Introduction
Synthetic meshes composed of polyester or polypropylene are widely considered the standard approach in hernia repair. To prevent mesh displacement and subsequent hernia recurrence, prosthetic meshes require secure fixation to ensure adequate stabilization and optimal integration with the surrounding tissues [
1]. Although meshes and sutures are generally well tolerated, chronic pain and foreign body sensation may occur after repair and are multifactorial, and implantation may still provoke local tissue reaction, as with any implanted material. Consequently, there is a continued interest in developing surgical techniques and biomaterials that minimize adverse reactions while facilitating safe and effective mesh implantation and stabilization. Conventional fixation methods primarily include surgical sutures and staples. However, these penetrating techniques have been associated with acute and chronic postoperative pain [
2,
3] as well as local irritation, potentially resulting from the tissue tension or nerve compression by sutures and staples [
4,
5]. Such complications have driven the development of atraumatic fixation approaches, including the use of natural sealants such as fibrin glue [
6,
7], genetically engineered protein glues [
8] or synthetic cyanoacrylate-based adhesives [
9,
10]. Despite their clinical availability, these alternatives present notable limitations. Fibrin-based adhesives exhibit relatively low mechanical strength [
11] and a limited shelf-life after thawing. Cyanoacrylate adhesives, while providing strong bonding, may induce an inflammatory reaction and become rigid after polymerization [
12]. Furthermore, cyanoacrylates are characterized by rapid polymerization kinetics [
13], which limit intraoperative control; their fast setting time can complicate precise positioning and increase the risk of irreversible misapplication, as the adhesive cannot be repositioned or removed once polymerization has occurred.
Therefore, there is a need to investigate novel fixation strategies that enable improved procedural control, shorter operative time, and potentially decreased postoperative complications. In this context, light-sensitive biomaterials have emerged as potential candidates. These systems undergo rapid liquid-to-solid transition upon ultraviolet (UV) irradiation, potentially allowing better spatial and temporal control during fixation [
14,
15]. Their sensitivity to UV light is typically conferred by terminal methacrylate functional groups, whereas their mechanical properties, such as elasticity and tensile strength, are determined by the chemical structure of a polymer precursor [
16,
17]. Moreover, their chemical composition can be tailored to achieve controlled biodegradability over performance defined timeframes.
Recently, UV-curable biomaterials with tunable chemistry and degradation profiles have been developed and evaluated for soft tissue repair applications, demonstrating encouraging preclinical results [
14,
16,
17]. Newly developed UV-curable, biodegradable polymers [
18] provide controlled curing, enabling accurate placement while minimizing unintended adhesion to adjacent tissues during surgery. Moreover, these materials exhibit favorable mechanical flexibility and elasticity along with progressive
in vivo biodegradation (exceeding 65% mass loss after one year of implantation in rabbits) and a shelf-life exceeding two years (unpublished data). Collectively, these properties suggest that such a system may represent a viable alternative to currently available fixation modalities.
Importantly, the evaluation of fixation techniques must extend beyond technical performance to include patient-centered outcomes, such as postoperative pain and hernia recurrence rate. Chronic postoperative pain, including persistent neuralgia, has been recognized as a potential long-term complication following inguinal hernia repair, with symptoms persisting beyond one year after surgery [
19]. Pain severity may range from mild discomfort to debilitating symptoms that substantially impair quality of life [
20].
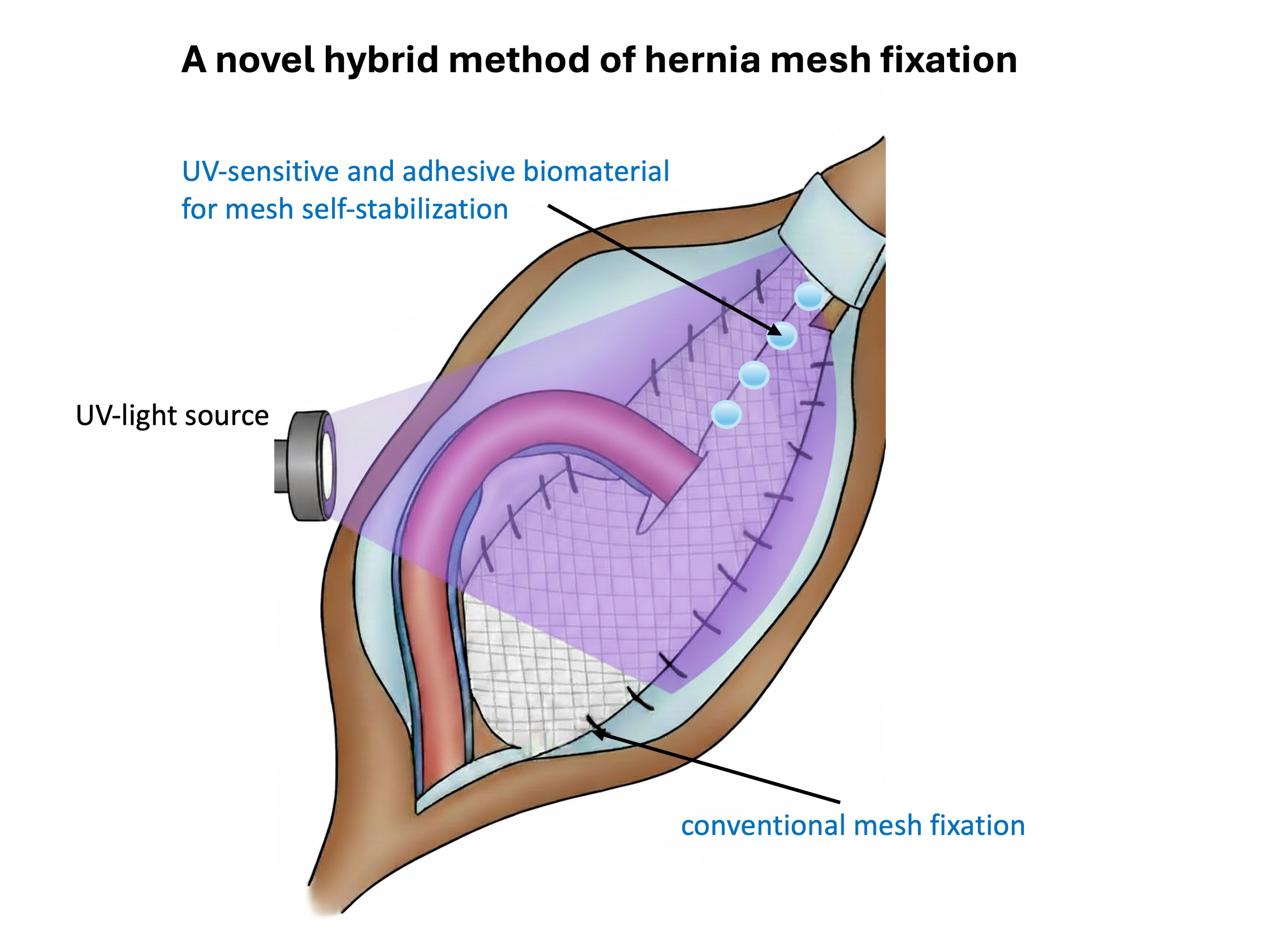
The present study aimed to evaluate the feasibility and short- and long-term clinical outcomes of a novel hybrid fixation approach in inguinal hernia repair: part of the mesh was secured conventionally, while the remaining portion was stabilized with the UV-curable adhesive biomaterial. Short-term outcomes, including postoperative pain, local hypoesthesia, clinically assessed hematoma formation, wound infection, and urinary retention, as well as long-term outcomes such as chronic pain, foreign body sensation, and hernia recurrence, were assessed. Operative time was also recorded in both groups and compared between hybrid fixation and conventional fixation.
Materials and Methods
Adhesive and UV-Sensitive Biomaterial
A UV-sensitive biomaterial with viscous and adhesive properties (experimental formulation, PolTiss sp. z o.o., Poland) was supplied in sterile, light-impermeable 1 mL syringes (single-use). The fundamental material characteristics have been previously described in [
21]. Briefly, the biomaterial is a viscous, syringe-delivered formulation intended to remain at the application site and allow controlled placement before curing. Upon UV exposure, it rapidly converts from a liquid to a flexible solid, enabling on-demand stabilization after mesh positioning (curing time: 3 minutes).
Patients
The study cohort comprised ten male patients who underwent elective inguinal hernia repair using the Lichtenstein tension-free technique (open approach). A standard oblique incision was made above the inguinal ligament, followed by identification and mobilization of the spermatic cord and dissection of the hernia sac. After separation of the spermatic cord from the hernia sac, the sac was managed according to established surgical principles. In cases of indirect (oblique) inguinal hernia, the sac contents were reduced into the peritoneal cavity, the redundant sac was excised, and the stump was ligated with a purse-string suture. In cases of direct inguinal hernia, the sac contents were reduced without opening the sac, and reinforcement of the transversalis fascia was performed. Subsequently, the posterior wall of the inguinal canal was reinforced with implantation of a polypropylene mesh (UltraproTM , Ethicon). The mesh was secured to the inguinal ligament using a continuous non-absorbable polypropylene suture (Prolene® 3-0). To prevent mesh folding or displacement, additional fixation to the external oblique aponeurosis was achieved using interrupted absorbable sutures (Novosyn, B.Brown).
Patients were randomly allocated into two groups. In the control group (n=5), the mesh was fixed with non-absorbable polypropylene sutures (Prolene® 3-0) according to the standard technique described above. In the study group (n=5), a hybrid fixation approach was used: part of the mesh was secured conventionally, while the remaining portion was stabilized with an adhesive biomaterial and then cured with UV irradiation, as demonstrated in
Figure 1. The biomaterial was cured with UV light, with a curing time of 3 minutes. The UV source was Labino® UVG2, with an emission peak at 365 nm. Eight fixation points were applied with the UV-sensitive biomaterial (one drop per point; 0.04 mL per drop). All procedures were performed under standard epidural or spinal anesthesia, as determined by the anesthesiology team. Perioperative antibiotic prophylaxis consisted of a single intravenous dose of cefazolin (Biofazolin, 1 g) administered approximately 30 minutes prior to incision, consistent with standard protocols for prosthetic implantation.
Inclusion Criteria
Eligible participants were physically active males aged 20-40 years with a Body Mass Index (BMI) of 25-27 kg/m2 and diagnosis of uncomplicated, unilateral, primary inguinal hernia. All participants were scheduled for elective hernia repair using the Lichtenstein technique and provided written informed consent prior to enrolment.
Exclusion Criteria
Exclusion criteria included recurrent hernia, prior laparotomy, history of deep vein thrombosis or pulmonary embolism, and significant comorbidities such as autoimmune, cardiovascular, or respiratory diseases. Patients with known allergies to implant materials, substance abuse disorders, or psychiatric illnesses were also excluded.
Postoperative Care
Postoperative management included routine monitoring of general clinical status, body temperature, heart rate, and arterial blood pressure. Surgical wound evaluation comprised assessment of local edema, and clinical signs of fluid collections within the implant area. Ultrasonographic examination of the operated regions was performed to assess tissue integrity and implant placement. Additionally, non-invasive thermographic analysis of the surgical site was conducted using a FLIR T335 thermal imaging camera to objectively evaluate local wound temperature as a surrogate marker of inflammatory response. Ultrasonography and thermography were analysed when imaging data were available; a sample size of five is reported for these assessments.
Ethical Approval
The study (medical research experiment) was conducted in accordance with the approval of the Ethics Committee of the Pomeranian Medical University (Resolution no. 04/2022 dated 24.03.2022) and adhered to the principles outlined in the 1975 Declaration of Helsinki and its subsequent amendments. Written informed consent was obtained from all participants, and patient confidentiality and anonymity were strictly preserved.
Statistical Analysis
Statistical analyses were performed using Statistica version 13.3 software (Statistica Software Inc., Palo Alto, CA, USA). Descriptive statistics were expressed as means ± standard deviations (SD). Given the pilot sample size, analyses were primarily descriptive. When inferential testing was applied, nonparametric methods were used (Mann-Whitney U test for between-group comparisons and Friedman test for within-group repeated measures). A p-value < 0.05 was considered statistically significant.
Results
We describe a novel technique for inguinal hernia repair that incorporates a UV-sensitive adhesive biomaterial to achieve partial self-stabilization of the implanted mesh (
Figure 2). In male patients with inguinal hernia—the most prevalent form of hernia in this population—appropriate mesh tailoring is required to accommodate the spermatic cord. Specifically, the mesh is incised over a length of approximately 2-3 cm to allow passage of spermatic cord. Following cord placement, the lateral edges of the incision are re-approximated and secured with sutures, thereby creating a slit-like aperture (“keyhole”) through which the spermatic cord traverses. The configuration enables anatomical positioning of the cord while maintaining adequate mesh coverage and reinforcement of the posterior wall of the inguinal canal.
In the study group, fixation of the incised mesh was achieved using a UV-curable adhesive biomaterial in place of conventional suturing (
Figure 2a,b). The biomaterial demonstrated satisfactory adhesive strength and provided effective stabilization of the mesh margins (
Figure 2c). The slit created to accommodate the spermatic cord maintained structural integrity and functioned as intended, ensuring appropriate cord positioning without evidence of displacement. All patients were discharged on the first postoperative day following hernia repair.
Postoperative follow-up demonstrated that all patients were in good general condition. Laboratory investigations, including serum electrolyte levels (ionogram), creatinine, urea, and routine urinalysis, were within normal reference ranges. Clinical evaluation revealed no abnormalities, with patients maintaining normal body temperature, heart rate, and blood pressure.
Operative time was shorter in the study group than in the control group (52.0 ± 3.1
vs 60.2 ± 3.7 min; p < 0.05; Mann-Whitney U test) (
Table 1). The application of the UV-curable polymer proved to be technically straightforward and less time-consuming than the placement of multiple sutures. This simplified fixation method reduced the extent of surgical manipulation required, thereby contributing to overall shorter operative times.
Clinical follow-up showed an overall stable postoperative course. No intraoperative complications were observed. During scheduled follow-up visits (postoperative day 1, day 8, 6 weeks, 12 months, and 24 months), no clinically significant early or late postoperative complications were recorded. No hernia recurrences were observed at 24 months.
Postoperative pain was assessed using the Visual Analogue Scale (VAS; 0–10, where 0 indicates no pain and 10 the worst pain imaginable) at postoperative day 1, day 8, 6 weeks, 12 months, and 24 months (
Table 2). VAS results are reported for the study group. The mean VAS pain score on the first postoperative day was 2.6 ± 0.55, corresponding to mild-to-moderate postoperative pain. By postoperative day 8, the mean pain score had decreased substantially to 0.8 ± 0.84, indicating a rapid resolution of early postoperative discomfort. Notably, no pain was reported at the 6-week, 12-month, or 24-month follow-up evaluations, with a mean VAS score of 0 at each time point, suggesting the absence of chronic postoperative pain in this cohort.
Assessment of foreign body sensation in the inguinal region was performed using validated Carolinas Comfort Scale (CCS) (
Table 3). The analysis demonstrated a progressive decline in symptom severity over time in both the study (hybrid mesh self-stabilization with UV-curable biomaterial) and the control group (conventional suture fixation). Overall, patient-reported foreign-body sensation was similar in both groups.
On the first postoperative day, the mean CCS-derived foreign body sensation score was 54.08% ± 9.74 in the study group and 65.32%± 4.26 in the control group, reflecting substantial early postoperative discomfort. In the UV-curable biomaterial fixation group, the mean score decreased to 40.98% ± 9.54 by postoperative day 8 and further declined to 30.38% ± 8.94 at the 6-week follow-up. A continued reduction in symptom severity was observed over time, reaching minimal levels at 24 months (1.38% ±1.50).
These findings indicate a consistent and marked improvement in patient-reported foreign body sensation over the follow-up period, with near-complete resolution of symptoms at long-term evaluation.
Chronic pain and activity limitation were evaluated using the EuraHS Quality of Life (EuraHS-QoL) questionnaire, and the results are summarized in
Table 4. The analysis demonstrated a significant overall improvement in all assessed parameters following inguinal hernia repair in both fixation groups. Preoperatively, mean pain intensity was 8.60 in both groups. Pain scores increased on postoperative day 1 and then decreased by day 8, with a further decline during follow-up, reaching 0 at 12 and 24 months in both groups. Pain levels continued to decline progressively during follow-up, reaching complete resolution at 12 months postoperatively.
Similarly, activity limitations attributable to hernia-related pain showed a marked reduction over time. The main activity restriction score decreased from 35.00 ± 3.16 on the first postoperative day to 6.60 ± 1.34 at the 6-week follow-up. Postoperative pain experienced in the supine position and activity restrictions secondary to hernia pain decreased irrespective of the fixation technique used. This improvement was consistent with uncomplicated wound healing and the absence of adverse events.
In this pilot sample, no clear differences between fixation methods were observed for EuraHS-QoL pain and activity restriction scores. These findings indicate that both fixation techniques yielded comparable outcomes with respect to chronic pain and functional recovery over time.
Postoperative quality of life was assessed using the validated 36-Item Short Form Health Survey (SF-36). As presented in
Table 5, SF-36 scores decreased at 6 weeks compared with preoperative values and then improved at 12 and 24 months.
Ultrasonographic evaluation of hybrid mesh placement was available in a subset of patients (n = 5) and is reported as an exploratory assessment. Out of five examined patients, the mesh was correctly positioned, with no sonographic evidence of hernia recurrence. No signs of peri-implant inflammatory infiltration were observed in two patients, whereas one patient showed features suggestive of localized inflammatory infiltration. A postoperative hematoma was detected in one patient. One of the five patients declined further imaging follow-up but reported no clinical symptoms during a structured telephone interview conducted at 24 months postoperatively.
Thermography was available for a subset of patients (n=5) and is reported as an exploratory assessment. Infrared thermography was used to assess temperature differences between unaffected tissue and the surgical site. Representative thermographic images illustrating tissue temperature distribution before and after surgery are shown in
Figure 3. Preoperatively (
Figure 3a), the hernia region exhibited elevated surface temperature, visualized as areas of increased intensity (red and yellow), consistent with localized inflammatory activity. Six hours postoperatively (
Figure 3b), increased temperature persisted in the perioperative region, with demarcated hyperthermic areas. On postoperative day 1 (
Figure 3c), elevated temperature remained detectable. However, a gradual reduction in thermal intensity was observed compared to earlier time points, consistent with a gradual attenuation of early postoperative thermal changes.
Discussion
Inguinal hernia repair remains one of the most frequently performed surgical procedures worldwide, and optimization of patient-centered outcomes is a primary objective of contemporary surgical practice. The principal goals of repair include rapid restoration of normal physical function, early return to work, a low recurrence rate (<1%), and minimization of postoperative discomfort, sensory disturbance rate, and chronic neuralgia. Although mesh fixation using sutures is well established and widely practiced, the present study evaluated a novel hybrid technique employing a UV-sensitive adhesive biomaterial to achieve mesh self-stabilization. This strategy represents a potential atraumatic fixation option, with the aim of reducing postoperative pain and supporting early recovery. In this pilot cohort, no hernia recurrences were observed in either group during follow-up. Operative time was shorter in the hybrid group, and early postoperative pain in the hybrid group was low. However, VAS data were available only for the study group, which limits between-group comparisons Our findings are consistent with previous reports indicating that alternative, non-penetrating fixation method—particularly tissue adhesives—may reduce postoperative pain compared with suture fixation [
22,
23,
24]. For example, E. Wassenaar et al., reported 3-month VAS scores of 4.5 ± 10.5 for absorbable sutures and 11.2 ± 21.2 for non-absorbable sutures. In contrast, patients treated with the UV-curable biomaterial in the present study reported lower early postoperative pain levels (VAS 2.6 ± 0.55 on postoperative day 1). Pain intensity decreased rapidly during follow-up, with the most pronounced reduction occurring within the first postoperative week (VAS 0.8 ± 0.84 on day 8), and complete resolution observed by 6 weeks.
Similarly, S.K. Jain and A. Vindal [
23] reported complete resolution of pain by day 7 following atraumatic fixation using tissue glue (GRF glue), a finding comparable to our results, although our day-8 VAS score (VAS 0.8) remained marginally above zero. In contrast, Amera Odobasic
et al. observed postoperative VAS scores ranging from 2.23 to 3.16 at day 7 with fibrin glue fixation, while cyanoacrylate-based adhesives yielded a mean VAS of 2.28 (SD = 1.79) at the same time point [
24]. Collectively, these data suggest that non-penetrating fixation methods, such as partial mesh self-stabilization, effectively reduce early postoperative pain and associated discomfort, thereby facilitating more rapid recovery. The reduction in pain may be attributable to the atraumatic nature of adhesive fixation, which avoids tissue penetration, nerve entrapment, and mechanical irritation commonly associated with sutures [
4,
25]. Thermographic assessment further supported this interpretation, demonstrating a gradual decrease in tissue temperature within the first 24 hours postoperatively, consistent with a physiological inflammatory response and uncomplicated wound healing.
Evaluation of chronic pain using the EuraHS QoL instrument confirmed progressive symptom resolution over time. Moreover, assessment of foreign body sensation using the Carolinas Comfort Scale revealed a substantial reduction in groin discomfort within 6 weeks postoperatively in the UV-sensitive and adhesive biomaterial group, with near-complete resolution by 24 months. Although improvements were observed over time in both groups, no clear between-group differences were observed in this pilot sample.
Quality-of-life assessment using the SF-36 questionnaire decreased at 6 weeks compared with preoperative values and then improved at 12 and 24 months, consistent with outcomes reported for other atraumatic mesh fixation methods [
26]. Importantly, no hernia recurrences were observed, and no clinically significant late complications were recorded during follow-up. While these findings are encouraging, the limited group size and duration of follow-up necessitate further investigation in larger, multicenter cohorts to establish long-term safety and comparative effectiveness relative to established fixation techniques.
Beyond clinical benefits, the novel biomaterial may offer economic advantages. Hybrid mesh self-stabilization was associated with a mean operative time reduction of 13.63% compared with conventional suture fixation. Reduced operative duration may decrease resource utilization and procedural costs, while potentially lowering infection risk through shorter wound exposure [
27]. Additionally, minimizing postoperative complications could further reduce long-term healthcare expenditures. Larger-scale studies are required to validate these economic implications.
Importantly, the absence of increased postoperative pain following polymer application supports the biocompatibility of the UV-curable adhesive and suggest minimal adverse tissue reaction in the human biological environment.
Conclusions
This study presents a novel hybrid mesh fixation technique for inguinal hernia repair using a UV-curable, biodegradable adhesive biomaterial to achieve partial mesh self-stabilization. In this pilot cohort, the introduction of atraumatic fixation method demonstrated a meaningful advancement in surgical practice without increasing perioperative or postoperative risks, demonstrated shorter operative time, and no hernia recurrences observed during 24-month follow-up.
The biomaterial demonstrated favorable biocompatibility, did not impair wound healing, and did not provoke adverse tissue reactions. By eliminating the need for multiple sutures and knot tying, this approach may reduce the risk of injury to delicate sensory and motor nerves in the vicinity of the spermatic cord, potentially lowering the incidence of chronic postoperative neuralgia.
The adhesive properties of the UV-activated biomaterial provide secure mesh fixation while allowing gradual biodegradation, thereby reducing long-term foreign body presence and supporting physiological tissue integration.
Although preliminary results are promising, further larger-scale, long-term studies are warranted to evaluate the degradation kinetics, safety profile, and broader clinical applicability of this technology across diverse patient populations and hernia subtypes.
Funding
Financial support from the Regional Operational Program Project RPZP.01.01.00-32-0002/20 of this medical research experiment is acknowledged.
Data availability
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
Declarations. Disclosures
M. El Fray is a co-inventor of patents that are licensed to PolTiss Sp. z o.o. A. Goszczyńska and G. Demirci have performed paid consulting for PolTiss Sp. z o.o., which is commercializing photocurable biomaterials. The other authors have no disclosures. All Authors declared no competing interests.
References
- Hollinsky, C; Kolbe, T; Walter, I; et al. Comparison of a New Self-Gripping Mesh with Other Fixation Methods for Laparoscopic Hernia Repair in a Rat Model. J Am Coll Surg. 2009, 208(6), 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Nikkolo, C; Lepner, U. Chronic pain after open inguinal hernia repair. In Postgrad Med; Taylor and Francis Inc., 2016; Volume 128, 1, pp. 69–75. [Google Scholar] [CrossRef]
- Nguyen, DK; Amid, PK; Chen, DC. Groin Pain After Inguinal Hernia Repair. In Adv Surg; Academic Press Inc., 2016; Volume 50, 1, pp. 203–220. [Google Scholar] [CrossRef]
- Kim-Fuchs, C; Angst, E; Vorburger, S; Helbling, C; Candinas, D; Schlumpf, R. Prospective randomized trial comparing sutured with sutureless mesh Wxation for Lichtenstein hernia repair: Long-term results. Hernia 2012, 16(1), 21–27. [Google Scholar] [CrossRef]
- Helbling, C; Schlumpf, R. Sutureless Lichtenstein: First results of a prospective randomised clinical trial. Hernia 2003, 7(2), 80–84. [Google Scholar] [CrossRef]
- Campanelli, G; Pettinari, D; Cavalli, M; Avesani, EC. A modified Lichtenstein hernia repair using fibrin glue. J Minim Access Surg. 2006, 2(3), 129–133. [Google Scholar] [CrossRef] [PubMed]
- Lovisetto, F; Zonta, S; Rota, E; et al. Use of human fibrin glue (Tissucol) versus staples for mesh fixation in laparoscopic transabdominal preperitoneal hernioplasty: A prospective, randomized study. Ann Surg. 2007, 245(2), 222–231. [Google Scholar] [CrossRef] [PubMed]
- Liu, H; Zheng, X; Gu, Y; Guo, S. A meta-analysis examining the use of fibrin glue mesh fixation versus suture mesh fixation in open inguinal hernia repair. Dig Surg. 2014, 31(6), 444–451. [Google Scholar] [CrossRef]
- Trisca, R; Oprea, V; Toma, M; et al. The Effectiveness of Cyanoacrylates versus Sutures for Mesh Fixation after Lichtenstein Repair (SCyMeLi STUDY) A Systematic Review and Meta-Analyze of Randomized Controlled Trials. Chirurgia (Romania) 2024, 119(1), 87–101. [Google Scholar] [CrossRef]
- Da̧browiecki, S; Pierściński, S; Szczȩsny, W. The Glubran 2 glue for mesh fixation in Lichtenstein’s hernia repair: A double-blind randomized study. Wideochirurgia I Inne Techniki Maloinwazyjne 2012, 7(2), 96–104. [Google Scholar] [CrossRef]
- Odobasic, A; Krdzalic, G; Hodzic, M; Hasukic, S; Sehanovic, A; Odobasic, A. The role of fibrin glue polypropylene mesh fixation in open inguinal hernia repair. Med Arch. 2014, 68(2), 90–93. [Google Scholar] [CrossRef]
- Ladurner, R; Drosse, I; Bürklein, D; et al. Cyanoacrylate glue for intra-abdominal mesh fixation of polypropylene-polyvinylidene fluoride meshes in a rabbit model. Journal of Surgical Research 2011, 167(2). [Google Scholar] [CrossRef]
- Haroon, M; Morarasu, S; Morarasu, BC; Al-Sahaf, O; Eguare, E. Assessment of feasibility and safety of cyanoacrylate glue versus absorbable tacks for inguinal hernia mesh fixation. A prospective comparative study. Wideochirurgia I Inne Techniki Maloinwazyjne 2023, 18(1), 90–98. [Google Scholar] [CrossRef] [PubMed]
- Skrobot, J; Zair, L; Ostrowski, M; El Fray, M. New injectable elastomeric biomaterials for hernia repair and their biocompatibility. Biomaterials 2016, 75, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Taboada, GM; Yang, K; Pereira, MJN; et al. Overcoming the translational barriers of tissue adhesives. Nat Rev Mater. Nature Research 2020, 5(4), 310–329. [Google Scholar] [CrossRef]
- Pradas, MM; Vicent, MJ. Polymers in Regenerative Medicine: Biomedical Applications from Nano- to Macro-Structures; 2014. [Google Scholar] [CrossRef]
- El Fray, M; Skrobot, J; Bolikal, D; Kohn, J. Synthesis and characterization of telechelic macromers containing fatty acid derivatives. React Funct Polym. 2012, 72, 781–790. [Google Scholar] [CrossRef]
- El Fray, M; Skrobot, J; Zair, L. Application of composition containing telechelic macromer and photoinitiator for producing implant for hernia repair. Published online January 5, 2016:US 9,228,043B2.
- Fortelny, RH; Petter-Puchner, AH; Redl, H; May, C; Pospischil, W; Glaser, K. Assessment of Pain and Quality of Life in Lichtenstein Hernia Repair Using a New Monofilament PTFE Mesh: Comparison of Suture vs. Fibrin-Sealant Mesh Fixation. Front Surg. 2014, 1(November), 1–8. [Google Scholar] [CrossRef]
- Jeroukhimov, I; Dykman, D; Hershkovitz, Y; et al. Chronic pain following totally extra-peritoneal inguinal hernia repair: a randomized clinical trial comparing glue and absorbable tackers. Langenbecks Arch Surg. 2023, 408(1), 1–5. [Google Scholar] [CrossRef]
- Demirci, G; Goszczyńska, A; Sokołowska, M; Żwir, M; Gorący, K; El Fray, M. Synthesis and Characterization of Photocurable Difunctional Monomers for Medical Applications. Polymers 2024, 16, 3584. [Google Scholar] [CrossRef]
- Mathes, T; Prediger, B; Walgenbach, M; Siegel, R. Mesh fixation techniques in primary ventral or incisional hernia repair. In Cochrane Database of Systematic Reviews; John Wiley and Sons Ltd, 2021; 5, p. 2021. [Google Scholar] [CrossRef]
- Jain, SK; Vindal, A. Gelatin-resorcin-formalin (GRF) tissue glue as a novel technique for fixing prosthetic mesh in open hernia repair. Hernia 2009, 13(3), 299–304. [Google Scholar] [CrossRef]
- Hoyuela, C; Juvany, M; Carvajal, F; et al. Randomized clinical trial of mesh fixation with glue or sutures for Lichtenstein hernia repair. British Journal of Surgery 2017, 104(6), 688–694. [Google Scholar] [CrossRef] [PubMed]
- Mitura, K; Garnysz, K; Wyrzykowska, D; Michałek, I. The change in groin pain perception after transabdominal preperitoneal inguinal hernia repair with glue fixation: a prospective trial of a single surgeon’s experience. Surg Endosc. 2018, 32(10), 4284–4289. [Google Scholar] [CrossRef]
- Fortelny, RH; Petter-Puchner, AH; May, C; et al. The impact of atraumatic fibrin sealant vs. staple mesh fixation in TAPP hernia repair on chronic pain and quality of life: Results of a randomized controlled study. Surg Endosc. 2012, 26(1), 249–254. [Google Scholar] [CrossRef] [PubMed]
- Tish, S; Krpata, D; AlMarzooqi, R; et al. Comparing 30-day outcomes between different mesh fixation techniques in minimally invasive inguinal hernia repair. Hernia 2020, 24(5), 961–968. [Google Scholar] [CrossRef] [PubMed]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).