
Submitted:
03 December 2024
Posted:
04 December 2024
You are already at the latest version
Abstract
Background: Healthcare workers are exposed to an unhealthy environment that increases the risk of developing tuberculosis. Objective: To analyze the prevalence and factors associated with tuberculosis among healthcare workers. Methods: A systematic review with meta-analysis was conducted using six databases. Methodological quality was assessed according to JBI recom-mendations. A random-effects meta-analysis was performed. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines were followed for reporting. Results: Thir-ty-two articles were included in the evidence synthesis. The prevalence of tuberculosis among healthcare workers was found to be 15.92% [95%CI 8.49–27.88 | I² = 99% | p = 0]. Female sex was associated with 1.27 times higher odds of infection [95%CI 0.68–2.38, I² = 80%, p = 0.01]. Advanced age increased the odds by 2.48 times [95%CI 1.33–4.62, I² = 76%, p = 0.01], and having 10 or more years of professional experience increased the odds by 1.08 times [95%CI 1.02–1.15, I² = 57%, p = 0.05] for developing tuberculosis in the healthcare setting. Conclusion: Early diagnosis of tuber-culosis in the workplace and the implementation of continuing education programs with preventive strategies are essential to control contamination and the spread of the disease. PROSPERO registration: CRD42022320153.
Keywords:
Tuberculosis
; Health Professionals
; Health Services
1. Introduction
Tuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis and is considered one of the main communicable diseases of global public health concern. [1,2] Early detection and control of TB represent a challenge for health services, especially for low-income countries with high levels of social inequality. [3]
Brazil is on the list of 30 countries with a high TB burden, accounting for 87% of all TB cases worldwide. [4] TB also results in 1.5 million deaths annually and is classified as the second leading cause of death from a single infectious agent, second only to COVID-19. The disease is also the ninth leading cause of death globally. [5,6] The global annual incidence of TB is estimated at 142 cases per 100,000 inhabitants. [6] In Brazil, 78,057 cases were reported in 2022, resulting in 36.3 cases per 100,000 inhabitants. [7] TB often affects vulnerable groups, [8] including healthcare workers, whether in primary care, outpatient, or hospital settings. [9,10] These professionals are exposed to aerosols produced by infected patients during coughing or sneezing while providing care. [2,9,11] It is estimated that healthcare workers are 1.9 to 5.7 times more likely to develop TB compared to the general population. This risk increases according to the TB burden in the country and the levels of infection control measures. [12] This reality makes the disease an important occupational problem of global concern. [2]
To address this challenge and provide a safer working environment for healthcare workers, the World Health Organization (WHO) established the “End TB” Strategy in 2015, which aims to reduce the incidence of TB by 95% by 2030. To achieve this goal, infection control in healthcare settings was included as a priority component. [13] In Brazil, the Ministry of Health (MoH), in 2014, included in the Notifiable Diseases Information System (SINAN) a field referring to specific populations in which there is a category for healthcare workers, allowing the monitoring of cases in this population. [9]
According to the Ministry of Health, in 2022, 1,141 cases of TB were reported among health workers in Brazil. [7] However, it is important to highlight that these professionals can be infected with M. tuberculosis and not develop the disease, as the bacillus can remain in a latent state for decades. This condition is called Latent Tuberculosis Infection (LTBI), and its prevalence exceeds 30% among healthcare workers. Furthermore, the risk of illness in this group is nearly three times higher than in the general population. [14]
Systematic reviews have been conducted on the subject [15,16,17], most of which present an analysis of prevalence in the general population but do not distinguish among healthcare workers. As mentioned, healthcare workers are considered a risk group for TB, as they are often in direct contact with large loads of the bacillus, depending on their area of work. Particularly healthcare workers in countries with high TB prevalence are at increased risk of TB infection and disease development due to their frequent, prolonged, and close exposure to infectious TB cases. [18]
Therefore, this study becomes relevant because it proposes to understand the prevalence of the disease in this specific population, as well as its related factors, aiming to minimize this knowledge gap still present in the current literature. It is, therefore, essential to carry out a systematic review that updates the evidence on the subject, allowing a critical reflection on the occurrence of TB among health service workers, especially considering the cascade of care. This study aims to analyze the prevalence and factors associated with tuberculosis among healthcare workers.
2. Materials and Methods
Protocol and Registration
This is a systematic literature review with meta-analysis, [19] conducted according to the recommendations and criteria of the Joanna Briggs Institute (JBI)[20] and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. [21] The protocol for this review was registered on York University’s International Prospective Register of Systematic Review (PROSPERO) platform under number CRD42022320153 on April 27, 2022.
Research Question and Eligibility Criteria
The research question was: What is the prevalence and the factors associated with tuberculosis among healthcare workers? The acronym CoCoPop (Condition, Context, and Population) was used. [20] The chosen condition was TB, the context considered was healthcare settings, and the population was healthcare workers.
The inclusion criteria were studies involving healthcare workers (of technical or higher education level) working in healthcare settings, regardless of the level of care. Studies that presented partial results and/or did not directly address the research question were excluded, as were those that investigated associations between TB and other health conditions; those in which it was not possible to access the full data after three attempts to contact the authors by e-mail. It is worth mentioning that there were no time or language restrictions.
Data Source Search
The database search took place in December 2023, covering the following databases: SCOPUS (Elsevier), Web of Science (WoS), MEDLINE (PubMed), CINAHL (Cumulative Index to Nursing and Allied Health Literature), and LILACS (Latin American and Caribbean Health Sciences Literature).
Search Strategy
The search strategy was developed based on terms from the Medical Subject Headings (MeSH). After defining the search terms, the Boolean operators “AND” and “OR” were used. Initially, a pilot test was conducted in MEDLINE. Thus, the following high-sensitivity search strategy was applied to all databases, taking into account the specificities of each source: (Tuberculosis[Title] OR Latent Tuberculosis[Title]) AND (Health Care[Title] OR Health Care Workers[Title] OR Healthcare[Title] OR Physical Therapists[Title] OR Nursing Assistants[Title] OR Patient Care Team[Title] OR Nurse Midwives[Title] OR Nurse Anesthetists[Title] OR Nurses[Title] OR Community Health Workers[Title] OR Physician Assistants[Title] OR Physicians Hospitalists[Title] OR Family Nurse Practitioners[Title] OR Allied Health Personnel Health Occupations[Title] OR Occupational Health Nursing[Title] OR Public Health Nursing Occupational Health[Title] OR Nurses, Community Health[Title] OR Nurses, Public Health[Title] OR Nutritionists[Title] OR Health Services Accessibility[Title] OR Hospital Care[Title] OR Prehospital Care[Title] OR Day Care, Medical[Title] OR Home Care Services, Hospital-Based[Title] OR Health Centers[Title] OR Primary Health Care[Title] OR Healthcare workes[Title] OR Emergency Medical Services[Title] OR Family Health Strategy[Title] OR Intensive Care Units[Title] OR Primary Nursing[Title] OR Mental Health Services[Title] OR Mobile Health Units[Title] OR Radiology Department, Hospital[Title] OR Ambulatory Care[Title] OR Essential Public Health Functions[Title] OR Health Facilities, Proprietary[Title] OR Home Care Services[Title] OR Community Health Services[Title] OR Delivery of Health care[Title] OR Women’s Health Service[Title] OR Secondary Care[Title] OR Tertiary Healthcare[Title] OR Health Services, Indigenous[Title] OR School Health Service[Title] OR Student Health Services[Title] OR Basic Health Services[Title] OR Maternal Health Service[Title] OR Urban Health Services[Title] OR Suburban Health Service[Title] OR Rural Health Services[Title] OR Occupational Health Service[Title] OR Health Services for the Aged[Title] OR Laundry Service, Hospital[Title] OR Adolescent Health Service[Title] OR Public Health Services[Title] OR Emergency Service, Hospital[Title])
Study Selection Process
After screening the articles in the databases, the studies were imported into the literature citation manager Start of the Art through Systematic Review. Subsequently, the references of all the selected studies were searched to identify additional relevant studies. The studies were selected independently and blindly by two reviewers/authors, both with experience in systematic review and the study area. A first reading of titles and abstracts was conducted, with the selected materials being fully reviewed later. Consensus meetings were held regarding the inclusion of articles, and any disagreements were discussed with the participation of a third reviewer/author of the study.
Data Extraction, Processing, and Analysis Process
The results were synthesized in a Microsoft Excel® spreadsheet, taking into account the following variables for extraction: study characteristics (author, year, title, journal, country of origin), methodological aspects (study type, level of care, professionals, and sample), and prevalence results and factors associated with tuberculosis, as well as objectives, main findings, and conclusions.
Evaluation of Methodological Quality
The eligible studies underwent a methodological quality assessment, using the JBI recommendations, by two independent reviewers/authors. In cases of disagreement, the opinion of a third reviewer/author was requested. On a scale consisting of nine criteria, the studies were classified as follows: zero to three criteria (low quality), four to six criteria (medium quality), and seven or more (high quality). [22]
Subsequently, all the articles, regardless of their methodological quality, were subjected to data extraction and narrative synthesis.
Meta-Analysis
To assess the prevalence of TB among health professionals, random effects models were used to present the prevalence as a percentage, together with 95% confidence intervals. Heterogeneity between studies was assessed using the I2 test, in which values above 50% and p-values less than 0.05 indicate high heterogeneity. [23]
For a study to be included in the meta-analysis, it had to provide both the number of workers with TB and the total sample size. In cases where the studies only provided prevalence data, they studied the sample size. The years of data collection for each study were considered to analyze the trend in TB prevalence. [24] Subgroup analyses were conducted considering age, sex, education level, and years of service. The analysis was performed using the R program, with the Meta package.
3. Results
Descriptive Characteristics and Quality of Included Studies
Using the search strategies, 7,392 articles were initially identified, 706 of which were duplicates, 146 records were marked as ineligible by automation tools and 72 records were removed for other reasons. Leaving 6,468 for screening. Next, 5,589 articles that did not meet the inclusion criteria were excluded, including 879 full-text studies. After reading all the articles, 32 were included in the review, as shown in Figure 1.
When evaluating the methodological quality of the studies, 21 articles (65.6%) scored between seven and nine, that is, high quality; of these, eight scored nine, covering all items analyzed for excellence in methodological quality, as described in Table 1.
When analyzing the characterization of the studies included, the majority were published in 2023 (six publications), the first being published in 1985. The investigations were carried out in different countries, including Germany, Saudi Arabia, South Korea, Spain, India, Portugal, and Japan, published in international journals and with a cross-sectional epidemiological design. The characteristics of the articles reveal groups composed mainly of doctors and nurses, developed in high complexity, with an average population of 803.06 health professionals (maximum 4,735 and minimum 35 professionals), As described in Table 2.
Table 3 identified risk factors for developing TB among health workers, such as educational level below higher education (ID: 1372), length of service of more than ten years, absence of BCG (Bacille Calmette-Guérin) vaccination, occupational exposure to TB, female gender, advanced age (workers over 50), smoking, presence of comorbidities such as diabetes mellitus (DM) and hepatitis (ID: 1372; 1376; 1417; 1455; 2020; 2491; 3784; 4336; 4478; 5481; and 6145). The pulmonary clinical form was the most frequently identified (ID: 4572; 6015).
Concerning the type of worker, it was found that the incidence of TB is high among nurses and doctors (ID: 1417; 1448; 4478; 6015; 6145). The incidence of ILTB among health workers is high in the occupational environment, and the main contamination environments for these professionals are wards, the Intensive Care Unit (ICU), the Emergency Room, and Primary Care (ID: 1448; 4478; 6145 and 6328).
The high prevalence of ILTB among healthcare workers means that studies (ID: 1448;1455; 2234; 3784; 4075; 4271; 4478; 5503; 5829) emphasize the need for preventive measures such as pre-employment screening, especially for those employed in areas of high endemicity, annual screening, regular infection control training, frequent use of hand rubbing and use of N95 masks as Personal Protective Equipment, as well as maintaining surveillance programs and adopting and stricter preventive strategies against infection.
Prevalence of Tuberculosis Among Healthcare Workers
In the analysis of prevalence, 23 studies were included, highlighting high heterogeneity between the studies, with an I² value of 99% = 2.5350, p = 0. The result of the meta-analysis showed an active TB prevalence of 15.98% [9.00 – 26.78], with a total population across all studies of 63,371 healthcare workers (Figure 2).
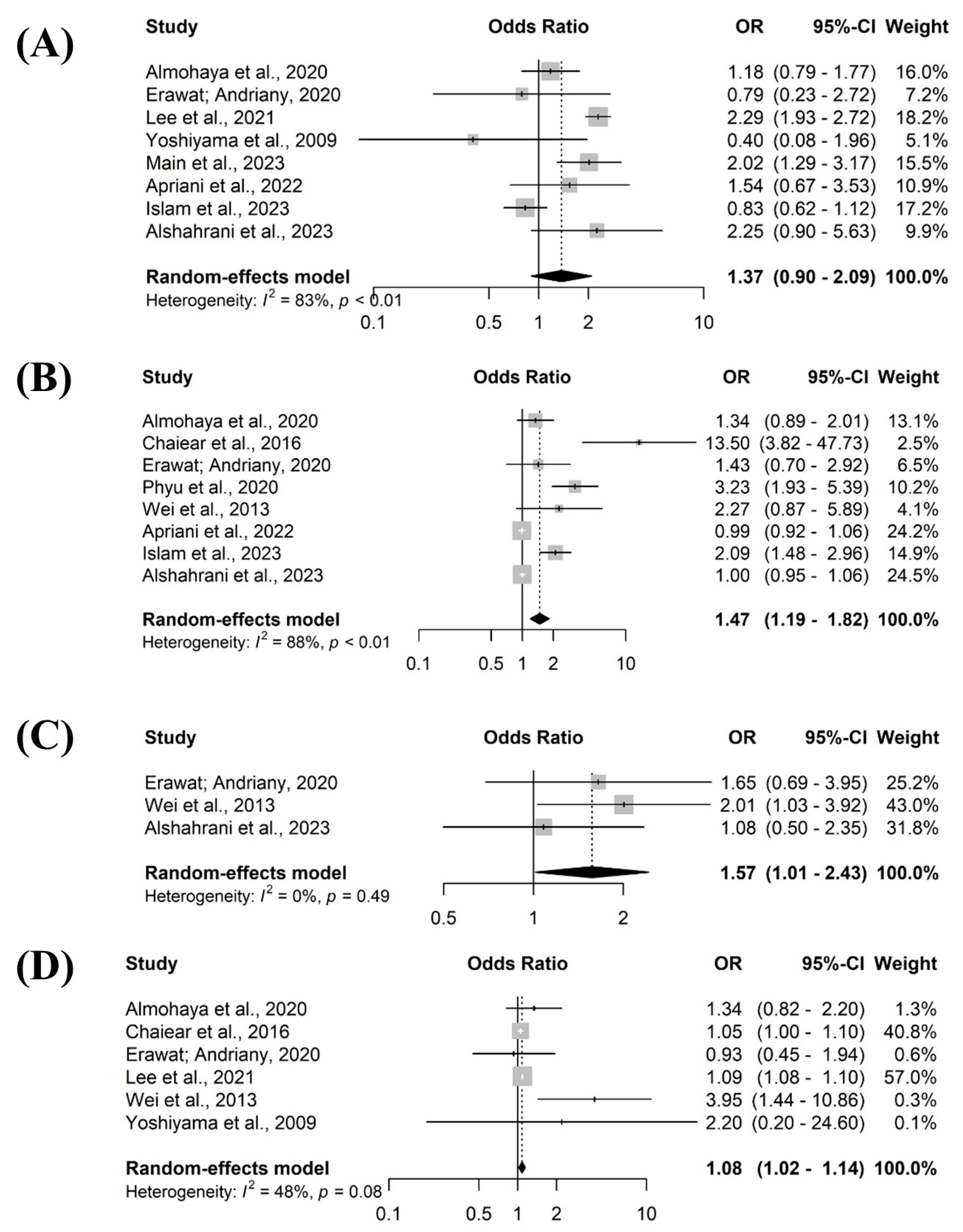
The meta-analysis of associated factors revealed that the older the professional, the greater the chance of developing TB 1.47 [95% CI 1.19 – 1.82 I2 = 88%, p = 0.01] (figure B/ 3), being a graduate was 1.57 more likely [95% CI 1.01 – 2.43 I2 = 0%, p = 0.49] (figure C/3) and having ten years or more of professional experience increased the chances at 1.08 [95% CI 1.02 - 1.14 I2 = 48%, p = 0.08] (figure D/3).
Figure 3.
Factors related to tuberculosis among health professionals. Rio Grande do Sul, Brazil, 2024.
Figure 3.
Factors related to tuberculosis among health professionals. Rio Grande do Sul, Brazil, 2024.
4. Discussion
Through the synthesis of this review, the prevalence and associated factors of TB in healthcare workers were found. The meta-analysis revealed that the prevalence of active TB among workers was 15.98% [9.00 – 26.78], and when analyzing the associated factors, female sex showed 1.27 times higher chances of developing TB, while older age and more than 10 years of professional experience had 2.48 and 1.08 times higher chances, respectively, of developing the disease.
These results corroborate the systematic review, which showed a prevalence of TB among health workers of 28% (95% CI 21-36) and occupational risk factors are related to direct contact with patients with active TB and having more professional experience, i.e., the longer the time in the health service, the greater the chances of developing the disease. [25]
TB, being a serious public health problem in health services, directly affects workers in these service institutions. This problem has been forgotten or minimized for a long time by health institution managers and/or government representatives but is back in the discussion today by incorporating health workers as a target population, that is, a priority for combating and eliminating TB in the world. [9,18,26]
These results are in line with the proposals made by the WHO [13] in conjunction with the Ministry of Health, [9] which include health workers as a population with a higher probability of developing TB due to exposure and work characteristics, i.e., workers have direct and indirect contact with Mycobacterium tuberculosis during patient care. [27,28] Furthermore, the risk of exposure and acquisition of TB in the workplace is a concrete factor, and professional categories such as nursing, medicine, and physiotherapy are more exposed to infection, considering their duties. [29]
It is worth noting that TB is transmitted via the respiratory tract through inhaling aerosols produced by the coughing, talking, or sneezing of a patient with active TB. Thus, when the bacilli are expelled, they remain dispersed in the occupational environment in the form of aerosols for a period that depends on the environmental characteristics of the location, i.e., ventilation conditions and direct sunlight. [30] Bacillus is highly contagious and has serious effects on workers’ health. Signs and symptoms can take a long time to manifest in the airways, which poses a challenge for early prevention measures to eliminate the bacteria. [29]
In addition, the transmission of the bacteria to healthcare workers depends on different factors, such as the type of job they do, the length of time they have been exposed to it in the workplace, and the number of years they have worked, i.e., the longer they have worked, the greater the risk of developing the disease. [31]
It is also worth noting that the transmission of TB within healthcare services is related to the effectiveness of preventive interventions carried out by managers, as well as the implementation of ongoing education among workers and the use of personal protective equipment. [26] Healthcare professionals use personal protective equipment to shield themselves from cough droplets, sneezes, or other bodily fluids from infected patients and contaminated surfaces that could infect them. Therefore, using such equipment helps reduce the chances of contamination. [32]
A study carried out in Nepal, which sought to assess the knowledge and practice of nurses in preventing and controlling TB infection, found that most nurses had an inadequate level of knowledge and poor practice of TB prevention and control. In terms of practice, none of the nurses reported using an N95 mask or respirator when caring for TB patients. [33]
Therefore, health workers are vulnerable to TB infection, Labor laws mention that TB is considered a disease related to the work environment and, in Brazil, it is an occupational disease that is compulsorily notifiable to the SINAN. [34]
Concerning the categories of health workers and their expectation of TB infection compared to the general population, the literature shows a risk 3 to 20 times higher among nursing staff, 6 to 11 times higher among clinical pathologists, four to eight times higher among students (nursing, physiotherapy, and medicine); and two to nine times higher among bacteriology laboratory technicians. [35]
A study of nurses in China found that the prevalence of TB among nurses working in TB-related departments is 5.1 times higher than in the general population, and the incidence of LTBI among healthcare workers is between 17 and 36%. [27] In a study of 1,870 healthcare workers in South Korea, 12% (229) tested positive for TB, and those of advanced age were 0.96 times more likely to develop the disease. [33] In a cross-sectional study assessing the burden of LTBI among health workers in Afghanistan, with 4,648 health workers, the prevalence of latent TB infection was 47.2% (1,738 workers). [37] In Germany, the prevalence of LTBI is estimated at 10% based on examinations carried out in connection with the country’s occupational and preventive medicine. [38]
Authors have found that nursing staff in hospitals are the most at risk of contracting TB, which corroborates the results of this review, which shows that nursing staff are the most likely to fall ill with TB. In addition, the disease is highly prevalent among other professional categories, such as healthcare assistants and maintenance workers, radiology technicians, pharmacists, physiotherapists, nutritionists, and medical students. [28]
Health workers, in addition to being at increased risk of developing TB due to their working environment, as already noted, are also at risk of developing drug-resistant TB compared to the general population. [40]
However, when analyzing Brazilian studies on TB in health workers, there is a gap in knowledge, in other words, invisibility. [41] Furthermore, controlling TB effectively is a matter of extreme concern since the lack of research in a given area of knowledge makes this population invisible to public health policies, leading to negative consequences for workers’ health and a lack of health coverage and prevention.
In order to achieve the ambitious targets set by the WHO through the End TB by 2035 strategy, countries need to incorporate innovation, investment, and the authority of effective public policies that reach vulnerable populations, including health workers. [9,13] The burden of TB on healthcare workers is a negative labor-related factor and, due to its nosocomial transmission, can make it difficult to achieve the goals of eliminating and eradicating TB since healthcare workers act as a reservoir of the bacillus, thus contributing to maintaining the cycle of transmission of the disease in society. [28]
The transmission of TB in health services to workers is related to non-existent or inadequate infection control measures, especially in places with few material and physical resources. [28,31] This risk is proportionally more alarming in low- and middle-income countries due to increased exposure and the lack of preventive measures, such as poor ventilation in the workplace and inadequate precautions during sputum collection and bronchoscopy. [38]
Other occupational risk factors associated with LTBI include being a nurse, a diabetic, a smoker, being over 35 years old, working in cleaning services, hospitalization units with high patient turnover, assisting people living with HIV, not having been vaccinated with Bacille Calmette-Guérin or being immunocompromised. [37]
Thus, investment in research, policies and programs aimed at this high-priority population must be implemented and incorporated, especially in countries that have a high burden of circulating TB. In addition, by incorporating measures in health services to protect against ILTB through TB Preventive Therapy (TPT), with the implementation of this measure in health services, there is a potential reduction in the risk of progression of the disease by up to 90%; TPT aims to eliminate bacteria during their dormant state, thus maintaining a low rate of progression of the bacillus in the work environment, which consequently reduces transmission among health workers. [38]
To reduce the rate of contamination among healthcare workers, it is recommended to implement screening and treatment of ILTB to prevent TB development among workers and transmission to other individuals. [42] Furthermore, a systematic review [43] highlighted the need to standardize methods for researching TB recurrence, promote actively seeking prevention of drug resistance, facilitate treatment retention and provide integrated care for patients with HIV that can reduce recurrence rates. Some countries, such as China, include in their institutional policies annual screening for ILTB among workers at high risk of exposure, as well as treatment. [36]
Therefore, to invest in data reduction measures associated with the risk of bacillus contamination in the occupational environment, it is essential that managers recognize the risk factors and develop actions and strategies for minimizing, reducing, and eliminating the risk of developing and maintaining TB in the occupational environment.
It should be noted that studies have pointed to weaknesses in the implementation of infection control measures in health services, resulting in health professionals understanding that only the use of personal protective equipment is sufficient for individual and collective protection. There is still a lack of knowledge on the part of many health professionals about the importance of screening as a biosafety measure. [41]
Health institutions must carry out periodic screening programs to identify and monitor TB among health workers and establish effective administrative, environmental, and individual protection measures to prevent infection in professionals at risk of exposure to M. tuberculosis. These measures are necessary because they contribute to achieving the targets set by the WHO. [33]
Considering the above, it should be emphasized that the risk of acquiring TB in the workplace among health workers, especially those on the front line, is real. As such, joint actions are needed between these workers and managers to implement TB prevention strategies, reduce the number of illnesses, and provide appropriate treatment.
Finally, it is important to emphasize that systematic reviews are at the top of the levels of evidence and that this study rigorously followed the JBI recommendations to find evidence on the prevalence and factors associated with TB in healthcare workers. However, as a limitation of the study, it is important to mention that this meta-analysis should be interpreted considering the methodological quality of the studies included, and another limitation is the heterogeneity of the studies, which made further comparisons impossible.
5. Conclusions
This review provided relevant data on TB in health workers and helped to identify the risk factors associated with its infection. There is a need for early diagnosis of TB in the workplace and ongoing education with a rigorous preventive strategy to control contamination and spread, both in the workplace and in the social environment where the professional is inserted.
Author Contributions
The following statements should be used “Conceptualization, A.R.S. and P.O.B.; methodology, A.R.S and O.L.M.; software, M.C.S and F.M.D.; validation, A.R.S and O.L.M.; formal analysis, J.T.M., F.M.P and E.C.M.; investigation, A.R.S., P.O.B and M.C.S.; resources, F.M.D.; data curation, A.R.S., J.T.M., J.D.A and M.Y.; writing—original draft preparation, A.R.S., T.Z.B, and Y.M.A.; writing—review and editing, A.R.S., T.Z.B and O.L.M.; visualization, M.J.Q.G and R.A.A.; supervision, A.R.S.; project administration, A.R.S and R.A.A.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lv H, Zhang X, Zhang X, et al. Global prevalence and burden of multidrug-resistant tuberculosis from 1990 to 2019. BMC Infect Dis. 2024;24(1):243. [CrossRef]
- Silva TC, Pinto ML, Orlandi GM, et al. Tuberculosis from the perspective of men and women. Rev Esc Enferm USP. 2022;56:e20220137. [CrossRef]
- Amare D, Getahun FA, Mengesha EW, et al. Effectiveness of healthcare workers and volunteers training on improving tuberculosis case detection: A systematic review and meta-analysis. PLoS One. 2023;18(3):e0271825. [CrossRef]
- Chitwood MH, Alves LC, Bartholomay P, et al. A spatial-mechanistic model to estimate subnational tuberculosis burden with routinely collected data: An application in Brazilian municipalities. PLOS Glob Public Health. 2022;2(9):e0000725. [CrossRef]
- Ryuk DK, Pelissari DM, Alves K, et al. Predictors of unsuccessful tuberculosis treatment outcomes in Brazil: an analysis of 259,484 patient records. BMC Infect Dis. 2024;24(1):531. [CrossRef]
- Żukowska L, Zygała-Pytlos D, Struś K, et al. An overview of tuberculosis outbreaks reported in the years 2011-2020. BMC Infect Dis. 2023;23(1):253. [CrossRef]
- Ministry of Health. Tuberculosis: Epidemiological Bulletin. 1st ed. Brazil: Ministry of Health, 2022.
- Santos MNA, Sá AMM, Quaresma JAS. Meanings and senses of being a health professional with tuberculosis: an interpretative phenomenological study. BMJ Open. 2020;10(8):e035873. [CrossRef]
- Ministry of Health. Brazil Free of Tuberculosis: National Plan to End Tuberculosis as a Public Health Problem. Ministry of Health, Secretariat of Health Surveillance, Department of Communicable Disease Surveillance. – Brasília: Ministry of Health, 2017.
- Pustiglione M, Galesi VMN, Santos LAR, et al. Tuberculosis in health care workers: a problem to be faced. Rev Med 2020;99(1):16-26. [CrossRef]
- Monroe LW, Johnson JS, Gutstein HB, et al. Preventing spread of aerosolized infectious particles during medical procedures: A lab-based analysis of an inexpensive plastic enclosure. PLoS One. 2022;17(9):e0273194. [CrossRef]
- Shiferaw MB, Sinishaw MA, Amare D, et al. Prevalence of active tuberculosis disease among healthcare workers and support staff in healthcare settings of the Amhara region, Ethiopia. PLoS One. 2021;16(6):e0253177. [CrossRef]
- World Health Organization. Global Tuberculosis Report 2019. Geneva: WHO, 2019.
- Caruso E, Mangan JM, Maiuri A, et al. Tuberculosis Testing and Latent Tuberculosis Infection Treatment Practices Among Health Care Providers - United States, 2020-2022. MMWR Morb Mortal Wkly Rep. 2023;72(44):1183-1189. [CrossRef]
- Silva EH, Lima E, Santos TR, et al. Prevalence and incidence of tuberculosis in health workers: A systematic review of the literature. Am J Infect Control. 2022;50(7):820-827. [CrossRef]
- Sossen B, Richards AS, Heinsohn T, et al. The natural history of untreated pulmonary tuberculosis in adults: a systematic review and meta-analysis. Lancet Respir Med. 2023;11(4):367-379. [CrossRef]
- Ismail H, Reffin N, Wan Puteh SE, et al. Compliance of Healthcare Worker’s toward Tuberculosis Preventive Measures in Workplace: A Systematic Literature Review. Int J Environ Res Public Health. 2021;18(20):10864. [CrossRef]
- Klayut W, Srisungngam S, Suphankong S, et al. Prevalence, Risk Factors, and Result Features in the Detection of Latent Tuberculosis Infection in Thai Healthcare Workers Using QuantiFERON-TB Gold Plus. Cureus. 2024;16(5):e60960. [CrossRef]
- Peters MDJ, Godfrey C, McInerney P, et al. Systematic reviews of prevalence and incidence — JBI manual for evidence synthesis—JBI Global Wiki. 2020.
- Munn Z, Barker TH, Moola S, et al. Methodological quality of case series studies: an introduction to the JBI critical appraisal tool. JBI Evidence Synthesis 18(10):p 2127-2133. [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. [CrossRef]
- Joanna Briggs Institute. Critical appraisal tools—critical appraisal tools | JBI. 2020.
- Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539-1558. [CrossRef]
- Schwarzer G. General package for meta-analysis. 4.19–1. 2021.
- Silva EH, Lima E, Santos TR, Padoveze MC. Prevalence and incidence of tuberculosis in health workers: A systematic review of the literature. Am J Infect Control. 2022;50(7):820-827. [CrossRef]
- Meregildo-Rodriguez ED, Yuptón-Chávez V, Asmat-Rubio MG, et al. Latent tuberculosis infection (LTBI) in health-care workers: a cross-sectional study at a northern Peruvian hospital. Front Med (Lausanne). 2023;10:1295299. [CrossRef]
- Wang F, Ren Y, Liu K, et al. Large gap between attitude and action in tuberculosis preventive treatment among tuberculosis-related healthcare workers in eastern China. Front Cell Infect Microbiol. 2022;12:991400. [CrossRef]
- Main S, Triasih R, Greig J, et al. The prevalence and risk factors for tuberculosis among healthcare workers in Yogyakarta, Indonesia. PLoS One. 2023;18(5):e0279215. [CrossRef]
- Pustiglione M, Galesi VMN, Santos LAR, et al. Tuberculosis in health care workers: a problem to be faced. Rev Med (São Paulo). 2020;99(1):16-26. [CrossRef]
- Alsayed SSR, Gunosewoyo H. Tuberculosis: Pathogenesis, Current Treatment Regimens and New Drug Targets. Int J Mol Sci. 2023;24(6):5202. [CrossRef]
- Azeredo ACV, Holler SR, Almeida EGC, et al. Tuberculosis in Health Care Workers and the Impact of Implementation of Hospital Infection-Control Measures. Workplace Health & Safety. 2020;68(11):519-525. [CrossRef]
- Verbeek JH, Rajamaki B, Ijaz S, et al. Personal protective equipment for preventing highly infectious diseases due to exposure to contaminated body fluids in healthcare staff. Cochrane Database Syst Rev. 2020;5(5):CD011621. [CrossRef]
- Baral MA, Koirala S. Knowledge and Practice on Prevention and Control of Tuberculosis Among Nurses Working in a Regional Hospital, Nepal. Front Med. 2022;8:788833. [CrossRef]
- Danielle P, Maria-Catarina M, Fabiana S, et al. Occupational tuberculosis: document analysis of a university hospital in Rio de Janeiro. Rev. Cubana Enfermer. 2015; 31 (4). http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-03192015000400002&lng=e.
- Ministry of Health. Guidelines for the prevention and diagnosis of tuberculosis in healthcare professionals. Brasília: Ministry of Health, 2021. 36 p.
- Kim JY, Jung J, Jung KJ, et al. Frequency of and risk factors for reversion of QuantiFERON test in healthcare workers in an intermediate-tuberculosis-burden country. Clin Microbiol Infect. 2021 ;27(8):1120-1123. [CrossRef]
- Qader GQ, Seddiq MK, Rashidi KM, et al. Prevalence of latent tuberculosis infection among health workers in Afghanistan: A cross-sectional study. PLoS One. 2021;16(6):e0252307. [CrossRef]
- Zielinski N, Stranzinger J, Zeeb H, et al. Latent Tuberculosis Infection among Health Workers in Germany-A Retrospective Study on Progression Risk and Use of Preventive Therapy. Int J Environ Res Public Health. 2021;18(13):7053. [CrossRef]
- Aldhawyan NM, Alkhalifah AK, Kofi M, et al. Prevalence of Latent Tuberculosis Infection Among Nurses Working in Critical Areas at a Tertiary Care Hospital in Riyadh, Saudi Arabia. Cureus. 2024;16(2):e53389. [CrossRef]
- Tudor C, Walt MLV, Margot B, et al. Occupational Risk Factors for Tuberculosis Among Healthcare Workers in KwaZulu-Natal, South Africa. Clin Infect Dis. 2016 May 15;62 Suppl 3(Suppl 3):S255-61. [CrossRef]
- Prado TN, Galavote HS, Brioshi AP, et al. Epidemiological profile of reported cases of tuberculosis among health professionals at the University Hospital in Vitória (ES) Brazil. J bras pneumol. 2008;34(8):607-13. [CrossRef]
- Aksornchindarat W, Yodpinij N, Phetsuksiri B, et al. T-SPOT®.TB test and clinical risk scoring for diagnosis of latent tuberculosis infection among Thai healthcare workers. J Microbiol Immunol Infect. 2021;54(2):305-311. [CrossRef]
- Vega V, Cabrera-Sanchez J, Rodríguez S, et al. Risk factors for pulmonary tuberculosis recurrence, relapse and reinfection: a systematic review and meta-analysis. BMJ Open Respir Res. 2024;11(1):e002281. [CrossRef]
Figure 1.
Flowchart illustrating the process of including and excluding studies. Paraná, Brazil, 2024.
Figure 1.
Flowchart illustrating the process of including and excluding studies. Paraná, Brazil, 2024.
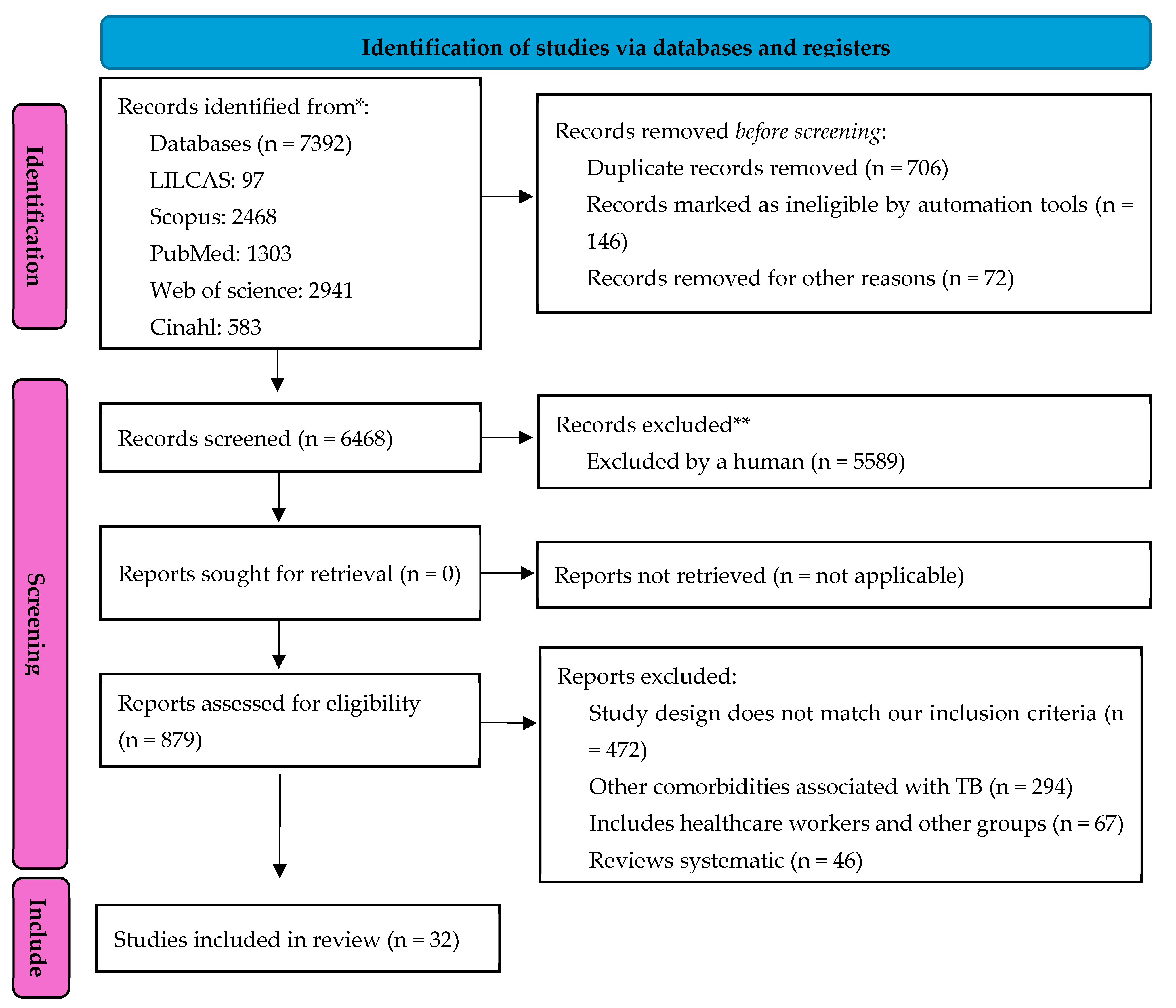
Figure 2.
Prevalence of tuberculosis among health professionals.
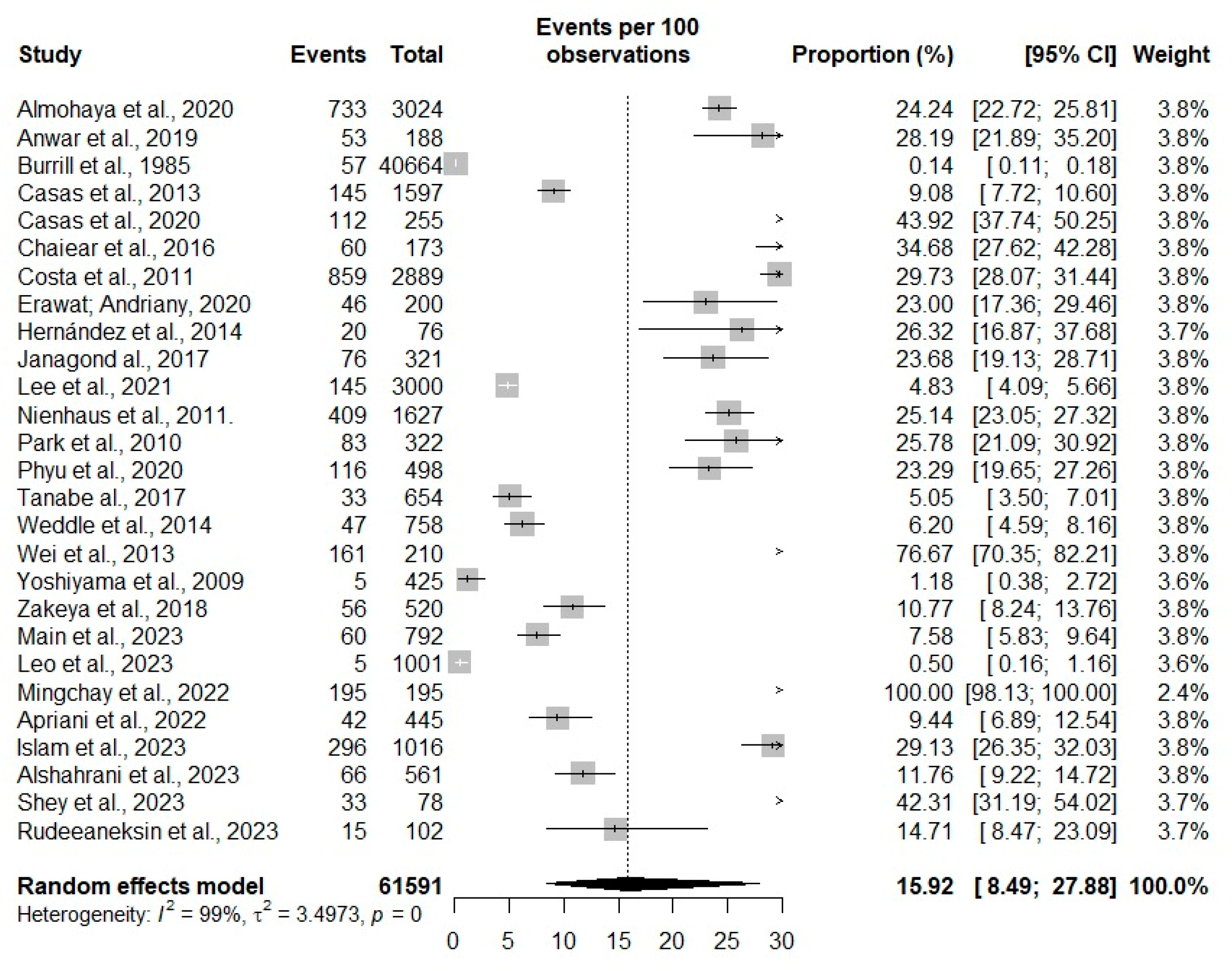

Table 1.
Critical assessment of methodological quality JBI. Paraná, Brazil, 2024.
| ID | AUTHOR (DATE) | 1. Is the sampling frame appropriate to address the target population? | 2. Were study participants sampled appropriately? | 3. Was the sample size adequate? | 4. Were the participants and study design described in detail? | 5. Was data analysis performed with sufficient sample coverage? | 6. Were valid methods used to identify the condition? | 7. Was condition measured in a standardized and reliable manner? | 8. Was there appropriate statistical analysis? | 9. Was the response rate adequate, and if not, was the low response rate managed correctly? | Final score |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 78 | Main et al., 2023 | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (+) | 9 |
| 570 | Leo et al., 2023 | (+) | (+) | (+) | (+) | (+) | (+) | (I) | (I) | (+) | 7 |
| 6321 | Islam et al., 2023 | (+) | (+) | (+) | (-) | (-) | (+) | (I) | (-) | (+) | 5 |
| 6323 | Alshahrani et al., 2023 | (+) | (-) | (+) | (-) | (+) | (+) | (+) | (-) | (+) | 6 |
| 6330 | Shey et al., 2023 | (I) | (I) | (I) | (-) | (-) | (+) | (+) | (-) | (+) | 3 |
| 6337 | Rudeeaneksin et al., 2023 | (I) | (I) | (I) | (-) | (-) | (+) | (+) | (+) | (+) | 4 |
| 6298 | Apriani et al., 2022 | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (+) | 9 |
| 574 | Mingchay et al., 2022 | (I) | (-) | (-) | (-) | (-) | (+) | (+) | (+) | (+) | 4 |
| 1372 | Phyu et al., 2020 | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (I) | 8 |
| 1376 | Casas et al., 2020 | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (+) | 9 |
| 1417 | Erawat; Andriany, 2020 | (+) | (+) | (+) | (-) | (+) | (+) | (+) | (-) | (+) | 7 |
| 1448 | Janagond al., 2017 | (+) | (+) | (+) | (-) | (I) | (+) | (+) | (+) | (+) | 7 |
| 1455 | Anwar et al., 2019 | (+) | (+) | (+) | (-) | (+) | (+) | (+) | (+) | (+) | 8 |
| 1490 | Zakeya et al., 2018 | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (+) | 9 |
| 1572 | Raitio et al., 2003 | (+) | (+) | (+) | (I) | (+) | (+) | (+) | (+) | (+) | 9 |
| 2020 | Costa et al., 2011 | (+) | (+) | (+) | (-) | (+) | (+) | (+) | (+) | (+) | 8 |
| 2234 | Casas et al., 2013 | (+) | (-) | (I) | (-) | (I) | (+) | (I) | (+) | (+) | 4 |
| 2491 | Lee et al., 2021 | (+) | (+) | (+) | (-) | (+) | (+) | (+) | (+) | (+) | 8 |
| 3784 | Chaiear et al., 2016 | (+) | (-) | (+) | (-) | (I) | (-) | (-) | (-) | (+) | 3 |
| 4075 | Wei et al., 2013 | (+) | (+) | (+) | (I) | (+) | (+) | (+) | (-) | (+) | 7 |
| 4225 | Nienhaus et al., 2011. | (+) | (-) | (+) | (-) | (I) | (+) | (I) | (+) | (+) | 5 |
| 4271 | Park et al., 2010 | (+) | (+) | (+) | (I) | (+) | (+) | (+) | (-) | (+) | 8 |
| 4336 | Yoshiyama et al., 2009 | (+) | (+) | (+) | (-) | (+) | (+) | (+) | (+) | (+) | 8 |
| 4478 | Drobniewski et al., 2007 | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (+) | 9 |
| 4572 | Gopinatha et al., 2003 | (-) | (+) | (+) | (-) | (-) | (+) | (+) | (-) | (+) | 5 |
| 5481 | Weddle et al., 2014 | (+) | (+) | (+) | (-) | (+) | (+) | (+) | (-) | (+) | 7 |
| 5503 | Burrill et al., 1985 | (+) | (+) | (+) | (-) | (+) | (+) | (+) | (-) | (+) | 7 |
| 5829 | Costa et al., 2009 | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (+) | 9 |
| 5839 | Tanabe al., 2017 | (+) | (I) | (+) | (-) | (+) | (+) | (+) | (+) | (+) | 7 |
| 6145 | Almohaya et al., 2020 | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (+) | (+) | 9 |
| 6329 | Ringshausen et al 2011 | (I) | (+) | (I) | (-) | (I) | (+) | (+) | (+) | (+) | 5 |
| 6436 | Hernández et al., 2014 | (I) | (-) | (-) | (-) | (-) | (+) | (+) | (+) | (I) | 3 |
Source: Prepared by the authors, adapted from JBI. [22] Note: (-) did not meet this criterion; (+) met this criterion; (I) uncertain/not clear. The score ranges from 0 to 9, with higher scores indicating better study quality.
Table 2.
Distribution of study characterization. Rio Grande do Sul, Brazil, 2024.
| ID | Title | Authors/years | Journal | Location | Study design | Level of care | Workers investigated | Sample |
|---|---|---|---|---|---|---|---|---|
| 78 | The prevalence and risk factors for tuberculosis among healthcare workers in Yogyakarta, Indonesia | Main et al., 2023 | Plos One | Indonesia | Cross-sectional | Primary care And Medium complexity |
Doctor, nurse, dentist, nutritionist, and pharmacist. | 792 |
| 570 | Active case finding for tuberculosis among health care workers in a teaching hospital, Puducherry, India | Leo et al., 2023 | Indian J Occup Environ Med. | India | Cross-sectional | High complexity | Doctor, nurse, and laboratory yechnician | 1001 |
| 6321 | Prevalence and incidence of TB infection among healthcare workers in chest diseases hospitals, Bangladesh: Putting infection control into context. | Islam et al., 2023 | Plos One | Bangladesh | Prospectivo | High complexity | Doctor, nurses, pharmacists, administrative staff, laboratory team, and auxiliary workers | 1.016 |
| 6323 | The Risk of Latent Tuberculosis Infection Among Healthcare Workers at a General Hospital in Bisha, the Kingdom of Saudi Arabia. | Alshahrani et al., 2023 | Cureus | Saudi Arabia | Cross-sectional | High complexity | Doctor, nurses and Other technicians | 561 |
| 6330 | Mycobacterial-specific secretion of cytokines and chemokines in healthcare workers with apparent resistance to infection with Mycobacterium TB. | Shey et al., 2023 | Front Immunol | South Africa | Cross-sectional | Primary care And Medium complexity |
Healthcare professionals | 78 |
| 6337 | QuantiFERON-TB Gold Plus and QuantiFERON-TB Gold In-tube assays for detecting latent TB infection in Thai healthcare workers. | Rudeeaneksin et al., 2023 | Rev Inst Med Trop Sao Paulo | Thailand | Cross-sectional | Medium complexity | Healthcare professionals | 102 |
| 574 | Tuberculosis at a university hospital, Thailand: A surprising incidence of TB among a new generation of highly exposed health care workers who may be asymptomatic | Mingchay et al., 2022 | Plos One | Thailand | Cross-sectional | High complexity | Healthcare professionals | 195 |
| 6298 | Mycobacterium tuberculosis infection and disease in healthcare workers in a tertiary referral hospital in Bandung, Indonesia. | Apriani et al., 2022 | J Infect Prev | Thailand | Cross-sectional | High complexity | Doctor, nurses, nutritionists, pharmacists, midwives, and dentists | 445 |
| 2491 | Decreased annual risk of TB infection in South Korean healthcare workers using interferon-gamma release assay between 1986 - 2005 | Lee et al., 2021 | BMC Infectious Diseases | South Korea | Cross-sectional retrospective | High complexity | Doctors, nursing staff, pharmacists, physiotherapists, administrative staff, and cleaners | 3.233 |
| 1372 | Comparison of Latent Tuberculosis Infections among General versus Tuberculosis Health Care Workers in Myanmar | Phyu, et al., 2020 | Tropical Medicine and Infectious Disease | Asia | Cross-sectional | Medium complexity | Nursing staff, doctors, pharmacists, administrative staff | 500 |
| 1376 | Serial testing of health care workers for TB infection: A prospective cohort study | Casas, et al., 2020 | Plos One | Spain | Cross-sectional | High complexity | Nursing staff, doctors, pharmacists, administrative staff | 255 |
| 1417 | The Prevalence and Demographic Risk Factors for Latent TB Infection Among Healthcare Workers in Semarang, Indonesia | Erawat; Andriany, 2020 | J Multidiscip Healthc | Indonesia | Cross-sectional | Primary care | Nursing staff, doctors, pharmacists, administrative staff, and cleaners | 195 |
| 6145 | Latent tuberculosis infection among health-care workers using Quantiferon-TB Gold-Plus in a country with a low burden for TB: prevalence and risk factors | Almohaya et al., 2020 | ASM Annals of Saudi Medicine | Saudi Arabia | Cross-sectional and case control | High complexity | Doctors, nurses, laboratory technicians, and radiology technicians | 3.024 |
| 1455 | Screening for Latent TB among Healthcare Workers in an Egyptian Hospital Using Tuberculin Skin Test and QuantiFERON-TB Gold In-Tube Test | Anwar et al., 2019 | Indian Journal of Occupational & Environmental Medicine | Egypt | Cross-sectional | High complexity | Nursing staff, doctors, pharmacists, administrative staff, and cleaners | 153 |
| 1490 | Screening of latent TB infection among health care workers working in Hajj pilgrimage area in Saudi Arabia, using interferon gamma release assay and tuberculin skin test | Zakeya et al., 2018 | ASM Annals of Saudi Medicine Saudita | Saudi Arabia | Cross-sectional prospective | High complexity | Nursing staff and doctors | 520 |
| 1448 | Screening of health-care workers for latent tuberculosis infection in a Tertiary Care Hospital | Janagond al., 2017 | International Journal of Mycobacteriology | India | Prospective | High complexity | Nursing staff, doctors, pharmacists, administrative staff, and cleaners | 2.290 |
| 5839 | The Direct Comparison of Two Interferon-gamma Release Assays in the TB Screening of Japanese Healthcare Workers | Tanabe al., 2017 | Internal Medicine | Japan | Cross-sectional | High complexity | Doctors, nursing staff, pharmacists, physiotherapists, administrative staff, and cleaners | 654 |
| 3784 | Age is associated with latent tuberculosis in nurses | Chaiear et al., 2016 | Asian Pacific Journal of Tropical Disease | Thailand | Comparative study | High complexity | Nurses and nursing assistants | 213 |
| 5481 | QuantiFERON-TB Gold In-Tube Testing for Tuberculosis in Healthcare Professionals | Weddle et al., 2014 | Oxford Academic | United States | Cohort | High complexity | Doctors, nursing staff, pharmacists, physiotherapists, administrative staff and cleaners | 758 |
| 6436 | Latent TB infection screening in healthcare workers in four large hospitals in Santiago, Chile | Hernández et al., 2014 | Revista Chilena de Infectologia | Chile | Cross-sectional | High complexity | Doctors, nurses, physiotherapists, technologists, technical, and administrative assistants | 76 |
| 2234 | Incidence of tuberculosis infection among healthcare workers: risk factors and 20-year evolution | Casas et al., 2013 | Medicina Respiratória | Spain | Prospective cohort | High complexity | Doctors, nursing staff, pharmacists, physiotherapists, administrative staff. and cleaners | 614 |
| 4075 | Prevalence of latent TB infection among healthcare workers in China as detected by two interferon-gamma release assays | Wei et al., 2013 | Journal of Hospital Infection | China | Cross-sectional | High complexity | Doctors, nursing staff, pharmacists, physiotherapists, administrative staff and cleaners | 210 |
| 2020 | Screening for tuberculosis and prediction of disease in Portuguese healthcare workers. | Costa et al., 2011 | Journal of occupational Medicine and Toxicology | Portugal | Cohort | Medium complexity | Nursing staff, doctors, pharmacists, administrative staff, and cleaners | 2.889 |
| 4225 | The prevalence of latent tuberculosis infections among health-care workers - A three-country comparison | Nienhaus et al., 2011 | Pneumologie | Germany | Cohort | High complexity | Doctors, nursing staff, pharmacists, physiotherapists, administrative staff, and cleaners | 2.028 |
| 6329 | Within-Subject Variability of Mycobacterium tuberculosis-Specific Gamma Interferon Responses in German Health Care Workers | Ringshausen et al 2011 | CVI Clinical and Vaccine Immunology | Germany | Cross-sectional | High complexity | Doctors, nursing staff, pharmacists, physiotherapists, administrative staff, and cleaners | 35 |
| 4271 | Interferon-γ release assay for TB screening of healthcare workers at a Korean tertiary hospital | Park et al., 2010 | Scandinavian Journal of Infectious Diseases | South Korea | Clinical trial | High complexity | Doctors and nurses | 322 |
| 4336 | Estimation of incidence of tuberculosis infection in health-care workers using repeated interferon-γ assays | Yoshiyama et al., 2009 | Epidemiology E Infection | Japan | Cross-sectional | High complexity | Doctors, nursing staff, pharmacists, physiotherapists, administrative staff, and cleaners | 425 |
| 5829 | TB screening in Portuguese healthcare workers using the tuberculin skin test and the interferon-gamma release assay | Costa et al., 2009 | European Respiratory Journal | Portugal | Cross-sectional | High complexity | Doctors, nursing staff, pharmacists, physiotherapists, administrative staff, and cleaners | 4.735 |
| 4478 | Rates of latent tuberculosis in health care staff in Russia | Drobniewski et al., 2007 | Plos Medicine | Russia | Cross-sectional | Primary care and High complexity | Doctors, nursing staff, pharmacists, physiotherapists, administrative staff, cleaners, nursing, and medical students | 630 |
| 1572 | Is the risk of occupational tuberculosis higher for young health care workers? | Raitio et al., 2003 | The International Journal of Tuberculosis and Lung Disease | Finland | Cross-sectional | High complexity | Equipe de Enfermagem, Médicos e funcionários administrativos. | 447 |
| 4572 | Tuberculosis among healthcare workers in a tertiary-care hospital in South India | Gopinatha et al., 2003 | The Journal of Hospital Infection | India | Cohort | High complexity | Doctors, Nursing Staff, Pharmacists, Physiotherapists, Administrative Staff | 125 |
| 5503 | TB in female nurses in british-columbia - implications for control programs | Burrill et al., 1985 | Canadian Medical Association Journal | Canada | Cross-sectional | Medium complexity | Nurses | 57 |
Table 3.
Distribution of the main results of the articles analyzed. Rio Grande do Sul, Brazil, 2024.
Table 3.
Distribution of the main results of the articles analyzed. Rio Grande do Sul, Brazil, 2024.
| ID | Factors associated with tuberculosis |
|---|---|
| 1372 | The risk factors for ILTB included: education level below higher education, 10 or more years of service, insufficient knowledge about regular TB screening, and teaching cough etiquette to TB patients. |
| 1376 | The factors associated with a positive TT or IGRA test were: BCG vaccination status and the degree of occupational exposure to tuberculosis. |
| 1417 | Healthcare workers with current diseases (DM and hepatitis) were more susceptible to LTBI (OR = 3.39, 95% CI: 0.99–11.62, p = 0.04), and midwives were at higher risk of LTBI than other healthcare professions. |
| 1448 | The factors were high exposure to TB patients in the absence of TB control measures. Furthermore, the analysis suggested that age, years of service, literacy, and working in wards/ICU were associated with TB infection. |
| 1455 | Among the participants with a positive test, all had more than 10 years of professional experience, a history of BCG vaccination, were diabetic, and were active smokers. |
| 1490 | The average age and duration of employment were significantly higher in the positive participants. |
| 1572 | Among nurses, nursing assistants, and doctors, the incidence rate was higher in the 20-39 age group. |
| 2020 | Age (50 years or older) and the number of years working in healthcare services increase the likelihood of positive TST and IGRA results (higher OR of 2.5 for working 20 years or more in healthcare). Repeated BCG vaccination was associated with a reduced likelihood of a positive IGRA. |
| 2234 | The cumulative incidence was higher among healthcare workers working in high-risk areas during the periods from 1990 to 1995. The majority were women, with an average age of 31 years. |
| 2491 | The multivariate analysis indicated that advanced age, healed TB lesions on chest X-ray, and male sex were risk factors for positive IGRA, while working in high-risk TB departments was not. |
| 3784 | Advanced age, male sex, longer duration of employment, having BCG scars, family history of TB, TB in the past year, prevention by any methods, and the use of surgical masks. |
| 4075 | Age >30 years and working in a chest hospital for more than five years were significantly associated with a positive QFT-GIT result and TB. Furthermore, in the multivariate analysis, age >30 years and working as a nurse were associated with a positive QFT-GIT result and TB. |
| 4225 | Age over 55 years, family history of TB, migration from a country with high TB incidence, prolonged contact (>40 hours) with a sputum-positive index case (OR = 18.6). |
| 4271 | History of BCG vaccination was significant for TB. |
| 4336 | Staff working in TB isolation wards were more likely to have a positive QFT-G response (OR 8.6, 95% CI 1.4–54). |
| 4478 | The proportion of people diagnosed with ILTB was higher among doctors and nurses in primary care compared to the low-exposure medical student group, and among doctors and nurses compared to primary healthcare workers or medical students. |
| 4572 | They occurred in individuals under 32 years of age, with a higher incidence among nurses (25.6%) and nursing students (19.2%). |
| 5481 | The risk factors associated with TB were living in a country where TB is endemic and receiving the BCG vaccination. |
| 5503 | Female sex and caregiving occupations, as well as those whose tuberculin test results were negative but who were not vaccinated, had twice the likelihood of contracting TB. |
| 5829 | The likelihood of a positive IGRA increased with the diameter of the TT induration, age, and years spent as a healthcare professional. A positive IGRA was less likely when ≤ 10 years had passed since the last vaccination. |
| 5839 | Having a previous chest X-ray and/or IGRA abnormalities, a history of TB treatment, comorbidities associated with immunodeficiency, and a history of TB exposure. |
| 6145 | Higher risk of ILTB was present in healthcare professionals over 50 years of age, working as nurses and radiology technicians, and working in the emergency department or intensive care unit. |
| 6329 | Age was significantly associated with IGRAs (P < 0.05). |
| 6436 | A higher proportion of latent TB infection was found in older age. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



