
Submitted:
13 November 2024
Posted:
15 November 2024
You are already at the latest version
Abstract
Background: The sector-wide approach (SWAp) is an instrument of cooperation between external development partners (EDPs) and the Government of a country. Its main purpose is the coordination, alignment and harmonization of activities between EDPs and between EDPs and the respective Government by covering the entire sector with one major program.
Methods: This paper analyzes the development and achievements of the SWAp in healthcare of Bangladesh and Nepal. We scrutinized the respective documents and conducted qualitative interviews with key stakeholders of the country’s sectors. The design of the questionnaires and the analysis of the interviews was built utilizing a framework model reflecting the DAC-criteria of development cooperation and the principles of the declarations of Paris and Accra.
Findings: The SWAps in Nepal and Bangladesh started rather early and cover about 20 years of cooperation. The components and interventions of SWAps were quite relevant for the health of the population, their implementation was effective and efficient. The cohesion between partners strongly improved. However, for both countries, the interview partners do not perceive SWAps as the future of healthcare financing.
Conclusions: SWAps were an appropriate instrument of cooperation between the respective Governments and EDPs for almost two decades. However, as the share of Government budgets in the sector finance has strongly increased and the management capacity of the respective ministries has gone up, there will come a point in time where EDPs can focus more on financing and implementing innovations instead of standard care.
Keywords:
Aid effectiveness
; Bangladesh Healthcare financing
; Nepal Sector-wide approach SWAp
Disclaimer
This research was established based on two evaluations of SWAps in the health Sector of Nepal and Bangladesh for Kreditanstalt für Wiederaufbau (KfW), Germany. The paper reflects the research of the author and does not necessarily represent the position of Kreditanstalt für Wiederaufbau (KfW).
Introduction
Global development assistance for health (DAH) amounts to some 70 billion US$ (2021) p.a. and has increased strongly in the last years (11 % p.a. 2011-2019) (IHME, 2023). The strongest expansion was seen during the Covid-19 pandemic when DAH grew by 43.9% between 2019 and 2020, but even the absolute DAH in 2019 of 43 billion US$ was impressive. On a global level, DAH is almost negligible (1991: 0.3 % of total healthcare expenditure; 2019: 0.5 %), but for some countries external aid contributes more than 50 % of the total healthcare expenditure. Micronesia (73 %), South Sudan (64 %), Zimbabwe (56 %) and Mozambique (52 %) finance their healthcare systems predominantly by foreign assistance. The (sub-) continent mostly relying on external health assistance is Sub-Saharan Africa with 13.1 %. The two focus countries of this paper receive 10.5% (Nepal) and 5.4 % (Bangladesh) external help of the total current health expenditure (World Bank, 2023b). Consequently, the effectiveness and efficiency of DAH are crucial for the quality of life and survival of millions of people.
Table 1 exhibits different concepts of DAH. Traditionally, most external development partners (EDP) initiated projects of limited scope and time, e.g. establishing a hospital. Most of these projects were hardly coordinated with other projects and with healthcare activities of the respective Government. It was soon realized that many healthcare problems cannot be addressed by stand-alone projects or a discontinuous series of projects. Instead, development programs are required which run until a problem is solved or until the effort is taken over by the country’s healthcare services. Prevention (e.g. the Aids-Control-Program), training or running certain curative facilities can still be initiated and operated by EDPs, but they require more long-term coordination, in particular with the Government of the respective country.
The sector-wide approach (SWAp) coordinates all healthcare activities of the Government and EDPs as “…an approach to a locally-owned program for a coherent sector in a comprehensive and coordinated manner, moving towards the use of country systems. SWAps represent a … shift in the focus, relationship and behaviour of donors and Governments. They involve high levels of donor and country coordination for the achievement of program goals, and can be financed through parallel financing, pooled financing, general budget support, or a combination” (Vaillancourt, 2009). Ideally, all partners (i.e. Government and all EDPs) pay into one basket out of which all healthcare activities are paid for without earmarking certain donations for certain activities. Sometimes this is not possible, so that the basket-fund is supplemented by a single donor trust fund, still contributing to the sector budget but with a limitation on the application of his funds.
While the SWAp is limited to a certain sector (usually health or education), the general budget support provides funds for a Government without limitation to a certain sector. The control by the EDP is very low, i.e., funds might be used in a manner which does not reflect the value system of the EDP.
For some time, SWAps were seen as the magic bullet of DAH (Woode, Mortimer, & Sweeney, 2021). In particular, after the formulation of the Paris (2005) and Accra (2008) Declarations calling for more aid effectiveness by aligning development assistance and the ownership of programmes by the partner country (Dabelstein & Patton, 2013), SWAps were fostered and implemented in many countries in Sub-Saharan Africa and Asia. Several evaluations have shown that the alignment between EDPs and between EDPs and the country’s Government has improved while the feeling of “our program” of the respective country increased by SWAps (Ahsan et al., 2016; D. H. Peters, Paina, & Schleimann, 2013). Nevertheless, SWAps are on the decline, i.e., more EDPs return to specific programs with a lower degree of coordination and alignment. This calls for an analysis of the underlying reasons and for an assessment of the strengths and weaknesses of health SWAps.
This paper provides some insights into the development and relevance of SWAps in health care by the examples of Nepal and Bangladesh. In the next section, we will present the respective SWAps and the country setting as well as the methodology of the study. Afterwards, some statistics and the results of qualitative interviews will be described. In the discussion, we will use these results for an assessment based on the perception of the interview partners. The paper closes with some conclusions.
Methods
Setting
This paper is based on surveys in Nepal and Bangladesh. Both countries have become lower middle-income countries within the last decade. The Democratic Republic of Nepal has a GDP of 1337 US$ p.c. (current 2022) with a high growth rate (2022: 5.6 %) (World Bank, 2023b). The Human Development Index (HDI) improved from 2014 to 2021 from 0.56 to 0.60 (UNDP, 2023). A major challenge in the country is the tremendous disparity between provinces, urban and rural regions, social and ethnic groups, casts and gender concerning income, education, quality of life and health (Dhungel, 2022; Thapa, van Teijlingen, Regmi, & Heaslip, 2021; Ghimire Umesh et al., 2019).
Health is a focus area of the Government of the country. This prompted the development of several national, sector-wide programs. The first SWAp was the National Health Sector Programme I (NHSP-I, 2005-2010) with a budget of 620 million US$ (Ministry of Health, 2004) , followed by NHSP-II (2010-2016) with a budget of 1.2 billion US$ and the National Health Sector Strategy (NHSS 2016-2022) with a total of 2.662 billion US$ (Ministry of Health and Population, 2015). These national programs were a response of the Government of Nepal as well as its external development partners to the comparably poor state of health of the population. Between 2010/11 and 2019/20, the share of health expenditure covered by EDPs strongly declined from 41 to 21 %. During the Covid-19 pandemic, the respective expenditure increased again to 63 % (2020/21) and 55 % (2021/22) (UNICEF, 2018), however, this appears to be a special Corona-effect.
The situation in Bangladesh is similar although the country is slightly richer with a GPD of 2688 US$ (current p.c.) and a growth rate of 7.1 % (World Bank, 2023b) resulting in a higher HDP of 0.66 (2021) (UNDP, 2023). Bangladesh is the country with the highest population density worldwide (1313 inhabitants per sqkm) if we disregard city-states like Singapore. Urbanisation and the enormous growth of meta-cities such as Dhaka are a major challenge for the country.
Bangladesh has a rather homogenous population concerning ethnicity and religion, but disparities between poor and rich are wide and pose a challenge. The first half of the population owns only 4.8 % of all wealth and 17.1 % of all income (WID, 2023). In peripheral regions, women and children have a lower average income (Titumir, 2021), education (Chowdhury & Sarkar, 2018; Huda, Hayes, El Arifeen, & Dibley, 2018), nutrition (Akram, Sultana, Ali, Sheikh, & Sarker, 2018) and health status (Biswas, Islam, Linton, & Rawal, 2016).
The first sector-wide program was the “Health and Population Program“ (HPSP, 1998 to 2003) and had a total budget of 2.2 billion US$. This was followed by the „Health, Nutrition and Population Sector Program“ (HNPDP) which was implemented from 2003 to 2011 with a budget of 5.4 billion US$ and followed by the „Health, Population and Nutrition Sector Development Program“ (HPNSDP), which ran from 2011 to 2017 with a total budget of 7.7 billion US$. This program was succeeded by the „Health, Population and Nutrition Sector Program“ (HPNSP) from 2017 to 2022 with a total budget of 14.7 billion US$.
Figure 1 shows the timelines of the SWAps including the budget per inhabitant of the respective country under the assumption that the average population within the duration of the respective program is the correct denominator (World Bank, 2023b). It can be seen that Bangladesh started earlier with the SWAps which are stronger per capita according to the higher wealth of the nation. Otherwise, the SWAps are rather similar.
Mixed-Methods Evaluation
In this study, we used a mixed-methods approach to evaluate the SWAps implemented in Nepal and Bangladesh. We performed a secondary data analysis of documents and statistics of EDPs and the respective Governments, in particular programs, demographic and health surveys, health management information systems (HMIS), policy reports, healthcare financing strategies, as well as mid-term and final evaluations of the programs. Based on these reports we could assess the objective outcomes of the programs. However, it is impossible to evaluate whether these outcomes were a consequence of the implementation of the SWAps. Consequently, we also had to collect qualitative evidence through key informant interviews and focus group discussions with leaders of EDPs, ministries and healthcare facilities in both countries. For Nepal, we conducted 10 interviews with EDPs, 9 interviews with co-workers of the Ministry of Health (MoH) and Ministry of Finance (MoF), 24 interviews with leaders of hospitals and health centers and 12 others (e.g. warehouse managers). For Bangladesh, we interviewed 10 EDPs, 15 members of the MoH and MoF, 25 managers of healthcare facilities and three others.
In accordance with Mayring (Mayring, 2021), we developed categories based on an evaluation framework exhibited in Figure 2. The theoretical basis of this model is the work of (D’Aquino et al., 2019). In the core, we see the five dimensions of the Declaration of Paris of effective aid, namely (1) ownership of partner countries, (2) alignment of EDPs, (3) harmonization among EDPs, (4) managing for results and (5) mutual accountability. These universal principles are influenced by a frame of parameters for successful implementation for the case of a health SWAp, i.e. (a) Government commitment to the SWAp, (b) legitimacy, (c) accountability and (d) leadership of the Government, (e) focus on systems strengthening, (f) institutional development and (g) EDP commitment to the SWAp. The evaluation of these parameters is based on the DAC criteria of development cooperation, i.e. relevance, cohesion, effectiveness, efficiency, impact and sustainability (Chianca, 2008).
The DAC criteria build on each other. The interventions with a certain input (e.g. budget) are supposed to produce certain outputs that will generate outcomes. It is assumed that these outcomes will have an impact on the general objectives of the society or the healthcare system. For instance, procurement of contraceptives (input) will increase the availability of contraceptives in health centers (output) which is the prerequisite that contraceptives are used (outcome). This might reduce the total fertility rate of the population (impact). The input is a necessary but insufficient condition of the output, which is a necessary but insufficient condition of the outcome, which is a necessary but insufficient condition for the impact. The criteria of efficiency compare the input with the output, outcome and impact, while the criteria of relevance ask whether all of these achievements were not only done right but were the right things to do. Finally, sustainability analyses the long-term viability of efforts.
The interview guideline followed the structure of the DAC criteria but left sufficient space for the interviewees to stress facts we did not consider before, i.e. we conducted semi-structured interviews that were recorded by taking detailed notes on a laptop. For the official interviews with the Ministry of Health, all findings were summarized and presented at the end of the mission, resulting in signed minutes of meetings. The final analysis followed a simplified qualitative content analysis by Mayring with the principal categories (1-5) and (a-g) (Mayring, 2021).
Results
In this section, we will present the findings of the quantitative and qualitative research structured by the DAC-criteria.
Relevance
Both programs developed a comprehensive set of interventions for each SWAp to improve the healthcare situation and health status of the population. The SWAps entail a broad set of instruments (see also Attachment for Bangladesh). However, the analysis of the respective documents and the interviews clearly showed that a strong focus is on health care for the vulnerable, i.e., Mother and Child Health Care (MCH), health for the poor, people residing in peripheral regions and minorities. For both countries, it is assumed that the majority of men of the middle and upper class have comparably small problems obtaining health care while the situation for children, mothers, ethnic and religious minorities and the poor is much more difficult and requires strong support. Based on international and national health policies it can be stated that these objectives and priorities are highly relevant to the health of the whole population with a focus on the most vulnerable (Fendall, 1978; OECD, 2005; WHO, 2019).
Furthermore, all seven SWAps included a component on health systems strengthening which intends to improve health services by improving human resources, infrastructure, governance etc. Based on the WHO-building blocks of a healthcare system, several instruments were selected that could improve healthcare services in the long run (WHO, 2010).
Based on the interviews it can be stated that the commitment of the respective Governments and the EDPs was very high at least until 2020. There is a consensus on the relevance of these instruments to this day, although some interview partners have doubts about whether the SWAp is the best instrument to achieve the respective goals in the future. There is agreement that the SWAp strongly contributed to the increase in ownership of the respective Government of the program, in particular when it was combined with a basket funding mechanism. Figure 3 shows the log frame of the NHSP-II SWAp in Nepal. Based on the discussion we can state that the main advantage of the SWAp was the increase of trust amongst development partners, as well as between EDPs and the respective Government. The interviewees underlined that this trust sped up processes, reduced friction and improved the results. It also contributed to the development of ownership by the respective Government. These achievements are seen as highly relevant by all interview partners. It was stated several times that trust is the foundation of alignment, ownership and good management.
Cohesion
The set-up of a SWAp makes it likely that all interventions and processes are consistent with national and international policies of healthcare. Based on the document analyses and the interviews it can be stated that the SWAps reflect the objectives of the donors, e.g. WHO (WHO, 2014), USAID (USAID, 2021), and (World Bank, 2023a). At the same time, we compared national strategies with the SWAp, e.g. for Bangladesh the National Health Policy (Ministry of Health and Family Welfare, 2011), the Health Care Financing Strategy (2012-2032) (MOHFW, 2012), the National Social Security Strategy (Planning Commission, 2015), as well as the Bangladesh National Strategy for Maternal Health (2019-2030) (Ministry of Health and Family Welfare, 2019); for Nepal the Nepal Health Sector Strategy 2015/16–2020/21, the Reaching the Unreached Strategy, and the Social Health Insurance Act (Ministry of Finance, 2018). It can be concluded that the SWAps are in line with the country’s policies, but they excluded the demand-side perspective, i.e., all seven SWAps ignored that different concepts of insurance and risk-sharking were called for by the respective governmental strategies. In the case of Nepal, a rudimentary health insurance was developed. However, the SWAps did not include this but focused on the provision of healthcare services by strengthening healthcare facilities and programs (e.g. prevention). This might change in the future, but for the SWAps reflected on in this paper, the ignorance of the demand side, as called for in these strategies poses a challenge.
At the core of a SWAp is the sectoral dialogue between EDPs and the respective Governments which is based on a set of committees. They have different names in Nepal and Bangladesh, but they have similar functions. There is always a committee consisting of all EDPs working within the SWAp. In Nepal, it is called the Donor Forum, and in Bangladesh the Development Partner Consortium. The group also includes partners who do not contribute to the basket but align their activities with the SWAps. Furthermore, there were regular meetings between the EDPs and the respective MoH for exchange, planning, and reviewing. In Nepal these meetings were called Joint Consultative Meeting and Joint Annual Review, and in Bangladesh Local Consultative Group and Annual Program Review.
For all SWAps reflected on in this study, the World Bank was the greatest contributor. Furthermore, it also acted as administrator of the pooled fund and shouldered the fiduciary risk for most of the phases. However, this also meant that the administrative rules of the World Bank, such as procurement policies, auditing guidelines, etc. were implemented for the SWAps and were all based on World Bank standards. Some EDPs, such as AusAid and KFW, carefully expressed that these rules did not always coincide with their own legal requirements, while Government officials of the partner countries complained about the high administrative workload enforced by the World Bank.
However, there is overall agreement that the commitment of the EDPs and the respective Governments to the SWAps was high, resulting in alignment and ownership.
Effectiveness
Figure 3 shows the logic of the DAC evaluation criteria as described above. The criteria of effectiveness ask whether the interventions produced results on the outcome level as a prerequisite of the results on the impact level. All SWAps define outcome indicators which were regularly analysed in the respective committees described above. For instance, the HPNSDP consisted of 32 operational plans (OP) which were implemented by the respective directorates of the Ministry of Health with corresponding outcome indicators (OI) (MOHFW, 2017; World Bank, 2017). In total, the HPNSDP had 158 indicators for 32 operational plans in the two components. In a final report on this SWAp, the World Bank concludes that 65 % (102 indicators) were fully achieved and 20 % were partly achieved. Merely 15 % (24 indicators) were hardly or not achieved at all. It must be noted that the majority of indicators that were not achieved are in the fields of health system development, in particular personal management, development of physical infrastructure, health care financing, documentation, and data management. Another area that was not satisfactory was the reduction of spatial disparities (MOHFW, 2017; World Bank, 2017).
Table 2 shows some examples of outcome indicators of HPNSDP which can be used to assess the effectiveness of the respective SWAps. The contraceptive prevalence rate (CPR) objective was not achieved, while the other examples show success. When comparing the different outcomes of the SWAps it can be seen that the number of indicators within one country increases from SWAp to SWAp. At the same time, the strategic objective (“improve the health of the population”) and the majority of indicators in Nepal and in Bangladesh are quite similar. For instance, the NHSP-II focused on “modern contraception methods” while the HPNSDP incorporated the outcome of any contraception. Nevertheless, the utilization of contraceptives is a major objective of all SWAps.
Until the end of the NHSP-II and the HPNSDP, the financing of the SWAps was completely input-based, i.e., the respective Government disbursed funds. Afterwards, the EDPS refunded the Ministry of Health based on the presentation of invoices submitted and the indicators fulfilled. The NHSS and the HPNSP introduced an element of results-based financing with so-called „disbursement-linked indicators“ (DLI). The EDPs released funds when certain targets were met, such as a vaccination rate, successful audit, safe delivery rate, etc. (compare also Attachment for Bangladesh). As no final report on HPNSP is available yet, a concluding assessment is not feasible. However, the interview partners in both countries indicated some dissatisfaction with this approach stating that DLI define a result irrespective of whether the achievement can be influenced by the interventions. The chain of input-output-outcome-impact is not linear or deterministic. Instead, many other variables influence the results. The contribution of the interventions of a SWAp towards defined outcomes (and finally impacts) cannot be easily assessed.
Efficiency
The assessment of a sector-wide activity over many years is cumbersome. However, certain proxies can be used to evaluate whether resources have been wasted. For most SWAps reflected on in this paper, the World Bank monitored and supervised the basket as a joint donor trust fund. All payments were made based on standardized procedures, i.e., the Joint Financing Arrangement between EDP and the respective Government stipulated that payments were made based on refunds for expenditures already made by the Government on a US-$ account without interest. For these services, the World Bank received a fee from EDPs between 2.5 and 3.5 % of their contribution. The interview partners stressed that the transaction costs of independent programs would have been much higher, i.e., the SWAp increased the efficiency of development assistance. None of the interview partners voiced that the administration of SWAps would be too expensive.
Another proxy is the technical efficiency of healthcare facilities. As the SWAp includes all facilities as main recipients of funds, their efficiency is of the highest relevance for the entire sector. We visited a set of representative facilities on all levels, from village clinics to tertiary hospitals in both countries, and interviewed the respective leaders. It was found that buildings and equipment are generally used according to their intended purpose, but maintenance is poor. The budget allocated to the maintenance of equipment is too low (in all facilities visited < 1 % of the annual total budget) so several buildings are in poor condition and will face a premature end of useful life. However, once funds are accessible, civil engineers and craftsmen are available on the private market in both countries.
The budget for repairing the equipment seems to be higher, but two major challenges can be observed. Firstly, bio-technical engineers capable of maintaining and repairing more sophisticated medical equipment are rare and hardly available on the open market. As part of the NHSP-II in Nepal, respective staff was trained and employed by the Government, but this was discontinued when the NHSP-II ended. Secondly, there is hardly any preventive maintenance. There is some effort (and funding) for repair once equipment is out of order, but the prevention of damage and breakdown is a bottleneck in both countries. The interview partners unanimously confirmed that this is not only a question of funds and personnel, but also of tradition and mentality.
Based on reports of the respective ministries and EDPs, it was expected that the facilities would be grossly understaffed. Indeed, all leaders of healthcare facilities visited confirmed that they would need more staff. However, we calculated the number of patient contacts and the occupancy per professional and found that quite a number of institutions were sufficiently staffed. Some interview partners responded to this figure by pointing out that this is a recent development, i.e., the situation has improved. There is, however, a strong disparity between urban and rural, or central and peripheral regions. Remote hospitals, for instance, have major problems in attracting doctors, while institutions in cities do not face similar challenges. One reason that was frequently given to us by the facility leadership is the fact that doctors in state healthcare facilities can only find a second job with higher income (“moonlighting”) in the city, while doctors in rural facilities can hardly survive with their government income.
We conducted a spot survey of patients in three small hospitals in Bangladesh, which found that 90 % of interview partners felt that the facility had adequate staff to support them while only 60 % stated that the facility had sufficient drugs and examination facilities. Drug shortages in particular are an issue. While the availability of drugs, medical materials, and vaccines has generally improved, stockouts even of essential drugs still exist, particularly in primary care facilities in both countries.
Management training and capacity are a bottleneck in many healthcare institutions, particularly in rural areas. Management is still entirely in the hands of the medical doctors. In Nepal, a new cadre of administrators is being trained, but it is still too early to assess whether this will have an impact on the efficiency of the facilities.
In both countries, we found that the mobility of the population has increased over the last 20 years. Roads are getting better, and the availability of cheap transport (bikes, motorbikes, Tuktuk) enables patients to commute to hospitals in cities bypassing one or more health centers. In principle, this is a favourable development as the quality of services in urban hospitals is usually higher than in health centers. For instance, it allows mothers to decide to deliver in a hospital with an operating theatre rather than in small health centers without any emergency support. However, the SWAps invested a considerable amount in the development of small healthcare facilities close to the people in particular in rural areas. The number of curative services provided by these small facilities is declining. We found some health centers performed fewer than 50 deliveries per year which is insufficient to ensure adequate quality. Consequently, some of the facilities which were established with funds from SWAps will have to be closed/shut-down.
At the same time, the number of patients with chronic-degenerative diseases (e.g. diabetes, hypertensions …) is increasing. They need supervision and medication for which they do not have to travel to a larger city. The transformation of rural health centers into support centers for chronically-ill patients has not started and will be the content/subject matter of future programs. Currently, the interview partners agreed that some of the funds that were invested primarily in rural delivery facilities could have been invested more efficiently in more centralized services. However, there was also consensus that the situation in different regions of the countries might differ, e.g. public transport is less of a challenge in Southern Nepal, whereas the situation in the North with high mountains and deep valleys needs to be assessed differently.
Impact
The overarching developmental objective (impact) of all SWAps considered in this paper is the improvement of the health of the entire population. Figure 4 show some health indicators for the example of Nepal. For both countries, the trends are very positive. In particular, the mortality rates (infant, <5-, neonatal, maternal mortality rate) declined tremendously from the beginning of SWAps until today. These are „hard“ indicators measuring different aspects of the total mortality with high relevance for the life and quality of life of the population. Bangladesh and Nepal have made extraordinary progress regarding these indicators which are also recognized, e.g.: „Bangladesh was selected as an Exemplar due to rapid reductions in neonatal and maternal mortality rates. Bangladesh had the fastest decline in neonatal mortality of any country in the South Asia region, and the speed of its decline in maternal mortality is comparable to other neighbouring Exemplar countries, such as India and Nepal” (Exemplars, 2024).
Another highly relevant indicator is the total fertility rate. Both countries are densely populated with Bangladesh having the highest population density worldwide (without city states). However, the total fertility rate has neared the reproductive value. While the population is aging, it will still grow, but the tremendous population growth of the past with huge challenges for the social system has come to an end.
In Bangladesh, nutrition was a major issue so the reduction of different forms of malnutrition (stunting, wasting, and underweight) were included as impact indicators. Generally, these components of the SWAps were not as successful as other interventions. The interview partners assumed that nutrition is very complex and involves many traditional believes and cultural habits.
For both countries, the interview partners concluded that the commitment and leadership of the Government was high resulting in ownership and alignment. At the same time, it was realized that a sector-wide approach is an instrument that is tailored to the coordination between the central Government and EDPs. During the last SWAp, Nepal has gone through a federalisation and decentralisation process resulting in much higher autonomy of regions. Consequently, the coordination and alignment between the central Government, EDPs, and several regional Governments has become more difficult. Whether this had an impact on the respective indicators cannot be analysed. Some interview partners (from the central level) had the “feeling” but this could not be verified by the data.
The greatest problems of the healthcare system of Bangladesh are still regional and social disparities. Location (urban/rural), region (divisions), education and wealth/income determine the most relevant social and health indicators. In principle, the situation of the urban population (in particular in Dhaka and Khulna) is better than in rural and remote areas, as/while the situation of the poor and people with lower education is challenging. This is not surprising, but the range between the quintiles is still considerably high. For instance, the share of safe deliveries of the richest 20 % of the population is more than 90 %, and of the poorest 20 % less than 50 % (Ministry of Health and Family Welfare, 2023). Similar results can be observed for Nepal, but here the impact indicators differ strongly between ethnic groups, religions and castes. For instance, the rate of teenage pregnancies of Muslims is much higher than that of Brahmin/Chhetri (15.5 % vs. 5.7 %). The lowest caste (Dalits) has the highest total fertility rates, and the Dalits in Terai/Madhesi have a < 5 mortality rate which is 2-3 higher than the country average. In the same region, malnutrition is severe for this group where low caste, poverty, poor education and remote location frequently coincide (Ministry of Health and Population, 2022).
At the same time, the situation has improved. For instance, the range of the total fertility rate in rural and urban regions was 0.5 in 2011, and in 2022 only 0.3. Between divisions, the range was 1.2 and decreased to 0.7. The respective figures for the wealth quintiles were 1.2 and 0.8 (Ministry of Health and Family Welfare, 2013, 2023). Consequently, we can state that the situation has improved but is still challenging. Umesh et al. found similar results for Nepal where the statistics remain challenging for the above described population groups (G Umesh et al., 2019).
Sustainability
The interview partners agreed that the development of the healthcare sectors and the capacity of the respective Governments to sustain the efforts of improving the health situation of the population have developed positively. The healthcare budgets in absolute and relative terms increased during the period of the SWAps as well as the number of professionals in ministries and healthcare facilities. The phases of SWAps built on each other without interruption, in two cases the SWAps were prolonged in order to allow a smooth flow. The harmonization and coordination mechanisms continued and were well utilized. At the same time, the Governments passed a number of relevant strategies and policies during the period of SWAps, in particular the health financing strategies.
However, the EDPs and Government officials stated several times that SWAps will face/phase out in the next few years, i.e., the current SWAp in Nepal and the next SWAp in Bangladesh will be the last SWAps. Cooperation and coordination are supposed to continue, but the components of the existing SWAps will be taken over completely by the national Governments while EDPs will focus on new, innovative challenges, such as climate change and health. It seems that the era of SWAps will come to an end soon in these countries.
We asked the interview partners for reasons. Firstly, it was stated several times, that it is a positive development that SWAps seem to be less necessary than before. The national budgets have grown significantly so that the EDPs’ contribution is less relevant. Secondly, both countries have improved their managerial capacities so that they need less technical assistance. Thirdly, both countries have now become lower-middle income countries. This entails that external support is not given any more as a grant but as a loan which is rather unattractive in the healthcare field. However, there is also some disappointment with the SWAps. In both countries, it seems that the cooperation worked best in the years from 2012 to 2018. In the first phase of the SWAps, it took some effort to make the processes work and get used to the cooperation. Afterwards, everybody seemed to be satisfied with the SWAp. One interview partner called it the “golden age of cooperation”. However, this period came to an end with major changes in personnel with EDPs and the respective ministries.
The interview partners could not state why – in both countries – quite some key personnel moved in 2019. For the ministries and EDPs, shifting of positions is quite common. But it seems that the cooperation and trust was discontinued in this year. There would have been a great chance to build- up this trust again based on the existing formats of exchange and alignment, but then Corona made an end to all efforts. Both countries suffered severely under the pandemic with long periods of lock-down and home-office. New staff came, but they did not meet in person for a long time. When physical meetings were feasible again, it was difficult to build-up the commitment and unity that had been there before. The interview partners included officials who had been in the sector of the respective country for a long time in different positions. Several of them stated that this feeling of “my SWAp” never came back after the Corona pandemic.
Discussion
State-of-the-Art
Based on the document analyses and the interviews it can be stated that the SWAps reflected on in this paper follow the standards given by international development cooperation (Cassels, 1997; UNFPA, 2005). Consequently, the set-ups of the SWAps in both countries are quite similar although components and foci differ. At the core of all SWAps in Bangladesh and Nepal is the collaboration between EDPs as well as between EDPs and the respective Governments. This leads to alignment of activities and policies as well as ownership of the Governments as it was described for other SWAp in a number of countries (D. H. Peters et al., 2013; Rabinowitz, 2015; Woode et al., 2021).
The basket funding is at the core of the SWAp. Certainly, some partners might form “single donor trust funds” with ear-marked contributions to the SWAp, but the basket is the main instrument of coordination, harmonization and alignment (Ahsan et al., 2016; Woode et al., 2021).
As early as in the year 2009, the World Bank published an evaluation of health SWAps in Bangladesh, Ghana, Kirgizstan, Malawi, Nepal, and Tanzania (Vaillancourt, 2009). It showed that the SWAps in Nepal and Bangladesh were quite successful in the fields of harmonization and alignment while monitoring, evaluation, and „stewardship“ (i.e. efficiency) would require some more effort. This result was confirmed by our interviews almost 15 years later. The cohesion between partners was generally seen as a major success for most of the SWAps, while efficiency remains a challenge.
The Ministry of Finance of Nepal analyzed the SWAps in education and healthcare in 2018 (Ministry of Finance, 2018). It was stated/reported that the International Economic Cooperation Coordination Division (IECCD) in the Ministry of Finance in Nepal speared the coordination and cooperation – a statement that was not altogether confirmed by our interview partners who put more stress on the efforts of the Ministry of Health. However, it was important that Nepal had a “Government of Nepal’s Development Cooperation Policy”, which “sets out its preferences in terms of aid modalities and encourages Development Partners to harmonize their support in a given sector by setting up pooled funds and providing their assistance through Program-Based Approaches or Sector-wide Approaches (SWAp)”. In total, about half of official development assistance ODA (44-56 % 2014/15- 2015/16) was channeled through a SWAp, i.e., in Nepal is „still room for improvement as around 50% aid is still delivered outside SWAp module. Similarly, other health providers such as those outside the system are also not recorded here which means a sizable amount of investment is still done outside the SWAp framework in Nepal.” Scientific evidence that is not published by the Government of Nepal or an EDP is rare. Interchangeably with Nepal, Bangladesh has set-up an “Economics Relations Division” within the Ministry of Finance to coordinate development cooperation activities. Based on a “National Policy on Development Cooperation” this department intended “to ensure that foreign assistance follows national development priorities as determined by national development plans and strategies and supports the country’s development efforts to bring benefits to the lives of the people”. The term “SWAp” is not mentioned in this policy, but it is obvious that the SWAp is fully in line with this target. The interview partners in Bangladesh mentioned the role of the Ministry of Finance more frequently than in Nepal, but this might also be coincidental.
Summarizing we can state that according to the literature and the perception of the interview partners, the health SWAps in both countries worked quite well and achieved their objectives. Nevertheless, there are some differences between the countries. For both countries, mother and child healthcare is pivotal, but Nepal puts even more emphasis on it than Bangladesh. Nepal had developed the “Aama Surakshya Programme” (Aama) to improve the health of pregnant women and mothers. It includes free institutional delivery, payment of transport costs, and an incentive to go for four antenatal care visits. As early as 2005, the Maternity Incentive Scheme (MIS) was initiated, and in 2009 maternity fees were abolished nationwide. In 2012, MIS merged with the programme for four ANC visits to become the Aama programme. It was an essential component of the NHSP-I, the NHSP-II and the NHSS (Toolan et al., 2022; Upreti et al., 2012). In Bangladesh, MCH is highly relevant as well, but there is no specific sub-program with such a focus within the SWAps.
At the same time, the population and landscape of Bangladesh are more homogenous than in Nepal where health and demographic indicators differ more significantly between regions, castes and ethnic groups. About 82 % of the population in Nepal are Hindu, 9% are Buddhist and 4 % Muslims, while 91 % of the population in Bangladesh are Muslim and 8 % Hindu. Generally, the health and demographic indicators of Muslims in Nepal are significantly worse than those of Hindus or Buddhists (Ministry of Health and Population, 2022). However, the population group with the worst problems are the Dalits, as the lowest group in the Hindu caste system, with above-average reproduction rate (for Dalits and Muslims), contraceptives (below-average frequency of use amongst Newars, Terai/Madhesi Brahmin/Chhetri and Hill Brahmins; the Dalit caste shows the highest number of children per woman and the lowest incomes), vaccinations (vaccination rates and drop-out rates differ significantly between regions), obstetrics (comparable results to those with the use of contraceptives), child mortality (2–3 times higher than the national average among Terai/Madhesi Dalits) and undernutrition (especially strong among Terai/Madhesi Dalit and Terai/Madhesi) (G Umesh et al., 2019). In particular, the Annual Report 2020/21 (Department of Health Services, 2021) depicts on numerous maps (e.g. vaccination rate), how severe the disparity still is, which is expressed not only by the geographical location with regard to the centre or periphery, but above all by belonging to a certain caste. Many of them live in Madhesi in the south-west of Nepal with poor education, early pregnancies, low contraceptive rates, high mortality etc. These differences in castes and religious groups are much lower in Bangladesh so they did not have to be addressed by the SWAps. However, spatial disparities between urban and rural places as well as between provinces exist in both countries and were addressed by the respective instruments of their SWAps.
Advantages and Disadvantages of SWAps
Based on the analysis and interviews we can underline a number of advantages of SWAps. Firstly, a major advantage is (full agreement of all interview partners) the coordination, harmonization and alignment of partners and activities. In this way, dual/duplicate activities as well as underserved areas can be avoided. Firstly, this results in higher efficiency as no efforts of different partners are wasted on the same or competing interventions. Secondly, this leads to a higher ownership of the respective Government. The respective ministries, predominantly the Ministry of Health and of Finance, sit in the driver’s chair/have full authority from the beginning, they have the final say and they are responsible for the results. This significantly increases the chance of identification with the program and its components. And it becomes obvious that development aid is only a short- and medium-term solution. In the long run, the Government of the partner country will be fully self-sustaining and provide healthcare services for its people with its own funds and managed by its own professionals.
Thirdly, the SWAp safeguards that the priority of the country is followed, not that of the external development partners. There are certain “fashions” even in the development field, i.e., priorities of the external partners can influence the healthcare situation in the partner country. A SWAp safeguards that the healthcare activities are aligned with national policies and reflect the value system of the country. Needless to say, this is not always the case, but the interview partners saw this as a major advantage of SWAps at least increasing the likelihood of following national priorities.
Fourthly, a SWAp is a learning system. In Nepal and Bangladesh, the smooth flow of consecutive SWAps included a learning experience in the sense that components that were missing in a SWAp were frequently taken-up by the consecutive SWAp. For instance, emergency care and telemedicine were not included in the NHSP-II but became components of the NHSS. Similarly, the demand-side components (health insurance) were completely ignored during the HPNSDP but included at least rudimentary in the HPNSP. During the annual review meetings in both countries, achievements, as well as gaps, were discussed so that the new programs could be tailored to the perceived needs of the population.
Finally, the interview partners stated that a major advantage of the SWAp was the development of trust between the partners. This trust resulted in a smooth flow of the program, but it also strongly contributed towards the coordination between EDPs and the respective Governments during crises. Nepal experienced two major external shocks during the period of the SWAps, i.e. the major earthquakes of 25.02. and 12.05.2015 as well as the Corona crisis in 2020-2022. The interview partners indicated that the Government responded in time while extensively involving the EDPs with financial and technical advice. They stated that the coordination and channeling of aid during these crises worked well because it could build on long-term trust and well-established communication platforms.
In Bangladesh, some 850,000 Rohingya came to Bangladesh as refugees in 2017 requiring extensive support and care (Joarder, Sutradhar, Hasan, & Bulbul, 2020). The respective international support was strongly backed by existing platforms and channels based on the trust between the EDPs and the Government of Bangladesh. Furthermore, Bangladesh was severely hit by Corona (Al-Zaman, 2020) and in particular the delta wave in 2021 (Devnath, Hossain, Emran, & Mitra, 2022). While there was strong agreement that the trust built up during the SWAp was instrumental during the Rohingya crisis, the interview partners did not agree on whether this was also relevant during the Corona pandemic. However, all partners agreed that trust was built more on the integrity and professionality of individuals than on systems, i.e., once the key persons left the country or their job, trust had to be re-built. This is also in line with other authors, i.e. “…there are many who believe that the success in developing the SWAps has had more to do with the strength of the partnerships and level of trust that have been formed than the technical soundness of the new policies and programs” (D. Peters & Chao, 1998), and the WHO concludes that “formal agreements are not an effective substitute for good working relationships, mutual trust, and strong Government ownership” (Foster, Brown, Conway, & Organization, 2000). However, some analyses do not even mention the word “trust”, e.g. (D’Aquino et al., 2019).
The experiences from Nepal and Bangladesh reflected in the interviews also underlined some disadvantages of the SWAps. Firstly, “sector-wide” does not always involve the entire sector, i.e., EDPs and Governments still exclude certain elements (Whyle & Olivier, 2016). In Bangladesh, the operating budget of the healthcare facilities was included in the SWAp, but not in Nepal, i.e., the SWAps in Nepal were “development SWAps”, not “operating SWAps”. Furthermore, some EDPs still do not cooperate with the SWAp. This is frequently the case with NGOs which do not always align their activities with the Government system. But also big/major players, such as USAID or the Global Fund have their own rules, not allowing a basket contribution or a global contribution to the healthcare budget. The main reasons for this policy are either that their funds are earmarked for a very specific purpose (such as from the Global Fund) or that the respective Government of the EDP does not trust the national monitoring system and consequently does not allow any channelling of funds outside its own audit system (e.g. USAID). This finding was also reported by other SWAps, e.g. “notable donors including US Government and the Global Fund did not participate in the SWAp, and increased vertical funding weakened the SWAp in favour of non-governmental organizations (NGOs)” (Pfeiffer et al., 2017).
Secondly, SWAps have a tendency to postpone or hinder innovations in healthcare. As the SWAp takes 2-3 years to develop and runs for at least 4 years, the technology of the SWAp is up to 7 years old. The NHSP-II, for instance, did not include any interventions against chronic-degenerative diseases although the country entered the third phase of the epidemiological transition with a dominance of chronic-degenerative disease even before the NHSP-II started, i.e., the number of death cases due to chronic-degenerative diseases dominated death cases due to infectious diseases in 2003. For loss of quality of life (DALYs) the respective break-even was in the year 2009 (Ministry of Health and Population, Nepal Health Research Council, Institute for Health Metrics and Evaluation, & UKaid, 2021). In 2019 (latest figures), 71 % of death cases were due to NCDs (non-communicable diseases), 21 % due to CMNN (communicable, maternal, neonatal and nutritional diseases) and 8 % due to accidents (Ministry of Health and Population et al., 2021). However, the NHSP-II focussed only on CMNNs.
Generally, it can be stated that innovations, such as NCDs, telemedicine, insurance, emergency care etc., take quite a long time to find their way in the SWAp. There is little evidence and our interview partners did not contribute to this debate, but based on general innovation theory (Howell & Higgins, 1990) it might be guessed that the disadvantage of delayed inclusion of an innovation might be compensated at least partly by a greater adoption speed once the innovation has entered the SWAp as it might be implemented throughout the country in the entire healthcare sector. But this would require more research.
Thirdly, from the perspective of the EDPs, a SWAp has the disadvantage that its monitoring and evaluation are crucial but difficult. An individual project or program is usually monitored and audited by the standards of the respective donor and his Government, e.g., a project of the German Financing Cooperation implemented by Kreditanstalt für Wiederaufbau (KfW, Germany) follows German regulations of procurement, accounting, and auditing. A SWAp consortium has to agree on one specific standard. This is frequently the standard of the receiving country or the EDP with the highest budget. In the case of the SWAps of Nepal and Bangladesh, the World Bank was the strongest contributor to the basket and it set the rules and shouldered the fiduciary risk. Consequently, other EDPs had to follow World Bank regulations even if they were not identical with their own approach. Irrespective of whether the entire financial management, evaluation, and auditing are done by the partner Government or by one EDP, a SWAp always means that most EDPs give up some degree of control. Without trust, this is not possible.
Fourthly, providing funds via a SWAp does not guarantee that these funds can be used efficiently by the partner. In some cases, the ability to absorb and use these funds can be so poor that a major share of the SWAp-funds remains unused (Whyle & Olivier, 2016). The “absorption capacity” of the Ministry of Health was analysed by the Government of Nepal. It was as low as 76 % in the financial year 2010/11 (Ministry of health and Population, 2017), but it increased up to 84 % in 2018/19 (latest figures). The interview partners from Nepal stated that the SWAps were generally somewhat over-budgeted, so that the lack of absorption may not necessarily be the result of weakness in implementation management, but rather of caution. Consequently, from the very beginning, it was infeasible to spend the entire fund (Ministry of Health and Population, 2021).
The absorption rate of the SWAps in Bangladesh seems to be higher than in Nepal, but we only have data for HPNSDP showing that on average the expenditure was some 93 % of the original budget. However, the interview partners underlined that there was a strong delay within a financial year, i.e., delayed activities and expenditures at the beginning of the year were followed by a strong increase in procurements and payments towards the end of the year. More important is the fact that the absorption rate differs between the operational plans. While the rate was high for the control of infectious disease, physical facilities development and pre-service-education (96 %, 97 %, 97 %), it was poor for human resource management, management information systems, and drug administration and management (58 %, 68 %, 58 %). Most alarming is the fact that less than half (48 %) of the funds for health economics and financing were spent as expected (MOHFW, 2017). This reflects the impression of the interview partners that the rudimentary attempt to initiate a health insurance scheme for the poor in Tangail district (SSK, Shasthyo Shurokhsha Karmasuchi) (m4H, 2023) was never fully integrated into the SWAp. Similar experiences of low absorption rates within SWAps were described elsewhere (Ahsan et al., 2016; Chansa, Sundewall, McIntyre, Tomson, & Forsberg, 2008), partly due to the low administrative capacity of the Ministries (Whyle & Olivier, 2016).
“Best” time for SWAps
Based on these pros and cons of the SWAp one might ask whether there is a “best” time for a SWAp. During our discussions it was stressed by a number of interview partners that there had been a “golden age” of SWAps, lasting roughly from 2012 to 2018. In both countries, it is clear that there will be no more SWAps in the long run. There seems to be general agreement that this will be the last phase of health SWAps. It is already difficult to find more pooling partners. The majority of EDPs would like to stay on the coordination mechanism of SWAp, but channel their own funds into specific programmes outside the basket. In Nepal, the new SWAp (National Health Sector Support Program, NHSSP) could attract only FCDO (Foreign, Commonwealth & Development Office, UK) and GAVI (The Vaccine Alliance) as pooling partners, in Bangladesh the process is still ongoing and cumbersome. The interview partners from the Government stressed that they do not see a need for a SWAp anymore as their own contribution is dominant now. The EDPs stress the fact that they would like to focus more on innovations which are not so much the focus of the partner Government. For instance, climate change and health seem to have a higher priority among EDPs, while this is not on top of the priority list of the partner countries.
Figure 5 sketches the capacity of partners as well as the advantage of SWAps. In the beginning, the financial and managerial capacity of the respective Government are both low. They would not be able to install and maintain a SWAp within their system. In comparison to the local contribution, the financial and technical assistance of EDPs is quite high. Consequently, a SWAp is infeasible. However, with the growing financial and managerial capacity of the Government, SWAps become possible. For the time being, external partners still prefer independent programs because the efforts of monitoring the SWAp seem to be too high. With a growing capacity, however, SWAps become efficient and feasible and should be fostered.
Over the years, the government’s managerial capacity grows considerably, so that external technical support will generally no longer be needed. At the same time, the share of the Government budget in the entire health sector increases, while the contribution of the EDPs becomes more and more irrelevant. Finally, the SWAp entails a lot of coordination effort without stronger relevance for the sector so the SWAp becomes inefficient and should be given-up. EDPs can still support programs or even projects that are generally aligned but without the strong effort of coordinating every step. This last phase is the step towards full independence.
Bangladesh gives a good example of this development. The country started the first SWAp in 1998 with 62 % Government contribution. As stated before, it was a comprehensive SWAp including the operation costs of running healthcare facilities. In HNPSP (2003-2011), the Government contribution increased to 67 %, in HPNSDP to 76 % (2011-2016) and in HPNSP to 84 % (2017-2014). The successor program which is supposed to be the last SWAp will have even a higher Government contribution. Likewise, the Government’s contribution towards the healthcare budget in Nepal increased von 58 % (2010/11) to 79 % (2018/19). As Nepal did not include the operational budget in the SWAp, it is appropriate to analyze this statistic for the entire healthcare budget (Ministry of health and Population, 2017; UNICEF, 2018). However, the years 2019/20 and 2020/21 were exceptional due to a strong flow of financial assistance because of the Corona crisis.
At the same time, the interview partners (with very few exemptions) agreed that the managerial capacity of the Governments of Nepal and Bangladesh strongly improved. The public administration is capable of managing its own funds without (major) technical support from EDPs.
This analysis demonstrates that it was the right decision to initiate SWAps in both countries. They helped to improve the health situation and to build-up the managerial capacity of the respective ministries. However, this does not mean that SWAps have to be prolonged indefinitely. It is likely that SWAps will come to an end. This will not mean the end of cooperation, but external aid will be focused more on very specific issues, in particular innovations.
Limitations
This analysis must be seen in the light of major limitations. Firstly, it is based on documents and interviews in two countries. Thus, further research would have to prove whether these findings are representative of other countries as well. It could be that the era of SWAps is still highly relevant for Sub-Saharan African countries while it approaches its end in South Asia. But this is beyond the scope of this paper. Secondly, the majority of conclusions are based on interviews with officers of EDPs, ministries, and health care facilities. We tried our best to select these interview partners thoroughly, but we cannot be absolutely sure that our interviews are not biased. In a number of cases, interview partners and facilities to be visited were recommended by Government officials. It is likely that these were not the most critical stakeholders.
Finally, Corona had a strong impact on the healthcare sector in both countries. The external funding strongly increased. At the same time, the prolonged lock-downs and era of home-office paired with major changes of personnel at EDPs and even ministries resulted in a loss of social capital. Before the pandemic, partners knew each other quite well. Afterwards, trust had to be rebuilt. In the case of Bangladesh this seemed to work rather well, while in the case of Nepal the collaboration of the year 2023 (when we visited the country and made the interviews) was still perceived as worse than before the pandemic, by those few who had been on the job for several years. Whether this social capital can be built-up again, cannot be assessed today and calls for exploration in future research/additional research.
Conclusions
The SWAps in Bangladesh and Nepal addressed the right health challenges and improved the cohesion between EDPs and between EDPs and the respective Governments. They were effective and efficient and had an impact on the health situation of the countries. However, their sustainability can be challenged due to factors mainly outside the SWAp, such as the Corona pandemic. Generally, the majority of interview partners conclude that coordination, alignment, and harmonization improved during the era of SWAps. However, it seems that the next SWAps will be the last ones in the healthcare field. The respective Governments do not need close coordination with EDPs anymore because they are almost self-governing and self-financing. One alternative would be the general budget support beyond the healthcare sector, but many development partners fear the risk of limited control over the funds provided. An alternative is the shift towards assistance in narrow and specialized programs of innovations, including policy-based financing mechanism to overcome structural weaknesses of the partner countries. The future role of EDPs might not be so much the financial and technical assistance for standard programs, but the development of innovation seedlings with the potential to be included in the health sector under the control of the respective Government.
References
- Ahsan, K. Z., Streatfield, P. K., Ijdi, R.-E.-., Escudero, G. M., Khan, A. W., & Reza, M. (2016). Fifteen years of sector-wide approach (SWAp) in Bangladesh health sector: an assessment of progress. Health Policy Plan, 31(5), 612-623. [CrossRef]
- Akram, R., Sultana, M., Ali, N., Sheikh, N., & Sarker, A. R. (2018). Prevalence and determinants of stunting among preschool children and its urban–rural disparities in Bangladesh. Food Nutr Bull, 39(4), 521-535. [CrossRef]
- Al-Zaman, M. S. (2020). Healthcare crisis in Bangladesh during the COVID-19 pandemic. The American Journal of Tropical Medicine and Hygiene, 103(4), 1357.
- Biswas, T., Islam, M. S., Linton, N., & Rawal, L. B. (2016). Socio-economic inequality of chronic non-communicable diseases in Bangladesh. PLoS One, 11(11), e0167140. [CrossRef]
- Cassels, A. (1997). A guide to sector-wide approaches for health development: concepts, issues and working arrangements. Geneva: World Health Organisation.
- Chansa, C., Sundewall, J., McIntyre, D., Tomson, G., & Forsberg, B. C. (2008). Exploring SWAp's contribution to the efficient allocation and use of resources in the health sector in Zambia. Health Policy Plan, 23(4), 244-251.
- Chianca, T. (2008). The OECD/DAC criteria for international development evaluations: An assessment and ideas for improvement. Journal of Multidisciplinary Evaluation, 5(9), 41-51. [CrossRef]
- Chowdhury, R., & Sarkar, M. (2018). Education in Bangladesh: Changing contexts and emerging realities. Engaging in educational research: Revisiting policy and practice in Bangladesh, 1-18.
- D’Aquino, L., Pyone, T., Nigussie, A., Salama, P., Gwinji, G., & van den Broek, N. (2019). Introducing a sector-wide pooled fund in a fragile context: mixed-methods evaluation of the health transition fund in Zimbabwe. BMJ Open, 9(6), e024516. [CrossRef]
- Dabelstein, N., & Patton, M. Q. (2013). The Paris declaration on aid effectiveness: History and significance. Canadian Journal of Program Evaluation, 27(3), 19-36. [CrossRef]
- Department of Health Services. (2021). Annual Report 2019/20. Kathmandu: Government of Nepal Retrieved from https://dohs.gov.np/category/annual-report/.
- Devnath, P., Hossain, M. J., Emran, T. B., & Mitra, S. (2022). Massive third-wave COVID-19 outbreak in Bangladesh: A co-epidemic of dengue might worsen the situation (Vol. 17, pp. 347-350): Future Medicine.
- Dhungel, K. R. (2022). Income Inequality in Nepal. Law and Economy, 1(3), 51-54. [CrossRef]
- Exemplars. (2024). Why is Bangladesh an Exemplar? Retrieved from https://www.exemplars.health/topics/neonatal-and-maternal-mortality/bangladesh/why-is-bangladesh-an-exemplar.
- Fendall, N. R. (1978). Declaration of Alma-Ata. Lancet, 2(8103), 1308. [CrossRef]
- Foster, M., Brown, A., Conway, T., & Organization, W. H. (2000). Sector-wide approaches for health development: a review of experience.
- Howell, J. M., & Higgins, C. A. (1990). Champions of technological innovation. Administrative Science Quarterly, 317-341. [CrossRef]
- Huda, T. M., Hayes, A., El Arifeen, S., & Dibley, M. J. (2018). Social determinants of inequalities in child undernutrition in Bangladesh: A decomposition analysis. Matern Child Nutr, 14(1), e12440. [CrossRef]
- IHME. (2023). Financing Global Health 2021: Global Health Priorities in a Time of Change. Seattle, WA: Institute for Health Metrics and Evaluation, University of Washington.
- Joarder, T., Sutradhar, I., Hasan, M. I., & Bulbul, M. M. I. (2020). A record review on the health status of Rohingya refugees in Bangladesh. Cureus, 12(8).
- m4H. (2023). SSK (Shasthyo Surokhsha Karmasuchi) Social Health Protection Scheme, Bangladesh. Retrieved from https://m4health.pro/ssk-shasthyo-surokhsha-karmasuchi-social-health-protection-scheme-bangladesh/.
- Mayring, P. (2021). Qualitative Content Analysis: A Step-by-Step Guide. Los Angeles et al.: SAGE.
- Ministry of Finance. (2018). An Assessment of Sector Wide Approach (SWAp) in Health and Education Sectors of Nepal. Kathmandu: Government of Nepal.
- Ministry of Health. (2004). Nepal Health Sector Programme Implementation Plan 2004-2009. Kathmandu: Government of Nepal.
- Ministry of Health and Family Welfare. (2011). Health Policy 2011. Dhaka: Government of Bangladesh.
- Ministry of Health and Family Welfare. (2013). Bangladesh Demographic and Health Survey 2011. Key Indicators Report. Dhaka: Government of Bangladesh.
- Ministry of Health and Family Welfare. (2019). Bangladesh National Strategy for Material Health (2019-2030). Dhaka: Government of Bangladesh.
- Ministry of Health and Family Welfare. (2023). Bangladesh Demographic and Health Survey 2022. Key Indicators Report. Dhaka: Government of Bangladesh.
- Ministry of Health and Population. (2015). National Health Sector Strategy 2015-2020. Kathmandu: Government of Nepal.
- Ministry of health and Population. (2017). Annual Progress Report of Health Sector Fiscal Year 2015/16. Kathmandu: Government of Nepal.
- Ministry of Health and Population. (2021). Progress of the Health and Population Sector, 2020/21. Kathmandu: Government of Nepal.
- Ministry of Health and Population. (2022). Demographic and Health Survey 2022. Key Indicators Report. Kathmandu: Nepal.
- Ministry of Health and Population, Nepal Health Research Council, Institute for Health Metrics and Evaluation, & UKaid. (2021). Nepal Burden of Disease 2019. A Country Report based on the 2019 Global Burden of Disease study. Kathmandu: Government of Nepal.
- MOHFW. (2012). Expanding Social Protection for Health Towards Universal Coverage – Health Financing Strategy 2012-2032. Dhaka: Government of the People's Republic of Bangladesh.
- MOHFW. (2017). Report on End-Line Evaluation of Health, Population and Nutrition Sector Development Program (HPNSDP) July 2011- December 2016. Dhaka: Government of Bangladesh.
- Natuzzi, E. S., & Novotny, T. (2014). Sector wide approaches in health care: do they work? Global Health Governance, 8(1).
- OECD, D. (2005). Paris declaration on aid effectiveness. http://www1. worldbank. org/harmonization/Paris/FINALPARISDECLARATION. pdf.
- Peters, D., & Chao, S. (1998). The sector-wide approach in health: What is it? Where is it leading? Int J Health Plann Manage, 13(2), 177-190.
- Peters, D. H., Paina, L., & Schleimann, F. (2013). Sector-wide approaches (SWAps) in health: what have we learned? Health Policy Plan, 28(8), 884-890.
- Pfeiffer, J., Gimbel, S., Chilundo, B., Gloyd, S., Chapman, R., & Sherr, K. (2017). Austerity and the “sector-wide approach” to health: The Mozambique experience. Soc Sci Med [Med Econ], 187, 208-216.
- Planning Commission. (2015). National Social Security Strategy. Dhaka: Government of Bangladesh.
- Rabinowitz, G. (2015). The Power of Owernship. Literature Review on aid ownership and participation. London: Overseas Development Institute report.
- Thapa, R., van Teijlingen, E., Regmi, P. R., & Heaslip, V. (2021). Caste exclusion and health discrimination in South Asia: A systematic review. Asia Pacific Journal of Public Health, 33(8), 828-838. [CrossRef]
- Titumir, R. A. M. (2021). Poverty and inequality in Bangladesh. In R. A. M. Titumir (Ed.), Numbers and narratives in Bangladesh's economic development (pp. 177-225). Singapore: Palgrave Macmillan.
- Toolan, M., Barnard, K., Lynch, M., Maharjan, N., Thapa, M., Rai, N., . . . Burden, C. (2022). A systematic review and narrative synthesis of antenatal interventions to improve maternal and neonatal health in Nepal. AJOG Global Reports, 2(1), 100019. [CrossRef]
- Umesh, G., Jyoti, M., Arun, G., Sabita, T., Yogendra, P., & Tesfayi, G. (2019). Inequalities in health outcomes and access to services by caste/ethnicity, province, and wealth quintile in Nepal. . DHS Further Analysis Report, 117.
- Umesh, G., Jyoti, M., Arun, G., Sabita, T., Yogendra, P., & Tesfayi, G. (2019). Inequalities in health outcomes and access to services by caste/ethnicity, province, and wealth quintile in Nepal. DHS Further Analysis Report(117).
- UNDP. (2023). Human Development Index. Retrieved from https://hdr.undp.org/data-center/human-development-index#/indicies/HDI.
- UNFPA. (2005). Sector Wide Approaches: A Resource Document for UNFPA Staff. United Nations Population Fund. New York.
- UNICEF. (2018). Health Expenditure Brief. Kathmandu: UNICEF Nepal.
- Upreti, S., Baral, S., Tiwari, S., Elsey, H., Aryal, S., Tandan, M., . . . Lievens, T. (2012). Rapid Assessment of the Demand Side Financing Schemes: Aama programme and 4ANC, 2012. Kathmandu: Government of Nepal; HERD.
- USAID. (2021). USAID Bangladesh Health Strategy 2022-2027. Dhaka: USAID.
- Vaillancourt, D. (2009). Do Health Sector-Wide Approaches Achieve Results? : Washington, DC: World Bank.
- WHO. (2010). Monitoring the building blocks of health systems: a handbook of indicators and their measurement strategies. Geneva: World Health Organization.
- WHO. (2014). WHO Country Cooperation Strategy: Bangladesh 2014-2017. (9290224533). Geneva: World Health Organization.
- WHO. (2019). Declaration of Astana: Global Conference on Primary Health Care: Astana, Kazakhstan, 25 and 26 October 2018. Retrieved from Geneva.
- Whyle, E. B., & Olivier, J. (2016). Models of public–private engagement for health services delivery and financing in Southern Africa: a systematic review. Health Policy Plan, 31(10), 1515-1529. [CrossRef]
- WID. (2023). Bangladesh. Retrieved from https://wid.world/country/bangladesh/.
- Woode, M. E., Mortimer, D., & Sweeney, R. (2021). The impact of health Sector-Wide approaches on aid effectiveness and infant mortality. J Int Dev, 33(5), 826-844. [CrossRef]
- World Bank. (2017). Bangladesh - Health Sector Development Program Project. Retrieved from http://documents.worldbank.org/curated/en/201211514407103482/Bangladesh-Health-Sector-Development-Program-Project.
- World Bank. (2023a). The World Bank In Bangladesh. Retrieved from https://www.worldbank.org/en/country/bangladesh/overview.
- World Bank. (2023b). World Development Indicators. Retrieved from https://databank.worldbank.org/source/world-development-indicators#.
Figure 1.
Timeline SWAps in Nepal and Bangladesh. Source: own.

Figure 2.
Evaluation-Framework. Source: Own, based on (D’Aquino et al., 2019).
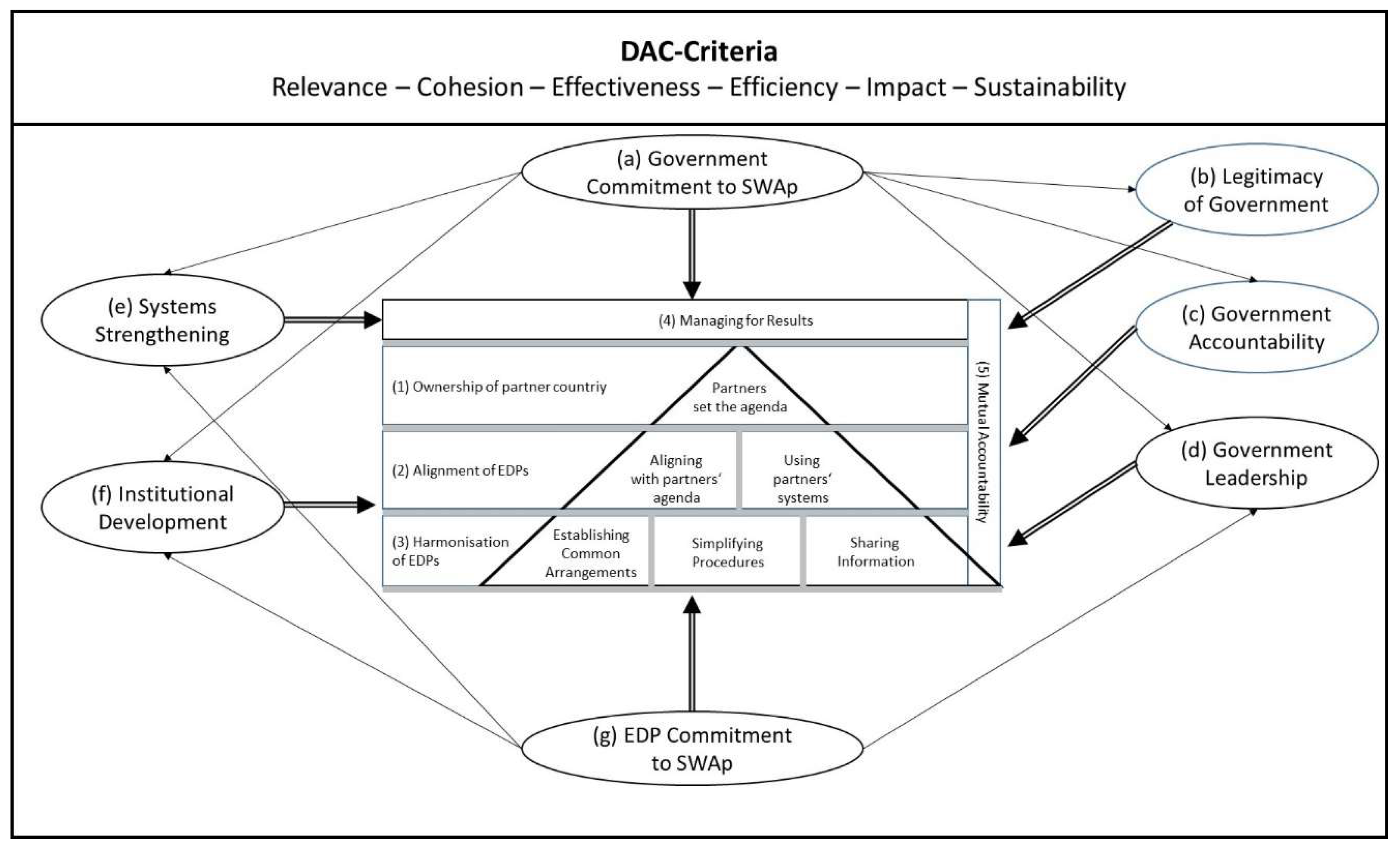
Figure 3.
Logframe of NHSP-II. Source: own.
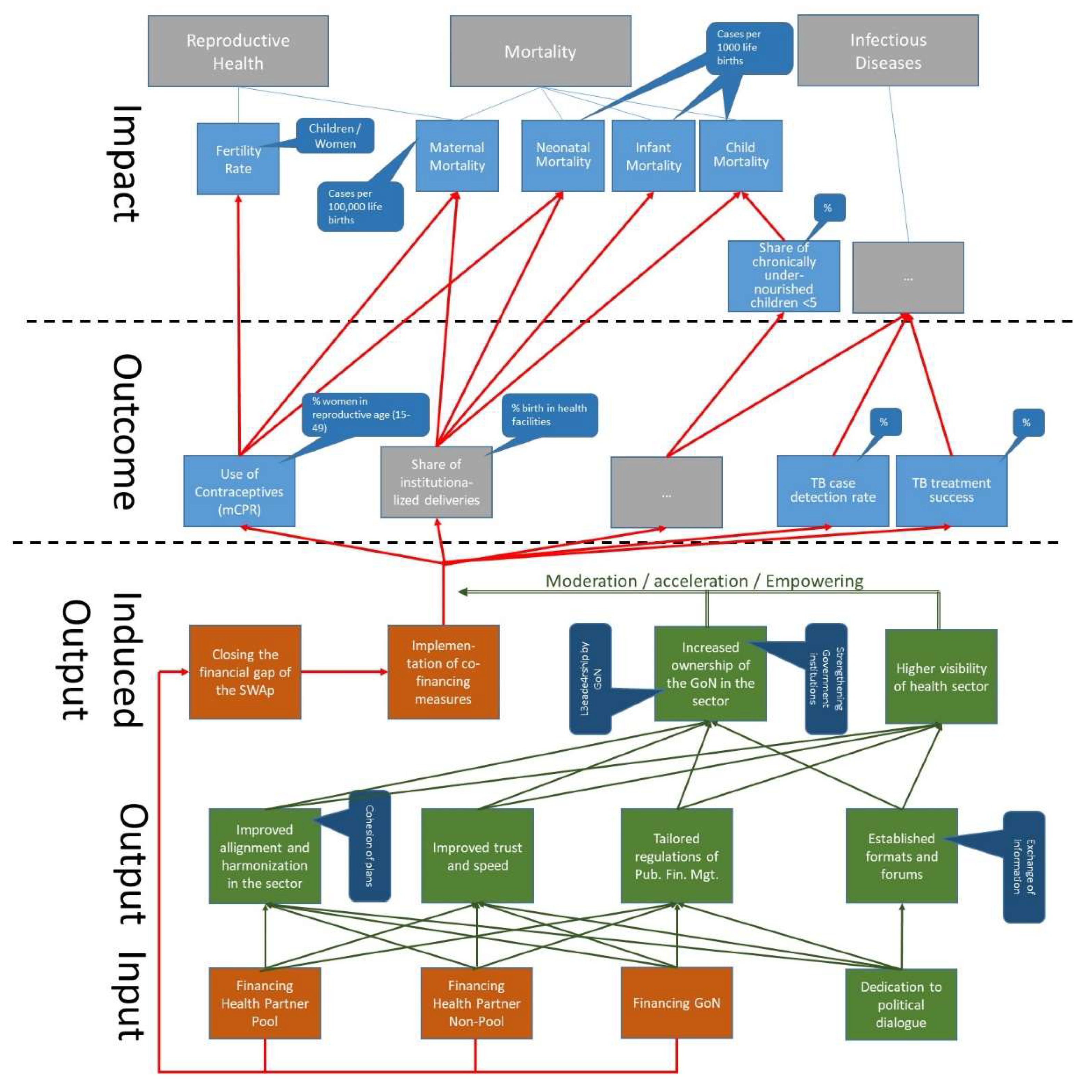
Figure 4.
Health Indicators of Nepal. Source: (World Bank, 2023b).
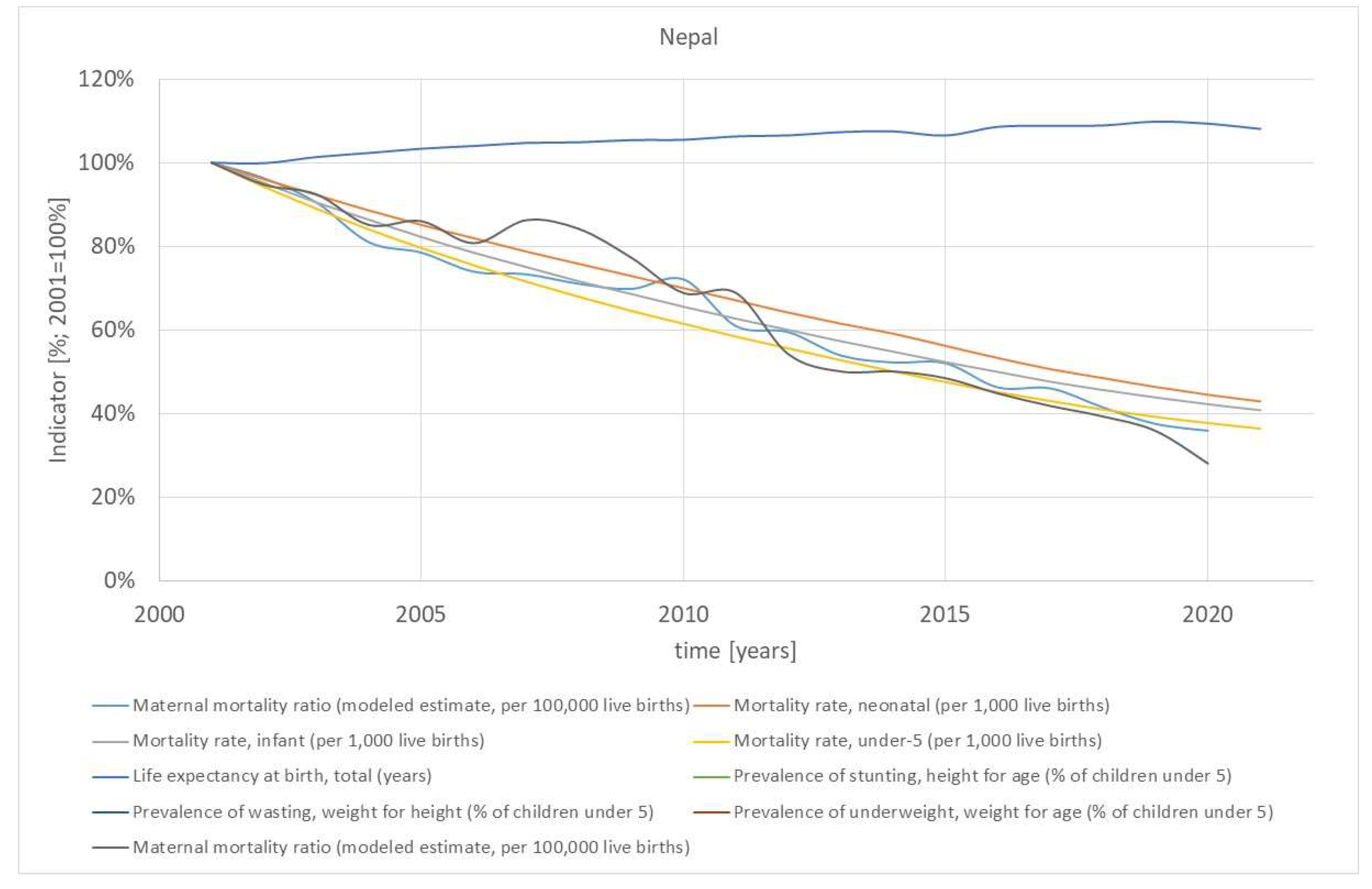
Figure 1.
Capacities and SWAp. Source: own.
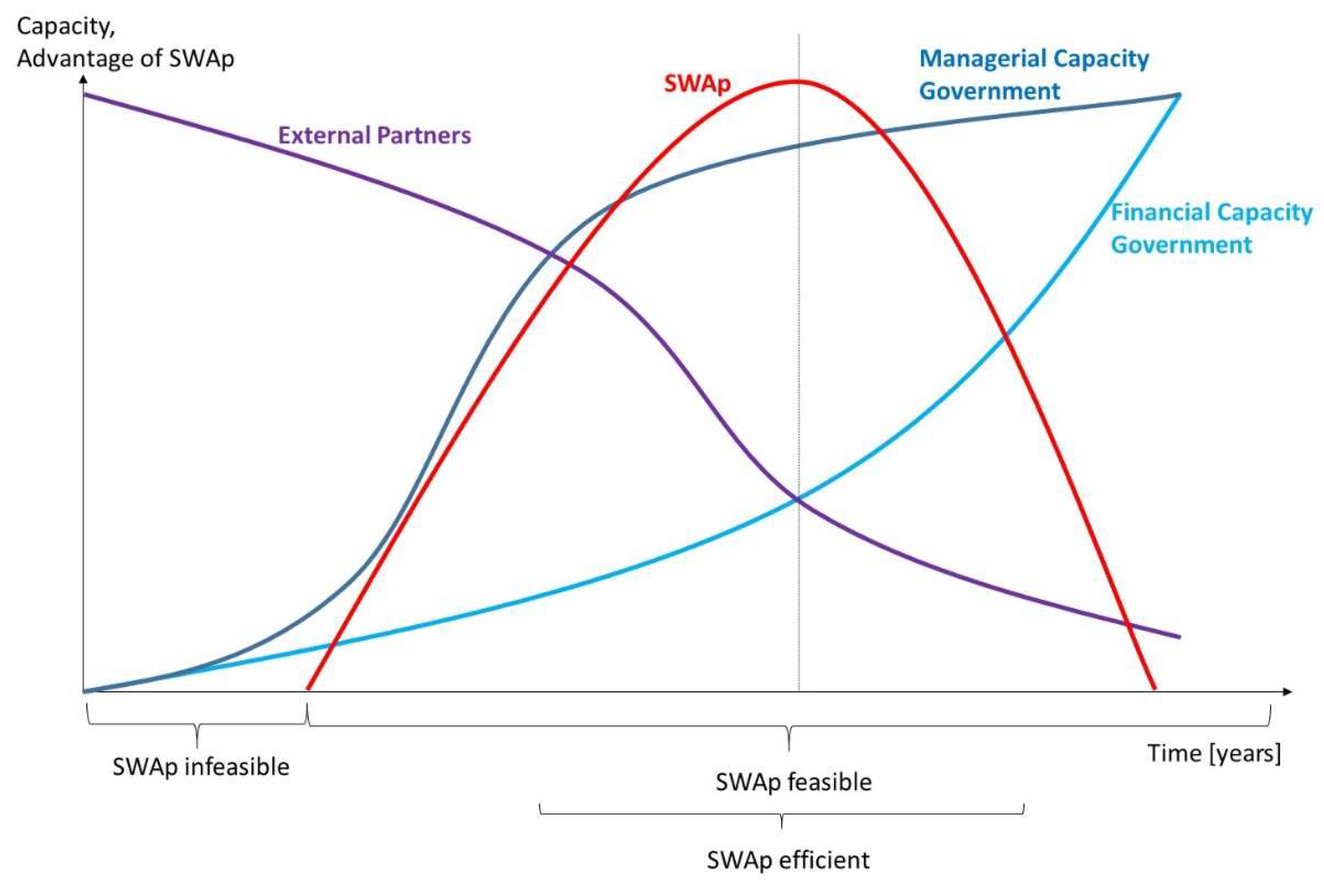

Table 1.
Conceptions of development assistance for health. Source: own, based on (UNFPA, 2005).
| Method | Horizon | Content | Ownership | Target | Coordination | Financing | Risk |
|---|---|---|---|---|---|---|---|
| Project | fixed | tailor-made intervention with limited scope | can be external development partner | specific challenge | limited | one source or consortium | poor coordination and alignment, poor sustainability, poor ownership |
| Program | until problem is solved or taken over | tailor-made intervention with broader scope | can be external development partner | specific challenge | limited | one source or consortium | poor coordination and alignment, medium sustainability, poor ownership |
| Sector-wide program | phases of a continuous sector program | entire sector | Government | entire health sector | completely within health sector | basket financing or single donor trust fund | limited control by external development partners |
| General budget support | annual support | entire Government | Government | all sectors | completely with all sectors | non-earmarked budget | very limited control by external development partners |
Quelle: Own, based on (Natuzzi & Novotny, 2014; UNFPA, 2005).
Table 2.
Examples of Outcome Indicators for Effectiveness of HPNSDP. Source: (World Bank, 2017, 2023b).
Table 2.
Examples of Outcome Indicators for Effectiveness of HPNSDP. Source: (World Bank, 2017, 2023b).
| Indicator | Value 2011 | Objective | Latest Value |
|---|---|---|---|
| Use of contraceptives (CPR; % women in reproductive age (15-49 years) [%] | 62 % | 72 % | 63 % (2019) |
| Share of safe deliveries (births with professional support) [%] | 26 % | 50 % | 59 % (2019) |
| Vitamin A Supplement (share of children from 6-59 months receiving Vitamin A during the last six months) [%] | 83 % | 90 % | 97 % (2020) |
| Breast-Feeding (Share of children ≤ 6 months fully breast-fed) [%] | 43 % | 50 % | 63 % (2019) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



