
Submitted:
28 November 2024
Posted:
28 November 2024
You are already at the latest version
Abstract
Leishmaniasis, a neglected tropical disease caused by the protozoan parasite Leishmania, remains a significant public health concern in endemic regions. This disease manifests in various forms like cutaneous, mucocutaneous, and visceral leishmaniasis, each associated with specific Leishmania species and influenced by host immune responses. Over the past few decades, treatment for leishmaniasis has relied on a limited range of drugs, including Pentavalent Antimonials, Amphotericin B formulations, Miltefosine, and Paromomycin. However, widespread drug resistance has emerged, particularly in visceral leishmaniasis, threatening treatment efficacy and leading to increased cases of treatment failure. This review provides a comprehensive overview of the mechanisms underlying Leishmania drug resistance, including changes in parasite uptake and efflux, intracellular sequestration, and stress response modulation. Additionally, we examine the impact of environmental factors, such as arsenic exposure in endemic areas, on resistance development, and review recent studies exploring molecular and genomic markers associated with resistance. The review highlights the urgent need for new therapeutic strategies and emphasizes a multi-faceted approach to tackle resistance through surveillance, molecular insights, and global collaborations.
Keywords:
Leishmaniasis
; neglected tropical disease
; immune responses
; treatment efficacy
1. Introduction
A Zoonotic infection parasitic vector born disease, Leishmaniasis with a flagellated protozoan parasite is caused by the genus Leishmania. This dimorphic intracellular parasite transmits the infection from the bite of phlebotomine (Old world) sand fly vector with over 90 species of these sandfly has the ability to transmit. In the New World, primary vectors Lutzomyia spp transmits infection. More than 20 species of Leishmania protozoan parasite are expected to cause infectious disease. These parasites have the ability to inhabitant in two different hosts with different morphological changes. Clinical feature differs according to the different species of Leishmania that are involved and immune response of the host. Including tropical, sub-tropical and in few European countries these parasitic diseases are found in more than 98 countries, mostly developing countries are at risk [1]. Each year more than 1 million cases were reported for this disease. Mostly the poorest people and people in the rural areas with lack of sanity, poor housing along with the weak immune system are prone to this disease [2].
Globally countries like Asia, Africa and America are much affected by this endemic. Initially the clinical description of this endemic disease was first observed in Aleppo, Syria by Alexander Russell in 1756, so it was called as the “Aleppo Boil”. After more than a century sergeant major Cunningham of the Indian medical service in 1885 across Calicut reported this as a parasitic organisms which was collected from the tissue samples from a patient who was reported by a “Delhi boil” [3]. Leishmaniasis infection has three different clinical manifestations, Cutaneous Leishmaniasis (CL), Mucocutaneous leishmaniasis(ML) and Visceral leishmaniasis(VL). Among these three clinical forms of Leishmaniasis Visceral leishmaniasis which is also called as “Kala Azar” (which means Black fever) and disease of developing countries and infection of spleen, liver, bone marrow and lymph nodes which are rich in lymphocytes, with almost 1300 cases across 70 countries Visceral leishmaniasis is the most fatal if it is not treated [4,5]. Leishmania donovani and Leishmania infantum are the two main species that cause VL. Cutaneous Leishmaniasis is the common manifestation of the disease that develops a ulcerative skin lesions and multiple non-ulcerative nodules also at the site of the sand fly bite [6], with 70 countries that are endemic with CL, 90% of the disease has spread across Asian countries [7]. In Mucocutaneous leishmaniasis both the skin and Mucous membrane gets infected [8], lesions can been visible on the upper part of the mouth and nose in mucocutaneous phase [9]. Depending on the Host immune system the clinical aspects and symptoms varies according to the species of Leishmania that has been involved [10].
Leishmania have Digenetic life style which makes this species to acclimatize both in host mammalian cell and in Vector carrier [11]. If the host is animals then it is considered as Zoonotic leishmaniasis where the parasite transmission cycle is maintained by animals such as Goat, canines, rodents [12], if the host is human then it is called as Anthroponotic leishmaniasis [1]. Two forms of Leishmania have been reported extracellular form of Parasitic Promastigotes in Vector carrier and intracellular Amastigote parasitic form in host mammalian cell. On up taking of blood meal from the host the saliva of the sandfly is injected into the blood that prevents from clotting and then sand fly vector transfers the metacyclics Promastigote form into the Host by passing into the mammalian skin and invading neutrophils not only neutrophils Langerhans cells and fibroblasts are also infected by these metacyclics Promastigote [13], at the site of infection the macrophages invades and engulfs the Promastigote where these parasites attaches to the macrophages and gets internalized into a parasitophorous vacuole which is phagocytosed by the macrophages [14]; within the macrophage the amplification along with the differentiation of the Promastigote form into Amastigotes form undergoes [15]. While some amastigotes attach themselves to the vacuole membrane, others stay free inside the vacuole and start to multiply by splitting several times. The macrophage membrane bursts after a vigorous multiplication, releasing the amastigotes into the tissue. These amastigotes can either infect fresh macrophages or be consumed by a fresh female phlebotomine when it feeds on blood [16] as shown in the Figure 1.
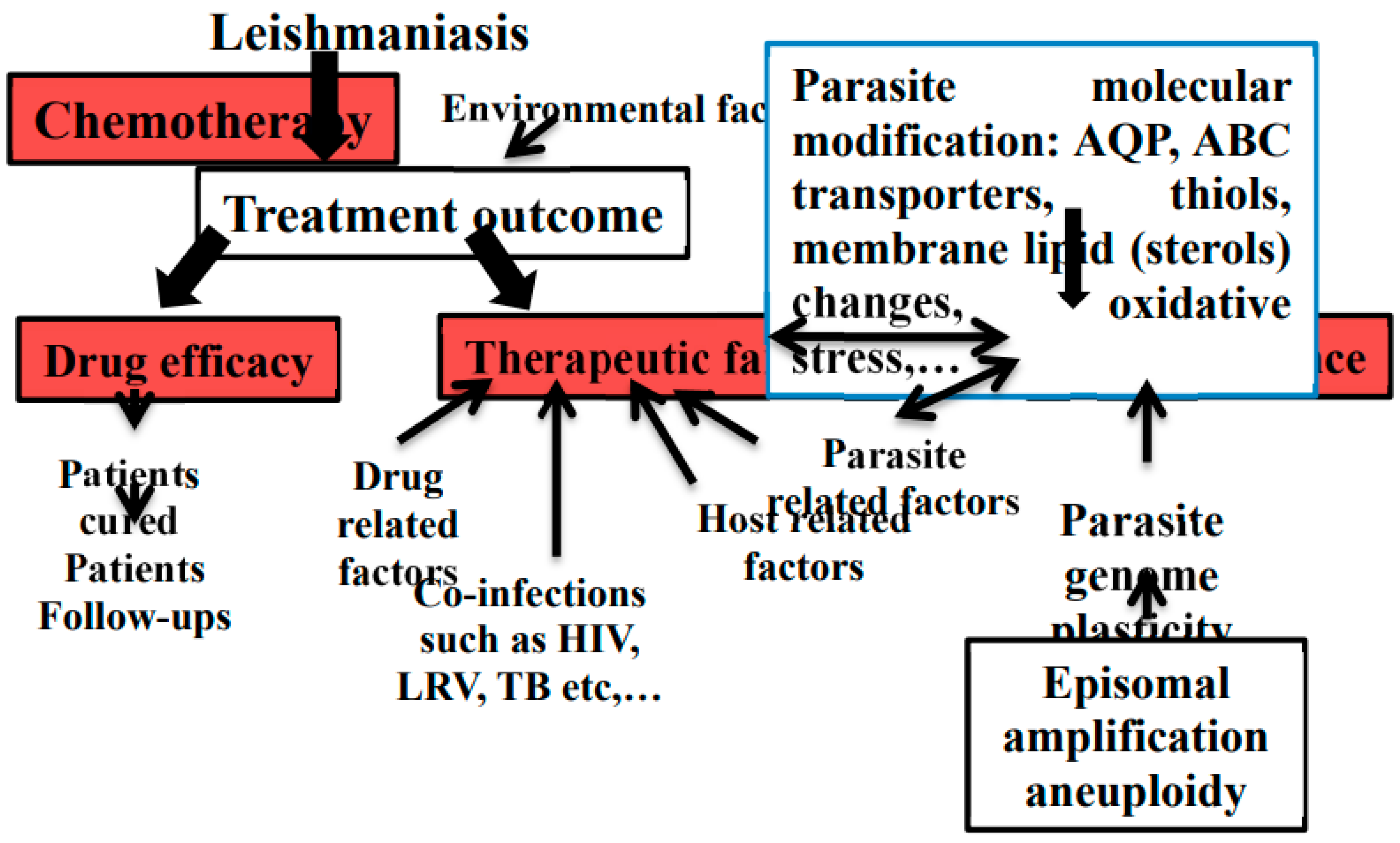
For the current treatment many drugs such as Sodium Stibogluconate, Pentamidine, Amphotericin B and Liposomal Amphotericin B, Miltefosine, Paromomycin are the suggested drugs used to treat leishmaniasis. Many alternatives like herbal plants with potential metabolites has also been studied and reported which are a possible source of new anti-leishmanial medication [17]. From the last 25 years the clinical outcome of few Antileishmanial drugs was compromised due to the over establishment of the resistance against these drugs by leishmanial strains [18]. Current Antileishmanial therapies have led to a increase in Treatment failure due to the Drug resistance with emerging cross resistance, although both treatment failure and Drug resistance are not interlinked but many factors contributes for the treatment outcomes like hosts immune system, parasite and the environment as showed in the Figure 2 [19].The aim of this review is to assess the Drug resistance that has been reported against anti leishmanial drugs and the studies on drug resistance mechanisms Along with case studies reported to the treatment failures against leishmaniasis.
Figure 2.
Factors leading to treatment failure and drug resistance in Leishmania [19] (HIV: Human immunodeficiency virus, LRV: Leishmania RNA virus, TB: Tuberculosis, AQP: Aquaporin) .
Figure 2.
Factors leading to treatment failure and drug resistance in Leishmania [19] (HIV: Human immunodeficiency virus, LRV: Leishmania RNA virus, TB: Tuberculosis, AQP: Aquaporin) .
2. Treatment Strategies and Challenges
Preventing mortality and morbidity are the main objectives of treatment for all types of leishmaniasis. As there are no immunoprotection and current vaccine therapies against leishmaniasis, there are few compounds and formulations that has Antileishmanial properties but for the primary treatment Pentavalent antimonials are the first drug choice used to treat all forms of leishmaniasis [20]. There are presently no vaccinations or chemoprophylaxis available to prevent leishmaniasis. The only leishmaniasis treatments that have received FDA approval are oral miltefosine for CL, ML, and VL caused by certain species, and intravenous liposomal amphotericin B (L-AmB) for VL [21].

Table 1.
List of approved medication for leishmaniasis [22].
Table 1.
List of approved medication for leishmaniasis [22].
| Drug Name | Generic Name | Drug Class | Brand names | Treatement |
|---|---|---|---|---|
| Pentavalent antimony | sodium stibogluconate(SSG) | pentavalent antimonials | Pentostam® | Visceral, Cutaneous, and Mucosal forms of leishmaniasis and PKDL |
| Amphotericin b | Amphotericin b systemic | Polyenes | Amphocin, Fungizone | Visceral leishmaniasis or Kala-azar, second-line treatment for mucosal leishmaniasis and Cutaneous leishmaniasis |
| Amphotericin b liposomal | Amphotericin b liposomal systemic | Polyenes | AmBisome | Visceral leishmaniasis or Kala-azar, second-line treatment for mucosal leishmaniasis and Cutaneous leishmaniasis |
| Miltefosine | Miltefosine systemic | Anthelmintics | Impavido | Visceral, Cutaneous, and Mucosal forms of leishmaniasis |
| Pentamidine, Pentamidine isethionate, Pentamidine mesylate | Pentamidine systemic | Miscellaneous antibiotics, inhaled anti-infectives | Pentam, Nebupent, Pentam 300, Pentacarinat®, Lomidine® | Visceral, Cutaneous, and Mucosal forms of leishmaniasis |
| Amphotericin b lipid complex | Amphotericin b lipid complex systemic | Polyenes | Abelcet | Visceral leishmaniasis or Kala-azar, second-line treatment for mucosal leishmaniasis and Cutaneous leishmaniasis |
| Paromomycin sulfate, Paromomycin sulfate (15 %) ointment, | Humatin | aminoglycoside | Leshcutan® | Visceral, Cutaneous forms of leishmaniasis |
Sodium stebogluconate (SSG) and meglumine antimoniate, which are pentavelent antimonials, are the first line of treatment initially for leishmaniasis. While effective in other parts of the world, particularly in Africa, their high toxicity, particularly cardiotoxicity, is a significant disincentive. During Stebogluconate therapy, HIV-positive individuals experience more severe side effects, decreased efficacy, and increased mortality [23,24]. From the beginning of the treatment by pentavelent antimonials till 80s in India, treatment failure has been observed due to the resistant of pentavelent antimonials drugs. To overcome these problems Pentamidine were used to treat antimony-resistant VL [25]. But its use is restricted because to well-known toxicities which includes hypotension, heart problems, gastrointestinal adverse effects, diabetes mellitus, and pancreatitis that results in insulin-dependent diabetes [26]. Due to these drawbacks The other drug, polyene antibiotic amphotericin B deoxycholate was widely used for VL and is also advised for the treatment of PKDL in the Indian subcontinent that is resistant to antimonial therapy and recommended over the use of Pentamidine [27]. Even if the therapy works effectively, the side effects, such as nephrotoxicity, myocarditis, and hypokalemia make it necessary to monitor the patient [25].
To overcome these adverse effects of the drugs, Lipid formulations of the drugs, which substitute alternative lipids for deoxycholate, such as liposomal amphotericin B, amphotericin B lipid complex, and amphotericin B cholesterol dispersion, were developed to reduce these side effects. These formulations are quickly absorbed by the liver, spleen, and other organs, concentrating in the reticuloendothelial tissue, which is where the disease occurs in patients with VL. It stays there for a long time, making it possible to administer high dosages of the medication quickly. Nephrotoxicity is reduced since it spares vital organs such as the kidney. A number of lipid formulations of Amphotericin B have been thoroughly investigated for leishmaniasis; of them, only liposomal Amphotericin B (L-AmB) has received US FDA approval. Liposomal amphotericin B dosages can differ according on the area and region [28].
A alkyl phospholipid compound was discovered and developed as an oral medication for the treatment of solid tumors in the early 1980s by two scientific groups—one from Germany investigating antitumor activity and the other from the UK investigating anti-inflammatory properties [29,30]. However, the drug was discontinued due to dose-limiting gastrointestinal adverse events in multiple clinical studies. The compound is Miltefosine now known for its Antileishmanial properties. Because of its excellent oral absorption in mouse models and its superiority over intravenous Pentavalent antimonials in animal models studies [31,32], revealed that Miltefosine is a promising candidate for the treatment of human VL [33].
Paromomycin previously existed as a paromomycin sulfate [34] is an aminoglycoside antibiotic which was originated from the bacterial pathogen Streptomyces rimosus var paromomycinus was also considerd for the treatment of parasitic infestation. It has been established that treating patients with visceral leishmaniasis with paromomycin is safe and effective. This medication is cheap and approved as a first-line substitute when traditional antileishmanial medications are no longer effective.
3. Drug Resistance in Leishmania
Initial drug resistance was reported in the sodium stibogluconate which were first line of the drug to treat leishmaniasis and due to this resistance it has lead to the treatment failure in the patients from endemic regions [35]. As an alternative drug Miltefosine has been used to replace sodium stibogluconate, which was oral drug but from the past few decades Miltefosine showed less effects in the south Asian countries like India [36] and Nepal [37] which were later replace by liposomal Amphotericin B. For Clinical resistance, the problem of resistance in these parasites can arise experimentally for any drug, under stressful condition parasites undergoes for genetic mutation which ultimately helps the parasite to overcome the drug response this is the basic representation for the resistant mechanism but this might not occur all the time for the parasites. So Antileishmanial treatments responds varies accordingly in different regions and the drugs are also recommended according to the different regions.
In the late 1970s, India's sandfly population surge led to a visceral leishmaniasis epidemic, with declining cure rates for antimonial treatments despite increasing dosages and extended treatment durations. Few cases of sodium stibogluconate resistant parasite, these parasites are not even exposed to sodium stibogluconate [38]. Basically Antimony and arsenic which are Group 15 metalloids, exhibit similar structural and chemical properties [39] whereas in the India subcontinent High concentrations of arsenic naturally occurring in groundwater’s have been accumulated by tube wells which have been found in endemic region Bihar [40], where it is believed that 90% of India's VL cases has been reported [41]. If a person from this endemic region who is exposed to arsenic for a long term got infected with VL parasitic infection then these parasites also get easily exposed to arsenic as their presence would be within the lymphoreticular organs [42]. This might result in the emergence of a Leishmania strain resistant to arsenic that would resist antimonial treatment as shown in Figure 3. As this study in Bihar, found a 59% SSG failure rate, with higher risks linked to arsenic-contaminated groundwater. [43].
The diagrammatically explanation of molecular mechanism of drug resistance against antimonials has given in Figure 4. SSG a pentavelent antimonial is a anti-leishmanial compound. Instead of being a single molecule, SSG is a chemically produced combination developed by the reaction of gluconic and stibonic acids [44]. The parasite resists antimonials by modulating its cell influx. Sb(V) is reduced to Sb(III), partially in the host macrophage, and enters via the AQP1 carrier. An unknown mechanism helps Sb(V) enter the parasite, where it’s further reduced Sb(III) and Sb(V) accumulate in promastigote and amastigote forms of Leishmania, but their entry routes differ. Accumulation levels don't correlate with antimony susceptibility, suggesting other factors in drug action. Resistant parasites accumulate less antimony than sensitive ones, but the correlation between accumulation levels and sensitivity in wild-type cells is unclear [45]. Down-regulation of AQP1 is also linked to drug resistance in Indian VL and PKDL isolates, correlating with Sb(III) accumulation, with some exceptions [46] and when AQP1 is overexpressed, the parasites become extremely sensitive to Sb(III) [47]. In India, treatment for visceral leishmaniasis (VL) is hampered by antimony (Sb) insensitivity. In vitro investigations reveal elevated thiols and drug efflux pumps in Sb-resistant parasites. Through a reduction in oxidative stress, this study discovered clinical isolates that have higher thiols and faster regeneration, which contribute to Sb resistance [48]. Ultimately these antimony causes oxidative stress in cells, and resistance arises from the parasite’s ability to manage this stress.
Antimony-resistant parasites show increased intracellular trypanothione, and the levels of increased thiol redox potential which are linked to overexpression of key enzymes in glutathione and polyamine synthesis, namely gamma glutamylcysteine synthetase and ornithine decarboxylase [49]. When it comes to the Leishmania ATP-binding cassette PGPA (P-glycoprotein A) confers arsenite and antimonite resistance by sequestering metal-thiol conjugates, its exact antimony resistance mechanism is unclear [50]
Drug resistance is conferred in another resistant protein of ABC transporter MRPA (ABCC3/PgpA), which sequesters drug-trypanothione conjugates in an organelle close to the flagellar pocket at this site antimonial targets are expected to be absent [50]. At the flagellar pocket, exocytosis is used to eject these conjugates. Furthermore, TSH-antimonial substances are actively effluxed by a surface protein [51]. Overexpression of ABC transporters in Leishmania influences drug efflux and antimony resistance. MRPA, an ABC transporter, is localized in membrane vesicles near the flagellar pocket [52].
Pentamidine resistance protein 1(PRP1) which is a P-glucoprotein/ ATP-binding cassette transporter protein has the ability to provide resistance against pentamidine resistance when overexpressed in Leishmania major [53]. ABCI4 is also an intracellular ATP-binding cassette transporter in L. major, involved in heavy metal export and resistance to antimonial. It reduces mitochondrial toxicity and reactive oxygen species, enhancing parasite replication and drug resistance [54]. Another ATP-binding cassette transporter LABCG2 is linked to resistance by reducing Sb(III) accumulation and aiding drug efflux, contributing to antimony resistance [55].In other study antimony-resistant Leishmania donovani (SbRLD) increases IL-10 and MDR1 levels in infected macrophages. SbRLD's unique glycan, which can be removed, influences this process. SbRLD uses Toll-like receptors to activate pathways leading to IL-10 and MDR1 up-regulation, with IL-10 being crucial for MDR1 induction [56]. Antimony resistance in Leishmania arises from various factors and events, complicating treatment outcomes. Understanding these mechanisms, observed in labs, helps explain the rise and spread of resistance to SSG.
Polyene antibiotic amphotericin B deoxycholate was widely used for VL and is also advised for the treatment of PKDL in the Indian subcontinent that is resistant to antimonial therapy and recommended over the use of Pentamidine [27].As reported Amphotericin B (AmB) binds to ergosterol and episterol in the parasite's membrane [57]. Amphipathic structure of AmB allows the hydrophobic part to interact with membrane lipids while the hydrophilic part creates pores, increasing membrane permeability and leading to cell death. However, some resistant strains of L. donovani and L. mexicana substitute cholesterol-associated sterols for ergosterol in their membrane sterol composition, decreasing the binding affinity of AmB [58,59,60]. These changes also increase membrane fluidity and AmB efflux, due to upregulation of the MDR1 efflux pump, making the parasites more tolerant to oxidative stress. The effectiveness of amphotericin B for treating visceral leishmaniasis in Bihar, India, is at risk due to emerging drug resistance. A resistant Leishmania donovani strain requires an 8-fold higher dose to be lethal compared to a sensitive strain. This resistance is linked to elevated thiol levels, and enhanced thiol metabolic pathways. These factors collectively contribute to resistance, which can be partially reversed using inhibitors targeting thiol metabolism and ABC transporters refer Figure 5. [58].
Miltefosine, an alkyl phospholipid molecule with antileishmanial porperties, has been shown to have treatment failure for L. pneumoniae infections [61] and relapsed cases of VL in Indian sub continent has been increased when Miltefosine was used as a mono-therapy [36]. The clinical isolates of Leishmania donovani which are isolated from both cured and relapsed patients showed similar susceptibility by the in vitro analysis [62] that indicates that treatment failure is not directly related to the parasites intrinsic sensitivity against Miltefosine. The treatment failure in these clinical isolates has showed increase in drug tolerance against anti leishmanial drugs like to amphotericin B (AmB) due to the absence of ergosterol(increased membrane fluidity and reduced AmB binding), infectivity, and resistance to oxidative stress. For AmB resistant strains showed enhanced efflux by up regulating MDR1 (multidrug resistance) efflux pump. Miltefosine also disrupts intracellular Ca2+ homeostasis which can be a significant target for drug action in trypanosomatids [63]. Developing Miltefosine resistance in the isolates of leishmania In vitro has reviled mutations in two genes, ROS3 and MT, which encode the Leishmania miltefosine transporter complex (LdMT) [64] as this complex helps in translocation of phospholipid across the parasite's membrane and is responsible for Miltefosine uptake [65]. Please refer Figure 6.
In the case of amino glycoside antibiotic Paromomycin, a cost-effective antibiotic, is considered among the safest Antileishmanial drugs. It generally causes only mild adverse effects, including injection site pain and cytotoxicity, making it a favorable treatment option for leishmaniasis [66]. The Mode of action along with resistance against Paromomycin has been studied in bacteria but the in the parasite it is not clearly understood. Many studies reported that Paromomycin impairs the mitochondrial activities of Leishmania donovani Promastigotes, leading to a decline in energy supply due to a disturbance in the proton gradient generated by respiration [67]. When it comes to the resistance mechanism Paromomycin (PMM) resistance in Leishmania donovani is associated with altered membrane fluidity, decreased intracellular drug accumulation, increased expression of ABC transporters, and greater tolerance to host defense mechanisms, such as nitrosative stress and complement-mediated lysis. Despite these changes, the PMM-resistant parasites maintain susceptibility to other antileishmanial agents like sodium antimony gluconate and miltefosine [68]. In other resistance mechanism study [69] the Paromomycin is by associating with the parasite’s cell surface, binding to the glycocalyx, and ultimately disrupting mitochondrial function. The drug inhibits protein synthesis in both cytoplasmic and mitochondrial compartments. Additionally, resistance to Paromomycin is linked to reduced drug accumulation and less pronounced effects on membrane potential and protein synthesis, suggesting that resistance involves changes in drug binding and uptake mechanisms. Paromomycin cure rate among the patients has been decreased along with time, in South East Asia, a phase IV trial showed cure rates of over 94% with a systemic dose of 11 mg/kg for 21 days against L. donovani [70,71]. However in 2010, the same dose was insufficient in East Africa, where higher doses of 20 mg/kg or longer treatment periods of 28 days were needed to achieve cure rates up to 84.3% [72,73]. Please refer Figure 7
4. Reported Case Study
Multiple case studies have been reported across the globe where the patient has been not responding to the Antileishmanial treatment. There could be a multiple reason for such treatment failures among the patients which includes Hosts immunological factors, resistance among the parasites, Dose-dependent resistance of the species, Route of drug administration, Inappropriate initial treatment for the patients and in some cases mixed infection between two strains [74]. Multiple cases accordingly has been given in the Table 2.
When it comes to Asian countries, which has declared leishmaniasis as endemic in those regions where multiple treatment failures has been reported. A case study in discusses a 31-year delayed recurrence of leishmaniasis, likely triggered by local trauma and topical steroids. A cutaneous disease caused by Leishmania tropica, parasite appears to persist at the original infection site, reactivating due to changes in the local immune environment. While TGF-β may play a role in reactivation, IL-10 was not detected. The patient responded well to treatment with itraconazole and local sodium stibogluconate, and healing was achieved after stopping steroids. The case suggests that leishmaniasis might never be fully cured but is instead controlled by a balanced immune response involving both CD4 and CD8 T cells. [75]. In India where it contributes 20% for the global VL cases has shown treatment failure with the single drug therapies and due to the co infection with HIV it has became difficult to treat the patients. In a case study reported by S. Patole et.al [76] a patient who has been infected by VL and has a co-infecteion of HIV was initially treated with mono therapies of Miltefosine but eventually the disease relapsed has been showed multiple times, even after different regimens of liposomal Amphotericin B. due to the immune suppression and the synergistic effects of HIV and VL single-drug therapies often fail.
In a case study [77] an 8-year-old Syrian boy experienced lip swelling and lesions over four years where he was diagnosed with Leishmaniasis Recidiva Cutis (LRC). Initially he was treated with intralesional meglumine antimoniate, but the treatment was not efficient and scarring remained with new papules developed later. Later the lesions were improved significantly after a month of treatment with systemic meglumine antimoniate, oral fluconazole, and cryotherapy. Similarly another case study [78] describes a Palestinian Bedouin child who was diagnosed with Leishmaniasis recidivans, a rare form of cutaneous leishmaniasis characterized by chronic, recurring skin lesions. The child underwent multiple treatment rounds with sodium stibogluconate, but relapses occurred, possibly due to therapy non-compliance or drug-resistant strains. Traditional treatments were considered but not pursued. This emphasizes the importance of diagnostic precision and tailored treatments for resistant or recurring leishmaniasis cases.
A case study [79] where a visceral leishmaniasis (VL) relapses in a patient after Miltefosine treatment is reported. The patient initially responded well to the 28-day Miltefosine course, showing no detectable Leishmania upon discharge. However, ten months later, symptoms returned, including high fever and splenomegaly. Diagnostic tests confirmed VL relapse, prompting treatment with Amphotericin B, which led to complete recovery. This case highlights the potential for VL relapse even after full Miltefosine treatment. In other case study [80] an 80-year-old immunosuppressed man diagnosed with visceral leishmaniasis (VL) 15 years after exposure. Despite receiving standard treatment with liposomal Amphotericin B, his condition deteriorated, ultimately leading to death. The case emphasizes the unusual long latency of VL in a non-endemic area, challenges in diagnosis due to atypical presentation, and treatment failure with Amphotericin B. The report suggests considering pentavalent antimony as an alternative treatment for cases resistant to Amphotericin B.
In South America, Brazil accounts for over 99% of the estimated 3,500 annual cases in Latin America. While the number of cases remains stable, the spread is extending southwest across the continent [5]. Multiple case reports has been reported in South America where, In one such case report [81] detailing the failure of standard-dose liposomal amphotericin B (L-AmB) treatment for a 58-year-old Japanese man with New World cutaneous leishmaniasis (NWCL) caused by Leishmania braziliensis. The patient developed a cutaneous ulcer after traveling in Venezuela. Initial treatment with L-AmB (3 mg/kg/day) for 6 days was ineffective, leading to ulcer persistence and later expansion despite subsequent treatment with fluconazole. Even after the successful treatment with Antileishmanial drugs the reoccurrence chances has been increased in latin American countries, where one of the case study on Leishmaniasis recidiva cutis (LRC) [82], a recurrent form of cutaneous leishmaniasis (CL) previously thought to occur only in Old World cases. The study reports seven instances of LRC in French Guiana among military personnel who were treated for CL caused by Leishmania guyanensis. Although initial treatment with pentamidine injections cured the lesions, the disease recurred within 3-6 months, manifesting as new lesions around healed scars.
Reoccurrence of the infection can’t be predicted even after the complete treatment due to the ineffective drugs, few of the parasites enters the latent stage in spleenocytes or in hepatocytes they may be inactive but the chances of reoccurrence of this parasites is high. In a case study [83] of recurrent cutaneous leishmaniasis (RCL) an 18-year-old male from northeastern Brazil. The patient initially developed an ulcer on his thigh, which healed after treatment with N-methylglucamine. However, two years later, verrucous nodules appeared around the healed scar, indicating a recurrence of the disease. A positive culture confirmed the diagnosis of RCL, and the causative species, Leishmania braziliensis, was identified as endemic to the region. The patient was treated with a combination of N-methylglucamine and pentoxifylline, which led to a long-term clinical cure over a three-year follow-up.
In patients with normal immune function Relapses are rare but are common in those with compromised immunity, especially in cases of AIDS and Leishmania RNA virus. As the patients with compromised immune system and co-infection with HIV has been difficult to treat and led to multiple treatment failure or multiple relapses. As similar case report [84] which was the first documented instance in Brazil of a co-infection involving Leishmania amazonensis, the causative agent of diffuse cutaneous leishmaniasis (DCL), and HIV. The patient, a 46-year-old man from Maranhão, Brazil, initially presented with a non-healing ulcerative lesion and later developed disseminated erythematous nodules across his body. Diagnosis confirmed L. amazonensis as the pathogen, and he was subsequently diagnosed with HIV, with a low CD4+ count indicating a compromised immune system. Treatment included antiretrovirals alongside leishmaniasis therapy with liposomal amphotericin B (AmB-L) and Glucantime®, but the patient experienced multiple relapses. In a other case report describes a 32-year-old Brazilian man with cutaneous leishmaniasis (CL) caused by Leishmania (Viannia) naiffi, acquired during military training in the Amazon [85]. The patient’s infection was unusual, as it did not respond to standard pentamidine treatment, which typically succeeds in cases of L. naiffi. The lesion was surgically removed for resolution, and testing later identified the presence of the Leishmania RNA virus (LRV) within the isolated parasites. The presence of LRV, which is known to increase parasite virulence in other Leishmania species, might explain the patient’s resistance to therapy.
Table 2.
Treatment failure case reports among the 5 continents: CL- cutaneous leishmaniasis; VL- visceral leishmaniasis; MCL- mucocutaneous leishmaniasis; DCL- diffuse cutaneous leishmaniasis; FLU- fluconazole; GLU- meglumine antimoniate (Glucantime®) ; SSsodium stiboglucanate (Pentostan®); PENT- pentamidine; PAR- paromomycin; AmB- amphotericin B; L-AmB- liposomal amphotericin B; MIL- miltefosine; IL- intralesional; IM- intramuscular.
Table 2.
Treatment failure case reports among the 5 continents: CL- cutaneous leishmaniasis; VL- visceral leishmaniasis; MCL- mucocutaneous leishmaniasis; DCL- diffuse cutaneous leishmaniasis; FLU- fluconazole; GLU- meglumine antimoniate (Glucantime®) ; SSsodium stiboglucanate (Pentostan®); PENT- pentamidine; PAR- paromomycin; AmB- amphotericin B; L-AmB- liposomal amphotericin B; MIL- miltefosine; IL- intralesional; IM- intramuscular.
| S.no | Region | Patients | Clinical Manifestation | Species | Unsuccessful Treatment | Proposed Mechanisms for Failure/Relapse | Reference |
|---|---|---|---|---|---|---|---|
| 1 | Asia | Male(6) | CL(3), VL(3) | L. tropica (CL), L. donovani (VL) | SS, AmB, AmB-L, MIL, GLU IL and GLU IM | CL- Hosts immunological factors and Parasite Resistance, VL- Hosts immunological factors and Parasite Resistance | [75,76,77,78,79,80] |
| 2 | South America | Male(21), Female (2) | CL(15), VL(6), MCL(1), DCL(1) | L. guyanensis (CL), L. panamensis (CL), L. naiffi (CL) L. tropica (CL), L. braziliensis (CL), L. infantum (VL), L. braziliensis (MCL), L. amazonensis (DCL) | SS, AmB, AmB-L, MIL, GLU IL and GLU IM, AmB e PENT / GLU e AmB, PENT (IL or IM) | CL- Dose-dependent resistance of the species, Route of drug administration, Inappropriate initial treatment, Presence of LRV virus, VL- Not Reported, MCL- Host immunological factors, DCL- Host immunological factors | [81,82,83,84,85,86,87,88,89,90], |
| 3 | North America | Male (1) | VL(1) | NR | GLU | VL- Inappropriate initial treatment | [91] |
| 4 | Europe | Male(4), Female (6) | CL(2), VL(8) | L. infantum (VL), L. tropica (CL), | L-AmB e AmB lipid complex, MIL e AmB, GLU | CL- Inappropriate initial treatment , VL- Host immunological factors, Mixed infection by two strains | [88,92,93,94,95,96,97] |
| 5 | Africa | Male(1), Female (1) | VL(2) | L. infantum (VL) | GLU, AmB IV, GLU / L-AmB, L-AmB, L-AmB + MIL / L-AmB, L-AmB + MIL / L-AmB and GLU / L-AmB | VL- Host immunological factors | [97] |
Multiple cases of treatment failure among children under five has also been reported in Colombia [87]. Two cases such cases of visceral leishmaniasis (VL) in Colombia, Resistant was the standard treatment with meglumine antimoniate (Glucantime®) has been reported. Usually standard first-line treatment involves pentavalent antimonial compounds, but those two children have showed no response to Glucantime® or pentamidine treatments. The report emphasizes the need for alternative treatments due to rising resistance and suggests further research into effective, accessible therapies for endemic regions. Multiple drug treatments has also been failed among the patients in Brazil [90] where two cases of recurrent kala-azar (visceral leishmaniasis) by Leishmania infantum was reported. Despite attempts with standard treatments (pentavalent antimonials, liposomal amphotericin B, and pentamidine), both patients experienced recurring symptoms due to drug-resistant kala-azar and severe splenomegaly with hypersplenism, causing frequent hospitalizations
When it comes to European countries, only southern countries are impacted, with a high prevalence of asymptomatic human carriers of L. infantum, indicating that this parasite poses a latent public health risk [98]. Multiple cases of treatment failure among immunosuppressed patients has been reported in European countries where A 52-year-old immunosuppressed Belgian woman [92] with severe rheumatoid arthritis was diagnosed with visceral leishmaniasis after a bone marrow biopsy revealed Leishman-Donovan (LD) bodies. Initial treatment with liposomal Amphotericin B succeeded, but she later developed cutaneous leishmaniasis, which was managed with Amphotericin-B lipid complex. She subsequently experienced relapsing cutaneous lesions and rapidly enlarging lymph nodes, confirmed as leishmaniasis. Multiple treatments, including Miltefosine, Amphotericin B, and N-methyl-glucamine antimoniate, were attempted. Later, a recurrent bone marrow infection was treated with Paromomycin and Miltefosine. Two years later, she died from leukemia with severe nasal mucosal destruction. Leishmania infantum was identified as the causative agent by PCR. As discussed few of the parasites enters the latent stage in spleenocytes or in hepatocytes, parasites may be inactive but the chances of reoccurrence of this parasites is high, similarly in a case study of 64-year-old [93] who was infected with cutaneous leishmaniasis 22 years ago treated partially with antimonies. The lesions became disfiguring over time, worsening in summer, leading her to seek medical help. Biopsy showed tuberculoid granulomas and a few Leishmania organisms, identified as Leishmania tropica by PCR. She was diagnosed with Leishmaniasis recidiva cutis (LRC).
A therapeutic failure due to mixed infection with two different strains of leishmaniasis has also been a concern, A study has been reported [94], where of therapeutic failure in a visceral leishmaniasis patient without HIV was linked to a mixed infection with two different Leishmania infantum zymodemes: the rare MON-98, reported for the first time in Greece, and the more common MON-1 from the Mediterranean region. The strains were isolated from two bone marrow samples taken before and 20 days after treatment, as the patient showed no clinical improvement. The MON-98 and MON-1 strains displayed different behaviors and sensitivities to meglumine antimoniate, both in vitro and in vivo. Mixed infections with distinct Leishmania strains could account for variations in disease progression and potential treatment failures in some patients. In 2001, a 4-year-old girl from an area endemic for Leishmania infantum in France developed juvenile idiopathic arthritis (JIA) and uveitis. She received immunosuppressive treatments, including prednisolone and anti-TNFα therapies (etanercept, then infliximab). In 2005, after several infliximab doses, she developed visceral leishmaniasis (VL) confirmed by bone marrow examination and PCR. Treatment with liposomal amphotericin B resolved VL, but prophylactic therapy was discontinued due to side effects. In 2007, she developed a nasal granuloma containing L. infantum parasites, confirmed by biopsy and PCR, but no systemic relapse occurred [95]. In another case study, An 87-year-old woman with a persistent erythematous forehead lesion was diagnosed with leishmaniasis after histopathological confirmation of amastigotes. Initial treatments with rifampicin and topical paromomycin failed which may be due to resistant parasites or response of a patient to the drugs later Intralesional therapy with n-methylglucamine antimoniate over two months the patient was cured [96]. In other case study of treatement failure a 44-year-old man from southern France with a history of Hodgkin's disease and splenectomy developed visceral leishmaniasis (VL), Bone marrow smears revealed Leishmania amastigotes and confirmed by positive cultures and serological tests, the isolates were identified as Leishmania infantum MON-1. Despite multiple treatments, including amphotericin B, meglumine antimoniate, and pentamidine, some cultures remained intermittently positive over months. Eventually, blood and bone marrow cultures turned negative, though lymph node cultures remained positive [88]. Similarly a 33-year-old pregnant woman from central France presented with pancytopenia and cervical lymphadenopathy was confirmed by Leishmania infantum infection.. She was treated with liposomal amphotericin B, which normalized her blood counts but caused transient skin rashes. Post-treatment, residual lymph node lesions contained Leishmania amastigotes [88]. A four cases of visceral leishmaniasis, including one immunocompetent and three immunosuppressed patients, where the disease became unresponsive or relapsed after standard treatment with liposomal amphotericin B. These cases highlight the challenges of treating visceral leishmaniasis (VL) in immunosuppressed patients [97]. A 58-year-old kidney transplant recipient experienced multiple relapses despite liposomal amphotericin B (L-AmB) and adjunct therapieS. A 15-month-old infant and a 37-year-old HIV-positive male also experienced VL relapses but achieved remission through combined therapies, including miltefosine and meglumine antimoniate. Lastly, a 75-year-old HIV-positive patient with persistent VL and splenomegaly achieved resolution after prolonged meglumine antimoniate treatment. These cases underscore the importance of tailored treatments, integrating combination therapies and immunosuppressive management, to achieve sustained parasitological cure in complex VL cases.
9. Conclusion
As Leishmaniasis continues to be a major parasitic disease globally, especially impacting vulnerable populations in endemic regions. Although drugs like Amphotericin B, Miltefosine, Paromomycin, and pentavalent antimonials have greatly enhanced treatment efficacy, the rise of drug resistance presents a significant challenge to global health efforts. This review explores the diverse mechanisms behind drug resistance in Leishmania species, including changes in drug transport, efflux pump activity, genetic mutations, and metabolic adaptations. These resistance mechanisms collectively reduce the effectiveness of current treatments, complicating the management and control of the disease.
Through case studies of treatment failures, it becomes evident that drug resistance in leishmaniasis is not only a biological phenomenon but also a consequence of systemic issues such as inappropriate drug use, inconsistent treatment regimens, and socio-economic factors in endemic areas. For example, cases of relapses and persistent infections despite treatment with liposomal amphotericin B or miltefosine underscore the urgent need for more therapeutic approaches and improved healthcare infrastructure. These treatment failures highlight gaps in our understanding of host-parasite dynamics, immunosuppression, and drug bioavailability, further complicating the clinical management of resistant Leishmania strains. The evidence presented in this review underscores the critical need for a multidisciplinary approach to tackle antileishmanial drug resistance. Strengthening pharmacovigilance and treatment monitoring systems is imperative to detect early signs of resistance and guide policy adaptations. Concurrently, research efforts should focus on developing new drugs, repurposing existing ones, and identifying synergistic drug combinations that can overcome resistance mechanisms. Moreover, exploring immunomodulatory therapies and vaccines could provide a complementary strategy to bolster host defenses against Leishmania infections.
Equally important is addressing the socio-economic factors that perpetuate the spread and severity of leishmaniasis. Enhancing access to healthcare, ensuring the availability of affordable and effective treatments, and implementing community-based awareness campaigns are pivotal to reducing the burden of the disease. Collaborative efforts between governments, global health organizations, and researchers will be critical to achieving these goals. In conclusion, the fight against leishmaniasis demands a comprehensive and integrated approach, balancing scientific innovation with public health initiatives. Understanding the mechanisms of drug resistance and learning from case studies of treatment failures provide valuable insights into the complexities of the disease. By leveraging these insights, the global health community can work toward developing sustainable solutions that not only curb drug resistance but also improve the overall outcomes for patients suffering from this neglected tropical disease. While significant challenges remain, the collective efforts of the scientific and medical communities offer hope for a future where leishmaniasis is effectively managed, if not eradicated.
References
- Inceboz, T.; Inceboz, T. , “Epidemiology and Ecology of Leishmaniasis,” Curr. Top. Neglected Trop. Dis., Oct. 2019. [CrossRef]
- “Leishmaniasis.” https://www.who.int/news-room/fact-sheets/detail/leishmaniasis (accessed Jan. 31, 2024).
- “On the presence of peculiar parasitic organisms in the tissue of a specimen of Delhi boil | WorldCat.org.” https://search.worldcat.org/title/on-the-presence-of-peculiar-parasitic-organisms-in-the-tissue-of-a-specimen-of-delhi-boil/oclc/11826455 (accessed Jan. 31, 2024).
- Ruiz-Postigo, J.A.; et al. “Global leishmaniasis surveillance: 2019-2020, a baseline for the 2030 roadmap/Surveillance mondiale de la leishmaniose: 2019-2020, une periode de reference pour la feuille de route a l’horizon 2030.,” Wkly. Epidemiol. Rec., vol. 96, no. 35, pp. 401–420, Sep. 2021, Accessed: Feb. 22, 2024. [Online]. Available: https://go.gale.com/ps/i.do?p=HRCA&sw=w&issn=00498114&v=2. 6752. [Google Scholar]
- Burza, S.; Croft, S.L.; Boelaert, M. , “Leishmaniasis,” Lancet, vol. 392, no. 10151, pp. 951–970, Sep. 2018. [CrossRef]
- Reithinger, R.; Dujardin, J.C.; Louzir, H.; Pirmez, C.; Alexander, B.; Brooker, S. , “Cutaneous leishmaniasis,” Lancet Infect. Dis., vol. 7, no. 9, pp. 581–596, Sep. 2007. [CrossRef]
- Desjeux, P.; et al. “Leishmaniasis,” Nat. Rev. Microbiol., vol. 2, no. 9, pp. 692–693, Sep. 2004. [CrossRef]
- “Cutaneous and Mucosal Leishmaniasis - PAHO/WHO | Pan American Health Organization.” https://www.paho.org/en/topics/leishmaniasis/cutaneous-and-mucosal-leishmaniasis (accessed Feb. 22, 2024).
- Sangueza, O.P.; Sangueza, J.M.; Stiller, M.J.; Sangueza, P. , “Mucocutaneous leishmaniasis: A clinicopathologic classification,” J. Am. Acad. Dermatol., vol. 28, no. 6, pp. 927–932, Jun. 1993. [CrossRef]
- Andrade-Narváez, F.J.; Vargas-González, A.; Canto-Lara, S.B.; Damián-Centeno, A.G. , “Clinical picture of cutaneous leishmaniases due to Leishmania (Leishmania) mexicana in the Yucatan peninsula, Mexico,” Mem. Inst. Oswaldo Cruz, vol. 96, no. 2, pp. 163–167, 2001. [CrossRef]
- Sunter, J.; Gull, K. , “Shape, form, function and Leishmania pathogenicity: from textbook descriptions to biological understanding,” Open Biol., vol. 7, no. 9, 2017. [CrossRef]
- Peer, G.D.G.; et al. “A Systematic Assessment of Leishmania donovani Infection in Domestic and Wild Animal Reservoir Hosts of Zoonotic Visceral Leishmaniasis in India,” Microbiol. Res. 2024, Vol. 15, Pages 1645-1654, vol. 15, no. 3, pp. 1645–1654, Aug. 2024. [CrossRef]
- Peters, N.C.; et al. “In vivo imaging reveals an essential role for neutrophils in leishmaniasis transmitted by sand flies,” Science, vol. 321, no. 5891, pp. 970–974, Aug. 2008. [CrossRef]
- Stuart, K.; et al. “Kinetoplastids: related protozoan pathogens, different diseases,” J. Clin. Invest., vol. 118, no. 4, pp. 1301–1310, Apr. 2008. [CrossRef]
- Teixeira, D.E.; Benchimol, M.; Rodrigues, J.C.F.; Crepaldi, P.H.; Pimenta, P.F.P.; de Souza, W. , “The Cell Biology of Leishmania: How to Teach Using Animations,” PLoS Pathog., vol. 9, no. 10, Oct. 2013. [CrossRef]
- Teixeira, D.E.; Benchimol, M.; Rodrigues, J.C.F.; Crepaldi, P.H.; Pimenta, P.F.P.; de Souza, W. , “The Cell Biology of Leishmania: How to Teach Using Animations,” PLoS Pathog., vol. 9, no. 10, Oct. 2013. [CrossRef]
- Peer, G.D.G.; et al. “Exploration of Antileishmanial Compounds Derived from Natural Sources,” Antiinflamm. Antiallergy. Agents Med. Chem., vol. 23, Jan. 2024. [CrossRef]
- Capela, R.; Moreira, R.; Lopes, F. , “An Overview of Drug Resistance in Protozoal Diseases,” Int. J. Mol. Sci. 2019, Vol. 20, Page 5748, vol. 20, no. 22, p. 5748, Nov. 2019. [CrossRef]
- Ponte-Sucre, A.; et al. “Drug resistance and treatment failure in leishmaniasis: A 21st century challenge,” PLoS Negl. Trop. Dis., vol. 11, no. 12, p. e0006052, Dec. 2017. [CrossRef]
- “Current Treatment of Leishmaniasis: A Review.” https://benthamopen.com/ABSTRACT/TOANTIMJ-1-9 (accessed Jun. 18, 2022).
- Aronson, N.; et al. “Diagnosis and Treatment of Leishmaniasis: Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA) and the American Society of Tropical Medicine and Hygiene (ASTMH),” Am. J. Trop. Med. Hyg., vol. 96, no. 1, p. 24, Jan. 2017. [CrossRef]
- “List of 14 Leishmaniasis Medications Compared - Drugs.com.” https://www.drugs.com/condition/leishmaniasis.html?submitted=true&category_id=&drugNameType=generics&approvalStatus=approved&rxStatus=all#sortby (accessed Mar. 26, 2024).
- Ritmeijer, K.; et al. “A comparison of miltefosine and sodium stibogluconate for treatment of visceral leishmaniasis in an Ethiopian population with high prevalence of HIV infection,” Clin. Infect. Dis., vol. 43, no. 3, pp. 357–364, Aug. 2006. [CrossRef]
- Diro, E.; Lynen, L.; Mohammed, R.; Boelaert, M.; Hailu, A.; van Griensven, J. , “High Parasitological Failure Rate of Visceral Leishmaniasis to Sodium Stibogluconate among HIV Co-infected Adults in Ethiopia,” PLoS Negl. Trop. Dis., vol. 8, no. 5, p. e2875, 2014. [CrossRef]
- Chakravarty, J.; Sundar, S. , “Current and emerging medications for the treatment of leishmaniasis,” Expert Opin. Pharmacother., vol. 20, no. 10, pp. 1251–1265, Jul. 2019. [CrossRef]
- “Changing response to diamidine compounds in cases of kala-azar unresponsive to antimonial - PubMed.” https://pubmed.ncbi.nlm.nih.gov/1938817/ (accessed Jul. 29, 2024).
- Mishra, M.; Biswas, U.K.; Jha, D.N.; Khan, A.B. , “Amphotericin versus pentamidine in antimony-unresponsive kala-azar,” Lancet, vol. 340, no. 8830, pp. 1256–1257, Nov. 1992. [CrossRef]
- Sundar, S.; Chakravarty, J.; Agarwal, D.; Rai, M.; Murray, H.W. , “Single-dose liposomal amphotericin B for visceral leishmaniasis in India,” N. Engl. J. Med., vol. 362, no. 6, pp. 504–512, Feb. 2010. [CrossRef]
- Croft, S.L.; Engel, J. , “Miltefosine--discovery of the antileishmanial activity of phospholipid derivatives,” Trans. R. Soc. Trop. Med. Hyg., vol. 100 Suppl 1, no. SUPPL. 1, Dec. 2006. [CrossRef]
- Dorlo, T.P.C.; Balasegaram, M.; Beijnen, J.H.; de vries, P.J. , “Miltefosine: a review of its pharmacology and therapeutic efficacy in the treatment of leishmaniasis,” J. Antimicrob. Chemother., vol. 67, no. 11, pp. 2576–2597, Nov. 2012. [CrossRef]
- Kuhlencord, A.; Maniera, T.; Eibl, H.; Unger, C. , “Hexadecylphosphocholine: oral treatment of visceral leishmaniasis in mice,” Antimicrob. Agents Chemother., vol. 36, no. 8, pp. 1630–1634, 1992. [CrossRef]
- Croft, S.L.; Neal, R.A.; Pendergast, W.; Chan, J.H. , “The activity of alkyl phosphorylcholines and related derivatives against Leishmania donovani,” Biochem. Pharmacol., vol. 36, no. 16, pp. 2633–2636, Aug. 1987. [CrossRef]
- Sunyoto, T.; Potet, J.; Boelaert, M. , “Why miltefosine—a life-saving drug for leishmaniasis—is unavailable to people who need it the most,” BMJ Glob. Heal., vol. 3, no. 3, p. 709, Nov. 2018. [CrossRef]
- Wiwanitkit, V. , “Interest in paromomycin for the treatment of visceral leishmaniasis (kala-azar),” Ther. Clin. Risk Manag., vol. 8, p. 323, 2012. [CrossRef]
- Ponte-Sucre, A.; et al. “Drug resistance and treatment failure in leishmaniasis: A 21st century challenge,” PLoS Negl. Trop. Dis., vol. 11, no. 12, Dec. 2017. [CrossRef]
- Sundar, S.; et al. “Efficacy of miltefosine in the treatment of visceral leishmaniasis in India after a decade of use,” Clin. Infect. Dis., vol. 55, no. 4, pp. 543–550, Aug. 2012. [CrossRef]
- Rijal, S.; et al. “Increasing failure of miltefosine in the treatment of Kala-azar in Nepal and the potential role of parasite drug resistance, reinfection, or noncompliance,” Clin. Infect. Dis., vol. 56, no. 11, pp. 1530–1538, Jun. 2013. [CrossRef]
- Zerpa, O.; Padrón-Nieves, M.; Ponte-Sucre, A. , “American Tegumentary Leishmaniasis,” Drug Resist. Leishmania Parasites Consequences, Mol. Mech. Possible Treat., pp. 177–191, Aug. 2018. [CrossRef]
- Yan, S.; Jin, L.; Sun, H. , “51Sb Antimony in Medicine,” Met. Drugs Met. Diagnostic Agents Use Met. Med., pp. 441–461, Dec. 2005. [CrossRef]
- Chakraborti, D.; et al. “Arsenic groundwater contamination in Middle Ganga Plain, Bihar, India: a future danger?,” Environ. Health Perspect., vol. 111, no. 9, p. 1194, Jul. 2003. [CrossRef]
- “Visceral leishmaniasis (kala-azar): challenges ahead - PubMed.” https://pubmed.ncbi.nlm.nih.gov/16778314/ (accessed Aug. 02, 2024).
- Mazumder, D.N.G. , “Effect of chronic intake of arsenic-contaminated water on liver,” Toxicol. Appl. Pharmacol., vol. 206, no. 2, pp. 169–175, Aug. 2005. [CrossRef]
- Perry, M.R.; et al. “Visceral Leishmaniasis and Arsenic: An Ancient Poison Contributing to Antimonial Treatment Failure in the Indian Subcontinent?”. [CrossRef]
- Roychoudhury, J. ; N. A.-I. journal of biochemistry; undefined 2008, “Sodium stibogluconate: Therapeutic use in the management of leishmaniasis,” Repos. Roychoudhury, N AliIndian J. Biochem. Biophys. 2008•repository.ias.ac.in, vol. 45, pp. 16–22, 2008, Accessed: Aug. 05, 2024. [Google Scholar]
- Brochu, C.; et al. “Antimony uptake systems in the protozoan parasite Leishmania and accumulation differences in antimony-resistant parasites,” Antimicrob. Agents Chemother., vol. 47, no. 10, pp. 3073–3079, Oct. 2003. [CrossRef]
- Mandal, S.; Maharjan, M.; Singh, S.; Chatterjee, M.; Madhubala, R. , “Assessing aquaglyceroporin gene status and expression profile in antimony-susceptible and -resistant clinical isolates of Leishmania donovani from India,” J. Antimicrob. Chemother., vol. 65, no. 3, pp. 496–507, Mar. 2010. [CrossRef]
- Marquis, N.; Gourbal, B.; Rosen, B.P.; Mukhopadhyay, R.; Ouellette, M. , “Modulation in aquaglyceroporin AQP1 gene transcript levels in drug-resistant Leishmania,” Mol. Microbiol., vol. 57, no. 6, pp. 1690–1699, Sep. 2005. [CrossRef]
- Mandal, G.; Wyllie, S.; Singh, N.; Sundar, S.; Fairlamb, A.H.; Chatterjee, M. , “Increased levels of thiols protect antimony unresponsive Leishmania donovani field isolates against reactive oxygen species generated by trivalent antimony,” Parasitology, vol. 134, no. Pt 12, p. 1679, Nov. 2007. [CrossRef]
- Croft, S.L.; Sundar, S.; Fairlamb, A.H. , “Drug resistance in leishmaniasis,” Clin. Microbiol. Rev., vol. 19, no. 1, pp. 111–126, Jan. 2006. [CrossRef]
- Légaré, D.; et al. “The Leishmania ATP-binding Cassette Protein PGPA Is an Intracellular Metal-Thiol Transporter ATPase,” J. Biol. Chem., vol. 276, no. 28, pp. 26301–26307, Jul. 2001. [CrossRef]
- Dey, S.; Ouellette, M.; Lightbody, J.; Papadopoulou, B.; Rosen, B.P. , “An ATP-dependent As(III)-glutathione transport system in membrane vesicles of Leishmania tarentolae.,” Proc. Natl. Acad. Sci. U. S. A., vol. 93, no. 5, p. 2192, Mar. 1996. [CrossRef]
- Ashutosh, *!!! REPLACE !!!*; Sundar, S.; Goyal, N. Ashutosh; Sundar, S.; Goyal, N., “Molecular mechanisms of antimony resistance in Leishmania,” J. Med. Microbiol., vol. 56, no. Pt 2, pp. 143–153, Feb. 2007. [CrossRef]
- Coelho, A.C.; Beverley, S.M.; Cotrim, P.C. , “Functional genetic identification of PRP1, an ABC transporter superfamily member conferring pentamidine resistance in Leishmania major,” Mol. Biochem. Parasitol., vol. 130, no. 2, pp. 83–90, Aug. 2003. [CrossRef]
- Manzano, J.I.; García-Hernández, R.; Castanys, S.; Gamarro, F. , “A new ABC half-transporter in Leishmania major is involved in resistance to antimony,” Antimicrob. Agents Chemother., vol. 57, no. 8, pp. 3719–3730, Aug. 2013. [CrossRef]
- Perea, A.; Manzano, J.I.; Castanys, S.; Gamarro, F. , “The LABCG2 Transporter from the Protozoan Parasite Leishmania Is Involved in Antimony Resistance,” Antimicrob. Agents Chemother., vol. 60, no. 6, pp. 3489–3496, Jun. 2016. [CrossRef]
- Mukherjee, B.; et al. “Antimony-resistant but not antimony-sensitive Leishmania donovani up-regulates host IL-10 to overexpress multidrug-resistant protein 1,” Proc. Natl. Acad. Sci. U. S. A., vol. 110, no. 7, pp. E575–E582, Feb. 2013. [CrossRef]
- Sundar, S.; Chakravarty, J. , “Liposomal amphotericin B and leishmaniasis: Dose and response,” J. Glob. Infect. Dis., vol. 2, no. 2, p. 159, 2010. [CrossRef]
- Purkait, B.; et al. “Mechanism of amphotericin B resistance in clinical isolates of Leishmania donovani,” Antimicrob. Agents Chemother., vol. 56, no. 2, pp. 1031–1041, Feb. 2012. [CrossRef]
- Mwenechanya, R.; et al. “Sterol 14α-demethylase mutation leads to amphotericin B resistance in Leishmania mexicana,” PLoS Negl. Trop. Dis., vol. 11, no. 6, p. e0005649, Jun. 2017. [CrossRef]
- Bansal, R.; Sen, S.S.; Muthuswami, R.; Madhubala, R. , “Stigmasterol as a potential biomarker for amphotericin B resistance in Leishmania donovani,” J. Antimicrob. Chemother., vol. 75, no. 4, pp. 942–950, Apr. 2020. [CrossRef]
- del M, M.; Cossio, A.; Velasco, C.; Osorio, L. , “Risk factors for therapeutic failure to meglumine antimoniate and miltefosine in adults and children with cutaneous leishmaniasis in Colombia: A cohort study,” PLoS Negl. Trop. Dis., vol. 11, no. 4, p. e0005515, Apr. 2017. [CrossRef]
- Prajapati, V.K.; et al. “In vitro Susceptibility of Leishmania donovani to Miltefosine in Indian Visceral Leishmaniasis,” Am. J. Trop. Med. Hyg., vol. 89, no. 4, pp. 750–754, Oct. 2013. [CrossRef]
- Pinto-Martinez, A.K.; Rodriguez-Durán, J.; Serrano-Martin, X.; Hernandez-Rodriguez, V.; Benaim, G. , “Mechanism of action of miltefosine on Leishmania donovani involves the impairment of acidocalcisome function and the activation of the sphingosine-dependent plasma membrane Ca 2+ channel,” Antimicrob. Agents Chemother., vol. 62, no. 1, Jan. 2018. [CrossRef]
- Pérez-Victoria, F.J.; Sánchez-Cañete, M.P.; Castanys, S.; Gamarro, F. , “Phospholipid translocation and miltefosine potency require both L. donovani miltefosine transporter and the new protein LdRos3 in Leishmania parasites,” J. Biol. Chem., vol. 281, no. 33, pp. 23766–23775, Aug. 2006. [CrossRef]
- Khanra, S.; Sarraf, N.R.; Das, A.K.; Roy, S.; Manna, M. , “Miltefosine Resistant Field Isolate From Indian Kala-Azar Patient Shows Similar Phenotype in Experimental Infection,” Sci. Reports 2017 71, vol. 7, no. 1, pp. 1–12, Sep. 2017. [CrossRef]
- “Control of the leishmaniases WHO TRS n° 949.” https://www.who.int/publications/i/item/WHO-TRS-949 (accessed Sep. 19, 2024).
- Maarouf, M.; De Kouchkovsky, Y.; Brown, S.; Petit, P.X.; Robert-Gero, M. , “In VivoInterference of Paromomycin with Mitochondrial Activity ofLeishmania,” Exp. Cell Res., vol. 232, no. 2, pp. 339–348, 97. 19 May. [CrossRef]
- Bhandari, V.; Sundar, S.; Dujardin, J.C.; Salotra, P. , “Elucidation of cellular mechanisms involved in experimental paromomycin resistance in leishmania donoVani,” Antimicrob. Agents Chemother., vol. 58, no. 5, pp. 2580–2585, 2014. [CrossRef]
- Jhingran, A.; Chawla, B.; Saxena, S.; Barrett, M.P.; Madhubala, R. , “Paromomycin: Uptake and resistance in Leishmania donovani,” Mol. Biochem. Parasitol., vol. 164, no. 2, pp. 111–117, Apr. 2009. [CrossRef]
- Sinha, P.K.; et al. “Phase 4 Pharmacovigilance Trial of Paromomycin Injection for the Treatment of Visceral Leishmaniasis in India,” J. Trop. Med., vol. 2011, 2011. [CrossRef]
- Sundar, S.; Chakravarty, J. , “Paromomycin in the treatment of leishmaniasis,” Expert Opin. Investig. Drugs, vol. 17, no. 5, pp. 787–794, 08. 20 May. [CrossRef]
- Musa, A.M.; et al. “Paromomycin for the Treatment of Visceral Leishmaniasis in Sudan: A Randomized, Open-Label, Dose-Finding Study,” PLoS Negl. Trop. Dis., vol. 4, no. 10, p. e855, Oct. 2010. [CrossRef]
- Hailu, A.; et al. “Geographical Variation in the Response of Visceral Leishmaniasis to Paromomycin in East Africa: A Multicentre, Open-Label, Randomized Trial,” PLoS Negl. Trop. Dis., vol. 4, no. 10, p. e709, Oct. 2010. [CrossRef]
- de A, G.; et al. “Systematic Review of Treatment Failure and Clinical Relapses in Leishmaniasis from a Multifactorial Perspective: Clinical Aspects, Factors Associated with the Parasite and Host,” Trop. Med. Infect. Dis., vol. 8, no. 9, Sep. 2023. [CrossRef]
- Marovich, M.A.; et al. “Leishmaniasis recidivans recurrence after 43 years: A clinical and immunologic report after successful treatment,” Clin. Infect. Dis., vol. 33, no. 7, pp. 1076–1079, Oct. 2001. [CrossRef]
- Patole, S.; Burza, S.; Varghese, G.M. , “Multiple relapses of visceral leishmaniasis in a patient with HIV in India: a treatment challenge,” Int. J. Infect. Dis., vol. 25, 2014. [CrossRef]
- Ekiz, Ö.; Rifaio, E.N.; Şen, B.B. ; G. C¸ulha; Özgür, T.; Do, A.C., “Leishmaniasis recidiva cutis of the lips mimicking granulomatous cheilitis,” Indian J. Dermatol., vol. 60, no. 2, p. 216, Apr. 2015.
- Al-Jawabreh, A. ; A. N.-Skin. D. for the; undefined 2007, “Leishmaniasis recidivans in a Palestinian Bedouin child,” Wiley Online Libr. Al-Jawabreh, A NasereddinSKINmed Dermatology Clin. 2007•Wiley Online Libr., vol. 6, no. 5, pp. 250–252, 2007. [CrossRef]
- Pandey, B.; Pandey, K. ; O. K.-A. J. of; undefined 2009, “Relapse of visceral leishmaniasis after miltefosine treatment in a Nepalese patient,” Res. Pandey, K Pandey, O Kaneko, T Yanagi, K HirayamaAmerican J. Trop. Med. Hyg. 2009•researchgate.net, vol. 80, no. 4, pp. 580–582, 2009. [CrossRef]
- Eichenberger, A.; et al. “A severe case of visceral leishmaniasis and liposomal amphotericin B treatment failure in an immunosuppressed patient 15 years after exposure,” BMC Infect. Dis., vol. 17, no. 1, Jan. 2017. [CrossRef]
- Kosaka, A.; et al. “Failure of Liposomal-amphotericin B Treatment for New World Cutaneous Leishmaniasis due to Leishmania braziliensis,” Intern. Med., vol. 59, no. 9, pp. 1227–1230, 2020. [CrossRef]
- Gangneux, J.P.; et al. “Recurrent American Cutaneous Leishmaniasis - Volume 13, Number 9—07 - Emerging Infectious Diseases journal - CDC,” Emerg. Infect. Dis., vol. 13, no. 9, pp. 1436–1438, 2007. 20 September. [CrossRef]
- Gomes, C.M.; et al. “Recurrent cutaneous leishmaniasis,” An. Bras. Dermatol., vol. 88, no. 3, pp. 462–464, 13. 20 May. [CrossRef]
- Soares, G.H.C.; et al. “Case Report: Coinfection by Leishmania amazonensis and HIV in a Brazilian Diffuse Cutaneous Leishmaniasis Patient,” Am. J. Trop. Med. Hyg., vol. 103, no. 3, pp. 1076–1080, 20. 20 May. [CrossRef]
- Vieira-Gonçalves, R.; et al. “First report of treatment failure in a patient with cutaneous leishmaniasis infected by Leishmania (Viannia) naiffi carrying Leishmania RNA virus: a fortuitous combination?,” Rev. Soc. Bras. Med. Trop., vol. 52, p. e20180323, Apr. 2019. [CrossRef]
- Freitas, J.J.A.; Cunha, M.A.; Diniz, S.R.; Monteiro, M.G.L.; Araújo, S.P.; Luz, K.G. , “TRATAMENTO DE RECIDIVA DE LEISHMANIOSE VISCERAL EM CRIANÇA COM TERAPIA TRIPLA: RELATO DE CASO,” Brazilian J. Infect. Dis., vol. 25, p. 101206, Jan. 2021. [CrossRef]
- Vélez, I.D.; Colmenares, L.M.; Muñoz, C.A. , “Two cases of visceral leishmaniasis in Colombia resistant to meglumine antimonial treatment,” Rev. Inst. Med. Trop. Sao Paulo, vol. 51, no. 4, pp. 231–236, Jul. 2009. [CrossRef]
- Dereure, J.; et al. “Visceral leishmaniasis. Persistence of parasites in lymph nodes after clinical cure,” J. Infect., vol. 47, no. 1, pp. 77–81, Jul. 2003. [CrossRef]
- Arboleda, M.; Barrantes, S.; Úsuga, L.Y.; Robledo, S.M. , “Successful treatment of cutaneous leishmaniasis with intralesional meglumine antimoniate: A case series,” Rev. Soc. Bras. Med. Trop., vol. 52, 2019. [CrossRef]
- Reinaldo, L.G.C.; et al. “Recurrent kala-azar: report of two cured cases after total splenectomy,” Rev. Inst. Med. Trop. Sao Paulo, vol. 62, p. e31, 20. 20 May. [CrossRef]
- Martínez, C.E.V.; et al. “Therapeutic failure of meglumine antimoniate in the treatment of visceral leishmaniasis,” Rev. Esc. M Rivera, J AlgerEDITORIAL BOARD, 2005 • Rev., no. 4, 2005, Accessed: Oct. 01, 2024. [Online]. Available: https://www.revistamedicahondurena.hn/assets/Uploads/Vol73-4-2005.
- Darcis, G.; et al. “Recurrence of visceral and muco-cutaneous leishmaniasis in a patient under immunosuppressive therapy,” BMC Infect. Dis., vol. 17, no. 1, Jul. 2017. [CrossRef]
- Stefanidou, M.P.; et al. “A rare case of leishmaniasis recidiva cutis evolving for 31 years caused by Leishmania tropica,” Int. J. Dermatol., vol. 47, no. 6, pp. 588–589, Jun. 2008. [CrossRef]
- Antoniou, M.; Doulgerakis, C.; Pratlong, F.; Dedet, J.P.; Tselentis, Y. , “Treatment failure due to mixed infection by different strains of the parasite Leishmania infantum,” Acad. Antoniou, C Doulgerakis, F Pratlong, JP Dedet, Y TselentisAmerican J. Trop. Med. Hyg. 2004•academia.edu, 2004, Accessed: Oct. 01, 2024. [Online]. Available: https://www.academia.edu/download/31633346/71.
- Jeziorski, E.; et al. “Mucosal relapse of visceral leishmaniasis in a child treated with anti-TNFα,” Int. J. Infect. Dis., vol. 33, pp. e135–e136, Apr. 2015. [CrossRef]
- Ruiz-Villaverde, R.; Melguizo, J.B.; Solano, J.L.; Pérez, M.P.B.; Sintes, R.N. , “Leishmaniasis cutánea crónica: Respuesta a n-metil glucamina intralesional tras fracaso con paramomicina tópica,” Actas Dermosifiliogr., vol. 93, no. 4, pp. 263–266, 2002. [CrossRef]
- Morizot, G.; et al. “Antimony to Cure Visceral Leishmaniasis Unresponsive to Liposomal Amphotericin B,” PLoS Negl. Trop. Dis., vol. 10, no. 1, p. e0004304, Jan. 2016. [CrossRef]
- RP, P. ; Mukherjee R; Priyadarshini A; Gupta A; Vibhuti A; Leal E; Sengupta U; VM, K.; Sharma P; CE, M.; VS, R., Lyu X. Potential of nanoparticles encapsulated drugs for possible inhibition of the antimicrobial resistance development. Biomed Pharmacother. 2021 Sep;141:111943. [CrossRef]
- RP, P. ; Vidic J; Mukherjee R, Chang CM. Experimental Methods for the Biological Evaluation of Nanoparticle-Based Drug Delivery Risks. Pharmaceutics. 2023 Feb 11;15(2):612. [CrossRef]
- “Leishmaniasis emergence in Europe.” https://www.ecdc.europa.eu/en/news-events/leishmaniasis-emergence-europe (accessed Nov. 14, 2024).
- Kumar, S; Dhiman, R; CR, P.; AC, C.; Vibhuti, A; Leal, E; CM, C.; VS, R. Kumar S; Dhiman R; CR, P.; AC, C.; Vibhuti A; Leal E; CM, C.; VS, R., Pandey RP. Chitosan: Applications in Drug Delivery System. Mini Rev Med Chem. 2023;23(2):187-191. [CrossRef]
- Ruby, M; CC, G.; Pandey, R; VS, R.; VS, S. Ruby M; CC, G.; Pandey R; VS, R.; VS, S., Ajay AK. Autophagy as a Therapeutic Target for Chronic Kidney Disease and the Roles of TGF-β1 in Autophagy and Kidney Fibrosis. Cells. 2023 Jan 26;12(3):412. [CrossRef]
- Khatri, P; Rani, A; Hameed, S; Chandra, S; CM, C. Khatri P; Rani A; Hameed S; Chandra S; CM, C., Pandey RP. Current Understanding of the Molecular Basis of Spices for the Development of Potential Antimicrobial Medicine. Antibiotics (Basel). 2023 Jan 29;12(2):270. [CrossRef]
- Tripathi, S; Khatri, P; Fatima, Z; RP, P. Tripathi S; Khatri P; Fatima Z; RP, P., Hameed S. A Landscape of CRISPR/Cas Technique for Emerging Viral Disease Diagnostics and Therapeutics: Progress and Prospects. Pathogens. 2022 Dec 29;12(1):56. [CrossRef]
- RP, P. ; Mukherjee R, Chang CM. Antimicrobial resistance surveillance system mapping in different countries. Drug Target Insights. 2022 Nov 30; 16:36-48. [CrossRef]
Figure 1.
The life cycle of Leishmania donovani.
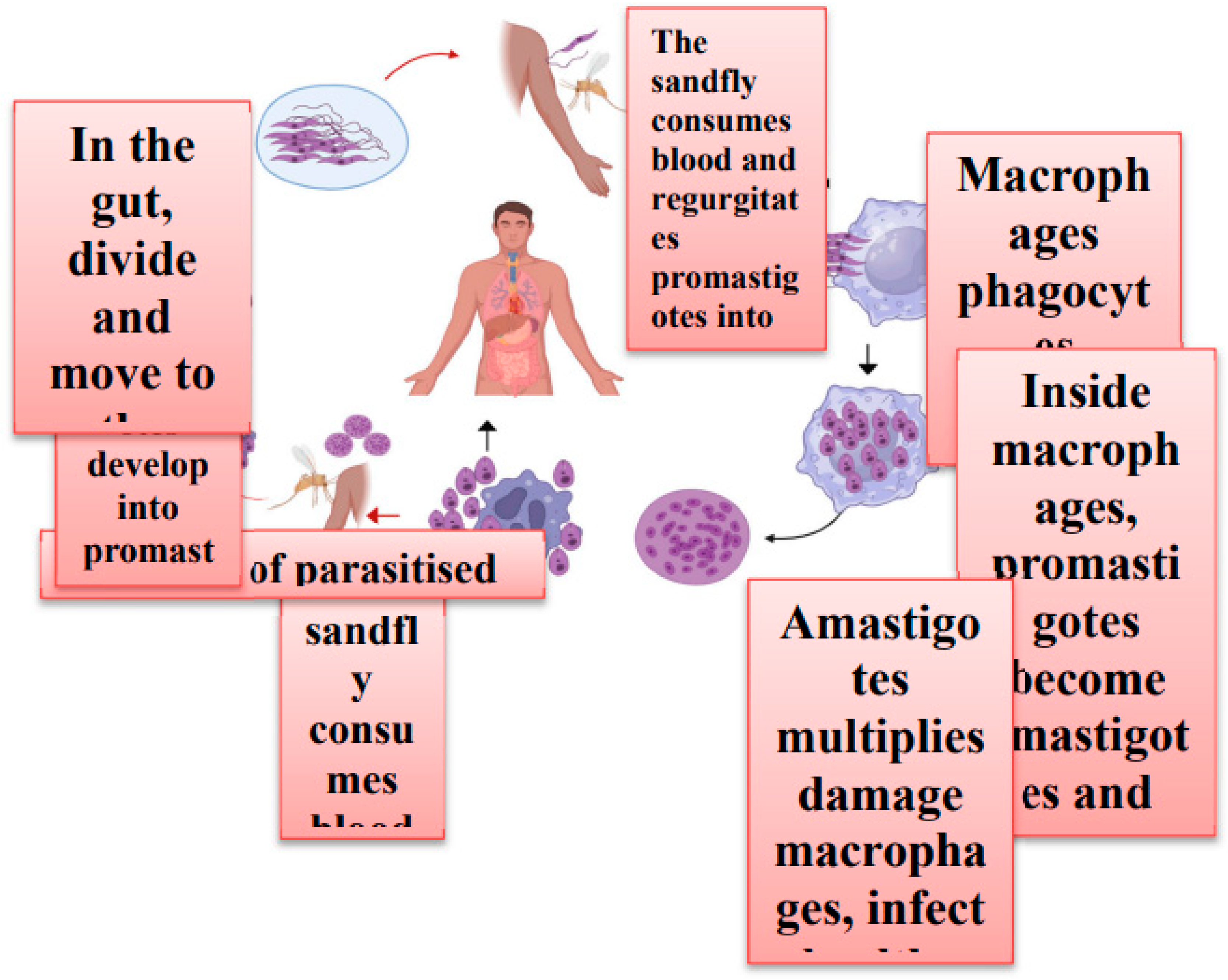
Figure 3.
Representation of Parasite developing resistant against antimonials along with arsenic.
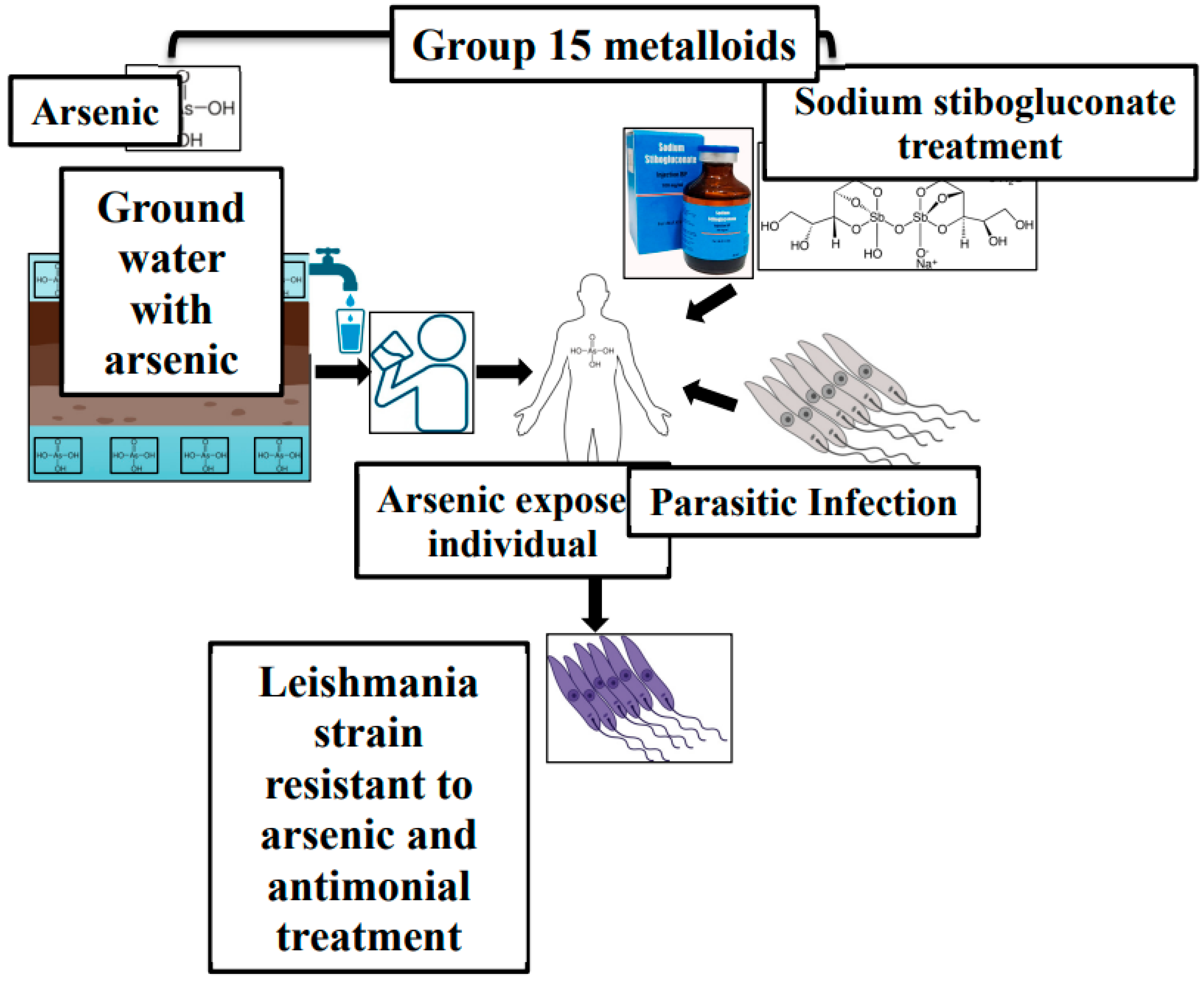
Figure 4.
Molecular mechanism of Drug Resistance against Pentavalent antimonials (The figure shows an amastigote within a macrophage's phagolysosome, detailing how antimonials enter the parasite and the intracellular processes that lead to drug resistance. It highlights the roles of ABC transporters, aquaporins (AQP), and proteins involved in drug resistance (DR), including MDR1 and interleukin 10 (IL-10).) [19].
Figure 4.
Molecular mechanism of Drug Resistance against Pentavalent antimonials (The figure shows an amastigote within a macrophage's phagolysosome, detailing how antimonials enter the parasite and the intracellular processes that lead to drug resistance. It highlights the roles of ABC transporters, aquaporins (AQP), and proteins involved in drug resistance (DR), including MDR1 and interleukin 10 (IL-10).) [19].

Figure 5.
(A) The mechanism of action of Amphotericin and Leishmania resistance mechanisms are shown in red. (AmB, Amphotericin B; RNI, reactive nitrogen intermediates; ROI, reactive oxygen intermediates; T [SH2], trypanothione; TR, trypanothione reductase.
Figure 5.
(A) The mechanism of action of Amphotericin and Leishmania resistance mechanisms are shown in red. (AmB, Amphotericin B; RNI, reactive nitrogen intermediates; ROI, reactive oxygen intermediates; T [SH2], trypanothione; TR, trypanothione reductase.
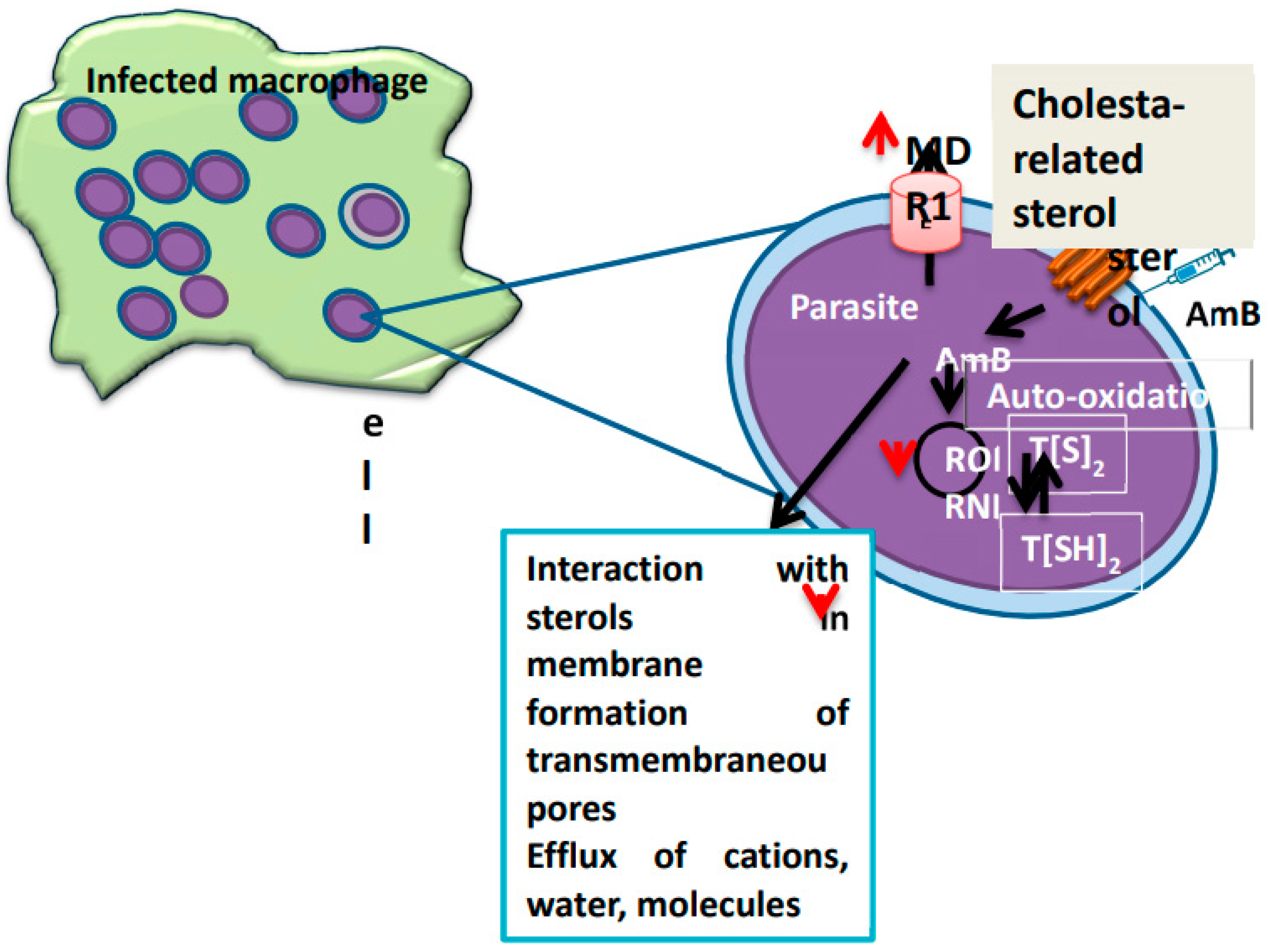
Figure 6.
The Leishmania modes of action of Miltefosine along with potential mechanism of resistance against Miltefosine. (MDR, multidrug resistance transporter; LdROS3, subunit of the LdMT transporter; Leishmania donovani Miltefosine transporter).
Figure 6.
The Leishmania modes of action of Miltefosine along with potential mechanism of resistance against Miltefosine. (MDR, multidrug resistance transporter; LdROS3, subunit of the LdMT transporter; Leishmania donovani Miltefosine transporter).
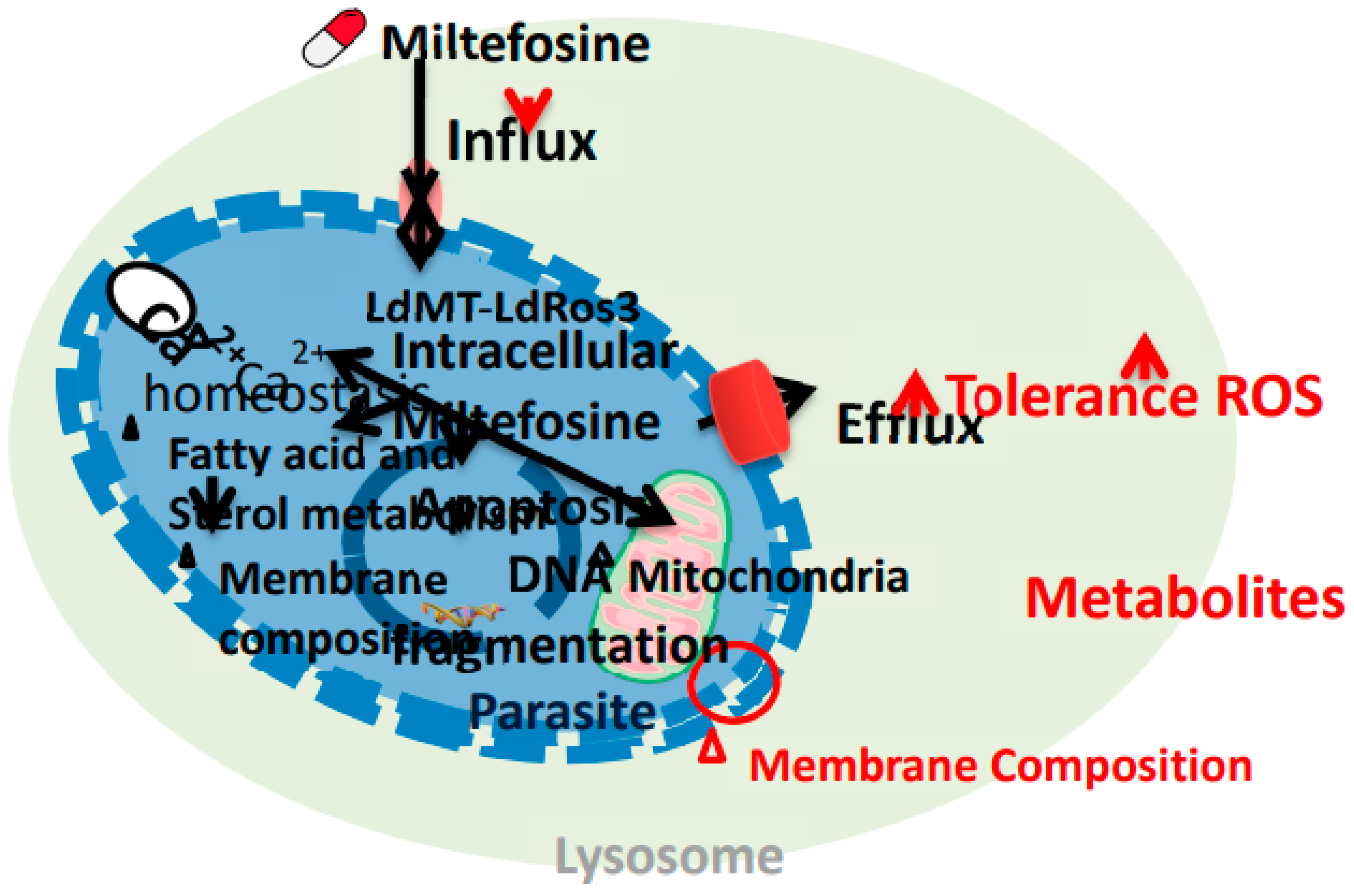
Figure 7.
The mechanism of action of paromomycin involves inhibiting protein synthesis in Leishmania by binding to the ribosomal RNA. Possible resistance mechanisms in Leishmania include overexpression of multidrug resistance transporter 1 (MDR) and multidrug resistance-associated protein A (MRPA), which may reduce the drug's efficacy by decreasing its intracellular concentration.
Figure 7.
The mechanism of action of paromomycin involves inhibiting protein synthesis in Leishmania by binding to the ribosomal RNA. Possible resistance mechanisms in Leishmania include overexpression of multidrug resistance transporter 1 (MDR) and multidrug resistance-associated protein A (MRPA), which may reduce the drug's efficacy by decreasing its intracellular concentration.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



