
Submitted:
03 December 2024
Posted:
04 December 2024
You are already at the latest version
Abstract
Background/Objectives: Breast cancer-related lymphedema (BCRL) is one of the major morbidity in breast cancer. Since lymphedema treatment is difficult, especially once it progresses, screening and early detection should be prioritized to prevent the progression. This study used indocyanine green lymphography (ICG-L) as a sensitive diagnostic tool for BCRL screening after axillary lymph node dissection (ALND). Methods: This prospective cohort study included breast cancer patients who underwent ALND from October 2022 to October 2024 at Dharmais National Cancer Hospital. ICG-L was performed to diagnose BCRL. Our study outcome was a 2-year BCRL cumulative incidence and ICG-L stage distribution. Results: This study included 69 patients with a mean body mass index of 26.3±5.1 kg/m2. The median (IQR) of dissected lymph nodes was 18 (14-21), with the number of lymph node metastases 2 (0-10). Forty-six patients (66.7%) were in the locally advanced stage and 42 (60.9%) received radiotherapy. Based on ICG-L, our 2-year BCRL cumulative incidence was 58.0% (45.2-71.4). A total of 25 patients (71.4%) who had BCRL experienced symptoms, with heaviness (60%) and swelling (48%) being the most common signs. The upper extremity lymphedema index increase of > 10 % was only found in 11 (31.4%) patients. Most patients were in ICG-L stage II, as shown in 18 (51.4%) subjects. Conclusions: ICG-L was able to detect early BCRL more frequently. This finding showed its sensitivity as a screening method and that it should be used in preventive BCRL management.
Keywords:
axillary lymph node dissection
; breast cancer-related lymphedema
; immediate lymphatic reconstruction
; indocyanine green lymphography
1. Introduction
Breast cancer-related lymphedema (BCRL) is one of the significant morbidity in breast cancer patients, with a cumulative incidence of 10-50% [1,2,3]. Axillary lymph node dissection (ALND) is considered the major contributing treatment risk factor besides radiotherapy and chemotherapy [4,5,6]. Indonesia's breast cancer population is centered at a locally advanced stage [7]. Therefore, ALND is still commonly performed, which increases the risk of BCRL [5,8]. We believe that prioritizing screening and early detection is essential to preventive care [9,10,11].
Several studies show methods for BCRL diagnosis, such as clinical symptoms, relative arm volume increase (RAVI), water volumetry, lymphoscintigraphy, bioimpedance spectroscopy (BIS), and perometry [8,12,13]. Among those methods, the most commonly used are 1) clinical symptoms such as swelling and heaviness, 2) RAVI of 10%, and 3) BIS, which is frequently used for screening (48%) [14,15,16]. However, BIS has a false negative rate of 25% compared to volume displacement measurement. Moreover, bioimpedance spectroscopy is related to a lower positive predictive value (34%) than perometry (54%) [13,16]. Therefore, a more sensitive measurement is needed for BCRL screening.
Indocyanine green lymphography (ICG-L) is currently considered the most sensitive diagnostic tool for lymphedema as it has high sensitivity compared to lymphoscintigraphy or BIS [17,18]. Therefore, ICG-L has previously been used for BCRL diagnosis in several studies [19,20]. One of the advantages of ICG-L is the ability to show in real-time the normal (linear pattern) and abnormal (dermal backflow pattern) lymphatic function. The dermal backflow (DB) pattern consists of splash, stardust, and diffuse pattern [21]. Splash pattern is the earliest ICG-L finding in asymptomatic patients and becomes the hallmark of lymphedema early signs [22].
In Indonesia, diagnostic modalities for BCRL are not widely provided. For example, lymphoscintigraphy is unavailable in every hospital, and no BIS technology exists in Indonesia. Currently, we use clinical symptoms, upper extremity lymphedema (UEL) index, and ICG-L for diagnostic modalities [23]. To our knowledge, only a few studies investigating BCRL incidence using ICG-L [19]. Therefore, our study aims to analyze BCRL cumulative incidence and ICG-L stage among breast cancer patients with ALND.
2. Materials and Methods
2.1. Study Design and Subjects
This prospective cohort study was conducted among breast cancer patients with ALND at Dharmais Cancer Hospital from October 2022 to October 2024. The institutional review board approved the study. The inclusion criteria were breast cancer patients aged >18 years old with ECOG score >1, clinically node-positive, and with or without neoadjuvant systemic therapy. We excluded patients with previous breast and axillary surgeries, radiotherapy, preoperative abnormal lymphatic drainage detected by ICG-L, and patients with iodine allergy, asthma, decreased kidney function, pregnancy, and lactation.
2.2. Surgical Technique
Breast cancer surgery was performed with standard mastectomy or lumpectomy technique. The ALND was done at level I and II, if necessary level III axillary region. During surgery, we collected lymphatic speciments for histopathological assessment which was described previously in our study [24].
2.3. ICG Lymphography Examination
The ICG-L procedure was carried out before and after the surgery as per the scheduled time. We used ICG dye (Premix Indocyanine Green USP 0.5%) that was injected subcutaneously (@0.1 ml) at the second and fourth web spaces of the hand and the ulnar border of the palmaris longus tendon at the wrist joint level. Superficial lymphatic circulation was assessed at 5 minutes (transient phase) and 2 hours (plateau phase).
At this point, we determined the ICG-L stages that is classified as follows: stage 0, the linear pattern only; stage I, linear and splash patterns; stage II, linear and stardust/diffuse pattern in one region; stage III, linear and stardust/diffuse pattern in two regions; stage IV, linear and stardust/diffuse pattern in three regions; stage V, stardust and/or diffuse pattern [25].
BCRL was defined by the presence of minimum ICG-L stage II in area of at least 30% in each arm region, with or without clinical symptoms and UEL index >10%.
2.4. Follow-up and Outcomes
We evaluated the patients’ clinical symptoms, UEL index, and ICG-L every two months in the first year and three months in the second year. The study outcome were 2-years BCRL cumulative incidence and ICG-L stage proportion.
2.5. Statistical Analysis
Numerical data was presented in mean ± SD if normally distributed or median (IQR) if not normally distributed, while categorical data was shown as n (%). Two years-BCRL cumulative incidence were analyzed using Kaplan-Meier survival analysis. Data analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 27.0.
3. Results
In two years, 69 patients were included in this study. The median (IQR) age was 47 (40-54) years, and the mean±SD BMI was 26.3±5.1 kg/m2. There were 46 patients (66.7%) in the locally advanced stage with mastectomy as the common surgery type in 53 patients (76.8%). ALND was performed most frequently on lymph node level I-II in 51 patients (73.9%), although 18 patients (26.1%) underwent ALND level I-III. Radiotherapy was given to 42 patients (60.9%), chemotherapy to 64 patients (93.8%), and hormonal therapy to 49 patients (71%).
The median (IQR) dissected lymph node was 18 (14-21), with the number of lymph node metastases 2 (0-10). There were 16 patients (23.2%) with lymph vessel obstruction, which already occurred during surgery. A total of 66 patients (95.7%) were presented with no special type (NST) histopathology, with luminal B as the most frequent subtype in 26 patients (37.7%). Demographic data of the study subjects are summarized in Table 1.
BCRL occurred in 35 (50.7%) patients with a 2-year cumulative incidence of 58.0% (45.2-71.4) and a median (95% CI) cumulative incidence 16.0 (11.2-20.8) months as shown in Figure 1. Table 2 shows that 25 BCRL patients experienced symptoms (71.4%). The most common signs were heaviness in 15 (60%) and swelling in 12 patients (48%). The UEL index increment > 10 % was only discovered in 11 patients (31.4%). Most BCRL patients had ICG-L stage II, as shown in 18 (51.4%) subjects. The ICG-L stage distribution and clinical features are presented in Table 2 and Figure 2, respectively. In those without lymphedema, ICG-L Stage I or splash pattern occurred in 24 subjects (71%).
4. Discussion
The subjects in our study had a high risk of developing BCRL because they had high BMI, received radiotherapy, greater number of dissected lymph nodes, and had a high frequency of lymph node metastasis. Based on theoretical understanding, obesity is a systemic condition that impacts the lymphatic system. Fat deposition in the organs of obese patients leads to structural, metabolic, and inflammatory changes, which contribute to lymphatic system dysfunction [26,27].
Since most of our patients were in a locally advanced stage, they needed adjuvant radiotherapy. Radiotherapy causes lymphatic vessel fibrosis, which increases the risk of lymphedema after ALND [28]. Radiation exposure upregulates the endothelial nitric oxide synthase expression, which leads to the production of nitric oxide and decreases lymphatic vessel contractility. In addition, radiation induces the release of pro-inflammatory cytokines such as TGF-β, which give rise to fibrosis of the lymphatic vessels that leads to BCRL [6,29,30,31].
The majority of our patients also had a high number of dissected lymph nodes. Furhtermore, around 30% of our subjects experienced ALND level I-III. Extensive axillary lymph node removal may damage the lymphatic system of the upper limb [32]. As a result, a series of inflammation can occur that will cause fibrosis and BCRL [5,33]. Therefore, the risk of lymphedema directly correlates with the number of lymph nodes removed [32]. Kilbreath et al. study revealed that retrieval of more than five lymph nodes accounted for a higher incidence of lymphedema (18.2%) compared to less than five lymph nodes (3.3%) [34]. A study by Di Sipio et al. also showed that a high number of lymph nodes dissected is also a risk factor [8].
Histopathological examination of the lymphatic vessel exhibited that 23% of them experienced hypertrophy and fibrosis of the tunica media as well as narrowing of the lumen. This finding can be associated with lymph node metastasis and extracapsular extension, leading to lymphatic flow obstruction. As a result, it increases intraluminal pressure, thickens the lumen wall, and obstructs the lymphatic vessels [35,36]. Our data shows that early-stage lymphatic vessel obstruction can occur before ALND without signs of lymphatic system abnormalities or lymphedema symptoms. If this condition is not treated immediately, BCRL will eventually occur.
The BCRL cumulative incidence is commonly reported to be between 20-30% [8], but with variation between 10-50% [1,2,3]. Differences in measurement methods, length of follow-up, and types of study design could explain the variability of the incidence. The 2-year BCRL cumulative incidence in our study was 58%. It exhibited a higher BCRL proportion that is commonly reported (20-30%) [8]. The difference can be explained by the fact that the previous studies commonly defined lymphedema by symptoms and arm volume measurement [8], which is a less sensitive method [16]. Since ICG-L is more sensitive to diagnosing lymphedema, therefore, the 2-year BCRL cumulative incidence in our study is relatively high.
Since curing lymphedema is difficult once it progresses [9,37], choosing the most sensitive tool to detect early-stage lymphedema is the key to effective BCRL prevention. ICG-L screening in our study provides evidence that BCRL can be diagnosed in an early stage. This was indicated by the following findings: 1) BCRL was detected before the symptoms occurred in 30% of patients; 2) The UEL index increased by more than 10% was only found in 30% of patients; and 3). Fifty-one percent of the participants were diagnosed with ICG-L stage II. Moreover, 71% of patients without lymphedema had ICG-L stage I or splash pattern, which showed early signs of lymphatic abnormalities [22]. Therefore, in accordance with other studies, we recommend ICG-L for BCRL screening since it is sensitive to diagnose lymphedema before the onset of clinical symptoms and arm volume changes.
Our study supports BCRL preventive management through screening and early detection so that early intervention can be initiated. There are several methods for lymphedema prevention; the first one is conservative treatment using compression therapy [38,39]. Recent randomized controlled trials verify the efficacy of compression sleeves after ALND to prevent BCRL. However, it requires long-term usage, which causes low adherence in some patients [40,41,42]. Hence, compression therapy adherence poses a challenge that may limit the risk-reduction strategy of BCRL [43]. This opinion may correspond with the situation in Indonesia; moreover, compression sleeve garments are not covered by public insurance.
The second preventive intention is to utilize immediate lymphatic reconstruction (ILR), which has emerged as the primary prevention for BCRL [2,44,45]. The concept of ILR using lymphaticovenous anastomosis (LVA) has also been used for secondary prevention of lymphedema [46,47]. Yamamoto et al. utilized efferent lymphatic vessel anastomosis when lymphedema was still in the subclinical stage (splash pattern). The technique prevented lymphedema progression, as shown by the reduction from splash to linear pattern [47]. Our previous study also showed that LVA could prevent BCRL progression when detected in the early stage, even before the surgery was performed [48]. Hence, based on those studies, our findings support BCRL screening with ICG-L since it can detect lymphedema in the early stage. Therefore, immediate intervention such as compression therapy or LVA can be deployed to prevent lymphedema progression.
We are aware that our study has limitations. Transient and subclinical lymphedema could be counted in our BCRL definition. But, the key to prevention is to find lymphedema as early as possible. This can only be performed by ICG-L since it detects early changes in lymphatic circulation. Another limitation is our short follow-up time; therefore, the long-term delayed onset of BCRL cannot yet be evaluated. Longer follow-up time is needed. Despite this, we found that ICG-L is a sensitive diagnostic tool for BCRL screening and early detection.
5. Conclusions
Based on ICG-L analysis, BCRL can be detected more frequently and at an early stage. This highlights the high sensitivity of ICG-L as a screening diagnostic tool. Such findings emphasize its value in initiating timely interventions to prevent the progression of lymphedema. Therefore, we recommend ICG-L for BCRL screening and early detection in breast cancer patients with ALND.
Author Contributions
Conceptualization, B.B., T.Y., and S.S.P.; methodology, B.B. and K.H.; software, P.A.Y. and P.S.P.; validation, S.S.P., S.J.H. and A.T.; formal analysis, B.B., R.I.P., and K.H.; investigation, B.B. and R.I.P.; resources, B.B. and R.I.P.; data curation, B.B. and R.I.P; writing—original draft preparation, B.B. and T.Y.; review, S.J.H., P.A.Y., and A.T.; supervision, T.Y., S.S.P., S.J.H., K.H., and A.T. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by research funding from Islamic Development Bank (IsDB) 2024.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Dharmais Cancer Hospital – National Cancer Center (227/KEPK/IX/2022, 19 September 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Further information on the data collected can be sought from the
Authors (B.B.).
Acknowledgments
The authors wish to thank Faza Soelaeman MD, Maghfira Maura MD, and Adhitya Bayu Perdana for their encouragement and support on this project, especially for manuscript preparation.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Boccardo, F.M.; Ansaldi, F.; Bellini, C.; Accogli, S.; Taddei, G.; Murdaca, G.; Campisi, C.; Villa, G.; Icardi, G.; Durando, P.; et al. Prospective evaluation of a prevention protocol for lymphedema following surgery for breast cancer. Lymphology 2009, 42, 1–9. [Google Scholar] [PubMed]
- Hahamoff, M.; Gupta, N.; Munoz, D.; Lee, B.T.; Clevenger, P.; Shaw, C.; Spiguel, L.; Singhal, D. A Lymphedema Surveillance Program for Breast Cancer Patients Reveals the Promise of Surgical Prevention. J. Surg. Res. 2018, 244, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Ciudad, P.; Escandón, J.M.; Bustos, V.P.; Manrique, O.J.; Kaciulyte, J. Primary Prevention of Cancer-Related Lymphedema Using Preventive Lymphatic Surgery: Systematic Review and Meta-analysis. Indian J. Plast. Surg. 2022, 55, 018–025. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Hoskin, T.L.; Habermann, E.B.; Cheville, A.L.; Boughey, J.C. Breast Cancer-Related Lymphedema Risk is Related to Multidisciplinary Treatment and Not Surgery Alone: Results from a Large Cohort Study. Ann. Surg. Oncol. 2017, 24, 2972–2980. [Google Scholar] [CrossRef] [PubMed]
- McDuff, S.G.R.; Mina, A.I.; Brunelle, C.L.; Salama, L.; et al. Timing of Lymphedema After Treatment for Breast Cancer: When Are Patients Most At Risk? Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 62–70. [Google Scholar] [CrossRef]
- Kwon, S.; Janssen, C.F.; Velasquez, F.C.; Zhang, S.; Aldrich, M.B.; Shaitelman, S.F.; DeSnyder, S.M.; Sevick-Muraca, E.M. Radiation Dose-Dependent Changes in Lymphatic Remodeling. Int. J. Radiat. Oncol. 2019, 105, 852–860. [Google Scholar] [CrossRef]
- Setyawan, I.B.; Kurnia, D.; Setiaji, K.; Anwar, S.L.; Purwanto, D.J.; Azhar, Y.; Budijitno, S.; Suprabawati, D.G.A.; Priyono, S.H.; Siregar, B.A.; et al. Sociodemographic disparities associated with advanced stages and distant metastatic breast cancers at diagnosis in Indonesia: a cross-sectional study. Ann. Med. Surg. 2023, 85, 4211–4217. [Google Scholar] [CrossRef]
- DiSipio, T.; Rye, S.; Newman, B.; Hayes, S. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 2013, 14, 500–515. [Google Scholar] [CrossRef]
- Agarwal, S.; Garza, R.M.; Chang, D.W. Lymphatic Microsurgical Preventive Healing Approach (LYMPHA) for the prevention of secondary lymphedema. Breast J. 2019, 26, 721–724. [Google Scholar] [CrossRef]
- Silva, A.K.; Chang, D.W. Vascularized lymph node transfer and lymphovenous bypass: Novel treatment strategies for symptomatic lymphedema. J. Surg. Oncol. 2016, 113, 932–939. [Google Scholar] [CrossRef]
- Dayan, J.H.; Ly, C.L.; Kataru, R.P.; Mehrara, B.J. Lymphedema: Pathogenesis and Novel Therapies. Annu Rev Med 2018, 69, 263–276. [Google Scholar] [CrossRef] [PubMed]
- Brunelle, C.L.; Taghian, A.G. Lymphoedema screening: setting the standard. Br. J. Cancer 2020, 123, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Barrio, A.V.; Eaton, A.; Frazier, T.G. A Prospective Validation Study of Bioimpedance with Volume Displacement in Early-Stage Breast Cancer Patients at Risk for Lymphedema. Ann. Surg. Oncol. 2015, 22, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Gursen, C.; Dylke, E.S.; Moloney, N.; Meeus, M.; De Vrieze, T.; Devoogdt, N.; De Groef, A. Self-reported signs and symptoms of secondary upper limb lymphoedema related to breast cancer treatment: Systematic review. Eur. J. Cancer Care 2021, 30, e13440. [Google Scholar] [CrossRef]
- Rafn, B.S.; Christensen, J.; Larsen, A.; Bloomquist, K. Prospective Surveillance for Breast Cancer–Related Arm Lymphedema: A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2022, 40, 1009–1026. [Google Scholar] [CrossRef]
- Bundred, N.; Foden, P.; Todd, C.; Morris, J.; Watterson, D.; Purushotham, A.; Bramley, M.; Riches, K.; Hodgkiss, T.; et al.; the Investigators of BEA/PLACE studies Increases in arm volume predict lymphoedema and quality of life deficits after axillary surgery: a prospective cohort study. Br. J. Cancer 2020, 123, 17–25. [Google Scholar] [CrossRef]
- Qin, E.S.; Bowen, M.J.; Chen, W.F. Diagnostic accuracy of bioimpedance spectroscopy in patients with lymphedema: A retrospective cohort analysis. J. Plast. Reconstr. Aesthetic Surg. 2018, 71, 1041–1050. [Google Scholar] [CrossRef]
- Mihara, M.; Hara, H.; Araki, J.; Kikuchi, K.; Narushima, M.; Yamamoto, T.; Iida, T.; Yoshimatsu, H.; Murai, N.; Mitsui, K.; et al. Indocyanine Green (ICG) Lymphography Is Superior to Lymphoscintigraphy for Diagnostic Imaging of Early Lymphedema of the Upper Limbs. PLOS ONE 2012, 7, e38182. [Google Scholar] [CrossRef]
- Akita, S.; Nakamura, R.; Yamamoto, N.; Tokumoto, H.; Ishigaki, T.; Yamaji, Y.; Sasahara, Y.; Kubota, Y.; Mitsukawa, N.; Satoh, K. Early Detection of Lymphatic Disorder and Treatment for Lymphedema following Breast Cancer. Plast. Reconstr. Surg. 2016, 138, 192e–202e. [Google Scholar] [CrossRef]
- Soran, A.; Bengur, F.B.; Rodriguez, W.; Chroneos, M.Z.; Sezgin, E. Early Detection of Breast Cancer-Related Lymphedema: Accuracy of Indocyanine Green Lymphography Compared with Bioimpedance Spectroscopy and Subclinical Lymphedema Symptoms. Lymphat. Res. Biol. 2023, 21, 359–365. [Google Scholar] [CrossRef]
- Yamamoto, T.; Azuelos, A. Near-Infrared Based Technologies. In Supermicrosurgical Lymphatico Venular Anastomosis: A Practical Textbook; Visconti, G., Hayashi, A., Eds.; Lulu, 2020; pp. 1–404. [Google Scholar]
- Yamamoto, T.; Matsuda, N.; Doi, K.; Oshima, A.; Yoshimatsu, H.; Todokoro, T.; Ogata, F.; Mihara, M.; Narushima, M.; Iida, T.; et al. The Earliest Finding of Indocyanine Green Lymphography in Asymptomatic Limbs of Lower Extremity Lymphedema Patients Secondary to Cancer Treatment. Plast. Reconstr. Surg. 2011, 128, 314e–321e. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Yamamoto, N.; Hara, H.; Mihara, M.; Narushima, M.; Koshima, I. Upper Extremity Lymphedema Index. Ann. Plast. Surg. 2013, 70, 47–49. [Google Scholar] [CrossRef] [PubMed]
- Brahma, B.; Putri, R.I.; Reuwpassa, J.O.; Tuti, Y.; Alifian, M.F.; Sofyan, R.F.; Iskandar, I.; Yamamoto, T. Lymphaticovenular Anastomosis in Breast Cancer Treatment-Related Lymphedema: A Short-Term Clinicopathological Analysis from Indonesia. J. Reconstr. Microsurg. 2021, 37, 643–654. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Yamamoto, N.; Kageyama, T.; Sakai, H.; Fuse, Y.; Tsuihiji, K.; Tsukuura, R. Technical pearls in lymphatic supermicrosurgery. Glob. Heal. Med. 2020, 2, 29–32. [Google Scholar] [CrossRef]
- Savetsky, I.L.; Torrisi, J.S.; Cuzzone, D.A.; Ghanta, S.; Albano, N.J.; Gardenier, J.C.; Joseph, W.J.; Mehrara, B.J. Obesity increases inflammation and impairs lymphatic function in a mouse model of lymphedema. Am. J. Physiol. Circ. Physiol. 2014, 307, H165–H172. [Google Scholar] [CrossRef]
- Blum, K.S.; Karaman, S.; Proulx, S.T.; Ochsenbein, A.M.; Luciani, P.; Leroux, J.-C.; Wolfrum, C.; Detmar, M. Chronic High-Fat Diet Impairs Collecting Lymphatic Vessel Function in Mice. PLOS ONE 2014, 9, e94713. [Google Scholar] [CrossRef]
- Straub, J.M.; New, J.; Hamilton, C.D.; Lominska, C.; Shnayder, Y.; Thomas, S.M. Radiation-induced fibrosis: mechanisms and implications for therapy. J. Cancer Res. Clin. Oncol. 2015, 141, 1985–1994. [Google Scholar] [CrossRef]
- Avraham, T.; Daluvoy, S.; Zampell, J.; Yan, A.; Haviv, Y.S.; Rockson, S.G.; Mehrara, B.J. Blockade of Transforming Growth Factor-β1 Accelerates Lymphatic Regeneration during Wound Repair. Am. J. Pathol. 2010, 177, 3202–3214. [Google Scholar] [CrossRef]
- Clavin, N.W.; Avraham, T.; Fernandez, J.; Daluvoy, S.V.; et al. TGF-β 1 is a negative regulator of lymphatic regeneration during wound repair. Am. J. Physiol.-Heart Circ. Physiol. 2008, 295, H2113–H2127. [Google Scholar] [CrossRef]
- Nelson, T.S.; Nepiyushchikh, Z.; Hooks, J.S.T.; Razavi, M.S.; Lewis, T.; Clement, C.C.; Thoresen, M.; Cribb, M.T.; Ross, M.K.; Gleason, R.L.; et al. Lymphatic remodelling in response to lymphatic injury in the hind limbs of sheep. Nat. Biomed. Eng. 2019, 4, 649–661. [Google Scholar] [CrossRef]
- Hara, Y.; Otsubo, R.; Shinohara, S.; Morita, M.; Kuba, S.; Matsumoto, M.; Yamanouchi, K.; Yano, H.; Eguchi, S.; Nagayasu, T. Lymphedema After Axillary Lymph Node Dissection in Breast Cancer: Prevalence and Risk Factors—A Single-Center Retrospective Study. Lymphat. Res. Biol. 2022, 20, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Warren, A.G.; Brorson, H.; Borud, L.J.; Slavin, S.A. Lymphedema. Ann Plast Surg 2007, 59, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Kilbreath, S.; Refshauge, K.; Beith, J.; Ward, L.; Ung, O.; Dylke, E.; French, J.; Yee, J.; Koelmeyer, L.; Gaitatzis, K. Risk factors for lymphoedema in women with breast cancer: A large prospective cohort. Breast 2016, 28, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Invernizzi, M.; Corti, C.; Lopez, G.; Michelotti, A.; Despini, L.; Gambini, D.; Lorenzini, D.; Guerini-Rocco, E.; Maggi, S.; Noale, M.; et al. Lymphovascular invasion and extranodal tumour extension are risk indicators of breast cancer related lymphoedema: an observational retrospective study with long-term follow-up. BMC Cancer 2018, 18, 935. [Google Scholar] [CrossRef]
- Iyigun, Z.E.; Duymaz, T.; Ilgun, A.S.; Alco, G.; Ordu, C.; Sarsenov, D.; Aydin, A.E.; Celebi, F.E.; Izci, F.; Eralp, Y.; et al. Preoperative Lymphedema-Related Risk Factors in Early-Stage Breast Cancer. Lymphat. Res. Biol. 2018, 16, 28–35. [Google Scholar] [CrossRef]
- Johnson, A.R.; Singhal, D. Immediate lymphatic reconstruction. J. Surg. Oncol. 2018, 118, 750–757. [Google Scholar] [CrossRef]
- Lasinski, B.B. Complete Decongestive Therapy for Treatment of Lymphedema. Semin. Oncol. Nurs. 2013, 29, 20–27. [Google Scholar] [CrossRef]
- Ezzo, J.; Manheimer, E.; McNeely, M.L.; Howell, D.M.; Weiss, R.; I Johansson, K.; Bao, T.; Bily, L.; Tuppo, C.M.; Williams, A.F.; et al. Manual lymphatic drainage for lymphedema following breast cancer treatment. Cochrane Database Syst. Rev. 2015, 2015, CD003475–CD003475. [Google Scholar] [CrossRef]
- Paramanandam, V.S.; Dylke, E.; Clark, G.M.; Daptardar, A.A.; Kulkarni, A.M.; Nair, N.S.; Badwe, R.A.; Kilbreath, S.L. Prophylactic Use of Compression Sleeves Reduces the Incidence of Arm Swelling in Women at High Risk of Breast Cancer–Related Lymphedema: A Randomized Controlled Trial. J. Clin. Oncol. 2022, 40, 2004–2012. [Google Scholar] [CrossRef]
- Ochalek, K.; Gradalski, T.; Partsch, H. Preventing Early Postoperative Arm Swelling and Lymphedema Manifestation by Compression Sleeves After Axillary Lymph Node Interventions in Breast Cancer Patients: A Randomized Controlled Trial. J. Pain Symptom Manag. 2017, 54, 346–354. [Google Scholar] [CrossRef]
- Ochalek, K.; Partsch, H.; Gradalski, T.; Szygula, Z. Do Compression Sleeves Reduce the Incidence of Arm Lymphedema and Improve Quality of Life? Two-Year Results from a Prospective Randomized Trial in Breast Cancer Survivors. Lymphat. Res. Biol. 2019, 17, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Paskett, E.D.; Le-Rademacher, J.; Oliveri, J.M.; Liu, H.; Seisler, D.K.; Sloan, J.A.; Armer, J.M.; Naughton, M.J.; Hock, K.; Schwartz, M.; et al. A randomized study to prevent lymphedema in women treated for breast cancer: CALGB 70305 (Alliance). Cancer 2020, 127, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Coriddi, M.; Mehrara, B.; Skoracki, R.; Singhal, D.; Dayan, J.H. Immediate Lymphatic Reconstruction: Technical Points and Literature Review. Plast. Reconstr. Surg.- Glob. Open 2021, 9, e3431. [Google Scholar] [CrossRef] [PubMed]
- Boccardo, F.; Casabona, F.; De Cian, F.; Friedman, D.; Villa, G.; Bogliolo, S.; Ferrero, S.; Murelli, F.; Campisi, C. Lymphedema Microsurgical Preventive Healing Approach: A New Technique for Primary Prevention of Arm Lymphedema After Mastectomy. Ann. Surg. Oncol. 2009, 16, 703–708. [Google Scholar] [CrossRef] [PubMed]
- Akita, S.; Mitsukawa, N.; Kuriyama, M.; Hasegawa, M.; Kubota, Y.; Tokumoto, H.; Ishigaki, T.; Hanaoka, H.; Satoh, K. Suitable therapy options for sub-clinical and early-stage lymphoedema patients. J. Plast. Reconstr. Aesthetic Surg. 2014, 67, 520–525. [Google Scholar] [CrossRef]
- Yamamoto, T.; Yamamoto, N.; Yamashita, M.; Furuya, M.; Hayashi, A.; Koshima, I. Efferent Lymphatic Vessel Anastomosis. Ann. Plast. Surg. 2016, 76, 424–427. [Google Scholar] [CrossRef]
- Brahma, B.; Yamamoto, T.; Agdelina, C.; Adella, D.; Putri, R.I.; Hanifah, W.; Sundah, V.H.; Perdana, A.B.; Putra, M.R.A.; Taher, A.; et al. Immediate-delayed lymphatic reconstruction after axillary lymph nodes dissection for locally advanced breast cancer-related lymphedema prevention: Report of two cases. Microsurgery 2023, 44, e31033. [Google Scholar] [CrossRef]
Figure 1.
Two-years BCRL cumulative incidence.
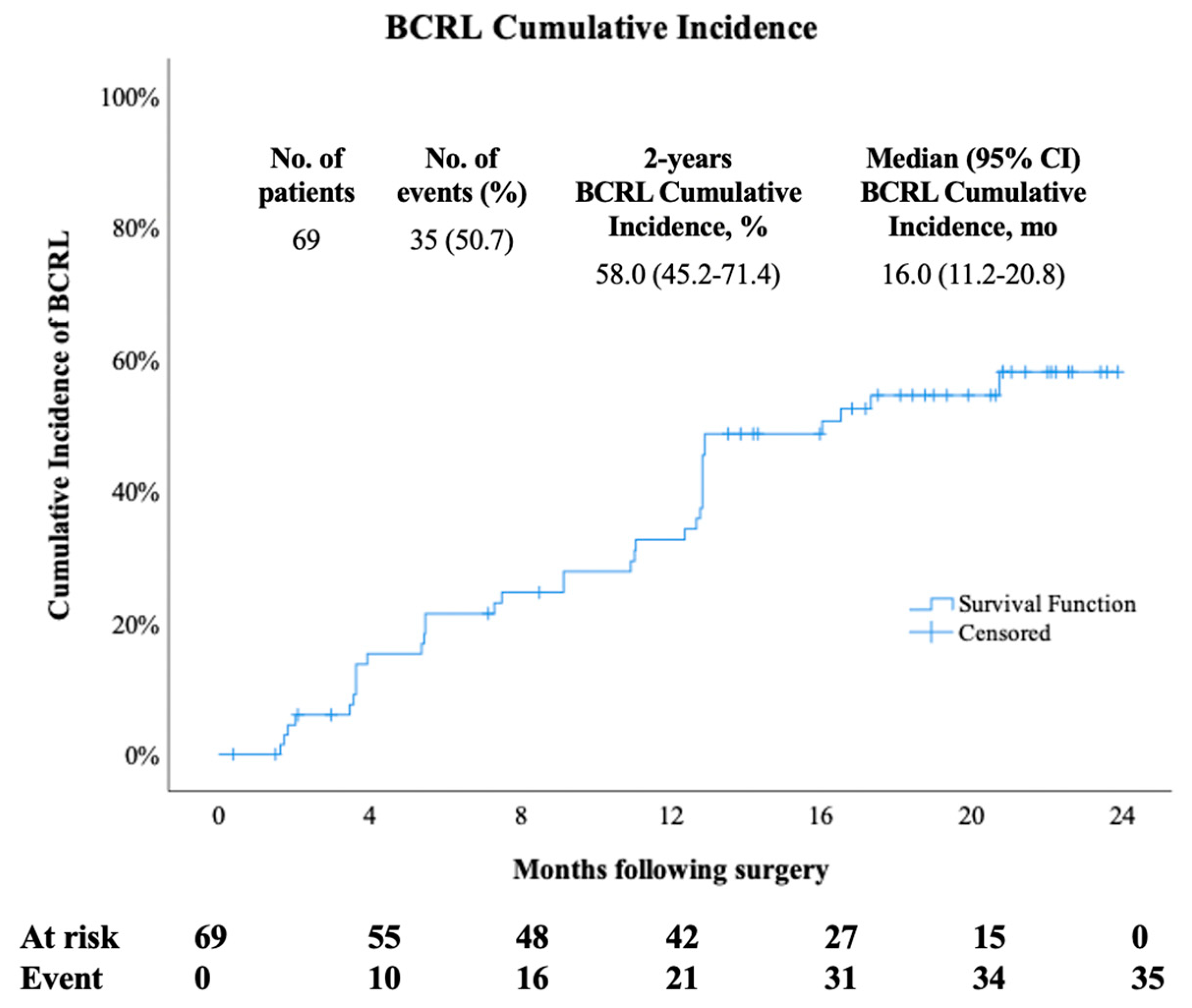
Figure 2.
BCRL clinical and ICG-L image; (A) ICG-L stage II; (B) ICG-L stage III; (C) ICG-L stage IV. *DB pattern showing stardust and diffuse pattern.
Figure 2.
BCRL clinical and ICG-L image; (A) ICG-L stage II; (B) ICG-L stage III; (C) ICG-L stage IV. *DB pattern showing stardust and diffuse pattern.
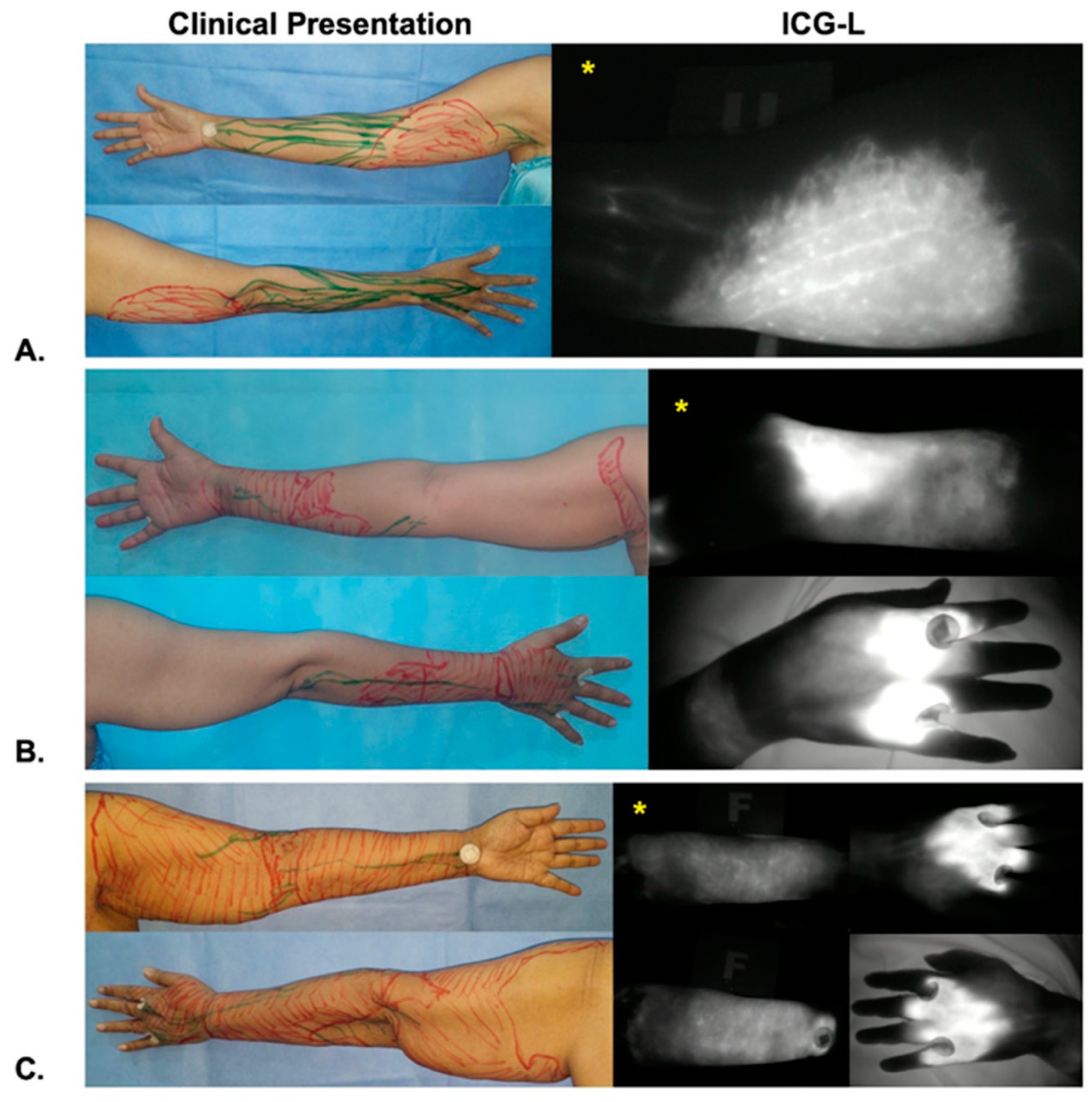

Table 1.
Characteristics of the patients.
| Variable | Patients, no (%) n=69 |
|---|---|
| Age, median (IQR), years | 47.0 (40.0-54.0) |
| BMI, mean± SD kg/m2 | 26.3 ± 5.1 |
| Breast cancer stage | |
| II A | 11 (15.9) |
| II B | 8 (11.6) |
| III A | 15 (21.7) |
| III B | 15 (21.7) |
| III C | 16 (23.2) |
| IV | 4 (5.8) |
| Breast surgery | |
| Mastectomy | 53 (76.8) |
| BCS | 15 (21.7) |
| Wide excision | 1 (1.4) |
| ALND Level | |
| I-II | 51 (73.9) |
| I-III | 18 (26.1) |
| Radiotherapy | |
| Yes | 42 (60.9) |
| No | 27 (39.1) |
| Chemotherapy | |
| Yes | 64 (93.8) |
| No | 5 (7.2) |
| Hormonal therapy | |
| Yes | 49 (71.0) |
| No | 20 (29.0) |
| Dissected Lymph Nodes, median (IQR) | 18 (14-21) |
| Lymph Nodes Metastases, median (IQR) | 2 (0-10) |
| Lymph Vessel Obstruction | |
| Yes | 16 (23.2) |
| No | 52 (75.4) |
| Missing | 1 (1.4) |
| Histopathology Feature | |
| NST | 66 (95.7) |
| Lobular | 1 (1.4) |
| Others | 2 (2.9) |
| Breast Cancer Subtype | |
| Luminal A | 4 (5.8) |
| Luminal B HER2- | 17 (24.6) |
| Luminal B HER2+ | 9 (13) |
| HER2+ | 18 (26.1) |
| TNBC | 21 (30.4) |
ALND= axillary lymph node dissection; BCRL= breast cancer-related lymphedema; BCS= breast conserving surgery; BMI= body mass index; UEL= upper extremity lymphedema; HER2= human epidermal growth factor receptor 2, NST= no special type, TNBC= triple negative breast cancer.
Table 2.
Characteristics of BCRL
| Variable | Patients, n (%) N = 35 |
|---|---|
| Symptoms | |
| Yes | 25 (71.4) |
| Heaviness | 15 (60) |
| Swelling | 12 (48) |
| Pain | 6 (24) |
| No | 10 (28.6) |
| UEL Index percentage difference > 10% | |
| Yes | 11 (31.4) |
| No | 24 (68.6) |
| ICG-L Stage at Onset | |
| II | 18 (51.4) |
| III | 14 (40.0) |
| IV | 3 (8.6) |
* BCRL = breast cancer-related lymphedema; ICG-L= indocyanine green lymphography; UEL = upper extremity lymphedema.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



