Submitted:
12 November 2024
Posted:
13 November 2024
You are already at the latest version
Abstract
Malaria is caused by parasites of the genus Plasmodium spp. and it is transmitted to humans when infected female Anopheles mosquito bite or feed for blood meal. According to World Health Organization, an estimated 249 million malaria incidences were reported in 2022. Diagnostic methods are vital for dealing with the global malaria burden and declining malaria incidence. The diagnosis by microscopy is considered a gold standard; however, rapid diagnostic tests (RDTs) have become a primary diagnostic test in many malaria endemic areas. RDT have many advantages like fast preparation and diagnosis results, easy handling, low-cost diagnosis, species identification. But this most implemented method is also not free of disadvantages. The deletion of pfHRP2/3, low sensitivity with low parasite levels, cross-reactivity and prozone effect are certain disadvantages of RDTs. In addition to microscopy and RDTs molecular methods have also been developed. The Quantitative Buffy Coat (QBC) has fast preparation and diagnosis results with high specificity, however, the requirement of fluorescent microscope and expert personnel along with the low sensitivity under field conditions are the disadvantages. Another molecular technique such as Polymerase chain reaction (PCR) and loop-mediated isothermal amplification (LAMP) provides results with higher specificity and sensitivity but have drawbacks in terms of requirements of specialized instrumentation and difficult implementation in endemic areas. On the other hand the mass spectrometry based diagnostic have certain drawbacks like low sensitivity and requirement of specialized costly instruments and reagents. Another molecular method based on flow cytometry has advantages like quantification of infected erythrocytes and automated parasite level calculations. However, low sensitivity, specialized instrumentation and difficult implementation in endemic areas are the dragging forces behind its large scale implications in diagnosis of malaria. Recently malaria diagnosis based on artificial intelligence system such as Artificial intelligence based object detection system (AIDMAN), Automated AI-based Microscopy (Easy Go scan) and smart phone based application for malaria diagnosis (Malaria Screener & PVF-Net) have been developed which can be implemented in the fields once the high sensitivity and specificity is achieved. Thus, there is an urgent need of the development of malaria diagnostic tools which has minimal disadvantage and show high sensitivity and specificity on the one hand and low cost on the other hand. Recently the gene deletions events have created a vacuum which can be filled with more advanced RDT. Recently we have identified a T-cell immunomodulatory protein which is secreted in the blood of infected mice and can be detected by ELISA. The RDT implying the T-cell immunomodulatory protein of P. falciparum is being developed in our lab, which may have advantages over other RDTs.
Keywords:
diagnostic
; malaria
; RDT
; LAMP
; PCR
; QBC
1. Introduction
Malaria is the most common parasitic infection caused by protozoan parasite Plasmodium and transmitted through the bite of female Anopheles mosquito [1].Out of 200 Plasmodium species, majorly 5 species have been found to show significant infection in humans (Plasmodium vivax, Plasmodium knowlesi, Plasmodium falciparum, Plasmodium ovale, Plasmodium malariae [2].
According to the global malaria report 2023 by World Health Organization (WHO), there were an approximately two hundred forty-nine million incidences of malaria in eighty-five malaria endemic countries and regions with an increment of five million of malaria cases [3]. Malaria is also prevalent in India, which accounts for approximately 1.4 % of the global burden [3]. Around 70% of malaria cases in India comes from five states that includes Odisha (36%), Chhattisgarh (12%), Jharkhand (9%), Madhya Pradesh (9%) and Maharashtra (5%) [4].
Malaria remains a leading cause of mortality and morbidity around the world. Timely and precise diagnosis plays a critical role in effectively managing the disease. The diagnosis of malaria can be achieved through various diagnostic methods such as Light microscopy, PCR-based tests, and Rapid diagnostic tests (RDTs) etc. [5,6,7].
Emerging advanced technologies like Loop-mediated Isothermal Amplification (LAMP), Mass-Spectrometry, and Enzyme-linked immunosorbent assay are showing promising results for diagnosing the malaria parasite [8,9]. Since 2010, it has been recommended by WHO that every suspected case of malaria should be verified either with Rapid diagnostic test or Light microscopy [10].
The development of novel technologies based on artificial intelligence and image analysis are revolutionizing malaria diagnostics by automating the diagnostic process and reducing reliance on expert microscopists. Convolutional Neural Network (CNN) models can now analyze microscopic images to detect parasitic infection and quantify parasitemia levels. Additionally the development of smart phone based applications such as Malaria screener and PVF-Net for the diagnosis of malaria is also emerging and potentially useful in endemic areas to screen larger populations efficiently with minimal resources [11,12].
Light microscopy is in use for over a century and considered as the standard method for malaria diagnosis [13]. However, it does have some limitations like it is time consuming, require skilled staff and infrastructure. The RDTs overcome all the major problems associated with microscopy and have been found to be very useful in endemic areas but recently, problems have been observed with the currently available RDTs as well [11]. Recently, deletion of HRP2 and HRP3 gene in Plasmodium falciparum have been observed in South America, African regions, and in some parts of India as well [14,15,16]. The Plasmodium lactate dehydrogenase (pLDH) based RDT cannot detect parasite in low density parasitemia and the sensitivity of the aldolase-based RDT also completely depends on the parasite-density [11]. Consequently, there is still a need for a reliable diagnostic test for the effective management and treatment of the disease.
The global malaria diagnostic market plays a critical role in the fight against malaria and the market has grown significantly due to the growing demand for early and accurate diagnosis. This rise has fueled the development of diagnostic technologies like RDTs, PCR, and LAMP etc. Global malaria market was valued at approximately $819 million and anticipated to expand at 5% compound annual growth rate (CAGR) by 2024-2032 [17].
2. Diagnosis of Malaria
The malarial infection symptoms are unspecific and thus unreliable to distinguish it from other tropical diseases(Health Organization, 2023).The effective diagnosis of the disease depends on several factors such as different species of the Plasmodium,different stages, parasitemia, immunity, and population movement etc.[1].
Diagnostic methods for infectious diseases should be rapid, easy, accurate, and cost effective. There are various techniques currently available for malaria diagnosis ranging from the earliest conventional light microscopy using blood smear to the cutting-edge techniques using rapid molecular method. In the past decade there has been growing interest in immunoassay based RDTs, flow cytometry, ELISA, and molecular method which includes real-time PCR, nested PCR, and LAMP [8,9].
2.1. Traditional Diagnostics Methods
Malaria is an age-old disease, and the traditional diagnostic methods of malaria predominantly involve clinical diagnosis on the basis of symptoms such as fever, headache, and chills etc. The light microscopy based examination of blood smears considered as the gold standard method to identify malarial parasites efficiently. In addition, serology testing that detects the antibodies produced in response to the infection was found to be ineffective to diagnose malaria as antibodies could persist even after clearance of infection.
2.1.1. Clinical Diagnosis of Malaria
Clinical diagnosis is the most widely used method by doctors around the world despite the early symptoms of malaria being indistinguishable.The initial malarial symptoms or indications are non-specific (flu-like) includes higher body temperature, headache, shivering, vomiting, nausea, wooziness, and anorexia (Figure 1)that makes it challenging to differentiate from other tropical illness [18,19].
The recent study in Ghana assessing different diagnostic method suggested that the sensitivity and specificity of clinical diagnosis are much lower as compared to the conventional microscopy and immuno-chromatographic assays [20].
2.1.2. Light Microscopy Based Diagnosis of Malaria
The microscopic detection of malaria involves the identification of Plasmodium species in the Giemsa-stained smears of peripheral blood films.The diagnosis of malaria by light microscopy (Figure 2) involves preparation of thin and thick blood films (thin film for species confirmation and thick for parasite detection) on clean glass slide followed by staining with 10% Giemsa stain and incubation for 10 min at RT, then removal of the stain by washing with water and its examination under the microscope usinghigh power immersion oil lens (100X) [21].
The percentage of parasitemia is used to determine malaria parasite load [22], and it is calculated by the following formula: % Parasitemia = No. of infected RBCs/ Total no. of red blood cells x 100. Parasite density is categorized as high parasitemia (>10%), moderate parasitemia (1–10%), and low parasitemia (<1%) [23]. Expert microscopy makes it possible to differentiate all four major species of malaria parasite that are competent to cause infection in humans [24].
The light microscopy based methods have certain advantages like low cost diagnosis; Parasite level calculations and species identification [25,26,27,28,29,30,31,32]. The conventional method of diagnosing malaria by microscopic analysis of stained blood films has a number of disadvantages. Because of its labor-intensive nature and need for specialized infrastructure and well-trained personnel, it is less viable in environments with low resources. In endemic locations, its reliability declines, and when parasitemia levels are low, it has difficulty in correctly detecting infections particularly in areas where malaria is most common (Table-1) [25,26,27,28,29,30,31,32].

Table 1.
Advantages, disadvantages, sensitivity and specificity of different Malaria diagnostic techniques.
Table 1.
Advantages, disadvantages, sensitivity and specificity of different Malaria diagnostic techniques.
| Diagnostic technique | Advantages | Disadvantages | Sensitivity | Specificity |
|---|---|---|---|---|
| Traditional Diagnostics methods | ||||
| Clinical Diagnosis | (i) No instrument or specific facility required [18,19] | (i) Challenging to differentiate from other tropical illness[18,19] | 17.2 % [20] | 86.5 % [20] |
| (ii) Only symptoms based [18,19] | ||||
| Microscopic examination | (i) Availability [1,25] | (i) Requires expert personnel [1,26,30] | 56 % [58] | 100 % [58] |
| (ii) Low-cost diagnosis [1,25] | (ii) Results are expert-dependent [1,26,30] | |||
| (iii) Parasite level calculations [29,30,32] | (iii) Thin vs thick blood film variations [1,28- 32, 61] | |||
| (iv)Species identification [1,27,29,30,31,32] | ||||
| Serology | (i) Seroprevalence study [1,34] | (i) Non-reliable diagnostic technique [35] | ||
| (ii) Malaria transmission [1,35] | (ii) Not indicative of active infection [35] | |||
| (iii) screening of potential blood donors[ 1,34] | ||||
| Advanced Diagnostic Methods | ||||
| Rapid Diagnostic Tests (RDTs) | (i) Fast preparation and diagnosis results [1,49,54,59] | (i) pfHRP2/3 gene deletions [49, 59,62,63] | 84.2% [55] | 99.8% [55] |
| (ii) Easy handling [1,49,54,59] | (ii) Low sensitivity with low parasite levels [49,59] | 63.4-100% [56] | 53.4-99.9% [56] | |
| (iii) Low-cost diagnosis [1,49,59] | (iii) Low sensitivity with P. ovale and P. malariae species [45,54]. | 84.2% [57] | 95.2%[57] | |
| (iv) Species identification [45,49,59] (usually P. falciparum from non-P. falciparum species) | (iv) Cross-reactivity [45,63] | 37–88% [58] | 93–100%[58] | |
| (v) Prozone effect [49,60] | 95% (HRP2)[11] | 95.2%(HRP2) [11] 98.5%(pLDH) [11] | ||
| 93.2% (pLDH) [11] | ||||
| Quantitative Buffy Coat (QBC) | (i) simple, reliable, and user-friendly [1,67,68,70,72] | (i) Requires expert personnel [1,67] | 70.5% [57] | 92.1%[57] |
| (ii) Rapid and sensitive [1,66,67,68,70] | (ii) Requires fluorescent microscopy set up [1,67] | 55.9 %[67] | 88.8 %[67] | |
| (iii) High specificity [65,66] | (iii) low sensitivity in field [70] | 93 % [69] | 99% [69] | |
| (iv) Less training time [66] | 97.7 %[70] | 99.7 %[70] | ||
| 70.9 %[70] (field) | 97.4 %[70] (field) | |||
| PCR | (i) High sensitivity and specificity [30,84,85,86,87,88,89,90,91] | (i) Specialized instrumentation [1,30,84,85,91] | 100% [84,90,91] | 100% [84,90,91] |
| (ii) Accurate Species identification [84,85,86,87,88,91] | (ii) Difficult implementation in endemic areas [30,84,85,87,91] | |||
| (iii) Reference tool for comparative studies [84,90,91] | (iii) Expensive diagnosis [1,30,84,85,88,91] | |||
| (iv) Works in low parasite density [87,88,89,91] | ||||
| LAMP | (i) High sensitivity and specificity [92,94,95,96,97] | (i) Less sensitive for other species (other than P. falciparum and P. vivax) [97] | 99 % (Pan) [96] | 100%(Pan)[96] |
| (ii) Species identification [94,96,97] | 90%(P. falciparum) [96] | 93%(P. falciparum) [96] | ||
| (iii) Inexpensive, No thermocyclers needed [92,94,95] | 95% [92] | 99% [92] | ||
| (iv) Less turnaround time, comparable to RDT [94] | 98.89% [94] | 100% [94] | ||
| 100% [58] | 86–99% [58] | |||
| 95–98% [95] | 91–99% [95] | |||
| Mass Spectrometry | (i) High specificity [102,103] | (i) Low sensitivity [102,103] | 52 % [101] | 92 % [101] |
| (ii) Early detection of infection [100] | (ii) Specialized and costly instrumentation [102, 103] | 80.2 % [102] | >95% [102] | |
| Flow cytometry | (i) Quantification of infected erythrocytes [102,103,105,106,107,108] | (i) Low sensitivity than PCR [106] | 100 % [107] | 98.39% [107] |
| (ii) Automated parasite level calculations [105,106,107,108] | (ii) Difficult implementation in endemic areas [105,106,107,108] | |||
2.1.3. Serological Test
Serological testing is commonly based on the detection of antibodies generated against the Plasmodium parasite. However, these tests are not considered to be appropriate as they arenot capable of determining whether the antibodies are produced due to the past or ongoing infection but they are usually utilized for epidemiological studies and for screening of potential blood donors [33]. There are several assays such as IFA, ELISA and hemagglutination tests etc. Despite being time consuming the immunofluorescence antibody testing (IFA) is a reliable test for detecting antimalarial antibodies. It is specifically useful for screening prospective blood donors to avoid transfusion-transmitted malaria (Table 1) [1,34,35].
2.2. Advancements in Malaria Diagnosis
Recent advancements focus on the identification of disease specific biomarkers that allow for more precise detection and characterization of the malarial infections. While traditional diagnostic methods of malaria primarily relies on blood or its products for detection of the disease but recent developments of non-invasive techniques using other bodily fluids such as saliva and urine have shown promising results. Techniques like nested-PCR targeting malarial small-subunit rRNA (18S PCR), Quantitative PCR, Chemiluminescent ELISA and UMT (Urine malaria test), which detects Pf-HRP2 in urine sample, are being used to diagnose malaria. In addition, there have been improvements in blood based assays as well that include methods like Loop-mediated isothermal amplification, Photo induced electron transfer (PET)-PCR, Biosensor based Quartz crystal Microbalance technology, SELEX (Systematic Evolution of Ligands by Exponential Enrichment) holds the potential to revolutionize the field of malaria diagnostics [36,37,38,39].
In order to reduce the dependency on conventional microscopy several software, applications, and tools are also being developed to detect malaria parasite in thick and thin blood smear’s microscopic images [32]. These approaches aim to automate the detection of the disease using deep learning Artificial Intelligence (AI) and advanced image analysis to streamline the procedure of diagnosis. Convolutional neural networks are used as trained classifier models to identify specific objects or features in images and videos using deep learning algorithms; it is specifically used in healthcare for medical diagnosis of various diseases [40].
2.2.1. Rapid Diagnostic Test
RDT is a lateral flow device that is based on the principle of immunochromatography which involves the movement of liquid across the nitrocellulose membrane (Figure 3). During testing the parasitic antigen from the patient’s blood is captured by a monoclonal antibody that is attached to a gold particle or a liposome with dye, these monoclonal antibodies are raised against the target malaria antigen. Another antibody captures the antigen-antibody complex as it moves across the nitrocellulose membrane in the immobile phase which results in generating a clear line. A labeled goat anti-mouse antibody is used as a control to ensure if test works properly or not [41,42].
Currently there are several RDT kits available that targets HRP2 (Histidine-rich protein2), Aldolase, and pLDH antigen for the detection of the malaria. HRP2 is a surface membrane protein in RBC which is produced in abundance during asexual stage of the Plasmodium parasite and it has been found highly specific for Plasmodium falciparum infection [43,44,45,46,47,48]. LDH is a soluble glycolytic enzyme which is expressed at high-levels in blood-stage of Plasmodium. PLDH based RDTs effectively detect two species of Plasmodium i.e P. vivax and P. falciparum [47,48]. Aldolase is also an enzyme produced during glycolytic pathway of malaria parasite and its presence has been observed in all Plasmodium species that makes it capable to detect all infections of malaria [48,49].
RDT test involves the collection of blood samples and placing the sample on the pad specified for samples. Then few drops of buffers are placed in the sample pad and the results are obtained within minutes (Figure 4).
Many studies have demonstrated that RDT-based diagnosis of malaria shows robust performance in terms of sensitivity and specificity of the test [50,51,52,53]. Although RDTs cannot determine the parasite burden of patients and its sensitivity also decreases with low parasitemia (<100 parasites/uL), still it is thought to be the most reliable method for screening large populations in resource-limited areas [49].
The development of RDTs around 1990s resolved some of the issues linked with conventional microscopy and PCR based diagnosis, it is rapid and easy to use and requires minimal understanding [54]. Also, it was found very reliable in endemic areas to screen large population in short period of time. In a comparative study the sensitivity and specificity for P. falciparum using HRP2 based RDT has been found to be 95 % and 95.2% respectively. Similarly, for pLDH based RDT 93.2% and 98.5% sensitivity and specificity were respectively obtained [11,55,56,57,58]. But, recently deletion of HRP2 gene in Plasmodium falciparum have been observed in South America, African regions, and in some parts of India as well [14,15,16], the PLDH based RDT cannot detect parasite in low density parasitemia and parasite released aldolase enzyme in low concentrations decreases sensitivity of the aldolase-based RDT [11]. Large number of studies has highlighted issues with the currently available antigen-based RDTs [49,59,60,61,62,63,64]. Thus there is a critical need to find a novel species-specific target that can efficiently detect parasite infection and free from all the issues.
2.2.2. Quantitative Buffy Coat (QBC) Test
The quantitative buffy coat analysis is a well-known and a highly sensitive test which was developed to enhance the detection of malaria in peripheral blood [65]. QBC method relies on fluorescence and density-gradient centrifugation of malaria infected erythrocytes [66]. In QBC technique fluorescent dyes are used (Acridine orange) to stain the parasitic DNA in infected blood specimen followed by centrifugation at high speed for five minutes and then the detection of the malaria causing parasite under fluorescent microscope [1]. Within non-fluorescing red blood cells, the parasite is spotted as green under fluorescence microscope [67].
In addition, the QBC test has been found to be highly specific in identifying malaria in Indian set-up, where two species of Plasmodium i.e P. falciparum and P. vivax predominantly cause malaria [70]. QBC test is also a helpful technique in correctly diagnosing filariasis and visceral leishmaniasis [65].Studies demonstrated that QBC test is a reliable diagnostic tool for malaria.It shows excellent specificity, sensitivity, and possesses good accuracy in identifying both positive and negative results[57,67,68,69]. The field sensitivity of QBC test has been reported to decrease significantly under field condition [70].
Despite its high specificity and sensitivity QBC is not a suitable diagnostic test in resource-limited endemic areas, because it requires specialized equipments, trained lab staff, and a good infrastructure to carry out the testing operations (Table-1). The quantitative buffy coat test that involves centrifugation and use of acridine orange dye to visualize parasite under fluorescent microscope, the studies demonstrated that QBC possess better sensitivity compared to the microscopic examination, however, it requires skilled lab staff, infrastructure to carry out testing, and high costs (Table-1) [1,31,65,71,72].
2.3.3. Molecular Diagnosis of Malaria
The molecular amplification of 18S rRNA which is conserved in all Plasmodiumspecies was first implemented by scientists using Nested PCR technique [73] since then molecular based diagnosis of malaria is constantly evolving with the development of RT-PCR, Nucleic Acid Sequence-Based Amplification (NASBA), Reverse-transcriptase PCR and LAMP. These PCR based diagnosis can detect multiple gene targets and it has been shown to be more sensitive than microscopy [74].
RDT and Microscopy can detect 100-200 parasites/μl whereas molecular diagnostic methods such as PCR, LAMP, mass spectrometry, and flow cytometry can detect 5-50 parasites/μl [75,76]. Thus, studies have demonstrated the higher sensitivity of molecular methods as compared to other methods.,
2.3.3.1. Polymerase Chain Reaction (PCR)
The polymerase chain reaction attributed as a reliable test for identifying the mixed infections with better sensitivity as compared to the other laboratory tests. It involves the use of two sets of primers, from which one set of primer is used to detect the presence of the Plasmodium and the other set is species-specific that will only amplify when the particular-species is present in the sample such as Plasmodium falciparum [77,78].
Real Time PCR use fluorescence based technology and can efficiently detect the target amplicons in real time and the melting curve analysis is done to precisely differentiate the Plasmodium species [10,79,80,81,82]. Whereas the multiplex-PCR is capable of amplifying multiple target sequences in a single reaction using different pair of primers for each target but it is also associated with several problems such as non-specific amplification and mispriming artifacts. However, the nested-PCR performs two steps of amplification, the product from first step amplification serves as the template for secondary amplification and use different set of primers internal to those used in primary PCR to avoid mispriming artifacts and primer dimer. Nested-PCR can detect submicroscopic malaria parasite with a low density of 10 parasite/µl of blood [83].
Diverse studies suggests that PCR based diagnosis of malaria possesses better sensitivity and specificity in comparison with the other two most widely used diagnostics and is also able to identify missed cases by these tests [29,84,85,86,87,88,89,90,91]. PCR based molecular diagnosis of malaria considered as more suitable technique compared to other conventional methods as it possess better sensitivity and specificity [88]. While it is more sensitive and capable of identifying the parasite at the species level, it is linked to multiple challenges such as it is not very reliable in remote areas, diagnosis takes 2-3h and associated with high costs [29,84].
2.3.3.2. Loop-Mediated Isothermal Amplification (LAMP)
The LAMP technique is considered to be more simplified and affordable technique. It identifies the Plasmodium falciparum’s conserved 18s ribosomal RNA gene and is also able to detect other Plasmodium species as well [92]. In LAMP assay amplification is done at a constant temperature i.e. around 62-65℃. DNA is amplified 109-1010 times in 15-60 min and the amplification is monitored using SYBR Green dye and automated monitoring using a turbidity meter (Figure 5) [36].
A meta-analysis of multiple studies demonstrated the LAMP method's sensitivity is between 93.9 to 100% and specificity is ranged between 93.8 to 100%, which makes it comparable with PCR based diagnostics [58,93,94,95]. Further it is less time consuming and capable of detecting all Plasmodium species efficiently [95,96,97,98].
The molecular technique known as loop-mediated isothermal amplification (LAMP) has been released into the market to detect malaria. LAMP satisfies the requirements for a point-of-care diagnostic screening test since it is easy to use and doesn't require sophisticated equipment or training [95,96,97]. So far LAMP technique producing better results as compared to other methods but more research and field studies has to be done to validate its results (Table 1).
2.3.3.3. Mass Spectrometry
The laser desorption mass-spectrometry based diagnostic for malaria has been developed two decades ago. It is based on the principle of identifying a heme group of hemozoin in a malaria infected samples and does not detect heme bound to hemoglobin or other proteins in uninfected samples [99].Based on a study Liquid Chromatography-Mass Spectrometry (LC-MS) was found to be a rapid and sensitive test and could detect <10 parasites/μl (Plasmodium falciparum) in infected blood samples. The comparative study demonstrated the detection of Plasmodium infection within 2 days post infection in 0.3μl of blood sample whereas the microscopy and colorimetric hemozoin detects the infection between 2-5 days [100]. Samples from pregnant women with submicroscopic parasitemia, hemozoin screening using Laser desorption-time of flight (LD-TOF) showed sensitivity of 52% and specificity of 92% when compared with PCR [101]. Recently, a study has shown a high specificity (>95%) but insufficient sensitivity (80.2%) of LD-TOF-based detection of hemozoin for malaria screening [102]. In yet another study more than 10 peaks specific for P. falciparum were identified in the blood of infected patient by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF-MS) suggesting the potential of the technique for the diagnosis of malaria. However the sensitivity was not sufficient in this study also [103].
2.3.3.4. Flow Cytometry
Flow cytometry is a high throughput technique to count and separate viable cells in a stream of fluid using a laser device that reveal the fluorescent markers on the cells [104].Flow cytometry provide more insights about the growth and development of malaria parasite compared to any other currently available techniques [8]. The flow cytometry based investigation of malaria parasite in blood stage relies on the absence of DNA in normal RBCs, The ratio of RBCs that stain positive for DNA to the total number of RBCs analyzed can be used to accurately determine the parasitemia in blood samples (Figure 6).
In the first use of flow cytometry to detect malaria parasite, the test blood samples were mixed with saponin that lyse the RBC without affecting parasite and WBCs. Cells were then stained using two fluorescent dyes i.e. Hoechst 33258 and a FACStarto analyze the parasitic DNA. Parasite and WBCs were then differentiated by blue Hoechst 33258 fluorescence and forward scattering [105]. More simpler and rapid tri-colour flow cytometry assay was developed in 2011 which helps to quantify, characterize and differentiate different Plasmodium species. Leukocytes were detected using an antibody against CD45, and the parasites were stained with dihydroethidium, Hoechst 33342, or SYBR Green I. [106]. In a recent study compared to microscopy sensitivity of 100% (95% CI: 97.13–100) and specificity of 98.39% (95% CI: 95.56–100), has been reported for the diagnosis of imported malaria cases. Moreover, the study showed determination of parasitemia in a very short time compared to other methods [107]. Flow cytometry based diagnosis of malaria has significant disadvantages like it is an expensive, labour-intensive, and requires trained laboratory staff though it is incredibly useful in malaria studies and for malaria screening [29,108].
2.3. Artificial Intelligence and Image Analysis Techniques
Artificial intelligence is a transformative technology that has potential to revolutionize the field of malaria diagnosis. Convolutional neural networks (CNNs) are AI models (such as YOLOv5, R-CNN, SSD, and RetinaNet) can help in analyzing microscopic images of thick and thin blood smear sample using deep learning tools. Deep Malaria convolutional neural network classifier model (Deep MCNN) capable of estimating parasitemia in malarial parasite MP/ul as recommended by WHO. It can calculate total malaria parasite and WBCs count and achieves a sensitivity and specificity ratio of 0.92/0.90 compared to expert level microscopy [109]. Additional, development of handheld microscopes or smartphone microscope also has a great potential in the field of diagnosis. Several studies have been done for the use of cyscope which is a portable fluorescent microscope. It is considered as a rapid detection test for malaria and provides result within 10 minutes. This technique has capability to quantify parasitemia from blood specimen [110,111,112,113,114,115,116].
2.3.1. Artificial Intelligence Based Object Detection System (AIDMAN)
AIDMAN is an AI tool that uses deep learning algorithms to detect Plasmodium parasite in thin blood smear images with an accuracy of 98.4% comparable to the expert microscopists. It uses a combination of YOLOv5 and Transformer model for image analysis for detection of malaria parasite [117]. It may be utilized to screen more samples in limited-resource areas in order to reduce cost and time. Other AI systems for Plasmodium detection using smartphone have been reported [118,119,120].
2.3.2. Automated AI-Based Microscopy (Easy Go Scan)
A fully automated microscopy that scans the blood film sample of patients and uses an AI software to detect and quantify malaria parasite through image processing with an accuracy of 88% has been developed by UK scientist. The system called EasyScan GO detects malaria parasites in field-prepared Giemsa-stained blood films [121].
For clinical validation researchers have sampled around 1200 blood samples of people who traveled to UK from malaria endemic areas, out of 113 positive samples for malaria automated microscope were able to detect 99 positive samples with an accuracy of 88%. AI software cannot be considered as good as expert microscopist as it has also given 122 false positive samples, but it can be improved further and trained on large datasets to provide more outstanding results [121].
2.3.3. Smartphone Based Application for Malaria Diagnosis (Malaria Screener & PVF-Net)
Malaria screener is a first smartphone-based application that can detect Plasmodium falciparum infection from Giemsa-stained blood smears with an accuracy of 74% compared to the expert microscopy and 71% when compared with the nested PCR as reference. During microscopy the malaria screener app requires mounting a smartphone onto the microscope’s eyepiece then app will automatically capture an image, process it instantly, and displays the result on the screen. Its accuracy reaches 91.8% when threshold of parasite count (number of parasite used to determine whether a patient was infected or uninfected) was shifted [122]. Plasmodium VF-Net was developed as a more improved algorithm that can detect both P. falcifarum and P. vivax infections. It is trained using a sample datasets from Bangladesh [123] and provides an accuracy of 83.1% when compared with microscopy and 81% when compared with the nested PCR. Smartphone based application shows immense potential to be used in limited-resource settings for routine screening of malaria in endemic areas.It will help to reduce the reliance on expert microscopists and saves both time and cost.
2.4. Malaria Diagnostic Market
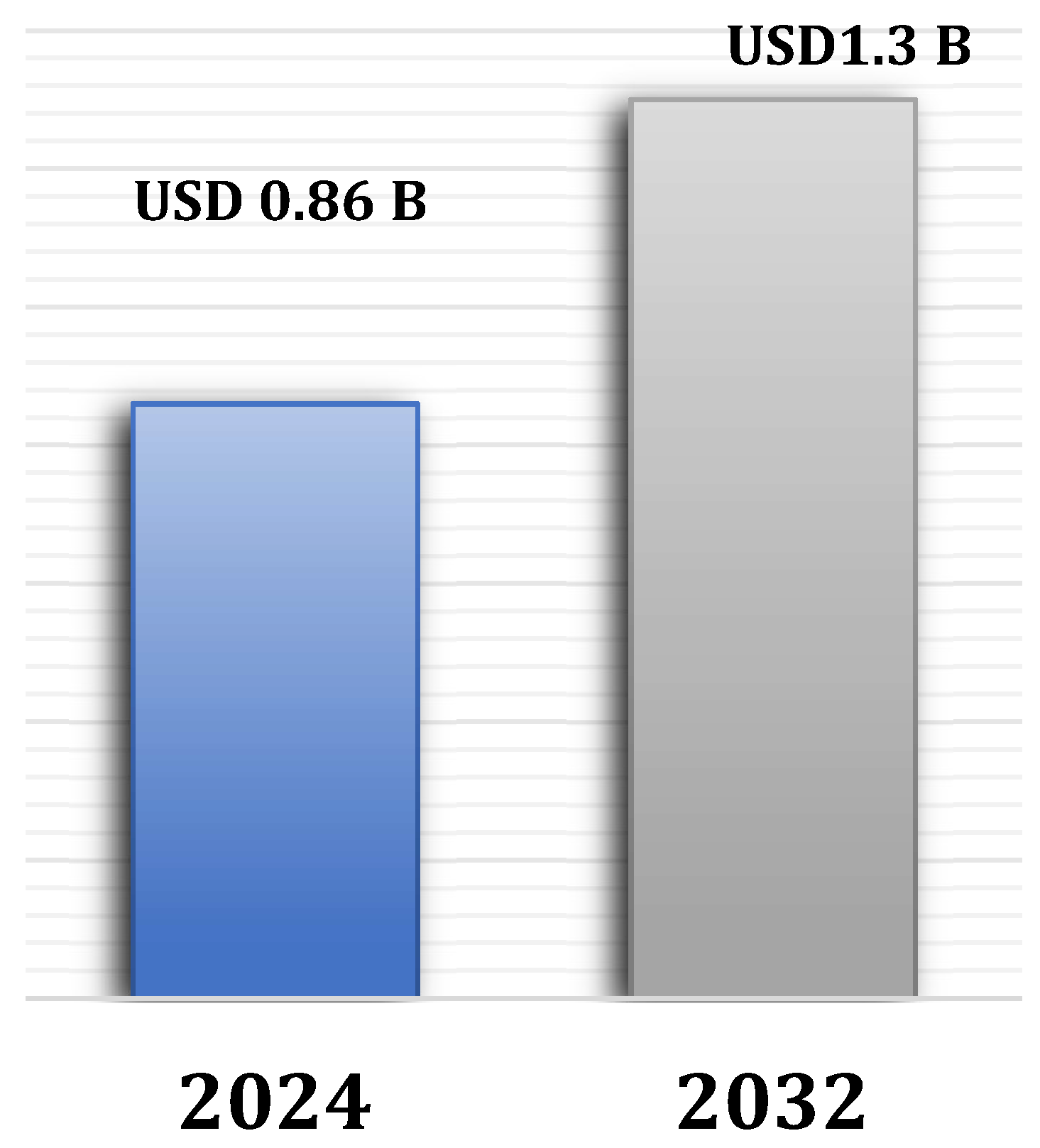
Malaria remains the prevalent, life-threatening disease worldwide. Malaria diagnostic market is becoming dynamic and evolving sector that plays a crucial rolein the global fight against malaria. The list of available malarial RDTs shows worldwide existence [124]. The primary factor that drives the market is the elevating incidences of malaria which leads to the increasing demand for effective malaria diagnostics. In 2023, the global malaria diagnostic market was valued at approximately USD 819.1 million and it is anticipated that it will grow at 5%CAGRduring the projection period from2024 to 2032 (Figure 7) [17]. The major factor behind this enormous growth is the ongoing advancements in diagnostic technologies, increasing investment in global health initiatives, increased emphasis on enhancing diagnostic accessibility and accuracy in endemic areas [17].
2.4.1. Challenges and Opportunities
The precise and timely detection of malaria infection is indeed critical for effective management and treatment. In many regions delays in diagnosis and treatment often leads to severe complications and fatalities. However, diagnosing malaria presents significant challenges especially in resource-limited countries where malaria is highly prevalent. There is lack of more accurate, rapid and cost-effective diagnostic tool which highlights the urgent need of an improved diagnostic tool to streamline the testing process.
Incentives to drive innovation in malaria diagnostic are constrained due to narrow profit margins and mostly innovations are donors funded leading to slow progress. The malaria RDTs that detect Pf-HRP2 continue to be the leading product in the donor-funded market, accounting for 70-80% of the total volume [46]. In 2022, RDTs segment led the malarial diagnostic market, having the valuation of 53.69% in the revenue share. WHO estimates show that more than 312 million RDTs were distributed worldwide in the year 2016 [125]. At present, there are multiple prequalified RDT options that are available for each standard case management test type (such as HRP2-detecting tests for Plasmodium falciparum, Pf/pan, and Pf/Pv). However, there are still very few options for regions experiencing Pf-HRP2/3 gene deletions. The molecular technique known as loop-mediated isothermal amplification (LAMP) was just released into the market to detect malaria (Loopamp™ Malaria Pv, Eiken Chemical, Tokyo, Japan). LAMP satisfies the requirements for a point-of-care diagnostic screening test since it is easy to use and doesn't require sophisticated equipment or training [98]. So far LAMP technique producing better results as compared to other methods but more research and field studies has to be done to validate its results.In the post COVID-19 era, now governments and international health organizations are likely to be more focused towards malaria, which could result in increased funding for malaria diagnostics.
Ongoing innovations and development of new diagnostic tools present significant opportunities for early detection particularly in resource-limited areas, where advanced diagnostics can play key role to effectively manage and treat malaria. Recently we have shown the effectiveness of ELISA in detecting the T-Cell immunomodulatory protein of P. berghei in the sera of infected mice [126]. Presently we are working on the development of RDT diagnostic kit based on T-cell immunomodulatory protein of P. falciparum.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, X.X. and Y.Y.; methodology, X.X.; software, X.X.; validation, X.X., Y.Y. and Z.Z.; formal analysis, X.X.; investigation, X.X.; resources, X.X.; data curation, X.X.; writing—original draft preparation, X.X.; writing—review and editing, X.X.; visualization, X.X.; supervision, X.X.; project administration, X.X.; funding acquisition, Y.Y. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
Please add: “This research received no external funding” or “This research was funded by NAME OF FUNDER, grant number XXX” and “The APC was funded by XXX”. Check carefully that the details given are accurate and use the standard spelling of funding agency names at https://search.crossref.org/funding. Any errors may affect your future funding.
Data Availability Statement
In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Please refer to suggested Data Availability Statements in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics. If the study did not report any data, you might add “Not applicable” here.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
Declare conflicts of interest or state “The authors declare no conflict of interest.” Authors must identify and declare any personal circumstances or interest that may be perceived as inappropriately influencing the representation or interpretation of reported research results. Any role of the funders in the design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript; or in the decision to publish the results must be declared in this section. If there is no role, please state “The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results”.
References
- Tangpukdee, N., Duangdee, C., Wilairatana, P., &Krudsood, S. (2009). Malaria Diagnosis: A Brief Review. The Korean Journal of Parasitology, 47(2), 93. [CrossRef]
- Kantele, A., &Jokiranta, T. S. (2011). Review of cases with the emerging fifth human malaria parasite, Plasmodium knowlesi. In Clinical Infectious Diseases (Vol. 52, Issue 11, pp. 1356–1362). [CrossRef]
- World malaria report 2023. Available online: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2023 (accessed on 05-09-2024). Available online:.
- Narain, J. P. , &Nath, L. M. (2018). Eliminating malaria in India by 2027: The countdown begins! In Indian Journal of Medical Research (Vol. 148, Issue 2, pp. 123–126). Indian Council of Medical Research. [CrossRef]
- Bell, D. , Wongsrichanalai, C., & Barnwell, J. W. (2006). Ensuring quality and access for malaria diagnosis: how can it be achieved? Nature Reviews Microbiology, 4(S9), S7–S20. [CrossRef]
- Bhandari PL, Raghuveer CV, Rajeev A, Bhandari PD. Comparative study of peripheral blood smear, quantitative buffy coat and modified centrifuged blood smear in malaria diagnosis. Indian J PatholMicrobiol. 2008;51(1):108-112. [CrossRef]
- Ngasala, B. , Mubi, M., Warsame, M., Petzold, M. G., Massele, A. Y., Gustafsson, L. L., Tomson, G., Premji, Z., &Bjorkman, A. (2008). Impact of training in clinical and microscopy diagnosis of childhood malaria on antimalarial drug prescription and health outcome at primary health care level in Tanzania: A randomized controlled trial. Malaria Journal, 7(1), 199. [CrossRef]
- Grimberg, B. T. (2011). Methodology and application of flow cytometry for investigation of human malaria parasites. Journal of Immunological Methods, 367(1–2), 1–16. [CrossRef]
- Wilson, M. L. (2013). Laboratory Diagnosis of Malaria: Conventional and Rapid Diagnostic Methods. Archives of Pathology & Laboratory Medicine, 137(6), 805–811. [CrossRef]
- Fitri, L. E. , Widaningrum, T., Endharti, A. T., Prabowo, M. H., Winaris, N., &Nugraha, R. Y. B. (2022). Malaria diagnostic update: From conventional to advanced method. Journal of Clinical Laboratory Analysis, 36(4). [CrossRef]
- Mouatcho, J. C. , & Dean Goldring, J. P. (2013). Malaria rapid diagnostic tests: Challenges and prospects. In Journal of Medical Microbiology (Vol. 62, Issue PART10, pp. 1491–1505). [CrossRef]
- Yu H, Mohammed FO, Abdel Hamid M, et al. Patient-level performance evaluation of a smartphone-based malaria diagnostic application. Malar J. 2023;22(1):33. Published 2023 Jan 27. [CrossRef]
- Ledermann D, W. (2008). [Laveran, Marchiafava and paludism]. RevistaChilena de Infectologia : OrganoOficial de La SociedadChilena de Infectologia, 25(3), 216–221.
- Baker, J. , Ho, M.-F., Pelecanos, A., Gatton, M., Chen, N., Abdullah, S., Albertini, A., Ariey, F., Barnwell, J., Bell, D., Cunningham, J., Djalle, D., Echeverry, D. F., Gamboa, D., Hii, J., Kyaw, M. P., Luchavez, J., Membi, C., Menard, D., … Cheng, Q. (2010). Global sequence variation in the histidine-rich proteins 2 and 3 of Plasmodium falciparum: implications for the performance of malaria rapid diagnostic tests. Malaria Journal, 9(1), 129. [CrossRef]
- Gamboa, D. , Ho, M.-F., Bendezu, J., Torres, K., Chiodini, P. L., Barnwell, J. W., Incardona, S., Perkins, M., Bell, D., McCarthy, J., & Cheng, Q. (2010). A Large Proportion of P. falciparum Isolates in the Amazon Region of Peru Lack pfhrp2 and pfhrp3: Implications for Malaria Rapid Diagnostic Tests. PLoS ONE, 5(1), e8091. [CrossRef]
- 16. Kumar, N., Pande, V., Bhatt, R. M., Shah, N. K., Mishra, N., Srivastava, B., Valecha, N., & Anvikar, A. R. (2013). Genetic deletion of HRP2 and HRP3 in Indian Plasmodium falciparum population and false negative malaria rapid diagnostic test. Acta Tropica, 125(1), 119–121. [CrossRef]
- Malaria Diagnostics Market Size. Available onine: https://www.gminsights.com/industry-analysis/malaria-diagnostics-market/market-size (accessed on 07.10.2024). (accessed on 07.10.2024).
- Bartoloni, A., & Zammarchi, L. (2012). Clinical aspects of uncomplicated and severe malaria. Mediterranean Journal of Hematology and Infectious Diseases, 4(1), e2012026. 4. [CrossRef]
- Warrell, D. A. (2017). Essential Malariology, 4Ed. CRC Press. [CrossRef]
- Prah, J. K., Amoah, S., Yartey, A. N., Ampofo-Asiama, A., &Ameyaw, E. O. (2021). Assessment of malaria diagnostic methods and treatments at a Ghanaian health facility. The Pan African Medical Journal, 39, 251. [CrossRef]
- Cheesbrough, M. (2005). District Laboratory Practice in Tropical Countries. Cambridge University Press. [CrossRef]
- Azikiwe, C. C. A. , Ifezulike, C. C., Siminialayi, I. M., Amazu, L. U., Enye, J. C., &Nwakwunite, O. E. (2012). A comparative laboratory diagnosis of malaria: microscopy versus rapid diagnostic test kits. Asian Pacific Journal of Tropical Biomedicine, 2(4), 307–310. [CrossRef]
- Bayisa, G., &Dufera, M. (2022). Malaria Infection, Parasitemia, and Hemoglobin Levels in Febrile Patients Attending Sibu Sire Health Facilities, Western Ethiopia. BioMed Research International, 2022, 1–8. 2022. [CrossRef]
- WHO. Malaria Microscopy Quality Assurance Manual—Ver. 2. WHO. WHO Press; 2016. 1-2 p.
- Diagnosing malaria. Available online: www.who.int/westernpacific/activities/diagnosing-malaria# (accessed on 10.10.2024). Available online:.
- Guintran, J.-O. , Delacollette, C., and Trigg, P. (2006). Systems for the Early Detection of Malaria Epidemics in Africa, 1–100 http://www.li.mahidol.ac.th/ thainatis/pdf-ebook/ebook77.pdf.
- Collins, W. E. , and Jeffery, G. M. (2007). Plasmodium malariae: parasite and disease. Clin. Microbiol. Rev. 20, 579–592. [CrossRef]
- Dowling, M. A. , and Shute, G. T. ( 1966). A comparative study of thick and thin blood films in the diagnosis of scanty malaria parasitaemia. Bull. World Health Organ. 34, 249–267. [PubMed]
- Wangai, L. N. , Karau, M. G., Njiruh, P. N., Sabah, O., Kimani, F. T., Magoma, G., et al. (2011). Sensitivity of microscopy compared to molecular diagnosis of P. falciparum: implications on malaria treatment in epidemic areas in Kenya. Afr. J. Infect. Dis. 5, 1–6. [CrossRef]
- Poostchi, M., Silamut, K., Maude, R. J., Jaeger, S., and Thoma, G. (2018). Image analysis and machine learning for detecting malaria. Transl. Res. 194, 36–55. [CrossRef]
- Evaluation and Diagnosis (2019). Shujatullah-Malaria-Diagnosis and Treatment (United States)– Diagnosis (U.S.). Centres for Diseases Control and Prevention CDC, CDC. Available at: https://www.cdc.gov/malaria/hcp/clinical-guidance/evaluation-diagnosis.html.
- Maturana, C. R. , de Oliveira, A. D., Nadal, S., Bilalli, B., Serrat, F. Z., Soley, M. E., Igual, E. S., Bosch, M., Lluch, A. V., Abelló, A., López-Codina, D., Suñé, T. P., Clols, E. S., & Joseph-Munné, J. (2022). Advances and challenges in automated malaria diagnosis using digital microscopy imaging with artificial intelligence tools: A review. Frontiers in Microbiology, 13. [CrossRef]
- Voller, a. , &Draper, C. C. (1982). Immunodiagnosis and sero-epidemiology of malaria. British Medical Bulletin, 38(2), 173–178. [CrossRef]
- Mungai, M. , Tegtmeier, G., Chamberland, M., &Parise, M. (2001). Transfusion-Transmitted Malaria in the United States from 1963 through 1999. New England Journal of Medicine, 344(26), 1973–1978. [CrossRef]
- Oviedo, A., Knipes, A., Worrell, C., Fox, L. A. M., Desir, L., Fayette, C., et al. (2020). Combination of serological, antigen detection, and DNA data for Plasmodium falciparum provides robust geospatial estimates for malaria transmission in Haiti. Sci. Rep. 10, 8443–8449. [CrossRef]
- Lucchi, N. W. , Demas, A., Narayanan, J., Sumari, D., Kabanywanyi, A., Kachur, S. P., Barnwell, J. W., &Udhayakumar, V. (2010). Real-Time Fluorescence Loop Mediated Isothermal Amplification for the Diagnosis of Malaria. PLoS ONE, 5(10), e13733. [CrossRef]
- Lucchi, N. W. , Karell, M. A., Journel, I., Rogier, E., Goldman, I., Ljolje, D., Huber, C., Mace, K. E., Jean, S. E., Akom, E. E., Oscar, R., Buteau, J., Boncy, J., Barnwell, J. W., & Udhayakumar, V. (2014). PET-PCR method for the molecular detection of malaria parasites in a national malaria surveillance study in Haiti, 2011. Malaria Journal, 13(1), 462. [CrossRef]
- Putaporntip, C. , Buppan, P., &Jongwutiwes, S. (2011). Improved performance with saliva and urine as alternative DNA sources for malaria diagnosis by mitochondrial DNA-based PCR assays. Clinical Microbiology and Infection, 17(10), 1484–1491. [CrossRef]
- Krampa, F. D., Aniweh, Y., Kanyong, P., &Awandare, G. A. (2020). Recent Advances in the Development of Biosensors for Malaria Diagnosis. Sensors, 20(3), 799. [CrossRef]
- Sarvamangala, D. R. , &Kulkarni, R. V. (2022). Convolutional neural networks in medical image understanding: a survey. Evolutionary Intelligence, 15(1), 1–22. [CrossRef]
- Moody, A. (2002). Rapid Diagnostic Tests for Malaria Parasites. Clinical Microbiology Reviews, 15(1), 66–78. [CrossRef]
- Murray, C. K., D. Bell, R. A. Gasser, and C. Wongsrichanalai. 2003. Rapid diagnostic testing for malaria. Trop. Med. Int. Health 8:876-883.
- Rock, E. P. , Marsh, K., Saul, A. J., Wellems, T. E., Taylor, D. W., Maloy, W. L., & Howard, R. J. (1987). Comparative analysis of the Plasmodium falciparumhistidine-rich proteins HRP-I, HRP-II and HRP-III in malaria parasites of diverse origin. Parasitology, 95(2), 209–227. [CrossRef]
- Bell D, Wongsrichanalai C, Barnwell JW. Ensuring quality and access for malaria diagnosis: how can it be achieved?. Nat Rev Microbiol. 2006;4(9):682-695. [CrossRef]
- Murray, C. K. , and Bennett, J. W. ( 2009). Rapid diagnosis of malaria. Interdiscip. Perspect. Infect. Dis. 2009, 1–7. [CrossRef]
- World Health Organization. "Malaria rapid diagnostic test performance: results of WHO product testing of malaria RDTs: round 8 (2016–2018)." (2018).
- Michael L. Wilson, Malaria Rapid Diagnostic Tests, Clinical Infectious Diseases, Volume 54, Issue 11, 1 June 2012, Pages 1637–1641. [CrossRef]
- Barney R, Velasco M, Cooper CA, et al. Diagnostic Characteristics of Lactate Dehydrogenase on a Multiplex Assay for Malaria Detection Including the Zoonotic Parasite Plasmodium knowlesi. Am J Trop Med Hyg. 2021;106(1):275-282. Published 2021 Nov 15. [CrossRef]
- Kavanaugh, M. J. , Azzam, S. E., &Rockabrand, D. M. (2021). Malaria Rapid Diagnostic Tests: Literary Review and Recommendation for a Quality Assurance, Quality Control Algorithm. Diagnostics, 11(5), 768. [CrossRef]
- Kyabayinze, D. J. , Tibenderana, J. K., Odong, G. W., Rwakimari, J. B., &Counihan, H. (2008). Operational accuracy and comparative persistent antigenicity of HRP2 rapid diagnostic tests for Plasmodium falciparum malaria in a hyperendemic region of Uganda. Malaria Journal, 7(1), 221. [CrossRef]
- Berzosa, P. , de Lucio, A., Romay-Barja, M., Herrador, Z., González, V., García, L., Fernández-Martínez, A., Santana-Morales, M., Ncogo, P., Valladares, B., Riloha, M., & Benito, A. (2018). Comparison of three diagnostic methods (microscopy, RDT, and PCR) for the detection of malaria parasites in representative samples from Equatorial Guinea. Malaria Journal, 17(1), 333. [CrossRef]
- Ogunfowokan, O. , Ogunfowokan, B. A., &Nwajei, A. I. (2020). Sensitivity and specificity of malaria rapid diagnostic test (mRDTCareStatTM) compared with microscopy amongst under five children attending a primary care clinic in southern Nigeria. African Journal of Primary Health Care & Family Medicine, 12(1). [CrossRef]
- Badiane, A. , Thwing, J., Williamson, J., Rogier, E., Diallo, M. A., &Ndiaye, D. (2022). Sensitivity and specificity for malaria classification of febrile persons by rapid diagnostic test, microscopy, parasite DNA, histidine-rich protein 2, and IgG: Dakar, Senegal 2015. International Journal of Infectious Diseases, 121, 92–97. [CrossRef]
- Cunningham, J. , Jones, S., Gatton, M. L., Barnwell, J. W., Cheng, Q., Chiodini, P. L., Glenn, J., Incardona, S., Kosack, C., Luchavez, J., Menard, D., Nhem, S., Oyibo, W., Rees-Channer, R. R., Gonzalez, I., & Bell, D. (2019). A review of the WHO malaria rapid diagnostic test product testing programme (2008–2018): performance, procurement and policy. Malaria Journal, 18(1), 387. [CrossRef]
- DiMaio, M. A., Pereira, I. T., George, T. I., andBanaei, N. (2012). Performance of BinaxNOW for diagnosis of malaria in a U.S. hospital. J. Clin. Microbiol. 50, 2877–2880. [CrossRef]
- Boyce, M. R. , and O’Meara, W. P. (2017). Use of malaria RDTs in various health contexts across sub-Saharan Africa: a systematic review. BMC Public Health 17, 470–415. [CrossRef]
- Ifeorah, I. K., Brown, B. J., and Sodeinde, O. O. (2017). A comparison of rapid diagnostic testing (by plasmodium lactate dehydrogenase), and quantitative buffy coat technique in malaria diagnosis in children. Afr. J. Infect. Dis. 11, 31–38. [CrossRef]
- Feleke, D. G. , Alemu, Y., and Yemanebirhane, N. (2021). Performance of rapid diagnostic tests, microscopy, loop-mediated isothermal amplification (LAMP) and PCR for malaria diagnosis in Ethiopia: a systematic review and meta-analysis. Malar. J. 20, 384–311. [CrossRef]
- Wongsrichanalai, C. , Barcus, M., Muth, S., Sutamihardja, A., and Wernsdorfer, W. (2007). A review of malaria diagnostic tools: microscopy and rapid diagnostic test (RDT). Am. J. Trop. Med. Hyg. 77, 119–127. [CrossRef]
- Gillet, P., Mori, M., Van Esbroeck, M., Van den Ende, J., and Jacobs, J. (2009). Assessment of the prozone effect in malaria rapid diagnostic tests. Malar. J. 8, 1–7. [CrossRef]
- Bejon, P., Andrews, L., Hunt-Cooke, A., Sanderson, F., Gilbert, S. C., and Hill, A. V. S. (2006). Thick blood film examination for plasmodium falciparum malaria has reduced sensitivity and underestimates parasite density. Malar. J. 5, 5–8. [CrossRef]
- Nima, M. K. , Hougard, T., Hossain, M., Kibria, M., Mohon, A., Johora, F., et al. (2017). Case report: a case of plasmodium falciparum hrp2 and hrp3 gene mutation in Bangladesh. Am. J. Trop. Med. Hyg. 97, 1155–1158. [CrossRef]
- Orish, V. N., De-Gaulle, V. F., and Sanyaolu, A. O. (2018). Interpreting rapid diagnostic test (RDT) for Plasmodium falciparum. BMC. Res. Notes 11, 1–6. [CrossRef]
- Response plan to pfhrp2 gene deletions. Available online: https://www.who.int/publications/i/item/WHO-CDS-GMP-2019.02 (accessed on 12.10.2024).
- Ahmed, N. H. (2014). Quantitative Buffy Coat Analysis-An Effective Tool For Diagnosing Blood Parasites. JOURNAL OF CLINICAL AND DIAGNOSTIC RESEARCH. [CrossRef]
- Kochareka, M., Sarkar, S., Dasgupta, D., &Aigal, U. (2012). A preliminary comparative report of quantitative buffy coat and modified quantitative buffy coat with peripheral blood smear in malaria diagnosis. Pathogens and Global Health, 106(6), 335–339. [CrossRef]
- Adeoye, G. O. , &Nga, I. C. (2007). Comparison of Quantitative Buffy Coat technique (QBC) with Giemsa-stained thick film (GTF) for diagnosis of malaria. Parasitology International, 56(4), 308–312. [CrossRef]
- Pinto, M. J., Rodrigues, S. R., Desouza, R., &Verenkar, M. P. (2001). Usefulness of quantitative buffy coat blood parasite detection system in diagnosis of malaria. Indian Journal of Medical Microbiology, 19(4), 219–221.
- Gay, F., Traoré, B., Zanoni, J., Danis, M., &Gentilini, M. (1994). Evaluation of the QBC system for the diagnosis of malaria. Sante (Montrouge, France), 4(4), 289–297.
- Vaidya, K. A. , &Sukesh. (2012). Quantitative buffy coat (QBC) test and other diagnostic techniques for diagnosing malaria: review of literature. National Journal of Medical Research, 2(03), 386–388.
- Shujatullah, F., Malik, A., Khan, H. M., and Malik, A. (2006). Comparison of different diagnostic techniques in plasmodium falciparum cerebral malaria. J. Vector Borne Dis. 43, 186–190. [PubMed]
- Bhandari, P. L., Raghuveer, C. V., Rajeev, A., &Bhandari, P. D. (2008). Comparative study of peripheral blood smear, quantitative buffy coat and modified centrifuged blood smear in malaria diagnosis. Indian Journal of Pathology and Microbiology, 51(1), 108-112.
- Snounou, G. , Viriyakosol, S., Xin Ping Zhu, Jarra, W., Pinheiro, L., do Rosario, V. E., Thaithong, S., & Brown, K. N. (1993). High sensitivity of detection of human malaria parasites by the use of nested polymerase chain reaction. Molecular and Biochemical Parasitology, 61(2), 315–320. [CrossRef]
- Lazrek, Y., Florimond, C., Volney, B., Discours, M., Mosnier, E., Houzé, S., Pelleau, S., & Musset, L. (2023). Molecular detection of human Plasmodium species using a multiplex real time PCR. Scientific Reports, 13(1), 11388. [CrossRef]
- Menard, D. , Popovici, J., Meek, S., Socheat, D., Rogers, W. O., Taylor, W. R. J., Lek, D., Vinjamuri, S. B., Ariey, F., & Bruce, J. (2016). National Malaria Prevalence in Cambodia: Microscopy Versus Polymerase Chain Reaction Estimates. The American Journal of Tropical Medicine and Hygiene, 95(3), 588–594. [CrossRef]
- Tedla, M. (2019). A focus on improving molecular diagnostic approaches to malaria control and elimination in low transmission settings: Review. Parasite Epidemiology and Control, 6, e00107. [CrossRef]
- Magnaval, J. F. , Morassin, B., Berry, A., & Fabre, R. (2002). One year’s experience with the polymerase chain reaction as a routine method for the diagnosis of imported malaria. The American Journal of Tropical Medicine and Hygiene, 66(5), 503–508. [CrossRef]
- Anthony C, Mahmud R, Lau YL, Syedomar SF, Sri La Sri Ponnampalavanar S. Comparison of two nested PCR methods for the detection of human malaria. Trop Biomed. 2013;30(3):459-466.
- Looareesuwan S, Krudsood S, Sloan L, et al. Evaluation of a real-time polymerase chain reaction assay for the diagnosis of malaria in patients from Thailand. Am J Trop Med Hyg. 2005;73(5):850-854.
- Mangold KA, Manson RU, Koay ESC, et al. Real-time PCR for detection and identification of Plasmodium spp. J ClinMicrobiol. 2005;43(5):2435-2440.
- Tajebe A, Magoma G, Aemero M, Kimani F. Detection of mixed infection level of Plasmodium falciparum and Plasmodium vivax by SYBR Green I-based real-time PCR in North Gondar, north-west Ethiopia. Malar J. 2014;13(1):411. [CrossRef]
- Chua KH, Lim SC, Ng CC, et al. Development of high resolution melting analysis for the diagnosis of human malaria. Sci Rep. 2015;5:15671.
- Awosolu, O. B. , Yahaya, Z. S., Farah Haziqah, M. T., &Olusi, T. A. (2022). Performance Evaluation of Nested Polymerase Chain Reaction (Nested PCR), Light Microscopy, and Plasmodium falciparum Histidine-Rich Protein 2 Rapid Diagnostic Test (PfHRP2 RDT) in the Detection of Falciparum Malaria in a High-Transmission Setting in Southwestern Nigeria. Pathogens, 11(11), 1312.
- Johnston, S. P., Pieniazek, N. J., Xayavong, M. V., Slemenda, S. B., Wilkins, P. P., and da Silva, A. J. (2006). PCR as a confirmatory technique for laboratory diagnosis of malaria. J. Clin. Microbiol. 44, 1087–1089. [CrossRef]
- Siwal, N., Singh, U. S., Dash, M., Kar, S., Rani, S., Rawal, C., et al. (2018). Malaria diagnosis by PCR revealed differential distribution of mono and mixed species infections by plasmodium falciparum and p. vivax in India. PLoS One 13, 1–14. [CrossRef]
- Haanshuus, C. G. , Mørch, K., Blomberg, B., Strøm, G. E. A., Langeland, N., Hanevik, K., et al. (2019). Assessment of malaria real-time PCR methods and application with focus on lowlevelparasitaemia. PLoS One 14, 1–15. [CrossRef]
- Eshag, H. A. , Elnzer, E., Nahied, E., Talib, M., Mussa, A., Muhajir, A. E. M. A., et al. (2020). Molecular epidemiology of malaria parasite amongst patients in a displaced people’s camp in Sudan. Trop. Med. Health 48, 1–7. [CrossRef]
- Leski, T. A. , Taitt, C. R., Swaray, A. G., Bangura, U., Reynolds, N. D., Holtz, A., et al. (2020). Use of real-time multiplex PCR, malaria rapid diagnostic test and microscopy to investigate the prevalence of plasmodium species among febrile hospital patients in Sierra Leone. Malar. J. 19, 84–88. [CrossRef]
- Feufack-Donfack, L. B. , Sarah-Matio, E. M., Abate, L. M., BouopdaTuedom, A. G., NganoBayibéki, A., MaffoNgou, C., et al. (2021). Epidemiological and entomological studies of malaria transmission in Tibati, Adamawa region of Cameroon 6 years following the introduction of long-lasting insecticide nets. Parasit. Vectors 14, 1–14. [CrossRef]
- Mwenda, M. C. , Fola, A. A., Ciubotariu, I. I., Mulube, C., Mambwe, B., Kasaro, R., et al. (2021). Performance evaluation of RDT, light microscopy, and PET-PCR for detecting plasmodium falciparum malaria infections in the 2018 Zambia National Malaria Indicator Survey. Malar. J. 20, 386–310. [CrossRef]
- Ahmad, A., Soni, P., Kumar, L., Singh, M. P., Verma, A. K., Sharma, A., Das, A., & Bharti, P. K. (2021). Comparison of polymerase chain reaction, microscopy, and rapid diagnostic test in malaria detection in a high burden state (Odisha) of India. Pathogens and Global Health, 115(4), 267–272. [CrossRef]
- Poon, L. L. , Wong, B. W., Ma, E. H., Chan, K. H., Chow, L. M., Abeyewickreme, W., Tangpukdee, N., Yuen, K. Y., Guan, Y., Looareesuwan, S., &Peiris, J. M. (2006). Sensitive and Inexpensive Molecular Test for Falciparum Malaria: Detecting Plasmodium falciparum DNA Directly from Heat-Treated Blood by Loop-Mediated Isothermal Amplification,.Clinical Chemistry, 52(2), 303–306. [CrossRef]
- Clinical Guidance: Malaria Diagnosis & Treatment in the U.S. Available online: https://www.cdc.gov/malaria/diagnosis_treatment/clinicians1.html (accesed on 01.09.2024).
- Puri, M. , Kaur Brar, H., Madan, E., Srinivasan, R., Rawat, K., Gorthi, S. S., et al. (2022). Rapid diagnosis of Plasmodium falciparum malaria using a point of- care loop-mediated isothermal amplification device. Front. Cell. Infect. Microbiol. 12:961832. [CrossRef]
- Morris, U. , and Aydin-Schmidt, B. (2021). Performance and application of commercially available loop-mediated isothermal amplification (LAMP) kits in malaria endemic and non-endemic settings. Diagnostics 11, 1–18. [CrossRef]
- Ocker, R. , Prompunjai, Y., Chutipongvivate, S., and Karanis, P. (2016). Malaria diagnosis by loop-mediated isothermal amplification (LAMP) in Thailand. Rev. Inst. Med. Trop. São Paulo 58, 2–7. [CrossRef]
- Selvarajah, D. , Naing, C., Htet, N. H., and Mak, J. W. (2020). Loop-mediated isothermal amplification (LAMP) test for diagnosis of uncomplicated malaria in endemic areas: a meta-analysis of diagnostic test accuracy. Malar. J. 19, 1–10. [CrossRef]
- Antinori, S. , Ridolfo, A. L., Grande, R., Galimberti, L., Casalini, G., Giacomelli, A., &Milazzo, L. (2021). Loop-mediated isothermal amplification (LAMP) assay for the diagnosis of imported malaria: a narrative review. Le Infezioni in Medicina, 29(3), 355–365. [CrossRef]
- Demirev, P. A. (2004). Mass spectrometry for malaria diagnosis. Expert Review of Molecular Diagnostics, 4(6), 821–829. [CrossRef]
- Scholl, P. F. , Kongkasuriyachai, D., Demirev, P. A., Feldman, A. B., Lin, J. S., Sullivan, D. J., & Kumar, N. (2004). Rapid detection of malaria infection in vivo by laser desorption mass spectrometry. The American Journal of Tropical Medicine and Hygiene, 71(5), 546–551.
- Nyunt, M. , Pisciotta, J., Feldman, A. B., Thuma, P., Scholl, P. F., Demirev, P. A.,...& Sullivan Jr, D. J. (2005). Detection of Plasmodium falciparum in pregnancy by laser desorption mass spectrometry. Am J Trop Med Hyg. 2005;73(3):485-490.
- Christner M, Frickmann H, Klupp E, Rohde H, Kono M, Tannich E, et al. Insufficient sensitivity of laser desorption-time of flight mass spectrometry-based detection of hemozoin for malaria screening. J Microbiol Methods. 2019;160:104–6.
- Stauning, M.A. , Jensen, C.S., Staalsøe, T. et al. Detection and quantification of Plasmodium falciparum in human blood by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry: a proof of concept study. Malar J 22, 285, 2023.
- Robinson, J. P. (2022). Flow Cytometry: Past and Future. BioTechniques, 72(4), 159–169. [CrossRef]
- vanVianen, P. H. , van Engen, A., Thaithong, S., van der Keur, M., Tanke, H. J., van der Kaay, H. J., Mons, B., &Janse, C. J. (1993). Flow cytometric screening of blood samples for malaria parasites. Cytometry, 14(3), 276–280. [CrossRef]
- Malleret, B. , Claser, C., Ong, A. S. M., Suwanarusk, R., Sriprawat, K., Howland, S. W., Russell, B., Nosten, F., &Rénia, L. (2011). A rapid and robust tri-color flow cytometry assay for monitoring malaria parasite development. Scientific Reports, 1(1), 118. [CrossRef]
- Stéphane Picot, Thomas Perpoint, Christian Chidiac, Alain Sigal, Etienne Javouhey, Yves Gillet, Laurent Jacquin, Marion Douplat, Karim Tazarourte, Laurent Argaud, Martine Wallon, CharlineMiossec, Guillaume Bonnot and Anne-LiseBienvenu. Diagnostic accuracy of fluorescence flow-cytometry technology using Sysmex XN-31 for imported malaria in a non-endemic setting, Parasite, 29, 2022, 31.
- Khartabil, T. A. , de Rijke, Y. B., Koelewijn, R., van Hellemond, J. J., andRusscher, H. (2022). Fast detection and quantification of plasmodium species infected erythrocytes in a non-endemic region by using the Sysmex XN-31 analyzer. Malar. J. 21, 119–110. [CrossRef]
- Manescu, P. , Shaw, M. J., Elmi, M., Neary-Zajiczek, L., Claveau, R., Pawar, V., Kokkinos, I., Oyinloye, G., Bendkowski, C., Oladejo, O. A., Oladejo, B. F., Clark, T., Timm, D., Shawe-Taylor, J., Srinivasan, M. A., Lagunju, I., Sodeinde, O., Brown, B. J., & Fernandez-Reyes, D. (2020). Expert-level automated malaria diagnosis on routine blood films with deep neural networks. American Journal of Hematology, 95(8), 883–891. [CrossRef]
- Okello PE, Van Bortel W, Byaruhanga AM, Correwyn A, Roelants P, Talisuna A, D'Alessandro U, Coosemans M: Variation in malaria transmission intensity in seven sites throughout Uganda. Am J Trop Med Hyg. 2006, 75: 219-225.
- Wanji S, Kimbi HK, Eyong JE, Tendongfor N, Ndamukong JL. Performance and usefulness of the Hexagon rapid diagnostic test in children with asymptomatic malaria living in the Mount Cameroon region. Malar J. 2008;7. [CrossRef]
- Nkrumah B, Acquah SE, Ibrahim L, May J, Brattig N, Tannich E, et al. Comparative evaluation of two rapid field tests for malaria diagnosis: Partec Rapid Malaria Test® and Binax Now® Malaria Rapid Diagnostic Test. BMC Infect Dis. 2011;11. [CrossRef]
- Hassan SE, Okoued SI, Mudathir MA, Malik EM: Testing the sensitivity and specificity of the fluorescence microscope (Cyscope(R)) for malaria diagnosis. Malar J. 2010, 9: 88. [CrossRef]
- Kimbi HK, Ajeagah HU, Keka FC, Lum E, Nyabeyeu HN, Tonga CF, et al. Asymptomatic malaria in school children and evaluation of the performance characteristics of the PartecCyscope® in the Mount Cameroon Region. J BacteriolParasitol. 2012;3:5.
- Ndamukong-Nyanga J, Kimbi H, Sumbele I, Bertek S, Lafortune K, Larissa K, et al. Comparison of the PartecCyScope® rapid diagnostic test with light microscopy for malaria diagnosis in Rural Tole, Southwest Cameroon. British J Med Med Res. 2015;8:623–633. [CrossRef]
- Birhanie, M. Comparison of Partec rapid malaria test with conventional light microscopy for diagnosis of malaria in Northwest Ethiopia. J Parasitol Res. 2016;1:5. [CrossRef]
- Liu, R. , Liu, T., Dan, T., Yang, S., Li, Y., Luo, B., Zhuang, Y., Fan, X., Zhang, X., Cai, H., &Teng, Y. (2023). AIDMAN: An AI-based object detection system for malaria diagnosis from smartphone thin-blood-smear images. Patterns, 4(9), 100806. [CrossRef]
- Pirnstill, C.W. , Coté G.L. Malaria diagnosis using a mobile phone polarized microscope. Sci. Rep. 2015;5:1–13. [CrossRef]
- Yang, F. , Poostchi M., Yu H., Zhou Z., Silamut K., Yu J., Maude R.J., Jaeger S., Antani S. Deep learning for smartphone-based malaria parasite detection in thick blood smears. IEEE J. Biomed. Health Inform. 2020;24:1427–1438. [CrossRef]
- Yu, H. , Yang F., Rajaraman S., Ersoy I., Moallem G., Poostchi M., Palaniappan K., Antani S., Maude R.J., Jaeger S. Malaria Screener: a smartphone application for automated malaria screening. BMC Infect. Dis. 2020;20:825. [CrossRef]
- Rees-Channer, R. R., Bachman, C. M., Grignard, L., Gatton, M. L., Burkot, S., Horning, M. P., Delahunt, C. B., Hu, L., Mehanian, C., Thompson, C. M., Woods, K., Lansdell, P., Shah, S., &Chiodini, P. L. (2023). Evaluation of an automated microscope using machine learning for the detection of malaria in travelers returned to the UK. Frontiers in Malaria, 1. [CrossRef]
- Yu, H. , Mohammed, F. O., Abdel Hamid, M., Yang, F., Kassim, Y. M., Mohamed, A. O., Maude, R. J., Ding, X. C., Owusu, E. D. A., Yerlikaya, S., Dittrich, S., & Jaeger, S. (2023). Patient-level performance evaluation of a smartphone-based malaria diagnostic application. Malaria Journal, 22(1), 33. [CrossRef]
- Kassim, Y. M., Yang, F., Yu, H., Maude, R. J., & Jaeger, S. (2021). Diagnosing Malaria Patients with Plasmodium falciparum and vivax Using Deep Learning for Thick Smear Images. Diagnostics, 11(11), 1994. [CrossRef]
- LIST OF RAPID DIAGNOSTIC TEST (RDT) KITS FOR MALARIA classified according to the Global Fund Quality Assurance Policy. Available online: https://www.theglobalfund.org/media/5891/psm_qadiagnosticsmalaria_list_en.pdf (accessed on 15.10.2024).
- Malaria Diagnostics Market Insights. Available online: https://www.skyquestt.com/report/malaria-diagnostics-market (accessed on 14.10.2024).
- Kalia, I. , Anand, R., Quadiri, A., Bhattacharya, S., Sahoo, B., & Singh, A.P. (2021). Plasmodium berghei-Released Factor, PbTIP, Modulates the Host Innate Immune Responses. Front. Immunol. 12:699887. [CrossRef]
Figure 1.
Clinical diagnosis based on symptoms.
Figure 2.
Diagnosis of malaria using light microscopy.
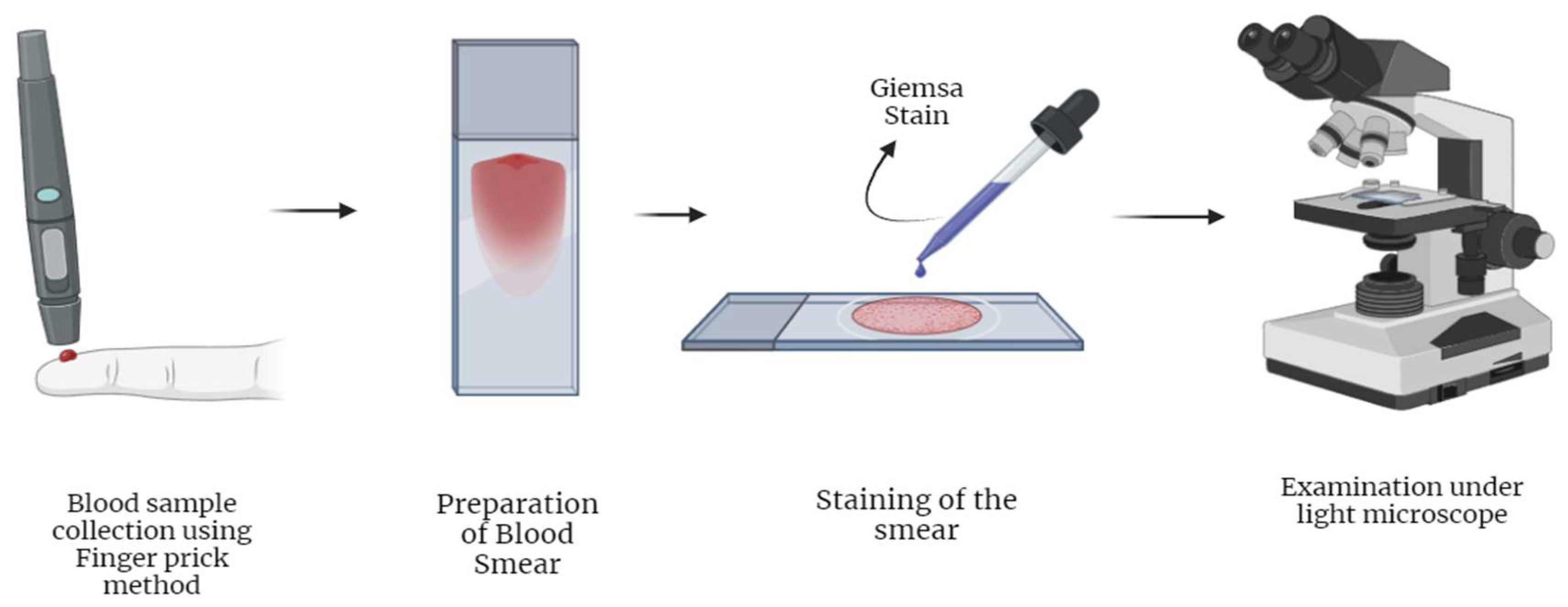
Figure 3.
Typical lateral flow device.
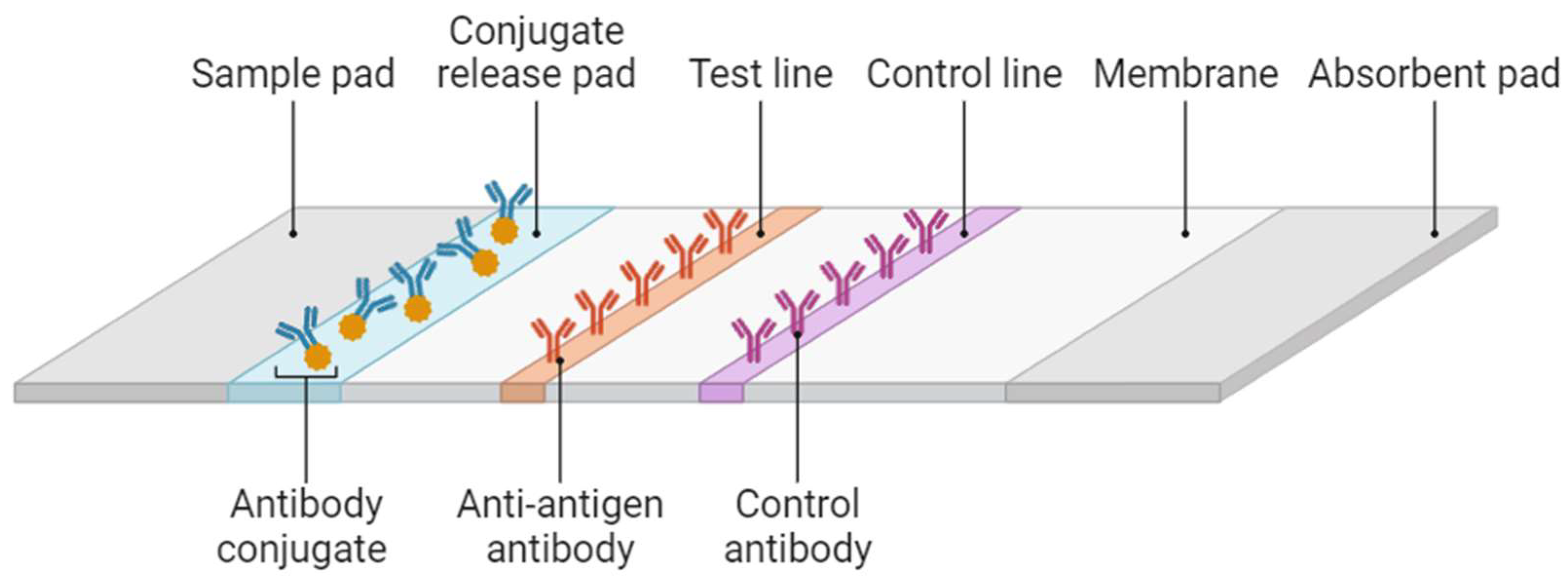
Figure 4.
Malaria Diagnosis using a RDT kit.
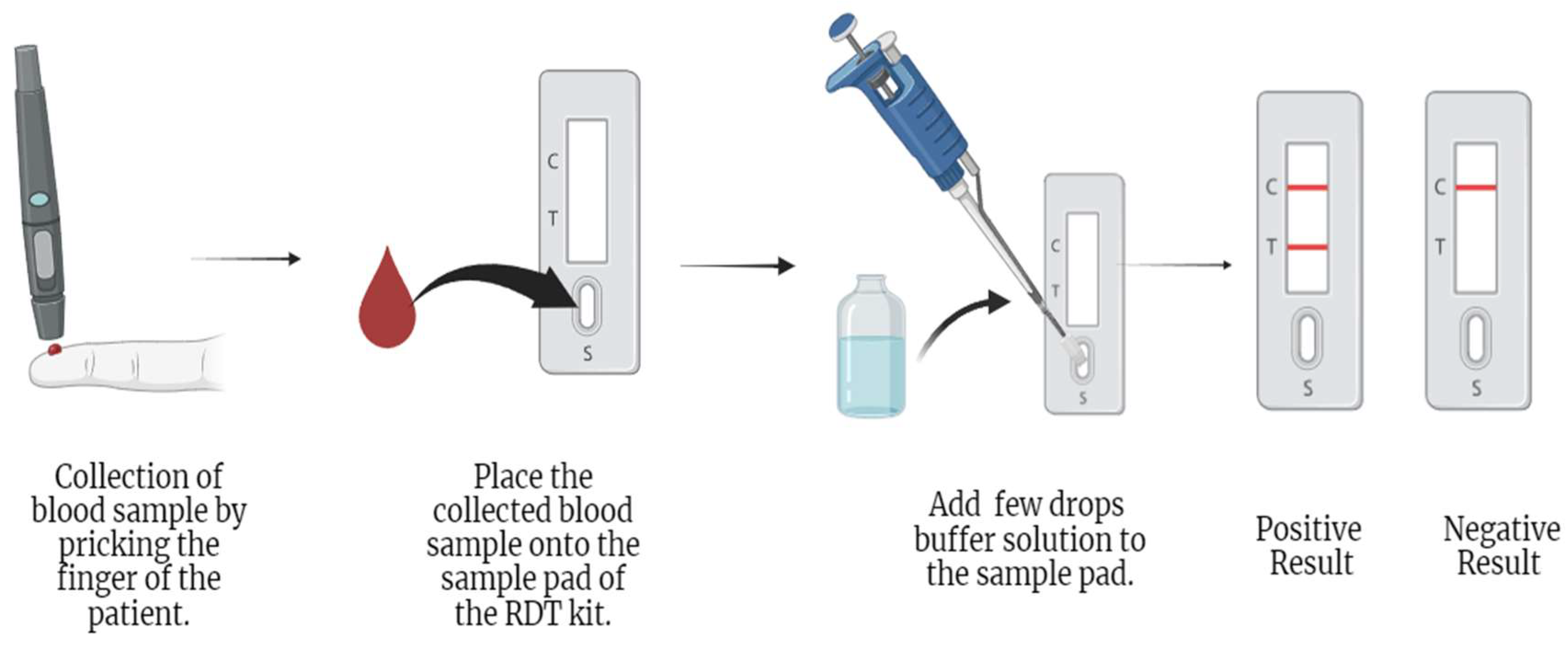
Figure 5.
Basic workflow of LAMP technique.
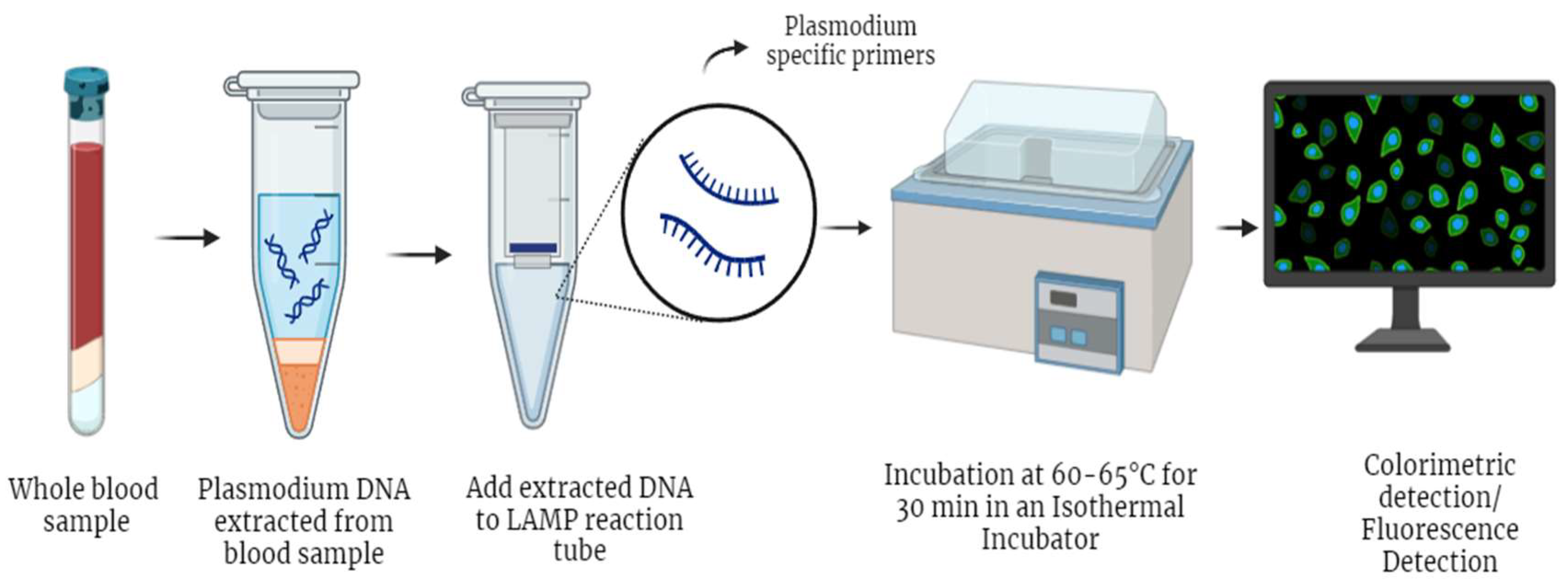
Figure 6.
Flow-cytometry based detection of malaria parasite.
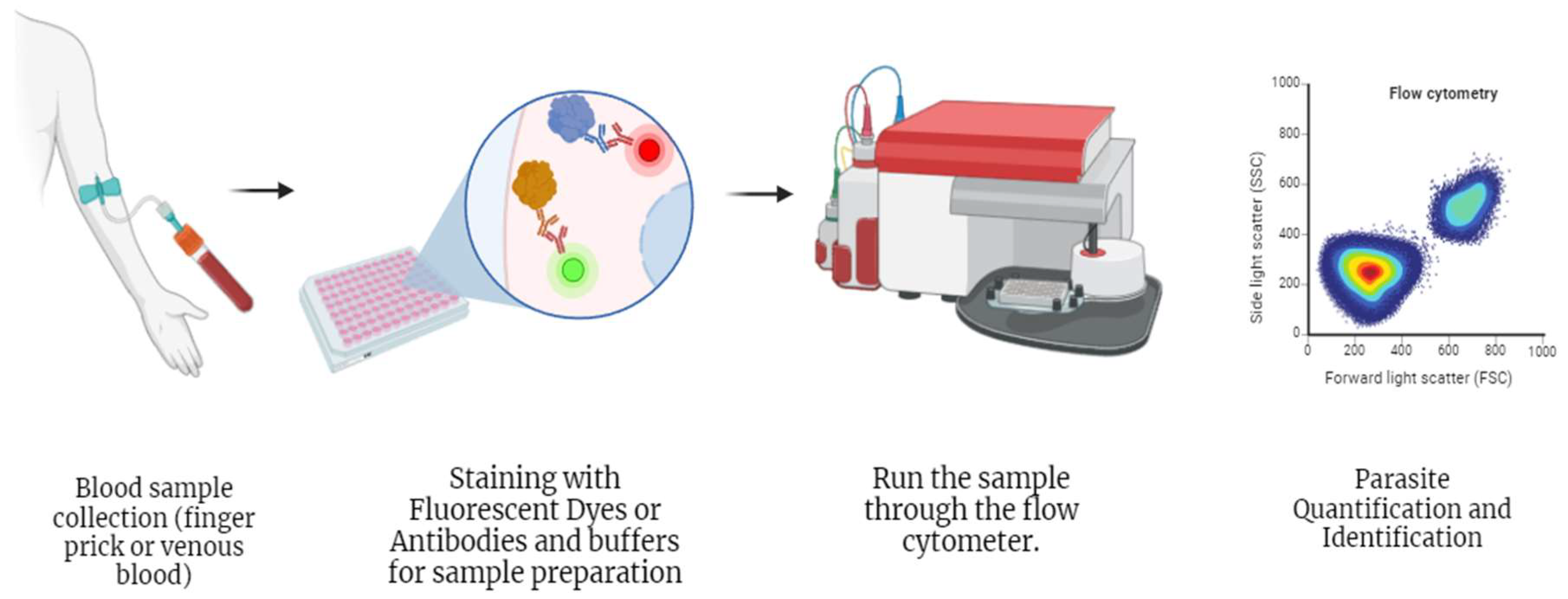
Figure 7.
Forecast period from 2024-2032.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



