1. Brief Introduction to Aortic Valve Replacement
Aortic valve replacement (AVR) is a surgical treatment for people who have a severely diseased aortic valve (AV). The disease etiology can be aortic stenosis (AS), aortic insufficiency (AI), endocarditis, and congenital diseases such as a bicuspid aortic valve (BAV). AS is the most common valvular heart disease (VHD) in the developed world, accounting for two-thirds of VHD deaths between 1999-2020 [
1]. Many studies have found that the prevalence of AS is age dependent [
1,
2,
3], and with an aging population in the United States, the prevalence is up to 4.6% in adults older than 75 years old [
3]. AI is also associated with increasing age in developed countries but is found to be increasingly associated with infectious etiologies in developing countries [
4,
5]. In the Framingham study, the prevalence of AI was estimated to be up to 4.9% [
5]. In today’s age, there are many options on how to surgically treat AV disease (AVD), along with many valve options that are available to use. Surgical options include surgical AVR (SAVR) and transcatheter AVR (TAVR). The most common valve types that are available include mechanical and bioprosthetic valves. Overall, AVR is an indispensable treatment option for those with AVD.
2. Indications for Aortic Valve Replacement
2.1. Overview
AVD has multiple etiologies, including AS, AI, and endocarditis. All three etiologies are best evaluated with a transthoracic echocardiography (TTE) [
6]. While medical management can be used to treat these conditions temporarily, surgical treatment is considered a primary long-term treatment option, especially in severe disease. There have been many advances in the surgical options for AVR as well. TAVR became a popular treatment option in 2012 [
1] which was very beneficial for those who were considered inoperable. Also, the selection of the type of valve to use has evolved as new technologies continue to emerge. The 2020 American College of Cardiology (ACC)/American Heart Association (AHA) guidelines and the 2020 European Society of Cardiology (ESC)/European Association for Cardio-Thoracic Surgery (EACTS) guidelines will be referenced throughout this paper with specific classes and levels of recommendations listed in
Table 1,
Table 2,
Table 3,
Table 4,
Table 5,
Table 6,
Table 7,
Table 8 and
Table 9.
2.2. Aortic Stenosis
AS is the most common VHD in the developed world, accounting for 62.1% and 61.7% of VHD deaths between 1999-2020 in females and males, respectively [
1]. The progression of AS is variable between patients, with many being asymptomatic. However, studies have found that 75% of patients die within three years of symptom onset if no interventions are performed [
7]. Due to the increasing disease severity as one ages, current guidelines state AVR is indicated in patients that have severe symptomatic AS, and severe asymptomatic AS with a left ventricular ejection fraction (LVEF) of less than 50% [
3,
6]. It has been observed that there is a mortality benefit to perform AVR for those with mild AS that have LV dysfunction, especially as studies suggest myocardial fibrosis is occurring with progression of AS [
7,
8]. Samad et al. found that patients with moderate or severe AS with LV systolic dysfunction (LVSD) had a lower mortality rate when they received AVR compared to treatment with medical therapy alone [
9]. Kang et al. evaluated the outcomes of early surgery with AVR vs conservative care in asymptomatic patients with severe AS. They found that the early surgery group had a decreased incidence of death from cardiovascular causes as well as decreased incidence of any cause mortality compared to the conservative care group [
2]. Patients with AS, even when asymptomatic, can begin to lose functionality of the LV. This can lead to many deleterious consequences, and as such, eventual surgical repair is largely expected.
2.3. Aortic Insuffiency
AI is defined as regurgitation of blood into the LV due to insufficient closing of the AV [
4]. This disease has a prevalence of up to 4.9%, which increases with age, and accounts for greater than 50% of AVRs in the United States [
5]. AI can be an acute or chronic manifestation. Acute manifestations are typically due to infective endocarditis (IE), aortic dissection, and traumatic rupture [
4,
5]. Chronic AI can be due to calcific disease, BAV, connective tissue diseases, and rheumatic heart disease [
4,
5]. Acute AI is a higher acuity situation as severe LV overload can occur very rapidly leading to pulmonary edema, hypotension, and cardiogenic shock. Therefore, early surgical intervention of acute AI is necessary and should not be delayed [
5,
6]. Current guidelines state that patients with severe symptomatic AI should obtain an AVR regardless of LV status, and patients with severe asymptomatic AI should obtain an AVR when LVEF is less than 55% [
6]. While acute AI requires surgical intervention immediately, chronic AI can be asymptomatic as LV remodeling occurs over time. This, however, can lead to heart failure, and surgical intervention may be warranted at this stage [
5]. AVR is a very important treatment option for those with AI, especially in acute situations when surgery is necessary.
2.4. Endocarditis
Endocarditis is broadly defined as an infection of the endocardium. IE is a rare condition; however, it carries a 15-30% mortality rate [
10,
11,
12]. Prior conditions, such as rheumatic heart disease, degenerative valve disease, intravenous drug use, and congenital heart diseases are all key risk factors for the development of IE [
10]. In order to treat IE, broad antibiotic treatment against the pathogen needs to be initiated, and further analysis on surgical intervention should be evaluated by a Multidisciplinary Heart Valve Team (MDT) [
6]. Other etiologies of endocarditis include nonbacterial thrombotic endocarditis, Libman-Sacks endocarditis, vasculitis, and connective tissue disease [
11]. Rather than being caused by an infection, these conditions may be due to hypercoagulable states, systemic lupus erythematosus, and congenital disorders [
11]. Surgical intervention is indicated when patients present with valvular dysfunction, complications such as heart block, aortic abscess, or destructive lesions ensue, and when patients have persistent or recurrent infections [
6,
11]. Up to 50% of patients will require surgical intervention due to heart failure, failure to control the infection, and to prevent septic emboli [
12]. Endocarditis, particularly IE, is a disease with many complications and carries a poor prognosis. Antibiotic treatment and surgery are part of the limited options patients have to treat this disease.
3. Selection of Valve Type
3.1. Overview
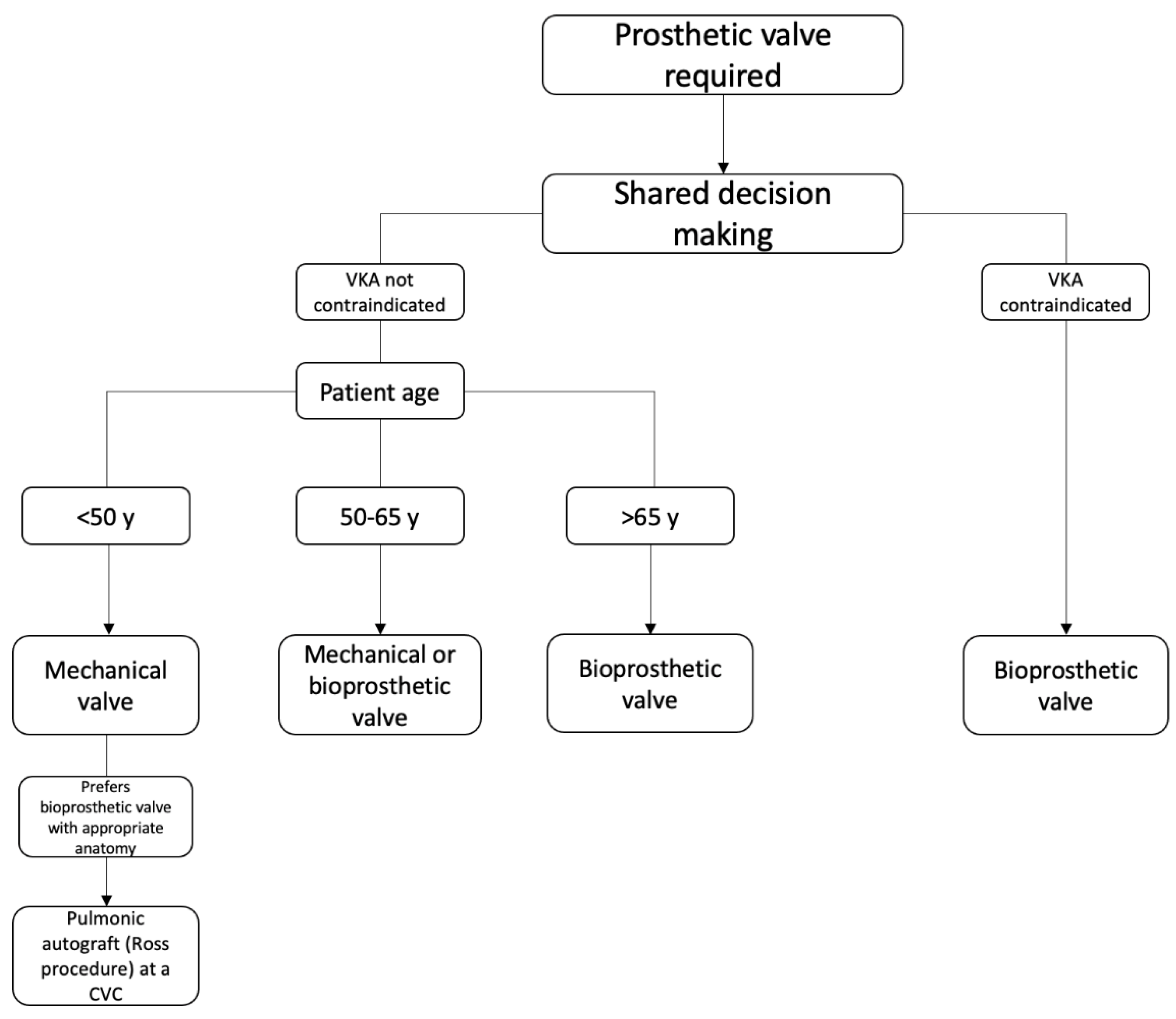
The selection of valve type in AVR depends on many factors. Above all else, shared decision making is the largest consideration in this process [
6]. This is because the selection of valve type comes with significant lifestyle changes for the patient. The main valve types that are available include mechanical, bioprosthetic, and using a pulmonic valve autograft – the Ross procedure. Sutureless valves are subtypes of bioprosthetic valves, and TAVR is transcatheter delivery option for bioprosthetic valves. Other considerations in deciding which valve to use include age, life expectancy, and medication adherence [
13]. These considerations are very important in ensuring a successful valve replacement for these patients. A simplified decision process is outlined in
Figure 1.
3.2. Mechanical
The first successful AVR was done in the 1960s using a mechanical valve [
13]. There have been many advances in the types of mechanical valves available since then. For example, the caged ball valve, which was a metal cage with a ball inside that would change positions based on pressure within the chamber, is no longer used due to the high risk of clotting and adverse hemodynamic effects. Current models include the tilting disc valve and the bileaflet valve. These are less thrombogenic, which is very important in mechanical valves where thromboemboli are the main concern post-procedure [
13,
14]. Therefore, lifelong anticoagulation using vitamin K antagonists (VKAs) are a requirement for patients receiving this valve [
6,
13,
14] and major bleeding events are the largest consequence [
14]. As stated above, age is a very important consideration when deciding if a patient should receive a mechanical valve or not. Mechanical valves are known for their longevity, lasting over 20 years [
13]. Therefore, patients less than 50 years old should be considered for a mechanical valve as long as there are no contraindications to VKA therapy [
6].
3.3. Bioprosthetic
Bioprosthetic valves are generally made of bovine pericardium or porcine aortic valves, but they can also be made of equine or porcine pericardium [
14,
15]. These valves can be stented, reinforced with a stent frame and a sewing ring, or stentless, lacking the stent frame and sewing ring [
15]. The main consideration in receiving a bioprosthetic valve is age. Even though VKA therapy is not needed post bioprosthetic valve placement, structural valve degeneration (SVD) is a known consequence. The 15-year risk for reoperation is 22%, 30%, and 50% for patients receiving the valve at 50, 40, and 20 years old, respectively [
6]. Therefore, patients older than 65 years old, or those with a contraindication to VKA therapy, are recommended to receive a bioprosthetic valve [
6]. More research into the pathophysiology of SVD is necessary to mitigate long-term risks for these patients, especially as the use of bioprosthetic valves are increasing compared to mechanical valves [
15].
3.4. Sutureless Valves
Sutureless valves are types of bioprosthetic valves that do not require extensive sutures to anchor them into place (although they do still require placement of sutures) [
16]. There are three commercially available for use. Those include the 3F Enable, Perceval S, and Intuity Elite. The diseased valve is excised prior to positioning of these valves. The 3F Enable requires one suture while the Perceval S requires none. These both work using a nitinol metal frame that is positioned and deployed into the valve for adherence [
16]. The Intuity Elite valve is a balloon expandable valve that is stainless steel and cloth covered. It works by using balloon catheter guidance for the correct positioning, then it is expanded to the correct annular size, and is secured with three sutures [
16]. As these valves do not need extensive suturing, the operation time and cross-clamp time is decreased [
16] making these valves great options for those who cannot undergo cardiopulmonary bypass (CPB) for an extended amount of time.
An important consideration prior to using sutureless valves is the size of the aortic annulus and therefore the size of the valve. As the anchoring process is mainly achieved by correct positioning before deploying the valve rather than the use of sutures, paravalvular leak and valve migration are rare complications [
16]. Studies have shown that the incidence of paravalvular leaks, about 2-4%, was correlated with the learning curve required for this surgery and was significantly reduced over time [
16]. Another possible consequence includes conduction disorders. To investigate this, van Boxtel et al. observed 31 patients who underwent sutureless AVR with Perceval S in the Netherlands. They found 11 patients developed a new left bundle branch block (LBBB) and four patients required permanent pacemaker placement due to complete atrioventricular block [
17]. The use of sutureless valves has become more popular with the increasing use of TAVR. This could possibly be due to an increasing number of patients, even those not classically considered candidates for AVR, being referred for TAVR and if their anatomy not amenable, sutureless valve placement can still be an option. However, it is still a relatively new surgical option and therefore, more research is needed to investigate the risks and benefits of this procedure, both short-term and long-term.
3.5. Transcatheter Aortic Valve Replacement
A transcatheter heart valve was first described in 1992 by HR Andersen et al. [
18,
19]. Now the two most common valves used in TAVR are currently the SAPIEN 3, a balloon expandable valve, and the Evolut, a self-expandable valve [
20]. The design of these two valves have contributed to the development of TAVR as a safe, routine procedure [
21]. There are four different sizes of the SAPIEN 3 valve available: 20 mm, 23 mm, 26 mm, and 29 mm. The Evolut PRO System valve consists of an outer tissue wrap to enhance the seal the valve creates around the aortic annulus [
22]. The Evolut PRO valves comes in four sizes: 23 mm, 26 mm, 29 mm, and 34 mm [
22]. The SAPIEN 3 valve has been associated lower risk of 30 day mortality and permanent pacemaker implantation, but the SAPIEN 3 and Evolut PRO has been shown to be comparable for risk of stroke, major vascular complications, device success, and moderate-severe residual aortic regurgitation [
23].
3.6. Ross Procedure
The Ross procedure, which has fluctuated in and out of favor over since it was first introduced in the 1960s, is a notable option for AVR. The procedure consists of removal of the diseased aortic valve, followed by excision of the patient’s own pulmonic valve and transplanting it in the aorta. The pulmonic valve is then replaced with a homograft [
6]. An autograft provides numerous benefits in both short-term and particularly long-term outcomes of patients undergoing the Ross procedure as opposed to mechanical and bioprosthetic AVR. In a network meta-analysis conducted by Yokoyama et al., patients who underwent the Ross procedure had lower rates of pacemaker placement within 30 days of the procedure when compared to mechanical AVR (M-AVR) patients [
24]. Long-term outcomes as measured through the studies (~7.4 years) found that those who underwent the Ross procedure had significantly lower all-cause mortality and long-term strokes when compared to both bioprosthetic AVR (B-AVR) and M-AVR [
24]. Additionally, the Ross procedure resulted in significantly lower rates of reintervention and endocarditis when compared to B-AVR and major bleeding when compared to M-AVR [
24]. Patients who received the Ross procedure do not require long term anticoagulation therapy and maintain neurohumoral responsiveness, indicating a more promising quality of life [
24]. These outcomes are of particular interest in the young adult and child population as the Ross procedure has shown to have greater survival, decreased risk of complications, growth potential, and avoidance of anticoagulation therapy [
25]. The Ross procedure is currently the mainstay recommendation for aortic valve replacement in adolescents and young adults [
6].
Despite its promising results in numerous studies and meta-analyses, the Ross procedure does come with limitations. Of note, this study found that reintervention was higher in the Ross procedure when compared to M-AVR; however, this could likely be attributed to two valves being involved in the Ross procedure as compared to one valve in M-AVR [
24]. Beyond this, recent data suggests that the Ross procedure may lead to increased development of aortic regurgitation, especially if there is a mismatch between the aortic and pulmonic root at the time of surgery, and for those with a larger aortic annulus [
24]. Additionally, the surgery has numerous absolute and relative contra-indications including Marfan syndrome, pulmonary valve disease, immune disorders, 3-vessel coronary artery disease (CAD), rheumatic valve disease, and a dilated aortic root [
26]. Despite these limitations, the Ross procedure is a very promising alternative option for select patient populations and thus requires advanced patient education and thorough discussion.
4. Specific Clinical Scenarios
4.1. Annular Size
Annular sizing plays a crucial role in achieving successful outcomes in AVR. Selecting the correct valve size is essential, as a patient’s unique annular dimensions often determine which procedure, SAVR or TAVR, will be most beneficial [
27,
28].
For patients with a smaller annulus, issues with patient-prosthesis mismatch (PPM) are common. This mismatch occurs when the valve is too small relative to body size, leading to elevated gradients across the valve and potentially reducing survival rates [
29]. When the patient is undergoing SAVR, an annular enlargement procedure can be performed (such as Manougian, Nicks, Konno, or Y technique) in order to place a larger valve [
30]. In TAVR specifically, accurate annular measurements are critical to avoiding complications like paravalvular leaks, valve migration, or annular rupture [
31]. Despite this, post-operative complications arise in patients with a small annulus who undergo TAVR or SAVR.
Patients with larger annuli, on the other hand, may face challenges with device positioning and anchoring [
32]. Patients with larger annuli who undergo TAVR are at higher risk for paravalvular regurgitation, which has been linked to worse long-term outcomes if left untreated [
33]. Therefore, these patients may be better suited for SAVR [
34].
Regardless of annulus size, when the prosthesis and annulus are misaligned, structural valve deterioration may occur over time, negatively impacting patient outcomes and potentially requiring additional interventions [
35,
36]. Proper annular sizing in both TAVR and SAVR is associated with improved hemodynamics, reduced re-intervention rates, and a better quality of life post-replacement.
4.2. Bicuspid Aortic Valve
A bicuspid aortic valve (BAV) is the most common congenital heart defect in adults, affecting 1-2% of the population [
37,
38,
39]. There are many etiologies leading to a BAV, but the most common is when two of the three aortic valve leaflets fuse, specifically the left and right cusps [
37]. It is recommended patients are evaluated in specialized BAV clinics due to the increased complexity of their care [
37]. Kang et al. found that depending on which leaflets are fused, the degree of valvular dysfunction and aortic enlargement differed [
38]. Importantly, more than half of patients with BAV will receive AVR in their lifetime [
40]. Furthermore, bicuspid aortopathy, considered the outcome of aortic dilatation and aneurysm in patients with BAV, is seen in up to 50% of patients, and about 1% can have an aortic dissection [
37]. As patients with BAV are also at a higher risk of AS, AI, and endocarditis, it is very important to follow their disease progression and ensure interventions are happening at ideal times [
37,
39].
Determining the optimal time for surgical intervention is still a debate for this patient population. For example, deciding to wait to intervene until symptoms begin is one question that still needs more research [
40]. SAVR is the recommended procedure for this patient population as the anatomy of the valve can be difficult for TAVR, but as sutureless valves continue to improve, this may become another option as well [
40]. More research is needed to determine when it is best to surgically intervene on this patient population.
Borger et al. investigated when the ascending aorta should be concomitantly replaced when patients with BAV were receiving AVR. They determined that when patients have an aortic diameter of 4.5cm or greater, the ascending aorta should be replaced at the time of AVR [
41].
4.3. Concomitant Procedures
Current guidelines for determining whether a patient can undergo concomitant procedures during AVR emphasize a comprehensive, individualized risk assessment. This assessment considers factors such as age, frailty, comorbidities, and input from a multidisciplinary heart team to guide the decision-making process, ensuring that the addition of procedures to AVR will provide a clear benefit to the patient. The ACC/AHA and the ESC/EACTS each provide key recommendations in this regard.
For patients with significant coronary artery disease (CAD)—typically defined as >50% stenosis in major coronary arteries—the guidelines recommend combining coronary artery bypass grafting (CABG) with SAVR, as this approach has been shown to improve long-term survival [
6,
42,
43]. In cases where patients have an ascending aortic diameter of ≥4.5 cm, guidelines also advocate for simultaneous aortic aneurysm repair to reduce the risk of rupture [
41,
43,
44,
45,
46,
47,
48,
49,
50,
51]. Patients with severe asymptomatic AS who are receiving cardiac surgery for other reasons are recommended to receive AVR as well [
6]. Studies suggest patients undergoing SAVR for AS who also have severe primary mitral regurgitation, mitral valve repair is advised at the time of surgery [
43]. Lastly, for patients undergoing surgery for CABG, the ascending aorta, or another valve, studies suggest concomitant AVR should be performed for both symptomatic and asymptomatic aortic regurgitation to optimize outcomes and reduce the need for future interventions [
43,
52,
53].
4.4. Lifelong Management of Valve Disease
After TAVR, managing heart block is crucial due to the risk of conduction complications. Patients with preexisting conduction abnormalities, such as right bundle branch block (RBBB) or significant aortic valve calcification, are at higher risk. They benefit from 48 to 72 hours of ECG monitoring post-procedure and temporary pacing may be used during this period to address transient blocks [
54,
55]. If persistent high-grade AV block or symptomatic bradycardia develops, permanent pacemaker implantation is considered based on the likelihood of conduction recovery [
54]. For mild, potentially reversible blocks, a conservative approach with extended monitoring helps avoid unnecessary permanent pacing [
54,
55]. Regular follow-up and ECGs are essential to monitor for late-onset conduction issues and confirm stability.
After AVR, the choice of antithrombotic and anticoagulant therapy depends largely on the type of valve and individual patient risk factors. For mechanical valves, lifelong anticoagulation with VKA is required to prevent thromboembolism, with a target INR of 2.5 to 3.5 depending on the valve position and patient-specific factors. Aspirin may be added in high-risk cases, though bleeding risks must be carefully managed [
56]. In contrast, bioprosthetic valves require less intensive anticoagulation. Typically, low-dose aspirin alone is recommended long-term [
56]. For TAVR, a short course of anticoagulation, usually three months of VKA or a direct oral anticoagulant (DOAC), may be prescribed initially, followed by aspirin alone if there are no other indications for anticoagulation [
56]. Dual antiplatelet therapy (DAPT) with aspirin and clopidogrel may also be used temporarily after TAVR to lower thromboembolic risk [
56]. Patient-specific factors, such as a history of atrial fibrillation or thromboembolism, are critical in guiding long-term anticoagulation needs, as these patients may require ongoing anticoagulation with VKA or a DOAC regardless of valve type. Regular INR monitoring for VKA users and clinical follow-ups to assess bleeding risks are essential to ensure that therapy remains safe and effective. This individualized approach balances the need for thrombotic prevention with the risk of bleeding complications.
5. Outcomes Between Surgical Aortic Valve Replacement and Transcatheter Aortic Valve Replacement
5.1. Stroke
Multiple meta-analyses have demonstrated no difference in risk of stroke between TAVR and SAVR across many patient characteristics [
57,
58,
59,
60]. TAVR is associated with a lower risk of stroke for patients that have had prior cardiac surgery [
61,
62]. For high-risk surgical patients, TAVR has been associated with greater risk of stroke up to three years post intervention [
63]. The PARTNER 3 (Safety and Effectiveness of the SAPIEN 3 Transcatheter Heart Valve in Low Risk Patients with Aortic Stenosis) Trial showed lower risk of stroke in TAVR vs SAVR patients at 1 year follow up, but not at 2 years [
64].
5.2. Length of Stay
TAVR’s shorter length of stay in comparison to SAVR makes TAVR a favorable option [
65]. The average length of stay in TAVR patients is about 6.2 days vs 10.2 days for SAVR, though this is an older study [
66]. A meta-analysis in 2017 examining five randomized controlled trials reported average length of inpatient stay to be 9.6 and 12.2 days for TAVR and SAVR, respectively [
67]. For female patients, average length of stay following TAVR has been reported as 7.8 days compared to 10.5 days for SAVR [
68]. When TAVR is performed concurrently with PCI, it has a shorter length of stay than SAVR with concurrent CABG, on average [
69]. Furthermore, length of stay for TAVR has decreased overtime [
70]. In 2013, length of stays for TAVR and SAVR where comparable; however, by 2016 length of stay for TAVR was significantly shorter [
70]. Lengths of stay for TAVR has continued to decrease since the studies above were published. Recent evidence from the Cleveland Clinic revealed that 85.9% of patients who underwent transfemoral TAVR in 2020 were discharged the same day or the following day [
71].
5.3. Heart Block
Following intervention, heart block is more common in patients who underwent TAVR than SAVR [
64]. Heart block is a common indicator for pacemaker placement following TAVR [
72]. As TAVR carries a higher risk for heart block over SAVR, TAVR is also associated with elevated 30-day risk for pacemaker implantation [
73]. Risk of pacemaker implantation for TAVR patients remains elevated when compared to minimally invasive SAVR [
74]. When examining 2-year outcomes following the NOTION trial, 41.3% of patients randomized to TAVR underwent pacemaker implantation compared to 4.2% in the SAVR group [
75].
5.4. Myocardial Infarction
At 30 days post intervention, risk of myocardial infarction (MI) following TAVR is less than half of the risk of MI following SAVR; however, the risk of MI is comparable in both at 1 and 2 year follow up [
73,
75]. These results are inconsistent with a multicenter randomized trial which demonstrated no significant difference of risk of MI between SAVR and TAVR at 1 month, 1 year, and 2 year follow up [
35]. It has been shown that females and patients with diabetes who undergo TAVR vs SAVR are less likely to experience a MI [
68,
76].
5.5. Death
TAVR and SAVR at 1 month and 1 year have been demonstrated to have comparable mortality rates [
73]. This comparable risk of mortality extends to 2 years, as demonstrated by the NOTION trial studying TAVR vs SAVR in patients with severe AS [
75]. A recent meta-analysis investigating low-risk patients with severe AS revealed all-cause mortality at a 10 year follow up to be 45.8% and 56.6% for TAVR and SAVR patients, respectively. [
57]. Risk for cardiovascular death following TAVR or SAVR do not differ significantly at 1- and 5-year follow up [
77].
5.6. Need for Repeat Intervention
There is evidence to show that TAVR carries a larger risk for repeat intervention than SAVR [
78]. The PARTNER 2 study in 2016 showed increased risk for reintervention following TAVR compared to SAVR [
35]. More recent studies have shown a similar increased risk for reintervention following TAVR compared to SAVR, but these were not significant findings [
79,
80]. Recent evidence shows that increased risk for reintervention following TAVR is concentrated within the first-year post procedure [
81]. The need for repeat intervention following TAVR is decreasing over time, with patients in the early 2010s having a 50% increased risk of reintervention than patients treated more recently [
82]. Suspected reasons for reintervention in TAVR include paravalvular leak, valve embolization, and coronary obstruction [
82]. For SAVR, endocarditis is a common cause for reintervention [
81]. Reintervention with SAVR following TAVR carries an increased risk of mortality compared to repeat SAVR after prior SAVR [
83].
6. Importance of the Multidisciplinary Heart Valve Team
The 2020 VHD guidelines list the multidisciplinary heart valve team (MDT) and heart valve centers as having high importance regarding treatment decisions in VHD. Patients with severe VHD are more strongly recommended to use this service, but asymptomatic patients, patients with multiple comorbidities, or any patient that is deciding on which treatment option is best for them is also recommended to consult an MDT. This team consists of many members, including a primary care cardiologist, VHD cardiac specialists, specialists in cardiac imaging, interventional cardiologists, and more. The goal of this team is to thoroughly discuss treatment options with patients and allow for shared decision making so the best outcome is obtained [
6].
7. Discussion
Aortic valve disease is common and highly prevalent around the world. Many patients will require surgical intervention in order to improve hemodynamics, and AVR is the primary treatment option. Between SAVR and TAVR, SAVR has a lower risk of post-operative heart block and decreased reintervention rates. However, TAVR is less invasive and has a shorter length of hospital stay post-procedure. The two techniques are comparable in stroke and MI risk, and mortality rates. Valve-in-valve (VIV) techniques are increasing in popularity as well. This procedure allows for a transcatheter rather than surgical approach when the bioprosthetic valve has degenerated and reintervention needs to occur [
84]. The main adverse events include malpositioning of the valve, coronary obstruction, and elevated post-procedure gradient [
84,
85]. The largest considerations for patients receiving this procedure are the internal diameter of the current valve, etiology of SVD, and the type of valve that needs to be implanted. Studies have found an association between small internal diameter sizes, <21mm, and worse survival for patients [
84,
85]. VIV is a valuable option for those who need reintervention and fit the surgical considerations for positive outcomes.
Valve selection is an important consideration, with the ability to adhere to VKA therapy and age being the largest deciding factors. Between bioprosthetic and mechanical valves, mechanical valves have increased longevity. However, a downfall of mechanical valves is the need to be on chronic VKA therapy which places these patients at a higher bleed risk. Bioprosthetic valves do not require VKA therapy, so this option is important for those who have contraindications. SVD is an important consequence of bioprosthetic valves; however, there is a current trend towards using more bioprosthetic valves. This may be due to the increasing age of those receiving AVR, patients not wanting to be on chronic VKA, and bioprosthetics having better hemodynamic stability [
15]. The age cutoffs listed in the ACC/AHA guidelines are reasonable with current research. However, it is important to note that shared decision making is a huge factor. With the rise of VIV surgery, those with failing bioprosthetic valves have a noninvasive surgical option for reoperation. As long as all considerations are discussed with the patient, including the likelihood of reoperation, then either valve is reasonable to use with any age.
The Ross procedure is used mainly in children and young adults who have no anatomic contraindications to the use of a pulmonic autograft. The positive long-term outcomes of this procedure make it a valuable option for those who need intervention early in life. Sutureless valves, a subtype of bioprosthetic valves, are a decent option for those who cannot undergo prolonged CPB. Due to their nature of not needing as many anchoring sutures placed, patients who have decreased hemodynamic stability prior to procedure benefit from their use. The increasing population age and therefore the increasing prevalence of AVD ensures that AVR will continue to hold a primary role in treatment.
Author Contributions
Conceptualization, S.P., J.T.W., T.E.H., P.T., and A.E.M; methodology, S.P., J.T.W., T.E.H., P.T., and A.E.M.; software, S.P.; validation, S.P., J.T.W., T.E.H., P.T., and A.E.M; formal analysis, S.P., J.T.W., T.E.H., P.T., and A.E.M; investigation, S.P., J.T.W., and T.E.H.; resources, S.P., J.T.W., T.E.H., P.T., and A.E.M; data curation, S.P., J.T.W., and T.E.H.; writing—original draft preparation, S.P., J.T.W., and T.E.H.; writing—review and editing, S.P., J.T.W., T.E.H., P.T., and A.E.M; visualization, S.P.; supervision, P.T. and A.E.M.; project administration, S.P., J.T.W., T.E.H., P.T., and A.E.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Tan, M.C., et al., Trends and Disparities in Valvular Heart Disease Mortality in the United States From 1999 to 2020. J Am Heart Assoc, 2024. 13(8): p. e030895. [CrossRef]
- Kang, D.H., et al., Early Surgery or Conservative Care for Asymptomatic Aortic Stenosis. N Engl J Med, 2020. 382(2): p. 111-119. [CrossRef]
- Kanwar, A., J.J. Thaden, and V.T. Nkomo, Management of Patients With Aortic Valve Stenosis. Mayo Clin Proc, 2018. 93(4): p. 488-508. [CrossRef]
- Sassis, L., et al., Valve Repair in Aortic Insufficiency: A State-of-the-art Review. Curr Cardiol Rev, 2023. 19(1): p. e270422204131. [CrossRef]
- Akinseye, O.A., A. Pathak, and U.N. Ibebuogu, Aortic Valve Regurgitation: A Comprehensive Review. Curr Probl Cardiol, 2018. 43(8): p. 315-334. [CrossRef]
- Otto, C.M., et al., 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation, 2021. 143(5): p. e72-e227. [CrossRef]
- Carabello, B.A. and W.J. Paulus, Aortic stenosis. Lancet, 2009. 373(9667): p. 956-66.
- Stassen, J., et al., Managing Patients With Moderate Aortic Stenosis. JACC Cardiovasc Imaging, 2023. 16(6): p. 837-855. [CrossRef]
- Samad, Z., et al., Aortic valve surgery and survival in patients with moderate or severe aortic stenosis and left ventricular dysfunction. Eur Heart J, 2016. 37(28): p. 2276-86. [CrossRef]
- Khalid, N., E. Shlofmitz, and S.A. Ahmad, Aortic Valve Endocarditis, in StatPearls. 2024: Treasure Island (FL).
- Ahmad, S.A., E. Shlofmitz, and N. Khalid, Aortic Valve Endocarditis Surgical Treatment, in StatPearls. 2024: Treasure Island (FL).
- Rajani, R. and J.L. Klein, Infective endocarditis: A contemporary update. Clin Med (Lond), 2020. 20(1): p. 31-35. [CrossRef]
- Gopal, S., J.M. Hauser, and S.K. Mahboobi, Mechanical Aortic Valve Replacement, in StatPearls. 2024: Treasure Island (FL).
- Head, S.J., M. Celik, and A.P. Kappetein, Mechanical versus bioprosthetic aortic valve replacement. Eur Heart J, 2017. 38(28): p. 2183-2191. [CrossRef]
- Rodriguez-Gabella, T., et al., Aortic Bioprosthetic Valve Durability: Incidence, Mechanisms, Predictors, and Management of Surgical and Transcatheter Valve Degeneration. J Am Coll Cardiol, 2017. 70(8): p. 1013-1028.
- Di Eusanio, M. and K. Phan, Sutureless aortic valve replacement. Ann Cardiothorac Surg, 2015. 4(2): p. 123-30.
- van Boxtel, A.G., et al., Postoperative conduction disorders after implantation of the self-expandable sutureless Perceval S bioprosthesis. J Heart Valve Dis, 2014. 23(3): p. 319-24.
- Rheude, T., et al., Spotlight on the SAPIEN 3 transcatheter heart valve. Med Devices (Auckl), 2018. 11: p. 353-360. [CrossRef]
- Andersen, H.R., L.L. Knudsen, and J.M. Hasenkam, Transluminal implantation of artificial heart valves. Description of a new expandable aortic valve and initial results with implantation by catheter technique in closed chest pigs. Eur Heart J, 1992. 13(5): p. 704-8. [CrossRef]
- Witberg, G., et al., Center Valve Preference and Outcomes of Transcatheter Aortic Valve Replacement: Insights From the AMTRAC Registry. JACC Cardiovasc Interv, 2022. 15(12): p. 1266-1274.
- Vahl, T.P., S.K. Kodali, and M.B. Leon, Transcatheter Aortic Valve Replacement 2016: A Modern-Day "Through the Looking-Glass" Adventure. J Am Coll Cardiol, 2016. 67(12): p. 1472-1487.
- Medtronic. Transcatheter Aortic Heart Valves - Evolut PRO. November 14, 2024]; Available from: https://europe.medtronic.com/xd-en/healthcare-professionals/products/cardiovascular/transcatheter-aortic-heart-valves/evolut-pro.html.
- Alperi, A., et al., Meta-analysis Comparing Early Outcomes Following Transcatheter Aortic Valve Implantation With the Evolut Versus Sapien 3 Valves. Am J Cardiol, 2021. 139: p. 87-96. [CrossRef]
- Yokoyama, Y., et al., Ross Procedure Versus Mechanical Versus Bioprosthetic Aortic Valve Replacement: A Network Meta-Analysis. J Am Heart Assoc, 2023. 12(1): p. e8066. [CrossRef]
- Moroi, M.K., E.A. Bacha, and D.M. Kalfa, The Ross procedure in children: a systematic review. Ann Cardiothorac Surg, 2021. 10(4): p. 420-432. [CrossRef]
- Brown, K.N. and A. Kanmanthareddy, Ross Procedure for Aortic Valve Replacement, in StatPearls. 2024: Treasure Island (FL).
- Deeb, G.M., et al., 3-Year Outcomes in High-Risk Patients Who Underwent Surgical or Transcatheter Aortic Valve Replacement. J Am Coll Cardiol, 2016. 67(22): p. 2565-74. [CrossRef]
- Genereux, P., et al., Paravalvular leak after transcatheter aortic valve replacement: the new Achilles' heel? A comprehensive review of the literature. J Am Coll Cardiol, 2013. 61(11): p. 1125-36.
- Pibarot, P. and J.G. Dumesnil, Prosthesis-patient mismatch: definition, clinical impact, and prevention. Heart, 2006. 92(8): p. 1022-9. [CrossRef]
- Malfitano, M.J., et al., Modified Manouguian technique for aortic root enlargement: A case series. J Card Surg, 2022. 37(3): p. 574-578. [CrossRef]
- Makkar, R.R., et al., Transcatheter aortic-valve replacement for inoperable severe aortic stenosis. N Engl J Med, 2012. 366(18): p. 1696-704. [CrossRef]
- Baumgartner, H., et al., 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J, 2017. 38(36): p. 2739-2791. [CrossRef]
- Athappan, G., et al., Incidence, predictors, and outcomes of aortic regurgitation after transcatheter aortic valve replacement: meta-analysis and systematic review of literature. J Am Coll Cardiol, 2013. 61(15): p. 1585-95.
- Thourani, V.H., et al., Contemporary real-world outcomes of surgical aortic valve replacement in 141,905 low-risk, intermediate-risk, and high-risk patients. Ann Thorac Surg, 2015. 99(1): p. 55-61. [CrossRef]
- Leon, M.B., et al., Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med, 2016. 374(17): p. 1609-20. [CrossRef]
- Sa, M.P., et al., Impact of Prosthesis-Patient Mismatch After Surgical Aortic Valve Replacement: Systematic Review and Meta-Analysis of Reconstructed Time-to-Event Data of 122 989 Patients With 592 952 Patient-Years. J Am Heart Assoc, 2024. 13(7): p. e033176. [CrossRef]
- Verma, R., et al., Bicuspid aortic valve associated aortopathy: 2022 guideline update. Curr Opin Cardiol, 2023. 38(2): p. 61-67. [CrossRef]
- Kang, J.W., et al., Association between bicuspid aortic valve phenotype and patterns of valvular dysfunction and bicuspid aortopathy: comprehensive evaluation using MDCT and echocardiography. JACC Cardiovasc Imaging, 2013. 6(2): p. 150-61. [CrossRef]
- Borger, M.A., et al., The American Association for Thoracic Surgery consensus guidelines on bicuspid aortic valve-related aortopathy: Full online-only version. J Thorac Cardiovasc Surg, 2018. 156(2): p. e41-e74. [CrossRef]
- Bulut, H.I., et al., A Comprehensive Review of Management Strategies for Bicuspid Aortic Valve (BAV): Exploring Epidemiology, Aetiology, Aortopathy, and Interventions in Light of Recent Guidelines. J Cardiovasc Dev Dis, 2023. 10(9). [CrossRef]
- Borger, M.A., et al., Should the ascending aorta be replaced more frequently in patients with bicuspid aortic valve disease? J Thorac Cardiovasc Surg, 2004. 128(5): p. 677-83.
- Thalji, N.M., et al., The prognostic impact of concomitant coronary artery bypass grafting during aortic valve surgery: implications for revascularization in the transcatheter era. J Thorac Cardiovasc Surg, 2015. 149(2): p. 451-60. [CrossRef]
- Vahanian, A., et al., 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Rev Esp Cardiol (Engl Ed), 2022. 75(6): p. 524. [CrossRef]
- Davies, R.R., et al., Yearly rupture or dissection rates for thoracic aortic aneurysms: simple prediction based on size. Ann Thorac Surg, 2002. 73(1): p. 17-27; discussion 27-8. [CrossRef]
- Russo, C.F., et al., Aortic complications after bicuspid aortic valve replacement: long-term results. Ann Thorac Surg, 2002. 74(5): p. S1773-6; discussion S1792-9. [CrossRef]
- Svensson, L.G., et al., Relationship of aortic cross-sectional area to height ratio and the risk of aortic dissection in patients with bicuspid aortic valves. J Thorac Cardiovasc Surg, 2003. 126(3): p. 892-3. [CrossRef]
- Davies, R.R., et al., Natural history of ascending aortic aneurysms in the setting of an unreplaced bicuspid aortic valve. Ann Thorac Surg, 2007. 83(4): p. 1338-44. [CrossRef]
- Ergin, M.A., et al., Surgical treatment of the dilated ascending aorta: when and how? Ann Thorac Surg, 1999. 67(6): p. 1834-9; discussion 1853-6.
- Svensson, L.G., et al., Bicuspid aortic valve surgery with proactive ascending aorta repair. J Thorac Cardiovasc Surg, 2011. 142(3): p. 622-9, 629 e1-3. [CrossRef]
- Yasuda, H., et al., Failure to prevent progressive dilation of ascending aorta by aortic valve replacement in patients with bicuspid aortic valve: comparison with tricuspid aortic valve. Circulation, 2003. 108 Suppl 1: p. II291-4. [CrossRef]
- Park, C.B., et al., Fate of nonreplaced sinuses of Valsalva in bicuspid aortic valve disease. J Thorac Cardiovasc Surg, 2011. 142(2): p. 278-84. [CrossRef]
- Tribouilloy, C.M., et al., Excess mortality due to coronary artery disease after valve surgery. Secular trends in valvular regurgitation and effect of internal mammary artery bypass. Circulation, 1998. 98(19 Suppl): p. II108-15.
- Fiedler, A.G., et al., Aortic valve replacement associated with survival in severe regurgitation and low ejection fraction. Heart, 2018. 104(10): p. 835-840. [CrossRef]
- Mazzella, A.J., et al., Evaluation and Management of Heart Block After Transcatheter Aortic Valve Replacement. Card Fail Rev, 2021. 7: p. e12. [CrossRef]
- Lilly, S.M., et al., 2020 ACC Expert Consensus Decision Pathway on Management of Conduction Disturbances in Patients Undergoing Transcatheter Aortic Valve Replacement: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol, 2020. 76(20): p. 2391-2411.
- Carnicelli, A., Anticoagulation for Valvular Heart Disease. American College of Cardiology, 2015.
- Caminiti, R., et al., Long-Term Results Following Transcatheter Versus Surgical Aortic Valve Replacement in Low-Risk Patients With Severe Aortic Stenosis: A Systematic Review and Meta-Analysis of Randomized Trials. Am J Cardiol, 2024. 230: p. 6-13. [CrossRef]
- Cao, C., et al., Transcatheter Aortic Valve Implantation versus Surgical Aortic Valve Replacement: Meta-Analysis of Clinical Outcomes and Cost-Effectiveness. Curr Pharm Des, 2016. 22(13): p. 1965-77. [CrossRef]
- Khan, S.U., et al., Transcatheter vs surgical aortic-valve replacement in low- to intermediate-surgical-risk candidates: A meta-analysis and systematic review. Clin Cardiol, 2017. 40(11): p. 974-981.
- Sakurai, Y., et al., Transcatheter versus surgical aortic valve replacement for stenotic bicuspid aortic valve: Systematic review and meta-analysis. JTCVS Open, 2023. 13: p. 75-94. [CrossRef]
- Shehada, S.E., et al., Transcatheter versus Surgical Aortic Valve Replacement after Previous Cardiac Surgery: A Systematic Review and Meta-Analysis. Cardiol Res Pract, 2018. 2018: p. 4615043. [CrossRef]
- Latif, A., et al., Transcatheter Versus Surgical Aortic Valve Replacement in Patients with Cardiac Surgery: Meta-Analysis and Systematic Review of the Literature. J Cardiovasc Dev Dis, 2020. 7(3). [CrossRef]
- Liu, Z., et al., Transcatheter aortic valve implantation for aortic stenosis in high surgical risk patients: A systematic review and meta-analysis. PLoS One, 2018. 13(5): p. e0196877. [CrossRef]
- Leon, M.B., et al., Outcomes 2 Years After Transcatheter Aortic Valve Replacement in Patients at Low Surgical Risk. J Am Coll Cardiol, 2021. 77(9): p. 1149-1161. [CrossRef]
- Kermanshahchi, J., et al., Transcatheter Aortic Valve Replacement (TAVR) Versus Surgical Aortic Valve Replacement (SAVR): A Review on the Length of Stay, Cost, Comorbidities, and Procedural Complications. Cureus, 2024. 16(2): p. e54435. [CrossRef]
- Brescia, A.A., et al., Transcatheter Versus Surgical Aortic Valve Replacement Episode Payments and Relationship to Case Volume. Ann Thorac Surg, 2018. 106(6): p. 1735-1741. [CrossRef]
- Burrage, M., et al., Transcatheter Aortic Valve Replacement is Associated with Comparable Clinical Outcomes to Open Aortic Valve Surgery but with a Reduced Length of In-Patient Hospital Stay: A Systematic Review and Meta-Analysis of Randomised Trials. Heart Lung Circ, 2017. 26(3): p. 285-295. [CrossRef]
- Ando, T., et al., Hospital outcomes of transcatheter versus surgical aortic valve replacement in female in the United States. Catheter Cardiovasc Interv, 2018. 91(4): p. 813-819. [CrossRef]
- Abugroun, A., et al., Outcomes of Transcatheter Aortic Valve Replacement With Percutaneous Coronary Intervention versus Surgical Aortic Valve Replacement With Coronary Artery Bypass Grafting. Am J Cardiol, 2020. 137: p. 83-88. [CrossRef]
- Goldsweig, A.M., et al., Relative Costs of Surgical and Transcatheter Aortic Valve Replacement and Medical Therapy. Circ Cardiovasc Interv, 2020. 13(5): p. e008681. [CrossRef]
- Krishnaswamy, A., et al., Feasibility and Safety of Same-Day Discharge Following Transfemoral Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv, 2022. 15(6): p. 575-589. [CrossRef]
- Maeno, Y., et al., A Highly Predictive Risk Model for Pacemaker Implantation After TAVR. JACC Cardiovasc Imaging, 2017. 10(10 Pt A): p. 1139-1147. [CrossRef]
- Arora, S., et al., Meta-analysis of transfemoral TAVR versus surgical aortic valve replacement. Catheter Cardiovasc Interv, 2018. 91(4): p. 806-812. [CrossRef]
- Ahmed, A., et al., Minimally Invasive Versus Transcatheter Aortic Valve Replacement: An Updated Meta-Analysis and Systematic Review. Innovations (Phila), 2023. 18(5): p. 424-434. [CrossRef]
- Sondergaard, L., et al., Two-Year Outcomes in Patients With Severe Aortic Valve Stenosis Randomized to Transcatheter Versus Surgical Aortic Valve Replacement: The All-Comers Nordic Aortic Valve Intervention Randomized Clinical Trial. Circ Cardiovasc Interv, 2016. 9(6).
- Ando, T., et al., Comparison of Hospital Outcome of Transcatheter Versus Surgical Aortic Valve Replacement in Patients With Diabetes Mellitus (from the Nationwide Inpatient Sample). Am J Cardiol, 2017. 119(8): p. 1250-1254. [CrossRef]
- Mack, M.J., et al., 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet, 2015. 385(9986): p. 2477-84. [CrossRef]
- Ajmal, Z., et al., Comparative Outcomes of Transcatheter Versus Surgical Aortic Valve Replacement in Moderate-Risk Patients With Aortic Stenosis: A Systematic Review of Clinical Trials. Cureus, 2024. 16(9): p. e70268. [CrossRef]
- Blankenberg, S., et al., Transcatheter or Surgical Treatment of Aortic-Valve Stenosis. N Engl J Med, 2024. 390(17): p. 1572-1583. [CrossRef]
- Investigators, U.T.T., et al., Effect of Transcatheter Aortic Valve Implantation vs Surgical Aortic Valve Replacement on All-Cause Mortality in Patients With Aortic Stenosis: A Randomized Clinical Trial. JAMA, 2022. 327(19): p. 1875-1887.
- Grubb, K.J., et al., Reinterventions After CoreValve/Evolut Transcatheter or Surgical Aortic Valve Replacement for Treatment of Severe Aortic Stenosis. JACC Cardiovasc Interv, 2024. 17(8): p. 1007-1016. [CrossRef]
- Baron, S.J., et al., Long-term risk of reintervention after transcatheter aortic valve replacement. Am Heart J, 2024. 267: p. 44-51. [CrossRef]
- Hawkins, R.B., et al., Redo Surgical Aortic Valve Replacement After Prior Transcatheter Versus Surgical Aortic Valve Replacement. JACC Cardiovasc Interv, 2023. 16(8): p. 942-953. [CrossRef]
- Tarantini, G., D. Dvir, and G.H.L. Tang, Transcatheter aortic valve implantation in degenerated surgical aortic valves. EuroIntervention, 2021. 17(9): p. 709-719. [CrossRef]
- Yao, R.J., M. Simonato, and D. Dvir, Optimising the Haemodynamics of Aortic Valve-in-valve Procedures. Interv Cardiol, 2017. 12(1): p. 40-43. [CrossRef]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).