
Submitted:
27 November 2024
Posted:
28 November 2024
You are already at the latest version
Abstract
Giant cell tumor of bone (GCTb), formerly also known as osteoclastoma, is a pathological entity that in veterinary medicine is still undefined and, probably, underdiagnosed. In humans, GCTb, is recognized as a primary benign bone tumor, locally aggressive, with high local recurrence rates, with controversial histogenesis that can rarely progress or present as a malignant form.
In pets, this tumor is still considered rare, though the possibility of underdiagnosis is significant. Hence, the aim of the present study is to provide a histological and immunohistochemical characterization of a small case series of presumptive feline GCTb, comparing our results to the data reported for the human counterpart.
Searching our archive we found, from 2010 to 2023, only three diagnosed cases of feline GCTb. After diagnosis revision, the samples were submitted to immunohistochemistry for Iba1, TRAP, SATB2, RUNX2, RANK, karyopherin α2 (KPNA-2), and osteocalcin. Ki-67 index was also evaluated.
Results showed that the multinucleated giant cells were positive for Iba1, TRAP, and RANK, accounting for their osteoclastic origin. On the other side, mononuclear cells were mostly positive for osteoblast markers such as RUNX2, SATB2, and KPNA-2, whereas tumor-associated macrophages, showed positivity for Iba1. Hence, results were comparable to those described in the human form of the tumor.
Currently, diagnostic criteria for GCTBs in cats and, in domestic animals more broadly, are still lacking. Larger case series, complete with follow-up information, molecular analyses for specific mutations, and imaging of both tumor and patients, are needed to improve identification and achieve greater sensitivity in diagnosing this unique tumor.
Keywords:
feline
; giant cell tumor of bone
; immunohistochemistry
; osteoclast-like cells
; RUNX2
; Karyopherin α2
; IBA1
; TRAP
; RANK
1. Introduction
In humans, giant cell tumor of bone (GCTb, also known as osteoclastoma) is a primary benign tumor of bones, that displays a locally aggressive behavior, with high local recurrence rates; also, it can occasionally progress to a malignant form [1]. This tumor typically arises in individuals with complete skeletal maturation and mainly affects long bones epiphyses, causing deep alteration to bone structure and impacting on joint functions. GCTb is the most common benign tumor of bones in humans representing up to 20% of benign primary bone tumors and 4-10% on the total primary bone tumors [1,2,3].
GCTbs are reported to affect all ethnical groups, but a higher prevalence (up to 20% of primary bone tumors) has been reported in Chinese patients [4] and in India (20.3% of primary bone tumors [5]), where the incidence of GCTBs is higher than in the Western populations [6]. A recent data collection from suburban New York healthcare system, revealed instead a 4.9% of GCTb diagnoses on total benign bone lesions, with osteochondroma representing the most common, with 47% on the total number of diagnoses [7].
Several studies report a slight predominance of this diagnosis in women over men, particularly in Western countries [8], with variable percentages [9] (54.6% women - 45.4% men reported in a Brazilian study [10]; 58% women - 42% men in a Dutch study from Pathology Registry [11]; 54% women - 46% men in a report from the Swedish Cancer Registry) and a female-to-male ratio ranging from 1:1.1 to 1:1.5 [3]. On the other hand, other studies indicate a higher prevalence in men, with a male/female sex ratio of 1.27-1.77:1 [8].
It is commonly reported in young adults, with age comprised between 20 and 40 years, but there are reports of this tumor also for patients >50 years. Some studies report a second peak in diagnoses among 50-59 years.
Histologically, GCTbs are typically composed by a striking number of multinucleated osteoclast-like giant cells intermingled with a stromal mononuclear population [12], partially composed of macrophages [13,14]. In human medicine, giant multinucleated cells have been demonstrated to be reactive osteoclasts [15]. The mononuclear stromal cell population is supposed to be the neoplastic and proliferative GCTb component, inducing the massive osteoclast-like cell differentiation. This cellular population is composed by stromal cells and mononuclear monocyte cells, considered to be either reactive macrophages (tumor-associated macrophages, TAMs) or osteoclasts precursors [16]. Some studies demonstrated that the stromal cells expressed many osteoblastic markers and showed properties of pre-osteoblast-like cells, leading to the hypothesis that GCTb is of osteoblast lineage origin [17]; some other studies supported a mesenchymal stem cell origin of the lesion.
Immunohistochemically, human GCTb show mononuclear stromal cells strongly positive for SATB2 and RUNX2, while the giant cell component is negative for both markers. [18,19,20]
In humans, the presence of a driver mutation in the histone 3.3 (H3.3) gene H3F3A is the key to confirm the diagnosis, being described in more than 90% of cases [21,22]. These studies, to the best of the authors’ knowledge, have never been conducted on domestic animals or in cats.
In domestic animals, particularly in dogs and cats, the reports on this type of tumor are rare, being mostly recognized in the feline population [23,24,25,26,27]. As a consequence, data on epidemiology, tumor biology, molecular characterization, and therapeutic approach are very limited.
Indeed, in veterinary medicine, the prevalence of this tumor has never been reported, being most of the cases described in scientific literature as single case reports [23,24,25,28,29] or small case series [26]. Nevertheless it appears that GCTb is more commonly diagnosed in adult cats rather than dogs [27]. In the archives of our Pathology Service (Department of Veterinary Medicine, University of Perugia, Italy) in a period that goes from 2008 to 2024, a diagnosis of GCTb was reported in <1% on the total bone lesions of cats. Case reports of GCTb in dogs are even more sporadic in veterinary medicine scientific literature [30,31]. To support this, no diagnosis of GCTb has been reported in the Canine Cancer Registry of Umbria Region (Italy), on a total of >18.500 diagnoses recorded from October 2013 to September 2024 [32].
The histological diagnosis of GCTb is based on features that are similar to the human counterpart; a neoplasm composed of a large number of multinucleated giant cells often defined “osteoclast-like”, intermingled with mononuclear round to oval cells, recognized as the real neoplastic component of the lesion, and a third cellular population of macrophages/monocytes, probably representing the osteoclast percursors [14,15]. Immunohistochemically, feline GCTb have been described for the mononuclear stromal cell component, positivity for osteoblast markers (i.e., osterix), and for the giant cell component, the expression of macrophage markers (i.e., Iba1). [25]
Different authors report that, in domestic animals, the main challenge is the differentiation with giant cell-rich osteosarcoma, particularly when based only on histological and cytological features [27,33]. As differential features, in giant cell-rich osteosarcoma, cellular anisocytosis and anisokaryosis are expected to be more evident and associated with a variable deposition of osteoid matrix. [33] Moreover, imaging characteristics can be valuable in the diagnostic process; however, the limited number of studies that examine both clinical and pathological features in tandem makes it challenging to identify imaging features that strongly suggest a diagnosis of GCTb in pets.
The present short case series aims at providing a histological and phenotypical description of three feline GCTB, comparing our results with the data available for the human counterpart.
2. Materials and Methods
Case Selection
Cases of tumors compatible with GCTB were retrieved from the archive of the Department of Veterinary Medicine of the University of Perugia (Italy), starting from 2010.
Criteria for the inclusion in the case series was:
- -
- -
- neoplastic mononuclear stromal cell with mild cellular atypia (but mitoses can be numerous), together with numerous multinucleated giant cells;
- -
- scant/absent osteoid deposition. [35]
Histology, Histochemistry and Immunohistochemistry
Histological slides were re-evaluated by three pathologists (LL, GG, IP) to confirm the initial diagnosis. Von Kossa stain was performed to evaluate the presence of mineralized matrix and bone spicules in the examined samples.
To perform the immunohistochemical characterization, five-μm sections were cut and mounted on poly-L-lysine-coated slides from formalin-fixed and paraffin-embedded samples, which were then dewaxed and dehydrated. Immunohistochemistry was performed on serial sections with antibodies raised against Iba1 [36], TRAP, SATB2, RUNX2 [37], RANK, karyopherin α2 (KPNA-2) [37], and osteocalcin to evaluate the expression of osteoblast and macrophagic markers in the various population of GCTb. Additionally, Ki-67 was used as a proliferation marker, as commonly use for the human GCTb. [20,38,39] Immunohistochemistry was performed following the protocols reported in Table 1. Positive controls were obtained from canine reactive lymph nodes for Iba1 and Ki-67 antibodies, whereas for TRAP, SATB2, RUNX2, KPNA-2, and osteocalcin, normal bone and osteosarcoma were used. Negative controls were run omitting the primary antibody and incubating control sections with TBS. Positivity for the characterization markers (Iba1, TRAP, SATB2, RUNX2, RANK, KPNA-2, Osteocalcin) was reported as “-“, when the examined population completely lacked immunoreactivity; as “+/-“, when < than 50% of the examined population showed immunoreactivity; as “+” when > than 50% of the examined population showed immunoreactivity.
Ki-67 index was calculated with QuPath (v0.5.0) on a single field (FN22, x400) image. To obtain the percentage of positive nuclei, a full image annotation was created followed by the positive cell detection analysis. Cell detection analysis parameters were as follows: detectionImageBrightfield": "Optical density sum", "background radius": 35 px, "median filter radius": 2.0 px, "sigma": 2.0 px, "minimum area": 10 px^2, "maximum area": 400.0 px, "Threshold": 0.18, "maxBackground": 1, "cell expansion": 5.0 px, "include cell nucleus": true, "smooth boundaries": true, "make measurements": true, "threshold compartment": "Nucleus: DAB OD mean", "thresholdPositive1": 0.6, "thresholdPositive2": 0.6, "thresholdPositive3": 0.7, "singleThreshold": true.
3. Results
3.1. Case Selection and Histological Features
From our archive, we selected three feline cases that met the inclusion criteria. The signalment and anamnesis of the three cats are reported in Table 2.
Histologically, the examined sections showed a well-demarcated, expansile, highly cellular proliferative process characterized by three distinctive cellular populations. The first one was represented by mononucleated, oval to spindle-shaped stromal cells with indistinct cell borders, scant amount of eosinophilic cytoplasm and an oval nucleus with irregularly dispersed chromatin and nucleoli. These cells exhibited mild atypia, while the mitotic count was high (20 to 43 mitotic figures on 2.37mm2; FN 22, x400). Stromal cells were supported by a scant fibrovascular stroma. Intermingled with the stromal cells were a high number of macrophages and numerous and large cells (up to 150 μm) with abundant homogeneously eosinophilic cytoplasm and multiple nuclei (up to >50), defined as osteoclast-like multinucleated giant cells, evenly distributed through the lesion (Figure 1a). At the periphery of the tumor growth there were multifocal small areas of hemorrhage associated with macrophages containing intracytoplasmic ocher pigment (hemosiderin). Only rarely, bone spicules (grayish in color after Von Kossa staining) and scant amount of extracellular homogeneous eosinophilic matrix were detected between cells.
3.2. Immunohistochiemistry
Neoplastic stromal cells showed diffuse nuclear positivity for RUNX2, SATB2, KPNA2 (Figure 1b-d). Multinucleated giant cells and occasional stromal cells showed a diffuse cytoplasmic positivity for TRAP (Figure 1e), while only multinucleated giant cells showed positivity for RANK, and Iba1 (Figure 1f-g), all characterized by a finely granular cytoplasmic reaction.
Multinucleated giant cells where invariably negative for SATB2, RUNX2, and KPNA2. Detailed results of the immunohistochemical characterization of the three cases is reported in Table 3. Additionally, neoplastic stromal cells but not multinucleated giant cells were rarely osteocalcin-positive. This was instead visibly positive in remodeled bone spicules and scant and rare deposits of extracellular matrix (Figure 1h).
Regarding the proliferative index (Ki-67), the nuclear positivity ranged from 0 to 8% of neoplastic mononuclear stromal cells (Figure 1i).
4. Discussion
Giant cell tumor of bone (GCTb) is a rare entity in veterinary medicine, that apparently shares numerous similarities with the human counterpart.
Multinucleated giant cells within the lesion showed a marked cytoplasmic positivity for IBA1, tartrate-resistant acid phosphatase (TRAP), and a moderate immunolabeling for RANK.
IBA1 is a marker commonly used in dogs and cats for the identification of cells of the monocytic/macrophagic origin [40] since CD68, which is considered a pan-macrophagic marker in humans, is not suitable for canine or feline tissues, particularly when formalin-fixed and paraffin-embedded. [36] Multinucleated giant cells in feline GCTB were invariably IBA1-positive, similarly to what reported in humans, where CD68 was investigated. Moreover, this result has been observed also by Carrete et al. in a feline vertebral GCTB recently described. [41] Within the tumor analyzed also occasional intratumoral mononucleated cells, interpreted as histiocytes, were present, as described also in the human counterpart. [40]
Similarly to our results, TRAP expression was assessed in multinucleated giant cells and a subpopulation of mononucleated cells in different studies on human GCTb. [42,43,44] This peculiar TRAP pattern of expression has been hypothesized to be indicative of a monocytic osteoclast precursor phase of differentiation of giant cells. [43] Interestingly, after therapy with denosumab, that is used in humans for the treatment of unresectable GCTb, TRAP-positive cells decreased and became undetectable, suppressing tumor activity via inhibition of the RANK-RANKL pathway. [42]
RANK pathway has been associated with the pathogenesis of GCTb in humans, being involved in an imbalance between bone formation and its resorption, hence being involved in the osteolytic nature of the tumor. [45] Also, expression of RANK on osteoclast-like giant cells has been demonstrated in human GCTb and also in occasional mononuclear cells [46], similarly to what we observed in our cases.
Taken together, these result support an osteoclastic origin of the multinucleated cellular population within the tumor also in feline GCTBs, supporting their similarity with the human form.
Furthermore, all our cases were characterized by a diffuse nuclear SATB2 expression in most of the mononuclear cells, with multinucleated giant cells that were invariably negative for the marker. Also this result mirrors what has previously been reported in human medicine, where Amzajerdi and coll. suggest that, whenever a positivity of multinucleated cells should be observed, a diagnosis of osteosarcoma should be favored [18].
RUNX2 is a transcription factor which is pivotal for osteoblast differentiation [47]. The nuclear expression of this protein has been described also in canine osteosarcoma [48] and extra-skeletal osteosarcomas, where it was positive only in the osteoblastic component, being invariably negative in osteoclast-like giant multinucleated cells [37]. This is similar to what we observed in GCTb, supporting the hypothesis that, at least a part of the stromal cells, are likely originating from the osteoblastic lineage. Moreover, in human GCTb, RUNX2 expression is associated with the upregulation of MMP13, which is the main proteinase expressed by the stromal cell component of the tumor [49]. Hence, the expression of this transcription factor could be implicated also in the prognosis and clinical behavior of the tumor, which could be assessed also in cats, including in future studies tumors with a complete follow-up.
Karyopherin α2 (KPNA-2) is a transport protein that mediates the nuclear translocation of numerous target proteins through the nuclear pore complex [50]. The expression of this protein has been associated with prognosis in different types of tumors, but, interestingly, has been also demonstrated differentially expressed in osteosarcoma and other bone tumors, such as chondrosarcoma and Ewing sarcoma [51]. The authors report negativity in different benign bone lesions, but GCTb were not included in their study.
The positivity of most of the mononuclear cells, where also most of the Ki-67 positive nuclei were observed, support the hypothesis of an osteoblastic origin of the stromal component of the tumor. To support this hypothesis, there is also the evidence SATB2 expression, which has been described also in a significant number of human GCTb [18].
Unfortunately, the main limit of this study is the lack of established diagnostic criteria for GCTB in cats and the impossibility to definitively confirm the diagnosis. Our small case series was obtained borrowing information from the human counterpart. Nevertheless, we are completely aware that knowledge on this peculiar entity is still scant would need the support of clinical and biomolecular data.
5. Conclusions
Currently, the diagnostic criteria for GCTBs in cats and domestic animals are still lacking, leading to possible misdiagnosis that may suggest worst prognosis in cats affected by osteoclast-rich bone tumors. Larger case series, including follow-up information and comprehensive diagnostic imaging of the lesions and the patient, associated with histopathology, phenotyping, and biomolecular analyses, are needed to enhance the clinicopathological diagnostic capability of identifying this unique oncological entity.
Author Contributions
Conceptualization, L.L. and I.P.; methodology, I.P. and G.G.; validation, I.P.; formal analysis, G.G.; investigation, I.P., G.G. and L.L..; resources, L.L.; data curation, I.P., G.G. and L.L.; writing—original draft preparation, I.P. and G.G.; writing—review and editing, L.L.; visualization, L.L.; supervision, L.L.; project administration, L.L.; funding acquisition, L.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by University of Perugia “Bando per il finanziamento di Progetti di Ricerca di Ateneo, anno 2020” (D.R. n. 2868 del 19 November 2021).
Informed Consent Statement
Written consent for the use of the formalin-fixed and paraffin-embedded tissues were obtained by the owners together with the sample for histological diagnosis.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Acknowledgments
The authors would like to thank Valeria Migni, Sara Leto, Luca Stefanelli and Giampaolo Ceccarani for their technical support.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Jha, Y.; Chaudhary, K. Giant Cell Tumour of Bone: A Comprehensive Review of Pathogenesis, Diagnosis, and Treatment. Cureus 2023, 15, e46945. [Google Scholar] [CrossRef]
- Hartmann, W.; Harder, D.; Baumhoer, D. Giant Cell-Rich Tumors of Bone. Surg Pathol Clin 2021, 14, 695–706. [Google Scholar] [CrossRef] [PubMed]
- Mavrogenis, A.F.; Igoumenou, V.G.; Megaloikonomos, P.D.; Panagopoulos, G.N.; Papagelopoulos, P.J.; Soucacos, P.N. Giant Cell Tumor of Bone Revisited. SICOT J 2017, 3, 54. [Google Scholar] [CrossRef]
- Sung, H.W.; Kuo, D.P.; Shu, W.P.; Chai, Y.B.; Liu, C.C.; Li, S.M. Giant-Cell Tumor of Bone: Analysis of Two Hundred and Eight Cases in Chinese Patients. J Bone Joint Surg Am 1982, 64, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Saikia, K.C.; Bhuyan, S.K.; Borgohain, M.; Ahmed, F.; Saikia, S.P.; Bora, A. Giant Cell Tumour of Bone: An Analysis of 139 Indian Patients. Journal of Orthopaedic Science 2011, 16, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Gundavda, M.K.; Agarwal, M.G.; Reddy, R.; Wagh, Y.; Ghanate, V. Is Vitamin D Deficiency behind the Scenes for High Incidence of Giant Cell Tumor amongst the Indian Population? Unraveling the Vitamin D – RANKL Association. Medical Hypotheses 2019, 123, 67–71. [Google Scholar] [CrossRef]
- Muran, A.; Fallon, J.; Jung, B.; Dzaugis, P.; Zhang, A.; Fitzgerald, M.; Goodman, H.J.; Kenan, S.; Kenan, S. Treatment Trends of Benign Bone Lesions in a Suburban New York Healthcare System. J Family Med Prim Care 2023, 12, 1979–1983. [Google Scholar] [CrossRef]
- Hu, Y.; Zhao, L.; Zhang, H.; Yu, X.; Wang, Z.; Ye, Z.; Wu, S.; Guo, S.; Zhang, G.; Wang, J.; et al. Sex Differences in the Recurrence Rate and Risk Factors for Primary Giant Cell Tumors Around the Knee in China. Sci Rep 2016, 6, 28173. [Google Scholar] [CrossRef] [PubMed]
- Sobti, A.; Agrawal, P.; Agarwala, S.; Agarwal, M. Giant Cell Tumor of Bone - An Overview. Arch Bone Jt Surg 2016, 4, 2–9. [Google Scholar]
- Becker, R.G.; Galia, C.R.; Pestilho, J.F.C.S.; Antunes, B.P.; Baptista, A.M.; Guedes, A. GIANT CELL TUMOR OF BONE: A MULTICENTER EPIDEMIOLOGICAL STUDY IN BRAZIL. Acta ortop. bras. 2024, 32, e273066. [Google Scholar] [CrossRef] [PubMed]
- Verschoor, A.J.; Bovée, J.V.M.G.; Mastboom, M.J.L.; Sander Dijkstra, P.D.; Van De Sande, M.A.J.; Gelderblom, H. Incidence and Demographics of Giant Cell Tumor of Bone in The Netherlands: First Nationwide Pathology Registry Study. Acta Orthop 2018, 89, 570–574. [Google Scholar] [CrossRef] [PubMed]
- Turcotte, R.E. Giant Cell Tumor of Bone. Orthopedic Clinics 2006, 37, 35–51. [Google Scholar] [CrossRef]
- Wang, C.; Guo, Y.; Wang, L.; Nie, Z.; Zhu, J.; Yan, Q. Rare Features of Giant Cell Tumors of the Bone: A Case Report. Exp Ther Med 2024, 28, 409. [Google Scholar] [CrossRef]
- Çomunoğlu, N.; Kepil, N.; Dervişoğlu, S. Histopathology of Giant Cell Tumors of the Bone: With Special Emphasis on Fibrohistiocytic and Aneurysmal Bone Cyst like Components. Acta Orthopaedica et Traumatologica Turcica 2019, 53, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.H.; Robbins, P.; Xu, J.; Huang, L.; Wood, D.J.; Papadimitriou, J.M. The Histogenesis of Giant Cell Tumour of Bone: A Model of Interaction between Neoplastic Cells and Osteoclasts. Histology and Histopathology 2001, 16, 297–307. [Google Scholar] [PubMed]
- Kim, Y.; Nizami, S.; Goto, H.; Lee, F.Y. Modern Interpretation of Giant Cell Tumor of Bone: Predominantly Osteoclastogenic Stromal Tumor. Clin Orthop Surg 2012, 4, 107–116. [Google Scholar] [CrossRef]
- Murata, A.; Fujita, T.; Kawahara, N.; Tsuchiya, H.; Tomita, K. Osteoblast Lineage Properties in Giant Cell Tumors of Bone. J Orthop Sci 2005, 10, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Amzajerdi, A.N.; Banuelos, E.; Sassoon, A. SATB2 Expression in Locally Aggressive Giant Cell Tumor of Bone Can Be a Pitfall in Bone Pathology. American Journal of Clinical Pathology 2016, 146, 39. [Google Scholar] [CrossRef]
- Milton, S.; Prabhu, A.J.; Titus, V.T.K.; John, R.; Backianathan, S.; Madhuri, V. Special AT-Rich Sequence-Binding Protein 2 (SATB2) in the Differential Diagnosis of Osteogenic and Non-Osteogenic Bone and Soft Tissue Tumors. J Pathol Transl Med 2022, 56, 270–280. [Google Scholar] [CrossRef] [PubMed]
- Arndt, S.; Hartmann, W.; Rókusz, A.; Leinauer, B.; von Baer, A.; Schultheiss, M.; Pablik, J.; Fritzsche, H.; Mogler, C.; Antal, I.; et al. Histomorphometric Analysis of 38 Giant Cell Tumors of Bone after Recurrence as Compared to Changes Following Denosumab Treatment. Cancers (Basel) 2023, 15, 4249. [Google Scholar] [CrossRef]
- Scotto di Carlo, F.; Divisato, G.; Iacoangeli, M.; Esposito, T.; Gianfrancesco, F. The Identification of H3F3A Mutation in Giant Cell Tumour of the Clivus and the Histological Diagnostic Algorithm of Other Clival Lesions Permit the Differential Diagnosis in This Location. BMC Cancer 2018, 18, 358. [Google Scholar] [CrossRef] [PubMed]
- Ambrosi, F.; Righi, A.; Benini, S.; Magagnoli, G.; Chiaramonte, I.; Manfrini, M.; Gasbarrini, A.; Frisoni, T.; Gambarotti, M. Giant Cell Tumor of Bone in Patients under 16 Years Old: A Single-Institution Case Series. Cancers 2021, 13, 2585. [Google Scholar] [CrossRef]
- Walsh, B.A.; Rhodes, W.H. Giant Cell Tumour of Bone in a Cat. J Small Anim Pract 1995, 36, 325–329. [Google Scholar] [CrossRef]
- Ferreras, M.C.; Fuertes, M.; Pérez, V.; Benavides, J.; García-Pariente, C.; Reyes, L.E.; García-Marín, J.F. Giant Cell Tumour of Bone in a Cat with Extraskeletal Metastases: Pathological and Immunohistochemical Study. J Vet Med A Physiol Pathol Clin Med 2005, 52, 225–229. [Google Scholar] [CrossRef]
- Caldero Carrete, J.; Tabanez, J.; Civello, A.; Rusbridge, C. Vertebral Giant Cell Tumour of Bone in a Domestic Shorthair Cat. JFMS Open Rep 2023, 9, 20551169231160227. [Google Scholar] [CrossRef]
- Leonardi, L.; Quattrini, I.; Roperto, F.; Benassi, M.S. Protease Expression in Giant Cell Tumour of Bone: A Comparative Study on Feline and Human Samples. Research in Veterinary Science 2013, 95, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, L. Bone Tumors in Domestic Animals: Comparative Clinical Pathology; Springer Nature; ISBN 978-3-030-90210-0.
- Thornburg, L.P. Giant Cell Tumor of Bone in a Cat. Vet Pathol 1979, 16, 255–257. [Google Scholar] [CrossRef] [PubMed]
- Schneck, G.W. A Case of Giant Cell Epulis (Osteoclastoma) in a Cat. Vet Rec 1975, 97, 181–182. [Google Scholar] [CrossRef] [PubMed]
- Blondel, M.; Gros, L.; Semin, M.-O.; Delverdier, M.; Palierne, S.; Autefage, A. A Case of Giant Cell Tumour of Bone in a Dog. VCOT Open 2019, 02, e64–e69. [Google Scholar] [CrossRef]
- Lecouteur, R.; Nimmo, J.; Price, S.M.; Pennock, P. A Case of Giant Cell Tumor of Bone (Osteoclastoma) in a Dog. Journal of The American Animal Hospital Association 1978. [Google Scholar]
- Manuali, E.; Morgante, R.A.; Maresca, C.; Leonardi, L.; Purificato, I.; Giaimo, M.D.; Giovannini, G. A Web-Based Tumor Registration System for a Regional Canine Cancer Registry in Umbria, Central Italy. Ann Ist Super Sanita 2019, 55, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Meuten, D.J. Tumors in Domestic Animals; John Wiley & Sons, 2020; ISBN 978-0-8138-2179-5.
- Dittmer, K.; Roccabianca, P.; Bell, C.; Murphy, B.; R A, F.; Scruggs, J.; Schulman, Y.; Thompson, D.; Avallone, G.; Kiupel, M. Surgical Pathology Of Tumors Of Domestic Animals. 4: Tumors of Bone, Cartilage and Other Hard Tissues; C. L. Davis Thomson Foundation, 2021; ISBN 978-1-73374-913-8.
- Maxie, M.G.; Miller, M.A. Chapter 1 - Introduction to the Diagnostic Process. In Jubb, Kennedy & Palmer’s Pathology of Domestic Animals: Volume 1 (Sixth Edition); Maxie, M.G., Ed.; W.B. Saunders, 2016; pp. 1-15.e1 ISBN 978-0-7020-5317-7.
- Porcellato, I.; Sforna, M.; Lo Giudice, A.; Bossi, I.; Musi, A.; Tognoloni, A.; Chiaradia, E.; Mechelli, L.; Brachelente, C. Tumor-Associated Macrophages in Canine Oral and Cutaneous Melanomas and Melanocytomas: Phenotypic and Prognostic Assessment. Front. Vet. Sci. 2022, 9. [Google Scholar] [CrossRef]
- Leonardi, L.; Manuali, E.; Bufalari, A.; Porcellato, I. Canine Soft Tissue Sarcomas: The Expression of RUNX2 and Karyopherin Alpha-2 in Extraskeletal (Soft Tissues) and Skeletal Osteosarcomas. Front Vet Sci 2024, 11, 1292852. [Google Scholar] [CrossRef]
- Cheng, D.; Hu, T.; Zhang, H.; Huang, J.; Yang, Q. Factors Affecting the Recurrence of Giant Cell Tumor of Bone After Surgery: A Clinicopathological Study of 80 Cases from a Single Center. Cell Physiol Biochem 2015, 36, 1961–1970. [Google Scholar] [CrossRef]
- Lujic, N.; Sopta, J.; Kovacevic, R.; Stevanovic, V.; Davidovic, R. Recurrence of Giant Cell Tumour of Bone: Role of P53, Cyclin D1, β-Catenin and Ki67. Int Orthop 2016, 40, 2393–2399. [Google Scholar] [CrossRef] [PubMed]
- Pierezan, F.; Mansell, J.; Ambrus, A.; Rodrigues Hoffmann, A. Immunohistochemical Expression of Ionized Calcium Binding Adapter Molecule 1 in Cutaneous Histiocytic Proliferative, Neoplastic and Inflammatory Disorders of Dogs and Cats. J Comp Pathol 2014, 151, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Carrete, J.C.; Tabanez, J.; Civello, A.; Rusbridge, C. Vertebral Giant Cell Tumour of Bone in a Domestic Shorthair Cat. JFMS Open Reports 2023, 9, 20551169231160227. [Google Scholar] [CrossRef]
- Noguchi, T.; Sakamoto, A.; Murotani, Y.; Murata, K.; Hirata, M.; Yamada, Y.; Toguchida, J.; Matsuda, S. Inhibition of RANKL Expression in Osteocyte-like Differentiated Tumor Cells in Giant Cell Tumor of Bone After Denosumab Treatment. Journal of Histochemistry and Cytochemistry 2023, 71, 131. [Google Scholar] [CrossRef] [PubMed]
- Ramos, R.Y.; Haupt, H.M.; Kanetsky, P.A.; Donthineni-Rao, R.; Arenas-Elliott, C.; Lackman, R.D.; Martin, A.-M. Giant Cell Tumors: Inquiry into Immunohistochemical Expression of CD117 (c-Kit), Microphthalmia Transcription Factor, Tartrate-Resistant Acid Phosphatase, and HAM-56. Arch Pathol Lab Med 2005, 129, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Kimura, A.; Toda, Y.; Matsumoto, Y.; Yamamoto, H.; Yahiro, K.; Shimada, E.; Kanahori, M.; Oyama, R.; Fukushima, S.; Nakagawa, M.; et al. Nuclear β-Catenin Translocation Plays a Key Role in Osteoblast Differentiation of Giant Cell Tumor of Bone. Sci Rep 2022, 12, 13438. [Google Scholar] [CrossRef]
- Wu, P.-F.; Tang, J.; Li, K. RANK Pathway in Giant Cell Tumor of Bone: Pathogenesis and Therapeutic Aspects. Tumour Biol 2015, 36, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Roux, S.; Amazit, L.; Meduri, G.; Guiochon-Mantel, A.; Milgrom, E.; Mariette, X. RANK (Receptor Activator of Nuclear Factor Kappa B) and RANK Ligand Are Expressed in Giant Cell Tumors of Bone. Am J Clin Pathol 2002, 117, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Komori, T. Roles of Runx2 in Skeletal Development. Adv Exp Med Biol 2017, 962, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Barger, A.; Baker, K.; Driskell, E.; Sander, W.; Roady, P.; Berry, M.; Schnelle, A.; Fan, T.M. The Use of Alkaline Phosphatase and Runx2 to Distinguish Osteosarcoma from Other Common Malignant Primary Bone Tumors in Dogs. Vet Pathol 2022, 59, 427–432. [Google Scholar] [CrossRef]
- Mak, I.W.Y.; Cowan, R.W.; Popovic, S.; Colterjohn, N.; Singh, G.; Ghert, M. Upregulation of MMP-13 via Runx2 in the Stromal Cell of Giant Cell Tumor of Bone. Bone 2009, 45, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Moroianu, J.; Hijikata, M.; Blobel, G.; Radu, A. Mammalian Karyopherin Alpha 1 Beta and Alpha 2 Beta Heterodimers: Alpha 1 or Alpha 2 Subunit Binds Nuclear Localization Signal and Beta Subunit Interacts with Peptide Repeat-Containing Nucleoporins. Proceedings of the National Academy of Sciences 1995, 92, 6532–6536. [Google Scholar] [CrossRef]
- Jiang, L.; Liu, J.; Wei, Q.; Wang, Y. KPNA2 Expression Is a Potential Marker for Differential Diagnosis between Osteosarcomas and Other Malignant Bone Tumor Mimics. Diagn Pathol 2020, 15, 135. [Google Scholar] [CrossRef]
Figure 1.
Histological and immunohistochemical features of feline GCTb. a) Histologically, the proliferative process is characterized by neoplastic stromal cells with frequent mitotic figures, macrophages and multinucleated giant cells (MGC) (H&E; x400); b) neoplastic stromal cells show nuclear positivity for RUNX2 while MGC are diffusely negative (IHC; x400); c) neoplastic stromal cells, but not MGC show diffuse nuclear positivity for SATB2 (IHC; x400); d) neoplastic stromal cells with intense nuclear positivity for KPNA2 (IHC, x400); e) TRAP in MGC and neoplastic stromal cells (IHC; x400); f) MGC positivity for RANK (IHC; x400); g) Iba1 in macrophages and MGC (IHC; x400); h) osteocalcin expression in rare stromal cells and in bone spicules (IHC; x400); i) Ki-67 positive nuclei in neoplastic stromal cells (IHC; x400).
Figure 1.
Histological and immunohistochemical features of feline GCTb. a) Histologically, the proliferative process is characterized by neoplastic stromal cells with frequent mitotic figures, macrophages and multinucleated giant cells (MGC) (H&E; x400); b) neoplastic stromal cells show nuclear positivity for RUNX2 while MGC are diffusely negative (IHC; x400); c) neoplastic stromal cells, but not MGC show diffuse nuclear positivity for SATB2 (IHC; x400); d) neoplastic stromal cells with intense nuclear positivity for KPNA2 (IHC, x400); e) TRAP in MGC and neoplastic stromal cells (IHC; x400); f) MGC positivity for RANK (IHC; x400); g) Iba1 in macrophages and MGC (IHC; x400); h) osteocalcin expression in rare stromal cells and in bone spicules (IHC; x400); i) Ki-67 positive nuclei in neoplastic stromal cells (IHC; x400).
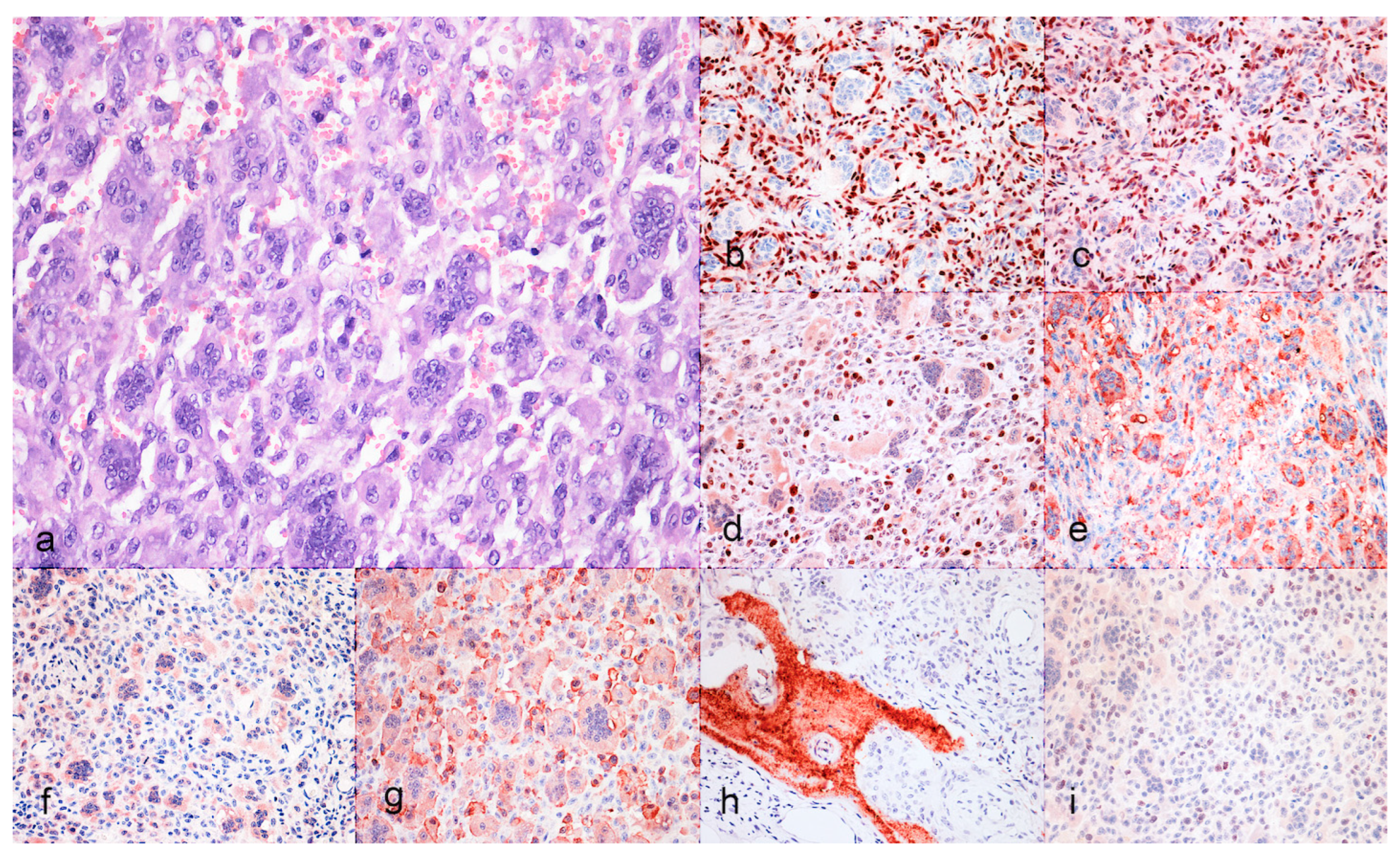

Table 1.
Antibodies and protocols for the immunohistochemical characterization of the tumors.
| Antibody | Manufacturer | Dilution | Antigen retrieval |
|---|---|---|---|
| Iba1 | Merck Millipore | 1:100 | HIER, Tris-EDTA buffer; pH 9.0 |
| TRAP | Santa Cruz Biotechnology | 1:50 | HIER, Tris-EDTA buffer; pH 9.0 |
| SATB2 | Cell Signaling Technology | 1:200 | HIER, Tris-EDTA buffer; pH 9.0 |
| RUNX2 | Santa Cruz Biotechnology | 1:200 | HIER, Tris-EDTA buffer; pH 9.0 |
| RANK | Santa Cruz Biotechnology | 1:50 | HIER, Tris-EDTA buffer; pH 9.0 |
| KPNA-2 | Santa Cruz Biotechnology | 1:150 | HIER, Tris-EDTA buffer; pH 9.0 |
| Osteocalcin | BioGenex LifeSciences | 1:50 | HIER, Tris-EDTA buffer; pH 9.0 |
| Ki-67 | Agilent Dako | 1:200 | HIER, Tris-EDTA buffer; pH 9.0 |
Table 2.
Signalment and tumor location of the three selected cases of GCTb.
| Case | Breed | Age | Sex | Tumor Location |
|---|---|---|---|---|
| 1 | Domestic shorthair | 15 | M | Tibia |
| 2 | Domestic shorthair | 15 | F | Tibia |
| 3 | Siamese | 5 | M | Dewclaw |
Table 3.
Results of the immunohistochemical analysis on mononucleated cells (MC: stromal neoplastic cells and macrophages) and multinucleated giant cells (MGC: osteoclast-like cells).
Table 3.
Results of the immunohistochemical analysis on mononucleated cells (MC: stromal neoplastic cells and macrophages) and multinucleated giant cells (MGC: osteoclast-like cells).
| Case | Iba1 | TRAP | SATB2 | RUNX2 | RANK | KPNA-2 | Osteocalcin | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MC | MGC | MC | MGC | MC | MGC | MC | MGC | MC | MGC | MC | MGC | MC | MGC | |
| 1 | +/- | + | +/- | + | + | - | + | - | +/- | + | - | + | +/- | - |
| 2 | +/- | + | +/- | + | + | - | + | - | +/- | + | - | + | - | - |
| 3 | +/- | + | - | + | +/- | - | + | - | +/- | + | - | + | +/- | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



