
Submitted:
02 December 2024
Posted:
03 December 2024
You are already at the latest version
Abstract
Patellofemoral pain (PFP) significantly affects patients’ daily activities and consequently reduces their quality of life. Custom-made foot orthoses (FO) are a common method of medical treatment that positively influence biomechanical factors such as the kinematics of the lower extremity and reduce pain perception in patients. However, there is a gap in the research regarding the influence of different FO treatments on knee pain. Therefore, this study addresses the impact of biomechanical foot orthoses (BMFO) and sensorimotor foot orthoses (SMFO) on patients with foot deformity and PFP. A total of 26 participants (9 men, 17 women; 27.7 ± 10.7 years; 175.0 ± 0.1 cm; 75.7 ± 18.8 kg; BMI: 24.7 ± 5.6) took part in this randomized-controlled clinical trial. In the pre-test, knee pain was evaluated using the Kujala anterior knee pain scale after the physician’s anamnesis and plantar pressure measurement. A 3-month intervention with SMFO and BMFO was performed, and weekly development was evaluated using 11-item visual analog scales (VASs). Repeated measures analyses of variance were used to assess differences between time of measurements (ToMs) and the interaction effect between ToMs and treatment groups (SMFO, BMFO). Statistical analysis revealed no statistically significant interaction between ToMs and treatment groups but a significant main effect on Kujala anterior knee pain scores (MDiff = 10.189; p = .014) and 12-week VAS (p = .001). The findings indicate that both treatment approaches effectively alleviate perceived knee pain in the PFP sample with foot deformity, with neither approach demonstrating superior efficacy. This trial was retrospectively registered in the WHO International Clinical Trials Registry Platform (ICTRP) and German Clinical Trials Register (DRKS00035082).
Keywords:
sensorimotor system
; SMFO
; foot orthoses
; insoles
; knee pain patients
; chondropathia patellae
; orthopedic treatment
; Kujala anterior knee pain scale
; visual analog scale
1. Introduction
Patellofemoral pain (PFP) syndrome is one of the most common causes of anterior knee pain in adolescents and adults [1,2]. It affects 23% of the total population [3]. There is evidence that PFP significantly restricts the quality of life of those affected [4,5], particularly as it is discussed as an indicator of patellofemoral osteoarthritis [6]. These pathologies often place a substantial burden on the healthcare system [7,8]. The term chondropathia patellae is also frequently used, associated with impaired patellofemoral kinematics [9]. The causes of these pain symptoms are multifactorial; therefore, many biomechanically-related etiological factors and treatments are linked to the pathology of PFP [1]. Static and dynamic components, including axial and rotational errors of the lower extremity [10], altered tibial and femoral kinematics [11], increased knee abduction, and muscular overpowering due to increased muscle forces negatively affecting patella guidance [12], might be causative factors. It is unclear whether this influences the development of PFP [1,13]. Foot and ankle postures and excessive pronation of the foot are considered to influence the knee abduction moment in the frontal plane and the ground reaction forces [14,15]. A high pronation speed during running can lead to internal rotation of the tibia [16]. From a biomechanical perspective, the target is to redirect the forces acting on the knee. Hoglund et al. [17] found that PFP patients had increased hip and pelvic range of motion during the step-down test in the frontal and transverse planes but reduced or nearly equal range of motion for these variables during single-leg squats. Correction of increased rear foot eversion might reduce the internal rotation of the tibia and femur, thereby reducing pelvic anteversion [18]. In general, the influence of altered foot function and plantar pressure on PFP is variable and unclear [11].
Custom-made foot orthoses (FOs) are medical aids used to help patients with lower extremity pain [19], foot and ankle motion [20], and excessive foot pronation in gait and running. Depending on the cause and symptoms, the FOs are customized to achieve more favorable kinematic (e.g., joint angle) and kinetic (e.g., force peaks) conditions to relieve lower extremity joint pain [21]. On the one hand, Saxena and Haddad [22] concluded that FOs are an effective treatment option for relieving clinical symptoms of PFP, especially in young people. Gross and Foxworth [24] stated that FOs have a positive impact on PFP patients with excessive foot pronation, lower extremity alignment, and increased Q-angle. A randomized clinical trial by Collins et al. (2008) concluded that FOs improve perceived knee pain rated on a visual analog scale (VAS), exhibit better short-term improvements than flat inserts, and have a similar effect to physiotherapy. Barton et al. [25] provided limited evidence suggesting that prefabricated FOs may reduce transverse plane knee rotation and offer greater short-term relief than flat insoles for individuals with PFP syndrome. Lewinson et al. [26] investigated the potential of modifying the angular impulse magnitude of knee abduction through lateral and medial wedged FOs to alleviate pain in runners with PFP and found a clinically significant pain reduction. On the other hand, Kayll et al. [27] concluded that medial support insoles did not alter patellofemoral joint loads during walking and running.
In orthopedic care, it is common to prescribe FOs to influence knee pathologies. In general, there is a distinction between the two main FO approaches: biomechanical foot orthoses (BMFO) and sensorimotor foot orthoses (SMFO) [23,28]. The BMFO is characterized by supporting and bedding elements that are primarily intended to provide support, correction, and relief, comparable to the aforementioned approaches with a medial and lateral wedge. In contrast, SMFO primarily aims to influence the activity of defined muscles via corresponding elements (e.g., medial or lateral hindfoot elements, toe bridges, and retrocapital elements) at a specific time interval in the step cycle in a targeted manner (tonizing and detonizing) [29,30]. The key therapeutic target of SMIs is to activate the M. peroneus longus and M. tibialis posterior, which stabilize the ankle joint. This stabilization improves foot positioning and pressure distribution, potentially reducing foot pain. In consequence, the adjustment in joint kinematics might alleviate discomfort in other joint segments due to biomechanical interconnections [23]. Kerkhoff et al. [31,32] examined prefabricated BMFOs and SMFOs and their effects on lower-extremity muscle activity in participants with non-specific knee pain. The data showed that the prefabricated BMFO and custom-made SMFO led to different activation patterns compared with the shoe without FOs during a single-leg landing test, whereas SMFOs led to an increased Musculus semitendinosus and M. peroneus longus influence. Chondropathia patellae is listed by Greitemann et al. [30]; on the German DGOOC advisory committee as an indication for SMFO; however, there is a lack of randomized controlled clinical trials investigating whether FOs, especially SMFOs, have a positive effect on knee pain [32] and which patients benefit most from FOs [25]. Therefore, this study targeted to address this research gap.
This study aimed to investigate the following research questions: Do SMFOs reduce the perception of knee pain in PFP patients with foot deformity over a 3-month intervention period, observing between- and within-FO-group differences?
2. Materials and Methods
2.1. Study Design
This was a stratified randomized controlled clinical trial with pre- and post-testing. The intervention period was three months. The sample was randomly assigned by the test supervisor to an orthopedic custom-made device (SMFO, BMFO) over the intervention period after diagnostic and orthopedic anamnesis by the physician, considering the inclusion and exclusion criteria (Table 1 and chapter 2.2) and stratified according to the localization of knee pain (anterior, retro patellar). This trial was blinded which means that the participants were not informed about their assigned intervention. The health provider was also not informed about this fact. The study was conducted from March to November 2024.
Scientific evaluation was performed without disrupting the standard procedure of the physician and orthopedic technician who treated patients with corresponding orthopedic indications. The study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee (Nr. 70, 16.02.2024) and registered in the German Clinical Trials Register (DRKS00035082; 17 September 2024).
A sample size of 24 participants was determined for an analysis of variance (ANOVA) to assess the interaction effect (effect size f = 0.25, 2 groups, 2 ToMs, α error probability = 0.05, correlation among repeated measures: 0.8) using G*Power [33]. More than 30 participants were assessed for eligibility, owing to expected dropouts (see Figure 1). This study adheres to CONSORT guidelines.
2.2. Sample
Participants were recruited within everyday patient care provided by the responsible physician. Anthropometric data are shown in Table 1.
The following inclusion and exclusion criteria were defined, and the same physician was responsible for the medical assessment of patients.
Inclusion criteria:
- ●
- Age between 15 and 60 years
- ●
- Discomfort in the knee joint area during at least two weight-bearing activities (walking stairs, squatting, standing up) for at least three weeks: pain during these activities on most days in the last month that is ≥ 30 mm on a 100 mm VAS
- ●
- Indication (at least one diagnosis from the following list):
- ○
- Femoropatellar pain syndrome
- ○
- Chondropathia patellae up to grade 3 with pathological alignment and femoral antetorsion
- ○
- Runner’s knee, jumper’s knee
- ○
- Osteochondral defects, inflammation, and impingement of the Hoffa fat body
- ○
- Tendinopathies of the patellar or quadriceps tendon, patellofemoral osteoarthritis, plica syndrome
- ●
- Altered Q-angle [34] of the lower extremity/recognizable rotational abnormality of ankle joints, tibia, and femur during gait
- ●
- Foot deformity: Pes planus, Pes valgus, Pes planovalgus, Pes cavus, and Pes transversoplanus
Exclusion criteria:
- ●
- Medical history of knee joint arthroplasty or osteotomy
- ●
- Previous (surgical) treatment (< 12 months) in the ankle, knee, or hip joint
- ●
- X-ray evidence of fixed bone deformity or joint erosion
- ●
- Moderate or severe concomitant tibiofemoral OA (Kellgren and Lawrence grade ≥ 3 on anteroposterior radiograph [35])
- ●
- Underlying neurological pathology
- ●
- Known underlying rheumatic disease with drug treatment
- ●
- Previous treatment with orthopedic FO according to the above concepts while treating the given knee pain indication
- ●
- Acute muscle/ligament injury (< 4 weeks) with associated restriction of the musculoskeletal system
2.3. Procedure
After anamnesis and diagnosis by the physician, the participant was instructed to attend a plantar pressure measurement appointment with an experienced orthopedic technician. The navicular index (NI) [36,37] was determined (0.22-0.31 = normal; < 0.17 = pes planus; > 0.35 = pes cavus) and the Arch Index (AI) [38] was evaluated using a plantar pressure measuring plate (Multisens, go-tec GmbH, Münster, Germany) (< 0.20 = high arch, 0.21-0.26 = normal arch, > 0.26 = flattened arch). All parameters for medically indicated foot orthosis fitting were determined based on a 2D-foot scan and 3D-foot impression. The same orthopedic technician was responsible for manufacturing the FOs for the sample. First, the patient’s medical history and the necessary foot and shoe measurements were obtained using German specifications in the list of aids (product group 08) [30]. A wearing time of at least eight hours per day in the FOs was determined. As a termination criterion during the intervention, an increase in subjectively perceived pain by two points or more during the intervention period was defined. Additional therapy was not restricted due to ethical reasons but was documented. Seven of the 24 participants underwent additional physiotherapeutic treatment once a week.
2.4. Intervention with Foot Orthoses
2.5. Knee Pain, Effectiveness, and Comfort Rating
The participants had to complete the Kujala Anterior Knee Pain Scale [39,40] pre- and post-tests. The questionnaire is a valid and reliable measuring instrument [40]. It is particularly suitable for patients complaining of patellofemoral joint or anterior knee pain [41]. Dammerer et al. [40] validated it for patients with patellofemoral instability using the German version. The total score is 100 points for a symptom-free result and the worst score; therefore, a severe limitation is represented by 0 points.
In addition, 11-item VASs were administered to patients during the intervention time [23,42]. After each week, patients were asked to rate their knee pain perception ( 0 = no pain and 10 = maximum pain) and document the average steps per day within the week according to their individual smartwatch device.
Furthermore, the overall subjective FO effectiveness and level of comfort of the worn FO were rated using an 11-item VAS (0 [least comfort] to 10 [max. comfort]). This approach was adapted from Murley et al. (2010), who used a 150 mm VAS to measure orthosis comfort [43] because the patients were already used to the scale ranging from 0 to 10 for pain rating by VAS. Participants were instructed to document their daily step counts. Daily steps with FOs during treatment were measured using the participant’s individual smartphone and/or smartwatch and assessed within the post-test.
2.6. Statistical Analysis
After preliminary testing for normal distribution using the Shapiro–Wilk test and variance homogeneity using the Levene’s test, two repeated measures ANOVA were used for Kujala knee pain scores and 12-week VAS (within-subject factor: time of measurements (ToMs); between-subject factors: treatment groups (SMFO, BMFO)). Physiotherapeutic treatment was added as a between-subject factor to control for its influence on knee pain development. The Kujala anterior knee pain scores were normally distributed for both groups, as assessed using the Shapiro-Wilk test (p > .05). Therefore, sphericity was assumed. The error variances were homogeneous, as assessed using Levene’s test (p > .05).
Regarding effectiveness and comfort ratings, Levene’s test demonstrated that variance homogeneity was not present in the comfort rating of the BMFO group, and the Shapiro-Wilk test showed that normal distribution was not present in the SMFO group. Therefore, Welch’s t-test was used to assess group differences between subjective FO effectiveness and comfort ratings. Potential differences between the treatment and control groups regarding anthropometric characteristics were additionally explored using independent t-tests and the Holm-Bonferroni method.
Generally, a p-value ≤ 0.05 was chosen as the statistical cut-off point. Calculations and visualizations were performed using SPSS (IBM, version 29, SPSS Inc., Chicago, IL, USA) and JASP (Version 0.19.0, JASP Team, Netherlands) [44].
3. Results
3.1. Perceived Knee Pain
3.1.1. Kujala Knee Pain Score
There was no statistically significant interaction between ToM and treatment groups (F(1, 20) = 0.01, p = .92) or ToM and physiotherapeutic treatment (F(1,20) = 0.09, p = .77), but there was a significant main effect for ToM (F(1,20) = 7.23, p = .01, partial η² = .27). Bonferroni-adjusted post-hoc analysis revealed significantly (p = .01) increased Kujala anterior knee pain scores between pre- and post-test (Diffpost-pre = 10.19 ± 3.79) with Cohen’s d = .71, which represents a medium effect [45] (see Figure 3 and Figure 4).
3.1.2. 12-Week Visual Analog Scales (VASs)
Repeated measures ANOVA showed a highly significant main effect for ToM (F(11, 231) = 12.04, p < .001, partial η² = .36), but there was no statistically significant interaction between ToM and treatment groups (F(11,231) = 1.40, p = .18) or ToM and physiotherapeutic treatment (F(11,231) = 1.47, p = .15). The results of the post-hoc tests are presented in the appendix. Descriptive data are shown in Figure 5.
Mean effectiveness rating was 1.42 (95%-CI[-0.81, 3.64]) higher in the SMFO group and mean comfort rating was 0.36 (95%-CI[-0.99, 1.70]) higher for the SMFO group. Welch-test showed no significant group differences in effectiveness (t(17.93) = 1.33, p = .20) and comfort ratings (t(15.03) = 0.57, p = .58). Descriptive results of effectiveness and comfort, daily steps, and wearing time per day are shown in Table 3. Regarding anthropometric data, t-tests revealed no significant group differences, except for the NI of the right foot. The Holm-Bonferroni correction led to a non-significant result.
4. Discussion
The results indicate that both treatments significantly reduced perceived pain in patients with PFP (p = .01) with a medium effect size (d = 0.71). The lack of a statistically significant interaction between the FO treatment and ToM suggests that neither FO approach is superior. Both interventions led to significant pain reduction between baseline and follow-up measurements, as well as in the 12-week pain development measured by VAS. SMFO were rated more efficient (MeanDiff = 1.42) and slightly more comfortable (MeanDiff = 0.36) than BMFO on a 11-item VAS; however, statistical analysis revealed no significance for either parameter. In both types of FO, a high level of comfort was detected (BMFO: 7.91; SMFO: 8.27); however, it is clinically questionable whether high comfort is an appropriate criterion. For example, Vicenzino et al. [46] investigated predictors of FO success and stated that lower overall comfort had a significant univariate relationship with successful treatment outcomes. Since the FOs target has a primarily kinetic and kinematic influence on the foot and lower extremity, this could potentially lead to discomfort. However, a lack of comfort for patients often leads to decreased compliance with wearing the FOs. With more than an average of 8.000 daily steps with FOs, both treatment groups used the FOs almost equally frequently. The results of this study are consistent with those of Lewinson et al. [26] and Skou et al. [19] who confirmed a significant reduction in perceived knee pain. Several possible explanatory models exist for these results. According to Almeida et al. [47], FOs improve the alignment of the knees, hips, pelvis, and spine by adjusting the distribution of plantar foot pressure from the initial contact to the mid-stance phase. Consequently, the improved biomechanical coupling may be a plausible explanation. Overall, influencing foot position and load in both types of treatments can always have the opposite effect in terms of a stronger sensation of discomfort or even pain due to altered joint kinematics; this must always be considered by the physician and orthopedic technician. Both FO treatments had the same therapeutic target (improved biomechanical coupling and pain reduction) based on different mechanisms of action. The BMFOs primarily target stabilization of the rearfoot, help improve plantar pressure distribution, and reduce peak forces, whereas the main target of the SMFO is earlier activation of the peroneus longus and tibialis posterior muscles by the lateral and medial spots, which stabilize the ankle joint [48]. Therefore, it can be assumed that a targeted improvement in foot position might lead to improved foot kinetics and kinematics. This stabilization and its influence on the other joints of the lower extremity might explain the reduced discomfort in the knee joint due to biomechanical coupling from the foot and knee [49,50].
When interpreting the data, it must be noted that each patient was treated based on their anatomy and the physician’s initial examination. A clear distinction between the two concepts can still be discussed even though both approaches demonstrate clear differences in the therapeutic approach [28,29,30]. It must be also considered that footwear FOs can be influenced by the type of shoes participants wore, as (im)proper or (un)supportive footwear may influence the impact of the FOs. Therefore, the orthopedic technician checked the FOs and footwear for suitability. While the study showed promising results in reducing PFP patients’ pain perception with both SMFO and BMFO, contextual factors such as the placebo effect [51], increased body awareness, and psychological changes likely contributed. Patients may have different pain thresholds, and their reporting could be influenced by personal factors, such as mood, stress, or pain tolerance. Engaging in a clinical trial such as this approach might lead patients to become more aware of their health behaviors, such as exercise habits, activity levels, or posture. The increased motivation to follow prescribed treatments or modify behaviors during the intervention period to positively influence outcomes cannot be controlled. Furthermore, natural and autonomous healing processes of the human body might influence pain relief [23]. However, to measure this effect, another group without any treatment would have been necessary, which was not possible for ethical reasons. Based on the statistical results, the SMFO seems to be an effective treatment option compared to the alternative of BMFO. A review by Barton et al. [25] further indicated that a combination of physiotherapy and prefabricated FOs could be more effective than FOs alone in managing PFPS symptoms. In this trial, physiotherapeutic treatment was shown not to have any significant influence on pain development in Kujala anterior knee pain score and 12-week VAS, but only 7 of 24 participants were documented who had physiotherapeutic treatment once a week. The small number of participants and the short treatment period may have played a significant role; the no control group only used physiotherapy. The focus of this approach was on the effect of FOs rather than on further therapeutic methods; however, this should be investigated in future studies.
The sample size can be seen as an average compared to current studies in the field of SMFO effects, such as [31,48,52,53,54,55]. PFP patients were chosen because of their expected altered gait kinematics [17] and their clinical need for treatment with individually manufactured FOs recommended by a physician. The authors observed a significant improvement in the study’s methodology, as all participants’ FOs were manufactured by the same orthopedic technician with decades of experience. The NI of the sample was reduced [56]. A low NI can favor increased pronation when walking and running, and for this reason, can also be a possible risk factor for PFP. It must be considered that the SMFO group had a lower NI than the control group at baseline measurement. The body mass index of the sample was within the normal range, and the age of the sample corresponded to the target group of younger adults, which was comparable to that reported by Kerkhoff et al. [31]. During participant acquisition, the same physician was responsible for detecting whether the patient fulfilled the defined inclusion criteria and further analyzed foot posture and functionally related lower extremity causes of knee pathology.
Medical examinations included standard diagnostic tools and examinations for physicians and patients [5]. However, the diagnosis of PFP involves different symptoms and manifestations, and it is ultimately impossible to definitively determine whether functional causes of the disease can be found in movement, such as altered tibiofemoral or patellofemoral mechanics [57]. The Kujala anterior knee pain score is a validated measurement tool for detecting subjective pain in patients with knee pain. However, this represents a subjective parameter. The subjective nature of pain reporting can introduce variability into the results. To strengthen the validity by controlling for further disturbing variables, steps and activity levels were assessed, but these were based on self-documentation. It must be considered that there was no standardization in measurement systems (e.g., smartphones or smartwatches), possibly for legal reasons (data law).
A major limitation, which is why studies on custom-made FOs in general and SMFO in particular, are very limited, is that custom-made FO must always be individually adapted to the anatomical and physiological conditions of the patient. This makes standardization of the treatment, and thus, comparability between participants difficult [29]. However, this study examined pain development (ToM) as a within-subject factor. The FOs were made by the same orthopedic technician with over four decades of professional experience. Each FO was individually fitted to a shoe prior to testing. Furthermore, there was an unequal distribution between sexes including 9 men and 17 women. In addition, investigating the long-term effects of FOs beyond the 3-month intervention period is crucial, as sustained efficacy remains unclear. Incorporating functional assessments and quality-of-life metrics could provide a more comprehensive understanding of the overall impact of FOs on patients’ daily lives.
Future studies should investigate kinetic and kinematic changes achieved through FOs, more specifically in all planes, and the differentiation of ankle movements. In addition, larger and gender-equal samples as well as older age groups should be investigated. Furthermore, more research must be conducted regarding different indications for FO treatment, as there is still no consensus in science regarding when and to what extent FOs can be used for the orthopedic treatment of different lower extremity pathologies. There is a need for further clinical randomized controlled trials and longitudinal studies investigating not only the short term but also the long term.
5. Conclusions
In conclusion, the data of this study support the hypothesis that SMFO and BMFO are equally effective treatment options for PFP patients with foot deformities. Although neither approach proved significantly superior, both interventions contributed to meaningful pain relief as the primary therapeutic target. SMFO were rated as more effective and slightly more comfortable by the participants at the follow-up measurement, but no significant group differences were detected. Future studies should include objective biomechanical assessments to provide a more comprehensive understanding of the exact mechanism of action.
Author Contributions
Conceptualization, S.S.; methodology, S.S., A.H. & S.B.; software, S.S. & J.D.; validation, S.S., S.B. & J.D.; formal analysis, S.S. & J.D.; investigation, S.S., A.H.; resources, M.F., S.S. & A.H.; data curation, J.D..; writing—original draft preparation, S.S.; writing—review and editing, S.S., S.B., O.L., J.D., C.D., M.F..; visualization, S.S. & C.D.; supervision, M.F., S.B.; project administration, S.S.; funding acquisition, S.S. All authors have read and agreed to the published version of the manuscript.
Funding
This study received no external funding.
Institutional Review Board Statement
This research was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee (Ethikkommission des Fachbereichs Sozialwissenschaften, Nr. 70, 16.02.2024) for studies involving humans and pre-registered in the German Clinical Trials Register (DRKS00035082).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study. Written informed consent was obtained from all participants prior to their inclusion in the study. For participants under the age of 18, consent was additionally obtained from their legal guardians.
Acknowledgments
We would like to thank the orthopedic technician Stefan Woltring for manufacturing the FOs used in this study.
Conflicts of Interest
The author Steven Simon has a part-time job at Springer Aktiv AG.
Data statement: The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
- Bazett-Jones, D.M.; Neal, B.S.; Legg, C.; Hart, H.F.; Collins, N.J.; Barton, C.J. Kinematic and kinetic gait characteristics in people with Patellofemoral Pain: a systematic review and Meta-analysis. Sports Medicine 2023, 53, 519–547. [Google Scholar] [CrossRef] [PubMed]
- Kellish, A.S.; Kellish, P.; Hakim, A.; Miskiel, S.; Shahi, A.; Kellish, A. What is the effect on kinesio taping on pain and gait in patients with patellofemoral pain syndrome? Cureus 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Crossley, K.M.; van Middelkoop, M.; Callaghan, M.J.; Collins, N.J.; Rathleff, M.S.; Barton, C.J. 2016 Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester. Part 2: recommended physical interventions (exercise, taping, bracing, foot orthoses and combined interventions). British journal of sports medicine 2016, 50, 844–852. [Google Scholar] [CrossRef]
- Coburn, S.L.; Barton, C.J.; Filbay, S.R.; Hart, H.F.; Rathleff, M.S.; Crossley, K.M. Quality of life in individuals with patellofemoral pain: a systematic review including meta-analysis. Physical Therapy in Sport 2018, 33, 96–108. [Google Scholar] [CrossRef]
- Fulkerson, J.P. Diagnosis and treatment of patients with patellofemoral pain. The American journal of sports medicine 2002, 30, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Utting, M.; Davies, G.; Newman, J. Is anterior knee pain a predisposing factor to patellofemoral osteoarthritis? The knee 2005, 12, 362–365. [Google Scholar] [CrossRef]
- Afzali, T.; Fangel, M.V.; Vestergaard, A.S.; Rathleff, M.S.; Ehlers, L.H.; Jensen, M.B. Cost-effectiveness of treatments for non-osteoarthritic knee pain conditions: A systematic review. PLoS One 2018, 13, e0209240. [Google Scholar] [CrossRef] [PubMed]
- Glaviano, N.R.; Kew, M.; Hart, J.M.; Saliba, S. Demographic and epidemiological trends in patellofemoral pain. International journal of sports physical therapy 2015, 10, 281. [Google Scholar] [PubMed]
- Aysin, I.K.; Askin, A.; Mete, B.D.; Guvendi, E.; Aysin, M.; Kocyigit, H. Investigation of the relationship between anterior knee pain and chondromalacia patellae and patellofemoral malalignment. The Eurasian journal of medicine 2018, 50, 28. [Google Scholar] [CrossRef] [PubMed]
- Fairbank, J.; Pynsent, P.; van Poortvliet, J.A.; Phillips, H. Mechanical factors in the incidence of knee pain in adolescents and young adults. The Journal of Bone & Joint Surgery British Volume 1984, 66, 685–693. [Google Scholar] [CrossRef]
- Powers, C.M.; Witvrouw, E.; Davis, I.S.; Crossley, K.M. Evidence-based framework for a pathomechanical model of patellofemoral pain: 2017 patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester, UK: part 3. British journal of sports medicine 2017, 51, 1713–1723. [Google Scholar] [CrossRef]
- Stefanyshyn, D.J.; Stergiou, P.; Lun, V.M.; Meeuwisse, W.H.; Worobets, J.T. Knee angular impulse as a predictor of patellofemoral pain in runners. The American journal of sports medicine 2006, 34, 1844–1851. [Google Scholar] [CrossRef]
- Lankhorst, N.E.; Bierma-Zeinstra, S.M.; van Middelkoop, M. Risk factors for patellofemoral pain syndrome: a systematic review. Journal of orthopaedic & sports physical therapy 2012, 42, 81–94. [Google Scholar] [CrossRef]
- Powers, C.M. The influence of altered lower-extremity kinematics on patellofemoral joint dysfunction: a theoretical perspective. Journal of Orthopaedic & Sports Physical Therapy 2003, 33, 639–646. [Google Scholar] [CrossRef]
- Barton, C.J.; Bonanno, D.; Levinger, P.; Menz, H.B. Foot and ankle characteristics in patellofemoral pain syndrome: a case control and reliability study. Journal of Orthopaedic & Sports Physical Therapy 2010, 40, 286–296. [Google Scholar] [CrossRef]
- Hintermann, B.; Nigg, B.M. Pronation in runners: Implications for injuries. Sports medicine 1998, 26, 169–176. [Google Scholar] [CrossRef]
- Hoglund, L.T.; Hulcher, T.A.; Amabile, A.H. Males with patellofemoral pain have altered movements during step-down and single-leg squatting tasks compared to asymptomatic males: A cross-sectional study. Health Science Reports 2024, 7, e2193. [Google Scholar] [CrossRef] [PubMed]
- Duval, K.; Lam, T.; Sanderson, D. The mechanical relationship between the rearfoot, pelvis and low-back. Gait & posture 2010, 32, 637–640. [Google Scholar] [CrossRef]
- Skou, S.T.; Hojgaard, L.; Simonsen, O.H. Customized foot insoles have a positive effect on pain, function, and quality of life in patients with medial knee osteoarthritis. Journal of the American Podiatric Medical Association 2013, 103, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Collins, N.; Crossley, K.; Beller, E.; Darnell, R.; McPoil, T.; Vicenzino, B. Foot orthoses and physiotherapy in the treatment of patellofemoral pain syndrome: randomised clinical trial. Bmj 2008, 337. [Google Scholar] [CrossRef]
- Mündermann, A.; Nigg, B.M.; Humble, R.N.; Stefanyshyn, D.J. Foot orthotics affect lower extremity kinematics and kinetics during running. Clinical biomechanics 2003, 18, 254–262. [Google Scholar] [CrossRef]
- Saxena, A.; Haddad, J. The effect of foot orthoses on patellofemoral pain syndrome. Journal of the American Podiatric Medical Association 2003, 93, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.; Simon, S.; Mühlen, J.; Dindorf, C.; Fröhlich, M. Assessing the Subjective Effectiveness of Sensorimotor Insoles (SMIs) in Reducing Pain: A Descriptive Multicenter Pilot Study. Journal of Functional Morphology and Kinesiology 2023, 8, 66. [Google Scholar] [CrossRef]
- Gross, M.T.; Foxworth, J.L. The role of foot orthoses as an intervention for patellofemoral pain. Journal of Orthopaedic & Sports Physical Therapy 2003, 33, 661–670. [Google Scholar] [CrossRef]
- Barton, C.J.; Munteanu, S.E.; Menz, H.B.; Crossley, K.M. The efficacy of foot orthoses in the treatment of individuals with patellofemoral pain syndrome: a systematic review. Sports Medicine 2010, 40, 377–395. [Google Scholar] [CrossRef] [PubMed]
- Lewinson, R.T.; Wiley, J.P.; Humble, R.N.; Worobets, J.T.; Stefanyshyn, D.J. Altering knee abduction angular impulse using wedged insoles for treatment of patellofemoral pain in runners: a six-week randomized controlled trial. PloS one 2015, 10, e0134461. [Google Scholar] [CrossRef]
- Kayll, S.A.; Hinman, R.S.; Bryant, A.L.; Bennell, K.L.; Rowe, P.L.; Paterson, K.L. Do biomechanical foot-based interventions reduce patellofemoral joint loads in adults with and without patellofemoral pain or osteoarthritis? A systematic review and meta-analysis. British Journal of Sports Medicine 2023. [Google Scholar] [CrossRef]
- Ranker, A. Sensomotorische Schuheinlagen–Wirkprinzipien und Evidenz. manuelletherapie 2020, 24, 168–172. [Google Scholar] [CrossRef]
- Becker, S.; Ludwig, O.; Woltring, S.; Simon, S.; Fröhlich, M. Sensomotorische Einlagen: Grundlagen und Funktionen; Springer-Verlag, 2024. [Google Scholar]
- Greitemann, B.; Franzen, M.; Stinus, H.; Walther, M.; Dierolf, W.; Schievink, F.; Perick, H.; Stief, T.; Stumpf, J. DGOOC-Beratungsausschuss Orthopädieschuhtechnik. Orthopädie und Unfallchirurgie-Mitteilungen und Nachrichten 2016, 5, 283–286. [Google Scholar] [CrossRef]
- Kerkhoff, A.; Wagner, H.; Nagel, A.; Möller, M.; Peikenkamp, K. Effects of two different foot orthoses on muscle activity in female during single-leg landing. German Journal of Exercise and Sport Research 2017, 4, 305–314. [Google Scholar] [CrossRef]
- Kerkhoff, A.; Wagner, H.; Peikenkamp, K. Different effects of sensorimotor and soft bedding foot orthoses on muscle activity during single-leg landing in sports. Footwear Science 2019, 11, S37–S38. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behavior research methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Mizuno, Y.; Kumagai, M.; Mattessich, S.M.; Elias, J.J.; Ramrattan, N.; Cosgarea, A.J.; Chao, E.Y. Q-angle influences tibiofemoral and patellofemoral kinematics. Journal of orthopaedic research 2001, 19, 834–840. [Google Scholar] [CrossRef] [PubMed]
- Schiphof, D.; Boers, M.; Bierma-Zeinstra, S.M. Differences in descriptions of Kellgren and Lawrence grades of knee osteoarthritis. Annals of the rheumatic diseases 2008, 67, 1034–1036. [Google Scholar] [CrossRef] [PubMed]
- Murley, G.S.; Menz, H.B.; Landorf, K.B. A protocol for classifying normal-and flat-arched foot posture for research studies using clinical and radiographic measurements. Journal of foot and ankle research 2009, 2, 1–13. [Google Scholar] [CrossRef]
- Queen, R.M.; Mall, N.A.; Hardaker, W.M.; Nunley, J.A. Describing the medial longitudinal arch using footprint indices and a clinical grading system. Foot & ankle international 2007, 28, 456–462. [Google Scholar]
- Cavanagh, P.R.; Rodgers, M.M. The arch index: a useful measure from footprints. Journal of biomechanics 1987, 20, 547–551. [Google Scholar] [CrossRef]
- Kujala, U.M.; Jaakkola, L.H.; Koskinen, S.K.; Taimela, S.; Hurme, M.; Nelimarkka, O. Scoring of patellofemoral disorders. Arthroscopy: The Journal of Arthroscopic & Related Surgery 1993, 9, 159–163. [Google Scholar] [CrossRef]
- Dammerer, D.; Liebensteiner, M.; Kujala, U.; Emmanuel, K.; Kopf, S.; Dirisamer, F.; Giesinger, J. Validation of the German version of the Kujala score in patients with patellofemoral instability: a prospective multi-centre study. Archives of Orthopaedic and Trauma Surgery 2018, 138, 527–535. [Google Scholar] [CrossRef]
- Crossley, K.M.; Bennell, K.L.; Cowan, S.M.; Green, S. Analysis of outcome measures for persons with patellofemoral pain: which are reliable and valid? Archives of physical medicine and rehabilitation 2004, 85, 815–822. [Google Scholar] [CrossRef]
- Bijur, P.E.; Silver, W.; Gallagher, E.J. Reliability of the visual analog scale for measurement of acute pain. Academic emergency medicine 2001, 8, 1153–1157. [Google Scholar] [CrossRef] [PubMed]
- Murley, G.S.; Landorf, K.B.; Menz, H.B. Do foot orthoses change lower limb muscle activity in flat-arched feet towards a pattern observed in normal-arched feet? Clinical Biomechanics 2010, 25, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Team, J. JASP. 2024.
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, 1988; Volume 2, p. 567. [Google Scholar]
- Vicenzino, B.; Collins, N.; Cleland, J.; McPoil, T. A clinical prediction rule for identifying patients with patellofemoral pain who are likely to benefit from foot orthoses: a preliminary determination. British journal of sports medicine 2010, 44, 862–866. [Google Scholar] [CrossRef] [PubMed]
- Almeida, J.S.; Vanderlei, F.M.; Pastre, E.C.; Martins, R.A.; Padovani, C.R.; Guaracy Filho, C. Comparison of two types of insoles on Musculoskeletal symptoms and plantar pressure distribution in a work environment: a randomized clinical trial. Clinical Medicine & Research 2016, 14, 67–74. [Google Scholar] [CrossRef]
- Ludwig, O.; Kelm, J.; Fröhlich, M. The influence of insoles with a peroneal pressure point on the electromyographic activity of tibialis anterior and peroneus longus during gait. Journal of foot and ankle research 2016, 9, 1–9. [Google Scholar] [CrossRef]
- Burnfield, M. Gait analysis: normal and pathological function. Journal of Sports Science and Medicine 2010, 9, 353. [Google Scholar]
- Ohlendorf, D.; Natrup, J.; Niklas, A.; Kopp, S. Veränderung der Körperhaltung durch haltungsverbessernde, sensomotorische, Einlegesohlen. Manuelle Medizin 2008, 46, 93–98. [Google Scholar] [CrossRef]
- Chen, A.T.; Shrestha, S.; Collins, J.E.; Sullivan, J.K.; Losina, E.; Katz, J.N. Estimating contextual effect in nonpharmacological therapies for pain in knee osteoarthritis: a systematic analytic review. Osteoarthritis Cartilage 2020, 28, 1154–1169. [Google Scholar] [CrossRef]
- Mabuchi, A.; Kitoh, H.; Inoue, M.; Hayashi, M.; Ishiguro, N.; Suzuki, N. The biomechanical effect of the sensomotor insole on a pediatric intoeing gait. International Scholarly Research Notices 2012, 2012. [Google Scholar] [CrossRef]
- Ferreira, L.A.B.; Cimolin, V.; Neto, H.P.; Grecco, L.A.C.; Lazzari, R.D.; Dumont, A.J.L.; Galli, M.; Oliveira, C.S. Effect of postural insoles on gait pattern in individuals with hemiparesis: A randomized controlled clinical trial. Journal of Bodywork and Movement Therapies 2018, 22, 792–797. [Google Scholar] [CrossRef]
- Klein, T.; Lastovicka, O.; Janura, M.; Svoboda, Z.; Chapman, G.J.; Richards, J. The immediate effects of sensorimotor foot orthoses on foot kinematics in healthy adults. Gait & Posture 2021, 84, 93–101. [Google Scholar] [CrossRef]
- MacFarlane, C.; Hing, W.; Orr, R. Using the Edinburgh visual gait score to compare ankle-foot orthoses, sensorimotor orthoses and barefoot gait pattern in children with cerebral palsy. Children 2020, 7, 54. [Google Scholar] [CrossRef] [PubMed]
- Murley, G.S.; Menz, H.B.; Landorf, K.B. A protocol for classifying normal-and flat-arched foot posture for research studies using clinical and radiographic measurements. Journal of foot and ankle research 2009, 2, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Salsich, G.B.; Perman, W.H. Tibiofemoral and patellofemoral mechanics are altered at small knee flexion angles in people with patellofemoral pain. Journal of Science and Medicine in Sport 2013, 16, 13–17. [Google Scholar] [CrossRef]
Figure 1.
Consort flow diagram of the randomized-controlled trial.
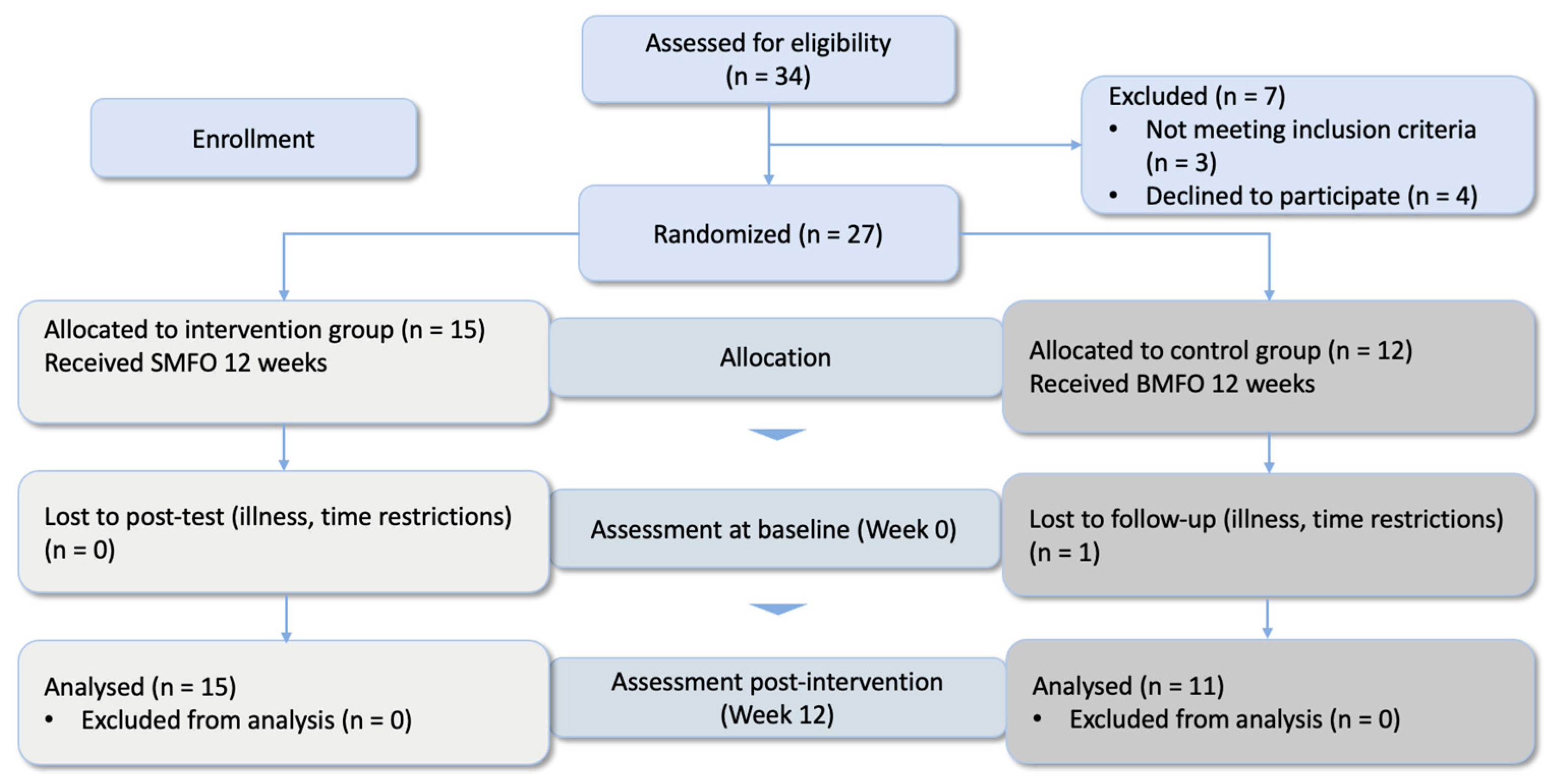
Figure 2.
Custom-made sensorimotor foot orthoses (SMFO) in sandwich material and biomechanical foot orthoses (BMFO).
Figure 2.
Custom-made sensorimotor foot orthoses (SMFO) in sandwich material and biomechanical foot orthoses (BMFO).
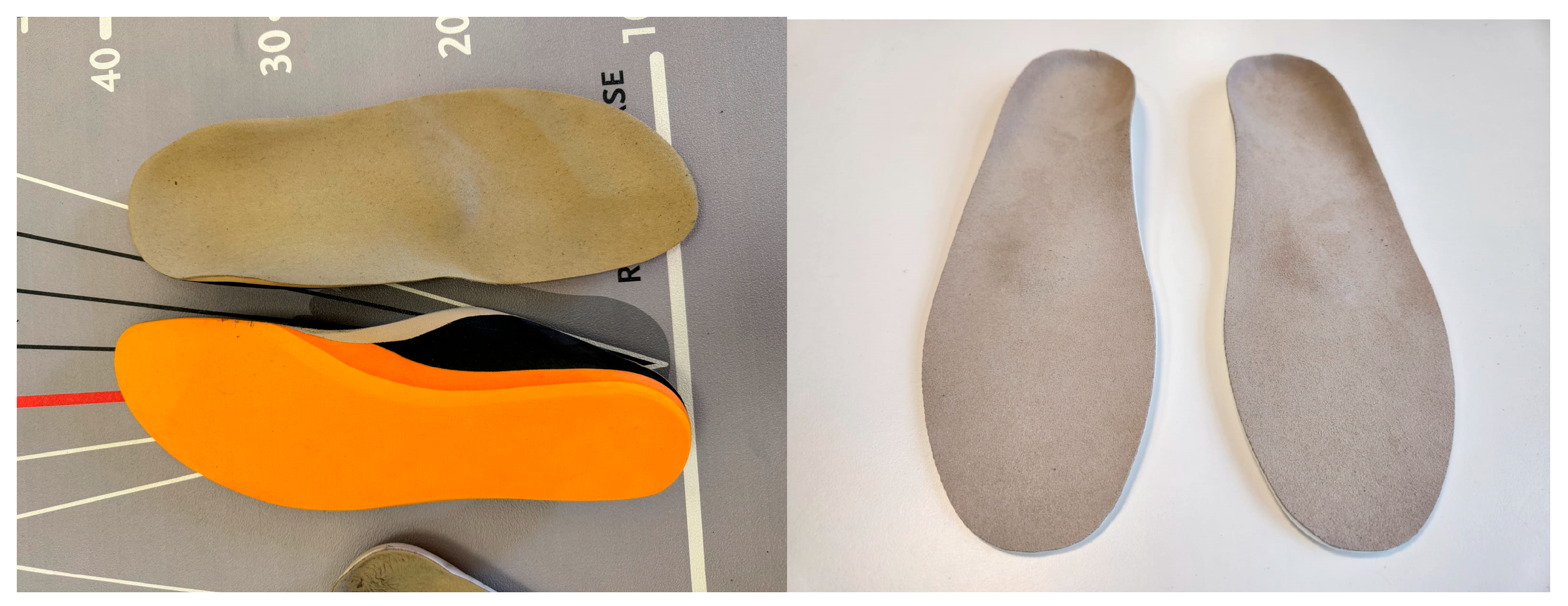
Figure 3.
Line diagram and boxplots representing the intervention group in baseline (green dots and bars) and follow-up measurement (red dots and bars). The overall score is 100 points for a maximum good result. Abbreviation: SMFO = sensorimotor foot orthoses. Colors: green = pre-test, orange = post-test.
Figure 3.
Line diagram and boxplots representing the intervention group in baseline (green dots and bars) and follow-up measurement (red dots and bars). The overall score is 100 points for a maximum good result. Abbreviation: SMFO = sensorimotor foot orthoses. Colors: green = pre-test, orange = post-test.
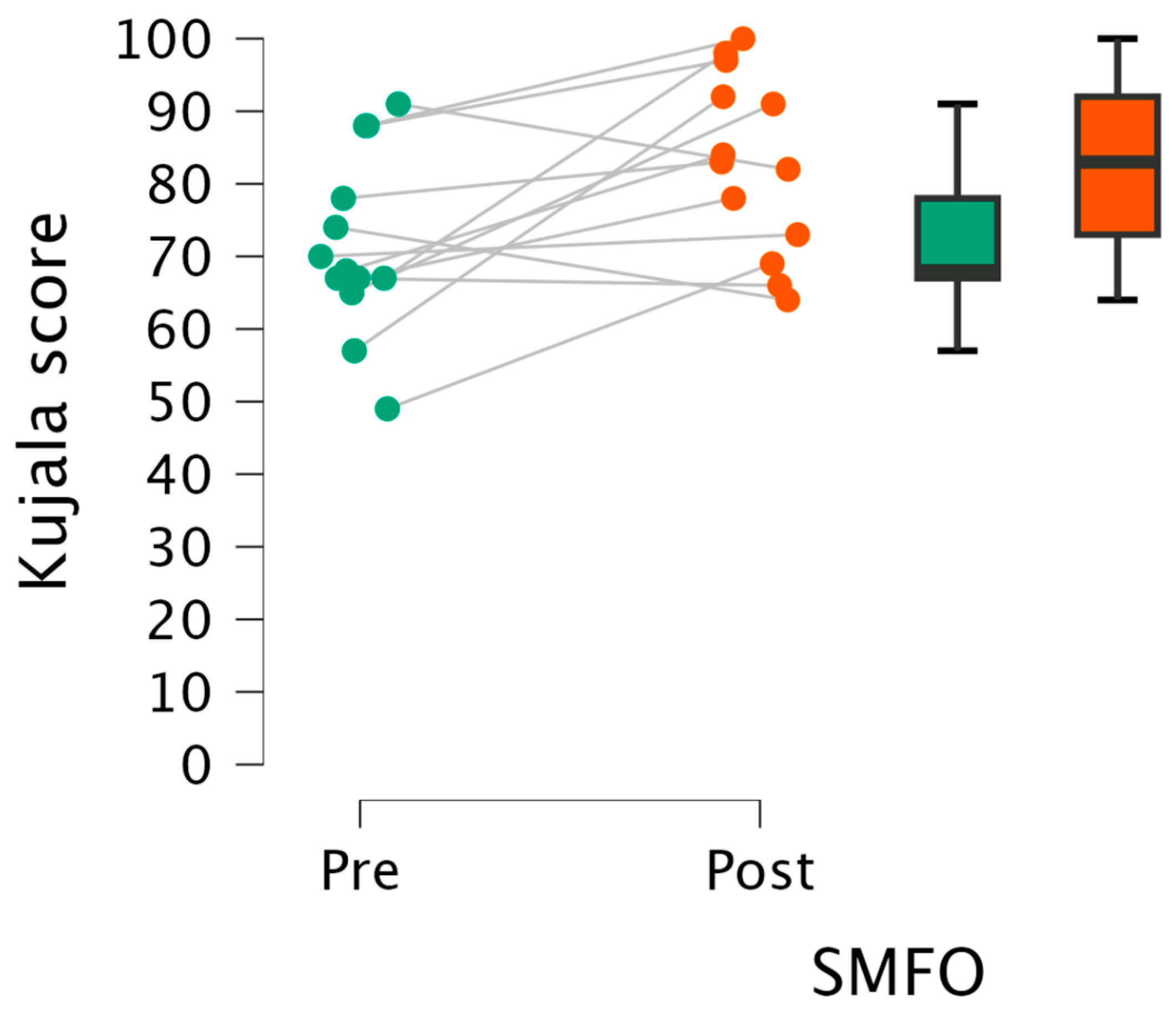
Figure 4.
Line diagram and boxplots representing control group in baseline and follow-up measurement. The overall score is 100 points for a maximum good result. The worst score, and therefore a severe restriction, is 0 points. Abbreviation: BMFO = biomechanical foot orthosis. Colors: green = pre-test, orange = post-test.
Figure 4.
Line diagram and boxplots representing control group in baseline and follow-up measurement. The overall score is 100 points for a maximum good result. The worst score, and therefore a severe restriction, is 0 points. Abbreviation: BMFO = biomechanical foot orthosis. Colors: green = pre-test, orange = post-test.
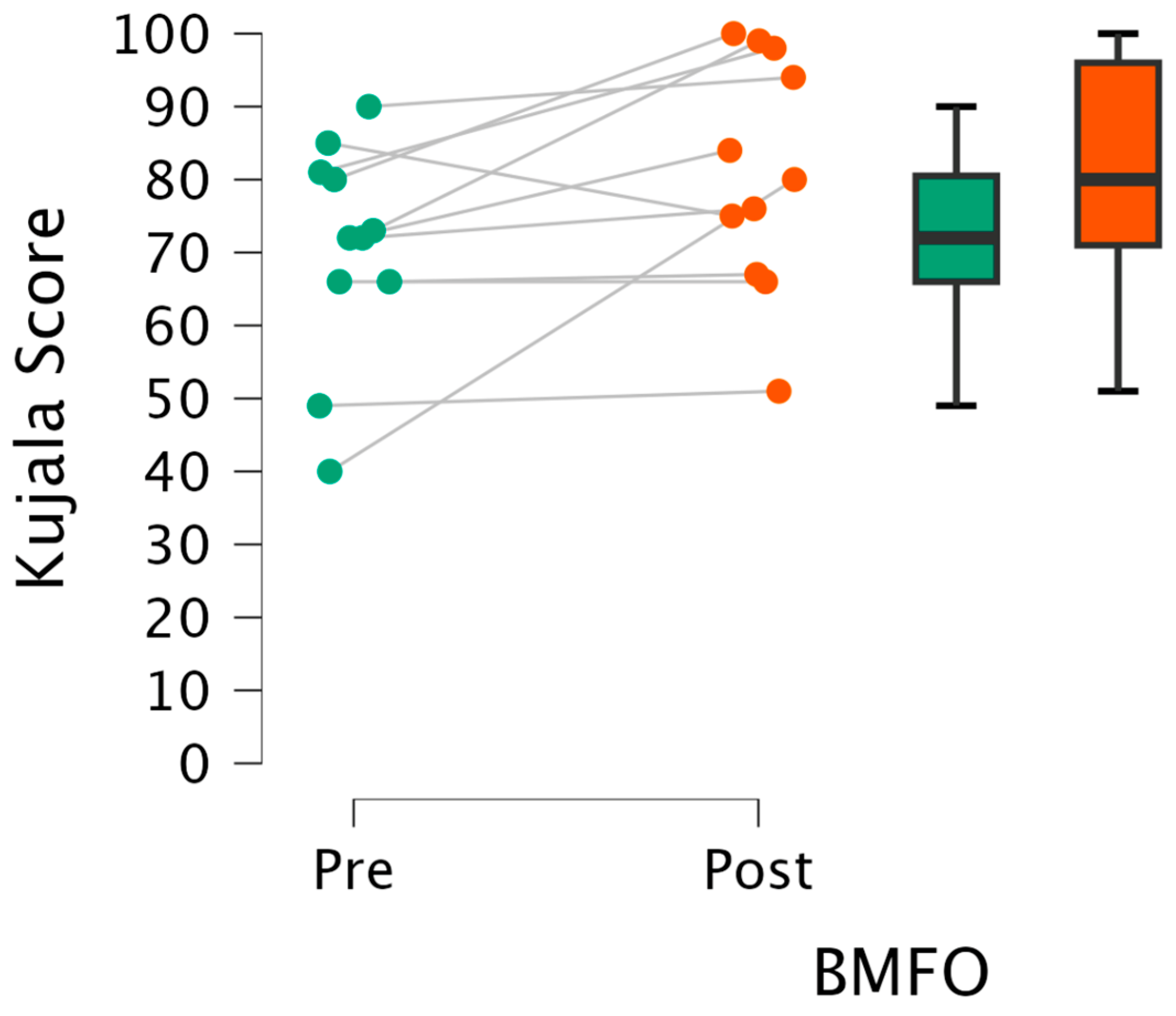
Figure 5.
Bar charts representing mean values and 95% confidence interval (error bars) representing VAS development during intervention period. X-axis = intervention weeks; Y-axis = VAS Score. Abbreviations: VAS = Visual Analog Scale, SMFO = Intervention group, BMFO = control group, W1–12 = weeks.
Figure 5.
Bar charts representing mean values and 95% confidence interval (error bars) representing VAS development during intervention period. X-axis = intervention weeks; Y-axis = VAS Score. Abbreviations: VAS = Visual Analog Scale, SMFO = Intervention group, BMFO = control group, W1–12 = weeks.
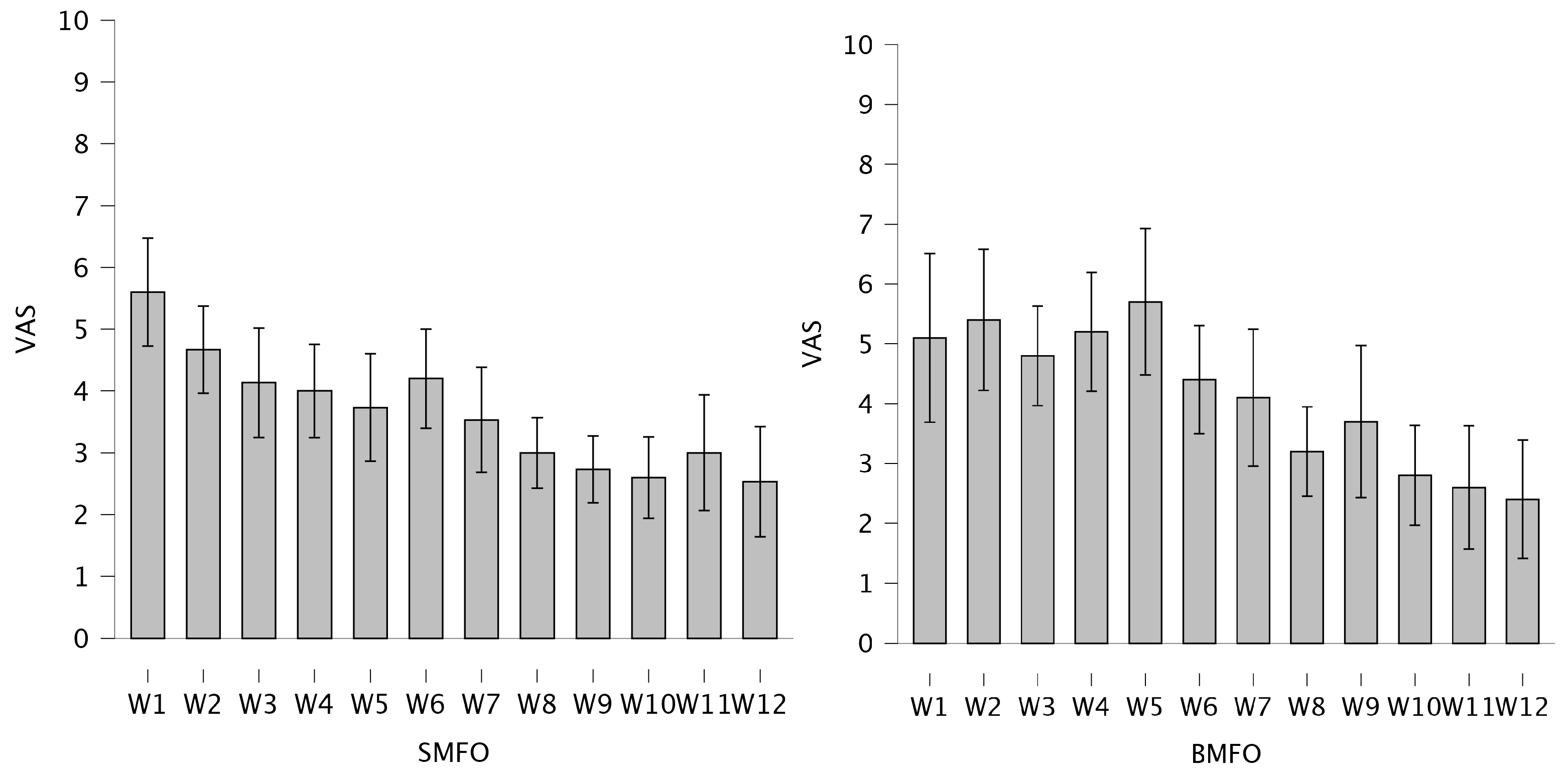

Table 1.
Anthropometric data of the sample (n = 26).
| Age (y) | Height (m) | Weight (kg) | BMI | NI links | NI rechts | AI links | AI rechts | ||
| SMFO | Mean | 27.27 | 1.76 | 75.40 | 24.30 | 0.17 | 0.17 | 0.22 | 0.22 |
| SD | 9.19 | 0.10 | 18.24 | 4.64 | 0.04 | 0.04 | 0.07 | 0.06 | |
| Max | 42.00 | 1.92 | 115.00 | 33.24 | 0.25 | 0.24 | 0.31 | 0.31 | |
| Min | 15.00 | 1.56 | 47.00 | 17.26 | 0.11 | 0.11 | 0.09 | 0.09 | |
| BMFO | Mean | 29.67 | 1.75 | 77.58 | 25.32 | 0.20 | 0.21 | 0.24 | 0.24 |
| SD | 13.39 | 0.09 | 20.22 | 6.53 | 0.06 | 0.06 | 0.06 | 0.02 | |
| Max | 54 | 1.97 | 120 | 42.52 | 0.33 | 0.33 | 0.30 | 0.27 | |
| Min | 16 | 1.64 | 50 | 16.14 | 0.13 | 0.13 | 0.10 | 0.21 |
* Abbreviations: y = years; m = meters; kg = kilograms; NI = Navicular index; AI = Arch Index.
Table 2.
Characteristics and technical data of foot orthoses (SMFO = sensorimotor foot orthoses, BMFO = biomechanical foot orthoses).
Table 2.
Characteristics and technical data of foot orthoses (SMFO = sensorimotor foot orthoses, BMFO = biomechanical foot orthoses).
| FO type | Manufacturer | Primary medical target | Elements | Materials |
| SMFO | Springer Aktiv AG | Stimulating M. tibialis posterior and M. peroneus longus and brevisStretching plantar fascia and toes | Medial spot (oriented toward M. tibialis posterior tendon at sustentaculum tali)Lateral spot (oriented toward M. peroneus longus and brevis tendon near Os cuboideum)Retrocapital bar (supporting the transversal arch and stretching plantar fascia)Toe bar (placing and stretching of toes) | EVA-material; Sandwich construction consisting of 35 Shore (outsole), 25 Shore (midsole), 35 Shore (top-layer) |
| BMFO | Hema Orthopädische Systeme GmbH | Medial arch supportTransversal arch support Pressure relief |
Heel padSupination wedgeMetatarsal pad (pelotte) | Injection molded foam25 Shore |
Table 3.
Mean and standard deviation (SD) of subjective effectiveness rating (0 = no help at all, 10 = maximal help) and comfort (0 = no comfort at all, 10 = maximal comfort) by the participants. Abbreviations: IG = intervention group; CG = control group; FO = foot orthoses.
Table 3.
Mean and standard deviation (SD) of subjective effectiveness rating (0 = no help at all, 10 = maximal help) and comfort (0 = no comfort at all, 10 = maximal comfort) by the participants. Abbreviations: IG = intervention group; CG = control group; FO = foot orthoses.
| FO effectiveness | Wearing comfort | Daily steps in FOs |
Wearing time/ day (h) |
||
| IG | Mean | 7.87 | 8.27 | 8360 | 9.68 |
| SD | 2.23 | 1.10 | 6464 | 4.10 | |
| CG | Mean | 6.45 | 7.91 | 8947 | 10.00 |
| SD | 2.94 | 1.87 | 4842 | 2.67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



