
Submitted:
02 May 2025
Posted:
07 May 2025
You are already at the latest version
Abstract
The Sustainable Development Goals affirm healthcare as a universal right, with Target 3.8 calling for Universal Health Coverage (UHC) for all, including displaced populations. Yet in Southern and Eastern Africa (SEA), refugees, asylum seekers, internally displaced people (IDPs), and undocumented migrants continue to face systemic health exclusions shaped by restrictive legal frameworks, under resourced health systems, and fragmented governance. This paper applies a ‘whole-of-route- rights based approach to examine how health access is shaped across displacement trajectories – from origin to transit, destination and return – focusing on w well-established migratory corridor linking the Democratic Republic of Congo and Somalia to Kenya and South Africa. Drawing on 70 key informant interviews and policy analysis conducted in two phases (2020-2022 and 2023-2025), the paper identifies critical implementation gaps between UHC commitments and the lived realities of displaced populations. Key challenges include an over-reliance on restrictive legal classifications, weak policy coordination, and migration-aware reforms that embed rights-based approaches into national and continual UHC strategies to ensure displaced populations are not left behind in the pursuit of health for all.
Keywords:
Universal Health Coverage (UHC)
; Internally Displaced People (IDPs)
; Healthcare
; Mental Health
; Gender-Aware
; Legislative frameworks South Africa
; Somalia
; Democratic Republic of Congo (DRC)
; Kenya
1. Introduction
1.1. Migration, Displacement and Health in the SDGs
Adopted in 2015, the 2030 Agenda for Sustainable Development includes 17 Sustainable Development Goals (SDGs) and 169 targets that “seek to realise the human rights of all”1 [1](p1). However, progress remains highly uneven; as of 2024, only 16% of SDG targets are on track to be achieved by 2030, while 84% show limited progress or reversal. Meanwhile, the gap between the world's poorest countries and the global average continues to widen [2]. A key contributing factor to these failures is the continued exclusion of large population groups from policies and programmes designed to advance the SDGs [3].
Whilst the 2030 Agenda explicitly emphasises inclusion referring to “refugees, internally displaced persons (IDPs)2 and migrants” and “people living in areas affected by complex humanitarian emergencies” [1](p7) - these groups are too often left behind. Inclusive implementation of the SDGs requires recognition of migration as encompassing all forms of population movement and as a cross-cutting issue within the SDGs. Eleven of the seventeen goals include targets and indictors directly related to migration, emphasising the importance of addressing displacement to achieve “health for all” [8,9,10,11,12].
This agenda is reinforced by two key global governance documents: the Global Compact on Safe, Regular and Orderly Migration (GCM) [13], which operationalises SDG target 10.7; and the Global Compact on Refugees (GCR) [14], which promotes the inclusion of refugees and IDPs in the 2030 Agenda [15]. Despite these frameworks, the limitations of both Compacts in guiding rights-based and inclusive development responses have been widely critiqued [16,17,18,19].
The right to health is enshrined in numerous international instruments and recognised as a key driver of development. The 2030 Agenda states that “(t)o promote physical and mental health and well-being, and to extend life expectancy for all, we must achieve universal health coverage (UHC) and access to quality health care. No one must be left behind” [1](p7). SDG Target Goal 3.8 calls for UHC that ensures financial protection and access to quality essential services, medicines and vaccines for all [1](p16). Yet, in 2025, marginalised groups – including undocumented migrants3, refugee, asylum seeking and IDPs (from now on referred to collectively as ‘displaced populations’) – continue to be ‘left-behind’ in efforts to achieve UHC by 2030 [3].
1.2. Determining Health in Contexts of Displacement
The inclusion of displaced populations in UHC and broader health governance is well established across the SDGs, global health and migration frameworks [20,21,22,23,24,25,26,27,28,29,30,31,32,33]. However, these populations continue to face significant barriers to realising their right to health [34,35,36,37,38]. This is due to both formal exclusion - where the rights of particular groups are not legislated for - and structural and social factors that constrain individuals’ access to entitlements, services and protection [36,39,40,41,42].
Migration and displacement - whether driven by conflict, socio-political instability, or environmental crises - are defining determinants of health [38,43,44,45,46,47,48,49,50]. Displaced individuals face continuous exposure to various forms of structural and direct violence – including intimate partner and GBV - that negatively impact physical and mental health outcomes [51,52,53,54,55,56,57]. These exposures shift and change over time and space and can be mapped onto trajectories of displacement as people move within and between the regions, countries and contexts that impact their health and wellbeing in varied and cumulative ways.
Yet – counter-intuitively - current legislative, policy and programmatic responses to the interlinked domains of health, (im)migration management and refugee protection often fail to engage adequately with the temporal and spatial dimensions of displacement. In doing so they are (albeit in some instances unintentionally) positioning migrants and displaced persons as static, thus failing to address the dynamic health-related experiences of these populations as they move over time and space. Such approaches go some way in explaining the over-representation of citizen-focused, state-led responses to health that fail to engage with processes of migration, therefore deliberately excluding, or indirectly overlooking, displaced populations and the associated need for responsive, cross-regional, inclusive and intersectoral health policy instruments.
1.3. A Whole-of-Route, Rights-Based Approach to Health and Displacement
In this paper, we explore the right to health of displaced people from the Democratic Republic of Congo (DRC) and Somalia who move both within and beyond their countries of origin, often along a well-established migratory route that connect the Horn, East and Southern Africa via Kenya and South Africa (see Figure 1).
An extensive body of literature highlights the ways in which these displaced populations experience fragmented and discriminatory access to healthcare, due to legal barriers, weak health systems, and structural marginalisation [58,59,60,61,62,63,64,65,66,67,68]. However, much of this evidence is generated in a single location at a single point of time, therefore failing to engage with the temporal and spatial dimensions that define migration and displacement.
In recognising this, we adopt a whole-of-route approach to explore displacement and health that acknowledges the ways in which health outcomes are cumulative, reflecting changing exposures to varied determinants of health across contexts of origin, transit, destination, and return [69]. Health vulnerabilities are shaped dynamically by displacement, including through exposure to changing contexts of violence, precarity and state inaction, This necessitating both the analysis and development of governance responses that look beyond static, state-centric models of healthcare access [70].
Central to this analysis is a rights-based framework, grounded in international and regional human rights instruments such as the International Covenant on Economic, Social and Cultural Rights (ICESC) and the African Charter on Human and Peoples’ Rights (hereafter referred to as “African Charter”) [71]. This perspective positions healthcare as a legal entitlement and demands state accountability for providing non-discriminatory, timely, and affordable access to essential health services for all, regardless of their migration status. Addressing the social determinants of health—such as documentation status, access to employment, safe housing, and protection from violence—is integral to realising this right [47,72].
Together, the whole-of-route and rights-based frameworks provide a comprehensive lens for assessing how health systems and governance respond -or fail to respond – to the needs of displaced populations as they move across complex migratory pathways.
1.4. Governance Gaps, Implementation Voids and Static Responses
This paper examines the (dis)connections between the lived realities and formal commitments to the right to health and UHC for displaced populations and their implementation in DRC, Somalia, Kenya and South Africa. Through policy analysis and empirical research with key informants (n=70), we employ a whole-of-route approach to addresses the temporal-spatial dynamics of displacement and health, and assess whether identified governance, legislative and policy frameworks are responsive to the health needs of displaced populations as they move along complex migratory pathways. Our analysis is structured around three key aims:
- To review relevant global, continental, regional governance frameworks related to UHC alongside national legislation, policy and frameworks for each country;
- To examine the lived experiences of interviewed healthcare professionals and policy-makers (n=70) engaged with displacement and health, with attention to legal status, gender, and mental health across the four countries; and
- To identify legal, operational, and governance gaps, and propose actionable recommendations for inclusive, migrant-aware health system reform.
Our findings highlight critical governance gaps, implementation voids and static health responses that, collectively, undermine the right to health for displaced populations in the DRC, Somalia, Kenya and South Africa. By exposing the disconnect between persistent - and increasing - normative governance frameworks, restrictive legislation and policy, and lived realities, this paper contributes urgent conversations around UHC in the southern and eastern African region (SEA)4; in this paper, SEA refers to: the Southern African Development Community (SADC), East African Community (EAC) and the Intergovernmental Authority on Development (IGAD).These link to calls systematic transformation to dismantle exclusion, address social determinants of health, and implement coordinated, regionally and nationally inclusive responses that uphold the right to health for all.
Achieving UHC and the broader health targets of SDG 3 in these regions requires integrated, rights-based reforms that align refugee protection, immigration management and public health governance using a whole-of-route approach. Without this shift – a move beyond securitised political rhetoric that is currently shaping migration policy - displaced populations will remain outside the protective reach of global health commitments, deepening health inequities and undermining sustainable development efforts.
2. Methodology
This study involved a comprehensive policy review and 70 semi-structured interviews across the DRC, Somalia, Kenya and South Africa. The research was undertaken in two phases. The initial phase (2020-2023), involving the co-authors and non-author contributors listed in the Acknowledgement section, was conducted as part of the GCRF Protracted Displacement project, ‘Improving healthcare at the intersection of gender and protracted displacement amongst Somali and Congolese refugees and IDPs (DiSoCo)’ supported by a grant (reference number ES/T004479/1) from the UK Economic and Social Research Council (ESRC) via the Global Challenges Research Fund (GCRF) Development-based approaches to Protracted Displacement scheme5. The second phase (2023-2025), including an updated review of global and regional governance frameworks and an updated review for South Africa [73], was undertaken by JV and RW as part of the Gendered violence and poor mental health among migrants in precarious situations Global Health Research Group (GEMMS) supported by the NIHR (grant ref: NIHR134629)6.
2.1. Policy and Legislative Review
A comprehensive review of relevant global, continental and regional governance frameworks was undertaken, along with reviews of national legislation, policy and frameworks in the DRC, Somalia, Kenya and South Africa, with a particular focus on UHC and rights-based access to healthcare for displaced populations. An analysis framework was developed and applied to assess the extent to which each document addressed four intersecting concerns:
- 1)
- Recognised and provided the right to health for migrants and displaced populations;
- 2)
- Integrated migration into healthcare planning and implementation (through access to public healthcare services);
- 3)
- Addressed mental health and psychosocial support within broader health system strategies;
- 4)
- Incorporated gender-sensitive approaches, including protection for displaced women, girls and, other gender-diverse groups.
Global and regional governance frameworks and associated documents were identified and reviewed iteratively. The identified documents are available online7 and as supplementary materials:supplementary materials: Table S1, Table S2, Table S3 and Table S4.
For each country, legislative and policy texts were systematically analysed using a framework (see Figure 2) adapted from previous work undertaken by RW and JV [74,75] to determine their engagement with the four core focus areas. Additional analysis determined the alignment of each document with key international and regional frameworks—including the SDGs, the African Union’s Migration Policy Framework [76], and the Kampala Convention on IDPs [77].
The findings were synthesised and presented in comparative tables illustrating the levels of engagement in legislation and policy with the four core focus areas for each country. These tables were adapted into graphical representations for each county and can be found online [78,79,80,81] and as supplementary materials:supplementary materials: Figures S1; S2; S3 and S4.
2.2. Key Informant Interviews (KIIs)
In-depth, semi-structured interviews were conducted with 70 key informants involved in migration, health policy, and service delivery:
- DRC: 32 interviews (national and provincial levels)
- Somalia: 12 interviews (federal and state levels)
- Kenya: 25 interviews (national and subnational levels)
- South Africa: 25 interviews (national, provincial and local levels)
Participants included government officials, healthcare providers, civil society actors, and representatives of international organisations. Interviews explored policy design and implementation processes; healthcare access barriers faced by IDPs including the role of legal status and documentation; gender-specific challenges; and, the visibility of mental health in service delivery. Participants provided informed consent. Interviews were conducted in-person or remotely (Zoom or telephone call); in English, Swahili, Lingala and Somali. Where possible and consent was provided, interviews were audio-recorded however, in many cases respondents were uncomfortable and/or reluctant and therefore notes were taken instead. Recordings or notes were then transcribed; translated to English (where required); and analysed thematically using a deductive-inductive approach. It is important to note that interviews were conducted during the COVID-19 pandemic, a period during which health challenges and barriers to healthcare access were fluid and significantly heightened across all settings, impacting the availability of key informants and the ability to undertake face-to-face interviews in some contexts [82,83,84]. Although this study does not focus specifically on the impacts of the pandemic, the broader effects of COVID-19 on health systems and displaced populations are acknowledged and have been discussed elsewhere [85,86,87,88,89].
These KIIs provided critical insights into the disjuncture between policy and practice, the drivers of policy change, and the operational challenges of addressing the healthcare needs of displaced populations across diverse governance settings
3. Results
This study reveals significant and persistent gaps between national Constitutional, legislative and policy commitments to upholding the right to access healthcare for all and the lived realities of displaced populations in the DRC, Kenya, Somalia and South Africa. Across all four countries, displacement and migration remain poorly integrated into health system planning, resulting in vague or exclusionary legal frameworks, fragmented service delivery, and critical gaps in the provision of mental health services and gender-sensitive care to displaced people. This section presents an overview of the key results from the reviews and interviews with key informants. These results are then discussed in detail in the subsequent discussion section.
3.1. The Migration, Displacement and Health Governance Ecosystem: Global, Continental and Regional
Access to healthcare in displacement contexts is often determined by legal classification. Refugees and asylum seekers are protected under international legal instruments such as the 1951 Refugee Convention and the OAU Refugee Convention (1969), which obligate states to ensure access to essential services, including healthcare. In contrast, IDPs—who have not crossed international borders—are, in principle, entitled to full constitutional rights in their country of origin [73,82]. However, in practice, these distinctions often blur, and protection remains uneven. IDPs frequently face entrenched marginalisation, inadequate service delivery, and limited political recognition, reflecting the structural and systemic barriers that undermine formal rights-based commitments [83].
Despite the existence of comprehensive international and regional frameworks—such as the African Charter on Human and Peoples’ Rights, the Migration Policy Framework for Africa (MPFA), and the Global Compact for Safe, Orderly and Regular Migration (GCM)—national implementation is often fragmented. Policies continue to prioritise citizens, leaving the health needs of migrants, refugees, and IDPs under-addressed within mainstream health systems [3,84]. The reality of displacement is dynamic and intersects with legal, social, and economic exclusions, which are not always accounted for in rigid policy approaches.
Table S1 provides an overview of the key global, continental, and regional governance frameworks that inform national responses to health and displacement across Africa [90]. These frameworks articulate the normative foundations for the right to health and serve as policy blueprints for state-level action.
3.1.1. Global Frameworks
At the global level, foundational instruments such as the Universal Declaration of Human Rights and the International Covenant on Economic, Social and Cultural Rights provide a legal and ethical basis for the right to health for all, irrespective of citizenship. These are supported by the 2030 Agenda for Sustainable Development, which embeds UHC as a core target under SDG 3. The GCM further advances the principle of inclusivity by mandating access to basic services for all migrants, regardless of status. The WHO Global Action Plan on Refugees and Migrants translates these global commitments into targeted strategies, addressing the practical health needs of displaced populations.
3.1.2. Continental Level: The African Union
At the continental level, the African Union (AU) has developed an integrated policy landscape addressing both health and mobility. The African Charter on Human and Peoples’ Rights reaffirms the right to health, while the Migration Policy Framework for Africa and the AU Health Strategy (2016–2030) provide direction for states to integrate migration into health planning. The Kampala Convention stands out as a globally unique, legally binding framework for the protection of IDPs, although its implementation remains limited across several member states. The AU Free Movement Protocol aims to enhance mobility and access to rights, but its uptake has been slow and inconsistent.
3.1.3. Regional Governance Frameworks: Southern and Eastern Africa
At the regional level, the Southern African Development Community (SADC) and East African regional bodies such as the Intergovernmental Authority on Development (IGAD) and the East African Community (EAC) have developed regionally tailored governance instruments. SADC frameworks focus on cross-border health responses, particularly in the context of HIV/AIDS and labour migration. IGAD and the EAC have promoted migrant-inclusive health systems through regional investment plans, mobility protocols, and pandemic preparedness strategies. These frameworks increasingly emphasise health system harmonization, regional health security, and inclusive access for displaced populations. Collectively, these governance instruments create a multi-layered framework that supports the right to health in contexts of migration and displacement.
Further details can be found in Supplementary Materials: Table S1 lists all frameworks identified and reviewed globally, continentally (AU) and in the three key regions involved in this study - the Southern African Development Community (SADC), East African Community (EAC) and the Intergovernmental Authority on Development (IGAD). These resources are also available online8.
3.2. Upholding the Right to Health for Displaced Populations in the DRC, Somalia, Kenya and South Africa
This section presents a summary of key findings from the reviews and 70 KIIs, which are explored in greater depth in the subsequent discussion. The results illustrate how the distinct, national contexts and policy priorities shape divergent approaches to migration governance, displacement management, and uphold (or not) the rights of migrant and displaced populations, particularly in relation to access to healthcare. While there are signs of progress towards UHC across all four countries none has sufficiently incorporated and implemented migration, displacement and health into their legislative and policy frameworks in a comprehensive or consistent way. Figure 3 summarises the differences in the national policy landscape across the four countries, highlighting their level of engagement with the right to health for displaced populations; and the extent to which national health systems are migration-aware, gender-aware and responsive to mental-health needs. Figures S1-S4 present graphical summaries of the findings for the DRC, Somalia and South Africa; these are also available online9 [78,79,80,81].
3.2.1. Upholding the Right to Health for Displaced Populations
Constitutionally, all four countries - the DRC, Somalia, Kenya and South Africa – recognise the right to health for all. However, the realisation of this right – which is mostly operationalised through the guarantee of access to healthcare - is often undermined due to a lack of alignment between Constitutional guarantees, legislation and policy frameworks. Such misalignment provides opportunities for (mis)interpretations of Constitutional guarantees in the drafting and promulgation of legislation and subsequent policy development. For example, failing to include explicit provisions in national legislation and/or associated policies to uphold a Constitutional guarantee of access to healthcare can result in practices that fail to affirm this right.
Such is the case in South Africa and Kenya where Constitutional guarantees to uphold health as a fundamental human right through rights-based legislative frameworks are not accurately translated into policy, resulting in exclusionary practices. In South Africa, the 2024 National Health Insurance (NHI) Bill legislates for restricting access to healthcare services on the basis of legal status, contradicting the Constitution and other current legislation, including the National Health and Refugee Acts. In Somalia, the Provisional Federal Constitution guarantees the right to health for all, yet national frameworks such as the Health Sector Strategic Plan (HSSP) and Essential Packages of Health Services (EPHS) do not explicitly include refugees and migrants, leaving their right to access services open to interpretation. Similarly, in the DRC, although the right to health is constitutionally affirmed, the ‘Law on the Status of Refugees’ stipulates administrative restrictions which – depending on interpretation – can be applied to foreign nationals, thus limiting their access to healthcare.
3.2.2. Migration-Aware Health Systems Planning
All four countries have made some progress toward the development of migration-aware health systems, though the extent to which this supports access to healthcare for displaced populations varies significantly. Neither the DRC or Somalia have comprehensive legal frameworks for governing immigration or refugee protection, relying instead on fragmented legislation and policies that govern access to healthcare. This limits the extent to which health systems can be migration-aware and leading to policies and practices that risk undermining the right to health for all. While the DRC’s National Health Policy acknowledges the needs of IDPs and refugees, and seeks to integrate them within the national health system, Somalia’s federal Government continues to face significant challenges in doing so due to limited territorial control and resource constraints, hindering effective migration governance and health systems-planning.
In contrast, South Africa and Kenya have more comprehensive frameworks that uphold the rights of migrants and displaced populations to access healthcare. For South Africa, the National Health Act (NHA) (2003) is supported by the progressive National Integrated Sexual and Reproductive Health and Rights Policy (2019), which specifically includes gender-sensitive, and migrant-friendly reproductive health services. Similarly, Kenya’s Health Policy 2014-2030, and the associated UHC Policy 2020-2030 align with UHC principles and legislate for inclusive health service delivery for both citizens and refugees. However, both countries face significant implementation gaps. Moreover, their respective approaches to National Health Insurance have been criticised for being more exclusionary than inclusive, undermining current legislative and policy provisions that uphold the Constitutional guarantee of the right to healthcare, thus undermining the ambitions of UHC.
3.2.3. Mental Health Aware Health Systems Planning
The integration of mental health services into broader health systems remains weak in Somalia, Kenya and South Africa; the DRC stands out as the only country that effectively engages with mental healthcare for migrants and refugees at a primary care level, including through community-based mental health programmes. These positive developments, however, are made against the backdrop of protracted political instability and conflict, presenting significant challenges to the effective delivery of healthcare services in the country, including limiting the reach and sustainability of community-based programmes. Somalia outlines nominal rights and obligations for mental healthcare service provisions in certain strategies but these are not guaranteed in the Constitution, nor prioritised in the National Roadmap to Universal Healthcare. Like the DRC, protracted instability presents challenges to the provision of services in Somalia. In Kenya, although the right to good mental health is Constitutionally protected, the country’s Refugee Policy Framework lacks specific provisions relating to the delivery of psychosocial support for refugees, contributing to the significant barriers – or outright exclusion - faced by refugees and asylum seekers when trying to access services. In South Africa, despite progressive mental health policies and frameworks, migrant and displaced populations have not been adequately considered in implementation strategies and service delivery frameworks; this is compounded by the fact that existing legislation does not explicitly refer to the provision of mental healthcare services to non-citizen groups.
3.2.4. Gender-Aware Health Systems Planning
Whilst some exceptions exist, gender – in the context of migration, displacement and health – is predominantly reduced to the needs of ‘women and girls’ across all four countries. South Africa has integrated gender into health systems planning. However, there is a clear gap between policy and practice and a failure to engage with the intersections of migration, displacement, gender and health. In the DRC, the National Migration Policy (2012) and the National Health Development Plan (2016) emphasise the importance of gender-sensitive approaches however, effective implementation is undermined by limited resources, capacity and coordination. Similarly, Kenya has various gender-sensitive policies relevant to migration, displacement and health, including the National Policy for Prevention and Response to Gender-Based Violence (2014). Nonetheless, these frameworks are constrained by fragmented coordination and insufficient recognition and integration of the heightened needs of refugee and asylum seeking women and girls. In Somalia efforts towards gender inclusion are reflected in The National Development Plan (2019-2023), which recognises the need for gender-sensitive approaches to the governance of migration and health. While sexual offence legislation exists, broader health and mental health legislation in Somalia does not adequately address gender -specific needs, particularly for displaced populations.
The above findings are expanded on in the following discussion.
4. Discussion
We organise our discussion around five cross-cutting themes that emerged from the policy review and key informant interviews:
- 1)
- Gaps between UHC commitments and healthcare access for displaced populations;
- 2)
- Limited integration of migration into national health system planning;
- 3)
- Neglect of mental health needs among displaced communities;
- 4)
- Lack of gender-sensitive health programming; and
- 5)
- Structural barriers to care.
4.1. Gaps Between UHC Commitments and Healthcare Access for Displaced Populations
Although the DRC, Kenya, Somalia, and South Africa have all made formal commitments to achieving UHC (see Figure 5 and Figures S1-4), major gaps persist between policy ambitions and the healthcare realities experienced by displaced populations. Across all four countries, access to health services remains heavily shaped by migration status, resource constraints, and structural exclusions.
Figure 4.
Comparative Overview of Universal Health Coverage (UHC) Approaches.
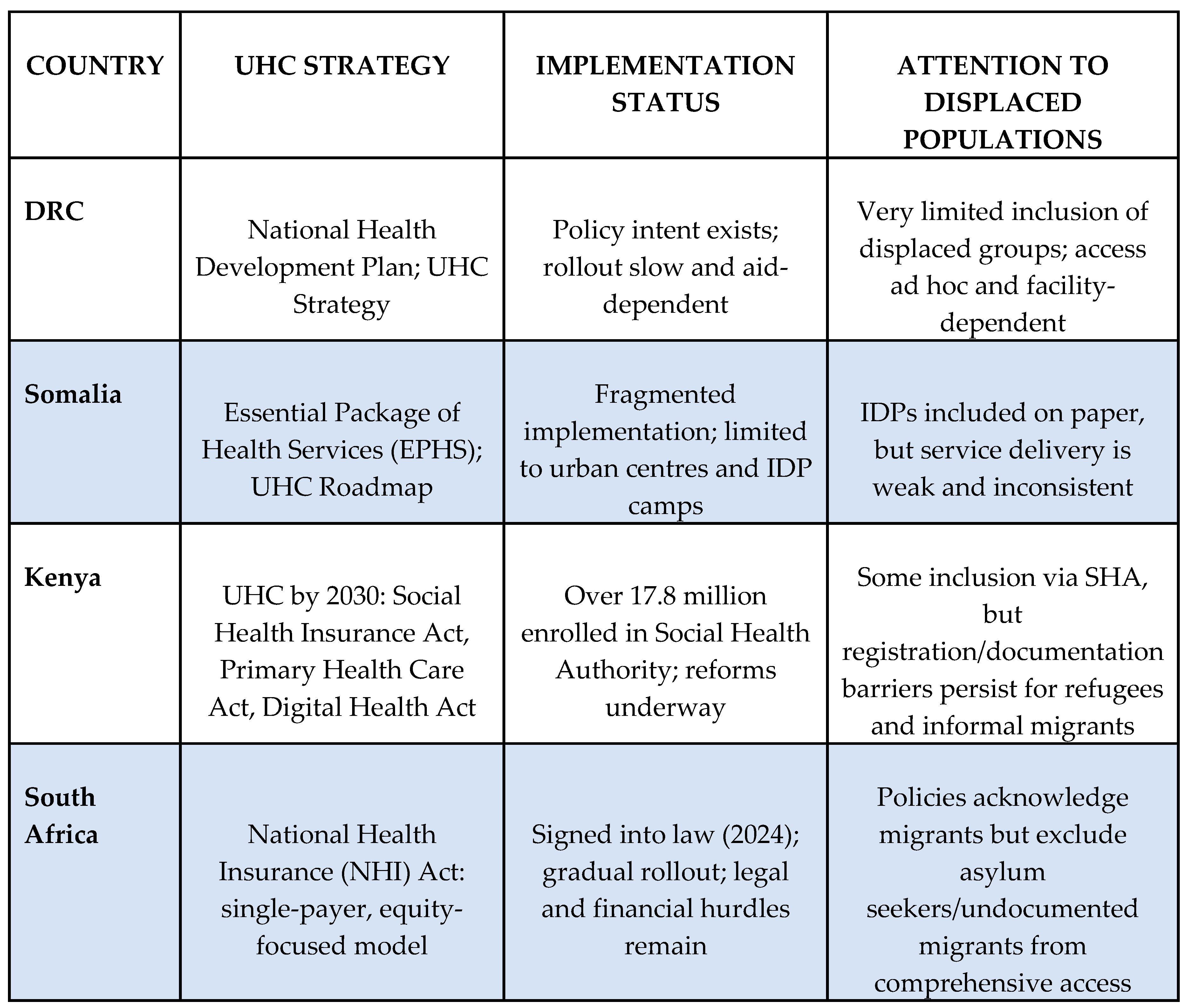
In South Africa, the National Health Insurance (NHI) Act (2023) and the District Health System (DHS) model aim to unify health financing and reduce inequalities [91]. However, access is deeply stratified: citizens, permanent residents, and recognised refugees are entitled to comprehensive services, while asylum seekers and undocumented migrants are restricted to emergency care and treatment for notifiable conditions. As one healthcare worker observed,
“The NHI is sending mixed signals—only some get the so-called universal access, for others, it categorises people and the most vulnerable are the most excluded” (KII, SA 03).
The NHI’s selective inclusion of migrants has been widely criticised as incompatible with South Africa’s constitutional and human rights obligations, and as undermining public health goals, particularly in managing infectious diseases [92].
Kenya’s UHC reforms - anchored in the Primary Health Care Act and the Social Health Insurance Act,- have enabled registration under the new Social Health Authority (SHA) to over 17.8 million individuals. However, displaced populations continue to face persistent barriers. Although the 2010 Constitution guarantees the right to health for "every person," refugees and asylum seekers. Are often excluded in practice due to documentation requirements, mobility restrictions, and an overstretched health system. As a Kenyan respondent explained,
“Even though refugees are entitled in theory, in practice, the system still asks for documents they cannot easily produce.” (KII, Kenya 01)
Kenya’s adoption of the Comprehensive Refugee Response Framework (CRRF) and 2021 Refugee Act demonstrate an intent to integrate refugees beyond camp-based models [93]. However, implementation remains limited and refugees in Kakuma and Dadaab camps primarily access health services through parallel systems run by UNHCR and partner agencies, rather than national health structures. As a Kenyan respondent noted,
“There’s a clear separation — host communities and refugees have parallel services but no real integration.” (KII, Kenya 01)
In the DRC, the government 2021 National UHC Strategic Plan, established institutional bodies such as the Health Solidarity Fund and the National Institute of Public Health [94,95]. Early initiatives, like free maternity care programme, represent important steps towards supporting vulnerable groups [96]. Yet, health system implementation remains heavily reliant on international funding and technical support, particularly outside Kinshasa and other urban centres [97,98].
Somalia’s UHC Roadmap and the Essential Package of Health Services (EPHS), nominally prioritise IDPs and vulnerable groups, including displaced women and children [99,100]. However, health planning for displaced populations remains highly fragmented between the Federal Government and Federal Member States, and operationalisation is weak. As one Somali participant described,
“With the help of international NGOs, we set up health centres in IDP camps where the health services are free of charge, but these centres cannot cover all the health needs of the IDPs so we must prioritise essential packages such as maternal and child health” (KII, Somalia, 02).
Another added,
“In our policies and plans, we emphasise the right of displaced persons to housing, access to land and security, health, education and other assistance, but it is impossible to implement these plans because all our activities rely on funding from the donor community.” (KII, Somalia 04)
In South Africa, despite strong Constitution protections, migration-aware planning is largely absent from major national health reforms. While migrants are mentioned in targeted strategies such as the National HIV, TB, and STIs Strategic Plan (2023–2028), broader reforms like the National Health Insurance (NHI) Act exclude asylum seekers and undocumented migrants from comprehensive care. Legal status continues to determine access reflecting increasingly restrictive migration governance [101,102]. Frontline discretion also continues to shape experiences. As a South African health worker explained,
“Access depends on how you are treated at the facility, not on your rights.” (KII SA 02).
Across all four countries, policy frameworks commit to UHC and recognise the right to health, displaced and migrant populations continue to experience systemic barriers to healthcare access. These exclusions reflect broader patterns of structural violence and the failure to realise rights-based reforms to ensure that UHC commitments apply to all in theory and practice, regardless of migration status [103].
4.1.1. Lack of Migration-Awareness in Health Systems Planning
Although displacement and migration are critical health determinants across Sub-Saharan Africa, health system planning in the DRC, Kenya, Somalia, and South Africa remains predominantly citizen-centric. Across all four countries, migration and mobility are poorly integrated into health strategies, leading to fragmented service delivery, inconsistent entitlements, and the exclusion of displaced populations [104].
In the DRC and Somalia , there are no dedicated national frameworks that address the health needs of refugees, asylum seekers, or IDPs beyond general humanitarian responses. Health services for displaced populations rely overwhelmingly on international Non-Governmental Oragnisations (NGOs) with little integration into national health systems. Kenya and South Africa have taken more explicit steps to include migrants in policy, but implementation is weak, and exclusion persists through administrative and structural barriers. Across all four contexts, health and migration sectors operate in silos, with limited cross-sectoral collaboration, a lack of reliable data on migrant health, and no clear planning for the health needs of mobile and displaced populations.
4.1.2. Neglect of Mental Health Needs Among Displaced Populations
Despite growing recognition of mental health as a critical component of UHC [105], mental health services for displaced populations across the DRC, Kenya, Somalia and South Africa remain critically underdeveloped. Chronic underfunding, severe workforce shortages, pervasive stigma, and a lack of trauma-informed, mobile-friendly services consistently restrict access. Mental health needs—particularly those arising from conflict, displacement, and GBV - are insufficiently addressed in both health policy frameworks and service delivery across all four contexts.
In the DRC, mental health has been formally integrated into primary healthcare frameworks, and a draft Multi-Sectoral Strategic Plan for Mental Health and Psychosocial Support (2024–2028) [106]signals growing policy commitment. However, resource constraints are severe: fewer than 60 trained mental health professionals serve a population exceeding 90 million. Services for displaced populations are also sparse, primarily concentrated in urban areas or delivered by humanitarian projects [107]. As a Congolese health planner explained,
“There’s a strong will to act, but the system is overloaded. For migrants, access depends on ad hoc decisions at the facility level.” (KII, DRC, O1)
IDPS in particular rely on short-term NGO initiatives, with little systematic provision from national health systems.
In Somalia, mental health is referenced in the Essential Package of Health Services (EPHS) and a draft National Mental Health Policy, yet implementation remains extremely weak. Outside Mogadishu, services are almost non-existent, and both federal and state-level governments provide minimal support [108]. As one Somali healthcare professional stated,
“Mental health is a forgotten component of health services in Somalia, not only for IDPs but for even the general population.” (KII, Somalia, 11)
Persistent funding shortages, stigma, and the shortage of trained personnel further erode displaced populations’ access to psychosocial support.
Kenya’s Mental Health Policy (2015–2030) and Mental Health Act (2012) establish a strong legal framework for expanding mental health services [109,110]. However, service provision for refugees and migrants remains extremely limited, particularly within camp settings. Refugee health programs prioritise primary healthcare and infectious diseases, with mental health often considered secondary or optional [61]. As one key informant working in Kakuma explained,
“Mental health remains underfunded and understaffed.” (KII, Kenya 02)
Financial barriers, workforce shortages, and the weak integration of mental health into primary care models continue to restrict access for displaced communities.
In South Africa, the National Mental Health Policy Framework and Strategic Plan (2023–2030) adopt a rights-based approach [32] but operational barriers undermine access for migrant populations. Language discordance, xenophobia, and lack of institutional clarity often exclude migrants in practice.. As a health policy stakeholder noted,
“migrants are effectively invisible in mental health service delivery.” (KII SA 05).
Though migrants may be technically entitled to services, eligibility does not equate to access where systemic discrimination and administrative barriers persist [82].
Across all four countries, mental health is increasingly recognised in policy rhetoric, but displaced populations remain structurally excluded from care. This entrenched neglect reinforces health inequities and undermines both UHC and broader rights-based commitments. Addressing mental health for displaced populations—who experience high levels of trauma, psychosocial distress, and ongoing instability—must move beyond frameworks and towards adequately resourced, accessible, and inclusive service delivery models tailored to the needs of displaced communities [86].
4.1.3. Lack of Gender-Sensitive Health Programming
While gender equity is formally recognised within the health and migration policy frameworks of the DRC, Kenya, Somalia, and South Africa, practical implementation of gender-sensitive health programming remains limited, particularly for displaced populations. Across all four contexts, displaced women and girls face persistent barriers to accessing sexual and reproductive health services, while marginalised groups—including LGBTQ+ migrants—receive little targeted attention [75,111].
In the DRC, although the Constitution and the 2015 Law on Parity outline strong commitments to gender equality and non-discrimination, delivery remains uneven. In conflict-affected regions hosting large internally displaced populations, access to GBV and sexual and reproductive health (SRH) services, and psychosocial support is severely constrained by insecurity, underfunding, and the concentration of services in urban centres. As a result displaced women in rural areas are often dependent on intermittent, NGO-led initiatives with limited scope and continuity [96,98].
Somalia’s National Gender Policy (2016) and the Health Sector Strategic Plan (HSSP III) identify the specific vulnerabilities of displaced women and girls. However, gender-sensitive health services remain fragmented and largely donor-driven. As Somali interviewees explained,
“With the help of international NGOs, we set up health centres in IDP camps... but these centres cannot cover all the health needs of the IDPs so we must prioritise essential packages such as maternal and child health.” (KII, Somalia 02)
Structural barriers, insecurity, and weak federal-state coordination continue to constrain the delivery of comprehensive gender-responsive healthcare beyond a basic emergency model.
Kenya has enacted progressive legal protections, including the Sexual Offences Act (2006), alongside refugee frameworks that endorse protection for survivors. While dedicated GBV services exist in Kakuma and Dadaab refugee camps; service quality and accessibility remain inconsistent and often fails to reach urban refugees outside formal camps. As a humanitarian health worker noted,
“We talk about gender-based violence in refugee camps, but the services are basic, and many cases go unreported.”(kII, Kenya, 02)
Although UHC reforms and refugee integration policies theoretically promote health equity, Documentation requirements, overstretched resources, and implementation gaps continue to limit displaced women’s access to holistic sexual and reproductive healthcare services [62].
South Africa has one of the strongest gender rights frameworks among the four countries, anchored in the Constitution, and legislation such as the Promotion of Equality and Prevention of Unfair Discrimination Act (2000) [112], and national health strategies. Despite this, displaced and migrant women face systemic discrimination, xenophobia, and administrative barriers when accessing healthcare. Although policy frameworks recognise gender diversity and sexual and reproductive rights, operational practices often focus narrowly on cisgender women and girls, excluding LGBTQ+ migrants from meaningful exclusion [75].
Across all four countries, the rhetoric of gender inclusion has yet to translate into systematic practice [36]. Health responses remain largely reactive, siloed, and dependant on external actors, with few mechanisms in place to ensure the sustained delivery of gender-sensitive services for displaced populations. Addressing these gaps required integrated gender and migration planning, institutional accountability, and targeted investments in health infrastructure that respond to the complex realities of displacement.
4.1.4. Structural Barriers to Inclusive Health Systems
Structural deficits—including chronic underfunding, governance weaknesses, restrictive immigration policies, and dependence on humanitarian assistance—continue to undermine the development of inclusive health systems across the DRC, Kenya, Somalia, and South Africa. The stakeholder interviews highlight how inconsistent protection, the securitisation of migration governance, and reliance on external support exacerbate the health vulnerabilities faced by displaced populations.
In the DRC, health service delivery for displaced populations remains heavily dependent on international humanitarian organisations and external funding. Government resources are insufficient to maintain healthcare facilities, particularly in conflict-affected provinces. As a DRC-based health provider observed,
“When humanitarian funding stops, the clinics for displaced people often close too.” (KII, DRC X)
National health budgets remain low, and coordination between humanitarian actors and state agencies is weak, leading to fragmented and unpredictable access to healthcare for IDPs and refugee communities [97].
Somalia faces profound structural challenges, including chronic political instability, fragmented governance between federal and member state authorities, and an extremely low health service coverage index. Health infrastructure remains severely underdeveloped, with IDP camps often lacking even basic healthcare services. Humanitarian assistance remains the cornerstone of service provision for displaced populations, but this dependence on volatile funding cycles is precarious. As one Somali official explained,
“It is impossible to implement our health plans fully because all our activities rely on funding from the donor community.” (KII, Somalia 06)
In Kenya, despite UHC reforms aiming to expand healthcare access, displaced populations remain marginalised by structural barriers. Documentation requirements under the Social Health Authority (SHA) system exclude many refugees and asylum seekers. The securitisation of migration through laws such as the Citizenship and Immigration Act (2012) and the Refugee Act (2021) reinforces administrative hurdles, often limiting healthcare access to those residing in designated refugee camps [93,113]. Overstretched public facilities, staffing shortages, and limited integration for urban refugees and undocumented migrants further restrict health access in practice.
South Africa’s healthcare system continues to reflect deep structural inequalities rooted in its two-tiered public-private division. Although the NHI seeks to unify service provision, the additional restrictions introduced for migrant groups compound the systemic barriers to access faced by displaced and undocumented migrants. Restrictive immigration laws, including the Refugees Amendment Act (2017), the Border Management Authority Act (2020) and the draft White Paper on Immigration have hardened access controls [114,115,116]. Despite constitutional protections, access often depends on frontline discretion. As a healthcare worker explained,
“Access depends on how you are treated at the facility, not on your rights.” (KII, SA, t06)
Therefore, the interplay of legal status, xenophobic attitudes, and administrative discretion creates a precarious environment for displaced individuals seeking healthcare services [82,117].
Across all four countries, chronic underfunding, fragmented governance, restrictive immigration regimes, and overreliance on humanitarian interventions systematically exclude displaced populations from equitable health access. Political instability in Somalia and the DRC, securitised migration governance in South Africa and Kenya, and the absence of cross-border health coordination further exacerbate systemic exclusion. Without comprehensive investments in public health infrastructure, inclusive health financing mechanisms, and deliberate regional cooperation, the goal of achieving UHC and fulfilling the right to health for displaced populations will remain out of reach.
The findings from South Africa, Kenya, Somalia, and the DRC illustrate persistent and systemic gaps between national policy commitments to health equity and the lived realities of displaced populations. Despite formal recognition of the right to health and public commitments to UHC, displaced communities continue to experience structural exclusion across all stages of displacement. Fragmented service delivery, weak migration-health integration, neglect of mental health needs, limited gender-sensitive programming, and chronic structural deficits undermine efforts to achieve inclusive health systems. The discussion below situates these findings within wider debates on the right to health, whole-of-route approaches, and the urgent need for rights-based, migration-aware health system reforms across Sub-Saharan Africa.
5. Conclusion
The SDGs envisage a “world with equitable and universal access…., to health care and social protection, where physical, mental and social well-being are assured” [1] (p3). Yet, with only five years remaining to the 2030 deadline, these ambitions remain out of reach for much of the global population. As demonstrated in this paper, displaced populations from the DRC and Somalia – whether moving within their countries of origin or along a well-established migration route to Kenya and South Africa – continue to face structural exclusion from national health systems, undermining their right to health.
Using a whole-of-route, rights-based approach, this paper has mapped how health vulnerabilities are (re)produced and sustained across time and space. Displaced populations face compounding exposure to violence (including GBV), instability, and policy exclusion that destabilise both physical and mental health outcomes of displaced populations [38,118]. Despite formal commitments to UHC and health equity, governance frameworks across the four countries consistently fail to deliver inclusive care for those on the move.
This paper concludes with three core messages that are critical to achieving the right to health for displaced populations across the eastern and southern African regions.
5.1. Disconnections and Contradictions Within and Between Governance Frameworks Undermine the Right to Health for Displaced Populations
Continental, regional and national efforts to address migration, health are often siloed, reactive and poorly coordinated [74]. At the national level, contradictory policy instruments and legislative frameworks frequently fail to translate constitutional guarantees into inclusive practice, particularly where legal status is used as a determinant of health entitlement [86]. These inconsistencies result in fragmented systems that exclude populations by design or default.
5.2. Rights-Based Approaches While Critical, Are Limited on Their Own
Although international frameworks call for the protection of health rights regardless of migration status (ICESCR 1966, African Charter 1981), the political realities of migration governance in many states reflect a shift towards securitisation, nationalism and citizen-focused health models [119]. As our findings show, placing rights front and centre in policy development does not automatically yield inclusive outcomes. Strategic, politically informed, and context-specific approaches are needed to reimagine how rights can be realised in practice.
5.3. Migration-Aware, Whole-of-Route Approaches Are Essential to Advance UHC and Uphold the Right to Health for Displaced People
Health systems in all four countries remain static, territorially bounded, and ill-equipped to address the cumulative and mobile nature of health vulnerabilities experienced by displaced populations [69]. Fragmented service delivery, particularly in refugee camps and IDP settlements, reinforce a humanitarian model of care that is short-term and unsustainable [120]. Genuinely inclusive UHC requires planning and financing mechanisms that recognise migration as a fundamental determinant of health, not an exception to it.
To achieve health for all and meet the goals of the 2030 Agenda, regional and national actors must shift from rhetoric to action. This requires coordinated, well-resourced, and migration-aware health systems that uphold the right to health for all- regardless of legal status, gender, or place of origin [121] Without this transformation, displaced populations will remain structurally excluded, and UHC will remain an unmet promise for some of the world’s most marginalised populations.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Governance frameworks shaping responses to migration, displacement and health; Figure S1: Democratic Republic of the Congo: overall country legislative and policy assessment towards migration, mental health, and gender aware health responses, including the right to access healthcare services; Figure S2: Somalia: overall country legislative and policy assessment towards migration, mental health, and gender aware health responses, including the right to access healthcare services; Figure S3: Kenya: overall country legislative and policy assessment towards migration, mental health, and gender aware health responses, including the right to access healthcare services; Figure S4: South Africa: overall country legislative and policy assessment towards migration, mental health, and gender aware health responses, including the right to access healthcare services.
Author Contributions
Conceptualization, R.W. and J.V.; methodology, R.W. and J.V.; formal analysis, R.W., J.V., A.B. and G.L.; investigation, R.W., J.V., A.B. and G.L.; resources, J.V.; data curation, R.W., J.V., A.B. and G.L.; writing—original draft preparation, R.W. and J.V.; writing—review and editing, R.W., J.V., A.B. and G.L.; visualization, R.W. and J.V.; supervision, R.W. and J.V.; project administration, R.W. and J.V.; funding acquisition, J.V. All authors have read and agreed to the published version of the manuscript.
Funding
The primary research presented was funded by the Economic and Social Research Council (ESRC) (UK) grant number ES/T004479/1 of which JV is a co-investigator. Further analysis was supported by the Gendered violence and poor mental health among migrants in precarious situations Global Health Research Group (GEMMS) co-Directed by JV and funded by the NIHR (grant ref: NIHR134629) using UK international development funding from the UK Government to support global health research. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the UK government.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Human Research Ethics Committee Non-Medical (HRECNM) of The University of the Witwatersrand. Protocol code HRECNM20-09-048, September 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The legislation, policies and frameworks identified and utilised in this paper can be found online: https://mighealth-policy-africa.org/.
Acknowledgments
The authors acknowledge the contributions of the seventy individuals who generously gave their time to the project, and wish to convey particular thanks for engaging with us during the difficult conditions associated with the height of the Covid19 pandemic, under which all participants were living and working. We acknowledge all team members involved in the DiSoCo project, specifically the Principle Investigator, Prof Laura Jeffry (PI) and Co-Investigators Professor Paulin Beya wa Bitadi Mutombo; Dr Joachim Osur; Dr Amina Jama Mahmud; Dr Jean-Benoit Falisse; Dr Lucy Lowe; and Professor Germaine Furaha Mirindi. The contributions of the team to the policy review work are acknowledged. We thank those who, with the co-authors of this manuscript, participated in a policy research workshop held in September 2023 at Wits University (organised and facilitated by JV and RW): (in alphabetical order): Mohamed Abdullahi Ali-Salad; Lydia Atambo; Clayton Boeynik; Dostin Lakika; Prisca Lusadiameso; Tackson Makandwa; Paulin Mutombo Beya; and Anya Sass. We thank Anya Sass for her contributions to the research project, including development of the graphics included as supplementary material; Craig Parker for producing the map presented in Figure 1; and, Lenore Longwe and Sisanda Gqoboka of the ACMS, Wits for their administrative support.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- UN Transforming Our World: The 2030 Agenda for Sustainable Development. A/RES/70/1 2015.
- Sachs, J.D.; Lafortune, G.; Fuller, G. The SDGs and the UN Summit of the Future: Sustainable Development Report 2024; Dublin University Press: Dublin, 2024. [Google Scholar]
- Mosler Vidal, E. Leave No Migrant Behind: The 2030 Agenda and Data Disaggregation; International Organization for Migration (IOM): Geneva, 2021. [Google Scholar]
- IOM Glossary on Migration; International Organization for Migration: Geneva, 2019.
- UNHCR Asylum-Seekers. Available online: https://www.unhcr.org/about-unhcr/who-we-protect/asylum-seekers (accessed on 28 April 2025).
- UNHCR Refugees. Available online: https://www.unhcr.org/about-unhcr/who-we-protect/refugees (accessed on 28 April 2025).
- OHCHR About Internally Displaced Persons. Available online: https://www.ohchr.org/en/special-procedures/sr-internally-displaced-persons/about-internally-displaced-persons (accessed on 28 April 2025).
- ODI Migration and the 2030 Agenda for Sustainable Development; Overseas Development Institute: London, 2017.
- Adger, W.N.; Fransen, S.; Safra de Campos, R.; Clark, W.C. Migration and Sustainable Development. Proc. Natl. Acad. Sci. 2024, 121, e2206193121. [Google Scholar] [CrossRef] [PubMed]
- Adger, W.N.; Boyd, E.; Fábos, A.; Fransen, S.; Jolivet, D.; Neville, G.; Campos, R.S. de; Vijge, M.J. Migration Transforms the Conditions for the Achievement of the Sustainable Development Goals. Lancet Planet. Health 2019, 3, e440–e442. [Google Scholar] [CrossRef] [PubMed]
- Mosler Vidal, E.; Laczko, F. Migration and the SDGs: Measuring Progress – An Edited Volume; International Organization for Migration (IOM): Geneva, 2022. [Google Scholar]
- IOM. Migration and the 2030 Agenda. A Guide for Practitioners; IOM: Geneva, 2018. [Google Scholar]
- United Nations Global Compact for Safe, Orderly and Regular Migration - A/RES/73/195 2018.
- United Nations Global Compact on Refugees - A/73/12 2018.
- UNHCR How the SDGs and the GCR Are Aligned; United Nations High Commissioner for Refugees: Geneva, undated.
- Oelgemöller, C. The Global Compacts, Mixed Migration and the Transformation of Protection. Interventions 2021, 23, 183–190. [Google Scholar] [CrossRef]
- Maple, N.; Reardon-Smith, S.; Black, R. Immobility and the Containment of Solutions: Reflections on the Global Compacts, Mixed Migration and the Transformation of Protection. Interventions 2021, 23, 326–347. [Google Scholar] [CrossRef]
- Pécoud, A. Narrating an Ideal Migration World? An Analysis of the Global Compact for Safe, Orderly and Regular Migration. Third World Q. 2021, 42, 16–33. [Google Scholar] [CrossRef]
- Nanopoulos, E.; Guild, E.; Weatherhead, K. Securitisation of Borders and the UN’s Global Compact on Safe, Orderly and Regular Migration; Social Science Research Network: Rochester, NY, 2018. [Google Scholar]
- Abubakar, I.; Zumla, A. Universal Health Coverage for Refugees and Migrants in the Twenty-Firs t Century. BMC Med. 2018, 16, 216–s12916. [Google Scholar] [CrossRef]
- Al-Oraibi, A.; Martin, C.A.; Hassan, O.; Wickramage, K.; Nellums, L.B.; Pareek, M. Migrant Health Is Public Health: A Call for Equitable Access to COVID- 19 Vaccines. Lancet Public Health 2021, 6, e144. [Google Scholar] [CrossRef]
- Barragan, E.; Dhavan, P.; Fortier, J.P.; Mosca, D.; Weekers, J.; Wickramage, K.P. Migration and Health in the Sustainable Development Goals. Migr. 2030 Agenda 2017. [Google Scholar]
- Bartovic, J.; Datta, S.S.; Severoni, S.; D’Anna, V. Ensuring Equitable Access to Vaccines for Refugees and Migrants during the COVID-19 Pandemic. Bull. World Health Organ. 2021, 99, 3–3A. [Google Scholar] [CrossRef]
- IOM Recommendations on Access to Health Services for Migrants in an Irregu Lar Situation: An Expert Consensus. 2016.
- IOM. Migration Health in the Sustainable Development Goals: ‘Leave No One B Ehind’ in an Increasingly Mobile Society; IOM MIGRATION HEALTH DIVISION: Position Paper; IOM: Geneva, 2017. [Google Scholar]
- IOM. Migrants’ Right to Health – Legal and Policy Instruments Related to Mi Grants’ Access to Health Care, Social Protection and Labour in Selecte d East African Countries; International Organization for Migration: Geneva, 2023. [Google Scholar]
- Legido-Quigley, H.; Pocock, N.; Tan, S.T.; Pajin, L.; Suphanchaimat, R.; Wickramage, K.; McKee, M.; Pottie, K. Healthcare Is Not Universal If Undocumented Migrants Are Excluded. BMJ 2019, 366, l4160. [Google Scholar] [CrossRef]
- Mosca, D.T.; Vearey, J.; Orcutt, M.; Zwi, A.B. Universal Health Coverage: Ensuring Migrants and Migration Are Include d. Glob. Soc. Policy 2020, 20, 247–253. [Google Scholar] [CrossRef]
- Onarheim, K.H.; Melberg, A.; Meier, B.M.; Miljeteig, I. Towards Universal Health Coverage: Including Undocumented Migrants. BMJ Glob. Health 2018, 3, e001031. [Google Scholar] [CrossRef] [PubMed]
- Tulloch, O.; Machingura, F.; Melamed, C. Health, Migration and the 2030 Agenda for Sustainable Development; Overseas Development Institute: London, 2016. [Google Scholar]
- Vearey, J.; Hui, C.; Wickramage, K. Chapter 7. Migration and Health: Current Issues, Governance and Knowle Dge Gaps’. In WORLD MIGRATION REPORT; 2020; p. 38.
- Wickramage, K.; Vearey, J.; Zwi, A.B.; Robinson, C.; Knipper, M. Migration and Health: A Global Public Health Research Priority. BMC Public Health 2018, 18, 987. [Google Scholar] [CrossRef] [PubMed]
- Zumla, A. Universal Health Coverage for Refugees and Migrants in the Twenty-Firs t Century. PubMed Cent. 2018. [Google Scholar] [CrossRef]
- IOM Recommendations on Access to Health Services for Migrants in an Irregular Situation: An Expert Consensus 2016.
- Adnan, S.A. Barriers to Healthcare Access by Undocumented Migrants in Low-and Middle-Income Countries: A Qualitative Systematic Review. 2023.
- Adrian Parra, C.; Stuardo Ávila, V.; Contreras Hernández, P.; Quirland Lazo, C.; Bustos Ibarra, C.; Carrasco-Portiño, M.; Belmar Prieto, J.; Barrientos, J.; Lisboa Donoso, C.; Low Andrade, K. Structural and Intermediary Determinants in Sexual Health Care Access in Migrant Populations: A Scoping Review. Public Health 2024, 227, 54–62. [Google Scholar] [CrossRef]
- WHO. Common Health Needs of Refugees and Migrants: Literature Review; WHO: Geneva, 2021. [Google Scholar]
- World Health Organization World Report on the Health of Refugees and Migrants; World Health Organization: Geneva, 2022; ISBN 978-92-4-005446-2.
- Viruell-Fuentes, E.A.; Miranda, P.Y.; Abdulrahim, S. More than Culture: Structural Racism, Intersectionality Theory, and Immigrant Health. Soc. Sci. Med. 2012, 75, 2099–2106. [Google Scholar] [CrossRef]
- Carruth, L.; Martinez, C.; Smith, L.; Donato, K.; Piñones-Rivera, C.; Quesada, J. Structural Vulnerability: Migration and Health in Social Context. BMJ Glob. Health 2021, 6, e005109. [Google Scholar] [CrossRef]
- Willen, S.S.; Knipper, M.; Abadía-Barrero, C.E.; Davidovitch, N. Syndemic Vulnerability and the Right to Health. The Lancet 2017, 389, 964–977. [Google Scholar] [CrossRef]
- Ormond, M.; Lunt, N. Transnational Medical Travel: Patient Mobility, Shifting Health System Entitlements and Attachments. J. Ethn. Migr. Stud. 2019, 0, 1–14. [Google Scholar] [CrossRef]
- Cuadrado, C.; Libuy, M.; Moreno-Serra, R. What Is the Impact of Forced Displacement on Health? A Scoping Review. Health Policy Plan. 2023, 38, 394–408. [Google Scholar] [CrossRef]
- Larchanché, S. Intangible Obstacles: Health Implications of Stigmatization, Structural Violence, and Fear among Undocumented Immigrants in France. Soc. Sci. Med. 2012, 74, 858–863. [Google Scholar] [CrossRef] [PubMed]
- Abbas, M.; Aloudat, T.; Bartolomei, J.; Carballo, M.; Durieux-Paillard, S.; Gabus, L.; Jablonka, A.; Jackson, Y.; Kaojaroen, K.; Koch, D.; et al. Migrant and Refugee Populations: A Public Health and Policy Perspective on a Continuing Global Crisis. Antimicrob. Resist. Infect. Control 2018, 7, 113. [Google Scholar] [CrossRef] [PubMed]
- Abubakar, I.; Aldridge, R.W.; Devakumar, D.; Orcutt, M.; Burns, R.; Barreto, M.L.; Dhavan, P.; Fouad, F.M.; Groce, N.; Guo, Y.; et al. The UCL–Lancet Commission on Migration and Health: The Health of a World on the Move. The Lancet 2018, 392, 2606–2654. [Google Scholar] [CrossRef] [PubMed]
- Castañeda, H.; Holmes, S.M.; Madrigal, D.S.; Young, M.-E.D.; Beyeler, N.; Quesada, J. Immigration as a Social Determinant of Health. Annu. Rev. Public Health 2015, 36, 375–392. [Google Scholar] [CrossRef]
- Castañeda, H.; Holmes, S.M.; Madrigal, D.S.; Young, M.-E.D.; Beyeler, N.; Quesada, J. Immigration as a Social Determinant of Health. Annu. Rev. Public Health 2015, 36, 375–392. [Google Scholar] [CrossRef]
- Davies, A.; Basten, A.; Frattini, C. Migration: A Social Determinant of Migrants’ Health. Migr. Health Eur. Union 2010, 16, 10–12. [Google Scholar]
- Ingleby, D. Ethnicity, Migration and the ‘Social Determinants of Health’ Agenda*. Psychosoc. Interv. 2012, 21, 331–341. [Google Scholar] [CrossRef]
- Hou, W.K.; Liu, H.; Liang, L.; Ho, J.; Kim, H.; Seong, E.; Bonanno, G.A.; Hobfoll, S.E.; Hall, B.J. Everyday Life Experiences and Mental Health among Conflict-Affected Forced Migrants: A Meta-Analysis. J. Affect. Disord. 2020, 264, 50–68. [Google Scholar] [CrossRef]
- World Health Organization Mental Health of Refugees and Migrants: Risk and Protective Factors and Access to Care. ; Global Evidence Review on Health and Migration (GEHM) series; World Health Organization: Geneva, 2023. [Google Scholar]
- Elshahat, S.; Moffat, T.; Newbold, K.B. Understanding the Healthy Immigrant Effect in the Context of Mental Health Challenges: A Systematic Critical Review. J. Immigr. Minor. Health 2022, 24, 1564–1579. [Google Scholar] [CrossRef]
- Siriwardhana, C.; Ali, S.; Roberts, B.; Stewart, R. A Systematic Review of Resilience and Mental Health Outcomes of Conflict-Driven Adult Forced Migrants’. Confl. Health 2014. [Google Scholar] [CrossRef]
- Sangaramoorthy, T.; Carney, M.A. Immigration, Mental Health and Psychosocial Well-Being. Med. Anthropol. 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Li, S.S.Y.; Liddell, B.J.; Nickerson, A. The Relationship Between Post-Migration Stress and Psychological Disorders in Refugees and Asylum Seekers. Curr. Psychiatry Rep. 2016, 18, 82. [Google Scholar] [CrossRef] [PubMed]
- Abu Suhaiban, H.; Grasser, L.R.; Javanbakht, A. Mental Health of Refugees and Torture Survivors: A Critical Review of Prevalence, Predictors, and Integrated Care. Int. J. Environ. Res. Public. Health 2019, 16. [Google Scholar] [CrossRef] [PubMed]
- IOM. Migrants’ Right to Health – Legal and Policy Instruments Related to Migrants’ Access to Health Care, Social Protection and Labour in Selected East African Countries; International Organization for Migration: Geneva, 2023. [Google Scholar]
- Vearey, J. Migration and Health in the WHO-AFRO Region: A Scoping Review’; ACMS, WITS University & World Health Organization: Johannesburg, 2023. [Google Scholar]
- Lokotola, C.L.; Mash, R.; Sethlare, V.; Shabani, J.; Temitope, I.; Baldwin-Ragaven, L. Migration and Primary Healthcare in Sub-Saharan Africa: A Scoping Review. Afr. J. Prim. Health Care Fam. Med. 2024, 16, 4507. [Google Scholar] [CrossRef]
- Mutiso, V.; Warsame, A.H.; Bosire, E.; Musyimi, C.; Musau, A.; Isse, M.M.; Ndetei, D.M. Intrigues of Accessing Mental Health Services Among Urban Refugees Living in Kenya: The Case of Somali Refugees Living in Eastleigh, Nairobi. J. Immigr. Refug. Stud. 2019, 17, 204–221. [Google Scholar] [CrossRef]
- Hossain, M.; Pearson, R.J.; McAlpine, A.; Bacchus, L.J.; Spangaro, J.; Muthuri, S.; Muuo, S.; Franchi, G.; Hess, T.; Bangha, M.; et al. Gender-Based Violence and Its Association with Mental Health among Somali Women in a Kenyan Refugee Camp: A Latent Class Analysis. J. Epidemiol. Community Health 2021, 75, 327–334. [Google Scholar] [CrossRef]
- Im, H.; Ferguson, A.B.; Warsame, A.H.; Isse, M.M. Mental Health Risks and Stressors Faced by Urban Refugees: Perceived Impacts of War and Community Adversities among Somali Refugees in Nairobi. Int. J. Soc. Psychiatry 2017, 63, 686–693. [Google Scholar] [CrossRef]
- Im, H.; Swan, L.E.; Warsame, A.H.; Isse, M.M. Risk and Protective Factors for Comorbidity of PTSD, Depression, and Anxiety among Somali Refugees in Kenya. Int. J. Soc. Psychiatry 2020, 0020764020978685. [Google Scholar] [CrossRef]
- Im, H.; Ferguson, A.; Hunter, M. Cultural Translation of Refugee Trauma: Cultural Idioms of Distress among Somali Refugees in Displacement. Transcult. Psychiatry 2017, 54, 626–652. [Google Scholar] [CrossRef]
- JINNAH, Z. Cultural Causations and Expressions of Distress: A Case Study of Buufis Amongst Somalis in Johannesburg. Urban Forum 2017, 28, 111–123. [Google Scholar] [CrossRef]
- Sharma, V.; Amobi, A.; Tewolde, S.; Deyessa, N.; Scott, J. Displacement-Related Factors Influencing Marital Practices and Associated Intimate Partner Violence Risk among Somali Refugees in Dollo Ado, Ethiopia: A Qualitative Study. Confl. Health 2020, 14, 17. [Google Scholar] [CrossRef] [PubMed]
- Swan, L.E.T.; Im, H. Risk and Protective Factors for Common Mental Disorders among Urban Somali Refugee Youth. J. Child Adolesc. Trauma 2020. [Google Scholar] [CrossRef] [PubMed]
- The United Nations Refugee Agency (UNHCR) A Route-Based Approach: Strengthening Protection and Solutions in the Context of Mixed Movements of Refugees and Migrants; 2024.
- Mobilizing Global Knowledge: Refugee Research in an Age of Displacement; Mcgrath, S., Young, J.E.E., Eds.; 1st ed.; University of Calgary Press, 2019; ISBN 978-1-77385-087-0.
- United Nations. International Covenant on Economic, Social and Cultural Rights (ICESCR); United Nations: New York, 1966. [Google Scholar]
- Correa-Agudelo, E.; Kim, H.-Y.; Musuka, G.N.; Mukandavire, Z.; Akullian, A.; Cuadros, D.F. Associated Health and Social Determinants of Mobile Populations across HIV Epidemic Gradients in Southern Africa. J. Migr. Health 2021, 3, 100038. [Google Scholar] [CrossRef]
- Vearey, J Legislation, Policy and Frameworks Relating to Migration and Health in South Africa. April 2025.; Governing migration & health in Africa: review series; African Centre for Migration & Society (ACMS), University of the Witwatersrand: Johannebsurg, 2025.
- IOM; ACMS, Wits. Migrants Rights to Health. A Legislative and Policy Review for Southern Africa; IOM and the African Centre for Migration and Society, WITS University: Pretoria, 2022. [Google Scholar]
- Sonke Gender Justice Gender, Migration and Health in SADC: A Focus on Women and Girls; Sonke Gender Justice: Johannesburg, 2019;
- African Union African Union Convention for the Protection and Assistance of Internally Displaced Persons in Africa (Kampala Convention) | African Union 2009.
- UNHCR 2009 Kampala Convention on IDPs 2019.
- Somalia Country Profile. Available online: https://mighealth-policy-africa.org/country-profile-somalia/ (accessed on 30 April 2025).
- DEMOCRATIC REPUBLIC OF CONGO (DRC). Gov. Migr. Health Afr. 2023.
- KENYA. Gov. Migr. Health Afr. 2023.
- SOUTH AFRICA. Gov. Migr. Health Afr. 2023.
- Walker, R.; Vearey, J. “Let’s Manage the Stressor Today” Exploring the Mental Health Response to Forced Migrants in Johannesburg, South Africa. Int. J. Migr. Health Soc. Care 2022. [Google Scholar] [CrossRef]
- De Gruchy, T.; Vearey, J.; Datta, K.; Chase, E.; Musariri, L. The “covidisation” of Migration and Health Research: Understanding the Implications of the Pandemic for the Field. In Research Handbook on Migration, Gender, and COVID-19; McAuliffe, M., Bauloz, C., Eds.; Edward Elgar Publishing, 2024; pp. 34–47 ISBN 978-1-80220-867-2.
- de Gruchy, T.; Vearey, J.; Datta, K.; Chase, E.; Musariri, L.; Tummers, H. ‘Great Leveler’? Covid-19’s Impact on Migration and Health Research. the Polyphony 2021.
- Walker, R.; Vearey, J. Behind the Masks: Mental Health, Marginalisation and COVID-19’, The Polyphony 2021.
- Walker, R.; Vearey, J. “Let’s Manage the Stressor Today” Exploring the Mental Health Response to Forced Migrants in Johannesburg, South Africa. Int. J. Migr. Health Soc. Care 2023, 19, 1–15. [Google Scholar] [CrossRef]
- Maple, N.; Walker, R.; Vearey, J. Covid-19 and Migration Governance in Africa; Researching Migration & Coronavirus in Southern Africa (MiCoSA): Occasional Paper; African Centre for Migration & Society, University of the Witwatersrand: Johannebsurg, 2021.
- Vearey, J.; de Gruchy, T.; Maple, N. Global Health (Security), Immigration Governance and Covid-19 in South(Ern) Africa: An Evolving Research Agenda. J. Migr. Health 2021, 3, 100040. [Google Scholar] [CrossRef]
- Walker, R.; Maple, N.; Vearey, J. Migrants & the Covid-19 Vaccine Roll-Out in Africa: Hesitancy & Exclusion; African Centre for Migration & Society, University of the Witwatersrand: Johannesburg, 2021. [Google Scholar]
- Vearey, J. Global and Regional Governance Frameworks Shaping Responses to Migration, Displacement and Health in the African Union and the Eastern and Southern African Regions. April 2025 2025.
- The Government of the Republic of South Africa The National Health Insurance Act 20 of 2023 2023.
- SALC SALC Submissions on the South African National Health Insurance Bill (NHI). Available online: https://www.southernafricalitigationcentre.org/2019/11/28/salc-submissions-on-the-south-african-national-health-insurance-bill-nhi/ (accessed on 9 May 2023).
- Government of the Republic of Kenya The Refugee Act 2021. No. 1o If 21 2021.
- Ministry of Public Health National Health Development Plan 2019-2022: Towards Universal Health Coverage 2019.
- Ministry of Public Health Strategy for Strengthening the System of Health 2006.
- Boeyink, C.; Ali-Salad, M.A.; Baruti, E.W.; Bile, A.S.; Falisse, J.-B.; Kazamwali, L.M.; Mohamoud, S.A.; Muganza, H.N.; Mukwege, D.M.; Mahmud, A.J. Pathways to Care: IDPs Seeking Health Support and Justice for Sexual and Gender-Based Violence through Social Connections in Garowe and Kismayo, Somalia and South Kivu, DRC. J. Migr. Health 2022, 6, 100129. [Google Scholar] [CrossRef]
- Mutombo, P.B.W.B.; Lobukulu, G.L.; Walker, R. Mental Healthcare among Displaced Congolese: Policy and Stakeholders’ Analysis. Front. Hum. Dyn. 2024, 5, 1273937. [Google Scholar] [CrossRef]
- International Organization for Migration (IOM) The DRC: Internal Displacement Overview 2024. Available online: https://drcongo.iom.int/en/news/internal-displacement-overview-2024-published (accessed on 24 April 2025).
- Federal Republic of Somalia Essential Package of Health Services (EPHS), Somalia, 2020 2020.
- Federal Republic of Somalia Somali Roadmap Towards Universal Health Coverage (2019-2023) 2018.
- National Department of Health The National Strategic Plan for HIV, TB and STIs 2023-2028 2023.
- The Republic of South Africa The Republic of South Africa National Health Act No. 61 of 2003 2003.
- UHC2030 Action on Health Systems, for Universal Health Coverage and Health Security A UHC2030 Strategic Narrative to Guide Advocacy and Action; 2022.
- Ridde, V.; Ramel, P. The Migrant Crisis and Health Systems: Hygeia Instead of Panacea. Lancet Public Health 2017, 2, e447. [Google Scholar] [CrossRef]
- Mills, C. From “Invisible Problem” to Global Priority: The Inclusion of Mental Health in the Sustainable Development Goals. Dev. Change 2018, 49, 843–866. [Google Scholar] [CrossRef]
- UN United Nations Population Fund Country Programme Document for Democratic Republic of the Congo. DP/FPA/CPD/COD/6; Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services: New York, 2024;
- Mukala Mayoyo, E.; Chenge, F.; Sow, A.; Criel, B.; Michielsen, J.; Van den Broeck, K.; Coppieters, Y. Health System Facilitators and Barriers to the Integration of Mental Health Services into Primary Care in the Democratic Republic of the Congo: A Multimethod Study. BMC Prim. Care 2024, 25, 214. [Google Scholar] [CrossRef]
- SOMALIA. Gov. Migr. Health Afr. 2023.
- Ministry of Health, Kenya Kenya Mental Health Policy 2015 - 2030 2015.
- Ministry of Health, Kenya Mental Health Act 2012 2012.
- Nwoke, C.C.; Cochrane, L. Systematic Review of Gender and Humanitarian Situations Across Africa. Afr. Spectr. 2022, 57, 301–326. [Google Scholar] [CrossRef]
- The Republic of South Africa Promotion of Equality and Prevention of Unfair Discrimination Act 4 of 2000 (as Amended in 2002, 2003, 2005, 2008) 2000.
- Government of the Republic of Kenya The Kenya Citizenship and Immigration Act, 2011. No. 12 of 2011 2011.
- The Republic of South Africa Refugees Amendment Act No.11 of 2017 2017.
- Republic of South Africa Act No. 2 of 2020: Border Management Act, 2020 2020.
- Department of Home Affairs, Republic of South Africa White Paper On Citizenship, Immigration and Refugee Protection: Towards a Complete Overhaul of the Migration System in South Africa. 2024.
- Walker, R. Migration, Trauma and Wellbeing: Exploring the Impact of Violence within the Healthcare System on Refugee Women in South Africa,. In Mobilities of Wellbeing: Migration, the State and Medical Knowledge; Carolina Academic Press, 2021.
- Castañeda, H.; Holmes, S.M.; Madrigal, D.S.; Young, M.-E.D.; Beyeler, N.; Quesada, J. Immigration as a Social Determinant of Health. Annu. Rev. Public Health 2015, 36, 375–392. [Google Scholar] [CrossRef] [PubMed]
- Vearey, J.; de Gruchy, T.; Maple, N. Global Health (Security), Immigration Governance and Covid-19 in South(Ern) Africa: An Evolving Research Agenda. J. Migr. Health 2021, 3, 100040. [Google Scholar] [CrossRef] [PubMed]
- International Organisation of Migration Rights-Based Approach to Migration Governance; 2024.
- Castañeda, H.; Holmes, S.M.; Madrigal, D.S.; Young, M.-E.D.; Beyeler, N.; Quesada, J. Immigration as a Social Determinant of Health. Annu. Rev. Public Health 2015, 36, 375–392. [Google Scholar] [CrossRef]
| 1 | The 2030 Agenda “is grounded in the Universal Declaration of Human Rights, international human rights treaties, the Millennium Declaration and the 2005 World Summit Outcome. It is informed by other instruments such as the Declaration on the Right to Development.” [1] |
| 2 | In this paper, we apply the following definitions: migrant - “An umbrella term, not defined under international law, reflecting the common lay understanding of a person who moves away from his or her place of usual residence, whether within a country or across an international border, temporarily or permanently, and for a variety of reasons. The term includes a number of well-defined legal categories of people, such as migrant workers; persons whose particular types of movements are legally defined, such as smuggled migrants; as well as those whose status or means of movement are not specifically defined under international law, such as international students” [4]; asylum seeker: “someone who intends to seek or is awaiting a decision on their request for international protection. In some countries, it is used as a legal term for a person who has applied for refugee status and has not yet received a final decision on their claim [5]; refugee - a person who "owing to well-founded fear of being persecuted for reasons of race, religion, nationality, membership of a particular social group or political opinion, is outside the country of [their] nationality and is unable or, owing to such fear, is unwilling to avail [themself] of the protection of that country" [6]; internally Displaced People (IDP): "persons or groups of persons who have been forced or obliged to flee or to leave their homes or places of habitual residence, in particular as a result of or in order to avoid the effects of armed conflict, situations of generalized violence, violations of human rights or natural or human-made disasters, and who have not crossed an internationally recognized border"[7]. |
| 3 | In this paper, we define an undocumented migrant as a foreign-born person who is currently in a country without the valid legal authorisation enter, live or work in that country. |
| 4 | In this paper, SEA refers to: the Southern African Development Community (SADC), East African Community (EAC) and the Intergovernmental Authority on Development (IGAD). |
| 5 | DiSoCo involved collaboration between (in alphabetical order): Amref International University (Kenya); ARQ International
(Netherlands); the Kinshasa School of Public Health (DRC); Panzi Foundation (DRC); Queen Margaret University (UK);
Somali Institute for Development and Research (Somalia); Université Evangélique en Afrique (DRC); the University of
Edinburgh (UK); and, the University of the Witwatersrand (South Africa). DiSoCo is a GCRF Protracted
Displacement project that aims to help Somali and Congolese displaced people to access appropriate healthcare for chronic
mental health conditions associated with protracted displacement, conflict, and sexual and gender‐based violence. DiSoCo is
a multi‐sited project focusing on Somali and Congolese Internally Displaced People (IDPs) in Somalia and Eastern DRC
respectively, and Somali and Congolese refugees and asylum seekers in Kenya and South Africa. The DiSoCo team brings
together researchers and practitioners from international development, migration studies, gender studies, medical
anthropology, public health and health policy, and medical sciences to undertake interdisciplinary empirical research in
these protracted displacement contexts. https://displacement.sps.ed.ac.uk/
|
| 6 | The Gendered violence and poor mental health among migrants in precarious situations Global Health Research Group (GEMMS) is supported by the NIHR (grant ref: NIHR134629). GEMMS involves collaboration between (in alphabetical order): Africa University (Zimbabwe); the African Centre for Migration & Society (ACMS), University of the Witwatersrand (South Africa); Health Poverty Action (HPA; Cambodia, Zimbabwe and UK); Oxford University (UK); the Tata Institute for Social Sciences (TISS, India); Towards Sustainable Use of Resources Organization (TSURO) Trust (Zimbabwe); University of Essex (UK); and, the University of Johannesburg (South Africa). https://gemms-research.org/
|
| 7 | |
| 8 | |
| 9 | |
| 10 | “Right to Health” here refers to the right to access healthcare. |
Figure 1.
Movements of displaced people from the DRC and Somalia often follow an established migratory pathway connecting Kenya and South Africa.
Figure 1.
Movements of displaced people from the DRC and Somalia often follow an established migratory pathway connecting Kenya and South Africa.
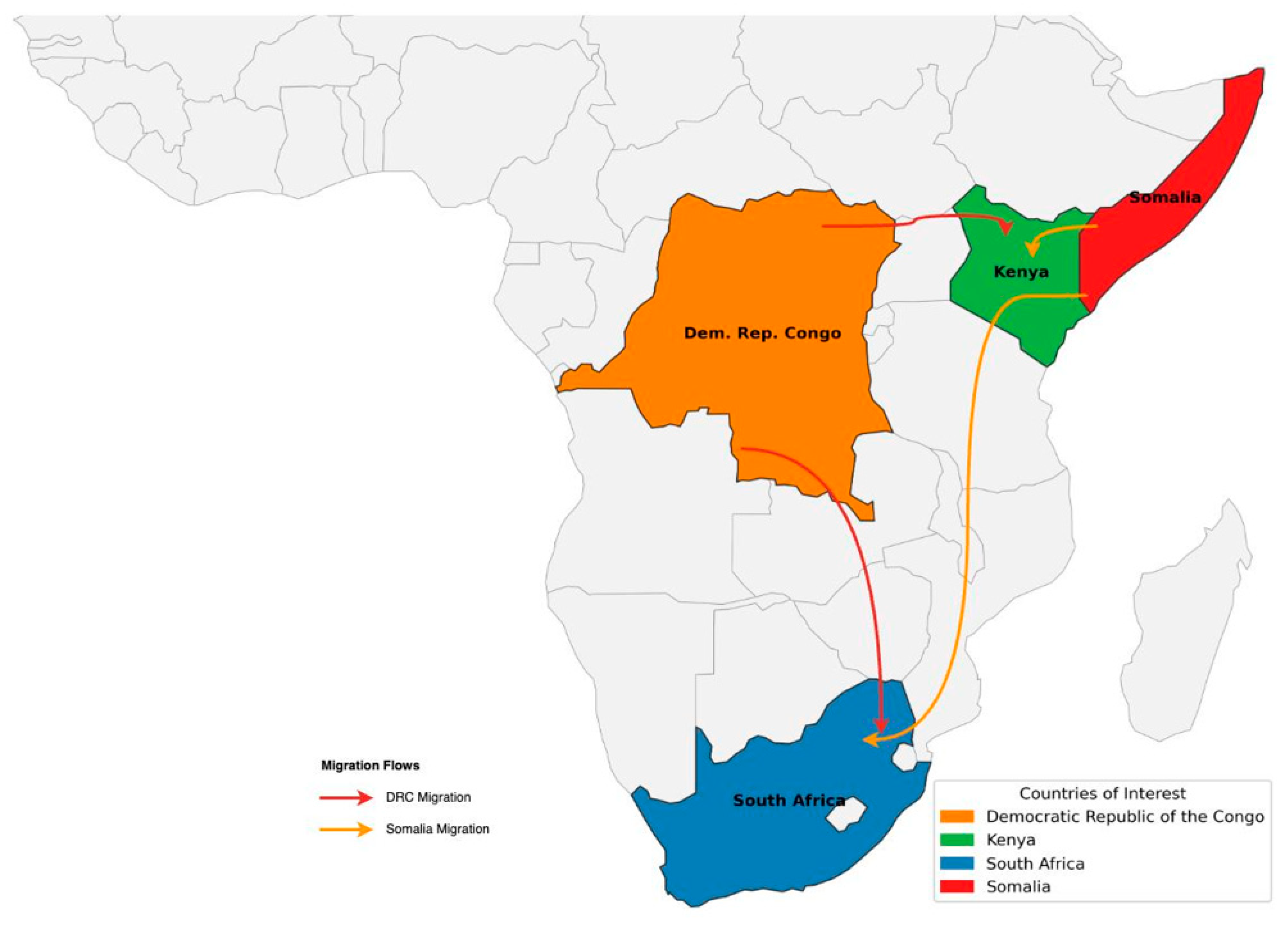
Figure 2.
Analysis framework.
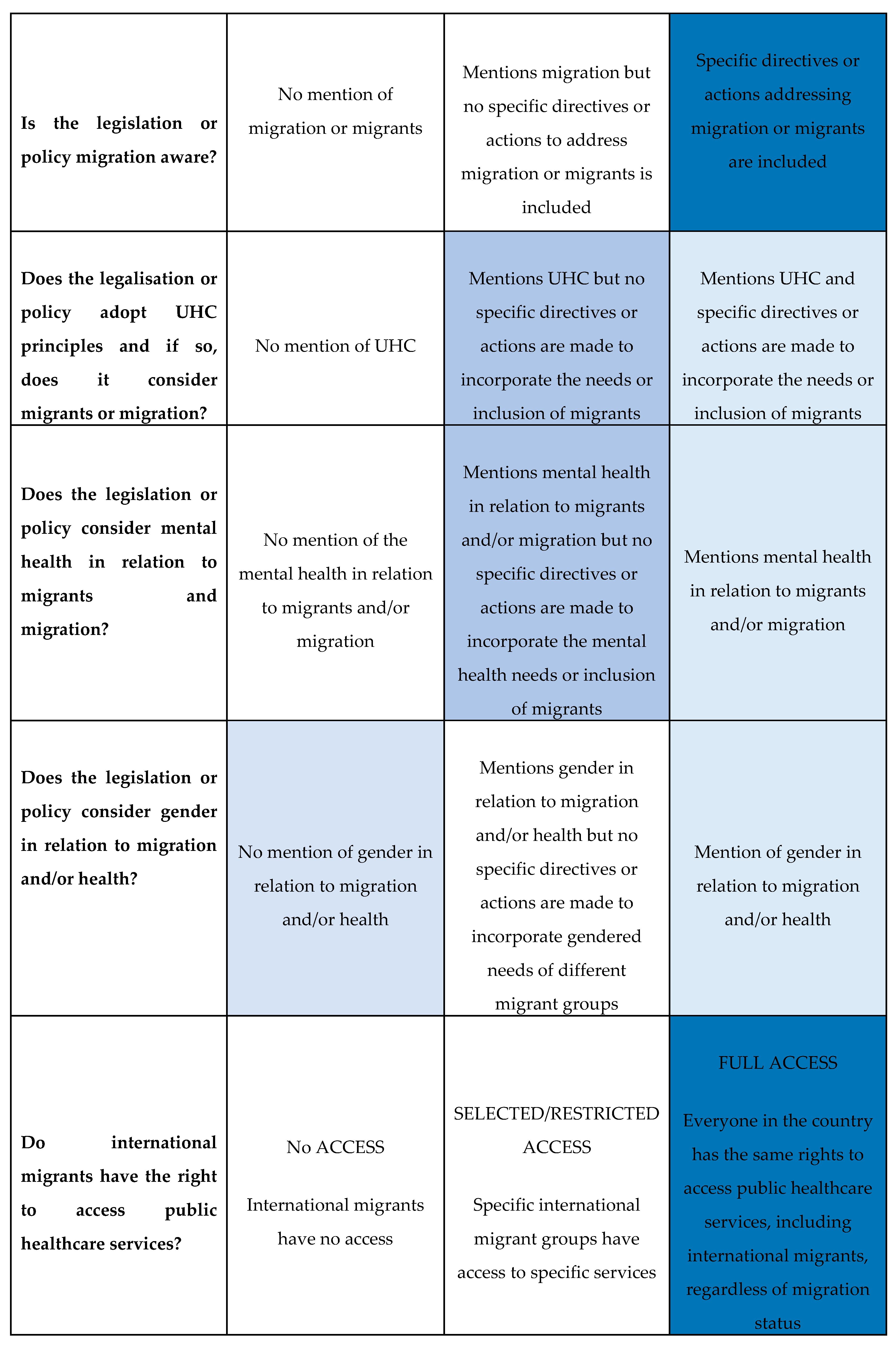
Figure 3.
Cross-comparison of the four countries.
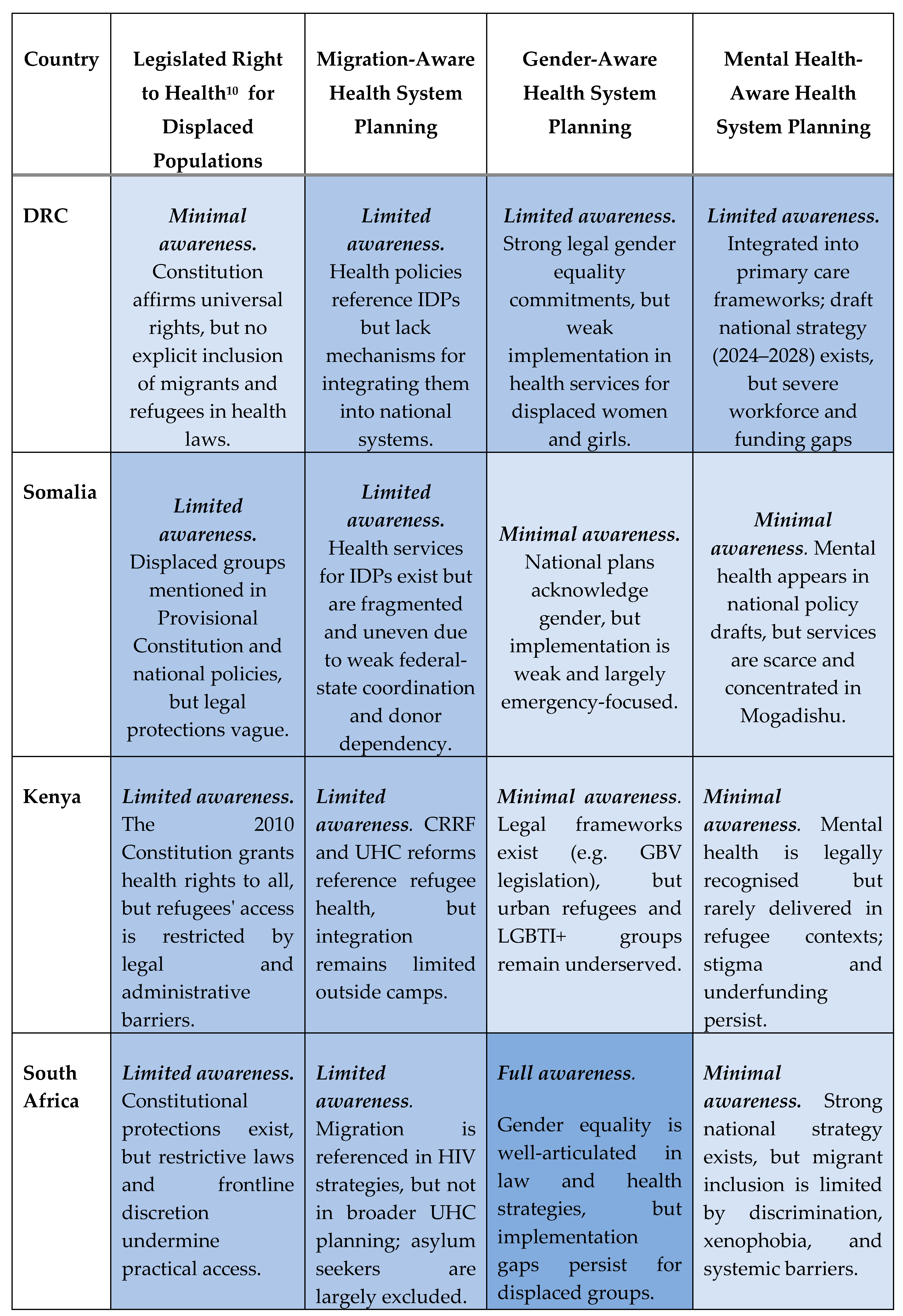
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



