Submitted:
23 January 2025
Posted:
23 January 2025
Read the latest preprint version here
Abstract
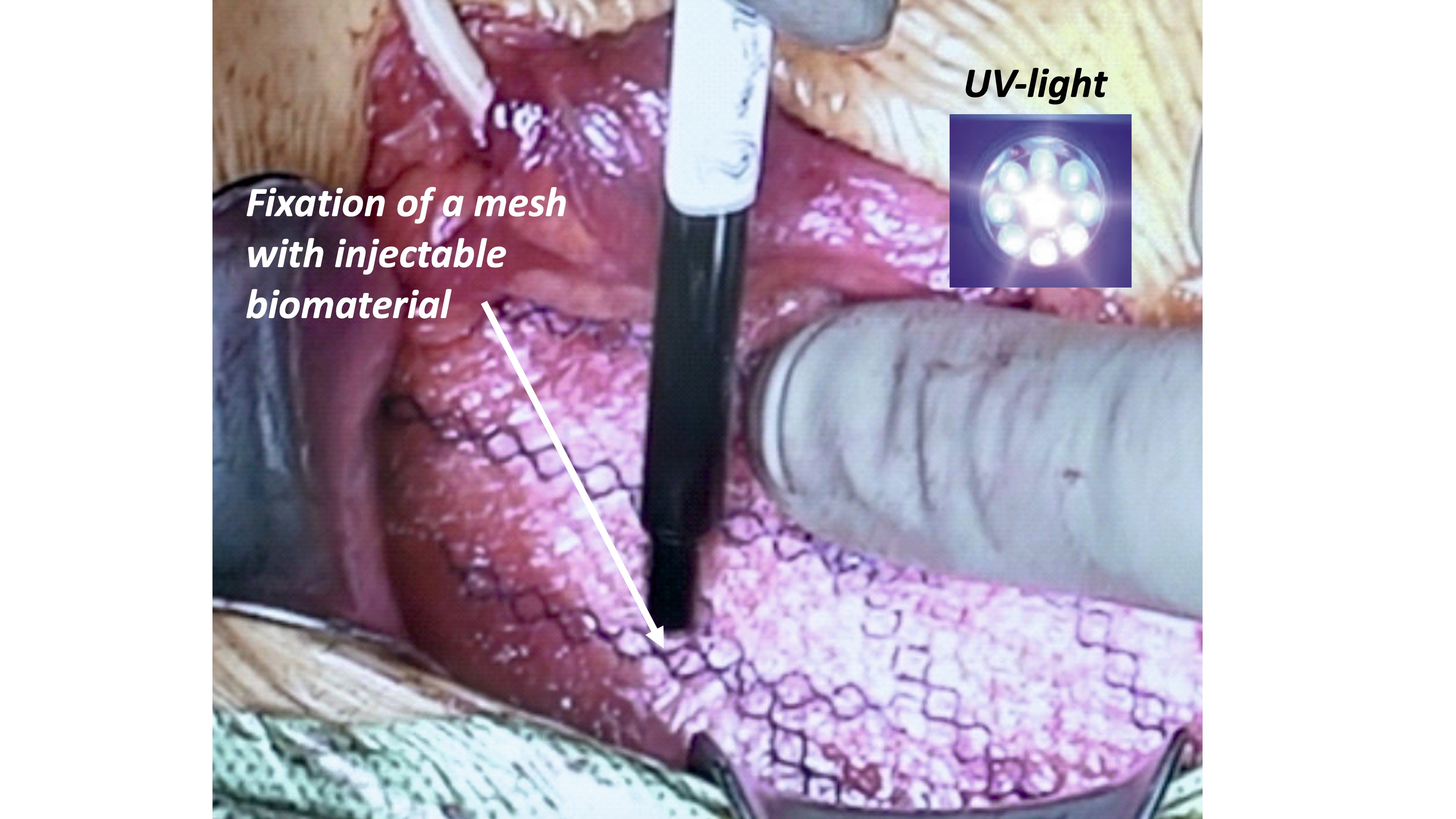
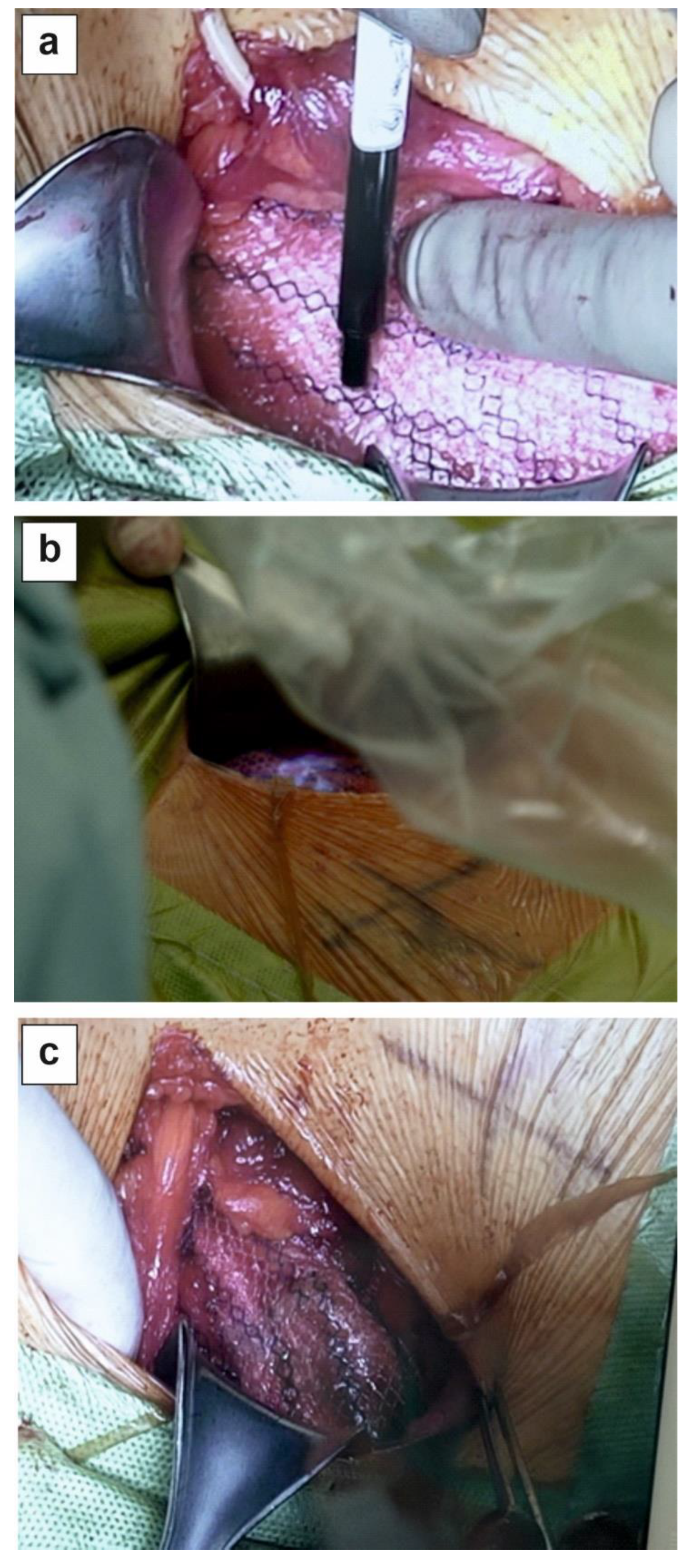
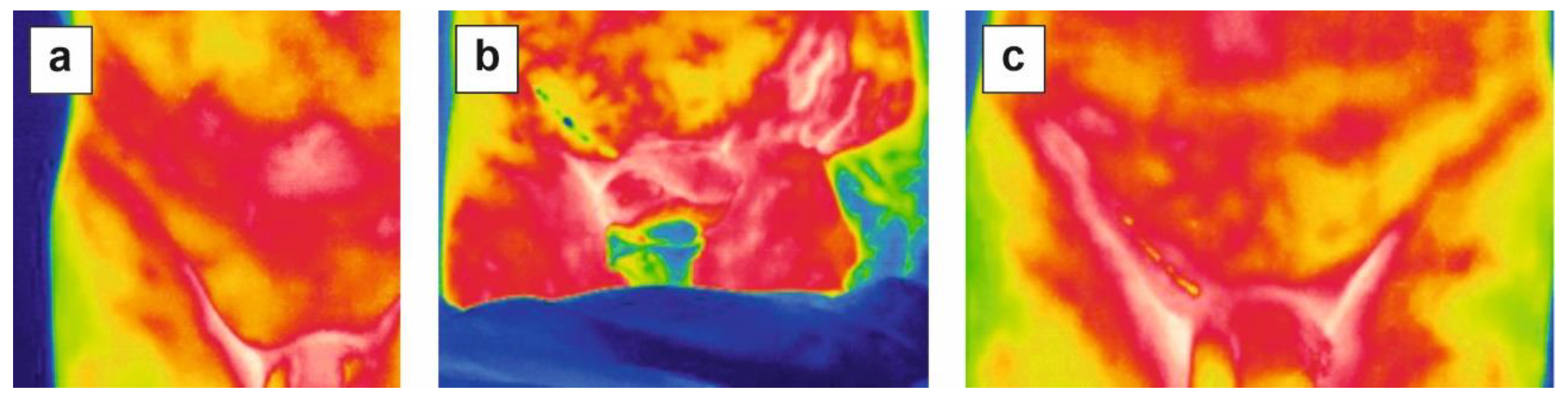
Surgical mesh is the standard for hernia repair, however, suture fixation can cause chronic pain and tissue irritation. Commonly used fibrin or cyanoacrylate glue have some limitations therefore, new UV-curable and biodegradable PhotoBioCure biomaterial was used for anastomosis of surgical mesh incisions in treating inguinal hernia. The mesh was fixed with PhotoBioCure biomaterial, which was UV-cured in 3 minutes. Follow-up lasted 24 months, with regular clinical supervision including ultrasonography, thermal imaging, and assessment of VAS, CCS, EuraHS QoL, and SF-36. The use of PhotoBioCure reduced surgical time compared to suture fixation. VAS pain scores decreased from 2.6 (± 0.55) on the first day after surgery to 0.8 (± 0.84) after 8 days, with complete pain resolution after 6 weeks. The CCS showed a gradual decline in foreign body sensation, from 54.08% on the first day post-surgery to 30.38% after 6 weeks. No recurrence or complications, like hematomas or infections, occurred over 24 months. Patients reported improved quality of life (based on SF-36 questionnaire) from 77.8 pre-surgery to 92.4 after 24 months. PhotoBioCure is an innovative biomaterial for efficient anastomosis of surgical mesh incisions in inguinal hernia repair, reducing procedure duration and surgical complexity without increasing the risk of post-operative complications.
Keywords:
Results
Discussion
Conclusion
Methods
PhotoBioCure Material
Patients
Inclusion Criteria
Exclusion Criteria
Postoperative Care
Ethical Approval
Statistical Method
Author Contributions
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hollinsky, C.; Kolbe, T.; Walter, I.; et al. Comparison of a New Self-Gripping Mesh with Other Fixation Methods for Laparoscopic Hernia Repair in a Rat Model. J. Am. Coll. Surg. 2009, 208, 1107–114. [Google Scholar] [CrossRef] [PubMed]
- Nikkolo, C.; Lepner, U. Chronic pain after open inguinal hernia repair. Vol. 128, Postgraduate Medicine. Taylor and Francis Inc.; 2016. p. 69–75.
- Nguyen, D.K.; Amid, P.K.; Chen, D.C. Groin Pain After Inguinal Hernia Repair. Vol. 50, Advances in Surgery. Academic Press Inc.; 2016. p. 203–220.
- Kim-Fuchs, C.; Angst, E.; Vorburger, S.; et al. Prospective randomized trial comparing sutured with sutureless mesh Wxation for Lichtenstein hernia repair: Long-term results. Hernia 2012, 16, 21–27. [Google Scholar] [CrossRef]
- Helbling, C.; Schlumpf, R. Sutureless Lichtenstein: First results of a prospective randomised clinical trial. Hernia 2003, 7, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Campanelli, G.; Pettinari, D.; Cavalli, M.; et al. A modified Lichtenstein hernia repair using fibrin glue. J. Minim. Access Surg. 2006, 2, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Lovisetto, F.; Zonta, S.; Rota, E.; et al. Use of human fibrin glue (Tissucol) versus staples for mesh fixation in laparoscopic transabdominal preperitoneal hernioplasty: A prospective, randomized study. Ann. Surg. 2007, 245, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Zheng, X.; Gu, Y.; et al. A meta-analysis examining the use of fibrin glue mesh fixation versus suture mesh fixation in open inguinal hernia repair. Dig. Surg. 2014, 31, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Trisca, R.; Oprea, V.; Toma, M.; et al. The Effectiveness of Cyanoacrylates versus Sutures for Mesh Fixation after Lichtenstein Repair (SCyMeLi STUDY) A Systematic Review and Meta-Analyze of Randomized Controlled Trials. Chirurgia 2024, 119, 87–101. [Google Scholar] [CrossRef]
- Dąbrowiecki, S.; Pierściński, S.; Szczęsny, W. The Glubran 2 glue for mesh fixation in Lichtenstein’s hernia repair: A double-blind randomized study. Wideochirurgia Tec. M. 2012, 7, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Odobasic, A.; Krdzalic, G.; Hodzic, M.; et al. The role of fibrin glue polypropylene mesh fixation in open inguinal hernia repair. Med. Arch. 2014, 68, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Ladurner, R.; Drosse, I.; Bürklein, D.; et al. Cyanoacrylate glue for intra-abdominal mesh fixation of polypropylene-polyvinylidene fluoride meshes in a rabbit model. J. Surg. Res. 2011, 167, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Haroon, M.; Morarasu, S.; Morarasu, B.C.; et al. Assessment of feasibility and safety of cyanoacrylate glue versus absorbable tacks for inguinal hernia mesh fixation. A prospective comparative study. Wideochirurgia Tec. M. 2023, 18, 90–98. [Google Scholar] [CrossRef]
- Skrobot, J.; Zair, L.; Ostrowski, M.; et al. New injectable elastomeric biomaterials for hernia repair and their biocompatibility. Biomaterials 2016, 75, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Taboada, G.M.; Yang, K.; Pereira, M.J.N.; et al. Overcoming the translational barriers of tissue adhesives. Nat. Rev. Mater. 2020, 5, 310–329. [Google Scholar] [CrossRef]
- Pradas, M.M.; Vicent, M.J. Polymers in Regenerative Medicine: Biomedical Applications from Nano- to Macro-Structures. 2014. p. 1–393. [CrossRef]
- El Fray, M.; Skrobot, J.; Bolikal, D.; et al. Synthesis and characterization of telechelic macromers containing fatty acid derivatives. React. Funct. Polym. 2012, 72, 781–790. [Google Scholar] [CrossRef]
- Fortelny, R.H.; Petter-Puchner, A.H.; Redl, H.; et al. Assessment of Pain and Quality of Life in Lichtenstein Hernia Repair Using a New Monofilament PTFE Mesh: Comparison of Suture vs. Fibrin-Sealant Mesh Fixation. Front. Surg. 2014, 1, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Jeroukhimov, I.; Dykman, D.; Hershkovitz, Y.; et al. Chronic pain following totally extra-peritoneal inguinal hernia repair: a randomized clinical trial comparing glue and absorbable tackers. Langenbecks Arch. Surg. 2023, 408, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Mathes, T.; Prediger, B.; Walgenbach, M.; et al. Mesh fixation techniques in primary ventral or incisional hernia repair. Vol. 2021, Cochrane Database of Systematic Reviews. John Wiley and Sons Ltd; 2021.
- Jain, S.K.; Vindal, A. Gelatin-resorcin-formalin (GRF) tissue glue as a novel technique for fixing prosthetic mesh in open hernia repair. Hernia 2009, 13, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Hoyuela, C.; Juvany, M.; Carvajal, F.; et al. Randomized clinical trial of mesh fixation with glue or sutures for Lichtenstein hernia repair. Br. J. Surg. 2017, 104, 688–694. [Google Scholar] [CrossRef]
- Mitura, K.; Garnysz, K.; Wyrzykowska, D.; et al. The change in groin pain perception after transabdominal preperitoneal inguinal hernia repair with glue fixation: a prospective trial of a single surgeon’s experience. Surg. Endosc. 2018, 32, 4284–4289. [Google Scholar] [CrossRef] [PubMed]
- Fortelny, R.H.; Petter-Puchner, A.H.; May, C.; et al. The impact of atraumatic fibrin sealant vs. staple mesh fixation in TAPP hernia repair on chronic pain and quality of life: Results of a randomized controlled study. Surg. Endosc. 2012, 26, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Tish, S.; Krpata, D.; AlMarzooqi, R.; et al. Comparing 30-day outcomes between different mesh fixation techniques in minimally invasive inguinal hernia repair. Hernia 2020, 24, 961–968. [Google Scholar] [CrossRef] [PubMed]
- Bellad, A.P.; Pratap, K.A. Effectiveness of tissue adhesive versus conventional sutures in the closure of inguinal hernia skin incisions: a prospective randomized controlled trial. Int. Surg. J. 2018, 5, 1797. [Google Scholar] [CrossRef]

| PhotoBioCure fixationa [min] (±SD) |
Suture fixationa [min] (±SD) |
|
|---|---|---|
| Average operating timeb | 52.00 (3.08) | 60.20 (3.70) |
| Postoperative hospital stay | 1 day | 1 day |
| Average time to resumption of normal activity | 6 weeks | 6 weeks |
| Duration of follow-up | 24 | 24 |
| Intraoperative complications (n) | 0 | 0 |
| Follow-up period | Fixation | Mean pain scorea (±SD) |
|---|---|---|
| 1st day | PhotoBioCure | 2.6 (0.55) |
| 8th day | PhotoBioCure | 0.8 (0.84) |
| 6th week | PhotoBioCure | 0 |
| 12th month | PhotoBioCure | 0 |
| 24th month | PhotoBioCure | 0 |
| PhotoBioCure fixationa,b | Suture fixationa,b | |
|---|---|---|
| Follow-up period | Mean value of severity [%](±SD) |
Mean value of severity [%](±SD) |
| 1st day | 54.08 (9.74) | 65.32 (4.26) |
| 8th days | 40.98 (9.54) | 49.45 (5.92) |
| 6th weeks | 30.38 (8.94) | 36.57 (2.21) |
| 12th months | 8.28 (1.71) | 8.97 (1.71) |
| 24th months | 1.38 (1.50) | 1.38 (0,96) |
| PhotoBioCure fixationa | Suture fixationa | |
|---|---|---|
| Domain | Mean value (±SD) | Mean value (±SD) |
| Pain | ||
| before surgery | 8.60 (2.19) | 8.60 (2.30) |
| 1st day | 22.60 (1.95) | 21.80 (2.17) |
| 8th days | 13.40 (1.14) | 12.40 (1.34) |
| 6th weeks | 3.40 (1.82) | 3.60 (1.14) |
| 12th months | 0.00 | 0.00 |
| 24th months | 0.00 | 0.00 |
| Restriction of activity | ||
| before surgery | 12.80 (4.66) | 11.80 (3.42) |
| 1st day | 35.00 (3.16) | 34.30 (3.35) |
| 8th days | 18.40 (3.65) | 17.40 (3.36) |
| 6th weeks | 6.60 (1.34) | 6.60 (2.41) |
| 12th months | 1.40 (1.14) | 1.00 (0.00) |
| 24th months | 1.20 (0.84) | 1.00 (0.00) |
| SF-36 | Mean valuea (±SD) |
|---|---|
| preoperatively | 77.8 (6.72)b |
| 6th weeks postoperatively | 71.6 (6.34)b |
| 12th months postoperatively | 88.2 (4.82)b |
| 24th months postoperatively | 92.4 (3.26)b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



