Submitted:
18 December 2024
Posted:
19 December 2024
You are already at the latest version
Abstract
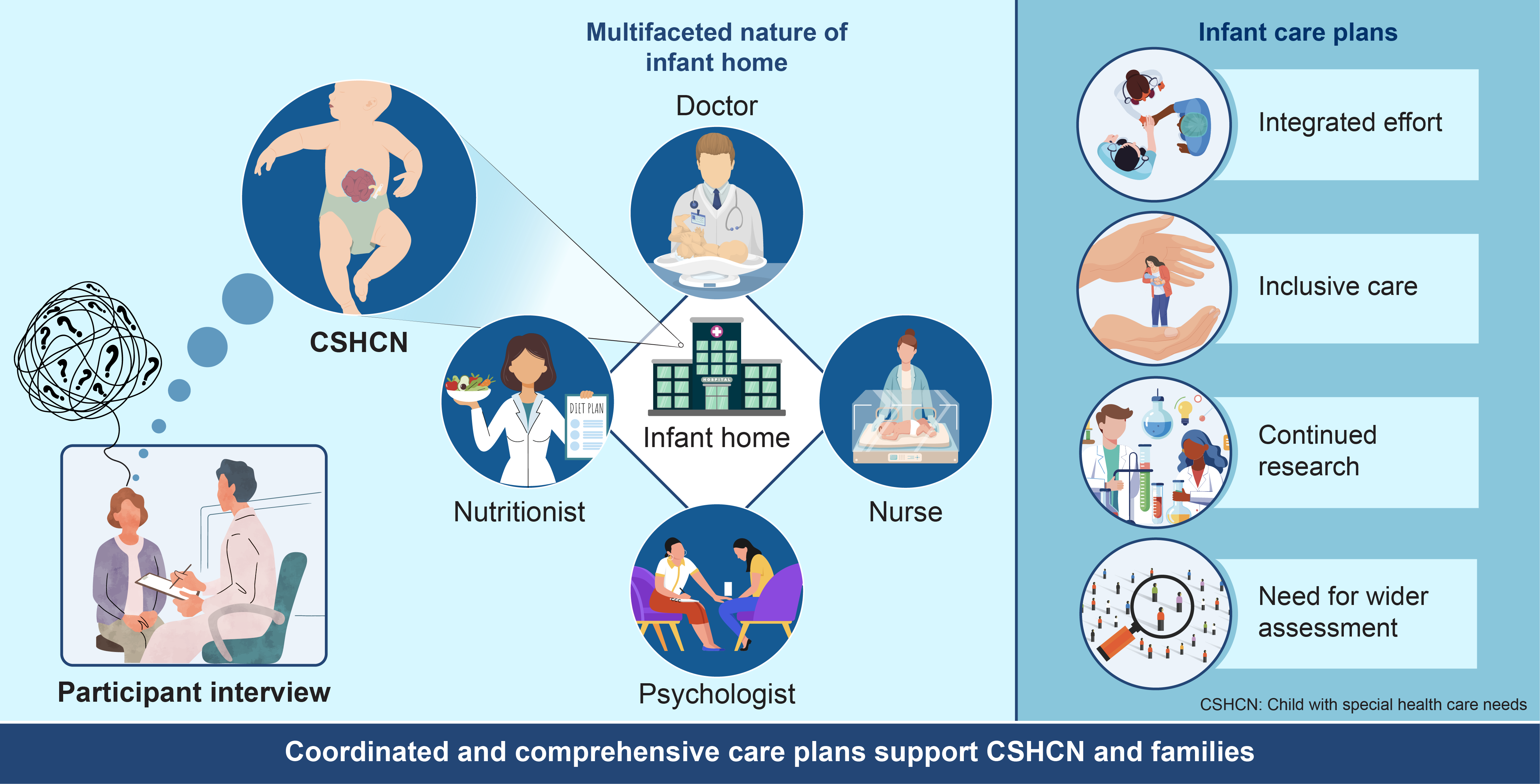
Background/Objectives: The number of children with special health care needs (CSHCN) has increased considerably owing to medical advances. However, the specifics of care that contribute to the well-being of CSHCN and their families and guarantee home nurturing have not been clarified. Methods: This exploratory single case study adhered to Yin's approach for case studies and used explanation-building methods for data analysis. Interviews were conducted with the staff in charge of CSHCN cases in a Japanese infant home, and information was collected from the records. Participant interview data and other data sources provided detailed case descriptions of care practices and outcomes. Results: Interviews on CSHCN with autoinflammatory diseases were conducted with three staff members and the child's mother. Data resources included childcare records, hospital visitation records, growth and development data, and case-related documents. The following factors were found to lead to a stronger system of care: accompanying growth through trial and error, supporting the family while sharing the child's growth and working with multiple agencies, and continuing to explore possibilities and support for family childcare. Conclusions: This case study describes the actual care provided to CSHCNs and their families in a single-infant home, revealing factors that lead to a stronger system of care. Here, the infant home provided a tried-and-true approach to CSHCNs and their families with multifaceted needs and attended to diverse child-development aspects while simultaneously supporting the family.
Keywords:
disabled child
; child care
; growth and development
; infant
; Japan
1. Introduction
The U.S. Maternal and Child Health Bureau defines children with special health care needs (CSHCN) as “those who have or are at increased risk for a chronic physical, developmental, behavioral, or emotional condition and require health and related services of a type or amount beyond that required by children generally” [1]. Survey data in Tokyo identified > 500 (12.5%) of the approximately 4,000 participants as having CSHCN. Additionally, caregivers of CSHCN reportedly experience higher rates of anxiety, depression, and other forms of emotional stress than caregivers of other children [2]. Notably, caregivers’ emotional challenges and stress may lead to child maltreatment [3].
Although caring for CSHCN imposes significant emotional, physical, and financial burdens on families, enhanced care coordination and respite care may help alleviate these challenges and address unmet needs [4].
Therefore, there is a need for institutions that can provide ongoing care coordination and respite care for CSHCNs and their families to promote well-being. In Japan, infant care centers support families facing child-rearing challenges by offering temporary alternative care. These centers bring together professionals, including childcare workers, nurses, commissioned physicians, social workers, psychologists, and nutritionists, who collaborate with multiple agencies to provide comprehensive care for children and support for families. Accordingly, infant care centers are being strengthened as institutions that provide multifaceted care for children with high care needs and their families [5].
However, the specifics of care that contribute to the well-being of CSHCN and their families and ensure a nurturing home environment remain unclear. Therefore, this study aimed to describe the actual care provided to CSHCN and their families in Japanese infant care centers and to identify factors that can strengthen the care system. The questions this study sought to answer are as follows: What is the actual state of care for CSHCN and their families in Japanese infant homes? What factors are important for strengthening the care system of CSHCN and their families?
2. Materials and Methods
2.1. Ethics Approval
This study obtained ethics approval from the Research Ethics Committee of the Nagoya City University Graduate School of Nursing (22003-3) and permission to conduct the study from the Nagoya University Bioethics Review Committee (2022-0175-2).
Written informed consent was obtained from each participant before the interviews began. Only adults aged ≥ 18 years were selected as interviewees.
2.2. Research Methods
2.2.1. Design
This study employed an exploratory embedded single-case study design following Yin’s approach [6]. This study design was used to address the research questions as the approach is suited to answering exploratory questions, such as the “how” and “why” a particular phenomenon occurs [6]. In addition, an explanation construction method was used to analyze the data, aiming to construct an explanation of the case, including how care was implemented and its outcomes.
The explanation construction method analyzes case study data by constructing explanations of the case with the purpose of generating ideas for further research rather than drawing final conclusions.
Case studies allow for in-depth exploration and are often used in health policy analyses when the phenomenon is happening and not within the researchers’ control [6].
A single-case study design was selected over a multiple-case study design, as this approach allows for a more extensive analysis of the embedded units, which yields greater insights into the case [6]. A single case study allows the researcher to explore new theoretical relationships to develop a deeper understanding of these phenomena [7]. Therefore, this study adopted a single-case rather than a multiple-case study design.
2.2.2. Defining the Case and Data Source
Within an embedded single-case study design, two or more embedded units of analysis are positioned within the case and context [6]. The context of this study is the care system for CSHCN and their families in Japan, and the case is the care provided to the CSHCN and their families. The two units of analysis are the thoughts and practices of the staff at the infant home and the impact and changes experienced by the CSHCN and their families.
For the selected case, nurses, childcare workers, family support specialists, and parents who were the child’s primary caregivers during the child’s stay at the infant care center were interviewed. Documents were also used to corroborate the interview data and provide a detailed context for the case.
2.2.3. Case Selection Criteria
The following selection criteria were used.
1) Children admitted in 2018 or later were admitted to the facility for at least 1 year and discharged at the time the survey was conducted.
2) Cases where the child’s parents were in a position to be informed of the research, fully understand the content of the research and decide to cooperate in the research.
3) Cases considered to be CSHCN at the time of admission to the facility based on the CSHCN definition and CSHCN screener.
The CSHCN screener items were as follows
☑ Use of medications (other than vitamins) prescribed by a physician
☑ Access to medical, mental health, and educational services
☑ Limitation or inhibition of capacity
☑ Use of physical, occupational, speech, and other therapies
☑ Emotional, developmental, or behavioral issues
The question is whether the problem is due to a medical, behavioral, or health condition and lasts for > 12 months; if any one of these two criteria is met, the patient is classified as a CSHCN.
2.2.4. Data Collection
All interviews were conducted face-to-face in a mutually agreed-upon private location. Parental interviews were conducted with the mother; however, the child’s father was also present. One researcher (TN) conducted all interviews and reviewed all the documentation. An interview guide was used to explore how care was provided to the child and family and their perceptions of the outcomes, methods, and quality of care. Documentation was used to construct a description of care practices in alignment with the interview data, although this was not coded.
2.2.5. Data Analysis
The data sets obtained from the case studies (the four types of data sources recommended by Yin, documentation, archival records, interviews, and physical artifacts) were analyzed based on a strict explanation-building protocol that had been set in advance [6]. The explanation-building analysis strategy was designed for case studies involving single-case sites and aimed to construct detailed explanations that are suited to each individual case. Yin states that this method is “similar to creating an overall explanation of the findings from multiple experiments in science” [6].
Multiple members of the research team performed iterative analysis. In the first stage, the interview data was transcribed, and the content related to care, initiatives, and the impact on children and families was extracted. Furthermore, the extracted content was classified based on the similarity of the initiatives and their impact. At that time, data was searched for in data resources, such as records and documents, to show whether the content of care and initiatives actually had an impact on children and families, and the impact was corroborated. When interpreting the interview data, we repeatedly referred back to the written data sources and compared them with the interview data to confirm the details of the cases and corroborate the content of the interview data. In the second stage, we confirmed how care was implemented and what results were produced based on the interview data obtained from each participant and other data sources. In particular, the narratives of the children’s families were used to check for any discrepancies or agreement in terms of the expected impact of the care and initiatives and any content for which the impact or effectiveness was uncertain for the infant home staff.
In the third stage, the data on the initiatives and impacts that had been classified were arranged by time period, from before admission to after discharge, and descriptions based on data sources were combined and written to explain the actual care in several categories.
2.2.6. Reliability and Validity
Several methods have been used to ensure its reliability and validity. The researcher utilized a data analysis strategy for explanation building, as advocated by Yin [6]. In view of this analysis, during the coding process, the researcher utilized observations and field notes to ensure the validity of the study.
Prior to the study, a list of interview questions and document types to be used as data sources was prepared. Additionally, to obtain diverse perspectives, participants included individuals from various occupations and positions as well as varied documentation sources. Although the staff of the infant care center and the child’s family provided narratives, the research team’s neutrality was established with the participants prior to the interviews. Nursing research experts reviewed the findings to ensure alignment with the actual case context.
Strategies such as credibility, transferability, dependability, and confirmability were used to ensure the trustworthiness of the data. Credibility was ensured through member checking and triangulation. Transferability was ensured by a detailed description of the research methods and contexts, as well as a detailed description of the participants and their experiences. Dependability was ensured through dense descriptions, peer examinations, and triangulation. Confirmability was ensured by the process of reflexivity, whereby the researcher’s own biases or assumptions were made apparent through a reflexive journal.
3.Results
3.1. Case Overview
- A child with a congenital autoinflammatory disease
- CSHCN Screener applicable (☑ Use of medications (other than vitamins) prescribed by a physician, ☑ Access to medical, mental health, and educational services, ☑ Limitation or inhibition of capacity, ☑ Use of physical, occupational, speech, and other therapies
- July, 20XX: Birth
- March, 20XX+1: Discharged (8 months old)
- April, 20XX+1: Admitted (9 months old)
- March, 20XX+4: Exit (3 years and 8 months old)
3.2. Interviewees
A summary of the interviewees is presented in Table 1.
3.3. Explanation of Care Practices for the Child and His/Her Family
(B, nurse in charge; C, family support specialist; D, childcare worker in charge; E, mother of the child)
3.3.1. Connect First with Families in Crisis and Begin Alternative Care (Birth of the Child to Admission)
(a) Connect first with families in crisis
The child was diagnosed with congenital disease after birth, accompanied by a chronic rash, joint pain throughout the body, and a weakened immune system, which left him vulnerable to severe illness and recurrent pneumonia. In addition to the child’s health sensitivity and difficulty with bedtime routines, his slow growth and developmental delays were evident, leading his parents to worry that these difficulties might persist indefinitely. The burden and anxiety stemming from the child’s unique needs placed the family in a state of crisis. In response, the hospital psychologist recognized the parents’ distress and, through the Child Guidance Center, arranged a temporary placement at an infant home as an alternative foster home. This intervention, along with the psychologist’s validation of their concerns, provided significant relief for the child’s parents. Despite this great burden, the mother made every effort to remain close and supportive of her child.
Living in Japan, there is a strong cultural belief that children should be raised by their parents. If support had not been provided, I think we would have pushed ourselves too hard and both of us would have broken down (E-5)
(b) Beginning alternative foster care despite hesitating to accept it
The infant home initially faced challenges regarding the child’s distinctive appearance and had concerns about his care needs. However, the staff did not place blame on the parents who were struggling with guilt about leaving their child at the facility. Instead, they were involved in building a relationship between trust and providing emotional support. The parents faced difficulties because they felt that children should be raised by their parents, and they had taken on the responsibility of raising the child. The family support counselor emphasized the significance of the infant home as a means of providing alternative childcare for families facing a crisis.
Sometimes, the most difficult temporary period can be saved by having someone else take over for you. The period immediately after birth is particularly difficult, and for infants, hospital visits are an additional burden. Infant care centers can provide support in transformative ways (C-26)
3.3.2. Responding to the Children’s Needs from All Aspects and Supporting Their Growth Through Trial and Error (During Admission)
(a) Trial and error in devising care in the face of difficulties
After the child’s admission, the infant care center had to devise various aspects to meet his unique needs. The staff paid careful attention to physical assessments, including monitoring of fever and respiratory status, and coordinated frequent hospital visits. From the time of admission, the staff collaborated closely with the commissioned physician and the child’s attending physician to establish standards for medications and hospital visits and ensure that all staff were informed of these protocols. In addition to establishing medical standards, the staff addressed specific challenges, such as managing walking distances due to shortness of breath and helping with sleep difficulties caused by irritability. The childcare team emphasized the importance of collaboration, drawing on the expertise of multiple professionals.
Saturation measurements and other measures were introduced and standards were established with commissioned physicians (B-11).
They, in turn, informed the other staff members of what they had confirmed with the physician (B-4).
The reason it takes a lot of work is not a personnel problem but the staff’s willingness to help each other (D-16)
(b) Support children’s growth by working with them regarding food, which is the foundation of their development and can be a great source of enjoyment.
Various efforts have been made from a wide range of perspectives, including attending to children’s growth and development, diet, physical activity, and emotional and spiritual involvement. In terms of food, milk was thickened appropriately for a child at high aspiration risk, and the timing and progress of weaning food were discussed in consultation with the child’s doctor, dietitian, and cook. The staff observed that food was a crucial part of the children’s upbringing. As children progressed to regular infant foods, parents’ attitudes shifted positively, witnessing their children’s development and prevention of aspiration risks. This dietary progression not only contributed to physical growth but also brought children daily enjoyment. Nurses remarked that mealtimes became a source of joy and an indication of children’s growth.
She started weaning herself on baby food after consulting with her doctor, and after she passed the middle to late stage of eating, she started eating crunchy foods, which she enjoyed very much, partly because her chewing and swallowing functions had improved (B-22).
(c) Carefully develop growth and development based on the child’s physical and emotional characteristics.
Regarding physical activities, staff repeatedly encouraged children to use their feet to reach the desired objects, celebrating each small success together. Through daily interactions, we attempted to help the children learn how to use their bodies independently by drawing out their gradual growth and joy. Instead of forcing them to accomplish a task, the staff perceived what children could do individually, praised them, and celebrated with them. In particular, regarding the emotional and mental development of children, for example, they did not restrain them from expressing their feelings, such as when they shouted but accepted them and then shared gentle and polite ways of expressing their feelings. As the children’s needs were met, they gradually began to show greater awareness of others, often imitating adults by caring for younger children. By spending time with adults who were receptive to their feelings, the children learned to interact calmly with others, which greatly contributed to their interactions with their families and changed how they felt about them.
The family appreciated having meaningful conversations with the child, such as discussing waiting here or waiting for you, which they felt may have sparked the hope that they could eventually raise the child at home (C-12)
He used to cry all the time and was irritable and grumpy, but we thought that being able to wait and move around on his own was a huge deal because we thought it would fulfill a need in him (E-9)
(d) Professionals should utilize their own strengths and complement each other to be involved with the characteristics of the child.
Professionals worked collaboratively to integrate the medical aspects of meeting children’s health needs with childcare aspects supporting their daily growth, leveraging each other’s strengths. Although each held a unique perspective on the child, the nurses provided repeated explanations and training to enhance disease understanding and develop care techniques while respecting the insights of childcare workers. Parents felt comfortable with the presence of nurses who could answer their questions and concerns while improving their knowledge and skills regarding the care of their children. The knowledge and skills of those providing daily care were vital, as nurses believed that a solid understanding of each child’s healthcare needs significantly influenced their daily interactions.
Understanding the disease and detecting abnormalities early enables us to see the child as who they truly are (B-31)
3.3.3. Support the Family While Sharing the Child’s Growth and Working with Multiple Agencies (During Admission)
(a) Remaining close to the family while monitoring the child’s growth
In addition to interprofessional collaboration within the infant care center, a multiagency and multiprofessional approach was adopted to support the child’s family beyond routine childcare. The frequency and timing of family visits were arranged using the Child Guidance Center to consider the mother’s psychological state, with the same staff members involved as often as possible. During visits, staff members shared updates on the child’s condition and humorous moments with the family and communicated the family’s reactions to other staff members. The staff members shared their reactions and observations with their family members. A system of cooperation with medical institutions was also in place to respond to the children’s needs. The mother also understood the importance of careful involvement.
I thought how grateful I was that he went to the hospital every day without a single look of disgust and kindly explained everything to me when I met him (E-18).
(b) Responding to conflicting feelings about inadequate understanding of other institutions
However, situations such as consultations with non-attending physicians often require staff or parents to repeatedly explain the child’s circumstances because of limited understanding from other institutions. The staff responded to this by providing supplementary explanations each time.
When visiting a doctor, the child’s background and the facility were unknown, and the situation often had to be explained first (B-16).
It would be beneficial if medical institutions, nursery schools, and educational institutions would quickly understand that the children are living in an infant care center because of something medical in terms of social participation of the children (E-19)
3.3.4. Continue to Explore Possibilities and Support for Family Childcare (Toward Leaving the Home)
(a) Explore all post-exit options
Through collaboration between multiple agencies and professionals, the infant home supported the child’s development while maintaining close communication with the family, leading to gradual progress in the child’s growth. However, in this case, the infant home was an institution that provided temporary alternative foster care, and there were many discussions about the child’s future. The parents discussed the difficulties with all options. They considered the possibility of returning the child to a specialized facility, such as a medical treatment and education center, foster care, or home. However, the parents, sensing the difficulty of all options, were concerned about their child’s future and gradually began to consider caring for their child at home.
I would be willing to consider consignment if there were foster parents who understood the child very well and who would remain connected and connected to the parents (D-23)
I kind of realized that there was no place for this child to go, and I thought that the situation would be more miserable elsewhere, so I started thinking about raising her at home (E-7)
(b) Attending to a child’s growth and development has a significant impact on the family
Considering the future course of the infant care center, the child’s remarkable growth greatly influenced the parents’ feelings. The staff made conscious efforts to move the child’s arms and legs and, in consultation with the doctor, introduced therapies, such as home-visit rehabilitation. For parents who had been burdened by merely observing their child’s struggles, these milestones provided a hopeful context for considering home-based care.
I was surprised at the amazing growth and thought I could manage to do it because I thought it would make a huge difference in my life and the amount of care I would receive (E-8)
(c) Work toward the child’s participation in society
In addition, the possibility of admission to a day care center when the child returned home was also significant for leaving the infant home. The staff worked with the Child Guidance Center and administrative agencies to provide after-school daycare services and nursery schools after the child was discharged from the infant home. The parents were anxious about their child’s eventual future, and being able to enroll their child in daycare meant the possibility of their child’s participation in the community. However, even in the process of considering the child’s future after leaving the daycare center, the parents took their time. They proceeded step-by-step, from visits to outings to overnight stays. When considering the family’s return home, the staff directly involved with the family shared their thoughts with other staff members so that they could understand how the child’s parents and siblings felt about the child. The family was hopeful about the possibility of their child participating in the community as steps were gradually taken.
I thought daycare would be important; when I saw her starting to walk, I thought daycare might be possible, allowing her to be part of the community (E-14)
(d) Establish a support system after leaving the facility and inform the family.
When families were able to visualize what they would like after leaving the infant home, the most important factor for their return home was the support system after leaving the home. The staff did not underestimate the difficulties of living together and believed that it was important to have an environment in which they could always obtain advice. Parents were informed that, even if they returned home, they could be supported again if they had any concerns through functions such as short stays. With this attitude and the backup system at the infant care center, parents were able to consider raising their children at home. In addition to the short stay, the support of professionals who knew the child well after leaving the center, such as accompanying the child to the hospital, played a crucial role, and the child was able to return home. The mothers were keenly aware of the significance of the post-discharge support.
I really appreciated the short stays and escorting me to the hospital when my life was not yet settled, and I was very anxious (E-23)
(e) Consider expanding support after leaving the facility.
However, the need for more extensive post-discharge support functions was also discussed. In particular, the Family Support Specialist Consultant emphasized the need for more extensive post-discharge support beyond short stays.
I think I would have needed to return within a few months like if I could come back again. It is normal to be away from them for a long time. It would be good if I could stay with them longer and help them with their housework (C-28)
It would have been nice if we could have had mothers come to stay and spend time at the infant home while preparing for an earlier return home(C-30)
3.3.5. Continue Childcare Support and Expand Functions Further (at the Time of Leaving the Center—After Leaving the Center)
(a) Fulfill the unique role of an infant care center
In this case, the infant care center’s unique expertise in fostering multidisciplinary and multi-organizational collaboration accompanied the child’s growth. It was able to accompany child-rearing from the time of admission to after discharge, playing a major role in the child’s growth and development and returning home. Although the parents of the children felt the importance of a specialized support organization in a crisis situation, the staff perceived the burden on the children’s families and the role played by the unique functions of the infant care center. In addition, with regard to post-discharge support, there was an emphasis on the importance of not only the facility but also society as a whole to develop a better understanding of children’s transitions post-discharge, aiming to cultivate expertise in welcoming them back with support, reflected in sentiments like, “You have come a long way.”
I had an image that relatives would take care of the children, and I had a vague knowledge that the only place to receive support was daycare, so I had no choice but to snap when I found out I could not get support from my family (E-3)
I think it was a heavy burden for the mothers to be worried about their children’s illnesses while the fathers were working and the grandparents were not able to provide support. I think that only an infant care center can provide such a stimulating environment for the children, where they can be seen at a distance (B-35).
(b) Responding to the child’s needs and accompanying family
Although a family-like environment is ideal for childcare, infant care centers have established a unique system in which professionals with diverse expertise exchange views to deepen their understanding of each child’s unique needs. It is very difficult for parents to raise a child who needs to go to the hospital every week while also taking care of their siblings after leaving the facility. The fact that the infant home provides support during infancy, enabling the child to eat, improving their skin condition, reducing prescription drugs, and reducing hospitalization has helped families feel that they may be able to raise their children at home. Mothers felt that they could raise their children at home. The mothers also valued specialized support, considering it a positive experience for their families.
I was surprised that there was a very solid system in place, and they really did a great job in areas that needed special care (E-17)
(c) Continue to develop a more comprehensive follow-up system
Finally, the actual care provided by the infant care center in the present case illustrates issues related to the function of the infant care center. In terms of responding to unique healthcare needs, although being attached to a medical institution can reduce travel time, this alone does not guarantee peace of mind. In Japan, there is a prevailing belief that children should be raised by their parents, which can create a barrier to accessing infant care center support. Furthermore, intermediary support services that bridge medical institutions and home care are limited. After accepting a child with distinctive healthcare needs and accompanying him as he grew up, the staff was concerned about coordinating and collaborating with him about his future career path and continuing to provide aftercare after he left the center, hoping that this would lead to expanded support in the future and leave a record of his achievements. The mother of one of the children emphasized the importance of a flexible follow-up system for childcare, as in this case.
Medical care, education, and life have become disconnected in Japan, making integration difficult. A societal system where these areas intersect would be beneficial. For instance, if there’s a ’yellow light’ in a child’s progress, there should be follow-up support to help guide them back to ’green’ or advise when it’s better to stop at ’red.’ There should be a place that watches over and supports children without focusing solely on whether they have a disability or illness (E-26)
4. Discussion
This single case study revealed the actual care provided in an infant home to a child with a congenital condition and multifaceted special healthcare needs and to a family that was experiencing difficulties in caring for the child. In this case, the infant care center initially engaged with the family during a crisis period, collaborating with other agencies to address the child’s needs holistically and support their growth and development. At the same time, however, they were unsure about accepting children with special health care needs, and they repeatedly went through a trial-and-error process in their care. At times, they felt that other institutions’ understanding of infant care was inadequate. Additionally, they demonstrated their expertise in taking on the responsibility of providing ongoing support by coordinating with multiple departments and other agencies while exploring the possibility of returning the children to their families when they were ready to leave.
Two points should be emphasized in this study. First, the temporary alternative care provided by the infant care center ultimately led to the realization of family reunification, thereby guaranteeing an important element of well-being. Second, the institution was able to address the unmet needs of the child and family by providing support not only for the child but also for the family through collaboration among multiple professions and institutions.
4.1. Interpretation of the Described Care in Practice
In this case, the parents felt relieved to connect with a professional organization when their child was admitted to the hospital. Although the professionals in the infant hospital initially experienced anxiety and confusion, they shared knowledge. They demonstrated expertise in delivering varied care and daily coordination, which is a crucial element for a child’s well-being [8]. In this case, coordination and support from multiple professionals contributed to the child’s growth. Moreover, temporary alternative care and the child’s growth during this time helped to relieve the family’s initial distress in caring for a CSHCN, ultimately enabling the child to return home.
Reports on care plans for CSHCNs and their families highlight the importance of personnel who coordinate with multiple professions and agencies, serving as central figures in care and support [9,10]. The staff members who served as interviewees played a central role in providing care and support. However, the experience of providing care involved trial and error, confusion, and a notable burden on coordinating care. Future refinements of care plans and programs should address not only the benefits and cost-effectiveness for children but also the expansion of support systems that enhance the physical and mental well-being of care providers.
In cases where collaboration with other institutions and community support is essential, a limited understanding of the child’s needs and the role of the infant care center can impede effective collaboration. Community resources are crucial for enhancing support for CSHCN and their families [11]. Expanding care systems that promote CSHCN and family well-being in various regions will require increased awareness of the importance of collaborative care from multiple institutions, including medical facilities and wider society.
The actual care of the CSHCN showed that the infant care center was not only looking at the child but also the state of mind and support of the family so that the family was not left behind and that a care system was in place for the family to leave or after leaving the center. The importance of family burden and alternative support for CSHCN has also been shown in previous studies [12,13]. It is important not to separate family care and support but to intervene simultaneously. Specialized agencies organized by care providers with diverse expertise must understand and support the importance of ongoing care for CSHCNs and their families.
4.2. Propositions for Strengthening the Care System
First, the professionals began by carefully ascertaining the needs of the child and family and then responded to those needs by drawing on the expertise of their respective professions and organizations, which led to the child’s growth and positive outcomes. Therefore, to strengthen the care system that contributes to the well-being of CSHCNs and their families and guarantees home care, it is necessary to form a team that fully understands the care needs of CSHCNs and their families, coordinates daily care, and coordinates with other organizations by demonstrating each specialty and collaborating with other professionals at specialized agencies that are central to the care system. It is necessary to form a team that coordinates daily care with other organizations by demonstrating each specialty and collaborating with other professionals.
Second, because the family’s feelings appreciably changed when they realized their child’s growth through the approach to the family, which led to family reunification, in alternative care, attention must extend beyond the child’s immediate needs to include shared care plans and regular updates on the child’s progress with family members and potential foster parents to aid future home care.
Third, because efforts towards collaboration with other facilities and the local community led to a multifaceted approach that was important for fulfilling support, it is also essential to promote an understanding of CSHCN and specialized agencies in medical institutions and the community and to establish a system of collaboration. In addition, attention should be paid to supporting the physical and mental health of professionals within professional organizations to strengthen sustainable systems of care, as these professionals are expected to have considerable expertise and will be challenged with the burden of providing ongoing support. These findings provide a basis for future cohort studies on the care systems for patients with CSHCN and their families.
4.3. Limitation
As this exploratory study is a single case study conducted at a Japanese facility, additional and multiple case studies are needed to provide refined insights into care systems that support the well-being of CSHCNs and their families. Moreover, this study did not use interview data from all staff members involved with the CSHCN, possibly excluding some perspectives. Similar studies across different countries and institutions could provide broader insights if reviewed along with the findings of this study.
5. Conclusions
This case study describes the actual care provided to CSHCN and their families in a single case in an infant care center and reveals some of the factors that lead to a stronger system of care. In this case, the infant care center provided support to the CSHCN and their family with multifaceted needs. Through trial and error, it was attending to the child’s development from a variety of aspects while simultaneously supporting the family. Establishing teams with advanced care coordination skills and creating comprehensive care plans that address the needs of the child and family are essential for developing a care system that promotes the well-being of the CSHCN and guarantees family support. Continued research and the synthesis of findings are necessary to refine these recommendations.
Author Contributions
Formal analysis, TN, AK; methodology, TN, AK; writing—original draft, TN; writing—review & editing, TN, AK.
Funding
This research was funded by JSPS KAKENHI (grant number JP23K10054).
Institutional Review Board Statement
This study was conducted in accordance with the guidelines of the Declaration of Helsinki and was approved by the Nagoya City University Graduate School of Nursing Research Ethics Committee (approval number 22003-3).
Informed Consent Statement
Written informed consent was obtained from each participant prior to the start of the interview. Only adults aged ≥18 years were selected to participate as interviewees.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
We would like to express our gratitude to the members of the JSPS research team who contributed to the successful completion of the study.
Conflicts of Interest
The authors declare no conflict of interest. The funders played no role in the study design, data collection, analysis, interpretation, report writing, or decision to submit the article for publication.
References
- McPherson, M.; Arango, P.; Fox, H.; Lauver, C.; McManus, M.; Newacheck, P.W.; Perrin, J.M.; Shonkoff, J.P.; Strickland, B. A new definition of children with special health care needs. Pediatrics 1998, 102, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Kaji, N.; Ando, S.; Nishida, A.; Yamasaki, S.; Kuwabara, H.; Kanehara, A.; Satomura, Y.; Jinde, S.; Kano, Y.; Hiraiwa-Hasegawa, M.; Igarashi, T.; Kasai, K. Children with special health care needs and mothers’ anxiety/depression: findings from the Tokyo Teen Cohort study. Psychiatry Clin. Neurosci. 2021, 75, 394–400. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Preventing child maltreatment: a guide to taking action and generating evidence, World Health Organization: Geneva, Switzerland. 2006. Available online: https://www.who.int/publications/i/item/9241594365 (accessed on 10 November 2024).
- Kuo, D.Z.; Cohen, E.; Agrawal, R.; Berry, J.G.; Casey, P.H. A national profile of caregiver challenges among more medically complex children with special health care needs. Arch. Pediatr. Adolesc. Med. 2011, 165, 1020–1026. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Document on ‘how to promote high functioning and multi-functionalization, functional transformation, and smaller scale and regional decentralization of infant homes and children’s homes.’, published 2018. Available online: https://www.mhlw.go.jp/content/11920000/000351959.pdf. (accessed on 14 November 2023).
- Yin, R. Case study research: design and methods. Los Angeles, 5th ed; SAGE: CA, USA 2014. [Google Scholar]
- Gustafsson, J. Single case studies vs. multiple case studies: a comparative study. Halmstad University: Halmstad, 2017. [Google Scholar]
- Ziring, P.R.; Brazdziunas, D.; Cooley, W.C.; Kastner, T.A.; Kummer, M.E.; Gonzalez de Pijem, L.; Quint, R.D.; Ruppert, E.S.; Sandler, A.D.; Anderson, W.C.; Arango, P.; Burgan, P.; Garner, C.; McPherson, M.; Michaud, L.; Yeargin-Allsopp, M.; Johnson, C.P.; Wheeler, L.S.; Nackashi, J.; Perrin, J.M. American Academy of Pediatrics. Committee on children with disabilities. Care coordination: integrating health and related systems of care for children with special health care needs. Pediatrics 1999, 104, 978–981. [Google Scholar]
- Matiz, L.A.; Kostacos, C.; Robbins-Milne, L.; Chang, S.J.; Rausch, J.C.; Tariq, A. Integrating nurse care managers in the medical home of children with special health care needs to improve their care coordination and impact health care utilization. J. Pediatr. Nurs. 2021, 59, 32–36. [Google Scholar] [CrossRef]
- Farmer, J.E.; Clark, M.J.; Drewel, E.H.; Swenson, T.M.; Ge, B. Consultative care coordination through the medical home for CSHCN: a randomized controlled trial. Matern. Child Health J. 2011, 15, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Cohen, E.; Jovcevska, V.; Kuo, D.Z.; Mahant, S. Hospital-based comprehensive care programs for children with special health care needs: a systematic review. Arch. Pediatr. Adolesc. Med. 2011, 165, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Champagne, M.; Mongeau, S. Effects of respite care services in a children’s hospice: the parents’ point of view. J. Palliat. Care 2012, 28, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Dubois, A.C.; Seghers, N.; Van Dorsselaer, I.; Dario, Y.; Swolfs, I.; Gérain, P. “Already too late”: a qualitative study of respite care among mothers of children with special healthcare needs and disabilities. J. Pediatr. Nurs. 2023, 72, e114–e121. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Summary of Interviewees.
| Job title/sequence | Years of experience | Interview Time | |
| Participant 1 (B) | Charge nurse and nurse leader | 2 years | 64 minutes |
| Participant 2 (C) | Family support specialist consultant in charge | 4 years | 56 minutes |
| Participant 3 (D) | Room leader childcare worker | 10 years | 55 minutes |
| Participant 4 (E) | Child’s biological mother | - | 44 inutes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



