
Submitted:
20 November 2024
Posted:
21 November 2024
You are already at the latest version
Abstract
Male infertility is a significant global health issue, comprising approx. 50% of all infertility cases. Semen cryopreservation, a critical component of assisted reproductive technologies (ART), is a method commonly used in a wide range of situations, including gonadotoxic treatments such as radiation or chemotherapy, hazardous occupational exposures, or various medical conditions. Although historically viewed as potentially damaging to sperm, recent findings suggest that cryopreservation, when performed with appropriate techniques, may in fact enhance semen quality by improving the proportion of healthy spermatozoa, particularly in terms of their morphological parameters. The aim of this study was to evaluate the impact of cryopreservation on sperm morphology and viability, utilizing advanced morphological assessments pre- and post-freezing. Semen samples from 97 patients were analyzed, revealing significant improvements in morphology, with increased percentages of normal sperm and reductions in deformation indices post-thaw. The findings indicate that optimized cryopreservation protocols may support the selection of higher-quality sperm, offering valuable benefits for ART applications. These results challenge certain past assumptions regarding the impact of cryopreservation and underscore the need for refined freezing techniques to maintain and potentially enhance semen quality for reproductive use.
Keywords:
male infertility
; cryopreservation
; assisted reproductive technologies
; semen quality
; sperm morphology
Introduction
Male infertility constitutes a global problem and is believed to be responsible for 40-60% of all infertility cases [1,2]. Globally, infertility affects around 2.5-12% of men, with particularly high rates observed in Africa (36-42%) and Eastern Europe (40-60%), compared to 7.5% in Western Europe and the United States [1]. As far as its etiology is concerned, male infertility has been classified into pre-testicular, testicular, post-testicular, mixed, and idiopathic [3]. Semen quality assessment is considered a fundamental method for evaluating male fertility [4] and involves both quantitative and qualitative measurements, which are compared against established reference ranges [5]. The process of selecting those parameters that are responsible for semen quality and thus allow to predict fertility outcomes with a satisfactory level of certainty is crucial in the context of assisted reproductive technologies (ART) used by fertility clinics.
To standardize these methods, in 1980 the WHO developed a manual which includes detailed descriptions of semen analysis procedures, reference values, and a nomenclature of disorders. As of 2024, the manual has been revised five times (1987, 1992, 1999, 2010, 2021). It is crucial to note that in the 2010 edition the reference values for semen parameters were significantly modified (lowered)—compared to previous editions—which led to less frequent diagnoses of male factor infertility, even though the actual number of affected men has not decreased [6,7]; on the contrary, over the past 50 years, an increase in disorders affecting the male reproductive system has been observed, resulting in a decline in the levels of parameters such as sperm count, motility, and morphology [8,9].
Although problems related to male infertility affect a large number of couples worldwide, research has traditionally focused mainly on female fertility. This bias has resulted in an insufficient number and robustness of studies on male fertility, highlighting the need for further research to test some of the assumptions prevalent in the literature. One such topic that requires reevaluation as new data emerges is semen cryopreservation. While long regarded as a procedure that damages semen, cryopreservation may, in fact, have the opposite effect and potentially improve semen quality.
In the context of this article—in order to properly clarify the meaning of improved semen quality in terms of cryopreservation—it needs to be remembered that the improvement in question signifies that the ejaculate contains a larger fraction of higher-quality spermatozoa, in comparison to fresh semen. What it does not mean is that a certain number spermatozoa becomes biologically improved through freezing. Such assertion would be both unfounded and impossible to prove, unless only a very small number of spermatozoa are tested that can be compared individually pre- and post-freezing.
Cryopreservation of sperm is an essential practice in assisted reproductive technologies (ART). Among the main reasons for using this technique are situations in which patients are undergoing gonadotoxic treatments, such as chemotherapy and radiotherapy, as well as in situations when there is a need for fertility preservation due to hazardous occupational exposures or for social reasons [10]. While pointing out that fresh sperm shows no advantage over cryopreserved sperm, Yu et al. [11] also suggest that sperm cryopreservation should be considered for all cases of surgical sperm retrieval, as freezing is viable even in patients where only a small number of testicular sperm are obtained. In other words, concerns that sperm which is difficult to obtain would be rendered unusable due to deteriorated quality after cryopreservation and thus wasted are unfounded.
The aforementioned situations are those that are usually associated with the need for cryopreservation; however, there are many more cases in which the procedure is essential. The European Association of Urology (EAU) [12] has prepared a detailed list of clinical indications for depositing male reproductive cells in a sperm bank. The list includes the aforementioned potentially sterilizing chemotherapy or radiotherapy for cancer or benign diseases, surgeries that may impact fertility, progressive deterioration in semen quality due to disease, paraplegia, psychogenic anejaculation, following gonadotropin treatment that has induced spermatogenesis in men with hypogonadotropic hypogonadism, in cases of non-obstructive azoospermia, in any situation where sperm is obtained through surgical procedures, and to reduce the risk of infection transmission from donors. According to Directive 2004/23/EC of the European Parliament and Council [13] and Commission Directive 2006/17/EC [14], fresh donor sperm may not be used for non-partner donation. In addition, non-malignant diseases requiring fertility preservation, which include autoimmune diseases, hematopoietic stem cell transplantation, and male genetic disorders, also comprise cases in which cryopreservation is recommended. As previously mentioned, in some countries cryopreservation is also offered to men in hazardous occupations, such as military defense forces, where posthumous procreation is permissible. As can be seen, the number of situations when cryopreservation of semen is a viable solution is large, and reaches far beyond those cases, such as malignancies, it is traditionally associated with [7].
Sperm cryopreservation is associated with several benefits. It mitigates the need for repeated sperm retrieval procedures, which can be invasive, costly, and uncomfortable for the patient. This is especially important for individuals with azoospermia, as sperm retrieval rates can vary significantly, leading to the potential need for repeated extractions if fresh sperm is used. Therefore, cryopreservation offers both logistical and therapeutic advantages, allowing for synchronized ART cycles and reducing the psychological and physical burden on patients [15]. Literature data also shows that the fear that using frozen sperm may negatively affect fertility rates seems to be largely ungrounded. No statistically significant difference has been found between the use of fresh testicular sperm and cryopreserved and thawed sperm in men with azoospermia caused by spermatogenesis dysfunction when assessing clinical pregnancy rates or fertilization outcomes in couples undergoing ICSI [11,15].
Kuczyński et al. [16], citing Tournaye [17], emphasize that cryopreservation can be helpful in eliminating aging or deficient spermatozoa. Based on their own prospective randomized study, the researchers showed that cryopreserved and fresh sperm have at least the same reproductive potential with regard to ICSI. They suggest that further prospective studies are needed to determine whether sperm cryopreservation before ICSI can be helpful in selecting the healthiest sperm and whether it can improve pregnancy rates. This aspect, i.e., the improvement of semen quality through the selection of higher-quality spermatozoa, is thus the main principle behind the beneficial aspects of cryopreservation.
Sperm cryopreservation has undergone many changes in terms of freezing methods, freezing and thawing rates, and the media used to preserve sperm functionality and DNA integrity [18]. However, it has been linked with a number of problematic issues, mostly related to various ethical issues and the question of its effectiveness. Borate and Meshram [19] point out several largely unresolved ethical concerns regarding sperm banking, including whether donor identities should be protected and whether sperm from a deceased person should be used after their death. Furthermore, it has even been suggested that long-term studies on offspring obtained from cryopreserved sperm should be conducted to fully assess the biological safety of this procedure [20], although do not support the hypothesis that such relationships exist [21]. In terms of the effectiveness of cryopreservation, i.e., the resultant semen quality and fertility issues, the main concerns that have been raised are connected with reduced semen parameters such as motility and morphology, DNA damage, and—ultimately—decreased fertilization rates [19,22,23].
A distinction that is absolutely crucial in the context of studies on cryopreservation is between a proper and improper freezing/thawing process. Obviously, numerous factors come into play in this area, e.g., biological, technical, or methodological. However, researchers have been able to identify those factors that need to be consider for cryopreservation to be performed adequately, although there is no consensus among researchers as to the ideal technique [10,18,24,25]. Some authors have proposed novel freezing protocols that lead to improved sperm parameters. One of the most significant proposals has been put forward by O’Neill et al. [26], who showed that a technique of their own design, which consisted in vitrification of human sperm using a sucrose- and dextran-based cryoprotectant (CPA4) with a novel vitrification device, resulted in significantly better sperm motility and progressive motility, along with improved DNA integrity and reduced DNA fragmentation compared to conventional slow freezing. The aforementioned distinction between proper and improper cryopreservation also shifts the focus of discussion from comparing the quality of fresh sperm vs. cryopreserved sperm to fresh sperm vs. properly cryopreserved sperm.
One of the aspects of proper cryopreservation is determining the optimal sperm selection technique after thawing. It is crucial to ensure recovery of the highest quality sperm with minimal iatrogenic damage. This not only enhances the chances of successful conception but also reduces the risk of genetic damage to the embryo. The results of a study performed by Hungerford et al. [27] showed that although cryopreservation led to a decline in sperm motility and viability due to increased lipid peroxidation and DNA damage, following sperm selection, all the three techniques used in the study resulted in improved motility, particularly with swim-up and electrophoretic separation procedures (the third tested procedure was density gradient centrifugation). Electrophoretic sperm selection offers substantial advantages over alternative separation strategies in terms of gamete quality and the time required to complete the procedure. These results both confirm the importance of the separation process and the different results achieved with various techniques.
As far as the quality of semen itself is concerned, there are a number conditions that lead to a decrease in the overall quality of semen. First of all, globozoospermia is a genetic cause of male infertility characterized by a predominant morphological sperm defect that involves a structural abnormality of the sperm head, in which acrosomal pathology coexists with a spherical/round head. No standard reference value has been established for the percentage of sperm with round heads. Electron microscopy studies of such sperm reveal acrosome hypoplasia, sometimes accompanied by a thickened neck, coiled tail, mitochondrial sheath disorganization, axonemal abnormalities, and residual cytoplasm. The use of such sperm for fertilization via ICSI yields a low success rate, i.e., fertilization (38%), pregnancy (20%), and live birth (14%) [29,30,31,32].
Macrozoospermia, on the other hand, is characterized by up to 100% of sperm in semen having an enlarged, irregularly shaped head, abnormal acrosome, and multiple tails. In typical cases of macrozoospermia, ultrastructural studies reveal a 3-fold increase in sperm head volume, with an average of 3.6 tails per sperm. Abnormalities in the sperm midpiece are also present. These sperm often exhibit triploidy, tetraploidy, aneuploidy, and increased DNA fragmentation. Currently, fertilization by ICSI is not recommended in such cases. Previous attempts to fertilize oocytes with sperm from men with macrozoospermia mostly resulted in miscarriages due to advanced genetic abnormalities [30,31,33].
Abnormal head-tail attachment in sperm is frequently associated with the absence or abnormal location of the two centrioles that are part of the sperm neck. The most extreme consequence is the independent development of the head and tail, resulting in the presence of pinhead sperm, or sperm without a head (deacapitated or acephalic sperm, headless tails, or detached tail defect). In addition to headless sperm, free heads also appear in semen, approx. 30 times fewer than tail fragments. In fertile men, the number of headless sperm can be around 20%, but in cases of male infertility, it is significantly higher, reaching 80-100%. Another form of attachment disorder is sperm with a lateral tail attachment. The midpiece of these gametes is positioned at various angles relative to the head (asymmetric midpiece). Sperm may also appear with a gap between the head and midpiece, visible under electron microscopy. These sperm are susceptible to mechanical stress, and spinning or micromanipulation may cause head-tail separation. Molecular diagnostics of sperm with abnormal head-tail attachment reveal multiple gene mutations, including in SUN5, PMFBP1, HOOK1, TSGA10, and BRDT. Patients with numerous sperm showing abnormal head-tail attachment should receive genetic counseling before undergoing ICSI. Success in IVF depends on the extent of the sperm's morphological and molecular defects [31,34,35].
MMAF Syndrome (Multiple Morphological Abnormalities of the Flagella) involves various structural anomalies of the sperm tail. These anomalies cause severe asthenozoospermia, in which there may be a complete lack of progressive sperm motility. Light microscopy reveals sperm with bent, abnormally attached, coiled, shortened, or thickened tails, often of irregular shape or entirely missing. The pathomechanism of MMAF syndrome is linked to dysfunction of genes responsible for the structure and growth of the axoneme, the fibrous sheath structure, flagellum biogenesis, and growth. Due to severe asthenozoospermia, ICSI is recommended. Since MMAF syndrome is frequently genetically determined and there is a risk of passing genetic abnormalities to offspring, genetic counseling is required. The success of ICSI depends on the type and extent of defects, as well as sperm viability in cases of complete immotility [29].
In order to ensure the highest possible semen quality pre-freezing, the appropriate pre-laboratory procedures should be observed [9]. These include:
the patient must observe a period of sexual abstinence (number of days since the last ejaculation prior to testing);
- -
- determining the most beneficial location of semen collection (in-lab or outside the lab);
- -
- determining the most beneficial method of semen collection (masturbation or intercourse with a special condom);
- -
- determining the most beneficial sample delivery method to the laboratory (time since ejaculation, sample transport temperature);
- -
- determining the most beneficial time from semen collection to the start of analysis;
- -
- choice of appropriate container (plastic or glass container or special condom);
- -
- including any comments from the patient (verbal or written) upon sample delivery (e.g., loss of part of the sample during collection).
In Poland, semen analysis is performed by a laboratory diagnostician or medical laboratory technician who has completed a specialized semen analysis course according to the current recommendations of the National Chamber of Laboratory Diagnosticians (KIDL) and the Polish Andrological Society (PTA) [36].
In addition, the authors’ experience in cryopreservation has led to the following conclusions in terms of various factors connected with sperm freezing that affect sperm motility and morphology after thawing. Such factors include:
- -
- genetic defects in sperm that have not been previously considered;
- -
- incorrect positioning relative to the liquid nitrogen mirror, which can lead to either too slow or too rapid cooling of the sperm;
- -
- immersion of prepared sperm directly into liquid nitrogen without an equilibration step in nitrogen vapors;
- -
- failure to follow freezing protocols, including freezing times;
- -
- incorrect medium volume to sperm volume ratio;
- -
- failure to pre-warm the freezing medium;
- -
- incorrect method of adding cryoprotectants to the sperm;
- -
- omitting or shortening the sperm thawing time;
- -
- too long a delay before starting the freezing procedure (>2 hours);
- -
- too long a time spent transferring frozen sperm to the collection container;
- -
- failure to maintain a constant temperature for frozen sperm;
- -
- improper conditions of transportation of sperm to the laboratory;
- -
- lack of experience in personnel performing the freezing process, haste, or lack of precision;
- -
- expired reagents;
- -
- improper storage conditions for the medium;
- -
- improper transport of the medium from the supplier to the laboratory;
- -
- failure to maintain optimal conditions in the laboratory during sperm thawing.
As far as cryopreservation methods are concerned, slow programmable freezing and liquid nitrogen vapor freezing have been used the most widely, though vitrification is gaining attention as an alternative technique with potential benefits in reducing ice crystal formation [24,26]. Slow freezing was considered a beneficial procedure as early as in 1990, with research findings pointing out that—despite higher costs and longer processing times—the method was particularly effective in preserving abnormal sperm and therefore superior to the standard rapid freezing method in nitrogen vapors [37]. Other studies comparing different cryoprotective media and freezing rates reveal that the choice of cryoprotectant and freezing method significantly influences outcomes such as DNA integrity, motility, and morphology of thawed sperm [20,38]. Adjustments in protocol, such as pre-freeze sperm selection and the incorporation of antioxidants or osmoprotectants, may further enhance the resilience of cryopreserved sperm, improving clinical outcomes and sperm functionality post-thaw [18,39,40]. In particular, the use of astaxanthin (ASTA) has been shown to improve sperm morphology, although it has no beneficial effect on DNA fragmentation repair [40]. Ghantabpour et al. [41] also reported improved sperm morphology, as well as protective action of freezing against oxidative stress after freezing with the use of astaxanthin. It has also been pointed out that single sperm cryopreservation requires a different technique than semen cryopreservation, potentially benefiting patients with severe oligospermia or azoospermia [42].
In terms of specific cryopreservation techniques, a crucial distinction in terms of possible cryoinjury is between slow and fast (or ultra-rapid) freezing, with literature data suggesting that the former is a safer technique. Hammadeh et al. [43] established that using a programmed slow freezer for sperm freezing and thawing is more effective than rapid freezing with liquid nitrogen vapor as far as preserving sperm chromatin and morphology in semen from both fertile (donor) and subfertile IVF/ICSI patients are concerned. Other studies support this finding, with Morris et al. [44] pointing out that at a rapid freezing rate, sperm cell damage is the result of osmotic imbalance encountered during thawing, rather than the formation of intracellular ice. In addition, slow programmable freezing has been shown to cause fewer morphological changes in sperm compared to freezing sperm in liquid nitrogen vapor [45]. Overall, however, the study shows that human sperm cryopreservation for one month significantly reduced sperm motility, morphology, and DNA integrity in both methods, with sperm motility more reduced by ultra-rapid freezing. It is thus worth noting that a successful cryopreservation procedure needs to take into account numerous complex associations between various process parameters and conditions, not only the freezing speed. For instance, Verheyen et al. [46] found freezing-thawing to be most effective when steam freezing was preceded by thawing at 37°C, and when slower, computer-controlled freezing was combined with thawing at 22°C, resulting in significant interactions between the freezing method and thawing temperature. For semen samples with high initial quality, both steam and computer-controlled freezing were equally effective in recovering morphologically normal, motile sperm. Other researchers focused on the impact of thawing temperature on semen parameters, showing that thawing at 40°C resulted in a statistically significant increase in sperm motility recovery compared to thawing at temperatures ranging from 20°C to 37°C. No statistically significant differences were found for sperm viability, acrosomal status, ATP content, and DNA integrity [47].
The aim of the study was to ascertain that the long-held assertion that cryopreservation may lead to sperm damage—although historically valid—is inaccurate in the light of advances in technologies and methodologies used to cryopreserve semen. In other words, the growing awareness that the quality of semen freezing and thawing processes depends on numerous factors has prompted the need to experimentally test hypotheses and replicate results of those studies that demonstrate the benefits of cryopreservation. Hence, the study aims to show that the chief advantage of properly performed cryopreservation is the selection of high-quality sperm, which is precisely the outcome expected in infertility treatment.
Materials and Methods
Semen samples (n=97) were collected via masturbation from patients undergoing infertility treatment at the KRIOBANK clinic (Białystok, Poland).
Before analysis, the semen was liquefied for 30 minutes at 37°C. To assess sperm morphology, the Sperm Stain dye (Microptic, Spain) and the Sperm Class Analyzer SCA v 6.6.0.6 software (Microptic, Spain) were used. A 15 µl aliquot of liquefied semen was placed on a glass slide and a smear was prepared. The slide was left to dry for 15 minutes on a heated plate (37°C). Staining was performed according to the manufacturer’s instructions for the staining kit, and the slide was again left to dry on the heated plate (37°C) for 30 minutes.
Sperm morphology was assessed using an OLYMPUS BX40 microscope at 60x magnification. The following parameters were evaluated using the SCA software:
- -
- Morphology: normal/abnormal sperm, Teratozoospermia Index, Sperm Deformation Index, and Multiple Anomalies Index;
- -
- Head size: normal, micro, and macro;
- -
- Head shape: normal, conical, thin, round, pear-shaped, and amorphous;
- -
- Acrosome: normal/abnormal;
- -
- Midpiece: normal, abnormal size, abnormal insertion, and abnormal angle;
- -
- Morphometrics: head length, head width, head area, head circumference, ellipsoidal heads, elongated heads, smooth heads, regular heads, midpiece width, midpiece area, midpiece angle, and acrosome-to-head ratio.
Figure 1.
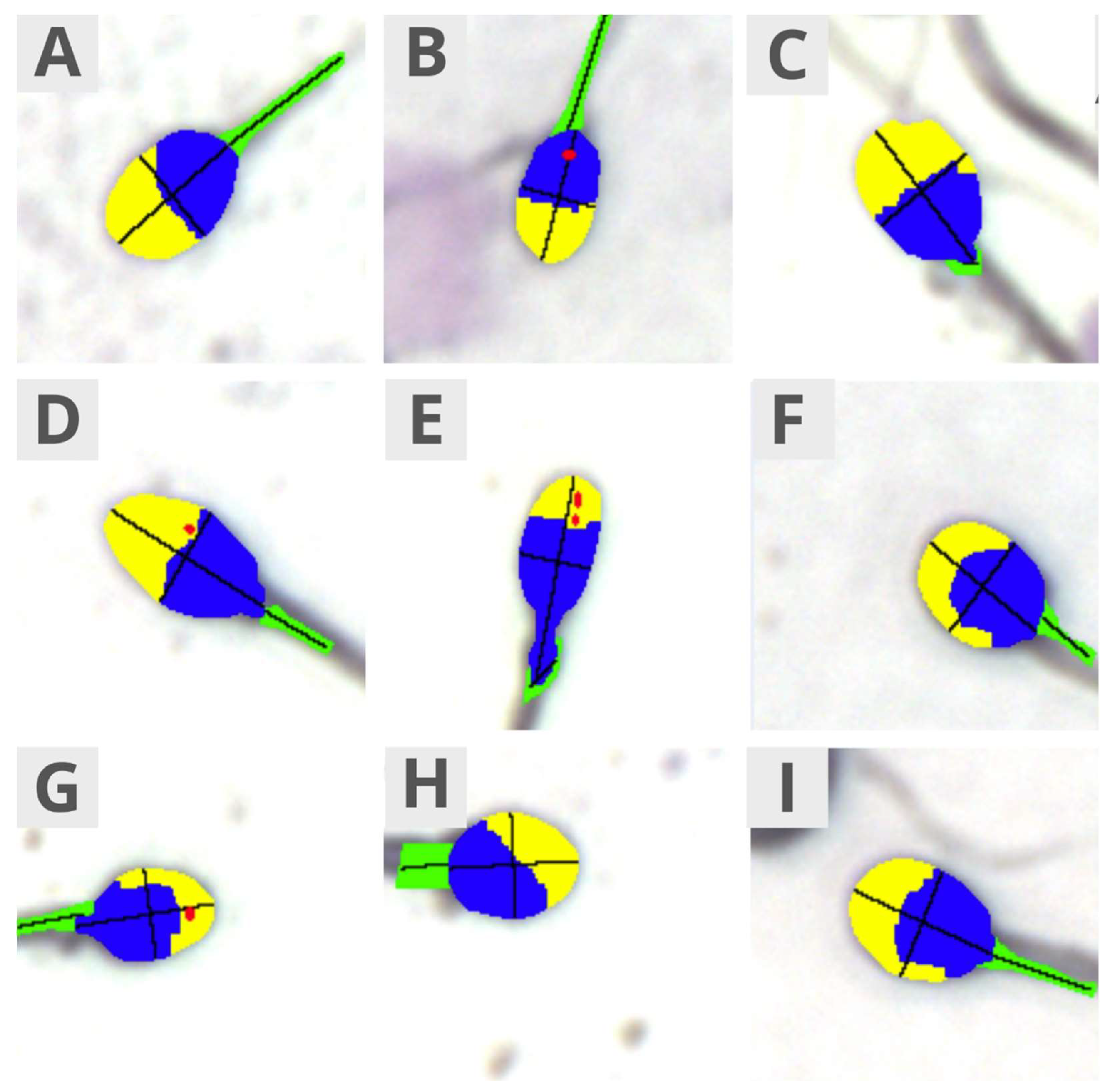
False-color microscopic images taken using the SCA Analyzer representing the following sperm features – head size: normal (A), micro (B), and macro (C); head shape: normal (A), conical (D), thin (E), round (F), pear-shaped (G), and amorphous (H); acrosome: normal (A) and abnormal (E); midpiece: normal (A), abnormal size (I), abnormal insertion (G), and abnormal angle (C); morphometrics: head ellipsoid shape (E), head elongation (E), head smoothness (A), head regularity (A). The colors denote the following parts: yellow – acrosome, blue – head, green – midpiece, red – vacuoles.
Figure 1.
False-color microscopic images taken using the SCA Analyzer representing the following sperm features – head size: normal (A), micro (B), and macro (C); head shape: normal (A), conical (D), thin (E), round (F), pear-shaped (G), and amorphous (H); acrosome: normal (A) and abnormal (E); midpiece: normal (A), abnormal size (I), abnormal insertion (G), and abnormal angle (C); morphometrics: head ellipsoid shape (E), head elongation (E), head smoothness (A), head regularity (A). The colors denote the following parts: yellow – acrosome, blue – head, green – midpiece, red – vacuoles.
Quinn’s Advantage Sperm Freezing Medium (SAGE, Denmark) was used for freezing semen. To 0.5 ml of semen, 0.5 ml of medium was added drop by drop at room temperature while mixing was performed continuously for 30 seconds. The mixture was then packed into a CBS High Security straw (0.5 ml of the mixture per straw), and the straw was sealed using a sealer. The straws were placed 10 cm above the surface of liquid nitrogen for 20 minutes, and then immersed in liquid nitrogen (-196°C). After a minimum of 24 hours, the straws were placed on a heated plate at 37°C until the semen sample was thawed (approx. 5 minutes). The preparation and analyses were performed in the same way as in the case of fresh semen.
Statistical Analysis
Normality of distribution was tested using the Kolmogorov-Smirnov test with the Lillefors correction, and the Shapiro-Wilk test. Normal distribution was not found for the analyzed quantitative variables. The non-parametric Wilcoxon test was used for comparing two dependent ordinal or quantitative variables. Statistically significant results were considered at p<0.05. The statistical calculations were performed using the Statistica 13.3 software package (TIBCO Software Inc.).
Results
A total of 32 semen parameters were analyzed before and after freezing. For 26 parameters, freezing resulted in statistically significant changes in their levels.
After freezing, the percentage of normal sperm averaged 10%, while in fresh semen, the percentage was lower, averaging 4% (p<0.001). Freezing reduced the values of the deformation index, teratozoospermia index, and multiple anomalies index (p<0.001) – Table 1, Figure 2.
Frozen semen had a higher percentage of sperm with normal-shaped heads compared to fresh semen (32% vs. 21%, p<0.0001). Freezing significantly reduced the percentage of sperm with macrocephalic heads, from 69% to 60.5% (p<0.001) – Table 2, Figure 3.
The percentage of sperm with a normal head shape in frozen semen was, on average, 57%, compared to 31% in the case of fresh semen (p<0.0001). Freezing increased the percentage of sperm with round heads, while the percentage of pear-shaped and amorphous heads decreased (p<0.0001). In frozen semen, 67.5% of sperm had a normal acrosome structure, while in fresh semen, only 61% showed a normal appearance (p=0.0009) – Table 3, Figure 4.
The evaluation of the midpiece’s appearance revealed that in frozen semen, on average, 61.5% of sperm had a normal midpiece, compared to 45% in the case of fresh semen (p<0.0001). The percentage of sperm with abnormal midpiece size, abnormal insertion, or abnormal angle was significantly lower in frozen semen (p<0.0001) – Table 4, Figure 5.
The heads of sperm in frozen semen are statistically significantly shorter than those in fresh semen (5.20 µm vs. 5.57 µm, p<0.0001). The head circumference is also smaller after freezing, but the average head width is greater (p<0.0001). Freezing reduced the percentage of sperm with ellipsoidal, elongated, and regular heads, while the percentage of sperm with smooth heads increased (p<0.0001). The width of the sperm midpiece in frozen semen averages 1.29 µm, compared to 1.42 µm in fresh semen (p<0.0001). The midpiece angle is smaller in frozen semen than in fresh semen (19.36° vs 27.05°, p<0.0001) – Table 5, Figure 6.
Discussion
The results of the study show that cryopreservation of sperm has a beneficial impact on a number of morphological parameters, which challenges the previous assumptions concerning the harmfulness of the procedure. However, in order to interpret the results correctly, the results must be viewed in the broader context of various issues connected with the process of freezing and thawing of semen, particularly those connected with technological and methodological aspects.
TZI (Teratozoospermia Index) indicates the average number of defects per abnormal sperm (reflecting the coexistence of defects in various structural components of the sperm). Hence, TZI is the ratio of the number of sperm with ≥1 defect in the head, midpiece, tail, or with excess residual cytoplasm, to the total number of morphologically abnormal sperm. The maximum possible value of this index is 4. Semen analysis of fertile and subfertile men has revealed a correlation between a sperm’s ability to fertilize an oocyte and its morphology, as expressed by the TZI value. Studies involving 103 fertile couples and 107 couples experiencing infertility found differences in TZI values, i.e., the average TZI for fertile men was 1.51±0.2 (range 1.04-2.38), while for infertile men it was 1.81±0.3 (range 1.26-2.60) [7,48]. Based on these findings, a TZI threshold value of 2.09 is proposed to distinguish fertile from infertile men.
SDI (Sperm Deformity Index) reflects the average number of defects per sperm. It is calculated as the sum of all identified head defects, the number of sperm with ≥1 midpiece and tail defects, and the number of sperm with residual cytoplasm, divided by the total number of sperm (both morphologically normal and abnormal). The maximum SDI value is 3. Studies have shown that the SDI for fertile men is between 1.50-1.60, for infertile men with low levels of reactive oxygen species (ROS) it is 1.60-1.70, while for infertile men with high ROS levels and leukocytospermia, the SDI value is significantly higher, at 1.90-2.00 [49,50,51,52].
MAI (Multiple Anomalies Index) measures the presence of multiple abnormalities within a single sperm, indicating the average number of defects per sperm [7]. This is the ratio of the total number of head, midpiece, and tail abnormalities to the number of abnormal sperm. Unlike the TZI and SDI indices, the MAI does not consider sperm with excess residual cytoplasm, and its value remains undefined.
As mentioned earlier in this article, although the use of fresh sperm for ICSI is widely practiced, it comes with several drawbacks. First of all, each IVF cycle necessitates a separate sperm extraction, which in the case of sperm retrieval by biopsy increases the costs and the risk of procedural complications, including potential damage to an already suboptimal testis. In addition, with low sperm retrieval rates in men with spermatogenic azoospermia, using cryopreservation allows to preserve successfully retrieved sperm. This makes it possible to avoid additional stress for couples, who are spared unnecessary repetitions of retrieval procedures [15]. For this reason, in men with azoospermia due to spermatogenic dysfunction, the role of cryopreservation has become significant.
Historically, there was considerable skepticism regarding the viability of cryopreserved sperm, despite the fact that the necessity for its use in certain situations [12,15] has been widely accepted. The initial concern stemmed from observations that the freezing process could be destructive to sperm, potentially impacting fertility outcomes when using frozen-thawed sperm compared to fresh sperm [43]. Early studies emphasized the risk of cryoinjury, suggesting that cryopreservation might compromise both the structural integrity and functionality of sperm cells, thus negatively influencing clinical pregnancy rates and embryo quality in ART [19], despite results to the contrary, showing that cryopreservation of testicular sperm is feasible, even in patients with non-obstructive azoospermia, and the ICSI outcomes using frozen and thawed testicular sperm are similar to those obtained with fresh testicular sperm [53]. Additionally, it was believed that cryopreservation leads to a significant deterioration in sperm morphology and thus lower fertilization rates [22,23]. Ulug et al. [54] performed a comparative study whose results showed that cryopreservation harms both testicular and ejaculated sperm by causing intracellular ice formation, which ruptures the plasma membrane and allows oxidative damage to DNA. It has to be emphasized that the adverse effect of cryopreservation on semen quality was not a consensual view in literature. For instance, Friedler et al. [55] showed that sperm cryopreservation using a simple freezing protocol in patients with obstructive azoospermia is feasible and effective, and should be offered to optimize pregnancy outcomes following such procedures. Similarly, another study from the same year (1998) did not show significant differences in the outcomes of using fresh or frozen epididymal sperm for intracytoplasmic sperm injection (ICSI) [56].
Despite the concerns discussed above, advances in freezing techniques, including improved cryoprotectants and controlled freezing protocols, have largely mitigated these early limitations, rendering cryopreserved sperm comparable in efficacy to fresh sperm in many contexts [11,24,57]. It should be noted, however, that cryopreservation can indeed damage sperm through several processes, primarily involving cellular dehydration, oxidative stress, and osmotic stress. The formation of intracellular ice crystals during freezing can disrupt the sperm’s plasma membrane and organelles, while oxidative stress from reactive oxygen species (ROS) leads to lipid peroxidation, DNA fragmentation, and compromised motility [58,59]. Moreover, stress from temperature fluctuations and osmotic imbalances can induce regulated cell death (RCD) mechanisms such as apoptosis and ferroptosis, which further deteriorate semen quality [58]. These cumulative effects, known as cryoinjury, underscore the importance of selecting optimal cryoprotectants that can shield sperm cells during the freeze-thaw cycle. Notably, antioxidants have been investigated as supplementary agents to counteract oxidative damage, though the ideal combination remains to be established [18].
Another aspect that plays a crucial role in the success or failure of ART procedures is the fact that sperm selection prior to freezing improves the quality of the cryopreserved semen sample immediately before insemination [39]. This aspect reflects a broader issue connected with semen quality, i.e., the quality vs. quantity dichotomy. As only a single sperm is necessary for a successful conception, procedures that increase the chances that the most viable, high-quality spermatozoa will be used for fertilization also increase the chances of success of the process. It has been shown that sperm selection results in an increase in sperm motility regardless of the separation technique used, but is particularly evident with the swim-up and Felix™ procedures [18]. Donnelly et al. [60] suggest that isolating the subpopulation of sperm with the highest motility and DNA integrity and freezing them in seminal plasma may be the optimal approach for obtaining high-quality sperm. This conclusion was based on their finding that sperm frozen unprocessed in seminal fluid proved to be more resistant to freezing damage than processed frozen sperm. The results of a study performed by Spanò et al. [61] showed that, post-selection, sperm comprise a subpopulation that is characterized by an overall improvement in morphological parameters and kinetic properties. This fraction also demonstrated improved chromatin structure characteristics, confirming that these cells have good structural and functional traits, indicating optimal fertilizing potential. This result emphasizes that the process of selection is the key feature of cryopreservation that influences the overall quality of semen post-thawing.
Another aspect that needs to be considered in view of the quality of semen post-freezing is sperm preparation. Palomar Rios et al. [28] suggest that freezing sperm prior to swim-up selection should be considered to achieve better outcomes after thawing, especially in patients presenting with a poor baseline sperm profile.
The results of the present study suggest that freezing may enhance certain sperm parameters, potentially improving the quality of samples for assisted reproductive techniques. Many of the parameters improved by cryopreservation are those related to sperm morphology. The proportion of morphologically normal sperm post-freezing increased from 4% in fresh samples to 10%. Similarly, a reduction in anomaly indices was observed, with indices describing deformation, teratozoospermia, and multiple anomalies were significantly lower after freezing. In addition, frozen sperm samples showed a higher percentage of normally shaped heads (32% vs. 21%) and correct tail insertions and sizes, with a reduction in macro head sizes and abnormal insertions. These results are in line with literature data [15] which show that cryopreservation—when performed properly—does not lead to the deterioration of semen quality, but may in fact improve it by increasing the fractions of higher-quality spermatozoa in a sample.
It is worth emphasizing that improved sperm morphology may also be associated with improved motility parameters. The results of a recent systematic review and meta-analysis performed by Umirbaeva et al. [62] show that the percentage of morphological abnormalities and the DNA Fragmentation Index (DFI) were lower in sperm with high viability, while mitochondrial membrane potential (MMP) and motility were the most important sperm quality parameters, with minimal publication bias and a notable correlation with sperm viability. Although the study concerns cattle, its findings may be considered valid in terms of human reproduction due to the robust methodology of the study and the inherent similarities between the sperm of various mammalian species.
One of the most important findings of this study is the fact that properly performed cryopreservation may in fact lead to the improvement of semen quality. This corroborates the findings of a prospective randomized study performed by Kuczyński et al. [16], who investigated the fertilization and pregnancy outcomes using fresh versus cryopreserved ejaculated sperm in ICSI. The results demonstrated no significant difference in fertilization and pregnancy rates, suggesting that cryopreservation does not adversely affect reproductive potential. Interestingly, cryopreserved sperm achieved a higher rate of ongoing pregnancies compared to fresh sperm, indicating that cryopreservation may serve as an effective method for selecting viable sperm with greater resilience. These findings reinforce that cryopreservation can be a valuable procedure, especially for patients with compromised semen quality, by enabling the identification and selection of sperm that are more likely to withstand the stresses of ART procedures.
Sperm cryopreservation remains a pivotal technique in reproductive medicine, despite inherent challenges associated with cryoinjury. The evolution of cryoprotectants, freezing protocols, and sperm selection techniques continues to improve post-thaw semen quality, making cryopreserved sperm a viable option in ART and fertility preservation. Future research should aim to refine cryopreservation techniques further to enhance post-thaw semen parameters and investigate the molecular pathways involved in cryoinjury to optimize outcomes in reproductive health.
Conclusions
This study demonstrates that cryopreservation, when performed with refined protocols, can improve semen parameters, contradicting the traditional view that freezing compromises semen quality. Post-freezing analyses performed in the study showed significant improvements in sperm morphology. These findings suggest that modern cryopreservation techniques may not only preserve but also enhance the quality of semen, facilitating better outcomes in ART. The ability to select higher-quality sperm through freezing presents practical benefits for patients requiring fertility preservation. Both the results of this study and literature data suggest that instead of avoiding cryopreservation due to the adherence to outdated misconceptions, it is instead crucial to ensure that the procedure is performed properly. Optimal cryopreservation protocols are thus critical to minimize cryoinjury and maintain sperm viability post-thawing. Future studies should further explore cryopreservation protocols and their impact on sperm resilience, aiming to optimize outcomes for male fertility preservation and reproductive health.
Limitations of the Study
The study analyzed a relatively small sample size of 97, limiting the generalizability of the findings. Future research involving larger populations could provide a broader understanding of cryopreservation effects. Additionally, since this study primarily focused on sperm morphology, its results do not allow to make direct inferences in relation to the impact of cryopreservation on other semen parameters that are important in terms of infertility treatment, sperm motility in particular.
Author Contributions
Conceptualization, A.J.M., W.K. and R.M.; methodology, A.J.M., W.K. and R.M.; software, A.J.M., W.K. and R.M.; validation, A.J.M and R.M; formal analysis, A.J.M; investigation, I.M, S.D.-B., and P.S.; resources, A.K. and W.K; data curation, W.K.; writing—original draft preparation, A.J.M.; writing—review and editing, A.J.M., M.P., and R.M.; visualization, A.J.M.; supervision, W.K. and R.M.; funding acquisition, W.K. and R.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. According to applicable Polish law, Bioethics Committee approval was not required, as the study involved research on biological material for which such approval is not necessary.
Informed Consent Statement
Informed consent was obtained from subjects for the use of their biological material in scientific studies.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Agarwal, A.; Mulgund, A.; Hamada, A.; Chyatte, M.R. A unique view on male infertility around the globe. Reproductive Biology and Endocrinology 2015, 13. [Google Scholar] [CrossRef] [PubMed]
- Zańko, A.; Martynowicz, I.; Citko, A.; Konopka, P.; Paszko, A.; Pawłowski, M.; Szczerbiński, Ł.; Siewko, K.; Krętowski, A.J.; Kuczyński, W.; Milewski, R. The Influence of Lifestyle on Male Fertility in the Context of Insulin Resistance—Identification of Factors That Influence Semen Quality. J. Clin. Med. 2024, 13, 2797. [Google Scholar] [CrossRef] [PubMed]
- Cocuzza, M.; Alvarenga, C.; Pagani, R. The epidemiology and etiology of azoospermia. Clinics (Sao Paulo) 2013, 68, 15–26. [Google Scholar] [CrossRef]
- Barratt, C.L.R. Semen analysis is the cornerstone of investigation for male infertility. Practitioner 2007, 251, 8–10, 12, 15. [Google Scholar] [PubMed]
- Goyal, R.; Kotru, M.; Gogia, A.; Sharma, S. Qualitative defects with normal sperm counts in a patient attending infertility clinic. Indian J Pathol Microbiol 2018, 61, 233–235. [Google Scholar]
- Boitrelle, F.; Shah, R.; Saleh, R.; Henkel, R.; Kandil, H.; Chung, E.; Vogiatzi, P.; Zini, A.; Arfa, M.; Agarwal, A. The Sixth Edition of the WHO Manual for Human Semen Analysis: A Critical Review and SWOT Analysis. Life (Basel) 2021, 11, 1368. [Google Scholar] [CrossRef]
- WHO laboratory manual for the Examination and processing of human semen, 5th ed.; World Health Organization, 2010.
- López-Botella, A.; Velasco, I.; Acién, M.; Sáez-Espinosa, P.; Todolí-Torró, J.-L.; Sánchez-Romero, R.; Gómez-Torres, M.J. Impact of Heavy Metals on Human Male Fertility—An Overview. Antioxidants (Basel) 2021, 10, 1473. [Google Scholar] [CrossRef]
- WHO laboratory manual for the examination and processing of human semen, 6th Ed. ed; World Health Organization, 2021.
- Tamburrino, L.; Traini, G.; Marcellini, A.; Vignozzi, L.; Baldi, E.; Marchiani, S. Cryopreservation of Human Spermatozoa: Functional, Molecular and Clinical Aspects. Int J Mol Sci 2023, 24, 4656. [Google Scholar] [CrossRef]
- Yu, Z.; Wei, Z.; Yang, J.; Wang, T.; Jiang, H.; Li, H.; Tang, Z.; Wang, S.; Liu, J. Comparison of intracytoplasmic sperm injection outcome with fresh versus frozen-thawed testicular sperm in men with nonobstructive azoospermia: a systematic review and meta-analysis. J Assist Reprod Genet 2018, 35, 1247–1257. [Google Scholar] [CrossRef]
- Jungwirth, A.; Diemer, T.; Kopa, Z.; Krausz, C.; Minhas, S.; Tournaye, H. EAU Guidelines on Male Fertility. European Association of Urology 2019.
- DIRECTIVE 2004/23/EC OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL of 31 March 2004 on setting standards of quality and safety for the donation, procurement, testing, processing, preservation, storage and distribution of human tissues and cells, vol. L 102, 2004, pp. 48-58.
- Commission Directive 2006/17/EC of 8 February 2006 implementing Directive 2004/23/EC of the European Parliament and of the Council as regards certain technical requirements for the donation, procurement and testing of human tissues and cells (Text with EE, vol. L 330M, 2006, pp. 162-174.
- Ohlander, S.; Hotaling, J.; Kirshenbaum, E.; Niederberger, C.; Eisenberg, M.L. Impact of fresh versus cryopreserved testicular sperm upon intracytoplasmic sperm injection pregnancy outcomes in men with azoospermia due to spermatogenic dysfunction: a meta-analysis. Fertil Steril 2014, 101, 344–9. [Google Scholar] [CrossRef] [PubMed]
- Kuczyński, W.; Dhont, M.; Grygoruk, C.; Grochowski, D.; Wołczyński, S.; Szamatowicz, M. The outcome of intracytoplasmic injection of fresh and cryopreserved ejaculated spermatozoa--a prospective randomized study. Hum Reprod 2001, 16, 2109–13. [Google Scholar] [CrossRef] [PubMed]
- Tournaye, H.; Merdad, T.; Silber, S.; et al. No differences in outcome after intracytoplasmic sperm injection with fresh of with frozen-thawed epididymal spermatozoa. Hum Reprod 1999, 14, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Hungerford, A.; Bakos, H.W.; Aitken, R.J. Sperm cryopreservation: current status and future developments. 2023, 35, 265–281. [Google Scholar] [CrossRef]
- Borate, G.M.; Meshram, A. Cryopreservation of Sperm: A Review. Cureus 2022, 14, e31402. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Tang, Y.-L.; Hu, J.-L.; Zhou, W.-J.; Huang, Z.-H.; Luo, X.-F.; Li, Z.; Zhu, W.-B. Update on techniques for cryopreservation of human spermatozoa. Asian J Androl 2022, 24, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Eastick, J.; Venetis, C.; Cooke, S.; Storr, A.; Susetio, D.; Chapman, M. Is early embryo development as observed by time-lapse microscopy dependent on whether fresh or frozen sperm was used for ICSI? A cohort study. J Assist Reprod Genet 2017, 34, 733–740. [Google Scholar] [CrossRef]
- O'Connell, M.; McClure, N.; Lewis, S.E.M. The effects of cryopreservation on sperm morphology, motility and mitochondrial function. Hum Reprod 2002, 17, 704–9. [Google Scholar] [CrossRef]
- Hammadeh, M.E.; Askari, A.S.; Georg, T.; Rosenbaum, P.; Schmidt, W. Effect of freeze-thawing procedure on chromatin stability, morphological alteration and membrane integrity of human spermatozoa in fertile and subfertile men. 1999, 22, 155. [Google Scholar] [CrossRef]
- Ozimic, S.; Ban-Frangez, H.; Stimpfel, M. Sperm Cryopreservation Today: Approaches, Efficiency, and Pitfalls. Curr. Issues Mol. Biol 2023, 45, 4716–4734. [Google Scholar] [CrossRef]
- Di Santo, M.; Tarozzi, N.; Nadalini, M.; Borini, A. Human Sperm Cryopreservation: Update on Techniques, Effect on DNA Integrity, and Implications for ART. Adv Urol 2012, 13, 854837. [Google Scholar] [CrossRef] [PubMed]
- O'Neill, H. C.; Nikoloska, M.; Ho, H.; Doshi, A.; Maalouf, W. Improved cryopreservation of spermatozoa using vitrification: comparison of cryoprotectants and a novel device for long-term storage. J Assist Reprod Genet 2019, 36, 1713–1720. [Google Scholar] [CrossRef] [PubMed]
- Hungerford, A.J.; Bakos, H.W.; Aitken, R.J. Analysis of sperm separation protocols for isolating cryopreserved human spermatozoa. Reprod Fertil 2023, 4, 220133. [Google Scholar] [CrossRef] [PubMed]
- Rios, A.P.; Gascón, A.; Martínez, J.V.; Balasch, S.; Botella, I.M. Sperm preparation after freezing improves motile sperm count, motility, and viability in frozen-thawed sperm compared with sperm preparation before freezing-thawing process. J Assist Reprod Genet 2018, 35, 237–245. [Google Scholar] [CrossRef]
- Coutton, C.; Escoffier, J.; Martinez, G.; Arnoult, C.; Ray, P.F. Teratozoospermia: spotlight on the main genetic actors in the human. Human Reproduction Update 2015, 21, 455–485. [Google Scholar] [CrossRef]
- De Braekeleer, M.; Nguyen, M.H.; Morel, F.; Perrin, A. Genetic aspects of monomorphic teratozoospermia: a review. J Assist Reprod Genet 2015, 32, 615–623. [Google Scholar] [CrossRef]
- Chemes, H.E. Sperm Ultrastructure in Fertile Men and Male Sterility: Revisiting Teratozoospermia. In The Sperm Cell: Production, Maturation, Fertilization, Regeneration; Cambridge University Press, 2017; pp. 36–58. [Google Scholar]
- Fesahat, F.; Henkel, R.; Agarwal, A. Globozoospermia syndrome: An update. Andrologia 2019. [CrossRef]
- Carmignac, V.; Dupont, J.-M.; Fierro, R.C.; Berberet, J.; Bruno, C.; Lieury, N.; Dulioust, E.; Auger, J.; Fauque, P. Diagnostic genetic screening for assisted reproductive technologies patients with macrozoospermia. Andrology 2017, 5, 37–380. [Google Scholar] [CrossRef]
- Elkhatib, R.A.; Paci, M.; Longepied, G.; Saias-Magnan, J.; Courbiere, B.; Guichaoua, M.-R.; Levy, N.; Metzler-Guillemain, C.; Mitchell, M.J. Homozygous deletion of SUN5 in three men with decapitated spermatozoa. Human Molecular Genetics 2017, 26, 3167–3171. [Google Scholar] [CrossRef]
- Fang, J.; Zhang, J.; Zhu, F.; Yang, X.; Cui, Y.; Liu, J. Patients with acephalic spermatozoa syndrome linked to SUN5 mutations have a favorable pregnancy outcome from ICSI. Andrology 2018, 33, 372–377. [Google Scholar] [CrossRef]
- Walczak-Jędrzejowska, R.; Bakalczuk, S.; Berger, A.; Bergier, L.; Filipiak, E.; Frącki, S.; Jędrzejczak, P.; Kula, K.; Marchlewska, K.; Piasecka, M.; Puacz, E.; Słowikowska-Hilczer, J.; Zagocka, G.T.-H.I.E. Podstawowe badanie nasienia - rekomendacje Polskiego Towarzystwa Andrologicznego i Krajowej Izby Diagnostów Laboratoryjnych. w Postępy Andrologii Online, 2015.
- Ragini, G.; Caccamo, A.M.; Serra, A.D.; Guercilena, S. Computerized slow-staged freezing of semen from men with testicular tumors or Hodgkin's disease preserves sperm better than standard vapor freezing. Fertil Steril 1990, 53, 1072–5. [Google Scholar] [CrossRef] [PubMed]
- Raad, G.; Lteif, L.; Lahoud, R.; Azoury, J.; Tanios, J.; Hazzouri, M. Cryopreservation media differentially affect sperm motility, morphology and DNA integrity. Andrology 2018, 6, 836–845. [Google Scholar] [CrossRef] [PubMed]
- Androni, D.A.; Dodds, S.; Tomlinson, M.; Maalouf, W.E. Is pre-freeze sperm preparation more advantageous than post-freeze? Reprod Fertil 2021, 2, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Dede, G.; Saylan, A. The effect of astaxanthin on human sperm parameters after cryopreservation. Can Urol Assoc J 2022, 16, E552–E557. [Google Scholar] [CrossRef]
- Ghantabpour, T.; Nashtaei, M.S.; Nekoonam, S.; Razaei, H.; Amidi, F. The Effect of Astaxanthin on Motility, Viability, Reactive Oxygen Species, Apoptosis, and Lipid Peroxidation of Human Spermatozoa During the Freezing-Thawing Process. Biopreserv Biobank 2022, 22, 367–373. [Google Scholar] [CrossRef]
- Huang, C.; Gan, R.-X.; Hu, J.-L.; Liu, F.; Hong, Y.; Zhu, W.-B.; Li, Z. Clinical benefit for cryopreservation of single human spermatozoa for ICSI: A systematic review and meta-analysis. Andrology 2022, 10, 82–91. [Google Scholar] [CrossRef]
- Hammadeh, M.E.; Dehn, C.; Hippach, M.; Zeginiadou, T.; Stieber, M.; Georg, T.; Rosenbaum, P.; Schmidt, W. Comparison between computerized slow-stage and static liquid nitrogen vapour freezing methods with respect to the deleterious effect on chromatin and morphology of spermatozoa from fertile and subfertile men. Int J Androl 2001, 24, 66–72. [Google Scholar] [CrossRef]
- Morris, G.J.; Acton, E.; Murray, B.J.; Fonseca, F. Freezing injury: the special case of the sperm cell. Cryobiology 2012, 64, 71–80. [Google Scholar] [CrossRef]
- Tongdee, P.; Sukprasert, M.; Satirapod, C.; Wongkularb, A.; Choktanasiri, V. Comparison of Cryopreserved Human Sperm between Ultra Rapid Freezing and Slow Programmable Freezing: Effect on Motility, Morphology and DNA Integrity. J Med Assoc Thai 2015, 98. [Google Scholar]
- Verheyen, G.; Pletincx, I.; Van Steirteghem, A. Effect of freezing method, thawing temperature and post-thaw dilution/washing on motility (CASA) and morphology characteristics of high-quality human sperm. Hum Reprod 1993, 8, 1678–84. [Google Scholar] [CrossRef]
- Calamera, J.C.; Buffone, M.G.; Doncel, G.F.; Brugo-Olmeda, S.; de Vincentiis, S.; Calamera, M.M.; Storey, B.T.; Alvarez, J.G. Effect of thawing temperature on the motility recovery of cryopreserved human spermatozoa. Fertility and Sterility 2010, 93, 789–794. [Google Scholar] [CrossRef] [PubMed]
- Menkveld, R.; Wong, W.Y.; Lombard, C.J.; Wetzels, A.M.; Thomas, C.M.; Merkus, H.M. Semen parameters, including WHO and strict criteria morphology, in a fertile population: an effort towards standardization of in-vivo thresholds. Hum Reprod 2001, 16, 1165–71. [Google Scholar] [CrossRef] [PubMed]
- Aziz, N.; Said, T.; Paasch, U.; Agarwal, A. The relationship between human sperm apoptosis, morphology and the sperm deformity index. Hum Reprod 2007, 22, 1413–1419. [Google Scholar] [CrossRef] [PubMed]
- Said, T.M.; Agarwal, A.; Sharma, R.K.; Thomas, A.J., Jr.; Sikka, S.C. Impact of sperm morphology on DNA damage caused by oxidative stress induced by beta-nicotinamide adenine dinucleotide phosphate. Fertil Steril 2005, 83, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Said, T.M.; Aziz, N.; Sharma, R.K.; Lewis-Jones, I.; Thomas, A.J., Jr.; Agarwal, A. Novel association between sperm deformity index and oxidative stress-induced DNA damage in infertile male patients. Asian J Androl 2005, 7, 121–6. [Google Scholar] [CrossRef] [PubMed]
- Aziz, N.; Sharma, R.K.; Mahfouz, R.; Jha, R.; Agarwal, A. Association of sperm morphology and the sperm deformity index (SDI) with poly (ADP-ribose) polymerase (PARP) cleavage inhibition. 2011, 95, 2481–4. [Google Scholar]
- Gil-Salom, M.; Romero, J.; Minguez, Y.; Rubio, C.; De los Santos, M.J.; Remohí, J.; Pellicer, A. Pregnancies after intracytoplasmic sperm injection with cryopreserved testicular spermatozoa. Hum Reprod 1996, 11, 1309–13. [Google Scholar] [CrossRef]
- Ulug, U.; Bener, F.; Karagenc, L.; Ciray, N.; Bahceci, M. Outcomes in couples undergoing ICSI: comparison between fresh and frozen-thawed surgically retrieved spermatozoa. Int J Androl 2005, 28, 343–9. [Google Scholar] [CrossRef]
- Friedler, S.; Raziel, A.; Strassburger, D.; Komarovsky, D.; Ron-El, R. The outcome of intracytoplasmic injection of fresh and cryopreserved epididymal spermatozoa from patients with obstructive azoospermia--a comparative study. Hum Reprod 1998, 13, 1872–7. [Google Scholar] [CrossRef]
- Garrels, K.L.; Zini, A.S.; Casper, R.F.; Meriano, J.S.; Jarvi, K.A. Fresh and frozen epididymal sperm yield comparable pregnancy rates for intracytoplasmic sperm injection. Arch Androl 1998, 41, 159–65. [Google Scholar] [CrossRef]
- Cherouveim, P.; Vagios, S.; Hammer, K.; Fitz, V.; Jiang, V.S.; Dimitriadis, I.; Sacha, C.R.; James, K.E.; Bormann, C.L.; Souter, I. The impact of cryopreserved sperm on intrauterine insemination outcomes: is frozen as good as fresh? Front Reprod Health 2023, 31, 1181751. [Google Scholar] [CrossRef] [PubMed]
- Hai, E.; Zhang, J.; Zhang, J. Sperm freezing damage: the role of regulated cell death. Cell Death Discovery 2024, 10. [Google Scholar] [CrossRef] [PubMed]
- Gouhier, C.; Pons-Rejraji, H.; Dollet, S.; Chaput, L.; Bourgne, C.; Berger, M.; Pereira, B.; Tchirkov, A.; Brugnon, F. Freezing Does Not Alter Sperm Telomere Length despite Increasing DNA Oxidation and Fragmentation. Genes (Basel) 2023, 14, 1039. [Google Scholar] [CrossRef]
- Donnelly, E.T.; McClure, N.; Lewis, S.E. Cryopreservation of human semen and prepared sperm: effects on motility parameters and DNA integrity. 2001, 76, 892–900. [Google Scholar] [CrossRef]
- Spanò, M.; Cordelli, E.; Leter, G.; Lombardo, F.; Lenzi, A.; Gandini, L. Nuclear chromatin variations in human spermatozoa undergoing swim-up and cryopreservation evaluated by the flow cytometric sperm chromatin structure assay. Mol Hum Reprod 1999, 5, 29–37. [Google Scholar] [CrossRef]
- Umirbaeva, A.; Kurenkov, A.; Makhanbetova, A.; Seisenov, B.; Vorobjev, I.A.; Barteneva, N.S. Systematic review and meta-analysis of cryopreserved bovine sperm assessment: harnessing imaging flow cytometry for multi-parametric analysis. Front Vet Sci 2024, 11, 1371586. [Google Scholar] [CrossRef]
- Yurchuk, T.; Petrushko, M.; Gapon, A.; Piniaiev, V.; Kuleshova, L. The impact of cryopreservation on the morphology of spermatozoa in men with oligoasthenoteratozoospermia. Cryobiology 2021, 100, 117–124. [Google Scholar] [CrossRef]
Figure 2.
Comparison of sperm morphology in fresh and frozen semen – box plots for parameters that showed statistically significant differences.
Figure 2.
Comparison of sperm morphology in fresh and frozen semen – box plots for parameters that showed statistically significant differences.
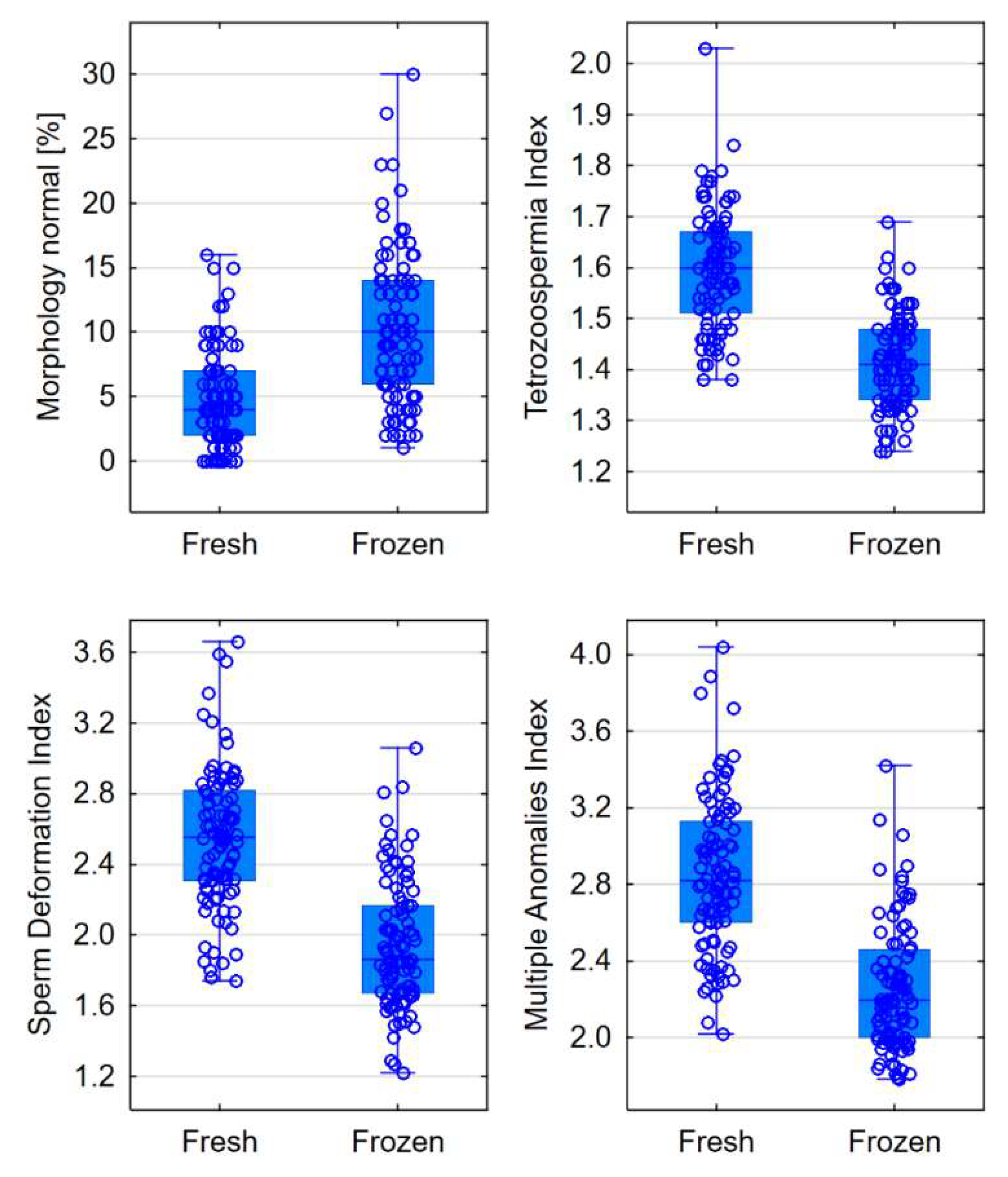
Figure 3.
Comparison of head sizes in fresh and frozen semen – box plots for parameters that showed statistically significant differences.
Figure 3.
Comparison of head sizes in fresh and frozen semen – box plots for parameters that showed statistically significant differences.
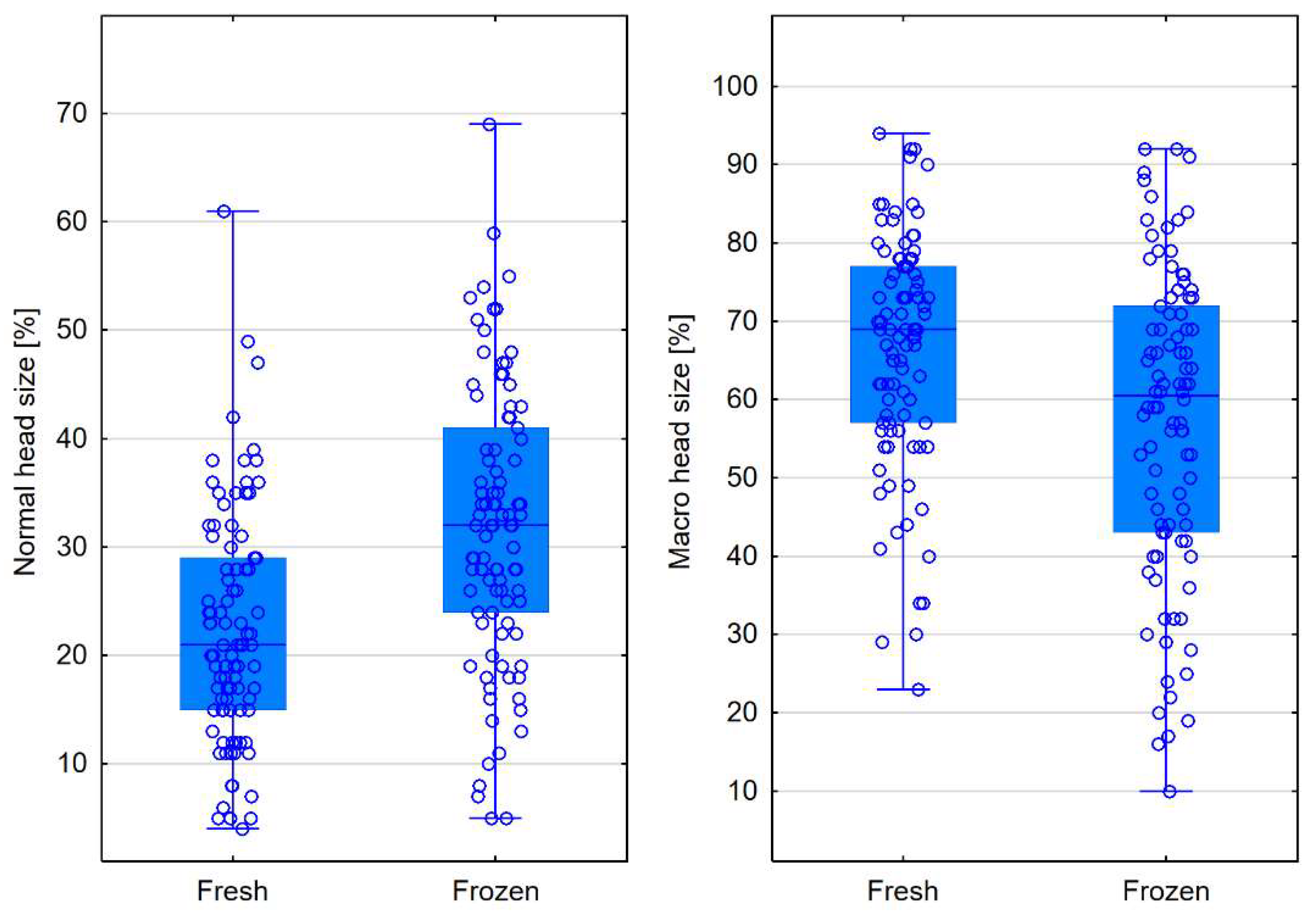
Figure 4.
Comparison of head shape and acrosome structure in fresh and frozen semen – box plots for parameters that showed statistically significant differences.
Figure 4.
Comparison of head shape and acrosome structure in fresh and frozen semen – box plots for parameters that showed statistically significant differences.
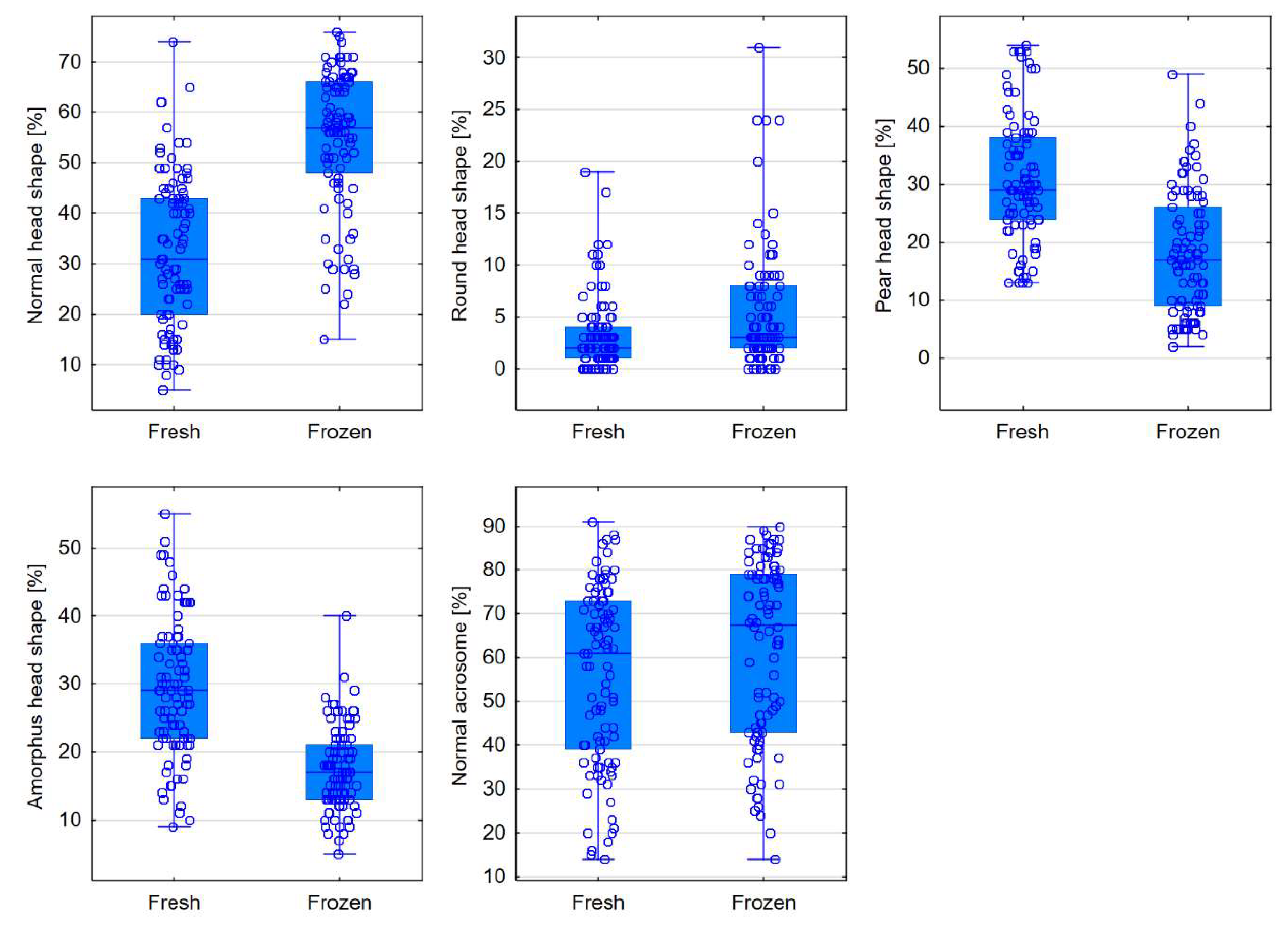
Figure 5.
Comparison of the midpiece in fresh and frozen semen – box plots for parameters that showed statistically significant differences.
Figure 5.
Comparison of the midpiece in fresh and frozen semen – box plots for parameters that showed statistically significant differences.
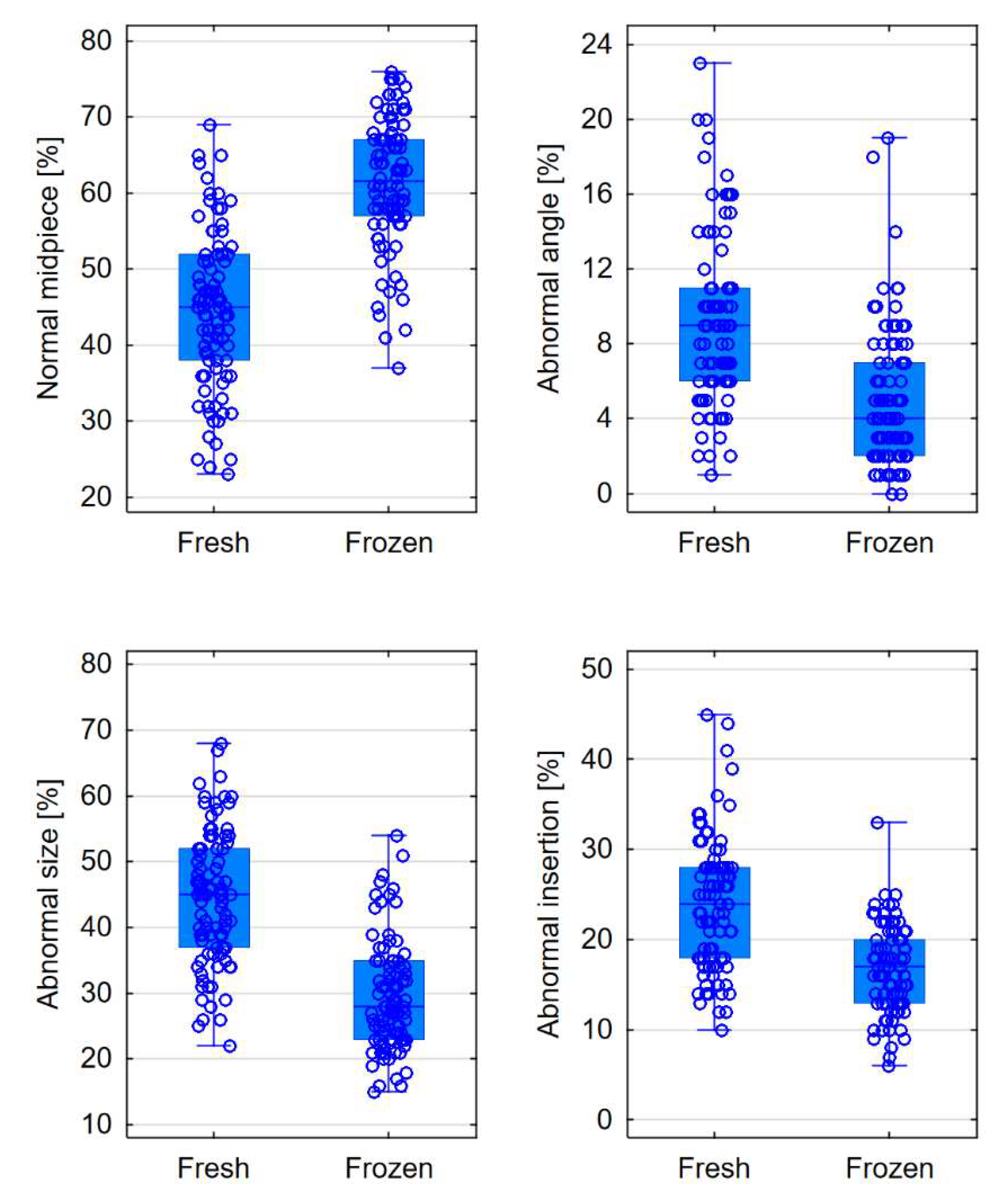
Figure 6.
Comparison of morphometric parameters in fresh and frozen semen – box plots for parameters that showed statistically significant differences.
Figure 6.
Comparison of morphometric parameters in fresh and frozen semen – box plots for parameters that showed statistically significant differences.
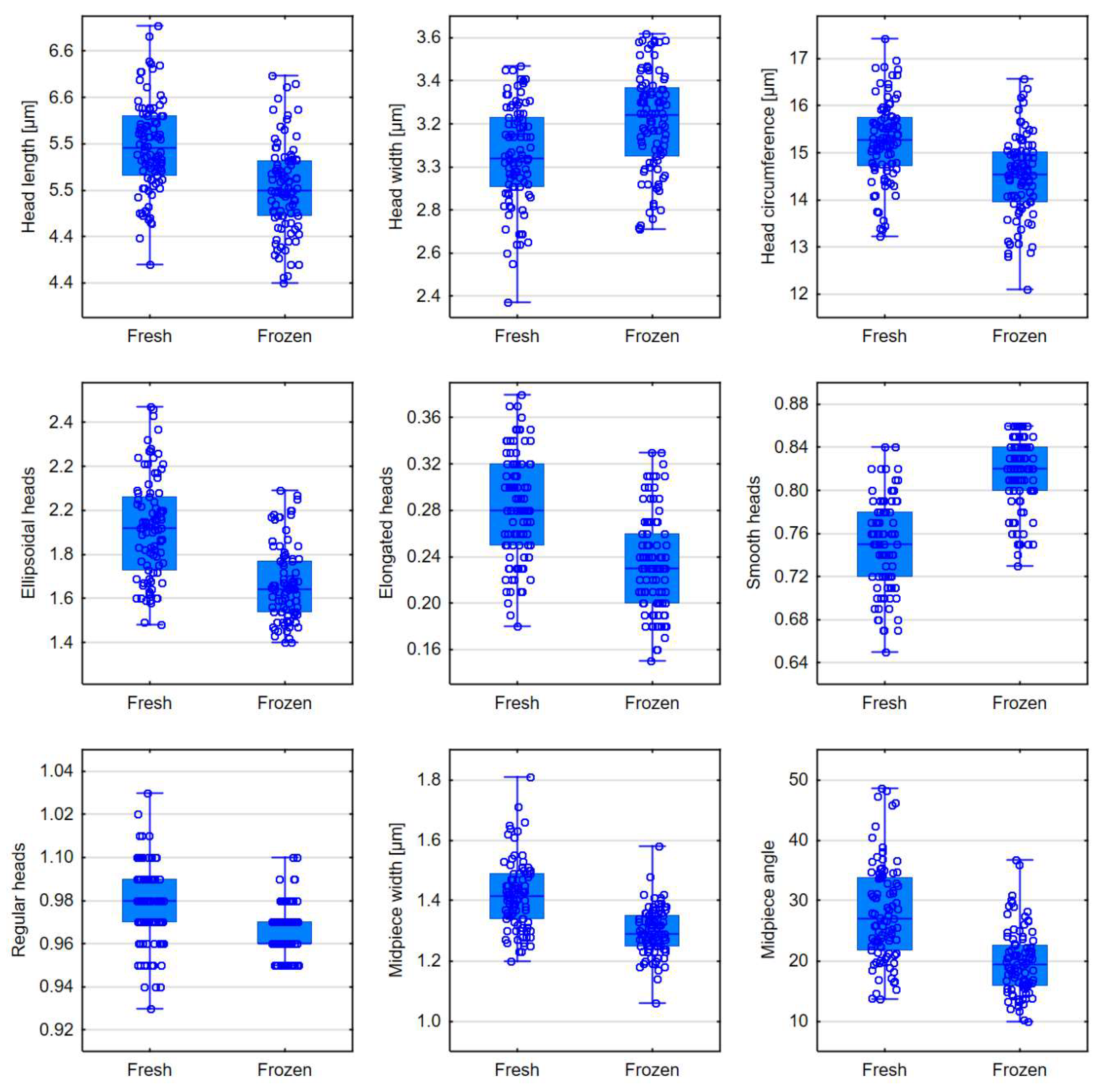

Table 1.
Comparison of semen morphology in fresh and frozen semen. Results are presented as median with the 25th and 75th percentiles.
Table 1.
Comparison of semen morphology in fresh and frozen semen. Results are presented as median with the 25th and 75th percentiles.
| Morphology | Fresh semen | Frozen semen | p level |
|---|---|---|---|
| Normal [%] | 4 (2-7) | 10 (6-14) | <0.0001 |
| Teratozoospermia Index (TZI) | 1.60 (1.51-1.67) | 1.41 (1.34-1.48) | <0.0001 |
| Sperm Deformation Index (SDI) | 2.56 (2.31-2.82) | 1.86 (1.67-2.17) | <0.0001 |
| Multiple Anomalies Index (MAI) | 2.82 (2.60-3.13) | 2.20 (2.00-2.46) | <0.0001 |
Table 2.
Comparison of head size in fresh and frozen semen. Results are presented as median with 25th and 75th percentiles.
Table 2.
Comparison of head size in fresh and frozen semen. Results are presented as median with 25th and 75th percentiles.
| Head size | Fresh semen | Frozen semen | p level |
|---|---|---|---|
| Normal [%] | 21 (15-29) | 32 (24-41) | <0.0001 |
| Micro [%] | 8 (5-15) | 6.5 (3-15) | 0.2694 |
| Macro [%] | 69 (57-77) | 60.5 (43-72) | <0.0001 |
Table 3.
Comparison of head shape and acrosome structure in fresh and frozen semen. Results are presented as median with 25th and 75th percentiles.
Table 3.
Comparison of head shape and acrosome structure in fresh and frozen semen. Results are presented as median with 25th and 75th percentiles.
| Head shape | Fresh semen | Frozen semen | p level |
|---|---|---|---|
| Normal [%] | 31 (20-43) | 57 (48-66) | <0.0001 |
| Conical [%] | 0 (0-1) | 1 (0-2) | 0.0665 |
| Thin [%] | 3 (1-5) | 2 (0-5) | 0.0580 |
| Round [%] | 2 (1-4) | 3 (2-8) | <0.0001 |
| Pear-shaped [%] | 29 (24-38) | 17 (9-26) | <0.0001 |
| Amorphous [%] | 29 (22-36) | 17 (13-21) | <0.0001 |
| Acrosome | |||
| Normal [%] | 61 (39-73) | 67.5 (43-79) | 0.0009 |
Table 4.
Comparison of the midpiece in fresh and frozen semen. Results are presented as median with 25th and 75th percentiles.
Table 4.
Comparison of the midpiece in fresh and frozen semen. Results are presented as median with 25th and 75th percentiles.
| Midpiece | Fresh semen | Frozen semen | p level |
|---|---|---|---|
| Normal midpiece [%] | 45 (38-52) | 61.5 (57-67) | <0.0001 |
| Abnormal size [%] | 45 (37-52) | 28 (23-35) | <0.0001 |
| Abnormal insertion [%] | 24 (18-28) | 17 (13-20) | <0.0001 |
| Abnormal angle [%] | 9 (6-11) | 4 (2-7) | <0.0001 |
Table 5.
Comparison of morphometric parameters in fresh and frozen semen. Results are presented as median with 25th and 75th percentiles.
Table 5.
Comparison of morphometric parameters in fresh and frozen semen. Results are presented as median with 25th and 75th percentiles.
| Morphometrics | Fresh semen | Frozen semen | p level |
|---|---|---|---|
| Head length [μm] | 5.57 (5.33-5.84) | 5.20 (4.98-5.45) | <0.0001 |
| Head width [μm] | 3.04 (2.91-3.23) | 3.24 (3.05-3.37) | <0.0001 |
| Head area [μm2] | 13.78 (12.89-14.48) | 13.72 (12.69-14.54) | 0.7831 |
| Head circumference [μm] | 15.27 (14.73-15.75) | 14.55 (13.96-15.02) | <0.0001 |
| Ellipsoidal heads | 1.92 (1.73-2.06) | 1.64 (1.54-1.77) | <0.0001 |
| Elongated heads | 0.28 (0.25-0.32) | 0.23 (0.20-0.26) | <0.0001 |
| Smooth heads | 0.75 (0.72-0.78) | 0.82 (0.80-0.84) | <0.0001 |
| Regular heads | 0.98 (0.97-0.99) | 0.96 (0.96-0.97) | <0.0001 |
| Midpiece width [μm] | 1.42 (1.34-1.49) | 1.29 (1.25-1.35) | <0.0001 |
| Midpiece area [μm2] | 1.64 (1.52-1.82) | 1.69 (1.57-1.79) | 0.7777 |
| Midpiece angle [°] | 27.05 (21.86-33.85) | 19.36 (15.90-22.57) | <0.0001 |
| Acrosome-to-head ratio [%] | 53.46 (48.05-69.86) | 58.65 (50.41-70.53) | 0.0982 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



