
Submitted:
03 December 2024
Posted:
04 December 2024
You are already at the latest version
Abstract
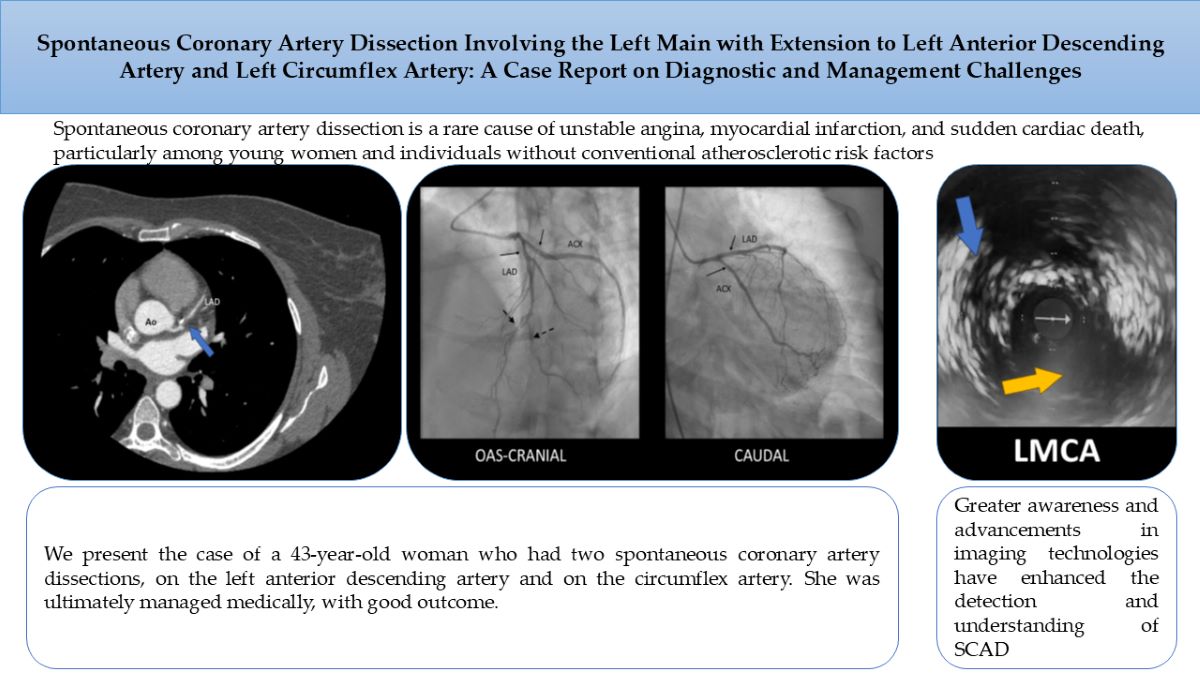
Background. Spontaneous coronary artery dissection is a rare cause of unstable angina, myocardial infarction, and sudden cardiac death, particularly among young women and individuals without conventional atherosclerotic risk factors. Case summary. We present the case of a 43-year-old woman who had two spontaneous coronary artery dissections, on the left anterior descending ar-tery and on the circumflex artery. She was ultimately managed medically, with good outcome. Discussion. SCAD is a unique and intricate condition that demands advanced diagnostic tech-niques and tailored management strategies. Greater awareness and advancements in imaging technologies have enhanced the detection and understanding of SCAD. However, continued re-search is crucial to resolve lingering uncertainties and further optimize patient outcomes.
Keywords:
case report
; spontaneous coronary artery dissection
; coronarography
; intravascular ultrasound
; conversative management
Figure 1.
The ECG of a 43-year-old female patient presenting to the Emergency Department (ED) with recurrent retrosternal chest pain at rest, radiating to the back, lasting approximately 10 minutes, showing no significant ST-T changes. Physical exam didn’t reveal any pathological signs, blood pressure was 120/60 mmHg bilaterally, heart rate 60 beats per minute. Echocardiography revealed akinesia of one third of the anterior, inferior, lateral walls and septum, with an estimated ejection fraction of 45%. There was no pericardial effusion noted and the aorta had normal dimensions and no intimal flap. Serological results showed normal cardiac necrosis markers. Of note, the patient denied significant medical family history. She was being treated for chronic anxiety.
Figure 1.
The ECG of a 43-year-old female patient presenting to the Emergency Department (ED) with recurrent retrosternal chest pain at rest, radiating to the back, lasting approximately 10 minutes, showing no significant ST-T changes. Physical exam didn’t reveal any pathological signs, blood pressure was 120/60 mmHg bilaterally, heart rate 60 beats per minute. Echocardiography revealed akinesia of one third of the anterior, inferior, lateral walls and septum, with an estimated ejection fraction of 45%. There was no pericardial effusion noted and the aorta had normal dimensions and no intimal flap. Serological results showed normal cardiac necrosis markers. Of note, the patient denied significant medical family history. She was being treated for chronic anxiety.
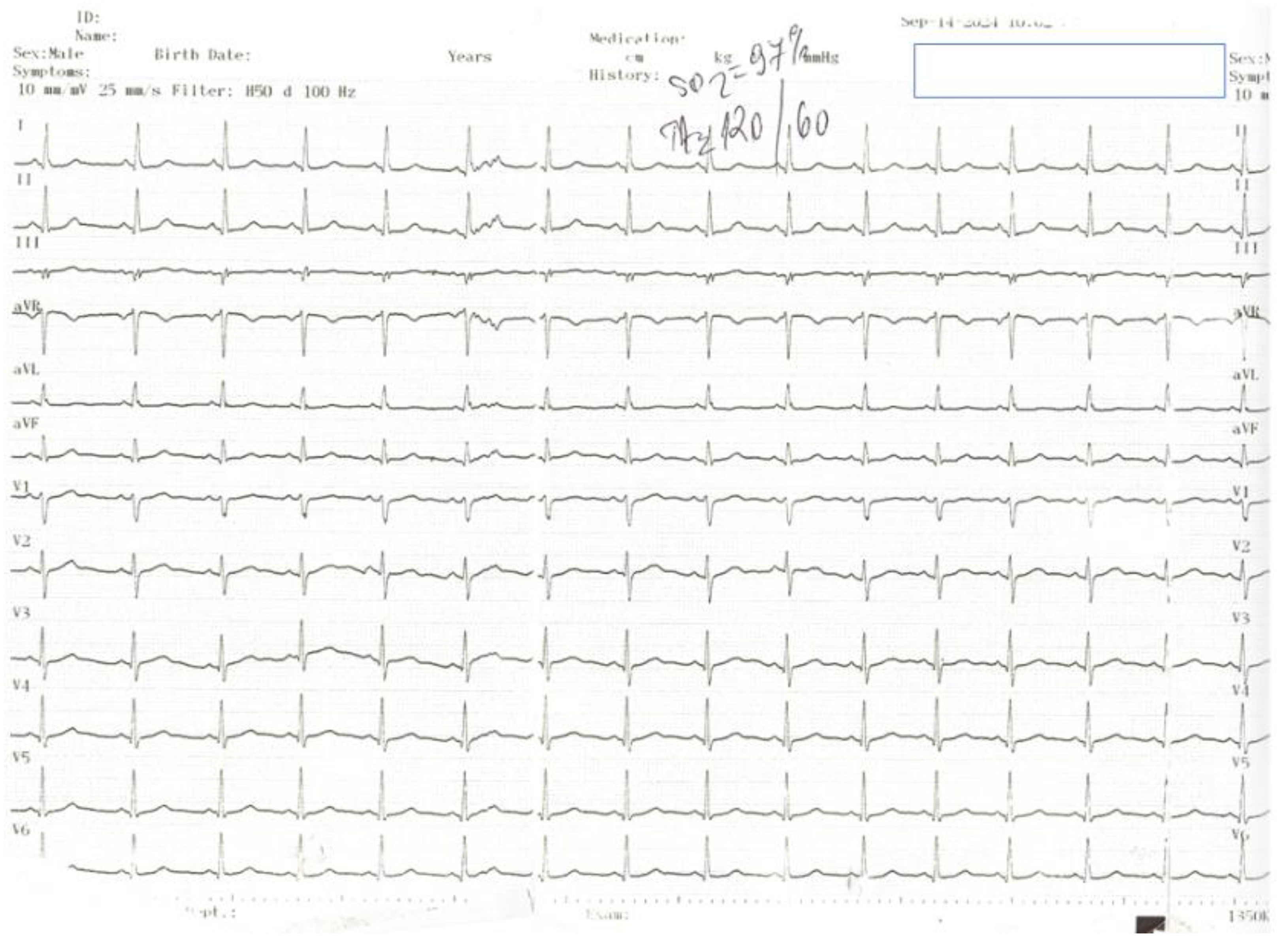
Figure 2.
Seeing as the patient had a low suspicion for atherosclerotic disease, we firstly performed a CT coronary angiography (CTCA) which revealed a significant stenosis of the left anterior descending artery (LAD).
Figure 2.
Seeing as the patient had a low suspicion for atherosclerotic disease, we firstly performed a CT coronary angiography (CTCA) which revealed a significant stenosis of the left anterior descending artery (LAD).
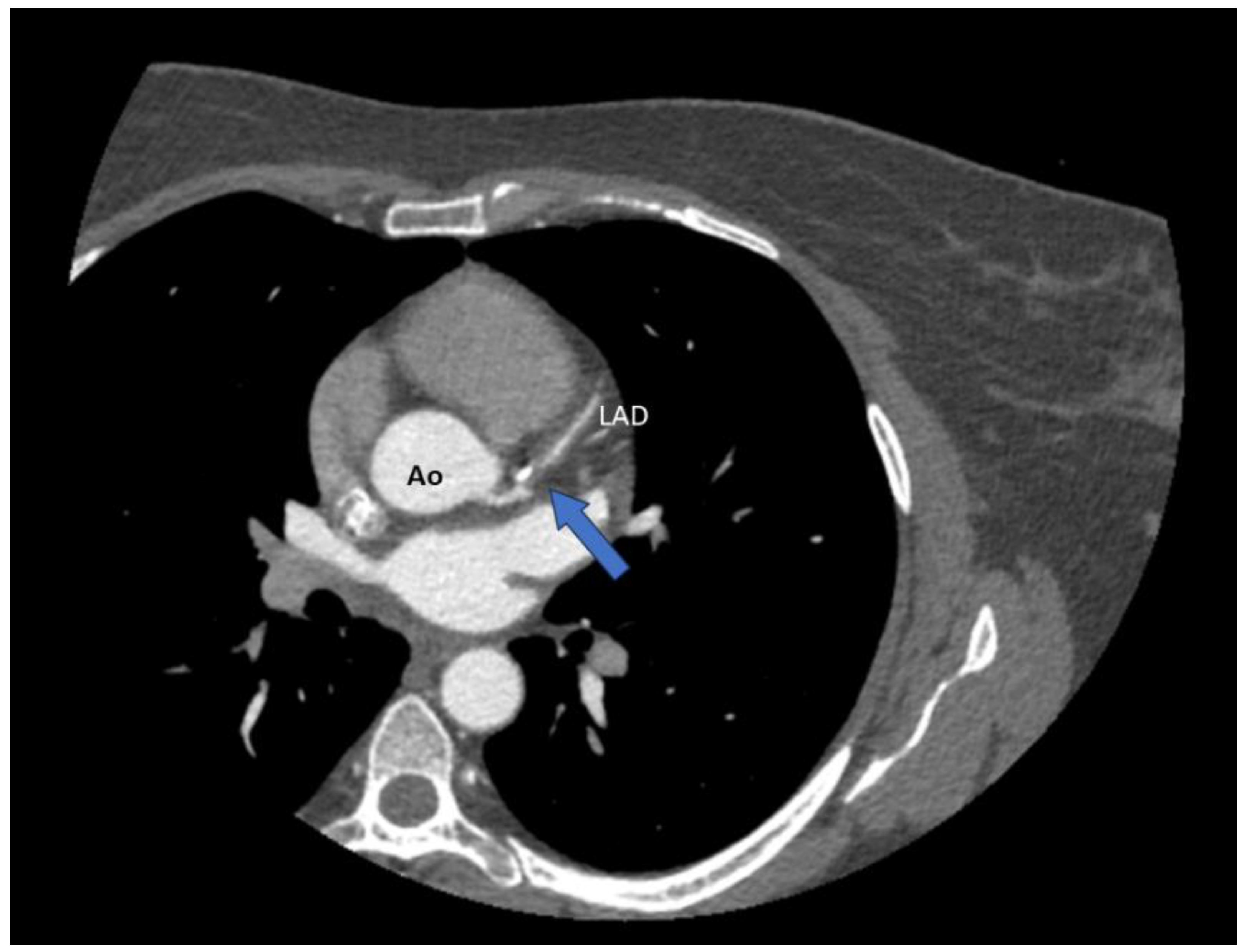
Figure 3.
The patient later experienced another episode of resting chest pain. An ECG performed at that time revealed deep, diffuse negative T waves in V1-V6, DI, DII, aVL and aVF.
Figure 3.
The patient later experienced another episode of resting chest pain. An ECG performed at that time revealed deep, diffuse negative T waves in V1-V6, DI, DII, aVL and aVF.
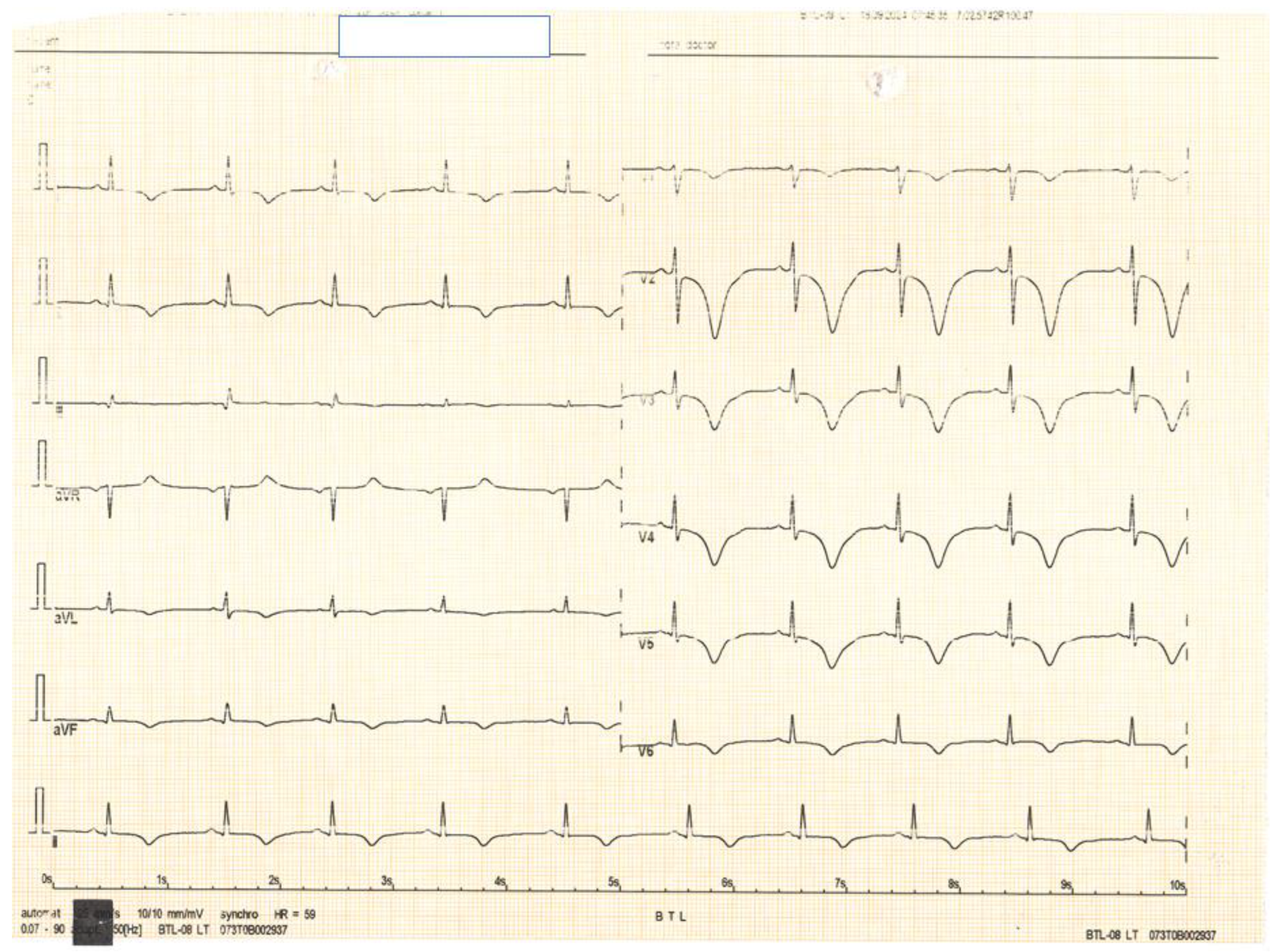
Figure 4.
Subsequent ECGs demonstrated evolution of the ST-T segment, consistent with a Wellens syndrome pattern. Cardiac necrosis markers increased.
Figure 4.
Subsequent ECGs demonstrated evolution of the ST-T segment, consistent with a Wellens syndrome pattern. Cardiac necrosis markers increased.
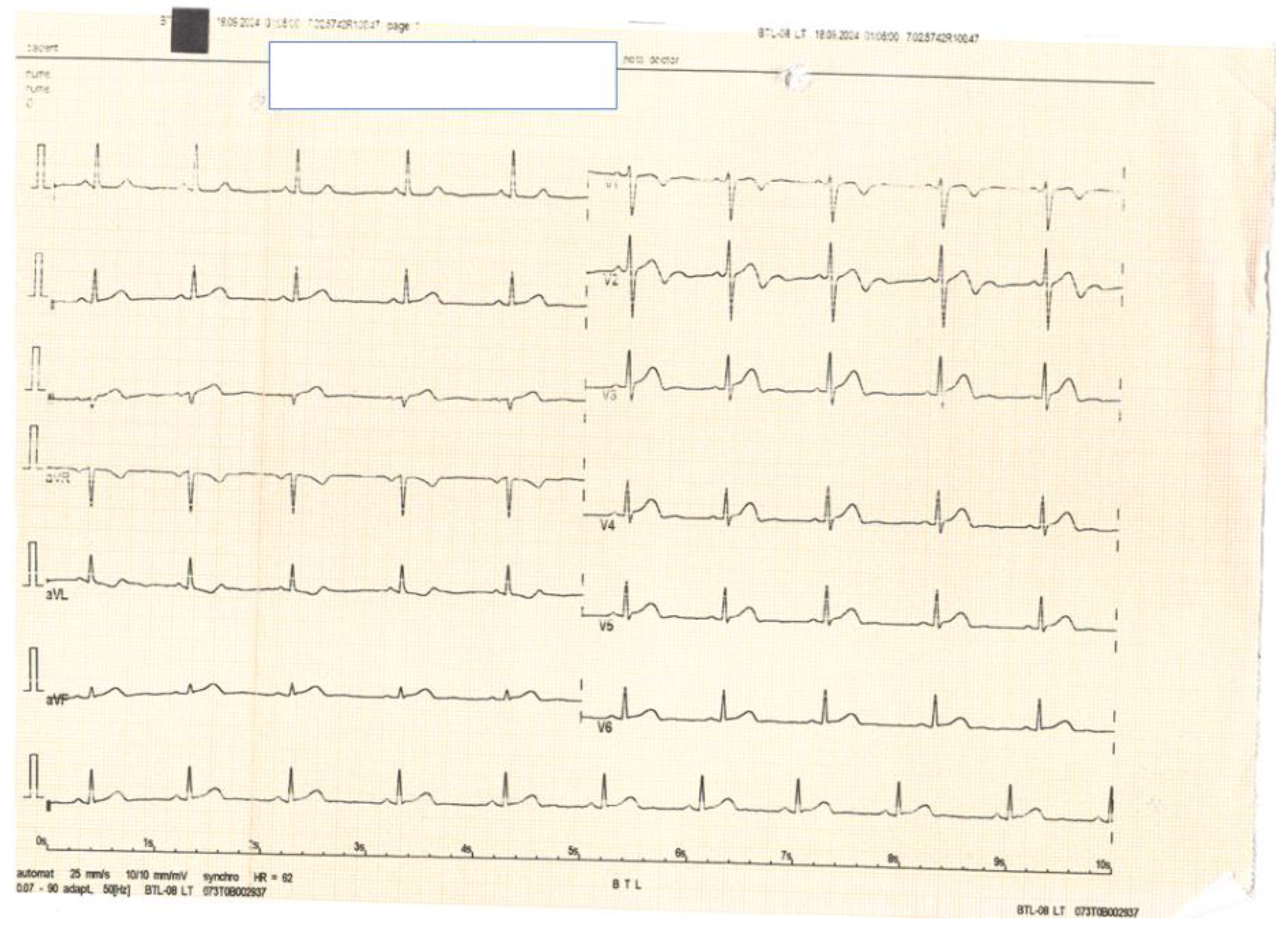
Figure 5.
We performed urgent coronarography which, surprisingly, revealed mild, smooth stenoses located in the proximal segments of the LAD and Cx coronary arteries (solid arrows) along with distal occlusions in LAD and diagonal branch (dashed arrows).
Figure 5.
We performed urgent coronarography which, surprisingly, revealed mild, smooth stenoses located in the proximal segments of the LAD and Cx coronary arteries (solid arrows) along with distal occlusions in LAD and diagonal branch (dashed arrows).
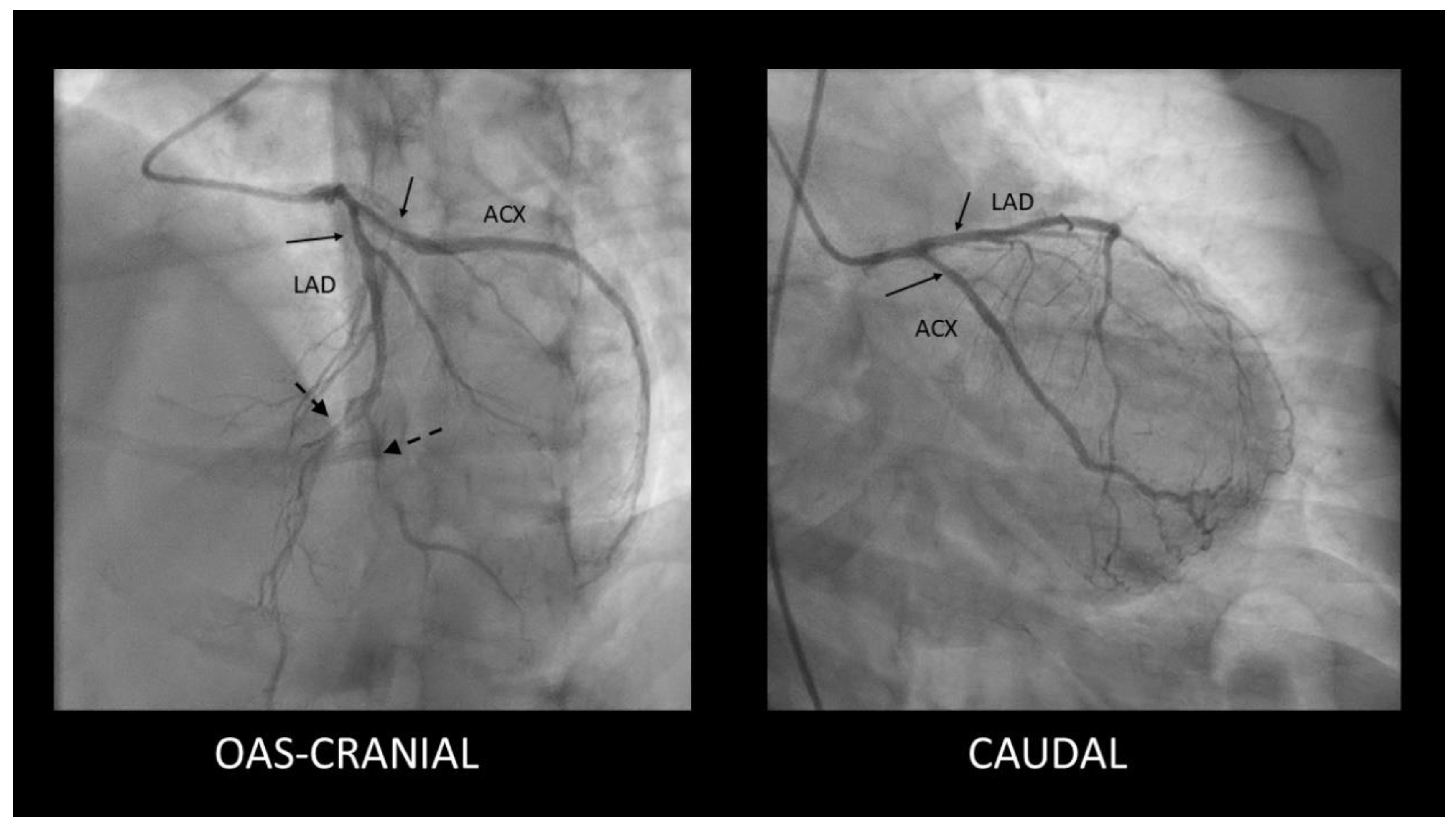
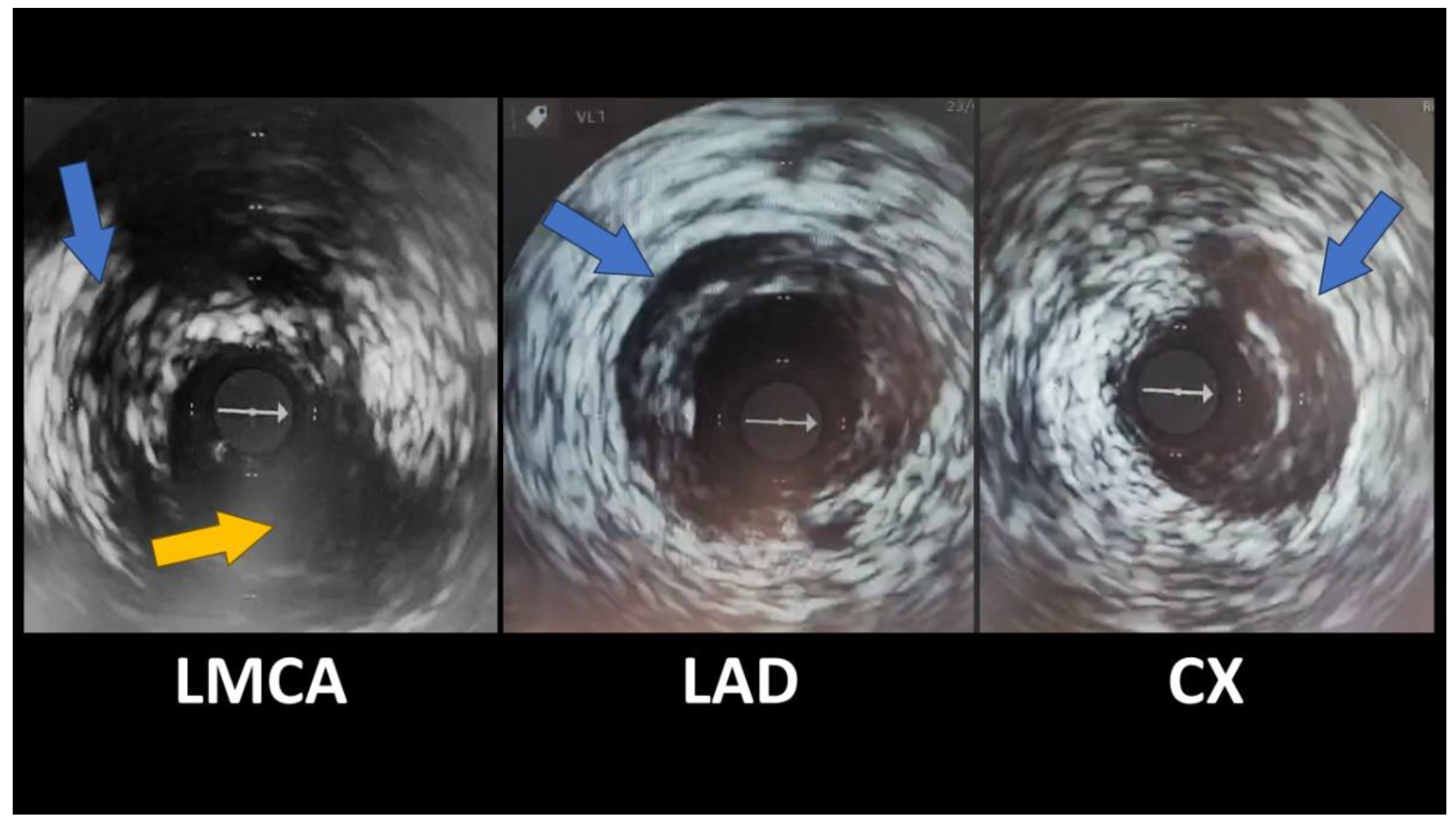
Figure 6.
Given the striking discrepancies between the patient’s symptoms, ECG and CTCA results, we decided to further investigate and an intravascular ultrasound (IVUS) was performed. It revealed spontaneous coronary artery dissection in the distal left main artery, with extensions in the LAD and proximal circumflex arteries, with hematomas present, classified as a type 2a. Given that the hematomas were most likely favorized by parenteral anticoagulation, we withdrew this medication, maintaining dual antiplatelet therapy with aspirin and clopidogrel. Conservative management was chosen for this patient because she was hemodynamically stable and angina free at the moment of coronarography. She was discharged in good health with minimal cardiac medication (aspirin, clopidogrel, beta-blocker, ACE inhibitor and statin) and scheduled for a follow-up coronarography at the 3-month mark (which have not elapsed at the moment of writing this article). The true incidence of spontaneous coronary artery dissection (SCAD) remains uncertain, but it is increasingly recognized as a cause of acute coronary syndrome (ACS) particularly in young to middle-aged women [1,2]. There are several known predisposing factors for SCAD: systemic inflammatory conditions, hormonal therapy, fibromuscular dysplasia, postpartum status, multiparity (≥4 births), connective tissue disorders [3]. Beside these predisposing factors, certain triggers can precede the anginal episode, such as emotional stress, exercise or hormonal changes (in vitro fertilization [4], hormonal replacement therapy [5], hormonal therapy in transgender individuals [6], oral contraception [7]) [8]. Management of spontaneous coronary dissection isn’t completely clarified. Both the European Society of Cardiology (ESC) and the American Heart Association (AHA) have published reports with recommendations. Both reports highlight conservative management as the preferred strategy [2,9]. The ESC states high healing rates over time (73%-100%), and the AHA emphasizes some cases need repeat angiography to confirm healing, typically after 35 days. Revascularization may be challenging due to fragile coronary vessel wall and angioplasty may have worse outcomes compared to atherosclerotic coronary disease. Close monitoring after the index event is recommended by both associations [2,9], with the AHA preferring extended inpatient monitoring for up to 7 days [9]. According to the ESC, 3.3% of conservatively managed patients may require revascularization during follow-up [2]. AHA states that the first 7 days are critical as patients may experience recurrent MI and need emergency revascularization [9]. In regards to percutaneous coronary intervention (PCI), both reports state that angioplasty is associates with significant complications (false lumen propagation, iatrogenic dissection) and procedural failure (stent restenosis and thrombosis) which may need emergent coronary artery by-pass graft (CABG) [2,9]. In general, angioplasty should only be attempted if strictly necessary. Both ESC and AHA agree that CABG is reserved as a bail-out strategy when PCI fails, especially in cases of ongoing ischaemia, infarction, or technical failure (e.g., inability to wire the true lumen). Left main coronary artery involvement or multiple dissections could require CABG [2,9]. CABG complications are graft failure which can occur due to competitive flow due to the healing of the native coronary artery. CABG does not prevent recurrent SCAD. When performing CABG one of the main concerns is anastomosis to the true lumen. AHA emphasizes conservative strategy when it comes to stable patients [9]. Given that SCAD involve bleeding and hematoma formation, the use of traditional acute coronary syndrome drugs such as antiaggregant and anticoagulation is controversial. In regards to antiplatelet therapy, aspiring and clopidogrel are preferred. While the ESC endorses dual antiplatelet therapy (DAPT) [2], the AHA is reserved due to lack of evidence and recommends single antiplatelet therapy (SAPT) in patients not undergoing PCI [9]. Both guidelines raise concerns about anticoagulation due to increased bleeding risk [2,9]. The AHA recommends discontinuation of anticoagulation therapy unless it is necessary for other comorbidities [9]. Statins are not particularly useful in SCAD due to its non-atherosclerotic pathophysiology. Statins can be recommended if the patient has dyslipidemia or diabetes. Hormonal contraception and hormone replacement therapy carry a potential risk for SCAD, especially since SCAD occurs often in young women, including during pregnancy or postpartum. Evidence in this direction is inconclusive and a causal link has not been established. Ischemia relief can be obtained using traditional antianginal medication (nitrates, calcium channel blockers).
Figure 6.
Given the striking discrepancies between the patient’s symptoms, ECG and CTCA results, we decided to further investigate and an intravascular ultrasound (IVUS) was performed. It revealed spontaneous coronary artery dissection in the distal left main artery, with extensions in the LAD and proximal circumflex arteries, with hematomas present, classified as a type 2a. Given that the hematomas were most likely favorized by parenteral anticoagulation, we withdrew this medication, maintaining dual antiplatelet therapy with aspirin and clopidogrel. Conservative management was chosen for this patient because she was hemodynamically stable and angina free at the moment of coronarography. She was discharged in good health with minimal cardiac medication (aspirin, clopidogrel, beta-blocker, ACE inhibitor and statin) and scheduled for a follow-up coronarography at the 3-month mark (which have not elapsed at the moment of writing this article). The true incidence of spontaneous coronary artery dissection (SCAD) remains uncertain, but it is increasingly recognized as a cause of acute coronary syndrome (ACS) particularly in young to middle-aged women [1,2]. There are several known predisposing factors for SCAD: systemic inflammatory conditions, hormonal therapy, fibromuscular dysplasia, postpartum status, multiparity (≥4 births), connective tissue disorders [3]. Beside these predisposing factors, certain triggers can precede the anginal episode, such as emotional stress, exercise or hormonal changes (in vitro fertilization [4], hormonal replacement therapy [5], hormonal therapy in transgender individuals [6], oral contraception [7]) [8]. Management of spontaneous coronary dissection isn’t completely clarified. Both the European Society of Cardiology (ESC) and the American Heart Association (AHA) have published reports with recommendations. Both reports highlight conservative management as the preferred strategy [2,9]. The ESC states high healing rates over time (73%-100%), and the AHA emphasizes some cases need repeat angiography to confirm healing, typically after 35 days. Revascularization may be challenging due to fragile coronary vessel wall and angioplasty may have worse outcomes compared to atherosclerotic coronary disease. Close monitoring after the index event is recommended by both associations [2,9], with the AHA preferring extended inpatient monitoring for up to 7 days [9]. According to the ESC, 3.3% of conservatively managed patients may require revascularization during follow-up [2]. AHA states that the first 7 days are critical as patients may experience recurrent MI and need emergency revascularization [9]. In regards to percutaneous coronary intervention (PCI), both reports state that angioplasty is associates with significant complications (false lumen propagation, iatrogenic dissection) and procedural failure (stent restenosis and thrombosis) which may need emergent coronary artery by-pass graft (CABG) [2,9]. In general, angioplasty should only be attempted if strictly necessary. Both ESC and AHA agree that CABG is reserved as a bail-out strategy when PCI fails, especially in cases of ongoing ischaemia, infarction, or technical failure (e.g., inability to wire the true lumen). Left main coronary artery involvement or multiple dissections could require CABG [2,9]. CABG complications are graft failure which can occur due to competitive flow due to the healing of the native coronary artery. CABG does not prevent recurrent SCAD. When performing CABG one of the main concerns is anastomosis to the true lumen. AHA emphasizes conservative strategy when it comes to stable patients [9]. Given that SCAD involve bleeding and hematoma formation, the use of traditional acute coronary syndrome drugs such as antiaggregant and anticoagulation is controversial. In regards to antiplatelet therapy, aspiring and clopidogrel are preferred. While the ESC endorses dual antiplatelet therapy (DAPT) [2], the AHA is reserved due to lack of evidence and recommends single antiplatelet therapy (SAPT) in patients not undergoing PCI [9]. Both guidelines raise concerns about anticoagulation due to increased bleeding risk [2,9]. The AHA recommends discontinuation of anticoagulation therapy unless it is necessary for other comorbidities [9]. Statins are not particularly useful in SCAD due to its non-atherosclerotic pathophysiology. Statins can be recommended if the patient has dyslipidemia or diabetes. Hormonal contraception and hormone replacement therapy carry a potential risk for SCAD, especially since SCAD occurs often in young women, including during pregnancy or postpartum. Evidence in this direction is inconclusive and a causal link has not been established. Ischemia relief can be obtained using traditional antianginal medication (nitrates, calcium channel blockers).
Author Contributions
writing—original draft preparation, L.I.C, U C-D and, R. L-M.; writing—review and editing, R.C.A and C.L. R.C.A. and C.L. contributed equally to this work and should be considered joint first authors.
Funding
none declared.
Informed Consent
Informed consent for the publication of this case report was obtained from the patient in line with COPE guidance.
Data Availability Statement
The data underlying this article will be shared on reasonable request to the corresponding author.
Conflict of Interest
none declared.
References
- Al-Hussaini, A.; Adlam, D. Spontaneous coronary artery dissection. Heart 2017, 103, 1043–1051. [Google Scholar] [CrossRef] [PubMed]
- Adlam, D.; Alfonso, F.; Maas, A.; Vrints, C. European Society of Cardiology, acute cardiovascular care association, SCAD study group: a position paper on spontaneous coronary artery dissection. In: European heart journal. NLM (Medline); 2018. p. 3353–68.
- Tweet, M.S.; Hayes, S.N.; Pitta, S.R.; Simari, R.D.; Lerman, A.; Lennon, R.J.; et al. Clinical features, management, and prognosis of spontaneous coronary artery dissection. Circulation 2012, 126, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Iyasere, C.; Potdar, N. Spontaneous Coronary Artery Dissection Associated With Infertility Treatment. Cureus. 2022. [CrossRef] [PubMed]
- Mori, R.; Macaya, F.; Giacobbe, F.; Moreno, V.; Quadri, G.; Chipayo, D.; et al. Association between hormone therapy and short-term cardiovascular events in women with spontaneous coronary artery dissection. Revista Española de Cardiología (English Edition) 2023, 76, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, K.; Yogeswaran, V.; Dean, L.S. Spontaneous coronary artery dissection and exogenous estrogen in a transgender female. Catheterization and Cardiovascular Interventions 2022, 100, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Evangelou, D.; Letsas, K.P.; Korantzopoulos, P.; Antonellis, I.; Sioras, E.; Kardaras, F. Spontaneous coronary artery dissection associated with oral contraceptive use: A case report and review of the literature. Int J Cardiol. 2006, 112, 380–382. [Google Scholar] [CrossRef] [PubMed]
- Adlam, D.; García-Guimaraes, M.; Maas, A.H.E.M. Spontaneous coronary artery dissection: No longer a rare disease. Eur Heart J. 2019, 40, 1198–1201. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.N.; Kim CESH, Saw, J. ; Adlam, D.; Arslanian-Engoren, C.; Economy, K.E.; et al. Spontaneous coronary artery dissection: Current state of the science: A scientific statement from the American Heart Association. Circulation 2018, 137, e523–57. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



