
Submitted:
11 December 2024
Posted:
12 December 2024
You are already at the latest version
Abstract
Background/Objectives: Interincisive midline deviation is frequent. Determining the cause (dental versus skeletal) is crucial for treatment planning. This study assessed the null hypothesis that neither clinical midline shift nor temporomandibular disorder (TMD)-affected side correlate with maxillary/mandibular asymmetry. Methods: Tomographic images were acquired using the i-CAT Imaging System; mandibular/maxillary measurements were obtained with the Planmeca Romexis software. This is an ancillary study of a clinical trial (NCT02144233) that included chronic pain (TMD diagnosis; DC/TMD criteria), fully dentate and stable normo-occlusion participants. Results: Thirty-eight CBCT scans were analyzed: 35 (92.1%) females, 3 (7.9%) males. Mean age 34.6 (11.9) years old. Sixteen (42.1%) midline deviations to the right and 13 (34.2%) to the left. In the study population the right side was more developed: hemimandible length 119.4 (5.7) mm versus 118.6 (5.3) mm, right and left sides, respectively (95% CI 0.21 to 1.51), p=0.01. Conclusions: Neither midline shift side nor affected side predicted a less developed hemimandible.
Keywords:
dental midline shift
; dental occlusion
; asymmetry
; jaw asymmetry
; jaw growth
; temporomandibular disorders (TMD)
1. Introduction
Dental midline shift (DMS) is a common finding in dentistry [1]. From the perspective of dental occlusion, DMS requires an assessment beyond the central incisors [2]. It may reflect a more distal position on the side towards which the lower midline deviates than on the opposite side [3]; this may imply an alteration in the nature of certain contacts that could modify the biodynamics and/or function of the stomatognathic system (SS) [4,5]. Centric occlusion should be explored to determine whether the deviation is organic or deflective in nature corresponding to a functional deviation during jaw closure [6].
Once the deviation is clinically evident (Figure 1), the question is whether it is the upper arch (i.e. maxillary bone) that deviates from the mid-sagittal plane, or whether the deviation is due to the mandibular structures, or both. Midline asymmetries demand specific consideration in rehabilitation (orthodontic or prosthetic procedures) during diagnosis and treatment planning, since they represent one of the most challenging, frequent, and enduring issues that dentists deal with [7,8].
The asymmetry of the mandible is the condition that exists when the right and left sides of the mandible are not mirror images of each other [5]. Lower facial asymmetries are a marker for environmental stress and cerebral lateralization during early development [9], and may be the result of asymmetry of bones [10], teeth, or soft tissues [10,11]. Factors such as tooth loosening, sleep position, or altered chewing function can contribute to facial asymmetry [12,13]. In particular, it has been shown that the volume of the chin becomes larger on the side opposite to the twins’ habitual chewing side [13].
Knowledge of the possible cause is important and to reach the correct diagnosis, the dentofacial structures must be properly examined1. If the cause is solely dental, treatment can be approached from an occlusal perspective. However, if the cause is basal bone asymmetry, treatment may vary [14,15]; mandibular development takes place during growth, but is virtually non-existent during adulthood [16]. The correction or prevention of bony asymmetry could take place during development, but not during adulthood [16,17]. It seems logical that it would be of interest to determine whether the shift of the midline is exclusively dental in origin (involving only the alveolar bone) or whether it is a consequence of asymmetry of the basal bones of the SS.
The most accurate method that can be used to determine the size of the bony structures is through cone beam computer tomography (CBCT) [18]. This procedure is not absolutely risk-free, meaning it should not be performed on healthy individuals [19]. The indication for CBCT for other reasons, such as certain types of TMDs, allows for measurements of the SS, specifically to assess the midline shift.
Interincisive midline is a clinical sign that carries implications in various diagnoses (orthodontic and rehabilitative, as well as in pediatric dentistry). In the case of TMDs, previous literature has reported a tendency to preferential chewing on the affected side [20,21,22]. This phenomenon could lead to a greater development of the non-chewing side bone size. Therefore, it is logical to assume that mandibular asymmetry could be a factor associated with TMD-affected side. Previous studies on mandibular asymmetry focused mainly on the asymmetry of temporomandibular joints, but not on mandibular growth [23].
We hypothesize that when midline shift is present, the hemimandible on the side towards which the mandibular midline deviates is shorter than the hemimandible on the opposite side.
2. Materials and Methods
2.1. Ethics Statement
This study was approved by the Regional Ethics Committee (CAEI, approval number 2009/017; updated on November 29, 2013). Informed consent was obtained from all participants, and the data released here are consistent with the consent obtained.
This study is an analysis of diagnostic aspects of TMDs that were pre-specified in the MAP Protocol: Restoring physiological jaw closure and Masticatory function as treatment for chronic facial Pain: a randomized clinical trial (ClinicalTrials.gov NCT02144233).
2.2. Participants
Participants in the MAP trial were eligible for this study. A prior diagnosis of chronic TMD, according to DC/TMD criteria [24], was required. The tomographic images were obtained using the 17-19 i-CAT® Imaging System (Imaging Sciences International Inc., Pennsylvania, USA). The criterion for CBCTs exploration in the MAP study was determined by chronic TMDs diagnostic needs. The following criteria were established for the selection and collection of data:
2.2.1. Inclusion Criteria
Persons with chronic TMDs refractory to conservative treatment, referred to a tertiary health care center, aged between 18 and 65 years. Participants should experience chronic pain (minimum 6 months duration) diagnosed as TMD, with a self-reported intensity of moderated to severe (≥4 to ≤9) scores on a visual analogue scale graded from 0 to 10, where 0 = no pain, 10 = worst possible pain [25,26].
The diagnosis of TMD was established according to the DC/TMD criteria [24]. Pain was presumed to be relevant since the patient demanded treatment of any kind. An examination of the dental status and occlusion of the participants was also performed. To avoid confounding factors, only fully dentate subjects (but third molars) or participants with fixed partial dentures allowing comfortable chewing with clinically normal or near-normal occlusion (stable Angle class I) were selected. Midline deviation was qualitatively assessed by two experienced trialists (disagreements solved by discussion) using frontal digital telephotographs where madibular interincisive midline shift (left or right) was registered using the maxillary midline as a reference. Condylar paths were assessed by conventional axiography.
2.2.2. Exclusion Criteria
These criteria included oncological pathology, traumatic or neurological injuries and congenital deformity. Participants with severe psychological disturbances (psychosis, major depression), cognitive impairment, dental health professionals, substance abuse, in litigation or claiming disability/retirement compensation for chronic pain, previous orthodontic treatment, severe periodontal disease (grade 3 mobility) were excluded as participants. Patients with systemic diseases that could affect the masticatory system were also excluded.
2.3. Data Collection/CBCT Acquisition
CBCT scans of the maxillofacial region were obtained using the 17-19 i-CAT® Imaging System (Imaging Sciences International Inc., Pennsylvania, USA) under the following parameters: 120 kVp, 0.4 mm3 voxel size, 8.9 seconds scan time, and 16.5 cm x 13.5 cm field of view. This scanning device allows patients to sit upright during the procedure and their head position, such as the Frankfort horizontal (FH) plane, was parallel to the floor. Throughout the scanning procedure, patients were instructed to maintain light contact of their teeth with the bite-peg, and the facial soft tissues at rest. CBCT scans were stored in Digital Imaging and Communications in Medicine (.dcm) format.
2.4. Morphometric Analysis
It is important to note that conventional CBCT software has some limitations. It is not possible to directly measure certain variables such as lengths in oblique directions, e.g. the length of the hemimandible. Therefore, an image processing software that would allow this measurement was employed. CBCT images were loaded into Planmeca Romexis® dental software; the reference points and anatomical planes detailed below were identified and measured. Each measurement was independently performed by two specifically trained examiners, at different times. Firstly, all CBCT images were oriented according to two planes: the Frankfort Horizontal Plane (FP) and the Mid-Sagittal Plane (MSP). This phase allowed the standardization of the method and was undertaken before any measurement.
The evaluation was completed independently and randomly in a well-lit space. The landmarks highlighted in Table 1 and Figure 2 were used and the following measurements were performed on each tomographic image scan [27,28,29,30,31,32,33]:
- Condylar process height: from point Cs to a horizontal line (parallel to FP) drawn at point SN. Measurement made on the right and left sides;
- Coronoid process height: From point Cp to a horizontal line (parallel to FP) drawn at point SN. Measurement taken on the right and left sides;
- Articular eminence (AE) height: From point GF to a horizontal line (parallel to FP) drawn at point AE. Measurement taken on the right and left sides;
- AE inclination: Angle formed between a line parallel to FP, drawn at point AE, with a line drawn between points AE and GF [34]. Measurement made on the right and left sides;
- Mandibular ramus height: From point Cs to MB1. Measurement made on the right and left sides;
- Mandibular body length: From point Rp to Pg. Measurement taken on the right and left sides;
- Hemimandible length: From point Cpt to point Pg. Measurement taken on the right and left sides (Figure 3);
- Right hemimaxilla width: From point P16 to MSP. The measurement is made only on the right side by drawing a horizontal line (parallel to the FP) between the two references;
- Left hemimaxilla width: From point P26 to MSP. The measurement is made only on the left side by drawing a horizontal line (parallel to the FP) between the two references;
- Distance Cl-MSP: From point Cl to MSP. The measurement is made by drawing a horizontal line (parallel to the FP) between the two references and must be taken on the right and left sides.
2.5. Statistical Analysis
Continuous variables were described through mean and standard deviation (SD). Dichotomic variables were described through frequency and percentage. The normality of the distribution was assessed with Shapiro-Wilk tests, while the homogeneity of variances was verified by Levene’s test. Normally distributed continuous variables were compared using a two-tailed paired Student’s t-test. Similarly, if the variables did not follow a normal distribution, paired non-parametric tests were applied. One-sample proportion test was carried out to assess possible differences in group proportions. Possible relations between variables were assessed through Pearson’s chi-square test. The reproducibility of the measurements was assessed using the intraclass correlation test (ICC). Statistical analysis was executed using SPSS (Statistical Package for the Social Sciences, IBM, v.29.0.2) [35]. The alpha level was set at p=0.05.
3. Results
Forty-one CBCT scans were evaluated. Of this sample, it was only possible to perform the intended measurements in 38 as the CBCT images obtained in 3 of the cases had artifacts that prevented the identification of key reference points and therefore did not allow the standardization of the measurement method. Two calibrated researchers performed independently all measurements, yielding an ICC ranged from 0.87 to 0.95.
The sample consisted of 3 (7.9%) males and 35 (92.1%) females. Mean age 34.6 (11.9) years. Regarding the location of the symptoms, 26/38 (68.4%) persons indicated that it was unilateral and 12/38 (31.6%) showed symptoms on both sides. The assessment of the midline deviation revealed that 42.1% (n=16) had a deviation to the right, 34.2% (n=13) to the left, and 21.1% (n=8) had no clinical midline shift. One person (2.6%) could not be assessed (participant wearing an upper fixed partial denture which did not allow the assessment of a midline between natural incisors). Table 2 shows the main biological characteristics of the subjects.
Overall (n=38), statistically significant asymmetry was observed in the study group. The magnitudes of these differences appear relatively small, so that they do not a priori show great clinical significance. One of the main study outcomes was the hemimandible length. The hemimandible was shorter on the left side (intraindividual paired differences 0.9 (95% CI 0.2 to 1.5), p=0.01). Other outcomes relative to the mandible also indicated a smaller size on the left side. This was not the case for the maxillary dimensions, which showed no evidence of differences between the right and left sides. Axiographic recordings showed that mean condylar path angles were higher on the left side than on the left one (mean difference -3.1(6.3 to 0.0), p=0.05) (Table 3).
The side toward the midline shift was deviated (16 persons to the right and 13 to the left) did not predict the shorter hemimandible nor the asymmetry of other bone structures. However, coronoid apophysis was larger on the side opposite to the side where the midline shift was deviated (Table 4).
Table 5 shows mean values of bone sizes on the affected versus unaffected side. There was no evidence of differences between the affected and unaffected side in the hemimandible length (27.07 (1.36) mm on the affected side and 26.96 (1.47) mm on the nonaffected side; mean difference 0.11; 95% CI -0.14 to 0.36; p=0.36) (n=34). The study revealed a tendency towards a greater mandibular ramus height on the unaffected side (p=0.06). Also, the condylar path angle was higher on the affected side in this group with unilateral symptoms (n=25).
4. Discussion
The mandible was asymmetric in this study population, with the left hemimandible being shorter than the right. However, unexpectedly, the side toward the jaw midline was deviated did not predict a shorter hemimandible.
The fact that the side with interincisive midline deviation does not coincide with the less developed side of the jaw seems to suggest that this purely dental relationship is due to the biomechanics of the SS. These biomechanics could explain an adaptive dental repositioning to the interarch occlusal forces, which could not only correspond to the developmental period but also to later periods. Since humans are sensitive to disruptions in a bilaterally symmetrical anatomy, like the face, symmetry plays a significant part in how we perceive beauty [36] but also in how jaw biodynamics and functional dental guidance occur [4]. There are currently a number of studies that have determined thresholds for midline shift perception [37]. For instance, a movement in the midline of at least 2 mm was observed by laypeople [38,39,40]. A different study found that a dental midline deviation of 2.9 (1.1) mm was no longer regarded as acceptable [36]. More recently, more precise discrepancy localization has been achieved using more advanced imaging techniques such as CBCT [18] and three-dimensional photography [13]. To ascertain the origin, degree, and location of asymmetry, a thorough examination of the patient’s numerous diagnostic records is required [1]. With their demonstrated accuracy and precision, more recent developments in three-dimensional photography have become a useful tool for the diagnosis and treatment planning of dentofacial asymmetries [41,42]. Decisions on dentofacial deformity intervention, however, are based on the patient’s awareness of the aesthetic issue, the severity of the occlusal deformity, and any associated vertical or sagittal jaw imbalance [43].
There were no differences between the size of the structures in both sides when the side with midline shift was considered. Hence, midline shift does not predict bony asymmetry. Since the jaw midline sometimes deviates towards the longer hemimandible, it is presumable to assume that this may have occurred as a function of biodynamic and masticatory function during the adult period. We therefore speculate that this type of alteration would be easier to correct, as it is only dependent on the alveolar process, which is more sensitive to orthodontic management.
There was no evidence for a relationship between the TMD affected side and the asymmetry of hard tissues (Table 5). A tendency was observed for a larger coronoid apophysis on the side opposite the side where the jaw midline shift was deviated (Table 4). Coronoid apophysis provides insertion to the temporal muscle. The temporalis muscle is a positioner of the jaw. This finding seems to suggest the influence of asymmetrical muscle coactivation of the temporalis muscles. There is a tendency to use the left side more frequently in this study population. The masseter muscle on the chewing side is mainly activated; this activity requires torque-like coactivation of the contralateral musculature, mainly the temporalis muscle, to position and stabilize the jaw, which may explain the greater development of the coronoids.
Flanze et al. [37], in 2023, asserted that dental midline shifts should be addressed as soon as feasible to prevent them from impairing face growth. The authors stated that these shifts are frequently functional in nature because of a lateral forced bite of the mandible and the altered chewing function [12]. This is in agreement with Heikkinen et al. [13] who have conducted a study in twins and observed that chin volume is increased on the non-habitual chewing side. These authors concluded that functional factors are more significant than genetic factors.
One of the strengths of our study is that the clinical condition of the participants was extremely homogeneous: complete natural dentition, normal or near-normal occlusion. Furthermore, the method used to perform the measurements had already been used in previous research [27,28,29,30,31,32,33] and was therefore proven to be reliable and standardized. Independent observer measurements in this study showed an ICC ranged from 0.87 to 0.95, confirming the high reliability of the measurement method.
This study has limitations. It has a low number of male subjects, which is common in people with TMDs referred to tertiary care services. Healthy adults or children were not assessed for ethical reasons. Therefore, these results should not be extrapolated to cohorts with different characteristics. Furthermore, the original study was designed to determine changes, regarding pain levels and mouth opening limitation, in participants who underwent real treatment versus placebo, but not directly to assess the asymmetry of bone structures. However, it provides access to information that is not accessible from healthy people. It can only be obtained when there is an indication for CBCT, which is a per se invasive procedure, as occurs in the present study.
This study also has some methodological concerns. The aim was to assess a clinical sign trichotomically (i.e. registering the mandible’s interincisive midline shift from the upper one, whether to the right or to the left, as a right, left or no deviation), as it is a sign easily observable on dental inspection. Nevertheless, although the interincisive midline is deviated, it should not be interpreted or assumed a priori as retrognathia on the side towards which the mandibular incisors are deviated. This could also be explained as a possible displacement of the teeth, but not necessarily of the basal bone.
This study does not permit determining the cause/s of SS asymmetry. Further longitudinal research, with a larger sample size, could elucidate the cause as a means to treat/prevent asymmetries of the SS.
5. Conclusions
The side to which the jaw interincisive midline deviates did not predict less development of the hemimandible. Unexpectedly, this study shows evidence for the asymmetry of mandible length: the mandible was larger on the right side than on the left side; we speculate that this asymmetry could be attributed to the hemispheric dominance. Future studies may serve to identify the possible cause of this asymmetry.
Author Contributions
Conceptualization, U.S.P., M.J.M. and J.L.C.; methodology, U.S.P and L.P.S..; investigation, L.P.S. and A.L.S.; data curation, L.P.S, U.S.P and U.S.M.; writing—original draft preparation, L.P.S. and A.L.S; writing—review and editing, U.S.P., U.S.M., A.R.F., A.G.M. and P.V.C.; supervision, U.S.P.; funding acquisition, U.S.P, M.J.M. and J.L.C. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
The study was approved by the Autonomic Research Ethics Committee of Galicia: CAEI approval number 2009/017; updated on November 29, 2013. Informed consent was obtained during each screening visit to perform the diagnostic procedures. All methods were performed in accordance with the Declaration of Helsinki. Information presented here is consistent with the consent obtained.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request. Correspondence and requests for materials should be addressed to U.S.P.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Agrawal, M.; Agrawal, J.; Nanjannawar, L.; Fulari, S.; Kagi, V. Dentofacial Asymmetries: Challenging Diagnosis and Treatment Planning. J Int Oral Health. 2015, 7, 128–131. [Google Scholar] [PubMed]
- Silinevica, S.; Lokmane, K.; Vuollo, V.; Jakobsone, G.; Pirttiniemi, P. The association between dental and facial symmetry in adolescents. American Journal of Orthodontics and Dentofacial Orthopedics 2023, 164, 340–350. [Google Scholar] [CrossRef]
- Koseoglu, M.; Bayindir, F. Effect of variations in facial flow curves on the perceptions of smile esthetics by laypeople. The Journal of Prosthetic Dentistry 2023, 129, 486–494. [Google Scholar] [CrossRef]
- Sagl, B.; Schmid-Schwap, M.; Piehslinger, E.; Kundi, K.; Stavness, I. A Dynamic Jaw Model With a Finite-Element Temporomandibular Joint. Front Physiol 2019, 13, 1156. [Google Scholar] [CrossRef]
- The Glossary of Prosthodontic Terms, Tenth edition. [No authors listed]. Journal of Prosthetic Dentistry 2023, 130, e7–e126. [Google Scholar]
- Goldstein, G. Centric relation: A needed reference position. Journal of prosthodontics 2023, 32, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Sharma, N.; Patni, P.; Jain, D. Association of midline discrepancy with tempromandibular joint disorder. A systematic review. Clujul Med 2018, 91, 151–156. [Google Scholar] [CrossRef]
- Ciavarella, D.; Maci, M.; Guida, L.; Cazzolla, A.P.; Muzio, E.L.; Tepedino, M. Correction of Midline Deviation and Unilateral Crossbite Treated with Fixed Appliance. Case Rep Dent 2023, 2023, 5620345. [Google Scholar] [CrossRef]
- Hujoel, P.; Masterson, E.; Bollen, A.-M. Lower face asymmetry as a marker for developmental instability. Am J Hum Biol 2017, 29. [Google Scholar] [CrossRef]
- Li, J.; Wu, S.; Mei, L.; Wen, J.; Marra, J.; Lei, L.; Li, H. Facial asymmetry of the hard and soft tissues in skeletal Class I, II, and III patients. Sci Rep 2024, 14, 4966. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Chun, Y.; Bae, H.; Lee, J.; Kim, H. Comparison of ultrasonography-based masticatory muscle thickness between temporomandibular disorders bruxers and temporomandibular disorders non-bruxers. Sci Rep 2024, 14, 6923. [Google Scholar] [CrossRef] [PubMed]
- Santana-Mora, U.; López-Cedrún, J.; Suárez-Quintanilla, J.; Varela-Centelles, P.; Mora, M.; Silva, J.; Figueiredo-Costa, F.; Santana-Penín, U. Asymmetry of dental or joint anatomy or impaired chewing function contribute to chronic temporomandibular joint disorders. Annals of Anatomy 2021, 238, 151793. [Google Scholar] [CrossRef] [PubMed]
- Heikkinen, E.; Vuollo, V.; Harila, V.; Sidlauskas, A.; Heikkinen, T. Facial asymmetry and chewing sides in twins. Acta Odontologica Scandinavica 2022, 80, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, H. Efficient surgical management of mandibular asymmetry. J Oral Maxillofac Surg 2011, 69, 645–654. [Google Scholar] [CrossRef]
- Chen, Y.; Liao, Y.; Chen, Y.; Chen, Y. Surgical-orthodontic treatment for class II asymmetry: outcome and influencing factors. Sci Rep 2019, 9, 17956. [Google Scholar] [CrossRef]
- Enlow, D.; Hans, M. Essentials of facial growth; W. B. Saunders: Philadelphia, 1996. [Google Scholar]
- Wen-Ching Ko, E.; Huang, C.; Lin, C.; Chen, Y. Orthodontic Perspective for Face Asymmetry Correction. Symmetry 2022, 14, 1822. [Google Scholar] [CrossRef]
- Venkatesh, E.; Elluru, S. Cone beam computed tomography: basics and applications in dentistry. J Istanb Univ Fac Dent 2017, 51, S102–S121. [Google Scholar] [CrossRef]
- Lindfors, N.; Ekestubbe, A.; Frisk, F.; Lund, H. Is cone-beam computed tomography (CBCT) an alternative to plain radiography in assessments of dental disease? A study of method agreement in a medically compromised patient population. Clinical Oral Investigations 2024, 28, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Santana-Mora, U.; López-Cedrún, J.; Mora, M.; Otero, X.; Santana-Penín, U. Temporomandibular Disorders: The Habitual Chewing Side Syndrome. PLoS ONE 2013, 8, e59980. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Huang, D.; Zhai, X.; Li, H.; Hu, M.; Liu, H.; Jiang, H. Occlusal analysis of patients with chewing side preference and symptoms of temporomandibular disorders. Hua Xi Kou Qiang Yi Xue Za Zhi 2022, 40, 457–467. [Google Scholar] [PubMed]
- Zheng, H.; Liu, Z.; Wang, H. Research progress in effect of chewing-side preference on temporomandibular joint and its relationship with temporo-mandibular disorders. Journal of Zhejiang University (Medical Sciences) 2023, 52, 386–397. [Google Scholar] [CrossRef]
- Sritara, S.; Matsumoto, Y.; Lou, Y.; Qi, J.; Aida, J.; Ono, T. Association between the Temporomandibular Joint Morphology and Chewing Pattern. Diagnostics (Basel) 2023, 13, 2177. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Hohenschurz-Schmidt, D.; Cherkin, D.; Rice, A.; Dworkin, R.; Turk, D.; McDermott, M.; Bair, M.; DeBar, L.; Edwards, R.; Farrar, J.; et al. Research objectives and general considerations for pragmatic clinical trials of pain treatments: IMMPACT statement. Pain 2023, 164, 1457–1472. [Google Scholar] [CrossRef] [PubMed]
- Price, D.; McGrath, P.; Rafii, A.; Buckingham, B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain 1983, 17, 45–56. [Google Scholar] [CrossRef]
- Tun Oo, L.; Miyamoto, J.; Takada, J.; Cheng, S.; Yoshizawa, H.; Moriyama, K. Three-dimensional characteristics of temporomandibular joint morphology and condylar movement in patients with mandibular asymmetry. Prog Orthod 2022, 23, 50. [Google Scholar] [CrossRef] [PubMed]
- Kusnoto, B.; Kaur, P.; Salem, A.; Zhang, Z.; Galang-Boquiren, M.; Viana, G.; Evans, C.; Manasse, R.; Monahan, R.; BeGole, E.; et al. Implementation of ultra-low-dose CBCT for routine 2D orthodontic diagnostic radiographs: cephalometric landmark identification and image quality assessment. Semin Orthod 2015, 21, 233e247. [Google Scholar] [CrossRef]
- Ayyildiz, E.; Orhan, M.; Bahsi, I.; Yalcin, E. Morphometric evaluation of the temporomandibular joint on cone-beam computed tomography. Surg Radiol Anat 2021, 43, 975–996. [Google Scholar] [CrossRef] [PubMed]
- Macri, M.; Festa, F. Three-dimensional evaluation using CBCT of the mandibular asymmetry and the compensation mechanism in a growing patient: A case report. Front Public Health 2022, 10, 921413. [Google Scholar] [CrossRef] [PubMed]
- Schlicher, W.; Nielsen, I.; Huang, J.; Maki, K.; Hatcher, D.; Miller, A. Consistency and precision of landmark identification in three-dimensional cone beam computed tomography scans. Eur J Orthod 2012, 34, 263–275. [Google Scholar] [CrossRef]
- Lin, M.; Xu, Y.; Wu, H.; Zhang, H.; Wang, S.; Qi, K. Comparative cone-beam computed tomography evaluation of temporomandibular joint position and morphology in female patients with skeletal class II malocclusion. J Int Med Res 2020, 48, 300060519892388. [Google Scholar] [CrossRef] [PubMed]
- Chae, J.; Park, J.; Tai, K.; Mizutani, K.; Uzuka, S.; Miyashita, W.; Seo, H. Evaluation of condyle-fossa relationships in adolescents with various skeletal patterns using cone-beam computed tomography. Angle Orthod 2020, 90, 224–232. [Google Scholar] [CrossRef]
- Katsavrias, E. Changes in articular eminence inclination during the craniofacial growth period. Angle Orthod 2002, 72, 258–264. [Google Scholar]
- Corp. , I. IBM SPSS Statistics for macOS, 29.0; IBM Corp.: Armonk, NY, 2022. [Google Scholar]
- Williams, R.; Rinchuse, D.; Zullo, T. Perceptions of midline deviations among different facial types. Am J Orthod Dentofacial Orthop 2014, 145, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Flanze, K.; Riemekasten, S.; Hirsch, C.; Koehne, T. Perception of facial and dental asymmetries and their impact on oral health-related quality of life in children and adolescents. J Orofac Orthop 2023. [Google Scholar] [CrossRef]
- Cardash, H.; Ormanier, Z.; Laufer, B.-Z. Observable deviation of the facial and anterior tooth midlines. J Prosthet Dent 2003, 89, 282–285. [Google Scholar] [CrossRef]
- Shyagali, T.; Chandralekha, B.; Bhayya, D.; Kumar, S.; Balasubramanyam, G. Are ratings of dentofacial attractiveness influenced by dentofacial midline discrepancies? Aust Orthod J 2008, 24, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Zhang, I.; Xiao, L.; Li, J.; Peng, Y.; Zhao, Z. Young people’s esthetic perception of dental midline deviation. Angle Orthod 2010, 80, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, S.; Naidoo, S.; Govier, D.; Martin, R.; Kane, A.; Marazita, M. Anthropometric precision and accuracy of digital three-dimensional photogrammetry: Comparing the Genex and 3 dMD imaging systems with one another and with direct anthropometry. J Craniofacc Surg 2010, 21, 763–767. [Google Scholar] [CrossRef]
- Lübbers, H.; Medinger, L.; Kruse, A.; Grätz, K.; Matthews, F. Precision and accuracy of the 3dMD photogrammetric system in craniomaxillofacial application. J Craniofac Surg 2010, 21, 763–767. [Google Scholar] [CrossRef] [PubMed]
- Ko, E.; Huang, C.; Chen, Y. Characteristics and corrective outcome of face asymmetry by orthognathic surgery. J Oral Maxillofac Surg 2009, 67, 2201–2209. [Google Scholar] [CrossRef]
Figure 1.
One typical jaw midline shift (toward the left side). A larger right hemimandible could be expected.
Figure 1.
One typical jaw midline shift (toward the left side). A larger right hemimandible could be expected.
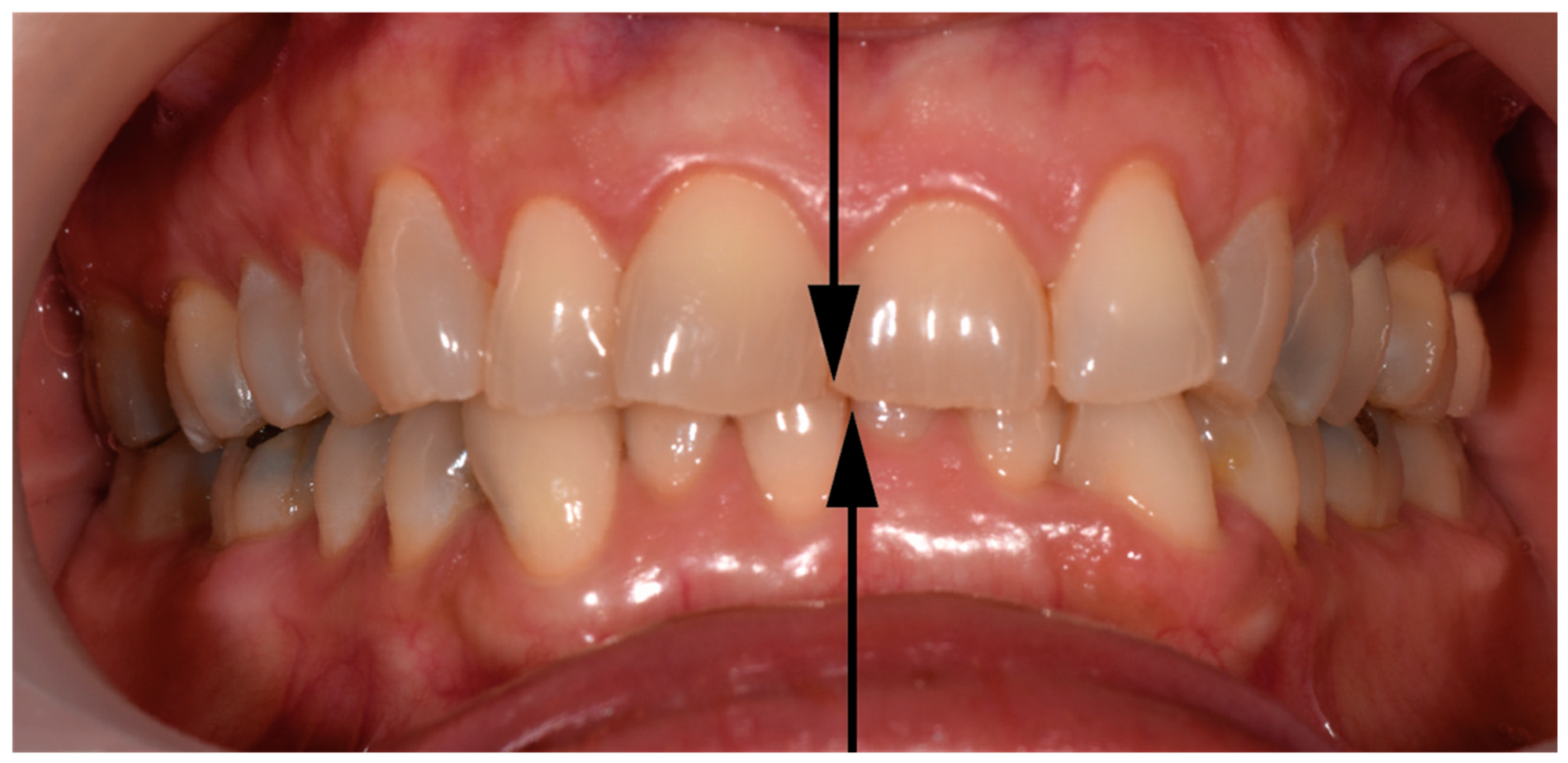
Figure 2.
Hard tissue landmarks: (a) Jaw landmarks; (b) Temporomandibular joint with reference points.
Figure 2.
Hard tissue landmarks: (a) Jaw landmarks; (b) Temporomandibular joint with reference points.
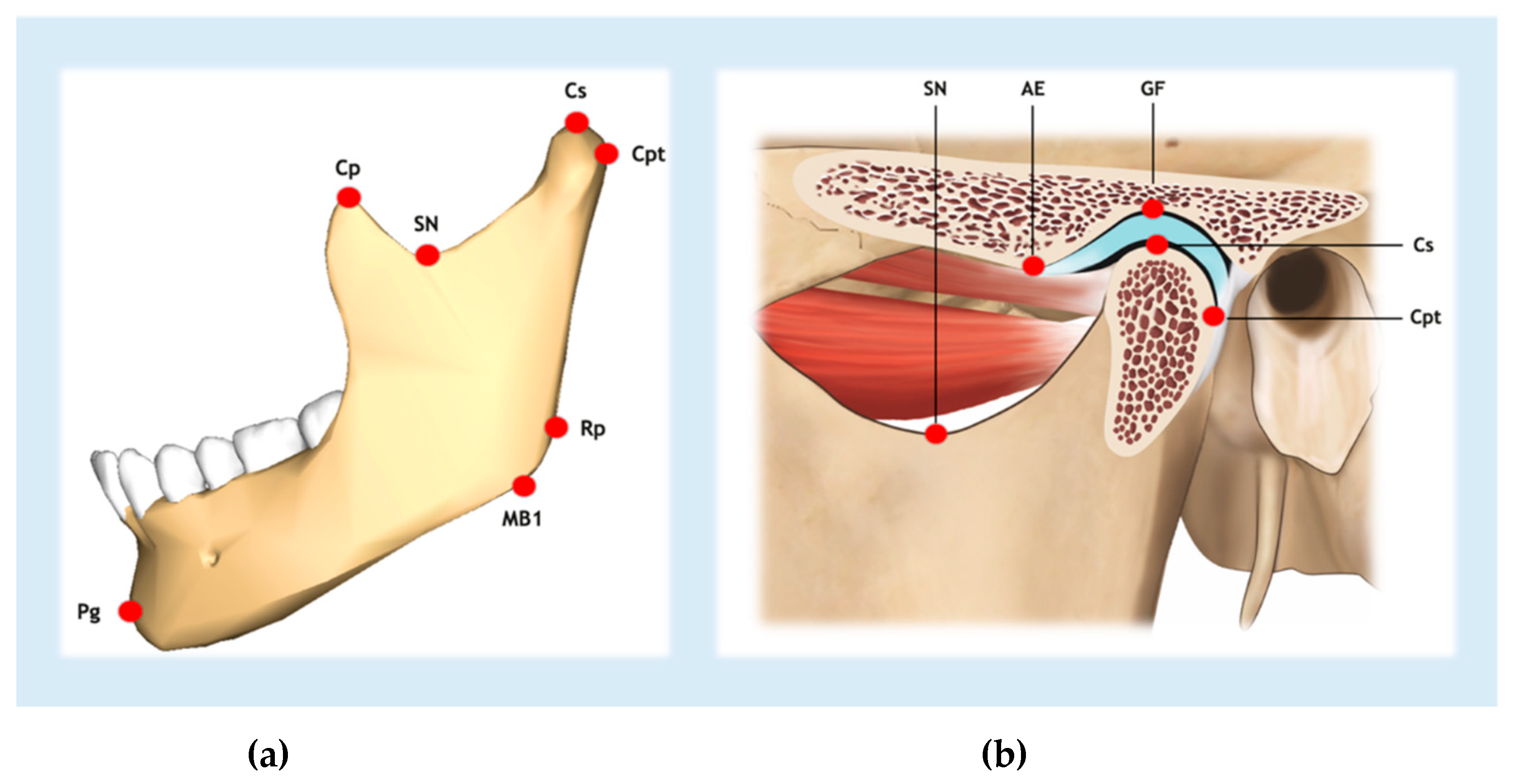
Figure 3.
Measurements of the lengths of both hemimandibles (blue or yellow lines).
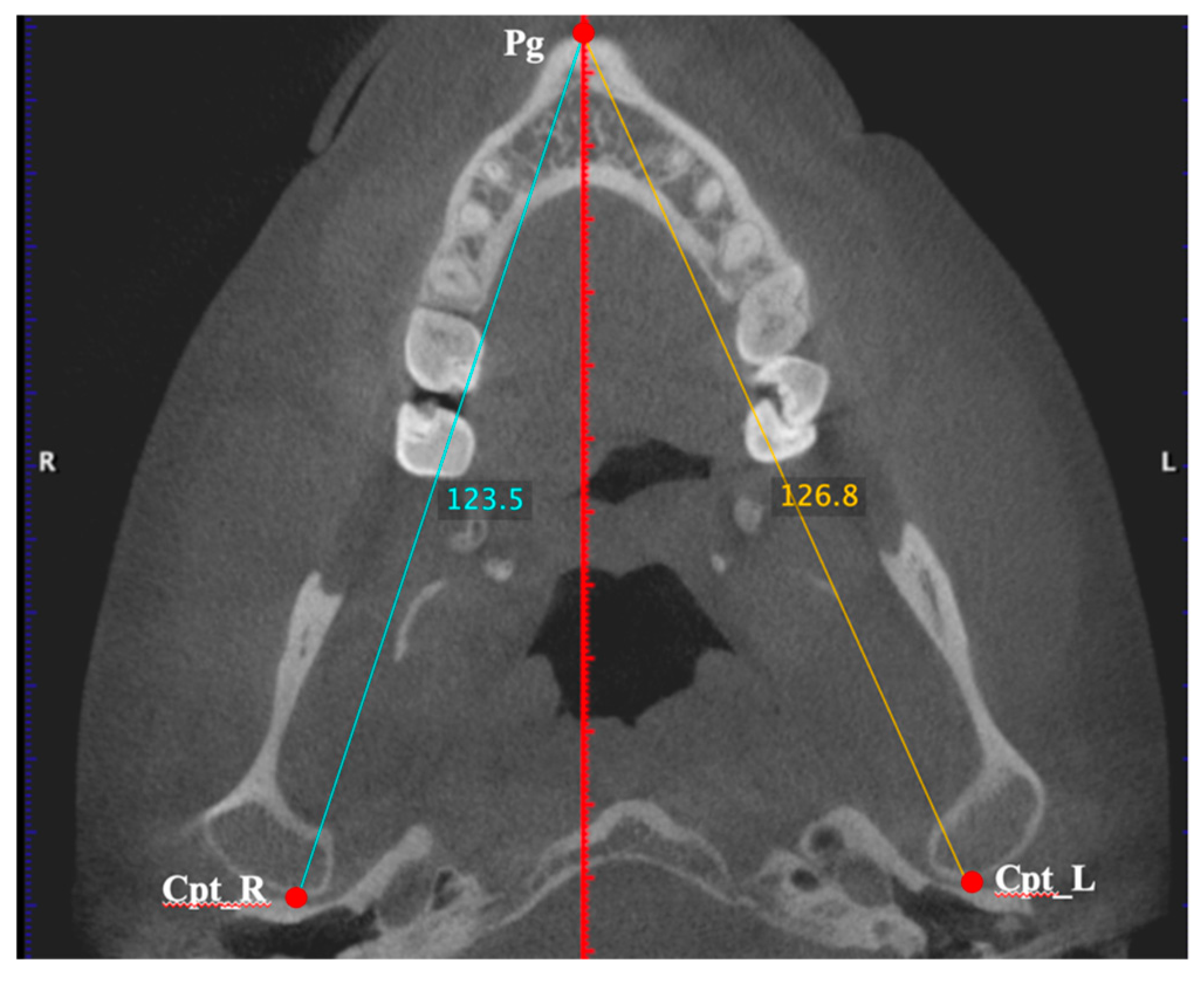

Table 1.
Landmarks in the CBCT analysis.
| Abbreviation | Reference point | Definition |
| AE | Articular eminence | Most inferior point of the apex of the articular eminence |
| Cl | Condyle-lateral | Most lateral point of the mandibular condyle |
| Cp | Coronoid | Most superior point of the coronoid process |
| Cpt | Condyle-posterior | Most posterior point of the mandibular condyle |
| Cs | Condyle-superior | Most superior point of the mandibular condyle |
| GF | Glenoid fossa | Most superior point of the glenoid fossa |
| MB1 | Mandibular ramus | Most inferior point of the inferior border of the mandibular ramus |
| Pg | Pogonion | Most anterior point of the outline of the mandibular symphysis |
| P16 | Tooth 16 | Most posterolateral point of the crown of tooth 16 |
| P26 | Tooth 26 | Most posterolateral point of the crown of tooth 26 |
| Rp | Mandibular angle | Most prominent posterosuperior point of the angle of the mandible at the mandibular ramus |
| SN | Sigmoid notch | Most inferior point of the sigmoid notch |
Table 2.
Biological characteristics of the participants (n=38). IQR, interquartile range; SD, standard deviation; VAS, 0-10 visual analogue scale.
Table 2.
Biological characteristics of the participants (n=38). IQR, interquartile range; SD, standard deviation; VAS, 0-10 visual analogue scale.
| Characteristic | Participants | ||
| Female sex – no. (%) | 35 (92.1) | ||
| Median age (IQR) – years | 29.5 (25 – 42) | ||
| Affected side/s – no. (%) | |||
| Right | 7 (18.4) | ||
| Left | 19 (50) | ||
| Both | 12 (31.6) | ||
| Arthralgia (with or without myalgia) – no. (%) | 32 (84.2) | ||
| Myalgia (without arthralgia) – no. (%) | 6 (15.8) | ||
| Jaw-pain score (VAS) | |||
| Median (IQR) | 7 (6 – 7.6) | ||
| Mean (SD) | 6.7 (1.2) | ||
| Habitual chewing side – no. (%) | |||
| Right | 12 (31.6) | ||
| Left | 18 (47.4) | ||
| Alternate | 8 (21.1) | ||
| Side toward midline shift was deviated – no. (%) | |||
| Right | 16 (42.1) | ||
| Left | 13 (34.2) | ||
| Both | 8 (21.1) | ||
| Cannot be assessed | 1 (2.6) | ||
| Condylar path angles in relation to Frankfort Horizontal Plane | |||
| Right side. Mean (SD) (degrees) | 50.5 (10.7) | ||
| Left side. Mean (SD) (degrees) | 50.1 (10.5) | ||
Table 3.
Dimensions of bone structures from CBCT images (n=38) and intraindividual (right versus left sides) comparisons. Additionally, the effect size values (Cohen’s d) are presented. A positive value of mean differences indicates larger dimensions on the right side and vice versa. SD – Standard deviation; CI – Confidence Interval; * – Two-tailed Student’s t test for paired samples.
Table 3.
Dimensions of bone structures from CBCT images (n=38) and intraindividual (right versus left sides) comparisons. Additionally, the effect size values (Cohen’s d) are presented. A positive value of mean differences indicates larger dimensions on the right side and vice versa. SD – Standard deviation; CI – Confidence Interval; * – Two-tailed Student’s t test for paired samples.
|
Variable Mean (SD) |
Side |
Paired differences (95% CI) |
P-value * | Effect size | |
| Right | Left | ||||
| Hemimandible length (mm) | 119.4 (5.7) | 118.6 (5.3) | 0.9 (0.2 to 1.5) | 0.01 | 0.4 |
| Mandibular body length (mm) | 92.2 (5.2) | 92.9 (5.1) | -0.7 (-1.4 to 0.1) | 0.08 | -0.3 |
| Mandibular ramus height (mm) | 65.6 (5.4) | 64.5 (4.3) | 1.1 (0.1 to 2.2) | 0.03 | 0.4 |
| Coronoid process height (mm) | 11.7 (3.2) | 11.6 (3.4) | 0.1 (-0.3 to 0.5) | 0.51 | 0.1 |
| Condylar process height (mm) | 16.0 (2.3) | 15.4 (2.1) | 0.7 (0.0 to 1.3) | 0.04 | 0.4 |
| Distance Cl-MSP (mm) | 56.5 (3.0) | 56.5 (3.2) | 0.0 (-0.8 to 0.8) | 0.97 | 0.9 |
| Hemimaxilla width (mm) | 27.0 (1.3) | 27.0 (1.6) | 0.0 (-0.5 to 0.5) | 0.99 | 0.0 |
| AE height (mm) | 7.0 (1.7) | 6.6 (1.5) | 0.5 (0.0 to 0.9) | 0.04 | 0.4 |
| AE inclination angle (degrees) | 33.5 (7.1) | 33.7 (6.5) | -0.2 (-2.0 to 1.6) | 0.80 | 0.0 |
| Condylar path angle (degrees) | 45.7 (9.9) | 48.8 (9.7) | -3.1 (-6.3 to 0.0) | 0.05 | -0.3 |
Table 4.
Bone dimensions measured on CBCT images (n=29). Intra-individual comparisons between the side towards which the lower midline is deviated (ipsilateral) and the opposite side (contralateral). Positive values of the differences mean that the dimensions are larger on the side to which the mandibular midline is deviated; negative values indicate that it is larger on the side opposite to that on which the lower midline is deviated. Results for Student’s t-test; SD; P-value and 95% coefficient interval (CI) and the effect size values (Cohen’s d) are presented. R – Right side; L – Left side.
Table 4.
Bone dimensions measured on CBCT images (n=29). Intra-individual comparisons between the side towards which the lower midline is deviated (ipsilateral) and the opposite side (contralateral). Positive values of the differences mean that the dimensions are larger on the side to which the mandibular midline is deviated; negative values indicate that it is larger on the side opposite to that on which the lower midline is deviated. Results for Student’s t-test; SD; P-value and 95% coefficient interval (CI) and the effect size values (Cohen’s d) are presented. R – Right side; L – Left side.
|
Variable Mean (SD) |
Side towards the jaw incisal midline deviates |
Paired differences (95% CI) |
P-value | Effect size | |
| Ipsilateral | Contralateral | ||||
| Hemimandible length (mm) | 118.8 (5.1) | 118.8 (5.4) | -0.2 (-1.1 to 0.6) | 0.60 | -0.1 |
| Mandibular body length (mm) | 92.1 (4.4) | 92.5 (4.7) | -0.4 (-1.4 to 0.6) | 0.41 | -0.1 |
| Mandibular ramus height (mm) | 65.4 (5.1) | 64.9 (5.2) | 0.5 (-0.7 to 1.6) | 0.44 | 0.1 |
| Coronoid process height (mm) | 11.7 (3.3) | 12.1 (3.7) | -0.4 (-0.9 to 0.0) | 0.05 | -0.4 |
| Condylar process height (mm) | 15.7 (1.8) | 16.1 (2.3) | -0.3 (-1.0 to 0.4) | 0.40 | -0.2 |
| Distance Cl-MSP (mm) | 56.9 (3.2) | 56.5 (3.2) | 0.4 (-0.5 to 1.3) | 0.35 | 0.2 |
| Hemimaxilla width (mm) | 27.1 (1.3) | 27.0 (1.3) | 0.0 (-0.4 to 0.5) | 0.87 | 0.03 |
| AE height (mm) | 7.0 (1.8) | 6.8 (1.5) | 0.2 (-0.4 to 0.8) | 0.47 | 0.1 |
| AE inclination angle (degrees) | 34.3 (7.1) | 33.7 (7.0) | 0.6 (1.5 to 2.7) | 0.56 | 0.1 |
| Condylar path angle (degrees) | 47.5 (10.8) | 48.9 (9.1) | 0.6 (-1.5 to 2.7) | 0.57 | 0.1 |
Table 5.
Bone’s dimensions FROM CBCT images (n=25) on the sides affected versus unaffected (with chronic unilateral TMD-pain). Comparisons were carried out by two-tailed Student t-test for paired samples. A positive value of differences means that measurements are higher on the affected side, and vice versa. R – Right side; L – Left side; SD – Standard deviation; CI – Confidence interval.
Table 5.
Bone’s dimensions FROM CBCT images (n=25) on the sides affected versus unaffected (with chronic unilateral TMD-pain). Comparisons were carried out by two-tailed Student t-test for paired samples. A positive value of differences means that measurements are higher on the affected side, and vice versa. R – Right side; L – Left side; SD – Standard deviation; CI – Confidence interval.
|
Variable Mean (SD) |
Chronic TMD (unilateral symptoms) |
Paired differences (95% CI) |
P-value | Effect size | |
| Affected side | Unaffected side | ||||
| Hemimandible length (mm) | 119.8 (5.6) | 120.1 (6.3) | -0.3 (-1.2 to 0.6) | 0.54 | -0.1 |
| Mandibular body length (mm) | 93.3 (5.9) | 93.2 (5.9) | 0.0 (-1.0 to 0.6) | 0.87 | -0.1 |
| Mandibular ramus height (mm) | 65.2 (4.4) | 66.5 (5.7) | -1.3 (-2.6 to 0.05) | 0.06 | -0.4 |
| Coronoid process height (mm) | 11.8 (3.9) | 11.6 (3.7) | 0.3 (-0.2 to 0.7) | 0.25 | 0.2 |
| Condylar process height (mm) | 15.7 (2.2) | 16.2 (2.7) | -0.5 (-1.3 to 0.4) | 0.31 | -0.2 |
| Distance Cl-MSP (mm) | 57.3 (3.2) | 56.8 (1.7) | 0.5 (-0.5 to 1.5) | 0.35 | 0.2 |
| Hemimaxilla width (mm) | 27.1 (1.7) | 27.1 (1.7) | 0.0 (-0.6 to 0.5) | 0.92 | 1.4 |
| AE height (mm) | 6.5 (1.6) | 7.1 (1.9) | -0.5 (-1.2 to 0.1) | 0.09 | 0.4 |
| AE inclination angle (degrees) | 32.6 (7.7) | 33.3 (7.1) | -0.7 (-1.9 to 0.5) | 0.25 | -0.2 |
| Condylar path angle (degrees) | 48.9 (9.5) | 45.2 (11.0) | 3.7 (0.3 to 7.2) | 0.04 | 0.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



