
Submitted:
11 November 2024
Posted:
12 November 2024
You are already at the latest version
Abstract
Background: Celiac disease (CD) is a chronic, permanent gluten-dependent disease that manifests itself with inflammation of the small intestine and malabsorption in genetically predisposed individuals with HLA-DQ2 and DQ8 (Human Leukocyte Antigen) histocompatibility antigens. Objective: The diagnostic criteria for celiac disease have undergone numerous modifications over the years. The aim of the study is to evaluate the frequency of HLA DQ2/DQ8 genes in a group of patients with celiac disease diagnosed years ago. The aim of the study was the verification of the primary diagnosis of CD in patients diagnosed between 1980-2010. Methods: The study group included 50 patients, 13 men and 37 women, who had been diagnosed with celiac disease many years ago based on histopathological criteria and improvement of health condition after receiving a gluten-free diet. The control group consisted of 31 healthy volunteers, 18 women and 13 men. All subjects underwent a genetic analysis assessing the presence of histocompatibility antigens HLA DQ2.2, DQ 2.5 and DQ8, along with the assessment of alleles encoding the α and β subunits of the antigens, according to ESPHEGAN guidelines from 2020, using the EUROarray technique at EUROIMMUNE®. Results: In the study group 12 (24%) patient did not meet the genetic criteria. Among the remaining patients (group 1) with celiac disease, the presence of HLA-DQ 2.5 (50.0% vs. 9.68%; p<0.01) and the co-occurrence of both alleles of HLA-DQ 2 (31.6% vs. 6.45%; p<0.05) were detected significantly more frequently than in the control group. Among celiac patients, the prevalence of HLA-DQ 8 was also slightly more frequent (13.2% vs. 3.23% p>0.05). Patients who did not meet the genetic criteria for celiac disease (group 2) had a single string α- HLA DQ 2.5 significantly more often than control subjects (66,67% vs 38,71% p<0,05). Conclusions: Among patients with celiac disease diagnosed before 2010, basing on the 2020 ESPGHAN criteria, it is advisable to verify the previous diagnosis taking into account genetic criteria.
Keywords:
celiac disease
; HLA-DQ2/DQ8
; gluten free diet
1. Introduction
Celiac disease (CD) is a chronic, permanent gluten-dependent disease that manifests itself with inflammation of the small intestine and malabsorption in genetically predisposed individuals with HLA-DQ2 and DQ8 (Human Leukocyte Antigen) histocompatibility antigens [1,2]. Due to the complaints and accompanying symptoms, two variants of celiac disease are distinguished with intestinal and extraintestinal manifestations [1,2].
CD is considered one of the most common autoimmune diseases. Its prevalence, depending on the studied population and methodology, is estimated at 0.75-1.6% of all screened subjects [3,4,5,6]. Among first-degree relatives of patients with celiac disease, the risk of developing the disease is 4.5–10.7% and among second-degree relatives 2.3–2.6% [7,8,9].
1.1. Criteria for the Diagnosis of Celiac Disease: Historical Outline and Current Status
Over the decades, the criteria for diagnosing celiac disease have gradually changed along with the increasing knowledge on its etiopathogenesis. The guidelines developed at an expert meeting in 1969 in Interlaken, Switzerland, included villous atrophy, which was reversible after a gluten-free diet and recurred following the period of gluten challenge and typical clinical symptoms (diarrhea, abdominal pain, vomiting, flatulence, fatty stools) that disappeared after a gluten-free diet. The criteria assumed performing three diagnostic gastroscopies to obtain biopsy samples from the duodenum [10,11]. Due to the low acceptance of returning to a gluten-free diet among patients, in 1979 ESPGHAN allowed the diagnosis of celiac disease based on a single biopsy, provided that there was clinical improvement after the applied diet [12]. In the subsequent ESPGHAN criteria from 1990, the determination of characteristic antibodies in the diagnosis of celiac disease was recommended [13]. Only the NICE (National Institute for Health and Care Excellence) 2009 guidelines for the diagnosis of celiac disease included the determination of antibodies against tissue transglutaminase II (anti-tTG) and antibodies against endomysium (anti-EMA). The important role of HLA-DQ2/DQ8 antigens in the pathogenesis of celiac disease was also recognized, however, they were not included in the criteria for the diagnosis of celiac disease [14]. Currently, in Poland the 2020 ESPGHAN guidelines for the diagnosis of celiac disease are in force, which are a modification of the 2012 criteria. According to the ESPGHAN criteria from 2012, the diagnosis included the clinical picture (both typical and atypical symptoms), villous atrophy Marsh grade 2 or 3, detection of characteristic anti-endomysial antibodies, anti tissue transglutaminase 2 (anti-tTG) or anti-deamidated gliadin peptides (anti-DGP), at a concentration that is at least three times higher than normal and the presence of specific histocompatibility antigens HLA-DQ2 or DQ8. However, the 2020 modification places the main emphasis on the determination of anti-tTG IgA antibodies and the determination of the total IgA level in order to exclude a deficiency and thus a false negative result. In the case of children and adolescents, the simultaneous finding of a ten times the upper limit of normal anti-tTG IgA antibodies with a normal level of total IgA and a typical clinical picture allows for the diagnosis of celiac disease omitting the necessity of histopathological examination of a duodenal biopsy [1,2].
In Poland, for years, due to low availability and the applicable criteria for diagnosing celiac disease which did not include serological tests, specific antibody tests were not performed in accordance with the ESPGHAN guidelines from 1989 [13].
1.2. Aim of the Study
Over the years, the guidelines for diagnosing CD have been changed as knowledge about it has deepened and new, widely available diagnostic tests have been developed, allowing for a more specific diagnosis. As a result, many patients who were diagnosed with the disease in the past do not currently meet the required criteria. The aim of the study was the verification of the primary diagnosis of CD in patients diagnosed between 1980-2010.
2. Material and Methods
Initially the study included 57 patients diagnosed with celiac disease between 1980 and 2010 who were on a gluten-free diet (mean 70 months ± 90 SD). In this group, the diagnosis made many years ago was verified according to the ESPHEGAN criteria from 1989. Five patients did not provide histopathological results or were unable to determine the histopathological findings of the duodenal biopsy. In 2 other patients, at the time of the diagnosis, histopathology revealed Marsh grade 1, which was insufficient to make a correct diagnosis of celiac disease in the light of the lack of other tests for celiac disease. Despite not meeting the criteria at the time of the diagnosis, these patients were on a gluten-free diet and were diagnosed with celiac disease.
After analyzing the medical history, taking into account the criterion of histopathological changes (in the study group, patients had to have villous atrophy of at least Marsh 3a) and the improvement found after a gluten-free diet, the study group included 50 patients, 13 men and 37 women. The control group consisted of 31 healthy volunteers, 18 women and 13 men.
Then, genetic analysis was performed to assess the presence of HLA-DQ2.2, DQ 2.5 and DQ8 along with the evaluation of alleles encoding the α and β subunits of the antigens, in accordance with the applicable ESPHEGAN guidelines from 2020. Evaluation of tissue antigen subunits allows the exclusion of false positive results. EUROIMMUNE® EUROarray was used for the investigations. Blood samples were placed in a thermal cycler with HLA- DQA1 and HLA-DQB1 primers. Amplification products were labeled with fluorescent markers. The obtained product was applied to EUROArrays (containing BIOCHiP probes with microarrays) by the TITERPLANE technique (a technique which, by using a hydrophilic material in the central field and a hydrophobic material outside the field, so that the samples cannot mix with each other). As a result of hybridization, a fluorescent reaction occurred at the site where the material contained HLA-DQA1 or HLA-DQB1, respectively. Microarray analysis was performed using the EUROIMMUN Microarray Scanner with EUROArrayScan software. The evaluation was performed in a fully automated device that excluded the possibility of human error and facilitated data archiving.
The project was accepted by the Ehical Committee of the Medical University of Lodz from November 20, 2012, nr RNN/215/12/K
Statistical Analysis
Independent groups were compared in the analyzed study. Nominal variables are presented as percentage. To compare two nominal variables, the Chi2 test with Yates' correction or the two-sided Fisher’s exact test was used, depending on the size of the investigated groups.
The level of statistical significance was assumed to be p<0.05.
Statistical analyses were performed using Statistica 10 (Statsoft, Tulsa, USA).
3. Results
Investigation of the Prevalence of HLA-DQ 2 and HLA-DQ 8
In the group of patients following a gluten-free diet who had been previously diagnosed with celiac disease, 12 (24%) did not meet the genetic criterion. Based on the performed analysis, the presence of two alleles of the HLA-DQ 2 or DQ 8 antigens was not detected. (Figure 1.)
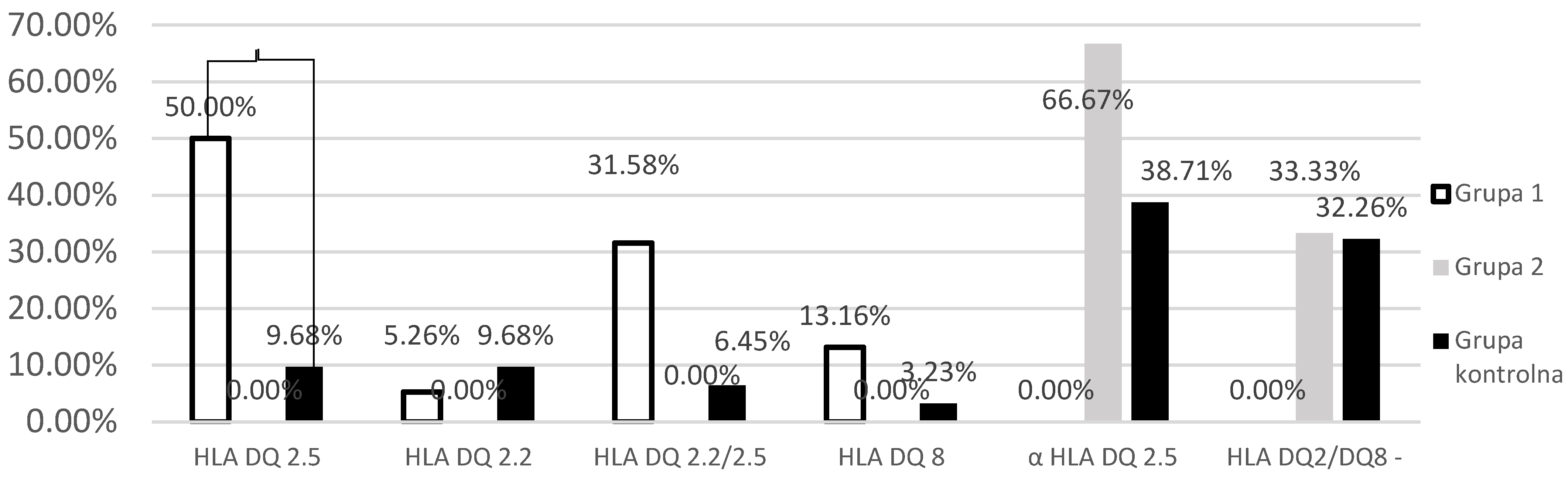
Among the remaining patients (group 1) with celiac disease, the presence of HLA-DQ 2.5 (50.0% vs. 9.68%; p<0.01) and the co-occurrence of both alleles of HLA-DQ 2 (31.6% vs. 6.45%; p<0.05) were detected significantly more frequently than in the control group. Among celiac patients, the prevalence of HLA-DQ 8 was also slightly more frequent (13.2% vs. 3.23% p>0.05). Patients who did not meet the genetic criteria for celiac disease (group 2) had a single string α- HLA DQ 2.5 significantly more often than control subjects (66,67% vs 38,71% p<0,05) (Figure 2).
In the analyzed Group 1, flatulence was observed significantly more frequently among patients with HLA-DQ 2.5 allele than in those with other genetic variants (77.8% vs. 45%; P<0.05). No other correlations were found between genetic variants and reported symptoms.
4. Discussion
Initially 57 patients diagnosed with celiac disease were enrolled into the study according to the 1990 ESPGHAN criteria. These criteria, described in the Introduction, were mainly based on clinical symptoms and characteristic histopathological abnormalities in the intestinal mucosa [13]. Meanwhile, many later reports indicated the occurrence of histopathological changes, similar to those observed in celiac disease, in the course of other chronic diseases [15]. In patients with a history of celiac disease who follow a gluten-free diet, HLA- DQ2/DQ8 should be tested to verify the primary diagnosis. According to the current knowledge, the presence of HLA-DQ2/DQ8 is necessary for the development of celiac disease, and the occurrence of the disease without their presence seems very unlikely [1,2].
Genetic diagnostics to verify the previous diagnosis questioned it in 12 cases. In 8 patients only HLA-DQ2 α allele was detected, whereas in 4 patients no HLA-DQ2/8 were found. Despite quite unambiguous 2020 ESPGHAN guidelines, some authors drew attention to the fulfillment of other criteria for the diagnosis of celiac disease also among patients with only a single HLA-DQ2 alpha subunit, as well as HLA-DQ7, which had not yet been considered important in the development of celiac disease and was not included in the analyzed study group. A large Karell et al., study on a group of 1008 celiac patients showed that 61 neither carried HLA-DQ2 nor HLA-DQ8 heterodimers. Fifty seven of these encoded half of the DQ2 heterodimer. In the remaining 4 patients, none of the previously recognized genes were detected [16]. Later studies by Tinto et al., confirmed the presence of HLA-DQ2/DQ8 in only 95.8% of the study participants. In the remaining group of patients, the presence of single alpha chains and increased frequency of HLA-DQ7 were demonstrated [17]. Similarly, in the study by Lund et al., the frequency of HLA-DQ2 and DQ8 was assessed in 128 patients with histologically confirmed celiac disease. The presence of HLA-DQ 2.5 or DQ8 was confirmed in 120 patients, the presence of HLA-DQ 2.2 or DQ2.5 (trans) was detected in 7 and in one patient no antigens were detected [18]. In a Turkish study among 78 patients with histologically confirmed celiac disease and positive anti-tTG antibodies, the presence of HLA-DQ 2 or DQ8 was detected in 97.4% of patients (n=76) [19]. However, in another Turkish study involving 94 patients, the presence of predisposing genes was confirmed in 73.4% of the study participants [20]. Similarly, in a meta-analysis based on data from Spain, in 3% of patients diagnosed with celiac disease many years ago, based on the clinical picture and histological changes according to the 1979 ESGPHAN criteria, the presence of HLA-DQ 2 or DQ8 was not observed [21]. In a study of 57 Iranian celiac patients, no genes predisposing to the development of the disease were found in 2 patients [22]. Kapitany et al., analyzing the frequency of HLA-DQ2 and DQ8 among 70 patients with previously diagnosed celiac disease based on histopathology found the presence of antigens in 56% of study participants. However, in the group of HLA-negative patients, a long-term gluten challenge did not lead to an increase in the concentration of anti-tissue transglutaminase antibodies, and thus celiac disease was not confirmed in this group [23]. Similarly, Hopman et al., did not observe any increase in antibody levels during the use of gluten challenge in HLA-negative patients [24]. However, Bergsens et al., based on molecular studies, confirmed the involvement of single alpha chains and HLA-DQ7 in the pathogenesis of celiac disease [25]. The latest studies conducted in Italy also indicated an important role of HLA-DQ7 in the development of celiac disease [17,26]. Werkstetter et al., multicenter study referred to ESPGHAN confirmed the presence of typical HLA in all 399 patients with newly diagnosed celiac disease [27]. Similarly, Wolf et al., found out that all 227 patients diagnosed with celiac disease had HLA-DQ2 or DQ8 [28]. Further studies conducted in France on 82, in Finland on 114, in Sweden on 153, in Pakistan on 59 and in Lebanon on 31 patients showed the presence of typical genes in 98.8-100% of the examined patients [29,30,31,32,33]. Interestingly, Siddiqui et al., also evaluated patients with symptoms resembling celiac disease and showed the presence of a single α or β chain in 100% of cases (11 patients) [33]. Among patients initially qualified for the study who had been diagnosed with celiac disease years ago, HLA-DQ 2 and DQ 8 were relatively frequently not detected, similarly to the studies cited above. In the light of the above reports and in accordance with current 2020 ESPHGAN guidelines, if patients carry a single DQ2 allele or are negative for both HLA-DQ 2 and DQ8 then it is very unlikely that they have celiac disease. At the same time, it should be noted that genetic verification of a diagnosis made years ago often questions the earlier diagnosis. Nevertheless, this group should be recommended gluten challenge. Rispo et al., showed that introducing 60-120 mg of gluten into the diet for 3 months is well tolerated and provides a definitive answer as to the occurrence of celiac disease [34]. Among HLA-DQ2 and DQ8 negative patients, the use of gluten challenge did not cause any symptoms [35]. In the analyzed group, the presence of the HLA-DQ 2.5 was detected in 31 patients (81.58%). Previous genetic studies for celiac disease conducted among large patient populations also showed the presence of HLA-DQ 2.5 in nearly 90% of patients. Similarly to the analyzed group, HLA-DQ 2.2 and DQ8 occurred much less frequently among patients with celiac disease [22,36,37,38]. It should be emphasized that detailed molecular and cytogenetic studies confirmed the presence of binding areas of gliadin peptide fragments with HLA-DQ 2.2 and DQ8 in patients with celiac disease [39,40].
In the study group, the presence of HLA-DQ 2.2 was detected less frequently than in the control group (5.26% vs. 9.68%). The reason for the reduced frequency of HLA-DQ 2.2 in the population of patients with celiac disease may be explained by the study by Bodd et al., who analyzed 7 patients with celiac disease with confirmed presence of HLA-DQ 2.2, in whom no other genes predisposing to celiac disease were detected. It was shown that in this group of patients different areas of gliadin became immunogenic than in patients with HLA-DQ2.5 [39]. Also Alam et al., demonstrated that the frequency of HLA-DQ 2.2 among celiac patients was similar (8% of the examined patients) to that obtained in group 1 [38]. Fallang et al., showed that bindings between gliadin and HLA-DQ2-presenting cells were more stable in HLA-DQ 2.5(+) than in HLA DQ 2.2(+) cells. Tyrosine present in the gliadin fragment establishing a bond to HLA-DQ 2.5(+) APCs may be responsible for binding stability [41]. In this way, it facilitates antigen presentation and may explain more frequent occurrence of HLA-DQ 2.5 in patients with celiac disease than other antigens involved in the presentation of gliadin fragments. For this reason, HLA-DQ 2.5 antigens are more frequently detected in patients with celiac disease than HLA-DQ 2.2; however, the presence of HLA-DQ 2.2 alone does not unequivocally exclude celiac disease. When conducting genetic tests, potential laboratory errors and misinterpretation of results should be taken into account [42].
5. Summary
As a result of the deepening knowledge on the etiopathogenesis and course of celiac disease, enormous progress has been made in recent years, which has directly translated into modifications of the criteria for diagnosing celiac disease. Today we know that some patients who met the diagnostic criteria for celiac disease years ago may not develop celiac disease, for instance, due to lack of appropriate histocompatibility antigens. At the same time, some studies indicate the imperfection of the techniques used to determine histocompatibility antigens. Furthermore, attention is drawn to other histocompatibility antigens not previously included in the diagnostic criteria but which may also be important in the development of celiac disease. However, taking into account the frequent absence of HLA-DQ2 and DQ8, re-evaluation of diagnoses made years ago seems necessary.
6. Conclusion
Among patients with celiac disease diagnosed before 2010, basing on the 2020 ESPGHAN criteria, it is advisable to verify the previous diagnosis taking into account genetic criteria.
This study was supported by the Scientific grant No. 503/1-002-01/503-11-001 from the Medical University of Lodz, Poland to Ewa Malecka Wojciesko
References
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.R.; Mearin, M.L.; Phillips, A.; Shamir, R.; Troncone, R.; Giersiepen, K.; Branski, D.; Catassi, C.; et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition Guidelines for the Diagnosis of Coeliac Disease. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 136–160. [Google Scholar] [CrossRef] [PubMed]
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.; Kurppa, K.; Mearin, M.L.; Ribes-Koninckx, C.; Shamir, R.; Troncone, R.; Auricchio, R.; Castillejo, G.; et al. European Society Paediatric Gastroenterology, Hepatology and Nutrition Guidelines for Diagnosing Coeliac Disease 2020. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 141–156. [Google Scholar] [CrossRef] [PubMed]
- Bingley, P.J.; Norcross, A.J.; Lock, R.J.; Ness, A.R.; Jones, R.W. Undiagnosed coeliac disease at age seven: population based prospective birth cohort study. BMJ 2004, 328, 322–323. [Google Scholar] [CrossRef] [PubMed]
- Mäki, M.; Mustalahti, K.; Kokkonen, J.; Kulmala, P.; Haapalahti, M.; Karttunen, T.; Ilonen, J.; Laurila, K.; Dahlbom, I.; Hansson, T.; et al. Prevalence of Celiac Disease among Children in Finland. New Engl. J. Med. 2003, 348, 2517–2524. [Google Scholar] [CrossRef] [PubMed]
- Laass, M.W.; Schmitz, R.; Uhlig, H.H.; Zimmer, K.-P.; Thamm, M.; Koletzko, S. The Prevalence of Celiac Disease in Children and Adolescents in Germany. Dtsch. Aerzteblatt Online 2015, 112, 553–60. [Google Scholar] [CrossRef]
- Singh, P. , et al., Prevalence of Celiac disease in Asia: A systematic review and meta-analysis. J Gastroenterol Hepatol, 2015.
- Fasano, A. , et al., Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: a large multicenter study, in Arch Intern Med. 2003: United States. p. 286-92.
- Singh, P.; Arora, S.; Lal, S.; Strand, T.A.; Makharia, G.K. Risk of Celiac Disease in the First- and Second-Degree Relatives of Patients With Celiac Disease: A Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2015, 110, 1539–1548. [Google Scholar] [CrossRef]
- Sahin, Y. and S. Mermer, Frequency of celiac disease and distribution of HLA-DQ2/DQ8 haplotypes among siblings of children with celiac disease. World J Clin Pediatr, 2022. 11(4): p. 351-359.
- GW., M. GW., M., Diagnostic criteria in celiac disease. 1970: Acta Paediatr Scand. p. 461–3.
- CC, B. Definition of adult coeliac disease. in Proceedings of the Second International Symposium. 1974. Noordwijkerhout, The Netherlands: H.E. Stenfert Kroese B.V., Leiden.
- McNeish AS, H.K. , Rey J, Shmerling DH, Walker-Smith JA., Re-evaluation of diagnostic criteria for celiac disease. 1979, Arch Dis Child. p. 783-6.
- Revised criteria for diagnosis of coeliac disease. Report of Working Group of European Society of Paediatric Gastroenterology and Nutrition. Arch Dis Child, 1990. 65(8): p. 909-11.
- Richey, R.; Howdle, P.; Shaw, E.; Stokes, T. ; on behalf of the Guideline Development Group Recognition and assessment of coeliac disease in children and adults: summary of NICE guidance. BMJ 2009, 338, b1684–b1684. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Bai, J.C.; Biagi, F.; Card, T.R.; Ciacci, C.; Ciclitira, P.J.; Green, P.H.R.; Hadjivassiliou, M.; Holdoway, A.; van Heel, D.A.; et al. Diagnosis and management of adult coeliac disease: guidelines from the British Society of Gastroenterology. Gut 2014, 63, 1210–1228. [Google Scholar] [CrossRef]
- Karell, K.; Louka, A.S.; Moodie, S.J.; Ascher, H.; Clot, F.; Greco, L.; Ciclitira, P.J.; Sollid, L.M.; Partanen, J. Hla types in celiac disease patients not carrying the DQA1*05-DQB1*02 (DQ2) heterodimer: results from the european genetics cluster on celiac disease. Hum. Immunol. 2003, 64, 469–477. [Google Scholar] [CrossRef]
- Tinto, N.; Cola, A.; Piscopo, C.; Capuano, M.; Galatola, M.; Greco, L.; Sacchetti, L. High Frequency of Haplotype HLA-DQ7 in Celiac Disease Patients from South Italy: Retrospective Evaluation of 5,535 Subjects at Risk of Celiac Disease. PLOS ONE 2015, 10, e0138324. [Google Scholar] [CrossRef]
- Lund, F.; Hermansen, M.N.; Pedersen, M.F.; Hillig, T.; Toft–Hansen, H.; Sölétormos, G. Mapping of HLA– DQ haplotypes in a group of Danish patients with celiac disease. Scand. J. Clin. Lab. Investig. 2015, 75, 519–522. [Google Scholar] [CrossRef] [PubMed]
- Çakır, M.; Baran, M.; Uçar, F.; Akbulut, U.E.; Kaklıkkaya, N.; Ersöz. Accuracy of HLA-DQ genotyping in combination with IgA anti-tissue transglutaminase serology and a "scoring system" for the diagnosis of celiac disease in Turkish children. Turk J Pediatr 2014, 56, 347–53. [Google Scholar] [PubMed]
- zgenel Ş, M. , et al., HLA-DQ2/DQ8 frequency in adult patients with celiac disease, their first-degree relatives, and normal population in Turkey. Turk J Gastroenterol.
- Fernández-Bañares, F.; Arau, B.; Dieli-Crimi, R.; Rosinach, M.; Nuñez, C.; Esteve, M. Systematic Review and Meta-analysis Show 3% of Patients With Celiac Disease in Spain to be Negative for HLA-DQ2.5 and HLA-DQ8. Clin. Gastroenterol. Hepatol. 2017, 15, 594–596. [Google Scholar] [CrossRef] [PubMed]
- Rostami-Nejad, M. Allele and haplotype frequencies for HLA-DQ in Iranian celiac disease patients. World J. Gastroenterol. 2014, 20, 6302–8. [Google Scholar] [CrossRef] [PubMed]
- Kapitány, A.; Tóth, L.; Tumpek, J.; Csípő, I.; Sipos, E.; Wooley, N.; Partanen, J.; Szegedi, G.; Oláh, É.; Sipka, S.; et al. Diagnostic significance of HLA-DQ typing in patients with previous coeliac disease diagnosis based on histology alone. Aliment. Pharmacol. Ther. 2006, 24, 1395–1402. [Google Scholar] [CrossRef]
- Hopman, E.G. , et al., Gluten tolerance in adult patients with celiac disease 20 years after diagnosis? Eur J Gastroenterol Hepatol, 2008. 20(5): p. 423-9.
- Bergseng, E.; Dørum, S.; Arntzen, M. .; Nielsen, M.; Nygård, S.; Buus, S.; de Souza, G.A.; Sollid, L.M. Different binding motifs of the celiac disease-associated HLA molecules DQ2.5, DQ2.2, and DQ7.5 revealed by relative quantitative proteomics of endogenous peptide repertoires. Immunogenetics 2015, 67, 73–84. [Google Scholar] [CrossRef]
- Flores-Marin, D.L.; Linden, J.; Frank, E.; Pena, R.; Silvester, J.A.; Therrien, A. HLA-DQ7 haplotype among individuals with suspected celiac disease. Dig. Liver Dis. 2024, 56, 1414–1416. [Google Scholar] [CrossRef]
- Werkstetter, K.J.; Korponay-Szabó, I.R.; Popp, A.; Villanacci, V.; Salemme, M.; Heilig, G.; Lillevang, S.T.; Mearin, M.L.; Ribes-Koninckx, C.; Thomas, A.; et al. Accuracy in Diagnosis of Celiac Disease Without Biopsies in Clinical Practice. Gastroenterology 2017, 153, 924–935. [Google Scholar] [CrossRef]
- Wolf, J.; Petroff, D.; Richter, T.; Auth, M.K.; Uhlig, H.H.; Laass, M.W.; Lauenstein, P.; Krahl, A.; Händel, N.; de Laffolie, J.; et al. Validation of Antibody-Based Strategies for Diagnosis of Pediatric Celiac Disease Without Biopsy. Gastroenterology 2017, 153, 410–419.e17. [Google Scholar] [CrossRef]
- Kurppa, K.; Salminiemi, J.; Ukkola, A.; Saavalainen, P.; Löytynoja, K.; Laurila, K.; Collin, P.; Mäki, M.; Kaukinen, K. Utility of the New ESPGHAN Criteria for the Diagnosis of Celiac Disease in At-risk Groups. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 387–391. [Google Scholar] [CrossRef]
- Sandström, O.; Rosén, A.; Lagerqvist, C.; Carlsson, A.; Hernell, O.; Högberg, L.; Ivarsson, A. Transglutaminase IgA Antibodies in a Celiac Disease Mass Screening and the Role of HLA-DQ Genotyping and Endomysial Antibodies in Sequential Testing. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 472–476. [Google Scholar] [CrossRef] [PubMed]
- Clouzeau-Girard, H. , et al., HLA-DQ genotyping combined with serological markers for the diagnosis of celiac disease: is intestinal biopsy still mandatory? J Pediatr Gastroenterol Nutr, 2011. 52(6): p. 729-33.
- Alarida, K.; Harown, J.; Di Pierro, M.R.; Drago, S.; Catassi, C. HLA-DQ2 and -DQ8 genotypes in celiac and healthy Libyan children. Dig. Liver Dis. 2010, 42, 425–427. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, K.; Uqaili, A.A.; Rafiq, M.; Bhutto, M.A. Human leukocyte antigen (HLA)-DQ2 and -DQ8 haplotypes in celiac, celiac with type 1 diabetic, and celiac suspected pediatric cases. Medicine 2021, 100, e24954. [Google Scholar] [CrossRef]
- Rispo, A.; Guarino, A.D.; Siniscalchi, M.; Imperatore, N.; Santonicola, A.; Ricciolino, S.; de Sire, R.; Toro, B.; Cantisani, N.M.; Ciacci, C. “The crackers challenge”: A reassuring low-dose gluten challenge in adults on gluten-free diet without proper diagnosis of coeliac disease. Dig. Liver Dis. 2024, 56, 1517–1521. [Google Scholar] [CrossRef]
- Schiepatti, A.; Rej, A.; Maimaris, S.; Cross, S.S.; Porta, P.; Aziz, I.; Key, T.; Goodwin, J.; Therrien, A.; Yoosuf, S.; et al. Clinical classification and long-term outcomes of seronegative coeliac disease: a 20-year multicentre follow-up study. Aliment. Pharmacol. Ther. 2021, 54, 1278–1289. [Google Scholar] [CrossRef]
- Araya, M.; Oyarzun, A.; Lucero, Y.; Espinosa, N.; Pérez-Bravo, F. DQ2, DQ7 and DQ8 Distribution and Clinical Manifestations in Celiac Cases and Their First-Degree Relatives. Nutrients 2015, 7, 4955–4965. [Google Scholar] [CrossRef]
- Castro-Antunes, M.M. , et al., Frequency distribution of HLA DQ2 and DQ8 in celiac patients and first-degree relatives in Recife, northeastern Brazil. Clinics (Sao Paulo), 2011. 66(2): p. 227-31.
- Alam, M. , et al., HLA-DQ2 and HLA-DQ8 Alleles in Celiac Disease Patients and Healthy Controls. J Coll Physicians Surg Pak, 2022. 32(2): p. 157-160.
- Bodd, M.; Kim, C.; Lundin, K.E.; Sollid, L.M. T-Cell Response to Gluten in Patients With HLA-DQ2.2 Reveals Requirement of Peptide-MHC Stability in Celiac Disease. Gastroenterology 2012, 142, 552–561. [Google Scholar] [CrossRef]
- Moustakas, A.K.; van de Wal, Y.; Routsias, J.; Kooy, Y.M.C.; van Veelen, P.; Drijfhout, J.W.; Koning, F.; Papadopoulos, G.K. Structure of celiac disease-associated HLA-DQ8 and non-associated HLA-DQ9 alleles in complex with two disease-specific epitopes. Int. Immunol. 2000, 12, 1157–1166. [Google Scholar] [CrossRef] [PubMed]
- Fallang, L.-E.; Bergseng, E.; Hotta, K.; Berg-Larsen, A.; Kim, C.-Y.; Sollid, L.M. Differences in the risk of celiac disease associated with HLA-DQ2.5 or HLA-DQ2.2 are related to sustained gluten antigen presentation. Nat. Immunol. 2009, 10, 1096–1101. [Google Scholar] [CrossRef]
- Pritchard, D.; Anand, A.; De'Ath, A.; Lee, H.; Rees, M.T. UK NEQAS and BSHI guideline: Laboratory testing and clinical interpretation of HLA genotyping results supporting the diagnosis of coeliac disease. Int. J. Immunogenetics 2024, 51 Suppl 1, 3–20. [Google Scholar] [CrossRef]
Figure 1.
Gene frequency among patients on a gluten-free diet.
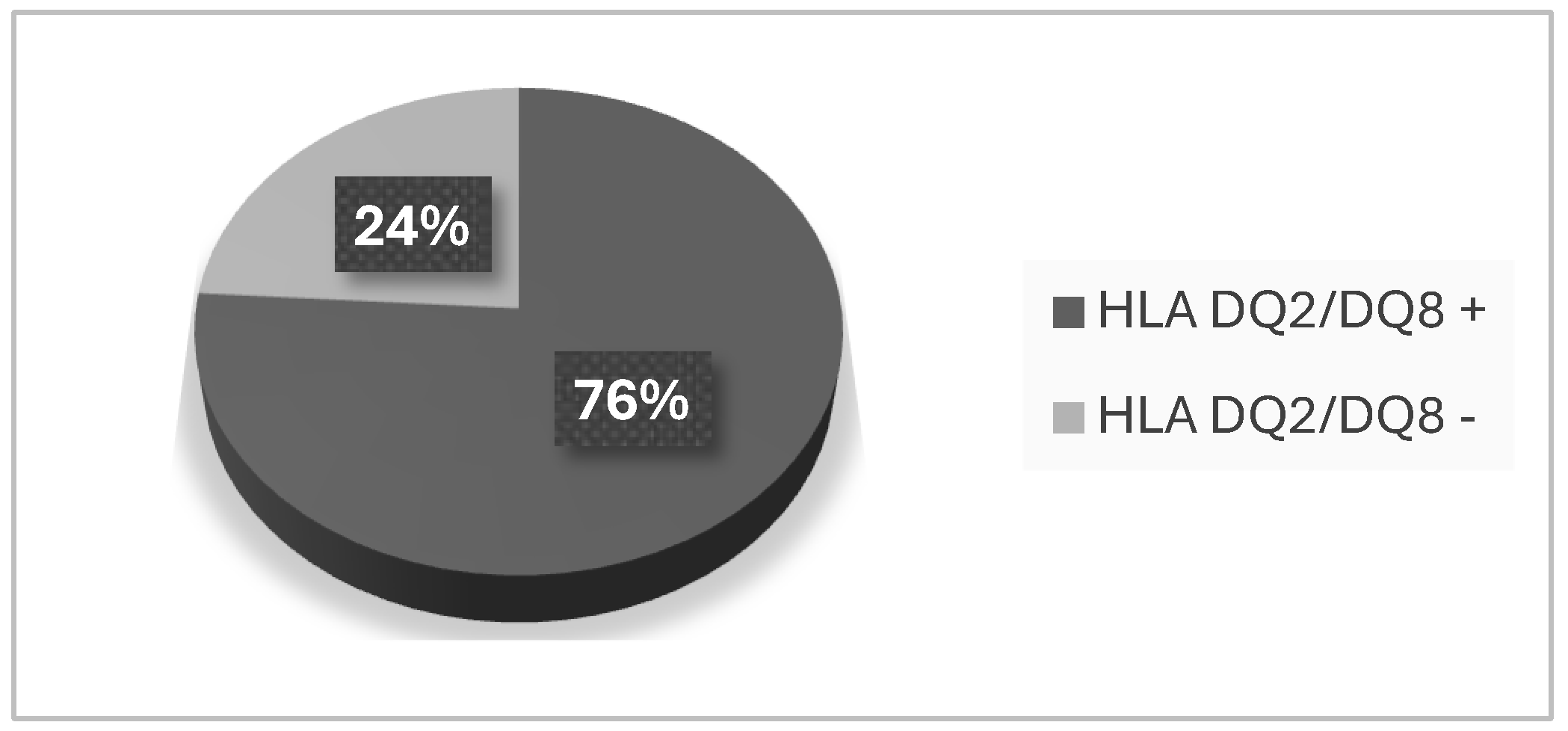
Figure 2.
Frequency of HLA-DQ 2.2, DQ 2.5 and HLA-DQ8 genes in the study groups and the control group.
Figure 2.
Frequency of HLA-DQ 2.2, DQ 2.5 and HLA-DQ8 genes in the study groups and the control group.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



