
Submitted:
12 November 2024
Posted:
14 November 2024
You are already at the latest version
Abstract
Objective: Food-borne trematodiases are a group of parasitic diseases primarily transmitted to humans via the consumption of raw or undercooked aquatic products. This study aims to assess the prevalence of and disability-adjusted life years (DALYs) due to food-borne trematodiases in China from 1990 to 2021 and to project the DALYs up to 2035.
Methods: Data for this study were obtained from the Global Burden of Disease Study (GBD) 2021. Temporal trends of age-standardized and age-specific prevalence and DALY rates were quantified using the estimated annual percentage change (EAPC). A Bayesian age-period-cohort (BAPC) model was applied to project DALY counts and rates through 2035.
Results: In 2021, the estimated number of prevalent cases of food-borne trematodiases in China was 33.32 million (95% uncertainty interval (UI): 29.25–38.35 million), contributing to 768,297.4 DALYs (95% UI: 383,882.8–1,367,826.1). From 1990 to 2021, the number of prevalent cases and DALYs declined by 9.02% and 18.11%, respectively. The age-standardized prevalence and DALY rates also showed downward trends (EAPC: -0.96 and -1.21, respectively). Higher prevalence and DALY rates were consistently observed in males compared with females. By age, the middle-aged group bore the highest burden, while the older population showed the most rapid increase in the number of prevalent cases and DALYs. Projected DALYs and DALY rate remain stable through 2035.
Conclusions: The burden of food-borne trematodiases in China declined from 1990 to 2021, but prevalence remains high, and it contributed considerably to disability and premature death. This study also revealed gender and age disparities in the burden of this disease. Continued control efforts and targeted interventions are essential to further reducing the burden of food-borne trematodiases in China.
Keywords:
food-borne trematodiases
; Global Burden of Disease
; China
; disability-adjusted life years
; prevalence
1. Introduction
Food-borne trematodiases are infections caused by trematodes transmitted to humans primarily through the consumption of raw or undercooked fish, crustaceans, or aquatic plants. These trematodes are classified into liver, lung, or intestinal flukes based on the organs they target in the host[1,2]. Although over 80 species of food-borne trematodes have been identified as causing human infections, only a few are of public health importance[3]. The World Health Organization (WHO) has identified four genera with the highest public health burden: Clonorchis and Opisthorchis (liver flukes), Paragonimus (lung fluke), and Fasciola (intestinal fluke)[4].
Infections with food-borne trematodiases are often asymptomatic, and when symptoms do occur, they are usually non-specific[5]. Current diagnostic techniques rely largely on microscopic detection of eggs in feces, sputum, or other biofluids, which is of suboptimal effectiveness and incapable of species-specific distinction[6,7]. These diagnostic limitations, along with the wide range of trematode species and the often non-specific symptoms, lead to underestimation of the burden of food-borne trematodiases, which continue to be classified as neglected tropical diseases (NTDs). Although being neglected, food-borne trematodiases can lead to serious consequences, including cholangiocarcinoma and ectopic infections[2]. According to the WHO Foodborne Disease Burden Epidemiology Reference Group [2015], the four above-mentioned genera of food-borne trematodes collectively account for over 2 million disability-adjusted life years (DALYs) globally[8]. Currently, food-borne trematodiases are targeted for control in the WHO NTD Road Map 2021–2030, which aims to reduce the incidence, prevalence, morbidity, and/or mortality of food-borne trematodiases to a locally acceptable level and to maintain this reduction through continued efforts[9].
Food-borne trematodiases have a long history in China, with documented cases dating back several thousand years ago [10]. Since the 1980s, China has conducted three national surveys on the status of important human parasitic diseases, covering the periods 1988-1992, 2001-2004, and 2014-2016. Across these surveys, the infection rate of Clonorchis sinensis demonstrated a fluctuating trend: it increased from 0.31% in the first survey to 0.58% in the second, then declined to 0.47% in the third. Meanwhile, the infection rates of Paragonimus, Fasciolopsis buski, and Fasciola hepatica all decreased constantly up to the third survey[11,12,13]. Unfortunately, no national survey has been conducted since, leaving a gap in national data after 2016. Additionally, the surveys did not cover the full spectrum of food-borne trematodiases nor assess the disease burden in terms of DALYs.
The Global Burden of Disease Study (GBD) provides a reliable and comprehensive database for examining the burden of various health conditions worldwide. Based on the latest GBD Study 2021 (GBD 2021) database, the current study evaluates the prevalence and DALYs of food-borne trematodiases in China from 1990 to 2021, and projects the DALYs of this disease in China through 2035.
2. Methods
2.1. Data Source
Data on the prevalence and DALYs of food-borne trematodiases in China were obtained from GBD 2021. GBD 2021 data resources provide a comprehensive epidemiological assessment of the burden associated with 371 diseases and injuries across 204 countries and territories. The data are accessible via the Global Data Health Exchange (GHDx) online platform (https://vizhub.healthdata.org/gbd-results/). The detailed methodological framework and data sources for GBD 2021 have been detailed in previous literature[14,15].
In brief, the GBD study employed DisMod-MR 2.1 (Disease Modelling Meta-Regression; version 2.1) for the estimation of prevalence. DisMod-MR 2.1 is a Bayesian meta-regression tool that generates internally consistent estimates of prevalence by sex, location, year, and age groups. This model accounts for variations in study design and methodology across diverse data sources, ensuring consistency and accuracy in estimates [16].
For China, data were primarily collected from the national population census, the disease surveillance point system, the maternal and child health surveillance system, the cause of death reporting system of the Chinese Center for Disease Control and Prevention, cancer registry system, and relevant published studies. Food-borne trematodiases cases were identified using the International Classification of Diseases (ICD) codes: ICD-9 (121–121.9, V75.6) and ICD-10 (B66–B66.9, B72.0). DALYs for food-borne trematodiases were calculated as the sum of years of life lost due to premature mortality (YLLs) and years lived with disability (YLDs) due to this disease.
All GBD estimates are reported with 95% uncertainty intervals (UIs), representing the 2.5th and 97.5th percentile values based on the distribution of 500 draws at each step of the GBD estimation process. These intervals reflect the uncertainty propagated through each stage of estimation. The age distribution of the world population from GBD 2021 was applied for estimation of age-standardized prevalence and DALY rates [2].
2.2. Statistical Analysis
To quantify temporal trends in age-standardized and age-specific prevalence and DALY rates, we calculated estimated annual percentage change (EAPC) using a linear regression model, where the natural logarithm of the value was regressed against the calendar year. The equation used was: y = α + βx + ε, where y represents the natural logarithm of the value, x indicates the calendar year, α is the intercept, β denotes the slope, and ε is the error term. The EAPC was then calculated as 100 × [exp(β) – 1], with its 95% confidence interval (CI) derived from the linear regression model.
An EAPC with a lower limit of the 95% CI above zero indicates a statistically significant upward trend, whereas that with an upper limit below zero signifies a downward trend. If the 95% CI includes zero, it suggests the lack of statistically significant change in the value of interest.
To predict future trends of food-borne trematodiases in China from 2022 to 2035, we applied a Bayesian age-period-cohort (BAPC) model, which incorporates integrated nested Laplace approximations (INLA) for full Bayesian inference[17]. Previous studies have shown that the BAPC model provides superior coverage and precision compared to alternative prediction methods[18,19,20,21]. Prior distributions for the age, period, and cohort effects were assumed to follow inverse gamma distributions. A second-order random walk was employed to model the age, period, and cohort effects. Population estimates from 1990 to 2035 were obtained from the United Nations Department of Economic and Social Affairs Population Division[22].
A two-tailed P value < 0.05 was considered statistically significant. All statistical analyses were performed with R software, version 4.4.1 (R Core Team, Vienna, Austria)[23].
3. Results
3.1. Prevalence and DALYs of Food-Borne Trematodiases in China from 1990 to 2021
In 2021, there were estimated 33.32 million prevalent cases of food-borne trematodiases in China (95% UI: 29.25–38.35 million), with an age-standardized prevalence of 1,930.21 per 100,000 people (95% UI: 1,700.47–2,240.51). From 1990 to 2021, the number of prevalent cases decreased by 9.02%, and the EAPC for the age-standardized prevalence rate was -0.96 (95% CI: -1.34 to -0.57) (Table 1). During this period, the age-standardized prevalence showed a consistent downward trend from 1990 to 2010, followed by a brief increase from 2010 to 2015, before declining again up to 2021 (Figure 1A).
In 2021, the estimated DALYs due to food-borne trematodiases in China was 768,297.4 (95% UI: 383,882.8–1,367,826.1), with an age-standardized DALY rate of 44.17 per 100,000 people (95% UI: 22.08–79.87). From 1990 to 2021, DALYs decreased by 18.11%, and the EAPC for the age-standardized DALY rate was -1.21 (95% CI: -1.65 to -0.77) (Table 1). Similar to the trend in the prevalence rate, the age-standardized DALY rate increased from 2010 to 2015, followed by a continued decrease from 2015 to 2021 (Figure 1B).
Gender-wise, both the number of prevalent cases and the age-standardized prevalence of food-borne trematodiases were higher in males than in females from 1990 to 2021. Both genders exhibited a downward trend in the number and rate of prevalent cases over this period. A similar pattern was observed for DALYs, with males having higher DALY counts and age-standardized DALY rates than females, while both genders followed a downward trend (Table 1). Consistent with the overall trends, both males and females experienced a brief increase in age-standardized prevalence and DALY rates from 2010 to 2015, followed by a continued decline (Figure 1A,B).
3.2. Age-specific Prevalence and DALYs of Food-Borne Trematodiases in China from 1990 to 2021
In 2021, the number of prevalent cases of food-borne trematodiases increased with age, peaking in the 50-54 year age group (3.98 million, 95% UI: 3.34–4.70 million), and declining progressively in along with age. Across most age groups, males had higher numbers of prevalent cases than females, except in age groups above 85 years, where females had slightly higher case counts. The prevalence rate followed a similar pattern, increasing with age and peaking slightly later in the 60-64 year age group at 3,613.95 per 100,000 population (95% UI: 3,105.81–4,203.59). After this peak, the prevalence rate declined in the older age groups. Gender-wise, males consistently showed higher prevalence rates across all age groups compared to females (Table 2, Figure 2A).
From 1990 to 2021, the number of prevalent cases of food-borne trematodiases decreased in younger age groups (under 45 years old) and increased in older age groups. The most significant growth occurred in the 95-plus age group, with a percentage increase of 1,465.37%. In contrast, the prevalence rate declined across most age groups during this period. The 10-14 year age group exhibited the largest decrease in the prevalence rate, with an EAPC of -1.46 (95% CI: -1.66 to -1.26) (Table 2). Most age groups experienced an upward trend in prevalence rate after 2010, followed by a decline after 2015. However, this pattern did not apply to the very young (under 15 years old) and the very old (above 95 years old), where the rates remained relatively stable (Figure 1C).
In 2021, the DALY count due to food-borne trematodiases increased with age, peaking in the 50-54 year age group with 90,924.1 DALYs (95% UI: 43,634.0–175,210.7), before declining in older age groups. Males had higher DALY counts than females across most age groups, although females surpassed males in counts after the age of 80. Similarly, the DALY rate increased with age, reaching a peak in the 60-64 year age group at 80.35 per 100,000 population (95% UI: 39.32–144.57), before gradually declining. Males consistently exhibited higher DALY rates across all age groups compared to females (Table 3, Figure 2B).
From 1990 to 2021, DALY counts decreased in younger age groups (under 45 years old) and increased in most older age groups. The most significant growth was observed in the 95-plus age group, with a percentage increase of 1,464.42%. However, the DALY rate declined in most age groups during this period. The largest decrease in DALY rate occurred in the 5-9 year age group, with an EAPC of -2.31 (95% CI: -2.51 to -2.10) (Table 3). Similar to the trend in prevalence rates, most age groups experienced a temporary increase in DALY rates after 2010, followed by a decline, except for the very young (under 15 years old) and the very old (above 95 years old), where rates remained relatively stable (Figure 1D).
3.3. Projected DALYs of Food-Borne Trematodiases in China through 2035
The DALY count due to food-borne trematodiases in China is projected to decrease by 2035, with an estimated DALY count of 636,726.2, representing a 17.13% reduction from 2021. In contrast, the DALY rate is expected to remain relatively stable through 2035. By 2035, the DALY rate is projected to be 46.10 per 100,000 population, reflecting only a modest increase from the rate in 2021.
Gender-wise, males are expected to continue having higher DALY counts and rates of food-borne trematodiases than females by 2035. The DALY count for males is projected to be 396,135.5, while for females, it is projected to be 236,549.9, both representing decreases from 2021 levels. Meanwhile, the DALY rate for males is expected to be 56.69 per 100,000 population, and for females, 34.66 per 100,000 population, with both rates remaining stable and showing no significant growth from 2021 (Figure 3).
4. Discussion
In this study, we utilized data from the GBD 2021 study to analyze the prevalence and DALYs of food-borne trematodiases in China from 1990 to 2021. Additionally, we applied the BAPC model to predict the DALYs of food-borne trematodiases through 2035.
Between 1990 and 2021, both the number of prevalent cases and DALY counts decreased. Similarly, the age-standardized prevalence and DALY rates showed an overall downward trend during this period. Several factors contributed to the reduction in the burden of food-borne trematodiases. First, China's continuous social and economic development led to improved living standards, better infrastructure, and enhanced sanitation of food and drinking water[24]. Additionally, the implementation of integrated public health strategies, such as drug administration and information, education, and communication (IEC) campaigns, significantly reduced the disease burden[25,26]. A study evaluating community-based integrated strategies for clonorchiasis control in two pilot counties in China between 2007 and 2009 reported a sharp reduction in prevalence, from 41.4% to 7.0%, highlighting the effectiveness of these strategies[27].
However, despite the overall decline, the prevalence of food-borne trematodiases in China remains high, and it continues to be a significant cause of disability and premature death. In 2021, an estimated 33.32 million prevalent cases of food-borne trematodiases remained in China, contributing to 768,297.4 DALYs. The persistence of this burden is partly attributed to entrenched cultural practices in endemic areas, where the consumption of raw fish, crustaceans, and aquatic plants is common. These dietary habits are difficult to change, even with improved hygiene and ongoing health education. For instance, in Shunde, Guangdong, where raw fish sashimi is a traditional delicacy, a 2014-2015 survey revealed that the infection rate of Clonorchis sinensis among local residents was as high as 42.38%[28]. Moreover, food-borne trematodiases have complex life cycles that involve multiple hosts, including intermediate hosts, reservoir hosts, and definitive hosts. The control of these non-human hosts can be challenging and resource-intensive[7].
Our data showed a brief increase in the prevalence and DALY rates of food-borne trematodiases after 2010, followed by a rapid decline after 2015. This decline can be attributed to China’s National Plan for the Prevention and Control of Echinococcosis and Other Important Parasitic Diseases (2016-2020) [29]. The plan emphasized integrated prevention strategies for food-borne trematodiases, particularly liver flukes, including environmental management, IEC programs, and deworming and treatment of high-risk populations. In addition, a national clonorchiasis surveillance system was established in 2016, providing high-precision data on the disease’s distribution down to the county level[30]. This system has facilitated early detection of clonorchiasis cases and collected comprehensive epidemiological data, supporting long-term control and prevention efforts.
Gender-wise, males consistently exhibited higher prevalence and DALY rates of food-borne trematodiases than females throughout the study period. This finding is consistent with an earlier systematic analysis of the global burden of human food-borne trematodiases, conducted as part of the GBD 2010 study and a WHO initiative. The analysis demonstrated that the prevalence rates of most food-borne trematodiases were higher in males than in females, except for fascioliasis, where slightly more females were infected[31]. Furthermore, the 2014-2016 national survey on the status of important human parasitic diseases in China (the third national survey), also reported that the infection rate of Clonorchis sinensis was higher in males than in females in both rural and urban areas[13]. The discrepancy in disease burden between genders may result from the fact that men consume more risky foods in certain communities or are more frequently engaged in activities such as fishing and fish farming, which increase exposure to contaminated water and food sources.
Regarding age-specific patterns, the disease burden increased in younger individuals, peaked in middle-aged groups, and then declined in older age groups. Previous studies analyzing the DALYs of major parasitic diseases in China using GBD 2019 data reported that over 60% of the burden of food-borne trematodiases was concentrated in the 30-69 age group[32]. Research examining different classifications of food-borne trematodiases has shown that the prevalence of liver and lung fluke infections typically increases steadily until plateauing in middle-aged individuals[31,33,34]. Although data on intestinal fluke infections are limited, it is assumed they follow a similar pattern. The high disease burden in middle-aged groups is believed to stem from the long lifespan of food-borne trematodiases and the likelihood of continuous reinfection over time[3]. Additionally, an increase in the absolute number of prevalent cases and DALY counts in older age groups was observed in this study, likely due to the aging of the patient population. Older individuals are more likely to experience complications related to food-borne trematodiases due to weaker immune systems, comorbidities, and delayed diagnosis. This increased burden in older populations poses challenges for the prevention and treatment of food-borne trematodiases.
Lastly, we projected the DALY counts and rates through 2035. The DALY counts of food-borne trematodiases are expected to decrease, while the DALY rates are projected to remain stable with a slight increase. These projections suggest that controlling food-borne trematodiases in China remains a significant challenge. Encouragingly, China’s National Comprehensive Implementation Plan for the Prevention and Control of Echinococcosis and Other Important Parasitic Diseases (2024–2030) was issued in 2024[35]. Building on the 2016–2020 plan, this updated version places greater emphasis on preventing food-borne parasitic diseases as a whole. It advocates for proactive identification and treatment of infected individuals through surveillance, screening, and regular hospital visits. It also addresses non-human hosts by recommending regular deworming of animals in endemic areas.
The plan aims to reduce the infection rate of liver fluke in key endemic provinces by 5% by 2025 and 15% by 2030. It also sets a goal to maintain control over lung fluke infections. To achieve these goals, it is recommended that future control strategies for food-borne trematodiases in China consider implementing more culturally sensitive interventions, such as introducing culturally acceptable alternatives to raw aquatic products and developing locally tailored health education materials. Additionally, based on our findings, future prevention strategies could adopt gender- and age-specific measures, particularly for males and middle- to older-aged individuals. For example, targeted IEC programs could be implemented in male-dominated industries, such as fishing or food vending, while regular screening and early detection are provided for middle- to older-aged groups in endemic areas.
To our knowledge, this study is the first to comprehensively analyze the disease burden of food-borne trematodiases in China using the latest GBD 2021 data, while also providing projections of the future disease burden through 2035. Nevertheless, the study acknowledges several limitations. First, our study shares the weaknesses of other GBD studies. The GBD data is based on model fitting rather than real-world data, which introduces uncertainty in disease burden estimates. Although the GBD employs rigorous statistical methods to address these uncertainties, the results should be interpreted with caution. Second, our analysis was conducted at the national level, and data on provincial or municipal disease burdens were not available. Further research is needed to examine the subnational disease burdens of food-borne trematodiases in China. Finally, while the BAPC model was used to project the future DALYs of food-borne trematodiases, it may not fully capture the impact of various influencing factors, as the projections rely solely on historical data and population estimates.
In conclusion, this study provides a systematic analysis of the prevalence and DALYs of food-borne trematodiases in China based on the latest GBD 2021 data. Although the overall burden showed a downward trend from 1990 to 2021, it remained substantial in 2021. Males experienced a higher disease burden than females. The middle-aged group bore the highest burden, while the older population saw the most rapid increase in absolute numbers of prevalence cases and DALYs. The projections indicate that DALYs are likely to remain stable until 2035. China has made significant progress in controlling food-borne trematodiases and reducing disease burden; however, sustained prevention and control efforts, including targeted interventions for high-risk groups, are needed to achieve the goals set out in China’s national plan for the prevention and control of important parasitic diseases (2024–2030) and the WHO NTD roadmap (2021–2030). This study provides valuable insights for public health planning and supports the development of more focused and effective intervention strategies.
Author Contributions
W.W. and Y.H. conceived and designed the study. Y.Z.Z. Y.H.L. and L.Q.T. performed data collection and data analysis. Y.L.Q., G.T., H.R.Z., L.P. and X.L.L. performed literature search and review. Y.Z.Z. prepared the first version of the manuscript. Y.H. provided critical comments on the revision of the manuscript. W.W. revised and finalized the manuscript. All authors read and approved the final version of the manuscript.
Funding
This study was supported by grants from Jiangsu Provincial Young Talents in Medical Sciences (grant no. QNRC2016621), Cultivation Specialized Project for Clinical Medical Research in Chinese People’s Armed Police Force, Wuxi Municipal Health Commission (grant no. Z202116) and Wuxi Municipal Department of Science and Technology (grant no. Y20212012).
Institutional Review Board Statement
Not available.
Informed Consent Statement
Not available.
Data Availability Statement
All data presented in this study are available upon request by contact with the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Fürst T, Duthaler U, Sripa B, Utzinger J, Keiser J. Trematode infections: liver and lung flukes. Infect Dis Clin North Am. 2012;26[2]:399-419.
- Fürst T, Sayasone S, Odermatt P, Keiser J, Utzinger J. Manifestation, diagnosis, and management of foodborne trematodiasis. BMJ (Clinical Research ed). 2012;344:e4093.
- Fürst T, Yongvanit P, Khuntikeo N, Lun Z-R, Haagsma JA, Torgerson PR, Odermatt P, Bürli C, Chitnis N, Sithithaworn P. Food-borne Trematodiases in East Asia: Epidemiology and Burden. In: Utzinger J, Yap P, Bratschi M, Steinmann P, editors. Neglected Tropical Diseases - East Asia. Cham: Springer International Publishing; 2019. p. 13-38.
- World Health Organization. Foodborne Trematodiases (Chapter 4.7). Investing to overcome the global impact of neglected tropical diseases: third WHO report on neglected tropical diseases. Geneva: World Health Organization; 2015. p. 105–9.
- Sripa B, Kaewkes S, Intapan PM, Maleewong W, Brindley PJ. Food-borne trematodiases in Southeast Asia: epidemiology, pathology, clinical manifestation and control. Advances in parasitology. 2010;72:305-50.
- Keiser J, Utzinger Jr. Food-borne trematodiases. Clinical microbiology reviews. 2009;22[3]:466-83.
- Toledo R, Esteban JG, Fried B. Current status of food-borne trematode infections. Eur J Clin Microbiol Infect Dis. 2012;31[8]:1705-18.
- World Health Organization. DALY Estimates: Parasites (Chapter 5.4). WHO estimates of the global burden of foodborne diseases: foodborne disease burden epidemiology reference group 2007-2015. Geneva: World Health Organization; 2015. p. 86.
- World Health Organization. 2030 targets and milestones (Chapter 2). Ending the neglect to attain the Sustainable Development Goals: a road map for neglected tropical diseases 2021–2030. Geneva: World Health Organization; 2020. p. 12-23.
- Wei DX, Yang WY, Huang SQ, Lu YF, Su TC, Ma JH, Hu WX, Xie NF. Parasitological investigation on the ancient corpse of the Western Han Dynasty unearthed from tomb No. 168 on Phoenix Hill in Jiangling county. Acta Acad Med Wuhan. 1981;1[2]:16-23.
- Chen YD, Zhou CH, Xu LQ. Analysis of the results of two nationwide surveys on Clonorchis sinensis infection in China. Biomed Environ Sci. 2012;25[2]:163-6.
- Qian M-B, Chen J, Bergquist R, Li Z-J, Li S-Z, Xiao N, Utzinger J, Zhou X-N. Neglected tropical diseases in the People's Republic of China: progress towards elimination. Infectious Diseases of Poverty. 2019;8[1]:86.
- Zhou, XN. Report on the national survey of important human parasitic diseases in China [2015]. Beijing: People’s Medical Publishing House; 2018.
- GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403[10440]:2133-61.
- GBD 2021 Demographics Collaborators. Global age-sex-specific mortality, life expectancy, and population estimates in 204 countries and territories and 811 subnational locations, 1950-2021, and the impact of the COVID-19 pandemic: a comprehensive demographic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403[10440]:1989-2056.
- Flaxman AD, Vos T, Murray CJ. An integrative metaregression framework for descriptive epidemiology. Seattle, WA: University of Washington Press; 2015.
- Rue H, Martino S, Chopin N. Approximate Bayesian inference for latent Gaussian models by using integrated nested Laplace approximations. Journal of the Royal Statistical Society Series B: Statistical Methodology. 2009;71[2]:319-92. [CrossRef]
- Knoll M, Furkel J, Debus J, Abdollahi A, Karch A, Stock C. An R package for an integrated evaluation of statistical approaches to cancer incidence projection. BMC medical research methodology. 2020;20:1-11. [CrossRef]
- Liu N, Yang D-W, Wu Y-X, Xue W-Q, Li D-H, Zhang J-B, He Y-Q, Jia W-H. Burden, trends, and risk factors for breast cancer in China from 1990 to 2019 and its predictions until 2034: an up-to-date overview and comparison with those in Japan and South Korea. BMC Cancer. 2022;22[1]:826. [CrossRef]
- Wu B, Li Y, Shi B, Zhang X, Lai Y, Cui F, Bai X, Xiang W, Geng G, Liu B. Temporal trends of breast cancer burden in the Western Pacific Region from 1990 to 2044: Implications from the Global Burden of Disease Study 2019. Journal of Advanced Research. 2024;59:189-99. [CrossRef]
- Zhang S-X, Yang G-B, Zhang R-J, Zheng J-X, Yang J, Lv S, Duan L, Tian L-G, Chen M-X, Liu Q. Global, regional, and national burden of dengue, 1990–2021: Findings from the global burden of disease study 2021. Decoding Infection and Transmission. 2024;2:100021.
- United Nations Department of Economic and Social Affairs Population Division. World Population Prospects 2024, Online Edition. [Available from: https://population.un.org/wpp/Download/Standard/Population/.
- R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2022.
- Wang Y-P, Zhou X-N. The year 2020, a milestone in breaking the vicious cycle of poverty and illness in China. Infectious Diseases of Poverty. 2020;9[1]:11.
- Zhang H, Liu C, Zheng Q. Development and application of anthelminthic drugs in China. Acta Tropica. 2019;200:105181.
- Huang Y, Huang D, Geng Y, Fang S, Yang F, Wu C, Zhang H, Wang M, Zhang R, Wang X. An integrated control strategy takes Clonorchis sinensis under control in an endemic area in South China. Vector-Borne and Zoonotic Diseases. 2017;17[12]:791-8.
- Chen Y-D, Li H-Z, Xu L-Q, Qian M-B, Tian H-C, Fang Y-Y, Zhou C-H, Ji Z, Feng Z-J, Tang M, Li Q, Wang Y, Bergquist R, Zhou X-N. Effectiveness of a community-based integrated strategy to control soil-transmitted helminthiasis and clonorchiasis in the People's Republic of China. Acta Tropica. 2021;214:105650.
- Song L, Xie Q, Lv Z. Foodborne parasitic diseases in China: a scoping review on current situation, epidemiological trends, prevention and control. Asian Pacific Journal of Tropical Medicine. 2021;14[9]:385-400.
- National Health and Family Planning Commission of the People’s Republic of China. National Plan for the Prevention and Control of Echinococcosis and Other Important Parasitic Diseases (2016-2020) [Available from: http://www.nhc.gov.cn/jkj/s5873/201702/dda5ffe3f50941a29fb0aba6233bb497.shtml.
- Qian MB, Chen YD, Zhu HH, Zhu TJ, Zhou CH, Zhou XN. Establishment and role of national clonorchiasis surveillance system in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2018;39[11]:1496-500.
- Fürst T, Keiser J, Utzinger J. Global burden of human food-borne trematodiasis: a systematic review and meta-analysis. The Lancet Infectious Diseases. 2012;12[3]:210-21.
- Zeng T, Lü S, Tian L, Li S, Sun L, Jia T. Temporal trends in disease burden of major human parasitic diseases in China from 1990 to 2019. Zhongguo Xue Xi Chong Bing Fang Zhi Za Zhi. 2023;35[1].
- Zhu T-J, Chen Y-D, Qian M-B, Zhu H-H, Huang J-L, Zhou C-H, Zhou X-N. Surveillance of clonorchiasis in China in 2016. Acta Tropica. 2020;203:105320.
- Choi M-H, Park SK, Li Z, Ji Z, Yu G, Feng Z, Xu L, Cho S-Y, Rim H-J, Lee S-H, Hong S-T. Effect of control strategies on prevalence, incidence and re-infection of clonorchiasis in endemic areas of China. PLoS Neglected Tropical Diseases. 2010;4[2]:e601.
- National Disease Control and Prevention Administration. National Comprehensive Implementation Plan for the Prevention and Control of Echinococcosis and Other Important Parasitic Diseases (2024-2030) 2024 [Available from: https://www.gov.cn/zhengce/zhengceku/202405/content_6950309.htm.
Figure 1.
Trends in age-standardized and age-specific prevalence and DALY rates of food-borne trematodiases in China from 1990 to 2021. A: Age-standardized prevalence rates for both genders, males, and females. B: Age-standardized DALY rates for both genders, males, and females. C: Age-specific prevalence rates across different age groups. D: Age-specific DALY rates across different age groups. Abbreviations: DALY, disability-adjusted life years.
Figure 1.
Trends in age-standardized and age-specific prevalence and DALY rates of food-borne trematodiases in China from 1990 to 2021. A: Age-standardized prevalence rates for both genders, males, and females. B: Age-standardized DALY rates for both genders, males, and females. C: Age-specific prevalence rates across different age groups. D: Age-specific DALY rates across different age groups. Abbreviations: DALY, disability-adjusted life years.
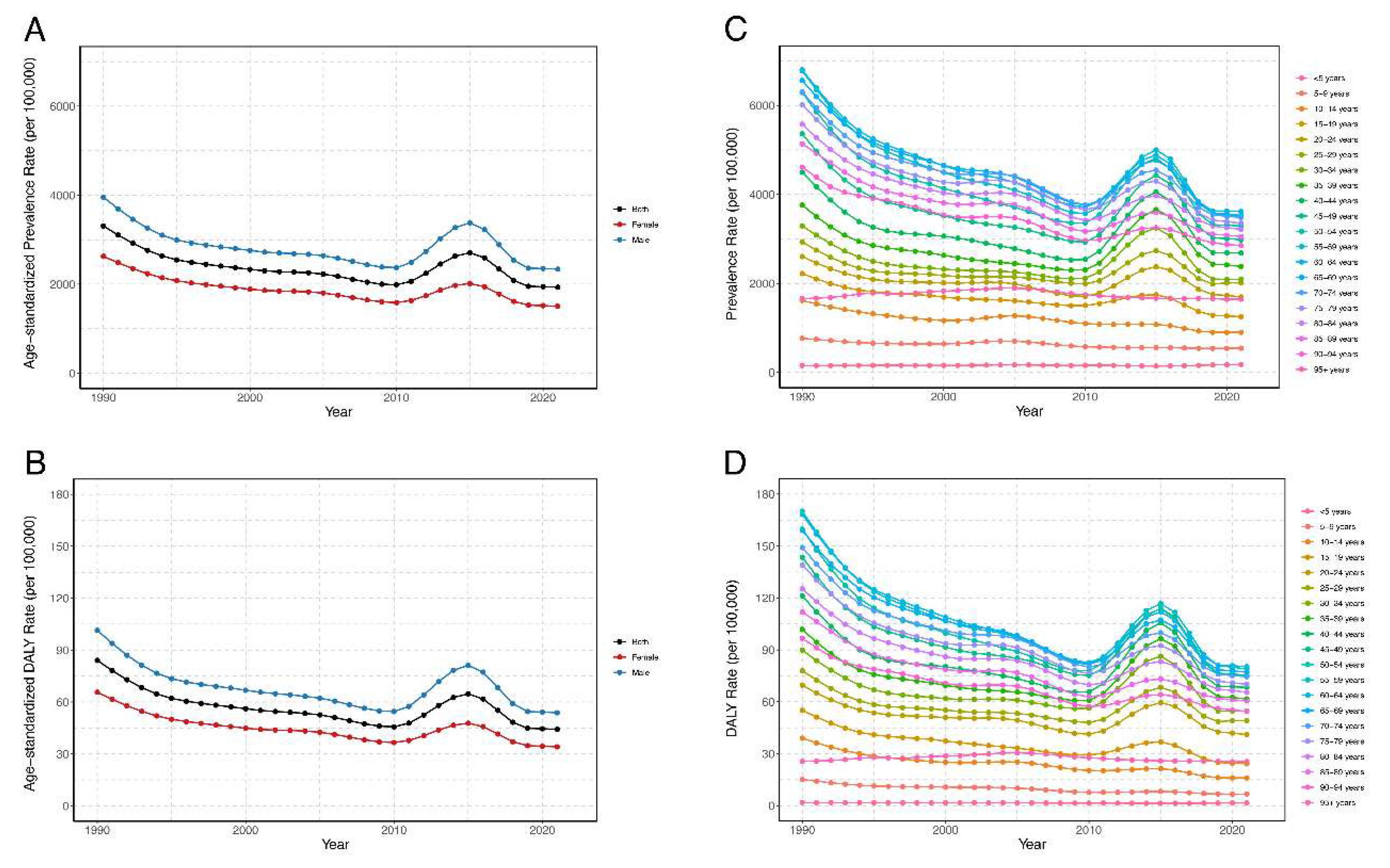
Figure 2.
Age-specific prevalence and DALY numbers and rates of food-borne trematodiases in China in 2021. A: Prevalence numbers and rates by age group and gender. B: DALY numbers and rates by age group and gender. Abbreviations: DALY, disability-adjusted life years.
Figure 2.
Age-specific prevalence and DALY numbers and rates of food-borne trematodiases in China in 2021. A: Prevalence numbers and rates by age group and gender. B: DALY numbers and rates by age group and gender. Abbreviations: DALY, disability-adjusted life years.
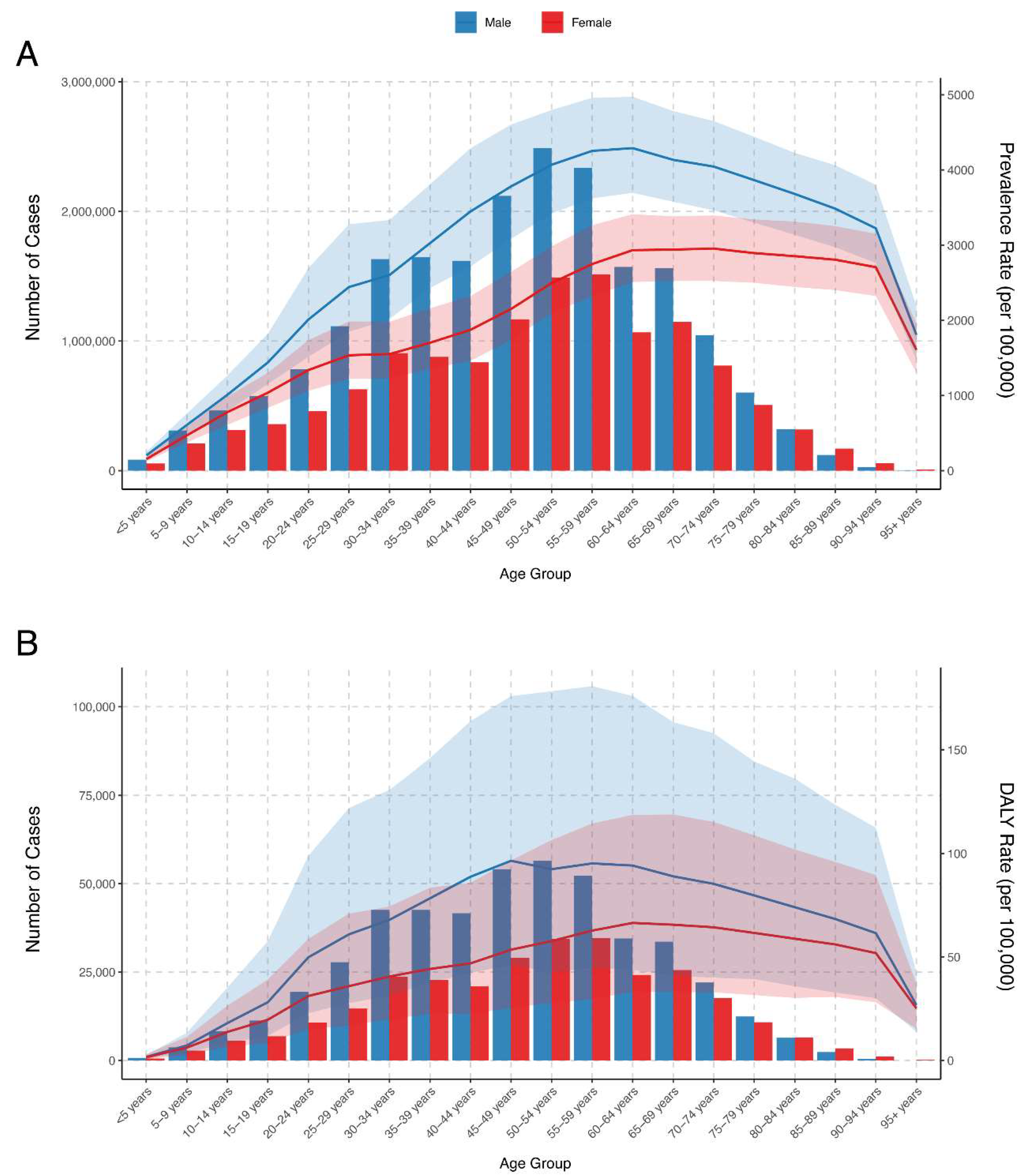
Figure 3.
Prediction of age-standardized DALY rates and DALY numbers for food-borne trematodiases in China from 2022 to 2035. A-B: Both genders; C-D: Males; E-F: Females. The shaded areas or error bars indicate the 95% CIs for the predicted rates and numbers. Abbreviations: DALY, disability-adjusted life years; CI, confidence interval.
Figure 3.
Prediction of age-standardized DALY rates and DALY numbers for food-borne trematodiases in China from 2022 to 2035. A-B: Both genders; C-D: Males; E-F: Females. The shaded areas or error bars indicate the 95% CIs for the predicted rates and numbers. Abbreviations: DALY, disability-adjusted life years; CI, confidence interval.
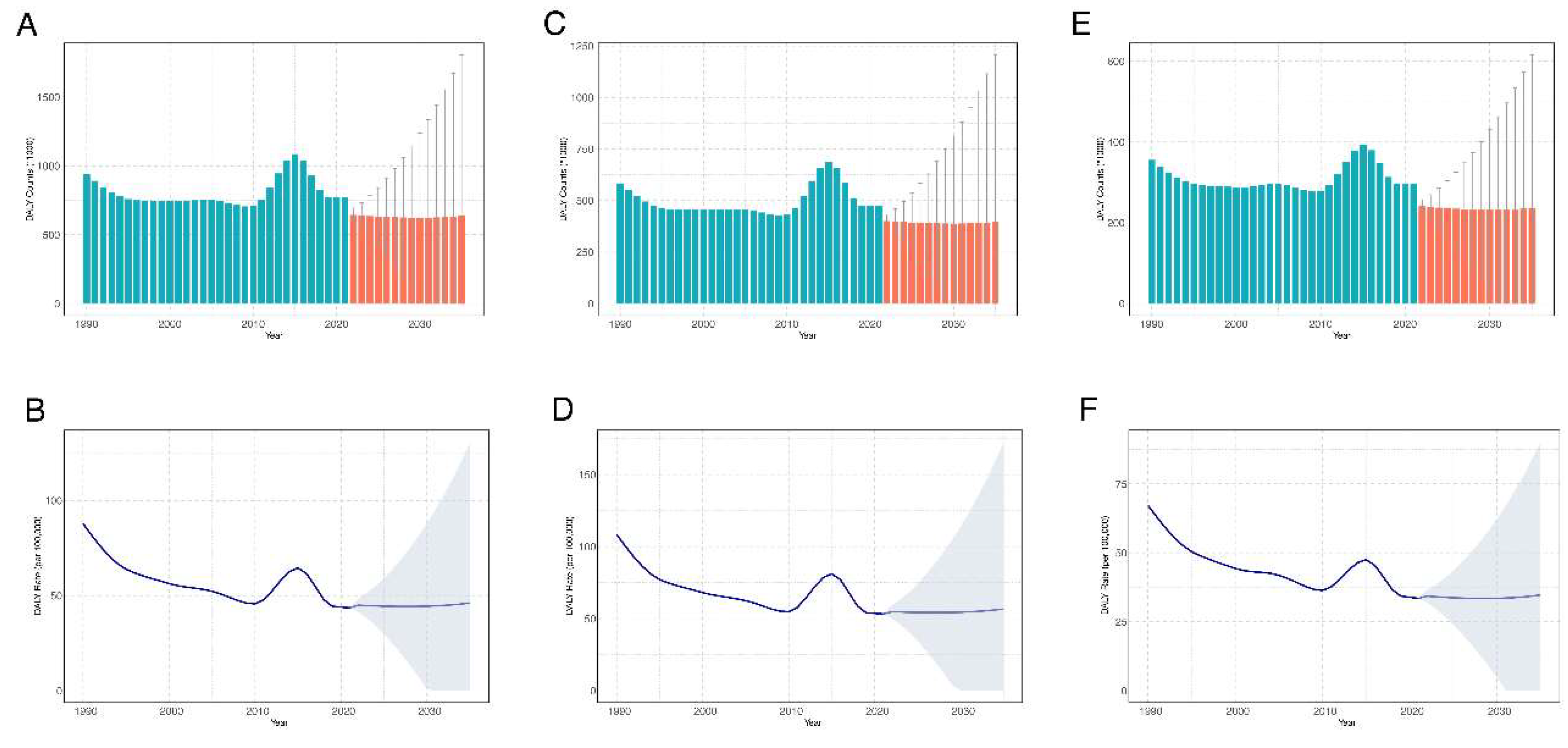

Table 1.
Overview of prevalence and DALYs for food-borne trematodiases in China (1990-2021).
| Parameter | Number | Percentage change(%) | Age-standardized rate (per 100 000 population) | EAPC (95% CI, %) | ||
|---|---|---|---|---|---|---|
| 1990 (95%UI) | 2021 (95%UI) | 1990 (95%UI) | 2021 (95%UI) | |||
| Prevalence | ||||||
| Both | 36621225.1 (31239359.0, 43237071.8) | 33317222.7 (29251038.7, 38353602.0) | -9.02 | 3307.89 (2845.59, 3875.81) | 1930.21 (1700.47, 2240.51) | -0.96 (-1.34, -0.57) |
| Male | 22476187.2 (19095640.6, 26580789.7) | 20418481.9 (17785189.7, 23654614.6) | -9.16 | 3954.06 (3377.44, 4640.68) | 2337.02 (2042.27, 2718.69) | -0.81 (-1.24, -0.38) |
| Female | 14145037.9 (12067609.2, 16774017.0) | 12898740.8 (11350526.9, 14870728.4) | -8.81 | 2626.23 (2255.27, 3066.96) | 1506.51 (1328.58, 1743.02) | -1.17 (-1.48, -0.85) |
| DALYs | ||||||
| Both | 938172.2 (365200.0, 1876414.7) | 768297.4 (383882.8, 1367826.1) | -18.11 | 84.04 (32.98, 168.04) | 44.17 (22.08, 79.87) | -1.21 (-1.65, -0.77) |
| Male | 582518.0 (224509.7, 1168057.0) | 472583.6 (231736.8, 849985.0) | -18.87 | 101.43 (39.26, 203.48) | 53.80 (26.54, 98.11) | -1.08 (-1.57, -0.59) |
| Female | 355654.2 (137444.6, 708492.9) | 295713.8 (151020.2, 519060.0) | -16.85 | 65.63 (25.81, 129.90) | 34.10 (17.27, 60.67) | -1.39 (-1.75, -1.04) |
Abbreviations: DALY, disability-adjusted life years; EAPC, estimated annual percentage change; UI, uncertainty interval; CI, confidence interval.
Table 2.
Age-specific prevalence of food-borne trematodiases in China (1990-2021).
| Age group | Number | Percentage change(%) | Prevalence rate (per 100 000 population) | EAPC (95% CI, %) | ||
|---|---|---|---|---|---|---|
| 1990 (95%UI) | 2021 (95%UI) | 1990 (95%UI) | 2021 (95%UI) | |||
| <5 years | 171914.5 (144671.2, 208443.7) | 139694.9 (114532.1, 171235.8) | -18.74 | 153.76 (129.39, 186.43) | 179.86 (147.46, 220.47) | 0.05 (-0.14, 0.24) |
| 5-9 years | 799728.8 (615585.6, 1010084.7) | 520272.9 (418052.3, 648896.7) | -34.94 | 766.92 (590.33, 968.65) | 543.25 (436.52, 677.55) | -0.99 (-1.17, -0.81) |
| 10-14 years | 1653399.4 (1218426.7, 2149169.6) | 776875.7 (610532.1, 979481.6) | -53.01 | 1616.35 (1191.12, 2101.01) | 901.32 (708.33, 1136.38) | -1.46 (-1.66, -1.26) |
| 15-19 years | 2812747.8 (2142971.6, 3626489.7) | 936264.0 (753794.3, 1173989.0) | -66.71 | 2220.62 (1691.84, 2863.05) | 1253.83 (1009.47, 1572.19) | -1.17 (-1.44, -0.91) |
| 20-24 years | 3436931.0 (2608526.7, 4458216.2) | 1240725.6 (955563.4, 1634296.6) | -63.90 | 2603.72 (1976.14, 3377.41) | 1695.58 (1305.88, 2233.43) | -0.63 (-0.98, -0.27) |
| 25-29 years | 3219883.5 (2475118.3, 4211276.7) | 1741653.7 (1345850.6, 2298166.3) | -45.91 | 2930.11 (2252.37, 3832.28) | 2013.89 (1556.22, 2657.39) | -0.40 (-0.78, -0.02) |
| 30-34 years | 2903003.4 (2268678.5, 3779118.4) | 2538187.6 (1984320.7, 3241193.0) | -12.57 | 3289.73 (2570.91, 4282.56) | 2095.02 (1637.86, 2675.28) | -0.39 (-0.91, 0.13) |
| 35-39 years | 3435818.6 (2709447.3, 4304031.1) | 2523380.2 (2014491.7, 3165399.0) | -26.56 | 3761.61 (2966.36, 4712.15) | 2381.37 (1901.12, 2987.26) | -0.41 (-0.95, 0.13) |
| 40-44 years | 3017969.3 (2405475.4, 3666181.0) | 2454304.9 (1957302.9, 3031967.6) | -18.68 | 4498.10 (3585.21, 5464.22) | 2681.31 (2138.34, 3312.41) | -0.64 (-1.19, -0.08) |
| 45-49 years | 2768369.1 (2274417.5, 3393964.6) | 3287197.4 (2690789.9, 4014219.7) | 18.74 | 5363.09 (4406.17, 6575.04) | 2979.65 (2439.04, 3638.65) | -0.93 (-1.44, -0.41) |
| 50-54 years | 3001413.2 (2502700.4, 3644828.9) | 3978362.9 (3342141.3, 4704312.9) | 32.55 | 6290.84 (5245.56, 7639.41) | 3291.74 (2765.32, 3892.40) | -1.23 (-1.71, -0.75) |
| 55-59 years | 2939965.3 (2472520.4, 3529015.9) | 3847655.0 (3277996.9, 4521053.7) | 30.87 | 6778.94 (5701.11, 8137.17) | 3499.70 (2981.56, 4112.20) | -1.37 (-1.81, -0.93) |
| 60-64 years | 2403019.1 (2035702.1, 2875610.9) | 2638368.9 (2267403.2, 3068835.9) | 9.79 | 6800.20 (5760.75, 8137.57) | 3613.95 (3105.81, 4203.59) | -1.42 (-1.79, -1.06) |
| 65-69 years | 1789766.7 (1518589.8, 2133235.4) | 2706401.5 (2339545.7, 3102609.6) | 51.22 | 6560.29 (5566.31, 7819.26) | 3528.39 (3050.12, 4044.94) | -1.41 (-1.72, -1.09) |
| 70-74 years | 1185961.6 (1003456.2, 1409151.9) | 1856504.5 (1589514.4, 2120836.3) | 56.54 | 6302.39 (5332.53, 7488.46) | 3483.36 (2982.40, 3979.32) | -1.33 (-1.60, -1.07) |
| 75-79 years | 684429.1 (580074.5, 817345.2) | 1109850.9 (951457.8, 1267878.7) | 62.16 | 6013.95 (5097.00, 7181.86) | 3351.11 (2872.85, 3828.26) | -1.31 (-1.56, -1.06) |
| 80-84 years | 295455.9 (248823.4, 352100.8) | 636509.6 (542502.1, 736544.2) | 115.43 | 5577.66 (4697.33, 6647.02) | 3216.02 (2741.04, 3721.45) | -1.28 (-1.51, -1.05) |
| 85-89 years | 86628.4 (72630.0, 103491.8) | 290944.6 (248501.3, 338972.4) | 235.85 | 5135.49 (4305.64, 6135.19) | 3054.30 (2608.73, 3558.48) | -1.32 (-1.53, -1.11) |
| 90-94 years | 14148.4 (11764.8, 17181.7) | 83548.5 (71718.7, 97227.5) | 490.52 | 4611.27 (3834.40, 5599.90) | 2849.55 (2446.08, 3316.10) | -1.28 (-1.44, -1.11) |
| 95+ years | 672.0 (561.3, 792.9) | 10519.3 (8546.3, 12752.3) | 1465.37 | 1659.66 (1386.12, 1958.21) | 1645.97 (1337.24, 1995.35) | -0.19 (-0.35, -0.02) |
Abbreviations: EAPC, estimated annual percentage change; UI, uncertainty interval; CI, confidence interval.
Table 3.
Age-specific DALYs of food-borne trematodiases in China (1990-2021).
| Age group | Number | Percentage change(%) | DALY rate (per 100 000 population) | EAPC (95% CI,%) | ||
|---|---|---|---|---|---|---|
| 1990 (95%UI) | 2021 (95%UI) | 1990 (95%UI) | 2021 (95%UI) | |||
| <5 years | 2031.6 (1081.8, 3458.7) | 1227.1 (633.5, 1972.2) | -39.60 | 1.82 (0.97, 3.09) | 1.58 (0.82, 2.54) | -0.74 (-0.90, -0.57) |
| 5-9 years | 15797.3 (6328.7, 32927.4) | 6441.4 (3175.8, 11675.0) | -59.22 | 15.15 (6.07, 31.58) | 6.73 (3.32, 12.19) | -2.31 (-2.51, -2.10) |
| 10-14 years | 39857.1 (14192.0, 86405.5) | 13801.5 (6714.9, 26475.6) | -65.37 | 38.96 (13.87, 84.47) | 16.01 (7.79, 30.72) | -2.28 (-2.51, -2.05) |
| 15-19 years | 69811.7 (24070.1, 148812.0) | 18072.2 (7724.6, 37470.3) | -74.11 | 55.12 (19.00, 117.48) | 24.20 (10.34, 50.18) | -1.83 (-2.19, -1.47) |
| 20-24 years | 91807.6 (34189.3, 191422.8) | 30048.7 (14278.4, 58379.7) | -67.27 | 69.55 (25.90, 145.02) | 41.06 (19.51, 79.78) | -0.87 (-1.27, -0.47) |
| 25-29 years | 85671.9 (31447.9, 169654.0) | 42446.5 (19397.0, 87010.0) | -50.45 | 77.96 (28.62, 154.39) | 49.08 (22.43, 100.61) | -0.64 (-1.06, -0.22) |
| 30-34 years | 79295.9 (31337.0, 160702.4) | 66289.6 (32003.2, 125248.6) | -16.40 | 89.86 (35.51, 182.11) | 54.72 (26.42, 103.38) | -0.49 (-1.01, 0.04) |
| 35-39 years | 92973.1 (36213.0, 189105.5) | 65380.4 (31594.7, 123636.0) | -29.68 | 101.79 (39.65, 207.04) | 61.70 (29.82, 116.68) | -0.51 (-1.05, 0.04) |
| 40-44 years | 81304.9 (30671.0, 163233.2) | 62564.1 (29975.6, 114785.1) | -23.05 | 121.18 (45.71, 243.29) | 68.35 (32.75, 125.40) | -0.77 (-1.34, -0.21) |
| 45-49 years | 74077.2 (27619.0, 147619.4) | 83120.4 (38906.2, 150098.9) | 12.21 | 143.51 (53.51, 285.98) | 75.34 (35.27, 136.06) | -1.08 (-1.60, -0.56) |
| 50-54 years | 76218.4 (28809.0, 157441.2) | 90924.1 (43634.0, 175210.7) | 19.29 | 159.75 (60.38, 329.99) | 75.23 (36.10, 144.97) | -1.51 (-2.02, -1.00) |
| 55-59 years | 73736.4 (27983.8, 150512.0) | 86778.8 (41879.9, 162705.9) | 17.69 | 170.02 (64.52, 347.05) | 78.93 (38.09, 147.99) | -1.65 (-2.11, -1.18) |
| 60-64 years | 59478.0 (23670.0, 119142.2) | 58659.0 (28705.5, 105542.6) | -1.38 | 168.31 (66.98, 337.16) | 80.35 (39.32, 144.57) | -1.71 (-2.13, -1.30) |
| 65-69 years | 43396.6 (17667.0, 88027.8) | 59120.3 (29032.5, 107203.1) | 36.23 | 159.07 (64.76, 322.66) | 77.08 (37.85, 139.76) | -1.69 (-2.05, -1.33) |
| 70-74 years | 28064.7 (11468.3, 56576.6) | 39708.1 (19789.4, 71793.7) | 41.49 | 149.14 (60.94, 300.66) | 74.50 (37.13, 134.71) | -1.61 (-1.92, -1.30) |
| 75-79 years | 15814.9 (6682.0, 31495.1) | 23228.6 (11931.7, 40927.0) | 46.88 | 138.96 (58.71, 276.74) | 70.14 (36.03, 123.58) | -1.58 (-1.87, -1.29) |
| 80-84 years | 6640.7 (2915.3, 13102.9) | 12959.5 (6550.4, 22750.2) | 95.15 | 125.36 (55.04, 247.36) | 65.48 (33.10, 114.95) | -1.54 (-1.81, -1.27) |
| 85-89 years | 1887.1 (822.7, 3588.0) | 5765.8 (3041.6, 9965.5) | 205.54 | 111.87 (48.77, 212.70) | 60.53 (31.93, 104.62) | -1.55 (-1.80, -1.31) |
| 90-94 years | 296.6 (134.6, 563.1) | 1598.4 (848.5, 2809.7) | 438.91 | 96.68 (43.85, 183.51) | 54.52 (28.94, 95.83) | -1.49 (-1.69, -1.29) |
| 95+ years | 10.4 (6.4, 15.0) | 162.7 (101.1, 234.1) | 1464.42 | 25.62 (15.90, 37.11) | 25.46 (15.81, 36.64) | -0.19 (-0.40, 0.03) |
Abbreviations: DALY, disability-adjusted life years; EAPC, estimated annual percentage change; UI, uncertainty interval; CI, confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



