Submitted:
11 November 2024
Posted:
12 November 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Interleukin-18 (IL-18) serves a dual function in the immune system, acting as a "double-edged sword" cytokine. Depending on the microenvironment and timing, IL-18 can either drive harmful inflammation or restore immune homeostasis. Pathologies characterized by elevated IL-18, known as IL-18’opathies, highlight the therapeutic potential for IL-18 blockade. IL-18 Binding Protein (IL-18BP) is one of only four natural cytokine antagonists encoded by a separate gene, distinguishing it from canonical soluble receptors. IL-18BP’s exceptionally high affinity and slow dissociation rate make it an effective regulator of IL-18, essential for maintaining immune balance and influencing disease outcomes, and positions IL-18BP as a promising alternative to more aggressive treatments that carry risks of severe infections and other complications. Tadekinig alfa, the drug form of IL-18BP, represents a targeted therapy that modulates the IL-18/IL-18BP axis, offering a safe adverse-effect-free option. With orphan drug designation, Phase III clinical trial completion, and seven years of compassionate use, Tadekinig alfa holds promise in treating autoimmune and inflammatory diseases, cancer and genetically-linked disorders. Levels of IL-18, free IL-18 and IL-18BP, may serve as biomarkers for disease severity and therapeutic response. Given its pivotal role in immune balance, the IL-18/IL-18BP dyad has attracted interest from over ten pharmaceutical companies and startups, which are currently developing innovative strategies to either inhibit or enhance IL-18 activity depending on the therapeutic need. The review focuses on the features of the dyad members and screens the therapeutic approaches.
Keywords:
IL-18
; IL-18BP
; Tadekinig alfa
; antidote
; antagonist
; agonist
; checkpoint
; CAR T
; MAS
; HLH
; Covid 19
; NLRC4
; XIAP
; inflammasome
; double-edged-sword
Introduction
Inflammation, an ancient response of innate immunity, is triggered by infection and by tissue damage with the goal of eliminating these threats. This response is followed by acute inflammatory processes that set the stage for adaptive immunity within a precise time frame and microenvironment. The induction of various intercellular communication proteins, known as interleukins and cytokines, including IL-18 (Landy et al., 2024) is crucial for this process. However, uncontrolled inflammation can lead to excessive tissue damage, chronic inflammation, autoimmunity, fibrosis, and eventual organ failure. To prevent such detrimental outcomes, a mechanism that includes a feedback regulation of the various cytokine pathways is required to resolve inflammation and to restore homeostasis. This regulatory role is played by naturally occurring soluble receptors and binding proteins. Natural soluble receptors (Novick & Rubinstein, 2007) that are the counterparts of cell- surface-receptors extracellular domain, such as those of IL-1, TNF and IFNs, are the canonical receptor antagonists. Natural binding proteins, with a similar function, are encoded by separate genes and are rare, unique and attractive candidates for therapeutic development. One such example is IL-18BP, the highly effective antagonist of IL-18 (Novick et al., 1999) (Fauteux-Daniel et al., 2023). This review focuses on the dual role of IL-18, the crucial function of its unique partner, IL-18BP, in regulating this cytokine to keep it in the normal range, and the strategies pursued by over ten pharmaceutical companies and startups to target IL-18 and IL-18BP in autoimmune diseases, rare mutations, cytokine storm, cancer and Covid 19.
Key Features of IL-18
- IL-18, originally named IFN-γ-inducing factor, is a member of the IL-1 family, links innate and adaptive immunity and is regulated by the cytokine it induces.
- IL-18 is a double-edged sword cytokine that can either be detrimental, by promoting inflammation, or beneficial, by regulating immune responses to restore homeostasis, depending on the microenvironment.
- IL-18 can function as a Th1or Th2 cytokine depending on the immune microenvironment.
- IL-18 does not require de novo synthesis. The inactive pro IL-18 is always on standby, ready to be processed by caspase 1 into its biologically active form.
- IL-18 is included in an exclusive dictionary of cytokines, a dictionary that provides a specific signature of the cellular response of each immune cell-type to a variety of cytokines. Induction of interferon-gamma (IFN-g) is IL-18’s signature and NK cells are its main target. IL-18 triggers the upregulation of more than 1,000 genes, an order of magnitude higher compared to other cytokines.
- IL-18 signals through an evolutionary conserved IL-18 receptor consisting of a ligand- binding chain and an accessory chain. Signal transduction involves recruitment of MyD88, the four IRAKs and TNF receptor activating factor-6 (TRAF-6) leading to IκB degradation, NFκB release and the activation of a proinflammatory cascade.
- IL-18 plays a role in autoimmune and inflammatory diseases, inborn disorders, infectious diseases including severe cases of Covid 19, and cancer.
- IL-18 serves as a biomarker in disorders characterized by elevated IL-18 levels, referred to as "IL-18opathies," a term coined to facilitate differential diagnosis in these pathologies.
- IL-18 is a checkpoint biomarker in cancer and IL-18-engineered CAR-T cells have demonstrated an enhanced tumor-killing ability in solid tumors particularly in immunotherapies involving PD-1 blockade.
- A cytokine storm, with IL-18 as one of its key players, represents the harmful side of IL-18. This storm can occur as a complication of viral infections, autoimmune diseases, cancer, and CAR-T therapy. Recently, the external administration of IL-18's antidote, IL-18BP, has been tested as a potential rescue treatment.
- Blocking IL-18 is a safer option compared to blocking its family member, the master cytokine IL-1, since prolonged IL-1 inhibition can lead to severe infections.
Key Features of IL-18BP
- IL-18 Binding Protein, unlike canonical soluble receptors, is a rare example of a cytokine antagonist encoded by a separate gene.
- IL-18BP is a glycosylated protein that binds to mature but not to the inactive pro-IL-18. In humans IL-18BPa is the most abundant and the most active of four splice variants.
- IL-18BPa is exceptional for its extremely high affinity to IL-18 and its slow dissociation rate (Koff), ensuring the stability of the dyad complex. This makes it an ideal regulator of IL-18 signaling and a promising therapeutic agent.
- IL-18BPa pharmacokinetics: IL-18BPa has an elimination half-life of 34-40 hours when administered subcutaneously at doses of 80 mg and 160 mg to patients three times a week. Unlike antibody treatments, with a half-life of 3-4 weeks, IL-18BP's shorter half-life allows for more rapid cessation, enabling timely IL-18 activity when needed for immune defense.
- The balance between IL-18 and IL-18BPa, and particularly the level of free IL-18, all regulated by IFN-g in a feedback loop mechanism, are crucial in maintaining homeostasis, and in determining disease outcomes.
- IL-18BP deficiency can be life-threatening and, when left untreated, has proven to be fatal.
- Tadekinig alfa, a recombinant IL-18BPa, is a life-saving drug that has rescued children with inborn IL-18 overexpression and organ failure. A Phase III clinical study had been completed and it is in compassionate use for seven years now with no reported adverse effects. Beneficial also in Still’s disease it shows promise for treating cytokine storms caused by viral infections, cancer and CAR-T therapy.
IL-18
1.1. IL-18 Is an IFN-g Inducing Factor (IGIF)
IL-18, initially named interferon-g inducing factor (IGIF) (Nakamura et al., 1989), is an IL-1 family member and a cytokine that links innate and adaptive immunity. The IL-1 family of cytokines and receptors is unique in immunology and shares functional similarities with the Toll-like receptor (TLR). Innate immune mechanisms are essential for survival by the vast majority of living organisms while less than 5% utilize T-cell and B-cell functions. Innate immunity is manifested by inflammation aimed at host defense, but when uncontrolled, it can be harmful to survival. This may explain the evolutionary emergence of IL-18BP, IL-18's potent natural antagonist and the other partner in the dyad.
1.2. IL-18 Is of a Dual Nature
IL-18’s dual nature, acting as either a "good guy" or a "bad guy", and its classification as a Th1 or Th2 cytokine, depend on the microenvironment in which it operates. Other members of this "double-edged sword" club of cytokines (Marx, 1988) include TNF (Aggarwal, 2003), IFN-g (Zaidi & Merlino, 2011), IL-6 (Blanchard et al., 2009), IL-25 (Monteleone et al., 2010), Type I IFNs (Snell et al., 2017), cytokines participating in sepsis (Chaudhry et al., 2013) and in tuberculosis (Etna et al., 2014). In a healthy immune system, IL-18 plays a beneficial role in a host defense against infections and in a regulation of immune responses aimed to maintain homeostasis. However, in a disease setting, such as autoimmune diseases, inborn disorders or chronic inflammatory conditions, IL-18 can become dysregulated, leading to excessive inflammation which may result in a cytokine storm, tissue damage, organ failure and even death. Thus, tight regulation of IL-18 is essential.
1.3. IL-18 Is a Th1 and a Th2 Cytokine
Traditionally, IL-18 has been associated with Th1 immune responses because it induces the production of IFN-g, a hallmark cytokine of Th1 cells. In Th1-dominated immune responses, IL-18 enhances the activity of NK cells and cytotoxic T cells to e.g. combat intracellular pathogens, fight cancer cells and trigger autoimmune diseases (Nakanishi et al., 2001) (Steinman, 2007) (Novick et al., 2013). IL-18 acts on non-polarized T cells, NK cells, NKT cells, B cells, dendritic cells, and macrophages. In the presence of IL-12, shown to increase the expression of the transducing chain of the IL-18 receptor, IL-18 induces the production IFN-g. It induces chemokines and cell adhesion molecules, stimulates inflammatory cytokine secretion such as IL-1 and TNFa, and enhances NK-cell cytotoxicity. Yet in a different microenvironment IL-18 can promote Th2 immune response that is characterized by the production of cytokines such as IL-4, IL-5, and IL-13, and is involved in allergic reactions, asthma and parasitic infections. IL-18 without IL-12 but with IL-2 induces Th2 cytokine production. IL-18 with IL-3 induces mast cells and basophils to produce IL-4 and IL-13 (Yasuda et al., 2019). IL-18 may also promote the differentiation and activation of regulatory T cells (Tregs), and thus suppress immune responses aiming to maintain tolerance (Alvarez et al., 2023). Cancer is yet an additional example in which IL-18’s dual nature is exhibited. In certain types of cancer, IL-18 has been shown to be anti-tumorigenic and to enhance immunotherapy and chemotherapy. In other types of cancer IL-18 was tumor-promoting (Fabbi et al., 2015) (Ihim et al., 2022). No surprise that with such a vast scope of activities and depending on its immediate vicinity, IL-18 it is tightly regulated by its partner in the dyad, IL-18BP.
1.4. Pro-IL-18: Always on Standby
IL-18 does not require a de novo synthesis. The inactive pro IL-18 is always on standby ready to be processed to its active form upon the right trigger. Thus, in response to a pathogen or stress-associated stimuli, pro IL-18 is proteolytically cleaved to its bioactive form by the cytosolic inflammasome component, Caspase 1. Caspase 1 also activates the pore-forming Gasdermin D (GSDMD) enabling the secretion of the leaderless cytokine, IL-18 (Xia et al., 2021). This process initiates pyroptosis, a lytic programmed cell death, aiming at rapid clearance of various bacterial, viral, fungal and protozoan infections.
1.5. IL-18 Dictionary of Interactions
IL-18 had been included in a novel dictionary of immune responses to cytokines at a single-cell resolution. This dictionary is an in vivo collection of 386,703 single-cell transcriptomic profiles of more than 17 immune cell types in response to each of 86 cytokines (>1,400 cytokine–cell type combinations) demonstrated in mouse lymph nodes. Most cytokines induce highly cell-type-specific responses. Based on this dictionary and using gene expression data, a software named Immune Response Enrichment Analysis (IREA), was developed, and cytokine activities and immune cell polarization were assessed. IFN-g was confirmed to be IL-18’s signature and NK cells its main target. More than 20 cell types were identified and differentially expressed genes (DEGs) in response to cytokine treatment in each cell type were computed aiming to compose cytokine signatures. In addition, a map that quantified transcriptomic changes upon cytokine treatment was created. Of note is that IL-18 triggered the upregulation of more than 1,000 genes, an order of magnitude more than demonstrated for other cytokines. IL-18-induced state was strongly enriched in a variety of processes such as the induction of Myc (which controls growth and proliferation), maturation of myeloid cells, recruitment of dendritic, cytotoxicity and regulators of differentiation (Kit and Batf). The value of this dictionary is indispensable in therapeutically applied cytokines, including IL-18. Indeed, this dictionary was applied to reveal cytokine networks in tumors following immune checkpoint blockade therapy such as PD-1 blockade (Cui et al., 2024). This high-resolution dictionary provides empiric evidence for IL-18’s role in immune response.
1.6. IL-18: A Non-Master Cytokine
IL-18 is not a master cytokine by itself but is a member of a master cytokine family, IL-1, and is regulated by the master cytokine IFN-g. While IL-1 exerts broad and systemic effects on immune and inflammatory pathways, IL-18’s actions are more specific and context-dependent. Therefore, blocking IL-18 signaling is less likely to disrupt the entire immune system, making it a more targeted therapeutic approach with potentially fewer adverse effects. This distinction emphasizes the therapeutic promise of targeting IL-18 rather than IL-1 in the relevant immune-mediated disorders.
1.7. IL-18 Regulation
IL-18 is regulated by the cytokine it induces, the master cytokine IFN-g (Hurgin et al., 2002). So far IFN-g is IL-18’s only known regulator. IFN-g modulates IL-18 production and activity via a negative feedback mechanism, and thereby fine tunes immune responses and inflammatory processes. In an excess of IFN-g, IL-18’s natural antidote, IL-18BP, is induced aimed to restore homeostasis.
1.8. Cells Producing IL-18
IL-18 is produced by both hematopoietic and non-hematopoietic cells, such as T cells, NK cells, dendritic cells, macrophages, endothelial cells, keratinocytes, intestinal epithelial cells, microglial cells and synovial fibroblasts (Yasuda et al., 2019).
2. IL-18 Receptor
2.1. IL-18 Receptor Composition
IL-18 receptor (IL-18R) is composed of two chains, the ligand binding chain, IL-18R alpha (IL-1R5), and the IL-18 receptor beta accessory chain, IL-18Rap (IL-1R7). IL-18 first binds to IL-18Ra, followed by the binding of IL-18Rap and this high affinity trimeric complex initiates signal transduction. Toll-IL-1-Receptor (TIR) intracellular domains of the receptor chains come into proximity and a cascade of sequential events is initiated. It involves recruitment of MyD88, the four IRAKs and TNF receptor activating factor-6, followed by the degradation of IκB, release of NFκB and activation of a proinflammatory process e.g. release of pro-inflammatory cytokines (Rex et al., 2020) (Tsutsumi et al., 2014). IL-18 receptor is most prominently expressed by NK cells and activated memory T-cells. Hoshino K et al. (Hoshino et al., 1999) have generated IL-18Rα-deficient mice and observed a lack of Th1 response upon IL-18 stimulation in these ligand-binding-chain-knockout mice.
2.2. IL-18 Receptor: Evolutionary Conserved
IL-18 Receptor is conserved throughout evolution. It belongs to the IL-1 family of receptors and shares functions with the TLR family. These receptors are pattern recognition receptors responsible for pathogen recognition and induction of innate immune responses and as such link IL-18 with innate immunity. Each member of these families contains a 50-amino-acids cytoplasmic TIR domain highly homologous to the ancient Toll gene found in Drosophila and other insects (Tsutsumi et al., 2014).
2.3. IL-18 Receptor Expression
Most cells express the ligand binding chain of the receptor, IL-18Ra, but not all cells express the transducing chain, IL-18Rb. IL-18R is mainly expressed in hematopoietic cells such as CD4+ NKT cells, mast cells, basophils, T-cells with the highest expression observed in NK cells driving its differentiation and activation (Nakamura et al., 2000). The expression of IL-18R on Th1 cells and B cells is mainly driven by IL-12 (Yoshimoto et al., 1998) (Sareneva et al., 2000) (Rex et al., 2020) (Tsutsumi et al., 2014).
2.4. IL-18 Receptor Binding Sites
IL-18 ligand binding sites to its receptor and to the IL-18 binding protein are formed upon conformational changes created following pro-IL-18 cleavage by caspase-1. A study by Dong et al. has shown why this cleavage is necessary for mature IL-18’s inflammatory activity (Dong et al., 2024).
2.5. IL-18 Affinity to Its Receptor
The affinity of IL-18 to its ligand-binding cell-surface-receptor chain is 18.5 nM. The affinity raises to 0.4 nM when the accessory chain joins to form a signal transducing functional triple complex (Wu et al., 2003) (Tsutsumi et al., 2014). This affinity is comparable to the affinity of IL-18 to its natural antagonist, IL-18BP (Kim et al., 2000) (Girard et al., 2016).
3. IL-18 Knockout Models
IL-18 knockout (KO) mouse models provide insights into the multifaceted roles of IL-18 in immune regulation, inflammation, autoimmune diseases, infectious diseases, metabolic disorders, and cancer. IL-18 KO mice show reduced levels of IFN-g and lower NK cell activity leading to a diminished ability to combat pathogens and protect against cancer. IL-18 KO mice show reduced severity of autoimmune diseases e.g. arthritis, lupus and inflammatory bowel disease (IBD) pointing to the deleterious effect of an excess of IL-18 in human diseases. IL-18 KO mice on high-fat diets have been shown to develop more severe obesity and insulin resistance indicating the role of IL-18 in metabolic syndrome. IL-18 KO mice showed cognitive impairment and depressive-like behavioral changes demonstrating the involvement of IL-18 in psychiatric and neurologic conditions. Cancer, metabolism and brain disorder related genes referring to IL-18 are listed in the review by Yamanishi K et al 2023 (Yamanishi et al., 2023). These models reveal potential therapeutic targets in the corresponding human pathologies and contribute to the development of novel treatments (Netea et al., 2006).
4. IL-18 in Health and Disease
4.1. IL-18 and Free IL-18 Levels in Healthy Individuals and in a Pathology
The level of IL-18 in healthy people is around 100 pg/ml. In IL-18’opathies the level may rise 10-10,000 fold e.g. in sepsis, Still’s disease, hemophagocytic lymphohistiocytosis (HLH) or macrophage activation syndrome (MAS) (Novick et al., 2001) (Mazodier et al., 2005) (Girard et al., 2016; Novick et al., 2013). Most of the circulating IL-18 is in a tight complex with its antagonist, IL-18BP, therefore in healthy people the blood concentration of free IL-18 does not exceed a few pg/ml (Novick et al., 2001) (Fauteux-Daniel et al., 2023). In a disease state, IL-18 levels rise significantly more than IL-18BP, leading to elevated free IL-18. This makes free IL-18 a major player, and likely the most critical factor, in the associated pathology (Novick et al., 2013).
4.2. IL-18’opathies
The term IL-18’opathies was coined for pathologies hallmarked by an excessive and unprecedented IL-18 production most probably a result of a severe imbalance between the levels of IL-18BP and IL-18 (Landy et al., 2024) (Fauteux-Daniel et al., 2023) (Mazodier et al., 2005) (Girard et al., 2016) (Weiss et al., 2018). Therefore, solely measuring total levels of IL-18 may sometimes not be sufficiently informative. Free IL-18, the one that is not in a complex with IL-18BP, may thus serve as a key biomarker in the diagnosis of these IL-18’opathies and as a criterion in the identification of patients that would benefit from IL-18 blockade. IL-18 levels, 2000-5000 pg/ml, that are at least 10-fold higher than the levels in healthy controls, are suggested to be the cut-off values for the differentiation of systemic juvenile idiopathic arthritis (sJIA) and adult-onset Still's disease (AOSD) from other pathologies e.g. Kawasaki Disease, FMF, TRAPS, other subtypes of JIA, SLE, JDM, and leukemia (Shimizu et al., 2022). The levels of IL-18 in MAS, HLH and in children with inborn mutations e.g. mutations in the inflammasome (NLRC4 gain of function) or XIAP (X-linked inhibition of apoptosis) deficiency mutation, are extremely high and are associated with diseases activity. Plasma levels in these pathologies may reach a microgram range of IL-18 namely a range that is 100-1,000 higher than in healthy controls (Canna et al., 2014) (Geerlinks & Dvorak, 2022). These findings may justify the inclusion of IL-18 in the international ACR/EULAR classification criteria for these pathologies.
4.2.1. IL-18 in NLRC4 Associated Inflammasomopathies
Inflammasomes are large cytosolic multiprotein complexes of the innate immunity. Their components assemble via cytosolic pattern recognition receptors- or stress-associated stimuli in response to detection of infection. This assembly leads to the activation of caspase-1-mediated inflammatory responses, including cleavage of the pro IL-1β and pro IL-18 into their active forms, and initiation of an inflammatory form of cell death, pyroptosis. Inflammasomes consist of a sensor protein, the adaptor protein apoptosis-associated speck-like protein containing a caspase-recruitment domain (ASC), and the proinflammatory caspase, caspase-1 (Schroder & Tschopp, 2010) (de Zoete et al., 2014). NLRC4 is one of the components associated with the formation of inflammasome.
Gain-of-function mutations in the gene encoding NLR-family CARD domain-containing protein 4 (NLRC4), may result in an often-fatal autoinflammatory diseases, the NLRC4-inflammasomopathies, thoroughly reviewed by Romberg et al. (Romberg et al., 2017). Autoinflammation with infantile enterocolitis (AIFEC) was the first autoinflammation reported that linked IL-18’s major contribution to gut inflammation in myeloid and intestinal epithelial cells. IL-18 level in these patients may reach over 10 microgram levels, 10,000-fold more than in healthy individuals. Additional phenotypes traditionally associated, with mutations in another component of the inflammasome, NLRP3, mutations like familial cold autoinflammatory syndrome and neonatal onset multisystem inflammatory disease (NOMID), have now also been associated with gain-of-function NLRC4 mutations. These findings highlight the need for specific diagnostic biomarkers and open new therapeutic avenues for treating AIFEC patients (Romberg et al., 2014 ) (Canna et al., 2014) (Canna et al., 2017) and the other pathologies with targeted agents like IL-18BP. Children born with the various mutations were safely and successfully treated with recombinant IL-18BP on a compassionate basis for seven years (see item 7.1.1) and Phase III clinical trial (NCT03113760) has been recently completed.
4.2.2. IL-18 in XIAP Deficiency
The XIAP gene in humans is located on the X chromosome and the protein encoded by this gene is an inhibitor of apoptosis induced by viral infection and by overproduction of caspases. XIAP is a negative regulator of inflammasome function and represses the production of inflammasome activated cytokines. Loss of functional mutations in XIAP may lead to life threatening HLH accompanied by highly elevated IL-18 often 1,000-fold higher than a level in healthy controls (Wada et al., 2014) (Geerlinks & Dvorak, 2022). Children born with this mutation were safely and successfully treated with recombinant IL-18BP on a compassionate basis for seven years (see item 7.1.1) and Phase III clinical trial (NCT03113760) has been recently completed.
4.2.3. IL-18 in Still’s Disease
The two forms of Still’s disease, AOSD sJIA, also known as juvenile Still’s disease, involve extremely high levels of IL-18. AOSD is a rare systemic autoinflammatory disorder of unknown etiology with an estimated prevalence of 1 in 100,000. This pathology is characterized by a clinical triad of high spiking fever, joint stiffness and transient skin rash, accompanied by macrophage activation, Th1 cells activation and an overproduction of IL-1, IL-6, IFN-g, TNF-a and particularly IL-18. The latter may reach nanogram and even microgram levels that are 100 to over 1,000 folds higher than in other diseases. 23% of AOSD patients may experience life-threatening complications, in a form of MAS characterized by a high mortality rate. It is no surprise that there is a need for diagnostic biomarkers and new treatment options, particularly for cases resistant to conventional therapies. Based on over 100 studies IL-18 is proposed to be a leading candidate to serve as a diagnostic biomarker in such cases (Canna & De Benedetti, 2024) (Bindoli et al., 2024) (Baggio et al., 2023) (Galozzi et al., 2022) (Shimizu, 2021) (Efthimiou et al., 2021) (Yasin, Fall, et al., 2020) (Kudela et al., 2019) (Giacomelli et al., 2018).
4.2.4. IL-18: Predictor of Mortality in Acute Renal Disease
Acute kidney injury (AKI) represents a common and devastating problem in clinical medicine. A major reason is the lack of early biomarkers for AKI, and hence an unacceptable delay in initiating therapy. Urinary interleukin-18 had been reported to be an earlier AKI biomarker than serum creatinine and its level in survivors and non-survivors predicted mortality in patients at the intensive care unit (Chen et al., 2020) (Parikh et al., 2005) (Washburn et al., 2008). Mouse models of ischemia-reperfusion have shown that blocking IL-18 prevents renal damage (Wu et al., 2008) and on the other hand IL-18BP transgenic mice are protected against renal injury (He et al., 2008). IL-18 plays a role also in kidney transplantation. Of note is a recent study that evaluated changes in serum concentrations of six IL-1 family cytokines (IL-1 alpha, IL-1 beta, IL-1RA, IL-18, IL-18BP, and IL-36 beta) in 138 kidney allograft recipients vs. healthy donors. IL-18, and specifically its free form, was the only cytokine that was significantly upregulated )ca. 100 fold, 4000-6000 pg/ml), in the acute rejection group without upregulation of its inhibitor, IL-18BP (Cecrdlova et al., 2024).
Thus, external administration of IL-18BP to selected renal failure patients may prove a kidney-saving and even life-saving therapy.
4.2.5. IL-18 in Acute Respiratory Distress Syndrome
Acute respiratory distress syndrome (ARDS) is yet another devastating pathology in which IL-18 is a player. Mehta et al. has shown that the elevated levels of ferritin in this pathology are mediated by IL-18 and are associated with systemic inflammation and mortality (Mehta et al., 2024). A multicenter, randomized controlled trials in patients with ARDS, found that, based on canonical classification, a third of patients were misdiagnosed. High levels of IL-18 (≥ 800 pg/mL) defined a distinct high-risk subgroup associated with mortality. Thus, measurement of IL-18, a marker of inflammasome, may provide crucial prognostic information missed by the measurement of traditional inflammatory biomarkers (Moore et al., 2023).
4.2.6. IL-18 in Gastrointestinal System
Based on publications from groups lead by Flavell and by Elinav (Levy et al., 2015) (Nowarski et al., 2015) Timothy W. Hand postulated that “IL-18 is the bouncer at the mucosal bar” (Hand, 2015). Intact intestinal barrier is essential to maintaining a healthy relationship between host immune system and the microbiota. In 2015, employing conditionally deficient mice in either IL-18 or IL-18 receptor or IL-18BP, Levy et al. and Nowarski et al. have shown the dual nature of IL-18 in the gastrointestinal system. In health, a normal bacterial microbiota produces metabolites, such as taurine, that support inflammasome-mediated production of IL-18 and anti-microbial proteins in the colon thus promoting microbial diversity and preventing commensal dysbiosis. In an inflammatory condition, a dysbiotic microbiota produce different metabolites, e.g. spermine, that inhibit the inflammasome and inhibit anti-microbial protein production, allowing for its invasive character. During inflammation-induced colitis, IL-18 prevents the development of goblet cells from uncommitted precursors, significantly reducing mucus production and intestinal barrier function. It is therefore suggested that IL-18 targeting may prevent the pathologic breakdown of the mucosal barrier in human ulcerative colitis. IL-18’s function as a safeguard maintaining a strict equilibrium of epithelial IL-18 signaling was further demonstrated by Jackson et al. in 2020 (Jarret et al., 2020).
A very recent case report (Guha et al., 2024) presents data on a dramatic improvement and remission of an IBD-associated IL-18’opathy in a four-year-old girl that at 6 weeks of age presented with recurrent fevers, rash and a severe gastrointestinal mucosal ulceration. Though the clinical phenotype mirrored the previously reported case of a child born with a mutation in the inflammasome (NLRC4 gain of function gene variant resulting in IL-18 over expression) and who responded to anti-IL-18BP treatment (Canna et al., 2017), in this girl despite detailed genetic analysis, no known pathogenic variant could be found. The clue to the pathology was found by testing a panel of serum cytokines including IL-1b, TNF-a, IL-6, IFN-a, IFN-g, IL-10, IL-12, IL-17A, IL-18, IL-23 and IL-33. Only IL-18 was highly elevated. Following two years of hospitalization and a failure of a standard therapy with high dose cortico-steroids and IL-1 inhibitors, remission was achieved by a treatment with anti-IL-18 antibody (GSK1070806). Similar to the girl with the NLRC4 mutation, also in this case, the squamous epithelium in the post-esophagus and the colonic mucosa were restored, parenteral nutrition was discontinued replaced by a normal diet, and the girl was discharged from the hospital. The authors conclude that these cases highlight the importance of measuring IL-18 in patients with autoinflammatory diseases and especially those unresponsive to conventional treatments. It also shows the advantage of blocking IL-18, a treatment associated with no adverse effects, compared to using heavy and potentially harmful medications like steroids.
Another study presents evidence that epithelial inflammasome under certain stress conditions mediates protection against intestinal autoinflammation (Zheng et al., 2023). Mertens et al. (Mertens et al., 2024) have recently demonstrated this other aspect of IL-18 dual role, showing that IL-18 may prove beneficial in the gastrointestinal system of mice. Based on their study these authors postulated that IL-18 programs long-lasting intestinal tolerance via an immune metabolic switch in macrophages. Mediated by IL-18 and confirmed in mice lacking the IL-18 natural antagonist, IL-18BP, the switch involves glycolytic polarization through metabolic re-programming to fatty acid oxidation. If applicable, these observations may open personalized therapeutic windows for targeting chronic inflammation in humans.
4.2.7. IL-18 in Covid 19
IL-18 is a player in severe cases of Covid 19. Cytokine storm, a condition described as a highway to hell, is one of Covid’s complications. IL-18 was identified as one of the biomarkers of a cytokine storm signature including that of Covid 19 and was associated with disease severity (Canna & Cron, 2020). We (Volfovitch et al., 2022) and others reported elevated levels of IL-18 in severe cases of Covid 19 with an emphasis on the levels of free IL-18 and IL-18BP (Nasser et al., 2023) (Peleman et al., 2023) (Korotaeva et al., 2024) (Mehta et al., 2024). Fraser et al. (Fraser et al., 2020) concluded from a study of over 2,000 Covid 19 patients that IL-18 is among the top six analytes uniquely elevated in severely ill patients hospitalized in an intensive care unit. A study by Sefik et al. (Sefik et al., 2022) confirmed the role of the inflammasome in general and IL-18 in particular in severe COVID-19. The authors suggest that the replicating SARS-CoV-2 virus in human macrophages activates the inflammasome and initiates an inflammatory cascade leading to pyroptosis. Pyroptosis is an inflammatory form of lytic programmed cell death, characterized by the activation of Caspase 1 and followed by the activation of IL-1, IL-18 and gasdermin. Gasdermin executes pyroptosis via formation of pores on the cell membrane leading to membrane rupture and release of the cytokines (Yu et al., 2021). Blocking one of the products of the inflammasome with IL-18BP may attenuate the overactive immune-inflammatory response, allowing lung tissue recovery and preventing a transition to fibrosis.
Long Covid affects 60 million people globally following severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. Two recent publication (Li et al., 2024) (Krishna et al., 2024) point to IFN-g as a mediator of this long Covid and elevated levels of serum IFN-γ are reported in the long Covid individuals. Comparative single-cell analysis revealed IFN-g as a driver of persistent pulmonary inflammation with tissue fibrosis respiratory sequelae after acute Covid-19. Neutralizing IFN-g after the resolution of acute SARS-CoV-2 infection reduced both these outcomes. The authors suggest blocking of IFN-g signaling axis as a therapeutic intervention, yet they warn that blocking IFN-g is risky because of the exposure of patients to other infections. Therefore, blocking IL-18, which is an IFN-g inducing cytokine but not a master cytokine, may serve a less risky option and an alternative way of therapy.
4.2.8. IL-18 in Cancer: A Double-Edged Sword
In certain cancer microenvironments IL-18 is beneficial. IL-18 anti-tumor activity is attributed among others to its ability to increase cytotoxicity and FAS ligand expression (Kaplanski, 2018). IL-18 has shown anti-tumor activity in different preclinical models of cancer immunotherapy and chemotherapy through the activation of NK and T cell responses. It has been tested in clinical studies in cancer patients, was well tolerated but showed limited efficacy (Robertson et al., 2008). This limited efficacy is associated with the presence of IL-18’s natural inhibitor, IL-18BP and its enhancement by IFN-g in response to IL-18 administration.
Menachem et al. (Menachem et al., 2024) screened over 50 gene-expression studies dealing with myeloid cells in their tumor microenvironment (TME) aiming to identify immune checkpoint proteins suitable for antibody targeting. They have shown that both IL-18 and IL-18BP are upregulated in tumor-associated macrophages (TAMs) but most of the IL-18 is not in a free form but in a biologically inactive complex with IL-18BP. To restore the activity of endogenous IL-18, they generated COM503, a high-affinity anti IL-18BP monoclonal antibody, that blocks the interaction between IL-18BP and IL-18 and displaces precomplexed IL-18, thereby enhancing T- and NK-cell activation. In vivo, this antibody, either alone or in combination with anti-PD-L1 antibody, resulted in tumor growth inhibition, an increase in polyfunctional non-exhausted T- and NK-cell numbers and better survival across multiple mouse tumor models. In patients which are resistant to check point immunotherapy, IL-18BP is a potential target aiming at releasing IL-18 from its complex with IL-18BP.
4.2.9. IL-18 and Immune Checkpoint Inhibitors
Immune checkpoint inhibitors (ICIs) therapy, effective in about 30% of cancer patients, is not an innocent therapy and might cause detrimental, life-long adverse effects. An additional problem that might occur during this treatment is what is termed “pseudoprogression”. Pseudoprogression is not a true tumor escape but a transient inflammatory response and as such requires special attention. Biomarkers that would enable selecting patients that may benefit from ICI therapy are lacking. One such biomarker candidate is IL-18. The rationale behind it is that ICI treatment enhances IFN-g production, which in turn controls the production of IL-18’s very potent antagonist, IL- 18BP. IL-18BP is responsible for the level of the complexed inactive IL-18 and the level of active free IL-18. In addition, it is accepted that the neutrophil-to-lymphocytes ratio serves as a biomarker of response to ICIs and represent the balance between pro-tumoral inflammatory status and anti-tumoral immune response. Indeed, in search of ICI therapy efficacy, Janho Dit Hreich et al. (Janho Dit Hreich et al., 2024) combined the two parameters, IL-18 level and neutrophil concentrations. They performed the study on 195 patients with metastatic non-small-cell lung cancer (NSCLC) treated with ICI anti PD-1 monotherapy. Based on the level of circulating IL-18 and combined with neutrophil count, they demonstrated that patients receiving ICI therapy that go into true tumor progression can be distinguished from patients going into “pseudoprogression”. This distinction is very important because the latter should proceed with the ICI therapy while the former need to stop. The authors measured the levels of the three players of the IL-18 system, free IL-18, IL-18BP and inactive IL-18 that is in complex with its antagonist, IL-18BP. They have confirmed that circulating levels of IL-18 are increased at baseline in NSCLC patients and also showed that compared with true progressors, pseudoprogressors have slightly increased levels of free IL-18. They propose that this difference requires a large-scale validation study to attain statistical significance. They also observe a gradual decrease in the concentration of free IL-18 in patients undergoing ICI therapy. Yet the main finding of their study is that the level of the inactive IL-18, that is complexed with IL-18BP, is the relevant one to the distinction of the patients with “pseudoprogression” from the patients with a true progression. Moreover, the authors state that patients with high levels of inactive IL-18 are linked to poor overall survival.
IL-18 has been shown to be detrimental in several types of cancer, including advanced gastric cancer, certain subsets of melanomas, and T-cell acute lymphoblastic leukemia. It has demonstrated tumor-promoting effects, such as pro-invasive and pro-angiogenic activities (Fabbi et al., 2015).
4.2.10. IL-18 Enhances CAR-T Treatment
IL-18 warrants special attention in the context of chimeric antigen receptor T cells (CAR T) therapy in which the patient’s own T cells are engineered and reprogrammed to destroy the patient’s cancer cells. While CAR T therapy “claim to fame” is almost exclusively in treating hematological malignancies, it has shown limited success in solid tumors, which make up over 90% of adult cancers. One contributing factor to this limitation point to increased levels of IL-18BP, which due to its exceptionally high affinity to IL-18 and a slow dissociation rate (Koff) (Kim et al., 2000) binds IL-18 almost irreversibly effectively removing it from circulation. Zhou et al. (Zhou et al., 2020), from the group of A.M. Ring in Yale (Yale School of Medicine, New Haven, CT, USA), postulated that IL- 18BP is a secreted immune checkpoint and barrier to IL-18 immunotherapy in NSCLC, colorectal cancer, and melanoma. This group engineered a recombinant ‘decoy-resistant’ IL-18 (DR-18) that is blind to IL-18BP, namely, binds IL-18 and transduces the signal, but does not bind IL-18BP. The combination of DR-18 and anti-PD-1 therapy produced a synergistic response that resulted in complete colorectal and melanoma tumor regression in mice. To increase the success rate of CAR T therapy in solid tumors, another strategy was worked out in Memorial Sloan Kettering Cancer Center (Memorial Sloan Kettering Cancer Center, New York, NY, USA). This strategy is aimed at enhancing relevant cytokines production, e.g. IL-18, and thus enabling the T cells to better infiltrate the solid tumor and to improve their specific function in the impaired immunosuppressive tumor microenvironment (Rafiq et al., 2020). Carl June from the University of Pennsylvania, a pioneer and worldwide known for CAR T cell therapy, reviewed these next generation therapies, particularly for solid tumors with an emphasis on brain cancer and including “armoring” CAR T cells with cytokines such as IL-18 (Posey et al., 2024) (Young et al., 2022). Uslu et al. from June’s laboratory showed how to turn immunologically “cold” tumors into “hot” tumors that then become sensitive to CAR-T cells therapy. This group employed IMSA101, a small molecule and an analogue of cGAMP, that is an agonist of STING (stimulator of interferon genes), and that induces a pro-inflammatory cytokine milieu in general and IL-18 secretion in particular, and thereby enhances CART anti-tumor efficacy (Uslu et al., 2024). A Phase I clinical study (NCT04684563) by the group of Carl June in patients with non-Hodgkin lymphoma, Chronic Lymphocytic Leukemia and Acute Lymphoblastic Leukemia, has shown that the product is safe and efficient. A complete response was obtained in six of eight infused patients (Svoboda, 2022).
Additional Phase I clinical studies (NCT05989204 and NCT06287528) were performed in patients with Relapsed or Refractory Acute Lymphoblastic Leukemia to evaluate IL-18 secretion by anti-CD19 CAR T cells engineered to constitutively secrete this cytokine in patients with CD19 positive cancers.
Fischer-Riepe et al. (Fischer-Riepe et al., 2024) employed a similar principle in neuroblastoma and initiated a clinical study (EU CT 2022– 501725–21–00). They have engineered GD2IL18CART cells, consisting of CAR-inducible IL-18 along with CAR T cells directed against a surface antigen originating in neuroectodermal tumor, ganglioside GD2. The interaction of GD2-positive tumor cells and the engineered CAR T cells, GD2IL18CART, resulted in higher IFNg and TNFa release and more effective target cytolysis. Promising results had been obtained in a preclinical study and mice treated with cells engineered with the GD2IL18CART construct did not develop tumors.
Studies in an attempt to improve CAR-T therapy via increase in IL-18 secretion keep accumulating. Hu et al. (Hu et al., 2017) generated IL-18-secreting chimeric antigen receptor T (IL-18-CAR T) cells to significantly boost CAR T cell proliferation and antitumor activity in melanoma mice. Chmielewski and Abken (Chmielewski & Abken, 2017) engineered IL-18-secreting CAR T cells and named them IL- 18 TRUCKs (T cells redirected for universal cytokine- mediated killing). These cells created a cytotoxic and pro-inflammatory environment in advanced tumors and improved the survival of mice with advanced pancreatic and lung tumors. In an automated manner, Glienke et al. (Glienke et al., 2022) scaled up the TRUCK cells to a clinical scale and worked out a procedure for manufacturing sufficient number of cells for clinical application. These CAR T engineered cells, which released inducible IL-18, exhibited cryopreservation stability and increased cytotoxicity towards target cells carrying the tumor antigen glycosphingolipid GD2.
4.2.11. IL-18 Toxicity in CAR T-Cell Therapy
CAR T-cell therapy toxicity comprises the other edge of the IL-18 sword. In Fischer-Riepe’s very recent study (Fischer-Riepe et al., 2024) attention had been paid to this other aspect of IL-18. Indeed, a proteomics screening in patients before and after treatment with CD19-specific CAR T cells have shown an association between serum IL-18 and immune-cell associated neurotoxicity syndrome (Diorio et al., 2022). To address this problem of hyperinflammation Fischer-Riepe et al. (Fischer-Riepe et al., 2024) engineered a construct with a limited systemic release of IL-18 via a strict dependence of this release on the interaction of GD2IL18CART construct with the GD2 target.
The toxicity of CAR T treatment occurs in a subset of CAR T treated patients and is a result of the life-threatening cytokine release syndrome (CRS) that resembles secondary HLH/MAS. A relatively high incidence of CAR T-cell-associated HLH presenting with highly elevated levels of IL-18 was observed in the CD22 CAR T treatment of relapsing patients or those nonresponsive to CD19 targeted therapies (Lichtenstein et al., 2021). This suggests a disruption in the endogenous feedback mechanism that regulates biologically active IL-18 levels and calls for preemptive strategies to prevent CRS. IL-18’s natural antidote, IL-18BP, is a major player in this fine-tuned regulation. Based on its efficacy in treating MAS, HLH, and Still’s disease, Tadekinig alfa™ (NCT03113760) is a promising candidate for managing severe adverse effects or cytokine release syndrome (CRS) in patients undergoing CAR T therapy (Canna et al., 2017) (Geerlinks & Dvorak, 2022) (Gabay et al., 2018) (Yasin, Solomon, et al., 2020).
4.2.12. IL-18 in Skin Diseases
To date, many reports reveal the dysregulation of IL-18 in several skin pathologies e.g. psoriasis, atopic dermatitis, rosacea, and bullous pemphigoid. Keratinocytes comprise a major part of the epidermis and have a critical role in skin inflammation and immune response. In human keratinocytes, pro-IL-18 is constitutively expressed and is activated to IL-18 upon UV irradiation that in turn affects immune cells leading to an inflammatory response. Compared to healthy controls patients with psoriasis exhibit higher levels of IL-18 both in lesions and in blood and the levels correlate with disease severity. As such IL-18 may serve as a potential biomarker in this pathology. A psoriasis-like mouse model in which IL-18 neutralizing antibody successfully blocked the harmful Th17 immune response confirmed that indeed IL-18 is a player in psoriasis. IL- 18 was reported to be the most significantly elevated biomarker also in the skin of Atopic Dermatitis (AD) patients and correlated with disease severity (Wang et al., 2023) (Rusiñol & Puig, 2024). Konishi et al. reported that IL-18 transgenic mice developed AD-like dermatitis (Konishi et al., 2002). Hidradenitis suppurativa (HS) is a chronic skin disease, characterized by clinical inflammation of the hair follicle with the recurrence of abscesses, nodules, and tunnels. Elevated levels of IL-18 and free IL-18 correlating with disease severity were very recently reported by Margiotta et al. in HS, interestingly with no elevation of IL-1b (Manzo Margiotta et al., 2024).
In view of these findings blocking IL-18 in skin diseases either through its natural antagonist, IL-18BP, or with antibodies presents a rationale therapeutic strategy. Indeed, Jang et al. (Jang et al., 2023) designed a form of IL-18 blockade. APB-R3, a long-acting recombinant human IL-18BP linked to human albumin-binding Fab fragment, SL335. APB-R3 has an extended half-life, reduces liver inflammation and splenomegaly in a mouse model of MAS, and controls skin inflammation in a model of atopic dermatitis.
4.2.13. IL-18 in Other Pathologies
Elevated levels of IL-18 and correlations to diseases activity are reported in rheumatoid arthritis, lupus erythematosus, Wegener’s disease, inflammatory bowel diseases and cardiac diseases (Novick et al., 2013) and most recently also in Kaposi sarcoma herpes-associated diseases (Lage et al., 2024). It is evident that IL-18 plays a key role in these pathologies, and its partner in the dyad, IL-18BP, shows promise as a therapeutic drug.
5. IL-18 Binding Protein (IL-18BP)
Tight regulation of cytokine-driven signaling, inflammation, and immunoactivation is required to enable counteracting possible deleterious effects such as transition to chronic inflammation, autoimmunity, fibrosis and even loss of organ function. The immune system evolved in such a way that the balance is kept via natural cytokine antagonists operating in a feedback regulation mode of action. Most of these regulators are soluble receptors while a few are unique binding proteins.
IL-18BP (Novick et al., 1999), osteoprotegerin (OPG), (Simonet et al., 1997), cytokine-like factor-1 (CLF 1) (Elson et al., 1998) and IL-22 binding protein (IL-22BP) (Mühl & Bachmann, 2019) belong to a group of receptor-like decoy proteins, if defined by their function, however are encoded by a separate gene, if judged by their structure. The members of this family of proteins exist solely in a soluble form.
OPG, a member of the TNF receptor family, a physiological antagonist of Receptor Activator of NF-κB Ligand (RANKL), and also known as osteoclastogenesis-inhibitory- factor (OCIF), is a player in bone-related diseases, cancer and neurodegenerative disorders thus is a potential biomarker and a therapeutic target (Baud'huin et al., 2013) (Freeman et al., 2024). Cytokine-like factor 1 (CLF1 or CRLF1) is a secreted receptor belonging to the IL-6 family. CLF1 form a secreted heterodimer together with its physiologic partner, cardiotrophin-like cytokine (CLC), and this complex is a part of the signaling pathways of ciliary neurotrophic factor receptor (CNTFR), leukemia inhibitory factor (LIFR) and gp130. Mutations in CLF1 gene are linked to the sometimes-fatal Crisponi or cold-induced sweating syndrome (Kass, 2011). IL-22BP, a member of the IL-10 cytokine family, is a high affinity antagonist of IL-22. Though encoded by a separate gene, IL-22BP shares 34% sequence homology with the extracellular domain of IL-22R. IL-22BP guards the dual-natured IL-22, that depending on the milieu, is either protective or pro-inflammatory. It balances IL-22’s main function in wound healing and in maintaining tissue homeostasis, it may reduce the tumor promoting activity of IL-22 in hepatocellular carcinoma, and may block IL-22 involvement in liver cirrhosis, chronic inflammation, psoriasis and arthritis (Dumoutier et al., 2001) (Mühl & Bachmann, 2019) (Zenewicz, 2021).
Though all four members of this unique family of naturally occurring soluble proteins have clinical significance, IL-18BP is the only one that has advanced to clinical trials. Moreover, it is in compassionate use for seven years now, awaiting the FDA approval following the recently completed Phase III clinical study (NCT03113760).
5.1. IL-18BP Is Not a Canonical Soluble Receptor
IL-18BP is a rare example of a naturally occurring and extremely potent antagonist. Structurally it includes a single Ig-like domain with little homology to either chain of the IL-18 receptor. It is unique by virtue of being encoded by a separate gene, located on chromosome 11 (11q13.4), that is distinct from that of the genes coding for IL-18 cell-bound receptor located on chromosome 2 (2q12.1). IL-18BP therefore deviates from the canonical definition of a soluble receptor. The shared ligand, IL-18, of both the receptor and the binding protein, is located on chromosome 11 (11q22.2). IL-18BP serves as a natural soluble decoy protein and its remarkable affinity for IL-18 prevents the shared ligand from interacting with its cellular receptors thus making IL-18BP an effective antagonist of IL-18 signaling (Novick et al., 1999).
IL-18BPa binds mature but not pro-IL-18 and is the most active of the four splice variants in humans: IL-18BPa, b, c and d. IL-18BPc shares the immunoglobulin domain of IL-18BPa except for the 29 C-terminal amino acids and the Kd of IL-18BPc is 10-fold lower than that of IL-18BPa. IL-18BPb and IL-18BPd isoforms lack the entire Ig domain and lack the ability to bind or neutralize IL-18 (Kim et al., 2000). IL-18BPa is constitutively expressed in hematopoietic and non-hematopoietic cells (Mühl & Bachmann, 2019).
5.2. IL-18BP Isolation and Cloning
Based on our laboratory’s success in isolating the canonical soluble TNF receptors, IL-6 receptor and both types of interferon receptors (Novick, 2022) (Novick, 2023) an attempt was made to isolate the soluble receptor of IL-18. Our strategy of isolation combined two key elements: a rich source of proteins, in our case human urine collected from healthy individuals and concentrated 500-fold, and a simple, specific and efficient isolation method, ligand (IL-18)-affinity-chromatography (Novick et al., 1999). A 500 mL batch of concentrated urine (equivalent to 250 liters of normal human urine) was applied onto IL-18 (2.5 mg) covalently coupled to Sepharose-beads (0.5 mL) column, followed by extensive washing and acidic elution of the IL-18-bound proteins (Figure 1). Notably, I observed that releasing IL-18BP from the affinity column required at least eight column volumes of a highly acidic elution buffer (pH 2.2), whereas all other soluble receptors we previously isolated eluted in a sharp peak within two column volumes as expected. This "smear" phenomenon hinted at IL-18BP’s exceptionally high affinity for its ligand, which was later confirmed. The pooled elution fractions were subjected to N-terminal sequencing (Edman, 1949) that yielded 40 amino acids. Based on this N-terminal amino acid sequence to deduce the corresponding DNA sequence, namely going from protein to DNA, Soo Hyun Kim in our laboratory successfully cloned the IL-18BP. cDNA libraries were screened with a probe generated from 40 N-terminal amino acid sequence of the purified urinary protein. A search in the human cDNA database of the Institute of Genomic Research (TIGR) resulted in an almost perfect match with the cDNA clone THC123801, derived from a human Jurkat T cell library and coding for a protein of unknown function. Interestingly, the transcript was homologous to transcripts encoded by all known Poxvirus, hinting at its function as a potent immunosuppressor. We further characterized the IL-18BP and have shown that the mature IL-18BP protein is a constitutively expressed glycosylated protein composed of 164 amino acids and with a molecular mass of ca. 40 kDa. It blocks the biological activities of IL-18 and inhibits the induction of IFN-g in vitro and in vivo. Four splice variants were identified, with IL-18BPa being the most abundant and the most active among them (Novick et al., 1999) and the subject of this review.
Isolation of the soluble IL-18 receptor failed due to its low affinity to IL-18, and to its low concentration in a healthy urine. However, we successfully isolated a second member of a novel family of proteins, the high affinity IL-18BP.
5.3. Regulation of IL-18BP
IFN-g is the primary regulator of IL-18BP, operating through a negative feedback mechanism. IFNa and IL-27 stimulate IL-18BP production (Mühl et al., 2000) (Hurgin et al., 2002) (Kaser et al., 2002) (Bosmann & Ward, 2013) (Wang, 2024).
5.4. IL-18BP Promoter
Hurgin et al. (Hurgin et al., 2002) in our laboratory characterized the IL-18BP promoter. He identified a gamma-activated sequence (GAS) proximal to the transcription start site, followed by an IFN regulatory factor 1 response element (IRF-E) and two CCAAT enhancer binding protein (C/EBP) sites. Furthermore, he showed that GAS and IRF-E were essential for IFN-g induced transcription. IL-18BP is a potent inhibitor of IL-18, an inducer of T helper 1 cytokines such as IFN-g. Thus, induction of IL-18BP by IFN-g provides a negative feedback mechanism that shuts off IL-18-elicited immune responses. To avoid premature termination of IL-18 activity, induction of IL-18BP must occur after some delay. Indeed, Hurgin et al. showed that induction was not mediated by the rapid IFN-g -induced Janus kinase-STAT signaling pathway but rather required de novo synthesis of the transcription factor IRF-1, which together with C/EBP activates the IL-18BP promoter.
5.5. IL-18BP Evolutionary Importance
IL-18BP is mimicked by viruses such as Molluscum contagiosum virus and Pox viruses, aiming to evade the host immune system. This phenomenon emphasizes IL-18BP’s critical role in host-pathogen interaction and underlines its evolutionary significance in immune defense mechanisms (Novick et al., 1999) (Smith et al., 2000).
5.6. IL-18BP Knockout Mice
In 2015, the groups of Flavell and Elinav showed that deletion of the IL-18 gene or its receptor (Il18r1) in mouse intestinal epithelial cells confers protection from colitis and mucosal damage, while the deletion of the IL-18BP gene results in severe colitis associated with the loss of mature goblet cells and lethality. They proposed that a strict equilibrium of epithelial IL-18 signaling must be maintained and suggested that IL-18 targeting may prevent the pathologic breakdown of the mucosal barrier in human ulcerative colitis (Nowarski et al., 2015). Others have shown that IL-18BP is required for normal NK cell maturation, abundance, and function, and that its deficiency results in aberrant proportions of NK cell subsets and increased TNF-a production (Harms et al., 2017). In yet another mouse model, upon repeated TLR9 stimulation, IL-18BP-knockout mice showed severe MAS manifestations, including increased weight loss, splenomegaly, anemia, thrombocytopenia, hyperferritinemia, and bone marrow hemophagocytosis, as well as elevated circulating free IL-18 levels, higher IFN-g production, and enhanced IFN-g molecular signature. Therefore, an imbalance between IL-18 and its natural inhibitor IL-18BP may lead to severe MAS, thus reflecting some of the clinical findings of autoinflammatory syndromes such as AOSD and MAS in humans (Girard-Guyonvarc'h et al., 2018).
5.7. IL-18BP Affinity and Dissociation Rate: Advantages for Drug Development
The affinity of IL-18BP to IL-18 is very high. Employing a surface plasma resonance, BIAcore, aimed at measuring biomolecular interactions, and using a sensor chip with immobilized human IL-18, we reported a KD of 0.4 nM (Kim et al., 2000). More recently a 10-fold higher KD of 0.05 nM was reported (Girard et al., 2016). This KD is more than two orders of magnitude higher than the affinity of the ligand binding chain of the IL-18 receptor, IL-18Ra, to the same ligand. Moreover, the dissociation rate (Koff) of the IL-18/IL-8BP dyad is extremely low (Kim et al., 2000) thus making it a very stable complex. Wu et al. (Wu et al., 2003) have shown that the affinity of IL-18BP to IL-18 is comparable to the affinity of IL-18 when bound to both chains of the IL-18 receptor. Notably, in this study, IL-18BP demonstrated superior inhibitory activity compared to three neutralizing monoclonal antibodies developed against IL-18. A slow dissociation rate indicates a prolonged binding of a compound to its target, a desirable trait for a prospective drug, as it increases its pharmacokinetics and may even eliminate the need for its modification. Indeed, unlike canonical soluble receptors, e.g. the soluble TNF receptor (Engelmann et al., 1990) that had been translated into the drug Enbrel ® as a fusion protein with the Fc portion of immunoglobulin, to increase its molecular weight, IL-18BP is an unmodified natural drug. The relatively low molecular weight of IL-18BP is compensated by its slow dissociation which allows it to form a very stable complex with IL-18 and prevents rapid clearance by the kidney. Employing a natural, unmodified drug minimizes the risk of provoking an immune response in the patient, thereby decreasing the chances of having to halt the treatment.
5.8. IL-18BP Level in Health and Disease
Our laboratory generated monoclonal antibodies against IL-18BP and developed a sandwich ELISA aimed to monitor IL-18BP levels in health and disease. In addition, we introduced the term of “free IL-18”, IL-18 that is not in a complex with IL-18BP, and most probably it is the level of a free cytokine that dictates the outcome of a pathology. We found that the level of IL-18BP in healthy individuals is around 2 ng/ml and in a disease state such as the level may rise more than 10-fold (Novick et al., 2001). In IL-18’opathies the increase in the level of IL-18BP is not sufficient for the neutralization of the also increased circulating IL-18 and thus the level of free IL-18 remains high (Novick et al., 2013). The balance and fine tuning between IL-18 and IL-18BP is crucial in determining immune responses and disease outcomes. Excessive IL-18 activity, in the absence of IL-18BP, can lead to devastating pathological inflammation and tissue damage, calling for external administration of the antidote.
6. The Clinical Relevance of IL-18 and IL-18BP
6.1. The Therapeutic Potential of IL-18/IL-18BP Axis
IL-18 and IL-18BP are associated with various diseases, including autoimmune disorders, inflammatory conditions, infectious diseases, and cancer (Mühl & Bachmann, 2019). By modulating the IL-18/IL-18BP axis, therapeutic interventions could aim to either enhance or suppress immune responses depending on the specific disease context. For example, in autoimmune diseases characterized by excessive IL-18 activity, blocking IL-18 or enhancing IL-18BP function could be beneficial. Conversely, in conditions where immune responses are suppressed, such as cancer, strategies to inhibit IL-18BP and boost IL-18 activity might be more appropriate. Indeed IL-18BP had been shown to be a secreted immune checkpoint and barrier to IL-18 immunotherapy. (Zhou et al., 2020).
6.2. IL-18 in Differential Diagnosis (HLH and MAS)
Hemophagocytic lymphohistiocytosis (HLH) is a life-threatening, hyper-inflammatory disorder, characterized by multiorgan failure, fever and cytopenia. Diagnosis of HLH and its subtype MAS remains a challenge. A massive increase in IL-18 blood level is a potential biomarker for HLH/MAS but is currently not a part of diagnostic criteria. The benefit of weaning these patients from steroids and other harsh medications concomitantly with the stabilization of the disease with IL-18BP is invaluable. Moreover, if in certain pathologies, e.g. sJIA, high IL-18 levels are detected early enough it may prevent progression to MAS (Canna & Marsh, 2020) (Krei et al., 2021).
6.3. IL-18BP in Covid 19
A study performed on two cohorts of severely ill patients in two hospitals in Washington identified IL-18BP as one of three biomarkers for COVID-19-associated- secondary-HLH (Canny et al., 2024). These biomarkers, soluble PDL-1, soluble TNFR1 and IL-18BP, are IFN inducible proteins and are antagonists of their corresponding ligands. IL-18BP and soluble TNF-R1 have been previously reported to be elevated in subjects with MAS/HLH (Shimizu et al., 2018) (Mazodier et al., 2005). IL-18 in Covid 19 is discussed under item 4.2.5.
6.4. Fatal IL-18BP Deficiency
Belkaya et al. (Belkaya et al., 2019) reported a death of an 11-year-old girl in France due to Fulminant viral hepatitis (FVH) upon infection with hepatitis A virus (HAV). Post-mortem analysis using whole exome sequencing revealed that she had an autosomal recessive single-gene inborn error of immunity, resulting in complete deficiency of IL-18BP. Both her parents and two siblings were heterozygous for the mutation therefore although they were seropositive for HAV they did not develop FVH. FVH is a life-threatening condition characterized by massive necrosis of the liver, jaundice, encephalopathy, impaired coagulation, all developing within weeks of the onset of the first symptoms in individuals without preexisting liver disease. IL-18 and IL-18BP are both secreted mostly by hepatocytes and macrophages in the liver. The authors suggest that this patient’s liver had been destroyed by NK and CD8 T cytotoxic cells via enhanced and uncontrolled IL-18 and IFN-g-dependent killing of hepatocytes. Based on the success of a treatment with IL-18BP in other conditions in which IL-18 is expressed in excess and based on its beneficial effect in experimental acetaminophen hepatotoxicity (Bachmann et al., 2018) as well as in human acute liver failure due to paracetamol overdosing or liver transplantation, Belkaya et al. proposed that IL-18BP may serve as an antidote in a devastating FVH condition (Belkaya et al., 2019).
6.5. Safety and Tolerability of IL-18BP Therapy
IL-18BP had been translated into the drug Tadekinig alfa and a Phase III clinical trial (NCT03113760) had been recently completed. The studies demonstrated its safety, tolerability and efficacy profiles. Phase I/II trials, along with seven years of compassionate use of this drug, have consistently demonstrated that IL-18BP therapy is well tolerated and associated with minimal adverse effects. These findings stress the clinical potential of IL-18BP as a safe and effective therapeutic intervention for immune-mediated diseases, making it a promising and low risk therapeutic option (Tak et al., 2006) (Gabay et al., 2018) (Kiltz et al., 2020). The fact that Tadekinig alfa is a self-protein is a significant advantage. Furthermore, its relatively short yet adequate half-life of 2-3 days makes it superior to IL-18-blocking antibodies, which have a half-life of 3-4 weeks. This characteristic is particularly beneficial in situations where treatment must be urgently discontinued to allow IL-18 to perform its role, such as combating a life-threatening infection.
Targeting IL-18
The significance of the IL-18/IL-18BP dyad in various pathologies is reflected in the diverse strategies aimed at targeting IL-18 and IL-18BP, and in the involvement of at least 11 companies in this task. The strategies focus on either blocking or enhancing of the relevant players. IL-18’s natural antagonist, IL-18BP, had been translated into a drug, Tadekinig alfa, and anti IL-18 antibodies had been designed, to address cases where IL-18 is detrimental. Conversely, in those cases that IL-18 is beneficial, modified IL-18 with increased biological activity and the ability to evade its decoy protein, is being developed. CAR T cells with dual specificity are engineered in an attempt to potentiate their anti-tumor activity by incorporating an IL-18 producing construct into these cells. Based on the role of IL-18 signaling in tumor immunotherapy, additional innovation combines cancer checkpoint therapy with IL-18 signaling. Variations of PD1-IL18 conjugates are under development showing a remarkable increase in anti PD-1 potency. Additionally, anti IL-18BP antibodies are being developed to ensure IL-18 remains in its active unbound form. A book titled "Interleukin-18 (IL-18) Inhibitor - Pipeline Insight, 2024" provides a comprehensive overview on the biology of IL-18, its targeting and the pipelines of several companies referring to IL-18 therapies. Simcha Therapeutics, GlaxoSmithKline, Novartis, Olatec Therapeutics, Compugen, Lassen Therapeutics, Xencor, Bright Peak Therapeutics, Werewolf Therapeutics are among these companies, but the most advanced is AB2 Bio in Lausanne that completed a Phase III clinical study for Tadekinig alfa (IL-18BP). Recombinant IL-18BP that was translated into Tadekinig alfa, proved safe and very effective in antagonizing IL-18 and is in compassionate use for seven years now (Bindoli et al., 2024).
IL-18 is an IFN-g inducing factor and member of the IL-1 family. It is a cytokine with a dual nature, participating in both innate and adaptive immunity, but is not a master cytokine. IL-18’s activity is tightly regulated by its highly potent natural antagonist, IL-18BP. IL-18 is mainly a proinflammatory cytokine for host defense against pathogens, but when out of balance with its dyad’s partner, IL-18 is associated with various autoimmune and inflammatory disorders, such as adult-onset Still’s disease, hemophagocytic syndrome, macrophage activation syndrome, fulminant hepatitis, lupus erythematosus, inflammatory bowel diseases, atopic dermatitis, psoriasis and more. Furthermore, IL-18 is among the cytokines implicated in a cytokine storm that may be a sequalae of autoimmune and inflammatory diseases, viral infections, cancer and severe cases of Covid 19. IL-18 was also described as an immune checkpoint in cancer treatments such as CAR T cell therapy and anti PD-1 therapy. Enhancing IL-18 activity in the early stage of immunotherapy and inhibiting it in the late stage, proved beneficial. All these features make IL-18 an attractive target for both antagonistic and agonistic approaches. Indeed, academia and industry have taken on the challenge.
7.1. IL-18 Inhibitory Drugs (Table 1)
7.1.1. IL-18 Binding Protein (Tadekinig alfaTM) by AB2 Bio
Recombinant IL-18BP, the natural antagonist of IL-18, was translated 20 years ago by Ares Serono’s Inc. (now Merck) into the drug Tadekinig alfa. It binds IL-18 with extremely high affinity, forming a very stable complex that effectively neutralizes IL-18’s biological activity. Safety was demonstrated in Phase I and Phase Ib clinical studies with no observed adverse effects. Judged by the decrease in the level of IFN-g, Tadekinig alfa was effective in psoriatic arthritis patients chosen for the study, yet the patients did not get better since the duration of the study was too short (Tak et al., 2006). In 2010 Serono sublicensed Tadekinig alfa to AB2 Bio Ltd. (Lausanne, Switzerland) and several indications such as AOSD, refractory sJIA and recurrent MAS were considered for a Phase II clinical study. The Phase II clinical study in AOSD patients was successful and awaits Phase III in this indication (Gabay et al., 2018) (Yasin, Fall, et al., 2020). Two devastating pathologies caused by genetic mutations and characterized by an over-expression of IL-18 were chosen for a Phase III clinical study. Phase III was successfully completed in children with a life-threatening inborn mutation in the inflammasome (NLRC4 gain of function) (Canna et al., 2017) and in children with the devastating XIAP deficiency mutation (NCT03113760) (Geerlinks & Dvorak, 2022) (Higuchi et al., 2022). The NLRC4 gain-of-function mutation may result in MAS and a mutation in XIAP may lead to HLH. Treatment with Tadekinig alfa proved lifesaving for these children and years of continuous maintenance remained very effective. Consequently, the FDA approved skipping a Phase II study allowing direct progression to Phase III trials for these indications. Since 2017, Tadekinig alfa has held FDA orphan drug designation for the treatment of Still's disease, AOSD, sJIA and HLH. Moreover, the drug was also approved for compassionate use and over the past seven years, it has kept hospitalizations at bay, enabling these children to lead normal lives. Tadekinig alfa allowed weaning these children from toxic non-specific medications (e.g. steroids) and biologics such as IL-1 and TNF blockers, supporting normal growth and development as well as recovery of their damaged organs.
Tadekinig alfa treatment is being considered for the treatment of MAS, a potential sequalae of cancer and viral diseases, which otherwise has no cure and can have a mortality rate of up to 50%. Another potential candidate for IL-18-blocking therapy is the severe cytokine storm syndrome (Behrens, 2024) seen in conditions such as patients undergoing CAR T therapy (Lichtenstein et al., 2021) (Diorio et al., 2022) and in severe cases of COVID 19 (Sefik et al., 2022).
7.1.2. IL-18 Antibody (GSK-1070806) by GlaxoSmithKline
GSK-1070806 is a humanized IgG1/kappa antibody directed against IL-18. It was tested for the treatment of type 2 diabetes, delayed graft function after renal transplantation and Behcet's disease and is currently in Phase II clinical study for moderate to severe Atopic Dermatitis (NCT05999799). The study is planned to be completed by 2025.
7.1.3. IL-18 Antibody (Camoteskimab) by Apollo Therapeutics (Avalo Therapeutics and MedImmune)
Camoteskimab (also known as CERC 007, AEVI 007 or MEDI 2338) first developed by Avalo Therapeutics and MedImmune, is a fully human monoclonal antibody which targets IL-18. A Phase I open-label trial was performed in the USA (NCT04752371) and these antibodies are currently tested in Phase II (NCT06436183) for atopic dermatitis. It is planned to be completed in 2025.
7.1.4. IL-18 and IL-1 Bispecific Antibody (MAS825) by Novartis
MAS825 is a high-affinity bispecific monoclonal antibody directed against IL-18 and IL-1β. It was tested in Covid 19 pneumonia patients (NCT04382651) but did not meet the primary efficacy endpoint. Nevertheless, in that study MAS825 antibody combined with standard of care, inhibited relevant cytokine pathways, accelerated SARS-CoV-2 virus clearance, and improved impaired respiratory function compared with placebo (Hakim et al., 2023). Novartis is currently conducting a Phase II clinical study to evaluate the efficacy, safety and tolerability of MAS825 in indications previously tested by AB2 Bio using Tadekinig alfa (IL-18BP), namely in patients with monogenic IL-18 driven autoinflammatory diseases, including NLRC4-GOF, XIAP deficiency, or CDC42 mutations (NCT04641442). The study is anticipated to be completed 2031.
7.1.5. NLRP3 Inflammasome Inhibitor (Dapansutrile) by Olatec Therapeutics
Inflammasomes, extensively reviewed by Coll and Schroder (Coll & Schroder, 2024), can induce pathological inflammation and tissue damage and are thus new class of drug targets. One example is Olatec’s oral Dapansutrile (OLT1177®) small molecule, β-sulfonyl nitrile. It inhibits the conversion of the inactive pro IL-1β and pro IL-18 to their active forms by selectively targeting NLRP3 inflammasome. It is aimed to treat acute and chronic inflammatory diseases such as arthritis, heart failure, asthma, Alzheimer’s disease, Parkinson's disease, multiple sclerosis, spinal cord injury, type-2 diabetes, melanoma and breast cancers. OLT1177TM is the only known selective NLRP3 inflammasome inhibitor currently in Phase 2 clinical trials in the US and Europe.
7.2. IL-18 Enhancing Drugs (Table 2)
7.2.1. IL-18 Variant (ST-067) by Simcha Therapeutics (USA)
ST-067 is a “decoy-resistant” variant of IL-18, designed to be impervious to IL-18BP. In preclinical studies ST-067 has shown enhanced anti-tumor immune stimulation. This potential drug is currently in Phase 1/2 clinical study in a variety of solid tumors (melanoma, renal cell carcinoma, triple negative breast cancer, NSCLC, head and neck cancer and more) aimed to test for safety and preliminary efficacy in a form of a monotherapy and in combination with Merck’s checkpoint anti PD-1 antibody, pembrolizumab (NCT04787042). It is planned to be completed by 2030 (Zhou et al., 2020).
7.2.2. Modified IL-18 Fused to Fc (XmAb143) by Xencor
IL-18, as a single agent in cancer therapy, exhibits poor pharmacokinetics and an overall lack of efficacy. In attempt to upgrade IL-18’s therapeutic performance Xencor engineered an IL-18 heterodimeric Fc-fusion protein (XmAb143), with improved thermo-stability, increased half -life from hours to days and insensitivity to the inhibition by IL-18’s natural antagonist, IL-18BP. Moreover, this modified IL-18 exhibited increased potency in IFN-g induction by NK and T cells and over a 2,000-fold decrease in PD-L1 induction potency as compared to WT IL-18-Fc. XmAb143 exhibited toxicity only in high doses as demonstrated in pilot studies carried out in cynomolgus monkey (Nisthal, 2022).
7.2.3. Modified IL-18 Fused to Fc and Targeted to PD-1 (BPT 567/PD1-IL18-Fc) by Bright Peak Therapeutics
Bright Peak’s unique protein engineering and chemical conjugation platform is based on the studies of Codarri Deak et al. who developed a new generation of PD-1 cis-targeted cytokine agonists with enhanced therapeutic potential for the treatment of cancer (Codarri Deak et al., 2022). This strategy enabled the generation of BPT567 conjugate composed of IL-18BP-resistant IL-18 variant with anti-PD-1 antibody, Lipustobart. Following conjugation of the two, BPT567 retained the biologic activity of IL-18 and a functional PD-1/PD-L1 blockade. At the 2024 annual meeting of American Association for Cancer Research (AACR) Bright Peak presented in vitro data showing that BPT567 triggers maximal IFN-g release in NK92 cells expressing human PD-1, anti PD-1 enhanced potency, and increased IL-18BP resistance due to simultaneous binding to IL-18 receptor and PD-1 on the same cell (cis-signaling). BPT567 exhibits notable single agent anti-tumor efficacy superior to that of anti-PD-1 antibody single agent or non-targeted IL-18. In vivo, BPT567 is well tolerated, induces expansion of effector memory CD8 T cells and exhibits strong anti-tumor efficacy at significantly lower IL-18 doses compared to the combination of an untargeted antibody-IL-18 conjugate and an anti-PD1 antibody further substantiating the importance of cis-signaling.
7.2.4. Modified and Conditionally Activated IL-18 Resistant to IL-18BP (WTX 518) by Werewolf Therapeutics
Data referring to WTX-518 were presented at the 2024 AACR annual meeting. WTX-518 is being developed to maximize the potential clinical benefit of IL-18 when administered as monotherapy or in combination with checkpoint inhibitors in refractory and/or immunologically unresponsive tumors. WTX-518, an IL-18 pro-drug, resistant to IL-18BP inhibition, is conditionally activated within the tumor microenvironment, promotes increased influx and activation of NK cells and polyfunctional CD8 T cells and induces regressions in mouse tumor models (Morris, 2024).
7.2.5. Antibody Based IL-18 Agonist Resistant to IL-18BP
Lipinski et al. (Lipinski et al., 2023) in collaboration with Merck (Merck Healthcare KGaA, Darmstadt, Germany), employed a strategy that enables the generation of IL-18 mimetics with tailor-made cytokine functionalities aimed at promoting IL-18’s antitumor therapeutic activity. First, they generated a bispecific antibody derivatives that mimic the function of IL-18 via cross linking the IL-18 receptor subunit. This construct was based on single-domain antibodies raised in camelids, specific to IL-18 receptor chains, IL-18 Rα and IL-18 Rβ. |They used these antibodies for the screening of yeast surface display and selected variable domains of the heavy chain (VHH) targeting the individual receptor subunits. These bispecific cytokine mimetics constructs were more potent than IL-18 in triggering proinflammatory cytokine release, e.g. IFN-g, and were unaffected by IL-18 binding protein.
Synthekine further developed this concept, focusing on three key aspects: (1) IL-18 can enhance both innate and adaptive anti-cancer immune responses through signaling across a wide range of cells; (2) IL-18’s proinflammatory activity can counteract the tumor microenvironment’s immunosuppressive state; and (3) IL-18 has shown good tolerance as a single agent in clinical trials. However, IL-18’s efficacy has been limited due to inhibition by IL-18BP. To address this limitation Synthekine engineered IL-18 surrogate cytokine agonists (SCAs). Employing yeast/phage display Synthekine sorted IL-18 surrogate cytokine agonists composed of the two IL-18 receptor chains relevant epitopes that can mimic cytokine signaling. They have shown that the selected SCA expand and activate NK and CD8 positive cells in vitro and in vivo, e.g IFN-g induction and NFkB signaling and is not inhibited by IL-18BP.
7.3. IL-18 Activity Enhancement Strategy Using IL-18BP Antibodies
7.3.1. IL-18BP Antibody (COM503) by Compugen and Gilead
COM503 is a fully human high affinity antibody which blocks the interaction between IL-18 binding protein and IL-18, thereby freeing IL-18 in the tumor microenvironment to inhibit cancer growth. The rationale behind it is that in a certain cancer microenvironment IL-18 activates anti-tumor effector cells, such as T and NK cells but the tumor uses IL-18’s natural antagonist, IL-18BP, to block this activity and thus evades the host’s immune system. Compugen employed its proprietary computational discovery platform to identify new drug targets with the ability to enhance anti-cancer immune responses and selected the COM503 anti IL-18BP antibody aimed for the treatment of solid tumors. Compugen is in charge for the ongoing pre-clinical development of COM503 and the Phase 1 study planned to commence at the end of 2024, while Gilead has the sole right to develop and commercialize COM503. So far Compugen has shown that COM503 restores human tumor infiltrating lymphocytes (TILs) and NK cell activity in human assays and that anti-mouse IL-18BP antibody is effective as a monotherapy in mouse breast cancer, colorectal cancer and melanoma tumor models (Menachem et al., 2024). Compugen believes that blocking IL-18BP with an antibody represents a promising approach in leveraging cytokine biology in cancer treatment.
7.3.2. IL-18BP Antibody (LASN500) by Lassen Therapeutics
Lassen Therapeutics’ anti IL-18BP antibody is a candidate for human cancer immunotherapy. The company presented preclinical data at the 2023 AACR annual meeting demonstrating that these antibodies inhibit tumor growth in a mouse syngeneic tumor model. These antibodies also mediate a beneficial proinflammatory response in cancer through enhanced induction of IFN-g and other cytokines, and in combination with the PD-1 antibody they potentiate the activity of IL-18 immunotherapy by inhibiting the checkpoint activity of IL-18BP and enhancing the immune response of NK cell and T cell (Jun, 2023).
7.4. IL-18 and CAR T Combined Therapy (Table 3)
7.4.1. IL-18 and CAR T Combined Therapy by Janssen Research & Development
Two basic findings are the rationale and the major catalyst behind IL-18 engineering aimed for CAR T therapy: (1) IL-18 increases the potency of CAR T cells in tumor immunotherapy via the enhancement of T-cell proliferation, INF-g production, and cytolytic activity, including cytotoxic T cell and NK cell mediated cell killing; (2) In the tumor microenvironment IL-18’s natural inhibitory decoy protein, IL-18BP, reduces IL-18’s activity. The most advanced data on IL-18-armored CAR T cells comes from the team led by Carl H. June at the University of Pennsylvania. An ongoing Phase I clinical study (NCT04684563) by Gilead, employing autologous CAR T cells directed against the human CD19 antigen that also express human IL-18 (HuCART19-IL18. It is known that a significant proportion of patients with relapsed/refractory non- Hodgkin lymphomas (NHL) will not derive a long-term benefit from the existing anti-CD19 CAR T cells. June’s team approached this problem by engineering huCART19-IL18, a 4th generation 4-1BB anti-CD19 construct, armored with the ability to secrete IL-18. So far it was shown that treatment with huCART19-IL18 is relatively safe and produces durable remissions in heavily pre-treated lymphoma patients (Svoboda, 2022, 2024).
7.4.2. Eutilex Co. Ltd. in Korea Engineered a Combination of a Targeted Hepatocellular Carcinoma Tumor (HCC) Marker, Glypican-3 (GPC3) and an IL-18-Secreting CAR T Cell Therapy (EU-307 GPC3-IL18) Which Is in Phase I and Designated for the Treatment of HCC and Non-Small Cell Lung Carcinoma
7.4.3. Memorial Sloan Kettering Cancer Center Is Conducting an Ongoing Phase I Study (NCT06017258) that Tests CAR T Cell Therapy Using a Combination of Acute Myelogenous Leukemia (AML) Marker and an IL- 18-Armored Construct (CD371-YSNVZIL-18). This Study Is Expected to Be Completed in 2026
8. Concluding Remarks
The quote from the prophet Amos, "Can two walk together unless meant for each other," perfectly captures the essence of the IL-18/IL-18BP dyad. This unique biological partnership deserves attention from both basic science and clinical research. The importance of the IL-18/IL-18BP dyad lies in its ability to balance the immune system, making it a potential therapeutic target for autoimmune, inflammatory diseases, and cancer, conditions that require precise immune modulation. The rare and distinct features of this dyad make it ideally suited for its regulatory function. IL-18, an IFN-g inducing factor, and its evolutionary conserved receptor, are IL-1 family members. IL-18 bridges innate and adaptive immunity, is produced by most cells, is always on standby, and induces and is regulated by IFN-g. It mainly acts as a Th1-associated proinflammatory cytokine but has a dual nature, depending on the microenvironment. Clinical studies have confirmed this duality: IL-18 can be harmful in autoimmune diseases and conditions involving rare mutations, yet beneficial in pathogen defense and certain cancers. IL-18BP is one of only four naturally occurring antagonists that bind the same ligand as cell surface receptors but are encoded by a separate gene. Unlike canonical soluble receptors, these binding proteins, including IL-18BP, lack membrane-bound counterparts. Viral mimicking of IL-18BP suggests its evolutionary significance. Its genetic absence in humans might be fatal. With an exceptionally high affinity for IL-18, much higher than any canonical soluble receptor has to its ligand, IL-18BP controls free IL-18 levels, which are critical in disease. IL-18BP is therapeutically safe and beneficial in various IL-18’opathies and has been in compassionate use for many years.
So, what makes the IL-18/IL-18BP dyad special? IL-18, a ready to act cytokine, is a member of the IL-1 family of cytokines yet is not a master cytokine. It is nevertheless responsible for chronic and acute IL-18’opathies, sometimes fatal. To keep IL-18 level in a normal range nature has provided a unique, potent and therapeutically safe antidote, IL-18BP. In the Covid-19 pandemic, this pair IL-18/IL-18BP, had been reported to play a role in severe cases of the disease. IL-18, recognized as a checkpoint is an attractive target in one of the most advanced therapies for cancer, CAR-T. These characteristics call for taking advantage of what nature has provided, namely, using IL-18 as an easily measurable biomarker for differential diagnosis, and employing its antidote, IL-18BP, as a safe therapeutic agent. Therefore, IL-18BP should be the primary therapeutic choice for relevant conditions, replacing more aggressive treatments like IL-1 and IL-6 blockers, which carry risks of complications and severe infections. Finally, the dynamic interplay between IL-18 and IL-18BP is context-dependent, with varying effects in different physiological and pathological conditions. While IL-18 promotes inflammation and immune activation, IL-18BP counterbalances it, mitigating excessive IL-18 activity and dampening inflammatory responses. This finely tuned regulation underscores the sophistication of the immune system’s complexity in orchestrating precise immune responses.
Author Contributions
D.N. Conceptualization, writing-original draft preparation, review and editing the final version.
Acknowledgments
The author is grateful to all members of the lab and collaborators who participated throughout the years in the relevant research projects to this review.
Conflicts of Interest
The author declares no conflict of interest.
References
- Aggarwal, B. B. (2003). Signalling pathways of the TNF superfamily: a double-edged sword. Nat Rev Immunol, 3(9), 745-756. [CrossRef]
- Alvarez, F., Istomine, R., Da Silva Lira Filho, A., Al-Aubodah, T. A., Huang, D., Okde, R., Olivier, M., Fritz, J. H., & Piccirillo, C. A. (2023). IL-18 is required for the T(H)1-adaptation of T(REG) cells and the selective suppression of T(H)17 responses in acute and chronic infections. Mucosal Immunol, 16(4), 462-475. [CrossRef]
- Bachmann, M., Pfeilschifter, J., & Mühl, H. (2018). A Prominent Role of Interleukin-18 in Acetaminophen-Induced Liver Injury Advocates Its Blockage for Therapy of Hepatic Necroinflammation. Front Immunol, 9, 161. [CrossRef]
- Baggio, C., Bindoli, S., Guidea, I., Doria, A., Oliviero, F., & Sfriso, P. (2023). IL-18 in Autoinflammatory Diseases: Focus on Adult Onset Still Disease and Macrophages Activation Syndrome. Int J Mol Sci, 24(13). [CrossRef]
- Baud'huin, M., Duplomb, L., Teletchea, S., Lamoureux, F., Ruiz-Velasco, C., Maillasson, M., Redini, F., Heymann, M. F., & Heymann, D. (2013). Osteoprotegerin: multiple partners for multiple functions. Cytokine Growth Factor Rev, 24(5), 401-409. [CrossRef]
- Behrens, E. M. (2024). Cytokines in Cytokine Storm Syndrome. Adv Exp Med Biol, 1448, 173-183. [CrossRef]
- Belkaya, S., Michailidis, E., Korol, C. B., Kabbani, M., Cobat, A., Bastard, P., Lee, Y. S., Hernandez, N., Drutman, S., de Jong, Y. P., Vivier, E., Bruneau, J., Béziat, V., Boisson, B., Lorenzo-Diaz, L., Boucherit, S., Sebagh, M., Jacquemin, E., Emile, J. F., . . . Casanova, J. L. (2019). Inherited IL-18BP deficiency in human fulminant viral hepatitis. J Exp Med, 216(8), 1777-1790. [CrossRef]
- Bindoli, S., Baggio, C., Doria, A., & Sfriso, P. (2024). Adult-Onset Still's Disease (AOSD): Advances in Understanding Pathophysiology, Genetics and Emerging Treatment Options. Drugs, 84(3), 257-274. [CrossRef]
- Blanchard, F., Duplomb, L., Baud'huin, M., & Brounais, B. (2009). The dual role of IL-6-type cytokines on bone remodeling and bone tumors. Cytokine Growth Factor Rev, 20(1), 19-28. [CrossRef]
- Bosmann, M., & Ward, P. A. (2013). Modulation of inflammation by interleukin-27. J Leukoc Biol, 94(6), 1159-1165. [CrossRef]
- Canna, S. W., & Cron, R. Q. (2020). Highways to hell: Mechanism-based management of cytokine storm syndromes. J Allergy Clin Immunol, 146(5), 949-959. [CrossRef]
- Canna, S. W., & De Benedetti, F. (2024). The 4(th) NextGen therapies of SJIA and MAS, part 4: it is time for IL-18 based trials in systemic juvenile idiopathic arthritis? Pediatr Rheumatol Online J, 21(Suppl 1), 79. [CrossRef]
- Canna, S. W., de Jesus, A. A., Gouni, S., Brooks, S. R., Marrero, B., Liu, Y., DiMattia, M. A., Zaal, K. J., Sanchez, G. A., Kim, H., Chapelle, D., Plass, N., Huang, Y., Villarino, A. V., Biancotto, A., Fleisher, T. A., Duncan, J. A., O'Shea, J. J., Benseler, S., . . . Goldbach-Mansky, R. (2014). An activating NLRC4 inflammasome mutation causes autoinflammation with recurrent macrophage activation syndrome. Nat Genet, 46(10), 1140-1146. [CrossRef]
- Canna, S. W., Girard, C., Malle, L., de Jesus, A., Romberg, N., Kelsen, J., Surrey, L. F., Russo, P., Sleight, A., Schiffrin, E., Gabay, C., Goldbach-Mansky, R., & Behrens, E. M. (2017). Life-threatening NLRC4-associated hyperinflammation successfully treated with IL-18 inhibition. J Allergy Clin Immunol, 139(5), 1698-1701. [CrossRef]
- Canna, S. W., & Marsh, R. A. (2020). Pediatric hemophagocytic lymphohistiocytosis. Blood, 135(16), 1332-1343. [CrossRef]
- Canny, S. P., Stanaway, I. B., Holton, S. E., Mitchem, M., O'Rourke, A. R., Pribitzer, S., Baxter, S. K., Wurfel, M. M., Malhotra, U., Buckner, J. H., Bhatraju, P. K., Morrell, E. D., Speake, C., Mikacenic, C., & Hamerman, J. A. (2024). Identification of biomarkers for COVID-19 associated secondary hemophagocytic lymphohistiocytosis. bioRxiv. [CrossRef]
- Cecrdlova, E., Krupickova, L., Fialova, M., Novotny, M., Tichanek, F., Svachova, V., Mezerova, K., Viklicky, O., & Striz, I. (2024). Insights into IL-1 family cytokines in kidney allograft transplantation: IL-18BP and free IL-18 as emerging biomarkers. Cytokine, 180, 156660. [CrossRef]
- Chaudhry, H., Zhou, J., Zhong, Y., Ali, M. M., McGuire, F., Nagarkatti, P. S., & Nagarkatti, M. (2013). Role of cytokines as a double-edged sword in sepsis. In Vivo, 27(6), 669-684.
- Chen, Y. T., Jenq, C. C., Hsu, C. K., Yu, Y. C., Chang, C. H., Fan, P. C., Pan, H. C., Wu, I. W., Cherng, W. J., & Chen, Y. C. (2020). Acute kidney disease and acute kidney injury biomarkers in coronary care unit patients. BMC Nephrol, 21(1), 207. [CrossRef]
- Chmielewski, M., & Abken, H. (2017). CAR T Cells Releasing IL-18 Convert to T-Bet(high) FoxO1(low) Effectors that Exhibit Augmented Activity against Advanced Solid Tumors. Cell Rep, 21(11), 3205-3219. [CrossRef]
- Codarri Deak, L., Nicolini, V., Hashimoto, M., Karagianni, M., Schwalie, P. C., Lauener, L., Varypataki, E. M., Richard, M., Bommer, E., Sam, J., Joller, S., Perro, M., Cremasco, F., Kunz, L., Yanguez, E., Hüsser, T., Schlenker, R., Mariani, M., Tosevski, V., . . . Umaña, P. (2022). PD-1-cis IL-2R agonism yields better effectors from stem-like CD8(+) T cells. Nature, 610(7930), 161-172. [CrossRef]
- Coll, R. C., & Schroder, K. (2024). Inflammasome components as new therapeutic targets in inflammatory disease. Nat Rev Immunol. [CrossRef]
- Cui, A., Huang, T., Li, S., Ma, A., Pérez, J. L., Sander, C., Keskin, D. B., Wu, C. J., Fraenkel, E., & Hacohen, N. (2024). Dictionary of immune responses to cytokines at single-cell resolution. Nature, 625(7994), 377-384. [CrossRef]
- de Zoete, M. R., Palm, N. W., Zhu, S., & Flavell, R. A. (2014). Inflammasomes. Cold Spring Harb Perspect Biol, 6(12), a016287. [CrossRef]
- Diorio, C., Shraim, R., Myers, R., Behrens, E. M., Canna, S., Bassiri, H., Aplenc, R., Burudpakdee, C., Chen, F., DiNofia, A. M., Gill, S., Gonzalez, V., Lambert, M. P., Leahy, A. B., Levine, B. L., Lindell, R. B., Maude, S. L., Melenhorst, J. J., Newman, H., . . . Teachey, D. T. (2022). Comprehensive Serum Proteome Profiling of Cytokine Release Syndrome and Immune Effector Cell-Associated Neurotoxicity Syndrome Patients with B-Cell ALL Receiving CAR T19. Clin Cancer Res, 28(17), 3804-3813. [CrossRef]
- Dong, Y., Bonin, J. P., Devant, P., Liang, Z., Sever, A. I. M., Mintseris, J., Aramini, J. M., Du, G., Gygi, S. P., Kagan, J. C., Kay, L. E., & Wu, H. (2024). Structural transitions enable interleukin-18 maturation and signaling. Immunity, 57(7), 1533-1548.e1510. [CrossRef]
- Dumoutier, L., Lejeune, D., Colau, D., & Renauld, J. C. (2001). Cloning and characterization of IL-22 binding protein, a natural antagonist of IL-10-related T cell-derived inducible factor/IL-22. J Immunol, 166(12), 7090-7095. [CrossRef]
- Edman, P. (1949). A method for the determination of amino acid sequence in peptides. Arch Biochem, 22(3), 475.
- Efthimiou, P., Kontzias, A., Hur, P., Rodha, K., Ramakrishna, G. S., & Nakasato, P. (2021). Adult-onset Still's disease in focus: Clinical manifestations, diagnosis, treatment, and unmet needs in the era of targeted therapies. Semin Arthritis Rheum, 51(4), 858-874. [CrossRef]
- Elson, G. C., Graber, P., Losberger, C., Herren, S., Gretener, D., Menoud, L. N., Wells, T. N., Kosco-Vilbois, M. H., & Gauchat, J. F. (1998). Cytokine-like factor-1, a novel soluble protein, shares homology with members of the cytokine type I receptor family. J Immunol, 161(3), 1371-1379.
- Engelmann, H., Novick, D., & Wallach, D. (1990). Two tumor necrosis factor-binding proteins purified from human urine. Evidence for immunological cross-reactivity with cell surface tumor necrosis factor receptors. J Biol Chem, 265(3), 1531-1536.
- Etna, M. P., Giacomini, E., Severa, M., & Coccia, E. M. (2014). Pro- and anti-inflammatory cytokines in tuberculosis: a two-edged sword in TB pathogenesis. Semin Immunol, 26(6), 543-551. [CrossRef]
- Fabbi, M., Carbotti, G., & Ferrini, S. (2015). Context-dependent role of IL-18 in cancer biology and counter-regulation by IL-18BP. J Leukoc Biol, 97(4), 665-675. [CrossRef]
- Fauteux-Daniel, S., Girard-Guyonvarc'h, C., Caruso, A., Rodriguez, E., & Gabay, C. (2023). Detection of Free Bioactive IL-18 and IL-18BP in Inflammatory Disorders. Methods Mol Biol, 2691, 263-277. [CrossRef]
- Fischer-Riepe, L., Kailayangiri, S., Zimmermann, K., Pfeifer, R., Aigner, M., Altvater, B., Kretschmann, S., Völkl, S., Hartley, J., Dreger, C., Petry, K., Bosio, A., von Döllen, A., Hartmann, W., Lode, H., Görlich, D., Mackensen, A., Jungblut, M., Schambach, A., . . . Rossig, C. (2024). Preclinical Development of CAR T Cells with Antigen-Inducible IL18 Enforcement to Treat GD2-Positive Solid Cancers. Clin Cancer Res, 30(16), 3564-3577. [CrossRef]
- Fraser, D. D., Cepinskas, G., Slessarev, M., Martin, C., Daley, M., Miller, M. R., O'Gorman, D. B., Gill, S. E., Patterson, E. K., & Dos Santos, C. C. (2020). Inflammation Profiling of Critically Ill Coronavirus Disease 2019 Patients. Crit Care Explor, 2(6), e0144. [CrossRef]
- Freeman, C., A, S. M., & A, S. P. (2024). Unraveling the Intricacies of OPG/RANKL/RANK Biology and Its Implications in Neurological Disorders-A Comprehensive Literature Review. Mol Neurobiol. [CrossRef]
- Gabay, C., Fautrel, B., Rech, J., Spertini, F., Feist, E., Kötter, I., Hachulla, E., Morel, J., Schaeverbeke, T., Hamidou, M. A., Martin, T., Hellmich, B., Lamprecht, P., Schulze-Koops, H., Courvoisier, D. S., Sleight, A., & Schiffrin, E. J. (2018). Open-label, multicentre, dose-escalating phase II clinical trial on the safety and efficacy of tadekinig alfa (IL-18BP) in adult-onset Still's disease. Ann Rheum Dis, 77(6), 840-847. [CrossRef]
- Galozzi, P., Bindoli, S., Doria, A., & Sfriso, P. (2022). Progress in Biological Therapies for Adult-Onset Still's Disease. Biologics, 16, 21-34. [CrossRef]
- Geerlinks, A. V., & Dvorak, A. M. (2022). A Case of XIAP Deficiency Successfully Managed with Tadekinig Alfa (rhIL-18BP). J Clin Immunol, 42(4), 901-903. [CrossRef]
- Giacomelli, R., Ruscitti, P., & Shoenfeld, Y. (2018). A comprehensive review on adult onset Still's disease. J Autoimmun, 93, 24-36. [CrossRef]
- Girard, C., Rech, J., Brown, M., Allali, D., Roux-Lombard, P., Spertini, F., Schiffrin, E. J., Schett, G., Manger, B., Bas, S., Del Val, G., & Gabay, C. (2016). Elevated serum levels of free interleukin-18 in adult-onset Still's disease. Rheumatology (Oxford), 55(12), 2237-2247. [CrossRef]
- Girard-Guyonvarc'h, C., Palomo, J., Martin, P., Rodriguez, E., Troccaz, S., Palmer, G., & Gabay, C. (2018). Unopposed IL-18 signaling leads to severe TLR9-induced macrophage activation syndrome in mice. Blood, 131(13), 1430-1441. [CrossRef]
- Glienke, W., Dragon, A. C., Zimmermann, K., Martyniszyn-Eiben, A., Mertens, M., Abken, H., Rossig, C., Altvater, B., Aleksandrova, K., Arseniev, L., Kloth, C., Stamopoulou, A., Moritz, T., Lode, H. N., Siebert, N., Blasczyk, R., Goudeva, L., Schambach, A., Köhl, U., . . . Esser, R. (2022). GMP-Compliant Manufacturing of TRUCKs: CAR T Cells targeting GD(2) and Releasing Inducible IL-18. Front Immunol, 13, 839783. [CrossRef]
- Guha, A., Diaz-Pino, R., Fagbemi, A., Hughes, S. M., Wynn, R. F., Lopez-Castejon, G., & Arkwright, P. D. (2024). Very Early-Onset IBD-Associated IL-18opathy Treated with an Anti-IL-18 Antibody. J Clin Med, 13(20). [CrossRef]
- Hakim, A. D., Awili, M., O'Neal, H. R., Siddiqi, O., Jaffrani, N., Lee, R., Overcash, J. S., Chauffe, A., Hammond, T. C., Patel, B., Waters, M., Criner, G. J., Pachori, A., Junge, G., Levitch, R., Watts, J., Koo, P., Sengupta, T., Yu, L., . . . Matthews, J. (2023). Efficacy and safety of MAS825 (anti-IL-1β/IL-18) in COVID-19 patients with pneumonia and impaired respiratory function. Clin Exp Immunol, 213(3), 265-275. [CrossRef]
- Hand, T. W. (2015). Interleukin-18: The Bouncer at the Mucosal Bar. Cell, 163(6), 1310-1312. [CrossRef]
- Harms, R. Z., Creer, A. J., Lorenzo-Arteaga, K. M., Ostlund, K. R., & Sarvetnick, N. E. (2017). Interleukin (IL)-18 Binding Protein Deficiency Disrupts Natural Killer Cell Maturation and Diminishes Circulating IL-18. Front Immunol, 8, 1020. [CrossRef]
- He, Z., Lu, L., Altmann, C., Hoke, T. S., Ljubanovic, D., Jani, A., Dinarello, C. A., Faubel, S., & Edelstein, C. L. (2008). Interleukin-18 binding protein transgenic mice are protected against ischemic acute kidney injury. Am J Physiol Renal Physiol, 295(5), F1414-1421. [CrossRef]
- Higuchi, T., Izawa, K., Miyamoto, T., Honda, Y., Nishiyama, A., Shimizu, M., Takita, J., & Yasumi, T. (2022). An efficient diagnosis: A patient with X-linked inhibitor of apoptosis protein (XIAP) deficiency in the setting of infantile hemophagocytic lymphohistiocytosis was diagnosed using high serum interleukin-18 combined with common laboratory parameters. Pediatr Blood Cancer, 69(8), e29606. [CrossRef]
- Hoshino, K., Tsutsui, H., Kawai, T., Takeda, K., Nakanishi, K., Takeda, Y., & Akira, S. (1999). Cutting edge: generation of IL-18 receptor-deficient mice: evidence for IL-1 receptor-related protein as an essential IL-18 binding receptor. J Immunol, 162(9), 5041-5044.
- Hu, B., Ren, J., Luo, Y., Keith, B., Young, R. M., Scholler, J., Zhao, Y., & June, C. H. (2017). Augmentation of Antitumor Immunity by Human and Mouse CAR T Cells Secreting IL-18. Cell Rep, 20(13), 3025-3033. [CrossRef]
- Hurgin, V., Novick, D., & Rubinstein, M. (2002). The promoter of IL-18 binding protein: activation by an IFN-gamma -induced complex of IFN regulatory factor 1 and CCAAT/enhancer binding protein beta. Proc Natl Acad Sci U S A, 99(26), 16957-16962. [CrossRef]
- Ihim, S. A., Abubakar, S. D., Zian, Z., Sasaki, T., Saffarioun, M., Maleknia, S., & Azizi, G. (2022). Interleukin-18 cytokine in immunity, inflammation, and autoimmunity: Biological role in induction, regulation, and treatment. Front Immunol, 13, 919973. [CrossRef]
- Jang, Y. S., Lee, K., Park, M., Joo Park, J., Choi, G. M., Kim, C., Dehkohneh, S. B., Chi, S., Han, J., Song, M. Y., Han, Y. H., Cha, S. H., & Goo Kang, S. (2023). Albumin-binding recombinant human IL-18BP ameliorates macrophage activation syndrome and atopic dermatitis via direct IL-18 inactivation. Cytokine, 172, 156413. [CrossRef]
- Janho Dit Hreich, S., Humbert, O., Pacé-Loscos, T., Schiappa, R., Juhel, T., Ilié, M., Ferrari, V., Benzaquen, J., Hofman, P., & Vouret-Craviari, V. (2024). Plasmatic Inactive IL-18 Predicts a Worse Overall Survival for Advanced Non-Small-Cell Lung Cancer with Early Metabolic Progression after Immunotherapy Initiation. Cancers (Basel), 16(12). [CrossRef]
- Jarret, A., Jackson, R., Duizer, C., Healy, M. E., Zhao, J., Rone, J. M., Bielecki, P., Sefik, E., Roulis, M., Rice, T., Sivanathan, K. N., Zhou, T., Solis, A. G., Honcharova-Biletska, H., Vélez, K., Hartner, S., Low, J. S., Qu, R., de Zoete, M. R., . . . Flavell, R. A. (2020). Enteric Nervous System-Derived IL-18 Orchestrates Mucosal Barrier Immunity. Cell, 180(1), 50-63.e12. [CrossRef]
- Jun, H. T., Deborah A. Witherden, D. A., Elliot, E. K., Chidester, C. M., Willen, M., Peguero, B. R., Chai, M., Horlick, R. A. and King, D. J. (2023). Discovery and evaluation of an anti-IL18BP antibody to enhance anti-tumor immunity. Cancer Res 83. [CrossRef]
- .
- Kaplanski, G. (2018). Interleukin-18: Biological properties and role in disease pathogenesis. Immunol Rev, 281(1), 138-153. [CrossRef]
- Kaser, A., Novick, D., Rubinstein, M., Siegmund, B., Enrich, B., Koch, R. O., Vogel, W., Kim, S. H., Dinarello, C. A., & Tilg, H. (2002). Interferon-alpha induces interleukin-18 binding protein in chronic hepatitis C patients. Clin Exp Immunol, 129(2), 332-338. [CrossRef]
- Kass, D. J. (2011). Cytokine-like factor 1 (CLF1): life after development? Cytokine, 55(3), 325-329. [CrossRef]
- Kiltz, U., Kiefer, D., Braun, J., Schiffrin, E. J., Girard-Guyonvarc'h, C., & Gabay, C. (2020). Prolonged treatment with Tadekinig alfa in adult-onset Still's disease. Ann Rheum Dis, 79(1), e10. [CrossRef]
- Kim, S. H., Eisenstein, M., Reznikov, L., Fantuzzi, G., Novick, D., Rubinstein, M., & Dinarello, C. A. (2000). Structural requirements of six naturally occurring isoforms of the IL-18 binding protein to inhibit IL-18. Proc Natl Acad Sci U S A, 97(3), 1190-1195. [CrossRef]
- Konishi, H., Tsutsui, H., Murakami, T., Yumikura-Futatsugi, S., Yamanaka, K., Tanaka, M., Iwakura, Y., Suzuki, N., Takeda, K., Akira, S., Nakanishi, K., & Mizutani, H. (2002). IL-18 contributes to the spontaneous development of atopic dermatitis-like inflammatory skin lesion independently of IgE/stat6 under specific pathogen-free conditions. Proc Natl Acad Sci U S A, 99(17), 11340-11345. [CrossRef]
- Korotaeva, A. A., Samoilova, E. V., Pogosova, N. V., Fesenko, A. G., Evchenko, S. V., & Paleev, F. N. (2024). Ratios between the Levels of IL-18, Free IL-18, and IL-1β-Binding Protein Depending on the Severity and Outcome of COVID-19. Bull Exp Biol Med, 176(4), 423-427. [CrossRef]
- Krei, J. M., Møller, H. J., & Larsen, J. B. (2021). The role of interleukin-18 in the diagnosis and monitoring of hemophagocytic lymphohistiocytosis/macrophage activation syndrome - a systematic review. Clin Exp Immunol, 203(2), 174-182. [CrossRef]
- Krishna, B. A., Lim, E. Y., Metaxaki, M., Jackson, S., Mactavous, L., Lyons, P. A., Doffinger, R., Bradley, J. R., Smith, K. G. C., Sinclair, J., Matheson, N. J., Lehner, P. J., Sithole, N., & Wills, M. R. (2024). Spontaneous, persistent, T cell-dependent IFN-γ release in patients who progress to Long Covid. Sci Adv, 10(8), eadi9379. [CrossRef]
- Kudela, H., Drynda, S., Lux, A., Horneff, G., & Kekow, J. (2019). Comparative study of Interleukin-18 (IL-18) serum levels in adult onset Still's disease (AOSD) and systemic onset juvenile idiopathic arthritis (sJIA) and its use as a biomarker for diagnosis and evaluation of disease activity. BMC Rheumatol, 3, 4. [CrossRef]
- Lage, S. L., Ramaswami, R., Rocco, J. M., Rupert, A., Davis, D. A., Lurain, K., Manion, M., Whitby, D., Yarchoan, R., & Sereti, I. (2024). Inflammasome activation in patients with Kaposi sarcoma herpesvirus-associated diseases. Blood, 144(14), 1496-1507. [CrossRef]
- Landy, E., Carol, H., Ring, A., & Canna, S. (2024). Biological and clinical roles of IL-18 in inflammatory diseases. Nat Rev Rheumatol, 20(1), 33-47. [CrossRef]
- Levy, M., Thaiss, C. A., Zeevi, D., Dohnalová, L., Zilberman-Schapira, G., Mahdi, J. A., David, E., Savidor, A., Korem, T., Herzig, Y., Pevsner-Fischer, M., Shapiro, H., Christ, A., Harmelin, A., Halpern, Z., Latz, E., Flavell, R. A., Amit, I., Segal, E., & Elinav, E. (2015). Microbiota-Modulated Metabolites Shape the Intestinal Microenvironment by Regulating NLRP6 Inflammasome Signaling. Cell, 163(6), 1428-1443. [CrossRef]
- Li, C., Qian, W., Wei, X., Narasimhan, H., Wu, Y., Arish, M., Cheon, I. S., Tang, J., de Almeida Santos, G., Li, Y., Sharifi, K., Kern, R., Vassallo, R., & Sun, J. (2024). Comparative single-cell analysis reveals IFN-γ as a driver of respiratory sequelae after acute COVID-19. Sci Transl Med, 16(756), eadn0136. [CrossRef]
- Lichtenstein, D. A., Schischlik, F., Shao, L., Steinberg, S. M., Yates, B., Wang, H. W., Wang, Y., Inglefield, J., Dulau-Florea, A., Ceppi, F., Hermida, L. C., Stringaris, K., Dunham, K., Homan, P., Jailwala, P., Mirazee, J., Robinson, W., Chisholm, K. M., Yuan, C., . . . Shah, N. N. (2021). Characterization of HLH-like manifestations as a CRS variant in patients receiving CD22 CAR T cells. Blood, 138(24), 2469-2484. [CrossRef]
- Lipinski, B., Unmuth, L., Arras, P., Becker, S., Bauer, C., Toleikis, L., Krah, S., Doerner, A., Yanakieva, D., Boje, A. S., Klausz, K., Peipp, M., Siegmund, V., Evers, A., Kolmar, H., Pekar, L., & Zielonka, S. (2023). Generation and engineering of potent single domain antibody-based bispecific IL-18 mimetics resistant to IL-18BP decoy receptor inhibition. MAbs, 15(1), 2236265. [CrossRef]
- Manzo Margiotta, F., Gambino, G., Pratesi, F., Michelucci, A., Pisani, F., Rossi, L., Dini, V., Romanelli, M., & Migliorini, P. (2024). Interleukin-1 family cytokines and soluble receptors in hidradenitis suppurativa. Exp Dermatol, 33(9), e15179. [CrossRef]
- Marx, J. L. (1988). Cytokines are two-edged swords in disease. Science, 239(4837), 257-258. [CrossRef]
- Mazodier, K., Marin, V., Novick, D., Farnarier, C., Robitail, S., Schleinitz, N., Veit, V., Paul, P., Rubinstein, M., Dinarello, C. A., Harlé, J. R., & Kaplanski, G. (2005). Severe imbalance of IL-18/IL-18BP in patients with secondary hemophagocytic syndrome. Blood, 106(10), 3483-3489. [CrossRef]
- Mehta, P., Samanta, R. J., Wick, K., Coll, R. C., Mawhinney, T., McAleavey, P. G., Boyle, A. J., Conlon, J., Shankar-Hari, M., Rogers, A., Calfee, C. S., Matthay, M. A., Summers, C., Chambers, R. C., McAuley, D. F., & O'Kane, C. M. (2024). Elevated ferritin, mediated by IL-18 is associated with systemic inflammation and mortality in acute respiratory distress syndrome (ARDS). Thorax, 79(3), 227-235. [CrossRef]
- Menachem, A., Alteber, Z., Cojocaru, G., Fridman Kfir, T., Blat, D., Leiderman, O., Galperin, M., Sever, L., Cohen, N., Cohen, K., Granit, R. Z., Vols, S., Frenkel, M., Soffer, L., Meyer, K., Menachem, K., Galon Tilleman, H., Morein, D., Borukhov, I., . . . Ophir, E. (2024). Unleashing Natural IL18 Activity Using an Anti-IL18BP Blocker Induces Potent Immune Stimulation and Antitumor Effects. Cancer Immunol Res, 12(6), 687-703. [CrossRef]
- Mertens, R. T., Misra, A., Xiao, P., Baek, S., Rone, J. M., Mangani, D., Sivanathan, K. N., Arojojoye, A. S., Awuah, S. G., Lee, I., Shi, G. P., Petrova, B., Brook, J. R., Anderson, A. C., Flavell, R. A., Kanarek, N., Hemberg, M., & Nowarski, R. (2024). A metabolic switch orchestrated by IL-18 and the cyclic dinucleotide cGAMP programs intestinal tolerance. Immunity, 57(9), 2077-2094.e2012. [CrossRef]
- Monteleone, G., Pallone, F., & Macdonald, T. T. (2010). Interleukin-25: a two-edged sword in the control of immune-inflammatory responses. Cytokine Growth Factor Rev, 21(6), 471-475. [CrossRef]
- Moore, A. R., Pienkos, S. M., Sinha, P., Guan, J., O'Kane, C. M., Levitt, J. E., Wilson, J. G., Shankar-Hari, M., Matthay, M. A., Calfee, C. S., Baron, R. M., McAuley, D. F., & Rogers, A. J. (2023). Elevated Plasma Interleukin-18 Identifies High-Risk Acute Respiratory Distress Syndrome Patients not Distinguished by Prior Latent Class Analyses Using Traditional Inflammatory Cytokines: A Retrospective Analysis of Two Randomized Clinical Trials. Crit Care Med, 51(12), e269-e274. [CrossRef]
- Morris, K. R., Brodkin, H., Economides, K., Hicklin, D. J., LePrevost, J., Nagy-Domonkos, C., Nirschl, C., Salmeron, A., Seidel-Dugan, C., Spencer, C., Steuert, Z. and William M. Winston, W. M. (2024). Discovery of WTX-518, an IL-18 pro-drug that is conditionally activated within the tumor microenvironment and induces regressions in mouse tumor models. Cancer Res 84. [CrossRef]
- Mühl, H., & Bachmann, M. (2019). IL-18/IL-18BP and IL-22/IL-22BP: Two interrelated couples with therapeutic potential. Cell Signal, 63, 109388. [CrossRef]
- Mühl, H., Kämpfer, H., Bosmann, M., Frank, S., Radeke, H., & Pfeilschifter, J. (2000). Interferon-gamma mediates gene expression of IL-18 binding protein in nonleukocytic cells. Biochem Biophys Res Commun, 267(3), 960-963. [CrossRef]
- Nakamura, K., Okamura, H., Wada, M., Nagata, K., & Tamura, T. (1989). Endotoxin-induced serum factor that stimulates gamma interferon production. Infect Immun, 57(2), 590-595. [CrossRef]
- Nakamura, S., Otani, T., Okura, R., Ijiri, Y., Motoda, R., Kurimoto, M., & Orita, K. (2000). Expression and responsiveness of human interleukin-18 receptor (IL-18R) on hematopoietic cell lines. Leukemia, 14(6), 1052-1059. [CrossRef]
- Nakanishi, K., Yoshimoto, T., Tsutsui, H., & Okamura, H. (2001). Interleukin-18 is a unique cytokine that stimulates both Th1 and Th2 responses depending on its cytokine milieu. Cytokine Growth Factor Rev, 12(1), 53-72. [CrossRef]
- Nasser, S. M. T., Rana, A. A., Doffinger, R., Kafizas, A., Khan, T. A., & Nasser, S. (2023). Elevated free interleukin-18 associated with severity and mortality in prospective cohort study of 206 hospitalised COVID-19 patients. Intensive Care Med Exp, 11(1), 9. [CrossRef]
- Netea, M. G., Joosten, L. A., Lewis, E., Jensen, D. R., Voshol, P. J., Kullberg, B. J., Tack, C. J., van Krieken, H., Kim, S. H., Stalenhoef, A. F., van de Loo, F. A., Verschueren, I., Pulawa, L., Akira, S., Eckel, R. H., Dinarello, C. A., van den Berg, W., & van der Meer, J. W. (2006). Deficiency of interleukin-18 in mice leads to hyperphagia, obesity and insulin resistance. Nat Med, 12(6), 650-656. [CrossRef]
- Nisthal, A., Lee, S., Bonzon, C., Love, R., Avery, K., Rashid, R., Lertkiatmongkol, P., Rodriguez, N., Karki ,S., Barlow, N., Chu, S., Moore, G. and Desjarlais, J. . (2022). XmAb143, an engineered IL18 heterodimeric Fc-fusion, features improved stability, reduced potency, and insensitivity to IL18BP. Journal for ImmunoTherapy of Cancer. [CrossRef]
- Novick, D. (2022). Nine receptors and binding proteins, four drugs, and one woman: Historical and personal perspectives. Front Drug Discovery. [CrossRef]
- Novick, D. (2023). A natural goldmine of binding proteins and soluble receptors simplified their translation to blockbuster drugs, all in one decade. Front Immunol, 14, 1151620. [CrossRef]
- Novick, D., Kim, S., Kaplanski, G., & Dinarello, C. A. (2013). Interleukin-18, more than a Th1 cytokine. Semin Immunol, 25(6), 439-448. [CrossRef]
- Novick, D., Kim, S. H., Fantuzzi, G., Reznikov, L. L., Dinarello, C. A., & Rubinstein, M. (1999). Interleukin-18 binding protein: a novel modulator of the Th1 cytokine response. Immunity, 10(1), 127-136. [CrossRef]
- Novick, D., & Rubinstein, M. (2007). The tale of soluble receptors and binding proteins: from bench to bedside. Cytokine Growth Factor Rev, 18(5-6), 525-533. [CrossRef]
- Novick, D., Schwartsburd, B., Pinkus, R., Suissa, D., Belzer, I., Sthoeger, Z., Keane, W. F., Chvatchko, Y., Kim, S. H., Fantuzzi, G., Dinarello, C. A., & Rubinstein, M. (2001). A novel IL-18BP ELISA shows elevated serum IL-18BP in sepsis and extensive decrease of free IL-18. Cytokine, 14(6), 334-342. [CrossRef]
- Nowarski, R., Jackson, R., Gagliani, N., de Zoete, M. R., Palm, N. W., Bailis, W., Low, J. S., Harman, C. C., Graham, M., Elinav, E., & Flavell, R. A. (2015). Epithelial IL-18 Equilibrium Controls Barrier Function in Colitis. Cell, 163(6), 1444-1456. [CrossRef]
- Parikh, C. R., Abraham, E., Ancukiewicz, M., & Edelstein, C. L. (2005). Urine IL-18 is an early diagnostic marker for acute kidney injury and predicts mortality in the intensive care unit. J Am Soc Nephrol, 16(10), 3046-3052. [CrossRef]
- Peleman, C., Van Coillie, S., Ligthart, S., Choi, S. M., De Waele, J., Depuydt, P., Benoit, D., Schaubroeck, H., Francque, S. M., Dams, K., Jacobs, R., Robert, D., Roelandt, R., Seurinck, R., Saeys, Y., Rajapurkar, M., Jorens, P. G., Hoste, E., & Vanden Berghe, T. (2023). Ferroptosis and pyroptosis signatures in critical COVID-19 patients. Cell Death Differ, 30(9), 2066-2077. [CrossRef]
- Posey, A. D., Jr., Young, R. M., & June, C. H. (2024). Future perspectives on engineered T cells for cancer. Trends Cancer, 10(8), 687-695. [CrossRef]
- Rafiq, S., Hackett, C. S., & Brentjens, R. J. (2020). Engineering strategies to overcome the current roadblocks in CAR T cell therapy. Nat Rev Clin Oncol, 17(3), 147-167. [CrossRef]
- Rex, D. A. B., Agarwal, N., Prasad, T. S. K., Kandasamy, R. K., Subbannayya, Y., & Pinto, S. M. (2020). A comprehensive pathway map of IL-18-mediated signalling. J Cell Commun Signal, 14(2), 257-266. [CrossRef]
- Robertson, M. J., Kirkwood, J. M., Logan, T. F., Koch, K. M., Kathman, S., Kirby, L. C., Bell, W. N., Thurmond, L. M., Weisenbach, J., & Dar, M. M. (2008). A dose-escalation study of recombinant human interleukin-18 using two different schedules of administration in patients with cancer. Clin Cancer Res, 14(11), 3462-3469. [CrossRef]
- Romberg, N., Al Moussawi, K., Nelson-Williams, C., Stiegler, A. L., Loring, E., Choi, M., Overton, J., Meffre, E., Khokha, M. K., Huttner, A. J., West, B., Podoltsev, N. A., Boggon, T. J., Kazmierczak, B. I., & Lifton, R. P. (2014). Mutation of NLRC4 causes a syndrome of enterocolitis and autoinflammation. Nat Genet, 46(10), 1135-1139. [CrossRef]
- Romberg, N., Vogel, T. P., & Canna, S. W. (2017). NLRC4 inflammasomopathies. Curr Opin Allergy Clin Immunol, 17(6), 398-404. [CrossRef]
- Rusiñol, L., & Puig, L. (2024). A Narrative Review of the IL-18 and IL-37 Implications in the Pathogenesis of Atopic Dermatitis and Psoriasis: Prospective Treatment Targets. Int J Mol Sci, 25(15). [CrossRef]
- Sareneva, T., Julkunen, I., & Matikainen, S. (2000). IFN-alpha and IL-12 induce IL-18 receptor gene expression in human NK and T cells. J Immunol, 165(4), 1933-1938. [CrossRef]
- Schroder, K., & Tschopp, J. (2010). The inflammasomes. Cell, 140(6), 821-832. [CrossRef]
- Sefik, E., Qu, R., Junqueira, C., Kaffe, E., Mirza, H., Zhao, J., Brewer, J. R., Han, A., Steach, H. R., Israelow, B., Blackburn, H. N., Velazquez, S. E., Chen, Y. G., Halene, S., Iwasaki, A., Meffre, E., Nussenzweig, M., Lieberman, J., Wilen, C. B., . . . Flavell, R. A. (2022). Inflammasome activation in infected macrophages drives COVID-19 pathology. Nature, 606(7914), 585-593. [CrossRef]
- Shimizu, M. (2021). Macrophage activation syndrome in systemic juvenile idiopathic arthritis. Immunol Med, 44(4), 237-245. [CrossRef]
- Shimizu, M., Inoue, N., Mizuta, M., Nakagishi, Y., & Yachie, A. (2018). Characteristic elevation of soluble TNF receptor II : I ratio in macrophage activation syndrome with systemic juvenile idiopathic arthritis. Clin Exp Immunol, 191(3), 349-355. [CrossRef]
- Shimizu, M., Takei, S., Mori, M., & Yachie, A. (2022). Pathogenic roles and diagnostic utility of interleukin-18 in autoinflammatory diseases. Front Immunol, 13, 951535. [CrossRef]
- Simonet, W. S., Lacey, D. L., Dunstan, C. R., Kelley, M., Chang, M. S., Lüthy, R., Nguyen, H. Q., Wooden, S., Bennett, L., Boone, T., Shimamoto, G., DeRose, M., Elliott, R., Colombero, A., Tan, H. L., Trail, G., Sullivan, J., Davy, E., Bucay, N., . . . Boyle, W. J. (1997). Osteoprotegerin: a novel secreted protein involved in the regulation of bone density. Cell, 89(2), 309-319. [CrossRef]
- Smith, V. P., Bryant, N. A., & Alcamí, A. (2000). Ectromelia, vaccinia and cowpox viruses encode secreted interleukin-18-binding proteins. J Gen Virol, 81(Pt 5), 1223-1230. [CrossRef]
- Snell, L. M., McGaha, T. L., & Brooks, D. G. (2017). Type I Interferon in Chronic Virus Infection and Cancer. Trends Immunol, 38(8), 542-557. [CrossRef]
- Steinman, L. (2007). A brief history of T(H)17, the first major revision in the T(H)1/T(H)2 hypothesis of T cell-mediated tissue damage. Nat Med, 13(2), 139-145. [CrossRef]
- Svoboda, J., Gerson, J. N., Landsburg, D. J., Chong, E. A., Barta, S. K., Nasta, S.D., Ruella, M.,Hexner, E. O., Marshall, A. et al. and June, C. H. (2022). Interleukin-18 Secreting Autologous Anti-CD19 CAR T-Cells (huCART19-IL18) in Patients with Non-Hodgkin Lymphomas Relapsed or Refractory to Prior CAR T-Cell Therapy. Blood, 140, 4612-4614. [CrossRef]
- Svoboda, J., Landsburg, D. J., Dwivedy Nasta, S. D., Barta, S. K., Chong, E. A., Lariviere, M. J., Shea, J., Cervini, S., Hexner, E. O., Marshall, A., et al. and June, C. H. . (2024). Safety and efficacy of armored huCART19-IL18 in patients with relapsed/refractory lymphomas that progressed after anti-CD19 CAR T cells. Journal of Clinical Oncology 42. [CrossRef]
- Tak, P. P., Bacchi, M., & Bertolino, M. (2006). Pharmacokinetics of IL-18 binding protein in healthy volunteers and subjects with rheumatoid arthritis or plaque psoriasis. Eur J Drug Metab Pharmacokinet, 31(2), 109-116. [CrossRef]
- Tsutsumi, N., Kimura, T., Arita, K., Ariyoshi, M., Ohnishi, H., Yamamoto, T., Zuo, X., Maenaka, K., Park, E. Y., Kondo, N., Shirakawa, M., Tochio, H., & Kato, Z. (2014). The structural basis for receptor recognition of human interleukin-18. Nat Commun, 5, 5340. [CrossRef]
- Uslu, U., Sun, L., Castelli, S., Finck, A. V., Assenmacher, C. A., Young, R. M., Chen, Z. J., & June, C. H. (2024). The STING agonist IMSA101 enhances chimeric antigen receptor T cell function by inducing IL-18 secretion. Nat Commun, 15(1), 3933. [CrossRef]
- Volfovitch, Y., Tsur, A. M., Gurevitch, M., Novick, D., Rabinowitz, R., Mandel, M., Achiron, A., Rubinstein, M., Shoenfeld, Y., & Amital, H. (2022). The intercorrelations between blood levels of ferritin, sCD163, and IL-18 in COVID-19 patients and their association to prognosis. Immunol Res, 70(6), 817-828. [CrossRef]
- Wada, T., Kanegane, H., Ohta, K., Katoh, F., Imamura, T., Nakazawa, Y., Miyashita, R., Hara, J., Hamamoto, K., Yang, X., Filipovich, A. H., Marsh, R. A., & Yachie, A. (2014). Sustained elevation of serum interleukin-18 and its association with hemophagocytic lymphohistiocytosis in XIAP deficiency. Cytokine, 65(1), 74-78. [CrossRef]
- Wang, F. (2024). Interleukin-18 binding protein: Biological properties and roles in human and animal immune regulation (Review). Biomed Rep, 20(6), 87. [CrossRef]
- Wang, X., Wang, L., Wen, X., Zhang, L., Jiang, X., & He, G. (2023). Interleukin-18 and IL-18BP in inflammatory dermatological diseases. Front Immunol, 14, 955369. [CrossRef]
- Washburn, K. K., Zappitelli, M., Arikan, A. A., Loftis, L., Yalavarthy, R., Parikh, C. R., Edelstein, C. L., & Goldstein, S. L. (2008). Urinary interleukin-18 is an acute kidney injury biomarker in critically ill children. Nephrol Dial Transplant, 23(2), 566-572. [CrossRef]
- Weiss, E. S., Girard-Guyonvarc'h, C., Holzinger, D., de Jesus, A. A., Tariq, Z., Picarsic, J., Schiffrin, E. J., Foell, D., Grom, A. A., Ammann, S., Ehl, S., Hoshino, T., Goldbach-Mansky, R., Gabay, C., & Canna, S. W. (2018). Interleukin-18 diagnostically distinguishes and pathogenically promotes human and murine macrophage activation syndrome. Blood, 131(13), 1442-1455. [CrossRef]
- Wu, C., Sakorafas, P., Miller, R., McCarthy, D., Scesney, S., Dixon, R., & Ghayur, T. (2003). IL-18 receptor beta-induced changes in the presentation of IL-18 binding sites affect ligand binding and signal transduction. J Immunol, 170(11), 5571-5577. [CrossRef]
- Wu, H., Craft, M. L., Wang, P., Wyburn, K. R., Chen, G., Ma, J., Hambly, B., & Chadban, S. J. (2008). IL-18 contributes to renal damage after ischemia-reperfusion. J Am Soc Nephrol, 19(12), 2331-2341. [CrossRef]
- Xia, S., Zhang, Z., Magupalli, V. G., Pablo, J. L., Dong, Y., Vora, S. M., Wang, L., Fu, T. M., Jacobson, M. P., Greka, A., Lieberman, J., Ruan, J., & Wu, H. (2021). Gasdermin D pore structure reveals preferential release of mature interleukin-1. Nature, 593(7860), 607-611. [CrossRef]
- Yamanishi, K., Hata, M., Gamachi, N., Watanabe, Y., Yamanishi, C., Okamura, H., & Matsunaga, H. (2023). Molecular Mechanisms of IL18 in Disease. Int J Mol Sci, 24(24). [CrossRef]
- Yasin, S., Fall, N., Brown, R. A., Henderlight, M., Canna, S. W., Girard-Guyonvarc'h, C., Gabay, C., Grom, A. A., & Schulert, G. S. (2020). IL-18 as a biomarker linking systemic juvenile idiopathic arthritis and macrophage activation syndrome. Rheumatology (Oxford), 59(2), 361-366. [CrossRef]
- Yasin, S., Solomon, K., Canna, S. W., Girard-Guyonvarc'h, C., Gabay, C., Schiffrin, E., Sleight, A., Grom, A. A., & Schulert, G. S. (2020). IL-18 as therapeutic target in a patient with resistant systemic juvenile idiopathic arthritis and recurrent macrophage activation syndrome. Rheumatology (Oxford), 59(2), 442-445. [CrossRef]
- Yasuda, K., Nakanishi, K., & Tsutsui, H. (2019). Interleukin-18 in Health and Disease. Int J Mol Sci, 20(3). [CrossRef]
- Yoshimoto, T., Takeda, K., Tanaka, T., Ohkusu, K., Kashiwamura, S., Okamura, H., Akira, S., & Nakanishi, K. (1998). IL-12 up-regulates IL-18 receptor expression on T cells, Th1 cells, and B cells: synergism with IL-18 for IFN-gamma production. J Immunol, 161(7), 3400-3407.
- Young, R. M., Engel, N. W., Uslu, U., Wellhausen, N., & June, C. H. (2022). Next-Generation CAR T-cell Therapies. Cancer Discov, 12(7), 1625-1633. [CrossRef]
- Yu, P., Zhang, X., Liu, N., Tang, L., Peng, C., & Chen, X. (2021). Pyroptosis: mechanisms and diseases. Signal Transduct Target Ther, 6(1), 128. [CrossRef]
- Zaidi, M. R., & Merlino, G. (2011). The two faces of interferon-γ in cancer. Clin Cancer Res, 17(19), 6118-6124. [CrossRef]
- Zenewicz, L. A. (2021). IL-22 Binding Protein (IL-22BP) in the Regulation of IL-22 Biology. Front Immunol, 12, 766586. [CrossRef]
- Zheng, D., Mohapatra, G., Kern, L., He, Y., Shmueli, M. D., Valdés-Mas, R., Kolodziejczyk, A. A., Próchnicki, T., Vasconcelos, M. B., Schorr, L., Hertel, F., Lee, Y. S., Rufino, M. C., Ceddaha, E., Shimshy, S., Hodgetts, R. J., Dori-Bachash, M., Kleimeyer, C., Goldenberg, K., . . . Elinav, E. (2023). Epithelial Nlrp10 inflammasome mediates protection against intestinal autoinflammation. Nat Immunol, 24(4), 585-594. [CrossRef]
- Zhou, T., Damsky, W., Weizman, O. E., McGeary, M. K., Hartmann, K. P., Rosen, C. E., Fischer, S., Jackson, R., Flavell, R. A., Wang, J., Sanmamed, M. F., Bosenberg, M. W., & Ring, A. M. (2020). IL-18BP is a secreted immune checkpoint and barrier to IL-18 immunotherapy. Nature, 583(7817), 609-614. [CrossRef]
Figure 1.
Isolation of IL-18BP: IL-18BP purified from concentrated human urinary proteins by ligand-affinity-chromatography on a column of IL-18 covalently bound to Sepharose beads and analyzed by SDS-PAGE and silver staining (Novick et al., 1999) . Lane 1: Crude urinary proteins. Lanes 2–9: Eight acidic elution fractions from the IL-18 column. Lane m: Molecular mass markers (kDa). The arrow indicates the IL-18 binding protein.
Figure 1.
Isolation of IL-18BP: IL-18BP purified from concentrated human urinary proteins by ligand-affinity-chromatography on a column of IL-18 covalently bound to Sepharose beads and analyzed by SDS-PAGE and silver staining (Novick et al., 1999) . Lane 1: Crude urinary proteins. Lanes 2–9: Eight acidic elution fractions from the IL-18 column. Lane m: Molecular mass markers (kDa). The arrow indicates the IL-18 binding protein.
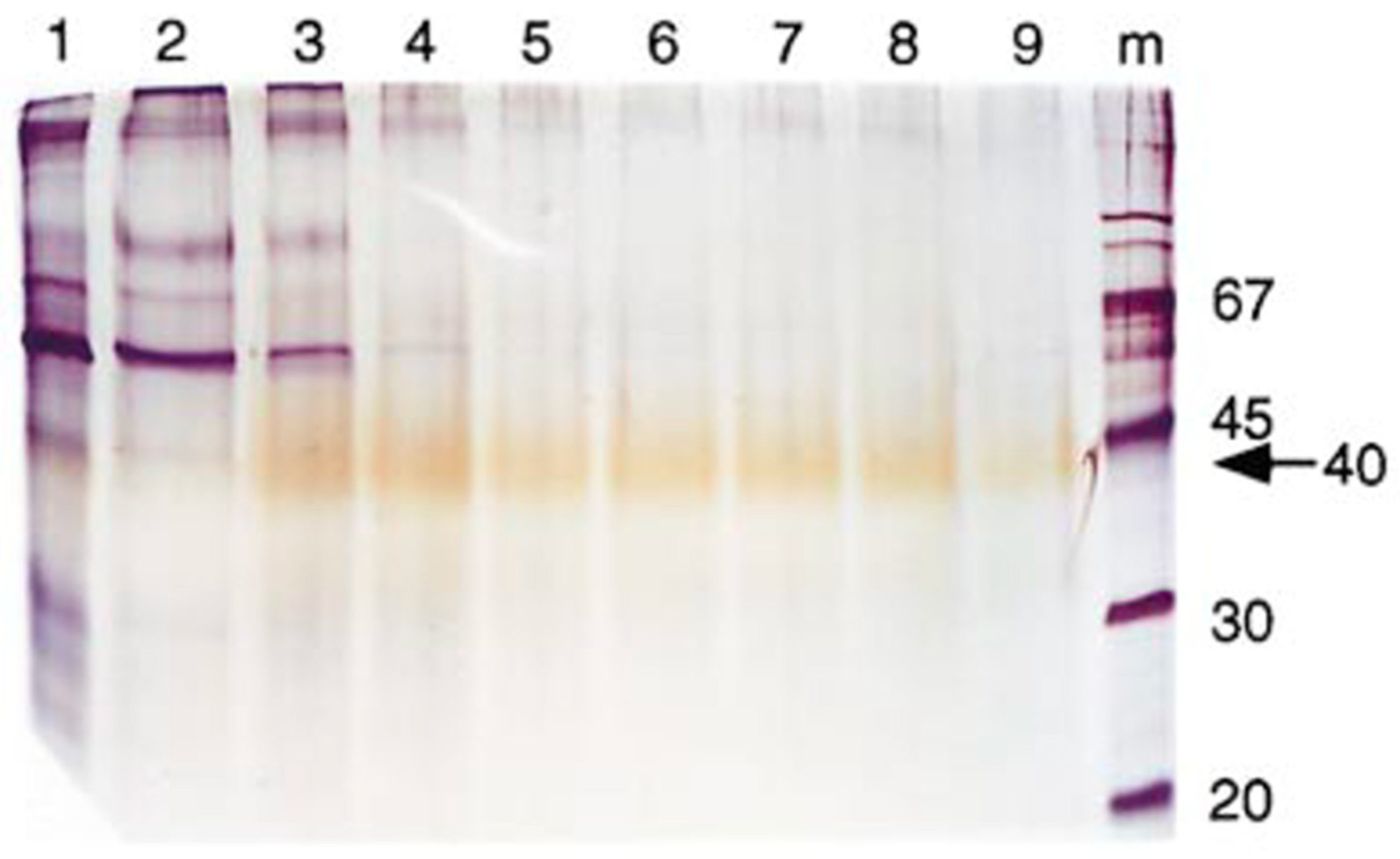

Table 1.
IL-18 inhibitory drugs.
| Drug Name | Company | Description | Indications | Clinical Trials | Clinical trial number |
|---|---|---|---|---|---|
| Tadekinig alfa | AB2 Bio Ltd. | Recombinant IL-18BP | -NLRC4 mutation -XIAP deficiency |
Phase III completed |
NCT03113760 |
| Tadekinig alfa | AB2 Bio Ltd. | Recombinant IL-18BP | AOSD | Phase II completed |
NCT02398435 |
| GSK 1070806 | GlaxoSmithKline | Humanized anti-IL-18 IgG1 monoclonal antibody | Atopic Dermatitis | Phase II | NCT05999799 |
| Camoteskimab | Apollo Therapeutics | Human anti IL-18 IgG1 monoclonal antibody | Atopic Dermatitis | Phase II | NCT06436183 |
| MAS825 | Novartis | Anti IL-18 and IL-1 Bispecific Antibody | -NLRC4 mutation -XIAP deficiency |
Phase II | NLRC4-GOF, NCT04641442 |
Table 2.
IL-18 Enhancing Drugs.
| Drug Name | Company | Description | Indications | Clinical Trials | Clinical trial number or Ref. |
|---|---|---|---|---|---|
| ST-067 | Simcha Therapeutics | A variant of IL-18 resistant to IL-18BP monotherapy or combined with anti PD-1 | Variety of solid tumors | Phase Ia/II | NCT04787042 |
| XmAb143 | Xencor | Modified IL-18 fused to Fc and resistant to IL-18BP | Cancer | Pre-clinical | Nishtal et al., 2022 |
| BPT 567/PD1-IL18-Fc | Bright Peak Therapeutics | A conjugate of IL-18 variant resistant to IL-18BP with anti-PD-1 antibody | Cancer | Pre-clinical | Codarri Deak et al., 2022 |
| WTX 518 | Werewolf Therapeutics | Modified and conditionally activated IL-18 resistant to IL-18BP monotherapy or combined with anti PD-1 | Cancer | Pre- clinical | Morris et al., 2024 |
| SCA | Merck Healthcare KGaA and Synthekine | IL-18 mimetic agonist resistant to IL-18BP | Cancer | Pre- clinical | Lipinski et al., 2023 |
| COM503 | Compugen and Gilead | Anti IL-18BP fully human antibody | Mouse breast cancer, colorectal cancer and melanoma | Pre- clinical and Phase I | Menachem et al., 2024 |
| LASN500 | Lassen Therapeutics | Anti IL-18BP Antibody monotherapy or combined with anti PD-1 | Cancer | Pre- clinical | Jun et al., 2023 |
Table 3.
IL-18 and CAR T Combined Therapy.
| Drug Name | Company | Description | Indications | Clinical Trials | Clinical trial number or Ref. |
|---|---|---|---|---|---|
| HuCART19-IL18 | Gilead | Anti CD19 construct secreting IL-18 | Lymphoma | Phase I | Svoboda et al. 2022; Svoboda et al., 2024 |
| GPC3-IL18 | Eutilex Co. Ltd. | Targeted hepatocellular carcinoma tumor (HCC) marker, Glypican-3 (GPC3) and an IL-18-secreting CAR T cell therapy | Hepatocellular carcinoma tumor and non-small cell lung carcinoma | Phase I | |
| CD371-YSNVZIL-18 | Memorial Sloan Kettering Cancer Center | Combination of acute myelogenous leukemia targeted marker and IL-18-secreting construct | Acute Myeloid Leukemia | Phase I | NCT06017258 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



