
Submitted:
27 November 2024
Posted:
28 November 2024
You are already at the latest version
Abstract
Extracorporeal carbon dioxide removal (ECCO2R) is an emerging technique designed to reduce carbon dioxide (CO2) levels in venous blood while enabling lung-protective ventilation or alleviating the work of breathing. Unlike high-flow extracorporeal membrane oxygenation (ECMO), ECCO2R operates at lower blood flows (0.4–1.5 L/min), making it less invasive, with smaller cannulas and simpler devices. Despite encouraging results in controlling respiratory acidosis, its broader adoption is hindered by complications, including haemolysis, thrombosis, and bleeding.
Technological advances, including enhanced membrane design, gas exchange efficiency, and anti-coagulation strategies, are essential to improving safety and efficacy. Innovations such as wearable prototypes that adapt CO2 removal to patient activity and catheter-based systems for lower blood flow are expanding the potential applications of ECCO2R, including as a bridge to lung transplantation and in outpatient settings. Promising experimental approaches include respiratory dialysis, carbonic anhydrase-coated membranes, and electrodialysis to maximise CO2 removal.
Further research is needed to optimise device performance, develop cost-effective systems, and establish standardised protocols for safe clinical implementation. As the technology matures, integration with artificial intelligence (AI) and machine learning may personalise therapy, improving outcomes. Ongoing clinical trials will be pivotal in addressing these challenges, ultimately enhancing the role of ECCO2R in critical care and its accessibility across healthcare settings.
Keywords:
extra-corporeal CO2 Removal (ECCO2R)
; acute respiratory distress syndrome (ARDS)
; Haemolysis
; thrombosis
1. Introduction
Extracorporeal carbon dioxide removal (ECCO2R) is a technique designed to remove carbon dioxide from the venous blood, thereby reducing the intensity of mechanical ventilation. Unlike high-flow extracorporeal membrane oxygenation (ECMO), ECCO2R does not provide oxygenation, as it operates at lower blood flows ranging from 0.4 up to 1.5 L/min, depending on the device. The lower blood flow reduces the procedure's invasiveness, allowing smaller cannulae and simpler extracorporeal devices. To refine this lung-support technology, various ECCO2R configurations and techniques have been explored in benchtop and animal models.
There is a specific interest in using ECCO2R to improve the management of acute respiratory distress syndrome (ARDS) and chronic obstructive pulmonary disease (COPD). ECCO2R shows potential for other applications, including serving as a bridge to lung transplantation and enabling long-term CO2 management in outpatient settings. ECCO2R faces barriers such as hemolysis, thrombosis and bleeding, which limit its clinical adoption. This review highlights recent advancements in ECCO2R technology, including device configurations, CO2 removal efficiency, and optimised anticoagulation strategies. We explore the physiological impacts of ECCO2R systems studied through animal models and mock circulation setups to evaluate safety and performance. We also explore key research priorities, including improving gas exchange membranes, refining blood flow and anticoagulation protocols to reduce complications, and investigating innovative approaches such as membrane acidification and hybrid devices.
2. Clinical Evidence for ECCO2R
ECCO2R has been investigated for its role in managing acute respiratory distress syndrome (ARDS) and acute hypercapnic respiratory failure, particularly acute exacerbations of chronic obstructive pulmonary disease (AECOPD). The earliest model of ECCO2R utilised a pumpless arterio-venous (AV) approach, diverting a portion of the patient’s cardiac output through the device [1] via a femoral arterio-venous circuit. Several case reports and case series documented the use of pumpless AV ECCO2R [2,3,4,5,6,7,8,9,10,11,12] and demonstrated their ability to decrease arterial CO2 and resolve respiratory acidosis. However, complications associated with the use of AV ECCO2R were considerable, including bleeding (18-47%), thrombosis (0-20%) and limb ischaemia (4.5-22%)[2,4].
Pumped ECCO2R systems were later developed, enabling a veno-venous (VV) approach, typically using a double-lumen cannula placed in the femoral or jugular vein[13]. Animal studies consistently show that VV ECCO2R can effectively control respiratory acidosis [14,15,16,17,18]. Similarly, uncontrolled clinical studies demonstrated similar results in patients with ARDS and AECOPD[4,16,19,20,21,22,23,24]. However, a retrospective propensity-matched case-control study using VV ECCO2R in COPD found no difference in outcome with ECCO2R use [25]. Recently, VV ECCO2R has been safely integrated with renal replacement therapy platforms in patients with acute respiratory distress syndrome [26,27] and AECOPD [28]. Case series have also reported reduced intubation rate in AECOPD and decreased respiratory rate when used alone or with non-invasive mechanical ventilation[29,30,31].
In ARDS management, the delivery of lung protective ventilation - reducing driving pressure, optimising PEEP, limiting plateau pressure and tidal volume – is hindered by significant respiratory acidosis and acute cor pulmonale. Trials, such as the SUPERNOVA study, investigated using ECCO2R to achieve ultra-low tidal volumes of 3-4 mL/kg in mechanically ventilated ARDS patients, demonstrating feasibility and safety in controlling arterial CO2 [26]. The UK-based REST trial, the first randomised controlled trial in this area, compared standard tidal volume ventilation (6-8 mL/kg) to ultra-low tidal volume ventilation (3-4 mL/kg) using ECCO2R. While the trial achieved significant separation between groups in tidal volume and maintained comparable PaCO2 and pH, it showed no difference in 90-day mortality. The ECCO2R group experienced significantly higher complication rates, including bleeding with intracranial haemorrhage, leading to early trial termination [32].
For AECOPD, non-invasive ventilation (NIV) remains the gold standard. However, ECCO2R has been explored as an option for patients who fail or cannot tolerate NIV. Trials have shown faster resolution of respiratory acidosis and work of breathing with ECCO2R, though they were not powered to assess mortality. Other studies have evaluated ECCO2R for preventing intubation or enabling early extubation, finding no differences in ventilator-free days or mortality, with higher mortality in the NIV group when ECCO2R was added[33].
Despite mixed results, interest in ECCO2R persists, particularly regarding the optimal blood flow rate for clinical benefit. Evidence suggests that higher-flow devices (500–1,000 mL/min) provide superior CO2 clearance compared to lower-flow systems (<500 mL/min)[34,35]. All the RCTs to date have used devices with a maximum blood flow below 500mL/minute. Future trials should investigate the potential of higher blood flow ECCO2R devices to improve clinical outcomes.
3. Key Areas of Future Research
The future of ECCO2R remains challenging due to the clinical outcomes observed so far and the significant complications associated with current devices. Priority should be given to addressing technical issues such as haemolysis, thrombosis, and bleeding. Research must also define optimal parameters for blood flow, sweep gas efficiency, and monitoring while developing methods to compare different devices for practical application. Experimental studies using appropriate circuits and biological models are essential to translate findings into clinical practice. Ultimately, well-designed clinical trials addressing patient-centred outcomes will be crucial in determining this technology's role in critically ill patients.
3.1 Hemolysis
Hemolysis is a significant complication of extracorporeal support and is independently associated with mortality [36,36,37]. A key contributor to hemolysis is shear stress caused by blood circulating through artificial circuits. This shear rate and stress arise from artificial surfaces and continuous flow patterns [38]. Factors such as catheter size and type, flow rates, pump design (roller or centrifugal), lung membrane characteristics, anticoagulation methods (coating and systemic), and ECCO2R settings all influence haemolysis rates and system performance.
Haemolysis is best detected by measuring plasma free Hb (PFHb), the most reliable marker of RBC injury and breakdown [39,40]. Evidence suggests that haemolysis increases non-linearly with reducing blood flows, as prolonged exposure to artificial surfaces amplifies the effective stress on blood components [41,34].
When the haemoglobin scavenging capacity of haptoglobin is exceeded, free haemoglobin dimers circulate in the bloodstream, releasing free heme [42]. This free haemoglobin depletes nitric oxide (NO) by converting it into nitrate, impairing NO’s regulatory role in vascular smooth muscle tone. The resulting NO depletion leads to potent vasoconstriction and increased systemic and pulmonary vascular resistance [43,44,45]. Additionally, NO depletion disrupts platelet and endothelial function, enhancing platelet aggregation and thrombus formation mediated by the von Willebrand factor [46,47,48].
Free haemoglobin initiates a cycle of inflammation that culminates in a procoagulant state and thrombus formation. This process exacerbates haemolysis, depletes clotting factors, and leads to thrombocytopenia and impaired platelet function [49], which may result in an acquired von Willebrand syndrome [50,51].
To address this frequent complication, we require improved devices and a greater clinical understanding of how device usage impacts haemolysis.
3.2 Thrombosis and Bleeding
Anticoagulation is a critical concern in extracorporeal circulation technology, given that anticoagulation and the impact of shear stress on coagulation proteins may lead to increased bleeding risk [21,32,52,53,54,55,56]. On the other hand, thrombosis is responsible for locally impaired flow conditions in cannulas, pumps and membrane lungs, which lead to mechanical stress and hemolysis. The coagulation cascade is activated when whole blood comes into contact with an artificial surface, exacerbated by slow blood flow. Relative slow blood flow occurs in low-shear circuit parts, such as tubing connectors, with increased thrombin generation[57,58] and minimal clot initiators required to trigger clot formation [59]. The artificial membrane oxygenator and the centrifugal head pump are the two main circuit components affected by higher mechanical stress and risk of thrombus formation. Centrifugal head pump thrombosis is usually associated with acute and severe hemolysis [37]. Membrane thrombosis reduces gas exchange impacting device efficiency.
Figure 1.
Example of different blood washouts depending on high and low blood flows in membrane oxygenator with impact on anticoagulation requirements to prevent membrane clotting. Pictures kindly provided by F. Hesselmann and R. Borchardt, Aachen, Germany.
Figure 1.
Example of different blood washouts depending on high and low blood flows in membrane oxygenator with impact on anticoagulation requirements to prevent membrane clotting. Pictures kindly provided by F. Hesselmann and R. Borchardt, Aachen, Germany.
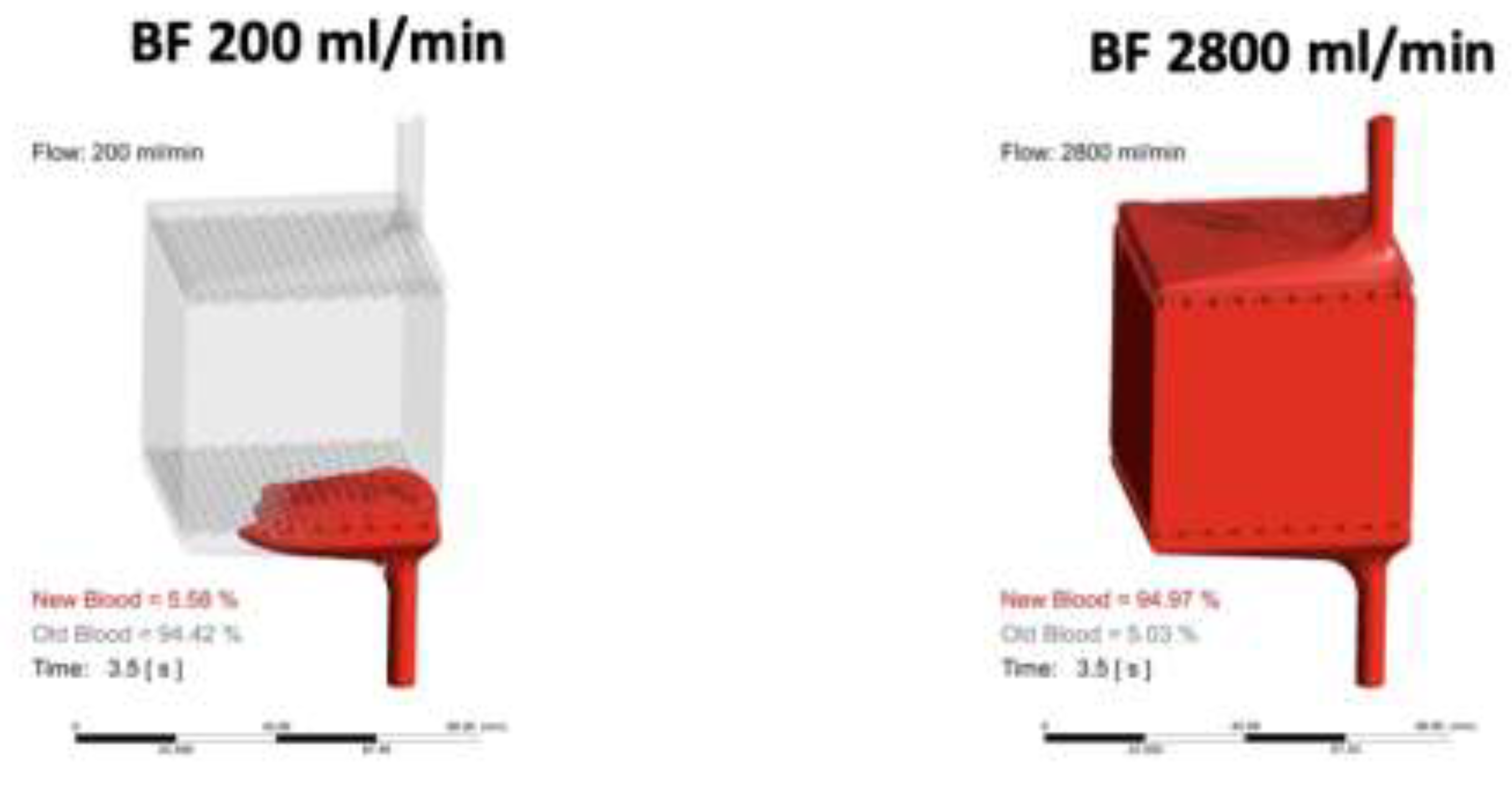
Contrary to expectations, low blood flow rates (1–1.5 L/min) are associated with a significantly higher risk of haemolysis (3.2 to 6.6 times greater Haemolysis Index) compared to higher blood flow (4 L/min). In low-flow systems (<1.5 L/min), citrate anticoagulation has been shown to outperform heparin by causing less haemolysis and platelet loss [60]. Citrate better preserves red blood cell density, membrane stability, and deformability, reducing haemolysis over three days of storage [61]. In animal studies, Cardenas et al. demonstrated no thrombus formation and hemolysis at different low flow levels (500ml/min, 800ml/min, 1000ml/min) using citrate anticoagulation in 24 hours. Although higher blood flows may reduce calcium chelation efficiency due to elevated ionised calcium levels, this did not correlate with thrombus formation. When comparing citrate to heparin anticoagulation at electronic microscopy, analysis of membrane oxygenator fibres revealed cellular and fibrin adhesion on heparin anticoagulation even after 6 hours of anticoagulation [62]. Despite these theoretical advantages, heparin remains the most commonly used anticoagulant in clinical ECCO2R due to concerns about citrate toxicity.
A significant complication of citrate anticoagulation in animal studies was progressive hypocalcaemia, even with calcium supplementation, due to the absence of a hemofilter to remove excess citrate. This increased systemic citrate load, heightening the risk of citrate toxicity [62,63,64]. Further research is needed to enhance the safety profile of citrate anticoagulation for clinical ECCO2R.
An emerging alternative to sodium citrate is citric acid anticoagulation, which provides a triple effect: calcium chelation, platelet inhibition, and a regional anticoagulant effect from an acidic environment [70]. Citric acid has also enhanced CO2 removal by blood acidification at the artificial membrane [65]. However, hepatic clearance of citrate in humans is limited [66], which reduces the maximum blood flow of ECCO2R to 150ml/min, which can be offset by an increase in CO2 removal efficiency driven by the acidification of the blood [67,68,69,70].
Other alternatives to heparin, such as nafamostat mesylate, bivalirudin, and argatroban, are being considered, especially for patients at high risk of bleeding or heparin-induced thrombocytopenia (HITT). These alternatives offer advantages regarding bleeding risks and drug monitoring but are limited by high costs and short half-lives.
4. CO2 Removal Rate Performance
4.1 Cannula
ECCO2R typically employs smaller cannulas (13–14 Fr) than the larger cannulas used in higher-flow ECMO. Venous access is generally achieved via the right internal jugular or femoral veins, with vessel puncture performed under ultrasound guidance. While the smaller cannulas offer advantages such as reduced invasiveness, their use presents several challenges that can impact both efficacy and patient safety. A key issue is maintaining adequate blood flow through the smaller cannulas. A smaller diameter cannula with higher flow rates increases shear stress, which may reduce CO2 removal efficiency due to insufficient flow, ultimately limiting the therapy’s effectiveness. Multiple single-lumen catheters can replace double-lumen catheters. This involves using separate access points in the jugular and femoral veins to achieve uninterrupted blood flow of approximately 450 mL/min with minimal recirculation [71]. Another relevant factor for ECCO2R efficiency is the minimisation of blood recirculation related to catheters. Catheter recirculation was related to catheter type and brand, site of placement, catheter length, time on dialysis, and time on the current catheter and was measured via ultrasound dilution technique [72]. Catheters placed in the internal jugular or subclavian veins, with the tip near the right atrium, minimise recirculation, making them more effective for ECCO2R. In contrast, femoral catheters have higher recirculation rates and are less suitable for this therapy.
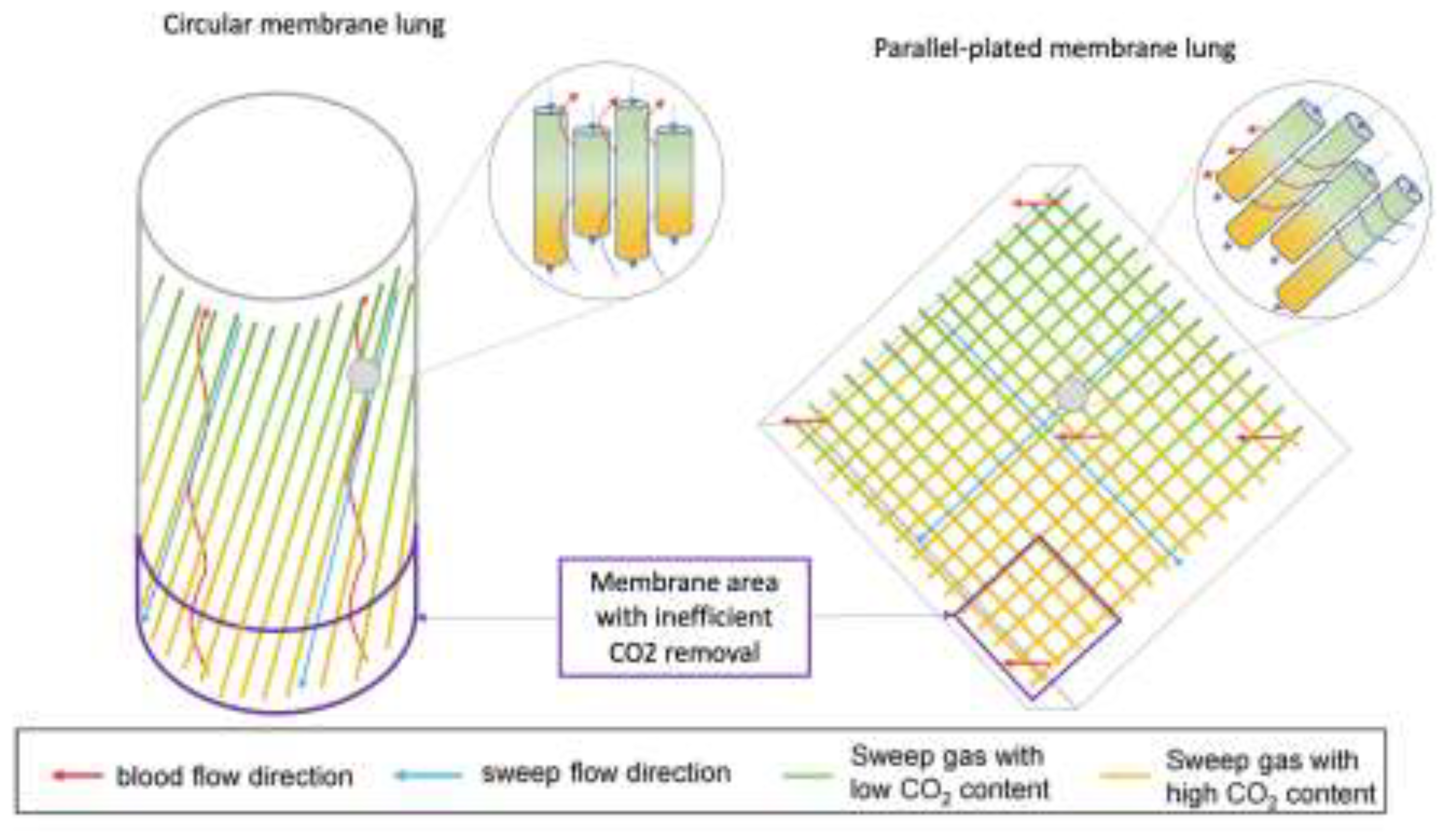
Figure 2.
Fiber arrangement in parallel plate and circular Membrane Lungs (ML).In the circular ML, blood flow is nearly antiparallel to the gas fibres and flow. At the lower part of the ML, where blood enters, it encounters sweep gas with the highest CO2 concentration. Since CO2 removal depends on the diffusion gradient between the gas and blood—small in this region—CO2 clearance is inefficient here. In the parallel-plate MLs, blood flows perpendicularly to the gas fibres. Similarly, at the lower part of the ML, where blood interacts with gas containing the highest CO2 levels, CO2 removal is less effective. With permission from Schwärzel et al. [73].
Figure 2.
Fiber arrangement in parallel plate and circular Membrane Lungs (ML).In the circular ML, blood flow is nearly antiparallel to the gas fibres and flow. At the lower part of the ML, where blood enters, it encounters sweep gas with the highest CO2 concentration. Since CO2 removal depends on the diffusion gradient between the gas and blood—small in this region—CO2 clearance is inefficient here. In the parallel-plate MLs, blood flows perpendicularly to the gas fibres. Similarly, at the lower part of the ML, where blood interacts with gas containing the highest CO2 levels, CO2 removal is less effective. With permission from Schwärzel et al. [73].
4.2 Pumps, Membranes and Circuits
4.2.1. Pumps
Conventionally, ECCO2R uses roller, centrifugal or diagonal, electric or electromagnetic pumps. The roller pumps used in ECCO2R systems were developed for renal replacement therapy (RRT) [74,75,76] or centrifugal pumps used for high-flow extracorporeal membrane oxygenation (ECMO) devices, with few systems explicitly designed for ECCO2R [14,29,77]. However, RRT devices driven by roller pumps are limited in blood flow rates (usually up to 500 mL/min), limiting the CO2 removal performance. Standard ECMO centrifugal pumps running below 2L/min cause increasing shear stress, leading to haemolysis [41].
Potential new pump technologies are on the horizon, for example, an innovative membrane and pump integrated to operate at very low flow (250ml/min) using six rotating impellers inside a cylindrical membrane configuration with a total surface area of 0.42m2. Blood moves from inside to outside through membrane fibres, allowing up to 75ml/min CO2 removal rate with a hemolysis level comparable to standard CO2 removal devices [78].
4.2.2. Membranes
Three major factors determine the amount of gas crossing membranes: the diffusion gradient, the membrane-blood contact time, and the characteristics of the membrane diffusion. The CO2 diffusion gradient is determined by the CO2 content of the blood and the air passing through the membrane lung, as well as the speed of the airflow. Membrane-blood contact time is determined by membrane geometry. Modern membrane lungs achieve adequate gas exchange with 1 to 3 m2 surface areas (Table 1).

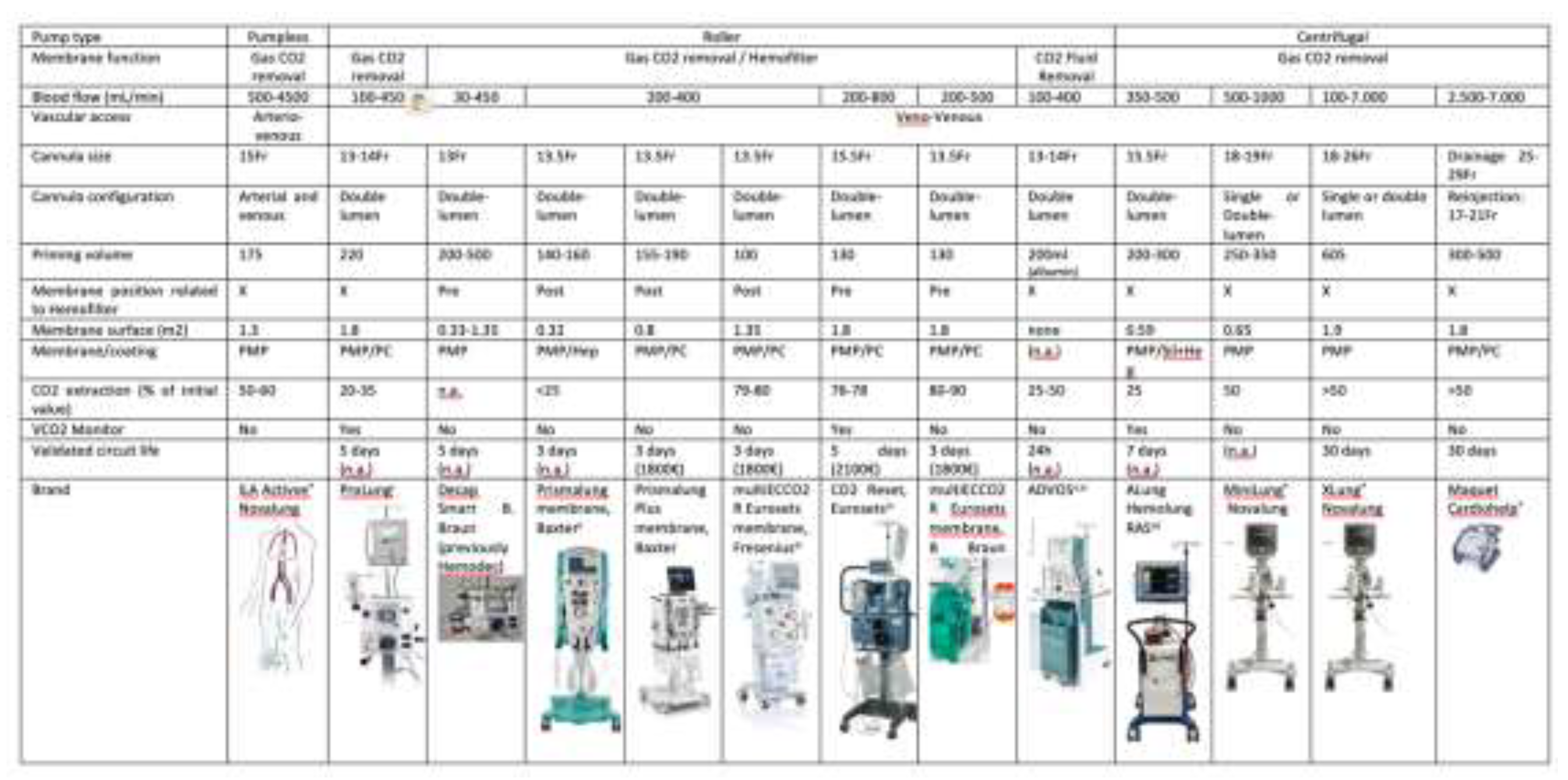
Table 1.
Comparison of available ECCO2R in the market based on the pump (pumpless, roller and centrifugal) and membrane function (gas and/or fluid CO2 removal). The table summarises the key characteristics of roller and centrifugal pumps, focusing on parameters such as blood flow limits, priming volume, membrane surface area, membrane material, CO2 extraction efficiency, VCO2
monitor and circuit life. [19,27,79–83]
Table 1.
Comparison of available ECCO2R in the market based on the pump (pumpless, roller and centrifugal) and membrane function (gas and/or fluid CO2 removal). The table summarises the key characteristics of roller and centrifugal pumps, focusing on parameters such as blood flow limits, priming volume, membrane surface area, membrane material, CO2 extraction efficiency, VCO2
monitor and circuit life. [19,27,79–83]
4.2.2.1 Materials
Early fibres were constructed with microporous polypropylene. Micropores create microscopic blood-gas interfaces, allowing efficient gas exchange and causing plasma leaks. Recently, non-microporous poly-4-methyl-1-pentene (PMP) has been used; it provides superior gas exchange, better biocompatibility, and is less susceptible to plasma leak [84,85,86]. The gas exchange has been improved by arranging fibres into a complex mat and running blood on the outside[87]. This arrangement allows perpendicular blood flow to the fibres, enhancing mass transfer by reducing the diffusion path length compared to parallel flow.
4.2.2.2 Novel Surfaces for ECCO2R
New materials and surface coatings are designed to reduce the inflammatory and coagulation responses triggered by artificial surfaces. Bioactive coatings, such as heparin-based and nitric oxide (NO) releasing materials, mimic natural endothelium and prevent blood clotting. Membranes may include a nitric oxide (NO)-eluting NO-eluting ECCO2R system, tubing with NO-catalyzing surface coating or NO gas (80ppm) delivered into the membrane that inhibits platelet activation and aggregation to minimise thrombosis during extracorporeal CO2 removal (ECCO2R) [88].
Endothelialisation of surfaces is an emerging approach, with efforts to create artificial materials that mimic the human endothelial layer, potentially reducing the need for systemic anticoagulation and preventing thrombosis. Further innovations focus on developing fully biocompatible materials to avoid bleeding and clotting complications without compromising oxygenation efficiency, raising the possibility for long-term respiratory support in chronic lung failure[89]. These include bioactive hollow fibre membranes (HFMs) coated with carbonic anhydrase (CA). CA immobilisation on HFMs increases the conversion of bicarbonate into CO₂, improving removal efficiency by creating a steeper diffusion gradient at the membrane surface. The CA-coated membranes also improved hemocompatibility, reducing platelet adhesion by 95% [90]. Acidic sweep gas containing sulfur dioxide (SO₂), in combination with carbonic anhydrase (CA) coated hollow fibre membranes (HFMs), can significantly enhance CO₂ removal from blood. This technique offers the potential for developing more efficient ECCO₂R devices. The findings could lead to smaller, less invasive respiratory support systems for patients with acute respiratory failure. [91].
Innovative therapies, such as intravascular gas exchange devices, hold promise for lung support in acute respiratory conditions both in and outside the hospital. They also have long-term potential for managing chronic lung diseases while preserving patient mobility through continuous ECCO2R. Despite their appeal, this technology has yet to reach clinical use. Only one device, the IVOX catheter, has advanced to human clinical trials but has yet to receive FDA approval. Technical challenges have hindered their progress, including optimising gas exchange within the vascular space and ensuring safety. Advancements in design may eventually offer a less invasive alternative to ECMO for managing acute respiratory failure [92].
4.2.2.3 Measuring device VCO2 to assess membrane performance
When comparing devices and evaluating efficiency, it is crucial to understand how CO2 is measured to estimate carbon dioxide transfer across the artificial membrane. This can be done by assessing trans-membrane CO2 content differences using whole blood CO2 content using the Douglas equation [93] or measuring the partial pressure of CO2 in the effluent gas using infrared CO2 sensors.[94] In both approaches, normalising to a standardised inlet PCO2 is essential to define the device’s operating range and enable meaningful efficiency comparisons.
One of the concerns with effluent gas VCO2 measurement is the need for more independent validation of VCO2. However, this has been done with one device, little is known about the accuracy of the devices in which VCO2 is measured with an infrared sensor measurement (Table 1)[95,96]. To improve comparative evaluations, the VCO2 of each membrane and device should be standardised to inlet CO2 and blood flow for consistent comparison and performance assessment. Manufacturers should ideally report their device’s index as VCO2 per membrane surface area (e.g., ml/min/m²).[78]
4.3. Combined CO2 Removal (“Lung Dialysis”) with renal support
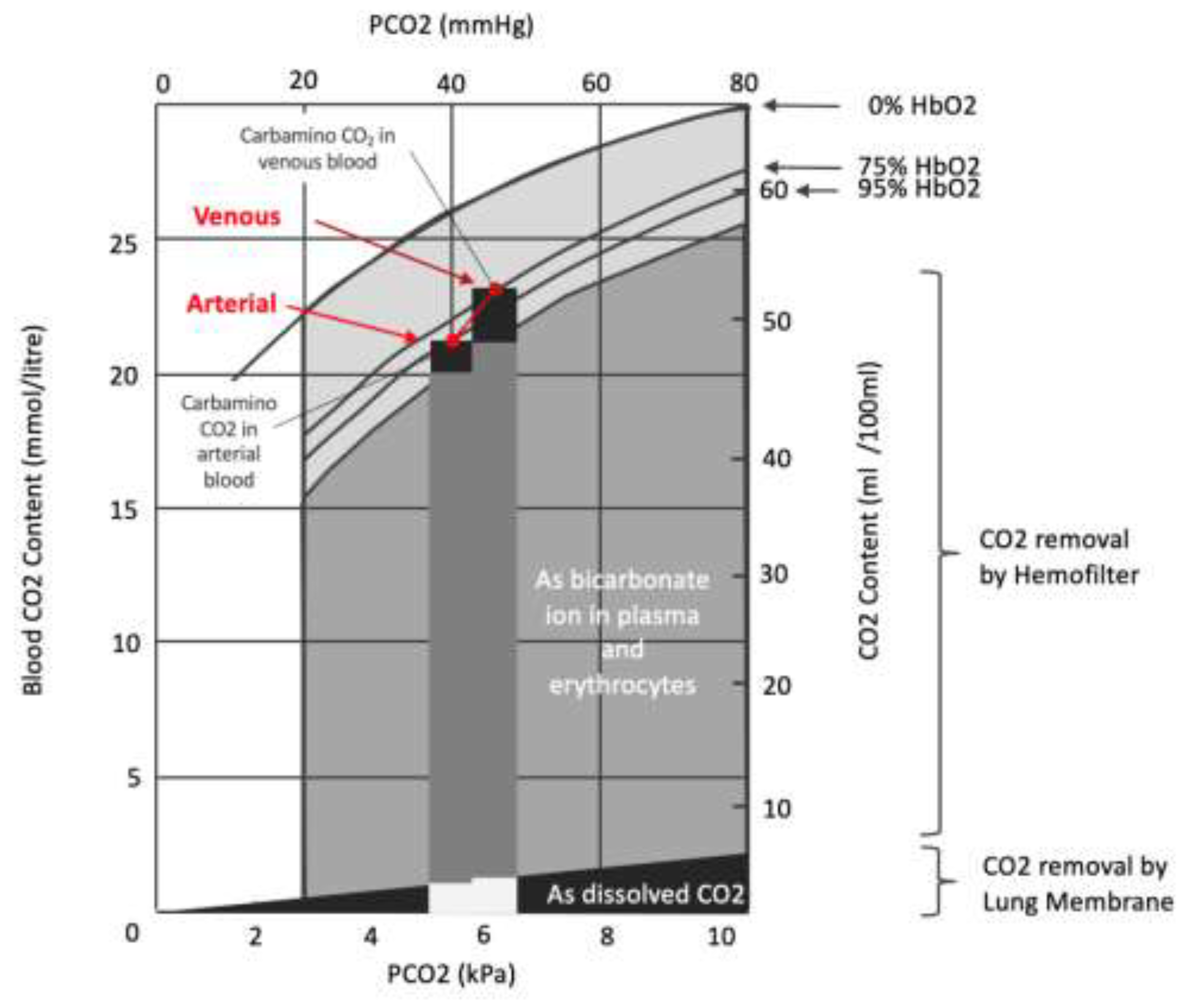
Other strategies for enhancing CO₂ removal from the blood focus on methods targeting bicarbonate, as around 90% of CO₂ in the blood is transported as bicarbonate (Figure 2). The gas exchange membrane can be isolated or combined with a “renal” membrane (hemofilter) to achieve this. Research has shown that combining extracorporeal CO₂ removal (ECCO₂R) with CRRT effectively reduces arterial CO₂ (PaCO₂), improves pH, and stabilises hemodynamics in patients with acute respiratory distress syndrome (ARDS) and renal failure. Despite these benefits, mortality rates in critically ill patients remain high, especially in the most severe cases [97]. Integrating a hollow-fibre gas exchanger into CRRT platforms is relatively simple, and the gas exchange membrane can be placed before or after the haemofilter. Some data suggest that the CO2 removal rate tends to be higher when the membrane is before the hemofilter. However, the clinical impact of this remains unknown [74]. An alternative strategy is integrating gas and fluid fibres in parallel using a shared circuit [98].
Figure 2.
The proportion of carbamino form contribution from arterial CO2 content to venous CO2 content is significantly higher than the other forms of CO2 content due to the Haldane effect (increasing Hemoglobin affinity to CO2 in lower oxygen concentration). The CO2 removal of the gaseous phase of CO2 represents only a small fraction of total CO2 content. The bicarbonate removal using zero bicarbonate dialytic solution through hemofilter could contribute to significantly higher CO2 removal of total CO2 content, however, the blood buffer must be replaced by other natural buffers to maintain the acid-base equilibrium.
Figure 2.
The proportion of carbamino form contribution from arterial CO2 content to venous CO2 content is significantly higher than the other forms of CO2 content due to the Haldane effect (increasing Hemoglobin affinity to CO2 in lower oxygen concentration). The CO2 removal of the gaseous phase of CO2 represents only a small fraction of total CO2 content. The bicarbonate removal using zero bicarbonate dialytic solution through hemofilter could contribute to significantly higher CO2 removal of total CO2 content, however, the blood buffer must be replaced by other natural buffers to maintain the acid-base equilibrium.
The optimal dialysis solution to use in combined devices remains to be discovered. Commonly available bicarbonate-based solutions increase total blood CO2 content, which is problematic when high dialysis rates are required for solute clearance. Alternative solutions allow the simultaneous removal of H⁺ and bicarbonate, maintaining acid-base balance whilst allowing CO₂ removal rates of up to 160 mL/min [99]. Several approaches seek to manipulate regional pH to alter bicarbonate or CO2 clearance. Alkalinisation with bicarbonate free solutions, enhance bicarbonate removal are being investigated in animal models [100]. However, these methods may prove impractical for clinical use due to acid-base derangements, hemolysis, cardiac arrhythmias, and depletion of micronutrients, even though several approaches to replace bicarbonate have been attempted [100,101]. Respiratory electrodialysis, which increases CO₂ partial pressure in the blood through regional acidification, has been shown to remove approximately 50% of the total CO₂ metabolic production, offering a promising strategy for efficient CO₂ removal. These varied strategies illustrate ongoing efforts to develop more effective means of extracorporeal CO₂ removal, particularly for critically ill patients with multiple organ failure [102].
5. Conclusions
The future of ECCO2R holds significant promise. However, two actions need to occur in parallel. First, the technology needs to be improved to reduce the impact on blood and coagulation whilst simultaneously increasing the efficiency of CO2 removal. Second, the population who may benefit and the timing of ECCO2R need to be better defined. ECCO2R is being evaluated for patients with ARDS and COPD, but other groups, including patients bridging to transplant, may benefit.
Advances in membrane technology and gas exchange efficiency could further reduce the size and blood flow requirements of ECCO2R systems, enhancing their safety and accessibility. These improvements could lead to the development of smaller, catheter-based systems that are less invasive and more practical for broader clinical use [100]. Developing new anticoagulation strategies for ECCO2R is crucial, given the delicate balance between preventing clot formation within the circuit and minimising the risk of bleeding complications in patients. Artificial intelligence (AI) and machine learning could act similarly to the respiratory centres, allowing automated changes in CO2 clearance based on changes in blood CO2 and pH [103]. Ultimately, miniaturisation, development of closed feedback loops, reduced impact on blood/coagulation, and efficiency improvements will benefit the ICU population and may also allow the development of wearable devices that act as destination or prolonged bridging therapies [104].
Clinical trials are ongoing and will determine ECCO2R 's efficacy, safety, and best practices. Overall, ECCO2R 's future looks bright, with ongoing innovation and research likely to expand its clinical applications and affect critical care practice.
Author Contributions
All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ohtake, S.; Kawashima, Y.; Hirose, H.; Matsuda, H.; Nakano, S.; Kaku, K.; Okuda, A. Experimental evaluation of pumpless arteriovenous ECMO with polypropylene hollow fiber membrane oxygenator for partial respiratory support. . 1983, 29, 237–41. [Google Scholar] [PubMed]
- Bein, T.; Weber, F.; Philipp, A.; Prasser, C.; Pfeifer, M.; Schmid, F.-X.; Butz, B.; Birnbaum, D.; Taeger, K.; Schlitt, H.J. A new pumpless extracorporeal interventional lung assist in critical hypoxemia/hypercapnia*. Crit. Care Med. 2006, 34, 1372–1377. [Google Scholar] [CrossRef] [PubMed]
- Bein, T.; Zimmermann, M.; Hergeth, K.; Ramming, M.; Rupprecht, L.; Schlitt, H.J.; Slutsky, A.S. Pumpless extracorporeal removal of carbon dioxide combined with ventilation using low tidal volume and high positive end-expiratory pressure in a patient with severe acute respiratory distress syndrome. Anaesthesia 2009, 64, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Pesenti, A.; Mascheroni, D.; Marcolin, R.; Fumagalli, R.; Rossi, F.; Lapichino, G.; Romagnoli, G.; Uziel, L.; Agostoni, A.; et al. Low-frequency positive-pressure ventilation with extracorporeal CO2 removal in severe acute respiratory failure. JAMA 1986, 256, 881–886. [Google Scholar] [CrossRef]
- Zimmermann, M.; Bein, T.; Arlt, M.; Philipp, A.; Rupprecht, L.; Mueller, T.; Lubnow, M.; Graf, B.M.; Schlitt, H.J. Pumpless extracorporeal interventional lung assist in patients with acute respiratory distress syndrome: a prospective pilot study. Crit. Care 2009, 13, R10–R10. [Google Scholar] [CrossRef]
- Zimmermann, M.; Bein, T.; Philipp, A.; Ittner, K.; Foltan, M.; Drescher, J.; Weber, F.; Schmid, F.-X. Interhospital transportation of patients with severe lung failure on pumpless extracorporeal lung assist. Br. J. Anaesth. 2006, 96, 63–66. [Google Scholar] [CrossRef]
- Fischer, S.; Hoeper, M.M.; Bein, T.; Simon, A.R.; Gottlieb, J.; Wisser, W.; Frey, L.; Van Raemdonck, D.; Welte, T.; Haverich, A.; et al. Interventional Lung Assist: A New Concept of Protective Ventilation in Bridge to Lung Transplantation. Asaio J. 2008, 54, 3–10. [Google Scholar] [CrossRef]
- Elliot, S.C.; Paramasivam, K.; Oram, J.; Bodenham, A.R.; Howell, S.J.; Mallick, A. Pumpless extracorporeal carbon dioxide removal for life-threatening asthma. Crit. Care Med. 2007, 35, 945–948. [Google Scholar] [CrossRef]
- Mallick, A.; Elliot, S.; McKinlay, J.; Bodenham, A. Extracorporeal carbon dioxide removal using the Novalung® in a patient with intracranial bleeding. Anaesthesia 2006, 62, 72–74. [Google Scholar] [CrossRef]
- Zwischenberger, J.B.; Alpard, S.K. Artificial lungs: a new inspiration. Perfusion 2002, 17, 253–268. [Google Scholar] [CrossRef]
- Zwischenberger, J.B.; Alpard, S.K.; Tao, W.; Deyo, D.J.; Bidani, A. Percutaneous extracorporeal arteriovenous carbon dioxide removal improves survival in respiratory distress syndrome: A prospective randomized outcomes study in adult sheep. J. Thorac. Cardiovasc. Surg. 2001, 121, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Zwischenberger, J.B.; Savage, C.; Witt, S.A.; Alpard, S.K.; Harper, D.D.; Deyo, D.J. Arterio-venous CO2 removal (AVCO2R) perioperative management: rapid recovery and enhanced survival. J. Investig. Surg. 2002, 15, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Terragni, P.; Maiolo, G.; Ranieri, V.M. Role and potentials of low-flow CO2 removal system in mechanical ventilation. Curr. Opin. Crit. Care 2012, 18, 93–98. [Google Scholar] [CrossRef]
- Batchinsky, A.I.; Jordan, B.S.R.; Regn, D.; Necsoiu, C.; Federspiel, W.J.; Morris, M.J.; Cancio, L.C. Respiratory dialysis: Reduction in dependence on mechanical ventilation by venovenous extracorporeal CO2 removal*. Crit. Care Med. 2011, 39, 1382–1387. [Google Scholar] [CrossRef]
- Ruberto, F.; Pugliese, F.; D'Alio, A.; Perrella, S.; D'Auria, B.; Ianni, S.; Anile, M.; Venuta, F.; Coloni, G.; Pietropaoli, P. Extracorporeal Removal CO2 Using a Venovenous, Low-Flow System (Decapsmart) in a Lung Transplanted Patient: A Case Report. Transplant. Proc. 2009, 41, 1412–1414. [Google Scholar] [CrossRef] [PubMed]
- Cardenas, V.J.; Lynch, J.E.; Ates, R.; Miller, L.; Zwischenberger, J.B. Venovenous Carbon Dioxide Removal in Chronic Obstructive Pulmonary Disease. Asaio J. 2009, 55, 420–422. [Google Scholar] [CrossRef]
- Dorrington, K.L.; McRae, K.M.; Gardaz, J.-. .-P.; Dunnill, M.S.; Sykes, M.K.; Wilkinson, A.R. A randomized comparison of total extracorporeal CO2 removal with conventional mechanical ventilation in experimental hyaline membrane disease. Intensiv. Care Med. 1989, 15, 184–191. [Google Scholar] [CrossRef]
- Livigni, S.; Maio, M.; Ferretti, E.; Longobardo, A.; Potenza, R.; Rivalta, L.; Selvaggi, P.; Vergano, M.; Bertolini, G. Efficacy and safety of a low-flow veno-venous carbon dioxide removal device: results of an experimental study in adult sheep. Crit. Care 2006, 10, R151–R151. [Google Scholar] [CrossRef]
- Wearden, P.D.; Federspiel, W.J.; Morley, S.W.; Rosenberg, M.; Bieniek, P.D.; Lund, L.W.; Ochs, B.D. Respiratory dialysis with an active-mixing extracorporeal carbon dioxide removal system in a chronic sheep study. Intensiv. Care Med. 2012, 38, 1705–1711. [Google Scholar] [CrossRef]
- Garcia, J.P.; Kon, Z.N.; Evans, C.; Wu, Z.; Iacono, A.T.; McCormick, B.; Griffith, B.P. Ambulatory veno-venous extracorporeal membrane oxygenation: Innovation and pitfalls. J. Thorac. Cardiovasc. Surg. 2011, 142, 755–761. [Google Scholar] [CrossRef]
- Kluge, S.; Braune, S.A.; Engel, M.; Nierhaus, A.; Frings, D.; Ebelt, H.; Uhrig, A.; Metschke, M.; Wegscheider, K.; Suttorp, N.; et al. Avoiding invasive mechanical ventilation by extracorporeal carbon dioxide removal in patients failing noninvasive ventilation. Intensiv. Care Med. 2012, 38, 1632–1639. [Google Scholar] [CrossRef] [PubMed]
- Extracorporeal lung support technologies - bridge to recovery and bridge to lung transplantation in adult patients: an evidence-based analysis. Ont Health Technol Assess Ser. 2010;10(5):1-47.
- Engel M, Albrecht H. Use of Extracorporeal CO2 Removal to Avoid Invasive Mechanical Ventilation in Hypercapnic Coma and Failure of Noninvasive Ventilation. J Pulm Respir Med. 2016;6(3). [CrossRef]
- Hilty, M.P.; Riva, T.; Cottini, S.R.; Kleinert, E.-M.; Maggiorini, A.; Maggiorini, M. Low flow veno-venous extracorporeal CO2 removal for acute hypercapnic respiratory failure. Minerva Anestesiol. 2017, 83, 812–823. [Google Scholar] [CrossRef] [PubMed]
- Braune, S.; Sieweke, A.; Brettner, F.; Staudinger, T.; Joannidis, M.; Verbrugge, S.; Frings, D.; Nierhaus, A.; Wegscheider, K.; Kluge, S. The feasibility and safety of extracorporeal carbon dioxide removal to avoid intubation in patients with COPD unresponsive to noninvasive ventilation for acute hypercapnic respiratory failure (ECLAIR study): multicentre case–control study. Intensiv. Care Med. 2016, 42, 1437–1444. [Google Scholar] [CrossRef]
- Combes, A.; Fanelli, V.; Pham, T.; Ranieri, V.M. European Society of Intensive Care Medicine Trials Group and the “Strategy of Ultra-Protective lung ventilation with Extracorporeal CO2 Removal for New-Onset moderate to severe ARDS” (SUPERNOVA) investigators Feasibility and safety of extracorporeal CO2 removal to enhance protective ventilation in acute respiratory distress syndrome: The SUPERNOVA study. Intensiv. Care Med. 2019, 45, 592–600. [Google Scholar] [CrossRef]
- Husain-Syed, F.; Birk, H.-W.; Wilhelm, J.; Ronco, C.; Ranieri, V.M.; Karle, B.; Kuhnert, S.; Tello, K.; Hecker, M.; Morty, R.E.; et al. Extracorporeal Carbon Dioxide Removal Using a Renal Replacement Therapy Platform to Enhance Lung-Protective Ventilation in Hypercapnic Patients With Coronavirus Disease 2019-Associated Acute Respiratory Distress Syndrome. Front. Med. 2020, 7, 598379. [Google Scholar] [CrossRef]
- Consales, G.; Zamidei, L.; Turani, F.; Atzeni, D.; Isoni, P.; Boscolo, G.; Saggioro, D.; Resta, M.V.; Ronco, C. Combined Renal-Pulmonary Extracorporeal Support with Low Blood Flow Techniques: A Retrospective Observational Study (CICERO Study). Blood Purif. 2021, 51, 299–308. [Google Scholar] [CrossRef]
- Burki, N.K.; Mani, R.K.; Herth, F.J.; Schmidt, W.; Teschler, H.; Bonin, F.; Becker, H.; Randerath, W.J.; Stieglitz, S.; Hagmeyer, L.; et al. A Novel Extracorporeal CO 2 Removal System. Chest 2013, 143, 678–686. [Google Scholar] [CrossRef]
- Spinelli, E.; Crotti, S.; Zacchetti, L.; Bottino, N.; Berto, V.; Russo, R.; Chierichetti, M.; Protti, A.; Gattinoni, L. Effect of extracorporeal CO2 removal on respiratory rate in spontaneously breathing patients with chronic obstructive pulmonary disease exacerbation. Crit. Care 2013, 17, P128–P128. [Google Scholar] [CrossRef]
- Diehl, J.-L.; Piquilloud, L.; Vimpere, D.; Aissaoui, N.; Guerot, E.; Augy, J.L.; Pierrot, M.; Hourton, D.; Arnoux, A.; Richard, C.; et al. Physiological effects of adding ECCO2R to invasive mechanical ventilation for COPD exacerbations. Ann. Intensiv. Care 2020, 10, 1–8. [Google Scholar] [CrossRef]
- McNamee, J.J.; Gillies, M.A.; Barrett, N.A.; Perkins, G.D.; Tunnicliffe, W.; Young, D.; Bentley, A.; Harrison, D.A.; Brodie, D.; Boyle, A.J.; et al. Effect of Lower Tidal Volume Ventilation Facilitated by Extracorporeal Carbon Dioxide Removal vs Standard Care Ventilation on 90-Day Mortality in Patients With Acute Hypoxemic Respiratory Failure. JAMA 2021, 326, 1013–1023. [Google Scholar] [CrossRef]
- Tonetti, T.; Pisani, L.; Cavalli, I.; Vega, M.L.; Maietti, E.; Filippini, C.; Nava, S.; Ranieri, V.M. Extracorporeal carbon dioxide removal for treatment of exacerbated chronic obstructive pulmonary disease (ORION): study protocol for a randomised controlled trial. Trials 2021, 22, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Karagiannidis, C.; Hesselmann, F.; Fan, E. Physiological and Technical Considerations of Extracorporeal CO2 Removal. Crit. Care 2019, 23, 75. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Strassmann, S.; Brodie, D.; Ritter, P.; Larsson, A.; Borchardt, R.; Windisch, W. Impact of membrane lung surface area and blood flow on extracorporeal CO2 removal during severe respiratory acidosis. Intensiv. Care Med. Exp. 2017, 5, 1–13. [Google Scholar] [CrossRef]
- Omar, H.R.; Mirsaeidi, M.; Socias, S.; Sprenker, C.; Caldeira, C.; Camporesi, E.M.; Mangar, D. Plasma Free Hemoglobin Is an Independent Predictor of Mortality among Patients on Extracorporeal Membrane Oxygenation Support. PLOS ONE 2015, 10, e0124034–e0124034. [Google Scholar] [CrossRef]
- Lehle, K.; Philipp, A.; Zeman, F.; Lunz, D.; Lubnow, M.; Wendel, H.-P.; Göbölös, L.; Schmid, C.; Müller, T. Technical-Induced Hemolysis in Patients with Respiratory Failure Supported with Veno-Venous ECMO – Prevalence and Risk Factors. PLOS ONE 2015, 10, e0143527. [Google Scholar] [CrossRef] [PubMed]
- Nascimbene, A.; Neelamegham, S.; Frazier, O.H.; Moake, J.L.; Dong, J.-F. Acquired von Willebrand syndrome associated with left ventricular assist device. Blood 2016, 127, 3133–3141. [Google Scholar] [CrossRef] [PubMed]
- Dufour, N.; Radjou, A.; Thuong, M. Hemolysis and Plasma Free Hemoglobin During Extracorporeal Membrane Oxygenation Support: From Clinical Implications to Laboratory Details. Asaio J. 2020, 66, 239–246. [Google Scholar] [CrossRef]
- Donadee, C.; Raat, N.J.; Kanias, T.; Tejero, J.; Lee, J.S.; Kelley, E.E.; Zhao, X.; Liu, C.; Reynolds, H.; Azarov, I.; et al. Nitric Oxide Scavenging by Red Blood Cell Microparticles and Cell-Free Hemoglobin as a Mechanism for the Red Cell Storage Lesion. Circulation 2011, 124, 465–476. [Google Scholar] [CrossRef]
- Gross-Hardt, S.; Hesselmann, F.; Arens, J.; Steinseifer, U.; Vercaemst, L.; Windisch, W.; Brodie, D.; Karagiannidis, C. Low-flow assessment of current ECMO/ECCO2R rotary blood pumps and the potential effect on hemocompatibility. Crit. Care 2019, 23, 1–9. [Google Scholar] [CrossRef]
- Langlois, M.R.; Delanghe, J.R. Biological and clinical significance of haptoglobin polymorphism in humans. Clin. Chem. 1996, 42, 1589–1600. [Google Scholar] [CrossRef]
- Rother, R.P.; Bell, L.; Hillmen, P.; Gladwin, M.T. The Clinical Sequelae of Intravascular Hemolysis and Extracellular Plasma Hemoglobin. JAMA 2005, 293, 1653–1662. [Google Scholar] [CrossRef] [PubMed]
- Minneci, P.C.; Deans, K.J.; Zhi, H.; Yuen, P.S.; Star, R.A.; Banks, S.M.; Schechter, A.N.; Natanson, C.; Gladwin, M.T.; Solomon, S.B. Hemolysis-associated endothelial dysfunction mediated by accelerated NO inactivation by decompartmentalized oxyhemoglobin. J. Clin. Investig. 2005, 115, 3409–3417. [Google Scholar] [CrossRef] [PubMed]
- Schaer, D.J.; Buehler, P.W.; Alayash, A.I.; Belcher, J.D.; Vercellotti, G.M. Hemolysis and free hemoglobin revisited: exploring hemoglobin and hemin scavengers as a novel class of therapeutic proteins. Blood 2013, 121, 1276–1284. [Google Scholar] [CrossRef] [PubMed]
- Da, Q.; Teruya, M.; Guchhait, P.; Teruya, J.; Olson, J.S.; Cruz, M.A. Free hemoglobin increases von Willebrand factor–mediated platelet adhesion in vitro: implications for circulatory devices. Blood 2015, 126, 2338–2341. [Google Scholar] [CrossRef]
- L'Acqua, C.; Hod, E. New perspectives on the thrombotic complications of haemolysis. Br. J. Haematol. 2014, 168, 175–185. [Google Scholar] [CrossRef]
- Wurzinger, L.; Blasberg, P.; Schmid-Schönbein, H. Towards a concept of thrombosis in accelerated flow: Rheology, fluid dynamics, and biochemistry. Biorheology 1985, 22, 437–450. [Google Scholar] [CrossRef]
- Oliver, W.C. Anticoagulation and Coagulation Management for ECMO. Semin. Cardiothorac. Vasc. Anesthesia 2009, 13, 154–175. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, M.V.; Pimenta, L.P.; von Bahr, V.; E Millar, J.; Obonyo, N.G.; Suen, J.; Pellegrino, V.; Fraser, J.F. Acquired von Willebrand syndrome in respiratory extracorporeal life support: a systematic review of the literature. . 2017, 19, 45–52. [Google Scholar]
- Kalbhenn, J.; Neuffer, N.; Zieger, B.; Schmutz, A. Is Extracorporeal CO2 Removal Really “Safe” and “Less” Invasive? Observation of Blood Injury and Coagulation Impairment during ECCO2R. Asaio J. 2017, 63, 666–671. [Google Scholar] [CrossRef]
- Burki, N.K.; Mani, R.K.; Herth, F.J.; Schmidt, W.; Teschler, H.; Bonin, F.; Becker, H.; Randerath, W.J.; Stieglitz, S.; Hagmeyer, L.; et al. A Novel Extracorporeal CO 2 Removal System. Chest 2013, 143, 678–686. [Google Scholar] [CrossRef]
- Del Sorbo, L.; Fan, E.; Nava, S.; Ranieri, V.M. ECCO2R in COPD exacerbation only for the right patients and with the right strategy. Intensiv. Care Med. 2016, 42, 1830–1831. [Google Scholar] [CrossRef]
- Braune, S.; Sieweke, A.; Brettner, F.; Staudinger, T.; Joannidis, M.; Verbrugge, S.; Frings, D.; Nierhaus, A.; Wegscheider, K.; Kluge, S. The feasibility and safety of extracorporeal carbon dioxide removal to avoid intubation in patients with COPD unresponsive to noninvasive ventilation for acute hypercapnic respiratory failure (ECLAIR study): multicentre case–control study. Intensiv. Care Med. 2016, 42, 1437–1444. [Google Scholar] [CrossRef]
- Bein, T.; Weber-Carstens, S.; Goldmann, A.; Müller, T.; Staudinger, T.; Brederlau, J.; Muellenbach, R.; Dembinski, R.; Graf, B.M.; Wewalka, M.; et al. Lower tidal volume strategy (≈3 ml/kg) combined with extracorporeal CO2 removal versus ‘conventional’ protective ventilation (6 ml/kg) in severe ARDS. Intensiv. Care Med. 2013, 39, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Fanelli, V.; Ranieri, M.V.; Mancebo, J.; Moerer, O.; Quintel, M.; Morley, S.; Moran, I.; Parrilla, F.; Costamagna, A.; Gaudiosi, M.; et al. Feasibility and safety of low-flow extracorporeal carbon dioxide removal to facilitate ultra-protective ventilation in patients with moderate acute respiratory distress syndrome. Crit. Care 2016, 20, 36. [Google Scholar] [CrossRef] [PubMed]
- Funakubo, A.; Taga, I.; McGillicuddy, J.W.; Fukui, Y.; Hirschl, R.B.; Bartlett, R.H. Flow vectorial analysis in an artificial implantable lung. . 2003, 49, 383–7. [Google Scholar] [PubMed]
- Meyer, A.D.; Rishmawi, A.R.; Kamucheka, R.; Lafleur, C.; Batchinsky, A.I.; Mackman, N.; Cap, A.P. Effect of blood flow on platelets, leukocytes, and extracellular vesicles in thrombosis of simulated neonatal extracorporeal circulation. J. Thromb. Haemost. 2019, 18, 399–410. [Google Scholar] [CrossRef]
- Okorie, U.M.; Denney, W.S.; Chatterjee, M.S.; Neeves, K.B.; Diamond, S.L. Determination of surface tissue factor thresholds that trigger coagulation at venous and arterial shear rates: amplification of 100 fM circulating tissue factor requires flow. Blood 2008, 111, 3507–3513. [Google Scholar] [CrossRef]
- Chan, C.H.H.; Ki, K.K.; Zhang, M.; Asnicar, C.; Cho, H.J.; Ainola, C.; Bouquet, M.; Heinsar, S.; Pauls, J.P.; Bassi, G.L.; et al. Extracorporeal Membrane Oxygenation-Induced Hemolysis: An In Vitro Study to Appraise Causative Factors. Membranes 2021, 11, 313. [Google Scholar] [CrossRef]
- Makhro, A.; Huisjes, R.; Verhagen, L.P.; Mañú-Pereira, M.d.M.; Llaudet-Planas, E.; Petkova-Kirova, P.; Wang, J.; Eichler, H.; Bogdanova, A.; van Wijk, R.; et al. Red Cell Properties after Different Modes of Blood Transportation. Front. Physiol. 2016, 7, 288. [Google Scholar] [CrossRef]
- Sharma, A.S.; Weerwind, P.W.; Bekers, O.; Wouters, E.M.; Maessen, J.G. Carbon dioxide dialysis in a swine model utilizing systemic and regional anticoagulation. Intensiv. Care Med. Exp. 2016, 4, 2. [Google Scholar] [CrossRef]
- Cardenas, V.J.J.; Miller, L.; Lynch, J.E.; Anderson, M.J.; Zwischenberger, J.B. Percutaneous Venovenous CO2 Removal With Regional Anticoagulation in an Ovine Model. Asaio J. 2006, 52, 467–470. [Google Scholar] [CrossRef] [PubMed]
- Morimont, P.; Habran, S.; Desaive, T.; Blaffart, F.; Lagny, M.; Amand, T.; Dauby, P.; Oury, C.; Lancellotti, P.; Hego, A.; et al. Extracorporeal CO2 removal and regional citrate anticoagulation in an experimental model of hypercapnic acidosis. Artif. Organs 2019, 43, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Scaravilli, V.; Di Girolamo, L.; Scotti, E.; Busana, M.; Biancolilli, O.; Leonardi, P.; Carlin, A.; Lonati, C.; Panigada, M.; Pesenti, A.; et al. Effects of sodium citrate, citric acid and lactic acid on human blood coagulation. Perfusion 2018, 33, 577–583. [Google Scholar] [CrossRef]
- Zheng, Y.; Xu, Z.; Zhu, Q.; Liu, J.; Qian, J.; You, H.; Gu, Y.; Hao, C.; Jiao, Z.; Ding, F. Citrate Pharmacokinetics in Critically Ill Patients with Acute Kidney Injury. PLOS ONE 2013, 8, e65992. [Google Scholar] [CrossRef]
- Zanella, A.; Patroniti, N.; Isgrò, S.; Albertini, M.; Costanzi, M.; Pirrone, F.; Scaravilli, V.; Vergnano, B.; Pesenti, A. Blood acidification enhances carbon dioxide removal of membrane lung: an experimental study. Intensiv. Care Med. 2009, 35, 1484–1487. [Google Scholar] [CrossRef]
- Zanella, A.; Mangili, P.; Giani, M.; Redaelli, S.; Scaravilli, V.; Castagna, L.; Sosio, S.; Pirrone, F.; Albertini, M.; Patroniti, N.; et al. Extracorporeal carbon dioxide removal through ventilation of acidified dialysate: An experimental study. J. Hear. Lung Transplant. 2014, 33, 536–541. [Google Scholar] [CrossRef]
- Zanella, A.; Giani, M.; Redaelli, S.; Mangili, P.; Scaravilli, V.; Ormas, V.; Costanzi, M.; Albertini, M.; Bellani, G.; Patroniti, N.; et al. Infusion of 2.5 meq/min of lactic acid minimally increases CO2 production compared to an isocaloric glucose infusion in healthy anesthetized, mechanically ventilated pigs. Crit. Care 2013, 17, R268–R268. [Google Scholar] [CrossRef] [PubMed]
- Scaravilli, V.; Kreyer, S.; Belenkiy, S.; Linden, K.; Zanella, A.; Li, Y.; Dubick, M.A.; Cancio, L.C.; Pesenti, A.; Batchinsky, A.I. Extracorporeal Carbon Dioxide Removal Enhanced by Lactic Acid Infusion in Spontaneously Breathing Conscious Sheep. Anesthesiology 2016, 124, 674–682. [Google Scholar] [CrossRef]
- De Bels, D.; Pierrakos, C.; Spapen, H.D.; Honore, P.M. A double catheter approach for extracorporeal CO2removal integrated within a continuous renal replacement circuit. J. Transl. Intern. Med. 2018, 6, 157–158. [Google Scholar] [CrossRef]
- Moossavi, S.; Vachharajani, T.J.; Jordan, J.; Russell, G.B.; Kaufman, T.; Moossavi, S. Retrospective Analysis of Catheter Recirculation in Prevalent Dialysis Patients. Semin. Dial. 2008, 21, 289–292. [Google Scholar] [CrossRef]
- Schwärzel, L.S.; Jungmann, A.M.; Schmoll, N.; Caspari, S.; Seiler, F.; Muellenbach, R.M.; Bewarder, M.; Dinh, Q.T.; Bals, R.; Lepper, P.M.; et al. Comparison of Circular and Parallel-Plated Membrane Lungs for Extracorporeal Carbon Dioxide Elimination. Membranes 2021, 11, 398. [Google Scholar] [CrossRef] [PubMed]
- Allardet-Servent, J.; Castanier, M.; Signouret, T.; Soundaravelou, R.; Lepidi, A.; Seghboyan, J.-M. Safety and Efficacy of Combined Extracorporeal CO2 Removal and Renal Replacement Therapy in Patients With Acute Respiratory Distress Syndrome and Acute Kidney Injury. Crit. Care Med. 2015, 43, 2570–2581. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Jaber, S.; Zogheib, E.; Godet, T.; Capellier, G.; Combes, A. Feasibility and safety of low-flow extracorporeal CO2 removal managed with a renal replacement platform to enhance lung-protective ventilation of patients with mild-to-moderate ARDS. Crit. Care 2018, 22, 122. [Google Scholar] [CrossRef] [PubMed]
- Nentwich, J.; Wichmann, D.; Kluge, S.; Lindau, S.; Mutlak, H.; John, S. Low-flow CO2 removal in combination with renal replacement therapy effectively reduces ventilation requirements in hypercapnic patients: a pilot study. Ann. Intensiv. Care 2019, 9, 3. [Google Scholar] [CrossRef] [PubMed]
- Zanella, A.; Castagna, L.; Salerno, D.; Scaravilli, V.; Deab, S.A.E.A.E.S.; Magni, F.; Giani, M.; Mazzola, S.; Albertini, M.; Patroniti, N.; et al. Respiratory Electrodialysis. A Novel, Highly Efficient Extracorporeal CO2 Removal Technique. Am. J. Respir. Crit. Care Med. 2015, 192, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Jeffries, R.G.; Lund, L.; Frankowski, B.; Federspiel, W.J. An extracorporeal carbon dioxide removal (ECCO2R) device operating at hemodialysis blood flow rates. Intensiv. Care Med. Exp. 2017, 5, 41–41. [Google Scholar] [CrossRef] [PubMed]
- Esposito, R.; Esposito, I.; Imperatore, F.; Liguori, G.; Gritti, F.; Cafora, C.; Marsilia, P.F.; De Cristofaro, M. Decapneization as supportive therapy for the treatment of status asthmaticus: a case report. J. Med Case Rep. 2021, 15, 1–4. [Google Scholar] [CrossRef]
- Hospach, I.; Goldstein, J.; Harenski, K.; Laffey, J.G.; Pouchoulin, D.; Raible, M.; Votteler, S.; Storr, M. In vitro characterization of PrismaLung+: a novel ECCO2R device. Intensiv. Care Med. Exp. 2020, 8, 1–18. [Google Scholar] [CrossRef]
- CO2 Reset – Eurosets. https://www.eurosets.com/en/product/co2-reset/. Accessed , 2024. 25 November.
- Huber, W.; Lorenz, G.; Heilmaier, M.; Böttcher, K.; Sahm, P.; Middelhoff, M.; Ritzer, B.; Schulz, D.; Bekka, E.; Hesse, F.; et al. Extracorporeal multiorgan support including CO2-removal with the ADVanced Organ Support (ADVOS) system for COVID-19: A case report. Int. J. Artif. Organs 2021, 44, 288–294. [Google Scholar] [CrossRef]
- Allescher, J.; Rasch, S.; Wiessner, J.R.; de Garibay, A.P.R.; Huberle, C.; Hesse, F.; Schulz, D.; Schmid, R.M.; Huber, W.; Lahmer, T. Extracorporeal carbon dioxide removal with the Advanced Organ Support system in critically ill COVID-19 patients. Artif. Organs 2021, 45, 1522–1532. [Google Scholar] [CrossRef]
- Peek, G.J.; Killer, H.M.; Reeves, R.; Sosnowski, A.W.; Firmin, R.K. Early Experience with a Polymethyl Pentene Oxygenator for Adult Extracorporeal Life Support. Asaio J. 2002, 48, 480–482. [Google Scholar] [CrossRef] [PubMed]
- Khoshbin, E.; Roberts, N.; Harvey, C.; Machin, D.; Killer, H.; Peek, G.J.; Sosnowski, A.W.; Firmin, R.K. Poly-Methyl Pentene Oxygenators Have Improved Gas Exchange Capability and Reduced Transfusion Requirements in Adult Extracorporeal Membrane Oxygenation. Asaio J. 2005, 51, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Toomasian, J.M.; Schreiner, R.J.; Meyer, D.E.; Schmidt, M.E.; Hagan, S.E.; Griffith, G.W.; Bartlett, R.H.; Cook, K.E. A Polymethylpentene Fiber Gas Exchanger for Long-Term Extracorporeal Life Support. Asaio J. 2005, 51, 390–397. [Google Scholar] [CrossRef]
- Gaylor, J. Membrane oxygenators: current developments in design and application. J. Biomed. Eng. 1988, 10, 541–547. [Google Scholar] [CrossRef]
- Supplement for the 10th EuroELSO Congress 4–6 May 2022 London/UK. Perfusion 2022, 37, 3–111. [CrossRef] [PubMed]
- Ontaneda, A.; Annich, G.M. Novel Surfaces in Extracorporeal Membrane Oxygenation Circuits. Front. Med. 2018, 5, 321. [Google Scholar] [CrossRef]
- Kimmel, J.D.; Arazawa, D.T.; Ye, S.-H.; Shankarraman, V.; Wagner, W.R.; Federspiel, W.J. Carbonic anhydrase immobilized on hollow fiber membranes using glutaraldehyde activated chitosan for artificial lung applications. J. Mater. Sci. Mater. Med. 2013, 24, 2611–2621. [Google Scholar] [CrossRef] [PubMed]
- Arazawa, D.; Kimmel, J.; Finn, M.; Federspiel, W. Acidic sweep gas with carbonic anhydrase coated hollow fiber membranes synergistically accelerates CO2 removal from blood. Acta Biomater. 2015, 25, 143–149. [Google Scholar] [CrossRef]
- Straube, T.L.; Farling, S.; A Deshusses, M.; Klitzman, B.; Cheifetz, I.M.; Vesel, T.P. Intravascular Gas Exchange: Physiology, Literature Review, and Current Efforts. Respir. Care 2022, 67, 480–493. [Google Scholar] [CrossRef]
- Douglas, A.R.; Jones, N.L.; Reed, J.W. Calculation of whole blood CO2 content. J. Appl. Physiol. 1988, 65, 473–477. [Google Scholar] [CrossRef]
- Hodgkinson, J.; Tatam, R.P. Optical gas sensing: A review. Meas. Sci. Technol. 2013, 24, 012004. [Google Scholar] [CrossRef]
- A Barrett, N.; Hart, N.; Camporota, L. In vivo carbon dioxide clearance of a low-flow extracorporeal carbon dioxide removal circuit in patients with acute exacerbations of chronic obstructive pulmonary disease. Perfusion 2020, 35, 436–441. [Google Scholar] [CrossRef] [PubMed]
- A Barrett, N.; Hart, N.; Camporota, L. In-vitro performance of a low flow extracorporeal carbon dioxide removal circuit. Perfusion 2019, 35, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Cappadona, F.; Costa, E.; Mallia, L.; Sangregorio, F.; Nescis, L.; Zanetti, V.; Russo, E.; Bianzina, S.; Viazzi, F.; Esposito, P. Extracorporeal Carbon Dioxide Removal: From Pathophysiology to Clinical Applications; Focus on Combined Continuous Renal Replacement Therapy. Biomedicines 2023, 11, 142. [Google Scholar] [CrossRef]
- Costa, A.M.; Halfwerk, F.; Wiegmann, B.; Neidlin, M.; Arens, J. Trends, Advantages and Disadvantages in Combined Extracorporeal Lung and Kidney Support From a Technical Point of View. Front. Med Technol. 2022, 4, 909990. [Google Scholar] [CrossRef]
- Allescher, J.; Rasch, S.; Wiessner, J.R.; de Garibay, A.P.R.; Huberle, C.; Hesse, F.; Schulz, D.; Schmid, R.M.; Huber, W.; Lahmer, T. Extracorporeal carbon dioxide removal with the Advanced Organ Support system in critically ill COVID-19 patients. Artif. Organs 2021, 45, 1522–1532. [Google Scholar] [CrossRef]
- Cove, M.E.; MacLaren, G.; Federspiel, W.J.; Kellum, J.A. Bench to bedside review: Extracorporeal carbon dioxide removal, past present and future. Crit. Care 2012, 16, 232–9. [Google Scholar] [CrossRef]
- Taccone, F.S.; Malfertheiner, M.V.; Ferrari, F.; Di Nardo, M.; Swol, J.; Broman, L.M.; Vercaemst, L.; Barrett, N.; Pappalardo, F.; Belohlavek, J.; et al. Extracorporeal CO2 removal in critically ill patients: a systematic review. Minerva Anestesiol. 2017, 83, 762–772. [Google Scholar] [CrossRef]
- Vivona, L.; Battistin, M.; Carlesso, E.; Langer, T.; Valsecchi, C.; Colombo, S.M.; Todaro, S.; Gatti, S.; Florio, G.; Pesenti, A.; et al. Alkaline Liquid Ventilation of the Membrane Lung for Extracorporeal Carbon Dioxide Removal (ECCO2R): In Vitro Study. Membranes 2021, 11, 464. [Google Scholar] [CrossRef]
- Gonzalez, F.A.; Santonocito, C.; Lamasb, T.; Costa, P.; Vieira, S.M.; Ferreira, H.A.; Sanfilippo, F. Is artificial intelligence prepared for the 24-h shifts in the ICU? Anaesth. Crit. Care Pain Med. 2024, 101431. [Google Scholar] [CrossRef]
- Zhang, A.; Haimowitz, B.J.; Tharwani, K.; Rojas-Peña, A.; Bartlett, R.H.; Potkay, J.A. A Wearable Extracorporeal CO2 Removal System with a Closed-Loop Feedback. Bioengineering 2024, 11, 969. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



