
Submitted:
14 December 2024
Posted:
16 December 2024
You are already at the latest version
Abstract
The aim of this study is to prepare patients for MRI procedures using a specialized training application. The software tracks participants’ movements within the MRI simulator and reproduces sounds characteristic of the scan. The Farneback optical flow algorithm detects even the slightest movements captured by the camera, allowing for movement assessment during the training session and enhancing patient readiness for real scanning. The project is aimed at reducing the likelihood of involuntary movements during scanning. For this purpose, specialized software and a simulator are used to provide effective preparation for the MRI diagnostic procedure. A pilot study was conducted on a group of 10 students aged 21 to 27. The findings reveal a significant reduction in the average of movements during testing, decreasing from 27.7 movements in the first test to 8.3 movements in the second test, representing an average reduction of 19.4 movements. Furthermore, two participants exhibited a notable decrease in self-reported anxiety levels after the first test.
Keywords:
MRI Simulator
; Patients
; MRI Preparation
; Motion Tracking
1. Introduction
Magnetic Resonance Imaging (MRI) is one of the most effective and informative diagnostic methods in modern medicine [1]. By harnessing the power of a strong magnetic field and radio frequency pulses, MRI provides detailed images of internal structures without using ionizing radiation. This makes the method safe for a wide range of patients, including children and those for whom X-ray exposure is contraindicated.
The primary advantages of MRI include its high accuracy in soft tissue visualization, which makes it indispensable for diagnosing diseases of the brain and spinal cord, joints, heart, and other vital organs. Due to its high resolution and the ability to detect pathologies at early stages, MRI enables doctors to make more precise diagnoses and effectively plan treatments. Additionally, the technology allows for the creation of three-dimensional models of organs, which is especially useful for preparing for complex surgeries.
The quality of MRI images directly depends on the patient’s ability to remain still [2]. Even minor movements can blur the images, reducing diagnostic accuracy. Therefore, when patients are unable to remain still, repeat scanning or sedation may be required, which increases risks. Sedation during MRI can lead to complications such as respiratory depression and airway obstruction, necessitating careful monitoring of the patient’s condition. Minimizing sedation levels, especially for those at risk of respiratory issues, helps reduce the likelihood of these complications and allows for a safer procedure [3].
Because MRI equipment demands substantial financial and staffing resources, it is not available in many medical facilities, especially in remote areas. This scarcity makes it extremely important to stay completely still during the MRI scan to avoid the need for additional scanning, which would result in further delays due to long waiting times.
This study focuses on preparing patients for a successful MRI procedure through the use of an early version of specialized training software. This software, in conjunction with an MRI simulator, not only gradually familiarizes patients with diagnostic conditions and, but also provides specialists with objective insights into the patient’s readiness for the procedure.
This study makes the following key contributions:
- We developed specialized software that connects to a camera installed in the MRI tube simulator and uses motion recognition algorithms to prepare patients for the procedure.
- We conducted a pilot study in which participants completed two 15-minute training sessions in the MRI simulator, allowing us to assess their adaptation to the procedure’s conditions.
- Our results demonstrated a significant reduction in participants’ movements after the training sessions. In the second session of the experiment, the number of participants’ movements was substantially lower compared to the first session. At the same time, the stress levels of 80% of participants remained unchanged after the first test, indicating that participants’ behavior during the simulated MRI procedure may be influenced not only by stress levels but also by other factors.
We believe this study expands scientific knowledge on MRI patient preparation by offering an alternative to standard approaches. Standard methods, such as those described in the ACR Manual on MR Safety (American College of Radiology, 2024, Chapter 5), generally do not take into account objective data on patient reactions to scanning conditions, which may limit diagnostic accuracy [4]. Our approach enables specialists to gather objective data on patient reactions, helping to minimize the impact of movements and improve diagnostic quality. This, in turn, reduces the need for sedatives and enhances the safety of the procedure for patients.
2. Previous Work
Currently, the topic of preparing patients for magnetic resonance imaging (MRI) procedures is of particular interest in the scientific and medical communities. Existing methods aim to reduce patient anxiety, improve their perception of the procedure, and enhance image quality, which helps minimize the need for anesthesia and sedative drugs, especially in the case of children and younger patients.
Among non-pharmacological preparation methods, training patients with MRI simulator models stands out, as it creates more realistic expectations and facilitates adaptation to the actual procedure. Ashmore et al. [8] demonstrated that using a mock scanner effectively reduced patient anxiety and minimized the need for sedatives. Hallowell et al. [9] highlight the importance of familiarizing patients with the sounds and process of the scanner, allowing them to mentally prepare for lying still in an enclosed space.
One of the popular approaches to preparation is the use of virtual reality (VR) technologies, which allow patients to familiarize themselves with the procedure in advance and reduce fear of the unknown. Studies show that VR helps patients better adapt to the MRI environment and reduces pre-scan anxiety [6]. These findings are supported by other research where VR is considered an effective tool for lowering stress levels in patients before scanning [7].
Another innovation has been the use of multimedia materials, such as animations and educational videos, to reduce patient anxiety. Animated videos and interactive stories help patients better understand the procedure, alleviating their anxiety and fear [10]. Recent data indicate that these methods significantly help patients perceive the procedure as more familiar and predictable [11].
Traditional methods, such as explaining the procedure by parents or caregivers and providing pamphlets, are still commonly used. However, comparative studies show that more innovative approaches, such as VR and multimedia methods, prove to be significantly more effective in preparing patients for MRI [12]. At the same time, involving parents or close family members in the preparation process positively influences the patient, as emotional support helps reduce anxiety, as confirmed by studies examining the role of support systems in psychological preparation for MRI [13].
To summarize, studies demonstrate that using VR, multimedia technologies, and MRI simulators significantly reduces anxiety and improves the patient experience during MRI procedures. This underscores the relevance of this topic in medical practice, where advancing methods of psychological preparation remain a crucial area. Our work aims to contribute to this field by proposing new approaches for further reducing patient stress before MRI.
3. Materials and Methods
Our project, "Mock MRI Software", aims to improve patient preparation for MRI procedures. To achieve this goal, a specialized program was developed to monitor patient movements and simulate sounds characteristic of the MRI procedure.
3.1. Functionalities and Interface Design of the System
The application is designed with an intuitive user interface optimized to enhance usability and operational efficiency. Figure 1 presents the main screen of the application, showcasing its key control elements. The interface structure provides streamlined access to core functional modules, including features for searching and adding new patients, as well as analyzing statistical data from previously conducted scans.
The application is equipped with camera integration, enabling real-time display of the patient’s image on the MRI simulator screen (see Figure 2). The interface provides the operator with access to key parameters, including volume adjustment and motion detector data. This window serves as the operator’s primary tool during patient testing in the MRI simulator, ensuring continuous monitoring of the patient’s condition and testing parameters to enhance the accuracy of preparation for the actual procedure.
Figure 3 illustrates an example of the statistical data displayed by the application. In the figure, we can see a summary of the participants who participated in the simulation, including the total number of participants, gender distribution, average age, and time metrics (maximum, minimum, and average time). The graph illustrates the gender distribution of participants, facilitating demographic analysis. It is important to note that the statistics do not contain any personal data, ensuring confidentiality. The data can be downloaded in two formats (i.e., Excel and PDF) for further analysis or use.
The developed application is a comprehensive multifunctional system designed to enhance the efficiency and reliability of patient preparation processes. Its integrated functionality includes data management, training test administration, result analysis, and automated report generation, which contribute to optimizing the administrator’s workflow. Table 1 presents the key functional modules of the system, their objectives, descriptions, and technical implementation details.
3.2. Motion Analysis Using Optical Flow
In the "Mock MRI Software" project, Gunnar Farnebäck’s optical flow algorithm is used for motion analysis. This algorithm plays a key role in accurately tracking patient movements and minimizing artifacts in MRI simulations [14].
Farnebäck’s optical flow algorithm is based on analyzing pixel brightness changes between successive frame, and is highly precise in evaluating small displacements. Its robustness to noise and ability to track even minor movements makes it ideal for medical imaging tasks requiring high accuracy in well-lit but noisy conditions [15]. Below, we provide the overview of the algorithm.
For each pixel in the initial image , the displacement is calculated to correspond to the subsequent image , under the condition:
A second-degree polynomial approximates local brightness:
where coefficients represent intensity within the pixel neighborhood. Substituting the displacement into the polynomial, we get:
Here, is the gradient, and is the Hessian matrix (second derivative of the image).
Minimizing quadratic deviation leads to:
An image pyramid improves accuracy through multiscale processing, making it resistant to noise and slight lighting variations, achieving high precision in real-time [16]. Studies confirm Farnebäck’s effectiveness in medical computer vision, such as MRI [17].
To refine accuracy, a threshold is set based on the average magnitude of optical flow vectors in the initial frames. The system calculates the mean of the first 800 vectors and adds a small offset (0.01) to ensure that the threshold slightly exceeds the average value.
3.3. Participants
As part of our study, ten healthy volunteers were selected: five women and five men aged between 21 and 27 years (mean 23.8, std 2.04). All participants were students who voluntarily took part in the study. The selection criteria included a lack of significant medical problems or chronic illnesses that could distort the results of the experiment, as well as psychological stability and readiness to undergo a procedure simulating an MRI.
Before inclusion in the study, each participant was thoroughly instructed about the objectives of the experiment, participation procedures, potential risks (e.g. discomfort or anxiety under simulation conditions), and benefits (familiarization with the MRI procedure). The experiment was approved by the college ethics committee, which ensured compliance with all ethical norms and standards. All participants provided their written consent, confirming their willingness to participate and understanding of the research procedures.
4. Experimental Setup and Test Layout
To test the motion recognition software, we created a mock-up of a magnetic resonance imaging scanner to simulate real scanning conditions, as illustrated in Figure 4. The mock-up was designed to provide the most realistic experience possible. It included a patient bed for participants to lie on, a built-in camera located on top of the mock-up to monitor movements and transmit real-time data to the developed software, and a sound simulation system that reproduced typical MRI noises, which further adapted the participants to real conditions.
The experiment consisted of three main phases, each aimed at preparing participants for magnetic resonance imaging to minimize anxiety and improve the quality of the acquired data. The pipeline of the experiment is presented in Figure 5. In the following, we describe each of the experimental phases.
- Phase 1: Participant Preparation.
-
The participants’ preparation consisted of two steps:
- 1.1
- Guidance and Explanation for Participants. In this step, the participants were informed about the study, including its objectives, structure, and all phases. Special attention was given to explaining the MRI simulation stages. Also, the participants were provided an opportunity to ask any questions, which were answered clearly to address any concerns.
- 1.2
- Signing of Consent. The participants signed a consent form confirming their understanding of and agreement to all study phases.
- Phase 2: Simulation Test Without Preparation.
-
The simulation test included the following steps:
- 2.1
- Completing the GAD-7 Questionnaire to Assess Anxiety Level. Assessing participants’ anxiety levels prior to the simulation represents a critical step aimed at identifying potential psychological barriers and subsequently adapting the preparatory process to enhance participant comfort and ensure the successful completion of the procedure. Participants completed the GAD-7 questionnaire, which consists of 7 questions aimed at assessing their level of anxiety before the simulation [18]. The anxiety level is evaluated on a scale from 0 to 21, where a higher score indicates a greater level of anxiety.
- 2.2
- Conducting the MRI Simulation. Participants underwent an MRI simulation under conditions resembling real ones (including sound and spatial constraints). The simulation lasted approximately 15 minutes, during which participant movements were monitored to assess their impact on the quality of MRI diagnostics.
- 2.3
- Data Analysis. Collected data were analyzed to evaluate the anxiety level and the number of registered movements that may affect the quality of the MRI scan.
- Phase 3: Mock Test After Training
This phase included three activities: filling out the questionnaire, conducting the second MRI simulation, and data analysis.
-
- 3.1
- Completing the GAD-7 Questionnaire Again to Assess Anxiety Level. After the first simulation, participants completed the GAD-7 questionnaire once more to evaluate changes in their anxiety levels.
- 3.2
- Conducting the MRI Simulation. Participants underwent a second MRI simulation under the same conditions as in Phase 2. The simulation lasted no less than 15 minutes, ensuring consistent conditions for comparison.
- 3.2
- Data Analysis. Results of the repeated simulation were analyzed to assess changes in the anxiety level and the number of registered movements that may have affect the quality of MRI diagnostics.
5. Results and Disscussions
This study assessed the motor activity of participants in an MRI simulator, taking into account their anxiety levels before the procedure. Specialized software, described in detail in previous sections, was used to detect and record movements captured by the camera during each simulation.
The analysis included only those movements that exceeded a predefined threshold value. This threshold was calculated as the average magnitude of the first 800 optical flow vectors, with a small corrective coefficient (0.01) added to exclude minor movements, such as breathing, from the final statistics.
The collected data included unique participant identifiers, gender, anxiety levels, and the number of movements recorded during each simulation. This approach allowed for a comprehensive evaluation of motor activity under simulation conditions and facilitated the identification of potential correlations between anxiety levels and simulation outcomes.
Figure 6 presents a chart showing the number of movements of each participant during the two simulations. The analysis of participants’ motor activity within the MRI simulator during the simulations demonstrated a significant reduction in the number of movements, indicating the impact of training activities. The average number of movements during the first simulation was 27.7, with a standard deviation of 11.44, while during the second simulation, it was 8.3, with a standard deviation of 4.32. The relative decrease in movements is 70.04%, highlighting the effectiveness of the simulation in reducing participants’ movements within the MRI simulator. These results emphasize the importance of training or adapting participants prior to conducting studies that require immobility.
The participants’ anxiety level was assessed before each simulation using the standardized GAD-7 scale. Analysis of the results showed that a decrease in anxiety before the second simulation compared to the first was observed only in 20% of participants (2 out of 10) (see Figure 7). In the remaining 80% of participants, the anxiety level remained stable between the two stages of testing. Such dynamics may be associated either with the absence of a significant effect of the simulation on the participants’ perception or with an initially low level of anxiety, which excluded further decrease.
6. Limitations and Future Study
To enhance the accuracy and generalizability of the study’s results, it is important to consider potential limitations that could have influenced its process and findings.
One such factor is the small sample size and lack of diversity among participants, which limits the reliability of the data and makes it challenging to apply the findings to a broader audience. Additionally, the simulator used in the study may not have fully replicated the real conditions of magnetic resonance imaging. This includes aspects such as noise level, lighting, and the overall environment, which could have influenced participants’ behavior and the final results.
In future research, the sample size is planned to be expanded by increasing the number of participants and including diverse groups, such as children and adolescents, to enhance data representativeness.
Additionally, a series of tests will be conducted to study the impact of participants’ emotional states on their motor activity during the simulation.
As part of the software update, a motion charting feature will be introduced to analyze not only the total number of movements but also their frequency and distribution over time.
Following testing with the new group of participants, the study will progress to conducting real MRI sessions for a comprehensive evaluation of the effectiveness of the developed training approach.
Furthermore, the MRI simulator will be refined to more accurately replicate real procedure conditions, including auditory, visual, and spatial parameters.
7. Conclusions
The results of the study demonstrated a significant reduction in participants’ motor activity during the second MRI test simulation. This highlights the importance of pre-procedure preparation, which enhances patients’ awareness and understanding of the processes involved in the examination.
Although the stress level questionnaires conducted before each simulation indicated no significant changes in stress levels for most participants, the observed reduction of 70% in motor activity during the MRI simulation suggests that the key factor in minimizing movements was participants’ awareness and understanding of the upcoming procedure. This finding leads to the conclusion that while stress levels remain an important aspect, the decisive factor in this case is patients’ knowledge about the examination process.
Author Contributions
“Conceptualization, V.E, H.C, and I.R.; methodology, V.E, H.C, and I.R.; software, V.E.; validation, V.E.; formal analysis, V.E, H.C, and I.R.; investigation, H.C, and I.R.; writing—original draft preparation, V.E.; writing—review and editing, V.E, H.C, and I.R.; supervision, H.C, and I.R.; project administration, V.E, H.C, and I.R.; All authors have read and agreed to the published version of the manuscript.”
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee (date of approval March 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The dataset is available at the following link: https://1drv.ms/b/c/1f8bdb0277025bb3/EdimHUW28oNAguay6fFBAQwBcHv5u1R70fCAfjKNNRV5cA?e=89yYar (accessed on December 14, 2024).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Jordan, D. State of the art in magnetic resonance imaging. Physics Today 2020, 73, 34–40. [Google Scholar] [CrossRef]
- Havsteen, I.; Ohlhues, A.; Madsen, K. H.; Nybing, J. D.; Christensen, H.; Christensen, A. Are movement artifacts in magnetic resonance imaging a real problem?—A narrative review. Front. Neurol. 2017, 8, 232. [Google Scholar] [CrossRef] [PubMed]
- American Society of Anesthesiologists Task Force on Anesthetic Care for Magnetic Resonance Imaging. Practice Advisory on Anesthetic Care for Magnetic Resonance Imaging: An Updated Report by the American Society of Anesthesiologists Task Force on Anesthetic Care for Magnetic Resonance Imaging. Anesthesiology 2015, 122, 495–520. [Google Scholar] [CrossRef] [PubMed]
- American College of Radiology. Manual on MR Safety. Available online: https://www.acr.org/-/media/ACR/Files/Radiology-Safety/MR-Safety/Manual-on-MR-Safety.pdf (accessed on 2 November 2024).
- Reyes-Santias, F.; García-García, C.; Aibar-Guzmán, B.; García-Campos, A.; Cordova-Arevalo, O.; Mendoza-Pintos, M.; Cinza-Sanjurjo, S.; Portela-Romero, M.; Mazón-Ramos, P.; Gonzalez-Juanatey, J.R. Cost Analysis of Magnetic Resonance Imaging and Computed Tomography in Cardiology: A Case Study of a University Hospital Complex in the Euro Region. *Healthcare* **2023**, *11*, 2084. [CrossRef]
- Ashmore, J.; Preparing paediatric patients for MRI with virtual reality. Rad Magazine, July 2021. Available online: https://www.radmagazine.com/wp-content/uploads/2021/07/July-2021-Preparing-paediatric-patients-for-MRI-with-virtual-reality-Dr-Jonathan-Ashmore.pdf (accessed on 2 November 2024).
- Stunden, C.; Stratton, K.; Zakani, S.; Jacob, J. Comparing a Virtual Reality–Based Simulation App (VR-MRI) With a Standard Preparatory Manual and Child Life Program for Improving Success and Reducing Anxiety During Pediatric Medical Imaging: Randomized Clinical Trial. Journal of Medical Internet Research 2021, 23. Available online: https://www.jmir.org/2021/9/e22942 (accessed on 2 November 2024). [CrossRef] [PubMed]
- Ashmore, J.; Di Pietro, J.; Williams, K.; Stokes, E.; Symons, A.; Smith, M.; Clegg, L.; McGrath, C. A Free Virtual Reality Experience to Prepare Pediatric Patients for Magnetic Resonance Imaging: Cross-Sectional Questionnaire Study. JMIR Pediatrics and Parenting 2019, 2. Available online: https://pediatrics.jmir.org/2019/1/e11684/ (accessed on 2 November 2024). [CrossRef] [PubMed]
- Hallowell, L.M.; Stewart, S.E.; de Amorim e Silva, C.T.; Ditchfield, M.R. Reviewing the process of preparing children for MRI. Pediatric Radiology 2008, 38, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Hamd, Z.Y.; Alorainy, A.I.; Alrujaee, L.A.; Alshdayed, M.Y.; Wdaani, A.M.; Alsubaie, A.S.; Binjardan, L.A.; Kariri, S.S.; Alaskari, R.A.; Alsaeed, M.M.; Alharbi, M.A.; Alotaibi, M.S.; Elhussein, N.; Khandaker, M.U. How Different Preparation Techniques Affect MRI-Induced Anxiety of MRI Patients: A Preliminary Study. Brain Sciences 2023, 13, https://www.mdpi.com/2076–3425/13/3/416. Available online: https://www.mdpi.com/2076-3425/13/3/416 (accessed on 2 November 2024). [CrossRef] [PubMed]
- Nakarada-Kordic, I.; Reay, S.; Bennett, G.; Kruse, J.; Lydon, A.-M.; Sim, J. Can virtual reality simulation prepare patients for an MRI experience? Radiography 2020, 26, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Szeszak, S.; Man, R.; Love, A.; et al. Animated educational video to prepare children for MRI without sedation: evaluation of the appeal and value. Pediatric Radiology 2016, 46, 1744–1750. [Google Scholar] [CrossRef] [PubMed]
- Harrington, S.G.; James, K.; Weagle, K.M.; et al. Strategies to perform magnetic resonance imaging in infants and young children without sedation. Pediatric Radiology 2022, 52, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, Y.; Zhang, Y.; Zhang, Y.; Zhang, Y.; Zhang, Y. An FPGA-Optimized Architecture of Real-time Farneback Optical Flow. In Proceedings of the 2020 IEEE International Conference on Artificial Intelligence Circuits and Systems (AICAS), Genova, Italy, 31 August–2 September 2020; p. 1. [Google Scholar] [CrossRef]
- Farnworth, T.; Renton, C.; Strydom, R.; Wills, A.; Perez, T. A heteroscedastic likelihood model for two-frame optical flow. IEEE Robotics and Automation Letters 2021, 6, 1200–1207. [Google Scholar] [CrossRef]
- Danudibroto, A.; Gerard, O.; Alessandrini, M.; Mirea, O.; D’hooge, J.; Samset, E. 3D Farnebäck Optic Flow for Extended Field of View of Echocardiography. In Functional Imaging and Modeling of the Heart; van Assen, H., Bovendeerd, P., Delhaas, T., Eds.; Lecture Notes in Computer Science, vol 9126; Springer: Cham, 2015; pp. 129–136. [Google Scholar] [CrossRef]
- Suji, R.J.; Bhadouria, S.S.; Dhar, J.; et al. Optical Flow Methods for Lung Nodule Segmentation on LIDC-IDRI Images. Journal of Digital Imaging 2020, 33, 1306–1324. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Archives of Internal Medicine 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Main Interface of the Mock MRI Software
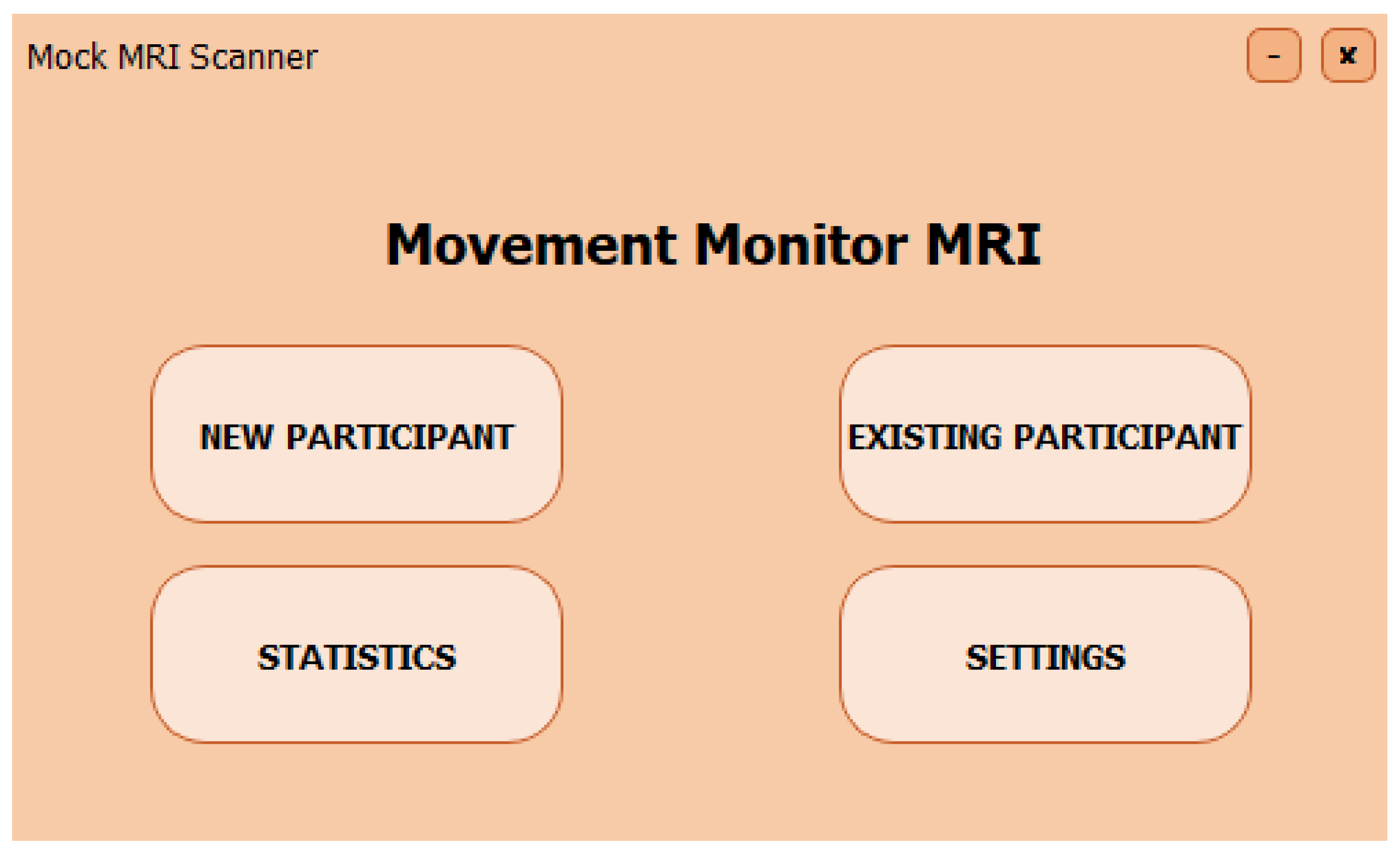
Figure 2.
Interface for Patient Monitoring During MRI Simulation
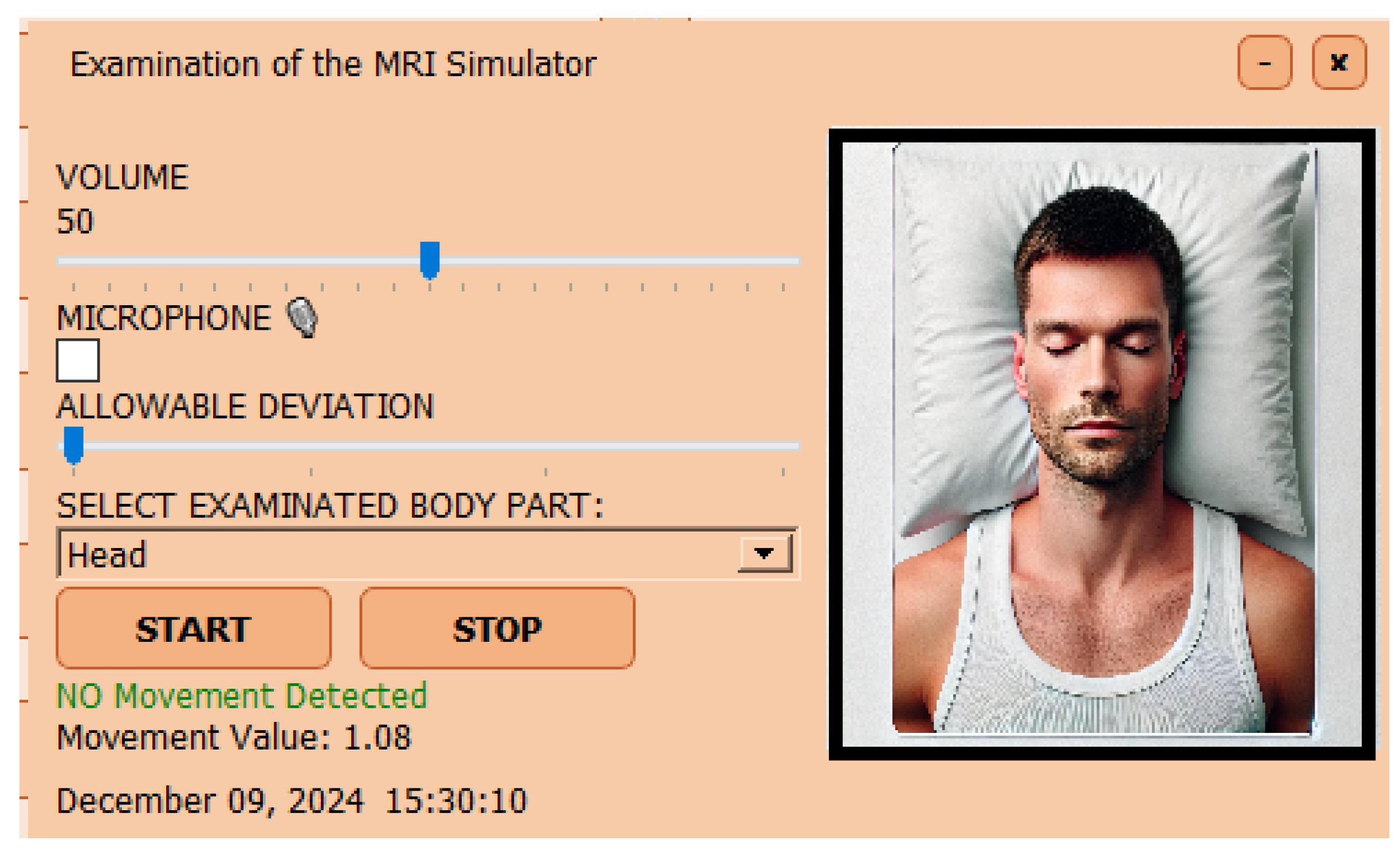
Figure 3.
Statistics Interface and Gender Distribution Graph
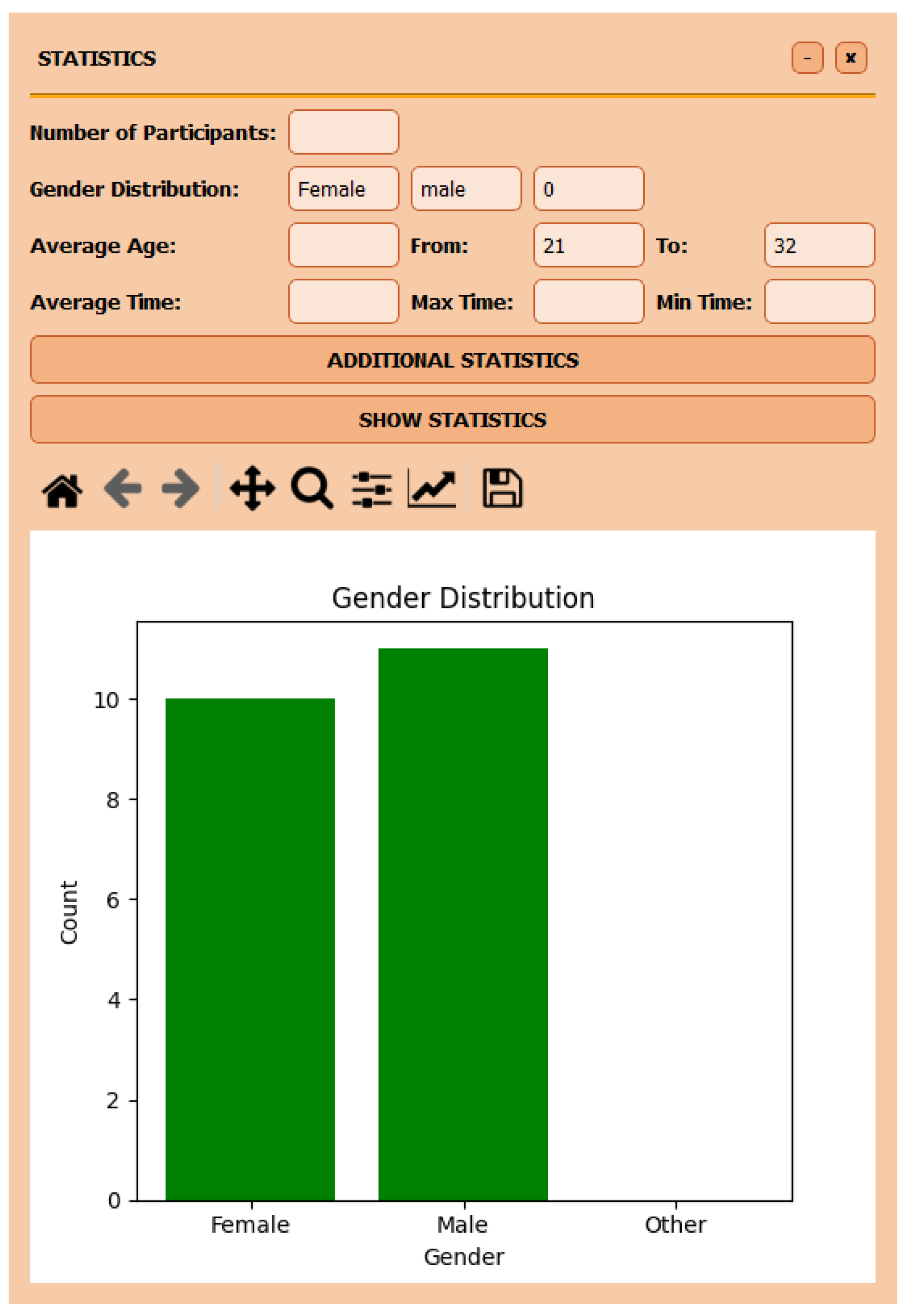
Figure 4.
Experimental MRI model
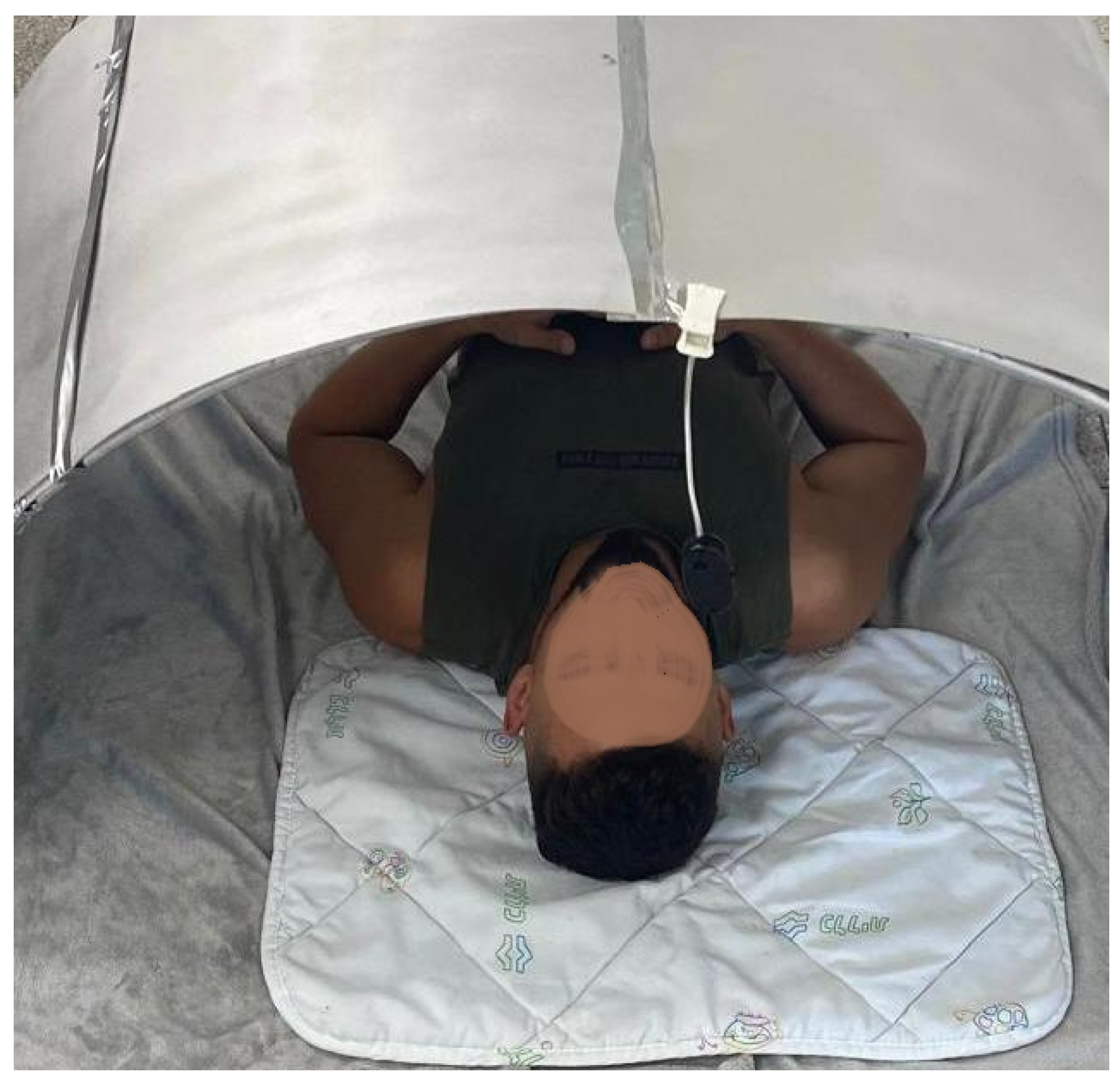
Figure 5.
Flowchart of the Experimental Process for MRI Preparationl
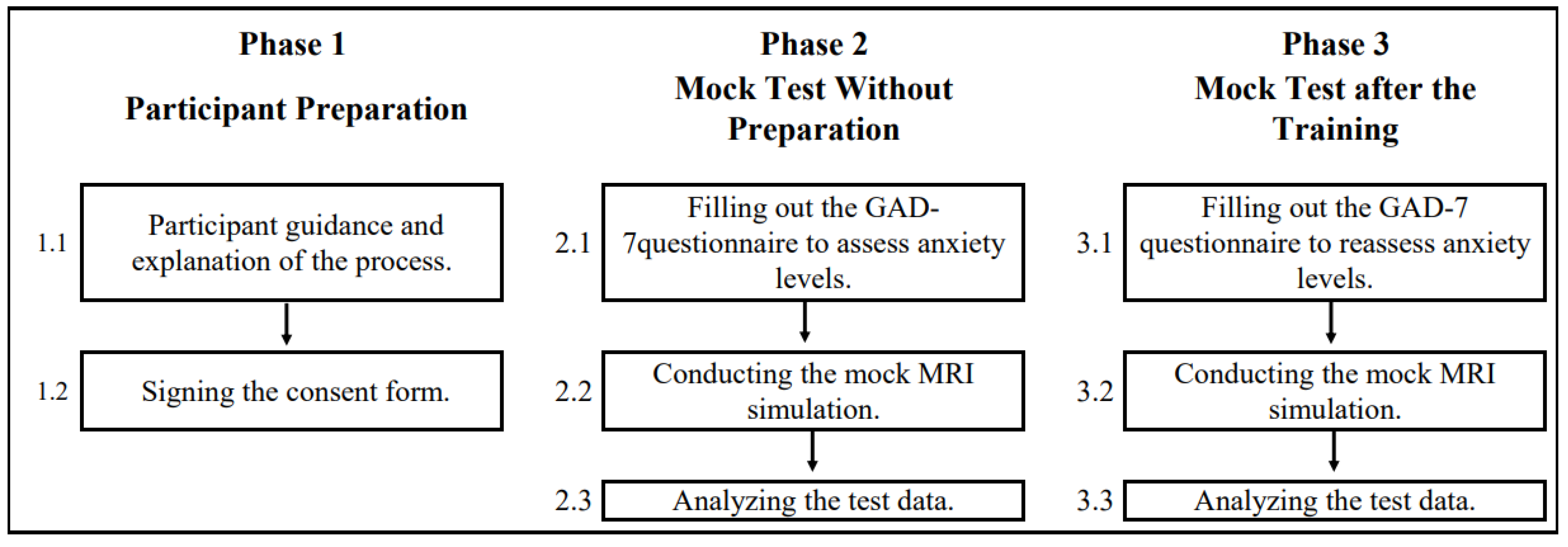
Figure 6.
Number of movements inside the MRI simulator during the first and second test sessions.
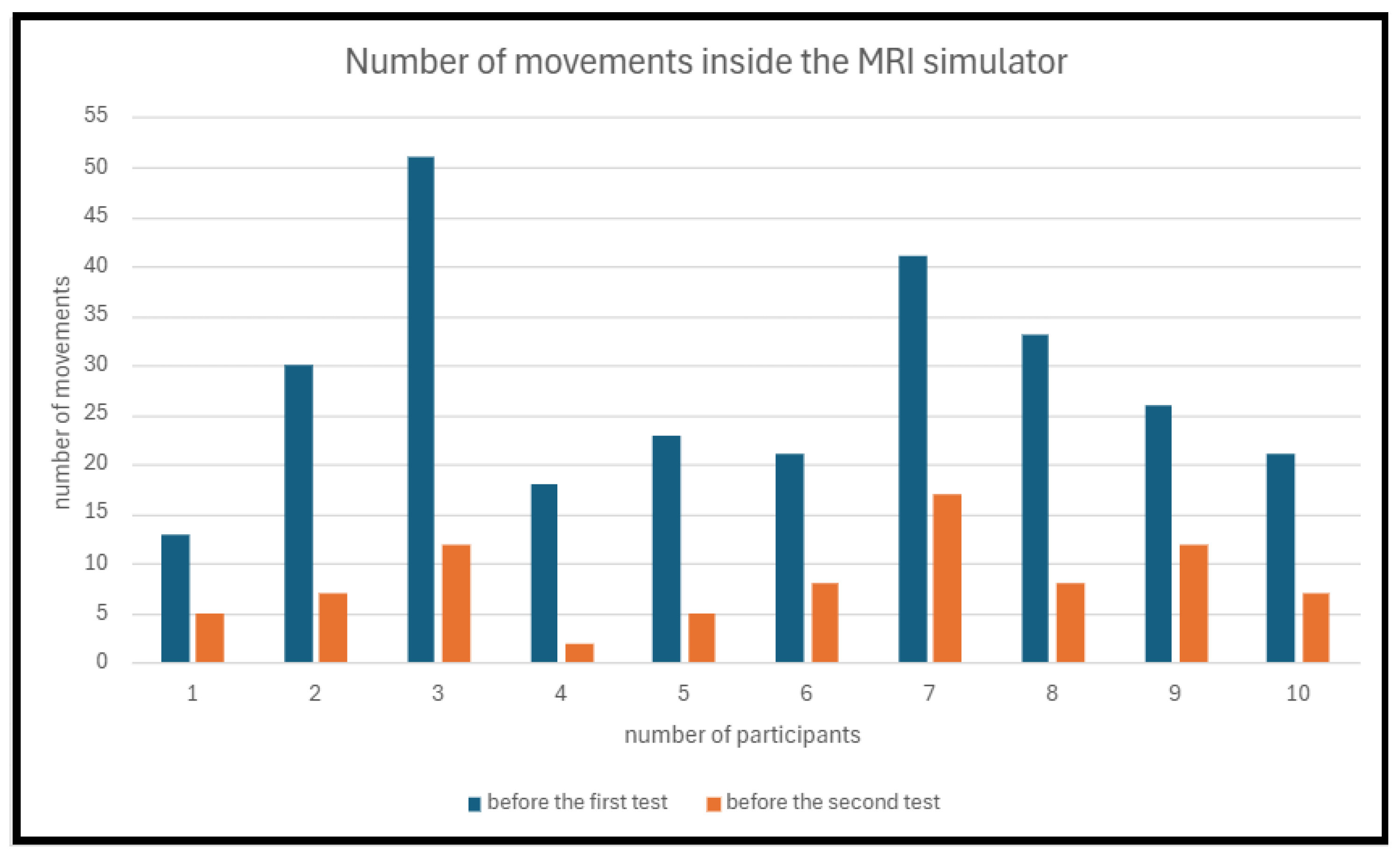
Figure 7.
Anxiety levels before the first and second tests for all participants.
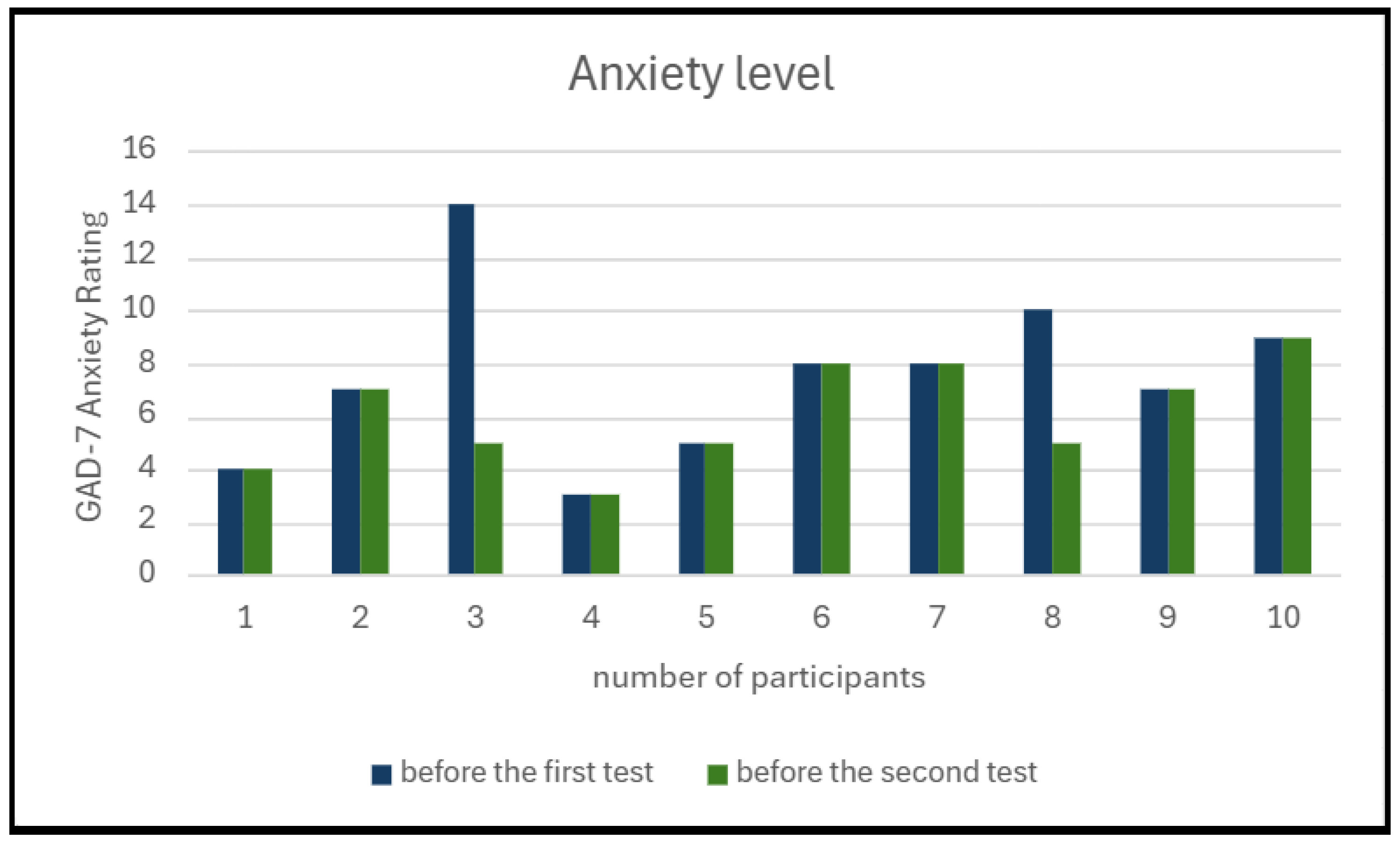

Table 1.
Functionalities of the Developed Application
| Functionality | Description | Objective | Technical Details |
| Authorization | The operator accesses the system using a unique login and password. | To ensure data security and prevent unauthorized access. | Verifies credentials with encryption and creates secure sessions. |
| Patient Registration and Data Storage | Registers new patients and stores their data in encrypted format. | To organize secure storage and processing of patient data. | Uses the SHA-256 algorithm for encryption and assigns a unique identifier to each patient. |
| Patient Search and Profile Viewing | Searches for a patient using a unique identifier and displays their profile with test history. | To provide quick access to patient data to track progress. | Retrieves data from the database by patient ID. |
| Test Initiation and Sound Simulation | Initiates or stops the test and adjusts MRI noise simulations. | To help patients acclimate to MRI conditions. | Synchronizes sound simulation with tests, allowing control of audio intensity. |
| Movement Detection and Value Generation | Tracks patient movements and generates values representing movement intensity. | To record movements and minimize MRI simulation artifacts. | Uses the optical flow algorithm to filter minor fluctuations and focus on significant movements. |
| Automated Result Generation | Generates a report of test results upon completion. | To automate documentation and eliminate manual review. | Records movements and generates reports stored in the database. |
| Test History and Statistics Viewing | Displays test history and analyzes statistical data. | To track patient progress and personalize preparation. | Presents historical data in graphs and tables for easy assessment. |
| Data History Storage and Security | Stores test history with encrypted identifiers for protection. | To ensure long-term secure storage of data. | Uses SHA-256 encryption to protect data from unauthorized access. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



