
Submitted:
25 November 2024
Posted:
26 November 2024
You are already at the latest version
Abstract
Type 1 Diabetes (T1D) is a progressive autoimmune disease often identified in childhood or adolescence, with early stages detectable through pre-diabetic markers such as autoantibodies and subclinical beta cell dysfunction. Identification of the pre-T1D stage is critical for preventing complications, such as diabetic ketoacidosis, and for enabling timely interventions that may alter disease progression. This review examines the multifaceted approach to managing T1D risk in adolescents and teens, emphasizing early detection, nutritional interventions, beta cell preservation strategies, and psychosocial support. Screening for T1D-associated autoantibodies offers predictive insight into disease risk, particularly when combined with education and family resources that promote lifestyle adjustments. Although nutritional interventions alone are not capable of preventing T1D, certain lifestyle interventions, such as weight management and specific nutritional choices, have shown potential in preserving insulin sensitivity, reducing inflammation, and mitigating metabolic strain. Pharmacological strategies, including immune-modulating drugs like teplizumab, alongside emerging regenerative and cell-based therapies, offer potential in delaying disease onset by protecting beta cell function. The social and psychological impacts of a T1D risk diagnosis are also significant, affecting adolescents’ quality of life, family dynamics, and mental health. Supportive interventions, including counseling, cognitive-behavioral therapy (CBT), and group support, are recommended for managing the emotional burden of pre-diabetes. Future directions call for integrating universal or targeted screening programs within schools or primary care, advancing research into nutrition and psychosocial support, and promoting policies that enhance access to preventive resources. Advocacy for insurance coverage of screening, nutritional counseling, and mental health services is also crucial to supporting families in managing T1D risk. By addressing these areas, healthcare systems can promote early intervention, improve beta cell preservation, and support the overall well-being of adolescents at risk of T1D.
Keywords:
Type 1 diabetes
; Youth screening
; Nutritional intervention
; Family support
; Beta cell preservation
1. Introduction
Type 1 Diabetes (T1D) is a chronic autoimmune disorder primarily characterized by the destruction of insulin-producing beta cells in the pancreas, leading to an absolute deficiency in insulin production [1,2,3,4]. While T1D often manifests in childhood or adolescence, the natural history of the disease indicates that beta cell destruction and autoimmune activation may begin years before the clinical onset [5,6]. Adolescents and teens with T1D experience lifelong challenges, including metabolic instability, the risk of severe acute complications, and an increased likelihood of developing secondary complications over time [7,8,9,10,11]. As such, understanding the early stages of T1D development, particularly the transition from pre-diabetes to overt T1D, has become critical in recent years to identify effective preventive strategies.
1.1. Overview of Type 1 Diabetes in Adolescents and Teens
T1D is the predominant form of diabetes in young populations, with peak incidence occurring between the ages of 10 and 14 [12,13]. Genetic susceptibility, environmental triggers, and immune dysregulation are all implicated in the pathogenesis of T1D, contributing to progressive loss of beta cells [14,15,16]. In adolescents and teens, this disease not only disrupts metabolic homeostasis but also imposes significant psychosocial burdens, as they navigate a chronic, life-altering condition during formative years. The disease’s pathophysiology in youth is often more aggressive than in adults, with faster rates of beta cell decline, a more challenging insulin management profile, and an increased risk of diabetic ketoacidosis (DKA) at diagnosis [17,18]. The high incidence of T1D in adolescents highlights the need for strategies aimed at early detection and intervention in this vulnerable age group.
1.2. Pre-Diabetes as an Intermediary Stage Characterized by Insulin Resistance, Autoantibody Presence, and Subclinical Beta Cell Dysfunction
Pre-diabetes in the context of T1D, often referred to as the "stages of T1D," is defined by the presence of diabetes-associated autoantibodies without overt hyperglycemia. Unlike pre-diabetes associated with Type 2 Diabetes, which is primarily characterized by insulin resistance, pre-diabetes in T1D is marked by an autoimmune-mediated attack on beta cells. This phase can be stratified into stages based on the presence and progression of specific autoantibodies (such as GAD65, IA-2, and ZnT8) and glycemic abnormalities that reflect subclinical beta cell dysfunction [17,18,19,20,21] (Table 1).
Early-stage pre-diabetes (Stage 1) is identified by multiple islet autoantibodies without dysglycemia, whereas Stage 2 is marked by the onset of dysglycemia alongside persistent autoimmunity (Figure 1). In Stage 3, diagnostic criteria for diabetes are met, typically when significant beta cell loss has occurred (Figure 1). This staging framework allows for a progressive understanding of T1D development, where each stage represents a distinct shift in the autoimmune and metabolic processes leading to clinical diabetes [17]. The identification of autoantibodies at these early stages provides a predictive tool for assessing T1D risk, especially in individuals with a family history of the disease or other genetic predispositions.
Beta cell dysfunction in the pre-diabetic stage is both autoimmune-driven and mediated by inflammatory processes. Mechanisms such as cytokine release and immune cell infiltration contribute to beta cell apoptosis, while metabolic stress from immune-mediated inflammation further impairs insulin production. The measurement of C-peptide levels and oral glucose tolerance tests can be used to assess beta-cell function [22,23,24,25,26,27,28] (Table 1). Recent studies in adolescents and children have utilized continuous glucose monitoring (CGM) data to detect early hyperglycemia and assess its potential as a diagnostic tool for T1D. By monitoring the percentage of time participants spend above 140 mg/dL, CGM helps characterize individuals who are progressing to stage 3 type 1 diabetes [29,30,31,32,33,34,35,36] (Table 1). This early-stage period is critical for intervention, as targeted therapies aimed at preserving beta cell function or modulating the immune response could potentially delay or prevent the onset of clinical T1D.
1.3. Importance of Early Identification and Intervention, Particularly in High-Risk Populations
Early identification of pre-diabetes in adolescents and teens is a pivotal component of diabetes prevention strategies. Screening for islet autoantibodies in high-risk populations, such as those with a family history of T1D or specific genetic markers (e.g., HLA-DR3/DR4 alleles), enables early stratification of individuals based on their likelihood of disease progression [17,18,37,38]. Moreover, early identification provides a window of opportunity for intervention during the pre-diabetes phase, where immunomodulatory therapies may alter the disease trajectory.
Interventional studies in at-risk youth have shown promise in modulating immune responses and preserving residual beta cell function. For example, therapies that target specific immune pathways, such as T-cell modulation (e.g., Teplizumab, an anti-CD3 monoclonal antibodies) and regulatory T-cell preservation, are under investigation for their potential to delay the onset of T1D [39,40,41,42].
Trials with teplizumab have reported reductions in the overall autoimmune response, with some patients showing decreased autoantibody titers or even undetectable levels after treatment [43]. While promising, these observations remain subject to variability across patient populations and require further investigation. It is also important to account for laboratory variability when interpreting changes in autoantibody status. Differences in assay sensitivity, specificity, and reproducibility may contribute to apparent transitions from detectable to undetectable states, especially for borderline or low-titer results [44].
The dynamics of T1D-related autoantibodies reflect a complex interplay of natural immune processes, disease progression, and potential therapeutic interventions. While persistent autoantibody positivity remains a hallmark of T1D pathogenesis, transient or declining autoantibody levels have been observed in specific contexts, such as low-risk populations or in response to immunotherapy. These findings emphasize the need for longitudinal monitoring and standardized methodologies to enhance our understanding of autoantibody behavior and its implications for T1D prediction and treatment.
In addition to promising recent pharmacological strategies aimed at delaying T1D progression, psychosocial support for adolescents identified as high-risk is recommended. The emotional and psychological burden associated with the risk of developing a chronic illness cannot be overstated, particularly in a population already facing the challenges of adolescence. Structured education programs, counseling, and community support can help these individuals, and their families cope with the stress of T1D risk and foster proactive engagement in preventive health practices [45].
In summary, pre-diabetes in adolescents and teens represents a critical stage in the development of T1D, marked by immunological and metabolic shifts that foreshadow clinical disease. Screening for autoantibodies and beta cell function in high-risk populations not only enhances predictive accuracy but also enables timely, targeted interventions aimed at delaying T1D onset. As research advances, integrating biomarker-based screening with immunological, metabolic, and psychosocial interventions may offer a comprehensive approach to reducing the burden of T1D among youth. Future studies must continue to refine the predictive tools and therapeutic strategies to facilitate pre-diabetes management in pediatric populations.
2. Screening and Early Detection of Autoantibodies in Adolescents and Teens
The early detection of pre-diabetes in youth populations at risk of progressing to T1D has become a focal point in early treatment research. Screening for autoantibodies, which signal an autoimmune response against insulin-producing beta cells, can identify at-risk adolescents before they exhibit clinical symptoms, enabling the use of strategies to delay disease onset and reduce the risk of diabetic ketoacidosis. This section discusses the importance and methodologies of autoantibody screening, recent advances in screening tools, and ethical considerations that accompany early T1D risk detection.
2.1. Prevalence and Importance of Screening
2.1.1. Rising Prevalence of Pre-Diabetes and T1D Risk in Youth Populations
In recent years, the prevalence of pre-diabetes and T1D risk factors has shown a marked increase among adolescents and teens, attributed to both genetic and environmental factors. Unlike Type 2 Diabetes, T1D is less associated with lifestyle risk factors, yet recent studies highlight a complex interplay of genetic predisposition, immune dysregulation, and environmental triggers (e.g., viral infections, dietary factors) that accelerate T1D risk even in previously unaffected youth [14,15,16]. Current estimates indicate that approximately 0.3% of adolescents in the U.S. are at high risk for T1D, evidenced by the presence of multiple islet autoantibodies [46].
2.1.2. Utility of Autoantibody Screening in Identifying At-Risk Individuals
The utility of autoantibody screening in early detection is well-established, as the presence of diabetes-associated autoantibodies significantly increases the likelihood of developing T1D [17,18,47] (Table 1). Key autoantibodies, including those against glutamic acid decarboxylase (GAD65), insulin (IAA), islet antigen-2 (IA-2), and zinc transporter 8 (ZnT8), serve as biomarkers for beta cell autoimmunity [17,18,47]. The presence of one autoantibody may indicate risk, but the detection of multiple autoantibodies correlates with a nearly inevitable progression to T1D, particularly in youth populations with a family history of the disease. Autoantibody screening not only identifies high-risk individuals but also aids in staging T1D progression and timing intervention strategies to preserve beta cell function before significant loss occurs.
2.2. Screening Strategies and Recommendations
2.2.1. Current Guidelines and Recommendations for Screening
Leading diabetes organizations, including the Breakthrough T1D (Formerly Juvenile Diabetes Research Foundation; JDRF) and the American Diabetes Association (ADA), have established guidelines for autoantibody screening in high-risk pediatric populations [48]. These guidelines recommend screening for children with a first-degree relative with T1D, particularly between the ages of 2 and 18, as this is the period of highest risk. Screening is also encouraged for youth with specific genetic markers associated with T1D susceptibility, such as HLA-DR3 and HLA-DR4 alleles [16,49,50,51,52,53] (Table 1). Guidelines suggest a stepwise approach, where a positive initial autoantibody screening is followed by regular monitoring to assess disease progression and allow for timely intervention [54,55]. The Diabetes Research Institute Foundation (DRIF) supports these efforts by funding research aimed at refining screening techniques and promoting early detection strategies to enable timely and effective interventions. DRIF emphasizes the importance of accessible and family-centered screening programs to reduce the burden of T1D on high-risk populations.
2.2.2. Community Screening Programs
In recent years, community screening programs, such as the TrialNet Pathway to Prevention and The Environmental Determinants of Diabetes in the Young (TEDDY) study, have facilitated widespread screening and contributed significantly to our understanding of T1D progression [56]. These programs employ standardized methodologies for autoantibody detection and follow at-risk youth longitudinally, enabling early detection and intervention on a broad scale. Data from these programs have highlighted the potential of community-wide screening in reducing T1D-associated complications at diagnosis and identifying intervention points to delay disease onset.
2.3. Advances in Screening Tools
2.3.1. Emerging Biomarkers Beyond Autoantibodies
While autoantibody screening remains the cornerstone of T1D risk detection, recent advances have identified additional biomarkers that enhance screening accuracy. Metabolomic profiling, which assesses patterns of metabolites in blood, has shown promise in distinguishing at-risk youth from those unlikely to progress to T1D. Studies indicate that changes in lipid metabolites, amino acid levels, and short-chain fatty acids are associated with T1D onset [57,58,59,60], suggesting that metabolomic markers could provide additional predictive value.
Genomic biomarkers, including specific gene variants related to immune regulation and beta cell function, also offer potential in refining risk assessment. For example, polymorphisms in genes associated with cytokine production and immune cell signaling (e.g., IL-2, CTLA-4) have been linked to T1D susceptibility and progression [61,62]. However, these biomarkers are still in the early stages of development, and a considerable path lies ahead before they can be fully utilized in clinical settings. Integrating these genetic markers with autoantibody data may enable a more individualized risk prediction model, which could ultimately guide personalized intervention strategies.
2.3.2. Evaluating Sensitivity, Specificity, and Predictive Value of Novel Biomarkers
The effectiveness of emerging biomarkers relies on their sensitivity, specificity, and predictive value, especially in diverse populations. Current studies aim to validate these markers in different ethnic and genetic backgrounds to ensure reliability. The inclusion of metabolomic and genomic markers alongside autoantibodies has shown to increase predictive accuracy, with specificity rates nearing 90% in some cohorts [63,64,65,66,67]. Continuous improvement of these markers will be essential to refining risk prediction models and expanding screening applicability to general populations beyond those with a family history of T1D.
2.4. Ethical Considerations
2.4.1. Ethical Implications of Screening for T1D in Light of Emerging Therapeutic Interventions
Screening asymptomatic youth for T1D risk now carries new ethical considerations, especially with the recent availability of FDA-approved therapies, such as teplizumab, and investigational treatments like anti-thymocyte globulin (ATG) that may delay disease progression. Identifying autoantibodies and predicting T1D onset can empower families with options for early intervention, potentially altering the disease course. However, the psychological impact of a preclinical diagnosis, which may include anxiety or stress over long-term outcomes, remains a concern. Families must balance the promise of emerging therapies with the emotional and logistical implications of engaging in early intervention strategies. Providing targeted counseling and support is essential to help families make informed decisions about risk-based treatment and to address the complex psychosocial aspects of a preclinical T1D diagnosis.
2.4.2. Family Counseling and Implications for Early Lifestyle Adjustments
Informed consent, education, and counseling are essential components of the T1D screening process. Families should be fully informed of the implications of screening results, including the limitations of predictive tools and the possibility of false positives or uncertainties in progression. Moreover, lifestyle recommendations following a positive screening result must be carefully managed to avoid undue burden on youth and their families. Nutritional and behavioral interventions should focus on promoting general health benefits without fostering restrictive or unsustainable lifestyle changes. Family-centered counseling can provide support and empower families to adopt manageable, health-promoting adjustments that may reduce metabolic stress on beta cells without significantly altering their quality of life.
3. Role of Nutrition in Pre-Diabetes Progression
3.1. Nutritional Interventions and Lifestyle Modification
Nutritional interventions and lifestyle modifications can help in managing pre-diabetes in adolescents and teens at elevated risk for T1D (Table 2). Drawing from extensive advocacy efforts, research data, and meta-analyses, the combined insights from patients, families, and healthcare professionals highlight the importance of these interventions in supporting metabolic health and overall well-being for high-risk groups. Although nutritional and lifestyle modifications cannot prevent T1D onset, they can enhance metabolic resilience, reduce complications, and improve quality of life for individuals predisposed to the disease.
Current studies suggest that a balanced, nutrient-dense diet stabilizes blood glucose levels, promotes insulin sensitivity, and reduces inflammation, an essential factor for protecting beta cells from stress [68,69]. Low-glycemic and high-fiber diets, combined with a focus on healthy fats and proteins, can improve glucose regulation and inflammatory response modulation [70,71]. Additionally, micronutrients such as Vitamin D and Omega-3 fatty acids have been hypothesized to have potential for immune support and beta-cell preservation, though further research is warranted to clarify their role in disease progression [72,73,74,75,76,77].
Physical activity, encompassing aerobic and resistance training, consistently benefits insulin responsiveness, cardiovascular health, and inflammation reduction. Even moderate exercise, such as daily walking, significantly supports both metabolic and mental health, providing a holistic approach to managing pre-diabetes. Physical activity is further linked to improved mental well-being, helping to reduce anxiety and improve mood, a critical aspect for adolescents facing T1D risk [78].
It has been suggested that lifestyle interventions in T1D offer more than metabolic advantages (Table 2); they provide a proactive, empowering approach that fosters confidence, resilience, and a positive stance toward health management. Structured support through counseling and educational initiatives can help families make informed, sustainable choices, mitigating the psychosocial stress often associated with a high-risk T1D status [79].
Hence, while lifestyle and nutritional modifications do not prevent T1D onset, they equip individuals and families with effective, practical strategies that positively impact health trajectories. By prioritizing education, resilience, and metabolic optimization, these interventions set a strong foundation for improved outcomes and ease the transition should T1D develop.
3.1.1. Impact of Dietary Patterns on Insulin Resistance and Inflammation
Dietary patterns profoundly influence insulin sensitivity and inflammatory pathways, shaping the progression of pre-diabetes and health outcomes for those at risk for T1D. Diets high in sugars and saturated fats are associated with increased insulin resistance and a pro-inflammatory state, exacerbating beta-cell stress and accelerating beta-cell loss. Adolescents consuming diets rich in sugary beverages, processed foods, and high-fat snacks face a heightened risk of metabolic imbalances that contribute to hyperglycemia, oxidative stress, and chronic inflammation [61]. This detrimental cycle—characterized by decreased insulin sensitivity, overcompensation by beta cells, and advancing autoimmune attacks—underscores the need for dietary interventions to mitigate these effects (Anderson et al., 2023).
3.1.2. Evidence-Based Dietary Guidelines
To counteract these risks, evidence-based dietary guidelines advocate for low glycemic index (GI) diets, plant-based foods, and anti-inflammatory nutrition. A low GI diet, featuring whole grains, legumes, and fiber-rich vegetables, prevents rapid blood sugar spikes and reduces insulin demand, alleviating metabolic strain on beta cells [61]. Meta-analyses confirm that low GI diets improve glucose regulation and support beta-cell function [80].
Plant-based diets, emphasizing fruits, vegetables, legumes, and whole grains, are linked to lower inflammatory markers and improved insulin sensitivity, potentially delaying T1D progression [62]. The benefits of such diets include reduced oxidative stress and improved immune function, further supporting their role in pre-diabetes management [81].
Anti-inflammatory foods, rich in omega-3 fatty acids, antioxidants, and phytonutrients (such as leafy greens, berries, and nuts), are effective in reducing systemic inflammation—a major contributor to autoimmune activity. Emerging evidence highlights the potential of these nutrients in modulating immune responses and preserving beta-cell health.
3.2. Specific Nutrients and Dietary Supplements
3.2.1. Role of Specific Nutrients in Insulin Sensitivity and Inflammation Reduction
Certain nutrients have been studied for their roles in promoting insulin sensitivity and reducing inflammation, both of which are vital for at-risk youth. Omega-3 fatty acids, from fish and flaxseed oils, are known to modulate inflammatory pathways and improve cell membrane integrity, thereby enhancing insulin sensitivity [82]. Antioxidants, such as vitamins C and E, neutralize free radicals and decrease oxidative stress on beta cells, supporting overall cell health [83].
Dietary fiber, particularly soluble fiber from sources like oats, legumes, and certain fruits, aids in regulating blood glucose by slowing carbohydrate absorption and improving insulin sensitivity. Fiber also supports gut microbiome health, which may indirectly influence inflammation and immune responses, adding a potential benefit for individuals at risk of autoimmune conditions like T1D.
3.2.2. Potential Benefits of Vitamin D, Zinc, and Magnesium
Vitamin D plays a dual role in immune function and insulin sensitivity, and deficiency in vitamin D has been linked to a higher risk of autoimmune diseases, including T1D [84,85,86]. Supplementation of this vitamin in youth at risk may support beta cell health and modulate immune responses [87,88,89,90]. Magnesium, an essential mineral involved in glucose metabolism and insulin action, have gained attention as potentially beneficial for youth at risk of T1D [91] . It has been associated with improved insulin sensitivity [92,93]. Low magnesium levels are often observed in individuals with poor metabolic health, making supplementation a relevant consideration for at-risk youth.
3.3. Impact of Exercise and Physical Activity
3.3.1. Relationship Between Physical Activity, Metabolic Health, and Beta Cell Preservation
Physical activity is a well-documented factor in improving insulin sensitivity, enhancing glucose metabolism, and supporting metabolic health. Exercise activates pathways in muscle cells that increase glucose uptake, reducing the need for insulin and thereby alleviating some of the metabolic pressure on beta cells [94]. Additionally, regular physical activity has been associated with reduced systemic inflammation, further aiding in beta cell preservation for adolescents with pre-diabetes. This mechanism is particularly relevant in individuals with impaired glucose tolerance or prediabetes, where regular physical activity has been shown to reduce systemic inflammation, a contributing factor to beta cell dysfunction and loss [95]. By mitigating chronic low-grade inflammation, physical activity promotes a more favorable metabolic environment for preserving beta cell function in adolescents and adults with prediabetes.
A specific and practical form of physical activity, walking, provides immediate benefits for postprandial blood glucose regulation. Muscle contractions during walking enhance glucose uptake directly from the bloodstream, bypassing the need for insulin [96]. This effect is particularly pronounced in the post-meal period, when blood glucose levels are at their peak. Studies indicate that even light to moderate intensity walking for 15-30 minutes after meals can significantly reduce postprandial glucose spikes, stabilizing glycemic control [97]. This reduction in glucose variability has important implications for individuals at risk of T1D or T2D, as prolonged hyperglycemia is a key driver of beta cell stress and apoptosis.
Regular post-meal walking also improves insulin sensitivity over time, further supporting glucose homeostasis. Enhanced insulin action reduces the burden on beta cells to secrete insulin, allowing for functional preservation [96]. Additionally, the cardiovascular benefits associated with consistent physical activity, such as improved lipid profiles and weight management, contribute to overall metabolic health and further reduce the risk of beta cell failure. These findings underscore the role of physical activity not only as a therapeutic intervention for managing blood glucose but also as a preventative measure for beta cell preservation.
3.3.2. Specific Exercise Recommendations for Adolescents and Teens
For youth at risk of T1D, a combination of aerobic and resistance exercises is recommended [96,98]. Aerobic exercises, such as running, swimming, and cycling, help improve cardiovascular fitness and enhance glucose metabolism, while resistance training builds muscle mass, which further supports glucose uptake and insulin sensitivity. Current recommendations suggest that adolescents should aim for at least 60 minutes of moderate to vigorous physical activity daily [99]. Integrating age-appropriate, enjoyable activities, such as sports, dance, or active play, can encourage consistency and long-term adherence to physical activity goals [96,98].
3.4. Case Studies and Trials
3.4.1. Clinical Trials and Observational Studies on Nutrition and Lifestyle Changes
Several clinical trials and observational studies highlight the benefits of nutritional and lifestyle interventions in delaying or preventing the onset of T1D in at-risk populations. For example, the Diabetes Prevention Trial-Type 1 (DPT-1) and TrialNet studies have explored dietary and pharmacological interventions, observing positive outcomes in delaying disease progression among participants with autoantibodies. Observational studies have shown that children with higher adherence to Mediterranean-style diets, characterized by high fruit, vegetable, and whole grain intake, demonstrate reduced markers of inflammation and better glycemic control, underscoring the potential of diet as a preventive measure [69].
In addition, lifestyle interventions that combine diet and physical activity components show promising outcomes in youth populations. For example, the Type 1 Diabetes Prediction and Prevention (DIPP) study in Finland indicated that infants and children adhering to dietary guidelines with lower intake of processed foods exhibited delayed onset of T1D-related autoimmunity [100]. Such findings emphasize the potential of integrated lifestyle interventions for modifying T1D risk factors and support the need for accessible dietary and physical activity education.
3.4.2. Instacart Health Initiatives and Business Partnerships for Nutritional Guidance
In recent years, business partnerships have become essential in promoting nutritional guidance and supporting educational outreach for at-risk youth and their families. Instacart Health, a health-focused initiative from Instacart, has collaborated with various organizations to support public access to nutritious foods and health education. By partnering with health providers and nutritionists, Instacart Health aims to make shopping for balanced, whole-food diets easier and more accessible, leveraging data-driven insights to recommend health-conscious grocery choices.
Through partnerships with diabetes-focused organizations, Instacart Health also offers educational resources for families, highlighting meal planning and shopping habits that align with pre-diabetes dietary guidelines. Such collaborations support community education and provide accessible tools that encourage healthier food choices, amplifying the social impact of business partnerships in preventive health. By making it easier for families to access nutritious foods and learn about healthy meal planning, initiatives like Instacart Health contribute to the larger goal of reducing T1D progression risk in youth through sustainable dietary changes.
In summary, nutritional interventions and lifestyle modifications are integral to managing pre-diabetes in adolescents and teens at risk for T1D. Emphasizing dietary patterns that improve insulin sensitivity and reduce inflammation, along with promoting regular physical activity, can help mitigate the metabolic challenges associated with T1D risk. Evidence from clinical studies and the increasing involvement of health-focused business initiatives provide a comprehensive approach to preventive care, combining accessible nutritional guidance with community-level support. Adopting evidence-based dietary habits and active lifestyles can help youth at risk for T1D delay or prevent disease onset, emphasizing the importance of multi-faceted, collaborative approaches in public health.
4. Section 4
4.1. Pharmacological Interventions
4.1.1. Overview of Immune-Modulating Drugs
Immune-modulating drugs are a primary pharmacological strategy to preserve beta cell function in individuals at high risk of T1D [101]. A comprehensive array of pharmacological interventions for T1D is presented in Table 3. Some of these agents remain under early-phase investigation and have not yet received approval for clinical application. These drugs work by targeting immune cells that mistakenly attack beta cells, slowing down the autoimmune progression toward full-blown diabetes. Teplizumab, a monoclonal antibody that modulates T-cell activity, is the most promising example of an immune-modulating drug [43,102,103] (Table 3). By binding to specific T-cells and preventing their activation, teplizumab can reduce the autoimmune attack on beta cells [104,105,106,107]. Studies such as the TN-10 trial demonstrated that teplizumab delays the onset of T1D by approximately two years in high-risk individuals [39,108], and was the first disease- modifying drug approved to slow disease progression, marking it as a significant step forward in preventive pharmacotherapy.
Another component, Glucagon-like peptide-1 (GLP-1) receptor agonists, traditionally used for managing T2D and obesity, are increasingly being explored for their potential to delay or prevent the onset of T1D. These agents improve glycemic control by enhancing glucose-dependent insulin secretion, suppressing glucagon release, and slowing gastric emptying. Importantly, they exhibit anti-inflammatory properties and promote beta-cell survival and regeneration, mechanisms that align with strategies to preserve beta-cell function and delay autoimmune-mediated destruction in T1D [109].
Recent evidence highlights the efficacy of tirzepatide, a dual GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) receptor agonist, in delaying diabetes progression in high-risk populations. According to Eli Lilly’s recent study on adults with prediabetes and obesity, treatment with tirzepatide resulted in a 94% reduction in the progression to T2D compared to placebo over a three-year period. Furthermore, participants achieved an average weight reduction of 22.9%, underscoring the metabolic benefits of this therapy [110]. These findings are significant, as improved metabolic health and reduced systemic inflammation directly contribute to preserving beta-cell function, which is essential in both prediabetes and T1D contexts.
While GLP-1 receptor agonists have not yet been extensively studied for preventing T1D, their ability to improve beta-cell survival and modulate the immune response positions them as promising candidates for future clinical trials in at-risk populations, such as individuals with autoantibody positivity or genetic predisposition to T1D. Current research into their anti-inflammatory effects and impact on glucose variability suggests that GLP-1 receptor agonists may complement existing preventive strategies for T1D, particularly when implemented early in the disease course.
4.1.2. Current Trials and Outcomes of Agents Targeting Inflammation and Beta Cell Preservation
Other agents are under investigation for their potential to delay T1D onset by targeting inflammation and immune responses. Trials with anti-CD20 antibodies (e.g., rituximab) and interleukin-2 (IL-2) therapy have shown some potential in modulating immune responses and preserving beta cell function, although with varied efficacy in the pediatric population [111,112,113,114]. Abatacept, a drug that interferes with T-cell costimulation, has also shown promise in slowing beta cell decline [41]. Ongoing trials are evaluating the safety and long-term effects of these drugs, with preliminary data indicating that such treatments may extend beta cell functionality, potentially delaying T1D onset.
Other pharmacological agents, such as anti-inflammatory drugs and antioxidants, are also being explored [115]. These agents aim to reduce inflammatory cytokine levels around beta cells, thereby protecting them from immune-mediated destruction. Early-stage trials have shown moderate success in reducing inflammation, but more research is needed to determine their effectiveness as standalone therapies or in combination with other immune-modulating agents.
4.2. Non-Pharmacological Interventions
Non-pharmacological strategies focus on factors such as stress management and adequate sleep, which are essential for metabolic health [116,117,118,119]. Chronic stress and poor sleep quality elevate cortisol and other stress hormones that increase blood glucose levels, exacerbating beta cell stress [120,121,122]. Techniques such as mindfulness, cognitive behavioral therapy (CBT), and relaxation exercises are beneficial for at-risk adolescents to help manage stress, while establishing regular sleep routines supports metabolic resilience [123,124,125,126]. Non-pharmacological interventions offer solutions that are quick, easy, and require almost nothing to implement. While non-pharmacological interventions cannot completely replace other therapies, they majorly help in preventing the disease.
4.3. Experimental and Novel Approaches
4.3.1. Advances in Regenerative Medicine and Cell-Based Therapies
Regenerative medicine and cell-based therapies offer innovative possibilities for beta cell preservation in high-risk individuals [127,128,129,130,131,132,133,134,135,136,137]. Stem cell-derived beta cell replacement is an emerging therapeutic avenue, where lab-grown beta cells can be transplanted into individuals with compromised beta cell function as well as in animal models of T1D [138,139,140,141]. Research on encapsulated beta cell implants, which protect transplanted cells from immune attack, is ongoing [130,142,143,144,145,146,147]. These implants have shown potential in animal models to restore insulin production and maintain glucose homeostasis, though they are still in experimental phases for adolescents and teens.
Gene therapy is another experimental approach focused on beta cell preservation [148,149,150,151]. By modifying immune or beta cell genes, gene therapy aims to reduce immune sensitivity to beta cells or enhance beta cell resilience [152]. Although this approach is in early development stages, gene editing technologies such as CRISPR offer the potential to correct genetic susceptibilities that contribute to beta cell dysfunction [153].
4.3.2. Role of the Microbiome in Beta Cell Health and Implications for Pre-Diabetes Interventions
The gut microbiome, which influences immune function and inflammation, has emerged as a potential factor in beta cell preservation [154]. Alterations in gut microbiota composition have been linked to autoimmune diseases, including T1D [155,156,157,158,159,160]. Preclinical studies indicate that certain gut bacteria may play a role in modulating immune responses and maintaining beta cell health [161,162,163] . Probiotic and prebiotic interventions that aim to improve gut microbiome balance are currently under investigation as potential pre-diabetes interventions [164,165,166].
Clinical trials are examining whether gut microbiome modulation can reduce T1D risk in at-risk youth by promoting beneficial bacteria that support immune tolerance and reduce autoimmune activity. While research is still in the early stages, the microbiome represents an exciting new frontier in understanding and potentially mitigating autoimmune processes that lead to beta cell destruction.
In summary, beta cell preservation strategies offer hope for delaying or preventing T1D onset in adolescents and teens. By combining pharmacological interventions, lifestyle modifications, and experimental therapies, researchers aim to slow beta cell decline and reduce the autoimmune attack in high-risk individuals. Advances in regenerative medicine and an increased understanding of the gut microbiome further broaden the scope of potential interventions. As research progresses, the integration of these strategies will play an essential role in preventive T1D care, ultimately improving quality of life and long-term outcomes for at-risk youth
5. Social, Emotional, and Psychological Impacts of Pre-Diabetes and T1D Risk
The psychological, social, and emotional implications of a pre-diabetes or T1D at-risk diagnosis can be significant for adolescents and their families. This stage of life is already marked by considerable emotional and social development, and an added health risk can intensify challenges for both the affected individuals and those around them. Addressing the mental health impacts of pre-diabetes, understanding the role of family and peer dynamics, and providing targeted mental health interventions are essential for supporting these youth. This section delves into these dimensions and highlights the importance of mental health care integration in T1D risk management.
5.1. Psychological Burden of Screening and Diagnosis
5.1.1. Mental Health Implications of an At-Risk or Pre-Diabetes Diagnosis
An at-risk or pre-diabetes diagnosis in adolescents often brings about a range of emotional reactions, including anxiety, fear, sadness, and confusion [167,168]. Adolescents aware of their potential T1D risk may experience heightened anxiety about the future, particularly regarding the potential development of a chronic, lifelong illness [169,170]. This anxiety can manifest as preoccupation with health, fear of disease progression, and a sense of uncertainty about life goals and physical capabilities.
The mental health burden also extends to families, as parents or guardians of at-risk youth may feel a sense of guilt, worry, and helplessness, fearing that they may not be able to prevent the child’s disease progression [171]. These families often undergo heightened vigilance, closely monitoring the adolescent's diet, physical activity, and overall lifestyle, which can create family tensions, stress, and parental burnout over time.
5.1.2. Impact of Continuous Glucose Monitoring (CGM) or Self-Monitoring Requirements on Quality of Life
In cases where adolescents are asked to use CGM or conduct self-monitoring as part of their risk management, there can be a significant impact on their quality of life. The routine nature of glucose monitoring can cause feelings of frustration, stress, and self-consciousness, particularly in social settings where self-monitoring or wearing CGM devices may draw unwanted attention. Some adolescents may feel “different” or “isolated” from their peers, leading to social withdrawal, especially in cases where they perceive their health routines as a source of embarrassment.
Moreover, frequent monitoring can lead to hyper-vigilance around blood sugar levels, with adolescents becoming increasingly preoccupied with minor glycemic fluctuations and concerned over the consequences. This heightened focus on health can inadvertently detract from other developmental experiences and contribute to a decline in overall life satisfaction.
5.2. Family and Peer Dynamics
5.2.1. Influence of Family Dynamics and Peer Relationships on Dietary Adherence and Lifestyle Changes
Family dynamics play a crucial role in the management of pre-diabetes in adolescents [172,173]. The support or lack of support from family members can influence how adolescents adhere to dietary and lifestyle modifications [173]. Supportive families often create environments that prioritize health-conscious meals, encourage regular physical activity, and foster open conversations about feelings related to health risks [174,175]. In such environments, adolescents are more likely to accept and adhere to recommended lifestyle changes, which can significantly improve their quality of life.
Conversely, family conflicts or strained relationships can hinder adherence to lifestyle modifications. For example, families with conflicting dietary preferences or unstructured mealtimes may struggle to implement recommended dietary changes, creating frustration and resistance in adolescents. Similarly, if family members do not understand the importance of lifestyle modifications, adolescents may feel unsupported in their efforts to adopt healthier habits, potentially increasing feelings of isolation and non-compliance.
Peer relationships also influence dietary adherence and lifestyle changes [176]. Adolescents with strong peer support may feel more motivated to adhere to health recommendations if they have friends who encourage or share their health goals. However, peer pressure to engage in unhealthy behaviors, such as consuming sugary or high-fat foods or neglecting physical activity, can challenge an adolescent’s ability to maintain their pre-diabetes management plan [177]. This peer influence can contribute to a heightened risk of non-adherence and potential disease progression.
5.2.2. Importance of Supportive Family Environments and Community Resources
A supportive family environment, combined with access to community resources, can help sustain lifestyle modifications and reduce the mental health burden of a pre-diabetes diagnosis. Community resources, such as diabetes support groups, nutritional counseling, and physical activity programs, provide adolescents and their families with knowledge and tools for effective disease management. When families participate in community-based programs, they not only reinforce the adolescent’s adherence but also gain social support and a sense of solidarity, which can alleviate feelings of isolation and stress.
Community resources that foster social engagement and healthy lifestyle habits allow adolescents to build relationships with others facing similar challenges, creating a sense of belonging and resilience. This sense of connectedness can be instrumental in supporting adolescents’ motivation to follow recommended lifestyle modifications, thus reducing the risk of disease progression.
5.3. Interventions to Support Mental Health and Coping Skills
5.3.1. Counseling, Group Support, and Cognitive-Behavioral Therapy (CBT) for Youth with Pre-Diabetes and Their Families
Given the significant psychological burden associated with T1D risk, counseling and therapeutic interventions are crucial for promoting mental well-being in at-risk adolescents (Table 4). Counseling services that address specific fears, anxieties, and uncertainties about health can empower adolescents to manage their emotions more effectively. Group support programs, which bring together adolescents facing similar challenges, provide a platform for mutual support, encouragement, and the sharing of coping strategies. Group support helps reduce the sense of isolation and provides reassurance that others face similar fears and anxieties.
Cognitive-Behavioral Therapy (CBT) is particularly effective for helping adolescents develop positive coping skills and reframe negative thought patterns associated with their health status (Table 4). CBT can be tailored to help adolescents manage anxiety related to disease progression, overcome feelings of social isolation, and build resilience to health-related stressors. Moreover, CBT techniques can be extended to family members, helping them manage their own anxieties and develop constructive strategies for supporting the adolescent’s journey.
5.3.2. Integrating Mental Health Services into T1D Prevention Programs
Integrating mental health services into T1D prevention programs provides a holistic approach to pre-diabetes management (Table 4). Addressing the mental health needs of adolescents with a high risk of T1D is essential for preventing anxiety, depression, and other mental health issues that can arise in the face of a health challenge. Incorporating regular mental health assessments and access to counseling as part of T1D risk management allows for early detection of emotional difficulties and provides timely interventions to address them.
Mental health services can also help adolescents build coping skills that are useful in long-term disease management. Stress reduction techniques, such as mindfulness-based stress reduction (MBSR), relaxation exercises, and guided imagery, can be incorporated into T1D prevention programs to promote emotional stability and reduce health-related anxiety. Additionally, psychoeducational programs that involve families can strengthen family cohesion, enhance communication, and equip family members with strategies to provide effective emotional support.
In summary, the social, emotional, and psychological impacts of a pre-diabetes or T1D risk diagnosis are profound, particularly for adolescents who face significant lifestyle changes and uncertainties about their health. Addressing these impacts requires a multi-dimensional approach that considers mental health, family dynamics, and community support. By incorporating psychological interventions, fostering supportive family and peer relationships, and integrating mental health services into T1D prevention programs, healthcare providers can help at-risk youth develop the resilience and coping skills needed to navigate the challenges of their diagnosis. This holistic approach not only supports beta cell preservation efforts but also promotes overall well-being, empowering adolescents to live fulfilling lives even in the face of health risks.
6. Future Directions and Recommendations
As our understanding of T1D and pre-diabetes in youth continues to advance, a comprehensive strategy integrating screening, preventive care, research, and supportive policies is essential to reduce disease progression and improve quality of life for at-risk adolescents. Future directions should focus on developing targeted screening initiatives, advancing research in diet and psychosocial care, and advocating for policies that support preventative and educational resources.
6.1. Integrating Screening with Preventative Care
6.1.1. Need for Universal or Targeted Screening Programs in Schools or Primary Care
Implementing universal or targeted screening programs in schools and primary care settings can significantly enhance early detection of T1D risk in children and adolescents. T1D is a chronic autoimmune condition that can affect individuals regardless of family history. While first-degree relatives of individuals with T1D are approximately 15 times more likely to develop the disease compared to the general population, the majority of new cases—approximately over 80%—occur in individuals without any known family history of the condition [178]. This highlights the complex interplay of genetic predisposition and environmental factors in T1D pathogenesis, underscoring the need for broader population-based screening strategies to identify at-risk individuals. Universal screening would make it possible to identify at-risk individuals without relying on family history alone, capturing those who may not be aware of their susceptibility. This approach could involve routine blood tests for diabetes-associated autoantibodies and glucose levels during pediatric check-ups or school health programs, allowing healthcare providers to flag at-risk youth early on.
Targeted screening, on the other hand, could be focused on youth with high-risk factors, such as those with a family history of T1D or genetic predispositions. This approach may be more feasible in terms of resources while still effectively identifying children who would benefit most from early intervention. However, both universal and targeted approaches require careful consideration of privacy and resource allocation to ensure screenings are conducted in a way that respects families’ rights and meets the healthcare system's capacity.
6.1.2. Combining Screening with Family Education and Resources for Early Intervention
Screening alone is not sufficient without the necessary educational and resource-based support to guide families and youth through early interventions. Combining screening efforts with educational resources, such as nutritional counseling and information about lifestyle adjustments, can empower families to adopt preventive measures. Family-centered education programs should include clear guidance on dietary choices, the importance of physical activity, and the benefits of regular health monitoring to mitigate T1D risk factors.
This integrated model could extend to providing families with access to online resources, support groups, and trained counselors who can answer questions and offer strategies for managing pre-diabetes risk. Schools, community centers, and pediatric clinics could serve as hubs for disseminating educational materials and connecting families with local health resources, maximizing the impact of early screening initiatives.
As authors and advocates for advancing care and support for individuals affected by T1D, we propose the development of a unified, disease-focused virtual platform to enhance community engagement, emotional well-being, and patient education. While smaller online groups and forums currently provide valuable support, a centralized forum led by trusted organizations such as the NIH, TrialNet, DRI, and ADA could be transformative. By combining monthly virtual peer support meetings with expert moderation and accurate information curation, such a platform would empower individuals with T1D, their families, and caregivers to connect, share experiences, and access reliable guidance. This initiative could foster resilience, improve mental health, and complement traditional medical care, setting a new standard for T1D community support and education.
6.2. Further Research on Nutrition, Beta Cell Preservation, and Psychosocial Support
6.2.1. Areas of Potential Research: Large-Scale Longitudinal Studies on Diet and Psychosocial Interventions
Further research is needed to clarify the role of dietary patterns, lifestyle modifications, and psychosocial interventions in the progression from pre-diabetes to T1D. Large-scale longitudinal studies tracking at-risk youth over time would provide valuable data on how various dietary choices and interventions impact beta cell function and disease progression. Such studies could investigate specific diets to determine their long-term effects on insulin sensitivity and beta cell preservation in youth populations.
Psychosocial research should also focus on the mental health impacts of living with T1D risk and explore which interventions best support emotional resilience and adherence to lifestyle recommendations. Studies evaluating the effectiveness of stress management programs, family therapy, and peer support groups for at-risk youth and their families could lead to standardized psychosocial protocols that enhance coping skills and reduce anxiety associated with pre-diabetes.
6.2.2. Expanding Access to Mental Health Support and Nutrition Education in At-Risk Populations
Improving access to mental health and nutrition support is essential to a holistic approach to T1D prevention. Mental health professionals trained in pediatric and adolescent diabetes can help young people and their families navigate the psychological challenges of a pre-diabetes diagnosis, building resilience and empowering them to adhere to preventive measures. Expanding mental health services, including telehealth options, would help ensure that more families can access counseling and support, regardless of geographic or economic barriers.
Nutrition education also plays a key role in T1D prevention, as balanced diets and healthy eating habits can positively impact metabolic health. Access to professional nutritional counseling can provide tailored dietary recommendations, which may be more effective than generic dietary advice. Ensuring that at-risk families have access to these services, possibly through school health programs or community health centers, could improve outcomes and establish healthier lifestyles from an early age.
6.3. Policy Implications and Advocacy
6.3.1. Role of Public Health Policies in Supporting Preventive Care, Nutrition, and Mental Health Resources for At-Risk Youth
Public health policies that prioritize preventive care, nutritional resources, and mental health support are essential to reducing the burden of T1D in at-risk youth. Policymakers should consider frameworks that promote routine screenings in schools and primary care as part of national health guidelines. Such policies could ensure that screening for diabetes risk is covered for children and adolescents, enabling early identification and timely interventions.
Nutrition-focused policies can support T1D prevention by promoting access to healthy foods in schools, particularly in underserved communities. Programs that provide funding for school meal programs, nutrition education, and access to fruits and vegetables in local markets can help create an environment that encourages healthier dietary choices. Public health policies should also address the mental health needs of at-risk youth by advocating for mental health resources in schools and healthcare facilities, ensuring that adolescents have access to professional support.
6.3.2. Advocacy for Insurance Coverage of Early Screening, Nutritional Counseling, and Psychosocial Support
One of the significant barriers to comprehensive care for pre-diabetes is the lack of insurance coverage for preventive screenings and counseling services. Advocacy efforts are needed to push for insurance policies that cover the costs of screening, nutritional counseling, and mental health support as preventive measures for at-risk youth. Coverage of these services would alleviate the financial burden on families, making it easier for them to access the resources necessary to manage pre-diabetes risk.
Collaborations between healthcare providers, advocacy groups, and policymakers are essential to driving these policy changes. Organizations focused on diabetes prevention, such as JDRF and ADA, can play an influential role by presenting data to support the cost-effectiveness of early intervention and the long-term health benefits of preventive measures. Advocacy for broader insurance coverage would support a proactive approach to healthcare, reducing the incidence of T1D and improving the quality of life for youth and families.
7. Conclusions
Effectively managing T1D risk in adolescents and teens requires a comprehensive, interdisciplinary approach that addresses the unique challenges of this age group. Integrating routine screening with preventive care offers a powerful opportunity to identify individuals with pre-diabetes early, particularly through targeted programs in schools and primary care settings. Paired with family-centered education, these screenings can equip at-risk youth and their families with the knowledge and resources to implement lifestyle modifications that may delay, prevent disease progression, or even improve quality of life.
Future research on nutrition, beta cell preservation, and psychosocial interventions is essential to refining the prevention landscape. Studies exploring the impact of diet, exercise, and mental health support on pre-diabetes in youth will deepen our understanding of the most effective strategies for disease prevention. Further, advances in pharmacological therapies and regenerative approaches, alongside evolving insights into the role of the microbiome, promise to unlock new avenues for preserving beta cell function in this vulnerable population.
Public health policies and insurance reforms are equally critical, ensuring that preventive resources, from screening and nutritional counseling to mental health support, are accessible to all adolescents at risk. Advocacy for such policies not only supports comprehensive, equitable care but also shifts the focus from reactive to proactive healthcare. By adopting these multifaceted strategies, the healthcare community can work toward a more preventive model of care that enhances long-term outcomes, empowers families, and improves quality of life for adolescents and teens at risk of T1D.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not Applicable.
Acknowledgments
We are grateful to Dr. Valerie Gramling for the critical reading of the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- DiMeglio, L.A.; Evans-Molina, C.; Oram, R.A. Type 1 diabetes. Lancet 2018, 391, 2449–2462. [Google Scholar] [CrossRef]
- Katsarou, A.; Gudbjörnsdottir, S.; Rawshani, A.; Dabelea, D.; Bonifacio, E.; Anderson, B.J.; Jacobsen, L.M.; Schatz, D.A.; Lernmark, Å. Type 1 diabetes mellitus. Nat Rev Dis Primers 2017, 3, 17016. [Google Scholar] [CrossRef] [PubMed]
- Mittal, R.; Camick, N.; Lemos, J.R.N.; Hirani, K. Gene-environment interaction in the pathophysiology of type 1 diabetes. Front Endocrinol (Lausanne) 2024, 15, 1335435. [Google Scholar] [CrossRef]
- Barnett, R. Type 1 diabetes. Lancet 2018, 391, 195. [Google Scholar] [CrossRef]
- VanBuecken, D.; Lord, S.; Greenbaum, C.J. Changing the Course of Disease in Type 1 Diabetes. In Endotext, Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., Hofland, J.; MDText.com, Inc. Copyright © 2000-2024, MDText.com, Inc.: South Dartmouth (MA), 2000. [Google Scholar]
- Subramanian, S.; Khan, F.; Hirsch, I.B. New advances in type 1 diabetes. Bmj 2024, 384, e075681. [Google Scholar] [CrossRef]
- Zajec, A.; Trebušak Podkrajšek, K.; Tesovnik, T.; Šket, R.; Čugalj Kern, B.; Jenko Bizjan, B.; Šmigoc Schweiger, D.; Battelino, T.; Kovač, J. Pathogenesis of Type 1 Diabetes: Established Facts and New Insights. Genes (Basel) 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Buchberger, B.; Huppertz, H.; Krabbe, L.; Lux, B.; Mattivi, J.T.; Siafarikas, A. Symptoms of depression and anxiety in youth with type 1 diabetes: A systematic review and meta-analysis. Psychoneuroendocrinology 2016, 70, 70–84. [Google Scholar] [CrossRef]
- Alfadhly, A.F.; Mohammed, A.; Almalki, B.; Alfaez, S.; Mubarak, A.; Alotaibi, E.; Alomran, G.; Almathami, J.; Bazhair, N.; AlShamrani, N.; et al. Moderating effect for illness uncertainty on the relationship of depressive and anxiety symptoms among patients with type 1 diabetes in Taif region, Saudi Arabia. J Family Med Prim Care 2024, 13, 3576–3589. [Google Scholar] [CrossRef]
- Vallis, M.; Willaing, I.; Holt, R.I.G. Emerging adulthood and Type 1 diabetes: Insights from the DAWN2 Study. Diabet Med 2018, 35, 203–213. [Google Scholar] [CrossRef]
- Bombaci, B.; Torre, A.; Longo, A.; Pecoraro, M.; Papa, M.; Sorrenti, L.; La Rocca, M.; Lombardo, F.; Salzano, G. Psychological and Clinical Challenges in the Management of Type 1 Diabetes during Adolescence: A Narrative Review. Children (Basel) 2024, 11. [Google Scholar] [CrossRef]
- Gong, B.; Yang, W.; Xing, Y.; Lai, Y.; Shan, Z. Global, regional, and national burden of type 1 diabetes in adolescents and young adults. Pediatr Res 2024. [Google Scholar] [CrossRef]
- Mayer-Davis, E.J.; Dabelea, D.; Lawrence, J.M. Incidence Trends of Type 1 and Type 2 Diabetes among Youths, 2002-2012. N Engl J Med 2017, 377, 301. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, M.A.; Eisenbarth, G.S.; Michels, A.W. Type 1 diabetes. Lancet 2014, 383, 69–82. [Google Scholar] [CrossRef]
- Lucier, J.; Mathias, P.M. Type 1 Diabetes. In StatPearls; StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC.: Treasure Island (FL), 2024. [Google Scholar]
- Noble, J.A.; Valdes, A.M. Genetics of the HLA region in the prediction of type 1 diabetes. Curr Diab Rep 2011, 11, 533–542. [Google Scholar] [CrossRef]
- Insel, R.A.; Dunne, J.L.; Atkinson, M.A.; Chiang, J.L.; Dabelea, D.; Gottlieb, P.A.; Greenbaum, C.J.; Herold, K.C.; Krischer, J.P.; Lernmark, Å.; et al. Staging presymptomatic type 1 diabetes: A scientific statement of JDRF, the Endocrine Society, and the American Diabetes Association. Diabetes Care 2015, 38, 1964–1974. [Google Scholar] [CrossRef]
- Siljander, H.T.; Hermann, R.; Hekkala, A.; Lähde, J.; Tanner, L.; Keskinen, P.; Ilonen, J.; Simell, O.; Veijola, R.; Knip, M. Insulin secretion and sensitivity in the prediction of type 1 diabetes in children with advanced β-cell autoimmunity. Eur J Endocrinol 2013, 169, 479–485. [Google Scholar] [CrossRef]
- Ziegler, A.G.; Rewers, M.; Simell, O.; Simell, T.; Lempainen, J.; Steck, A.; Winkler, C.; Ilonen, J.; Veijola, R.; Knip, M.; et al. Seroconversion to multiple islet autoantibodies and risk of progression to diabetes in children. JAMA 2013, 309, 2473–2479. [Google Scholar] [CrossRef] [PubMed]
- Pöllänen, P.M.; Ryhänen, S.J.; Toppari, J.; Ilonen, J.; Vähäsalo, P.; Veijola, R.; Siljander, H.; Knip, M. Dynamics of Islet Autoantibodies During Prospective Follow-Up From Birth to Age 15 Years. J Clin Endocrinol Metab 2020, 105, e4638–4651. [Google Scholar] [CrossRef]
- Skyler, J.S.; Bakris, G.L.; Bonifacio, E.; Darsow, T.; Eckel, R.H.; Groop, L.; Groop, P.H.; Handelsman, Y.; Insel, R.A.; Mathieu, C.; et al. Differentiation of Diabetes by Pathophysiology, Natural History, and Prognosis. Diabetes 2017, 66, 241–255. [Google Scholar] [CrossRef]
- Venugopal, S.K.; Mowery, M.L.; Jialal, I. Biochemistry, C Peptide. In StatPearls; StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC.: Treasure Island (FL), 2024. [Google Scholar]
- Leighton, E.; Sainsbury, C.A.; Jones, G.C. A Practical Review of C-Peptide Testing in Diabetes. Diabetes Ther 2017, 8, 475–487. [Google Scholar] [CrossRef]
- Jamiołkowska-Sztabkowska, M.; Głowińska-Olszewska, B.; Bossowski, A. C-peptide and residual β-cell function in pediatric diabetes - state of the art. Pediatr Endocrinol Diabetes Metab 2021, 27, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.N.; Collins, K.S.; Lam, A.; Karpen, S.R.; Greeno, B.; Walker, F.; Lozano, A.; Atabakhsh, E.; Ahmed, S.T.; Marinac, M.; et al. C-peptide and metabolic outcomes in trials of disease modifying therapy in new-onset type 1 diabetes: An individual participant meta-analysis. Lancet Diabetes Endocrinol 2023, 11, 915–925. [Google Scholar] [CrossRef] [PubMed]
- Latres, E.; Greenbaum, C.J.; Oyaski, M.L.; Dayan, C.M.; Colhoun, H.M.; Lachin, J.M.; Skyler, J.S.; Rickels, M.R.; Ahmed, S.T.; Dutta, S.; et al. Evidence for C-Peptide as a Validated Surrogate to Predict Clinical Benefits in Trials of Disease-Modifying Therapies for Type 1 Diabetes. Diabetes 2024, 73, 823–833. [Google Scholar] [CrossRef] [PubMed]
- Sims, E.K.; Cuthbertson, D.; Felton, J.L.; Ismail, H.M.; Nathan, B.M.; Jacobsen, L.M.; Paprocki, E.; Pugliese, A.; Palmer, J.; Atkinson, M.; et al. Persistence of β-Cell Responsiveness for Over Two Years in Autoantibody-Positive Children With Marked Metabolic Impairment at Screening. Diabetes Care 2022, 45, 2982–2990. [Google Scholar] [CrossRef] [PubMed]
- Ismail, H.M.; Cuthbertson, D.; Gitelman, S.E.; Skyler, J.S.; Steck, A.K.; Rodriguez, H.; Atkinson, M.; Nathan, B.M.; Redondo, M.J.; Herold, K.C.; et al. The Transition From a Compensatory Increase to a Decrease in C-peptide During the Progression to Type 1 Diabetes and Its Relation to Risk. Diabetes Care 2022, 45, 2264–2270. [Google Scholar] [CrossRef]
- Mittal, R.; Koutras, N.; Maya, J.; Lemos, J.R.N.; Hirani, K. Blood glucose monitoring devices for type 1 diabetes: A journey from the food and drug administration approval to market availability. Front Endocrinol (Lausanne) 2024, 15, 1352302. [Google Scholar] [CrossRef]
- Laffel, L.M.; Kanapka, L.G.; Beck, R.W.; Bergamo, K.; Clements, M.A.; Criego, A.; DeSalvo, D.J.; Goland, R.; Hood, K.; Liljenquist, D.; et al. Effect of Continuous Glucose Monitoring on Glycemic Control in Adolescents and Young Adults With Type 1 Diabetes: A Randomized Clinical Trial. Jama 2020, 323, 2388–2396. [Google Scholar] [CrossRef]
- Laffel, L.M.; Bailey, T.S.; Christiansen, M.P.; Reid, J.L.; Beck, S.E. Accuracy of a Seventh-Generation Continuous Glucose Monitoring System in Children and Adolescents With Type 1 Diabetes. J Diabetes Sci Technol 2023, 17, 962–967. [Google Scholar] [CrossRef]
- Abraham, M.B.; de Bock, M.; Smith, G.J.; Dart, J.; Fairchild, J.M.; King, B.R.; Ambler, G.R.; Cameron, F.J.; McAuley, S.A.; Keech, A.C.; et al. Effect of a Hybrid Closed-Loop System on Glycemic and Psychosocial Outcomes in Children and Adolescents With Type 1 Diabetes: A Randomized Clinical Trial. JAMA Pediatr 2021, 175, 1227–1235. [Google Scholar] [CrossRef]
- Helminen, O.; Pokka, T.; Tossavainen, P.; Ilonen, J.; Knip, M.; Veijola, R. Continuous glucose monitoring and HbA1c in the evaluation of glucose metabolism in children at high risk for type 1 diabetes mellitus. Diabetes Res Clin Pract 2016, 120, 89–96. [Google Scholar] [CrossRef]
- Steck, A.K.; Dong, F.; Taki, I.; Hoffman, M.; Klingensmith, G.J.; Rewers, M.J. Early hyperglycemia detected by continuous glucose monitoring in children at risk for type 1 diabetes. Diabetes Care 2014, 37, 2031–2033. [Google Scholar] [CrossRef] [PubMed]
- Steck, A.K.; Dong, F.; Taki, I.; Hoffman, M.; Simmons, K.; Frohnert, B.I.; Rewers, M.J. Continuous Glucose Monitoring Predicts Progression to Diabetes in Autoantibody Positive Children. J Clin Endocrinol Metab 2019, 104, 3337–3344. [Google Scholar] [CrossRef] [PubMed]
- Steck, A.K.; Dong, F.; Geno Rasmussen, C.; Bautista, K.; Sepulveda, F.; Baxter, J.; Yu, L.; Frohnert, B.I.; Rewers, M.J. CGM Metrics Predict Imminent Progression to Type 1 Diabetes: Autoimmunity Screening for Kids (ASK) Study. Diabetes Care 2022, 45, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Pöllänen, P.M.; Lempainen, J.; Laine, A.P.; Toppari, J.; Veijola, R.; Vähäsalo, P.; Ilonen, J.; Siljander, H.; Knip, M. Characterisation of rapid progressors to type 1 diabetes among children with HLA-conferred disease susceptibility. Diabetologia 2017, 60, 1284–1293. [Google Scholar] [CrossRef]
- Bougnères, P.; Le Fur, S.; Kamatani, Y.; Mai, T.N.; Belot, M.P.; Perge, K.; Shao, X.; Lathrop, M.; Valleron, A.J. Genomic variants associated with age at diagnosis of childhood-onset type 1 diabetes. J Hum Genet 2024, 69, 585–590. [Google Scholar] [CrossRef]
- Herold, K.C.; Bundy, B.N.; Long, S.A.; Bluestone, J.A.; DiMeglio, L.A.; Dufort, M.J.; Gitelman, S.E.; Gottlieb, P.A.; Krischer, J.P.; Linsley, P.S.; et al. An Anti-CD3 Antibody, Teplizumab, in Relatives at Risk for Type 1 Diabetes. N Engl J Med 2019, 381, 603–613. [Google Scholar] [CrossRef] [PubMed]
- Sims, E.K.; Bundy, B.N.; Stier, K.; Serti, E.; Lim, N.; Long, S.A.; Geyer, S.M.; Moran, A.; Greenbaum, C.J.; Evans-Molina, C.; Herold, K.C. Teplizumab improves and stabilizes beta cell function in antibody-positive high-risk individuals. Sci Transl Med 2021, 13. [Google Scholar] [CrossRef]
- Russell, W.E.; Bundy, B.N.; Anderson, M.S.; Cooney, L.A.; Gitelman, S.E.; Goland, R.S.; Gottlieb, P.A.; Greenbaum, C.J.; Haller, M.J.; Krischer, J.P.; et al. Abatacept for Delay of Type 1 Diabetes Progression in Stage 1 Relatives at Risk: A Randomized, Double-Masked, Controlled Trial. Diabetes Care 2023, 46, 1005–1013. [Google Scholar] [CrossRef]
- Ke, Q.; Kroger, C.J.; Clark, M.; Tisch, R.M. Evolving Antibody Therapies for the Treatment of Type 1 Diabetes. Front Immunol 2020, 11, 624568. [Google Scholar] [CrossRef]
- Herold, K.C.; Gitelman, S.E.; Ehlers, M.R.; Gottlieb, P.A.; Greenbaum, C.J.; Hagopian, W.; Boyle, K.D.; Keyes-Elstein, L.; Aggarwal, S.; Phippard, D.; et al. Teplizumab (anti-CD3 mAb) treatment preserves C-peptide responses in patients with new-onset type 1 diabetes in a randomized controlled trial: Metabolic and immunologic features at baseline identify a subgroup of responders. Diabetes 2013, 62, 3766–3774. [Google Scholar] [CrossRef]
- Steck, A.K.; Vehik, K.; Bonifacio, E.; Lernmark, A.; Ziegler, A.G.; Hagopian, W.A.; She, J.; Simell, O.; Akolkar, B.; Krischer, J.; et al. Predictors of Progression From the Appearance of Islet Autoantibodies to Early Childhood Diabetes: The Environmental Determinants of Diabetes in the Young (TEDDY). Diabetes Care 2015, 38, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Hilliard, M.E.; De Wit, M.; Wasserman, R.M.; Butler, A.M.; Evans, M.; Weissberg-Benchell, J.; Anderson, B.J. Screening and support for emotional burdens of youth with type 1 diabetes: Strategies for diabetes care providers. Pediatr Diabetes 2018, 19, 534–543. [Google Scholar] [CrossRef] [PubMed]
- Stene, L.C.; Norris, J.M.; Rewers, M.J. Risk Factors for Type 1 Diabetes. In Diabetes in America; Lawrence, J.M., Casagrande, S.S., Herman, W.H., Wexler, D.J., Cefalu, W.T., Eds.; National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK): Bethesda (MD), 2023. [Google Scholar]
- Insel, R.; Dutta, S.; Hedrick, J. Type 1 Diabetes: Disease Stratification. Biomed Hub 2017, 2, 111–126. [Google Scholar] [CrossRef]
- Moore, D.J.; Leibel, N.I.; Polonsky, W.; Rodriguez, H. Recommendations for Screening and Monitoring the Stages of Type 1 Diabetes in the Immune Therapy Era. Int J Gen Med 2024, 17, 3003–3014. [Google Scholar] [CrossRef]
- Aly, T.A.; Ide, A.; Humphrey, K.; Barker, J.M.; Steck, A.; Erlich, H.A.; Yu, L.; Miao, D.; Redondo, M.J.; McFann, K.; et al. Genetic prediction of autoimmunity: Initial oligogenic prediction of anti-islet autoimmunity amongst DR3/DR4-DQ8 relatives of patients with type 1A diabetes. J Autoimmun 2005, 25 Suppl, 40–45. [Google Scholar] [CrossRef]
- Aly, T.A.; Ide, A.; Jahromi, M.M.; Barker, J.M.; Fernando, M.S.; Babu, S.R.; Yu, L.; Miao, D.; Erlich, H.A.; Fain, P.R.; et al. Extreme genetic risk for type 1A diabetes. Proc Natl Acad Sci U S A 2006, 103, 14074–14079. [Google Scholar] [CrossRef] [PubMed]
- Erlich, H.; Valdes, A.M.; Noble, J.; Carlson, J.A.; Varney, M.; Concannon, P.; Mychaleckyj, J.C.; Todd, J.A.; Bonella, P.; Fear, A.L.; et al. HLA DR-DQ haplotypes and genotypes and type 1 diabetes risk: Analysis of the type 1 diabetes genetics consortium families. Diabetes 2008, 57, 1084–1092. [Google Scholar] [CrossRef]
- Noble, J.A. Fifty years of HLA-associated type 1 diabetes risk: History, current knowledge, and future directions. Front Immunol 2024, 15, 1457213. [Google Scholar] [CrossRef]
- Zhao, L.P.; Papadopoulos, G.K.; Skyler, J.S.; Pugliese, A.; Parikh, H.M.; Kwok, W.W.; Lybrand, T.P.; Bondinas, G.P.; Moustakas, A.K.; Wang, R.; et al. HLA Class II (DR, DQ, DP) Genes Were Separately Associated With the Progression From Seroconversion to Onset of Type 1 Diabetes Among Participants in Two Diabetes Prevention Trials (DPT-1 and TN07). Diabetes Care 2024, 47, 826–834. [Google Scholar] [CrossRef]
- Greenbaum, C.J. A Key to T1D Prevention: Screening and Monitoring Relatives as Part of Clinical Care. Diabetes 2021, 70, 1029–1037. [Google Scholar] [CrossRef]
- Phillip, M.; Achenbach, P.; Addala, A.; Albanese-O'Neill, A.; Battelino, T.; Bell, K.J.; Besser, R.E.J.; Bonifacio, E.; Colhoun, H.M.; Couper, J.J.; et al. Consensus Guidance for Monitoring Individuals With Islet Autoantibody-Positive Pre-Stage 3 Type 1 Diabetes. Diabetes Care 2024, 47, 1276–1298. [Google Scholar] [CrossRef] [PubMed]
- Sims, E.K.; Besser, R.E.J.; Dayan, C.; Geno Rasmussen, C.; Greenbaum, C.; Griffin, K.J.; Hagopian, W.; Knip, M.; Long, A.E.; Martin, F.; et al. Screening for Type 1 Diabetes in the General Population: A Status Report and Perspective. Diabetes 2022, 71, 610–623. [Google Scholar] [CrossRef]
- Lamichhane, S.; Ahonen, L.; Dyrlund, T.S.; Kemppainen, E.; Siljander, H.; Hyöty, H.; Ilonen, J.; Toppari, J.; Veijola, R.; Hyötyläinen, T.; et al. Dynamics of Plasma Lipidome in Progression to Islet Autoimmunity and Type 1 Diabetes - Type 1 Diabetes Prediction and Prevention Study (DIPP). Sci Rep 2018, 8, 10635. [Google Scholar] [CrossRef] [PubMed]
- Lamichhane, S.; Ahonen, L.; Dyrlund, T.S.; Dickens, A.M.; Siljander, H.; Hyöty, H.; Ilonen, J.; Toppari, J.; Veijola, R.; Hyötyläinen, T.; et al. Cord-Blood Lipidome in Progression to Islet Autoimmunity and Type 1 Diabetes. Biomolecules 2019, 9. [Google Scholar] [CrossRef]
- Sen, P.; Dickens, A.M.; López-Bascón, M.A.; Lindeman, T.; Kemppainen, E.; Lamichhane, S.; Rönkkö, T.; Ilonen, J.; Toppari, J.; Veijola, R.; et al. Metabolic alterations in immune cells associate with progression to type 1 diabetes. Diabetologia 2020, 63, 1017–1031. [Google Scholar] [CrossRef]
- Overgaard, A.J.; Weir, J.M.; Jayawardana, K.; Mortensen, H.B.; Pociot, F.; Meikle, P.J. Plasma lipid species at type 1 diabetes onset predict residual beta-cell function after 6 months. Metabolomics 2018, 14, 158. [Google Scholar] [CrossRef] [PubMed]
- Gootjes, C.; Zwaginga, J.J.; Roep, B.O.; Nikolic, T. Functional Impact of Risk Gene Variants on the Autoimmune Responses in Type 1 Diabetes. Front Immunol 2022, 13, 886736. [Google Scholar] [CrossRef]
- Hossen, M.M.; Ma, Y.; Yin, Z.; Xia, Y.; Du, J.; Huang, J.Y.; Huang, J.J.; Zou, L.; Ye, Z.; Huang, Z. Current understanding of CTLA-4: From mechanism to autoimmune diseases. Front Immunol 2023, 14, 1198365. [Google Scholar] [CrossRef]
- Frohnert, B.I.; Webb-Robertson, B.J.; Bramer, L.M.; Reehl, S.M.; Waugh, K.; Steck, A.K.; Norris, J.M.; Rewers, M. Predictive Modeling of Type 1 Diabetes Stages Using Disparate Data Sources. Diabetes 2020, 69, 238–248. [Google Scholar] [CrossRef]
- Watkins, R.A.; Evans-Molina, C.; Blum, J.S.; DiMeglio, L.A. Established and emerging biomarkers for the prediction of type 1 diabetes: A systematic review. Transl Res 2014, 164, 110–121. [Google Scholar] [CrossRef]
- Semova, I.; Levenson, A.E.; Krawczyk, J.; Bullock, K.; Williams, K.A.; Wadwa, R.P.; Shah, A.S.; Khoury, P.R.; Kimball, T.R.; Urbina, E.M.; et al. Type 1 diabetes is associated with an increase in cholesterol absorption markers but a decrease in cholesterol synthesis markers in a young adult population. J Clin Lipidol 2019, 13, 940–946. [Google Scholar] [CrossRef] [PubMed]
- Oresic, M.; Simell, S.; Sysi-Aho, M.; Näntö-Salonen, K.; Seppänen-Laakso, T.; Parikka, V.; Katajamaa, M.; Hekkala, A.; Mattila, I.; Keskinen, P.; et al. Dysregulation of lipid and amino acid metabolism precedes islet autoimmunity in children who later progress to type 1 diabetes. J Exp Med 2008, 205, 2975–2984. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Qi, X.; Zheng, Y.; Zhang, J.; Su, H. Lipid profile alterations and biomarker identification in type 1 diabetes mellitus patients under glycemic control. BMC Endocr Disord 2024, 24, 149. [Google Scholar] [CrossRef]
- Bantle, J.P.; Wylie-Rosett, J.; Albright, A.L.; Apovian, C.M.; Clark, N.G.; Franz, M.J.; Hoogwerf, B.J.; Lichtenstein, A.H.; Mayer-Davis, E.; Mooradian, A.D.; Wheeler, M.L. Nutrition recommendations and interventions for diabetes: A position statement of the American Diabetes Association. Diabetes Care 2008, 31 (Suppl 1), S61–S78. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.; Mitri, J. Dietary Advice For Individuals with Diabetes. In Endotext; Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., Hofland, J., Eds.; MDText.com, Inc. Copyright © 2000-2024, MDText.com, Inc.: South Dartmouth (MA), 2000. [Google Scholar]
- Tsitsou, S.; Athanasaki, C.; Dimitriadis, G.; Papakonstantinou, E. Acute Effects of Dietary Fiber in Starchy Foods on Glycemic and Insulinemic Responses: A Systematic Review of Randomized Controlled Crossover Trials. Nutrients 2023, 15. [Google Scholar] [CrossRef]
- Smart, C.E.; Annan, F.; Higgins, L.A.; Jelleryd, E.; Lopez, M.; Acerini, C.L. ISPAD Clinical Practice Consensus Guidelines 2018: Nutritional management in children and adolescents with diabetes. Pediatr Diabetes 2018, 19 Suppl 27, 136–154. [Google Scholar] [CrossRef]
- Gabbay, M.A.; Sato, M.N.; Finazzo, C.; Duarte, A.J.; Dib, S.A. Effect of cholecalciferol as adjunctive therapy with insulin on protective immunologic profile and decline of residual β-cell function in new-onset type 1 diabetes mellitus. Arch Pediatr Adolesc Med 2012, 166, 601–607. [Google Scholar] [CrossRef]
- Bogdanou, D.; Penna-Martinez, M.; Filmann, N.; Chung, T.L.; Moran-Auth, Y.; Wehrle, J.; Cappel, C.; Huenecke, S.; Herrmann, E.; Koehl, U.; Badenhoop, K. T-lymphocyte and glycemic status after vitamin D treatment in type 1 diabetes: A randomized controlled trial with sequential crossover. Diabetes Metab Res Rev 2017, 33. [Google Scholar] [CrossRef] [PubMed]
- Mishra, A.; Dayal, D.; Sachdeva, N.; Attri, S.V. Effect of 6-months' vitamin D supplementation on residual beta cell function in children with type 1 diabetes: A case control interventional study. J Pediatr Endocrinol Metab 2016, 29, 395–400. [Google Scholar] [CrossRef]
- Giri, D.; Pintus, D.; Burnside, G.; Ghatak, A.; Mehta, F.; Paul, P.; Senniappan, S. Treating vitamin D deficiency in children with type I diabetes could improve their glycaemic control. BMC Res Notes 2017, 10, 465. [Google Scholar] [CrossRef]
- Shih, E.M.; Mittelman, S.; Pitukcheewanont, P.; Azen, C.G.; Monzavi, R. Effects of vitamin D repletion on glycemic control and inflammatory cytokines in adolescents with type 1 diabetes. Pediatr Diabetes 2016, 17, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Biswal, N.; Bethou, A.; Rajappa, M.; Kumar, S.; Vinayagam, V. Does Vitamin D Supplementation Improve Glycaemic Control In Children With Type 1 Diabetes Mellitus? - A Randomized Controlled Trial. J Clin Diagn Res 2017, 11, Sc15–sc17. [Google Scholar] [CrossRef] [PubMed]
- Mahindru, A.; Patil, P.; Agrawal, V. Role of Physical Activity on Mental Health and Well-Being: A Review. Cureus 2023, 15, e33475. [Google Scholar] [CrossRef]
- Cox, E.; Palta, M.; Chewning, B.; Wysocki, T.; Wetterneck, T.; Fiallo-Scharer, R. PCORI Final Research Reports. In Tailoring Resources to Help Children and Parents Manage Type 1 Diabetes; Patient-Centered Outcomes Research Institute (PCORI). Copyright © 2019. University of Wisconsin-Madison. All Rights Reserved.: Washington (DC), 2019. [Google Scholar]
- Zafar, M.I.; Mills, K.E.; Zheng, J.; Regmi, A.; Hu, S.Q.; Gou, L.; Chen, L.L. Low-glycemic index diets as an intervention for diabetes: A systematic review and meta-analysis. Am J Clin Nutr 2019, 110, 891–902. [Google Scholar] [CrossRef]
- Tromba, V.; Silvestri, F. Vegetarianism and type 1 diabetes in children. Metabol Open 2021, 11, 100099. [Google Scholar] [CrossRef]
- Poggioli, R.; Hirani, K.; Jogani, V.G.; Ricordi, C. Modulation of inflammation and immunity by omega-3 fatty acids: A possible role for prevention and to halt disease progression in autoimmune, viral, and age-related disorders. Eur Rev Med Pharmacol Sci 2023, 27, 7380–7400. [Google Scholar] [CrossRef]
- Chaudhary, P.; Janmeda, P.; Docea, A.O.; Yeskaliyeva, B.; Abdull Razis, A.F.; Modu, B.; Calina, D.; Sharifi-Rad, J. Oxidative stress, free radicals and antioxidants: Potential crosstalk in the pathophysiology of human diseases. Front Chem 2023, 11, 1158198. [Google Scholar] [CrossRef] [PubMed]
- Norris, J.M.; Lee, H.S.; Frederiksen, B.; Erlund, I.; Uusitalo, U.; Yang, J.; Lernmark, Å.; Simell, O.; Toppari, J.; Rewers, M.; et al. Plasma 25-Hydroxyvitamin D Concentration and Risk of Islet Autoimmunity. Diabetes 2018, 67, 146–154. [Google Scholar] [CrossRef]
- Park, C.Y.; Shin, S.; Han, S.N. Multifaceted Roles of Vitamin D for Diabetes: From Immunomodulatory Functions to Metabolic Regulations. Nutrients 2024, 16. [Google Scholar] [CrossRef]
- Argano, C.; Mirarchi, L.; Amodeo, S.; Orlando, V.; Torres, A.; Corrao, S. The Role of Vitamin D and Its Molecular Bases in Insulin Resistance, Diabetes, Metabolic Syndrome, and Cardiovascular Disease: State of the Art. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef]
- Wei, Z.; Yoshihara, E.; He, N.; Hah, N.; Fan, W.; Pinto, A.F.M.; Huddy, T.; Wang, Y.; Ross, B.; Estepa, G.; et al. Vitamin D Switches BAF Complexes to Protect β Cells. Cell 2018, 173, 1135–1149.e1115. [Google Scholar] [CrossRef] [PubMed]
- Savastio, S.; Cadario, F.; D'Alfonso, S.; Stracuzzi, M.; Pozzi, E.; Raviolo, S.; Rizzollo, S.; Gigliotti, L.; Boggio, E.; Bellomo, G.; et al. Vitamin D Supplementation Modulates ICOS+ and ICOS- Regulatory T Cell in Siblings of Children With Type 1 Diabetes. J Clin Endocrinol Metab 2020, 105. [Google Scholar] [CrossRef] [PubMed]
- Cadario, F. Vitamin D and ω-3 Polyunsaturated Fatty Acids towards a Personalized Nutrition of Youth Diabetes: A Narrative Lecture. Nutrients 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Infante, M.; Ricordi, C.; Sanchez, J.; Clare-Salzler, M.J.; Padilla, N.; Fuenmayor, V.; Chavez, C.; Alvarez, A.; Baidal, D.; Alejandro, R.; et al. Influence of Vitamin D on Islet Autoimmunity and Beta-Cell Function in Type 1 Diabetes. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.Y.; Zhang, W.G.; Chen, J.J.; Zhang, Z.L.; Han, S.F.; Qin, L.Q. Vitamin D intake and risk of type 1 diabetes: A meta-analysis of observational studies. Nutrients 2013, 5, 3551–3562. [Google Scholar] [CrossRef]
- Akimbekov, N.S.; Coban, S.O.; Atfi, A.; Razzaque, M.S. The role of magnesium in pancreatic beta-cell function and homeostasis. Front Nutr 2024, 11, 1458700. [Google Scholar] [CrossRef]
- Veronese, N.; Watutantrige-Fernando, S.; Luchini, C.; Solmi, M.; Sartore, G.; Sergi, G.; Manzato, E.; Barbagallo, M.; Maggi, S.; Stubbs, B. Effect of magnesium supplementation on glucose metabolism in people with or at risk of diabetes: A systematic review and meta-analysis of double-blind randomized controlled trials. Eur J Clin Nutr 2016, 70, 1354–1359. [Google Scholar] [CrossRef]
- Merz, K.E.; Thurmond, D.C. Role of Skeletal Muscle in Insulin Resistance and Glucose Uptake. Compr Physiol 2020, 10, 785–809. [Google Scholar] [CrossRef]
- Qiu, S.; Cai, X.; Schumann, U.; Velders, M.; Sun, Z.; Steinacker, J.M. Impact of walking on glycemic control and other cardiovascular risk factors in type 2 diabetes: A meta-analysis. PLoS ONE 2014, 9, e109767. [Google Scholar] [CrossRef]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef]
- Reynolds, A.N.; Mann, J.I.; Williams, S.; Venn, B.J. Advice to walk after meals is more effective for lowering postprandial glycaemia in type 2 diabetes mellitus than advice that does not specify timing: A randomised crossover study. Diabetologia 2016, 59, 2572–2578. [Google Scholar] [CrossRef] [PubMed]
- MacMillan, F.; Kirk, A.; Mutrie, N.; Matthews, L.; Robertson, K.; Saunders, D.H. A systematic review of physical activity and sedentary behavior intervention studies in youth with type 1 diabetes: Study characteristics, intervention design, and efficacy. Pediatr Diabetes 2014, 15, 175–189. [Google Scholar] [CrossRef] [PubMed]
- Huerta-Uribe, N.; Ramírez-Vélez, R.; Izquierdo, M.; García-Hermoso, A. Association Between Physical Activity, Sedentary Behavior and Physical Fitness and Glycated Hemoglobin in Youth with Type 1 Diabetes: A Systematic Review and Meta-analysis. Sports Med 2023, 53, 111–123. [Google Scholar] [CrossRef] [PubMed]
- Hakola, L.; Vuorinen, A.L.; Takkinen, H.M.; Niinistö, S.; Ahonen, S.; Rautanen, J.; Peltonen, E.J.; Nevalainen, J.; Ilonen, J.; Toppari, J.; et al. Dietary fatty acid intake in childhood and the risk of islet autoimmunity and type 1 diabetes: The DIPP birth cohort study. Eur J Nutr 2023, 62, 847–856. [Google Scholar] [CrossRef]
- Tatovic, D.; Marwaha, A.; Taylor, P.; Hanna, S.J.; Carter, K.; Cheung, W.Y.; Luzio, S.; Dunseath, G.; Hutchings, H.A.; Holland, G.; et al. Ustekinumab for type 1 diabetes in adolescents: A multicenter, double-blind, randomized phase 2 trial. Nat Med 2024, 30, 2657–2666. [Google Scholar] [CrossRef]
- Ramos, E.L.; Dayan, C.M.; Chatenoud, L.; Sumnik, Z.; Simmons, K.M.; Szypowska, A.; Gitelman, S.E.; Knecht, L.A.; Niemoeller, E.; Tian, W.; Herold, K.C. Teplizumab and β-Cell Function in Newly Diagnosed Type 1 Diabetes. N Engl J Med 2023, 389, 2151–2161. [Google Scholar] [CrossRef]
- Sherry, N.; Hagopian, W.; Ludvigsson, J.; Jain, S.M.; Wahlen, J.; Ferry, R.J., Jr.; Bode, B.; Aronoff, S.; Holland, C.; Carlin, D.; et al. Teplizumab for treatment of type 1 diabetes (Protégé study): 1-year results from a randomised, placebo-controlled trial. Lancet 2011, 378, 487–497. [Google Scholar] [CrossRef]
- Kokori, E.; Olatunji, G.; Ogieuhi, I.J.; Aboje, J.E.; Olatunji, D.; Aremu, S.A.; Igwe, S.C.; Moradeyo, A.; Ajayi, Y.I.; Aderinto, N. Teplizumab's immunomodulatory effects on pancreatic β-cell function in type 1 diabetes mellitus. Clin Diabetes Endocrinol 2024, 10, 23. [Google Scholar] [CrossRef]
- Ma, X.L.; Ge, D.; Hu, X.J. Evaluation of teplizumab's efficacy and safety in treatment of type 1 diabetes mellitus: A systematic review and meta-analysis. World J Diabetes 2024, 15, 1615–1626. [Google Scholar] [CrossRef]
- Thakkar, S.; Chopra, A.; Nagendra, L.; Kalra, S.; Bhattacharya, S. Teplizumab in Type 1 Diabetes Mellitus: An Updated Review. touchREV Endocrinol 2023, 19, 22–30. [Google Scholar] [CrossRef]
- Fanaropoulou, N.M.; Tsatsani, G.C.; Koufakis, T.; Kotsa, K. Teplizumab: Promises and challenges of a recently approved monoclonal antibody for the prevention of type 1 diabetes or preservation of residual beta cell function. Expert Rev Clin Immunol 2024, 20, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Hagopian, W.; Ferry, R.J., Jr.; Sherry, N.; Carlin, D.; Bonvini, E.; Johnson, S.; Stein, K.E.; Koenig, S.; Daifotis, A.G.; Herold, K.C.; Ludvigsson, J. Teplizumab preserves C-peptide in recent-onset type 1 diabetes: Two-year results from the randomized, placebo-controlled Protégé trial. Diabetes 2013, 62, 3901–3908. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Zong, Y.; Ma, Y.; Tian, Y.; Pang, Y.; Zhang, C.; Gao, J. Glucagon-like peptide-1 receptor: Mechanisms and advances in therapy. Signal Transduction and Targeted Therapy 2024, 9, 234. [Google Scholar] [CrossRef] [PubMed]
- Lilly, E. Treatment with tirzepatide in adults with pre-diabetes and obesity or overweight resulted in sustained weight loss and nearly 99% remained diabetes-free at 176 weeks. Available online: https://investor.lilly.com/news-releases/news-release-details/treatment-tirzepatide-adults-pre-diabetes-and-obesity-or (accessed on).
- Herold, K.C.; Pescovitz, M.D.; McGee, P.; Krause-Steinrauf, H.; Spain, L.M.; Bourcier, K.; Asare, A.; Liu, Z.; Lachin, J.M.; Dosch, H.M. Increased T cell proliferative responses to islet antigens identify clinical responders to anti-CD20 monoclonal antibody (rituximab) therapy in type 1 diabetes. J Immunol 2011, 187, 1998–2005. [Google Scholar] [CrossRef]
- Pescovitz, M.D.; Greenbaum, C.J.; Krause-Steinrauf, H.; Becker, D.J.; Gitelman, S.E.; Goland, R.; Gottlieb, P.A.; Marks, J.B.; McGee, P.F.; Moran, A.M.; et al. Rituximab, B-lymphocyte depletion, and preservation of beta-cell function. N Engl J Med 2009, 361, 2143–2152. [Google Scholar] [CrossRef]
- Pescovitz, M.D.; Greenbaum, C.J.; Bundy, B.; Becker, D.J.; Gitelman, S.E.; Goland, R.; Gottlieb, P.A.; Marks, J.B.; Moran, A.; Raskin, P.; et al. B-lymphocyte depletion with rituximab and β-cell function: Two-year results. Diabetes Care 2014, 37, 453–459. [Google Scholar] [CrossRef]
- Rosenzwajg, M.; Salet, R.; Lorenzon, R.; Tchitchek, N.; Roux, A.; Bernard, C.; Carel, J.C.; Storey, C.; Polak, M.; Beltrand, J.; et al. Low-dose IL-2 in children with recently diagnosed type 1 diabetes: A Phase I/II randomised, double-blind, placebo-controlled, dose-finding study. Diabetologia 2020, 63, 1808–1821. [Google Scholar] [CrossRef]
- Agrawal, N.K.; Kant, S. Targeting inflammation in diabetes: Newer therapeutic options. World J Diabetes 2014, 5, 697–710. [Google Scholar] [CrossRef]
- Shao, T.; Verma, H.K.; Pande, B.; Costanzo, V.; Ye, W.; Cai, Y.; Bhaskar, L. Physical Activity and Nutritional Influence on Immune Function: An Important Strategy to Improve Immunity and Health Status. Front Physiol 2021, 12, 751374. [Google Scholar] [CrossRef]
- Booth, F.W.; Roberts, C.K.; Thyfault, J.P.; Ruegsegger, G.N.; Toedebusch, R.G. Role of Inactivity in Chronic Diseases: Evolutionary Insight and Pathophysiological Mechanisms. Physiol Rev 2017, 97, 1351–1402. [Google Scholar] [CrossRef]
- Norris, J.M. Infant and childhood diet and type 1 diabetes risk: Recent advances and prospects. Curr Diab Rep 2010, 10, 345–349. [Google Scholar] [CrossRef]
- Sperling, M.A.; Laffel, L.M. Current Management of Glycemia in Children with Type 1 Diabetes Mellitus. N Engl J Med 2022, 386, 1155–1164. [Google Scholar] [CrossRef]
- Sharma, K.; Akre, S.; Chakole, S.; Wanjari, M.B. Stress-Induced Diabetes: A Review. Cureus 2022, 14, e29142. [Google Scholar] [CrossRef]
- Hirotsu, C.; Tufik, S.; Andersen, M.L. Interactions between sleep, stress, and metabolism: From physiological to pathological conditions. Sleep Sci 2015, 8, 143–152. [Google Scholar] [CrossRef]
- Tsiouli, E.; Alexopoulos, E.C.; Stefanaki, C.; Darviri, C.; Chrousos, G.P. Effects of diabetes-related family stress on glycemic control in young patients with type 1 diabetes: Systematic review. Can Fam Physician 2013, 59, 143–149. [Google Scholar]
- Hilliard, M.E.; Harris, M.A.; Weissberg-Benchell, J. Diabetes resilience: A model of risk and protection in type 1 diabetes. Curr Diab Rep 2012, 12, 739–748. [Google Scholar] [CrossRef]
- Yi-Frazier, J.P.; Hilliard, M.E.; O'Donnell, M.B.; Zhou, C.; Ellisor, B.M.; Garcia Perez, S.; Duran, B.; Rojas, Y.; Malik, F.S.; DeSalvo, D.J.; et al. Promoting Resilience in Stress Management for Adolescents With Type 1 Diabetes: A Randomized Clinical Trial. JAMA Netw Open 2024, 7, e2428287. [Google Scholar] [CrossRef]
- Creswell, J.D.; Lindsay, E.K.; Villalba, D.K.; Chin, B. Mindfulness Training and Physical Health: Mechanisms and Outcomes. Psychosom Med 2019, 81, 224–232. [Google Scholar] [CrossRef]
- Lupini, F.; Basch, M.; Cooke, F.; Vagadori, J.; Gutierrez-Colina, A.; Kelly, K.P.; Streisand, R.; Shomaker, L.; Mackey, E.R. BREATHE-T1D: Using iterative mixed methods to adapt a mindfulness-based intervention for adolescents with type 1 diabetes: Design and development. Contemp Clin Trials 2024, 142, 107551. [Google Scholar] [CrossRef] [PubMed]
- Grattoni, A.; Korbutt, G.; Tomei, A.A.; García, A.J.; Pepper, A.R.; Stabler, C.; Brehm, M.; Papas, K.; Citro, A.; Shirwan, H.; et al. Harnessing cellular therapeutics for type 1 diabetes mellitus: Progress, challenges, and the road ahead. Nat Rev Endocrinol 2024. [Google Scholar] [CrossRef]
- Primavera, R.; Regmi, S.; Yarani, R.; Levitte, S.; Wang, J.; Ganguly, A.; Chetty, S.; Guindani, M.; Ricordi, C.; Meyer, E.; Thakor, A.S. Precision Delivery of Human Bone Marrow-Derived Mesenchymal Stem Cells Into the Pancreas Via Intra-arterial Injection Prevents the Onset of Diabetes. Stem Cells Transl Med 2024, 13, 559–571. [Google Scholar] [CrossRef]
- Berishvili, E.; Peloso, A.; Tomei, A.A.; Pepper, A.R. The Future of Beta Cells Replacement in the Era of Regenerative Medicine and Organ Bioengineering. Transpl Int 2024, 37, 12885. [Google Scholar] [CrossRef]
- Tomei, A.A.; Manzoli, V.; Fraker, C.A.; Giraldo, J.; Velluto, D.; Najjar, M.; Pileggi, A.; Molano, R.D.; Ricordi, C.; Stabler, C.L.; Hubbell, J.A. Device design and materials optimization of conformal coating for islets of Langerhans. Proc Natl Acad Sci U S A 2014, 111, 10514–10519. [Google Scholar] [CrossRef]
- Wu, Z.; Xu, X.; Cai, J.; Chen, J.; Huang, L.; Wu, W.; Pugliese, A.; Li, S.; Ricordi, C.; Tan, J. Prevention of chronic diabetic complications in type 1 diabetes by co-transplantation of umbilical cord mesenchymal stromal cells and autologous bone marrow: A pilot randomized controlled open-label clinical study with 8-year follow-up. Cytotherapy 2022, 24, 421–427. [Google Scholar] [CrossRef]
- Mourad, N.I.; Perota, A.; Xhema, D.; Duchi, R.; Lagutina, I.; Galli, C.; Gianello, P. Double transgenic neonatal porcine islets as an alternative source for beta cell replacement therapy. Proc Natl Acad Sci U S A 2024, 121, e2409138121. [Google Scholar] [CrossRef]
- Yao, X.; Gong, Z.; Yin, W.; Li, H.; Douroumis, D.; Huang, L.; Li, H. Islet cell spheroids produced by a thermally sensitive scaffold: A new diabetes treatment. J Nanobiotechnology 2024, 22, 657. [Google Scholar] [CrossRef]
- Wang, S.; Du, Y.; Zhang, B.; Meng, G.; Liu, Z.; Liew, S.Y.; Liang, R.; Zhang, Z.; Cai, X.; Wu, S.; et al. Transplantation of chemically induced pluripotent stem-cell-derived islets under abdominal anterior rectus sheath in a type 1 diabetes patient. Cell 2024, 187, 6152–6164.e6118. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, P.O.; Espes, D.; Sisay, S.; Davies, L.C.; Smith, C.I.E.; Svahn, M.G. Umbilical cord-derived mesenchymal stromal cells preserve endogenous insulin production in type 1 diabetes: A Phase I/II randomised double-blind placebo-controlled trial. Diabetologia 2023, 66, 1431–1441. [Google Scholar] [CrossRef] [PubMed]
- Keymeulen, B.; De Groot, K.; Jacobs-Tulleneers-Thevissen, D.; Thompson, D.M.; Bellin, M.D.; Kroon, E.J.; Daniels, M.; Wang, R.; Jaiman, M.; Kieffer, T.J.; et al. Encapsulated stem cell-derived β cells exert glucose control in patients with type 1 diabetes. Nat Biotechnol 2024, 42, 1507–1514. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, P.O.; Schwarcz, E.; Korsgren, O.; Le Blanc, K. Preserved β-cell function in type 1 diabetes by mesenchymal stromal cells. Diabetes 2015, 64, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Nair, G.G.; Liu, J.S.; Russ, H.A.; Tran, S.; Saxton, M.S.; Chen, R.; Juang, C.; Li, M.L.; Nguyen, V.Q.; Giacometti, S.; et al. Recapitulating endocrine cell clustering in culture promotes maturation of human stem-cell-derived β cells. Nat Cell Biol 2019, 21, 263–274. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, H.; Ko, U.H.; Oh, Y.; Lim, A.; Sohn, J.W.; Shin, J.H.; Kim, H.; Han, Y.M. Islet-like organoids derived from human pluripotent stem cells efficiently function in the glucose responsiveness in vitro and in vivo. Sci Rep 2016, 6, 35145. [Google Scholar] [CrossRef]
- Molakandov, K.; Berti, D.A.; Beck, A.; Elhanani, O.; Walker, M.D.; Soen, Y.; Yavriyants, K.; Zimerman, M.; Volman, E.; Toledo, I.; et al. Selection for CD26(-) and CD49A(+) Cells From Pluripotent Stem Cells-Derived Islet-Like Clusters Improves Therapeutic Activity in Diabetic Mice. Front Endocrinol (Lausanne) 2021, 12, 635405. [Google Scholar] [CrossRef]
- Shilleh, A.H.; Beard, S.; Russ, H.A. Enrichment of stem cell-derived pancreatic beta-like cells and controlled graft size through pharmacological removal of proliferating cells. Stem Cell Reports 2023, 18, 1284–1294. [Google Scholar] [CrossRef]
- Stock, A.A.; Gonzalez, G.C.; Pete, S.I.; De Toni, T.; Berman, D.M.; Rabassa, A.; Diaz, W.; Geary, J.C., Jr.; Willman, M.; Jackson, J.M.; et al. Performance of islets of Langerhans conformally coated via an emulsion cross-linking method in diabetic rodents and nonhuman primates. Sci Adv 2022, 8, eabm3145. [Google Scholar] [CrossRef]
- De Toni, T.; Stock, A.A.; Devaux, F.; Gonzalez, G.C.; Nunez, K.; Rubanich, J.C.; Safley, S.A.; Weber, C.J.; Ziebarth, N.M.; Buchwald, P.; Tomei, A.A. Parallel Evaluation of Polyethylene Glycol Conformal Coating and Alginate Microencapsulation as Immunoisolation Strategies for Pancreatic Islet Transplantation. Front Bioeng Biotechnol 2022, 10, 886483. [Google Scholar] [CrossRef]
- Safley, S.A.; Kenyon, N.S.; Berman, D.M.; Barber, G.F.; Cui, H.; Duncanson, S.; De Toni, T.; Willman, M.; De Vos, P.; Tomei, A.A.; et al. Microencapsulated islet allografts in diabetic NOD mice and nonhuman primates. Eur Rev Med Pharmacol Sci 2020, 24, 8551–8565. [Google Scholar] [CrossRef]
- Stock, A.A.; Manzoli, V.; De Toni, T.; Abreu, M.M.; Poh, Y.C.; Ye, L.; Roose, A.; Pagliuca, F.W.; Thanos, C.; Ricordi, C.; Tomei, A.A. Conformal Coating of Stem Cell-Derived Islets for β Cell Replacement in Type 1 Diabetes. Stem Cell Reports 2020, 14, 91–104. [Google Scholar] [CrossRef]
- Villa, C.; Manzoli, V.; Abreu, M.M.; Verheyen, C.A.; Seskin, M.; Najjar, M.; Molano, R.D.; Torrente, Y.; Ricordi, C.; Tomei, A.A. Effects of Composition of Alginate-Polyethylene Glycol Microcapsules and Transplant Site on Encapsulated Islet Graft Outcomes in Mice. Transplantation 2017, 101, 1025–1035. [Google Scholar] [CrossRef] [PubMed]
- Najjar, M.; Manzoli, V.; Abreu, M.; Villa, C.; Martino, M.M.; Molano, R.D.; Torrente, Y.; Pileggi, A.; Inverardi, L.; Ricordi, C.; et al. Fibrin gels engineered with pro-angiogenic growth factors promote engraftment of pancreatic islets in extrahepatic sites in mice. Biotechnol Bioeng 2015, 112, 1916–1926. [Google Scholar] [CrossRef] [PubMed]
- Chellappan, D.K.; Sivam, N.S.; Teoh, K.X.; Leong, W.P.; Fui, T.Z.; Chooi, K.; Khoo, N.; Yi, F.J.; Chellian, J.; Cheng, L.L.; et al. Gene therapy and type 1 diabetes mellitus. Biomed Pharmacother 2018, 108, 1188–1200. [Google Scholar] [CrossRef]
- Cheng, Y.; Wang, H.; Li, M. The promise of CRISPR/Cas9 technology in diabetes mellitus therapy: How gene editing is revolutionizing diabetes research and treatment. J Diabetes Complications 2023, 37, 108524. [Google Scholar] [CrossRef]
- El Nahas, R.; Al-Aghbar, M.A.; Herrero, L.; van Panhuys, N.; Espino-Guarch, M. Applications of Genome-Editing Technologies for Type 1 Diabetes. Int J Mol Sci 2023, 25. [Google Scholar] [CrossRef]
- Millette, K.; Georgia, S. Gene Editing and Human Pluripotent Stem Cells: Tools for Advancing Diabetes Disease Modeling and Beta-Cell Development. Curr Diab Rep 2017, 17, 116. [Google Scholar] [CrossRef] [PubMed]
- Cai, E.P.; Ishikawa, Y.; Zhang, W.; Leite, N.C.; Li, J.; Hou, S.; Kiaf, B.; Hollister-Lock, J.; Yilmaz, N.K.; Schiffer, C.A.; et al. Genome-scale in vivo CRISPR screen identifies RNLS as a target for beta cell protection in type 1 diabetes. Nat Metab 2020, 2, 934–945. [Google Scholar] [CrossRef]
- Lotfi, M.; Butler, A.E.; Sukhorukov, V.N.; Sahebkar, A. Application of CRISPR-Cas9 technology in diabetes research. Diabet Med 2024, 41, e15240. [Google Scholar] [CrossRef]
- Garcia-Gutierrez, E.; O'Mahony, A.K.; Dos Santos, R.S.; Marroquí, L.; Cotter, P.D. Gut microbial metabolic signatures in diabetes mellitus and potential preventive and therapeutic applications. Gut Microbes 2024, 16, 2401654. [Google Scholar] [CrossRef]
- Yuan, X.; Wang, R.; Han, B.; Sun, C.; Chen, R.; Wei, H.; Chen, L.; Du, H.; Li, G.; Yang, Y.; et al. Functional and metabolic alterations of gut microbiota in children with new-onset type 1 diabetes. Nat Commun 2022, 13, 6356. [Google Scholar] [CrossRef]
- de Goffau, M.C.; Luopajärvi, K.; Knip, M.; Ilonen, J.; Ruohtula, T.; Härkönen, T.; Orivuori, L.; Hakala, S.; Welling, G.W.; Harmsen, H.J.; Vaarala, O. Fecal microbiota composition differs between children with β-cell autoimmunity and those without. Diabetes 2013, 62, 1238–1244. [Google Scholar] [CrossRef]
- Giongo, A.; Gano, K.A.; Crabb, D.B.; Mukherjee, N.; Novelo, L.L.; Casella, G.; Drew, J.C.; Ilonen, J.; Knip, M.; Hyöty, H.; et al. Toward defining the autoimmune microbiome for type 1 diabetes. Isme j 2011, 5, 82–91. [Google Scholar] [CrossRef]
- de Goffau, M.C.; Fuentes, S.; van den Bogert, B.; Honkanen, H.; de Vos, W.M.; Welling, G.W.; Hyöty, H.; Harmsen, H.J. Aberrant gut microbiota composition at the onset of type 1 diabetes in young children. Diabetologia 2014, 57, 1569–1577. [Google Scholar] [CrossRef] [PubMed]
- Murri, M.; Leiva, I.; Gomez-Zumaquero, J.M.; Tinahones, F.J.; Cardona, F.; Soriguer, F.; Queipo-Ortuño, M.I. Gut microbiota in children with type 1 diabetes differs from that in healthy children: A case-control study. BMC Med 2013, 11, 46. [Google Scholar] [CrossRef]
- Vatanen, T.; Franzosa, E.A.; Schwager, R.; Tripathi, S.; Arthur, T.D.; Vehik, K.; Lernmark, Å.; Hagopian, W.A.; Rewers, M.J.; She, J.X.; et al. The human gut microbiome in early-onset type 1 diabetes from the TEDDY study. Nature 2018, 562, 589–594. [Google Scholar] [CrossRef]
- Kiner, E.; Willie, E.; Vijaykumar, B.; Chowdhary, K.; Schmutz, H.; Chandler, J.; Schnell, A.; Thakore, P.I.; LeGros, G.; Mostafavi, S.; et al. Gut CD4(+) T cell phenotypes are a continuum molded by microbes, not by T(H) archetypes. Nat Immunol 2021, 22, 216–228. [Google Scholar] [CrossRef]
- Nowosad, C.R.; Mesin, L.; Castro, T.B.R.; Wichmann, C.; Donaldson, G.P.; Araki, T.; Schiepers, A.; Lockhart, A.A.K.; Bilate, A.M.; Mucida, D.; Victora, G.D. Tunable dynamics of B cell selection in gut germinal centres. Nature 2020, 588, 321–326. [Google Scholar] [CrossRef]
- Yao, X.; Zhang, C.; Xing, Y.; Xue, G.; Zhang, Q.; Pan, F.; Wu, G.; Hu, Y.; Guo, Q.; Lu, A.; et al. Remodelling of the gut microbiota by hyperactive NLRP3 induces regulatory T cells to maintain homeostasis. Nat Commun 2017, 8, 1896. [Google Scholar] [CrossRef]
- de Groot, P.; Nikolic, T.; Pellegrini, S.; Sordi, V.; Imangaliyev, S.; Rampanelli, E.; Hanssen, N.; Attaye, I.; Bakker, G.; Duinkerken, G.; et al. Faecal microbiota transplantation halts progression of human new-onset type 1 diabetes in a randomised controlled trial. Gut 2021, 70, 92–105. [Google Scholar] [CrossRef]
- Ho, J.; Nicolucci, A.C.; Virtanen, H.; Schick, A.; Meddings, J.; Reimer, R.A.; Huang, C. Effect of Prebiotic on Microbiota, Intestinal Permeability, and Glycemic Control in Children With Type 1 Diabetes. J Clin Endocrinol Metab 2019, 104, 4427–4440. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.; Reimer, R.A.; Doulla, M.; Huang, C. Effect of prebiotic intake on gut microbiota, intestinal permeability and glycemic control in children with type 1 diabetes: Study protocol for a randomized controlled trial. Trials 2016, 17, 347. [Google Scholar] [CrossRef]
- Hagger, V.; Hendrieckx, C.; Sturt, J.; Skinner, T.C.; Speight, J. Diabetes Distress Among Adolescents with Type 1 Diabetes: A Systematic Review. Curr Diab Rep 2016, 16, 9. [Google Scholar] [CrossRef]
- Rodríguez-Muñoz, A.; Picón-César, M.J.; Tinahones, F.J.; Martínez-Montoro, J.I. Type 1 diabetes-related distress: Current implications in care. Eur J Intern Med 2024, 125, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Rechenberg, K.; Whittemore, R.; Holland, M.; Grey, M. General and diabetes-specific stress in adolescents with type 1 diabetes. Diabetes Res Clin Pract 2017, 130, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Iturralde, E.; Rausch, J.R.; Weissberg-Benchell, J.; Hood, K.K. Diabetes-Related Emotional Distress Over Time. Pediatrics 2019, 143. [Google Scholar] [CrossRef]
- Jaser, S.S.; Linsky, R.; Grey, M. Coping and psychological distress in mothers of adolescents with type 1 diabetes. Matern Child Health J 2014, 18, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Cheraghi, F.; Shamsaei, F.; Mortazavi, S.Z.; Moghimbeigi, A. The Effect of Family-centered Care on Management of Blood Glucose Levels in Adolescents with Diabetes. Int J Community Based Nurs Midwifery 2015, 3, 177–186. [Google Scholar] [CrossRef]
- Rostaminasab, S.; Nematollahi, M.; Jahani, Y.; Mehdipour-Rabori, R. The effect of family-centered empowerment model on burden of care in parents and blood glucose level of children with type I diabetes family empowerment on burden of care and HbA1C. BMC Nurs 2023, 22, 214. [Google Scholar] [CrossRef]
- Ispriantari, A.; Agustina, R.; Konlan, K.D.; Lee, H. Family-centered interventions for children and adolescents with type 1 diabetes mellitus: An integrative review. Child Health Nurs Res 2023, 29, 7–23. [Google Scholar] [CrossRef]
- Siminerio, L.M.; Albanese-O'Neill, A.; Chiang, J.L.; Hathaway, K.; Jackson, C.C.; Weissberg-Benchell, J.; Wright, J.L.; Yatvin, A.L.; Deeb, L.C. Care of young children with diabetes in the child care setting: A position statement of the American Diabetes Association. Diabetes Care 2014, 37, 2834–2842. [Google Scholar] [CrossRef]
- Chung, S.J.; Ersig, A.L.; McCarthy, A.M. The Influence of Peers on Diet and Exercise Among Adolescents: A Systematic Review. J Pediatr Nurs 2017, 36, 44–56. [Google Scholar] [CrossRef]
- Ward, S.A.; Bélanger, M.F.; Donovan, D.; Carrier, N. Relationship between eating behaviors and physical activity of preschoolers and their peers: A systematic review. Int J Behav Nutr Phys Act 2016, 13, 50. [Google Scholar] [CrossRef]
- Redondo, M.J.; Steck, A.K.; Pugliese, A. Genetics of type 1 diabetes. Pediatr Diabetes 2018, 19, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Marfella, R.; Ciotola, M.; Di Palo, C.; Giugliano, F.; Giugliano, G.; D'Armiento, M.; D'Andrea, F.; Giugliano, D. Effect of a mediterranean-style diet on endothelial dysfunction and markers of vascular inflammation in the metabolic syndrome: A randomized trial. Jama 2004, 292, 1440–1446. [Google Scholar] [CrossRef] [PubMed]
- Ovalle, F.; Grimes, T.; Xu, G.; Patel, A.J.; Grayson, T.B.; Thielen, L.A.; Li, P.; Shalev, A. Verapamil and beta cell function in adults with recent-onset type 1 diabetes. Nat Med 2018, 24, 1108–1112. [Google Scholar] [CrossRef] [PubMed]
- Dejgaard, T.F.; von Scholten, B.J.; Christiansen, E.; Kreiner, F.F.; Bardtrum, L.; von Herrath, M.; Mathieu, C.; Madsbad, S. Efficacy and safety of liraglutide in type 1 diabetes by baseline characteristics in the ADJUNCT ONE and ADJUNCT TWO randomized controlled trials. Diabetes Obes Metab 2021, 23, 2752–2762. [Google Scholar] [CrossRef] [PubMed]
- Bluestone, J.A.; Buckner, J.H.; Fitch, M.; Gitelman, S.E.; Gupta, S.; Hellerstein, M.K.; Herold, K.C.; Lares, A.; Lee, M.R.; Li, K.; et al. Type 1 diabetes immunotherapy using polyclonal regulatory T cells. Sci Transl Med 2015, 7, 315ra189. [Google Scholar] [CrossRef]
- Luo, D.; Cai, X.; Wang, H.; Wang, Y.; Xu, J. The role of peer social relationships in psychological distress and quality of life among adolescents with type 1 diabetes mellitus: A longitudinal study. BMC Psychiatry 2024, 24, 270. [Google Scholar] [CrossRef]
Figure 1.
Progressive Stages of Beta-Cell Dysfunction in Type 1 Diabetes (T1D). The figure illustrates the gradual decline in functional beta-cell mass over time, highlighting the progression through three stages of T1D development. Stage 1 represents the initiation of the immune attack in individuals with normoglycemia and the presence of two or more autoantibodies, indicating a presymptomatic phase. In Stage 2, dysglycemia occurs, with the continued presence of two or more autoantibodies, yet still in a presymptomatic state. By Stage 3, dysglycemia persists with symptoms, as beta-cell mass and insulin production are severely compromised. The figure highlights the impact of genetic and environmental factors contributing to T1D risk, leading to a progressive decline in beta-cell mass and insulin secretion. Created with Biorender.com.
Figure 1.
Progressive Stages of Beta-Cell Dysfunction in Type 1 Diabetes (T1D). The figure illustrates the gradual decline in functional beta-cell mass over time, highlighting the progression through three stages of T1D development. Stage 1 represents the initiation of the immune attack in individuals with normoglycemia and the presence of two or more autoantibodies, indicating a presymptomatic phase. In Stage 2, dysglycemia occurs, with the continued presence of two or more autoantibodies, yet still in a presymptomatic state. By Stage 3, dysglycemia persists with symptoms, as beta-cell mass and insulin production are severely compromised. The figure highlights the impact of genetic and environmental factors contributing to T1D risk, leading to a progressive decline in beta-cell mass and insulin secretion. Created with Biorender.com.
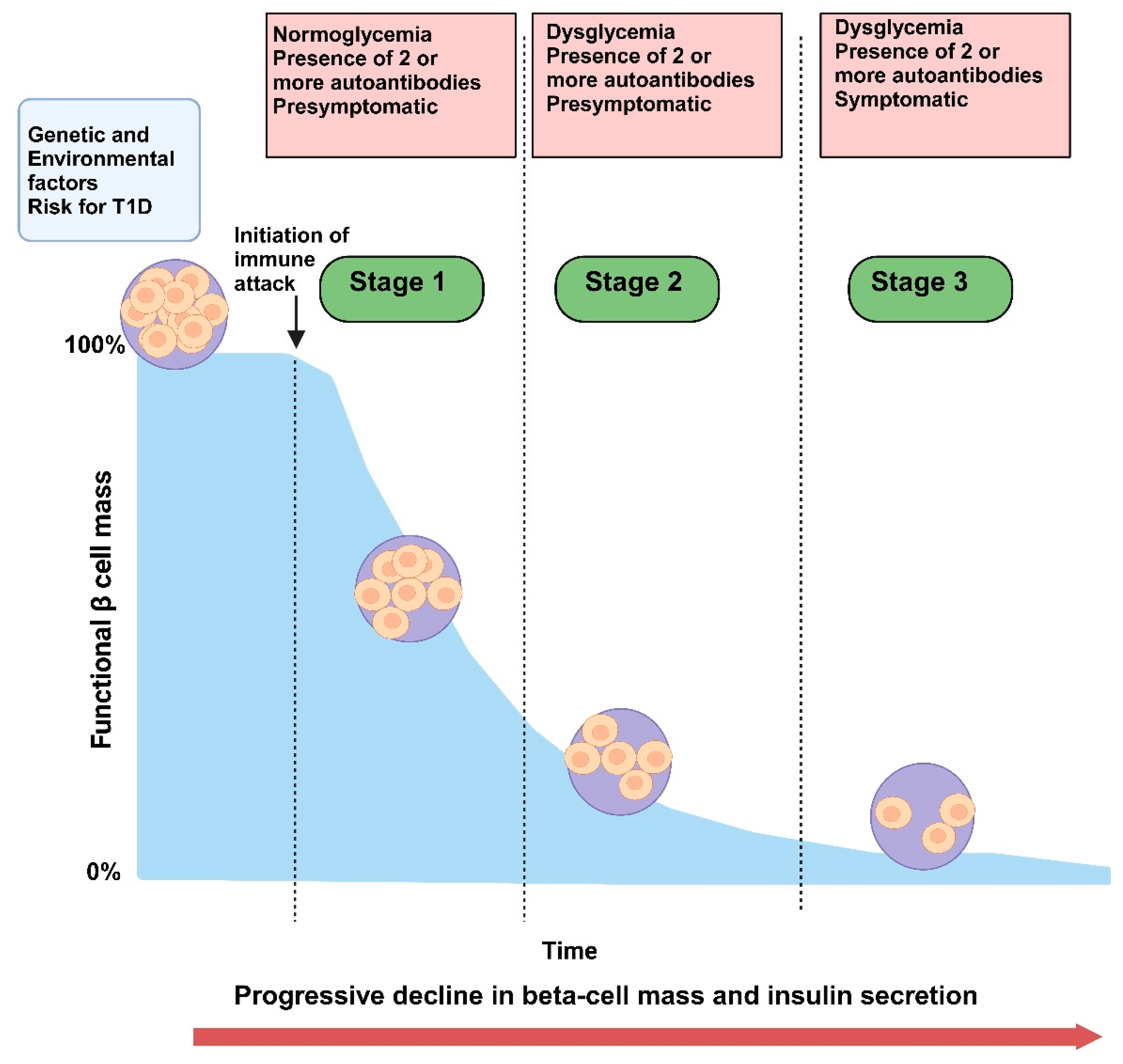

Table 1.
Screening Guidelines for Type 1 Diabetes in Adolescents.
| Screening Parameter | Description | Target Population | References |
|---|---|---|---|
| Autoantibody Screening | Detection of islet autoantibodies (such as GAD65, IA-2, ZnT8) indicating autoimmune activity | Adolescents with a family history of T1D or other autoimmune diseases | [17,18,19] |
| Genetic Screening | Identification of HLA genotypes associated with increased T1D risk | High-risk individuals, especially those with a first-degree relative with T1D | [16,49,50,51,52,53] |
| Metabolic Markers | Measurement of C-peptide levels and oral glucose tolerance tests to assess beta-cell function | Adolescents with positive autoantibodies or genetic predisposition | [22,23,24,25,26,27,28] |
| Continuous Glucose Monitoring (CGM) | Use of CGM devices to detect dysglycemia in at-risk adolescents | Adolescents with positive autoantibodies or early signs of glucose intolerance | [29,30,31,32,33,34,35,36] |
Table 2.
Nutritional and Lifestyle Interventions for Adolescents with Pre-Diabetes.
| Intervention | Description | Expected Outcome | References |
|---|---|---|---|
| Low Glycemic Index Diet | Emphasis on consuming foods with a low glycemic index to stabilize blood sugar levels | Improved glycemic control and reduced insulin resistance | [80] |
| Mediterranean Diet | Diet rich in fruits, vegetables, whole grains, and healthy fats | Reduction in inflammation and improvement in insulin sensitivity | [179] |
| Physical Activity | Regular aerobic and resistance training exercises | Enhanced glucose uptake and improved cardiovascular health | [94,95,96] |
| Behavioral Counseling | Structured programs focusing on lifestyle modification | Increased adherence to healthy behaviors and weight management | [125] |
Table 3.
Emerging Pharmacological Interventions in Pre-Diabetes for Adolescents.
| Drug Class | Example Agent | Mechanism of Action | Current Research Status | Expected Outcomes | Side Effects/Considerations | References |
|---|---|---|---|---|---|---|
| Immune Modulators | Teplizumab | Anti-CD3 monoclonal antibody modulating T-cell activity to reduce autoimmune beta cell attack | Phase III trials; shown to delay T1D onset | Delay in progression to clinical T1D, preservation of beta cell function | Possible immunosuppression; monitoring required | [39] |
| Abatacept | Interferes with T-cell costimulation to reduce immune response against beta cells | Early clinical trials | Slower beta cell decline, potential delay in T1D onset | Mild to moderate injection site reactions | [41] | |
| Anti-CD20 (e.g., Rituximab) | Depletes B-cells to modulate autoimmune activity | Phase II trials; varied efficacy | Reduction in autoimmune activity, partial beta cell preservation | Risk of infection due to B-cell depletion | [39,43] | |
| Anti-Inflammatory Agents | Interleukin-2 (IL-2) | Low-dose IL-2 therapy aimed at enhancing regulatory T-cell function | Ongoing clinical studies | Improved immune tolerance, reduced beta cell stress | Requires dosage optimization; risk of fever | [114] |
| Beta Cell Modulators | Verapamil | Calcium channel blocker potentially inhibiting beta cell apoptosis | Phase II trials; promising in T1D | Beta cell survival enhancement, improved glucose control | Dizziness, low blood pressure | [180] |
| GLP-1 Receptor Agonists | Enhance beta cell proliferation and insulin secretion in response to glucose | Phase III for T2D, exploratory for T1D | Increased beta cell function and insulin sensitivity | Nausea, potential risk of pancreatitis | [181] | |
| Other Novel Agents | Treg-enhancing agents | Agents aiming to boost regulatory T-cell numbers and function | Preclinical and early clinical trials | Enhanced immune tolerance, delayed beta cell decline | Long-term safety under investigation | [182] |
Table 4.
Psychosocial and Mental Health Interventions for Adolescents at Risk of T1D.
| Intervention | Description | Expected Outcome | References |
|---|---|---|---|
| Cognitive Behavioral Therapy (CBT) | Techniques to manage anxiety and stress related to health monitoring and disease risk | Reduced anxiety levels and improved coping mechanisms | [123,124,125,126] |
| Family Therapy | Counseling sessions involving family members to improve communication and support | Enhanced family cohesion and better adherence to lifestyle interventions | [45] |
| Peer Support Groups | Group sessions with peers facing similar health challenges | Increased emotional support and shared coping strategies | [183] |
| Stress Management Programs | Programs teaching stress reduction techniques such as mindfulness and relaxation exercises | Lowered stress levels and improved overall well-being | [45,123] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



