
Submitted:
02 December 2024
Posted:
03 December 2024
You are already at the latest version
Abstract
To analyze African countries’ performance in achieving the fourth ADI commitment of the Addis Declaration on Immunization (ADI), a cross-sectional retrospective study was conducted including the 54 African Member States of the World Health Organization (WHO) out of 55 African Union (AU) Member States. The fourth ADI commitment aims at increasing the effectiveness and efficiency of immunization delivery systems and has four performance indicators. The median percentage of districts with less than 10% of dropout rate between DTP1 and DTP3 was 86.5%, ranging from 22% to 100%. Thirty-four countries (63%) recorded 80% or above districts with less than 10% dropout rate between DTP1 and DTP3. Eleven countries (20.3%) and 10 countries (18.5%) sustained 90% or above coverage for DTP3 and MCV1, respectively, in the past three years (2021-2023). Four countries (7.4%) had 44.5 skilled health workers per 10,000 people. Out of the 54 WHO Member States, seven achieved at least three of the four indicators of the fourth ADI commitment. It is critical, as a follow-up to this study, to document best practices from these seven countries that achieved the fourth ADI commitment. Additionally, a deeper analysis of factors associated with achieving the ADI commitments is required.
Keywords:
Addis Declaration
; Immunization
; Universal access
; Africa
1. Introduction
The World Health Organization (WHO) established the Expanded Program on Immunization (EPI) in 1974 to ensure that all children in all countries have access to life-saving vaccines [1]. Since then, immunization coverage has increased significantly from 1980 to 2016. WHO and United Nations Children’s Fund (UNICEF) Estimates of National Immunization Coverage (WUENIC) show increases from 12% to 82% for the Bacille Calmette-Guérin vaccine (BCG), from 14% to 83% for the first dose of Diphtheria-Tetanus-Pertussis containing vaccine (DPT1), and from 9% to 81% for the first dose of Measles containing vaccine (MCV1). Despite this significant progress, immunization coverage was suboptimal in most African countries as of 2016. One in five African children had still not received life-saving vaccines, leading to persistent outbreaks of Vaccine-Preventable Diseases (VPD), pointing to gaps in immunization coverage and disease surveillance [2].
Recognizing the need for investing more in routine immunization to continue improving the health of African populations, in February 2016, the African Union (AU)’s Ministers of Health, Finances, Education, Social Affairs and Local governments adopted the declaration of Addis on universal access to immunization as a cornerstone for health and development in Africa, known as the Addis Declaration on Immunization (ADI) [3]. The ADI is made up of 10 commitments, and was officially endorsed by Heads of States on 31 January 2017, during the 28th African Union Heads of State Summit [2]. This endorsement represents a reaffirmation of Africa’s commitment to reaching all children with life-saving vaccines and keeping universal access to immunization at the forefront of efforts to achieve ambitious immunization goals and reduce child mortality.
The 10 ADI commitments outline concrete ways for countries to improve their immunization programs. To ensure successful implementation of the ADI, the African Union Member States agreed to establish an accountability framework comprising indicators and targets for monitoring countries’ progress [4]. The African Union Commission (AUC) and the World Health Organization (WHO) through its regional office for Africa (WHO AFRO) and for Eastern Mediterranean (WHO EMRO) were assigned the mission of overseeing the implementation and monitoring of the ADI’s accountability framework and providing updates on progress made towards achieving the set targets [4]. In 2019, the WHO AFRO and EMRO published the first progress report on ADI implementation [5]. This showed that more than half of African countries (29 of 54) made significant progress toward achieving equitable coverage with the administration of the third dose of DTP vaccine (DTP3) between 2015 and 2018 [5]. However, in terms of equity, there were still persistent barriers in vaccine and healthcare delivery systems, especially in the poorest, most vulnerable, and most marginalized communities [5]. Regarding domestic funding, only 19 out of 54 African countries (35%) increased their contributions to immunization programmes [5]. From then onwards, the COVID-19 pandemic substantially disrupted routine immunization services in Africa, leading to a precipitous decline in childhood vaccination rates compared to pre-pandemic levels, and resulting in a greater number of un- and under-immunized children [6].
Following the lifting of the public health emergency of international concern (PHEIC) status for the COVID-19 pandemic by WHO on 5 May 2023 [7], it is critical to assess the achievement of the fourth ADI commitment related to “Increasing the effectiveness and efficiency of immunization delivery systems as an integrated part of strong and sustainable primary health care systems” by African countries, as of end 2023.
This paper summarizes progress made by African countries in achieving the indicators related to the fourth ADI commitment as of end 2023.
2. Materials and Methods
A cross-sectional retrospective study analysing the African countries’ performance in achieving the fourth ADI commitment was conducted.
Presentation of the Fourth ADI Commitment
The ADI is a historic pledge aiming at increasing political will to achieve universal access to immunization services and includes ten commitments to shape the future of immunization in Africa (Table 1).
This study assesses achievement of the fourth ADI commitment. Four indicators were defined for the fourth ADI commitment as per the accountability framework: (i) proportion of countries with over 80% of districts that recorded less than 10% dropout rate between DTP1 and DTP3, (ii) proportion of countries with sustained DTP3 coverage of 90% or above in the past three years, (iii) proportion of countries with sustained MCV1 coverage of 90% or above in the past three years, and (iv) proportion of countries with at least 80% of districts or administrative units with a minimum threshold of 44.5 skilled health workers per 10,000 people. Given that data on skilled health workers density by district were not available, the proportion of countries with a minimum threshold of 44.5 skilled health workers per 10,000 people at national level was used as proxy.
Inclusion and Exclusion Criteria
Fifty-four African countries that are Member States of WHO were included [8]. The Sahrawi Arab Democratic Republic, a country that is Member State of the African Union but not a WHO Member State, and which does not report data on immunization coverage to WHO and UNICEF through Joint Report Forms (JRF), was not included.
Data Sources and Measurement
Table 2 shows the criteria of achievement and the source of data for the four indicators of the fourth ADI commitment.
Data Analysis
The achievement of each indicator of the fourth ADI commitment was assessed using the criteria specified in Table 2.
For each indicator the percentage of countries achieving the indicator was computed by dividing the number of countries that achieved the indicator by the total number of countries, i.e. 54.
The performance in achieving the fourth ADI commitment was computed for each country by dividing the number of indicators achieved by the total number of indicators, i.e. 4.
Using WUENIC data, the status of sustained coverage was assigned to each country for DTP3 and MCV1; Countries that recorded 90% coverage for each antigen each year from 2021 to 2023 were considered as those that sustained immunization coverage.
The commitment was considered as achieved for countries with 75% or above performance, corresponding to at least 3 out of 4 indicators achieved.
Subsequently, the proportion of countries that have achieved the fourth ADI commitment was computed by dividing the number of countries that achieved the fourth ADI commitment by 54.
3. Results
Indicator 1: Proportion of Countries with More Than 80% of Districts Recording Less Than 10% Dropout Rate Between DTP1 and DTP3
Figure 1 presents the distribution of the percentage of districts with less than 10% dropout rate between DTP1 and DPT3 in 2023 by country in Africa.
The median percentage of districts with less than 10% dropout rate between DTP1 and DTP3 was 86.5%, ranging from 22% in Botswana to 100% in Sao Tome and Principe, Sierra Leone, Rwanda, Libya, Lesotho, Egypt, and Djibouti.
Thirty-four (34) countries out of 54 (63%) achieved the first indicator of the fourth ADI commitment, i.e. they recorded 80% or more districts with less than 10% dropout rate between DTP1 and DTP3.
At the national level, the median dropout rate was 5% [range: 0%;20%]. Forty-five countries (83%) recorded less than 10% dropout rate at national level against 9 countries with 10% or above (17%) (Angola, Benin, Central African Republic, Chad, Democratic Republic of Congo, Guinea, Liberia, Mozambique and Somalia).
Indicator 2: Proportion of Countries with Sustained Coverage of at Least 90% for DPT3 in the Past Three Years (2021, 2022 and 2023)
Figure 2 presents the distribution of DTP3 coverage in 2021, 2022 and 2023 by country in Africa.
In 2023, 19 countries out of 54 recorded at least 90% DTP3 coverage (35%), including 11 (20.3%) that sustained at least 90% DTP3 coverage in the past three years (Burkina Faso, Cabo Verde, Egypt, Eritrea, Ghana, Kenya, Mauritius, Morocco, Seychelles, Sierra Leone and Tunisia).
Indicator 3: Proportion of Countries with Sustained Coverage of at Least 90% for MCV1 in the Past Three Years (2021, 2022 and 2023)
Figure 3 presents the distribution of MCV1 coverage in 2021, 2022 and 2023 by country in Africa.
In 2023, 20 countries out of 54 recorded at least 90% MCV1 coverage (37%), including 10 (18.5%) that sustained 90% or above MCV1 coverage in past three years (Botswana, Cabo Verde, Egypt, Eritrea, Ghana, Morocco, Seychelles, Tunisia, Uganda, and Zambia).
Proportion of Countries with a Minimum Threshold of 44.5 Skilled Health Workers per 10,000 People at National Level In 2022
Four countries out of 54 (7.4%) surpassed 44.5 skilled health workers per 10000 people: Eswatini (44.7/10000), Cabo Verde (60.4/10000), Libya (88.9/10000) and Seychelles (110.9/10000).
Achievement of the Commitment
Only seven countries out of 54 achieved at least three of the four indictors to measure the fourth ADI commitment. While Cabo Verde and Seychelles met all four indicators, Egypt, Eritrea, Ghana, Morrocco, and Tunisia each met three indicators.
Figure 4 presents the geographical distribution of the proportion of the four indicators of the fourth ADI commitment achieved in 2023 by country in Africa.
Table 3 presente a heatmap on the achievement of each of the four indicators of the ADI commitment as od end 2023.
4. Discussion
In January 2017, African Heads of States endorsed a historical pledge aiming at ensuring universal access to immunization across the continent [3]: the ADI. This high-level political commitment represents a major move to increasing and sustaining domestic investment and funding for routine immunization, but will only be beneficial for African children and families if translated into concrete actions. To achieve this, the African Union Commission (AUC) in collaboration with WHO and other immunization partners, developed a roadmap for the implementation of the ADI, which includes an accountability framework [4]. This framework set indicators to monitor progress in each of the 10 ADI commitments. This paper assesses progress, as of end 2023, in the implementation the ADI in Africa, through the fourth commitment, as per the accountability framework, while African countries are recovering from three years of the active phase of the COVID-19 pandemic. The fourth commitment was selected as it is related to the effectiveness and efficiency of immunization service delivery systems. Given constrained budgets and competing priorities, increasing the efficiency of health service delivery is seen as a way to free up resources for increasing the scale and quality of services [16]. This commitment provides a platform for assessing the ability of routine immunization to use the health workforce and investments in the immunization programmes to sustain high level coverage for all antigens and reduce dropout rates.
The first indicator of the fourth ADI commitment monitors the dropout rate at district level using dropout between DTP1 and DTP3 as a tracer. Each African country is expected to achieve a dropout rate of less than 10% between DTP1 and DTP3 in at least 80% of districts. The dropout rate is one of the determinants of immunization coverage and programme performance, continuity, and follow-up [17]. According to WHO, a dropout rate of over 10% is unfavorable and indicates underutilization of immunization services [18]. In this study, 63% of African countries recorded a dropout rate of less than 10% in over 80% of districts, versus 83% of countries recording a dropout rate of less than 10% at national level. Low national dropout rates can conceal large subnational inequities across countries. Kirkby et al. [19] found an average of 7.3% DTP1– DTP3 dropout rate in 2018 in districts in Ethiopia, ranging from 0% to 57%. In Kenya, a study that evaluated the impact of text messaging and sticker reminders to reduce dropouts from the vaccination program in 2014, found that having a caregiver with below secondary education and residing more than 5 km away from the health facility were associated with higher odds of dropping out [18,19]; caregivers who received reminder text messages were less likely to drop out [19]. Robust defaulter tracking systems and strategies are critical to reducing missed opportunities in order to address inequalities in immunization, especially in underserved areas [18].
Large inequalities in subnational dropout rate tend to be correlated with low DTP1 and DTP3 coverage at national level [19]. The second and third indicators of the fourth commitment are related to the proportion of countries with sustained DPT3 and MCV1 coverages of 90% or above in the past three years. In 2023, these indicators were achieved by 11 countries (20%) for DTP3 coverage and 10 countries (18%) for MCV1. This means that most countries in Africa did not sustain DTP1 and MCV1 coverages as of end 2023. Several authors have reported a drop in DTP3 and MCV1 coverage during the COVID-19 pandemic period [20,21,22]. LaFond et. Al. [22] identified four direct drivers of routine immunization coverage improvement, including (i) engaging more with community-centered health workers, (ii) strengthening the collaboration between health districts, local governments and community groups to plan and execute immunization services, raise awareness and define strategies to reach underserved areas, (iii) carrying out regular immunization data reviews to inform operational decisions, and (iv) tailoring immunization services to community needs and conditions. Addressing these drivers implies implementing the “reaching every district” strategy [23], developed and introduced in 2002 by WHO, the United Nations Children’s Fund (UNICEF) and other partners to improve immunization systems in areas with low coverage [24].
The link between health workers density and immunization services is well documented [21]. In recognition of this linkage, one of the four indicators on the fourth ADI commitment monitors the proportion of countries with a minimum threshold of 44.5 skilled health workers per 10000 people at national level. In this study, only 4 countries out the 54 African countries achieved this indicator including one high income country (Seychelles), one upper-middle income country (Libya) and two lower-middle income countries (Cabo Verde and Eswatini). Shortage of health workers in most African countries sounds as a call to continuously strengthen health systems to achieve results in specific health programmes, including immunization [21].
In this study, only seven of the 54 African countries assessed achieved at least 75% of the four indicators of the fourth ADI commitment: Egypt, Eritrea, Ghana, Ghana, Morocco, Cabo Verde, Seychelles and Eswatini. This means that most countries in Africa still need to put in additional efforts to achieve the fourth ADI commitment. Among the countries that achieved the fourth commitment, five are non-eligible for Gavi support, one is in the accelerated transition out of Gavi support (Ghana) and only one is the initial self-financing phase [25]. This highlights the need to increasing governments’ contributions to financing routine immunization programmes as well as developing innovative funding solutions at national level. None of the countries that have achieved the fourth ADI indicator are among the 12 countries on high or very high alert as per the fragile status index [26].
This study shows that a formal platform for regular monitoring of all ADI commitments is required, as well as better support by all stakeholders to countries’ efforts aiming at translating political commitments into concrete actions.
Limitations
The WUENIC estimates were used to assess two of the four indicators of the fourth ADI commitment. WHO and UNICEF annually review data on immunization coverage to estimate national coverage with routine service delivery of selected vaccines. The estimates are based on government reports submitted to WHO and UNICEF and are supplemented by survey results from the published and grey literature and may be different to administrative and official coverage, and sometimes not supported by national authorities for varying reasons. An analysis using administrative or official data on immunization coverage could lead to different results in some countries.
The assessment of the indicators related to the percentage of districts with a dropout rate of less than 10% between DTP1 and DTP3 was done using data reported by national authorities to WHO and UNICEF in the annual Joint Reporting Forms on Immunization. These reports are based on administrative data, which may be biased by inaccurate data on children vaccinated and/or on target populations.
The analysis on the indicator related to health workforce used data from the WHO national workforce accounts data portal. The latest available data were for the year 2022 and were used for an assessment related to the year 2023. This may be misleading in case of significant change in health workforce density in some countries.
The findings of this report should therefore be interpreted with these limitations.
5. Conclusions
The endorsement of the ADI by Heads of States raised the hope that universal immunization will be achieved in Africa with political support at the highest level. Six years later, the road towards universal access to immunization still seems very long. The results of this study have provided evidence that most African countries are still struggling to sustain childhood immunization coverage above set targets, and to lessen subnational inequalities. Suboptimal performance of immunization programmes in most countries suggests the urgent need to enhance application of the “reaching every district” strategy to strengthen routine immunization in health districts. However, seven countries in Africa out of 54 achieved the fourth ADI commitment in 2023, as an integrated part of strong and sustainable primary health care systems. It is critical, as a follow up to this study, to document best practices from these seven countries, that contributed to achieving the fourth ADI commitment. Additionally, deeper analysis of factors associated with achieving the ADI commitments is required.
The African Union Commission, with partners’ support, is urged to give a new impetus to the ADI through renewed commitment by Heads of States and strengthened accountability framework, to put most African countries on track towards achieving the ADI commitments and the 2030 Immunization Agenda targets.
Author Contributions
Conceptualization, F.M. ,C.S.W. and B.I.; methodology, F.M.,AB, A.A.,J.T , A.P,and S.W.; formal analysis, F.M.; data curation, R.O and F.M.; writing—original draft preparation, F.M. ,A.P,A.B and J.T.; writing—review and editing, B.F., B.I., M.M.B., S.N., S.W., C.S.W, and A.A.; visualization, F.M. and R.O.; supervision, B.I.,M.M.B and C.S.W.; project administration, F.M and B.F. and S.N All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available from the corresponding author upon request.
Acknowledgments
The authors would like to express their gratitude to Ministries of Health in WHO African Region for submitting their reports on immunization coverage to WHO and UNICEF through Joint Reporting Forms, and to all colleagues working within the Vaccine Preventable Disease Programme at WHO Regional Office for Africa and WHO Country Offices.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Feldstein, L.R.; Mariat, S.; Gacic-Dobo, M.; Diallo, M.S.; Conklin, L.M.; Wallace, A.S. Global Routine Vaccination Coverage, 2016. MMWR Morb Mortal Wkly Rep 2017, 66, 1252–1255. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Regional Office for Africa. 1 in 5 children in Africa do not have access to life-saving vaccines. Available online: https://www.afro.who.int/news/1-5-children-africa-do-not-have-access-life-saving-vaccines (accessed on day month year).
- Mihigo,R. M.; Okeibunor, J.C.; Karmal, F.; O’Malley, H.; Godinho,N.; Okero, L.; Poy, A.N.; Onyango, O.; Fitzgerald, N.. The Addis Declaration on Immunization: A binding reminder of the political support needed to achieve universal immunization in Africa. Vaccine, 2022, 40, 5126. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Regional Office for Africa. Roadmap for Implementing the Addis Declaration on Immunization: Advocacy, Action, and Accountability. Available online: https://www.afro.who.int/publications/roadmap-implementing-addis-declaration-immunization-advocacy-action-and-accountability (accessed on 23 November 2024).
- World Health Organization Regional Office for Africa. Fulfilling a promise: ensuring immunization for all in Africa. Available online: https://www.afro.who.int/sites/default/files/2017-12/MCIA%20Report.pdf (accessed on 18 November 2024).
- Sharma, M.; Singh, S.K.; Sharma, L.; Dwiwedi, M.K.; Agarwal, D.; Gupta, G.K.; Dhiman, R. Magnitude and causes of routine immunization disruptions during COVID-19 pandemic in developing countries. J. Fam. Med. Prim. Care 2021, 10, 3991. [Google Scholar] [CrossRef] [PubMed]
- Burki, T. WHO ends the COVID-1P public emergency. Lancet Respir Med. 2023, 11, 588. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Countries. Available online: https://www.who.int/countries (accessed on day month year).
- World Health Organization. WHO/UNICEF Joint Reporting Process. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/who-unicef-joint-reporting-process (accessed on 18 November 2024).
- World Health Organisation. Subnational immunization coverage data. Available online: Immunization Analysis and Insights (accessed on 24 November 2024).
- Burton, A.; Monasch, R.; Lautenbach, B.; Gacic-Dobo, M.; Neill, M.; Karimov, R.; Wolfson, L.; Jones, G.; Birmingham, M. WHO and UNICEF estimates of national infant immunization coverage: Methods and processes. Bull. World Health Organ. 2009, 87, 535–541. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Immunization Data Portal. Accessible on: https://immunizationdata.who.int/global? (accessed on 20 November 2024).
- World Health Organization. National Health Workforce Accounts Data Portal. Accessible online: https://apps.who.int/nhwaportal/. (accessed on 20 November 2024).
- R Core Team (2020) The R project for statistical computing. Available at https://www.r-project.org (Accessed ). 18 November.
- ESRI. ArcGIS: The Mapping and Analytics Platform. Available online: https://www.esri.com/en-us/arcgis/about-arcgis/overview (accessed on 1 February 2023).
- Di Giorgio, L.; Moses, MW.; Fullman, N.; Wollum, A.; Conner, R.O.; Achan, J; et al. The potential to expand antiretroviral therapy by improving health facility efficiency: evidence from Kenya, Uganda, and Zambia. BMC Med. 2016, 14, 108. [Google Scholar] [CrossRef] [PubMed]
- Dhalaria, P.; Kapur, S.; Singh, A.K.; Priyadarshini, P.; Dutta, M.; Arora, H.; Taneja, G. Exploring the Pattern of Immunization Dropout among Children in India: A District-Level Comparative Analysis. Vaccines 2023, 11, 836. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Routine Immunization Strategies and Practices (GRISP): A Companion Document to the Global Vaccine Action Plan (GVAP); Accessible online: https://www.who.int/teams/immunization-vaccines-and-biologicals/essential-programme-on-immunization/implementation/global-routine-immunization-strategies-and-practices-(grisp). (accessed on 22 November 2024).
- Kirkby K, Bergen N, Schlotheuber A, Sodha SV, Danovaro-Holliday MC, Hosseinpoor AR. Subnational inequalities in diphtheria-tetanus-pertussis immunization in 24 countries in the African Region. Bull World Health Organ. 2021, 99, 627–639. [Google Scholar] [CrossRef] [PubMed]
- Mboussou, F.; Kada, S.; Danovaro-Holliday, M.C.; Farham, B.; Gacic-Dobo, M.; Shearer, J.C.; Bwaka, A.; Amani, A.; Ngom, R.; Vuo-Masembe, Y.; et al. Status of Routine Immunization Coverage in the World Health Organization African Region Three Years into the COVID-19 Pandemic. Vaccines 2024, 12, 168. [Google Scholar] [CrossRef] [PubMed]
- Okesanya, O.J.; Olatunji, G.; Olaleke, N.O.; Mercy, M.O.; Ilesanmi, A.O.; Kayode, H.H.; Manirambona, E.; Ahmed, M. .;, Ukoaka, B.M.; Lucero-Prisno Iii, D.E. Advancing Immunization in Africa: Overcoming Challenges to Achieve the 2030 Global Immunization Targets. Adolesc Health Med Ther. 2024, 15, 83–91. [Google Scholar] [CrossRef] [PubMed]
- LaFond, A.; Kanagat, N.; Steinglass, R.; Fields, R.; Sequeira, J.; Mookherji, S. Drivers of routine immunization coverage improvement in Africa: findings from district-level case studies. Health Policy Plan. 2015, 30, 298–308. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Reaching Every District (RED) - A guide to increasing coverage and equity in all communities in the African Region. Available online: https://www.afro.who.int/publications/reaching-every-district-red-guide-increasing-coverage-and-equity-all-communities (accessed on 23 November 2024).
- Vandelaer, J.; Bilous, J.; Nshimirimana, D. Reaching Every District (RED) approach: a way to improve immunization performance. Bull World Health Organ. 2008, 86, A–B. [Google Scholar] [CrossRef] [PubMed]
- Gavi, the Vaccine Alliance. Eligibility. Available online: https://www.gavi.org/types-support/sustainability/eligibility (accessed on 23 November 2024).
- Fund for Peace. Fragile States Index annual report 2023. Available online: https://fragilestatesindex.org/2023/06/14/fragile-states-index-2023-annual-report/ (accessed on 23 November 2024).
Figure 1.
Distribution of the percentage of districts with less than 10% dropout rate between DTP1 and DTP3 in 2023 in African countries. DRC: Democratic Republic of Congo; STP: Sao Tome and Principe; CA: Central African Republic.
Figure 1.
Distribution of the percentage of districts with less than 10% dropout rate between DTP1 and DTP3 in 2023 in African countries. DRC: Democratic Republic of Congo; STP: Sao Tome and Principe; CA: Central African Republic.
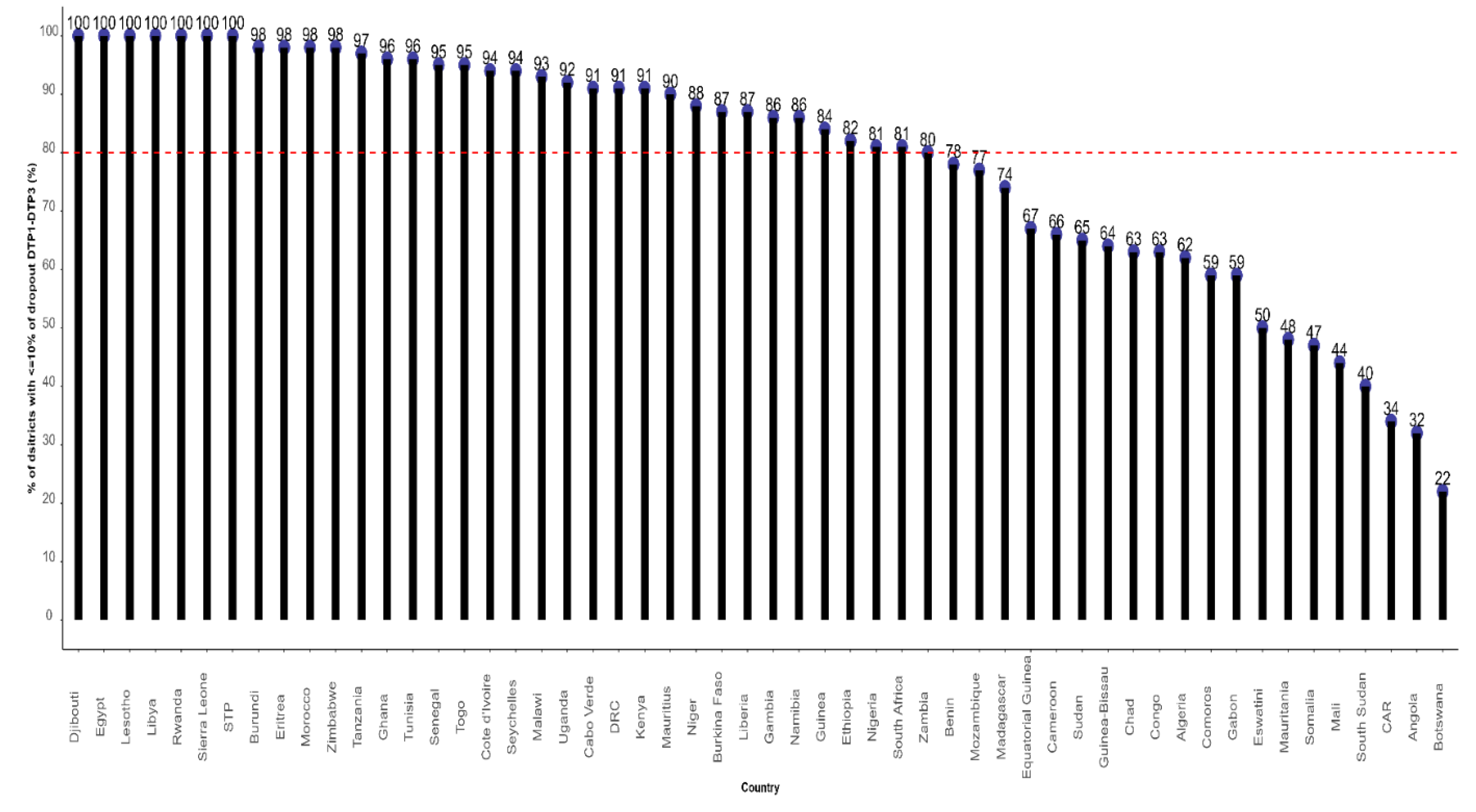
Figure 2.
DTP3 coverage in 2021, 2022 and 2023 by country in Africa (source 2023 WUENIC revision). DRC: Democratic Republic of Congo; STP: Sao Tome and Principe; CA: Central African Republic; Eq_Guinea: Equatorial Guinea.
Figure 2.
DTP3 coverage in 2021, 2022 and 2023 by country in Africa (source 2023 WUENIC revision). DRC: Democratic Republic of Congo; STP: Sao Tome and Principe; CA: Central African Republic; Eq_Guinea: Equatorial Guinea.
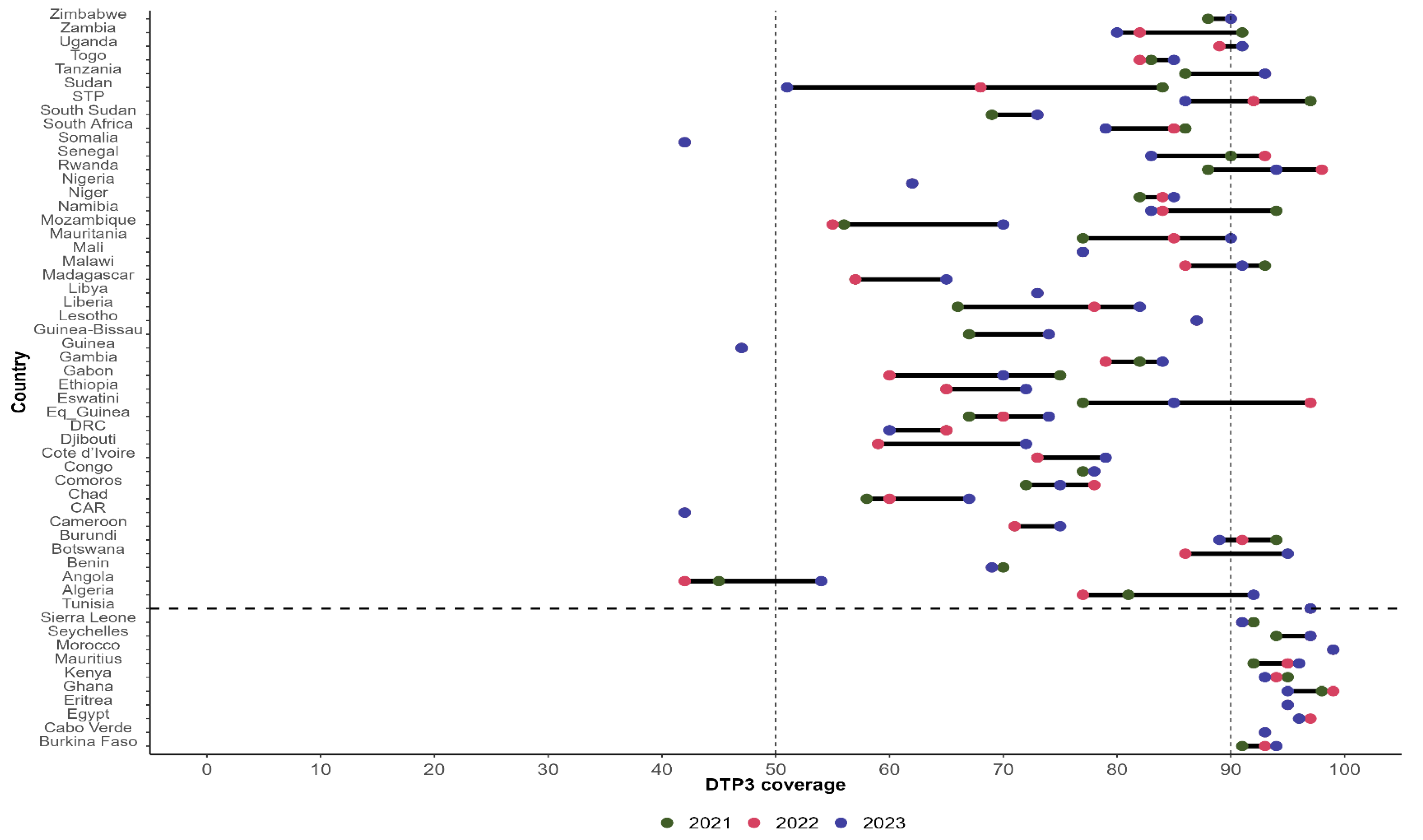
Figure 3.
MCV1 coverage in 2021, 2022 and 2023 by country in Africa (source 2023 WUENIC revision). DRC: Democratic Republic of Congo; STP: Sao Tome and Principe; CA: Central African Republic; Eq_Guinea: Equatorial Guinea.
Figure 3.
MCV1 coverage in 2021, 2022 and 2023 by country in Africa (source 2023 WUENIC revision). DRC: Democratic Republic of Congo; STP: Sao Tome and Principe; CA: Central African Republic; Eq_Guinea: Equatorial Guinea.
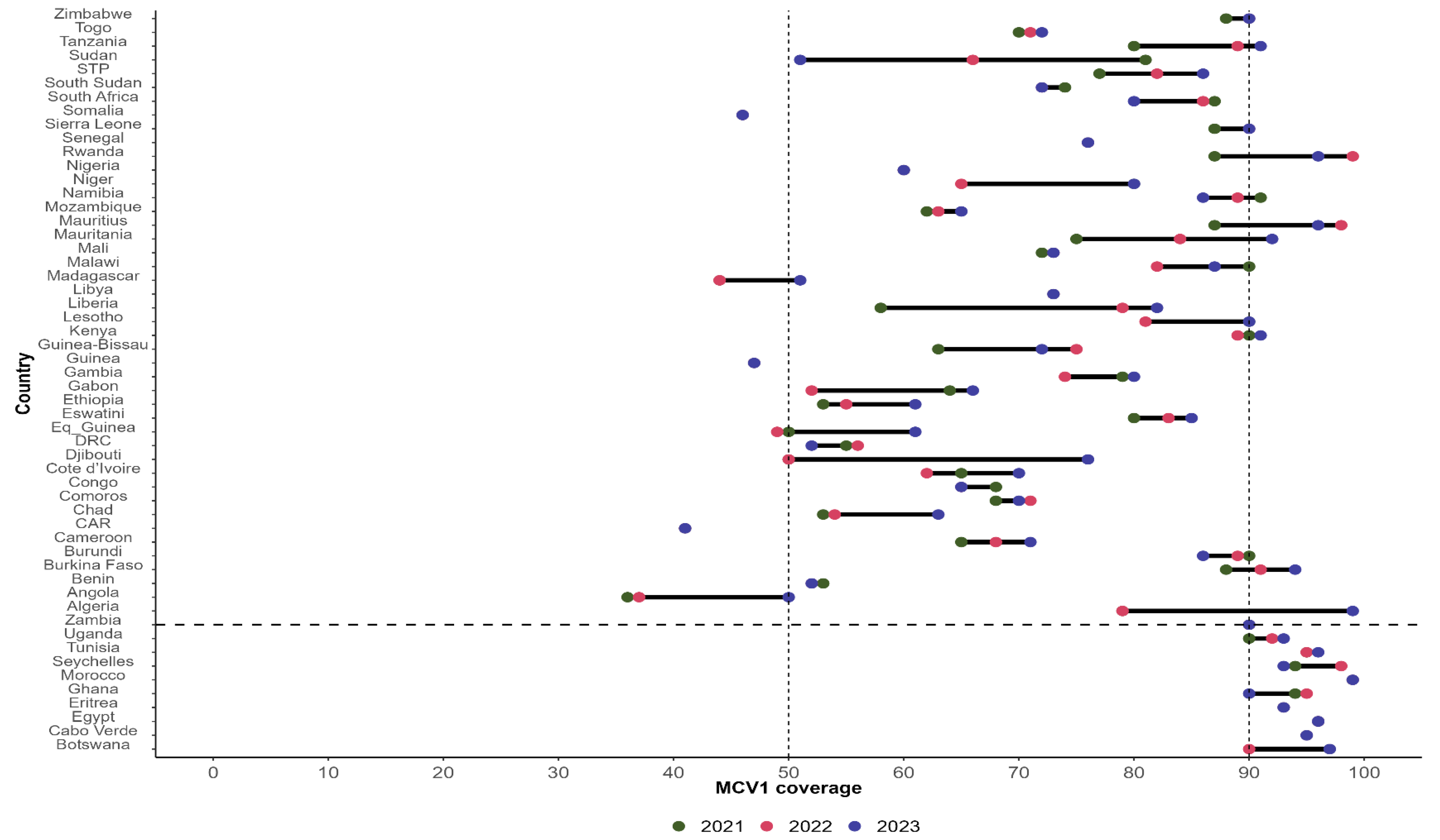
Figure 4.
Geographical distribution of the proportion of the four indicators of the fourth ADI commitment achieved in 2023 by country in Africa.
Figure 4.
Geographical distribution of the proportion of the four indicators of the fourth ADI commitment achieved in 2023 by country in Africa.
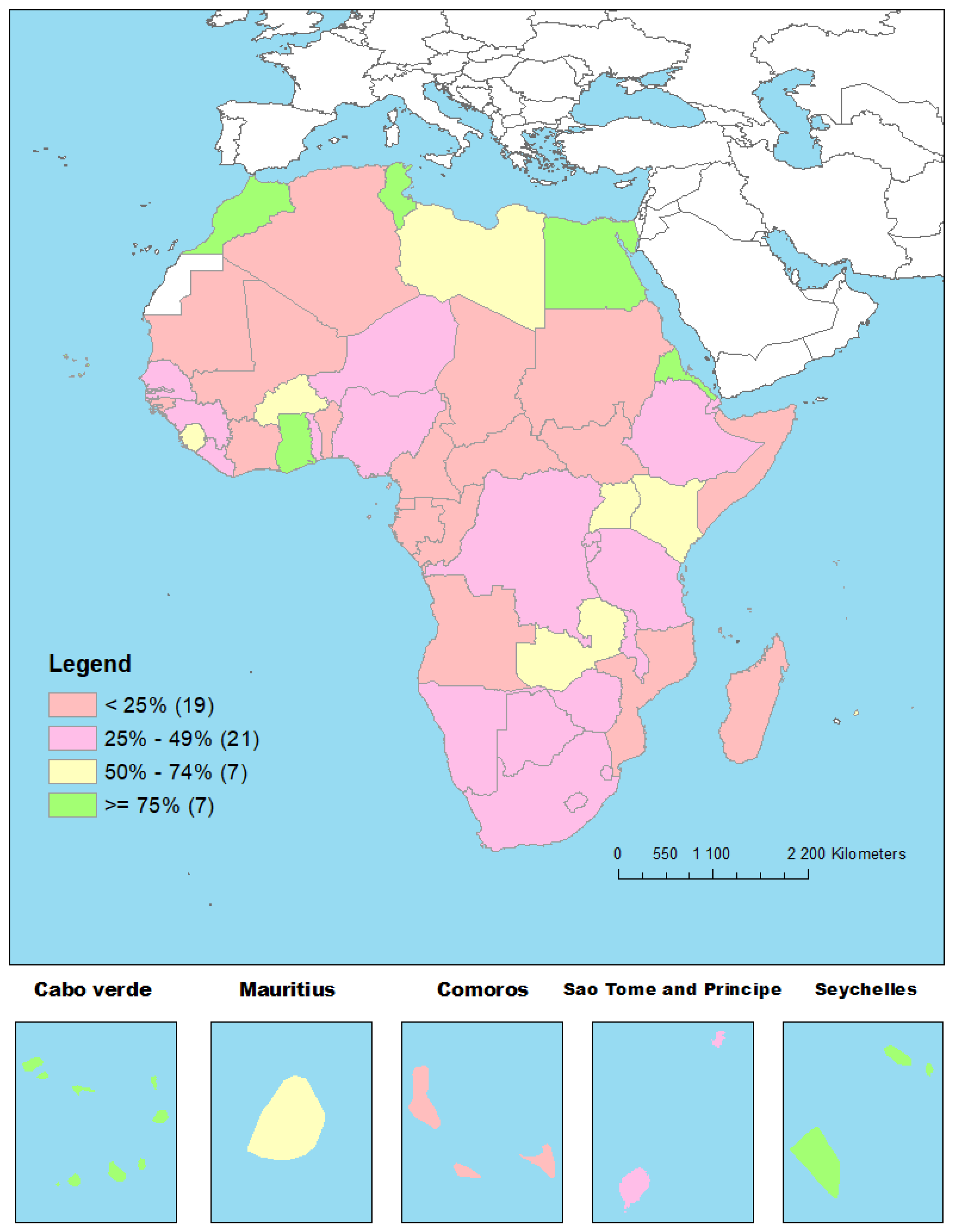

Table 1.
Ten commitments of the Addis Declaration on Immunization [4].
Table 1.
Ten commitments of the Addis Declaration on Immunization [4].
| Commitment number | Commitment description |
|---|---|
| 01 | Keep universal access to immunization at the forefront of efforts to reduce child mortality. |
| 02 | Increase and sustain domestic investments and funding allocations for immunization. |
| 03 | Address the persistent barriers in vaccine and healthcare delivery systems, especially in the poorest, vulnerable, and most marginalized communities. |
| 04 | Increase the effectiveness and efficiency of immunization delivery systems as an integrated part of strong and sustainable primary health care systems. |
| 05 | Attain and maintain high quality surveillance for targeted vaccine preventable diseases. |
| 06 | Monitor progress towards achieving the goals of the global and regional immunization plans. |
| 07 | Ensure polio legacy transition plans are in place. |
| 08 | Develop a capacitated African research sector to enhance immunization implementation and uptake. |
| 09 | Promote and invest in regional capacity for the development and production of vaccines. |
| 10 | Build broad political will for universal access to life-saving vaccines. |
Table 2.
Indicators and criteria of achievement of the fourth Addis Declaration on Immunization commitment.
Table 2.
Indicators and criteria of achievement of the fourth Addis Declaration on Immunization commitment.
| ADI commitment 4: Increase the effectiveness and efficiency of immunization delivery systems as an integrated part of strong and sustainable primary health care systems. | ||
|---|---|---|
| Indicator | Criteria of achievement for each country | Source of data |
| 1. Proportion of countries with over 80% of districts that recorded less than 10% dropout rate between DTP1 and DTP3 | The country has recorded more than 80% of districts with less than 10% dropout rate between DTP1 and DTP3 coverages in 2023. | JRF [9], accessible on WIISE Mart** [10] |
| 2. Proportion of countries with sustained coverage of 90% or above for DPT3 in the past three years | The country has recorded at least 90% DTP3 coverage at national level in 2021, 2022 and 2023 | WUENIC*** [11] accessible on the WHO Immunization Data Portal [12] |
| 3. Proportion of countries with sustained coverage of at least 90% for MCV1 in the past three years. | The country has recorded at least 90% MCV1 coverage at national level in 2021, 2022 and 2023 | WUENIC |
| 4. Proportion of countries with minimum threshold of 44.5 skilled health workers per 10000 people at national level | The country has recorded at least 44.5 skilled health workers per 10000 population at national level in 2022***** | NHWA**** [13] |
* JRF: WHO/UNICEF Joint Report Form. ** WIISE Mart: WHO Immunization Data Warehouse. *** WUENIC: 2023 revision of the WHO and UNICEF Estimates of National Immunization Coverage. **** NHWA: WHO National Health Workforce Accounts Data Portal. ***** The latest available data are from 2022.
Table 3.
Heatmap on the achievement of each of the four indicators of the ADI commitment as od end 2023.
Table 3.
Heatmap on the achievement of each of the four indicators of the ADI commitment as od end 2023.
| Country | Indicator 1 achieved? | Indicator 2 achieved? | Indicator 3 achieved? | Indicator 4 achieved? | Total indicators achieved | % indicators achieved |
|---|---|---|---|---|---|---|
| Algeria | No | No | No | No | 0 | 0 |
| Angola | No | No | No | No | 0 | 0 |
| Benin | No | No | No | No | 0 | 0 |
| Botswana | No | No | Yes | No | 1 | 25 |
| Burkina Faso | Yes | Yes | No | No | 2 | 50 |
| Burundi | Yes | No | No | No | 1 | 25 |
| Cabo Verde | Yes | Yes | Yes | Yes | 4 | 100 |
| Cameroon | No | No | No | No | 0 | 0 |
| Central African Republic | No | No | No | No | 0 | 0 |
| Chad | No | No | No | No | 0 | 0 |
| Comoros | No | No | No | No | 0 | 0 |
| Congo | No | No | No | No | 0 | 0 |
| Cote d’Ivoire | Yes | No | No | No | 1 | 25 |
| Democratic Republic of Congo | Yes | No | No | No | 1 | 25 |
| Djibouti | Yes | No | No | No | 1 | 25 |
| Egypt | Yes | Yes | Yes | No | 3 | 75 |
| Equatorial Guinea | No | No | No | No | 0 | 0 |
| Eritrea | Yes | Yes | Yes | No | 3 | 75 |
| Eswatini | No | No | No | Yes | 1 | 25 |
| Ethiopia | Yes | No | No | No | 1 | 25 |
| Gabon | No | No | No | No | 0 | 0 |
| Gambia | Yes | No | No | No | 1 | 25 |
| Ghana | Yes | Yes | Yes | No | 3 | 75 |
| Guinea | Yes | No | No | No | 1 | 25 |
| Guinea-Bissau | No | No | No | No | 0 | 0 |
| Kenya | Yes | Yes | No | No | 2 | 50 |
| Lesotho | Yes | No | No | No | 1 | 25 |
| Liberia | Yes | No | No | No | 1 | 25 |
| Libya | Yes | No | No | Yes | 2 | 50 |
| Madagascar | No | No | No | No | 0 | 0 |
| Malawi | Yes | No | No | No | 1 | 25 |
| Mali | No | No | No | No | 0 | 0 |
| Mauritania | No | No | No | No | 0 | 0 |
| Mauritius | Yes | Yes | No | No | 2 | 50 |
| Morocco | Yes | Yes | Yes | No | 3 | 75 |
| Mozambique | No | No | No | No | 0 | 0 |
| Namibia | Yes | No | No | No | 1 | 25 |
| Niger | Yes | No | No | No | 1 | 25 |
| Nigeria | Yes | No | No | No | 1 | 25 |
| Rwanda | Yes | No | No | No | 1 | 25 |
| Sao Tome and Principe | Yes | No | No | No | 1 | 25 |
| Senegal | Yes | No | No | No | 1 | 25 |
| Seychelles | Yes | Yes | Yes | Yes | 4 | 100 |
| Sierra Leone | Yes | Yes | No | No | 2 | 50 |
| Somalia | No | No | No | No | 0 | 0 |
| South Africa | Yes | No | No | No | 1 | 25 |
| South Sudan | No | No | No | No | 0 | 0 |
| Sudan | No | No | No | No | 0 | 0 |
| Togo | Yes | No | No | No | 1 | 25 |
| Tunisia | Yes | Yes | Yes | No | 3 | 75 |
| Uganda | Yes | No | Yes | No | 2 | 50 |
| Tanzania | Yes | No | No | No | 1 | 25 |
| Zambia | Yes | No | Yes | No | 2 | 50 |
| Zimbabwe | Yes | No | No | No | 1 | 25 |
| Total countries that achieved the indicator | 34 | 11 | 10 | 4 | ||
| % countries that achieved the indicator | 63 | 20 | 19 | 7 | ||
| Legend | ||||||
| Achieved | ||||||
| No achieved |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions, or products referred to in the content. The authors alone are responsible for the views expressed in this article and they do not necessarily represent the views, decisions or policies of the institutions with which they are affiliated. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



