colitis models. The second paper under consideration for the impact of Western-style high fat diets, suggests a detrimental effect could be mediated through ferroptosis in the Treg population [257]. A key logical consideration in the study was that fats are absorbed in the upper small intestine, so that high-fat diets should not directly impact the colon. This is like my complaint that papers invoke iron uptake in the gut as a factor in IBD associated ferroptosis, when the absorption occurs in the duodenum and jejunum [287]. Supplemental iron, given to some IBD sufferers, is known to aggravate IBD and one case-control study found even high-end levels of normal intake affected IBD [288]. In two experimental studies, however, the effects of dietary iron were attributed to an impact on neutrophils (DSS) and the intestinal microbiota (TNFΔARE mice) [202,289]. The Treg lamina propria population numbers were less upon feeding high fat diet (60% calories fat) to mice, down to one-third the normal levels. In vitro, Tregs took up arachidonic acids more readily than Tconv cells, that made its way into the membrane phospholipids. The GPX4 levels were marginally lower with high fat diet, but similar to that in the Tconv population. The subsequent elevated cell death was reversible by ferrostatin-1. To make the link to a ferroptosis role in IBD, they made a mouse line with a Treg specific GPX4 conditional KO (Fox3 YFP-Cre, GPX4 F/F). The KO mice and the colon tissues were fine on standard diet by in several analyses and developed severe colitis and other problems on high fat diet. Treg populations were depleted. This could be replicated on normal fat diet with vitamin E depletion. High levels of vitamin E countered the high fat diet effect. Here there is an example of metabolic priming favoring ferroptosis, based on a preference of the cells for arachidonic acid for cell membrane phospholipids. I would not declare that the consequent high fat diet effect is an example of advanced priming of Treg cells specifically for a ferroptopic response as it leads to a greater level of pathology. While the demonstration of ferroptosis in based on the inherent preference of the T-cells for AA, it was dependent not only on a high fat diet but also forced, reduced expression of GPX4.
A second case involving alter AA usage in immune cells and ferroptosis, studies M2 macrophages [290]. The paper is prefaced with disappointment over the inability of 5-ASA to control IBD. It then jumps to ferroptosis as having been demonstrated in enough cases to justify studying FER1 as combination therapy with 5-ASA in UC. This study is an instance of not tipping the balance in favor of ferroptosis from the beginning by suppressing expression of one or more pathways involved before screening for an impact of another entity. DSS is used to induce colon pathology with the finding that products of lipid peroxidation, like 4-HNE, were not impacted by 5-ASA, nor were ferroptosis suppressing factors like GPX4 and FPS1 elevated. FER1 addition aided in reversing this trend, suggesting ferroptosis was occurring unaided. On the assumption that M1/M2 polarization is a key factor in IBD, they found that combination of FER1 and 5-ASA enhanced the numbers of M2 macrophages in association with lessening of pathology. Finally, they do prime the macrophages with Erastin treatment to examine the relative sensitivity of M1 and M2 population, finding M2 macrophages to be more sensitive to ferroptosis. They suggest that the combination of the action of the PLA2, Pla2g4a, and Ascl4 (acyl-CoA synthetase long-chain family 4), act to remodel the cell membrane in favor of ferroptosis by increasing levels of AA [291]. These findings reveal a possible negative impact of PLA2 activities in ferroptosis in conjunction with ASCL4.
A third paper suggests that observed up-regulation of GPX4 levels in IBD, act to suppress ferroptosis in the ILC3 population of innate lymphoid cells, found in the mucosa [292,293]. Again, this paper operates on the premise that ferroptosis is a fact in induced rodent models of colitis, some based on indirect evidence in prior work (iron chelator effects as discussed and marker analysis) and one direct application of FER1 in the TNBS model following marker analysis to suggest involvement of ferroptosis [257,294,295,296]. Using Citrobacter rodentum to induce inflammation, they show that activated ILC3 cells are resistant to ferroptosis in a GPX4-dependant manner (IEC specific Gpx4-KO), like findings in human samples, although the primary factor may be LCN2. The net effect of resistance to ferroptosis was a lessening of the pathology.
A final paper suggest intraepithelial lymphocytes (IEL) are subject to ferroptosis, due to expression of another source of oxidants, CYP1A1 (cytochrome P450 family monooxygenase), regulated by the aryl-hydrocarbon receptor (AHR) [297]. AHR is heavily involved in shaping the immune system of the intestine [298]. One action of CYP1A1 is generation of 19-HETE from AA [299]. However, the catalytic cycle of CYP1A1 can be disrupted leading to production of superoxide and H2O2 [300]. This demonstration of ferroptosis was dependent on eliminating Ahrr, a repressor of AHR in mice. This resulted in a 2-fold increase in CYP1A1 activity (3-fold mRNA) in IELs, increases in lipid peroxidation being the sole direct link to ferroptosis. The net effect was fewer IELs in the intestine, which renders the KO mice more susceptible to DSS [301]. Providing the Ahrr-KO mice with selenium or vitamin E lessened the lipid peroxidation in the IELs and restored IEL numbers. The link to ferroptosis in plausible but weak and was dependent on Ahrr status. The authors say their findings might reveal a vulnerability of the IELs in association with AHR function, which includes CYP1A1 up-regulation and gain of function mutations associated with IBD [302,303]. AHR is also a link to the microflora by being a receptor for microbial generated ligands, largely tryptophan derivatives like l-kynurenine [304].
Additionally, other studies have found evidence of ferroptosis in neutrophils and NK cells in other pathologies, like systemic lupus erythematosus and gastric cancer [305,306,307]. One NK study links L-kynurenine production in the cancer to ferroptosis by way of GPX4 suppression rather than CYP1A1, while a paper on neutrophils shows INFα promotes transcriptional repressor CREMα recruitment to the GPX4 gene. Collectively, a host of immune cell types and epithelial cells are subject to modulation by ferroptosis based on work to date. To the extent that the studies involve cell culture, the results might be taken with a grain of salt, as suggested earlier. Some papers depended on compromising the target cell type before ferroptosis could be demonstrated, then suggested ferroptosis would be a major factor in their regulation [307]. This would not necessarily indicate a natural mechanism of regulation, as sometimes suggested, but indicate pharmacological means to exploit for elimination of the cell types. This could be nuanced, depending on the ferroptopic Achilles’ heel of the cell types, AA uptake, GPX4 levels, cystine and iron metabolism.
The impact of experimentally altering or eliminating the microbiota of Gpx1/2-DKO mice dramatically affecting the levels of ileum and or colon pathology is just one example of many studies demonstrating the impact of the microbiota composition, with ours running counter to the list of usual suspects [80,308]. Papers on high fat diet and supplemental iron, generally with DSS, often report on alteration of the microbiota (over 31 papers on high fat diet and 19 papers on iron, with 2 high fat diet papers and 6 iron papers on ferroptosis) [174,309,310,311,312]. This is not the only significant finding in these papers, with adipose tissue leptin found to inhibit DSS induced colitis/ ferroptosis by impact on apoptosis pathways [313]. Supplemental iron was found to activate NF-kappaB to promote DSS-colitis [202]. Also, bucking the trend for a worse outcome from high fat, one group found an inhibiting effect on Slc7a11 (cystine/glutamate transporter, Xc-), resulting from high fat diets and DSS blunting ferroptosis [197]. Associations with the microbiota and DSS colitis extent to bacterial metabolites, such as butyrate and as previously mentioned, L-kynurenine. Low butyrate levels in DSS were found to be low and supplemented DSS treated mice with Na butyrate relieved the colitis and ferroptosis based on GPX4 as a marker [314]. High fat diet and resultant ϣ-6 PUFAs are thought to aggravate CD [315]. A variation on this theme is a more direct impact of bacteria on epithelial lipid peroxidation. Adherent-invasive E. coli is linked to IBD [316]. One group showed that adherent-invasive E. coli given to DSS treated mice stimulated lipid peroxidation by lowering GPX4 and ferritin heavy chain levels, yielding 4-hydroxynonenal as a marker of ferroptosis [317]. In conjunction with AA feeding (surrogate high fat diet condition) the pathology was worse. FER1 lowered the levels of pathology suggesting another link to ferroptosis.
9. Use of Markers for Identifying Ferroptosis
One question is, how much papers based largely on marker analysis suggesting a tendency for ferroptosis can be held as evidence? Ferroptosis has been detected in IBD, although sometimes by rather weak marker analysis, operating by way of the epithelial cells, components of the immune system and by participation of the microbiota. Following as many papers as I can, leads me the notion that ferroptosis is not everywhere but certainly pervasive. The skeptic in me does question the breath of these claims. If ferroptosis is occurring in so many components of IBD, could they somehow cancel each other out, not necessarily in DSS-induced pathology but the human counterpart? I wonder whether there is a middle ground of more controlled lipid peroxidation, involving ALOX/PEBP1, that could serve a signaling purpose and be misclassified as ferroptosis. Signaling pathways, including those derived from esterified lipids have been long proposed, along with the idea that not all lipid peroxidation would contribute equally to ferroptosis because of different impact of products on cell membrane integrity [318,319]. Iron chelators might have action by inhibition of ALOXs whether full blown ferroptosis is involved or not [320,321,322].
There is some reliance on 4-hydroxynonenal (4-HNE) and malondialdehyde (MDA) as markers of ferroptosis. 4-HNE production is not universally bad and has been reported to confer resistance to ferroptosis at low levels [323,324,325,326,327,328]. MDA is notoriously unreliable as a marker of oxidative stress or lipid peroxidation [329]. It has been reported that LiperFluo is superior to the more widely used C11-BODIPY (10-times more usage) as a marker of lipid peroxidation in cell membranes [330]. Other markers, based on mRNA or protein levels, are shown to be increased or decreased in levels with the suggestion of altered susceptibility to ferroptosis. As mentioned, the confirmation of the findings is often relegated to cell line work, where standard culture conditions may promote the tendency for ferroptopic responses [63,213]. There is some room for doubt that ferroptosis is occurring in all the reported instances or would occur without pre-manipulation.
One use of mRNA level marker analysis resulted what I consider a very odd result [331]. Sun et al. decided to evaluate UC subject clustering based on a possible bifurcation into ferroptosis and immune driven (neutrophil infiltration) types. It is not clear how they came to this idea. They reference their earlier paper, finding signs of ferroptosis in UC [332]. One side point in this paper is the exaggeration of ferroptosis marker level differences in DSS pathology relative to UC vs. healthy controls with another paper showing this for GPX4 [333]. Using machine learning tools, the group examined Geo datasets of UC subjects to find that the marker analysis produced 3 groupings, one for ferroptosis, another for infiltration with a third set of combined markers, close to 1/3rd of subjects each, with another set labelled quiescent. The ferroptosis set was low for immune infiltration, NK cells one exception (> mixed and neutrophil groups) and CD8+ T cells (= neutrophil group; low vs. mixed) and tended to resemble the quiescent set. Based on the proposed roles of NK cells and granzymes in IBD they may have inadvertently found 3 UC subtypes; not based directly on ferroptosis, rather the degree and type of immune involvement in UC in 3 phases (transition from active to quiescent and the reverse via mixed and ferroptosis like phases?) or patterns of the disease. The proposed importance was the ability to predict success of infliximab treatment. NK cell involvement in IBD has been examined with similar findings for golimumab or ustekinumab and for granzyme B (NK and CD8+ T cells) with infliximab without invoking ferroptosis [334,335]. Granzyme A (NK and CD8+ T cells) is reported to suppress ferroptosis [336]. However, IFNγ secretion by CD8+ T-cells or NK cells may shift epithelial cells in the direction of ferroptosis sensitivity [337,338,339]. Aside from the mix of possible outcomes of NK cell action, there are various findings, some contrary to others, for levels and types of immune cell infiltration in IBD using marker analysis.
10. Concluding Remarks: Ferroptosis in IBD
If the goal is to genuinely find new ways to impact diseases, the study of ferroptosis is of value. Neurodegenerative diseases studies may benefit [340]. Cynically, the explosion of papers suggests to me that many studies are based on a low bar for credibility fueled by hamstringing cell lines or other samples at the outset, so the results are skewed in favor of finding ferroptosis with an extra nudge. This is in addition to standard methodologies in cell line culture also favoring ferroptosis [63,213]. Is ferroptosis a thing in IBD? The conditions of full blown IBD could certainly yield factors favoring ferroptosis, low selenium intake, and increases in tissue macrophages and other infiltrating immune cells could favor alterations to iron distribution and other metabolic changes that could promote ferroptosis, operating like the imposed experimental conditions used by many to enforce ferroptopic outcomes [341,342,343,344]. An increased impact of ferroptosis in IBD might result from high fat diets and iron supplementation and this might also act on the immune system. So, yes, it may be real factor in IBD. The problem is sorting through papers with such claims for overly enthusiastic tinkering of the sample materials to skew the outcomes. Any prior manipulations must be consistent with real trends that might be occurring in IBD and because of dietary habits or supplementary iron for any specific cell type. Knocking down GPX4 expression or suppressing cystine uptake, for example, must be justified and the extent employed matched to actual effects. Our use of the Gpx1/2-DKO construct in mice is clearly going too far to demonstrate the impact of selenium in IBD and misses the mark both in the extreme reduction of GPX1/2 based on what is possible in humans and the failure to affect levels of the other selenoproteins, notably, but not exclusive to GPX4. This places real limits on the expanse of things I can say about IBD from the evidence of Gpx1/2-DKO mice. Claims for ferroptosis may be often exceeding the limits.
11. Concluding Remarks: Oxidative Stress in IBD
As to oxidants and antioxidants in IBD, the evidence from Gpx1/2-DKO mice shows that NOX1 and DUOX2 are generating enough oxidants to require the presence of at least some GPX2 (Gpx1-/-Gpx2+/- mice, even with low selenium levels). However, the possible surplus of GPX1/2 (wild type mice) seems more than capable of handling the load from the summed sources of oxidants even with low selenium intake (perhaps PRDXs have a role here; or the canceling of effects of immune system and the gut epithelium). This seems to be independent of GPX4 and possibly ferroptosis. The available GPX4 and PRDX6 seemed capable of limiting cell membrane lipid peroxidation to tolerable levels even with the low selenium intake in our study with Gpx1-/-Gpx2+/- mice [86]. Historically, NOX2 and XO were implicated in oxidative stress by way of studies of ischemia-reflow and mitochondria have been discussed for as long as I can recall [345,346,347]. Now the focus is on NOX1/NOX4, DUOX2, and ER stress. Since ROOH signaling can globally impact cellular processes, oxidant composition and levels are expected to affect IBD with roles in control of the microbiota another major another factor. Currently the exploration is based on under-performance of oxidant sources as much as overabundance of oxidants.
Author Contributions
RSE was responsible for all aspects of this publication.
Funding
This research received no external funding
Institutional Review Board Statement
NA
Informed Consent Statement
NA
Data Availability Statement
Queries about data in this article can be sent to the author; at either sesworthy@coh.org or srsesworthy@outlook.com
Acknowledgments
This paper is written partially to commemorate my 40 years at COH. Upon my retirement, I thank all my colleagues who have aided in the investigation of GPXs during that time.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Chu FF, Esworthy RS, Doroshow JH, Grasberger H, Donko A, Leto TL, Gao Q, Shen B. Deficiency in Duox2 activity alleviates ileitis in GPx1- and GPx2-knockout mice without affecting apoptosis incidence in the crypt epithelium. Redox Biol. 2017 Apr;11:144-156. Epub 2016 Nov 22. [CrossRef] [PubMed] [PubMed Central]
- Chu FF, Esworthy RS, Shen B, Gao Q, Doroshow JH. Dexamethasone and Tofacitinib suppress NADPH oxidase expression and alleviate very-early-onset ileocolitis in mice deficient in GSH peroxidase 1 and 2. Life Sci. 2019 Dec 15;239:116884. Epub 2019 Nov 2. [CrossRef] [PubMed] [PubMed Central]
- Meulmeester FL, Luo J, Martens LG, Mills K, van Heemst D, Noordam R. Antioxidant Supplementation in Oxidative Stress-Related Diseases: What Have We Learned from Studies on Alpha-Tocopherol? Antioxidants (Basel). 2022 Nov 24;11(12):2322. doi: 10.3390/antiox11122322. PMID: 36552530; PMCID: PMC9774512; Myung SK, Kim Y, Ju W, Choi HJ, Bae WK. Effects of antioxidant supplements on cancer prevention: meta-analysis of randomized controlled trials. Ann Oncol. 2010 Jan;21(1):166-79. Epub 2009 Jul 21. [CrossRef] [PubMed]
- Bjelakovic G, Nikolova D, Gluud LL, Simonetti RG, Gluud C. Antioxidant supplements for prevention of mortality in healthy participants and patients with various diseases. Cochrane Database Syst Rev. 2012 Mar 14;2012(3):CD007176. [CrossRef] [PubMed] [PubMed Central]
- Xavier LEMDS, Reis TCG, Martins ASDP, Santos JCF, Bueno NB, Goulart MOF, Moura FA. Antioxidant Therapy in Inflammatory Bowel Diseases: How Far Have We Come and How Close Are We? Antioxidants (Basel). 2024 Nov 8;13(11):1369. [CrossRef] [PubMed] [PubMed Central]
- Hendrickson BA, Gokhale R, Cho JH. Clinical aspects and pathophysiology of inflammatory bowel disease. Clin Microbiol Rev. 2002 Jan;15(1):79-94. doi: 10.1128/CMR.15.1.79-94.2002. PMID: 11781268; PMCID: PMC118061 Baumgart DC, Carding SR. Inflammatory bowel disease: cause and immunobiology. Lancet. 2007 May 12;369(9573):1627-40. [CrossRef] [PubMed]
- Strober W, Fuss I, Mannon P. The fundamental basis of inflammatory bowel disease. J Clin Invest. 2007 Mar;117(3):514-21. [CrossRef] [PubMed] [PubMed Central]
- Wen Z, Fiocchi C. Inflammatory bowel disease: autoimmune or immune-mediated pathogenesis? Clin Dev Immunol. 2004 Sep-Dec;11(3-4):195-204. [CrossRef] [PubMed] [PubMed Central]
- Knight-Sepulveda K, Kais S, Santaolalla R, Abreu MT. Diet and Inflammatory Bowel Disease. Gastroenterol Hepatol (N Y). 2015 Aug;11(8):511-20. [PubMed] [PubMed Central]
- Gordon H, Trier Moller F, Andersen V, Harbord M. Heritability in inflammatory bowel disease: from the first twin study to genome-wide association studies. Inflamm Bowel Dis. 2015 Jun;21(6):1428-34. [CrossRef] [PubMed] [PubMed Central]
- Eckmann L, Karin M. NOD2 and Crohn's disease: loss or gain of function? Immunity. 2005 Jun;22(6):661-7. [CrossRef] [PubMed]
- Santana PT, Rosas SLB, Ribeiro BE, Marinho Y, de Souza HSP. Dysbiosis in Inflammatory Bowel Disease: Pathogenic Role and Potential Therapeutic Targets. Int J Mol Sci. 2022 Mar 23;23(7):3464. [CrossRef] [PubMed] [PubMed Central]
- Kuenzig ME, Manuel DG, Donelle J, Benchimol EI. Life expectancy and health-adjusted life expectancy in people with inflammatory bowel disease. CMAJ. 2020 Nov 9;192(45):E1394-E1402. [CrossRef] [PubMed] [PubMed Central]
- Laredo V, García-Mateo S, Martínez-Domínguez SJ, López de la Cruz J, Gargallo-Puyuelo CJ, Gomollón F. Risk of Cancer in Patients with Inflammatory Bowel Diseases and Keys for Patient Management. Cancers (Basel). 2023 Jan 31;15(3):871. [CrossRef] [PubMed] [PubMed Central]
- Mitropoulou MA, Fradelos EC, Lee KY, Malli F, Tsaras K, Christodoulou NG, Papathanasiou IV. Quality of Life in Patients with Inflammatory Bowel Disease: Importance of Psychological Symptoms. Cureus. 2022 Aug 28;14(8):e28502. [CrossRef] [PubMed] [PubMed Central]
- Aniwan S, Santiago P, Loftus EV Jr, Park SH. The epidemiology of inflammatory bowel disease in Asia and Asian immigrants to Western countries. United European Gastroenterol J. 2022 Dec;10(10):1063-1076. Epub 2022 Dec 8. [CrossRef] [PubMed] [PubMed Central]
- Dharni K, Singh A, Sharma S, Midha V, Kaur K, Mahajan R, Dulai PS, Sood A. Trends of inflammatory bowel disease from the Global Burden of Disease Study (1990-2019). Indian J Gastroenterol. 2024 Feb;43(1):188-198. Epub 2023 Oct 3. [CrossRef] [PubMed]
- Loew, O. A NEW ENZYME OF GENERAL OCCURRENCE IN ORGANISMIS. Science. 1900 May 4;11(279):701-2. [CrossRef] [PubMed]
- Hwang J, Jin J, Jeon S, Moon SH, Park MY, Yum DY, Kim JH, Kang JE, Park MH, Kim EJ, Pan JG, Kwon O, Oh GT. SOD1 suppresses pro-inflammatory immune responses by protecting against oxidative stress in colitis. Redox Biol. 2020 Oct;37:101760. Epub 2020 Oct 15. [CrossRef] [PubMed] [PubMed Central]
- O'Morain C, Smethurst P, Levi AJ, Peters TJ. Organelle pathology in ulcerative and Crohn's colitis with special reference to the lysosomal alterations. Gut. 1984 May;25(5):455-9. [CrossRef] [PubMed] [PubMed Central]
- MILLS GC. Hemoglobin catabolism. I. Glutathione peroxidase, an erythrocyte enzyme which protects hemoglobin from oxidative breakdown. J Biol Chem. 1957 Nov;229(1):189-97. PMID. [PubMed]
- McCord JM, Fridovich I. The utility of superoxide dismutase in studying free radical reactions. I. Radicals generated by the interaction of sulfite, dimethyl sulfoxide, and oxygen. J Biol Chem. 1969 Nov 25;244(22):6056-63. [CrossRef] [PubMed]
- Emerit J, Loeper J, Chomette G. Superoxide dismutase in the treatment of post-radiotherapeutic necrosis and of Crohn's disease. Bull Eur Physiopathol Respir. 1981;17 Suppl:287. [PubMed]
- Petkau, A. Scientific basis for the clinical use of superoxide dismutase. Cancer Treat Rev. 1986 Mar;13(1):17-44. [CrossRef] [PubMed]
- Ahnfelt-Rønne I, Nielsen OH. The antiinflammatory moiety of sulfasalazine, 5-aminosalicylic acid, is a radical scavenger. Agents Actions. 1987 Jun;21(1-2):191-4. [CrossRef] [PubMed]
- Grisham MB, MacDermott RP, Deitch EA. Oxidant defense mechanisms in the human colon. Inflammation. 1990 Dec;14(6):669-80. [CrossRef] [PubMed]
- Fleming CR, McCall JT, O'Brien JF, Forsman RW, Ilstrup DM, Petz J. Selenium status in patients receiving home parenteral nutrition. JPEN J Parenter Enteral Nutr. 1984 May-Jun;8(3):258-62. [CrossRef] [PubMed]
- Rotruck JT, Pope AL, Ganther HE, Swanson AB, Hafeman DG, Hoekstra WG. Selenium: biochemical role as a component of glutathione peroxidase. Science. 1973 Feb 9;179(4073):588-90. [CrossRef] [PubMed]
- Penny WJ, Mayberry JF, Aggett PJ, Gilbert JO, Newcombe RG, Rhodes J. Relationship between trace elements, sugar consumption, and taste in Crohn's disease. Gut. 1983 Apr;24(4):288-92. doi: 10.1136/gut.24.4.288. PMID: 6832625; PMCID: PMC1419969. Harries AD, Heatley RV. Nutritional disturbances in Crohn's disease. Postgrad Med J. 1983 Nov;59(697):690-7. [CrossRef] [PubMed] [PubMed Central]
- Barrett CW, Singh K, Motley AK, Lintel MK, Matafonova E, Bradley AM, Ning W, Poindexter SV, Parang B, Reddy VK, Chaturvedi R, Fingleton BM, Washington MK, Wilson KT, Davies SS, Hill KE, Burk RF, Williams CS. Dietary selenium deficiency exacerbates DSS-induced epithelial injury and AOM/DSS-induced tumorigenesis. PLoS One. 2013 Jul 4;8(7):e67845. [CrossRef] [PubMed] [PubMed Central]
- Sang L, Chang B, Zhu J, Yang F, Li Y, Jiang X, Sun X, Lu C, Wang D. Dextran sulfate sodium-induced acute experimental colitis in C57BL/6 mice is mitigated by selenium. Int Immunopharmacol. 2016 Oct;39:359-368. Epub 2016 Aug 15. [CrossRef] [PubMed]
- Schneider T, Caviezel D, Ayata CK, Kiss C, Niess JH, Hruz P. The Copper/Zinc Ratio Correlates With Markers of Disease Activity in Patients With Inflammatory Bowel Disease. Crohns Colitis 360. 2020 Jan;2(1):otaa001. Epub 2020 Jan 23. [CrossRef] [PubMed] [PubMed Central]
- Amerikanou C, Karavoltsos S, Gioxari A, Tagkouli D, Sakellari A, Papada E, Kalogeropoulos N, Forbes A, Kaliora AC. Clinical and inflammatory biomarkers of inflammatory bowel diseases are linked to plasma trace elements and toxic metals; new insights into an old concept. Front Nutr. 2022 Dec 8;9:997356. [CrossRef] [PubMed] [PubMed Central]
- Tian T, Wang Z, Zhang J. Pathomechanisms of Oxidative Stress in Inflammatory Bowel Disease and Potential Antioxidant Therapies. Oxid Med Cell Longev. 2017;2017:4535194. Epub 2017 Jun 28. [CrossRef] [PubMed] [PubMed Central]
- Paschall M, Seo YA, Choi EK. Low Dietary Manganese Levels Exacerbate Experimental Colitis in Mice. Curr Dev Nutr. 2020 May 29;4(Suppl 2):1831. [CrossRef] [PubMed Central]
- Choi EK, Aring L, Das NK, Solanki S, Inohara N, Iwase S, Samuelson LC, Shah YM, Seo YA. Impact of dietary manganese on experimental colitis in mice. FASEB J. 2020 Feb;34(2):2929-2943. Epub 2019 Dec 29. [CrossRef] [PubMed] [PubMed Central]
- Kruidenier L, Kuiper I, van Duijn W, Marklund SL, van Hogezand RA, Lamers CB, Verspaget HW. Differential mucosal expression of three superoxide dismutase isoforms in inflammatory bowel disease. J Pathol. 2003 Sep;201(1):7-16. [CrossRef] [PubMed]
- Nielsen OH, Ainsworth M, Coskun M, Weiss G. Management of Iron-Deficiency Anemia in Inflammatory Bowel Disease: A Systematic Review. Medicine (Baltimore). 2015 Jun;94(23):e963. [CrossRef] [PubMed] [PubMed Central]
- Besgen P, Trommler P, Vollmer S, Prinz JC. Ezrin, maspin, peroxiredoxin 2, and heat shock protein 27: potential targets of a streptococcal-induced autoimmune response in psoriasis. J Immunol. 2010 May 1;184(9):5392-402. Epub 2010 Apr 2. [CrossRef] [PubMed]
- Lee, YJ. Knockout Mouse Models for Peroxiredoxins. Antioxidants (Basel). 2020 Feb 22;9(2):182. [CrossRef] [PubMed] [PubMed Central]
- Esworthy, R.S.; Chu, F.-F. Using Information from Public Databases to Critically Evaluate Studies Linking the Antioxidant Enzyme Selenium-Dependent Glutathione Peroxidase 2 (GPX2) to Cancer. BioMedInformatics 2023, 3, 985-1014. [CrossRef]
- Hoehne MN, Spatial and temporal control of mitochondrial H2O2 release in intact human cells. EMBO J. 2022 Apr 4;41(7):e109169. Epub 2022 Feb 11. [CrossRef] [PubMed] [PubMed Central]
- Pace PE, Fu L, Hampton MB, Winterbourn CC. Effect of peroxiredoxin 1 or peroxiredoxin 2 knockout on the thiol proteome of Jurkat cells. Free Radic Biol Med. 2024 Oct 18;225:595-604. Epub ahead of print. [CrossRef] [PubMed]
- Sun Y, Qiao Y, Liu Y, Zhou J, Wang X, Zheng H, Xu Z, Zhang J, Zhou Y, Qian L, Zhang C, Lou H. ent-Kaurane diterpenoids induce apoptosis and ferroptosis through targeting redox resetting to overcome cisplatin resistance. Redox Biol. 2021 Jul;43:101977. doi: 10.1016/j.redox.2021.101977. Epub 2021 Apr 16. Erratum in: Redox Biol. 2024 Jun;72:103164. [CrossRef] [PubMed] [PubMed Central]
- Thapa, P, Jiang H, Ding N, Hao Y, Alshahrani A, Lee EY, Fujii J, Wei Q. Loss of Peroxiredoxin IV Protects Mice from Azoxymethane/Dextran Sulfate Sodium-Induced Colorectal Cancer Development. Antioxidants (Basel). 2023 Mar 9;12(3):677. [CrossRef] [PubMed] [PubMed Central]
- Esworthy RS, Aranda R, Martín MG, Doroshow JH, Binder SW, Chu FF. Mice with combined disruption of Gpx1 and Gpx2 genes have colitis. Am J Physiol Gastrointest Liver Physiol. 2001 Sep;281(3):G848-55. [CrossRef] [PubMed]
- Van Remmen H, Williams MD, Guo Z, Estlack L, Yang H, Carlson EJ, Epstein CJ, Huang TT, Richardson A. Knockout mice heterozygous for Sod2 show alterations in cardiac mitochondrial function and apoptosis. Am J Physiol Heart Circ Physiol. 2001 Sep;281(3):H1422-32. [CrossRef] [PubMed]
- Garcia-Irigoyen O, Bovenga F, Piglionica M, Piccinin E, Cariello M, Arconzo M, Peres C, Corsetto PA, Rizzo AM, Ballanti M, Menghini R, Mingrone G, Lefebvre P, Staels B, Shirasawa T, Sabbà C, Villani G, Federici M, Moschetta A. Enterocyte superoxide dismutase 2 deletion drives obesity. iScience. 2021 Dec 27;25(1):103707. [CrossRef] [PubMed] [PubMed Central]
- Brand MD, Affourtit C, Esteves TC, Green K, Lambert AJ, Miwa S, Pakay JL, Parker N. Mitochondrial superoxide: production, biological effects, and activation of uncoupling proteins. Free Radic Biol Med. 2004 Sep 15;37(6):755-67. [CrossRef] [PubMed]
- Crapo JD, McCord JM. Oxygen-induced changes in pulmonary superoxide dismutase assayed by antibody titrations. Am J Physiol. 1976 Oct;231(4):1196-203. [CrossRef] [PubMed]
- Bize IB, Oberley LW, Morris HP. Superoxide dismutase and superoxide radical in Morris hepatomas. Cancer Res. 1980 Oct;40(10):3686-93. [PubMed]
- Keyer K, Gort AS, Imlay JA. Superoxide and the production of oxidative DNA damage. J Bacteriol. 1995 Dec;177(23):6782-90. [CrossRef] [PubMed] [PubMed Central]
- Kim BW, Esworthy RS, Hahn MA, Pfeifer GP, Chu FF. Expression of lactoperoxidase in differentiated mouse colon epithelial cells. Free Radic Biol Med. 2012 May 1;52(9):1569-76. Epub 2012 Feb 15. [CrossRef] [PubMed] [PubMed Central]
- Antunes F, Brito PM. Quantitative biology of hydrogen peroxide signaling. Redox Biol. 2017 Oct;13:1-7. Epub 2017 May 8. [CrossRef] [PubMed] [PubMed Central]
- Winterbourn, CC. The biological chemistry of hydrogen peroxide. Methods Enzymol. 2013;528:3-25. [CrossRef] [PubMed]
- Won HY, Sohn JH, Min HJ, Lee K, Woo HA, Ho YS, Park JW, Rhee SG, Hwang ES. Glutathione peroxidase 1 deficiency attenuates allergen-induced airway inflammation by suppressing Th2 and Th17 cell development. Antioxid Redox Signal. 2010 Sep 1;13(5):575-87. [CrossRef] [PubMed]
- Dittrich AM, Meyer HA, Krokowski M, Quarcoo D, Ahrens B, Kube SM, Witzenrath M, Esworthy RS, Chu FF, Hamelmann E. Glutathione peroxidase-2 protects from allergen-induced airway inflammation in mice. Eur Respir J. 2010 May;35(5):1148-54. Epub 2009 Nov 6. [CrossRef] [PubMed] [PubMed Central]
- Kim HR, Lee A, Choi EJ, Kie JH, Lim W, Lee HK, Moon BI, Seoh JY. Attenuation of experimental colitis in glutathione peroxidase 1 and catalase double knockout mice through enhancing regulatory T cell function. PLoS One. 2014 Apr 17;9(4):e95332. [CrossRef] [PubMed] [PubMed Central]
- Hu R, Xiao J, Fan L. The Role of the Trace Element Selenium in Inflammatory Bowel Disease. Biol Trace Elem Res. 2024 Nov;202(11):4923-4931. Epub 2024 Feb 16. [CrossRef] [PubMed]
- Kryukov GV, Castellano S, Novoselov SV, Lobanov AV, Zehtab O, Guigó R, Gladyshev VN. Characterization of mammalian selenoproteomes. Science. 2003 May 30;300(5624):1439-43. [CrossRef] [PubMed]
- Touat-Hamici Z, Bulteau AL, Bianga J, Jean-Jacques H, Szpunar J, Lobinski R, Chavatte L. Selenium-regulated hierarchy of human selenoproteome in cancerous and immortalized cells lines. Biochim Biophys Acta Gen Subj. 2018 Nov;1862(11):2493-2505. Epub 2018 Apr 13. [CrossRef] [PubMed]
- Ocansey DKW, Yuan J, Wei Z, Mao F, Zhang Z. Role of ferroptosis in the pathogenesis and as a therapeutic target of inflammatory bowel disease (Review). Int J Mol Med. 2023 Jun;51(6):53. Epub 2023 May 19. [CrossRef] [PubMed] [PubMed Central]
- Takashima H, Toyama T, Mishima E, Ishida K, Wang Y, Ichikawa A, Ito J, Yogiashi S, Siu S, Sugawara M, Shiina S, Arisawa K, Conrad M, Saito Y. Impact of selenium content in fetal bovine serum on ferroptosis susceptibility and selenoprotein expression in cultured cells. J Toxicol Sci. 2024;49(12):555-563. [CrossRef] [PubMed]
- Yang WS, SriRamaratnam R, Welsch ME, Shimada K, Skouta R, Viswanathan VS, Cheah JH, Clemons PA, Shamji AF, Clish CB, Brown LM, Girotti AW, Cornish VW, Schreiber SL, Stockwell BR. Regulation of ferroptotic cancer cell death by GPX4. Cell. 2014 Jan 16;156(1-2):317-331. [CrossRef] [PubMed] [PubMed Central]
- Chu FF, Doroshow JH, Esworthy RS. Expression, characterization, and tissue distribution of a new cellular selenium-dependent glutathione peroxidase, GSHPx-GI. J Biol Chem. 1993 Feb 5;268(4):2571-6. [PubMed]
- Esworthy RS, Mann JR, Sam M, Chu FF. Low glutathione peroxidase activity in Gpx1 knockout mice protects jejunum crypts from gamma-irradiation damage. Am J Physiol Gastrointest Liver Physiol. 2000 Aug;279(2):G426-36. [CrossRef] [PubMed]
- Chu FF, Esworthy RS. The expression of an intestinal form of glutathione peroxidase (GSHPx-GI) in rat intestinal epithelium. Arch Biochem Biophys. 1995 Nov 10;323(2):288-94. [CrossRef] [PubMed]
- Kannan N, Nguyen LV, Makarem M, Dong Y, Shih K, Eirew P, Raouf A, Emerman JT, Eaves CJ. Glutathione-dependent and -independent oxidative stress-control mechanisms distinguish normal human mammary epithelial cell subsets. Proc Natl Acad Sci U S A. 2014 May 27;111(21):7789-94. Epub 2014 May 12. [CrossRef] [PubMed] [PubMed Central]
- Esworthy RS, Swiderek KM, Ho YS, Chu FF. Selenium-dependent glutathione peroxidase-GI is a major glutathione peroxidase activity in the mucosal epithelium of rodent intestine. Biochim Biophys Acta. 1998 Jul 23;1381(2):213-26. [CrossRef] [PubMed]
- Tham DM, Whitin JC, Kim KK, Zhu SX, Cohen HJ. Expression of extracellular glutathione peroxidase in human and mouse gastrointestinal tract. Am J Physiol. 1998 Dec;275(6):G1463-71. [CrossRef] [PubMed]
- Speckmann B, Bidmon HJ, Pinto A, Anlauf M, Sies H, Steinbrenner H. Induction of glutathione peroxidase 4 expression during enterocytic cell differentiation. J Biol Chem. 2011 Mar 25;286(12):10764-72. Epub 2011 Jan 20. [CrossRef] [PubMed] [PubMed Central]
- Cohn SM, Schloemann S, Tessner T, Seibert K, Stenson WF. Crypt stem cell survival in the mouse intestinal epithelium is regulated by prostaglandins synthesized through cyclooxygenase 1. J Clin Invest. 1997 Mar 15;99(6):1367-79. [CrossRef] [PubMed] [PubMed Central]
- Koeberle SC, Gollowitzer A, Laoukili J, Kranenburg O, Werz O, Koeberle A, Kipp AP. Distinct and overlapping functions of glutathione peroxidases 1 and 2 in limiting NF-κB-driven inflammation through redox-active mechanisms. Redox Biol. 2020 Jan;28:101388. Epub 2019 Nov 16. [CrossRef] [PubMed] [PubMed Central]
- Banning A, Florian S, Deubel S, Thalmann S, Müller-Schmehl K, Jacobasch G, Brigelius-Flohé R. GPx2 counteracts PGE2 production by dampening COX-2 and mPGES-1 expression in human colon cancer cells. Antioxid Redox Signal. 2008 Sep;10(9):1491-500. [CrossRef] [PubMed]
- Capdevila JH, Morrow JD, Belosludtsev YY, Beauchamp DR, DuBois RN, Falck JR. The catalytic outcomes of the constitutive and the mitogen inducible isoforms of prostaglandin H2 synthase are markedly affected by glutathione and glutathione peroxidase(s). Biochemistry. 1995 Mar 14;34(10):3325-37. [CrossRef] [PubMed]
- Kulmacz RJ, Wang LH. Comparison of hydroperoxide initiator requirements for the cyclooxygenase activities of prostaglandin H synthase-1 and -2. J Biol Chem. 1995 Oct 13;270(41):24019-23. [CrossRef] [PubMed]
- Chu FF, Esworthy RS, Doroshow JH. Role of Se-dependent glutathione peroxidases in gastrointestinal inflammation and cancer. Free Radic Biol Med. 2004 Jun 15;36(12):1481-95. [CrossRef] [PubMed]
- Wood ZA, Poole LB, Karplus PA. Peroxiredoxin evolution and the regulation of hydrogen peroxide signaling. Science. 2003 Apr 25;300(5619):650-3. [CrossRef] [PubMed]
- COHEN G, HOCHSTEIN P. GLUTATHIONE PEROXIDASE: THE PRIMARY AGENT FOR THE ELIMINATION OF HYDROGEN PEROXIDE IN ERYTHROCYTES. Biochemistry. 1963 Nov-Dec;2:1420-8. [CrossRef] [PubMed]
- Chu FF, Esworthy RS, Chu PG, Longmate JA, Huycke MM, Wilczynski S, Doroshow JH. Bacteria-induced intestinal cancer in mice with disrupted Gpx1 and Gpx2 genes. Cancer Res. 2004 Feb 1;64(3):962-8. [CrossRef] [PubMed]
- Talmon G, Manasek T, Miller R, Muirhead D, Lazenby A. The Apoptotic Crypt Abscess: An Underappreciated Histologic Finding in Gastrointestinal Pathology. Am J Clin Pathol. 2017 Nov 20;148(6):538-544. [CrossRef] [PubMed]
- Esworthy RS, Kim BW, Chow J, Shen B, Doroshow JH, Chu FF. Nox1 causes ileocolitis in mice deficient in glutathione peroxidase-1 and -2. Free Radic Biol Med. 2014 Mar;68:315-25. Epub 2013 Dec 25. [CrossRef] [PubMed] [PubMed Central]
- Williams JM, Duckworth CA, Burkitt MD, Watson AJ, Campbell BJ, Pritchard DM. Epithelial cell shedding and barrier function: a matter of life and death at the small intestinal villus tip. Vet Pathol. 2015 May;52(3):445-55. Epub 2014 Nov 26. [CrossRef] [PubMed] [PubMed Central]
- Kiesslich R, Duckworth CA, Moussata D, Gloeckner A, Lim LG, Goetz M, Pritchard DM, Galle PR, Neurath MF, Watson AJ. Local barrier dysfunction identified by confocal laser endomicroscopy predicts relapse in inflammatory bowel disease. Gut. 2012 Aug;61(8):1146-53. Epub 2011 Nov 24. [CrossRef] [PubMed] [PubMed Central]
- Turcotte JF, Wong K, Mah SJ, Dieleman LA, Kao D, Kroeker K, Claggett B, Saltzman JR, Wine E, Fedorak RN, Liu JJ. Increased epithelial gaps in the small intestine are predictive of hospitalization and surgery in patients with inflammatory bowel disease. Clin Transl Gastroenterol. 2012 Jul 26;3(7):e19. [CrossRef] [PubMed] [PubMed Central]
- Esworthy RS, Yang L, Frankel PH, Chu FF. Epithelium-specific glutathione peroxidase, Gpx2, is involved in the prevention of intestinal inflammation in selenium-deficient mice. J Nutr. 2005 Apr;135(4):740-5. [CrossRef] [PubMed]
- Pinto MA, Lopes MS, Bastos ST, Reigada CL, Dantas RF, Neto JC, Luna AS, Madi K, Nunes T, Zaltman C. Does active Crohn's disease have decreased intestinal antioxidant capacity? J Crohns Colitis. 2013 Oct;7(9):e358-66. Epub 2013 Mar 21. [CrossRef] [PubMed]
- Shi J, Ji S, Xu M, Wang Y, Shi H. Selenium inhibits ferroptosis in ulcerative colitis through the induction of Nrf2/Gpx4. Clin Res Hepatol Gastroenterol. 2024 Sep 21;48(9):102467. Epub ahead of print. [CrossRef] [PubMed]
- Barros SÉL, Dias TMDS, Moura MSB, Soares NRM, Pierote NRA, Araújo COD, Maia CSC, Henriques GS, Barros VC, Moita Neto JM, Parente JML, Marreiro DDN, Nogueira NDN. Relationship between selenium status and biomarkers of oxidative stress in Crohn's disease. Nutrition. 2020 Jun;74:110762. Epub 2020 Feb 12. [CrossRef] [PubMed]
- Chalcarz M, Grabarek BO, Sirek T, Sirek A, Ossowski P, Wilk M, Król-Jatręga K, Dziobek K, Gajdeczka J, Madowicz J, Strojny D, Boroń K, Żurawski J. Evaluation of Selenium Concentrations in Patients with Crohn's Disease and Ulcerative Colitis. Biomedicines. 2024 Sep 24;12(10):2167. [CrossRef] [PubMed] [PubMed Central]
- Liu S, Lin T, Wang W, Jing F, Sheng J. Selenium deficiency in inflammatory bowel disease: A comprehensive meta-analysis. Heliyon. 2024 Nov 5;10(22):e40139. [CrossRef] [PubMed] [PubMed Central]
- Alfthan G, Xu GL, Tan WH, Aro A, Wu J, Yang YX, Liang WS, Xue WL, Kong LH. Selenium supplementation of children in a selenium-deficient area in China: blood selenium levels and glutathione peroxidase activities. Biol Trace Elem Res. 2000 Feb;73(2):113-25. [CrossRef] [PubMed]
- Xia YM, Hill KE, Burk RF. Biochemical studies of a selenium-deficient population in China: measurement of selenium, glutathione peroxidase and other oxidant defense indices in blood. J Nutr. 1989 Sep;119(9):1318-26. [CrossRef] [PubMed]
- Combs, G.F., Jr. Biomarkers of selenium status. Nutrients 2015, 7, 2209–2236. [CrossRef]
- Beck MA, Esworthy RS, Ho YS, Chu FF. Glutathione peroxidase protects mice from viral-induced myocarditis. FASEB J. 1998 Sep;12(12):1143-9. [CrossRef] [PubMed]
- Davis C, Javid PJ, Horslen S. Selenium deficiency in pediatric patients with intestinal failure as a consequence of drug shortage. JPEN J Parenter Enteral Nutr. 2014 Jan;38(1):115-8. Epub 2013 Apr 15. [CrossRef] [PubMed]
- Kaur R, Thakur S, Rastogi P, Kaushal N. Resolution of Cox mediated inflammation by Se supplementation in mouse experimental model of colitis. PLoS One. 2018 Jul 31;13(7):e0201356. [CrossRef] [PubMed] [PubMed Central]
- Reeves, PG. Components of the AIN-93 diets as improvements in the AIN-76A diet. J Nutr. 1997 May;127(5 Suppl):838S-841S. [CrossRef] [PubMed]
- Shi C, Yue F, Shi F, Qin Q, Wang L, Wang G, Mu L, Liu D, Li Y, Yu T, She J. Selenium-Containing Amino Acids Protect Dextran Sulfate Sodium-Induced Colitis via Ameliorating Oxidative Stress and Intestinal Inflammation. J Inflamm Res. 2021 Jan 14;14:85-95. [CrossRef] [PubMed] [PubMed Central]
- Shi J, Ji S, Xu M, Wang Y, Shi H. Selenium inhibits ferroptosis in ulcerative colitis through the induction of Nrf2/Gpx4. Clin Res Hepatol Gastroenterol. 2024 Sep 21;48(9):102467. Epub ahead of print. [CrossRef] [PubMed]
- Suwendi E, Iwaya H, Lee JS, Hara H, Ishizuka S. Zinc deficiency induces dysregulation of cytokine productions in an experimental colitis of rats. Biomed Res. 2012 Dec;33(6):329-36. [CrossRef] [PubMed]
- Sun Y, Wang Z, Gong P, Yao W, Ba Q, Wang H. Review on the health-promoting effect of adequate selenium status. Front Nutr. 2023 Mar 16;10:1136458. [CrossRef] [PubMed] [PubMed Central]
- Ala M, Kheyri Z. The rationale for selenium supplementation in inflammatory bowel disease: A mechanism-based point of view. Nutrition. 2021 May;85:111153. Epub 2021 Jan 14. [CrossRef] [PubMed]
- Sousa JA, McKay DM, Raman M. Selenium, Immunity, and Inflammatory Bowel Disease. Nutrients. 2024; 16(21):3620. https://doi.org/10.3390/nu16213620; Khazdouz, M.; Daryani, N.E.; Alborzi, F.; Jazayeri, M.H.; Farsi, F.; Hasani, M.; Heshmati, J.; Shidfar, F. Effect of Selenium Supplementation on Expression of Sirt1 and Pgc-1alpha Genes in Ulcerative Colitis Patients: A Double Blind Randomized Clinical Trial. Clin. Nutr. Res. 2020, 9, 284–295.
- Khazdouz, M.; Daryani, N.E.; Alborzi, F.; Jazayeri, M.H.; Farsi, F.; Hasani, M.; Heshmati, J.; Shidfar, F. Effect of Selenium Supplementation on Expression of Sirt1 and Pgc-1alpha Genes in Ulcerative Colitis Patients: A Double Blind Randomized Clinical Trial. Clin. Nutr. Res. 2020, 9, 284–295.
- Jones, R.M.; Luo, L.; Ardita, C.S.; Richardson, A.N.; Kwon, Y.M.; Mercante, J.W.; Alam, A.; Gates, C.L.;Wu, H.; Swanson, P.A.; et al. Symbiotic lactobacilli stimulate gut epithelial proliferation via Nox-mediated generation of reactive oxygen species. EMBO J. 2013, 32, 3017–3028.
- Kato, M.; Marumo, M.; Nakayama, J.; Matsumoto, M.; Yabe-Nishimura, C.; Kamata, T. The ROS-generating oxidase Nox1 is required for epithelial restitution following colitis. Exp. Anim. 2016, 65, 197–205; Matsumoto, M.; Katsuyama, M.; Iwata, K.
- Ibi, M.; Zhang, J.; Zhu, K.; Nauseef, W.M.; Yabe-Nishimura, C. Characterization of N-glycosylation sites on the extracellular domain of NOX1/NADPH oxidase. Free Radic. Biol. Med. 2014, 68, 196–204.
- Esworthy, RS. Evaluation of the Use of Cell Lines in Studies of Selenium-Dependent Glutathione Peroxidase 2 (GPX2) Involvement in Colorectal Cancer. Diseases. 2024 Sep 10;12(9):207. [CrossRef] [PubMed] [PubMed Central]
- MacFie TS, Poulsom R, Parker A, Warnes G, Boitsova T, Nijhuis A, Suraweera N, Poehlmann A, Szary J, Feakins R, Jeffery R, Harper RW, Jubb AM, Lindsay JO, Silver A. DUOX2 and DUOXA2 form the predominant enzyme system capable of producing the reactive oxygen species H2O2 in active ulcerative colitis and are modulated by 5-aminosalicylic acid. Inflamm Bowel Dis. 2014 Mar;20(3):514-24. [CrossRef]
- Haberman Y, Tickle TL, Dexheimer PJ, Kim MO, Tang D, Karns R, Baldassano RN, Noe JD, Rosh J, Markowitz J, Heyman MB, Griffiths AM, Crandall WV, Mack DR, Baker SS, Huttenhower C, Keljo DJ, Hyams JS, Kugathasan S, Walters TD, Aronow B, Xavier RJ, Gevers D, Denson LA. Pediatric Crohn disease patients exhibit specific ileal transcriptome and microbiota signature. J Clin Invest. 2014 Aug;124(8):3617-33. Epub 2014 Jul 8. [CrossRef] [PubMed] [PubMed Central]
- Li J, Simmons AJ, Hawkins CV, Chiron S, Ramirez-Solano MA, Tasneem N, Kaur H, Xu Y, Revetta F, Vega PN, Bao S, Cui C, Tyree RN, Raber LW, Conner AN, Pilat JM, Jacobse J, McNamara KM, Allaman MM, Raffa GA, Gobert AP, Asim M, Goettel JA, Choksi YA, Beaulieu DB, Dalal RL, Horst SN, Pabla BS, Huo Y, Landman BA, Roland JT, Scoville EA, Schwartz DA, Washington MK, Shyr Y, Wilson KT, Coburn LA, Lau KS, Liu Q. Identification and multimodal characterization of a specialized epithelial cell type associated with Crohn's disease. Nat Commun. 2024 Aug 22;15(1):7204. [CrossRef] [PubMed] [PubMed Central]
- Deng L, He S, Li Y, Ding R, Li X, Guo N, Luo L. Identification of Lipocalin 2 as a Potential Ferroptosis-related Gene in Ulcerative Colitis. Inflamm Bowel Dis. 2023 Sep 1;29(9):1446-1457. [CrossRef] [PubMed]
- Fichman Y, Rowland L, Nguyen TT, Chen SJ, Mittler R. Propagation of a rapid cell-to-cell H2O2 signal over long distances in a monolayer of cardiomyocyte cells. Redox Biol. 2024 Apr;70:103069. Epub 2024 Feb 9. [CrossRef] [PubMed] [PubMed Central]
- Dang PM, Rolas L, El-Benna J. The Dual Role of Reactive Oxygen Species-Generating Nicotinamide Adenine Dinucleotide Phosphate Oxidases in Gastrointestinal Inflammation and Therapeutic Perspectives. Antioxid Redox Signal. 2020 Aug 10;33(5):354-373. Epub 2020 Feb 26. [CrossRef] [PubMed]
- LaBere B, Gutierrez MJ, Wright H, Garabedian E, Ochs HD, Fuleihan RL, Secord E, Marsh R, Sullivan KE, Cunningham-Rundles C, Notarangelo LD, Chen K. Chronic Granulomatous Disease With Inflammatory Bowel Disease: Clinical Presentation, Treatment, and Outcomes From the USIDNET Registry. J Allergy Clin Immunol Pract. 2022 May;10(5):1325-1333.e5. Epub 2022 Jan 14. [CrossRef] [PubMed] [PubMed Central]
- Aviello G, Knaus UG. NADPH oxidases and ROS signaling in the gastrointestinal tract. Mucosal Immunol. 2018 Jul;11(4):1011-1023. Epub 2018 May 9. [CrossRef] [PubMed]
- Bao S, Carr ED, Xu YH, Hunt NH. Gp91(phox) contributes to the development of experimental inflammatory bowel disease. Immunol Cell Biol. 2011 Nov;89(8):853-60. Epub 2011 Feb 15. [CrossRef] [PubMed]
- Hayes P, Dhillon S, O'Neill K, Thoeni C, Hui KY, Elkadri A, Guo CH, Kovacic L, Aviello G, Alvarez LA, Griffiths AM, Snapper SB, Brant SR, Doroshow JH, Silverberg MS, Peter I, McGovern DP, Cho J, Brumell JH, Uhlig HH, Bourke B, Muise AA, Knaus UG. Defects in NADPH Oxidase Genes NOX1 and DUOX2 in Very Early Onset Inflammatory Bowel Disease. Cell Mol Gastroenterol Hepatol. 2015 Sep 1;1(5):489-502. [CrossRef] [PubMed] [PubMed Central]
- Muise AM, Xu W, Guo CH, Walters TD, Wolters VM, Fattouh R, Lam GY, Hu P, Murchie R, Sherlock M, Gana JC; NEOPICS; Russell RK, Glogauer M, Duerr RH, Cho JH, Lees CW, Satsangi J, Wilson DC, Paterson AD, Griffiths AM, Silverberg MS, Brumell JH. NADPH oxidase complex and IBD candidate gene studies: identification of a rare variant in NCF2 that results in reduced binding to RAC2. Gut. 2012 Jul;61(7):1028-35. doi: 10.1136/gutjnl-2011-300078. Epub 2011 Sep 7. Erratum in: Gut. 2013 Oct;62(10):1432. [PubMed] [PubMed Central]
- Schwerd T, Bryant RV, Pandey S, Capitani M, Meran L, Cazier JB, Jung J, Mondal K, Parkes M, Mathew CG, Fiedler K, McCarthy DJ; WGS500 Consortium; Oxford IBD cohort study investigators; COLORS in IBD group investigators; UK IBD Genetics Consortium; Sullivan PB, Rodrigues A, Travis SPL, Moore C, Sambrook J, Ouwehand WH, Roberts DJ, Danesh J; INTERVAL Study; Russell RK, Wilson DC, Kelsen JR, Cornall R, Denson LA, Kugathasan S, Knaus UG, Serra EG, Anderson CA, Duerr RH, McGovern DP, Cho J, Powrie F, Li VS, Muise AM, Uhlig HH. NOX1 loss-of-function genetic variants in patients with inflammatory bowel disease. Mucosal Immunol. 2018 Mar;11(2):562-574. Epub 2017 Nov 1. [CrossRef] [PubMed] [PubMed Central]
- Jiang H, Wu J, Ke S, Hu Y, Fei A, Zhen Y, Yu J, Zhu K. High prevalence of DUOX2 gene mutations among children with congenital hypothyroidism in central China. Eur J Med Genet. 2016 Oct;59(10):526-31. Epub 2016 Aug 3. [CrossRef] [PubMed]
- Ohata H, Shiokawa D, Obata Y, Sato A, Sakai H, Fukami M, Hara W, Taniguchi H, Ono M, Nakagama H, Okamoto K. NOX1-Dependent mTORC1 Activation via S100A9 Oxidation in Cancer Stem-like Cells Leads to Colon Cancer Progression. Cell Rep. 2019 Jul 30;28(5):1282-1295.e8. [CrossRef]
- van der Post S, Birchenough GMH, Held JM. NOX1-dependent redox signaling potentiates colonic stem cell proliferation to adapt to the intestinal microbiota by linking EGFR and TLR activation. Cell Rep. 2021 Apr 6;35(1):108949. [CrossRef] [PubMed] [PubMed Central]
- Coant N, Ben Mkaddem S, Pedruzzi E, Guichard C, Tréton X, Ducroc R, Freund JN, Cazals-Hatem D, Bouhnik Y, Woerther PL, Skurnik D, Grodet A, Fay M, Biard D, Lesuffleur T, Deffert C, Moreau R, Groyer A, Krause KH, Daniel F, Ogier-Denis E. NADPH oxidase 1 modulates WNT and NOTCH1 signaling to control the fate of proliferative progenitor cells in the colon. Mol Cell Biol. 2010 Jun;30(11):2636-50. Epub 2010 Mar 29. [CrossRef] [PubMed] [PubMed Central]
- Kato M, Marumo M, Nakayama J, Matsumoto M, Yabe-Nishimura C, Kamata T. The ROS-generating oxidase Nox1 is required for epithelial restitution following colitis. Exp Anim. 2016 Jul 29;65(3):197-205. Epub 2016 Feb 15. [CrossRef] [PubMed] [PubMed Central]
- Hsu NY, Nayar S, Gettler K, Talware S, Giri M, Alter I, Argmann C, Sabic K, Thin TH, Ko HM, Werner R, Tastad C, Stappenbeck T, Azabdaftari A, Uhlig HH, Chuang LS, Cho JH. NOX1 is essential for TNFα-induced intestinal epithelial ROS secretion and inhibits M cell signatures. Gut. 2023 Apr;72(4):654-662. Epub 2022 Oct 3. [CrossRef] [PubMed] [PubMed Central]
- Koeberle SC, Gollowitzer A, Laoukili J, Kranenburg O, Werz O, Koeberle A, Kipp AP. Distinct and overlapping functions of glutathione peroxidases 1 and 2 in limiting NF-κB-driven inflammation through redox-active mechanisms. Redox Biol. 2020 Jan;28:101388. Epub 2019 Nov 16. [CrossRef] [PubMed] [PubMed Central]
- Matziouridou C, Rocha SDC, Haabeth OA, Rudi K, Carlsen H, Kielland A. iNOS- and NOX1-dependent ROS production maintains bacterial homeostasis in the ileum of mice. Mucosal Immunol. 2018 May;11(3):774-784. Epub 2017 Dec 6. [CrossRef] [PubMed]
- Drieu La Rochelle J, Ward J, Stenke E, Yin Y, Matsumoto M, Jennings R, Aviello G, Knaus UG. Dysregulated NOX1-NOS2 activity as hallmark of ileitis in mice. Mucosal Immunol. 2024 Sep 7:S1933-0219(24)00093-X. Epub ahead of print. [CrossRef] [PubMed]
- Benhar, M. Roles of mammalian glutathione peroxidase and thioredoxin reductase enzymes in the cellular response to nitrosative stress. Free Radic Biol Med. 2018 Nov 1;127:160-164. Epub 2018 Feb 3. [CrossRef] [PubMed]
- Dixon SJ, Lemberg KM, Lamprecht MR, Skouta R, Zaitsev EM, Gleason CE, Patel DN, Bauer AJ, Cantley AM, Yang WS, Morrison B 3rd, Stockwell BR. Ferroptosis: an iron-dependent form of nonapoptotic cell death. Cell. 2012 May 25;149(5):1060-72. [CrossRef] [PubMed] [PubMed Central]
- Wang M, Zheng C, Zhou F, Ying X, Zhang X, Peng C, Wang L. Iron and Inflammatory Cytokines Synergistically Induce Colonic Epithelial Cell Ferroptosis in Colitis. J Gastroenterol Hepatol. 2024 Nov 25. Epub ahead of print. [CrossRef] [PubMed]
- Wen X, Iwata K, Ikuta K, Zhang X, Zhu K, Ibi M, Matsumoto M, Asaoka N, Liu J, Katsuyama M, Yabe-Nishimura C. NOX1/NADPH oxidase regulates the expression of multidrug resistance-associated protein 1 and maintains intracellular glutathione levels. FEBS J. 2019 Feb;286(4):678-687. Epub 2019 Feb 6. [CrossRef] [PubMed]
- Haber AL, Biton M, Rogel N, Herbst RH, Shekhar K, Smillie C, Burgin G, Delorey TM, Howitt MR, Katz Y, Tirosh I, Beyaz S, Dionne D, Zhang M, Raychowdhury R, Garrett WS, Rozenblatt-Rosen O, Shi HN, Yilmaz O, Xavier RJ, Regev A. A single-cell survey of the small intestinal epithelium. Nature. 2017 Nov 16;551(7680):333-339. Epub 2017 Nov 8. [CrossRef] [PubMed] [PubMed Central]
- Grasberger H, Gao J, Nagao-Kitamoto H, Kitamoto S, Zhang M, Kamada N, Eaton KA, El-Zaatari M, Shreiner AB, Merchant JL, Owyang C, Kao JY. Increased Expression of DUOX2 Is an Epithelial Response to Mucosal Dysbiosis Required for Immune Homeostasis in Mouse Intestine. Gastroenterology. 2015 Dec;149(7):1849-59. doi: 10.1053/j.gastro.2015.07.062. Epub 2015 Aug 7. Erratum in: Gastroenterology. 2023 May;164(6):1033. [CrossRef] [PubMed] [PubMed Central]
- Lipinski S, Till A, Sina C, Arlt A, Grasberger H, Schreiber S, Rosenstiel P. DUOX2-derived reactive oxygen species are effectors of NOD2-mediated antibacterial responses. J Cell Sci. 2009 Oct 1;122(Pt 19):3522-30. [CrossRef] [PubMed]
- Davies JM, Abreu MT. The innate immune system and inflammatory bowel disease. Scand J Gastroenterol. 2015 Jan;50(1):24-33. [CrossRef] [PubMed]
- Paidimarri SP, Ayuthu S, Chauhan YD, Bittla P, Mirza AA, Saad MZ, Khan S. Contribution of the Gut Microbiota to the Perpetuation of Inflammation in Crohn's Disease: A Systematic Review. Cureus. 2024 Aug 24;16(8):e67672. [CrossRef] [PubMed] [PubMed Central]
- Jauregui-Amezaga A, Smet A. The Microbiota in Inflammatory Bowel Disease. J Clin Med. 2024 Aug 7;13(16):4622. [CrossRef] [PubMed] [PubMed Central]
- Gaschler MM, Hu F, Feng H, Linkermann A, Min W, Stockwell BR. Determination of the Subcellular Localization and Mechanism of Action of Ferrostatins in Suppressing Ferroptosis. ACS Chem Biol. 2018 Apr 20;13(4):1013-1020. Epub 2018 Mar 13. [CrossRef] [PubMed] [PubMed Central]
- Cochemé HM, Kelso GF, James AM, Ross MF, Trnka J, Mahendiran T, Asin-Cayuela J, Blaikie FH, Manas AR, Porteous CM, Adlam VJ, Smith RA, Murphy MP. Mitochondrial targeting of quinones: therapeutic implications. Mitochondrion. 2007 Jun;7 Suppl:S94-102. Epub 2007 Mar 16. [CrossRef] [PubMed]
- Kruidenier L, Kuiper I, Lamers CB, Verspaget HW. Intestinal oxidative damage in inflammatory bowel disease: semi-quantification, localization, and association with mucosal antioxidants. J Pathol. 2003 Sep;201(1):28-36. [CrossRef] [PubMed]
- Reynolds PD, Rhenius ST, Hunter JO. Xanthine oxidase activity is not increased in the colonic mucosa of ulcerative colitis. Aliment Pharmacol Ther. 1996 Oct;10(5):737-41. [CrossRef] [PubMed]
- Salim, AS. Role of oxygen-derived free radical scavengers in the management of recurrent attacks of ulcerative colitis: a new approach. J Lab Clin Med. 1992 Jun;119(6):710-7. [PubMed]
- Järnerot G, Ström M, Danielsson A, Kilander A, Lööf L, Hultcrantz R, Löfberg R, Florén C, Nilsson A, Broström O. Allopurinol in addition to 5-aminosalicylic acid-based drugs for the maintenance treatment of ulcerative colitis. Aliment Pharmacol Ther. 2000 Sep;14(9):1159-62. [CrossRef] [PubMed]
- Pacher P, Nivorozhkin A, Szabó C. Therapeutic effects of xanthine oxidase inhibitors: renaissance half a century after the discovery of allopurinol. Pharmacol Rev. 2006 Mar;58(1):87-114. [CrossRef] [PubMed] [PubMed Central]
- El-Mahdy NA, Saleh DA, Amer MS, Abu-Risha SE. Role of allopurinol and febuxostat in the amelioration of dextran-induced colitis in rats. Eur J Pharm Sci. 2020 Jan 1;141:105116. Epub 2019 Oct 23. [CrossRef] [PubMed]
- Li H, Li X, Wang Y, Han W, Li H, Zhang Q. Hypoxia-Mediated Upregulation of Xanthine Oxidoreductase Causes DNA Damage of Colonic Epithelial Cells in Colitis. Inflammation. 2024 Aug;47(4):1142-1155. Epub 2024 Jan 11. [CrossRef] [PubMed]
- Fang J, Yin H, Liao L, Qin H, Ueda F, Uemura K, Eguchi K, Bharate GY, Maeda H. Water soluble PEG-conjugate of xanthine oxidase inhibitor, PEG-AHPP micelles, as a novel therapeutic for ROS related inflammatory bowel diseases. J Control Release. 2016 Feb 10;223:188-196. doi: 10.1016/j.jconrel.2015.12.049. Epub 2015 Dec 29. PMID: 26739550. 119. Worledge CS, Kostelecky RE, Zhou L, Bhagavatula G, Colgan SP, Lee JS. Allopurinol Disrupts Purine Metabolism to Increase Damage in Experimental Colitis. Cells. 2024 Feb 21;13(5):373. [CrossRef] [PubMed] [PubMed Central]
- Worledge CS, Kostelecky RE, Zhou L, Bhagavatula G, Colgan SP, Lee JS. Allopurinol Disrupts Purine Metabolism to Increase Damage in Experimental Colitis. Cells. 2024 Feb 21;13(5):373. [CrossRef] [PubMed] [PubMed Central]
- Bayoumy AB, Mulder CJJ, Ansari AR, Barclay ML, Florin T, Kiszka-Kanowitz M, Derijks L, Sharma V, de Boer NKH. Uphill battle: Innovation of thiopurine therapy in global inflammatory bowel disease care. Indian J Gastroenterol. 2024 Feb;43(1):36-47. Epub 2024 Feb 21. [CrossRef] [PubMed] [PubMed Central]
- Riaz AA, Wan MX, Schäfer T, Dawson P, Menger MD, Jeppsson B, Thorlacius H. Allopurinol and superoxide dismutase protect against leucocyte-endothelium interactions in a novel model of colonic ischaemia-reperfusion. Br J Surg. 2002 Dec;89(12):1572-80. [CrossRef] [PubMed]
- Chiaro TR, Soto R, Zac Stephens W, Kubinak JL, Petersen C, Gogokhia L, Bell R, Delgado JC, Cox J, Voth W, Brown J, Stillman DJ, O'Connell RM, Tebo AE, Round JL. A member of the gut mycobiota modulates host purine metabolism exacerbating colitis in mice. Sci Transl Med. 2017 Mar 8;9(380):eaaf9044. doi: 10.1126/scitranslmed.aaf9044. Erratum in: Sci Transl Med. 2017 May 3;9(388):eaan5218. [CrossRef] [PubMed] [PubMed Central]
- Li H, Li X, Wang Y, Han W, Li H, Zhang Q. Hypoxia-Mediated Upregulation of Xanthine Oxidoreductase Causes DNA Damage of Colonic Epithelial Cells in Colitis. Inflammation. 2024 Aug;47(4):1142-1155. Epub 2024 Jan 11. [CrossRef] [PubMed]
- Esworthy RS, Smith DD, Chu FF. A Strong Impact of Genetic Background on Gut Microflora in Mice. Int J Inflam. 2010 Jun 1;2010(2010):986046. [CrossRef] [PubMed] [PubMed Central]
- Atiq A, Lee HJ, Khan A, Kang MH, Rehman IU, Ahmad R, Tahir M, Ali J, Choe K, Park JS, Kim MO. Vitamin E Analog Trolox Attenuates MPTP-Induced Parkinson's Disease in Mice, Mitigating Oxidative Stress, Neuroinflammation, and Motor Impairment. Int J Mol Sci. 2023 Jun 9;24(12):9942. [CrossRef] [PubMed] [PubMed Central]
- Esworthy RS, Kim BW, Larson GP, Yip ML, Smith DD, Li M, Chu FF. Colitis locus on chromosome 2 impacting the severity of early-onset disease in mice deficient in GPX1 and GPX2. Inflamm Bowel Dis. 2011 Jun;17(6):1373-86. Epub 2010 Sep 24. [CrossRef] [PubMed] [PubMed Central]
- Seiler A, Schneider M, Förster H, Roth S, Wirth EK, Culmsee C, Plesnila N, Kremmer E, Rådmark O, Wurst W, Bornkamm GW, Schweizer U, Conrad M. Glutathione peroxidase 4 senses and translates oxidative stress into 12/15-lipoxygenase dependent- and AIF-mediated cell death. Cell Metab. 2008 Sep;8(3):237-48. [CrossRef] [PubMed]
- Steinhilber, D. (2016). Lipoxygenases: An Introduction. In: Steinhilber, D. (eds) Lipoxygenases in Inflammation. Progress in Inflammation Research. Springer, Cham. [CrossRef]
- Friedmann Angeli JP, Schneider M, Proneth B, Tyurina YY, Tyurin VA, Hammond VJ, Herbach N, Aichler M, Walch A, Eggenhofer E, Basavarajappa D, Rådmark O, Kobayashi S, Seibt T, Beck H, Neff F, Esposito I, Wanke R, Förster H, Yefremova O, Heinrichmeyer M, Bornkamm GW, Geissler EK, Thomas SB, Stockwell BR, O'Donnell VB, Kagan VE, Schick JA, Conrad M. Inactivation of the ferroptosis regulator Gpx4 triggers acute renal failure in mice. Nat Cell Biol. 2014 Dec;16(12):1180-91. Epub 2014 Nov 17. [CrossRef] [PubMed] [PubMed Central]
- Shah R, Shchepinov MS, Pratt DA. Resolving the Role of Lipoxygenases in the Initiation and Execution of Ferroptosis. ACS Cent Sci. 2018 Mar 28;4(3):387-396. Epub 2018 Feb 7. [CrossRef] [PubMed] [PubMed Central]
- Wenzel SE, Tyurina YY, Zhao J, St Croix CM, Dar HH, Mao G, Tyurin VA, Anthonymuthu TS, Kapralov AA, Amoscato AA, Mikulska-Ruminska K, Shrivastava IH, Kenny EM, Yang Q, Rosenbaum JC, Sparvero LJ, Emlet DR, Wen X, Minami Y, Qu F, Watkins SC, Holman TR, VanDemark AP, Kellum JA, Bahar I, Bayır H, Kagan VE. PEBP1 Wardens Ferroptosis by Enabling Lipoxygenase Generation of Lipid Death Signals. Cell. 2017 Oct 19;171(3):628-641.e26. [CrossRef] [PubMed] [PubMed Central]
- Agarwal R, Wang ZY, Bik DP, Mukhtar H. Nordihydroguaiaretic acid, an inhibitor of lipoxygenase, also inhibits cytochrome P-450-mediated monooxygenase activity in rat epidermal and hepatic microsomes. Drug Metab Dispos. 1991 May-Jun;19(3):620-4. [PubMed]
- Koppenol WH. The centennial of the Fenton reaction. Free Radic Biol Med. 1993 Dec;15(6):645-51. doi: 10.1016/0891-5849(93)90168-t. PMID: 8138191; Gutteridge JM. Iron and oxygen: a biologically damaging mixture. Acta Paediatr Scand Suppl. 1989;361:78-85. [CrossRef] [PubMed]
- HOCHSTEIN P, ERNSTER L. ADP-ACTIVATED LIPID PEROXIDATION COUPLED TO THE TPNH OXIDASE SYSTEM OF MICROSOMES. Biochem Biophys Res Commun. 1963 Aug 14;12:388-94. [CrossRef] [PubMed]
- Bannai S, Tsukeda H, Okumura H. Effect of antioxidants on cultured human diploid fibroblasts exposed to cystine-free medium. Biochem Biophys Res Commun. 1977 Feb 21;74(4):1582-8. [CrossRef] [PubMed]
- Ursini F, Bosello Travain V, Cozza G, Miotto G, Roveri A, Toppo S, Maiorino M. A white paper on Phospholipid Hydroperoxide Glutathione Peroxidase (GPx4) forty years later. Free Radic Biol Med. 2022 Aug 1;188:117-133. Epub 2022 Jun 16. [CrossRef] [PubMed]
- Maiorino M, Chu FF, Ursini F, Davies KJ, Doroshow JH, Esworthy RS. Phospholipid hydroperoxide glutathione peroxidase is the 18-kDa selenoprotein expressed in human tumor cell lines. J Biol Chem. 1991 Apr 25;266(12):7728-32. [CrossRef] [PubMed]
- Xie Y, Hou W, Song X, Yu Y, Huang J, Sun X, Kang R, Tang D. Ferroptosis: process and function. Cell Death Differ. 2016 Mar;23(3):369-79. Epub 2016 Jan 22. [CrossRef] [PubMed] [PubMed Central]
- Damiani CR, Benetton CA, Stoffel C, Bardini KC, Cardoso VH, Di Giunta G, Pinho RA, Dal-Pizzol F, Streck EL. Oxidative stress and metabolism in animal model of colitis induced by dextran sulfate sodium. J Gastroenterol Hepatol. 2007 Nov;22(11):1846-51. Epub 2007 Apr 19. [CrossRef] [PubMed]
- Minaiyan M, Mostaghel E, Mahzouni P. Preventive Therapy of Experimental Colitis with Selected iron Chelators and Anti-oxidants. Int J Prev Med. 2012 Mar;3(Suppl 1):S162-9. [PubMed] [PubMed Central]
- Millar AD, Rampton DS, Blake DR. Effects of iron and iron chelation in vitro on mucosal oxidant activity in ulcerative colitis. Aliment Pharmacol Ther. 2000 Sep;14(9):1163-8. [CrossRef] [PubMed]
- Wu Y, Ran L, Yang Y, Gao X, Peng M, Liu S, Sun L, Wan J, Wang Y, Yang K, Yin M, Chunyu W. Deferasirox alleviates DSS-induced ulcerative colitis in mice by inhibiting ferroptosis and improving intestinal microbiota. Life Sci. 2023 Feb 1;314:121312. Epub 2022 Dec 21. [CrossRef] [PubMed]
- Mantzaris MD, Bellou S, Skiada V, Kitsati N, Fotsis T, Galaris D. Intracellular labile iron determines H2O2-induced apoptotic signaling via sustained activation of ASK1/JNK-p38 axis. Free Radic Biol Med. 2016 Aug;97:454-465. Epub 2016 Jul 5. [CrossRef] [PubMed]
- Vechalapu SK, Kumar R, Chatterjee N, Gupta S, Khanna S, Thimmappa PY, Senthil S, Eerlapally R, Joshi MB, Misra SK, Draksharapu A, Allimuthu D. Redox modulator iron complexes trigger intrinsic apoptosis pathway in cancer cells. iScience. 2024 ;27(6):109899. 3 May. [CrossRef] [PubMed] [PubMed Central]
- Gao M, Monian P, Quadri N, Ramasamy R, Jiang X. Glutaminolysis and Transferrin Regulate Ferroptosis. Mol Cell. 2015 Jul 16;59(2):298-308. Epub 2015 Jul 9. [CrossRef] [PubMed] [PubMed Central]
- Parant F, Mure F, Maurin J, Beauvilliers L, Chorfa C, El Jamali C, Ohlmann T, Chavatte L. Selenium Discrepancies in Fetal Bovine Serum: Impact on Cellular Selenoprotein Expression. Int J Mol Sci. 2024 Jul 1;25(13):7261. [CrossRef] [PubMed] [PubMed Central]
- Bannai S, Tsukeda H, Okumura H. Effect of antioxidants on cultured human diploid fibroblasts exposed to cystine-free medium. Biochem Biophys Res Commun. 1977 Feb 21;74(4):1582-8. [CrossRef] [PubMed]
- Dolma S, Lessnick SL, Hahn WC, Stockwell BR. Identification of genotype-selective antitumor agents using synthetic lethal chemical screening in engineered human tumor cells. Cancer Cell. 2003 Mar;3(3):285-96. [CrossRef] [PubMed]
- Yang WS, Stockwell BR. Synthetic lethal screening identifies compounds activating iron-dependent, nonapoptotic cell death in oncogenic-RAS-harboring cancer cells. Chem Biol. 2008 Mar;15(3):234-45. [CrossRef] [PubMed] [PubMed Central]
- Hirschhorn T, Stockwell BR. The development of the concept of ferroptosis. Free Radic Biol Med. 2019 Mar;133:130-143. Epub 2018 Sep 28. [CrossRef] [PubMed] [PubMed Central]
- Esworthy RS, Doan K, Doroshow JH, Chu FF. Cloning and sequencing of the cDNA encoding a human testis phospholipid hydroperoxide glutathione peroxidase. Gene. 1994 Jul 8;144(2):317-8. [CrossRef] [PubMed]
- Hurst R, Korytowski W, Kriska T, Esworthy RS, Chu FF, Girotti AW. Hyperresistance to cholesterol hydroperoxide-induced peroxidative injury and apoptotic death in a tumor cell line that overexpresses glutathione peroxidase isotype-4. Free Radic Biol Med. 2001 Nov 1;31(9):1051-65. [CrossRef] [PubMed]
- Kriska T, Levchenko VV, Chu FF, Esworthy RS, Girotti AW. Novel enrichment of tumor cell transfectants expressing high levels of type 4 glutathione peroxidase using 7alpha-hydroperoxycholesterol as a selection agent. Free Radic Biol Med. 2008 Sep 1;45(5):700-7. Epub 2008 Jun 3. [CrossRef] [PubMed] [PubMed Central]
- Esworthy RS, Baker MA, Chu FF. Expression of selenium-dependent glutathione peroxidase in human breast tumor cell lines. Cancer Res. 1995 Feb 15;55(4):957-62. [PubMed]
- Nguyen VD, Saaranen MJ, Karala AR, Lappi AK, Wang L, Raykhel IB, Alanen HI, Salo KE, Wang CC, Ruddock LW. Two endoplasmic reticulum PDI peroxidases increase the efficiency of the use of peroxide during disulfide bond formation. J Mol Biol. 2011 Feb 25;406(3):503-15. Epub 2011 Jan 5. [CrossRef] [PubMed]
- Wood ZA, Poole LB, Karplus PA. Peroxiredoxin evolution and the regulation of hydrogen peroxide signaling. Science. 2003 Apr 25;300(5619):650-3. [CrossRef] [PubMed]
- Sebastian SA, Kaiwan O, Co EL, Mehendale M, Mohan BP. Current Pharmacologic Options and Emerging Therapeutic Approaches for the Management of Ulcerative Colitis: A Narrative Review. Spartan Med Res J. 2024 Sep 9;9(3):123397. [CrossRef] [PubMed] [PubMed Central]
- Ye K, Chen Z, Xu Y. The double-edged functions of necroptosis. Cell Death Dis. 2023 Feb 27;14(2):163. [CrossRef] [PubMed] [PubMed Central]
- Gao M, Monian P, Pan Q, Zhang W, Xiang J, Jiang X. Ferroptosis is an autophagic cell death process. Cell Res. 2016 Sep;26(9):1021-32. Epub 2016 Aug 12. [CrossRef] [PubMed] [PubMed Central]
- Hou JK, Abraham B, El-Serag H. Dietary intake and risk of developing inflammatory bowel disease: a systematic review of the literature. Am J Gastroenterol. 2011 Apr;106(4):563-73. [CrossRef] [PubMed]
- Oldenburg B, Koningsberger JC, Van Berge Henegouwen GP, Van Asbeck BS, Marx JJ. Iron and inflammatory bowel disease. Aliment Pharmacol Ther. 2001 Apr;15(4):429-38. [CrossRef] [PubMed]
- Murphy TH, Miyamoto M, Sastre A, Schnaar RL, Coyle JT. Glutamate toxicity in a neuronal cell line involves inhibition of cystine transport leading to oxidative stress. Neuron. 1989 Jun;2(6):1547-58. [CrossRef] [PubMed]
- Tallima H, El Ridi R. Arachidonic acid: Physiological roles and potential health benefits - A review. J Adv Res. 2017 Nov 24;11:33-41. [CrossRef] [PubMed] [PubMed Central]
- Platt, SR. The role of glutamate in central nervous system health and disease--a review. Vet J. 2007 Mar;173(2):278-86. Epub 2005 Dec 22. [CrossRef] [PubMed]
- Zhang X, Ma Y, Ji J, Zhao X, Yuan J, Wang H, Lv G. High-fat diet alleviates colitis by inhibiting ferroptosis via solute carrier family seven member 11. J Nutr Biochem. 2022 Nov;109:109106. Epub 2022 Jul 17. [CrossRef] [PubMed]
- Zhang X, Li W, Ma Y, Zhao X, He L, Sun P, Wang H. High-fat diet aggravates colitis-associated carcinogenesis by evading ferroptosis in the ER stress-mediated pathway. Free Radic Biol Med. 2021 Dec;177:156-166. Epub 2021 Oct 21. [CrossRef] [PubMed]
- Mahalhal A, Burkitt MD, Duckworth CA, Hold GL, Campbell BJ, Pritchard DM, Probert CS. Long-Term Iron Deficiency and Dietary Iron Excess Exacerbate Acute Dextran Sodium Sulphate-Induced Colitis and Are Associated with Significant Dysbiosis. Int J Mol Sci. 2021 Mar 31;22(7):3646. [CrossRef] [PubMed] [PubMed Central]
- Moon S, Kim M, Kim Y, Lee S. Supplementation with High or Low Iron Reduces Colitis Severity in an AOM/DSS Mouse Model. Nutrients. 2022 May 12;14(10):2033. [CrossRef] [PubMed] [PubMed Central]
- Zhang Y, Yin L, Zeng X, Li J, Yin Y, Wang Q, Li J, Yang H. Dietary High Dose of Iron Aggravates the Intestinal Injury but Promotes Intestinal Regeneration by Regulating Intestinal Stem Cells Activity in Adult Mice With Dextran Sodium Sulfate-Induced Colitis. Front Vet Sci. 2022 Jun 15;9:870303. [CrossRef] [PubMed] [PubMed Central]
- Carrier JC, Aghdassi E, Jeejeebhoy K, Allard JP. Exacerbation of dextran sulfate sodium-induced colitis by dietary iron supplementation: role of NF-kappaB. Int J Colorectal Dis. 2006 May;21(4):381-7. Epub 2005 Aug 23. [CrossRef] [PubMed]
- Mahalhal A, Frau A, Burkitt MD, Ijaz UZ, Lamb CA, Mansfield JC, Lewis S, Pritchard DM, Probert CS. Oral Ferric Maltol Does Not Adversely Affect the Intestinal Microbiota of Patients or Mice, But Ferrous Sulphate Does. Nutrients. 2021 Jun 30;13(7):2269. [CrossRef] [PubMed] [PubMed Central]
- Mahalhal A, Burkitt MD, Duckworth CA, Hold GL, Campbell BJ, Pritchard DM, Probert CS. Long-Term Iron Deficiency and Dietary Iron Excess Exacerbate Acute Dextran Sodium Sulphate-Induced Colitis and Are Associated with Significant Dysbiosis. Int J Mol Sci. 2021 Mar 31;22(7):3646. [CrossRef] [PubMed] [PubMed Central]
- Mahalhal A, Williams JM, Johnson S, Ellaby N, Duckworth CA, Burkitt MD, Liu X, Hold GL, Campbell BJ, Pritchard DM, Probert CS. Oral iron exacerbates colitis and influences the intestinal microbiota. PLoS One. 2018 Oct 11;13(10):e0202460. [CrossRef] [PubMed] [PubMed Central]
- Song Y, Song Q, Tan F, Wang Y, Li C, Liao S, Yu K, Mei Z, Lv L. Seliciclib alleviates ulcerative colitis by inhibiting ferroptosis and improving intestinal inflammation. Life Sci. 2024 Aug 15;351:122794. Epub 2024 Jun 10. [CrossRef] [PubMed]
- Zhang Y, Yin L, Zeng X, Li J, Yin Y, Wang Q, Li J, Yang H. Dietary High Dose of Iron Aggravates the Intestinal Injury but Promotes Intestinal Regeneration by Regulating Intestinal Stem Cells Activity in Adult Mice With Dextran Sodium Sulfate-Induced Colitis. Front Vet Sci. 2022 Jun 15;9:870303. [CrossRef] [PubMed] [PubMed Central]
- Chen X, Yu C, Kang R, Tang D. Iron Metabolism in Ferroptosis. Front Cell Dev Biol. 2020 Oct 7;8:590226. [CrossRef] [PubMed] [PubMed Central]
- Maiorino M, Conrad M, Ursini F. GPx4, Lipid Peroxidation, and Cell Death: Discoveries, Rediscoveries, and Open Issues. Antioxid Redox Signal. 2018 Jul 1;29(1):61-74. Epub 2017 May 30. [CrossRef] [PubMed]
- Lee JY, Kim WK, Bae KH, Lee SC, Lee EW. Lipid Metabolism and Ferroptosis. Biology (Basel). 2021 Mar 2;10(3):184. [CrossRef] [PubMed] [PubMed Central]
- Kakhlon O, Cabantchik ZI. The labile iron pool: characterization, measurement, and participation in cellular processes(1). Free Radic Biol Med. 2002 Oct 15;33(8):1037-46. [CrossRef] [PubMed]
- Parant, F.;Mure, F.;Maurin, J.; Beauvilliers, L.; Chorfa, C.; El Jamali, C.; Ohlmann, T.; Chavatte, L. Selenium Discrepancies in Fetal Bovine Serum: Impact on Cellular Selenoprotein Expression. Int. J.Mol. Sci. 2024, 25, 7261. [CrossRef] [PubMed]
- Park VS, Pope LE, Ingram J, Alchemy GA, Purkal J, Andino-Frydman EY, Jin S, Singh S, Chen A, Narayanan P, Kongpachith S, Phillips DC, Dixon SJ, Popovic R. Lipid composition differentiates ferroptosis sensitivity between in vitro and in vivo systems. bioRxiv [Preprint]. 2024 Nov 15:2024.11.14.622381. [CrossRef] [PubMed] [PubMed Central]
- Santesmasses D, Gladyshev VN. Selenocysteine Machinery Primarily Supports TXNRD1 and GPX4 Functions and Together They Are Functionally Linked with SCD and PRDX6. Biomolecules. 2022 Jul 28;12(8):1049. [CrossRef] [PubMed] [PubMed Central]
- Stockwell BR, Friedmann Angeli JP, Bayir H, Bush AI, Conrad M, Dixon SJ, Fulda S, Gascón S, Hatzios SK, Kagan VE, Noel K, Jiang X, Linkermann A, Murphy ME, Overholtzer M, Oyagi A, Pagnussat GC, Park J, Ran Q, Rosenfeld CS, Salnikow K, Tang D, Torti FM, Torti SV, Toyokuni S, Woerpel KA, Zhang DD. Ferroptosis: A Regulated Cell Death Nexus Linking Metabolism, Redox Biology, and Disease. Cell. 2017 Oct 5;171(2):273-285. [CrossRef] [PubMed] [PubMed Central]
- Stockwell, BR. Ferroptosis turns 10: Emerging mechanisms, physiological functions, and therapeutic applications. Cell. 2022 Jul 7;185(14):2401-2421. [CrossRef] [PubMed] [PubMed Central]
- Lin S, Zheng Y, Chen M, Xu L, Huang H. The interactions between ineffective erythropoiesis and ferroptosis in β-thalassemia. Front Physiol. 2024 Feb 26;15:1346173. [CrossRef] [PubMed] [PubMed Central]
- Chassaing B, Aitken JD, Malleshappa M, Vijay-Kumar M. Dextran sulfate sodium (DSS)-induced colitis in mice. Curr Protoc Immunol. 2014 Feb 4;104:15.25.1-15.25.14. [CrossRef] [PubMed] [PubMed Central]
- Dieleman LA, Ridwan BU, Tennyson GS, Beagley KW, Bucy RP, Elson CO. Dextran sulfate sodium-induced colitis occurs in severe combined immunodeficient mice. Gastroenterology. 1994 Dec;107(6):1643-52. [CrossRef] [PubMed]
- Kim TW, Seo JN, Suh YH, Park HJ, Kim JH, Kim JY, Oh KI. Involvement of lymphocytes in dextran sulfate sodium-induced experimental colitis. World J Gastroenterol. 2006 Jan 14;12(2):302-5. [CrossRef] [PubMed] [PubMed Central]
- Gancarcikova S, Lauko S, Hrckova G, Andrejcakova Z, Hajduckova V, Madar M, Kolesar Fecskeova L, Mudronova D, Mravcova K, Strkolcova G, Nemcova R, Kacirova J, Staskova A, Vilcek S, Bomba A. Innovative Animal Model of DSS-Induced Ulcerative Colitis in Pseudo Germ-Free Mice. Cells. 2020 Dec 1;9(12):2571. [CrossRef] [PubMed] [PubMed Central]
- Yang C, Merlin D. Unveiling Colitis: A Journey through the Dextran Sodium Sulfate-induced Model. Inflamm Bowel Dis. 2024 May 2;30(5):844-853. [CrossRef] [PubMed] [PubMed Central]
- Maiorino M, Gregolin C, Ursini F. Phospholipid hydroperoxide glutathione peroxidase. Methods Enzymol. 1990;186:448-57. [CrossRef] [PubMed]
- Kato C, Suzuki Y, Parida IS, Kato S, Yamasaki H, Takekoshi S, Nakagawa K. Possible Glutathione Peroxidase 4-Independent Reduction of Phosphatidylcholine Hydroperoxide: Its Relevance to Ferroptosis. J Oleo Sci. 2022 Oct 28;71(11):1689-1694. Epub 2022 Oct 5. [CrossRef] [PubMed]
- Luo P, Liu D, Zhang Q, Yang F, Wong YK, Xia F, Zhang J, Chen J, Tian Y, Yang C, Dai L, Shen HM, Wang J. Celastrol induces ferroptosis in activated HSCs to ameliorate hepatic fibrosis via targeting peroxiredoxins and HO-1. Acta Pharm Sin B. 2022 May;12(5):2300-2314. Epub 2021 Dec 18. [CrossRef] [PubMed] [PubMed Central]
- Song Y, Wang X, Sun Y, Yu N, Tian Y, Han J, Qu X, Yu X. PRDX1 inhibits ferroptosis by binding to Cullin-3 as a molecular chaperone in colorectal cancer. Int J Biol Sci. 2024 Sep 23;20(13):5070-5086. [CrossRef] [PubMed] [PubMed Central]
- Lai W, Zhu W, Wu J, Huang J, Li X, Luo Y, Wang Y, Zeng H, Li M, Qiu X, Wen X. HJURP inhibits sensitivity to ferroptosis inducers in prostate cancer cells by enhancing the peroxidase activity of PRDX1. Redox Biol. 2024 Nov;77:103392. Epub 2024 Oct 10. [CrossRef] [PubMed] [PubMed Central]
- He J, Hou X, Wu J, Wang K, Qi X, Wei Z, Sun Y, Wang C, Yao H, Liu K. Hspb1 protects against severe acute pancreatitis by attenuating apoptosis and ferroptosis via interacting with Anxa2 to restore the antioxidative activity of Prdx1. Int J Biol Sci. 2024 Feb 25;20(5):1707-1728. doi: 10.7150/ijbs.84494. PMID: 38481805; PMCID: PMC10929186. 200. Chen P, Chen Z, Zhai J, Yang W, Wei H. Overexpression of PRDX2 in Adipose-Derived Mesenchymal Stem Cells Enhances the Therapeutic Effect in a Neurogenic Erectile Dysfunction Rat Model by Inhibiting Ferroptosis. Oxid Med Cell Longev. 2023 Feb 8;2023:4952857. [CrossRef] [PubMed] [PubMed Central]
- Sun Y, Qiao Y, Liu Y, Zhou J, Wang X, Zheng H, Xu Z, Zhang J, Zhou Y, Qian L, Zhang C, Lou H. ent-Kaurane diterpenoids induce apoptosis and ferroptosis through targeting redox resetting to overcome cisplatin resistance. Redox Biol. 2021 Jul;43:101977. doi: 10.1016/j.redox.2021.101977. Epub 2021 Apr 16. Erratum in: Redox Biol. 2024 Jun;72:103164. [CrossRef] [PubMed] [PubMed Central]
- Xu S, Liu Y, Yang S, Fei W, Qin J, Lu W, Xu J. FXN targeting induces cell death in ovarian cancer stem-like cells through PRDX3-Mediated oxidative stress. iScience. 2024 Jul 14;27(8):110506. [CrossRef] [PubMed] [PubMed Central]
- Cui S, Ghai A, Deng Y, Li S, Zhang R, Egbulefu C, Liang G, Achilefu S, Ye J. Identification of hyperoxidized PRDX3 as a ferroptosis marker reveals ferroptotic damage in chronic liver diseases. Mol Cell. 2023 Nov 2;83(21):3931-3939.e5. Epub 2023 Oct 19. [CrossRef] [PubMed] [PubMed Central]
- Rashba-Step J, Tatoyan A, Duncan R, Ann D, Pushpa-Rehka TR, Sevanian A. Phospholipid peroxidation induces cytosolic phospholipase A2 activity: membrane effects versus enzyme phosphorylation. Arch Biochem Biophys. 1997 Jul 1;343(1):44-54. [CrossRef] [PubMed]
- Scanavachi G, Coutinho A, Fedorov AA, Prieto M, Melo AM, Itri R. Lipid Hydroperoxide Compromises the Membrane Structure Organization and Softens Bending Rigidity. Langmuir. 2021 Aug 24;37(33):9952-9963. Epub 2021 Aug 10. [CrossRef] [PubMed]
- Saraev DD, Pratt DA. Reactions of lipid hydroperoxides and how they may contribute to ferroptosis sensitivity. Curr Opin Chem Biol. 2024 Aug;81:102478. Epub 2024 Jun 21. [CrossRef] [PubMed]
- Sun WY, Tyurin VA, Mikulska-Ruminska K, Shrivastava IH, Anthonymuthu TS, Zhai YJ, Pan MH, Gong HB, Lu DH, Sun J, Duan WJ, Korolev S, Abramov AY, Angelova PR, Miller I, Beharier O, Mao GW, Dar HH, Kapralov AA, Amoscato AA, Hastings TG, Greenamyre TJ, Chu CT, Sadovsky Y, Bahar I, Bayır H, Tyurina YY, He RR, Kagan VE. Phospholipase iPLA2β averts ferroptosis by eliminating a redox lipid death signal. Nat Chem Biol. 2021 Apr;17(4):465-476. Epub 2021 Feb 4. [CrossRef] [PubMed] [PubMed Central]
- Oh M, Jang SY, Lee JY, Kim JW, Jung Y, Kim J, Seo J, Han TS, Jang E, Son HY, Kim D, Kim MW, Park JS, Song KH, Oh KJ, Kim WK, Bae KH, Huh YM, Kim SH, Kim D, Han BS, Lee SC, Hwang GS, Lee EW, The lipoprotein-associated phospholipase A2 inhibitor Darapladib sensitises cancer cells to ferroptosis by remodelling lipid metabolism. Nat Commun. 2023 Sep 15;14(1):5728. [CrossRef] [PubMed] [PubMed Central]
- Adibhatla RM, Hatcher JF. Phospholipase A(2), reactive oxygen species, and lipid peroxidation in CNS pathologies. BMB Rep. 2008 Aug 31;41(8):560-7. [CrossRef] [PubMed] [PubMed Central]
- Chen JW, Dodia C, Feinstein SI, Jain MK, Fisher AB. 1-Cys peroxiredoxin, a bifunctional enzyme with glutathione peroxidase and phospholipase A2 activities. J Biol Chem. 2000 Sep 15;275(37):28421-7. [CrossRef] [PubMed]
- Fisher, AB. Peroxiredoxin 6 in the repair of peroxidized cell membranes and cell signaling. Arch Biochem Biophys. 2017 Mar 1;617:68-83. Epub 2016 Dec 6. [CrossRef] [PubMed] [PubMed Central]
- Chen Z, Inague A, Kaushal K, Fazeli G, N Xavier da Silva T, Ferreira Dos Santos A, Cheytan T, Porto Freitas F, Yildiz U, Gasparello Viviani L, Santiago Lima R, Peglow Pinz M, Medeiros I, Geronimo Pires Alegria T, Pereira da Silva R, Regina Diniz L, Weinzweig S, Klein-Seetharaman J, Trumpp A, Manas A, Hondal R, Fischer M, Bartenhagen C, Shimada BK, Seale LA, Fabiano M, Schweizer U, Netto LE, Meotti FC, Alborzinia H, Miyamoto S, Friedmann Angeli JP. PRDX6 contributes to selenocysteine metabolism and ferroptosis resistance. bioRxiv [Preprint]. 2024 Jun 6:2024.06.04.597364. [CrossRef] [PubMed] [PubMed Central]
- Doll S, Freitas FP, Shah R, Aldrovandi M, da Silva MC, Ingold I, Goya Grocin A, Xavier da Silva TN, Panzilius E, Scheel CH, Mourão A, Buday K, Sato M, Wanninger J, Vignane T, Mohana V, Rehberg M, Flatley A, Schepers A, Kurz A, White D, Sauer M, Sattler M, Tate EW, Schmitz W, Schulze A, O'Donnell V, Proneth B, Popowicz GM, Pratt DA, Angeli JPF, Conrad M. FSP1 is a glutathione-independent ferroptosis suppressor. Nature. 2019 Nov;575(7784):693-698. Epub 2019 Oct 21. [CrossRef] [PubMed]
- Mantle D, Heaton RA, Hargreaves IP. Coenzyme Q10 and Immune Function: An Overview. Antioxidants (Basel). 2021 May 11;10(5):759. [CrossRef] [PubMed] [PubMed Central]
- Fujita H, Tanaka YK, Ogata S, Suzuki N, Kuno S, Barayeu U, Akaike T, Ogra Y, Iwai K. PRDX6 augments selenium utilization to limit iron toxicity and ferroptosis. Nat Struct Mol Biol. 2024 Aug;31(8):1277-1285. Epub 2024 Jun 12. [CrossRef] [PubMed] [PubMed Central]
- Chen Z, Inague A, Kaushal K, Fazeli G, Schilling D, Xavier da Silva TN, Dos Santos AF, Cheytan T, Freitas FP, Yildiz U, Viviani LG, Lima RS, Pinz MP, Medeiros I, Iijima TS, Alegria TGP, Pereira da Silva R, Diniz LR, Weinzweig S, Klein-Seetharaman J, Trumpp A, Mañas A, Hondal R, Bartenhagen C, Fischer M, Shimada BK, Seale LA, Chillon TS, Fabiano M, Schomburg L, Schweizer U, Netto LE, Meotti FC, Dick TP, Alborzinia H, Miyamoto S, Friedmann Angeli JP. PRDX6 contributes to selenocysteine metabolism and ferroptosis resistance. Mol Cell. 2024 Nov 7:S1097-2765(24)00867-0. Epub ahead of print. [CrossRef] [PubMed]
- Torres-Velarde JM, Allen KN, Salvador-Pascual A, Leija RG, Luong D, Moreno-Santillán DD, Ensminger DC, Vázquez-Medina JP. Peroxiredoxin 6 suppresses ferroptosis in lung endothelial cells. Free Radic Biol Med. 2024 Jun;218:82-93. Epub 2024 Apr 3. [CrossRef] [PubMed] [PubMed Central]
- Fisher AB, Dodia C, Sorokina EM, Li H, Zhou S, Raabe T, Feinstein SI. A novel lysophosphatidylcholine acyl transferase activity is expressed by peroxiredoxin 6. J Lipid Res. 2016 Apr;57(4):587-96. Epub 2016 Feb 1. [CrossRef] [PubMed] [PubMed Central]
- Lagal DJ, Ortiz-Alcántara Á, Pedrajas JR, McDonagh B, Bárcena JA, Requejo-Aguilar R, Padilla CA. Loss of peroxiredoxin 6 (PRDX6) alters lipid composition and distribution resulting in increased sensitivity to ferroptosis. Biochem J. 2024 Nov 27:BCJ20240445. Epub ahead of print. [CrossRef] [PubMed]
- Esworthy RS, Chu FF, Doroshow JH. Analysis of glutathione-related enzymes. Curr Protoc Toxicol. 2001 May;Chapter 7:Unit7.1. [CrossRef] [PubMed]
- Storch J, McDermott L. Structural and functional analysis of fatty acid-binding proteins. J Lipid Res. 2009 Apr;50 Suppl(Suppl):S126-31. Epub 2008 Nov 17. [CrossRef] [PubMed] [PubMed Central]
- Catalá, A. Five decades with polyunsaturated Fatty acids: chemical synthesis, enzymatic formation, lipid peroxidation and its biological effects. J Lipids. 2013;2013:710290. Epub 2013 Dec 30. [CrossRef] [PubMed] [PubMed Central]
- Ek-Von Mentzer BA, Zhang F, Hamilton JA. Binding of 13-HODE and 15-HETE to phospholipid bilayers, albumin, and intracellular fatty acid binding proteins. implications for transmembrane and intracellular transport and for protection from lipid peroxidation. J Biol Chem. 2001 May 11;276(19):15575-80. Epub 2001 Jan 30. [CrossRef] [PubMed]
- Catalá, A. Interaction of fatty acids, acyl-CoA derivatives and retinoids with microsomal membranes: effect of cytosolic proteins. Mol Cell Biochem. 1993 Mar 24;120(2):89-94. [CrossRef] [PubMed]
- Guajardo MH, Terrasa AM, Catalá A. Retinal fatty acid binding protein reduce lipid peroxidation stimulated by long-chain fatty acid hydroperoxides on rod outer segments. Biochim Biophys Acta. 2002 Apr 15;1581(3):65-74. [CrossRef] [PubMed]
- Fan X, Xu M, Ren Q, Fan Y, Liu B, Chen J, Wang Z, Sun X. Downregulation of fatty acid binding protein 4 alleviates lipid peroxidation and oxidative stress in diabetic retinopathy by regulating peroxisome proliferator-activated receptor γ-mediated ferroptosis. Bioengineered. 2022 Apr;13(4):10540-10551. [CrossRef] [PubMed] [PubMed Central]
- Sun J, Esplugues E, Bort A, Cardelo MP, Ruz-Maldonado I, Fernández-Tussy P, Wong C, Wang H, Ojima I, Kaczocha M, Perry R, Suárez Y, Fernández-Hernando C. Fatty acid binding protein 5 suppression attenuates obesity-induced hepatocellular carcinoma by promoting ferroptosis and intratumoral immune rewiring. Nat Metab. 2024 Apr;6(4):741-763. Epub 2024 Apr 25. [CrossRef] [PubMed]
- Mayr L, Grabherr F, Schwärzler J, Reitmeier I, Sommer F, Gehmacher T, Niederreiter L, He GW, Ruder B, Kunz KTR, Tymoszuk P, Hilbe R, Haschka D, Feistritzer C, Gerner RR, Enrich B, Przysiecki N, Seifert M, Keller MA, Oberhuber G, Sprung S, Ran Q, Koch R, Effenberger M, Tancevski I, Zoller H, Moschen AR, Weiss G, Becker C, Rosenstiel P, Kaser A, Tilg H, Adolph TE. Dietary lipids fuel GPX4-restricted enteritis resembling Crohn's disease. Nat Commun. 2020 Apr 14;11(1):1775. [CrossRef] [PubMed] [PubMed Central]
- Yan J, Zeng Y, Guan Z, Li Z, Luo S, Niu J, Zhao J, Gong H, Huang T, Li Z, Deng A, Wen Q, Tan J, Jiang J, Bao X, Li S, Sun G, Zhang M, Zhi M, Yin Z, Sun WY, Li YF, He RR, Cao G. Inherent preference for polyunsaturated fatty acids instigates ferroptosis of Treg cells that aggravates high-fat-diet-related colitis. Cell Rep. 2024 Aug 27;43(8):114636. Epub 2024 Aug 17. [CrossRef] [PubMed]
- Xu M, Tao J, Yang Y, Tan S, Liu H, Jiang J, Zheng F, Wu B. Ferroptosis involves in intestinal epithelial cell death in ulcerative colitis. Cell Death Dis. 2020 Feb 3;11(2):86. [CrossRef] [PubMed] [PubMed Central]
- Hondal, RJ. Selenium vitaminology: The connection between selenium, vitamin C, vitamin E, and ergothioneine. Curr Opin Chem Biol. 2023 Aug;75:102328. Epub 2023 May 24. [CrossRef] [PubMed] [PubMed Central]
- Gao Q, Esworthy RS, Kim BW, Synold TW, Smith DD, Chu FF. Atherogenic diets exacerbate colitis in mice deficient in glutathione peroxidase. Inflamm Bowel Dis. 2010 Dec;16(12):2043-54. [CrossRef] [PubMed] [PubMed Central]
- Kaser A, Lee AH, Franke A, Glickman JN, Zeissig S, Tilg H, Nieuwenhuis EE, Higgins DE, Schreiber S, Glimcher LH, Blumberg RS. XBP1 links ER stress to intestinal inflammation and confers genetic risk for human inflammatory bowel disease. Cell. 2008 Sep 5;134(5):743-56. [CrossRef] [PubMed] [PubMed Central]
- Deka D, D'Incà R, Sturniolo GC, Das A, Pathak S, Banerjee A. Role of ER Stress Mediated Unfolded Protein Responses and ER Stress Inhibitors in the Pathogenesis of Inflammatory Bowel Disease. Dig Dis Sci. 2022 Dec;67(12):5392-5406. Epub 2022 Mar 22. [CrossRef] [PubMed]
- Cadwell K, Liu JY, Brown SL, Miyoshi H, Loh J, Lennerz JK, Kishi C, Kc W, Carrero JA, Hunt S, Stone CD, Brunt EM, Xavier RJ, Sleckman BP, Li E, Mizushima N, Stappenbeck TS, Virgin HW 4th. A key role for autophagy and the autophagy gene Atg16l1 in mouse and human intestinal Paneth cells. Nature. 2008 Nov 13;456(7219):259-63. Epub 2008 Oct 5. [CrossRef] [PubMed] [PubMed Central]
- Miotto G, Rossetto M, Di Paolo ML, Orian L, Venerando R, Roveri A, Vučković AM, Bosello Travain V, Zaccarin M, Zennaro L, Maiorino M, Toppo S, Ursini F, Cozza G. Insight into the mechanism of ferroptosis inhibition by ferrostatin-1. Redox Biol. 2020 Jan;28:101328. Epub 2019 Sep 20. [CrossRef] [PubMed] [PubMed Central]
- Wang C, Chu Q, Dong W, Wang X, Zhao W, Dai X, Liu W, Wang B, Liu T, Zhong W, Jiang C, Cao H. Microbial metabolite deoxycholic acid-mediated ferroptosis exacerbates high-fat diet-induced colonic inflammation. Mol Metab. 2024 Jun;84:101944. Epub 2024 Apr 18. [CrossRef] [PubMed] [PubMed Central]
- Cheli VT, Santiago González DA, Marziali LN, Zamora NN, Guitart ME, Spreuer V, Pasquini JM, Paez PM. The Divalent Metal Transporter 1 (DMT1) Is Required for Iron Uptake and Normal Development of Oligodendrocyte Progenitor Cells. J Neurosci. 2018 Oct 24;38(43):9142-9159. Epub 2018 Sep 6. [CrossRef] [PubMed] [PubMed Central]
- Singhal R, Mitta SR, Das NK, Kerk SA, Sajjakulnukit P, Solanki S, Andren A, Kumar R, Olive KP, Banerjee R, Lyssiotis CA, Shah YM. HIF-2α activation potentiates oxidative cell death in colorectal cancers by increasing cellular iron. J Clin Invest. 2021 Jun 15;131(12):e143691. [CrossRef] [PubMed] [PubMed Central]
- Zhao S, Gong Z, Zhou J, Tian C, Gao Y, Xu C, Chen Y, Cai W, Wu J. Deoxycholic Acid Triggers NLRP3 Inflammasome Activation and Aggravates DSS-Induced Colitis in Mice. Front Immunol. 2016 Nov 28;7:536. [CrossRef] [PubMed] [PubMed Central]
- Newmark HL, Lipkin M, Maheshwari N. Colonic hyperplasia and hyperproliferation induced by a nutritional stress diet with four components of Western-style diet. J Natl Cancer Inst. 1990 Mar 21;82(6):491-6. [CrossRef] [PubMed]
- Geiszt M, Lekstrom K, Brenner S, Hewitt SM, Dana R, Malech HL, Leto TL. NAD(P)H oxidase 1, a product of differentiated colon epithelial cells, can partially replace glycoprotein 91phox in the regulated production of superoxide by phagocytes. J Immunol. 2003 Jul 1;171(1):299-306. [CrossRef] [PubMed]
- Laleu B, Gaggini F, Orchard M, Fioraso-Cartier L, Cagnon L, Houngninou-Molango S, Gradia A, Duboux G, Merlot C, Heitz F, Szyndralewiez C, Page P. First in class, potent, and orally bioavailable NADPH oxidase isoform 4 (Nox4) inhibitors for the treatment of idiopathic pulmonary fibrosis. J Med Chem. 2010 Nov 11;53(21):7715-30. [CrossRef] [PubMed]
- Zhang X, Ma Y, Ji J, Zhao X, Yuan J, Wang H, Lv G. High-fat diet alleviates colitis by inhibiting ferroptosis via solute carrier family seven member 11. J Nutr Biochem. 2022 Nov;109:109106. Epub 2022 Jul 17. [CrossRef] [PubMed]
- Crawford RR, Prescott ET, Sylvester CF, Higdon AN, Shan J, Kilberg MS, Mungrue IN. Human CHAC1 Protein Degrades Glutathione, and mRNA Induction Is Regulated by the Transcription Factors ATF4 and ATF3 and a Bipartite ATF/CRE Regulatory Element. J Biol Chem. 2015 Jun 19;290(25):15878-15891. Epub 2015 Apr 30. [CrossRef] [PubMed] [PubMed Central]
- Sun J, Ren H, Wang J, Xiao X, Zhu L, Wang Y, Yang L. CHAC1: a master regulator of oxidative stress and ferroptosis in human diseases and cancers. Front Cell Dev Biol. 2024 Oct 29;12:1458716. [CrossRef] [PubMed] [PubMed Central]
- Wek, RC. Role of eIF2α Kinases in Translational Control and Adaptation to Cellular Stress. Cold Spring Harb Perspect Biol. 2018 Jul 2;10(7):a032870. [CrossRef] [PubMed] [PubMed Central]
- Esworthy RS, Kim BW, Rivas GE, Leto TL, Doroshow JH, Chu FF. Analysis of candidate colitis genes in the Gdac1 locus of mice deficient in glutathione peroxidase-1 and -2. PLoS One. 2012;7(9):e44262. Epub 2012 Sep 6. [CrossRef] [PubMed] [PubMed Central]
- Gao S, Sun C, Kong J. Vitamin D Attenuates Ulcerative Colitis by Inhibiting ACSL4-Mediated Ferroptosis. Nutrients. 2023 Nov 20;15(22):4845. [CrossRef] [PubMed] [PubMed Central]
- Wen W, Xu Y, Qian W, Huang L, Gong J, Li Y, Zhu W, Guo Z. PUFAs add fuel to Crohn's disease-associated AIEC-induced enteritis by exacerbating intestinal epithelial lipid peroxidation. Gut Microbes. 2023 Dec;15(2):2265578. Epub 2023 Oct 6. [CrossRef] [PubMed] [PubMed Central]
- Deng L, He S, Li Y, Ding R, Li X, Guo N, Luo L. Identification of Lipocalin 2 as a Potential Ferroptosis-related Gene in Ulcerative Colitis. Inflamm Bowel Dis. 2023 Sep 1;29(9):1446-1457. [CrossRef] [PubMed]
- Chen Z, Gu Q, Chen R. Promotive role of IRF7 in ferroptosis of colonic epithelial cells in ulcerative colitis by the miR-375-3p/SLC11A2 axis. Biomol Biomed. 2023 May 1;23(3):437-449. [CrossRef] [PubMed] [PubMed Central]
- Chen Y, Zhang P, Chen W, Chen G. Ferroptosis mediated DSS-induced ulcerative colitis associated with Nrf2/HO-1 signaling pathway. Immunol Lett. 2020 Sep;225:9-15. Epub 2020 Jun 12. [CrossRef] [PubMed]
- Brzozowa-Zasada M, Ianaro A, Piecuch A, Michalski M, Matysiak N, Stęplewska K. Immunohistochemical Expression of Glutathione Peroxidase-2 (Gpx-2) and Its Clinical Relevance in Colon Adenocarcinoma Patients. Int J Mol Sci. 2023 Sep 27;24(19):14650. [CrossRef] [PubMed] [PubMed Central]
- Takagi T, Homma T, Fujii J, Shirasawa N, Yoriki H, Hotta Y, Higashimura Y, Mizushima K, Hirai Y, Katada K, Uchiyama K, Naito Y, Itoh Y. Elevated ER stress exacerbates dextran sulfate sodium-induced colitis in PRDX4-knockout mice. Free Radic Biol Med. 2019 Apr;134:153-164. Epub 2018 Dec 19. [CrossRef] [PubMed]
- Miyamoto Y, Koh YH, Park YS, Fujiwara N, Sakiyama H, Misonou Y, Ookawara T, Suzuki K, Honke K, Taniguchi N. Oxidative stress caused by inactivation of glutathione peroxidase and adaptive responses. Biol Chem. 2003 Apr;384(4):567-74. [CrossRef] [PubMed]
- Melhem H, Spalinger MR, Cosin-Roger J, Atrott K, Lang S, Wojtal KA, Vavricka SR, Rogler G, Frey-Wagner I. Prdx6 Deficiency Ameliorates DSS Colitis: Relevance of Compensatory Antioxidant Mechanisms. J Crohns Colitis. 2017 Jul 1;11(7):871-884. [CrossRef] [PubMed]
- Liu J, Sun L, Chen D, Huo X, Tian X, Li J, Liu M, Yu Z, Zhang B, Yang Y, Qiu Y, Liu Y, Guo H, Zhou C, Ma X, Xiong Y. Prdx6-induced inhibition of ferroptosis in epithelial cells contributes to liquiritin-exerted alleviation of colitis. Food Funct. 2022 Sep 22;13(18):9470-9480. [CrossRef] [PubMed]
- Fuqua BK, Vulpe CD, Anderson GJ. Intestinal iron absorption. J Trace Elem Med Biol. 2012 Jun;26(2-3):115-9. Epub 2012 May 8. [CrossRef] [PubMed]
- Kobayashi Y, Ohfuji S, Kondo K, Fukushima W, Sasaki S, Kamata N, Yamagami H, Fujiwara Y, Suzuki Y, Hirota Y; Japanese Case-Control Study Group for Ulcerative Colitis. Association between dietary iron and zinc intake and development of ulcerative colitis: A case-control study in Japan. J Gastroenterol Hepatol. 2019 Oct;34(10):1703-1710. Epub 2019 Mar 21. [CrossRef] [PubMed]
- Werner T, Wagner SJ, Martínez I, Walter J, Chang JS, Clavel T, Kisling S, Schuemann K, Haller D. Depletion of luminal iron alters the gut microbiota and prevents Crohn's disease-like ileitis. Gut. 2011 Mar;60(3):325-33. Epub 2010 Nov 12. [CrossRef] [PubMed]
- Ye Y, Liu L, Feng Z, Liu Y, Miao J, Wei X, Li H, Yang J, Cao X, Zhao J. The ERK-cPLA2-ACSL4 axis mediating M2 macrophages ferroptosis impedes mucosal healing in ulcerative colitis. Free Radic Biol Med. 2024 Mar;214:219-235. Epub 2024 Feb 15. [CrossRef] [PubMed]
- Ding K, Liu C, Li L, Yang M, Jiang N, Luo S, Sun L. Acyl-CoA synthase ACSL4: an essential target in ferroptosis and fatty acid metabolism. Chin Med J (Engl). 2023 Nov 5;136(21):2521-2537. [CrossRef] [PubMed] [PubMed Central]
- Li X, He J, Gao X, Zheng G, Chen C, Chen Y, Xing Z, Wang T, Tang J, Guo Y, He Y. GPX4 restricts ferroptosis of NKp46+ILC3s to control intestinal inflammation. Cell Death Dis. 2024 Sep 19;15(9):687. [CrossRef] [PubMed] [PubMed Central]
- Zeng B, Shi S, Ashworth G, Dong C, Liu J, Xing F. ILC3 function as a double-edged sword in inflammatory bowel diseases. Cell Death Dis. 2019 Apr 8;10(4):315. [CrossRef] [PubMed] [PubMed Central]
- Yang F, Chen Y, Xiao Y, Jiang H, Jiang Z, Yang M, Li M, Su Y, Yan Z, Lin Y, Li D. pH-sensitive molybdenum (Mo)-based polyoxometalate nanoclusters have therapeutic efficacy in inflammatory bowel disease by counteracting ferroptosis. Pharmacol Res. 2023 Feb;188:106645. Epub 2023 Jan 4. [CrossRef] [PubMed]
- Wang S, Liu W, Wang J, Bai X. Curculigoside inhibits ferroptosis in ulcerative colitis through the induction of GPX4. Life Sci. 2020 Oct 15;259:118356. Epub 2020 Aug 28. [CrossRef] [PubMed]
- Xu J, Liu S, Cui Z, Wang X, Ning T, Wang T, Zhang N, Xie S, Min L, Zhang S, Liang C, Zhu S. Ferrostatin-1 alleviated TNBS induced colitis via the inhibition of ferroptosis. Biochem Biophys Res Commun. 2021 Oct 8;573:48-54. Epub 2021 Aug 8. [CrossRef] [PubMed]
- Panda SK, Peng V, Sudan R, Ulezko Antonova A, Di Luccia B, Ohara TE, Fachi JL, Grajales-Reyes GE, Jaeger N, Trsan T, Gilfillan S, Cella M, Colonna M. Repression of the aryl-hydrocarbon receptor prevents oxidative stress and ferroptosis of intestinal intraepithelial lymphocytes. Immunity. 2023 Apr 11;56(4):797-812.e4. Epub 2023 Feb 16. [CrossRef] [PubMed] [PubMed Central]
- Lamas B, Natividad JM, Sokol H. Aryl hydrocarbon receptor and intestinal immunity. Mucosal Immunol. 2018 Jul;11(4):1024-1038. Epub 2018 Apr 7. [CrossRef] [PubMed]
- Westphal C, Konkel A, Schunck WH. CYP-eicosanoids--a new link between omega-3 fatty acids and cardiac disease? Prostaglandins Other Lipid Mediat. 2011 Nov;96(1-4):99-108. Epub 2011 Sep 16. [CrossRef] [PubMed]
- Veith A, Moorthy B. ROLE OF CYTOCHROME P450S IN THE GENERATION AND METABOLISM OF REACTIVE OXYGEN SPECIES. Curr Opin Toxicol. 2018 Feb;7:44-51. Epub 2017 Oct 12. [CrossRef] [PubMed] [PubMed Central]
- Brandstätter O, Schanz O, Vorac J, König J, Mori T, Maruyama T, Korkowski M, Haarmann-Stemmann T, von Smolinski D, Schultze JL, Abel J, Esser C, Takeyama H, Weighardt H, Förster I. Balancing intestinal and systemic inflammation through cell type-specific expression of the aryl hydrocarbon receptor repressor. Sci Rep. 2016 May 17;6:26091. [CrossRef] [PubMed] [PubMed Central]
- Sen A, Stark H. Role of cytochrome P450 polymorphisms and functions in development of ulcerative colitis. World J Gastroenterol. 2019 Jun 21;25(23):2846-2862. [CrossRef] [PubMed] [PubMed Central]
- Buyukgoze O, Osmanoglu N, Arslan S, Sen A. Association of the CYP1A12A, GSTT1 null, GSTM1 null, mEPHX3, and XRCC1-399 genetic polymorphisms with ulcerative colitis. Int J Colorectal Dis. 2013 Apr;28(4):593-5. Epub 2012 Jun 5. [CrossRef] [PubMed]
- Dong F, Perdew GH. The aryl hydrocarbon receptor as a mediator of host-microbiota interplay. Gut Microbes. 2020 Nov 9;12(1):1859812. Epub 2020 Dec 17. [CrossRef] [PubMed] [PubMed Central]
- Li P, Jiang M, Li K, Li H, Zhou Y, Xiao X, Xu Y, Krishfield S, Lipsky PE, Tsokos GC, Zhang X. Glutathione peroxidase 4-regulated neutrophil ferroptosis induces systemic autoimmunity. Nat Immunol. 2021 Sep;22(9):1107-1117. Epub 2021 Aug 12. [CrossRef] [PubMed] [PubMed Central]
- Cui JX, Xu XH, He T, Liu JJ, Xie TY, Tian W, Liu JY. L-kynurenine induces NK cell loss in gastric cancer microenvironment via promoting ferroptosis. J Exp Clin Cancer Res. 2023 Mar 1;42(1):52. [CrossRef] [PubMed] [PubMed Central]
- Sok SPM, Pipkin K, Popescu NI, Reidy M, Li B, Van Remmen H, Kinter M, Sun XH, Fan Z, Zhao M. Gpx4 Regulates Invariant NKT Cell Homeostasis and Function by Preventing Lipid Peroxidation and Ferroptosis J Immunol. 2024 Oct 1;213(7):941-951. [CrossRef] [PubMed] [PubMed Central]
- Chu FF, Esworthy RS, Shen B, Doroshow JH. Role of the microbiota in ileitis of a mouse model of inflammatory bowel disease-Glutathione peroxide isoenzymes 1 and 2-double knockout mice on a C57BL background. Microbiologyopen. 2020 Oct;9(10):e1107. Epub 2020 Aug 18. [CrossRef] [PubMed] [PubMed Central]
- Mahalhal A, Frau A, Burkitt MD, Ijaz UZ, Lamb CA, Mansfield JC, Lewis S, Pritchard DM, Probert CS. Oral Ferric Maltol Does Not Adversely Affect the Intestinal Microbiota of Patients or Mice, But Ferrous Sulphate Does. Nutrients. 2021 Jun 30;13(7):2269. [CrossRef] [PubMed] [PubMed Central]
- Mahalhal A, Burkitt MD, Duckworth CA, Hold GL, Campbell BJ, Pritchard DM, Probert CS. Long-Term Iron Deficiency and Dietary Iron Excess Exacerbate Acute Dextran Sodium Sulphate-Induced Colitis and Are Associated with Significant Dysbiosis. Int J Mol Sci. 2021 Mar 31;22(7):3646. [CrossRef] [PubMed] [PubMed Central]
- Mahalhal A, Williams JM, Johnson S, Ellaby N, Duckworth CA, Burkitt MD, Liu X, Hold GL, Campbell BJ, Pritchard DM, Probert CS. Oral iron exacerbates colitis and influences the intestinal microbiota. PLoS One. 2018 Oct 11;13(10):e0202460. [CrossRef] [PubMed]
- Werner T, Wagner SJ, Martínez I, Walter J, Chang JS, Clavel T, Kisling S, Schuemann K, Haller D. Depletion of luminal iron alters the gut microbiota and prevents Crohn's disease-like ileitis. Gut. 2011 Mar;60(3):325-33. Epub 2010 Nov 12. [CrossRef] [PubMed]
- Lee YH, Kim H, Nam S, Chu JR, Kim JH, Lim JS, Kim SE, Sung MK. Protective Effects of High-Fat Diet against Murine Colitis in Association with Leptin Signaling and Gut Microbiome. Life (Basel). 2022 Jun 28;12(7):972. [CrossRef] [PubMed] [PubMed Central]
- Chen H, Qian Y, Jiang C, Tang L, Yu J, Zhang L, Dai Y, Jiang G. Butyrate ameliorated ferroptosis in ulcerative colitis through modulating Nrf2/GPX4 signal pathway and improving intestinal barrier. Biochim Biophys Acta Mol Basis Dis. 2024 Feb;1870(2):166984. Epub 2023 Dec 6. [CrossRef] [PubMed]
- Shoda R, Matsueda K, Yamato S, Umeda N. Epidemiologic analysis of Crohn disease in Japan: increased dietary intake of n-6 polyunsaturated fatty acids and animal protein relates to the increased incidence of Crohn disease in Japan. Am J Clin Nutr. 1996 May;63(5):741-5. [CrossRef] [PubMed]
- Zangara MT, Darwish L, Coombes BK. Characterizing the Pathogenic Potential of Crohn's Disease-Associated Adherent-Invasive Escherichia coli. EcoSal Plus. 2023 Dec 12;11(1):eesp00182022. Epub 2023 May 17. [CrossRef] [PubMed] [PubMed Central]
- Wen W, Xu Y, Qian W, Huang L, Gong J, Li Y, Zhu W, Guo Z. PUFAs add fuel to Crohn's disease-associated AIEC-induced enteritis by exacerbating intestinal epithelial lipid peroxidation. Gut Microbes. 2023 Dec;15(2):2265578. Epub 2023 Oct 6. [CrossRef] [PubMed] [PubMed Central]
- O'Donnell VB, Murphy RC. New families of bioactive oxidized phospholipids generated by immune cells: identification and signaling actions. Blood. 2012 Sep 6;120(10):1985-92. Epub 2012 Jul 16. [CrossRef] [PubMed] [PubMed Central]
- Saraev DD, Pratt DA. Reactions of lipid hydroperoxides and how they may contribute to ferroptosis sensitivity. Curr Opin Chem Biol. 2024 Aug;81:102478. Epub 2024 Jun 21. [CrossRef] [PubMed]
- Dufrusine B, Di Francesco A, Oddi S, Scipioni L, Angelucci CB, D'Addario C, Serafini M, Häfner AK, Steinhilber D, Maccarrone M, Dainese E. Iron-Dependent Trafficking of 5-Lipoxygenase and Impact on Human Macrophage Activation. Front Immunol. 2019 Jun 28;10:1347. [CrossRef] [PubMed] [PubMed Central]
- Abeysinghe RD, Roberts PJ, Cooper CE, MacLean KH, Hider RC, Porter JB. The environment of the lipoxygenase iron binding site explored with novel hydroxypyridinone iron chelators. J Biol Chem. 1996 Apr 5;271(14):7965-72. [CrossRef] [PubMed]
- Kenyon V, Rai G, Jadhav A, Schultz L, Armstrong M, Jameson JB 2nd, Perry S, Joshi N, Bougie JM, Leister W, Taylor-Fishwick DA, Nadler JL, Holinstat M, Simeonov A, Maloney DJ, Holman TR. Discovery of potent and selective inhibitors of human platelet-type 12-lipoxygenase. J Med Chem. 2011 Aug 11;54(15):5485-97. Epub 2011 Jul 8. [CrossRef] [PubMed] [PubMed Central]
- Kawade G, Kurata M, Matsuki Y, Fukuda S, Onishi I, Kinowaki Y, Watabe S, Ishibashi S, Ikeda M, Yamamoto M, Ohashi K, Kitagawa M, Yamamoto K. Mediation of Ferroptosis Suppressor Protein 1 Expression via 4-Hydroxy-2-Nonenal Accumulation Contributes to Acquisition of Resistance to Apoptosis and Ferroptosis in Diffuse Large B-Cell Lymphoma. Lab Invest. 2024 Apr;104(4):102027. Epub 2024 Feb 3. [CrossRef] [PubMed]
- Echtay KS, Esteves TC, Pakay JL, Jekabsons MB, Lambert AJ, Portero-Otín M, Pamplona R, Vidal-Puig AJ, Wang S, Roebuck SJ, Brand MD. A signalling role for 4-hydroxy-2-nonenal in regulation of mitochondrial uncoupling. EMBO J. 2003 Aug 15;22(16):4103-10. [CrossRef] [PubMed] [PubMed Central]
- Shoeb M, Ansari NH, Srivastava SK, Ramana KV. 4-Hydroxynonenal in the pathogenesis and progression of human diseases. Curr Med Chem. 2014;21(2):230-7. [CrossRef] [PubMed] [PubMed Central]
- Cherkas A, Zarkovic N. 4-Hydroxynonenal in Redox Homeostasis of Gastrointestinal Mucosa: Implications for the Stomach in Health and Diseases. Antioxidants (Basel). 2018 Sep 3;7(9):118. doi: 10.3390/antiox7090118. PMID: 30177630; PMCID: PMC6162398. 301. 301. Vatsyayan R, Lelsani PC, Chaudhary P, Kumar S, Awasthi S, Awasthi YC. The expression and function of vascular endothelial growth factor in retinal pigment epithelial (RPE) cells is regulated by 4-hydroxynonenal (HNE) and glutathione S-transferaseA4-4. Biochem Biophys Res Commun. 2012 Jan 6;417(1):346-51. Epub 2011 Dec 1. [CrossRef] [PubMed] [PubMed Central]
- Brown CW, Chhoy P, Mukhopadhyay D, Karner ER, Mercurio AM. Targeting prominin2 transcription to overcome ferroptosis resistance in cancer. EMBO Mol Med. 2021 Aug 9;13(8):e13792. Epub 2021 Jul 5. [CrossRef] [PubMed] [PubMed Central]
- Chen ZH, Yoshida Y, Saito Y, Noguchi N, Niki E. Adaptive response induced by lipid peroxidation products in cell cultures. FEBS Lett. 2006 Jan 23;580(2):479-83. Epub 2005 Dec 22. [CrossRef] [PubMed]
- Khoubnasabjafari M, Ansarin K, Jouyban A. Reliability of malondialdehyde as a biomarker of oxidative stress in psychological disorders. Bioimpacts. 2015;5(3):123-7. Epub 2015 Jul 26. [CrossRef] [PubMed] [PubMed Central]
- Kagan VE, Mao G, Qu F, Angeli JP, Doll S, Croix CS, Dar HH, Liu B, Tyurin VA, Ritov VB, Kapralov AA, Amoscato AA, Jiang J, Anthonymuthu T, Mohammadyani D, Yang Q, Proneth B, Klein-Seetharaman J, Watkins S, Bahar I, Greenberger J, Mallampalli RK, Stockwell BR, Tyurina YY, Conrad M, Bayır H. Oxidized arachidonic and adrenic PEs navigate cells to ferroptosis. Nat Chem Biol. 2017 Jan;13(1):81-90. Epub 2016 Nov 14. [CrossRef] [PubMed] [PubMed Central]
- Sun S, Mao Y, Le S, Zheng M, Li M, Chen Y, Chen J, Fan Y, Lv B. Biological characteristics of molecular subtypes of ulcerative colitis characterized by ferroptosis and neutrophil infiltration. Sci Rep. 2024 Apr 25;14(1):9510. [CrossRef] [PubMed] [PubMed Central]
- Sun SP, Lu YF, Li H, Weng CY, Chen JJ, Lou YJ, Lyu D, Lyu B. AMPK activation alleviated dextran sulfate sodium-induced colitis by inhibiting ferroptosis. J Dig Dis. 2023 Mar;24(3):213-223. Epub 2023 Jun 10. [CrossRef] [PubMed]
- Zhu F, Zou D, Shi P, Tang L, Wu D, Hu X, Yin F, Liu J. Dipeptidyl peptidase 4: A predictor of ferroptosis in ulcerative colitis. J Gene Med. 2024 Oct;26(10):e3742. [CrossRef] [PubMed]
- Dong S, Zhang Y, Ye L, Cao Q. Identification of a Novel Activated NK-Associated Gene Score Associated with Diagnosis and Biological Therapy Response in Ulcerative Colitis. Digestion. 2024 Aug 23;1-22. Epub ahead of print. [CrossRef] [PubMed]
- Heidari P, Haj-Mirzaian A, Prabhu S, Ataeinia B, Esfahani SA, Mahmood U. Granzyme B PET Imaging for Assessment of Disease Activity in Inflammatory Bowel Disease. J Nucl Med. 2024 Jul 1;65(7):1137-1143. [CrossRef] [PubMed] [PubMed Central]
- Niu R, Lan J, Liang D, Xiang L, Wu J, Zhang X, Li Z, Chen H, Geng L, Xu W, Gong S, Yang M. GZMA suppressed GPX4-mediated ferroptosis to improve intestinal mucosal barrier function in inflammatory bowel disease. Cell Commun Signal. 2024 Oct 4;22(1):474. [CrossRef] [PubMed] [PubMed Central]
- Lin Z, Zou S, Wen K. The crosstalk of CD8+ T cells and ferroptosis in cancer. Front Immunol. 2024 Jan 15;14:1255443. [CrossRef] [PubMed] [PubMed Central]
- Chan SH, Perussia B, Gupta JW, Kobayashi M, Pospísil M, Young HA, Wolf SF, Young D, Clark SC, Trinchieri G. Induction of interferon gamma production by natural killer cell stimulatory factor: characterization of the responder cells and synergy with other inducers. J Exp Med. 1991 Apr 1;173(4):869-79. [CrossRef] [PubMed] [PubMed Central]
- Yadav PK, Chen C, Liu Z. Potential role of NK cells in the pathogenesis of inflammatory bowel disease. J Biomed Biotechnol. 2011;2011:348530. Epub 2011 Jun 1. [CrossRef] [PubMed] [PubMed Central]
- Reichert CO, de Freitas FA, Sampaio-Silva J, Rokita-Rosa L, Barros PL, Levy D, Bydlowski SP. Ferroptosis Mechanisms Involved in Neurodegenerative Diseases. Int J Mol Sci. 2020 Nov 20;21(22):8765. [CrossRef] [PubMed] [PubMed Central]
- Fahoum L, Moshe-Belisowski S, Zaydel K, Ghatpande N, Guttmann-Raviv N, Zhang W, Li K, Tong WH, Nyska A, Waterman M, Weisshof R, Zuckerman A, Meyron-Holtz EG. Iron regulatory protein 1 is required for the propagation of inflammation in inflammatory bowel disease. J Biol Chem. 2024 Sep;300(9):107639. Epub 2024 Aug 7. [CrossRef] [PubMed] [PubMed Central]
- Jiang Q, Wan R, Jiang J, Li T, Li Y, Yu S, Zhao B, Li Y. Interaction between macrophages and ferroptosis: Metabolism, function, and diseases. Chin Med J (Engl). 2024 Sep 6. Epub ahead of print. [CrossRef] [PubMed]
- Yang Y, Wang Y, Guo L, Gao W, Tang TL, Yan M. Interaction between macrophages and ferroptosis. Cell Death Dis. 2022 Apr 16;13(4):355. [CrossRef] [PubMed] [PubMed Central]
- Sousa JA, Callejas BE, Wang A, Higgins E, Herik A, Andonian N, Yousuf M, Colarusso P, Raman M, McKay DM. GPx1 deficiency confers increased susceptibility to ferroptosis in macrophages from individuals with active Crohn's disease. Cell Death Dis. 2024 Dec 18;15(12):903. [CrossRef] [PubMed]
- Grisham MB, Hernandez LA, Granger DN. Xanthine oxidase and neutrophil infiltration in intestinal ischemia. Am J Physiol. 1986 Oct;251(4 Pt 1):G567-74. [CrossRef] [PubMed]
- Matsushima S, Tsutsui H, Sadoshima J. Physiological and pathological functions of NADPH oxidases during myocardial ischemia-reperfusion. Trends Cardiovasc Med. 2014 Jul;24(5):202-5. Epub 2014 Apr 1. [CrossRef] [PubMed] [PubMed Central]
- Wang F, Lee J, Roh YS. Mitochondrial Control in Inflammatory Gastrointestinal Diseases. Int J Mol Sci. 2022 Nov 28;23(23):14890. [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Nox1-KO mouse colon exhibiting some pathology.
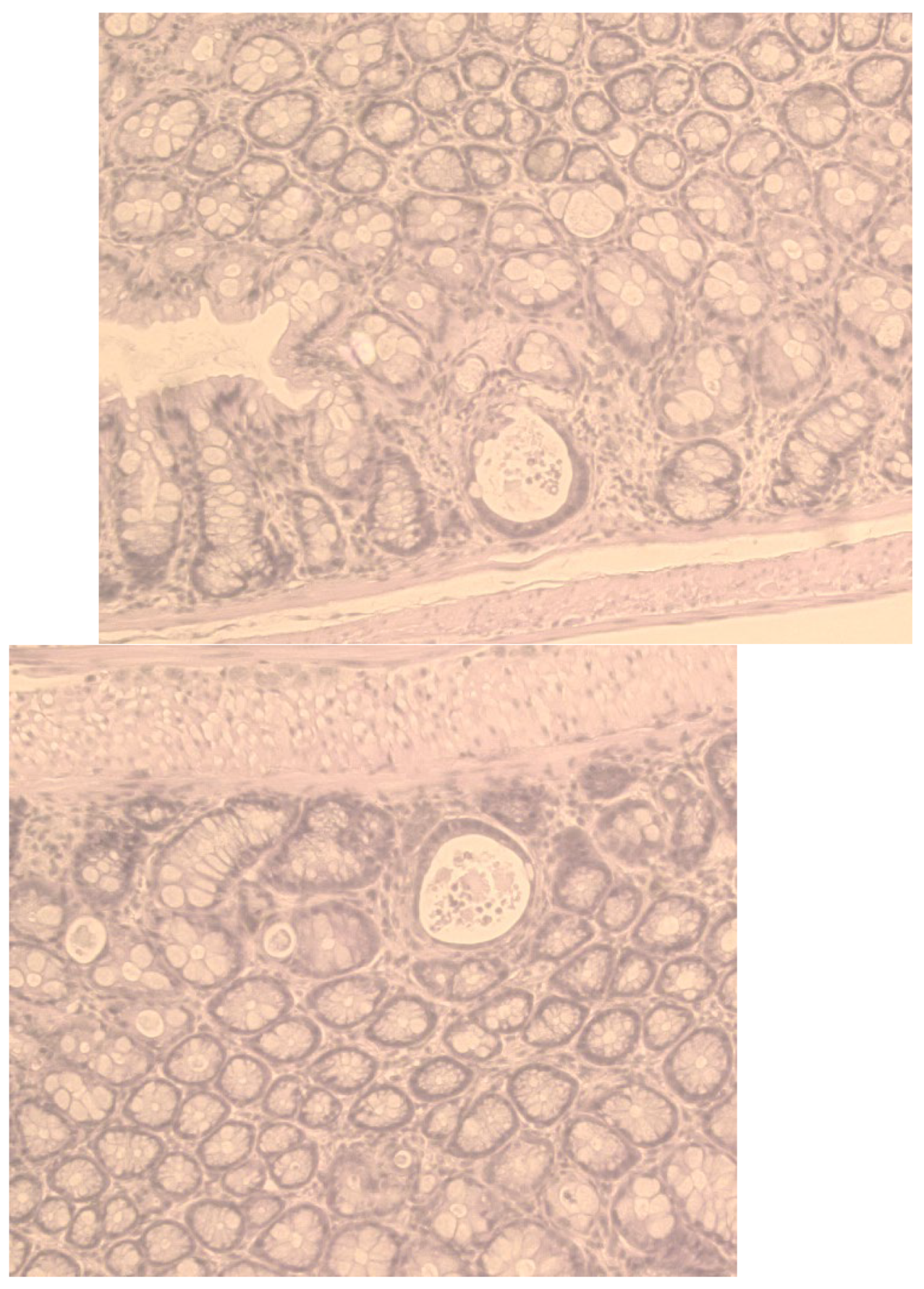
Figure 3.
Pathology scores of Gpx1/2-DKO (DKO; B6 background) mouse ileum (mean and STD), showing little impact of deferoxiamine (150mg/kg, daily IP) by comparison to mock treated controls, DTI (6mg/kg, daily IP) and mice deficient in expression of Duox2 or Nox1. Non-DKO mice are a mix of Gpx1+/-Gpx2-/- and Gpx1-/-Gpx2+/- mice, which on a B6 background have nearly normal histology. To simplify the display, statistically non-significant sets are show by bars, all others significant by pairwise comparison (<0.02).
Figure 3.
Pathology scores of Gpx1/2-DKO (DKO; B6 background) mouse ileum (mean and STD), showing little impact of deferoxiamine (150mg/kg, daily IP) by comparison to mock treated controls, DTI (6mg/kg, daily IP) and mice deficient in expression of Duox2 or Nox1. Non-DKO mice are a mix of Gpx1+/-Gpx2-/- and Gpx1-/-Gpx2+/- mice, which on a B6 background have nearly normal histology. To simplify the display, statistically non-significant sets are show by bars, all others significant by pairwise comparison (<0.02).
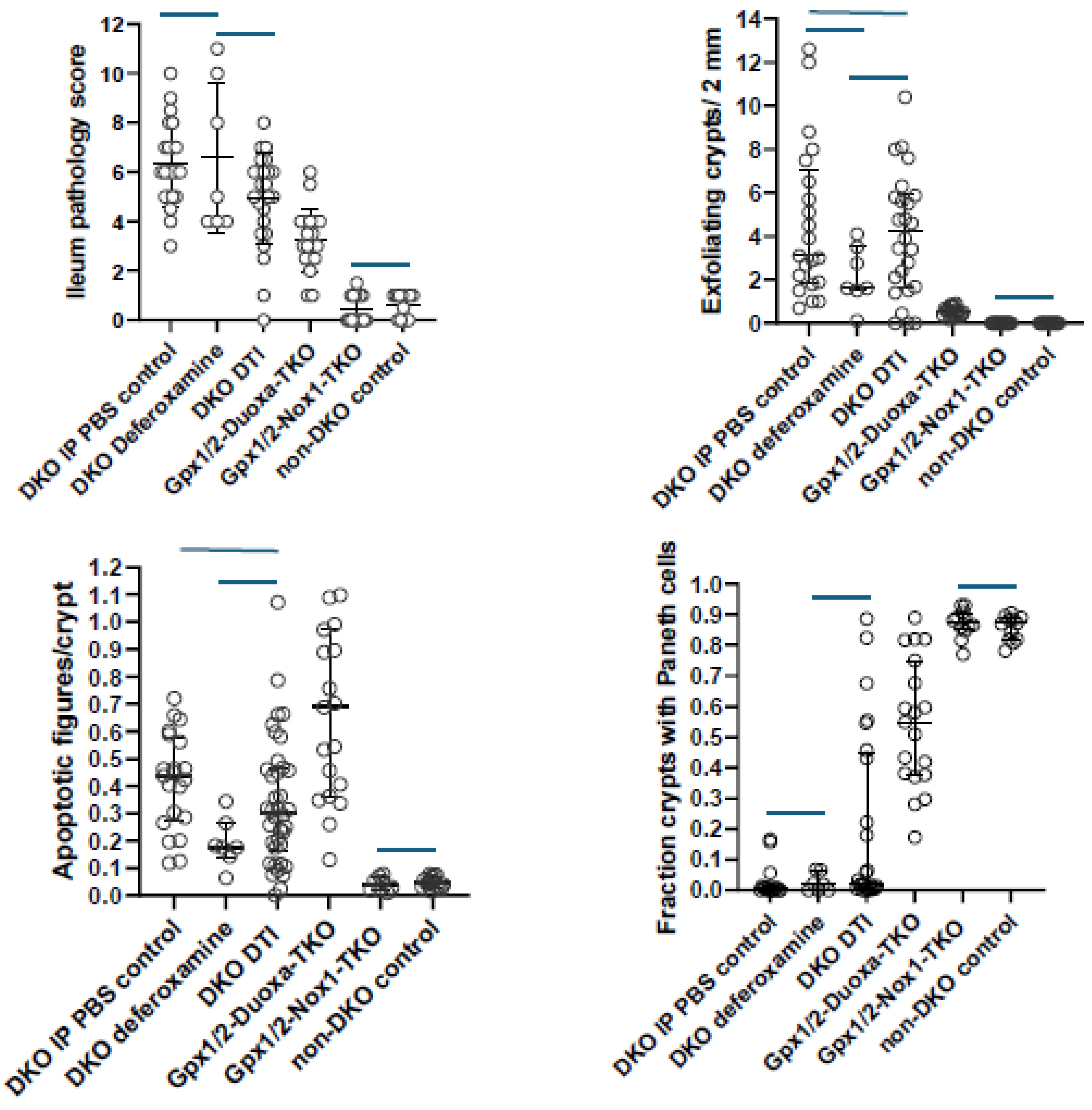
Figure 4.
Impact of two Western diet formulations and semi-purified AIN-76A diet (AIN) on Gpx1/2-DKO mouse (129 N10) morbidity in comparison with standard LabDiet® mouse chow.
Figure 4.
Impact of two Western diet formulations and semi-purified AIN-76A diet (AIN) on Gpx1/2-DKO mouse (129 N10) morbidity in comparison with standard LabDiet® mouse chow.
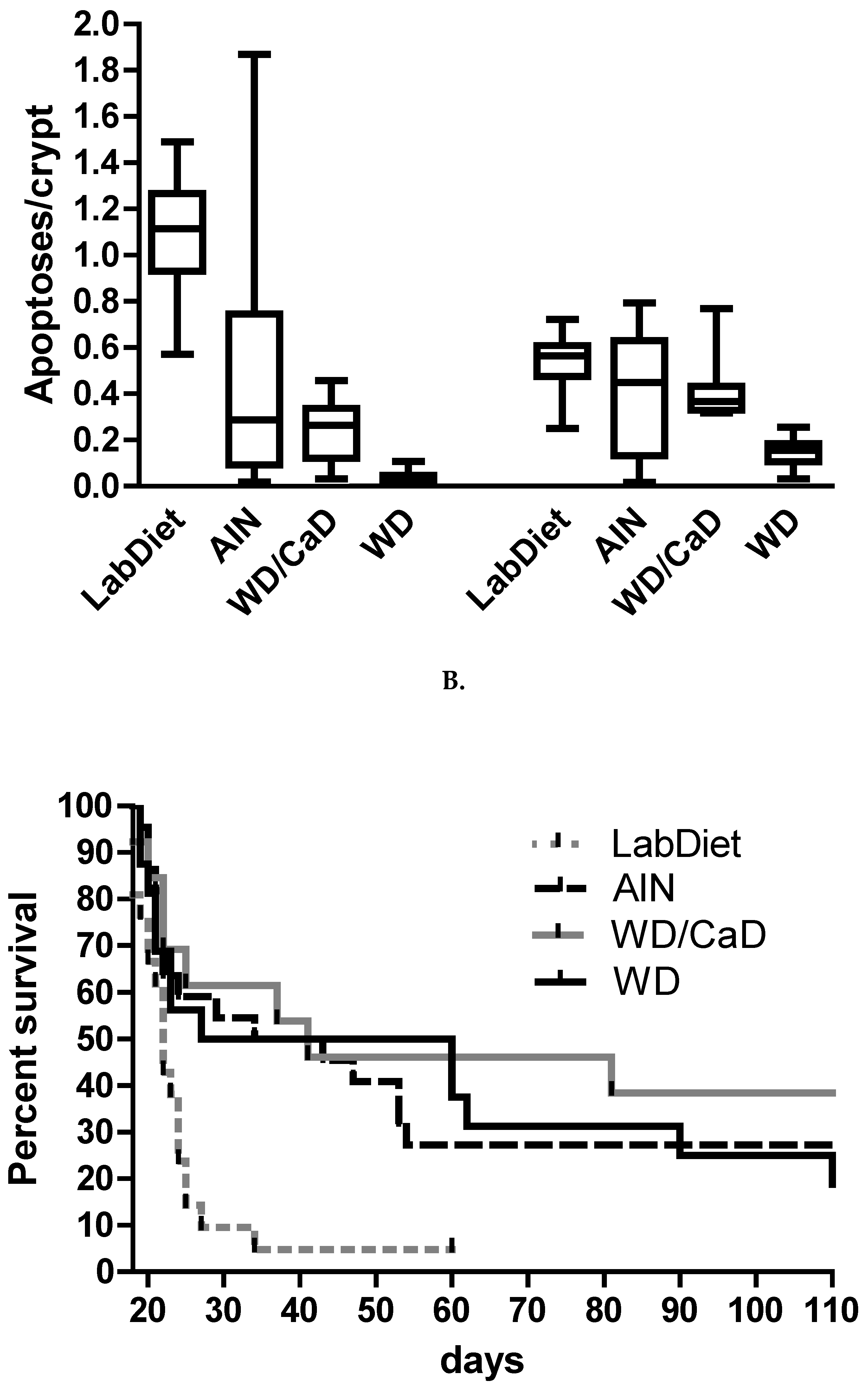
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



