Submitted:
27 November 2024
Posted:
28 November 2024
You are already at the latest version
Abstract
Major depressive disorder (MDD) can lead to cognitive dysfunction. The objective is to assess associative episodic memory and subjective memory complaints in daily life in people with a first episode of depression (FED). Analytical observational design. Fifteen patients with FED mean age 50.20 (8.04) years and 15 healthy control (HCtrl) mean age 45.07 (8.64) years participants, both middle-aged adults, were assessed. The recruitment was from Mental Health Units in Mallorca, and this lasted between March 2021 to October 2022. DSM-5® diagnostic criteria and the Interna-tional Neuropsychiatric Interview (MINI) were used to diagnose depression. This study was an analytical, cross-sectional, prospective, observational design. The following cognitive tests were used for cognitive assessment: 1) an adapted version of the Face-Name Associative Memory Exam (FNAME-12A), 2) the daily life memory questionnaire (MFE-30), and 3) the Montreal Cognitive Assessment Test (MoCA). People with FED showed a mean score of 43.33 (25.40) compared to the HCtrl 19.66 (10.12) significantly higher scores (p = .05) on the MFE-30, but there were no significant differences in the FNAME. Furthermore, no significant correlations were observed between sub-jective (MFE-30) and objective (FNAME) memory performance. We observed a dissociation be-tween FED patients’ perception of memory difficulties and their objectively measured memory. These results support the idea that patients suffering from depression (even in the first episode) tend to overestimate their memory difficulties.
Keywords:
Memoria asociativa
; depresión
; Nombre de usuario
; evaluación neuropsicológica
; Quejas subjetivas de memoria
1. Introduction
Depression is a common disorder worldwide, affecting 280 million people [1], and it is among the top ten causes of disability in the world [2]. It is presented as a set of predominantly affective symptoms impacting on people's functional status [3,4].
Importantly, major depressive disorder (MDD) can lead to cognitive dysfunction [5,6,7,8,9,10,11,12,13]. Memory complaints are amongst the most frequent complaints [12] and there is evidence that patients with depression have lower memory performance compared to healthy controls [6,14,15,16].
Research on memory complaints (i.e., the subjective perception of memory decline) in depression has gained significant attention recently [17,18,19]. Studies conducted in the general population found a relationship between depression and memory complaints [20,21,22,23,24,25]. Also, other studies with young adults show that depression is considered the only variable that explains memory complaints [26,27]. Furthermore, it has been shown that people with depression and severe anxiety report more memory complaints than people diagnosed with mild cognitive impairment (MCI) [28,29].
Another important aspect is that people's beliefs about their own memory abilities, known as memory self-efficacy, can influence how they actually use their memory in everyday situations [30,31]. Strongly negative beliefs about memory performance may have an important implication for cognitive biases [32,33], with a decrease in self-efficacy judgements observed in depression [34,35,36,37].
The relationship between memory complaints and objective memory has also sparked interest. Some studies showed that people with depression had a greater number of memory complaints and poorer performance on objective memory tests [38,39,40] showed that people with depression presented more cognitive complaints in daily life than in neuropsychological tests, probably due to the associated negative self-perception. In addition, a low correlation between objective and subjective assessment of memory has been observed in people with more severe depression [41].
In a recent review [42] concluded that the number of depressive episodes experienced might determine the type of cognitive impairment observed. While first episode of depression (FED) subjects performed significantly worse than controls on processing speed and executive/working memory, patients with recurrent depression performed significantly worse, with verbal learning and memory being the most impaired domain. Another recent review [43], assessing neurocognitive deficits in depression in the acute and remitted state, concluded that in the acute phase, there is strong support for impairment in processing speed, learning, and memory. Follow-up studies and direct comparisons revealed less pronounced deficits in remission, although deficits were still present in attention, learning and memory. A positive correlation between the number of episodes and cognitive deficits as well as depression severity and cognitive deficits was also reported.
In recent years, associative memory impairment has attracted interest in the field of neuropsychology [44,45,46,47,48] as a sensitive marker of cognitive decline. The focus of this study was to assess episodic memory using an ecologically valid and demanding test, namely, the adapted Face Name Associative Memory Exam (FNAME) [49,50,51,52,53,54,55,56,57] to detect differences in memory performance in people with FED.
In this study we use the adapted FNAME [54] because it can evaluate associative memory in a more ecological way. Furthermore, it is important to quantify memory complaints to obtain both subjective and objective measures of memory functioning in FED patients. Finally, MoCA was used as a reliable measure of general cognitive function that is sensitive to early changes in cognitive ability across domains but robust to depression symptoms within healthy cohorts [58].
Our prediction was that FED patients would present more memory complaints and lower memory performance than healthy participants.
2. Materials and Methods
2.1. Study Design
Analytical observational design. The primary study variables were FED and associative memory. Other secondary variables were memory complaints, global cognitive status, and symptoms and intensity of depression.
2.2. Participants
In this study, 30 participants were recruited and 15 of them met the criteria for FED. This group was recruited from the Mental Health Unit of the Psychiatric Hospital in Palma and the Mental Health Unit of the Regional Hospital of Inca. The other 15 participants were healthy controls (HCtrl) recruited from the general population. The recruitment lasted between March 2021 to October 2022.
FED participants met the following inclusion criteria: 1) they were between 18 and 65 years old and, 2) they had a diagnosis of FED fulfilling DSM-5® criteria. Exclusion criteria for both FED and HCtrl participants included: 1) substance abuse, such as alcohol (>24 g/day in women, 40 g/day in men) and other drugs, 2) people with other mental health or neurological disorders. HCtrl participants were volunteers with similar sociodemographic characteristics to FED participants. They reported no neurological or psychological disorders, and they did not take psychotropic drugs.
2.3. Material and Procedure
This study was an analytical, cross-sectional, prospective, observational design. Primary care physicians and/or psychiatrists from the different health centers in Palma initially assessed the participants considering the inclusion criteria. FED participants were then asked to voluntarily participate in the study and referred to the researchers to take a complete medical history and confirm the inclusion criteria. The approximate duration of each clinical and neuropsychological evaluation session was 50 minutes. On visit 1 (day 1), the psychiatrist explained the protocol to the participants and gave them the information sheet and the informed consent. The selection criteria were reviewed, and the clinical interview was conducted using the International Neuropsychiatric Interview (MINI)[59] to exclude other comorbid psychiatric disorders. Additionally, the interviewer-administered Montgomery-Asberg Depression Scale (MADRS)[60,61] was used to assess depressive severity. On visit 2 (day 7), the psychologist collected the sociodemographic data and used the Self-Reported Rapid Depressive Symptom Scale (QIDS-SR16)[62,63] to assess depressive severity of the last week.
The extended and modified Face-Name Associative Memory Exam (FNAME, Rentz et al., 2011) was then administered as shown in Figure 1 [54,64].
The administration of the FNAME was carried out in 12 steps: 1) Familiarization: participants underwent a trial where they only looked at faces, 2) Learning I: participants underwent the trial to look at the 12 face-name pairs, 3) Immediate recall I: they were asked to provide the name associated with each face, 4) Learning II: they looked at the face-name pairs they previously associated incorrectly, 5) Immediate recall II: again they were asked to provide the name associated with each face, 6) Re-learning: participants were presented again with the face-name pairs they did not remember, 7) Thirty minutes delay, 8) Spontaneous name recall: participants were asked to freely recall all the names they had learned in 2 minutes, 9) Face recognition: participants performed a face recognition and matching test, 10) Delayed recall: participants were asked again to say aloud the name associated with each face, 11) Name recognition: participants were asked to select the name associated with the face from among four. Finally, 12) Matching, where participants were asked to match the correct name with the corresponding face. Participants responded verbally and the responses were recorded on a scoring sheet.
The daily life memory failures questionnaire (MFE-30)[65] was administered during the 30-minutes delay within the administration of the FNAME. We used the version of the test validated in the Spanish population [66], which consists of 30 questions about daily situations and activities. Participants answered these using a Likert scale from 1 (never or almost never) to 5 (always or almost always), with a maximum score of 150.
The Montreal Cognitive Assessment test (MoCA)[67], a 30-items screening test that evaluates global cognitive status through different cognitive domains (memory, visuospatial ability, executive function, attention, concentration, working memory, language and orientation) was administered to observe whether participants had impaired global cognitive function. A cut-off score of 26 or higher out of 30 indicates normal cognitive state. One point was added to this score if the participant had 12 years or less of formal education when the total score was below 30.
2.4. Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics 20.1. Normality and homogeneity of variances were verified with the Shapiro-Wilk test and the Levene’s test, respectively. Descriptive statistics were carried out for the different sociodemographic, clinical, and cognitive variables of the FED and HCtrl groups, with means and standard deviation, and inferential statistics carried out by means of the Mann-Whitney (U) test and mixed model ANCOVA. Effect sizes were measured using rrb, rank biserial correlation, and Eta squared (η2). Moreover, correlations were calculated with Spearman's Rho (r) with the total sample (with p-value adjustments).
2.5. Ethical Aspects and Data Security
This study was conducted in compliance with the principles of the Declaration of Helsinki [68]. The processing, communication and transfer of personal data was in accordance with the provisions of Organic Law 3/2018, on the 5 December, on the protection of personal data and guarantee of digital rights. This study was approved by the Research Committee of the Son Espases University Hospital (HUSE) with dictum number CI-481-20 (approval date: 14th January 2021) and the Research Ethics Committee of the Balearic Islands (CEI-IB) with dictum number IB 4429/21 PI (approval date: 24th February 202). All participants signed the informed consent.
3. Results
Patients with FED obtained scores indicating that FED patients had moderate depression with MADRS = 26.63 (5.54) points and QIDS-SR16 = 15.3 (5.05) points.
Socio-demographic data and results from the different general cognitive tests are shown in Table 1.
There were more women than men in the FED group, but this was not the case in the control group. There was no significant difference between groups for age (U(29) = 66.5, p = .06), but a significant difference between groups was observed for years of education (U(29) = 19, p < .01).
Given the significant difference between groups at the level of years of education, the comparison of groups for the cognitive measures was carried out using ANCOVAs controlling this variable as a covariate. Results showed significant differences between groups for the MFE [F (1, 29) = .06, MSE = 1690.34, p = .05, η2 = 0.14], but not for the MoCA [F (1, 29) = .08, MSE = .06, p =.78, η2 = 0.01].
Table 2 presents the results of the different FNAME subtests.
The ANCOVA controlling for the effect of education revealed no significant effect of group on any of the FNAME subtests: Immediate Recall I [F (1,29) = .14, MSE = .89, p = .71, η2 = 0.01], Immediate Recall II [F (1,29) = .01 , MSE = .04, p = .93, η2 = 0.01], total immediate recall [F (1,29) = .03 , MSE = .54 , p = .87 , η2 = 0.01], Spontaneous Name Recall [F (1,29) = .58, MSE = 2.86, p = .45, η2 = 0.02], Face Recognition [F (1,29) = .003, MSE = .001, p = .96, η2 = 0.01], Delayed Recall [F (1,29) = .26, MSE = 1.79, p = .61, η2 = 0.01], Name Recognition [F (1,29) = .47, MSE = .06, p = .50, η2 = 0.02], Matching [F (1,29) = .54, MSE = 2.74 , p = .47, η2 = 0.02], and the total score [F (1,29) = .03, MSE = 3.60, p = .86, η2 = 0.01].
Recall means (subtest) (mixed model ANCOVA)
The immediate and delayed recall subtests were analysed using a 2 (groups) x 3 ANCOVA (subtest: immediate recall I, recall immediate II, delayed recall) controlling for education as a covariate. In this analysis, no significant group effect was observed [F (1, 26) = .09, MSE = 1.43, p = .76, η2 = 0.003]. Therefore, the HCtrl group did not recall significantly more face-name associations than the FED group (see Table 3). For the type of recall subtest, a significant effect was not observed either [F (1, 26) = 1.90, MSE = 8.64, p = .17, η2 = 0.13], and the interaction group by recall type (F (1,26) = .35, MSE = 1.29, p = .70, η2 = .13) was not significant.
Correlations between FNAME, MFE-30 and MoCA of all participants (FED and healthy controls) are presented in Table 3.
The score obtained on the subjective memory complaints questionnaire (MFE-30) did not significantly correlate with the FNAME subtests (p > .05). The score obtained from the MoCA was significantly correlated (p < .01) with the different FNAME subtests (total immediate recall, spontaneous name recall, delayed recall, association, total score). The total immediate recall measure and the rest of the FNAME subtests were significantly correlated with each other (p < .01).
4. Discussion
The main aim of this study was to assess possible associative episodic memory deficits and subjective memory complaints in FED by using the FNAME and the MFE-30, respectively.
Major depressive disorder (MDD) is a heterogeneous mental disorder that affects people throughout his life [70,71,72]. This mental disorder affects neurocognitive functions, including processing speed, attention and executive functions [73]. It is also important to explore associative memory, scarcely investigated in individuals with depression, especially FED.
The results did not show statistically significant differences between groups in relation to their performance on the different FNAME subtests. This result is aligned with the observation made by Alegret et al. (2015b), that worse performance on the S-FNAME was not related to depression symptoms. Additionally, other studies that have assessed episodic memory in FED patients found no differences in performance compared to healthy controls’s [74,75,76,77,78]. Therefore, these findings do not support the hypothesis that patients with FED have memory problems due to poor learning [5,7,11,12], consolidation [79,80] or recall [81,82,83].
Deficits in associative memory have been investigated in other clinical populations such as Alzheimer's disease [84,85] and Parkinson's disease [64,86,87], and in non-clinical populations such as ageing [53,54]. In the present study, associative memory performance in FED was analysed using supposedly more sensitive and cognitively demanding subtests, such as matching, which was shown to be sensitive to Parkinson's disease [64]. However, our results showed no significant differences between FED patients and healthy controls, even though FED participants reported a higher number of complaints than control participants in daily life.
These results support the findings from previous studies [22,24,25,28,38,88], showing that although patients with MDD had relatively preserved memory tests they under-estimated their memory functioning, a pattern distinct from HCtrl.
In our study, subjective memory complaints did not show a statistically significant correlation either with the different subtests of the FNAME. This lack of concordance between objective cognitive deficits and subjective memory complaints has also been shown in previous studies [72,83,89,90,91,92,93] in patients with heterogeneous referral depression diagnoses (severity, onset time, number of episodes, etc.).
Therefore, our results support the notion that patients with FED present a dissociation between objective memory (FNAME) and subjective memory (MFE-30). Beliefs about memory self-efficacy as an estimate of actual memory abilities may have an influence on the way people use their memory in everyday situations [30,31]. In this sense, when beliefs about memory performance are negative [32,33,94], this may result in a sort of self-fulfilling prophecy and, consequently, a confirmation bias. Therefore, our results suggest that FED patients may present a negative cognitive predisposition for their memory performance, which may affect subjective memory leading to a greater number of memory complaints in daily life [32,33] without objective memory being really affected. More specifically, self-efficacy moderates the relationship between self-rated memory function and depressive symptoms. Higher self-efficacy may buffer against the impact of subjective memory difficulty on one's mood and thereby mitigating the effect of depressive symptoms on memory [95,96].
The MoCA score was significantly correlated with the scores on all FNAME subtests. A stronger correlation was observed with matching, delayed recall, and spontaneous name recall, which have proven to be most sensitive to cognitive decline [64]. Noteworthy is that although FED participants and controls did not differ significantly on the MoCA score, FED presented on average a score below the cut-off score of 26 points [97,98]. This may be because the MoCA test evaluates attention and executive functions, while the FNAME evaluates associative episodic memory.
It is also important to refer to the limitations of this study. Firstly, we encountered the difficulty of recruiting patients with depression who met the inclusion criteria. In this sense, a relatively small sample was obtained that offered initial results and an approach to the objective of the study that requires broader research. Therefore, statistical analyses were carried out with a non-parametric approach. This is a pilot study that suggests new clues, but future research with larger samples should be carried out to obtain more consistent results. And secondly, this research began to be carried out during the COVID-19 pandemic, which led to significant fluctuations (non-recruitment periods) with participants. This is a pilot study that suggests new indications, but future research with larger samples should be carried out to obtain more consistent results. The difficulty in recruitment also determined that a 'one-to-one' match was not carried out between the participants in the experimental and control groups in relation to age, gender, and educational level. This gave rise to differences in educational level between participants in both groups, so it was controlled as a covariate. In addition, the control participants performed adequately on the cognitive tests, but a validated test was not used to evaluate mood; information was only collected through the participant's form about their general health status (they reported that they were active in the labour market, and self-employed). Therefore, in future research this would also be an aspect to consider.
Even considering the above limitations, the present study is relevant because: 1) FNAME is a more cognitively demanding test using sensitive measures in the assessment of associative memory, 2) patients with depression that underestimation in memory performance would be a premorbid state of functioning not identified in objective cognitive assessments, and 3) this assessment could have an important implication in the treatment of patients with a negative thought pattern. This could be incorporated for a section in cognitive restructuring therapy.
5. Conclusions
Although FED patients and healthy controls may present similar associative memory performance, FED tend to overestimate their memory difficulties, showing a dissociation between objective (FNAME) and subjective (MFE-30) memory.
Author Contributions
J.R., participated in conceptualization, investigation, data curation, methodology, supervision, formal analysis, project administration, validation, resources, and visualization. A.M., participated in conceptualization, investigation, methodology, project administration, resources, and visualization. C.N., participated in conceptualization, investigation, data curation, methodology, supervision, formal analysis, project administration, validation, resources, and visualization. F.C., participated in conceptualization, investigation, methodology, project administration, resources, and visualization. J.F.F.V., participated in conceptualization, investigation, methodology, validation, resources, and visualization. S.E.G., participated in conceptualization, investigation, methodology, validation, resources, and visualization. P.A., participated in conceptualization, investigation, data curation, methodology, supervision, formal analysis, project administration, validation, resources, and visualization. All authors read and wrote the manuscript and approved it in its final manuscript.
Funding
The author(s) declare that financial support was not received for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
This study was approved by the Research Committee of the Son Espases University Hospital (HUSE) with dictum number CI-481-20 and the Research Ethics Committee of the Balearic Islands (CEI-IB) with dictum number IB 4429/21 PI.
Informed Consent Statement
All participants signed the informed consent.
Data Availability Statement
The original contributions presented in this study are included in this article, and further inquiries can be directed to the corresponding authors.
Acknowledgments
The authors gratefully acknowledge the work of the reviewers that contribute to the improvement of this report. Authors thanks the staff of “Mental Health Unit Camí de Jesús” for their help in the recruitment and management of participants. And we are grateful to all depressive patients and healthy controls for their kind and disinterested collaboration.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization [WHO]. (March 31, 2023). Aging and health. http://www.who.int/mediacentre/factsheets/fs404/en/.
- Greer, T.L.; Kurian, B.T.; Trivedi, M.H. Defining and Measuring Functional. CNS Drugs 2010, 24, 267-284. [CrossRef]
- Evans-Lacko, S.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Alonso, J.; Benjet, C.; Bruffaerts, R.; Thornicroft, G. Socio-economic variations in the mental health treatment gap for people with anxiety, mood, and substance use disorders: Results from the WHO World Mental Health (WMH) surveys. Psychol. Med. 2018, 48, 1560-1571. [CrossRef]
- Vigo, D.; Thornicroft, G.; Atun, R. Estimating the true global burden of mental illness. Lancet Psychiatry 2016, 3, 171-178. [CrossRef]
- Butters, M.A.; Young, J.B.; Lopez, O.; Aizenstein, H.J.; Mulsant, B.H.; Reynolds III, C.F.; Becker, J.T. Pathways linking late-life depression to persistent cognitive impairment and dementia. Dialogues Clin. Neurosci. 2008, 10, 345. [CrossRef]
- Hammar, A.; Ardal, G. Verbal memory functioning in recurrent depression during partial remission and remission-Brief report. Front. Psychol. 2013, 4, 652. [CrossRef]
- Knight, M.J.; Air, T.; Baune, B. T. The role of cognitive impairment in psychosocial functioning in remitted depression. J. Affect. Disord. 2018, 235, 129-134.. [CrossRef]
- Paelecke-Habermann, Y.; Pohl, J.; Leplow, B. Attention and executive functions in remitted major depression patients. J. Affect. Disord. 2005, 89, 125-135. [CrossRef]
- Porter, R.J.; Gallagher, P.; Thompson, J.M.; Young, A.H. Neurocognitive impairment in drug-free patients with major depressive disorder. Br. J. Psychiatry 2003, 182, 214-220. [CrossRef]
- Salagre, E.; Solé, B.; Tomioka, Y.; Fernandes, B.S.; Hidalgo-Mazzei, D.; Garriga, M.; Grande, I. Treatment of neurocognitive symptoms in unipolar depression: A systematic review and future perspectives. J. Affect. Disord. 2017, 221, 205-221. [CrossRef]
- Song, L.; Che, W.; Min-Wei, W.; Murakami, Y.; Matsumoto, K. (2006). Impairment of the spatial learning and memory induced by learned helplessness and chronic mild stress. Pharmacol. Biochem. Behav. 2006, 83, 186-193. [CrossRef]
- Vázquez, C.; Hervás, G.; Hernangómez, L.; Romero, N. Modelos cognitivos de la depresión: Una síntesis y nueva propuesta basada en 30 años de investigación. Psicol. Conductual 2010, 18, 139.
- Trivedi, M.H.; Greer, T.L. Cognitive dysfunction in unipolar depression: Implications for treatment. J. Affect. Disord. 2014, 152, 19-27. [CrossRef]
- Elgamal, S.; Denburg, S.: Marriott, M.; MacQueen, G. Clinical factors that predict cognitive function in patients with major depression. Can. J. Psychiatry. 2010, 55, 653-661. [CrossRef]
- Hammar, Å.; Ronold, E.H.; Rekkedal, G.Å. Cognitive impairment and neurocognitive profiles in major depression-a clinical perspective. Front. Psychiatry 2022, 13, 764374. [CrossRef]
- James, T.A.; Weiss-Cowie, S.; Hopton, Z.; Verhaeghen, P.; Dotson, V.M.; Duarte, A. Depression and episodic memory across the adult lifespan: A metaanalytic review. Psychol. Bull. 2021, 147, 1184. [CrossRef]
- Dillon, D.G.; Pizzagalli, D.A. Mechanisms of memory disruption in depression. Trends Neurosci. 2018, 41, 137-149. [CrossRef]
- LeMoult, J.; Gotlib, I.H. Depression: A cognitive perspective. Clin. Psychol. Rev. 2019, 69, 51-66. [CrossRef]
- Ramponi, C.; Murphy, F.C.; Calder, A.J.; Barnard, P.J. Recognition memory for pictorial material in subclinical depression. Acta Psychol. 2010, 135, 293-301. [CrossRef]
- Bassett, S.S.; Folstein, M.F. Memory complaint, memory performance, and psychiatric diagnosis: A community study. J. Geriatr. Psychiatry Neurol. 1993, 6, 105-111. [CrossRef]
- Chandler, J.D.; Gerndt, J. Somatization, depression and medical illness in psychiatric inpatients. Acta Psychiatr. Scand. 1988, 77, 67-73. [CrossRef]
- Gagnon, M.; Dartigues, J. F.; Mazaux, J.; Dequae, L.; Letenneur, L.; Giroire, J.M.; Barberger-Gateau, P. Self-reported memory complaints and memory performance in elderly french community residents: Results of the PAQUID research program. Neuroepidemiology 1994, 13, 145-154. [CrossRef]
- O'Connor, D.W.; Pollitt, P.A.; Roth, M.; Brook, C.P.B.; Reiss, B.B. Memory complaints and impairment in normal, depressed, and demented elderly persons identified in a community survey. Arch. Gen. Psychiatry 1990, 47, 224-227. [CrossRef]
- Rohling, M.L.; Green, P.; Allen, L.M.; Iverson, G.L. Depressive symptoms and neurocognitive test scores in patients passing symptom validity tests. Arch. Clin. Neuropsychol. 2002, 17, 205-222. [CrossRef]
- Sachs-Ericsson, N.; Carr, D.; Sheffler, J.; Preston, T.J.; Kiosses, D.; Hajcak, G. Cognitive reappraisal and the association between depressive symptoms and perceived social support among older adults. Aging Ment. Health 2021, 25, 453-461. [CrossRef]
- Au, A.; Cheng, C.; Chan, I.; Leung, P.; Li, P.; Heaton, R.K. Subjective memory complaints, mood, and memory deficits among HIV/AIDS patients in Hong Kong. J. Clin. Exp. Neuropsychol. 2008, 30, 338-348. [CrossRef]
- Derouesné, C.; Lacomblez, L.; Thibault, S.; LePoncin, M. Memory complaints in young and elderly subjects. Int. J. Geriatr. Psychiatry 1999, 14, 291-301. [CrossRef]
- Mendes, T.; Cardoso, S.; Guerreiro, M.; Maroco, J.; Silva, D.; Alves, L.; de Mendonça, A. Memory awareness in patients with Major Depressive Disorder. J. Psychiatr. Res. 2021, 137, 411-418. [CrossRef]
- Sinforiani, E.; Zucchella, C.; Pasotti, C. Cognitive disturbances in nondemented subjects: Heterogeneity of neuropsychological pictures. Arch. Gerontol. Geriatr. 2007, 44, 375-380. [CrossRef]
- Bandura, A. Human agency in social cognitive theory. Am. Psychol. 1989, 44, 1175-1184. [CrossRef]
- Villamarín, F. Papel de la auto-eficacia en los trastornos de ansiedad y depresión. Análisis y Modificación de conducta 1990, 16, 55-79.
- Montejo, P.; Montenegro, M.; Claver, M.; Reinoso, A.; De Andrés, M.; García, A. Quejas subjetivas de memoria en adultos jóvenes y su relación con rendimiento de memoria, depresión, calidad de vida y rasgos de personalidad. Alzheimer (Barc., Internet), 2013, 6-15.
- Randolph, J.J.; Arnett, P.A.; Freske, P. Metamemory in multiple sclerosis: Exploring affective and executive contributors. Arch. Clin. Neuropsychol. 2004, 19, 259-279. [CrossRef]
- Kavanagh, D.J. Self-efficacy and depression. In Schwarzer, R (Ed.) Self-efficacy and depression. Self-efficacy: Thought control of action. Taylor & Francis, 1992, pp. 177-193.
- Lippke, S. Self-Efficacy Theory. In: Zeigler-Hill, V., Shackelford, T.K. (Ed.) Encyclopedia of Personality and Individual Differences. Springer 2020. [CrossRef]
- Maddux, J.E.; Meier, L.J. Self-Efficacy and Depression. In Maddux, J.E. (Ed.) Self-Efficacy, Adaptation, and Adjustment. The Plenum Series in Social/Clinical Psychology. Springer 1995. [CrossRef]
- Beaudoin, M.; Desrichard, O. Are memory self-efficacy and memory performance related? A meta-analysis. Psychol. Bull. 2011, 137, 211. [CrossRef]
- Comijs, H.C.; Deeg, D.J.H.; Dik, M.G.; Twisk, J.W.R.; Jonker, C. Memory complaints; the association with psycho-affective and health problems and the role of personality characteristics: A 6-year follow-up study. J. Affect. Disord. 2002, 72, 157-165. [CrossRef]
- Derouesné, C.; Rapin, J.R.; Lacomblez, L. Memory complaints in 200 subjects meeting the diagnostic criteria for age-associated memory impairment: Psychoaffective and cognitive correlates. Psychol. Neuropsychiatr. Vieil. 2004, 2, 67-74.
- Alegret, M.; García-Gutiérrez, F.; Muñoz, N.; Espinosa, A.; Ortega, G.; Lleonart, N.; Boada, M. (2024). FACEmemory®, an innovative online platform for episodic memory pre-screening: Findings from the first 3,000 participants. J. Alzheimer’s Dis. 2024, 97, 1173-1187. [CrossRef]
- Zandi, T. Relationship between subjective memory complaints, objective memory performance, and depression among older adults. Am. J. Alzheimer’s Dis. Other Demen. 2004, 19, 353-360. [CrossRef]
- Varghese, S.; Frey, B.N.; Schneider, M.A.; Kapczinski, F.; de Azevedo Cardoso, T. Functional and cognitive impairment in the first episode of depression: A systematic review. Acta Psychiatr. Scand. 2022, 145, 156–185. [CrossRef]
- Crumley, J.J.; Stetler, C.A.; Horhota, M. Examining the relationship between subjective and objective memory performance in older adults: A meta-analysis. Psychol. Aging 2014, 29, 250. [CrossRef]
- Kriesche, D.; Woll, C.F.; Tschentscher, N.; Engel, R.R.; Karch, S. Neurocognitive deficits in depression: A systematic review of cognitive impairment in the acute and remitted state. Eur. Arch. Psychiatry Clin. Neurosci. 2023, 273, 1105-1128. [CrossRef]
- Bird, C.M. The role of the hippocampus in recognition memory. Cortex 2017, 93, 155-165. [CrossRef]
- Chirico, M.; Custer, J.; Shoyombo, I.; Cooper, C.; Meldrum, S.; Dantzer, R.; Toups, M.S. Kynurenine pathway metabolites selectively associate with impaired associative memory function in depression. Brain Behav. Immun. 2020, 8, 100126. [CrossRef]
- Loewenstein, D. A.; Curiel, R. E.; Duara, R.; Buschke, H. (2017). Novel cognitive paradigms for the detection of memory impairment in preclinical Alzheimer’s disease. Assessment 2017, 25, 348-359. [CrossRef]
- Rentz, D.M.; Amariglio, R.E.; Becker, J.A.; Frey, M.; Olson, L.E.; Frishe, K.; Sperling, R.A.. Face-name associative memory performance is related to amyloid burden in normal elderly. Neuropsychologia 2011, 49, 2776-2783. [CrossRef]
- Yu, Q.; Cheval, B.; Becker, B.; Herold, F.; Chan, C.C.H.; Delevoye-Turrell, Y.N.; Zou, L. Episodic Memory Encoding and Retrieval in Face-Name Paired Paradigm: An fNIRS Study. Brain Sci. 2021, 11, 951. [CrossRef]
- Alegret, M.; Valero, S.; Ortega, G.; Espinosa, A.; Sanabria, A.; Hernández, I.; Boada, M. Validation of the Spanish version of the Face Name Associative Memory Exam (S-FNAME) in cognitively normal older individuals. Arch. Clin. Neuropsychol. 2015a, 30, 712-720. doi.: 10.1093/arclin/acv050.
- Alegret, M.; Rodríguez, O.; Espinosa, A.; Ortega, G.; Sanabria, A.; Valero, S.; Boada, M. Concordance between subjective and objective memory impairment in volunteer subjects. J. Alzheimer’s Dis. 2015b, 48, 1109-1117. [CrossRef]
- Amariglio, R.E.; Frishe, K.; Olson, L.E.; Wadsworth, L.P.; Lorius, N.; Sperling, R. A.; Rentz, D. M. Validation of the Face Name Associative Memory Exam in cognitively normal older individuals. J. Clin. Exp. Neuropsychol. 2012, 34, 580-587. [CrossRef]
- Enriquez-Geppert, S.; Flores-Vázquez, J.F.; Lietz, M.; Garcia-Pimenta, M.; Andrés, P. I know your face but can’t remember your name: Age-related differences in the FNAME-12NL. Arch. Clin. Neuropsychol. 2021, 1-6. [CrossRef]
- Flores-Vázquez, J.F.; Rubiño, J.; Contreras-López, J.J.; Contreras, C.C.; Sosa-Ortiz, A.L.; Enriquez-Geppert, S.; Andres, P. Worse associative memory recall in healthy older adults compared to young ones, a face-name study in Spain and Mexico. J. Clin. Exp. Neuropsychol. 2021, 43, 558-567. [CrossRef]
- Flores-Vázquez, J.F.; Contreras-López, J.J.; Stegeman, R.; Castellanos-Maya, O.; Ćurčić-Blake, B.; Andrés, P.; Enriquez-Geppert, S. Extended FNAME performance is preserved in subjective cognitive decline but highly affected in amnestic mild cognitive impairment. Neuropsychology 2023, 37, 650. [CrossRef]
- Rentz, D.M.; Weiss, B. K.; Jacobs, E.G.; Cherkerzian, S.; Klibanski, A.; Remington; A.; Goldstein, J.M. Sex differences in episodic memory in early midlife: Impact of reproductive aging. Menopause 2017, 24, 400. [CrossRef]
- Rubiño, J.; Andrés, P. The Face-Name Associative Memory Test as a tool for early diagnosis of Alzheimer’s disease. Front. Psychol. 2018, 9, 1464. [CrossRef]
- Freitas, S.; Simões, M.R.; Alves, L.; Vicente, M.; Santana, I. Montreal Cognitive Assessment (MoCA): Validation study for vascular dementia. J. Int. Neuropsycol. Soc. 2012, 18, 1031-1040. [CrossRef]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (MINI): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 22-33. [CrossRef]
- Montgomery, S.A.; Åsberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry 1979, 134, 382-389. [CrossRef]
- Lobo, A.; Chamorro, L.; Luque, A.; Dal-Ré, R.; Badia, X.; Baró, E.; Grupo de Validación en Español de Escalas Psicométricas (GVEEP). (2002). Validación de las versiones en español de la Montgomery-Asberg Depression Rating Scale y la Hamilton Anxiety Rating Scale para la evaluación de la depresión y de la ansiedad. Med. Clin. 2002, 118, 493-499. [CrossRef]
- Rush, A.J.; Trivedi, M.H.; Ibrahim, H.M.; Carmody, T.J.; Arnow, B.; Klein D.K.; Keller M. B. The 16-Item quick inventory of depressive symptomatology (QIDS), clinical rating (QIDS-C), and self-report (QIDS-SR): A psychometric evaluation in patients with chronic major depression. Biol. Psychiatry 2003, 54, 573-583. [CrossRef]
- Gili, M.; Lopez-Navarro, E.; Homar, C.; Castro, A.; García-Toro, M.; Llobera, J.; Roca, M. Psychometric properties of Spanish version of QIDS-SR16 in depressive patients. Actas Esp. Psiquiatr. 2014, 42, 292-299.
- Siquier, A.; Andrés, P. Face name matching and memory complaints in Parkinson’s disease. Front. Psychol. 2022, 13, 1051488. [CrossRef]
- Sunderland, A.; Harris, J.E.; Gleave, J. Memory failures in everyday life following severe head injury. J. Clin. Exp. Neuropsychol. 1984, 6, 127-142. [CrossRef]
- Lozoya-Delgado, P.; Ruiz-Sánchez de León, J.M.; Pedrero-Pérez, E.J. Validación de un cuestionario de quejas cognitivas para adultos jóvenes: Relación entre las quejas subjetivas de memoria, la sintomatología prefrontal y el estrés percibido. Rev. Neurol. 2012, 54, 137-50.
- Nasreddine, Z. S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695-699. [CrossRef]
- Declaration of Helsinki. Ethical principles for medical research involving research involving human subjects. 2013. Available online: Shorturl.at/sNUV4 (accessed on 3 June 2023).
- Cohen, J. A power primer. In. E. Kazdin (Ed.), Methodological issues and strategies in clinical research (4th ed.). APA PsycNet 2016, pp. 279-284. [CrossRef]
- Knight, M.J.; Lyrtzis, E.; Baune, B. T. The association of cognitive deficits with mental and physical Quality of Life in Major Depressive Disorder. Comprehensive psychiatry 2020, 97, 152147. [CrossRef]
- Lupien, S.J.; Juster, R.P.; Raymond, C.; Marin, M.F.. The effects of chronic stress on the human brain: From neurotoxicity, to vulnerability, to opportunity. Front. Neuroendocrinol. 2018, 49, 91-105. [CrossRef]
- Schwert, C.; Stohrer, M.; Aschenbrenner, S.; Weisbrod, M.; Schröder, A. (2018). Biased neurocognitive self-perception in depressive and in healthy persons. J. Affect. Disord. 2018, 232, 96-102. [CrossRef]
- Dotson, V.M.; McClintock, S.M.; Verhaeghen, P.; Kim, J.U.; Draheim, A.A.; Syzmkowicz, S.M.; Wit, L.D. Depression and cognitive control across the lifespan: A systematic review and meta-analysis. Neuropsychol. Rev. 2020, 30, 461-476. [CrossRef]
- Albus, M.; Hubmann, W.; Wahlheim, C.; Sobizack, N.; Franz, U.; Mohr, F. Contrasts in neuropsychological test profile between patients with first-eoisode schizophienia and first-episohe affective disorders. Acta Psychiatr. Scand. 1996, 94, 87-93. [CrossRef]
- Cullen, B.; Nicholl, B.I.; Mackay, D.F.; Martin, D.; Ul-Haq, Z.; McIntosh, A.; Smith, D.J. Cognitive function and lifetime features of depression and bipolar disorder in a large population sample: Cross-sectional study of 143,828 UK Biobank participants. Eur. Psychiatry 2015, 30, 950-958. [CrossRef]
- Fossati, P.; Ergis, A.M.; Allilaire, J.F.. Qualitative analysis of verbal fluency in depression. Psychiatry Res. 2003, 117, 17-24. [CrossRef]
- Kyte, Z.A.; Goodyer, I.M.; Sahakian, B.J. Selected executive skills in adolescents with recent first episode major depression. J. Child Psychol. Psychiatry 2005, 46, 995-1005. [CrossRef]
- van Eijndhoven, P.; van Wingen, G.; Fernández, G.; Rijpkema, M.; Verkes, R.J.; Buitelaar, J.; Tendolkar, I. Amygdala responsivity related to memory of emotionally neutral stimuli constitutes a trait factor for depression. Neuroimage 2011, 54, 1677-1684. [CrossRef]
- Dong, Z.; Gong, B.; Li, H.; Bai, Y.; Wu, X.; Huang, Y.; He, W.; Li, T.; Wang, YT. Mechanisms of hippocampal long-term depression are required for memory enhancement by novelty exploration. J. Neurosci. 2012, 32, 11980-11990. [CrossRef]
- Dzib-Goodin, A.; Sanders, L.; Yelizarov, D. Sistemas Neuro-Moleculares necesarios para el proceso de memoria. Cuadernos de Neuropsicología/Panamerican Journal of Neuropsychology 2017, 11.
- Halvorsen, M.; Sundet, K.; Eisemann, M.; Wang, C.E.A. Verbal learning and memory in depression: A 9-year follow-up study. Psychiatry Res. 2011, 188, 350-354. [CrossRef]
- Lahr, D.; Beblo, T.; Hartje, W. Cognitive performance and subjective complaints before and after remission of major depression. Cogn. Neuropsychiatry 2007, 12, 25-45. [CrossRef]
- Serra-Blasco, M.; Torres, I.J.; Vicent-Gil, M.; Goldberg, X.; Navarra-Ventura, G.; Aguilar, E.; Cardoner, N. Discrepancy between objective and subjective cognition in major depressive disorder. Eur. Neuropsychopharmacol. 2019, 29, 46-56. [CrossRef]
- Della Sala, S.; Parra, M.A.; Fabi, K.; Luzzi, S.; Abrahams, S.. Short-term memory binding is impaired in AD but not in non-AD dementias. Neuropsychologia 2012, 50, 833–840. [CrossRef]
- Liang, Y.; Pertzov, Y.; Nicholas, J.M.; Henley, S.M.D.; Crutch, S.; Woodward, F.;Husain, M. Visual short-term memory binding deficit in familial Alzheimer’s disease. Cortex 2016, 78, 150–164. [CrossRef]
- Bezdicek, O.; Ballarini, T.; Buschke, H.; Růžicka, F.; Roth, J.; Albrecht, F.;Jech, R. Memory impairment in Parkinson’s disease: The retrieval versus associative deficit hypothesis revisited and reconciled. Neuropsychology 2019, 33, 391-405. [CrossRef]
- Cohn, M.; Giannoylis, I.; De Belder, M.; Saint-Cyr, J.A.; McAndrews, M.P. Associative reinstatement memory measures hippocampal function in Parkinson’s Disease. Neuropsychologia 2016, 90, 25-32. [CrossRef]
- Miebach, L.; Wolfsgruber, S.; Frommann, I.; Buckley, R.; Wagner, M. Different Cognitive Complaint Profiles in Memory Clinic and Depressive Patients. Am. J. Geriatr Psychiatry 2018, 26, 463-475. [CrossRef]
- Antikainen, R.; Hänninen, T.; Honkalampi, K.; Hintikka, J.; Koivumaa-Honkanen, H.; Tanskanen, A.; Viinamäki, H. Mood improvement reduces memory complaints in depressed patients. Eur. Arch. Psychiatry Clin. Neurosci. 2001, 251, 6-11. [CrossRef]
- Baeza-Velasco, C.; Guillaume, S.; Olié, E.; Alacreu-Crespo, A.; Cazals, A.; Courtet, P. Decision-making in major depressive disorder: Subjective complaint, objective performance, and discrepancy between both. J. Affect. Disord. 2020, 270, 102-107. doi; 10.1016/j.jad.2020.03.064.
- Farrin, L.; Hull, L.; Unwin, C.; Wykes, T.; David, A. Effects of depressed mood on objective and subjective measures of attention. J. Neuropsychiatry Clin. Neurosci. 2003, 15, 98-104. [CrossRef]
- Mohn, C.; Rund, B.R. Neurocognitive profile in major depressive disorders: Relationship to symptom level and subjective memory complaints. BMC Psychiatry 2016, 16, 1-6. [CrossRef]
- Schweizer, S.; Kievit, R.A.; Emery, T.; Henson, R.N. Symptoms of depression in a large healthy population cohort are related to subjective memory complaints and memory performance in negative contexts. Psychol. Med. 2018, 48, 104-114. [CrossRef]
- Cavanaugh, J.C.; Murphy, N.Z. Personality and metamemory correlates of memory performance in younger and older adults. Educ. Gerontol. 1986, 12, 385-394. [CrossRef]
- Bhang, I.; Mogle, J.; Hill, N.; Whitaker, E.B.; Bhargava, S. Examining the temporal associations between self-reported memory problems and depressive symptoms in older adults. Aging Ment. Health 2020, 24, 1864-1871. [CrossRef]
- O'Shea, D.M.; Dotson, V.M.; Fieo, R.A.; Tsapanou, A.; Zahodne, L.; Stern, Y. Older adults with poor self-rated memory have less depressive symptoms and better memory performance when perceived self-efficacy is high. Int. J. Geriatr. Psychiatry 2016, 31, 783-790. [CrossRef]
- Blair, M.; Coleman, K.; Jesso, S., Jodoin, V.D., Smolewska, K.; Warriner, E.; Pasternak, S.H. Depressive symptoms negatively impact Montreal Cognitive Assessment performance: A memory clinic experience. Can. J. Neurol. Sci. 2016, 432, 513-517. [CrossRef]
- Sánchez-Nieto, J.M.; Mendoza-Núñez, V.M. Prevalencia de probable deterioro cognitivo en adultos mayores de una población mexicana utilizando el MMSE y el MoCA. Gerokomos 2021, 32, 168-171.
Figure 1.
Scheme representing the expanded and modified FNAME paradigm.
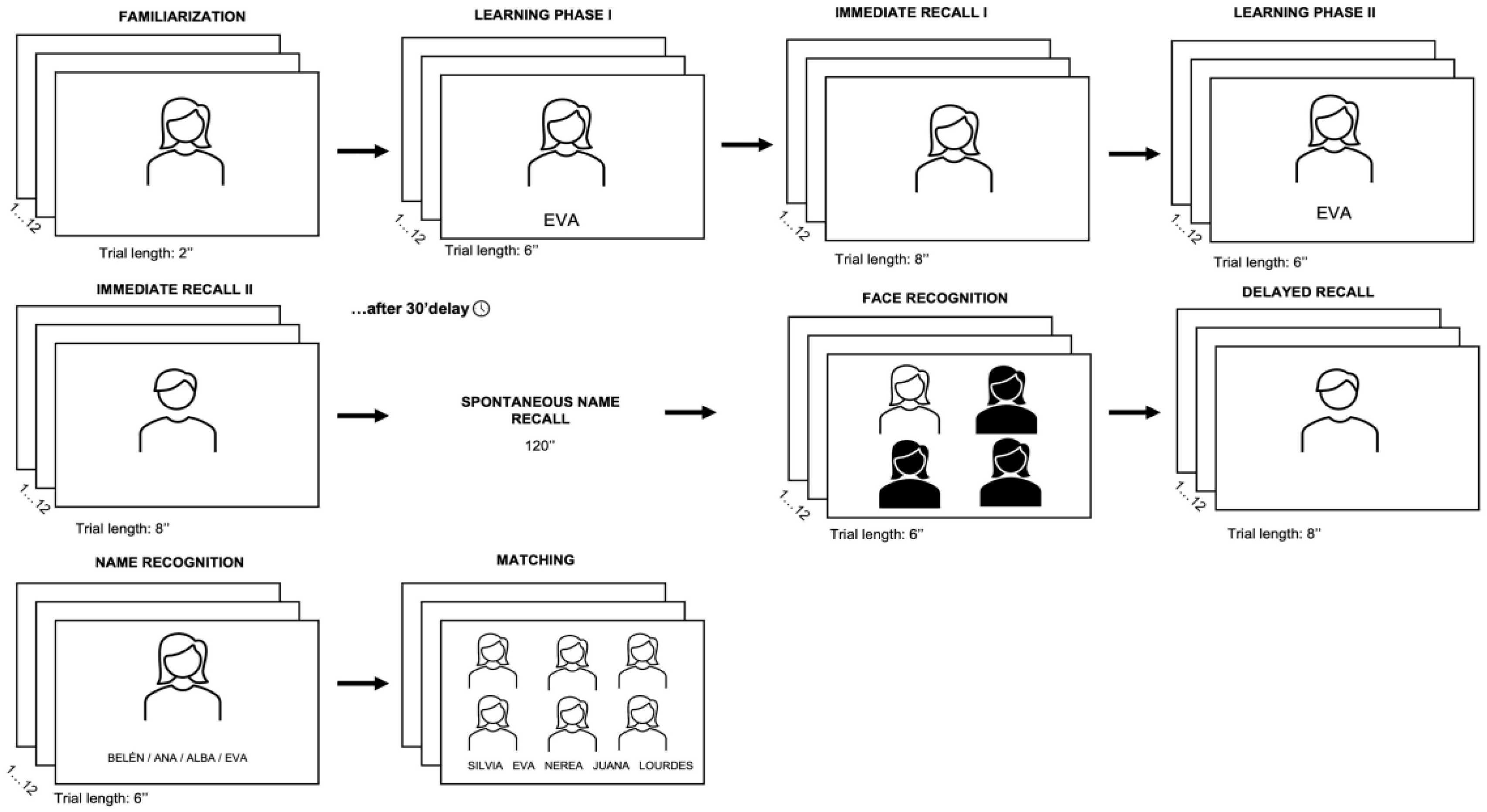

Table 1.
Demographic data (means and standard deviation) of FED and HCtrl. p values and effect sizes are provided.
Table 1.
Demographic data (means and standard deviation) of FED and HCtrl. p values and effect sizes are provided.
| FED | HCtrl | p-value | rrb/ η2 | |
|---|---|---|---|---|
| Males | 3 (20%) | 8 (53.33%) | ||
| Females | 12 (80%) | 7 (46.66%) | ||
| Age | 50.20 (8.04) | 45.07 (8.64) | .06 | .35 |
|
Education (years) MFE-30 MoCA |
10.30 (2.49) 43.33 (25.40) 22.02 (5.21) |
16.27 (3.47) 19.66 (10.12) 53.73 (7.05) |
.001 .05 .22 |
.73 .14 .05 |
FED, participants with first episode of depression; HCtrl, healthy controls; U, U-Mann-Whitney; p-value with significance levels: p < .001 (high), p < .01 (medium), p < .05 (low); rrb, rank biserial correlation (effect size): rrb < .3 small effect, rrb .3 to .50 medium effect, rrb > .5 large effect (Cohen, 2016), MFE, Memory Failures of Everyday Questionnaire; MoCA, Montreal Cognitive Assessment; η2, Eta squared (effect size): 0.01 = small effect size, 0.06 = medium effect size, 0.14 or higher = large effect size [69].
Table 2.
The different FNAME subtests (means and standard deviations) for FED and healthy controls. Significance levels are provided for the ANCOVAs controlling for the effect of education. Effect sizes are also included.
Table 2.
The different FNAME subtests (means and standard deviations) for FED and healthy controls. Significance levels are provided for the ANCOVAs controlling for the effect of education. Effect sizes are also included.
| FED | HCtrl | p-value | η 2 | |
|---|---|---|---|---|
| Immediate Recall I | 5.26 (3.26) | 7.5 (2.25) | .71 | .01 |
| Immediate Recall II | 7 (3.29) | 9.93 (1.98) | .93 | .01 |
| Total IR (I + II) | 12.26 (6.55) | 17.43(4.23) | .87 | .01 |
| Spontaneous name Recall | 8.06 (2.89) | 9.66 (1.98) | .45 | .02 |
| Face recognition | 11.86 (0.35) | 11.86 (0.50) | .96 | .01 |
| Delayed recall | 8.26 (3.39) | 10 (2.06) | .61 | .01 |
| Name recognition | 11.80 (0.41) | 11.93 (0.25) | .50 | .01 |
| Matching (Association) | 9.53 (3.14) | 11.53 (0.72) | .47 | .02 |
| Total score | 61.80 (14.99) | 72.46 (7.65) | .86 | .01 |
FED, participants with first episode of depression; HCtrl, healthy controls; Total IR, Total immediate recall; p-value, significance level; η2, Eta squared.
Table 3.
Correlations between FNAME, MFE-30, and MoCA.
| MoCA | TIR | SNR | RD | Matching | Total score | |
|---|---|---|---|---|---|---|
| MFE-30 | -.08 | -.04 | -.029 | -.032 | -.24 | -.045 |
| MoCA | .66** | .62** | .54** | .49** | .67** | |
| Total IR | .79** | .79** | .70** | .96** | ||
| SNR | .85** | .71** | .90** | |||
| DR | .78** | .90** | ||||
| Matching | .80** |
MFE, Memory Failures of Everyday Life Questionnaire; MoCA, Montreal Cognitive Assessment; FNAME, Face-Name Associative Memory Exam; Total IR, total immediate recall; SNR, spontaneous name recall; DR, delayed recall; **, the correlation is significant at the .01 level (bilateral); *, the correlation is significant at the .05 level (bilateral).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



