
Submitted:
14 July 2025
Posted:
16 July 2025
You are already at the latest version
Abstract
Background. Sentinel lymph node biopsy (SLNB) has traditionally been used to stage the axilla in early-stage breast cancer. However, its utility in women over 70 with hormone receptor-positive tumors and negative axillary imaging is increasingly questioned due to limited therapeutic benefit and potential complications.
Objectives. To assess the feasibility of omitting SLNB in women aged 70 and older with clinically node-negative, luminal-type breast cancer. Eligible patients were selected based on normal axillary ultrasound findings.
Methods. A retrospective analysis was conducted on women aged 70 and above with histologically confirmed invasive breast cancer, negative axillary imaging, and surgery between January 2021 and December 2024. All underwent SLNB. We examined demographics, clinical characteristics, surgical outcomes, and oncological variables such as recurrence and mortality.
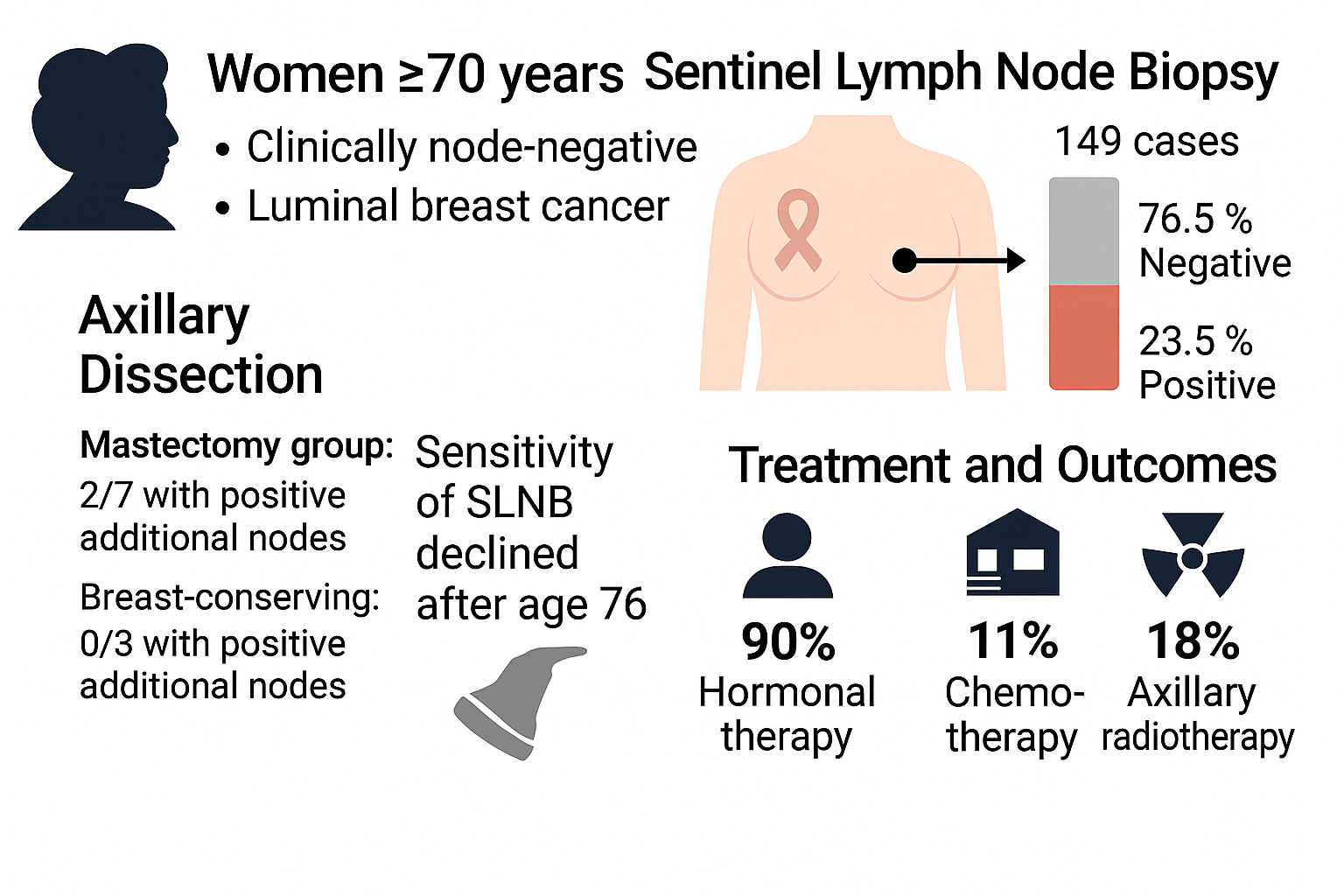
Results. A total of 149 women underwent surgery, with a mean age of 77.2 years. SLNB was positive in 23.5% of cases, but only 6.7% required axillary dissection. Sensitivity and specificity of SLNB declined notably after age 76. No axillary or breast recurrences were reported. Most patients (89.9%) received hormonal therapy, while 11.4% had chemotherapy and 17.5% axillary radiotherapy. Outpatient management was feasible in 87.9% of cases, and no clinically significant lymphedema was observed.
Conclusions. Omitting SLNB in women ≥70 years with luminal breast cancer and negative axillary imaging appears safe and does not compromise oncological outcomes. This strategy minimizes surgical risks and enhances quality of life, supporting a more tailored and less invasive approach to axillary management in older patients.
Keywords:
breast cancer
; sentinel lymph node
; elderly women
; axillary staging
; hormone receptor-positive
; de-escalation
1. Introduction
Breast cancer (BC), whose incidence increases with age, is the most common malignancy in women, with more than 30% of diagnoses occurring in women over the age of 70 [1].
Sentinel lymph node biopsy (SLNB) has traditionally been the standard procedure for axillary staging in patients with early-stage BC, allowing the identification of regional lymph node involvement with lower morbidity than complete axillary lymph node dissection [2]. However, in recent years, the necessity of performing this procedure in elderly patients has been questioned due to its limited impact on overall survival and its constrained influence on therapeutic decision-making [3].
In this regard, recent studies have investigated the feasibility of omitting SLNB in women over 70 years of age with luminal-type BC and clinically and sonographically negative axillae at diagnosis. Consequently, the Choosing Wisely initiative recommends avoiding SLNB in these patients, as the information obtained does not significantly alter the therapeutic approach in the majority of cases (1). Indeed, data from the NAFTA trial (North American Fareston versus Tamoxifen Adjuvant Trial) [4], which included 1813 postmenopausal women with hormone receptor-positive invasive BC, and the International Breast Cancer Study Group Trial 10-93 [5], have shown that omitting axillary evaluation does not affect overall survival or locoregional recurrence in women with early-stage disease [3]. These findings have fuelled ongoing debate about the necessity of SLNB in this patient subgroup [6].
Analysis of large cohort data and clinical trials has revealed that the rate of nodal involvement in patients with sonographically negative axillae ranges between 10% and 15% [3], suggesting that a significant proportion of women could avoid surgical intervention without compromising their prognosis. Furthermore, studies such as that by Marco Sanz et al. [7] have indicated that omitting SLNB in this patient group does not affect recurrence rates or overall survival, thereby supporting the use of axillary ultrasound as a primary staging tool, eliminating the need for intraoperative SLNB.
Despite these recommendations, more than 80% of women over the age of 70 continue to undergo SLNB [1]. Contributing factors include clinical inertia, concerns about potential undertreatment, and variability in risk perception among oncologists [1,3]. Nevertheless, evidence suggests that even when SLNB is omitted, the rate of subsequently detected nodal involvement remains low and does not substantially alter the requirement for adjuvant therapy [7]. Additionally, the impact on quality of life is significant, as omitting SLNB reduces the risk of lymphoedema, chronic pain, and arm dysfunction in elderly patients [6].
Against this background, our aim was to analyse our recent outcomes in patients over 70 years of age with breast cancer and a sonographically negative axilla, in order to evaluate the feasibility of omitting sentinel lymph node biopsy (SLNB) in this population. We hypothesised that, in the absence of suspicious findings on axillary ultrasound, SLNB may be safely avoided, potentially reducing surgical morbidity without compromising the oncologic management of breast cancer in older women.
This study seeks to contribute to the ongoing discussion regarding the optimisation of BC management in elderly patients, by exploring strategies that minimise unnecessary interventions while preserving treatment effectiveness and enhancing quality of life.
2. Materials and Methods
A retrospective study based on a prospective database was conducted including all patients aged 70 years or older with a diagnosis of breast cancer (BC) who underwent surgery at our centre between January 2021 and December 2024. Informed consent was waived as the study was retrospective and based on anonymised data.
Inclusion criteria:
- Age ≥70 years.
- Histologically confirmed diagnosis of invasive breast carcinoma.
- Negative axillary status confirmed by axillary ultrasound, magnetic resonance imaging (MRI), or positron emission tomography–computed tomography (PET-CT). Patients with suspicious imaging findings but negative preoperative biopsy (vacuum-assisted biopsy [VAB] or core needle biopsy [CNB]) were also included.
- No neoadjuvant treatment.
- Patients who underwent either mastectomy or breast-conserving surgery.
- Patients in whom sentinel lymph node biopsy (SLNB) was performed.
Exclusion criteria:
- Patients who did not undergo surgical intervention.
- Lack of axillary assessment via SLNB.
Preoperative assessment included clinical examination, bilateral mammography, and bilateral breast and axillary ultrasound. In selected cases, MRI and PET-CT were also performed. Suspicious lesions identified on imaging were confirmed histologically by VAB or CNB. In cases with suspicious axillary lymph nodes, VAB or CNB was carried out to confirm the absence of metastasis prior to surgery. Surgical procedures included mastectomy or breast-conserving surgery via lumpectomy, as well as SLNB.
The variables analysed included demographic characteristics, functional status based on the American Society of Anesthesiologists (ASA) classification, histological and molecular tumour features, axillary assessment through imaging, history of prior BC, and any neoadjuvant treatment received. Regarding surgery, we analysed the type of surgical intervention, SLNB (including the number of affected lymph nodes), axillary clearance, pathological nodal staging, and whether surgery was performed as an outpatient procedure. Additionally, data on subsequent treatments were collected, including adjuvant breast and axillary radiotherapy, adjuvant hormone therapy, and adjuvant chemotherapy. Axillary and breast recurrence, as well as mortality, were also evaluated.
2.1. Statistical Analysis:
Continuous variables were expressed as mean and standard deviation (SD) if normally distributed, or as median and interquartile range (IQR) if non-normally distributed. Categorical variables were described using absolute and relative frequencies (n and percentage). Normality of continuous variables was assessed using the Shapiro–Wilk test. Comparisons between groups for continuous variables were performed using Student’s t-test for normally distributed variables, or the Mann–Whitney U test for non-normally distributed variables. Categorical variables were compared using the chi-squared test or Fisher’s exact test when expected frequencies were less than 5. A p-value < 0.05 was considered statistically significant. Statistical analysis was performed using RStudio, version 2024.12.0+467.
3. Results
A total of 149 patients with breast cancer (BC) and clinically negative axillae were included. The mean age was 77.19 ± 5.24 years. The vast majority were women (99.33%; n=148). Regarding ASA classification, 77.18% (n=115) of the patients were classified as ASA II. A history of prior breast cancer was recorded in 12.75% (n=19) of patients (Table 1).
The most frequent histological type was invasive carcinoma of no special type (NST) (n=87, 58.39%). In terms of histological grade, 70.47% of tumours (n=105) were classified as grade II. Regarding tumour size, 45.64% (n=68) measured between 10 mm and 20 mm (T1c), followed by 24.83% (n=37) measuring between 20 mm and 50 mm (T2). The predominant molecular subtype was luminal (85.91%; n=128) (Table 2).
As for surgical approach, 98 patients (65.77%) underwent breast-conserving surgery, while 51 (34.23%) underwent mastectomy. Sentinel lymph node positivity was observed in 23.49% (n=35) of patients, of whom 20 (57.14%) had macrometastases. Axillary lymph node dissection (ALND) was performed in 10 patients (6.71%) (Figure 1). No cases of breast or axillary recurrence were identified.
Regarding adjuvant treatment, 68.46% (n=102) received breast radiotherapy, and 17.45% (n=26) received axillary radiotherapy. Hormone therapy was administered to 134 patients (89.93%), while only 17 (11.41%) received adjuvant chemotherapy (Table 3).
The overall mortality rate was 1.34% (n=2), and 87.92% (n=131) were managed on an outpatient basis without requiring hospitalisation.
3.1. Analysis by Type of Surgery:
3.1.1. Mastectomy Group:
Sentinel lymph node positivity was observed in 16 patients (31.37%). Of these, 9 had micrometastases and did not undergo ALND. Among the remaining 7 patients, the distribution of sentinel lymph node findings was as follows (Figure 2):
- 3 patients with one macrometastasis (2 of whom had no additional positive nodes on ALND).
- 4 patients with two or more macrometastases, all of whom had additional positive lymph nodes on ALND. In this subgroup, 100% of patients who underwent ALND had further nodal involvement.
Notably, all patients in the mastectomy group had tumours smaller than T3 (Table 4).
3.1.2. Breast-Conserving Surgery Group:
Sentinel lymph node positivity was observed in 19 cases (19.39%). ALND was performed in 3 patients (15.79%), while the remainder did not undergo further dissection, in accordance with the ACOSOG Z0011 trial criteria (8). Of the patients who underwent ALND, only one had an additional positive node. This patient had a macrometastatic sentinel node (total tumour load: 1,200,000 copies) (Figure 3).
Although the rate of positive nodes was higher in the mastectomy group compared to the breast-conserving group, the difference in sentinel lymph node positivity between the two groups was not statistically significant (p=0.1517).
3.1.3. Sensitivity and Specificity Analysis of Sentinel Node According to Age:
A receiver operating characteristic (ROC) curve (Figure 4) was constructed to evaluate the sensitivity and specificity of sentinel lymph node positivity in relation to age. It was observed that, from the age of 76 onwards, both sensitivity and specificity decreased significantly, reaching values of 57.14% and 53.95%, respectively (Table 5).
4. Discussion
The surgical approach to treating breast cancer (BC) in women over the age of 70—particularly those with luminal tumours and clinically negative axillae—has shifted towards a de-escalation strategy. This trend is supported by growing evidence indicating that invasive procedures such as sentinel lymph node biopsy (SLNB) may be unnecessary in selected cases. This consideration is especially relevant in older patients and is becoming increasingly accepted, particularly beyond the age of 80 (9,10). In our series, the nodal involvement rate was 23.49%. Studies such as that by Panadés et al. [11] report that women over 70 often present with larger, more advanced tumours, resulting in less frequent axillary surgical management—SLNB was performed in only 69.10% of cases. This highlights the importance of personalising treatment strategies based on comorbidities and life expectancy, without compromising disease control [11].
One of the most notable findings of our study was the marked decrease in the sensitivity (57.14%) and specificity (53.95%) of SLNB in patients over the age of 76—a phenomenon not yet widely reported in the literature. This reduced diagnostic performance aligns with increasing interest in omitting axillary procedures in the elderly. In a large retrospective analysis, Minami et al. [12] found that 50.9% of women aged 70 or older with luminal tumours received a de-escalated treatment, omitting axillary surgery and/or radiotherapy. Importantly, 35.3% of the variation in this practice was attributable to regional factors, such as institutional protocols and clinical preferences, while only 2.8% was explained by individual patient characteristics [13]. Similarly, Wang et al. [14], in a qualitative study, observed that 73% of women interviewed would prefer to omit radiotherapy if it did not improve survival, while 40% opted for SLNB, considering it low-risk and offering them “peace of mind” [15]. These findings underscore the need to individualise therapeutic decisions for older women, taking into account not only the real diagnostic value of SLNB but also patient preferences, comorbidities, and regional context.
When comparing types of surgery, we observed a 31.37% rate of nodal positivity in mastectomy cases versus 19.39% in breast-conserving surgery, though the difference was not statistically significant (p = 0.1517). Previous research has also shown higher rates of nodal positivity among patients undergoing mastectomy, likely reflecting a selection bias for larger or more aggressive tumours [6,16,17].
In patients with two or more macrometastases, all (100%) had additional nodal involvement on axillary lymph node dissection, reinforcing the conclusions of the ACOSOG Z0011 trial, which suggested that ALND should be reserved for patients with high nodal burden [5,8]. Studies by Chagpar et al. [18] and Esposito et al. [19] also support omitting ALND in patients with micrometastases or minimal involvement, given the lack of significant differences in survival or locoregional control [18,19,20].
At the systemic level, 89.93% of our patients received hormone therapy, while only 11.41% underwent chemotherapy. This trend aligns with current evidence suggesting that nodal status has limited impact on chemotherapy decisions for older women with luminal BC [21]. Treatment decisions should be guided more by tumour biology and functional status than by nodal involvement [22,23,24]. Axillary radiotherapy was administered in 17.45% of cases, with no locoregional recurrences reported. The PRIME II trial demonstrated that omitting radiotherapy is safe in older women with hormone receptor-positive tumours and negative margins receiving adjuvant endocrine therapy [25,26].
Our data also support the functional safety of avoiding axillary surgery: no clinically significant cases of lymphoedema or sensory disturbance were reported. Given that advanced age increases the risk of postoperative complications, surgical de-escalation offers a clear functional benefit [9,27].
From an organisational perspective, 87.92% of patients were managed on an outpatient basis. McEvoy et al. [28] highlight the benefits of reduced hospital stay and cost savings from omitting SLNB, particularly in high-volume surgical centres. From an economic standpoint, the cost-effectiveness of SLNB in elderly women with negative axillae is questionable. Hrebinko et al. [29] conducted a cost-effectiveness analysis showing that omitting SLNB not only reduces healthcare costs but also improves quality-adjusted life years (QALYs) in women over 70 with luminal BC and no clinical evidence of nodal involvement—supporting the notion that conservative surgical selection is not only safe and effective, but also more efficient in public health terms [29].
Minami et al. [12] also reported substantial institutional variability in SLNB practices, linked to resource availability and surgical team expertise [12,13,30]. Despite the recommendations of scientific societies such as the SSO and Choosing Wisely, systematic implementation remains challenging. In many centres, SLNB continues to be performed by default, without an individualised risk–benefit assessment [3,16].
Nevertheless, patient acceptance is high when adequate information is provided. The literature shows that most older women would prefer to avoid axillary surgery when it offers no clinical benefit, emphasising the importance of shared decision-making [21].
Alamoodi et al. [31] stress that de-escalation not only improves quality of life, but may also reduce psychological complications by avoiding interventions that heighten postoperative anxiety and fear. Carleton et al. [32] found that omitting SLNB has no impact on overall or disease-free survival and allows therapeutic strategies to focus on more relevant systemic treatments.
Chagpar et al. [18] further highlighted the evolution of surgical practice over the past fifteen years, showing that omission of SLNB is now common in academic centres with multidisciplinary teams. Jatoi et al. [25] provide a critical review of the history, indications, and future of SLNB, calling for a reassessment of its value in older women with early-stage BC.
Several studies also report that the rate of clinically significant nodal involvement is very low in older women, supporting the omission of SLNB in this group. Even in cases of micrometastases, clinical progression is uncommon in women receiving adequate hormonal therapy, while the risk of lymphoedema increases with unnecessary ALND [33]. In short, survival benefits are limited in comparison to the negative impact on quality of life [34].
Despite growing expert consensus on the need to de-escalate treatment in older women with luminal BC, few prospective studies have focused on this group. The study by Chung et al. [35] provides compelling data: among 125 women aged over 65 with ER+ BC treated with breast-conserving surgery without SLNB, the three-year axillary recurrence rate was 1.60% and the overall survival rate was 94.80%, even though only 48% were still on endocrine therapy after two years. These findings offer robust evidence supporting omission of SLNB in this population.
Beyond clinical outcomes, the debate has evolved through contributions from molecular biology. Reimer et al. [36] point out that the prognostic value of nodal status in clinically node-negative patients is now surpassed by information derived from tumour subtype and genomic profiling [37]. This challenges the utility of SLNB as a decision-making tool for adjuvant therapy. Similarly, the meta-analysis by Kell et al. [38] concluded that, while SLNB is less invasive than ALND, its clinical benefit is questionable when nodal risk is low and systemic therapy is already indicated based on other tumour characteristics.
In this context, Lewis et al. [39] demonstrated excellent survival outcomes with tamoxifen and toremifene in postmenopausal women with early-stage luminal BC, reinforcing the importance of endocrine therapy. Additionally, tumour size below 1 cm remains one of the best predictors of nodal negativity, supporting the decision to omit SLNB in patients with small tumours [40].
Data on women over the age of 80 provide an even more radical yet meaningful perspective. In the study by Acosta et al. [10], none of the 36 patients who did not undergo axillary intervention developed axillary recurrence. Disease-free survival reached 80.99% and overall survival 57% at five years, despite most patients receiving only breast surgery and endocrine therapy.
The recent INSEMA trial prospectively examined the omission of SLNB in women with early-stage BC (cN0) undergoing breast-conserving surgery plus radiotherapy. Results showed no significant differences in disease-free or locoregional recurrence, strongly supporting reduced axillary surgical management in appropriately selected patients [36].
Similarly, Li X [14] observed that practice in many European hospitals remains driven by protocol rather than clinical judgement, despite mounting evidence favouring less interventionist approaches. In patients with imaging-negative axillae, omitting SLNB does not increase locoregional recurrence or reduce survival, particularly in women over 70 with luminal tumours and low Ki-67 [41]. Williams et al. [42] concluded that eliminating intraoperative tools such as frozen section analysis reduces overtreatment and streamlines surgery without compromising oncological control.
Hu X et al. [43] proposed a preoperative nomogram to predict nodal involvement in BC patients. This model showed good discriminatory power and could help avoid SLNB in older women with low-risk clinical features, thus contributing to a more personalised surgical de-escalation.
In summary, our findings support the growing body of evidence indicating that omission of SLNB is safe, efficient, and clinically appropriate for women over 70 with luminal tumours, negative imaging of the axilla, and appropriate systemic treatment. Personalised approaches, shared decision-making, and proper clinical selection are key to advancing towards less invasive and more value-centred surgery.
5. Conclusions
Our research highlights a growing agreement that skipping sentinel lymph node biopsy is a safe and sensible choice for women aged 70 and older who have luminal breast cancer and negative axillary imaging. The low rates of axillary recurrence, the minimal need for axillary dissection, and the ease of managing patients on an outpatient basis all support a shift towards a more conservative strategy for this group. Additionally, the decreased effectiveness of SLNB in patients over 76, along with the limited influence of nodal status on systemic therapy choices, raises questions about the routine use of axillary staging in these cases.
This study was specifically designed to assess whether SLNB omission could be a viable strategy in our local setting, aiming to evaluate its true clinical utility. Based on our findings, a progressive change in clinical practice is currently underway at our institution, moving toward the omission of SLNB in this age group when appropriate clinical and radiological criteria are met. This transition reflects a broader shift toward personalized, less invasive, and value-based surgical management in elderly breast cancer patients.
Author Contributions
All authors contributed substantially to the conception and design of the study, data collection, analysis and interpretation, as well as the drafting and critical revision of the manuscript. All authors have approved the final version and agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to thank the Breast Unit at Hospital Clínico Universitario de Valencia for their support throughout this study. We also wish to express our appreciation to the Departments of Oncology, Radiology, and Pathology for their collaboration and contribution to the multidisciplinary management of the patients included.
Ethical Considerations
This study was conducted in accordance with the ethical standards of the institutional research committee and the 1964 Helsinki Declaration and its later amendments. Ethical approval was obtained from the Ethics Committee of Hospital Clínico Universitario de Valencia. Given the retrospective nature of the study and the anonymisation of patient data, informed consent was not required.
Conflict of Interest
The authors declare that they have no conflict of interest related to the content of this manuscript.
References
- Minami CA, Bryan AF, Freedman RA, Revette AC, Schonberg MA, King TA, et al. Assessment of Oncologists’ Perspectives on Omission of Sentinel Lymph Node Biopsy in Women 70 Years and Older with Early-Stage Hormone Receptor-Positive Breast Cancer. JAMA Netw Open. 2022;5(8): e2228524. [CrossRef]
- Sevensma KE, Lewis CR. Axillary sentinel lymph node biopsy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. PMID: 31985977.
- Boughey JC, Haffty BG, Habermann EB, Hoskin TL, Goetz MP. Has the Time Come to Stop Surgical Staging of the Axilla for All Women Age 70 Years or Older with Hormone Receptor-Positive Breast Cancer? Ann Surg Oncol. 2017;24(3):614-17. [CrossRef]
- Vogel CL, Johnston MA, Capers C, Braccia D. Toremifene for breast cancer: A review of 20 years of data. Clin Breast Cancer. 2014;14(1):1-9. [CrossRef]
- Rudenstam CM, Zahrieh D, Forbes JF, Crivellari D, Holmberg SB, Rey P, et al. Randomized trial comparing axillary clearance versus no axillary clearance in older patients with breast cancer: First results of International Breast Cancer Study Group trial 10-93. J Clin Oncol. 2006;24(3):337-44. [CrossRef]
- Heidinger M, Maggi N, Dutilh G, Mueller M, Eller RS, Loesch JM, et al. Use of sentinel lymph node biopsy in elderly patients with breast cancer – 10-year experience from a Swiss university hospital. World J Surg Oncol. 2023;21(1). [CrossRef]
- Marco Sanz L, del Olmo Bautista S, Sánchez Quirós H, Pérez Martínez Y, Gutiérrez García S, Palomo Cabañes V, et al. Breast cancer in patients aged over 80 years: Primary treatment. Revista de Senologia y Patologia Mamaria. 2025;38(3). [CrossRef]
- Giuliano AE, Ballman K V., McCall L, Beitsch PD, Brennan MB, Kelemen PR, et al. Effect of axillary dissection vs no axillary dissection on 10-year overall survival among women with invasive breast cancer and sentinel node metastasis: The ACOSOG Z0011 (Alliance) randomized clinical trial. JAMA. 2017;318(10):918–26. [CrossRef]
- Qualina Abreu PE, González Pereira S. Breast cancer in patients over 70 years of age: Clinical presentation, histopathological features and therapeutic approach in Argentina. Rev Argent Mastol. 2019;38(140):58–81.
- Acosta M V, Acosta F V, Ramírez C AK, Marín E, Contreras A, Longobardi I, et al. Breast cancer in patients over 80 years of age: Are we still performing sentinel lymph node biopsy? Rev Venez Oncol. 2024;36(4):212–21.
- Pijuan i Panadés N, Nogueiras Pérez R, Gumí Caballero I, López Mestres A, Medina Argemi S, Ramírez Pujadas A, et al. Do women with breast cancer older than 70 years receive equal treatment to younger women? Rev Senol Patol Mamar. 2020;33(2):50–6. [CrossRef]
- Minami CA, Jin G, Freedman RA, Schonberg MA, King TA, Mittendorf EA. Physician-level variation in axillary surgery in older adults with T1N0 hormone receptor-positive breast cancer: A retrospective population-based cohort study. J Geriatr Oncol. 2024 Jun 1;15(5). [CrossRef]
- Minami CA, Dey T, Chen YJ, Freedman RA, Lorentzen EH, King TA, et al. Regional Variation in Deescalated Therapy in Older Adults With Early-Stage Breast Cancer. JAMA Netw Open. 2024;7(10):e2441152. [CrossRef]
- Li X, Wang L, Wang Y, Ma L, Zheng R, Ding J, et al. Omission of sentinel lymph node biopsy in patients with clinically axillary lymph node-negative early breast cancer (OMSLNB): protocol for a prospective, non-inferiority, single-arm, phase II clinical trial in China. BMJ Open. 2024;14(9):e087700. [CrossRef]
- Wang T, Mott N, Miller J, Berlin NL, Hawley S, Jagsi R, et al. Patient Perspectives on Treatment Options for Older Women with Hormone Receptor-Positive Breast Cancer: A Qualitative Study. JAMA Netw Open. 2020;3(9). [CrossRef]
- Castelo M, Hansen BE, Paszat L, Baxter NN, Scheer AS. Omission of Axillary Staging and Survival in Elderly Women With Early Stage Breast Cancer. Ann Surg Open. 2022;3(2):e159. [CrossRef]
- Fitzal F, Helfgott R, Moinfar F, Gnant M. Sized Influences Nodal Status in Women Aged #70 with Endocrine Responsive Breast Cancer. Ann Surg Oncol. 2017;24(Suppl 3):555-6. [CrossRef]
- Chagpar AB, McMasters KM, Edwards MJ. Can sentinel node biopsy be avoided in some elderly breast cancer patients? Ann Surg. 2009;249(3):455–60. [CrossRef]
- Esposito E, Di Micco R, Gentilini OD. Sentinel node biopsy in early breast cancer. A review on recent and ongoing randomized trials. Breast. 2017;36:14-9. [CrossRef]
- Luo SP, Zhang J, Wu Q Sen, Lin YX, Song CG. Association of Axillary Lymph Node Evaluation With Survival in Women Aged 70 Years or Older With Breast Cancer. Front Oncol. 2021;10:596545. [CrossRef]
- Davey MG, Kerin EP, McLaughlin RP, Barry MK, Malone CM, Elwahab SA, et al. Evaluating the Necessity for Routine Sentinel Lymph Node Biopsy in Postmenopausal Patients Being Treated for Clinically Node Negative Breast Cancer the Era of RxPONDER. Clin Breast Cancer. 2023;23(5):500–7. [CrossRef]
- Lee J, Noh J, Jeong JY. Oncological outcomes of omitting sentinel lymph node biopsy in elderly patients with breast cancer. Asian J Surg. 2020;43(11):1090-2. [CrossRef]
- Daly GR, Dowling GP, Said M, Qasem Y, Hembrecht S, Calpin GG, et al. Impact of Sentinel Lymph Node Biopsy on Management of Older Women With Clinically Node-Negative, Early-Stage, ER+/HER2−, Invasive Breast Cancer: A Systematic Review and Meta-Analysis. Clin Breast Cancer. 2024;24(8):e681-8.e1. [CrossRef]
- Pilewskie M, Sevilimedu V, Eroglu I, Le T, Wang R, Morrow M, et al. How Often Do Sentinel Lymph Node Biopsy Results Affect Adjuvant Therapy Decisions Among Postmenopausal Women with Early-Stage HR+/HER2− Breast Cancer in the Post-RxPONDER Era? Ann Surg Oncol. 2022;29(10):6267–73. [CrossRef]
- Jatoi I, Kunkler IH. Omission of sentinel node biopsy for breast cancer: Historical context and future perspectives on a modern controversy. Cancer. 2021;127(23):4376-83. [CrossRef]
- Kunkler IH et al. Breast-conserving surgery with or without irradiation in women aged 65 years or older with early breast cancer (PRIME II): a randomised controlled trial. Lancet Oncol. 2015;16(3):266–73. [CrossRef]
- Wang T, Baskin A, Miller J, Metz A, Matusko N, Hughes T, et al. Trends in Breast Cancer Treatment De-Implementation in Older Patients with Hormone Receptor-Positive Breast Cancer: A Mixed Methods Study. Ann Surg Oncol. 2021;28(2):902–13. [CrossRef]
- McEvoy AM, Poplack S, Nickel K, Olsen MA, Ademuyiwa F, Zoberi I, et al. Cost-effectiveness analyses demonstrate that observation is superior to sentinel lymph node biopsy for postmenopausal women with HR + breast cancer and negative axillary ultrasound. Breast Cancer Res Treat. 2020;183(2):251-62. [CrossRef]
- Hrebinko KA, Bryce CL, Downs-Canner S, Diego EJ, Myers SP. Cost-effectiveness of Choosing Wisely guidelines for axillary observation in women older than age 70 years with hormone receptor–positive, clinically node-negative, operable breast tumors. Cancer. 2022;128(12):2258–68. [CrossRef]
- Piñero Madrona A, Giménez J, Merck B, Vázquez C. Consensus meeting on selective biopsy of the sentinel node in breast cancer. Spanish Society of Senology and Breast Disease. Rev Esp Med Nucl. 2007;26(3):176-80. [CrossRef]
- Alamoodi M, Wazir U, Mokbel K, Patani N, Varghese J, Mokbel K. Omitting Sentinel Lymph Node Biopsy after Neoadjuvant Systemic Therapy for Clinically Node Negative HER2 Positive and Triple Negative Breast Cancer: A Pooled Analysis. Cancers (Basel). 2023;15(13): 3325. [CrossRef]
- Carleton N, Zou J, Fang Y, Koscumb SE, Shah OS, Chen F, et al. Outcomes after Sentinel Lymph Node Biopsy and Radiotherapy in Older Women with Early-Stage, Estrogen Receptor-Positive Breast Cancer. JAMA Netw Open. 2021;4(4). [CrossRef]
- Rebaza Vasquez LP, Ponce de la Torre J, Alarco R, Ayala Moreno J, Gomez Moreno H. Axillary management in early-stage breast cancer with upfront surgery and positive sentinel lymph node. ecancermedicalscience. 2021;15:1193. [CrossRef]
- Tuttle TM, Hui JYC, Yuan J. Omitting Sentinel Lymph Node Biopsy in Elderly Patients: A Lost Opportunity? Vol. 28, Annals of Surgical Oncology. Ann Surg Oncol. 2021;28(9):5442-3. [CrossRef]
- Chung AP, Dang CM, Karlan SR, Amersi FF, Phillips EM, Boyle MK, et al. A Prospective Study of Sentinel Node Biopsy Omission in Women Age ≥ 65 Years with ER+ Breast Cancer. Ann Surg Oncol. 2024;31(5):3160–7. [CrossRef]
- Reimer T. Omission of axillary sentinel lymph node biopsy in early invasive breast cancer. Breast. 2023;67:124–8. [CrossRef]
- Reimer T, Stachs A, Veselinovic K, Kühn T, Heil J, Polata S et al. Axillary Surgery in Breast Cancer - Primary Results of the INSEMA Trial. N Engl J Med. 2025;392(11):1051-64. [CrossRef]
- Kell MR, Burke JP, Barry M, Morrow M. Outcome of axillary staging in early breast cancer: A meta-analysis. Breast Cancer Res Treat. 2010;120(2):441–7. [CrossRef]
- Lewis JD, Chagpar AB, Shaughnessy EA, Nurko J, McMasters K, Edwards MJ. Excellent outcomes with adjuvant toremifene or tamoxifen in early stage breast cancer. Cancer. 2010;116(10):2307–15. [CrossRef]
- Fitzal F, Helfgott R, Moinfar F, Gnant M. Sized Influences Nodal Status in Women Aged #70 with Endocrine Responsive Breast Cancer. Ann Surg Oncol. 2017;24(Suppl 3):555-6. [CrossRef]
- Reimer T, Engel J, Schmidt M, Offersen BV, Smidt ML, Gentilini OD. Is Axillary Sentinel Lymph Node Biopsy Required in Patients Who Undergo Primary Breast Surgery? Breast Care (Basel). 2018;13(5):324-30. [CrossRef]
- Williams AD, Khan AJ, Sevilimedu V, Barrio A V., Morrow M, Mamtani A. Omission of Intraoperative Frozen Section May Reduce Axillary Overtreatment Among Clinically Node-Negative Patients Having Upfront Mastectomy. Ann Surg Oncol. 2022;29(13):8037–43. [CrossRef]
- Hu X, Xue J, Peng S, Yang P, Yang Z, Yang L, et al. Preoperative Nomogram for Predicting Sentinel Lymph Node Metastasis Risk in Breast Cancer: A Potential Application on Omitting Sentinel Lymph Node Biopsy. Front Oncol. 2021;11:665240. [CrossRef]
Figure 1.
Violin plot illustrating the distribution of sentinel lymph node positivity.
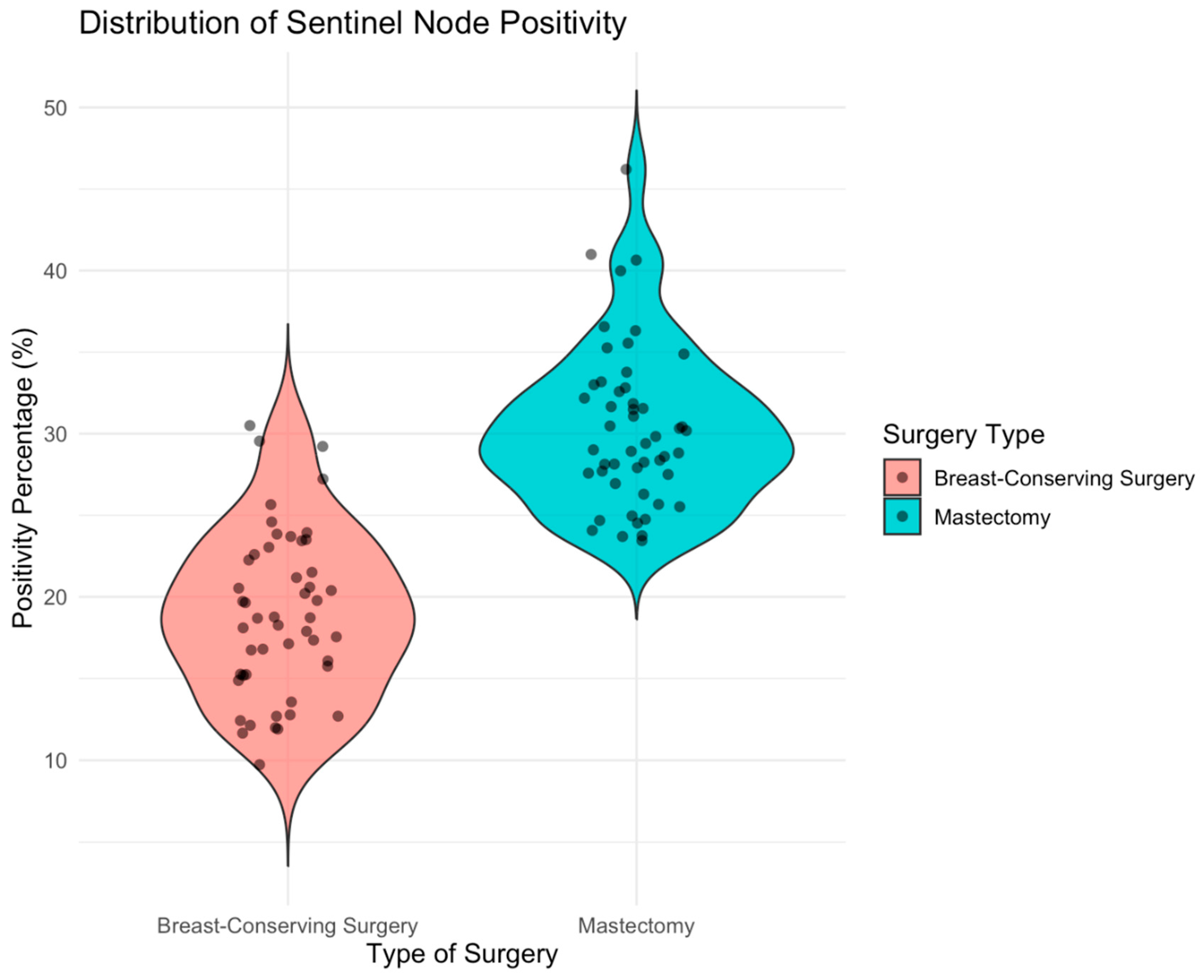
Figure 2.
Flowchart showing the distribution of axillary dissection outcomes in mastectomy patients with positive sentinel lymph node biopsy meeting criteria for axillary dissection. SN: Sentinel Node, ALND: Axillary Lymph Node Dissection.
Figure 2.
Flowchart showing the distribution of axillary dissection outcomes in mastectomy patients with positive sentinel lymph node biopsy meeting criteria for axillary dissection. SN: Sentinel Node, ALND: Axillary Lymph Node Dissection.
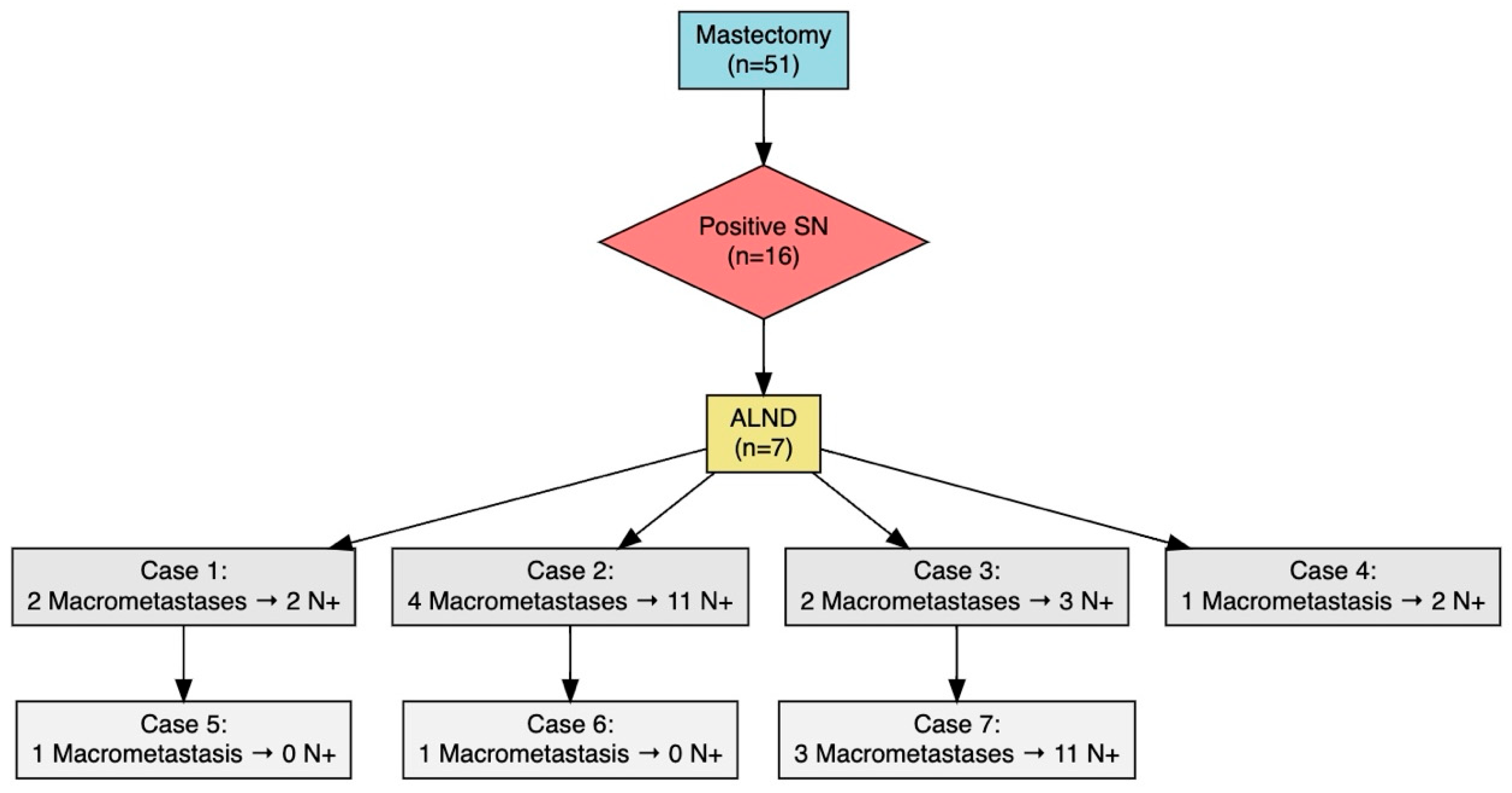
Figure 3.
Flowchart showing the distribution of axillary dissection outcomes in patients undergoing breast-conserving surgery with positive sentinel lymph node biopsy meeting criteria for axillary dissection. SN: Sentinel Node, ALND: Axillary Lymph Node Dissection.
Figure 3.
Flowchart showing the distribution of axillary dissection outcomes in patients undergoing breast-conserving surgery with positive sentinel lymph node biopsy meeting criteria for axillary dissection. SN: Sentinel Node, ALND: Axillary Lymph Node Dissection.
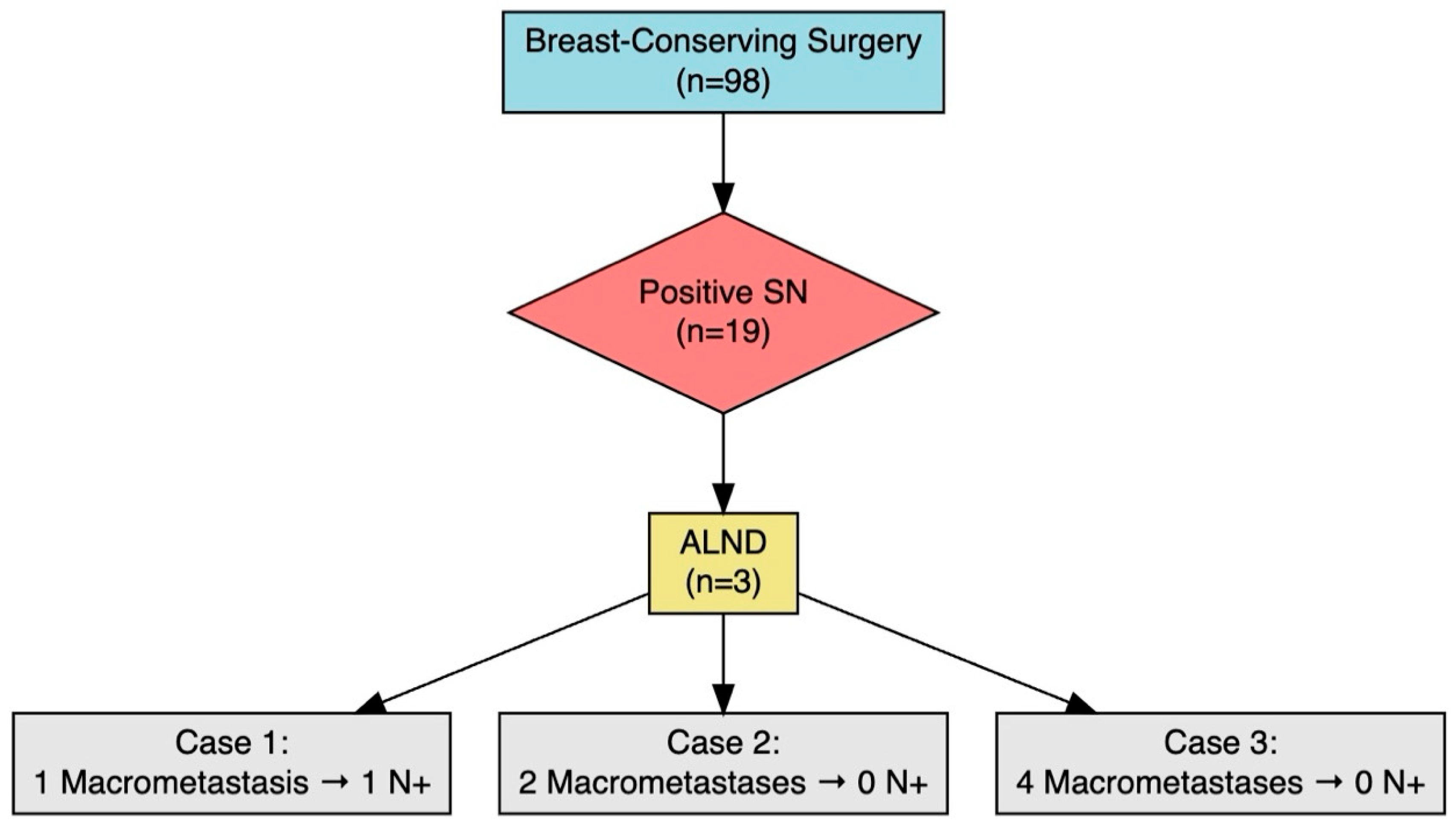
Figure 4.
ROC curve for age as predictor of sentinel node positivity.
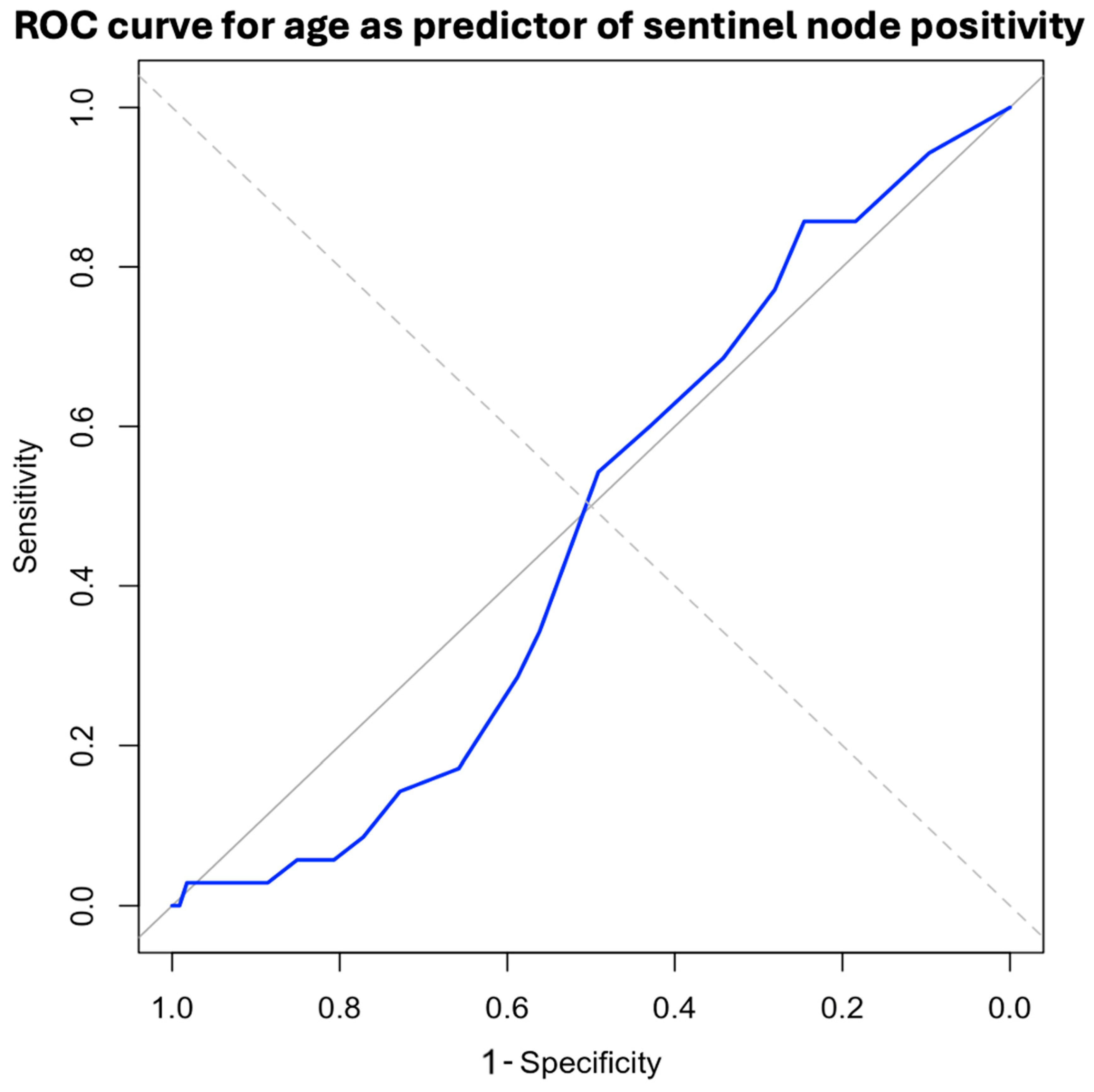

Table 1.
Clinical and demographic features.
|
Mastectomy (%) |
Breast-conserving surgery (%) |
Total (%) |
|||
| n | 51 (34.23) | 98 (65.7) | 149 | ||
| Age | Mean age ± SD (years) | 78.51 ± 5.83 | 76.50 ± 4,80 | 77.19 ± 5.24 | |
| 95% CI range (years) | 76.87 – 80.15 | 75.54 - 77,46 | 76.34 – 78.04 | ||
| Sexe | Female | 50 (98.04) | 98 (100.00) | 148 (99.33) | |
| Male | 1 (1.96) | 0 (0.00) | 1 (0.67) | ||
| ASA | I | 1 (1.96) | 0 (0.00) | 1 (0.67) | |
| II | 36 (70.59) | 79 (80.61) | 115 (77.18) | ||
| III | 13 (25.49) | 19 (19.39) | 32 (21.48) | ||
| IV | 1 (1.96) | 0 (0.00) | 1 (0.67) | ||
| V | 0 (0.00) | 0 (0.00) | 0 (0.00) | ||
| Breast laterality | Right | 22 (43.14) | 57 (58.16) | 79 (53.02) | |
| Left | 29 (56.86) | 41 (41.84) | 70 (46.98) | ||
| Previous breast neoplasm | 6 (11.76) | 13 (13.27) | 19 (12.75) | ||
| Breast laterality | Ipsilateral | 1 (16.67) | 1 (7.69) | 2 (10.53) | |
| Contralateral | 5 (83.33) | 12 (92.31) | 17 (89.47) | ||
| Molecular type | Same | 3 (50.00) | 5 (38.46) | 8 (42.11) | |
| Diferent | 2 (33.33) | 7 (53.85) | 9 (47.38) | ||
| Not available | 1 (16.67) | 1 (7.69) | 2 (10.53) | ||
| Imaging diagnosis | Ultrasound | 51 (100.00) | 98 (100.00) | 149 (100.00) | |
| MRI | 11 (21.57) | 19 (19.39) | 30 (20.13) | ||
| PET-CT | 0 (0.00) | 1 (1.02) | 1 (0.67) | ||
Categorical variables are presented as counts and percentages, n (%). SD: Standard Deviation, CI: Confidence Interval.
Table 2.
Anatomopathological features of the surgical specimen.
|
Mastectomy (%) |
Breast-conserving surgery (%) |
Total (%) |
|||
| Histological type | Invasive carcinoma of no special type | 24 (47.06) | 63 (64.29) | 87 (58.39) | |
| Invasive lobular carcinoma | 16 (31.37) | 14 (14.29) | 30 (20.13) | ||
| Invasive ductal carcinoma | 2 (3.92) | 3 (3.06) | 5 (3.36) | ||
| Mucinous carcinoma | 6 (11.76) | 4 (4.08) | 5 (3.36) | ||
| Solid papillary carcinoma | 1 (1.96) | 3 (3.06) | 4 (2.68) | ||
| Micropapillary carcinoma | 0 (0,00) | 0 (0.00) | 5 (3.36) | ||
| Mixed invasive carcinoma | 2 (3.92) | 0 (0.00) | 2 (1.34) | ||
| Invasive papillary carcinoma | 0 (0.00) | 1 (1.02) | 1 (0.67) | ||
| Neuroendocrine tumor | 0 (0.00) | 1 (1.02) | 1 (0.67) | ||
| Invasive apocrine carcinoma | 0 (0.00) | 1 (1.02) | 1 (0.67) | ||
| Adenoid cystic carcinoma | 0 (0.00) | 1 (1.02) | 1 (0.67) | ||
| Solid invasive carcinoma | 0 (0.00) | 1 (1.02) | 1 (0.67) | ||
| Tubular and cribriform invasive carcinoma | 0 (0.00) | 1 (1.02) | 1 (0.67) | ||
| Invasive micropapillary carcinoma | 0 (0.00) | 5 (5.10) | 5 (3.36) | ||
| T stage | T1 | 25 (49.02) | 82 (83.67) | 107 (71.81) | |
| T2 | 23 (45.10) | 14 (14.29) | 37 (24.83) | ||
| T3 | 3 (5.88) | 2 (2.04) | 5 (3.36) | ||
| T4 | 0 (0.00) | 0 (0.00) | 0 (0.00) | ||
| Histological grade | I | 8 (15.69) | 26 (26.53) | 34 (22.82) | |
| II | 40 (78.43) | 65 (66.33) | 105 (70.47) | ||
| III | 3 (5.88) | 7 (7.14) | 10 (6.71) | ||
| Molecular type | Luminal A | 15 (29.41) | 52 (53.06) | 67 (44.97) | |
| Luminal B | 27 (52.94) | 34 (34.69) | 61 (40.94) | ||
| Luminal B-Her2+ | 3 (5.88) | 2 (2.04) | 5 (3.36) | ||
| Her2+ | 3 (5.88) | 3 (3.06) | 6 (4.03) | ||
| Triple-negative | 3 (5.88) | 7 (7.14) | 10 (6.71) | ||
| SLNB | Positive | 16 (31.37) | 19 (19.39) | 35 (23.49) | |
| Negative | 35 (68.63) | 79 (80.61) | 114 (76.51) | ||
| SLNB features | >1 micrometastases | 8 (50.00) | 7 (36.84) | 15 (42.86) | |
| 1 macrometastases | 7 (43.75) | 8 (42.11) | 20 (57.14) | ||
| Macrometastases + micrometastases | 1 (6.25) | 4 (21.05) | 5 (27.30) | ||
| ALND | 7 (13.73) | 3 (3.06) | 10 (6.71) | ||
| ALND features | pN0 | 35 (66.67) | 77 (77.55) | 112 (75.17) | |
| pN1 | 13 (25.49) | 20 (20.41) | 33 (22.15) | ||
| pN2 | 1 (1.96) | 1 (1.02) | 2 (1.34) | ||
| pN3 | 2 (3.92) | 0 (0.00) | 2 (1.34) | ||
Categorical variables are presented as counts and percentages, n (%). ALND: Axillary lymph node dissection (ALND), SLNB: Sentinel Lymph Node Biopsy, T: Tumor.
Table 3.
Adjuvant treatment.
|
Mastectomy (%) |
Breast-conserving surgery (%) |
Total (%) |
||||
| Breast adjuvant radiotherapy | 16 (37.21 | 86 (87.76) | 102 (68.46) | |||
| Axillary adjuvant radiotherapy | 9 (20.93) | 17 (17.35) | 26 (17.45) | |||
| Irradiated lymph node levels | I | 6 (66.67) | 15 (88.24) | 20 (76.92) | ||
| II | 6 (66.67) | 15 (88.24) | 20 (76.92) | |||
| III | 7 (77.78) | 9 (52.94) | 13 (50.00) | |||
| IV | 1 (11.11) | 6 (35.29) | 7 (26.92) | |||
| V | 0 (0.00) | 1 (5.88) | 1 (3.85) | |||
| Breast adjuvant hormonotherapy | 45 (88.24) | 89 (90.82%) | 134 (89.93) | |||
| Breast adjuvant chemotherapy | 8 (15.69) | 9 (7.50%) | 17 (11.41) | |||
Categorical variables are presented as counts and percentages, n (%).
Table 4.
Cross-table of positive sentinel node with criteria for axillary lymph node dissection and positive nodes in axillary dissection.
Table 4.
Cross-table of positive sentinel node with criteria for axillary lymph node dissection and positive nodes in axillary dissection.
| Mastectomy: | ||||||
| ALND | ||||||
| N+ | 0 | 1 | 2 | 3 | 11 | |
| SLNB with criteria for ALND | 1 | 2 | 1 | |||
| 2 | 1 | 1 | ||||
| 3 | 1 | |||||
| 4 | 1 | |||||
|
Breast-conserving surgery: | ||||||
| ALND | ||||||
| N+ | 0 | 1 | 2 | 3 | 11 | |
| SLNB with criteria for ALND | 1 | 1 | ||||
| 2 | 1 | |||||
| 3 | ||||||
| 4 | 1 | |||||
SLNB: Sentinel Lymph Node Biopsy, ALND: Axillary Lymph Node Dissection.
Table 5.
Study of sensitivity and specificity of SLNB according to age.
| Age (years) | Sensibility | Specificity |
| 70 | 0.9429 | 0.9035 |
| 71 | 0.9 | 0.8596 |
| 72 | 0.8571 | 0.7851 |
| 73 | 0.8143 | 0.7368 |
| 74 | 0.7286 | 0.6886 |
| 75 | 0.6429 | 614 |
| 76 | 0.5714 | 0.5395 |
| 77 | 0.4429 | 0.4737 |
| 78 | 0.3143 | 0.4254 |
| 79 | 0.2286 | 0.3772 |
| 80 | 0.1571 | 307 |
| 81 | 0.1143 | 0.25 |
| 82 | 0.0714 | 0.2105 |
| 83 | 0.0571 | 0.1711 |
| 84 | 0.0429 | 0.1316 |
| 85 | 0.0286 | 0.0965 |
| 86 | 0.0286 | 0.0702 |
| 87 | 0.0286 | 0.0526 |
| 88 | 0.0286 | 0.0395 |
| 89 | 0.0286 | 0.0307 |
| 90 | 0.0286 | 0.0219 |
| 91 | 0.0214 | 0.0154 |
| 92 | 0.0071 | 11 |
| 93 | 0.0 | 0.0088 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



