
Submitted:
29 August 2025
Posted:
01 September 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: The COVID-19 outbreak began in December 2019 in China and quickly spread to other countries. Although most infected individuals experienced mild or moderate symptoms, 17% of patients were reported to have severe cases. Analysis of the available literature confirms the link between severe forms of COVID-19 and cyto-kine storm syndrome. Methods: A total of 57 patients participated in the study, divid-ed into a non-COVID group (24 people) and a COVID group (33 people). Each patient completed a questionnaire designed by the authors, followed by anthropometric measurements and venous blood sampling to determine cytokines, and pro- and an-ti-inflammatory chemokines using the Bio-Plex 200 system. Results: Showed statisti-cally significant higher values of IL-6, IL-13, TNF-α and the chemokines IP-10, MCP-1 (MCAF), MIP-1α, MIP-1β in the COVID-19 group. Conclusions: The results of our study support for the occurrence of elevated levels of IL-6, IL-13, TNF-α and selected chemokines in COVID-19 patients, which are associated with a worse course and prognosis of COVID-19. An in-depth understanding of the pathophysiology and im-mune dysfunction accompanying cyto-kine storm is crucial for identifying patients at increased risk, as well as for developing effective therapies and vaccines.
Keywords:
COVID–19
; cytokines
; chemokines
; SARS–CoV–2 virus
1. Introduction
The Coronavirus Disease Outbreak 2019 (COVID-19), caused by infection with Severe Acute Respiratory Syndrome 2 (SARS-CoV-2) virus, emerged in December 2019 in China and quickly spread to additional countries around the world [1]. Most of those infected experienced mild to moderate respiratory symptoms in the form of cough, runny nose, subfebrile state or sinusitis, without the need for specific treatment. However, it was reported that in 17% of patients, the course of COVID-19 was severe in the form of acute respiratory distress syndrome (ARDS), which was associated with organ damage and the development of acute renal failure, liver failure and septic shock [2,3]. SARS-CoV-2 infection has also been shown to be associated with an increased risk of thromboembolic incidents, which has been confirmed in numerous published scientific studies [4,5,6]. Various mechanisms underlying the development of atherosclerosis in patients after COVID-19 are considered, one of which is dysregulation of the immune system, leading to massive production of pro-inflammatory cytokines. Increasing evidence suggests that patients who have undergone COVID-19 have a cytokine release syndrome, responsible for a more severe course of infection. Increased pro-inflammatory cytokines contribute to increased clotting and the development of thromboembolic disease (thrombosis, pulmonary embolism), which is associated with a poor prognosis and increased patient mortality [2,7].
Due to the active involvement of pro-inflammatory cytokines in COVID-19 progression, they have been proposed as part of the molecular targets in the diagnosis, prognosis and treatment of COVID-19. The aim of the present study was to evaluate the role of pro-inflammatory cytokines, viz. interleukin-6 (IL-6), interleukin-13 (IL-13), tumour necrosis factor-alpha (TNF-α) and chemokines: inducible protein-10 (IP-10/CXCL10), monocyte chemoattractant protein-1 (MCP-1/MCAF/CCL2), macrophage inflammatory protein-1 alpha (MIP-1α/CCL3), macrophage inflammatory protein-1 beta (MIP-1β/CCL4), in the course and development of COVID-19 complications. Understanding the mechanisms of cytokine release syndrome is crucial for the development of effective therapeutic approaches in COVID-19. Knowledge of the pathomechanisms underlying this complex infection will allow the identification of risk factors for the development of atherosclerosis in COVID-19 patients. This will allow the selection of at-risk patients in whom early prophylaxis can be implemented, preventing the development of complications during future pandemics, thus relieving the burden on the health care system.
2. Results
The final study population consisted of 57 patients, divided into the non-COVID group (13 women and 11 men) and the COVID group (15 women and 18 men). Patients’ anthropometric data are shown in Table 1.
In the non-COVID group, the median age was 48.5 years (range: 41.0–75.0), while in the COVID group it was 49.0 years (range: 35.0–86.0). The median BMI was 26.03 kg/m² in the non-COVID group and 26.09 kg/m² in the COVID group (Table 1). The groups were homogeneous in terms of sample size, gender, smoking status, obesity, physical activity, age, height, and body weight.
Cytokine levels in the non-COVID and COVID groups are detailed in Table 2 and Figure 1 and Figure 2. In the COVID group, the median IL-6 was 0.45 (range: 0.14 - 3.03), while in the non-COVID group the median was 0.02 (range: 0.02 - 0.03), IL-6 cytokine levels were significantly higher in the COVID group compared to the non-COVID group (p < 0.05). In the COVID group, the median IL-13 level was 3.04 (range: 1.21 - 6.63), while in the non-COVID group the median was 2.07 (range: 0.26 - 4.28), the IL-13 cytokine level was also significantly higher in the COVID group compared to the non-COVID group (p < 0.05).
Table 3 and Figure 3, Figure 4, Figure 5, Figure 6 and Figure 7 show the levels of all chemokines assessed in this study (IP-10, MCP-1 (MCAF), MIP-1α, MIP-1β and TNF-α). Mean levels of the tested chemokines IP-10, MCP-1 (MCAF), MIP-1α, MIP-1β and TNF-α in the COVID group were significantly higher than in the non-COVID group. (p = 0.041, 0.002, 0.015, 0.0007, <0.0001, respectively - Table 2).
3. Discussion
In the present study, the expression levels of IL-6, IL-13, TNF-α and the chemokines IP-10, MCP-1 (MCAF), MIP-1α, MIP-1β in the blood of COVID-19 patients were quantified and compared with a group of patients without SARS-CoV-2 infection. Statistically significant higher values of the determined parameters were found in the COVID-19 group. These results are also confirmed by other scientific reports.
On the basis of an analysis of COVID-19 cases, the Chinese Centre for Disease Control and Prevention published conclusions on the COVID-19 pandemic. The most common course of the disease was mild - 81 per cent of cases. The proportion of patients with severe and critical course was 14% and 5% of cases, respectively [8]. Cytokines are thought to play a key role in the pathogenesis of the severe course of COVID-19. During infection, the body’s immune response is dysregulated, leading in subsequent stages to excessive cytokine production and thus autoinflammatory respiratory disease [9,10]. Individual cytokines and chemokines are differentially expressed depending on the severity and severity of the disease course and the time elapsed since infection. Consequently, cytokines can be useful as biomarkers, used to predict disease evolution, and are direct therapeutic targets [11].
Not only did our study confirm the significant role of IL-6 in the storm of COVID-19-associated cytokine release, Liu et al. showed that IL-6, interleukin-1β (IL-1β), IP-10 and MCP-1 were significantly elevated in patients with COVID-19, and some of these cytokines were more frequently observed in patients with severe disease than in patients without severe infection [12].
In a study by Liao et al. it was observed that in bronchoalveolar lavage fluid from patients with COVID-19, IL-6 levels gradually increased with disease severity, reaching a peak in critical patients [13]. A correlation of elevated IL-6 levels with higher viral titer, lymphopenia, neutrophilia, hypoxaemia and worse prognosis has been demonstrated in severe SARS-CoV-2 infection [14,15,16]. In addition, certain polymorphisms in the IL-6 receptor gene (IL-6R), leading to impaired IL-6 signalling, have been shown to result in a milder course of infection and a lower risk of hospitalisation and mortality. It follows that IL-6R blockade may be an effective treatment option [17].
IL-6 can act via three signalling pathways: cis, trans-signalling and transposition. In cis signalling, IL-6 binds to its receptor (IL-6R) on macrophages, hepatocytes, intestinal cells and megakaryocytes, mediating protection against intracellular pathogens. Trans-signalling stimulates pro-inflammatory activation of pneumocytes, adipose tissue-associated macrophages, neutrophils, intestinal epithelial cells and endothelial cells, while trans-signalling induces differentiation of regulatory T cells into pathogenic T helper 17 (TH17) cells [9,18]. Through trans-signalling, IL-6 can further increase the production of chemokines, adhesion molecules and coagulation factors, leading to increased endothelial permeability, neutrophil and monocyte migration into inflamed tissues, neutrophil-endothelial interaction and hypercoagulability. It is the trans-signalling and transposition that are likely to be the cause of the diffuse inflammatory process at multiple levels, such as pulmonary, vascular, intestinal inflammation, which is associated with the severe course of COVID-19 in the form of shock, microthrombosis and multi-organ dysfunction [9,19,20].
There are a huge number of studies in which elevated IL-6 levels have been observed, as in our case, in patients with COVID-19 [21,22,23,24]. Among the available literature, we were unable to find reports of reduced serum IL-6 levels in patients after SARS-CoV-2 infection. Although patients with COVID-19 present with elevated IL-6 levels, these have been found to be significantly lower than in other severe respiratory diseases [25]. Analysis of COVID-19 patients in Shanghai showed IL-6 levels in the range of 100-200 pg/ml 20-30 days after symptom onset [26]. Comparing to the results of a study on patients with acute respiratory distress syndrome (ARDS), mean IL-6 levels were found to be 712 pg/ml, and 834 pg/ml in patients with severe bacterial pneumonia [27]. Similarly, the SAILS study on patients with ARDS confirmed higher IL-6 levels [28]. Consequently, Hendrick et al. questioned the use of IL-6 antagonists as an effective treatment option for COVID-19. IL-6 is known to be a pleiotropic cytokine with both pro-inflammatory and anti-inflammatory effects. Therefore, it is uncertain whether elevated IL-6 levels in viral infections are an adverse effect or part of an adaptive immune response [25,29]. It has been reported that patients with a severe course of COVID-19 had a higher incidence of adverse effects in the form of secondary infections after the inclusion of anti-IL-6 therapy [30,31]. Although IL-6 determination appears to be an important biomarker of the course of COVID-19, the different biology of SARS-CoV-2 and other viral infections suggests not using a single cut-off value for all diseases. Furthermore, therapy based on IL-6 inhibition should be approached with caution.
Another biomarker of inflammation we investigated was IL-13, which appeared to be elevated in COVID-19 patients, consistent with previous reports [1,32,33].
A study by Vaz de Paul examined the expression of interleukin-4 (IL-4), IL-13, transforming growth factor-beta (TGF-β) and the number of M2 macrophages (sphingosine-1) in patients with lung injury who died from COVID-19, compared with those who died from H1N1pdm09 infection (a subtype of the H1N1 influenza A virus) and a control group without lung injury. Significantly higher levels of IL-4 and lower levels of IL-13 and M2 macrophages were observed in the COVID-19 group, compared to the H1N1 group. Compared to the control group, COVID-19 patients showed higher expression of IL-4 and sphingosine-1 in M2 macrophages. There were no statistically significant differences in IL-13 and TGF-β levels, between the COVID-19 group and the control group. These data are indicative of different immune response mechanisms among SARS-CoV-2 patients [34].
Also, a study by Donlan et al. confirmed the significant role of IL-13 in the pathogenesis of SARS-CoV-2 infection. They found elevated IL-13 levels in patients with severe COVID-19 who required mechanical ventilation. Dupilumab is a monoclonal antibody that blocks IL-13 and IL-4 signalling. The use of the anti-IL-13 drug, dupilumab, in COVID-19 patients contributed to a milder course of the disease. In an experiment on mice infected with SARS-CoV-2, it was observed that neutralisation of IL-13 reduced mortality and disease severity without affecting viral load [35,36]. These data and the fact that the use of dupilumab results in better outcomes in patients with COVID-19 demonstrate the pathogenic role of IL-13 in COVID-19.
Analysis of the available literature confirms the association of severe forms of COVID-19 with cytokine storm syndrome, caused by overproduction of pro-inflammatory cytokines and uncontrolled systemic inflammation [37]. As an example, a study by Chen et al. showed that patients who died from COVID-19 had higher levels of IL-2, IL-6, IL-8, IL-10 and TNF-α, compared to survivors of this infection [38]. A similar observation was made by Udomsinprasert et al., who showed elevated levels of IL-6, IL-10 and TNF-α in patients who died from COVID-19 [39]. In a study by Majeed et al. eight pro-inflammatory cytokines (IL-1α, IL-1β, IL-12, IL-17A, IL-17E, IL-31, IFN-γ and TNF-α), three anti-inflammatory cytokines (IL-1Ra, IL-10 and IL-13) and two chemokines (CXCL9 and CXCL10) were examined among COVID-19 patients and healthy controls. It was observed that COVID-19 patients had significantly higher levels of IL-1α, IL-1β, IL-10, IL-12, IL-13, IL-17A, IL-31, IFN-γ, TNF-α and CXCL10, and lower levels of IL-1Ra compared to controls. In contrast, IL-17E and CXCL9 showed no significant differences between groups. Hence, their potential as biomarkers for the diagnosis and prognosis of COVID-19 is indicated [40].
Another study that assessed the levels of selected cytokines and chemokines in patients with COVID-19 was conducted by Lu et al. It showed elevated levels of IL-1β, IL-6, IL-10, MCP-1, TNF-α, IL-4 in patients with COVID-19 compared to those without COVID-19. Levels of IP-10 were highest in the first two weeks of the disease, and therefore may be a biomarker of the early stage of infection. Levels of all cytokines were significantly positively correlated with age, which may indicate a worse course and prognosis in older people [41].
TNF-α is one of the early pro-inflammatory cytokines and is produced by innate immune cells to combat viral infections. However, excessive production of TNF-α over a prolonged period of time can sustain inflammation and thus negatively affect the body [42]. In addition to mediating a pro-inflammatory response, during SARS-CoV-2 infection, TNF-α may also cause harmful tissue damage and progressively promote lung fibrosis, which then leads to inflammation, pulmonary oedema and acute respiratory distress syndrome (ARDS). TNF-α antagonists have therefore been suggested as potential therapies in COVID-19 [43].
TNF-α levels were also assessed among patients with a severe course of COVID-19 to compare to a mild/moderate course. In a study by Mortaz et al. significantly higher TNF-α receptor levels were observed in COVID-19 patients in the ICU and outside the ICU than in healthy subjects. The findings also suggest the possibility of using TNF-α as a promising biomarker for predicting the severity of COVID-19 and related complications and as a target for anti-TNF-α therapy [43,44].
In addition, TNF-α leads to bronchial hyperresponsiveness in patients with COVID-19, indicating excessive airway inflammation. As a result, the airway epithelium is exposed to increased neutrophilia and adverse inflammatory responses via cytokines such as granulocyte-macrophage colony-stimulating factor (GM-CSF), IL-8 and intercellular adhesion molecules (ICAM) [45]. Aiming to limit the replication and spread of SARS-CoV-2 virus, TNF-α promotes neutrophil migration into the airways. The incoming neutrophils secrete matrix metalloproteinase (MMP)-9, which is strongly associated with irreversible pulmonary fibrosis in patients with COVID-19 [46].
They also reported that TNF-α overexpression causes more complications in COVID-19 patients with comorbidities such as obesity, hypertension and cardiovascular disease [47]. Wu et al. showed that those with pre-existing cardiovascular complications had a five times higher mortality rate than those without [8]. Patients with comorbidities presented higher levels of TNF-α, which promotes inflammation, endothelial dysfunction and the development of atherosclerosis. Chronic inflammation leads to destabilisation of atherosclerotic plaques and increases the risk of myocardial infarction [48]. Furthermore, activated leukocytes migrate to the lung tissue, causing local inflammation and thus vasodilation and pulmonary oedema [43,49]. Also Schultheiß et al. in their study found high levels of IL-1β, IL-6 and TNF-α in patients with long-lasting symptoms and complications of COVID-19 [50].
A study by Chi et al. assessed a wide range of cytokines and chemokines among symptomatic and asymptomatic individuals with COVID-19, compared to healthy controls. Symptomatic cases showed elevated levels of 27 cytokines or chemokines (IL-1β, IL-1ra, IL-2, IL-2Rα, IL-6, IL-7, IL-8, IL-9, IL-10, IL-13, IL-15, IL-17, IL-18, G-CSF, M-CSF, IFN-α2, IFN-γ, TNF-α, TRAIL, basic FGF, HGF, PDGF-BB, VEGF, GRO-α, IP-10, MCP-1 and MIG), increased levels of IP-10, IL-10 and IL-7 in the asymptomatic group, compared with healthy controls. These data indicate that these 3 molecules (IP-10, IL-10 and IL-7) can be used to identify asymptomatic patients among suspected individuals. Comparing groups of symptomatic and asymptomatic patients, significantly lower levels of IL-1ra, IL-1β, IL-6 and the chemokine IP-10 were found among asymptomatic individuals, indicating that they may be predictors of clinical symptoms. Levels of cytokines and chemokines were also examined in patients categorised into degrees of infection severity. It was observed that those with severe COVID-19 presented higher levels of IL-6, IL-7, IL-10, G-CSF, M-CSF, IP-10, MCP-1, MCP-3, MIG and MIP-1α compared to mild cases and higher levels of MCP-3, MIG and MIP-1α compared to moderate cases [51]. Other studies have also confirmed that induction of IL-6, IL-7, IL-10, G-CSF, IP-10, MCP-1 and MIP-1α is associated with COVID-19 severity [1,52]. In contrast, Huang et al. showed that patients with COVID-19 had higher levels of the following cytokines: IL-6, IL-10 and TNF-α and chemokines: CXCL10 / IP-10, CCL2 / MCP-1 and CCL3 / MIP-1α [1]. However, these studies, like ours, have limitations related to the lack of follow-up of patients over a time interval and the lack of analysis of these factors with disease progression.
It is noteworthy that chemokine levels in patients with COVID-19 vary according to health status, disease severity and time since infection. In addition, different levels are found in symptomatic and asymptomatic patients. Similar levels of CCL3, CCL4 and CCL5 have been observed in symptomatic and asymptomatic patients, and in recovering patients [51]. Another study found increased levels of CCL2, CCL7 and CCL8 at the onset of SARS-CoV-2 infection, while as the disease progressed, patients showed high levels of CXCL10 and CCL3 [53]. In addition, symptomatic patients presented higher levels of CXCL10, CCL2 and CXCL9 compared with recovered patients. It is important to note that CXCL10 is absent in healthy individuals, while it increases with disease severity, so it may be helpful in early diagnosis and can be used as a predictive marker of disease [51,54]. Furthermore, CXCL10 is a marker for detecting infection in asymptomatic patients [55].
Similar results were obtained in a study showing elevated levels of CXCL10, CCL2, CCL3 and CCL7 in COVID-19 patients in severe condition requiring ICU stay, compared to those with mild infection [33]. It was also observed that CXCL8, CCL2 and CCL3 were at similar levels in mild and severe cases of SARS-CoV-2 infection, in the early stages of infection, and were increased in the late stages of the disease only in fatal cases. In patients with a mild course, they remained stable [56]. The results of the above studies confirm the importance of the chemokine profile in stratifying the severity of patients and identifying those at higher risk of complications.
The above findings highlight the association between COVID-19 and IL-6, IL-13 and TNF-α, suggesting that these cytokines can be used as diagnostic markers and that their inhibitors can be used as potential therapeutic agents for affected individuals.
Despite the pivotal role of IL-6, IL-13, TNF-α and other antiviral molecules in controlling SARS-CoV-2 infection, they often induce systemic inflammation that is highly likely to lead to severe disease outcomes. The results of the cited studies suggest that pro-inflammatory cytokines are among the main contributors to severe forms of COVID-19, which are often associated with failure of vital organs and high mortality.
Most studies assessing the role of cytokines and chemokines in the pathogenesis of COVID-19 have revealed a wide range of elevated inflammatory mediators during the cytokine storm, without identifying the precise time points of their increase during infection. Therefore, it is important to analyse changes in the levels of selected cytokines and chemokines over time, during the course of the disease, which is lacking in our study.
Cytokine release syndrome leads to life-threatening multiorgan dysfunction and may therefore represent a potential therapeutic target. Understanding the mechanisms underlying the cytokine storm allows the design of novel immunotherapies. Targeting key inflammatory cytokines such as IL-6, IL-13 is a novel strategy for the treatment of SARS-CoV-2 infection, which requires further research.
4. Materials and Methods
4.1. Patients
The study was carried out in the Department of Biochemistry in Zabrze and the Medical Laboratory of Dr Teresa Fryda in Zabrze between 2021 and 2024. A total of 117 patients participated in the study, from which a group of 94 patients was selected after taking into account the exclusion criteria. Due to the need for homogeneity of the group and the small number of unvaccinated persons (8), statistics were compiled only within vaccinated patients (86). Vaccinated patients were divided into two groups:
1. Patients with a confirmed history of SARS-CoV-2 infection (COVID, n=33).
2. Control group - patients who declared that they had not experienced COVID-19 (non-COVID, n=24).
Those who ticked the “don’t know” option (n=29) in response to the question about a history of SARS-CoV-2 infection were not included in the statistical analysis, due to the impossibility of clearly classifying these patients.
Figure 8 below illustrates the distribution of vaccinated individuals within the study cohort.
4.2. Procedure
The study included patients who presented themselves for blood sampling at the Diagnostyka medical laboratory (Dr n. med. Teresa Fryda) in Zabrze. Prior to blood sampling, patients were provided with a consent form to be signed and a questionnaire of their own authorship, concerning current medical conditions, medications taken, stimulants, family history, and information on past SARS-CoV-2 infection and COVID-19 vaccination. Each patient underwent anthropometric measurements and an additional 10 ml of venous blood was collected for testing. The collected blood was then centrifuged to obtain serum, which was stored at -80 degrees Celsius until biochemical determinations were made.
Inclusion criteria were age >18 years, informed consent to participate in the study, and no therapy with drugs affecting lipid metabolism and coagulation. Exclusion criteria included patients with a history of coronary artery disease, atherosclerosis of the arteries of the lower extremities or carotid arteries, severe liver failure, renal failure, severe respiratory failure, circulatory failure, BMI>40, on-going cancer, psychiatric illness, impaired consciousness, alcohol and substance abuse and pregnancy.
4.3. Data Analysis
The Bio-Plex Pro Human Cytokine 27-Plex Panel system (M500KCAF0Y), developed by Bio-Rad, was used for biochemical analyses. The assay parameters were as follows: analyte cross-reactivity was less than 10%, intra-assay precision (%CV) did not exceed 15%, and accuracy and percentage recovery ranged from 70-130%. The Bio-Plex Suspension Array system used was based on fluorescently labelled microspheres and technology licensed from Luminex Corporation (Austin, TX, USA) by Bio-Rad Laboratories, Inc. Calibration curves were used to determine the concentrations of individual analytes, which were generated from reference standards included with the kits.
4.4. Statistical Analysis
The statistical analysis was carried out using STATISTICA software (TIBCO Software Inc., Palo Alto, CA, USA, 2017). The Shapiro–Wilk test was employed to assess the normality of data distribution. For variables not following a normal distribution, the non-parametric Mann–Whitney U test was used. Differences between groups in categorical variables were evaluated using the chi-square test. A p-value of less than 0.05 was considered statistically significant.
Author Contributions
Conceptualization: Alicja Marczewska, Jolanta Zalejska-Fiolka, Celina Wojciechowska; methodology: Alicja Marczewska, Zenon Czuba, Karolina Wróbel, Kamil Marczewski, Urszula Błaszczyk; validation: Kamil Marczewski, Natalia Gospodarczyk, Urszula Błaszczyk; formal analysis: Paweł Dolibog;, Natalia Gospodarczyk; investigation: Alicja Marczewska, Jolanta Zalejska-Fiolka, Celina Wojciechowska, Natalia Gospodarczyk, Kamil Marczewski, Zenon Czuba; resources: Alicja Marczewska, data curation: Alicja Marczewska, Paweł Dolibog, Karolina Wróbel; writing—original draft preparation: Alicja Marczewska, writing—review and editing: Alicja Marczewska, Jolanta Zalejska-Fiolka, Celina Wojciechowska; visualization: Paweł Dolibog; supervision: Jolanta Zalejska-Fiolka, Celina Wojciechowska; project administration: Alicja Marczewska, Jolanta Zalejska-Fiolka, Celina Wojciechowska; funding acquisition: Alicja Marczewska. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethics Committee of the Silesian Medical University (SUM) approved this study under ref-erence number PCN/CBN/0022/KB1/134/21 on 21 December 2021.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data used in the review are available upon request. Patients’ personal data were secured in accordance with the provisions of the General Data Protection Regulation (GDPR). To ensure unbiased analysis, all samples were anonymised and numbered.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| COVID-19 | Coronavirus Disease 2019 |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome 2 Virus |
| IL-1α | Interleukin-1α |
| IL-1β | Interleukin-1β |
| IL-1Ra | Interleukin 1 receptor antagonist |
| IL-2 | Interleukin-2 |
| IL-2Rα | Interleukin 2 receptor alpha |
| IL-4 | Interleukin-4 |
| IL-6 | Interleukin-6 |
| IL-7 | Interleukin-7 |
| IL-8 | Interleukin-8 |
| IL-9 | Interleukin-9 |
| IL-10 | Interleukin-10 |
| IL-12 | Interleukin-12 |
| IL-13 | Interleukin-13 |
| IL-15 | Interleukin-15 |
| IL-17 | Interleukin-17 |
| IL-18 | Interleukin-18 |
| IL-31 | Interleukin-31 |
| TNF-α | Tumour necrosis factor-alpha |
| IFN-γ | Interferon-gamma |
| IL-6R | IL-6 receptor |
| IP-10/CXCL10 | Inducible protein-10 |
| MCP-1/MCAF/CCL2 | Monocyte chemoattractant pro-tein-1 |
| MIP-1α/CCL3 | Macrophage inflammatory protein-1 alpha |
| MIP-1β/CCL4 | Macrophage inflammatory protein-1 beta |
| CCL7 | Chemokine ligand 7 |
| CCL8 | Chemokine ligand 8 |
| CCL9 | Chemokine ligand 9 |
| ARDS | Acute Respiratory Distress Syndrom |
| F | Female |
| M | Male |
| BMI | Body mass index |
| TH17 | T helper 17 cells |
| TGF-β | Transforming growth factor-beta |
| G-CSF | Granulocyte colony stimulating factor |
| M-CSF | Macrophage colony stimulating factor |
| GM-CS | Granulocyte-macrophage colony stimulating factor |
| ICAM | Intercellular adhesion molecules |
| FGF | Fibroblast growth factor |
| HGF | Hepatocyte growth factor |
| PDGF-BB | Platelet-derived growth factor-BB |
| VEGF | Vascular endothelial growth factor |
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; Cheng, Z.; Yu, T.; Xia, J.; Wei, Y.; Wu, W.; Xie, X.; Yin, W.; Li, H.; Liu, M.; Xiao, Y.; Gao, H.; Guo, L.; Xie, J.; Wang, G.; Jiang, R.; Gao, Z.; Jin, Q.; Wang, J.; Cao, B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Stockman, L.J.; Bellamy, R.; Garner, P. SARS: systematic review of treatment effects. PLoS Med. 2006, 3, 343. [Google Scholar] [CrossRef]
- World Health Organization. Clinical management of severe acute respiratory infection when novel coronavirus (nCoV) infection is suspected. Available online: https://www.who.int/internal-publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected (accessed on day month year).
- Chousterman, B.G.; Swirski, F.K.; Weber, G.F. Cytokine storm and sepsis disease pathogenesis. Semin. Immunopathol. 2017, 39, 517–528. [Google Scholar] [CrossRef]
- Liu, Q.; Zhou, Y.H.; Yang, Z.Q. The cytokine storm of severe influenza and development of immunomodulatory therapy. Cell Mol. Immunol. 2016, 13, 3–10. [Google Scholar] [CrossRef]
- Channappanavar, R.; Perlman, S. Pathogenic human coronavirus infections: causes and consequences of cytokine storm and immunopathology. Semin. Immunopathol. 2017, 39, 529–539. [Google Scholar] [CrossRef]
- Liu, J.; Li, S.; Liu, J.; Liang, B.; Wang, X.; Wang, H.; et al. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. medRxiv 2020, preprint. [Google Scholar]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Zizzo, G.; Tamburello, A.; Castelnovo, L.; Laria, A.; Mumoli, N.; Faggioli, P.M.; Stefani, I.; Mazzone, A. Immunotherapy of COVID-19: inside and beyond IL-6 signalling. Front. Immunol. 2022, 13, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zizzo, G.; Cohen, P.L. Imperfect storm: is interleukin-33 the Achilles heel of COVID-19? Lancet Rheumatol. 2020, 2, 779–790. [Google Scholar] [CrossRef] [PubMed]
- Buszko, M.; Nita-Lazar, A.; Park, J.H.; Schwartzberg, P.L.; Verthelyi, D.; Young, H.A.; et al. Lessons learned: new insights on the role of cytokines in COVID-19. Nat. Immunol. 2021, 22, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Li, M.; Zhou, Z.; Guan, X.; Xiang, Y. Can we use interleukin-6 (IL-6) blockade for coronavirus disease 2019 (COVID-19)-induced cytokine release syndrome (CRS)? J. Autoimmun. 2020, 111, 102452. [Google Scholar] [CrossRef]
- Liao, M.; Liu, Y.; Yuan, J.; Wen, Y.; Xu, G.; Zhao, J.; et al. Single-cell landscape of bronchoalveolar immune cells in patients with COVID-19. Nat. Med. 2020, 26, 842–844. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhao, B.; Qu, Y.; Chen, Y.; Xiong, J.; Feng, Y.; et al. Detectable serum severe acute respiratory syndrome coronavirus 2 viral load (RNAemia) is closely correlated with drastically elevated interleukin 6 level in critically ill patients with coronavirus disease 2019. Clin. Infect. Dis. 2020, 71, 1937–1942. [Google Scholar] [CrossRef]
- Wang, F.; Qu, M.; Zhou, X.; Zhao, K.; Lai, C.; Tang, Q.; et al. The timeline and risk factors of clinical progression of COVID-19 in Shenzhen, China. J. Transl. Med. 2020, 18, 270. [Google Scholar] [CrossRef]
- Santa Cruz, A.; Mendes-Frias, A.; Oliveira, A.I.; Dias, L.; Matos, A.R.; Carvalho, A.; et al. Interleukin-6 is a biomarker for the development of fatal severe acute respiratory syndrome coronavirus 2 pneumonia. Front. Immunol. 2021, 12, 613422. [Google Scholar] [CrossRef] [PubMed]
- Bovijn, J.; Lindgren, C.M.; Holmes, M.V. Genetic variants mimicking therapeutic inhibition of IL-6 receptor signaling and risk of COVID-19. Lancet Rheumatol. 2020, 2, 658–659. [Google Scholar] [CrossRef]
- Narazaki, M.; Kishimoto, T. The two-faced cytokine IL-6 in host defense and diseases. Int. J. Mol. Sci. 2018, 19, 3528. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Fu, B.; Zheng, X.; Wang, D.; Zhao, C.; Qi, Y.; et al. Pathogenic T cells and inflammatory monocytes incite inflammatory storm in severe COVID-19 patients. Natl. Sci. Rev. 2020, 7, 998–1002. [Google Scholar] [CrossRef] [PubMed]
- Mazzone, A.; Castelnovo, L.; Tamburello, A.; Gatti, A.; Brando, B.; Faggioli, P.; et al. Monocytes could be a bridge from inflammation to thrombosis on COVID-19 injury: a case report. Thromb. Update 2020, 1, 100007. [Google Scholar] [CrossRef]
- Mazzoni, A.; Salvati, L.; Maggi, L.; Capone, M.; Vanni, A.; Spinicci, M.; Mencarini, J.; Caporale, R.; Peruzzi, B.; Antonelli, A.; Trotta, M.; Zammarchi, L.; Ciani, L.; Gori, L.; Lazzeri, C.; Matucci, A.; Vultaggio, A.; Rossi, O.; Almerigogna, F.; Parronchi, P.; Fontanari, P.; Lavorini, F.; Peris, A.; Rossolini, G.M.; Bartoloni, A.; Romagnani, S.; Liotta, F.; Annunziato, F.; Cosmi, L. Impaired immune cell cytotoxicity in severe COVID-19 is IL-6 dependent. J. Clin. Invest. 2020, 130, 4694–4703. [Google Scholar] [CrossRef]
- Villaescusa, L.; Zaragozá, F.; Gayo-Abeleira, I.; Zaragozá, C. A new approach to the management of COVID-19. Antagonists of IL-6: siltuximab. Adv. Ther. 2022, 39, 1126–1148. [Google Scholar]
- Potere, N.; Batticciotto, A.; Alessandra, —.; Porreca, E.; Cappelli, A.; Abbate, A.; Dentali, F.; Bonaventura, A. The role of IL-6 and IL-6 blockade in COVID-19. Expert Rev. Clin. Immunol. 2021, 17, 601–618.
- Gao, Y.D.; Ding, M.; Dong, X.; Zhang, J.J.; Kursat Azkur, A.; Azkur, D.; et al. Risk factors for severe and critically ill COVID-19 patients: a review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- Hedrick, T.L.; Murray, B.P.; Hagan, R.S.; Mock, J.R. COVID-19: Clean up on IL-6. Am. J. Respir. Cell Mol. Biol. 2020, 63, 541–543. [Google Scholar] [CrossRef]
- Zhang, X.; Tan, Y.; Ling, Y.; Lu, G.; Liu, F.; Yi, Z.; et al. Viral and host factors related to the clinical outcome of COVID-19. Nature 2020, 583, 437–440. [Google Scholar] [CrossRef] [PubMed]
- Bauer, T.T.; Montón, C.; Torres, A.; Cabello, H.; Fillela, X.; Maldonado, A.; et al. Comparison of systemic cytokine levels in patients with acute respiratory distress syndrome, severe pneumonia, and controls. Thorax 2000, 55, 46–52. [Google Scholar] [CrossRef]
- Sinha, P.; Matthay, M.A.; Calfee, C.S. Is a “cytokine storm” relevant to COVID-19? JAMA Intern. Med. 2020, Online ahead of print, 30 June.
- Velazquez-Salinas, L.; Verdugo-Rodriguez, A.; Rodriguez, L.L.; Borca, M.V. The role of interleukin 6 during viral infections. Front. Microbiol. 2019, 10, 1057. [Google Scholar] [CrossRef] [PubMed]
- Kimmig, L.M.; Wu, D.; Gold, M.; Pettit, N.N.; Pitrak, D.; Mueller, J.; et al. IL6 inhibition in critically ill COVID-19 patients is associated with increased secondary infections. medRxiv 2020, Preprint. [CrossRef]
- Somers, E.C.; Eschenauer, G.A.; Troost, J.P.; Golob, J.L.; Gandhi, T.N.; Wang, L.; et al. Tocilizumab for treatment of mechanically ventilated patients with COVID-19. Clin. Infect. Dis. 2021, 73, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Petrey, A.C.; Qeadan, F.; Middleton, E.A.; Pinchuk, I.V.; Campbell, R.A.; Beswick, E.J. Cytokine release syndrome in COVID-19: Innate immune, vascular, and platelet pathogenic factors differ in severity of disease and sex. J. Leukoc. Biol. 2021, 109, 55–66. [Google Scholar] [CrossRef]
- Yang, Y.; Shen, C.; Li, J.; Yuan, J.; Wei, J.; Huang, F.; et al. Plasma IP-10 and MCP-3 levels are highly associated with disease severity and predict the progression of COVID-19. J. Allergy Clin. Immunol. 2020, 146, 119–127. [Google Scholar] [CrossRef]
- Vaz de Paula, C.B.; de Azevedo, M.L.V.; Nagashima, S.; Camargo Martins, A.P.; Scaranello Malaquias, M.A.; Ribeiro dos Santos Miggiolaro, A.F.; et al. IL-4/IL-13 remodeling pathway of COVID-19 lung injury. Sci. Rep. 2020, 10, 18689. [Google Scholar] [CrossRef]
- Donlan, A.N.; Sutherland, T.E.; Marie, C.; Preissner, S.; Bradley, B.T.; Carpenter, R.M.; et al. IL-13 is a driver of COVID-19 severity. JCI Insight 2021, 6, 150107. [Google Scholar] [CrossRef] [PubMed]
- Moreau, G.B.; Burgess, S.L.; Sturek, J.M.; Donlan, A.N.; Petri, W.A.; Mann, B.J. Evaluation of K18-hACE2 Mice as a Model of SARS-CoV-2 Infection. Am. J. Trop. Med. Hyg. 2020, 103, 1215–1219. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Liu, J.; Zhang, D.; Xu, Z.; Ji, J.; Wen, C. Cytokine Storm in COVID-19: The Current Evidence and Treatment Strategies. Front. Immunol. 2020, 11, 1708. [Google Scholar] [CrossRef]
- Chen, R.; Lan, Z.; Ye, J.; Pang, L.; Liu, Y.; Wu, W.; Qin, X.; Guo, Y.; Zhang, P. Cytokine Storm: The Primary Determinant for the Pathophysiological Evolution of COVID-19 Deterioration. Front. Immunol. 2021, 12, 589095. [Google Scholar] [CrossRef]
- Udomsinprasert, W.; Jittikoon, J.; Sangroongruangsri, S.; Chaikledkaew, U. Circulating Levels of Interleukin-6 and Interleukin-10, But Not Tumor Necrosis Factor-Alpha, as Potential Biomarkers of Severity and Mortality for COVID-19: Systematic Review with Meta-Analysis. J. Clin. Immunol. 2020, 41, 11–22. [Google Scholar] [CrossRef]
- Majeed, A.Y.; Zulkafli, N.E.S.; Ad’hiah, A.H. Serum Profiles of Pro-Inflammatory and Anti-Inflammatory Cytokines in Non-Hospitalized Patients with Mild/Moderate COVID-19 Infection. Immunol. Lett. 2023, 260, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Zhu, Z.; Tan, C.; Zhou, H.; Hu, Y.; Shen, G.; Zhu, P.; Yang, G.; Xie, X. Changes of Serum IL-10, IL-1β, IL-6, MCP-1, TNF-α, IP-10 and IL-4 in COVID-19 Patients. Int. J. Clin. Pract. 2021, 75, e13792. [Google Scholar] [CrossRef]
- Holbrook, J.; Lara-Reyna, S.; Jarosz-Griffiths, H.; McDermott, M.F. Tumour Necrosis Factor Signalling in Health and Disease. F1000Research 2019, 8, 111. [Google Scholar] [CrossRef]
- Zawawi, Z.M.; Kalyanasundram, J.; Zain, R.M.; Thayan, R.; Basri, D.F.; Yap, W.B. Prospective Roles of Tumor Necrosis Factor-Alpha (TNF-α) in COVID-19: Prognosis, Therapeutic and Management. Int. J. Mol. Sci. 2023, 24, 6142. [Google Scholar] [CrossRef]
- Mortaz, E.; Tabarsi, P.; Jamaati, H.; Roofchayee, N.D.; Dezfuli, N.K.; Hashemian, S.M.; Moniri, A.; Marjani, M.; Malekmohammad, M.; Mansouri, D.; et al. Increased Serum Levels of Soluble TNF-α Receptor Is Associated with ICU Mortality in COVID-19 Patients. Front. Immunol. 2021, 12, 592727. [Google Scholar] [CrossRef]
- Leija-Martínez, J.J.; Huang, F.; Del-Río-Navarro, B.E.; Sanchéz-Muñoz, F.; Muñoz-Hernández, O.; Giacoman-Martínez, A.; Hall-Mondragon, M.S.; Espinosa-Velazquez, D. IL-17A and TNF-α as Potential Biomarkers for Acute Respiratory Distress Syndrome and Mortality in Patients with Obesity and COVID-19. Med. Hypotheses 2020, 144, 109935. [Google Scholar] [CrossRef]
- Savin, I.A.; Zenkova, M.A.; Sen’kova, A.V. Pulmonary Fibrosis as a Result of Acute Lung Inflammation: Molecular Mechanisms, Relevant In Vivo Models, Prognostic and Therapeutic Approaches. Int. J. Mol. Sci. 2022, 23, 14959. [Google Scholar] [CrossRef]
- Zheng, K.; Gao, F.; Wang, X.-B.; Sun, Q.-F.; Pan, K.-H.; Wang, T.-Y.; Ma, H.-L.; Chen, Y.-P.; Liu, W.-Y.; George, J.; et al. Obesity as a Risk Factor for Greater Severity of COVID-19 in Patients with Metabolic Associated Fatty Liver Disease. Metabolism 2020, 108, 154244. [Google Scholar] [CrossRef]
- Medina-Leyte, D.; Zepeda-García, O.; Domínguez-Pérez, M.; González-Garrido, A.; Villarreal-Molina, T.; Jacobo-Albavera, L. Endothelial Dysfunction, Inflammation and Coronary Artery Disease: Potential Biomarkers and Promising Therapeutical Approaches. Int. J. Mol. Sci. 2021, 22, 3850. [Google Scholar] [CrossRef]
- Zelová, H.; Hošek, J. TNF-α Signalling and Inflammation: Interactions between Old Acquaintances. Inflamm. Res. 2013, 62, 641–651. [Google Scholar] [CrossRef] [PubMed]
- Schultheiß, C.; Willscher, E.; Paschold, L.; Gottschick, C.; Klee, B.; Henkes, S.-S.; Bosurgi, L.; Dutzmann, J.; Sedding, D.; Frese, T.; et al. The IL-1β, IL-6, and TNF Cytokine Triad Is Associated with Post-Acute Sequelae of COVID-19. Cell Rep. Med. 2022, 3, 100663. [Google Scholar] [CrossRef]
- Chi, Y.; Ge, Y.; Wu, B.; Zhang, W.; Wu, T.; Wen, T.; Liu, J.; Guo, X.; Huang, C.; Jiao, Y.; Zhu, F.; Zhu, B.; Cui, L. Serum Cytokine and Chemokine Profile in Relation to the Severity of Coronavirus Disease 2019 in China. J. Infect. Dis. 2020, 222, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of immune response in patients with COVID-19 in Wuhan, China. Clin. Infect. Dis. 2020, ciaa248. [Google Scholar] [CrossRef]
- Buszko, M.; Park, J.-H.; Verthelyi, D.; Sen, R.; Young, H.A.; Rosenberg, A.S. The dynamic changes in cytokine responses in COVID-19: a snapshot of the current state of knowledge. Nat. Immunol. 2020, 21, 1146–1151. [Google Scholar] [CrossRef] [PubMed]
- Khalil, B.A.; Elemam, N.M.; Maghazachi, A.A. Chemokines and chemokine receptors during COVID-19 infection. Comput. Struct. Biotechnol. J. 2021, 19, 976–988. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.; Liu, Y.; Cao, L.; Wang, D.; Guo, M.; Jiang, A.; et al. Transcriptomic characteristics of bronchoalveolar lavage fluid and peripheral blood mononuclear cells in COVID-19 patients. Emerg. Microbes Infect. 2020, 9, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.S.; Shu, T.; Kang, L.; Wu, D.; Zhou, X.; et al. Temporal profiling of plasma cytokines, chemokines and growth factors from mild, severe and fatal COVID-19 patients. Signal Transduct. Target. Ther. 2020, 5, 100. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Serum IL-6 levels in the study groups. Box represents 1st and 3rd quartile range, whiskers represent minimum and maximum values. Differences between groups are statistically significant at p < 0.05.
Figure 1.
Serum IL-6 levels in the study groups. Box represents 1st and 3rd quartile range, whiskers represent minimum and maximum values. Differences between groups are statistically significant at p < 0.05.
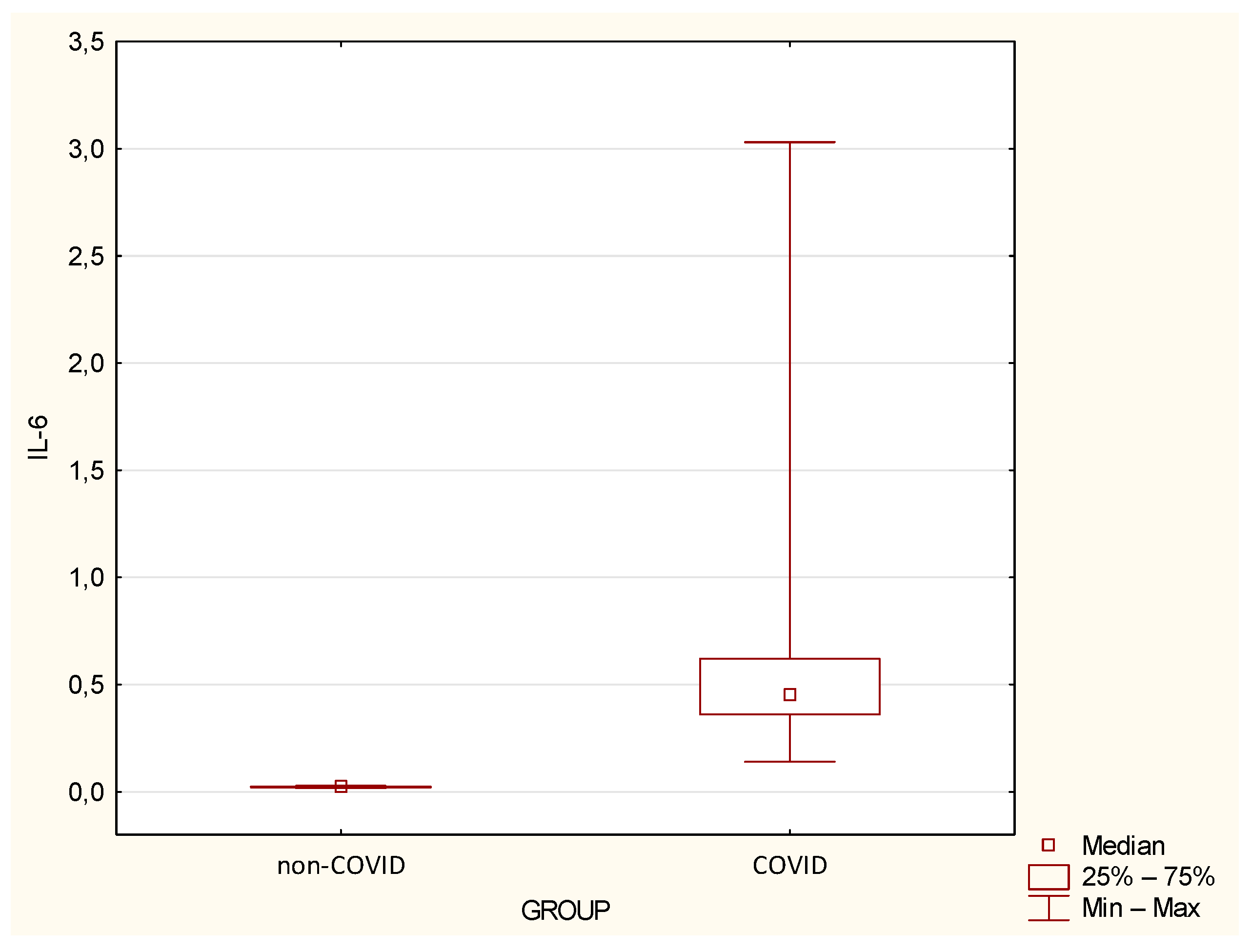
Figure 2.
Serum IL-13 levels in the study groups. Box represents 1st and 3rd quartile range, whiskers represent minimum and maximum values. Differences between groups are statistically significant at p < 0.05.
Figure 2.
Serum IL-13 levels in the study groups. Box represents 1st and 3rd quartile range, whiskers represent minimum and maximum values. Differences between groups are statistically significant at p < 0.05.
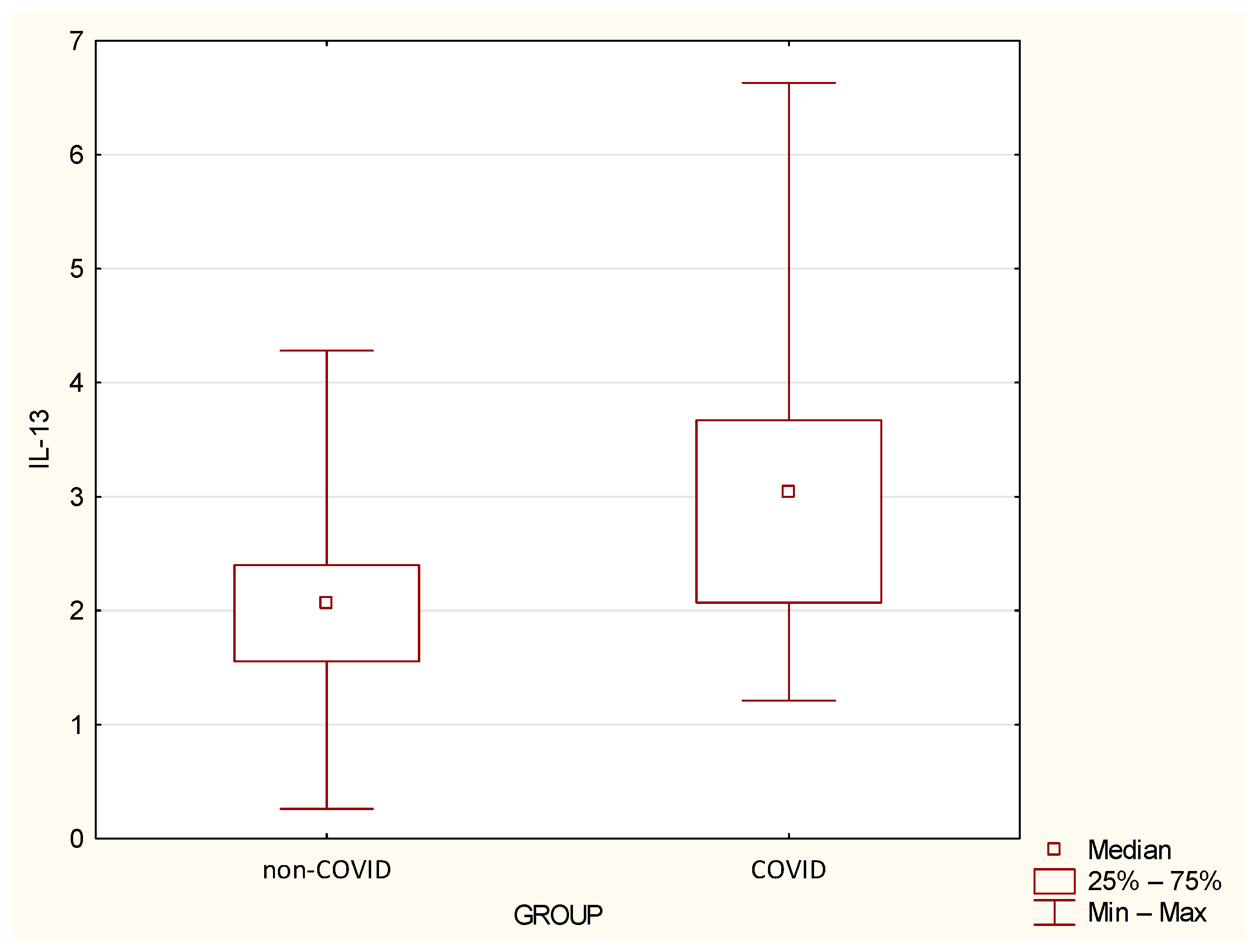
Figure 3.
Serum IP-10 levels in the study groups. Box represents 1st and 3rd quartile range, whiskers represent minimum and maximum values. Differences between groups are statistically significant at p < 0.05.
Figure 3.
Serum IP-10 levels in the study groups. Box represents 1st and 3rd quartile range, whiskers represent minimum and maximum values. Differences between groups are statistically significant at p < 0.05.
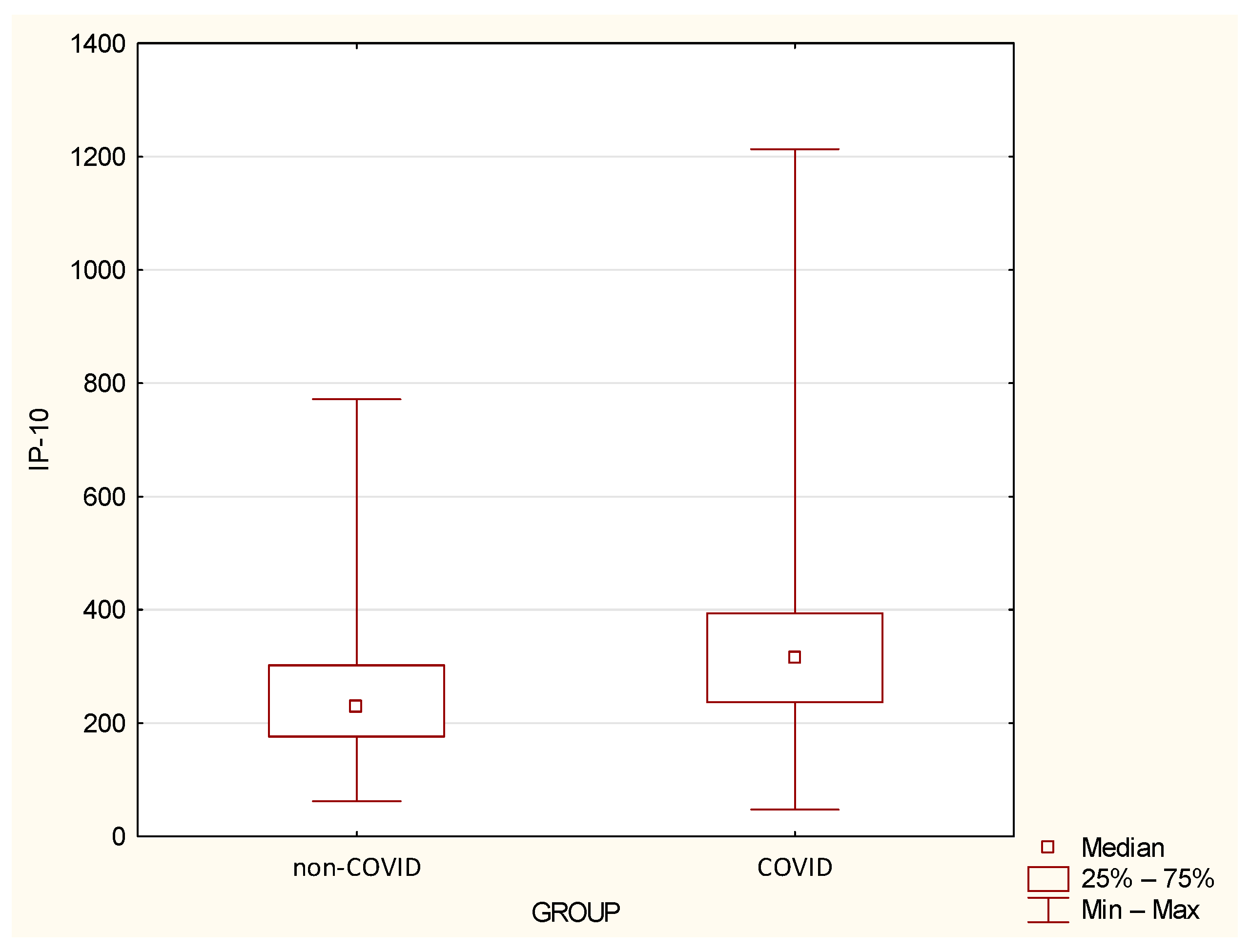
Figure 4.
Serum MCP-1 levels in the study groups. Box represents 1st and 3rd quartile range, whiskers represent minimum and maximum values. Differences between groups are statistically significant at p < 0.05.
Figure 4.
Serum MCP-1 levels in the study groups. Box represents 1st and 3rd quartile range, whiskers represent minimum and maximum values. Differences between groups are statistically significant at p < 0.05.
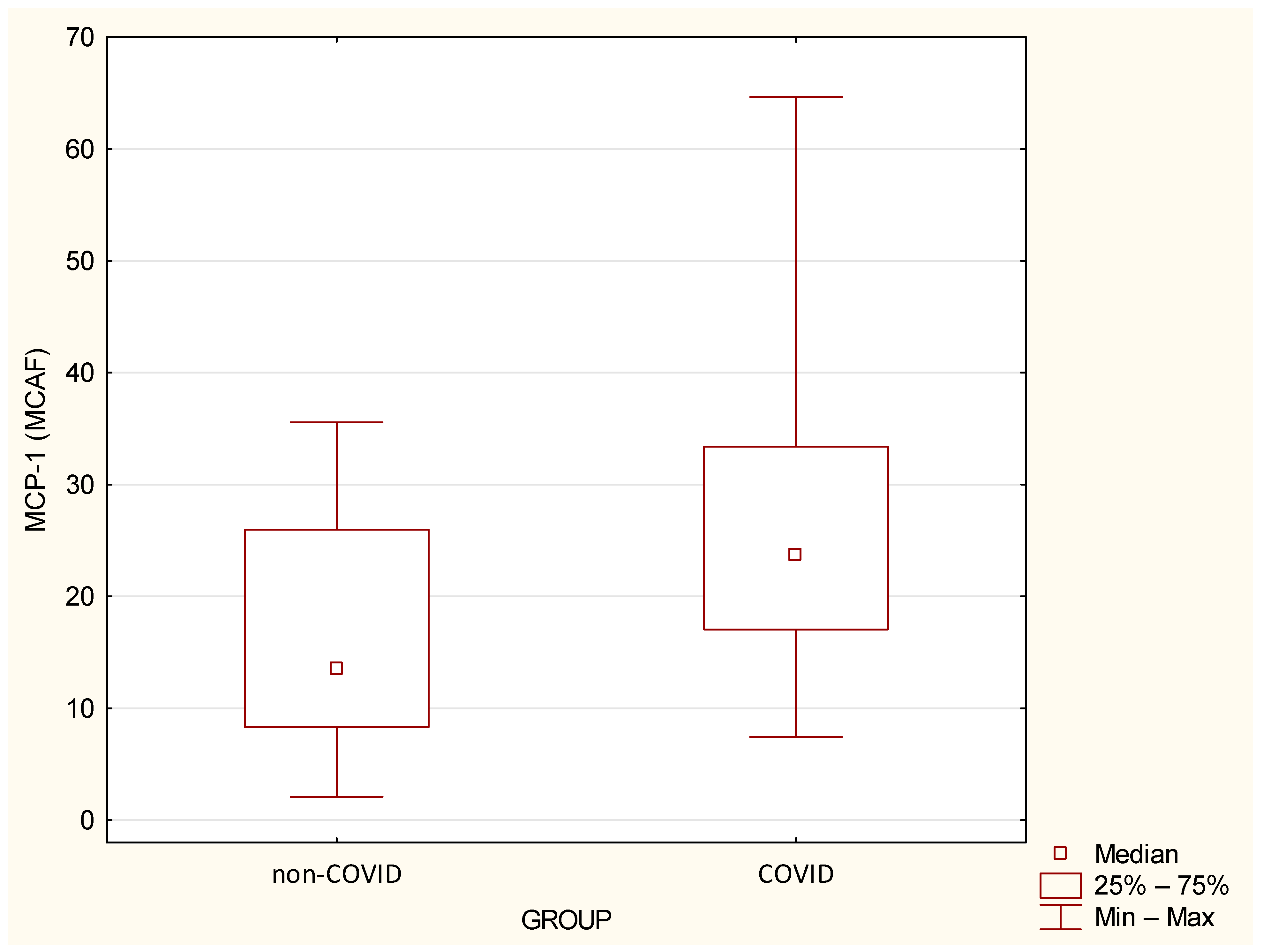
Figure 5.
Serum MIP-1α levels in the study groups. Box represents 1st and 3rd quartile range, whiskers represent minimum and maximum values. Differences between groups are statistically significant at p < 0.05.
Figure 5.
Serum MIP-1α levels in the study groups. Box represents 1st and 3rd quartile range, whiskers represent minimum and maximum values. Differences between groups are statistically significant at p < 0.05.
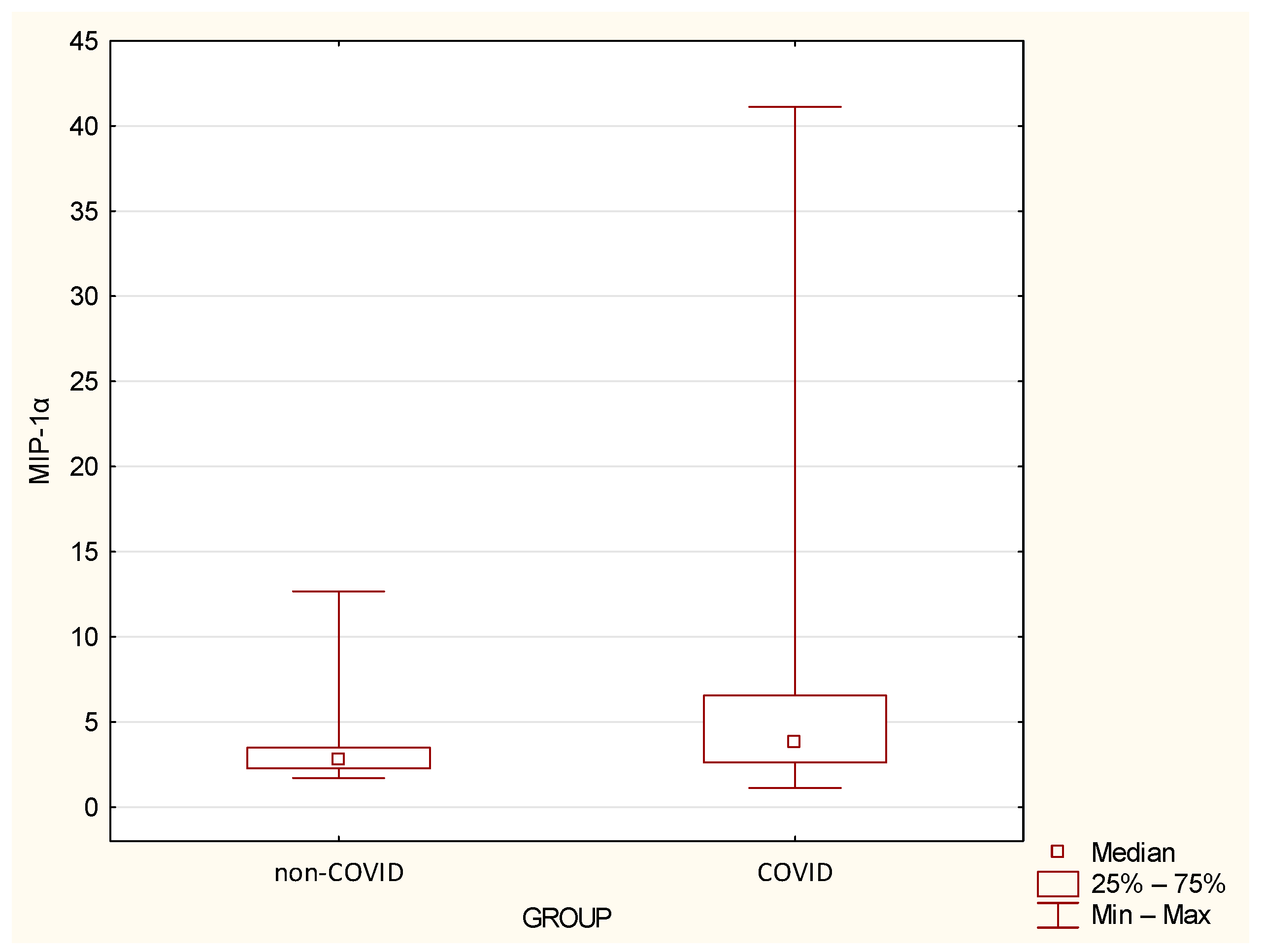
Figure 6.
Serum MIP-1β levels in the study groups. Box represents 1st and 3rd quartile range, whiskers represent minimum and maximum values. Differences between groups are statistically significant at p < 0.05.
Figure 6.
Serum MIP-1β levels in the study groups. Box represents 1st and 3rd quartile range, whiskers represent minimum and maximum values. Differences between groups are statistically significant at p < 0.05.
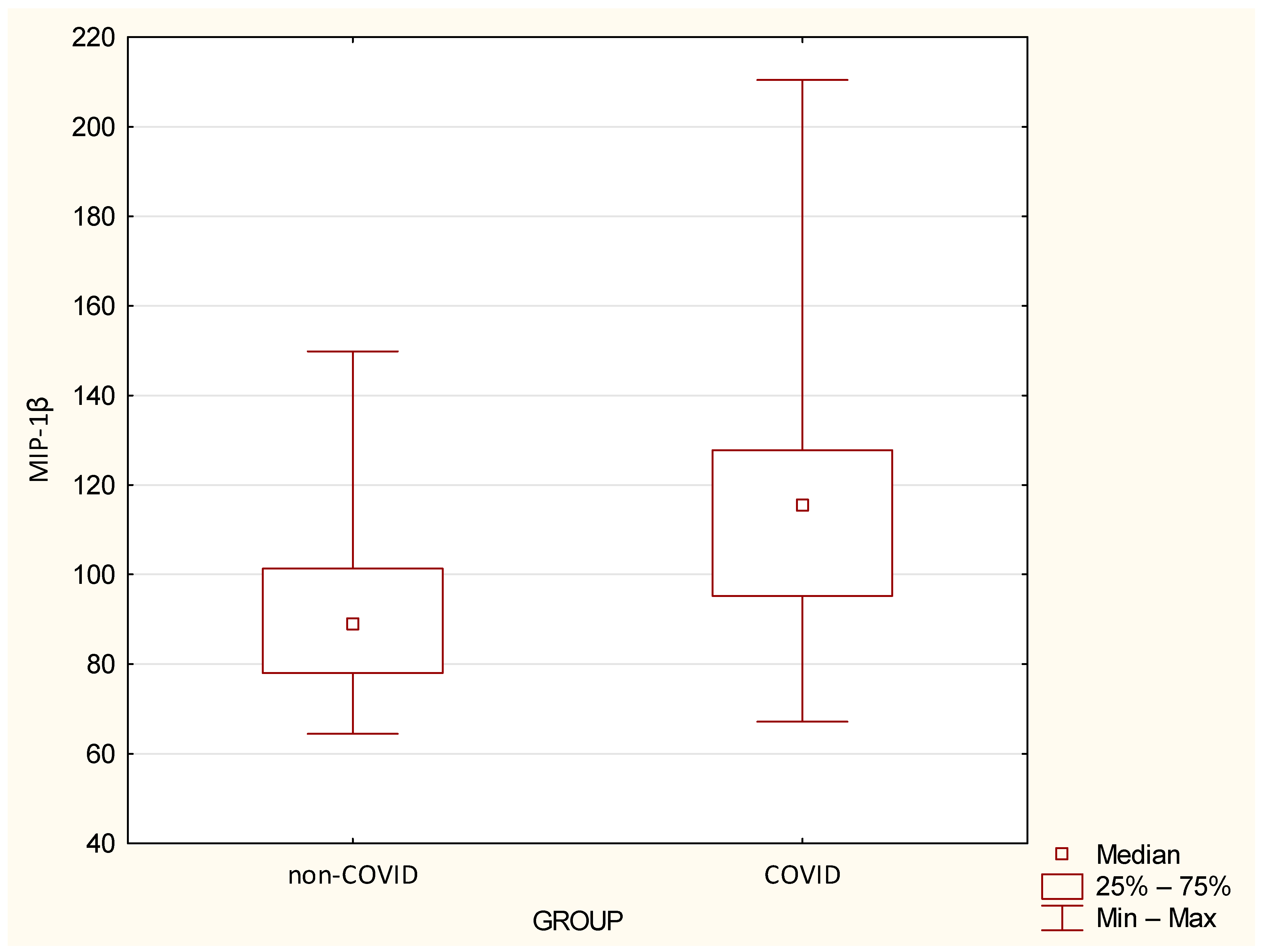
Figure 7.
Serum TNF-α levels in the study groups. Box represents 1st and 3rd quartile range, whiskers represent minimum and maximum values. Differences between groups are statistically significant at p < 0.05.
Figure 7.
Serum TNF-α levels in the study groups. Box represents 1st and 3rd quartile range, whiskers represent minimum and maximum values. Differences between groups are statistically significant at p < 0.05.
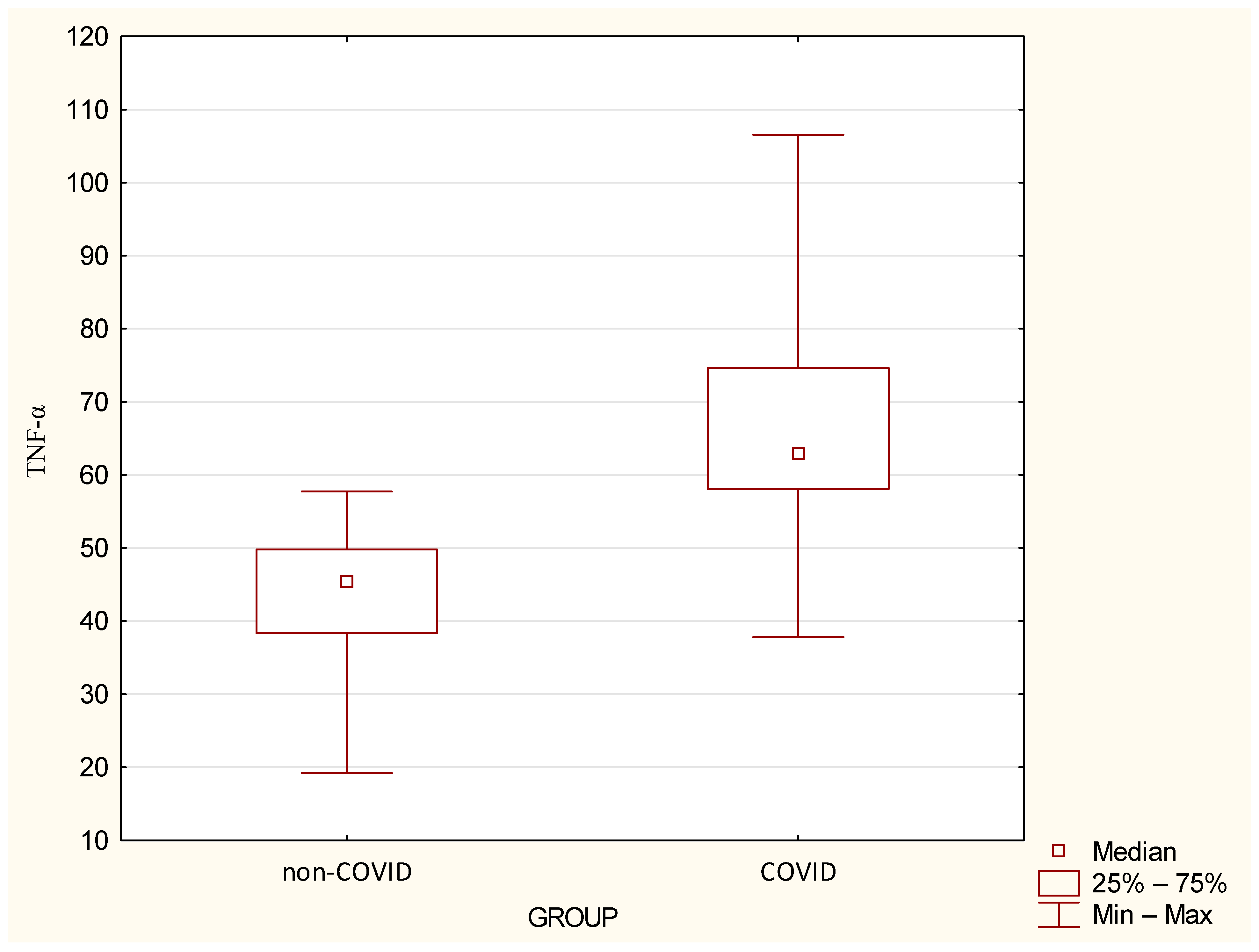
Figure 8.
Distribution of vaccinated individuals within the study cohort.
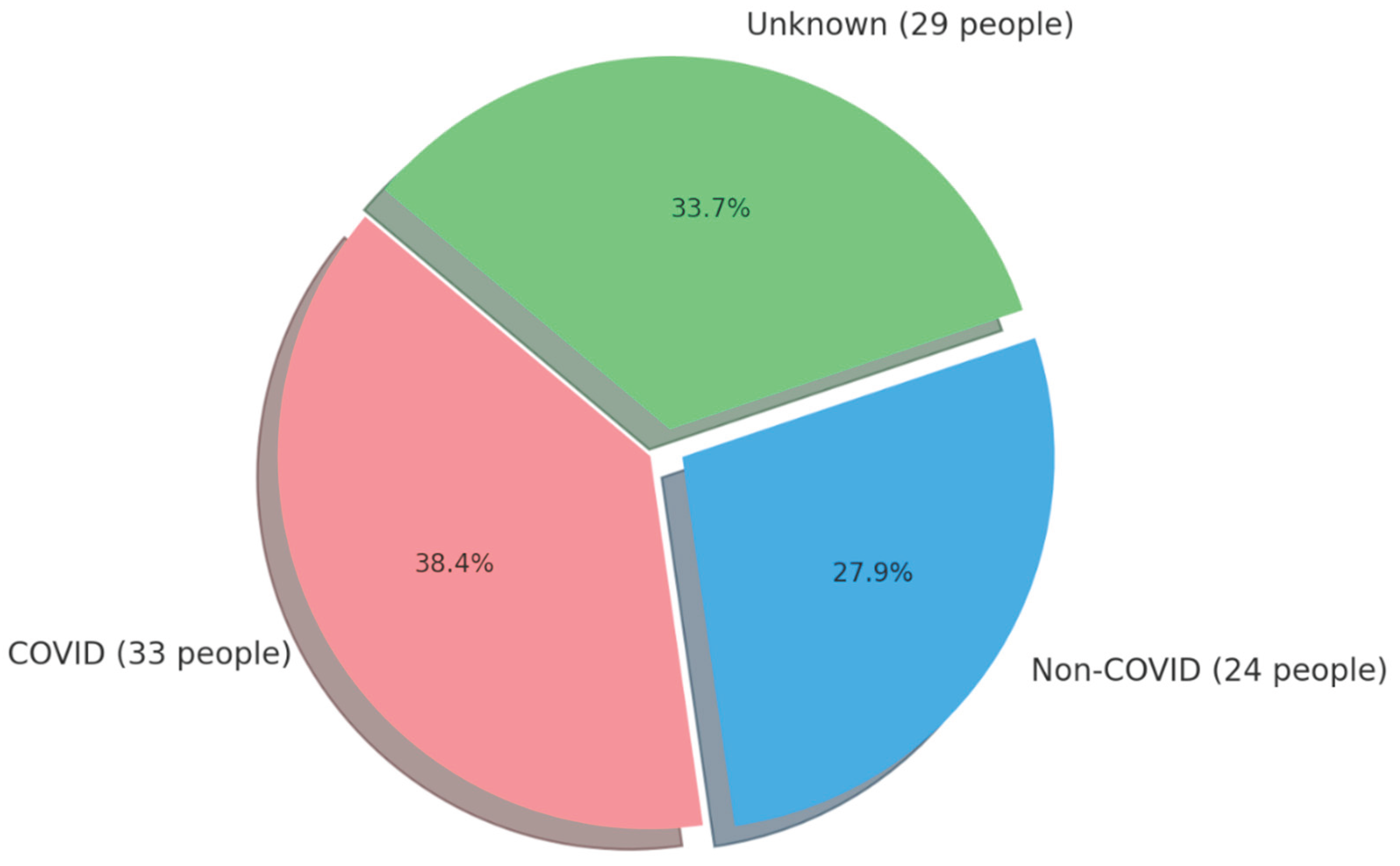

Table 1.
Basic anthropometric data of the participants from particular groups (* - U Mann-Whitney test; **- Chi-squared test).
Table 1.
Basic anthropometric data of the participants from particular groups (* - U Mann-Whitney test; **- Chi-squared test).
| Variable | NON–COVID GROUP (n=24) | COVID GROUP (n=33) | p-Value | ||||||||
| Mean | SD | Median | Min | Max | Mean | SD | Median | Min | Max | ||
| Age [years] | 52.21 | 9.38 | 48.5 | 41.0 | 75.0 | 50.97 | 9.83 | 49.0 | 35.0 | 86.0 | 0.6247* |
| BMI [kg/m2] | 26.85 | 4.99 | 26.03 | 21.19 | 39.84 | 26.31 | 3.63 | 26.09 | 19.94 | 34.09 | 0.9170* |
| Waist circumference [cm] | 91.45 | 10.49 | 94.0 | 76.0 | 111.0 | 90.77 | 10.06 | 92.0 | 71.0 | 107.0 | 0.9428* |
| Gender n (%) |
F = 13 (45.8) M = 11 (54.2) |
F = 15 (45.5) M = 18 (55.5) |
0.5160** | ||||||||
| Smoking n (%) |
NO = 19 (79.2) YES = 5 (20.8) |
NO = 30 (90.9) YES = 3 (9.1) |
0.2076** | ||||||||
| Alcohol consumption n (%) |
YES = 6 (25.0) NO = 18 (75.0) |
YES = 5 (15.1) NO = 28 (84.9) |
0.3523** | ||||||||
| Physical activity n (%) |
Low = 4 (16.7) Moderate =14 (58.3) High = 6 (25.0) |
Low = 8 (24.2) Moderate = 22 (66.7) High = 3 (9.1) |
0.2536** | ||||||||
Table 2.
Cytokine levels in the blood serum of patients in the study groups.
| Variable | NON–COVID GROUP (n=24) | COVID GROUP (n=33) | p-Value | ||||||||
| Mean | SD | Median | Min | Max | Mean | SD | Median | Min | Max | ||
| IL-6 | 0.02 | 0.00 | 0.02 | 0.02 | 0.03 | 0.6 | 0.53 | 0.45 | 0.14 | 3.03 | <0.0001 |
| IL-13 | 2.1 | 0.97 | 2.07 | 0.26 | 4.28 | 3.25 | 1.49 | 3.04 | 1.21 | 6.63 | 0.0016 |
Table 3.
Chemokine levels determined in serum of patients’ blood in the studied groups.
| Variable | NON–COVID GROUP (n=24) | COVID GROUP (n=33) | p-Value | ||||||||
| Mean | SD | Median | Min | Max | Mean | SD | Median | Min | Max | ||
| IP-10 | 260.88 | 145.33 | 228.81 | 62.22 | 771.66 | 335.46 | 203.53 | 316.22 | 47.47 | 1213.3 | 0.0419 |
| MCP-1 (MCAF) | 16.67 | 10.39 | 13.53 | 2.09 | 35.57 | 27.53 | 14.17 | 23.74 | 7.45 | 64.65 | 0.0024 |
| MIP-1α | 3.49 | 2.42 | 2.75 | 1.71 | 12.67 | 6.77 | 8.04 | 3.85 | 1.13 | 41.11 | 0.0155 |
| MIP-1β | 92.28 | 21.21 | 88.71 | 64.5 | 149.84 | 118.03 | 34.08 | 115.21 | 67.17 | 210.45 | 0.0007 |
| TNF-α | 43.52 | 10.89 | 45.37 | 19.19 | 57.71 | 66.05 | 15.13 | 62.86 | 37.79 | 106.56 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



