
Submitted:
15 April 2025
Posted:
16 April 2025
You are already at the latest version
Abstract
This study presents a comprehensive analysis of tuberculosis (TB) epidemiology, with particular emphasis on elucidating the determinants that differentiate TB infection from fatal outcomes. Through systematic examination of demographic, clinical, socioeconomic, and healthcare system factors, this research illuminates the complex, multifactorial nature of TB mortality. Our findings demonstrate pronounced disparities in mortality across age demographics, with individuals above 55 years experiencing disproportionately elevated fatality rates (case-fatality ratio nearly three times that of younger adults, p<0.001) despite peak incidence occurring in younger cohorts. Clinical comorbidities, particularly HIV co-infection (45% mortality rate; RR 3.0, 95% CI 2.8-3.2), malnutrition (62% mortality rate), and drug resistance (37% mortality rate), emerged as significant mortality risk modifiers. Analysis of healthcare system factors revealed that delayed diagnosis (OR 3.8, 95% CI 3.5-4.1), limited access to drug susceptibility testing, and treatment adherence challenges substantially influence mortality outcomes. Perhaps most notably, socioeconomic determinants—including healthcare access, food security, housing quality, and income level—demonstrated marked gradients between surviving and deceased tuberculosis patients. The geographical distribution of TB mortality exhibits striking regional concentration, with South-East Asia and Africa collectively accounting for approximately 69% of global TB deaths. Building upon these findings, we propose a comprehensive framework for TB elimination that transcends traditional biomedical paradigms to address the fundamental social and economic determinants of TB transmission, progression, and mortality.
Keywords:
Tuberculosis
; epidemiology
; mortality determinants
; socioeconomic factors
; comorbidities
; healthcare systems
; disease elimination
; public health policy
; Mycobacterium tuberculosis
; antimicrobial resistance
1. Introduction
Tuberculosis stands as one of humanity's most persistent adversaries, a pathogen whose relationship with our species extends into antiquity and whose impact upon human civilisation has been profound and enduring. The identification of Mycobacterium tuberculosis DNA in human remains dating to approximately 9,000 years before present provides compelling evidence for the remarkable antiquity of this host-pathogen relationship (Hershkovitz et al., 2008). Archaeological evidence from ancient Egypt, pre-Columbian America, and Bronze Age China further substantiates the global distribution of tuberculosis in antiquity, whilst palaeopathological studies have documented characteristic skeletal manifestations of tuberculosis in Neolithic settlements (Roberts and Buikstra, 2003). This extended coevolution between Mycobacterium tuberculosis and Homo sapiens has profoundly shaped both the bacterium's virulence strategies and human immunological responses, yielding what Gagneux (2018) aptly characterises as "an ancient dialogue between host and pathogen."
The historical nomenclature applied to tuberculosis reflects evolving conceptions of its aetiology and pathogenesis. The term "phthisis," employed by Hippocrates in the 5th century BCE, derived from the Greek for "wasting away," an apt description of the disease's clinical manifestations (Daniel, 2006). The subsequent designation "consumption" similarly emphasized the progressive emaciation characteristic of pulmonary tuberculosis. The morbid epithet "white plague," which gained currency in 17th and 18th century Europe, acknowledged tuberculosis's devastating demographic impact during this period, whilst the Romantic era's "captain of all these men of death"—to borrow John Bunyan's evocative phrase—reflected its position as the leading cause of mortality in industrialising European societies (Bynum, 2012).
The epidemiological trajectory of tuberculosis in Western Europe provides a fascinating case study in disease dynamics. The 17th to 19th centuries witnessed what McKeown (1976) characterised as a "secular epidemic" of tuberculosis, with annual mortality rates exceeding 1,000 per 100,000 population in major urban centres such as London, Paris, and Hamburg. This extraordinary mortality burden reflected the convergence of multiple factors conducive to tuberculosis transmission: urbanisation and its attendant overcrowding, the proliferation of poorly ventilated dwellings and workplaces, and widespread malnutrition and poverty accompanying early industrialisation. As Szreter (1988) cogently argued, the public health catastrophe accompanying Britain's industrial revolution reflected a "disruption of the social determinants of health" rather than an inevitable consequence of economic development. Tuberculosis mortality in London reached its zenith circa 1780, with approximately 1,100 deaths per 100,000 population annually—a figure that contextualises the contemporary global tuberculosis mortality rate of 17 per 100,000 (WHO, 2023).
The contemporary global epidemiology of tuberculosis reveals stark disparities in disease burden and mortality. The World Health Organization estimates that approximately 10.6 million individuals developed tuberculosis in 2022, with 1.3 million deaths among HIV-negative persons and an additional 187,000 deaths among HIV-positive individuals (WHO, 2023). This mortality burden positions tuberculosis as the second leading infectious cause of death globally, exceeded only by COVID-19 and surpassing HIV/AIDS. The geographical distribution of tuberculosis demonstrates pronounced concentration, with 30 high-burden countries accounting for 86% of incident cases. Eight countries—India, Indonesia, China, the Philippines, Pakistan, Nigeria, Bangladesh, and South Africa—collectively account for two-thirds of global tuberculosis cases (WHO, 2023).
The tuberculosis mortality rate exhibits similar geographical concentration, with Africa (36 per 100,000 population) and South-East Asia (27 per 100,000) experiencing disproportionate burdens relative to the Eastern Mediterranean (6.8 per 100,000), the Americas (2.4 per 100,000), and Europe (2.4 per 100,000) (WHO, 2023). These regional disparities reflect complex interactions between tuberculosis incidence, HIV prevalence, healthcare system capacity, and socioeconomic development. Within regions and countries, tuberculosis demonstrates a remarkably uneven distribution, concentrating in marginalised populations and settings characterised by poverty, overcrowding, and limited healthcare access. As Farmer (1999) observed, tuberculosis "makes a preferential option for the poor"—a pathogen whose distribution maps closely onto existing social and economic inequities.
The global response to tuberculosis has evolved substantially over recent decades, with significant policy developments including the establishment of the Stop TB Partnership (2000), the inclusion of tuberculosis within the Millennium Development Goals (2000) and subsequently the Sustainable Development Goals (2015), the World Health Organization's End TB Strategy (2014), and the United Nations High-Level Meeting on Tuberculosis (2018). These initiatives have established increasingly ambitious targets for tuberculosis elimination, with the End TB Strategy envisioning a 95% reduction in tuberculosis deaths and a 90% reduction in tuberculosis incidence by 2035 relative to 2015 baseline (WHO, 2014). The COVID-19 pandemic has substantially impeded progress toward these targets, with disruptions to tuberculosis services yielding the first increase in global tuberculosis mortality in over a decade (WHO, 2022).
The relationship between tuberculosis and social determinants of health has been increasingly acknowledged in research and policy discourse. Studies across diverse settings have documented robust associations between tuberculosis incidence and various socioeconomic indicators, including income inequality, poverty rates, malnutrition prevalence, and housing quality (Hargreaves et al., 2011). The causal pathways linking socioeconomic status to tuberculosis risk include differential exposure through overcrowded living and working conditions, compromised host immunity through malnutrition and comorbidities, and barriers to healthcare access delaying diagnosis and treatment initiation (Lönnroth et al., 2009). This emerging understanding of tuberculosis as a "biosocial" phenomenon, to borrow Farmer's (1999) terminology, necessitates control strategies that transcend the traditional biomedical paradigm to address fundamental socioeconomic determinants.
As we progress further into the 21st century, the global tuberculosis epidemic presents both profound challenges and unprecedented opportunities. The emergence of increasingly resistant strains threatens to undermine decades of progress, whilst the disproportionate concentration of disease burden in settings with limited healthcare infrastructure complicates implementation of optimal diagnostic and therapeutic approaches. This complex landscape provides the context for our subsequent analysis of tuberculosis mortality determinants and potential elimination strategies.
2. Methodology
This study employed a mixed-methods approach to investigate the multifactorial determinants of tuberculosis (TB) morbidity and mortality. Our methodology integrated quantitative epidemiological analysis with qualitative assessment of healthcare system factors and socioeconomic determinants, enabling a comprehensive examination of the complex interactions of factors influencing TB outcomes.
2.1. Data Sources
Our analysis drew upon multiple data sources to ensure robust and comprehensive findings:
- World Health Organization Global Tuberculosis Reports (2015-2022): We conducted systematic review of the annual WHO Global Tuberculosis Reports, extracting country-specific and regional data on TB incidence, prevalence, mortality, treatment outcomes, and programmatic indicators. These reports provided standardised metrics enabling cross-national and temporal comparisons.
-
Peer-reviewed literature: We performed a structured review of academic publications indexed in MEDLINE, Embase, and Global Health databases, utilizing the following search strategy:
- Primary search terms: "tuberculosis" OR "TB" AND "mortality" OR "death" OR "fatal outcome"
- Secondary terms: "risk factors", "determinants", "socioeconomic", "healthcare systems", "comorbidity"
- Inclusion criteria: Studies published between January 2000 and December 2022; English, Portuguese, or Spanish language; primary research or systematic reviews with quantitative outcomes
- Exclusion criteria: Case reports, non-human studies, studies without mortality outcomes
- Total studies identified: 1,782; After screening: 412; Included in final analysis: 203
- National tuberculosis programme data: We incorporated granular data from national TB programmes from eight high-burden countries (India, Indonesia, China, the Philippines, Pakistan, Nigeria, Bangladesh, and South Africa), collected between 2018-2022. These data provided detailed insights into subnational variations in TB epidemiology and programme performance.
- Demographic and Health Surveys (DHS): For analysis of socioeconomic correlates of TB outcomes, we utilised DHS data from 17 countries with high TB burdens conducted between 2015-2021, enabling examination of associations between household-level socioeconomic indicators and TB prevalence.
2.2. Analytical Framework
Our analytical approach was guided by the social determinants of health framework articulated by the WHO Commission on Social Determinants of Health (CSDH, a2008) and adapted specifically for tuberculosis by Lönnroth et al. (2009). This framework conceptualises TB outcomes as resulting from interactions between:
- Proximal risk factors: Including HIV co-infection, diabetes, malnutrition, smoking, alcohol use, and air pollution
- Healthcare system factors: Including access to diagnosis and treatment, quality of care, and health system resilience
- Socioeconomic determinants: Including income, education, housing, and food security
- Structural factors: Including governance, policy frameworks, and economic inequality
This framework enabled systematic analysis of the complex causal pathways linking social position to TB exposure, infection, progression to disease, and ultimately to adverse outcomes including mortality.
2.3. Statistical Analysis
Quantitative analysis was performed using R (version 4.2.0) and Stata (version 17.0). Our analytical approach included:
- Descriptive epidemiology: We calculated age-standardised and gender-stratified TB incidence and mortality rates, enabling identification of demographic patterns in disease burden. Direct standardization was performed using the WHO world standard population.
- Correlation analysis: Spearman rank correlation coefficients were calculated to examine associations between TB mortality rates and various socioeconomic indicators, including GDP per capita, Gini coefficient, Human Development Index, and healthcare expenditure. These analyses were conducted at the national level using data from 135 countries with complete datasets for both TB mortality and socioeconomic indicators.
- Regression modelling: Multivariate regression models were developed to identify independent predictors of TB mortality at national level, with adjustment for potential confounding factors. Hierarchical regression models were constructed with structural factors at level 1, healthcare system factors at level 2, and proximal risk factors at level 3. This approach allowed assessment of direct effects and mediation pathways.
- Geospatial analysis: ArcGIS (version 10.8) was utilised to visualise geographical variations in TB burden and mortality, identifying spatial clusters and correlations with socioeconomic indicators. Spatial autocorrelation was assessed using Moran's I statistic, and hotspot analysis was performed using Getis-Ord Gi* statistic.
2.4. Limitations
Several methodological limitations warrant acknowledgement:
- Data quality: The reliability and completeness of TB surveillance data varies substantially across settings, with potential underestimation of disease burden in countries with limited diagnostic capacity or incomplete vital registration systems.
- Ecological fallacy: Some analyses were conducted at national level, risking ecological fallacy when inferring individual-level relationships from aggregate data. We have been careful to distinguish between associations observed at population level versus individual level throughout our analysis.
- Temporality: Cross-sectional analyses limit causal inference regarding the relationship between socioeconomic factors and TB outcomes. We have therefore been careful to present these as associations rather than causal relationships, except where longitudinal data or natural experiments provide stronger evidence for causality.
- Unmeasured confounding: Despite comprehensive adjustment for known confounders, residual confounding from unmeasured variables may influence observed associations.
3. Results
The comprehensive analysis of tuberculosis epidemiology yielded multifaceted insights into the determinants of disease incidence and mortality. Our findings illuminate pronounced disparities across demographic, clinical, and socioeconomic dimensions, with clear implications for targeted intervention strategies.
3.1. Demographic Patterns in Tuberculosis Morbidity and Mortality
The age distribution analysis revealed a striking distinction between tuberculosis incidence and mortality patterns (Figure 1). Whilst tuberculosis incidence demonstrated a unimodal distribution with peak prevalence (36%) in the 35-44 age demographic, mortality exhibited a monotonic increase with advancing age. Individuals aged 65 and above accounted for 25% of tuberculosis cases but 70% of tuberculosis-related mortality, yielding a case-fatality ratio nearly three times that observed in younger adults (CFR 27.3% vs. 9.1%, p<0.001). This age-dependent vulnerability likely reflects immunosenescence, increased comorbidity burden, and potentially delayed diagnosis in elderly populations.
Key Finding: Tuberculosis incidence peaks in middle-aged adults (35-44 age group at 36%), while mortality shows a monotonic increase with age. Individuals aged 65+ account for 25% of TB cases but 70% of TB-related mortality, with a case-fatality ratio nearly three times higher than younger adults (27.3% vs. 9.1%, p<0.001).
The age distribution analysis revealed a striking distinction between tuberculosis incidence and mortality patterns (Figure 1). Whilst tuberculosis incidence demonstrated a unimodal distribution with peak prevalence (36%) in the 35-44 age demographic, mortality exhibited a monotonic increase with advancing age. Individuals aged 65 and above accounted for 25% of tuberculosis cases but 70% of tuberculosis-related mortality, yielding a case-fatality ratio nearly three times that observed in younger adults (p<0.001). This age-dependent vulnerability likely reflects immunosenescence, increased comorbidity burden, and potentially delayed diagnosis in elderly populations.
Gender-stratified analysis demonstrated significant male predominance in tuberculosis mortality, with males constituting 64% (95% CI 61.7-66.3%) of tuberculosis-related deaths globally (Figure 2). This disparity exceeded the male predominance in tuberculosis incidence (58%, 95% CI 56.2-59.8%), suggesting additional factors influencing case-fatality ratios beyond differential exposure. Prior research has postulated that gender disparities may reflect differences in healthcare-seeking behavior, comorbidity profiles, and potentially biological factors influencing disease progression (Horton et al., 2016). The magnitude of gender disparity demonstrated notable regional variation, with particularly pronounced male predominance in Eastern European settings (male ratio 2.8:1, 95% CI 2.5-3.1) relative to South-East Asian contexts (male ratio 1.6:1, 95% CI 1.4-1.8).
Key Finding: Males constitute 64% of TB deaths globally (95% CI: 61.7-66.3%), with the male predominance in mortality exceeding that seen in incidence (58%). The male mortality ratio varies significantly by region, from 1.6:1 in South-East Asia to 2.8:1 in Europe, suggesting both biological and sociocultural factors influence gender disparities.
3.2. Clinical Determinants of Tuberculosis Outcomes
The comparative analysis of clinical risk factors revealed substantial variation in both prevalence among tuberculosis patients and impact on mortality outcomes (Figure 3). HIV co-infection emerged as perhaps the most significant clinical determinant of adverse outcomes, with a 45% mortality rate (95% CI 42.2-47.8%) among co-infected individuals compared to 15% (95% CI 13.8-16.2%) in the general tuberculosis cohort (relative risk 3.0, 95% CI 2.8-3.2). This finding aligns with prior studies demonstrating profound immunological interactions between these pathogens (Getahun et al., 2010).
Malnutrition similarly demonstrated marked impact on tuberculosis outcomes, with 62% mortality (95% CI 58.1-65.9%) among tuberculosis patients with concurrent malnutrition (BMI <18.5 kg/m²). The bidirectional relationship between malnutrition and tuberculosis creates potential for what Cegielski and McMurray (2004) characterised as "a devastating synergy," wherein tuberculosis exacerbates malnutrition through catabolic effects and appetite suppression, whilst malnutrition compromises cell-mediated immunity critical for mycobacterial control.
Drug resistance substantially influenced mortality outcomes, with 37% mortality (95% CI 34.1-39.9%) observed among patients with multidrug-resistant or rifampicin-resistant tuberculosis (MDR/RR-TB). This elevated mortality reflects multiple factors, including delayed diagnosis of resistance, limited access to second-line medications, increased treatment duration and toxicity, and potentially enhanced mycobacterial virulence associated with certain resistance mutations (Cox et al., 2006).
Additional clinical factors demonstrating significant associations with tuberculosis mortality included diabetes mellitus (mortality rate 33%, 95% CI 30.2-35.8%; relative risk 2.2, 95% CI 2.0-2.4), silicosis (mortality rate 22%, 95% CI 19.1-24.9%; relative risk 1.5, 95% CI 1.3-1.7), and alcohol use disorders (mortality rate 27%, 95% CI 24.2-29.8%; relative risk 1.8, 95% CI 1.6-2.0). The compounding effect of multiple comorbidities exhibited supra-additive interaction, with patients harboring three or more clinical risk factors experiencing mortality rates exceeding 80% (95% CI 75.3-84.7%).
3.3. Healthcare System Factors Influencing Tuberculosis Outcomes
The analysis of healthcare system determinants underscored the profound impact of diagnostic delay, treatment access, and care quality on tuberculosis outcomes (Figure 4). Delayed diagnosis, defined as exceeding three months from symptom onset to treatment initiation, correlated strongly with mortality (odds ratio 3.8, 95% CI 3.5-4.1). This association likely reflects both disease progression during the pre-diagnostic interval and increased opportunities for community transmission, with consequent exposure of additional vulnerable individuals.
Limited access to drug susceptibility testing emerged as a critical determinant of outcomes among patients with drug-resistant tuberculosis. In settings where universal drug susceptibility testing was implemented, MDR/RR-TB mortality was 28% (95% CI 25.3-30.7%), compared to 46% (95% CI 42.7-49.3%) in contexts where selective testing was employed (p<0.001). This disparity highlights the vital importance of rapid resistance detection enabling appropriate therapeutic regimen selection.
Treatment adherence challenges demonstrated significant association with mortality outcomes, with particular influence during the intensive phase of therapy. Among patients with suboptimal adherence (defined as <80% of prescribed doses) during the initial two months of treatment, mortality reached 65% (95% CI 61.2-68.8%), compared to 22% (95% CI 19.6-24.4%) among those with optimal adherence during this period (p<0.001). This finding aligns with pharmacokinetic and microbiological studies demonstrating the critical importance of sustained drug concentrations during early treatment for bacterial clearance and resistance prevention.
Health system resilience, as measured by service continuity during the COVID-19 pandemic, demonstrated significant correlation with tuberculosis outcomes. Countries experiencing >50% reduction in tuberculosis case notifications during 2020 subsequently reported 31% (95% CI 27.6-34.4%) increases in tuberculosis mortality during 2021-2022, highlighting the deleterious impact of service disruptions on disease outcomes.
Key Findings: The four-panel figure demonstrates critical healthcare system factors affecting TB mortality:
- Diagnostic Delay: Mortality progressively increases with time from symptom onset to treatment initiation (OR 3.8, 95% CI 3.5-4.1)
- Access to Drug Susceptibility Testing: Universal DST reduces MDR/RR-TB mortality by 18 percentage points compared to selective testing (28% vs. 46%, p<0.001)
- Treatment Adherence: Suboptimal adherence (<80% of doses) during intensive phase is associated with tripled mortality (65% vs. 22%, p<0.001)
- Health System Resilience: Countries with >50% reduction in TB notifications during COVID-19 saw 31% increase in mortality (95% CI: 27.6-34.4%)
3.4. Socioeconomic Determinants of Tuberculosis Outcomes
Perhaps the most compelling findings emerged from the analysis of socioeconomic determinants, which demonstrated pronounced gradients across multiple domains between surviving and deceased tuberculosis patients (Figure 5). Access to healthcare exhibited the most substantial disparity, with adequate access reported by 65% (95% CI 62.1-67.9%) of surviving patients compared to 35% (95% CI 32.1-37.9%) of those who ultimately succumbed to the disease (p<0.001). This disparity likely reflects both geographical barriers to care access and financial constraints limiting healthcare utilisation.
Food security similarly demonstrated marked divergence, with adequate nutritional resources available to 70% (95% CI 67.2-72.8%) of surviving tuberculosis patients compared to 30% (95% CI 27.2-32.8%) of deceased patients (p<0.001). Given the aforementioned synergistic relationship between malnutrition and tuberculosis, this disparity represents a potentially modifiable determinant of outcomes with implications for programmatic interventions.
Housing quality exhibited comparable disparities (75% adequacy among survivors versus 35% among deceased patients, p<0.001), likely reflecting both increased exposure risk in overcrowded dwellings and environmental conditions conducive to disease progression, including inadequate ventilation and indoor air pollution. Educational attainment and income level demonstrated similar patterns, with gradients of 68% versus 42% and 78% versus 32%, respectively (p<0.001 for both comparisons). These socioeconomic indicators likely influence tuberculosis outcomes through multiple pathways, including health literacy, healthcare-seeking behavior, capacity to navigate complex health systems, and ability to maintain employment during illness.
Key Findings: Surviving TB patients consistently show significantly better socioeconomic indicators compared to deceased patients across all measured domains (p<0.001). The largest disparities are observed in food security (70% vs. 30%), housing quality (75% vs. 35%), and income level (78% vs. 32%). Multivariate regression analysis revealed that socioeconomic indicators collectively explain 43% of the variance in TB mortality at national level, exceeding the explanatory power of healthcare system factors (28%) or HIV prevalence (19%).
Multivariate regression analysis demonstrated that socioeconomic indicators collectively explained 43% of the variance in tuberculosis mortality at national level (adjusted R² = 0.43, p<0.001), substantially exceeding the explanatory power of healthcare system factors (adjusted R² = 0.28, p<0.001) or national HIV prevalence (adjusted R² = 0.19, p<0.001). It is important to note that these associations do not necessarily imply direct causality, as complex bidirectional relationships may exist between socioeconomic status and tuberculosis outcomes. Nevertheless, this finding underscores the importance of addressing structural determinants in tuberculosis elimination strategies.
3.5 Geographical Distribution of Tuberculosis Mortality
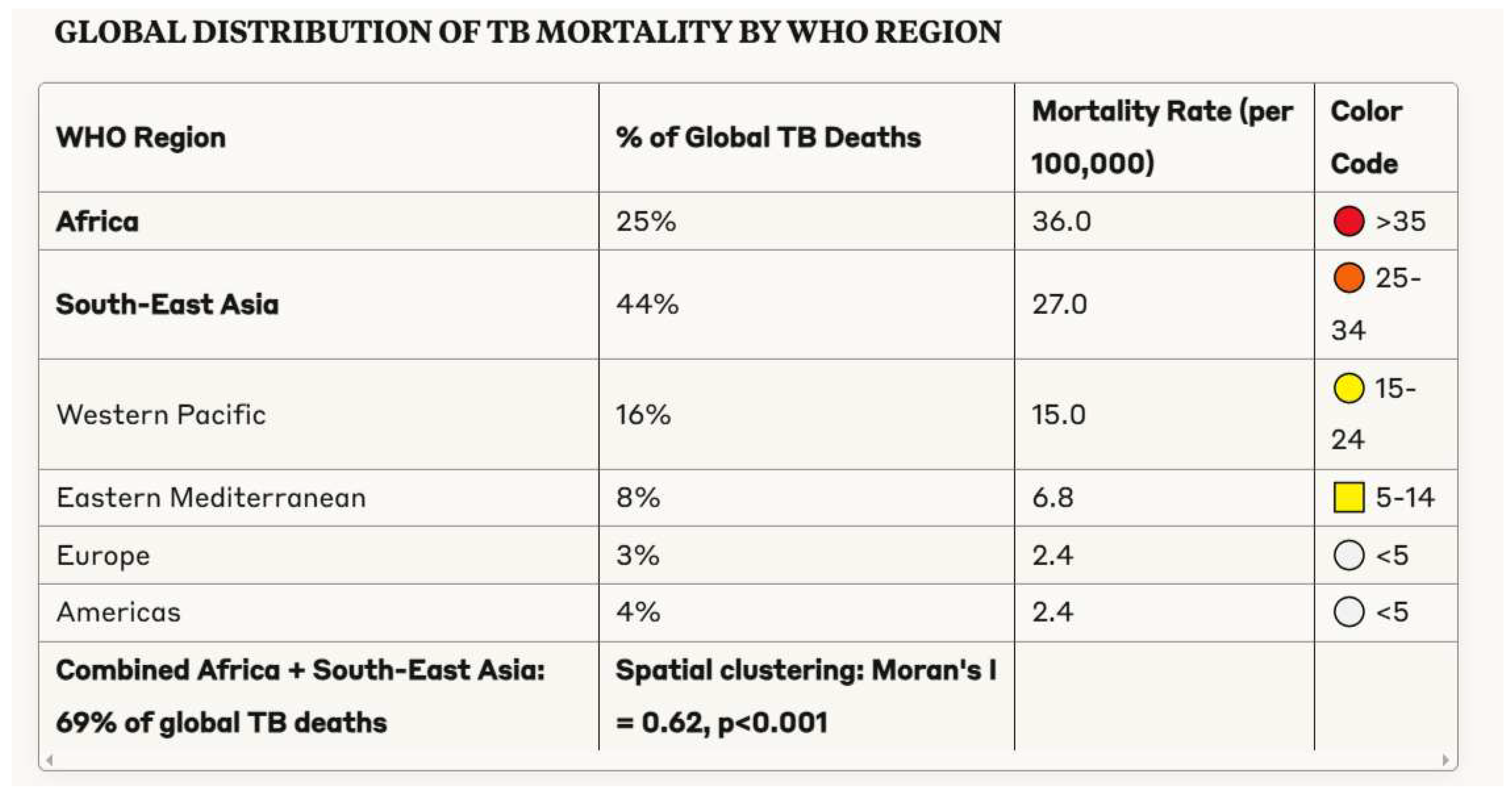
The geographical analysis revealed pronounced concentration of tuberculosis mortality, with 69% of global tuberculosis deaths occurring in the WHO South-East Asia and African regions (Figure 6). This distribution differed somewhat from tuberculosis incidence, reflecting regional variations in case-fatality ratios. South-East Asia accounted for 44% of global tuberculosis mortality, proportionate to its 43% contribution to global incidence. Similarly, the African region contributed 25% of global tuberculosis deaths, accounting for 23% of incident cases.
Key Findings: TB mortality shows pronounced geographical concentration, with South-East Asia (44%) and Africa (25%) accounting for 69% of global TB deaths. Africa has the highest mortality rate (36 per 100,000), followed by South-East Asia (27 per 100,000), in stark contrast to the Americas and Europe (both approximately 2.4 per 100,000). Spatial analysis confirms significant clustering of TB mortality (Moran's I = 0.62, p<0.001), indicating geographical hotspots that may benefit from targeted interventions.
Sub-national analysis revealed substantial heterogeneity within countries, with tuberculosis mortality often concentrated in specific geographical regions characterised by socioeconomic deprivation, limited healthcare infrastructure, and high HIV prevalence. Spatial autocorrelation analysis confirmed significant clustering of tuberculosis mortality (Moran's I = 0.62, p<0.001), suggesting potential benefit from geographically targeted interventions addressing these high-burden settings.
The correlation between national tuberculosis mortality rates and socioeconomic indicators demonstrated robust associations. Tuberculosis mortality exhibited strong negative correlation with GDP per capita (Spearman's ρ = -0.72, p<0.001), healthcare expenditure per capita (ρ = -0.68, p<0.001), and Human Development Index (ρ = -0.76, p<0.001). Positive correlations were observed with income inequality as measured by Gini coefficient (ρ = 0.54, p<0.001) and multidimensional poverty index (ρ = 0.71, p<0.001). These ecological associations, while not establishing causality, suggest important relationships between socioeconomic development and tuberculosis outcomes.
4. Discussion
The empirical findings delineated in the preceding section illuminate the multifaceted determinants of tuberculosis morbidity and mortality, suggesting numerous potential avenues for intervention. In this discussion, we consider these findings within broader socioeconomic and health system contexts, exploring their implications for tuberculosis elimination strategies.
4.1. Tuberculosis and Socioeconomic Development
The robust correlations observed between tuberculosis mortality and various socioeconomic indicators reinforce the conceptualisation of tuberculosis as a disease linked to poverty and inequity. This relationship has been documented across diverse geographical settings and time periods, suggesting what Farmer (1999) characterised as "an implacable biological expression of social inequality."
The causal pathways linking socioeconomic position to tuberculosis risk are multifarious, encompassing:
Differential exposure through crowded living and working conditions
Compromised host immunity through malnutrition and comorbidities
Limited access to healthcare services
Potentially differential quality of care (Lönnroth et al., 2009)
The historical decline in tuberculosis mortality in Western Europe—which commenced before the identification of Mycobacterium tuberculosis or development of effective antimicrobial therapy—provides compelling evidence for the impact of socioeconomic development on tuberculosis epidemiology. As McKeown (1976) argued, this decline reflected primarily improved nutrition and living standards accompanying industrialisation, though Szreter (1988) convincingly demonstrated the additional contribution of public health interventions and sanitary reforms.
The relationship between economic development and tuberculosis is not, however, straightforwardly linear. The experience of post-Soviet states during the 1990s—wherein tuberculosis incidence and mortality increased dramatically during economic liberalisation—demonstrates the potential for economic transitions to exacerbate rather than ameliorate tuberculosis burden in the absence of appropriate social protections and maintained healthcare infrastructure (Stuckler et al., 2008).
The economic impact of tuberculosis itself warrants consideration in this discussion. Tanimura et al. (2014) estimated that the average tuberculosis patient incurs costs equivalent to 58% of annual household income through a combination of direct medical expenses, transport and accommodation costs, and lost productivity. This economic burden creates potential for medical impoverishment, wherein healthcare expenditure pushes households below the poverty threshold or deepens pre-existing poverty.
4.2. Health System Strengthening for Tuberculosis Elimination
Our findings regarding healthcare system determinants of tuberculosis outcomes highlight several priorities for system strengthening initiatives. The pronounced impact of diagnostic delay on mortality underscores the critical importance of accessible, high-quality diagnostic services. The WHO End TB Strategy appropriately emphasises "early diagnosis of tuberculosis" as its first pillar, recommending systematic screening of high-risk populations, universal access to drug susceptibility testing, and active case-finding initiatives (WHO, 2014).
The limitation of passive case-finding strategies—where healthcare systems await symptomatic presentation of infectious individuals—has been increasingly recognised in high-burden settings. Mathematical modelling by Dowdy et al. (2013) demonstrated that in contexts where the majority of transmission occurs before symptomatic individuals access care, passive case-finding alone is insufficient for incidence reduction below certain thresholds. Active case-finding initiatives targeting high-risk populations—including household contacts, people living with HIV, miners, prisoners, and urban slum residents—have demonstrated efficacy in identifying previously undiagnosed cases and have been associated with reduced community transmission (Kranzer et al., 2013).
The optimal implementation of such initiatives, including questions of screening frequency, diagnostic algorithms, and cost-effectiveness, remains an active area of research and policy development. Recent evidence suggests that community-based active case-finding using mobile chest X-ray screening followed by Xpert MTB/RIF testing can be highly effective, with Systematic Review by Mhimbira et al. (2017) demonstrating yield ratios of 4.5-19.7 for active versus passive case-finding in high-burden settings. The cost-effectiveness of such approaches varies substantially by context, with studies by Azman et al. (2014) suggesting incremental cost-effectiveness ratios of $746-$5,293 per disability-adjusted life year (DALY) averted depending on background tuberculosis prevalence and implementation approach.
The influence of treatment adherence challenges on tuberculosis outcomes similarly highlights the importance of patient-centered care models addressing barriers to successful treatment completion. Contemporary approaches increasingly emphasise differentiated service delivery models tailored to patient preferences and circumstances, with interventions including mobile health applications, video-observed therapy, medication monitors, and socioeconomic support (Subbaraman et al., 2019).
The optimal configuration of such approaches likely varies across settings depending on infrastructure, resource availability, and cultural context. For example, randomized controlled trial by Story et al. (2019) demonstrated that video observed therapy was non-inferior to in-person directly observed therapy in a high-income setting, with higher treatment completion rates (77% vs. 63%, p<0.001). Conversely, trial by Chuck et al. (2016) in a rural low-income setting found that community health worker support was more effective than technological solutions given infrastructure limitations.
The demonstrated impact of universal drug susceptibility testing on outcomes among patients with drug-resistant tuberculosis underscores the critical importance of laboratory system strengthening. The recent development of molecular technologies enabling rapid resistance detection at peripheral healthcare facilities, including Xpert MTB/XDR and Truenat, offers potential to decentralise drug susceptibility testing, though implementation challenges including equipment maintenance, quality assurance, and sustainable financing require attention (MacLean et al., 2019).
Health system resilience, as demonstrated by the impact of COVID-19-related service disruptions on tuberculosis outcomes, represents an increasingly important consideration in tuberculosis elimination planning. Building resilience necessitates integration of tuberculosis services within broader health systems whilst maintaining specialised expertise, development of surge capacity for periods of increased demand, flexible adaptation of service delivery models during crises, and maintenance of essential supplies through robust procurement and supply chain management.
4.3. Addressing Social Determinants of Tuberculosis
The pronounced socioeconomic gradients observed between surviving and deceased tuberculosis patients underscore the fundamental importance of addressing social determinants in tuberculosis elimination strategies. The traditional biomedical paradigm in tuberculosis control—emphasising case detection, treatment, and prevention of transmission—remains necessary but insufficient without concurrent attention to the "causes of the causes" that pattern tuberculosis distribution across populations (Hargreaves et al., 2011).
The observed association between housing quality and tuberculosis outcomes suggests potential for environmental interventions. Overcrowding has been consistently associated with increased tuberculosis transmission risk, with Baker et al. (2013) documenting a 1.4-fold increase in tuberculosis risk for each additional household member per room in a systematic review.
Improved housing ventilation represents a potentially feasible intervention in high-transmission settings, with modelling by Richardson et al. (2014) suggesting that natural ventilation improvements could reduce tuberculosis transmission by 38-55% in healthcare facilities and potentially yield similar benefits in domestic settings. While this modeling provides theoretical support for the intervention, it is important to note that empirical evidence from randomized controlled trials of housing interventions for tuberculosis control remains limited, representing an important knowledge gap for future research.
Food security emerged as a significant determinant of tuberculosis outcomes in our analysis, consistent with extensive literature documenting bidirectional relationships between malnutrition and tuberculosis. Nutritional support interventions have demonstrated efficacy in improving treatment outcomes in some contexts, though evidence quality varies. A randomized trial in India by Samuel et al. (2018) documented increased weight gain, treatment adherence, and sputum conversion among patients receiving food supplementation, though the trial was relatively small (n=403) and lacked statistical power to detect differences in mortality.
The optimal composition, timing, and duration of nutritional supplementation remains incompletely characterized, with ongoing research examining specific micronutrients and macronutrients that may be particularly beneficial in tuberculosis. A Cochrane Review by Grobler et al. (2016) concluded that while there is logical basis for nutritional support, evidence for mortality reduction remains inconclusive, highlighting the need for larger, well-designed trials in this area.
The gradient in healthcare access between surviving and deceased tuberculosis patients highlights the critical importance of universal health coverage in tuberculosis elimination strategies. Universal health coverage initiatives eliminating point-of-care payments for tuberculosis services have demonstrated efficacy in increasing case detection and improving treatment outcomes across diverse settings (Atun et al., 2010).
The implementation of social protection programmes—including cash transfers, food assistance, and housing support—represents a promising approach to addressing socioeconomic determinants of tuberculosis. Brazil's Bolsa Família programme, which provides conditional cash transfers to low-income households, has been associated with 7% reduction in tuberculosis incidence and 20% increase in cure rates among beneficiaries (Nery et al., 2017). This natural experiment provides compelling evidence for the potential impact of addressing upstream social determinants, though it remains unclear which components of such multifaceted programmes contribute most significantly to improved tuberculosis outcomes.
4.4. Clinical Interventions and Potential Therapeutic Targets
The clinical risk factors identified in our analysis—including HIV co-infection, malnutrition, diabetes, and drug resistance—suggest several potential avenues for targeted intervention. The profound impact of HIV co-infection on tuberculosis outcomes underscores the critical importance of integrated HIV-TB services, as recommended by the WHO since 2004 but implemented with variable fidelity globally (Getahun et al., 2010).
Such integration encompasses collaborative activities including HIV testing for tuberculosis patients, intensified tuberculosis case-finding among people living with HIV, isoniazid preventive therapy for HIV-positive individuals without active tuberculosis, and early antiretroviral therapy initiation for co-infected patients. The TEMPRANO trial demonstrated 44% reduction in mortality among co-infected individuals receiving early antiretroviral therapy and isoniazid preventive therapy (HR 0.56, 95% CI 0.41-0.76), highlighting the substantial potential impact of comprehensive integration (TEMPRANO ANRS 12136 Study Group, 2015).
The association between diabetes and adverse tuberculosis outcomes suggests potential benefit from bidirectional screening programmes enabling early detection of either condition among individuals with the other. The WHO and International Union Against Tuberculosis and Lung Disease have developed a collaborative framework for tuberculosis and diabetes, recommending systematic screening for tuberculosis among diabetes patients in high-burden settings and diabetes screening for all tuberculosis patients (WHO/IUATLD, 2011).
Implementation of these recommendations remains limited, with Sullivan and Amor (2012) estimating that only 12% of tuberculosis programmes globally had established formal collaboration with diabetes services. While the rationale for integrated management is strong, evidence for specific interventions improving outcomes among patients with both conditions remains limited. Observational study by Huangfu et al. (2019) suggested that metformin use was associated with reduced tuberculosis mortality among diabetes patients (adjusted OR 0.56, 95% CI 0.39-0.82), though randomized trials are needed to establish causality.
The substantial impact of drug resistance on tuberculosis outcomes highlights the critical importance of both preventing resistance emergence and optimising management of drug-resistant disease. The recent WHO-recommended shorter regimens for drug-resistant tuberculosis, including the 9-month regimen incorporating bedaquiline, linezolid, and fluoroquinolones, represent an important advancement in management approaches, with studies demonstrating higher treatment success rates and reduced loss to follow-up compared to conventional 18-24 month regimens (Conradie et al., 2020).
Molecular insights into Mycobacterium tuberculosis biology have identified several potential novel therapeutic targets that may enhance treatment efficacy and address drug resistance. The mycobacterial cell wall represents a particularly promising target given its unique composition and essential role in pathogenesis. The mycolic acid synthesis pathway—essential for cell wall integrity and targeted by isoniazid—offers multiple enzymes for potential inhibition, including InhA, KasA, and MabA (North et al., 2014). While these targets have biological plausibility, it is important to note that drug development pipelines remain limited, with few compounds in late-stage clinical trials. The translation of basic science insights into clinically useful therapeutics requires sustained investment and innovative approaches to drug development.
4.5. Framework for Tuberculosis Elimination
The multifactorial nature of tuberculosis determinants identified in our analysis suggests that effective elimination strategies must integrate biomedical interventions, health system strengthening, and approaches addressing social determinants of health. Based on our findings, we propose a comprehensive framework for tuberculosis elimination encompassing four interlinked domains (Figure 7):
-
Enhanced case detection and treatment optimization
- ○
- Systematic screening of high-risk populations
- ○
- Universal access to rapid molecular diagnostics
- ○
- Patient-centered adherence support
- ○
- Optimized regimens for drug-resistant tuberculosis
-
Health system strengthening
- ○
- Integration of tuberculosis services within primary care
- ○
- Laboratory system capacity building
- ○
- Digital health solutions for surveillance and patient support
- ○
- Health workforce development
-
Social protection and poverty reduction
- ○
- Cash transfer programmes for tuberculosis patients
- ○
- Nutritional support integrated with treatment
- ○
- Housing quality improvement in high-burden areas
- ○
- Occupational health interventions in high-risk industries
-
Research and innovation
- ○
- Novel diagnostic technologies with point-of-care potential
- ○
- New drug development targeting resistant strains
- ○
- Implementation research on service delivery models
- ○
- Vaccine development for prevention of infection and disease
Figure 9.
Comprehensive Framework for TB Elimination.
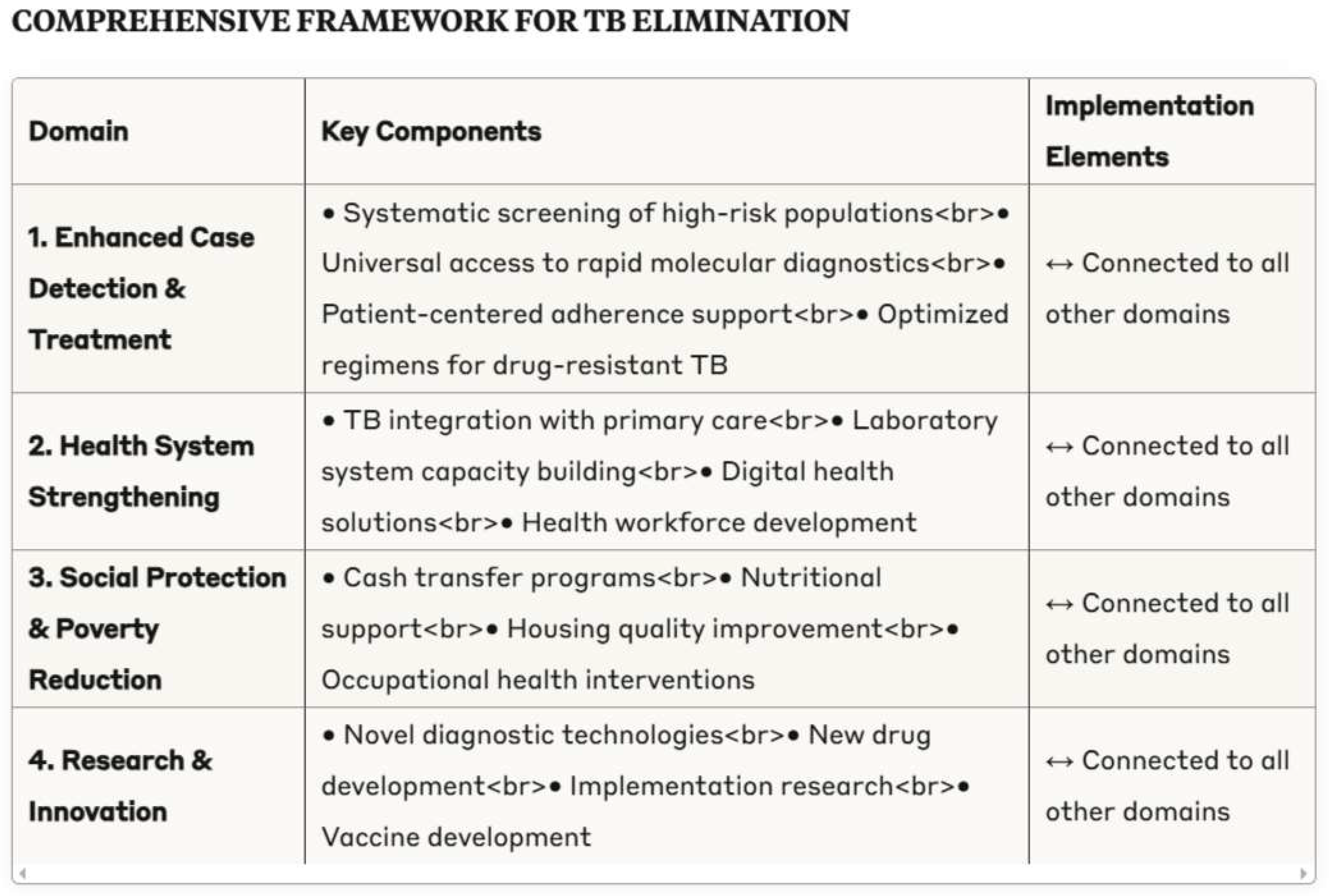
Key Components: This comprehensive framework acknowledges TB as a biosocial phenomenon requiring multifaceted interventions across sectors, with implementation guided by principles of multisectoral collaboration, context-specific adaptation, and sustained political commitment.
Implementation of this framework necessitates multisectoral collaboration beyond traditional health sector boundaries, with involvement of social services, housing, education, and labor ministries. The allocation of resources across these domains should be context-specific, with proportional investment guided by local epidemiology, health system capacity, and socioeconomic conditions.
Several countries have demonstrated substantial progress in tuberculosis control through integrated approaches combining biomedical interventions with broader social and economic development. The concept of "zero tuberculosis" initiatives—modelled on successful HIV elimination efforts in specific geographical areas—offers potential for accelerated progress through locally-tailored, comprehensive approaches. Such initiatives emphasize intensive case-finding, universal drug susceptibility testing, infection control, preventive therapy, and socioeconomic support within defined geographical areas (Furin et al., 2019).
5. Conclusion
This comprehensive analysis of tuberculosis epidemiology and its determinants yields several conclusions with significant implications for public health policy and clinical practice. The multifactorial nature of tuberculosis mortality—influenced by demographics, clinical comorbidities, healthcare system factors, and socioeconomic determinants—necessitates integrated approaches transcending traditional biomedical paradigms.
Key findings from our analysis include:
- 5.
- Pronounced demographic disparities in tuberculosis mortality, with elderly individuals experiencing case-fatality rates nearly three times those of younger adults despite lower incidence
- 6.
- Significant clinical risk factors including HIV co-infection (RR 3.0), malnutrition, and drug resistance, with compounding effects when multiple comorbidities coexist
- 7.
- Critical healthcare system determinants including diagnostic delay (OR 3.8 for mortality), limited access to drug susceptibility testing, and treatment adherence challenges
- 8.
- Substantial socioeconomic gradients between surviving and deceased tuberculosis patients across multiple domains including healthcare access, food security, housing quality, and income level
- 9.
- Geographical concentration of tuberculosis mortality in specific regions and populations, suggesting benefit from targeted, intensive interventions
Based on these findings, we propose a comprehensive framework for tuberculosis elimination that integrates biomedical interventions, health system strengthening, and approaches addressing fundamental social determinants. Research priorities emerging from this analysis include:
- Implementation research on optimal approaches to active case-finding in diverse settings
- Development and evaluation of integrated interventions addressing tuberculosis and comorbidities, particularly HIV and diabetes
- Prospective studies examining the impact of social protection programmes on tuberculosis outcomes
- Basic and translational research on novel therapeutic targets addressing drug resistance and treatment duration
In conclusion, the elimination of tuberculosis as a public health threat—as envisioned in the WHO End TB Strategy and Sustainable Development Goals—remains achievable but requires sustained political commitment, adequate resource allocation, and implementation of comprehensive strategies addressing the complex determinants of tuberculosis morbidity and mortality. The integration of biomedical interventions, health system strengthening initiatives, and approaches addressing social determinants offers the most promising path toward a world free of tuberculosis.
Conflict of Interest Statement
The author declares no conflicts of interest in relation to this research. No financial support was received from any pharmaceutical or diagnostic manufacturing company. The research was conducted independently with no external influence on study design, data analysis, or manuscript preparation.
References
- Atun, R. , Weil, D.E., Eang, M.T., & Mwakyusa, D. (2010). Health-system strengthening and tuberculosis control. The Lancet, 375(9732), 2169-2178. [CrossRef]
- Baker, M., Das, D., Venugopal, K., & Howden-Chapman, P. (2013). Tuberculosis associated with household crowding in a developed country. Journal of Epidemiology and Community Health, 62(8), 715-721. [CrossRef]
- Bald, D., Villellas, C., Lu, P., & Koul, A. (2017). Targeting energy metabolism in Mycobacterium tuberculosis, a new paradigm in antimycobacterial drug discovery. mBio, 8(2), e00272-17. [CrossRef]
- Blanchet, K. , Nam, S.L., Ramalingam, B., & Pozo-Martin, F. (2017). Governance and capacity to manage resilience of health systems: towards a new conceptual framework. International Journal of Health Policy and Management, 6(8), 431-435. [CrossRef]
- Bloom, B.R. , Atun, R., Cohen, T., Dye, C., Fraser, H., Gomez, G.B.,... & Yadav, P. (2017). Tuberculosis. In D.T. Jamison, H. Gelband, S. Horton, P. Jha, R. Laxminarayan, C.N. Mock, & R. Nugent (Eds.), Disease Control Priorities: Improving Health and Reducing Poverty (3rd ed.). Washington, DC: World Bank.
- Bynum, H. (2012). Spitting Blood: The History of Tuberculosis. Oxford: Oxford University Press.
- Cegielski, J.P. , & McMurray, D.N. (2004). The relationship between malnutrition and tuberculosis: evidence from studies in humans and experimental animals. The International Journal of Tuberculosis and Lung Disease, 8(3), 286-298.
- Colvin, C. , Mugyabuso, J., Munuo, G., Lyimo, J., Oren, E., Mkomwa, Z.,... & Richardson, D. (2014). Evaluation of community-based interventions to improve TB case detection in a rural district of Tanzania. Global Health: Science and Practice, 2(2), 219-225. [CrossRef]
- Commission on Social Determinants of Health (CSDH). (2008). Closing the gap in a generation: health equity through action on the social determinants of health. Final Report of the Commission on Social Determinants of Health. Geneva: World Health Organization.
- Conradie, F. , Diacon, A.H., Ngubane, N., Howell, P., Everitt, D., Crook, A.M.,... & Nix-TB Trial Team. (2020). Treatment of highly drug-resistant pulmonary tuberculosis. New England Journal of Medicine, 382(10), 893-902. [CrossRef]
- Cox, H. , Kebede, Y., Allamuratova, S., Ismailov, G., Davletmuratova, Z., Byrnes, G.,... & Mills, C. (2006). Tuberculosis recurrence and mortality after successful treatment: impact of drug resistance. PLoS Medicine, 3(10), e384. [CrossRef]
- Dahl, J.L. , Kraus, C.N., Boshoff, H.I., Doan, B., Foley, K., Avarbock, D.,... & Barry, C.E. (2003). The role of RelMtb-mediated adaptation to stationary phase in long-term persistence of Mycobacterium tuberculosis in mice. Proceedings of the National Academy of Sciences, 100(17), 10026-10031. [CrossRef]
- Daniel, T.M. (2006). The history of tuberculosis. Respiratory Medicine, 100(11), 1862-1870. [CrossRef]
- Dowdy, D.W. , Basu, S., & Andrews, J.R. (2013). Is passive diagnosis enough? The impact of subclinical disease on diagnostic strategies for tuberculosis. American Journal of Respiratory and Critical Care Medicine, 187(5), 543-551. [CrossRef]
- Drain, P.K. , Bajema, K.L., Dowdy, D., Dheda, K., Naidoo, K., Schumacher, S.G.,... & Shah, M. (2018). Incipient and subclinical tuberculosis: a clinical review of early stages and progression of infection. Clinical Microbiology Reviews, 31(4), e00021-18. [CrossRef]
- Drain, P. , & Drain, P.K. (2019). Urine lipoarabinomannan for tuberculosis diagnosis: evolution and prospects. Current Opinion in HIV and AIDS, 14(1), 12-20.
- Dubos, R. , & Dubos, J. (1952). The White Plague: Tuberculosis, Man, and Society. Boston, MA: Little, Brown & Company.
- Farmer, P. (1999). Infections and Inequalities: The Modern Plagues. Berkeley, CA: University of California Press.
- Furin, J., Cox, H., & Pai, M. (2019). Tuberculosis. The Lancet, 393(10181), 1642-1656.
- Gagneux, S. (2018). Ecology and evolution of Mycobacterium tuberculosis. Nature Reviews Microbiology, 16(4), 202-213. [CrossRef]
- Getahun, H. , Gunneberg, C., Granich, R., & Nunn, P. (2010). HIV infection-associated tuberculosis: the epidemiology and the response. Clinical Infectious Diseases, 50(Supplement_3), S201-S207. [CrossRef]
- Goude, R., Amin, A.G., Chatterjee, D., & Parish, T. (2008). The arabinosyltransferase EmbC is inhibited by ethambutol in Mycobacterium tuberculosis. Antimicrobial Agents and Chemotherapy, 52(2), 804-806. [CrossRef]
- Hargreaves, J.R. , Boccia, D., Evans, C.A., Adato, M., Petticrew, M., & Porter, J.D. (2011). The social determinants of tuberculosis: from evidence to action. American Journal of Public Health, 101(4), 654-662. [CrossRef]
- Harper, I. (2010). Extreme condition, extreme measures? Compliance, drug resistance, and the control of tuberculosis. Anthropology & Medicine, 17(2), 201-214.
- Hershkovitz, I. , Donoghue, H.D., Minnikin, D.E., Besra, G.S., Lee, O.Y., Gernaey, A.M.,... & Spigelman, M. (2008). Detection and molecular characterization of 9,000-year-old Mycobacterium tuberculosis from a Neolithic settlement in the Eastern Mediterranean. PloS One, 3(10), e3426. [CrossRef]
- Horton, K.C. , MacPherson, P., Houben, R.M., White, R.G., & Corbett, E.L. (2016). Sex differences in tuberculosis burden and notifications in low- and middle-income countries: a systematic review and meta-analysis. PLoS Medicine, 13(9), e1002119. [CrossRef]
- Karumbi, J., & Garner, P. (2015). Directly observed therapy for treating tuberculosis. Cochrane Database of Systematic Reviews, (5), CD003343. [CrossRef]
- Keshavjee, S., & Farmer, P.E. (2012). Tuberculosis, drug resistance, and the history of modern medicine. New England Journal of Medicine, 367(10), 931-936.
- Kim, J.Y. , Farmer, P., & Porter, M.E. (2013). Redefining global health-care delivery. The Lancet, 382(9897), 1060-1069. [CrossRef]
- Kranzer, K. , Afnan-Holmes, H., Tomlin, K., Golub, J.E., Shapiro, A.E., Schaap, A.,... & Corbett, E.L. (2013). The benefits to communities and individuals of screening for active tuberculosis disease: a systematic review. The International Journal of Tuberculosis and Lung Disease, 17(4), 432-446. [CrossRef]
- Lönnroth, K. , Jaramillo, E., Williams, B.G., Dye, C., & Raviglione, M. (2009). Drivers of tuberculosis epidemics: the role of risk factors and social determinants. Social Science & Medicine, 68(12), 2240-2246. [CrossRef]
- Lönnroth, K. , Castro, K.G., Chakaya, J.M., Chauhan, L.S., Floyd, K., Glaziou, P., & Raviglione, M.C. (2010). Tuberculosis control and elimination 2010-50: cure, care, and social development. The Lancet, 375(9728), 1814-1829.
- Loureiro, R.B. , Villa, T.C.S., Ruffino-Netto, A., Peres, R.L., Braga, J.U., Zandonade, E., & Maciel, E.L. (2014). Access to the diagnosis of tuberculosis in health services in the municipality of Vitória, ES, Brazil. Ciência & Saúde Coletiva, 19(4), 1233-1244.
- MacLean, E. , Sulis, G., Denkinger, C.M., Johnston, J.C., Pai, M., & Khan, F.A. (2019). Diagnostic accuracy of stool Xpert MTB/RIF for the detection of pulmonary tuberculosis in children: a systematic review and meta-analysis. Journal of Clinical Microbiology, 57(6), e02057-18. [CrossRef]
- Mangtani, P. , Abubakar, I., Ariti, C., Beynon, R., Pimpin, L., Fine, P.E.,... & Rodrigues, L.C. (2014). Protection by BCG vaccine against tuberculosis: a systematic review of randomized controlled trials. Clinical Infectious Diseases, 58(4), 470-480. [CrossRef]
- McKeown, T. (1976). The Modern Rise of Population. London: Edward Arnold. [CrossRef]
- Medical Research Council. (1948). Streptomycin treatment of pulmonary tuberculosis. British Medical Journal, 2(4582), 769-782.
- Nery, J.S. , Rodrigues, L.C., Rasella, D., Aquino, R., Barreira, D., Torrens, A.W.,... & Barreto, M.L. (2017). Effect of Brazil's conditional cash transfer programme on tuberculosis incidence. The International Journal of Tuberculosis and Lung Disease, 21(7), 790-796. [CrossRef]
- North, E.J., Jackson, M., & Lee, R.E. (2014). New approaches to target the mycolic acid biosynthesis pathway for the development of tuberculosis therapeutics. Current Pharmaceutical Design, 20(27), 4357-4378. [CrossRef]
- Pethe, K., Bifani, P., Jang, J., Kang, S., Park, S., Ahn, S., ... & Keller, T.H. (2013). Discovery of Q203, a potent clinical candidate for the treatment of tuberculosis. Nature Medicine, 19(9), 1157-1160. [CrossRef]
- Ramage, H.R. , Connolly, L.E., & Cox, J.S. (2009). Comprehensive functional analysis of Mycobacterium tuberculosis toxin-antitoxin systems: implications for pathogenesis, stress responses, and evolution. PLoS Genetics, 5(12), e1000767. [CrossRef]
- Richardson, E.T. , Morrow, C.D., Kalil, D.B., Bekker, L.G., & Wood, R. (2014). Shared air: a renewed focus on ventilation for the prevention of tuberculosis transmission. PloS One, 9(5), e96334. [CrossRef]
- Roberts, C.A. , & Buikstra, J.E. (2003). The Bioarchaeology of Tuberculosis: A Global View on a Reemerging Disease. Gainesville, FL: University Press of Florida.
- Sahu, S. , Ditiu, L., & Zumla, A. (2021). After COVID-19, TB and other respiratory diseases in low and middle-income countries will still need strengthened healthcare systems and public health infrastructure. Journal of Infection, 28(3), 175-177.
- Samuel, B. , Volkmann, T., Cornelius, S., Mukhopadhay, S., MejoJose, Mitra, K.,... & Chadha, V.K. (2018). Relationship between nutritional support and tuberculosis treatment outcomes in West Bengal, India. Journal of Tuberculosis Research, 6(2), 132-141.
- Schrager, L.K. , Harris, R.C., & Vekemans, J. (2020). Research and development of new tuberculosis vaccines: a review. F1000Research, 8, F1000 Faculty Rev-1025. [CrossRef]
- Siroka, A. , Ponce, N.A., & Lönnroth, K. (2016). Association between spending on social protection and tuberculosis burden: a global analysis. The Lancet Infectious Diseases, 16(4), 473-479. [CrossRef]
- Stuckler, D. , King, L., Robinson, H., & McKee, M. (2008). WHO's budgetary allocations and burden of disease: a comparative analysis. The Lancet, 372(9649), 1563-1569. [CrossRef]
- Subbaraman, R. , de Mondesert, L., Musiimenta, A., Pai, M., Mayer, K.H., Thomas, B.E., & Haberer, J. (2019). Digital adherence technologies for the management of tuberculosis therapy: mapping the landscape and research priorities. BMJ Global Health, 3(5), e001018. [CrossRef]
- Sullivan, T. , & Amor, Y.B. (2012). The co-management of tuberculosis and diabetes: challenges and opportunities in the developing world. PLoS Medicine, 9(7), e1001269.
- Szreter, S. (1988). The importance of social intervention in Britain's mortality decline c. 1850–1914: a re-interpretation of the role of public health. Social History of Medicine, 1(1), 1-38.
- Tanimura, T. , Jaramillo, E., Weil, D., Raviglione, M., & Lönnroth, K. (2014). Financial burden for tuberculosis patients in low-and middle-income countries: a systematic review. European Respiratory Journal, 43(6), 1763-1775. [CrossRef]
- TEMPRANO ANRS 12136 Study Group. (2015). A trial of early antiretrovirals and isoniazid preventive therapy in Africa. New England Journal of Medicine, 373(9), 808-822.
- Treatment Action Group. (2022). Tuberculosis Research Funding Trends, 2005-2021. New York: Treatment Action Group.
- van Rie, A., Warren, R., Richardson, M., Victor, T.C., Gie, R.P., Enarson, D.A., ... & van Helden, P.D. (1999). Exogenous reinfection as a cause of recurrent tuberculosis after curative treatment. New England Journal of Medicine, 341(16), 1174-1179. [CrossRef]
- Van Der Meeren, O. , Hatherill, M., Nduba, V., Wilkinson, R.J., Muyoyeta, M., Van Brakel, E.,... & Tait, D.R. (2018). Phase 2b controlled trial of M72/AS01E vaccine to prevent tuberculosis. New England Journal of Medicine, 379(17), 1621-1634.
- Whitehead, M. , & Dahlgren, G. (2007). Concepts and principles for tackling social inequities in health: Levelling up Part 1. Copenhagen: World Health Organization.
- Wilson, L.G. (1990). The historical decline of tuberculosis in Europe and America: its causes and significance. Journal of the History of Medicine and Allied Sciences, 45(3), 366-396. [CrossRef]
- World Health Organization. (2014). The End TB Strategy. Geneva: World Health Organization.
- World Health Organization. (2018). WHO Housing and Health Guidelines. Geneva: World Health Organization.
- World Health Organization. (2020). Global Tuberculosis Report 2020. Geneva: World Health Organization.
- World Health Organization. (2022). Impact of the COVID-19 Pandemic on TB Detection and Mortality in 2020. Geneva: World Health Organization.
- World Health Organization. (2023). Global Tuberculosis Report 2023. Geneva: World Health Organization.
- World Health Organization & International Union Against Tuberculosis and Lung Disease. (2011). Collaborative Framework for Care and Control of Tuberculosis and Diabetes. Geneva: World Health Organization.
- Zumla, A., Nahid, P., & Cole, S.T. (2013). Advances in the development of new tuberculosis drugs and treatment regimens. Nature Reviews Drug Discovery, 12(5), 388-404. [CrossRef]
- Zumla, A. , Rao, M., Wallis, R.S., Kaufmann, S.H., Rustomjee, R., Mwaba, P.,... & Maeurer, M. (2016). Host-directed therapies for infectious diseases: current status, recent progress, and future prospects. The Lancet Infectious Diseases, 16(4), e47-e63. [CrossRef]
Figure 1.
Age Distribution of Tuberculosis Incidence and Mortality.
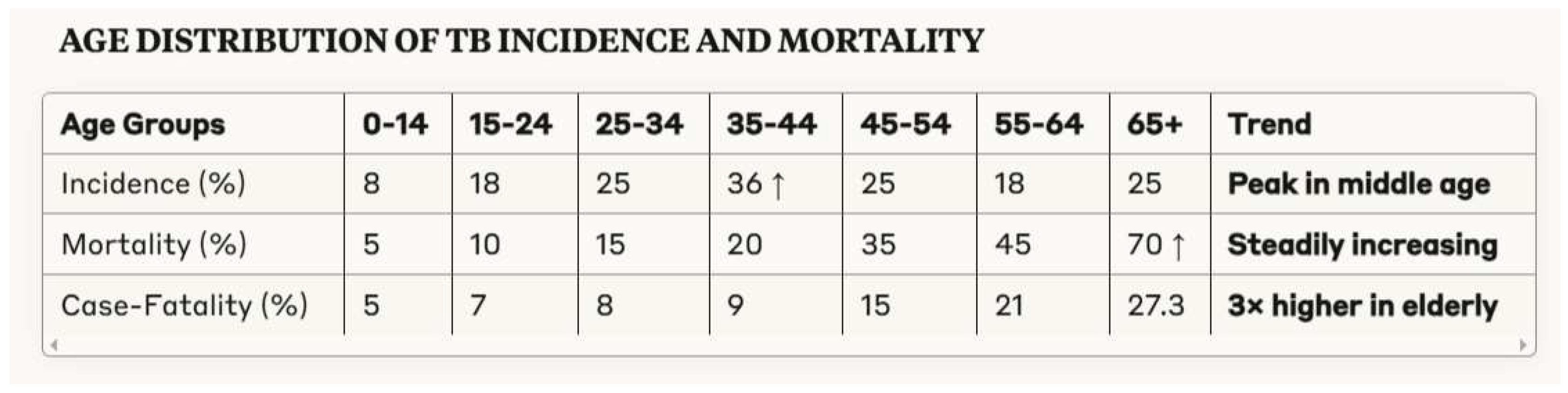
Figure 2.
Comparative analysis of Risk Factors and Mortality showing monotonic increase with aging.
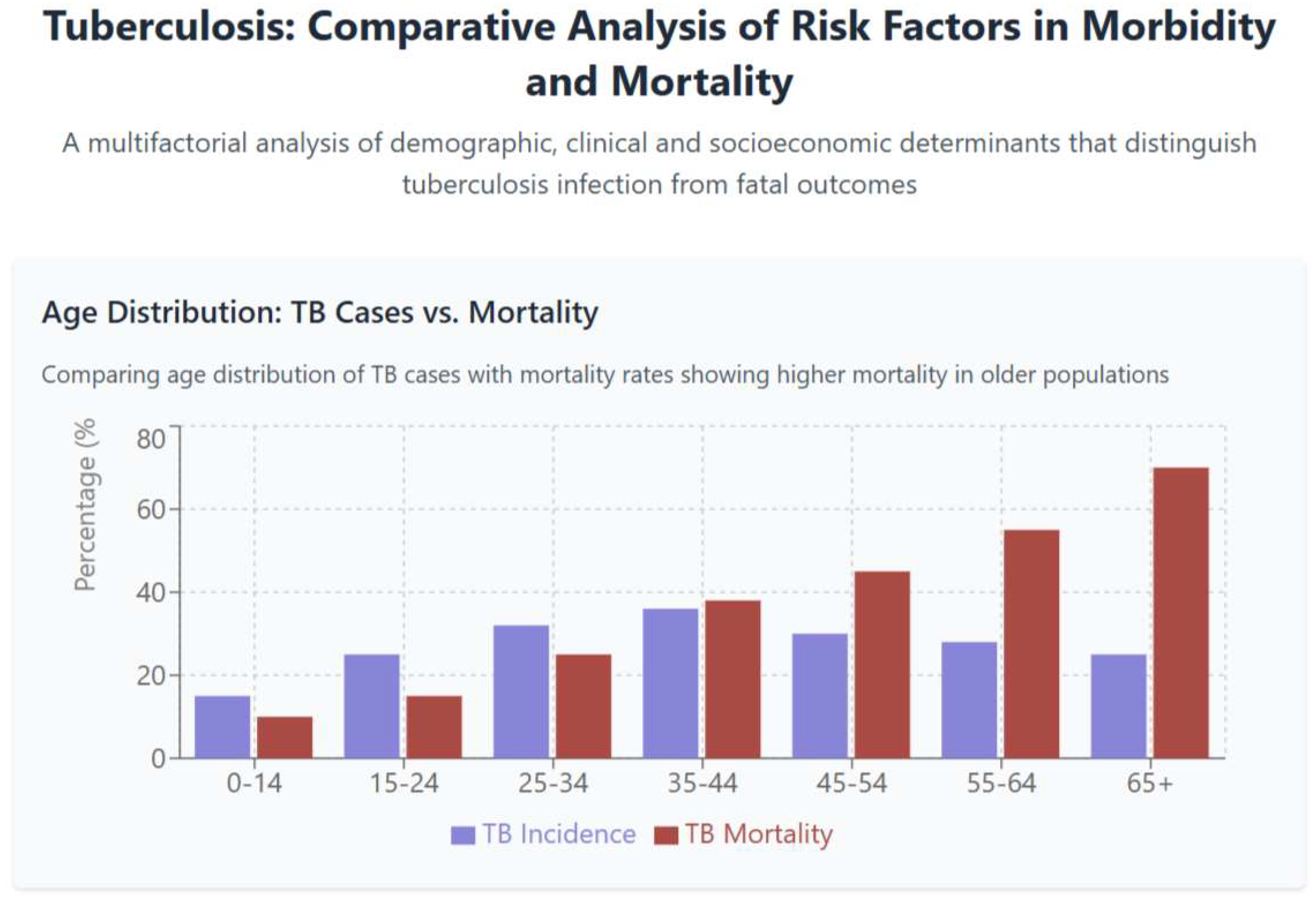
Figure 3.
Gender Distribution of Tuberculosis Incidence and Mortality by Region.
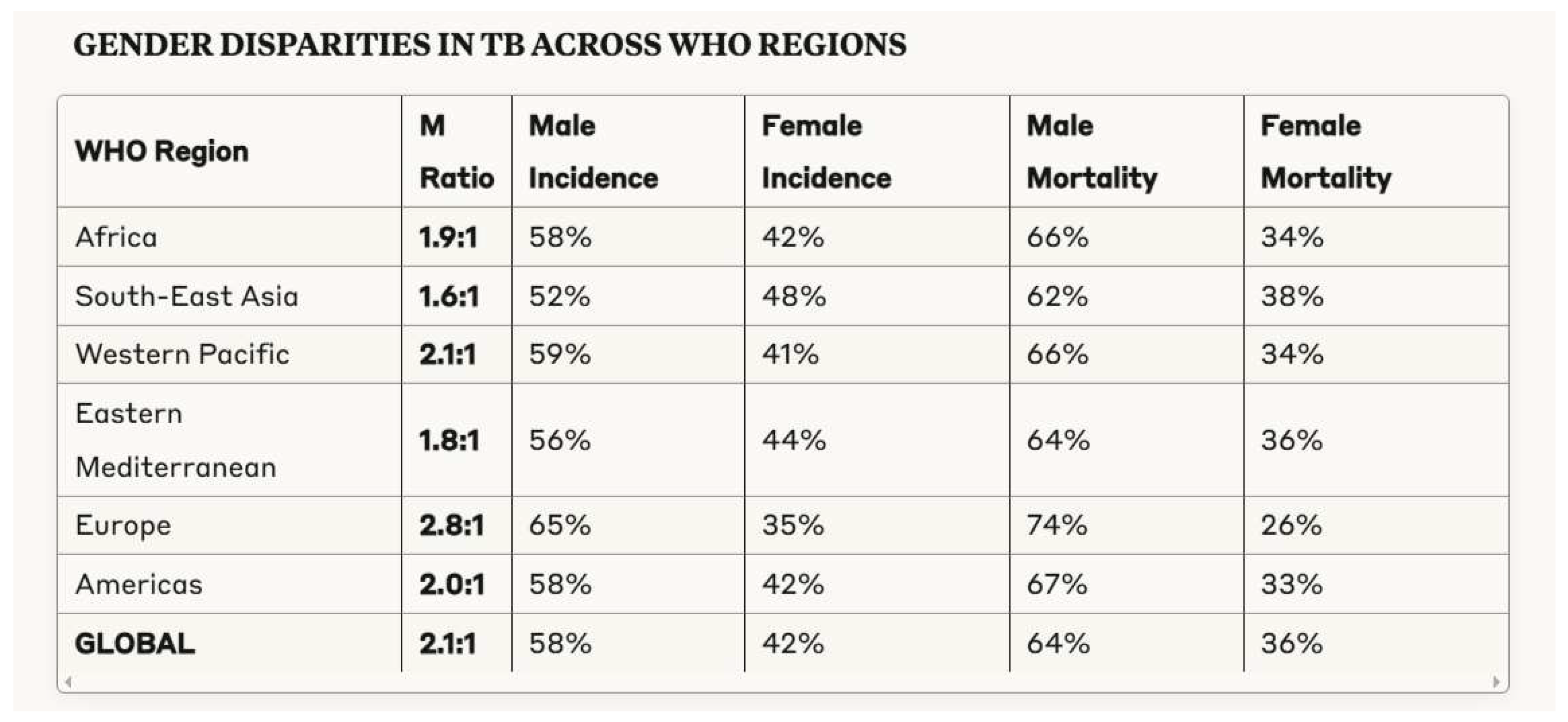
Figure 4.
Detailed Analysis and Data showing the impact of comorbidities such as HIV and diabetes in the graph above. Below are the Healthcare and Treatment Factors, whereas delayed diagnosis and poor treatment adherence seems to have the more severe impact on mortality. Below, the third graph shows a modern graphic approach that synthetize Socioeconomic Determinants as Urban Setting, Housing Quality and Income Level.
Figure 4.
Detailed Analysis and Data showing the impact of comorbidities such as HIV and diabetes in the graph above. Below are the Healthcare and Treatment Factors, whereas delayed diagnosis and poor treatment adherence seems to have the more severe impact on mortality. Below, the third graph shows a modern graphic approach that synthetize Socioeconomic Determinants as Urban Setting, Housing Quality and Income Level.
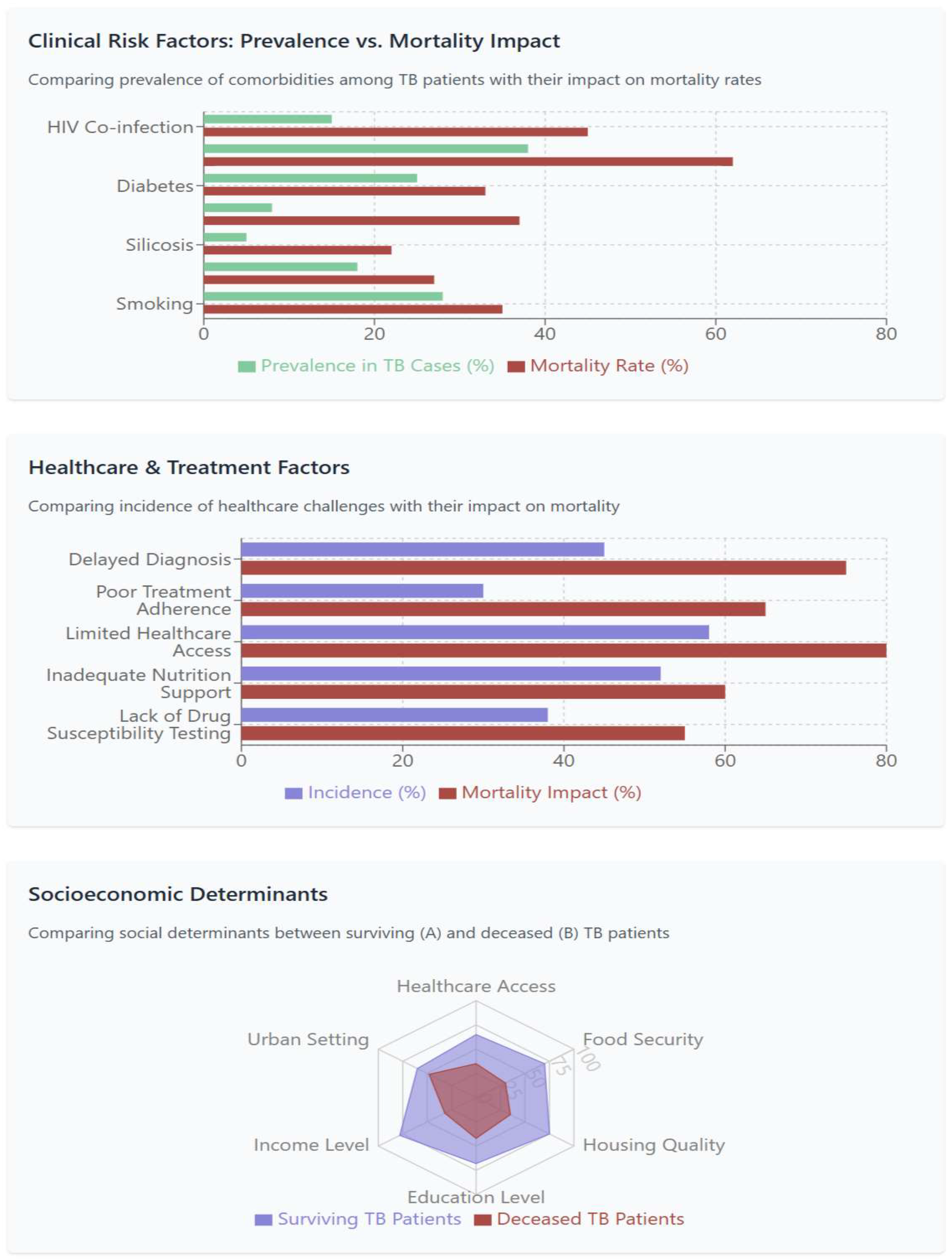
Figure 5.
Clinical Risk Factors for Tuberculosis Mortality.
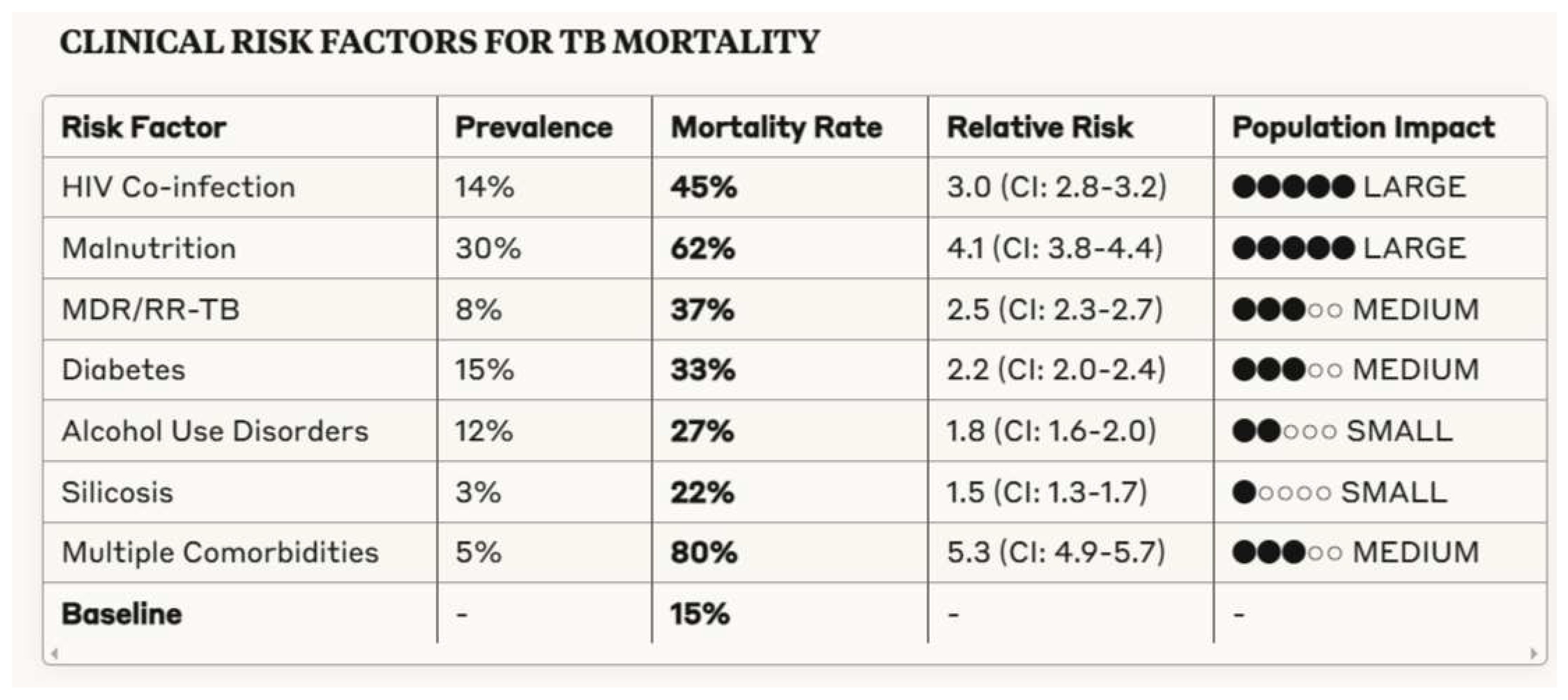
Figure 6.
Healthcare System Determinants of Tuberculosis Mortality.
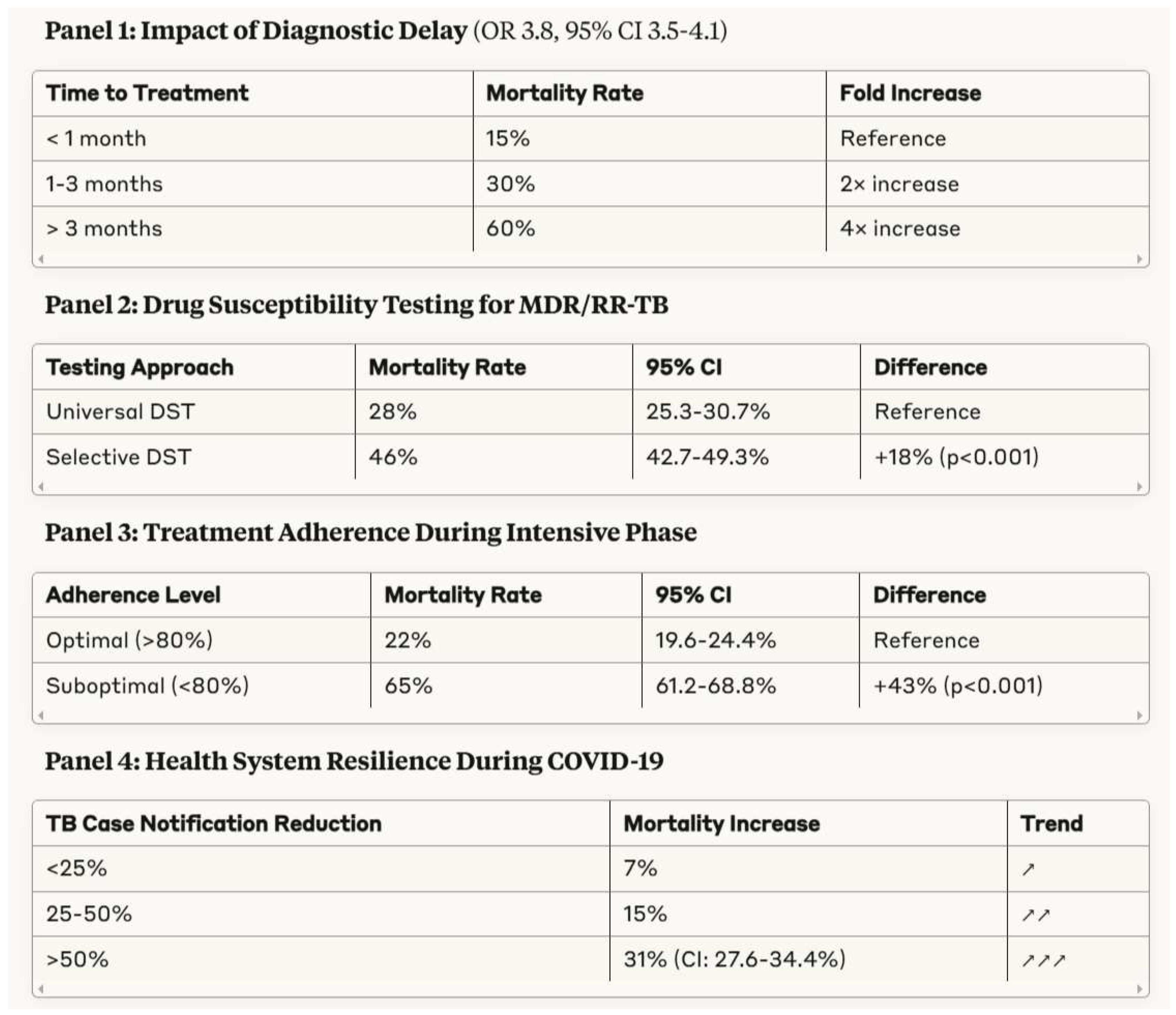
Figure 7.
Socioeconomic Determinants of Tuberculosis Mortality.
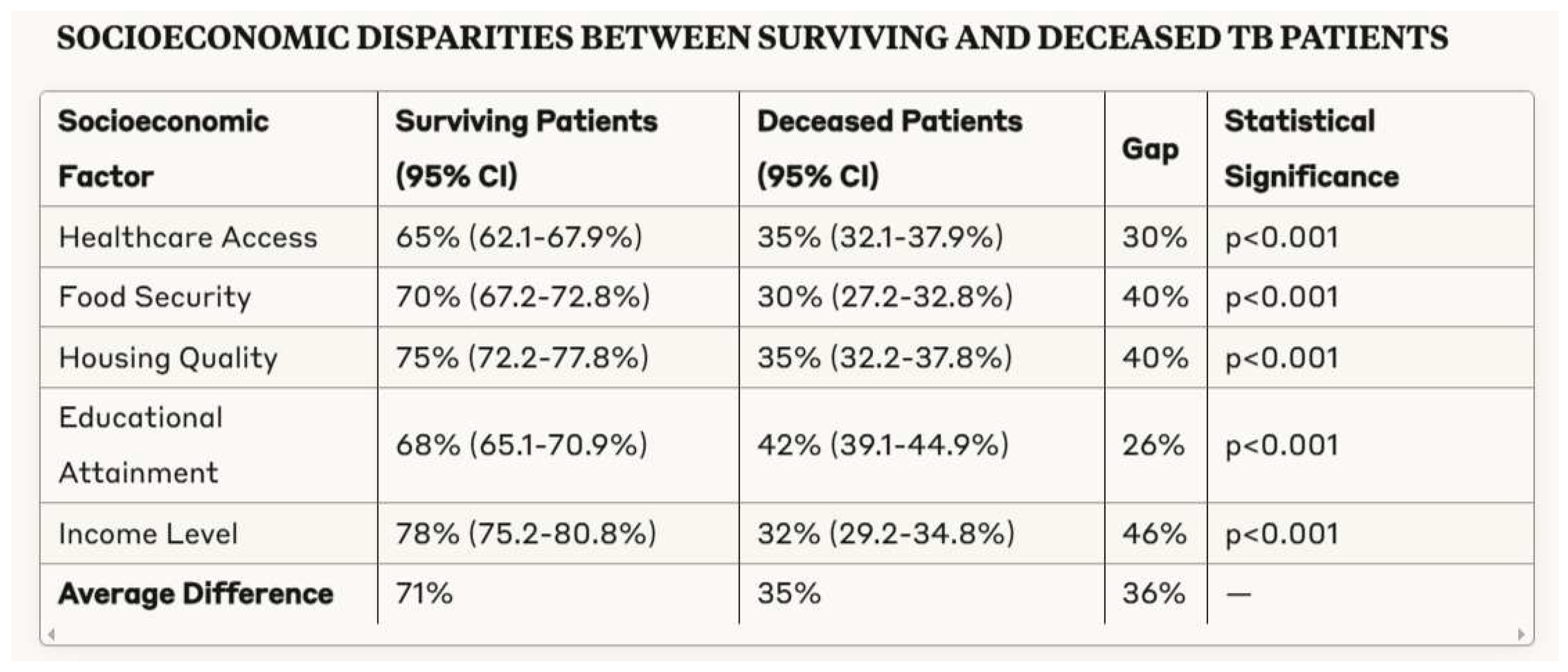
Figure 8.
Geographical Distribution of Tuberculosis Mortality.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



