
Submitted:
09 December 2024
Posted:
11 December 2024
You are already at the latest version
Abstract
The clinical manifestation of leishmaniasis, caused by protozoan parasites of the Leishmania genus, ranges from cutaneous lesions to severe visceral disease. The present study is a comprehensive overview of the neurologic manifestations of Leishmania spp. infection, highlighting the epidemiology, clinical presentation, pathogenesis, diagnosis, and management. Also, epidemiological factors, including geographical distribution, vector species, and host susceptibility, influence the prevalence and distribution of neuroleishmaniasis. Clinical presentation of neuroleishmaniasis varies widely and may include meningoencephalitis, encephalopathy, myelitis, peripheral neuropathy, seizures, and cognitive impairment. The diversity of neurological manifestations reflects the complex interactions between the parasite, host immune response and neural tissues. Diagnostic challenges arise due to the nonspecific nature of symptoms, limited sensitivity of available tests, and difficulties in accessing CNS tissues for definitive diagnosis. Treatment of neuroleishmaniasis requires a multidisciplinary approach, with antiparasitic drugs such as liposomal amphotericin B and miltefosine serving as the mainstays of therapy. Adjunctive therapies, including corticosteroids and anticonvulsants, may manage neurological complications and alleviate symptoms. However, challenges such as drug resistance, limited CNS penetration, and systemic toxicity pose significant obstacles to treatment success. Prevention of neuroleishmaniasis involves vector control measures, reservoir management, health education, and community engagement. Integrated control strategies to reduce human-vector contact and interrupt disease transmission are essential for mitigating the burden of neuroleishmaniasis and improving patient outcomes.
Keywords:
leishmaniasis
; neuroleishmaniasis
; kala-azar
; neurologic manifestations
; neurotoxicity
; neuroinflammation
; black fever
; dumdum fever
; pathogenesis
; clinical presentation
1. Introduction
1.1. Overview of Leishmaniasis
Leishmaniasis, a neglected tropical disease caused by protozoan parasites of the Leishmania genus, remains a significant public health concern globally, particularly in tropical and subtropical regions [1]. This complex disease manifests in various clinical forms, presenting unique diagnosis, treatment, and control challenges.
The etiological agents of leishmaniasis belong to the Leishmania genus, with over 20 species known to infect humans [2]. These parasites have a dimorphic life cycle alternating between motile promastigotes in the sand fly vector and intracellular amastigotes in mammalian hosts (Figure 1). Transmission occurs through the bite of infected female sand flies, primarily belonging to the Phlebotomus genus in the Old World and the Lutzomyia genus in the New World [3].
Clinical forms of leishmaniasis primarily include cutaneous leishmaniasis (CL) and visceral leishmaniasis (VL), with mucocutaneous leishmaniasis (MCL) representing a severe complication of CL [4]. Cutaneous leishmaniasis manifests in various presentations, from localized cutaneous lesions to diffuse forms characterized by ulcers and nodules on the skin. Mucocutaneous leishmaniasis, predominantly found in South America, affects mucous membranes, leading to destructive nose, mouth, and throat lesions [5]. Visceral leishmaniasis, known as kala-azar, affects internal organs such as the spleen, liver, and bone marrow, causing systemic symptoms including fever, weight loss, and hepatosplenomegaly [6].
The clinical presentation of leishmaniasis varies depending on the Leishmania species involved, the host's immune response, and environmental factors. Diagnosis relies on clinical evaluation, parasitological confirmation through microscopy or culture, serological tests, and molecular techniques such as polymerase chain reaction. However, accurate diagnosis remains challenging, particularly in resource-limited settings where diagnostic tools may be scarce [7].
Treatment options for leishmaniasis are limited and vary depending on the clinical form and geographical location [8]. Antimonials have been the mainstay of treatment for decades but are associated with toxicities and increasing resistance. Alternatives include liposomal amphotericin B, miltefosine, and pentamidine, each with efficacy and safety profile. However, access to these drugs may be limited in endemic regions, further complicating disease management. Preventive measures focus on vector control strategies, including insecticide spraying, environmental management, and bed nets to reduce sand fly bites. Additionally, efforts to develop vaccines against leishmaniasis continue, although none are available for widespread use [9]. This study aims to narratively review the epidemiological features, pathophysiology, and management of neuroleishmaniasis.
1.2. Epidemiology and Global Burden
Leishmaniasis affects millions worldwide, particularly in tropical and subtropical regions. Understanding its epidemiology and global burden is crucial for effective disease control and public health interventions [10]. Leishmaniasis is endemic in 98 countries, with most cases occurring in developing regions of Africa, Asia, Latin America, and the Mediterranean Basin [11]. The distribution of the disease is closely linked to environmental factors, such as temperature, humidity, and the presence of suitable vectors.
The global incidence of leishmaniasis is estimated to be around 0.7 to 1.2 million cases annually, with approximately 20,000 to 30,000 deaths attributed to the disease each year [12]. However, these numbers are likely underestimated due to underreporting and challenges in diagnosis, particularly in resource-limited settings. Leishmaniasis exhibits geographic variation in its clinical manifestations and Leishmania species involved. Cutaneous leishmaniasis (CL) is more prevalent in the Middle East, Central Asia, and parts of Africa and Latin America. In contrast, visceral leishmaniasis (VL) is endemic in East Africa, the Indian subcontinent, and Latin America [13].
Various socio-economic and environmental factors contribute to the risk of leishmaniasis transmission. These include poverty, malnutrition, displacement due to conflict or natural disasters, urbanization, deforestation, and climate change, which can alter the distribution and abundance of vectors [14]. Some populations are at higher risk of leishmaniasis, including rural communities living in endemic areas, migrant workers, refugees, and immunocompromised individuals such as those co-infected with HIV/AIDS. Children are also disproportionately affected, particularly by visceral leishmaniasis [15].
1.3. Classification of Leishmania spp.
Leishmania is a genus of protozoan parasites belonging to the family Trypanosomatidae and the order Kinetoplastida. Several species have distinct characteristics within the genus Leishmania, including morphology, geographical distribution, and clinical manifestations in humans and other mammalian hosts. Classification of Leishmania spp. is primarily based on molecular phylogenetic analyses, biochemical characteristics, and clinical features [16]. Classification within the Leishmania genus continues to evolve as new species are discovered and characterized through molecular techniques and epidemiological studies. Understanding the diversity and distribution of Leishmania spp. is essential for disease surveillance, diagnosis, treatment, and control efforts in endemic regions worldwide (Table 1) [17].
1.4. Importance of Understanding Neurologic Manifestations
Recognition of neurologic symptoms allows for timely diagnosis and appropriate treatment initiation [18]. Prompt management can prevent disease progression, reduce morbidity, and improve patient outcomes. Also, neurologic complications can significantly impact affected individuals’ quality of life. Understanding these manifestations ensures comprehensive patient care, addressing the disease's systemic and neurological aspects. Moreover, neurologic manifestations of leishmaniasis may mimic other neurological conditions, such as meningitis, encephalitis, or peripheral neuropathy. Knowledge of these presentations aids in accurate differential diagnosis, preventing misdiagnosis and inappropriate treatment.
Some neurologic manifestations, such as meningoencephalitis or myelitis, may indicate severe disease and poorer prognosis [19]. Recognizing these indicators allows healthcare providers to implement appropriate monitoring and management strategies to optimize patient outcomes. In addition, neurologic manifestations of leishmaniasis may pose challenges for disease control and prevention efforts. Understanding these complications' epidemiology and clinical impact informs public health strategies to reduce disease burden and transmission.
2. Pathogenesis of Neuroleishmaniasis
2.1. Mechanisms of Central Nervous System Invasion
The invasion of the CNS by Leishmania parasites, leading to neuroleishmaniasis, involves complex mechanisms that are not fully understood. Leishmania parasites may enter the CNS through the bloodstream, crossing the blood-brain barrier (BBB) either by passive diffusion or through infected immune cells [20]. Once in the CNS, parasites can infect resident cells such as microglia, astrocytes, and neurons, leading to neuroinflammation and tissue damage [21].
Some Leishmania species exhibit neurotropic properties facilitating their invasion and survival within the CNS. This neurotropism may be mediated by specific surface molecules or receptors on neuronal cells that interact with parasite ligands, allowing for adhesion and entry into neural tissues [22]. Inflammatory mediators released during the host immune response to Leishmania infection can disrupt the integrity of the BBB, facilitating the entry of parasites and immune cells into the CNS. This BBB disruption may be mediated by cytokines, chemokines, matrix metalloproteinases, and other inflammatory molecules produced in response to infection [23].
Leishmania parasites can exploit host immune cells, such as monocytes and dendritic cells, such as “Trojan horses,” to penetrate the CNS. Infected immune cells carrying intracellular parasites may cross the BBB and release parasites into the brain parenchyma, initiating local infection and inflammation [24]. Also, leishmania parasites produce various virulence factors and immune evasion mechanisms, contributing to their ability to invade and survive within the CNS. These factors may include surface glycoconjugates, proteases, lipophosphoglycan, and other molecules that modulate host immune responses and promote parasite persistence in neural tissues [25].
The host immune response is critical in determining the outcome of CNS invasion by Leishmania parasites. Dysregulated immune responses, including excessive inflammation or immunosuppression, can contribute to neuroinflammation, tissue damage, and clinical manifestations of neuroleishmaniasis [26].
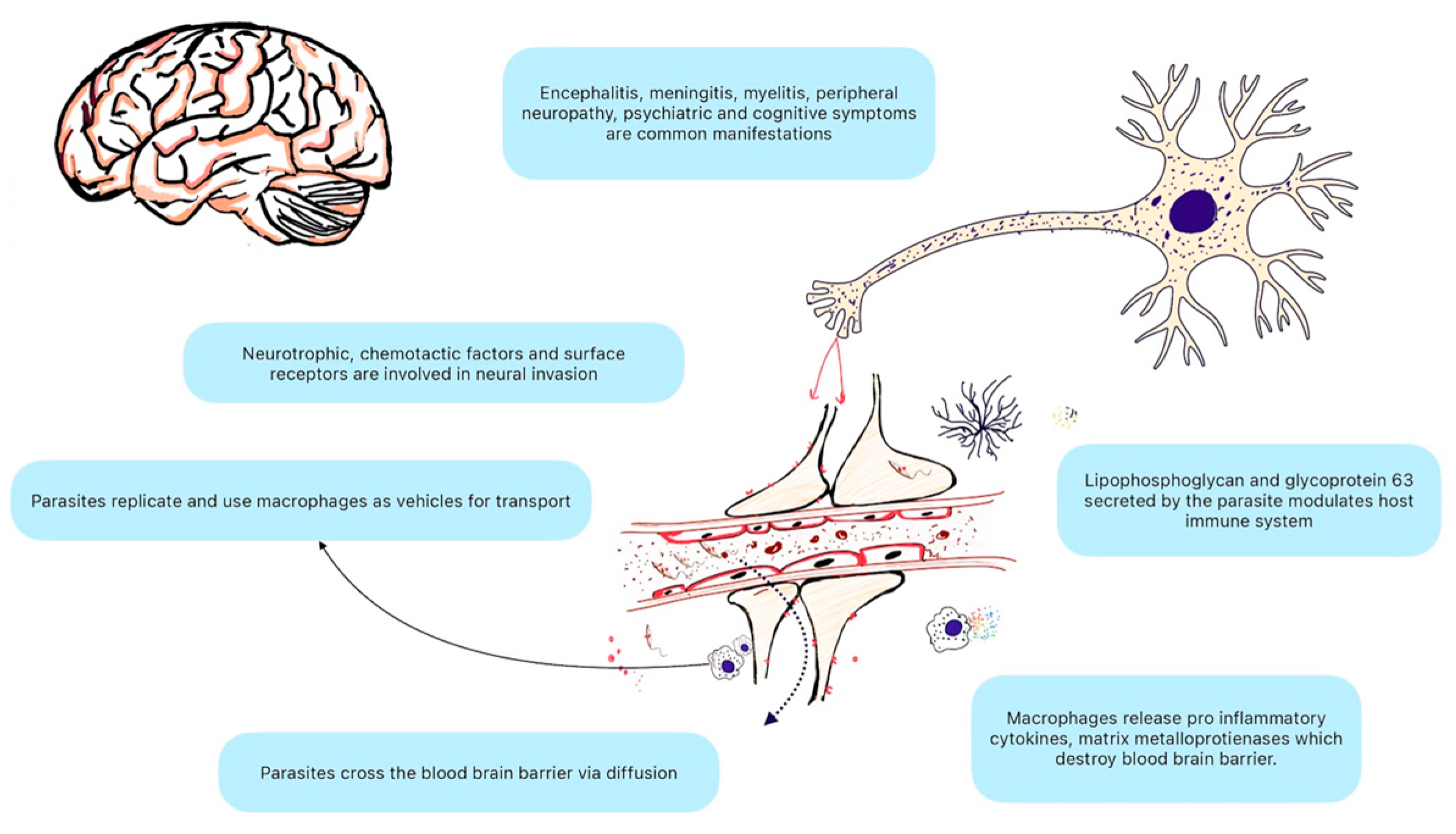
Figure 2.
Leishmania species neural invasion. Leishmania species breach the blood-brain barrier via interaction with the host immune system and the interplay of various cytokine factors. Macrophages and microglial cells play critical roles in immune response. Central nervous system manifestations of Leishmania can be acute and chronic.
Figure 2.
Leishmania species neural invasion. Leishmania species breach the blood-brain barrier via interaction with the host immune system and the interplay of various cytokine factors. Macrophages and microglial cells play critical roles in immune response. Central nervous system manifestations of Leishmania can be acute and chronic.
2.2. Immune Response in Neuroleishmaniasis
In neuroleishmaniasis, the immune response plays a crucial role in the disease's pathogenesis, control, and outcome. The interaction between Leishmania parasites and the host immune system within the CNS is complex and dynamic, involving various immune cells, cytokines, chemokines, and other immune mediators.
Microglia are central in initiating the innate immune response against Leishmania parasites [27]. Upon infection, microglia recognize parasite-associated molecular patterns through pattern recognition receptors, producing pro-inflammatory cytokines such as tumor necrosis factor-α, interleukin-1 β, and interleukin-6 [28]. Astrocytes also contribute to the innate immune response by producing cytokines and chemokines in response to Leishmania infection, thereby recruiting immune cells to the site of infection and modulating local inflammation [29].
T-lymphocytes, particularly CD4+ T cells, are critical in orchestrating the adaptive immune response against Leishmania parasites in the CNS. CD4+ T cells produce cytokines such as interferon-gamma and interleukin-12, which activate macrophages and promote parasite clearance [30]. Regulatory-T cells and T-helper 17 cells also influence the balance of immune responses in neuroleishmaniasis, regulating inflammation and tissue damage [31]. B lymphocytes and antibody responses may contribute to host defense against Leishmania parasites in the CNS, although their role in neuroleishmaniasis is less well-characterized than in systemic leishmaniasis [32].
Leishmania parasites have evolved various immunomodulatory strategies to evade host immune responses and establish chronic infection in the CNS [33]. These include suppressing macrophage activation, inhibiting pro-inflammatory cytokine production, and induction of anti-inflammatory and regulatory pathways. Parasite-derived molecules such as lipophosphoglycan and glycoprotein 63 contribute to immunomodulation by interfering with host signaling pathways and immune cell functions [34].
Excessive or dysregulated immune responses in the CNS can lead to neuroinflammation, tissue damage, and clinical manifestations of neuroleishmaniasis, including meningitis, encephalitis, and myelitis. Chronic inflammation and tissue destruction may result from the persistence of parasites within neural tissues, sustained immune activation, and the recruitment of inflammatory cells [35].
2.3. Factors Influencing Neurological Complications
Several factors can influence the development and severity of neurological complications in leishmaniasis. These factors include host-parasite interaction, host immune response, parasite biology, and clinical features. Understanding these factors is essential for effectively predicting, preventing, and managing neurological complications.
Different Leishmania species and strains exhibit varying neurotropism and virulence, influencing the likelihood and severity of neurological complications. For example, some strains of Leishmania donovani and Leishmania braziliensis have been associated with an increased risk of neuroleishmaniasis [36]. Also, the host immune response is critical in determining susceptibility to neurological complications. Immunocompromised individuals, such as those with HIV/AIDS or receiving immunosuppressive therapy, are at higher risk of developing severe neuroleishmaniasis due to impaired immune surveillance and parasite control [37]. Moreover, the balance between pro-inflammatory and anti-inflammatory responses within the CNS influences the pathogenesis of neuroleishmaniasis. Dysregulated immune responses, characterized by excessive inflammation or immunosuppression, can contribute to neuronal damage, tissue destruction, and clinical manifestations of neurological disease.
The magnitude of parasite burden within neural tissues and the distribution of parasites within the CNS can impact the severity and clinical presentation of neurological complications [38]. Higher parasite loads and widespread tissue involvement are associated with more severe disease manifestations. In addition, genetic factors in both the host and the parasite can influence susceptibility to neurological complications and the clinical course of neuroleishmaniasis. Host genetic polymorphisms related to immune function, inflammation, and neuronal susceptibility may modulate individual susceptibility to neurological disease [39].
Concurrent infections, such as HIV/AIDS, tuberculosis, or other opportunistic infections, can exacerbate neurological complications in individuals with leishmaniasis [40]. Additionally, underlying comorbidities such as malnutrition, diabetes, or chronic systemic diseases may impact disease severity and treatment outcomes [41]. Interestingly, delayed diagnosis and inadequate access to healthcare services can lead to advanced disease progression and more severe neurological complications in individuals with leishmaniasis [42]. Early detection, prompt treatment initiation, and comprehensive healthcare are crucial for effectively preventing and managing neurological sequelae.
3. Clinical Presentation
3.1. Forms of Neuroleishmaniasis
The clinical presentation of neuroleishmaniasis can vary widely depending on several factors, including the species of Leishmania involved, the immune status of the host, and the extent of CNS involvement. Neuroleishmaniasis can present as several distinct clinical syndromes, each with characteristic features [43].
Meningoencephalitis is the most common and severe form of neuroleishmaniasis, characterized by meningitis and encephalitis [19]. Neuroimaging may reveal meningeal enhancement, parenchymal lesions, and signs of cerebral edema. Also, encephalitis can occur as a primary manifestation of neuroleishmaniasis or as a complication of meningoencephalitis. MRI findings may show diffuse or focal brain parenchymal abnormalities, including edema, hemorrhage, and white matter lesions. Also, there are some reports of myelitis and peripheral neuropathy secondary to Leishmaniasis [44]. Moreover, neuroleishmaniasis can also present with cognitive impairment, behavioral changes, and psychiatric symptoms [45].
The clinical presentation of neuroleishmaniasis can be nonspecific and may overlap with other infectious, inflammatory, or neoplastic CNS disorders, posing diagnostic challenges [46]. A thorough clinical evaluation, including history-taking, neurological examination, imaging studies, and laboratory investigations, is essential for accurate diagnosis and appropriate management of neuroleishmaniasis. Prompt recognition and treatment of neuroleishmaniasis are crucial for preventing disease progression and improving patient outcomes [47].
3.2. Symptomatology and Disease Progression
The symptomatology and disease progression of neuroleishmaniasis can vary depending on factors such as the Leishmania species, host immune status, and extent of CNS involvement. While the clinical presentation can be diverse, neuroleishmaniasis typically follows a progressive course with various neurological manifestations. Neuroleishmaniasis often presents with nonspecific symptoms such as fever, headache, malaise, and fatigue, which may mimic other infectious or inflammatory conditions [48]. These initial symptoms may precede the onset of neurological manifestations in days to weeks. Patients may develop neurological symptoms related to CNS involvement as the disease progresses. But, these symptoms can vary widely.
Neuroleishmaniasis can progress rapidly, leading to worsening neurological deficits and systemic complications if left untreated [49]. The severity and rate of disease progression can vary depending on factors such as the host's immune status and the Leishmania species' virulence. In some cases, neuroleishmaniasis can take a chronic course with relapsing or persistent neurological symptoms despite treatment. Residual neurological deficits, including cognitive impairment, motor weakness, and sensory disturbances, may persist even after successful resolution of acute infection.
3.3. Variations Based on Leishmania Species
The clinical presentation and manifestations of neuroleishmaniasis can vary depending on the species of Leishmania involved. Different Leishmania species exhibit varying neurotropism, virulence, and propensity to cause neurological complications.
Leishmania donovani is primarily associated with visceral leishmaniasis (VL), but it can also cause neuroleishmaniasis, particularly in regions where VL is endemic. Neurological complications of L. donovani infection may include meningoencephalitis, encephalopathy, seizures, and focal neurological deficits. Visceral leishmaniasis caused by L. donovani can lead to hematogenous dissemination of parasites to the CNS, resulting in neurological involvement [50].
Leishmania infantum, also known as Leishmania chagasi, is another species associated with visceral leishmaniasis and can cause neuroleishmaniasis. Neurological manifestations of L. infantum infection may include meningoencephalitis, encephalopathy, and myelitis, similar to those observed with L. donovani infection [51].
Leishmania braziliensis and other species within the L. braziliensis complex are primarily associated with cutaneous and mucocutaneous leishmaniasis but can also cause neuroleishmaniasis. Neurological complications of L. braziliensis infection may include meningoencephalitis, encephalopathy, and myelitis, often presenting as severe and progressive [52].
Leishmania tropica is primarily associated with cutaneous leishmaniasis, particularly in the Middle East and Central Asia. While neurological complications of L. tropica infection are less commonly reported compared to other species, isolated cases of neuroleishmaniasis have been documented, typically presenting as meningoencephalitis [53].
Various other Leishmania species, including L. major, L. mexicana, L. amazonensis, L. guyanensis, and L. peruviana, have been associated with cutaneous and mucocutaneous leishmaniasis but may rarely cause neuroleishmaniasis [54]. Neurological complications associated with these species may include meningoencephalitis, encephalopathy, and myelitis, although their frequency and clinical significance may vary.
4. Diagnostic Challenges
Neuroleishmaniasis is a challenging diagnosis due to several factors, including the nonspecific nature of symptoms, limitations of available diagnostic tests, and the complexity of CNS involvement in the disease.
Neuroleishmaniasis often presents with nonspecific symptoms such as fever, headache, and altered mental status, which can mimic other infectious, inflammatory, or neoplastic CNS disorders. This can lead to delays in diagnosis and treatment initiation. Also, unlike systemic leishmaniasis, which can be diagnosed by detecting Leishmania parasites in tissue samples or by serological tests, neuroleishmaniasis lacks specific biomarkers for diagnosis. CSF analysis may show nonspecific abnormalities such as pleocytosis and elevated protein levels but does not provide definitive evidence of CNS involvement by Leishmania parasites [55]. Moreover, diagnostic tests for neuroleishmaniasis, such as CSF microscopy, culture, PCR, and antibody detection assays, may have limited sensitivity, especially in low parasite burden or atypical clinical presentations. False-negative results can occur, leading to missed diagnoses.
The diverse clinical presentations of neuroleishmaniasis further complicate diagnosis and may require a high index of suspicion. In addition, patients with neuroleishmaniasis may have concurrent infections, such as HIV/AIDS or tuberculosis, or underlying comorbidities that complicate diagnosis and management. Coexisting conditions can mask or exacerbate neurological symptoms, making it challenging to attribute them solely to Leishmania infection.
Obtaining diagnostic samples from the CNS, such as CSF, brain biopsy, or nerve biopsy, often requires invasive procedures that carry risks of complications and may not be feasible in all patients. Access to specialized diagnostic tools, such as PCR or advanced imaging modalities, may be scarce in resource-limited settings where leishmaniasis is endemic. This can hinder accurate diagnosis and appropriate management of neuroleishmaniasis.
5. Management Strategies
5.1. Pharmacological Interventions
Medications for neuroleishmaniasis aim to eradicate Leishmania parasites from the CNS, reduce neurological symptoms, prevent disease progression, and improve patient outcomes. Treatment approaches typically involve the use of antiparasitic drugs, adjunctive therapies to manage neurological complications and supportive care.
Pentavalent antimonials such as sodium stibogluconate and meglumine antimoniate have been the mainstay for visceral and cutaneous leishmaniasis treatment [56]. However, their efficacy in treating neuroleishmaniasis is limited due to poor CNS penetration and potential toxicity. Liposomal amphotericin B formulations are considered the first-line treatment for neuroleishmaniasis due to their superior efficacy and safety profile [57]. These formulations have better CNS penetration and are effective against Leishmania parasites resistant to other drugs. Oral miltefosine, an alkylphosphocholine compound, has shown efficacy in treating visceral and cutaneous leishmaniasis and may also be used for neuroleishmaniasis [58]. However, its CNS penetration is limited, and combination therapy with other antiparasitic drugs may be required. Other antileishmanial medications, such as paromomycin, pentamidine, and azoles, have been used in some cases of neuroleishmaniasis, although their efficacy and CNS penetration vary (Table 2) [59].
Systemic corticosteroids may be adjunctive therapy in neuroleishmaniasis to reduce inflammation, alleviate neurological symptoms, and prevent complications associated with immune-mediated pathology [60]. However, their use should be cautious due to the risk of immunosuppression and exacerbation of underlying infection. Close monitoring of patients undergoing treatment for neuroleishmaniasis is essential to assess treatment response, monitor for adverse effects of medications, and manage complications such as electrolyte imbalances, renal toxicity, and infusion-related reactions associated with antiparasitic drugs.
5.2. Challenges in Treatment
Treatment of neuroleishmaniasis poses several challenges due to the complex nature of the disease, limitations of available therapies, and difficulties associated with CNS penetration of antiparasitic drugs. Some antileishmanial drugs, particularly pentavalent antimonials, have limited efficacy in treating neuroleishmaniasis due to poor CNS penetration and resistance. Resistance to amphotericin B and miltefosine also have been reported, further limiting treatment options and effectiveness [61].
Achieving adequate drug concentrations in the CNS to eradicate Leishmania parasites is challenging due to the BBB, which restricts the entry of drugs into the brain and CSF [62]. Liposomal formulations of amphotericin B have improved CNS penetration compared to conventional formulations but may still be inadequate in some cases.
There is a lack of consensus on the optimal treatment regimens for neuroleishmaniasis, including the choice of antiparasitic drugs, dosing schedules, and duration of therapy. Combination therapy with multiple antileishmanial drugs or drug classes may be necessary to enhance efficacy, overcome resistance, and improve treatment outcomes, but optimal combinations have yet to be established [63].
6. Prevention and Control Measures
6.1. Vector and Reservoir Control
Preventing leishmaniasis involves integrated strategies to reduce human-vector contact, control reservoir hosts, improve diagnosis and treatment, and implement vector control measures. In this context, the distribution of bed nets treated with insecticides, such as pyrethroids, can reduce the biting rate of sand flies and prevent transmission of Leishmania parasites [64]. Applying residual insecticides to indoor surfaces can kill sand flies resting inside houses and reduce vector populations. Removing organic matter, vegetation, and animal shelters from peri-domestic areas can reduce sand fly breeding sites and decrease vector densities. Individuals can protect themselves from sand fly bites by wearing long-sleeved clothing and insect repellents and staying indoors during peak biting times [65]. Also, treating domestic animals, such as dogs, with insecticides or systemic medications can reduce their susceptibility to Leishmania infection and decrease the risk of transmission to humans. Implementing measures to control stray animal populations, such as dog culling or vaccination campaigns, can help reduce the reservoir of Leishmania parasites in endemic areas [66].
6.2. Public Health Strategies
Educating communities about the transmission, symptoms, and prevention of leishmaniasis can promote early detection, treatment-seeking behavior, and adoption of preventive measures [67]. Engaging local communities in vector control activities, environmental sanitation, and animal reservoir management can enhance the effectiveness and sustainability of control efforts. Screening high-risk populations, such as individuals with HIV/AIDS, migrants, and travelers to endemic areas for leishmaniasis, can facilitate early diagnosis and treatment [68]. Strengthening healthcare systems to improve access to diagnostic tests and treatment for suspected leishmaniasis cases can reduce morbidity and mortality associated with the disease. Monitoring sand fly populations, infection rates, and distribution can provide valuable information for targeting vector control interventions and assessing the effectiveness of control measures [69].
6.3. Research Needs and Future Directions
Research efforts focused on developing vaccines against leishmaniasis aim to provide long-term protection against infection and reduce disease transmission [70]. Continued research into new antileishmanial drugs, drug combinations, and treatment regimens is needed to overcome drug resistance, improve efficacy, and minimize side effects [71]. Collaboration between health authorities, veterinary services, environmental agencies, research institutions, and community organizations is essential for implementing integrated control strategies and addressing the multifaceted nature of leishmaniasis.
8. Conclusion
In conclusion, neuroleishmaniasis presents unique challenges in diagnosis, treatment, and management due to its involvement in the CNS and the potential for severe neurological complications. Despite advancements in our understanding of the disease, there are still significant gaps in knowledge regarding its pathogenesis, optimal treatment regimens, and long-term outcomes. The complexity of neuroleishmaniasis underscores the importance of multidisciplinary approaches.
Supplementary Materials
None.
Author Contributions
Conceptualization, J.P.R., V.V.B., and A.L.F.C.; methodology, A.L.F.C.; software, A.L.F.C.; validation, A.L.F.C., J.P.R. and V.V.B.; formal analysis, A.L.F.C.; investigation, A.L.F.C.; resources, A.L.F.C.; data curation, J.P.R.; writing—original draft preparation, J.P.R.; writing—review and editing, J.P.R.; visualization, V.V.B.; supervision, V.V.B.; project administration, V.V.B.; funding acquisition, J.P.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data created.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Thakur, L.; Singh, K.K.; Shanker, V.; Negi, A.; Jain, A.; Matlashewski, G.; Jain, M. Atypical Leishmaniasis: A Global Perspective with Emphasis on the Indian Subcontinent. PLoS Negl Trop Dis 2018, 12, e0006659. [Google Scholar] [CrossRef] [PubMed]
- Diniz, L.M.O.; Duani, H.; Freitas, C.R.; Figueiredo, R.M.; Xavier, C.C. Neurological Involvement in Visceral Leishmaniasis: Case Report. Revista da Sociedade Brasileira de Medicina Tropical 2010, 43, 743–745. [Google Scholar] [CrossRef] [PubMed]
- Sousa-Paula, L.C. de; Pessoa, F.A.C.; Otranto, D.; Dantas-Torres, F. Beyond Taxonomy: Species Complexes in New World Phlebotomine Sand Flies. Med Vet Entomol 2021, 35, 267–283. [Google Scholar] [CrossRef]
- Zobba, R.; Evangelisti, M.A.; Manunta, M.L.; Alberti, A.; Zucca, D.; Parpaglia, M.L.P. A Case of Canine Neurological Leishmaniasis. 2017.
- Abadías-Granado, I.; Diago, A.; Cerro, P.A.; Palma-Ruiz, A.M.; Gilaberte, Y. Cutaneous and Mucocutaneous Leishmaniasis. Actas Dermosifiliogr (Engl Ed) 2021, S1578-2190(21)00171-2. [CrossRef]
- Ahmed, B.-N.; Nabi, S.G.; Rahman, M.; Selim, S.; Bashar, A.; Rashid, M.M.; Lira, F.Y.; Choudhury, T.A.; Mondal, D. Kala-Azar (Visceral Leishmaniasis) Elimination in Bangladesh: Successes and Challenges. Current Tropical Medicine Reports 2014, 1, 163–169. [Google Scholar] [CrossRef]
- Karak, B.; Garg, R.K.; Misra, S.; Sharma, A.M. Neurological Manifestations in a Patient with Visceral Leishmaniasis. Postgrad Med J 1998, 74, 423–425. [Google Scholar] [CrossRef] [PubMed]
- Berkowitz, A.L.; Raibagkar, P.; Pritt, B.S.; Mateen, F.J. Neurologic Manifestations of the Neglected Tropical Diseases. J Neurol Sci 2015, 349, 20–32. [Google Scholar] [CrossRef]
- Pradhan, S.; Schwartz, R.A.; Patil, A.; Grabbe, S.; Goldust, M. Treatment Options for Leishmaniasis. Clin Exp Dermatol 2022, 47, 516–521. [Google Scholar] [CrossRef]
- Chunge, C.N.; Gachihi, G.; Muigai, R. Is Neurological Involvement Possible in Visceral Leishmaniasis in Kenya. Trans R Soc Trop Med Hyg 1985, 79, 872. [Google Scholar] [CrossRef]
- Alvar, J.; Vélez, I.D.; Bern, C.; Herrero, M.; Desjeux, P.; Cano, J.; Jannin, J.; den Boer, M. Leishmaniasis Worldwide and Global Estimates of Its Incidence. PLoS One 2012, 7, e35671. [Google Scholar] [CrossRef]
- Okwor, I.; Uzonna, J. Social and Economic Burden of Human Leishmaniasis. Am J Trop Med Hyg 2016, 94, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Ready, P.D. Epidemiology of Visceral Leishmaniasis. Clin Epidemiol 2014, 6, 147–154. [Google Scholar] [CrossRef]
- Yadav, N.; Upadhyay, R.K. Global Effect of Climate Change on Seasonal Cycles, Vector Population and Rising Challenges of Communicable Diseases: A Review. Journal of Atmospheric Science Research 2023, 6, 21–59. [Google Scholar] [CrossRef]
- Grifferty, G.; Shirley, H.; McGloin, J.; Kahn, J.; Orriols, A.; Wamai, R. Vulnerabilities to and the Socioeconomic and Psychosocial Impacts of the Leishmaniases: A Review. Res Rep Trop Med 2021, 12, 135–151. [Google Scholar] [CrossRef]
- Akhoundi, M.; Downing, T.; Votýpka, J.; Kuhls, K.; Lukeš, J.; Cannet, A.; Ravel, C.; Marty, P.; Delaunay, P.; Kasbari, M.; et al. Leishmania Infections: Molecular Targets and Diagnosis. Mol Aspects Med 2017, 57, 1–29. [Google Scholar] [CrossRef]
- Ghatee, M.A.; Taylor, W.R.; Karamian, M. The Geographical Distribution of Cutaneous Leishmaniasis Causative Agents in Iran and Its Neighboring Countries, A Review. Front Public Health 2020, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- Murray, H.W.; Berman, J.D.; Davies, C.R.; Saravia, N.G. Advances in Leishmaniasis. Lancet 2005, 366, 1561–1577. [Google Scholar] [CrossRef]
- Viñuelas, J.; García-Alonso, M.; Ferrando, L.; Navarrete, I.; Molano, I.; Mirón, C.; Carcelén, J.; Alonso, C.; Nieto, C.G. Meningeal Leishmaniosis Induced by Leishmania Infantum in Naturally Infected Dogs. Vet Parasitol 2001, 101, 23–27. [Google Scholar] [CrossRef]
- Melo, G.D.; Goyard, S.; Fiette, L.; Boissonnas, A.; Combadiere, C.; Machado, G.F.; Minoprio, P.; Lang, T. Unveiling Cerebral Leishmaniasis: Parasites and Brain Inflammation in Leishmania Donovani Infected Mice. Sci Rep 2017, 7, 8454. [Google Scholar] [CrossRef]
- Islek, Z.; Ucisik, M.H.; Sahin, F. Astrocytes Can Be Key Players Against Cerebral Leishmaniasis: In Vitro Co-Culture Model for the Assessment of Infection. Parasite Immunol 2024, 46, e13071. [Google Scholar] [CrossRef]
- Llanos-Cuentas, A.; Valencia, B.M.; Petersen, C.A. Neurological Manifestations of Human Leishmaniasis. Handb Clin Neurol 2013, 114, 193–198. [Google Scholar] [CrossRef]
- Melo, G.D.; Grano, F.G.; Silva, J.E.S.; Kremer, B.E.; Lima, V.M.F.; Machado, G.F. Blood-Brain Barrier Disruption during Spontaneous Canine Visceral Leishmaniasis. Parasite Immunol 2015, 37, 635–645. [Google Scholar] [CrossRef] [PubMed]
- Laskay, T.; van Zandbergen, G.; Solbach, W. Neutrophil Granulocytes--Trojan Horses for Leishmania Major and Other Intracellular Microbes? Trends Microbiol 2003, 11, 210–214. [Google Scholar] [CrossRef]
- Desjardins, M.; Descoteaux, A. Inhibition of Phagolysosomal Biogenesis by the Leishmania Lipophosphoglycan. J Exp Med 1997, 185, 2061–2068. [Google Scholar] [CrossRef]
- Lodi, L.; Voarino, M.; Stocco, S.; Ricci, S.; Azzari, C.; Galli, L.; Chiappini, E. Immune Response to Viscerotropic Leishmania: A Comprehensive Review. Front Immunol 2024, 15, 1402539. [Google Scholar] [CrossRef] [PubMed]
- Ramos, P.K.S.; Brito, M. de V.; Silveira, F.T.; Salgado, C.G.; De Souza, W.; Picanço-Diniz, C.W.; Picanço-Diniz, J.A.J. In Vitro Cytokines Profile and Ultrastructural Changes of Microglia and Macrophages Following Interaction with Leishmania. Parasitology 2014, 141, 1052–1063. [Google Scholar] [CrossRef]
- Moskowitz, N.H.; Brown, D.R.; Reiner, S.L. Efficient Immunity against Leishmania Major in the Absence of Interleukin-6. Infect Immun 1997, 65, 2448–2450. [Google Scholar] [CrossRef]
- Melo, G.D.; Machado, G.F. Glial Reactivity in Dogs with Visceral Leishmaniasis: Correlation with T Lymphocyte Infiltration and with Cerebrospinal Fluid Anti-Leishmania Antibody Titres. Cell Tissue Res 2011, 346, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Reiner, S.L.; Zheng, S.; Wang, Z.E.; Stowring, L.; Locksley, R.M. Leishmania Promastigotes Evade Interleukin 12 (IL-12) Induction by Macrophages and Stimulate a Broad Range of Cytokines from CD4+ T Cells during Initiation of Infection. J Exp Med 1994, 179, 447–456. [Google Scholar] [CrossRef]
- Ghosh, K.; Sharma, G.; Saha, A.; Kar, S.; Das, P.K.; Ukil, A. Successful Therapy of Visceral Leishmaniasis with Curdlan Involves T-Helper 17 Cytokines. J Infect Dis 2013, 207, 1016–1025. [Google Scholar] [CrossRef]
- Scott, P.; Natovitz, P.; Sher, A. B Lymphocytes Are Required for the Generation of T Cells That Mediate Healing of Cutaneous Leishmaniasis. J Immunol 1986, 137, 1017–1021. [Google Scholar] [CrossRef]
- Saha, P.; Mukhopadhyay, D.; Chatterjee, M. Immunomodulation by Chemotherapeutic Agents against Leishmaniasis. Int Immunopharmacol 2011, 11, 1668–1679. [Google Scholar] [CrossRef]
- Kamhawi, S. The Biological and Immunomodulatory Properties of Sand Fly Saliva and Its Role in the Establishment of Leishmania Infections. Microbes Infect 2000, 2, 1765–1773. [Google Scholar] [CrossRef] [PubMed]
- Engwerda, C.R.; Ato, M.; Kaye, P.M. Macrophages, Pathology and Parasite Persistence in Experimental Visceral Leishmaniasis. Trends Parasitol 2004, 20, 524–530. [Google Scholar] [CrossRef]
- Oliveira, E. de; Oshiro, E.T.; Pinto, R.V.; Castro, B.C. de; Daniel, K.B.; Oliveira, J.M. de; Júnior, M.S. da C.L.; Guimarães, E.B.; Silva, J.M.; Dorval, M.E.C. Presence of Amastigotes in the Central Nervous System of Hamsters Infected with Leishmania Sp. Rev Bras Parasitol Vet 2011, 20, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Desjeux, P.; Alvar, J. Leishmania/HIV Co-Infections: Epidemiology in Europe. Ann Trop Med Parasitol 2003, 97 Suppl 1, 3–15. [Google Scholar] [CrossRef]
- Moreira, N. das D.; Vitoriano-Souza, J.; Roatt, B.M.; Vieira, P.M. de A.; Ker, H.G.; de Oliveira Cardoso, J.M.; Giunchetti, R.C.; Carneiro, C.M.; de Lana, M.; Reis, A.B. Parasite Burden in Hamsters Infected with Two Different Strains of Leishmania (Leishmania) Infantum: “Leishman Donovan Units” versus Real-Time PCR. PLoS One 2012, 7, e47907. [Google Scholar] [CrossRef]
- Bharati, K. Human Genetic Polymorphism and Leishmaniasis. Infect Genet Evol 2022, 98, 105203. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-X.; Zhou, X.-N. Co-Infection of Tuberculosis and Parasitic Diseases in Humans: A Systematic Review. Parasit Vectors 2013, 6, 79. [Google Scholar] [CrossRef] [PubMed]
- Nweze, J.A.; Nweze, E.I.; Onoja, U.S. Nutrition, Malnutrition, and Leishmaniasis. Nutrition 2020, 73, 110712. [Google Scholar] [CrossRef] [PubMed]
- Ameen, M. Cutaneous Leishmaniasis: Advances in Disease Pathogenesis, Diagnostics and Therapeutics. Clin Exp Dermatol 2010, 35, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Maia, C.S.F.; Monteiro, M.C.; Gavioli, E.C.; Oliveira, F.R.; Oliveira, G.B.; Romão, P.R.T. Neurological Disease in Human and Canine Leishmaniasis--Clinical Features and Immunopathogenesis. Parasite Immunol 2015, 37, 385–393. [Google Scholar] [CrossRef]
- Brummitt, C.F.; Porter, J.A.; Herwaldt, B.L. Reversible Peripheral Neuropathy Associated with Sodium Stibogluconate Therapy for American Cutaneous Leishmaniasis. Clin Infect Dis 1996, 22, 878–879. [Google Scholar] [CrossRef]
- Chakroborty, N.K.; Baksi, S.; Bhattacharya, A. Cognitive Impairment in Parasitic Protozoan Infection. In Pathobiology of Parasitic Protozoa: Dynamics and Dimensions; Springer, 2023; pp. 61–94.
- Giannuzzi, A.P.; Ricciardi, M.; De Simone, A.; Gernone, F. Neurological Manifestations in Dogs Naturally Infected by Leishmania Infantum: Descriptions of 10 Cases and a Review of the Literature. J Small Anim Pract 2017, 58, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.T.M. Current Understandings on the Immunology of Leishmaniasis and Recent Developments in Prevention and Treatment. Br Med Bull 2005, 75–76, 115–130. [Google Scholar] [CrossRef]
- Kaye, P.M.; Beattie, L. Lessons from Other Diseases: Granulomatous Inflammation in Leishmaniasis. Semin Immunopathol 2016, 38, 249–260. [Google Scholar] [CrossRef]
- Petersen, C.A.; Greenlee, M.H.W. Neurologic Manifestations of Leishmania Spp. Infection. J Neuroparasitology 2011, 2, N110401. [Google Scholar] [CrossRef]
- Kumar Vaitheeswaran, K.; Gupta, B.K.; Krishnan G, R.; Soneja, M.; Vikram, N.K.; Baitha, U.; Singh, A.; Wig, N.; Azam, M.; Singh, R.; et al. Neuro-Leishmaniasis with Cauda Equina Syndrome and Cranial Nerve Palsy: A Rare Manifestation of Recurrent Atypical Visceral Leishmaniasis. BMC Infect Dis 2024, 24, 1253. [Google Scholar] [CrossRef]
- Maurício, I.L.; Stothard, J.R.; Miles, M.A. The Strange Case of Leishmania Chagasi. Parasitol Today 2000, 16, 188–189. [Google Scholar] [CrossRef]
- da Rosa, G.; Ries, A.S.; Cargnelutti, J.F.; Masuda, E.K.; Vogel, F.S.F. Detection of DNA of Leishmania Infantum in the Brains of Dogs without Neurological Signs in an Endemic Region for Leishmaniasis in the State of Rio Grande Do Sul, Brazil. Parasitol Res 2024, 123, 372. [Google Scholar] [CrossRef] [PubMed]
- Chopra, J.; Sawhney, I. Tropical Neurology. In Neurological Disorders; Elsevier, 2003; pp. 647–675.
- Arevalo, J.; Ramirez, L.; Adaui, V.; Zimic, M.; Tulliano, G.; Miranda-Verástegui, C.; Lazo, M.; Loayza-Muro, R.; De Doncker, S.; Maurer, A.; et al. Influence of Leishmania (Viannia) Species on the Response to Antimonial Treatment in Patients with American Tegumentary Leishmaniasis. J Infect Dis 2007, 195, 1846–1851. [Google Scholar] [CrossRef] [PubMed]
- Lima, V.M.F.; Gonçalves, M.E.; Ikeda, F.A.; Luvizotto, M.C.R.; Feitosa, M.M. Anti-Leishmania Antibodies in Cerebrospinal Fluid from Dogs with Visceral Leishmaniasis. Braz J Med Biol Res 2003, 36, 485–489. [Google Scholar] [CrossRef]
- Yesilova, Y.; Surucu, H.A.; Ardic, N.; Aksoy, M.; Yesilova, A.; Oghumu, S.; Satoskar, A.R. Meglumine Antimoniate Is More Effective than Sodium Stibogluconate in the Treatment of Cutaneous Leishmaniasis. J Dermatolog Treat 2016, 27, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Balasegaram, M.; Ritmeijer, K.; Lima, M.A.; Burza, S.; Ortiz Genovese, G.; Milani, B.; Gaspani, S.; Potet, J.; Chappuis, F. Liposomal Amphotericin B as a Treatment for Human Leishmaniasis. Expert Opin Emerg Drugs 2012, 17, 493–510. [Google Scholar] [CrossRef]
- Dorlo, T.P.C.; Balasegaram, M.; Beijnen, J.H.; de Vries, P.J. Miltefosine: A Review of Its Pharmacology and Therapeutic Efficacy in the Treatment of Leishmaniasis. J Antimicrob Chemother 2012, 67, 2576–2597. [Google Scholar] [CrossRef]
- Olías-Molero, A.I.; de la Fuente, C.; Cuquerella, M.; Torrado, J.J.; Alunda, J.M. Antileishmanial Drug Discovery and Development: Time to Reset the Model? Microorganisms 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Pittalis, S.; Nicastri, E.; Spinazzola, F.; Ghirga, P.; De Marco, M.; Paglia, M.G.; Narciso, P. Leishmania Infantum Leishmaniasis in Corticosteroid--Treated Patients. BMC Infect Dis 2006, 6, 177. [Google Scholar] [CrossRef]
- Purkait, B.; Kumar, A.; Nandi, N.; Sardar, A.H.; Das, S.; Kumar, S.; Pandey, K.; Ravidas, V.; Kumar, M.; De, T.; et al. Mechanism of Amphotericin B Resistance in Clinical Isolates of Leishmania Donovani. Antimicrob Agents Chemother 2012, 56, 1031–1041. [Google Scholar] [CrossRef] [PubMed]
- García-Hernández, R.; Manzano, J.I.; Castanys, S.; Gamarro, F. Leishmania Donovani Develops Resistance to Drug Combinations. PLoS Negl Trop Dis 2012, 6, e1974. [Google Scholar] [CrossRef]
- van Griensven, J.; Balasegaram, M.; Meheus, F.; Alvar, J.; Lynen, L.; Boelaert, M. Combination Therapy for Visceral Leishmaniasis. Lancet Infect Dis 2010, 10, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, R.; Chowdhury, V.; Faria, S.; Akter, S.; Dash, A.P.; Bhattacharya, S.K.; Maheswary, N.P.; Bern, C.; Akhter, S.; Alvar, J.; et al. Effect of Insecticide-Treated Bed Nets on Visceral Leishmaniasis Incidence in Bangladesh. A Retrospective Cohort Analysis. PLoS Negl Trop Dis 2019, 13, e0007724. [Google Scholar] [CrossRef]
- Sudarshani, K.; Eswaramohan, T.; Murugananthan, A.; Wegiriya, H. Peri-Domestic Risk Factors Associated with Transmission of Cutaneous Leishmaniasis in Selected Areas in Hambantota District, Sri Lanka. Ceylon Journal of Science 2023, 52, 99–105. [Google Scholar] [CrossRef]
- Costa, C.H.N. How Effective Is Dog Culling in Controlling Zoonotic Visceral Leishmaniasis? A Critical Evaluation of the Science, Politics and Ethics behind This Public Health Policy. Rev Soc Bras Med Trop 2011, 44, 232–242. [Google Scholar] [CrossRef] [PubMed]
- Polidano, K.; Wenning, B.; Ruiz-Cadavid, A.; Dawaishan, B.; Panchal, J.; Gunasekara, S.; Abebe, H.; Morais, M.; Price, H.; Dikomitis, L. Community-Based Interventions for the Prevention and Control of Cutaneous Leishmaniasis: A Systematic Review. Social Sciences 2022, 11, 490. [Google Scholar] [CrossRef]
- Van Griensven, J.; van Henten, S.; Kibret, A.; Kassa, M.; Beyene, H.; Abdellati, S.; Mersha, D.; Sisay, K.; Seyum, H.; Eshetie, H. Prediction of Visceral Leishmaniasis Development in a Highly Exposed HIV Cohort in Ethiopia Based on Leishmania Infection Markers: Results from the PreLeisH Study. EBioMedicine 2024, 110. [Google Scholar] [CrossRef]
- Balaska, S.; Khajehali, J.; Mavridis, K.; Akiner, M.; Papapostolou, K.M.; Remadi, L.; Kioulos, I.; Miaoulis, M.; Fotakis, E.A.; Chaskopoulou, A.; et al. Development and Application of Species ID and Insecticide Resistance Assays, for Monitoring Sand Fly Leishmania Vectors in the Mediterranean Basin and in the Middle East. PLoS Negl Trop Dis 2024, 18, e0012408. [Google Scholar] [CrossRef] [PubMed]
- Kedzierski, L.; Zhu, Y.; Handman, E. Leishmania Vaccines: Progress and Problems. Parasitology 2006, 133 Suppl, S87–112. [Google Scholar] [CrossRef]
- Ouellette, M.; Papadopoulou, B. Mechanisms of Drug Resistance in Leishmania. Parasitol Today 1993, 9, 150–153. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Life cycle of Leishmania species. Sand fly bites infected humans and ingests amastigotes of the parasite, which undergo maturation in the fly's gut. When the fly bites another human, promastigote form enters the bloodstream and replicates and transforms in the reticuloendothelial cells.
Figure 1.
Life cycle of Leishmania species. Sand fly bites infected humans and ingests amastigotes of the parasite, which undergo maturation in the fly's gut. When the fly bites another human, promastigote form enters the bloodstream and replicates and transforms in the reticuloendothelial cells.


Table 1.
Leishmania species.
| Species | Clinical manifestations | Geographic distribution |
|---|---|---|
| Leishmania donovani | VL | East Africa, Indian subcontinent, Middle East |
| Leishmania infantum | VL | Mediterranean, Middle East, North Africa, parts of Latin America |
| Leishmania tropica | CL | Middle East, Central Asia, North Africa |
| Leishmania braziliensis | CL & MCL | Brazil, Peru, and other parts of South America |
| Leishmania panamensis | CL | Central and South America |
| Leishmania mexicana | CL | Mexico, Central America |
| Leishmania amazonensis | CL | Brazil, South America |
| Leishmania guyanensis | CL & MCL | Amazon Basin and surrounding areas |
| Leishmania major | CL | Middle East, North Africa, Central Asia |
| Leishmania aethiopica | CL | Ethiopia, Kenya |
| Leishmania peruviana | CL | Peru, South America |
| Leishmania lainsoni | CL | Amazon Basin |
Abbreviations: CL, cutaneous leishmaniasis; MCL, mucocutaneous leishmaniasis; VL, visceral leishmaniasis.
Table 2.
Most commonly prescribed antileishmanial drugs.
| Drug | Mechanism of action | Formulation | Considerations |
|---|---|---|---|
| Pentavalent antimonials (sodium stibogluconate, meglumine antimoniate) | Inhibition of parasite glycolysis and thiol metabolism | Parenteral | Limited efficacy, potential toxicity, resistance |
| Amphotericin B | Binds to ergosterol in parasite cell membranes, leading to membrane disruption and cell death | Conventional and liposomal formulations | Broad-spectrum antifungal activity, liposomal formulations improve CNS penetration |
| Miltefosine | Inhibition of parasite cell membrane synthesis and modulation of host immune response | Oral | First oral drug for leishmaniasis. It may have limited CNS penetration. |
| Paromomycin | Inhibition of protein synthesis in Leishmania parasites | Intramuscular injection | Limited use due to parenteral administration, potential for ototoxicity |
| Pentamidine | Disruption of mitochondrial function in Leishmania parasites | Parenteral | Limited efficacy, toxicity, and availability |
| Azoles (ketoconazole, fluconazole) | Inhibition of ergosterol synthesis in Leishmania parasites | Oral | Broad-spectrum antifungal activity, limited efficacy against Leishmania species |
| Sitamaquine | Inhibition of parasite oxidative phosphorylation | Oral | Limited availability and use due to side effects |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



