
Submitted:
04 November 2024
Posted:
05 November 2024
You are already at the latest version
Abstract
Congenital Dermatofibrosarcoma Protuberans (DFSP) is an extremely rare low-grade soft tissue sarcoma arising from the dermis. Accounting for less than 0.1% of all malignancies and approximately 1% of soft tissue sarcomas, congenital DFSP presents a significant diagnostic challenge due to its atypical presentation in neonates and infants. Often mimicking benign skin lesions such as hemangiomas, vascular malformations or pigmented moles, it is frequently misdiagnosed, leading to delays in appropriate treatment. This narrative review highlights the importance of early recognition and accurate diagnosis of congenital DFSP to prevent aggressive local growth and reduce the risk of recurrence. We discuss the epidemiology, clinical presentation and diagnostic hurdles associated with this condition. Histopathological examination remains the gold standard for diagnosis, with characteristic findings of spindle-shaped cells in a storiform pattern and strong CD34 positivity on immunohistochemical staining. Imaging modalities such as MRI may be helpful in assessing the extent of the lesion. Surgical excision with clear margins, preferably using Mohs micrographic surgery, is the cornerstone of treatment, balancing oncological control with functional and aesthetic considerations in paediatric patients. A multidisciplinary approach involving dermatologists, paediatric surgeons, oncologists and pathologists is essential for optimal management. We also emphasise the need for clinician vigilance, early biopsy of suspicious lesions, patient education and long-term follow-up to improve outcomes and quality of life for affected children.
Keywords:
Congenital DFSP
; misdiagnosis
; pediatric sarcoma
; Dermatofibrosarcoma Protuberans
; pediatric skin cancer
; rare skin cancer
; dermatology
; soft tissue tumor
1. Introduction
Dermatofibrosarcoma protuberans (DFSP) is a rare, low-grade, soft tissue sarcoma that originates from the dermis layer of the skin [1]. Accounting for less than 0.1% of all malignancies and approximately 1% of all soft tissue sarcomas, DFSP is characterized by its slow growth and locally aggressive behavior [2,3]. While it predominantly affects adults between the ages of 20 and 50, a congenital variant exists that presents even more significant diagnostic challenges due to its rarity and atypical presentation in neonates and infants [4,5]. Congenital DFSP often manifests at birth or within the first year of life, frequently masquerading as benign skin lesions such as vascular birthmarks, hemangiomas, or benign fibrous tumors [5]. This resemblance to more common and less aggressive conditions leads to frequent misdiagnosis or delayed diagnosis, which can adversely affect treatment outcomes [6]. The tumor’s indolent nature and its ability to mimic benign lesions make clinical suspicion crucial for early detection [6]. Early and accurate diagnosis of congenital DFSP is imperative due to its infiltrative nature and potential for significant local recurrence if not entirely excised [7]. The tumor tends to infiltrate surrounding tissues, including subcutaneous fat, muscle, and even bone in advanced cases [7]. This aggressive local behavior necessitates complete surgical excision with clear margins to minimize the risk of recurrence [8]. In pediatric patients, achieving clear margins while preserving function and minimizing disfigurement adds an additional layer of complexity to management. The standard treatment for DFSP is wide local excision (WLE) with margins ranging from 2 to 5 centimeters, depending on the tumor size and location. However, in children, especially infants, such extensive surgery can be challenging due to the smaller size of anatomical structures and the potential impact on growth and development. [7,8,9]. Mohs micrographic surgery (MMS) has emerged as a tissue-sparing alternative that allows for the complete removal of the tumor while conserving as much healthy tissue as possible. MMS involves the systematic excision and microscopic examination of the tumor margins during surgery, providing a higher likelihood of achieving negative margins with less extensive tissue removal [10]. The rarity of congenital DFSP and its variable clinical presentation underscore the importance of heightened clinical vigilance [2,3]. Clinicians, including pediatricians and dermatologists, should maintain a high index of suspicion when evaluating skin lesions present at birth or arising in early infancy, especially those that do not regress or respond to standard treatments [11]. Biopsy and histopathological examination are essential for accurate diagnosis [7]. Histologically, DFSP is characterized by a storiform pattern of spindle-shaped cells and strong positivity for CD34 on immunohistochemical staining [12]. Molecular studies may reveal a characteristic chromosomal translocation t(17;22)(q22;q13), resulting in the COL1A1-PDGFB fusion gene, which plays a role in tumorigenesis [12,13]. This narrative review aims to dissect the complexities associated with the diagnosis and management of congenital DFSP, emphasizing the critical role of clinical awareness and timely intervention. By reviewing relevant literature, including case reports and series, we seek to enhance clinicians’ ability to recognize this rare malignancy early. Early recognition can lead to prompt and appropriate treatment, potentially reducing the need for extensive surgical interventions and improving long-term outcomes for affected children [10,11]. In addition to discussing the clinical features and diagnostic strategies, this review will explore the challenges in differentiating congenital DFSP from its benign mimickers [14]. We will examine the roles of imaging modalities, such as ultrasound and MRI, in the evaluation of suspected cases, and the importance of multidisciplinary collaboration among dermatologists, pediatric surgeons, oncologists, and pathologists in managing this condition [7,15]. Furthermore, we will address the psychological and developmental considerations unique to pediatric patients with DFSP. The impact of surgery on growth, function, and appearance is a significant concern, necessitating a balance between oncologic control and quality of life [16]. Advances in targeted therapies, such as the use of imatinib mesylate for tumors harboring the COL1A1-PDGFB fusion gene, offer potential adjuncts or alternatives to surgery in select cases, and these will be discussed in the context of current evidence [17].
2. Epidemiology
Congenital DFSP is an exceedingly rare condition, with its true incidence not well defined due to potential underreporting and misdiagnosis [2,3]. The rarity is partly because congenital DFSP can easily be mistaken for more common benign skin lesions present at birth, such as hemangiomas, vascular malformations, or pigmented birthmarks. These benign mimickers often lead to initial diagnostic confusion, causing delays in appropriate treatment [5]. DFSP in general affects adults predominantly in their third to fifth decades of life; however, approximately 6% of cases occur in children. Within this pediatric population, the congenital form specifically presents at birth or within the first year of life, emphasizing the importance of early recognition and intervention to prevent aggressive local growth and potential complications [4,18]. There is no significant gender predilection in congenital DFSP, with studies showing nearly equal representation of males and females [18]. This lack of gender bias suggests that both sexes are equally susceptible to developing the condition, which reinforces the need for clinicians to consider DFSP in all pediatric patients presenting with suspicious skin lesions, regardless of gender [18]. The extreme rarity of the condition means that many clinicians may never encounter a case during their careers, contributing to diagnostic challenges and potential oversight [2,3]. This unfamiliarity underscores the importance of raising awareness about congenital DFSP among healthcare providers. Enhanced education and a high index of suspicion are crucial for early diagnosis, which can lead to more effective management strategies, reduced surgical morbidity, and improved long-term outcomes for affected children.
3. Clinical Presentations
3.1. Lesion Characteristics
It presents a variety of morphological characteristics that often complicate diagnosis. Typically, congenital DFSP appears as a slow-growing, firm plaque or nodule [6]. These lesions can be skin-colored, reddish, purplish, or even bluish, which often leads to confusion with more common vascular lesions such as hemangiomas. Less frequently, congenital DFSP can present as a mass or a pigmented lesion, further adding to the diagnostic challenges, as these presentations can mimic other benign or even malignant conditions [5,19].
3.2. Common Sites (Table 1)
Lesions can occur anywhere on the body, but they are most frequently found on the trunk, followed by the proximal extremities. Certain anatomical sites, particularly in congenital presentations, pose a higher risk of misdiagnosis due to the complexity of the differential diagnosis and the overlap with benign conditions [22,23,27,28,29].
- Genital Area: The genital area has a lower rate of misdiagnosis, possibly due to more thorough evaluations being conducted because of the anatomical sensitivity. Lesions in this region typically prompt careful examination, which aids in correct identification [29].
4. Diagnostic Challenges (Table 2)
4.1. Misdiagnosis
It is particularly challenging to diagnose due to its rare occurrence and its frequent resemblance to benign skin conditions [2,3,5]. As a result, congenital DFSP is often initially misdiagnosed, leading to significant delays in appropriate treatment and adverse patient outcomes [5]. Some of the most common misdiagnoses include:
- Vascular Lesions: DFSP often presents with a reddish or purplish hue, which can easily lead clinicians to suspect vascular anomalies, such as hemangiomas or vascular malformations [30,31]. These benign conditions are common in infants, and DFSP’s similar coloration and presentation can result in inappropriate initial management or conservative follow-up, which delays proper treatment [32].
- Benign Proliferative Lesions: Conditions like hypertrophic scars, keloids, and fibromas are also frequently considered due to their appearance and benign nature [11,20,21]. These lesions are often characterized by localized skin thickening or growth, which may closely resemble DFSP, particularly in its plaque or nodular form. Misclassification as a benign proliferative lesion can lead to an underestimation of the potential seriousness of the condition, delaying the necessary surgical intervention [11,20,21,24].
- Dermatofibromas and Birthmarks: Dermatofibromas are common benign fibrous lesions of the skin, and congenital DFSP may present in a similar manner, with slow-growing plaques or nodules. Birthmarks present from birth can also confuse the diagnosis, particularly when the lesions are not rapidly changing [33]. DFSP lesions present at birth are often assumed to be benign congenital nevi or vascular birthmarks, leading to diagnostic errors [5,33].
4.2. Factors Contributing to Misdiagnosis
Several factors contribute to the frequent misdiagnosis of congenital DFSP, including:
Rarity of the Condition: Congenital DFSP is exceptionally rare, and its occurrence is something that many general practitioners, dermatologists, and pediatricians may never encounter during their careers. This lack of familiarity leads to an understandable but significant diagnostic gap. When faced with an unusual lesion, clinicians may be more inclined to diagnose more common, benign conditions rather than consider a rare sarcoma [2,3,5].
Variable Clinical Presentation: Congenital DFSP has a wide range of appearances, including skin-colored, reddish, purplish, or bluish plaques or nodules. The variability of presentation, particularly when the lesion mimics other benign conditions, creates diagnostic confusion [11,20,21,22,23,24]. The slow growth pattern of DFSP also contrasts with what many clinicians associate with malignant lesions, adding to the diagnostic difficulty [34].
Anatomical Complexity: The location of congenital DFSP lesions plays an important role in diagnosis. Lesions located in the head and neck or lower limbs are particularly challenging due to the anatomical complexity and the number of benign entities that present similarly in these areas. For example, a lesion in the head and neck may be mistaken for a benign cyst or vascular malformation due to the wide range of benign masses typically seen in this region [5,11,22,23,27].
15) Overlapping Symptoms: Both benign and malignant lesions may exhibit slow growth, firm texture, and a lack of alarming symptoms such as pain or rapid change. The indolent nature of DFSP, with its characteristic slow but steady progression, often leads to a false sense of security among clinicians and parents alike, leading to delays in further investigation [5,34,35].
4.3. Importance of Early Diagnosis
The importance of early diagnosis in congenital DFSP cannot be overstated. When diagnosis is delayed, there are several negative outcomes that become more likely, including:
- Increased Tumor Size: Due to its indolent but steady growth, congenital DFSP that is not recognized early can grow significantly in size before proper treatment is initiated. As the lesion increases in size, it becomes more complex to treat, often involving deeper invasion into underlying tissues, including muscle and sometimes even bone [7,8].
- More Extensive Surgery: Early diagnosis allows for a more conservative approach to surgical excision. However, as the lesion grows larger, wider excision becomes necessary to ensure complete removal and prevent recurrence. The larger the surgical excision, the more tissue must be sacrificed, which can lead to greater functional limitations, increased morbidity, and a more noticeable cosmetic defect [7,8,9].
- Higher Risk of Recurrence: DFSP is locally aggressive, with a high tendency to recur if not entirely removed. The risk of recurrence is increased significantly if initial surgical excision is incomplete, which can occur more frequently when the diagnosis is delayed. Early, precise surgical management, particularly using techniques like Mohs micrographic surgery, is key to minimizing recurrence [7,8,10].
- Psychological Impact: The need for larger surgeries and the potential for recurrence have significant psychological consequences, particularly in pediatric patients. Visible scars and potential disfigurement can have a lasting impact on a child’s self-esteem and quality of life. This highlights the importance of early, precise intervention that minimizes scarring and preserves as much healthy tissue as possible [16].
5. Diagnostic Approach (Figure 1)
- 20)Clinical Evaluation: The diagnostic approach to congenital DFSP begins with a thorough clinical evaluation. A high index of suspicion is paramount, particularly when clinicians encounter congenital skin lesions that exhibit atypical features or fail to respond to conventional treatments. Congenital DFSP often mimics benign lesions, such as hemangiomas or dermatofibromas, making a cautious and investigative approach essential [30,31,33]. Clinicians should be alert to slow-growing, firm plaques or nodules, especially those that do not resolve or behave atypically over time [6,36]. A detailed patient history and examination are also critical components of clinical evaluation [11]. Assessing the growth rate, characteristics of the lesion (e.g., color, firmness, location), and noting any changes over time can help differentiate DFSP from more common benign conditions. The presence of a lesion at birth that slowly grows, remains persistent, or becomes more irregular should prompt further investigation [3,9,34].
- Biopsy and Histopathology: An early biopsy is recommended for any congenital lesion that appears atypical or shows no response to initial treatments. A biopsy provides definitive information regarding the nature of the lesion [7]. Histopathologically, DFSP is characterized by spindle-shaped cells arranged in a storiform or cartwheel pattern, an important distinguishing feature [12]. Immunohistochemistry is also valuable; DFSP usually shows strong CD34 positivity, which serves as a useful diagnostic marker to differentiate it from other skin conditions [12]. Additionally, molecular testing can be instrumental in confirming a DFSP diagnosis. The detection of the COL1A1-PDGFB fusion gene—resulting from a characteristic chromosomal translocation—confirms the diagnosis and can aid in planning targeted therapy in advanced cases [12,13].
- Imaging Studies: For a comprehensive assessment of the lesion, imaging studies like MRI and CT scans may be utilized, particularly when the lesion involves complex anatomical areas or deeper tissue layers. MRI provides detailed images that can help evaluate the extent of soft tissue involvement, while CT scans can be useful in assessing the depth of invasion and involvement of surrounding structures. These imaging modalities are essential for surgical planning, especially in cases where the lesion is extensive or involves critical areas such as the head, neck, or extremities. Imaging helps delineate the tumor margins, providing crucial information that guides the extent of surgical excision needed to achieve negative margins and minimize recurrence risk [7,15].
6. Treatment
6.1. Surgical Management
6.2. Adjuvant Therapies
6.3. Multidisciplinary Approach
6.4. Prognosis and Follow-Up
7. Recommendations for Clinicians
Congenital DFSP is an uncommon but potentially serious condition that requires a high level of clinical awareness to ensure timely and effective treatment. Given the challenges associated with its diagnosis and management, the following recommendations are aimed at helping clinicians optimize patient outcomes [38].
- Maintain Vigilance:
Clinicians should maintain a high index of suspicion for congenital DFSP in the differential diagnosis of congenital skin lesions with atypical features, particularly those that are persistent, slow-growing, or unresponsive to standard treatments [3,9,34,38]. Given its rarity and resemblance to more common benign conditions like vascular malformations, dermatofibromas, or congenital nevi, DFSP is often overlooked [5,6,11,33]. Clinicians should approach congenital lesions that exhibit irregular growth or unusual characteristics with caution, considering a broader differential that includes malignant possibilities [7].
- Early Intervention:
Is critical to improving outcomes in congenital DFSP. A prompt biopsy is recommended for any congenital skin lesion that appears suspicious, does not respond to initial management, or demonstrates unusual growth [18,24]. A biopsy, followed by histopathological examination, can provide definitive information about the lesion, facilitating early treatment [7,12]. Early diagnosis not only ensures the correct identification of the lesion but also limits the need for more extensive surgical procedures that may be required if the tumor is allowed to grow unchecked [10,11,32].
- Patient Education:
Educating families is a crucial component of managing congenital DFSP. Families should be informed about the importance of early diagnosis, the need for further testing when skin lesions do not behave as expected, and the various treatment options available, including surgery [7,8,10]. Open communication with families helps ensure compliance with follow-up care, reduces anxiety, and allows parents to understand the rationale behind surgical intervention and the importance of monitoring for recurrence [16,32].
- Optimize Surgical Outcomes:
The treatment of congenital DFSP often involves surgery, and it is important to balance oncological control with minimizing morbidity, particularly in pediatric patients [7,8,10]. Optimizing surgical outcomes includes employing tissue-sparing techniques, such as Mohs micrographic surgery when possible. This approach enables precise removal of the tumor while conserving as much healthy tissue as possible, which is particularly significant in growing children where functional and aesthetic outcomes are a major concern [10]. When Mohs surgery is not available, wide local excision with histopathological margin assessment should be performed to reduce the risk of recurrence while considering the impact on the child’s development and quality of life [7,8].
8. Conclusions
In conclusion, misdiagnosis of skin lesions is a significant clinical issue frequently documented in the literature. Skin tumors can often mimic other dermatological conditions, making early and accurate diagnosis a critical challenge for physicians [39-46]. In this context, congenital DFSP represents a rare but significant challenge in pediatric dermatology due to its unusual presentation and its tendency to mimic benign skin conditions, such as vascular malformations, hemangiomas, or congenital nevi [2,3,19,30,31]. The rarity of congenital DFSP, combined with its typically subtle early presentation, often leads to misdiagnosis or delayed recognition [2,3,5]. As a result, many children with congenital DFSP experience treatment delays that can contribute to more extensive surgical requirements, an increased risk of recurrence, and greater overall morbidity [6,7]. Early recognition and accurate diagnosis are of paramount importance in managing congenital DFSP effectively [6]. Unlike more common benign lesions that are typically managed conservatively, DFSP requires definitive surgical intervention [7,10]. The indolent but infiltrative nature of DFSP can result in considerable tissue invasion if not treated promptly. Early diagnosis allows for smaller, more tissue-sparing surgical procedures, significantly reducing the risk of long-term functional and cosmetic impairment in pediatric patients [6,10,11,13]. Wide local excision, ideally performed with Mohs micrographic surgery to ensure complete removal while minimizing healthy tissue loss, remains the cornerstone of treatment [7,8,9,10]. The role of the clinician is pivotal in ensuring early detection. General practitioners, pediatricians, and dermatologists should maintain a high index of suspicion when evaluating congenital skin lesions that present atypical features or fail to respond as expected to standard therapies [3,9,34,38]. Any lesion that continues to grow, fails to regress, or presents with features such as firmness, irregular growth, or discoloration warrants closer evaluation and an early biopsy. Awareness of congenital DFSP among healthcare providers can lead to timely histopathological examination, allowing for definitive diagnosis and appropriate management [7,12]. A multidisciplinary approach is essential in managing congenital DFSP. The rarity and complexity of the condition necessitate collaboration across multiple specialties, including dermatology, pediatric surgery, pathology, and oncology. Dermatologists play a crucial role in identifying suspicious lesions, while pediatric surgeons are instrumental in executing precise, tissue-sparing excisions that limit disfigurement and functional impairment [15]. Pathologists confirm the diagnosis via histopathological examination and immunohistochemistry, while oncologists may be involved in cases where advanced or recurrent disease requires targeted therapies. Such a collaborative effort ensures that every aspect of the patient’s care is optimized to yield the best possible outcome [7,12,15]. In addition to medical and surgical management, the psychological and developmental impact of congenital DFSP should not be overlooked [16]. Surgical excision, particularly of large or prominent lesions, can have significant implications for the child’s physical appearance and psychological well-being [7]. Therefore, providing psychosocial support to the patient and their family is vital to alleviate anxiety and foster a positive outlook toward treatment and recovery. Parents must be educated about the importance of early detection, treatment options, and long-term follow-up to manage expectations and encourage adherence to medical advice. [16,32]. Finally, long-term follow-up is necessary to ensure that patients do not experience local recurrence, which can occur even after seemingly complete excision. Regular clinical assessments are essential for monitoring the treatment site and ensuring prompt intervention should a recurrence be detected [38]. With heightened clinical awareness, proactive diagnostic strategies, and a well-coordinated multidisciplinary approach, the prognosis for patients with congenital DFSP can be significantly improved [15]. Early intervention not only reduces the need for more aggressive treatments but also minimizes the potential for long-term morbidity, thereby enhancing the quality of life for affected children and their families [10,11,32]. By following these recommendations and focusing on early detection and comprehensive management, clinicians can help overcome the diagnostic challenges presented by congenital DFSP and contribute to better health outcomes for this vulnerable population [11,32]. To conclude we present an operational flow chart for pediatricians and dermatologists to aid in the diagnosis of DFSP and to prevent potential diagnostic errors or delays (Figure 1).
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Whittle C, Andrews A, Coulon G, Castro A. Different sonographic presentations of dermatofibrosarcoma protuberans. J Ultrasound. 2024;27(1):61-65. [CrossRef]
- Wang Y, Wang Y, Chen R, Tang Z, Liu S. A Rare Malignant Disease, Dermatofibrosarcoma Protuberans of the Breast: A Retrospective Analysis and Review of Literature. Biomed Res Int. 2020;2020:8852182. Published 2020 Nov 9. [CrossRef]
- Mendenhall WM, Zlotecki RA, Scarborough MT. Dermatofibrosarcoma protuberans. Cancer. 2004;101(11):2503-2508. [CrossRef]
- Rubio GA, Alvarado A, Gerth DJ, Tashiro J, Thaller SR. Incidence and Outcomes of Dermatofibrosarcoma Protuberans in the US Pediatric Population. J Craniofac Surg. 2017;28(1):182-184. [CrossRef]
- Dehner LP, Gru AA. Nonepithelial Tumors and Tumor-like Lesions of the Skin and Subcutis in Children. Pediatr Dev Pathol. 2018;21(2):150-207. [CrossRef]
- Han HH, Lim SY, Park YM, Rhie JW. Congenital Dermatofibrosarcoma Protuberans: A Case Report and Literature Review. Ann Dermatol. 2015;27(5):597-600. [CrossRef]
- Ramirez-Fort MK, Meier-Schiesser B, Niaz MJ, et al. Dermatofibrosarcoma Protuberans: The Current State of Multidisciplinary Management. Skinmed. 2020;18(5):288-293. Published 2020 Oct 1.
- Rust DJ, Kwinta BD, Geskin LJ, Samie FH, Remotti F, Yoon SS. Surgical management of dermatofibrosarcoma protuberans. J Surg Oncol. 2023;128(1):87-96. [CrossRef]
- Lindner NJ, Scarborough MT, Powell GJ, Spanier S, Enneking WF. Revision surgery in dermatofibrosarcoma protuberans of the trunk and extremities. Eur J Surg Oncol. 1999;25(4):392-397. [CrossRef]
- Loghdey MS, Varma S, Rajpara SM, Al-Rawi H, Perks G, Perkins W. Mohs micrographic surgery for dermatofibrosarcoma protuberans (DFSP): a single-centre series of 76 patients treated by frozen-section Mohs micrographic surgery with a review of the literature. J Plast Reconstr Aesthet Surg. 2014;67(10):1315-1321. [CrossRef]
- Cheon M, Jung KE, Kim HS, et al. Medallion-like dermal dendrocyte hamartoma: differential diagnosis with congenital atrophic dermatofibrosarcoma protuberans. Ann Dermatol. 2013;25(3):382-384. [CrossRef]
- Hao X, Billings SD, Wu F, et al. Dermatofibrosarcoma Protuberans: Update on the Diagnosis and Treatment. J Clin Med. 2020;9(6):1752. Published 2020 Jun 5. [CrossRef]
- Yang JH, Hu WH, Li F, et al. Zhonghua Bing Li Xue Za Zhi. 2003;32(5):409-412.
- Marcoval J, Moreno-Vílchez C, Torrecilla-Vall-Llosera C, et al. Dermatofibrosarcoma Protuberans: A Study of 148 Patients. Dermatology. 2024;240(3):487-493. [CrossRef]
- Mujtaba B, Wang F, Taher A, et al. Dermatofibrosarcoma Protuberans: Pathological and Imaging Review. Curr Probl Diagn Radiol. 2021;50(2):236-240. [CrossRef]
- Gurevitch D, Kirschenbaum SE. Dermatofibrosarcoma protuberans. Salvaging quality of life using two approaches to treatment. J Am Podiatr Med Assoc. 1996;86(9):439-446. [CrossRef]
- Penel N, El Bedoui S, Robin YM, Decanter G. Dermatofibrosarcome : prise en charge [Dermatofibrosarcoma: Management]. Bull Cancer. 2018;105(11):1094-1101. [CrossRef]
- Kreicher KL, Kurlander DE, Gittleman HR, Barnholtz-Sloan JS, Bordeaux JS. Incidence and Survival of Primary Dermatofibrosarcoma Protuberans in the United States. Dermatol Surg. 2016;42 Suppl 1:S24-S31. [CrossRef]
- Kim JW, Kim JE, Song HJ, Oh CH. Congenital Bednar’s tumour. Clin Exp Dermatol. 2009;34(5):e85-e87. [CrossRef]
- Weinstein JM, Drolet BA, Esterly NB, et al. Congenital dermatofibrosarcoma protuberans: variability in presentation. Arch Dermatol. 2003;139(2):207-211. [CrossRef]
- Thornton SL, Reid J, Papay FA, Vidimos AT. Childhood dermatofibrosarcoma protuberans: role of preoperative imaging. J Am Acad Dermatol. 2005;53(1):76-83. [CrossRef]
- Bouaoud J, Fraitag S, Soupre V, et al. Congenital fibroblastic connective tissue nevi: Unusual and misleading presentations in three infantile cases. Pediatr Dermatol. 2018;35(5):644-650. [CrossRef]
- Jafarian F, McCuaig C, Kokta V, Laberge L, Ben Nejma B. Dermatofibrosarcoma protuberans in childhood and adolescence: report of eight patients. Pediatr Dermatol. 2008;25(3):317-325. [CrossRef]
- Kutzner H, Mentzel T, Palmedo G, et al. Plaque-like CD34-positive dermal fibroma ("medallion-like dermal dendrocyte hamartoma"): clinicopathologic, immunohistochemical, and molecular analysis of 5 cases emphasizing its distinction from superficial, plaque-like dermatofibrosarcoma protuberans. Am J Surg Pathol. 2010;34(2):190-201. [CrossRef]
- Suzuki D, Kobayashi R, Yasuda K, et al. Congenital dermatofibrosarcoma protuberans in a newborn infant with a massive back tumor: favorable effects of oral imatinib on the control of residual tumor growth. J Pediatr Hematol Oncol. 2011;33(7):e304-e306. [CrossRef]
- Bernárdez C, Molina-Ruiz AM, Requena L. Bednar Tumor Mimicking Congenital Melanocytic Nevus. Tumor de Bednar simulando nevus melanocítico congénito. Actas Dermosifiliogr. 2016;107(6):523. [CrossRef]
- Karagianni P, Lambropoulos V, Stergidou D, Fryssira H, Chatziioannidis I, Spyridakis I. Recurrent giant cell fibroblastoma: Malignancy predisposition in Kabuki syndrome revisited. Am J Med Genet A. 2016;170A(5):1333-1338. [CrossRef]
- Tallegas M, Fraitag S, Binet A, et al. Novel KHDRBS1-NTRK3 rearrangement in a congenital pediatric CD34-positive skin tumor: a case report. Virchows Arch. 2019;474(1):111-115. [CrossRef]
- Eisner BH, McAleer SJ, Gargollo PC, Perez-Atayde A, Diamond DA, Elder JS. Pediatric penile tumors of mesenchymal origin. Urology. 2006;68(6):1327-1330. [CrossRef]
- Checketts SR, Hamilton TK, Baughman RD. Congenital and childhood dermatofibrosarcoma protuberans: a case report and review of the literature. J Am Acad Dermatol. 2000;42(5 Pt 2):907-913. [CrossRef]
- El Hachem M, Diociaiuti A, Latella E, et al. Congenital myxoid and pigmented dermatofibrosarcoma protuberans: a case report. Pediatr Dermatol. 2013;30(5):e74-e77. [CrossRef]
- Kunimoto K, Yamamoto Y, Jinnin M. ISSVA Classification of Vascular Anomalies and Molecular Biology. Int J Mol Sci. 2022;23(4):2358. Published 2022 Feb 21. [CrossRef]
- Gu W, Ogose A, Kawashima H, et al. Congenital dermatofibrosarcoma protuberans with fibrosarcomatous and myxoid change. J Clin Pathol. 2005;58(9):984-986. [CrossRef]
- Cabral R, Wilford M, Ramdass MJ. Dermatofibrosarcoma protuberans associated with trauma: A case report. Mol Clin Oncol. 2020;13(5):51. [CrossRef]
- Reddy C, Hayward P, Thompson P, Kan A. Dermatofibrosarcoma protuberans in children. J Plast Reconstr Aesthet Surg. 2009;62(6):819-823. [CrossRef]
- Menon G, Brooks J, Ramsey ML. Dermatofibrosarcoma Protuberans. In: StatPearls. Treasure Island (FL): StatPearls Publishing; April 18, 2024.
- Henry OS, Platoff R, Cerniglia KS, et al. Tyrosine kinase inhibitors versus radiation therapy in unresectable dermatofibrosarcoma protuberans (DFSP): A narrative systematic review. Am J Surg. 2023;225(2):268-274. [CrossRef]
- Alshaygy I, Mattei JC, Basile G, et al. Outcome After Surgical Treatment of Dermatofibrosarcoma Protuberans (DFSP): Does it Require Extensive Follow-up and What is an Adequate Resection Margin?. Ann Surg Oncol. 2023;30(5):3106-3113. [CrossRef]
- Cassalia F, Cavallin F, Danese A, et al. Soft Tissue Sarcoma Mimicking Melanoma: A Systematic Review. Cancers (Basel). 2023 Jul 12;15(14):3584. [CrossRef] [PubMed]
- Cassalia F, Danese A, Cocchi E, et al. Misdiagnosis and Clinical Insights into Acral Amelanotic Melanoma-A Systematic Review. J Pers Med. 2024 May 13;14(5):518. [CrossRef] [PubMed]
- Al-Farsi A, Al-Brashdi A, Al-Salhi S, et al Dermatofibrosarcoma Protuberans Mimicking Primary Breast Neoplasm: A case report and literature review. Sultan Qaboos Univ Med J. 2020 Aug;20(3):e368-e371. Epub 2020 Oct 5. [CrossRef] [PubMed]
- Alsharif TH, Gronfula A, Alanazi AT, et al. Dermatofibrosarcoma Protuberans of the Scalp Mimicking Trichilemmal Cyst: A Case Report. Cureus. 2023 May 21;15(5):e39315. [CrossRef] [PubMed]
- Suyama T, Yokoyama M, Matsushima J, et al. Dermatofibrosarcoma protuberance with a unique appearance mimicking neurofibroma arising from a conventional area. Int Cancer Conf J. 2024 Jun 15;13(4):382-386. [CrossRef] [PubMed]
- Fujisawa Y, Furuta J, Kawachi Y. Dermatofibrosarcoma protuberans mimicking cutaneous sarcoidosis in a patient with lung sarcoidosis. Eur J Dermatol. 2014 Mar-Apr;24(2):276-7. [CrossRef] [PubMed]
- Cohen PR, Riahi RR. Cutaneous metastases mimicking keratoacanthoma. Int J Dermatol. 2014 May;53(5):e320-2. Epub 2013 Nov 21. [CrossRef] [PubMed]
- Boyuk E, Saracoğlu ZN, Arık D. Cutaneous Leiomyoma Mimicking a Keloid. Acta Dermatovenerol Croat. 2020 Aug;28(2):116. [PubMed]
Figure 1.
Operative flowchart to aid in the diagnosis of DFSP.
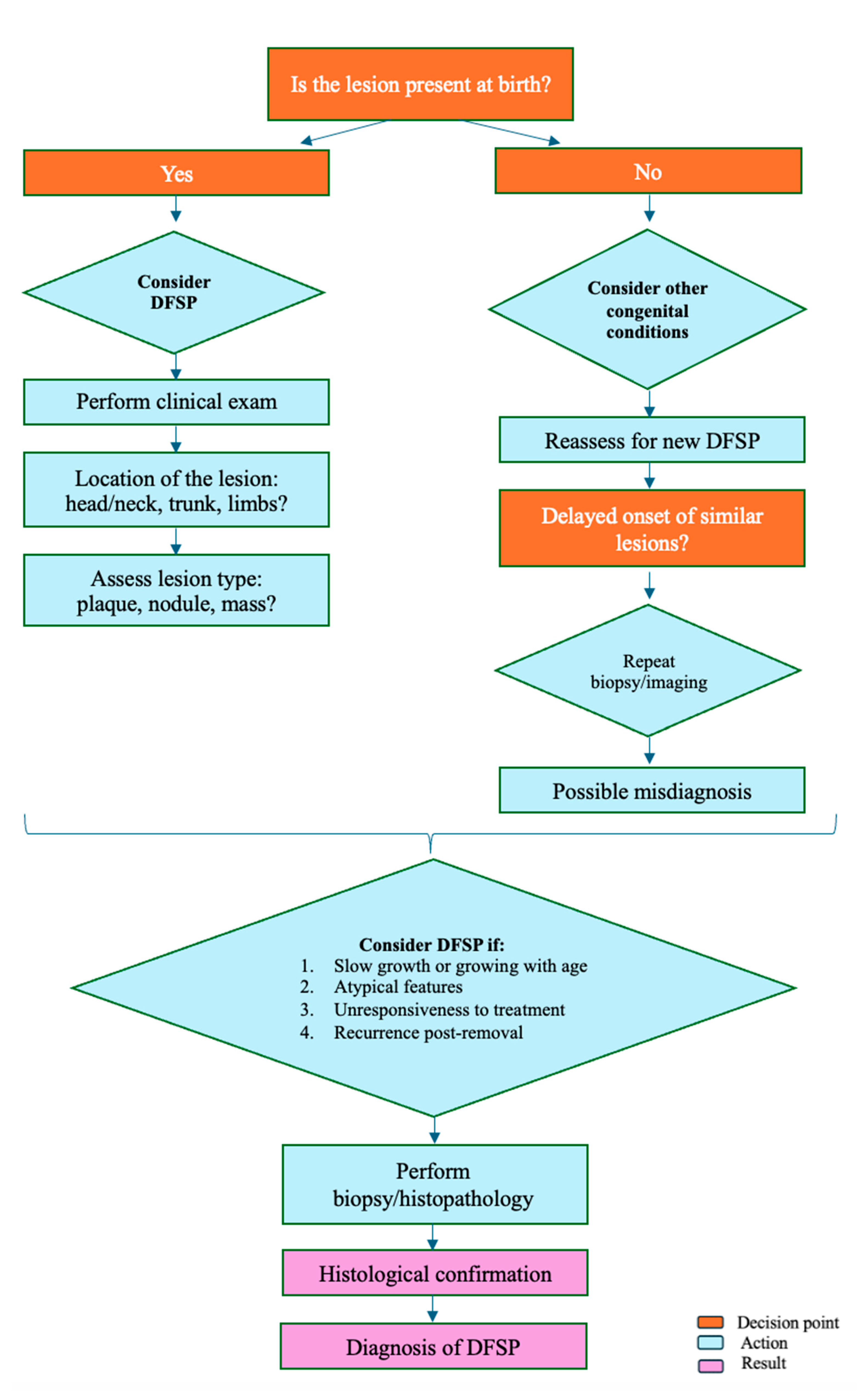

Table 1.
Clinical Characteristics of Congenital DFSP.
| Lesion Type | Description | Differential Diagnoses | Ref |
|---|---|---|---|
| Plaques | Flat or slightly raised, firm areas | Dermatofibromas, keloids, hypertrophic scars | 11,20,21 |
| Nodules | Firm, well-circumscribed masses | Lipomas, cysts, neurofibromas | 22,23,24 |
| Masses | Larger, more prominent growths | Sarcomas, deep-seated lipomas | 22,23,25 |
| Pigmented Lesions | Darker-colored lesions resembling melanocytic nevi or melanoma | Pigmented nevi, melanoma | 19,26 |
Table 2.
Common Misdiagnoses of Congenital DFSP.
| Category of Misdiagnosis | Reason for Misdiagnosis | Clinical Implications | Ref |
|---|---|---|---|
| Vascular Lesions:- Hemangiomas - Vascular Malformations | Similar coloration (reddish, purplish, bluish), common in neonates and infants | Inappropriate initial management. Delayed diagnosis of malignant potential | 30,31 |
| Benign Lesions:- Hypertrophic Scars - Keloids Fibromas | Similar appearance as firm, raised growths, benign nature often leads to underestimation of severity | Assumption of non-malignancy results in delayed treatment and potential lesion growth | 20,21 |
| Dermatofibromas | Slow-growing, firm plaques resembling benign congenital skin lesions | Misinterpretation as a common benign lesion can prevent timely biopsy and histopathological confirmation | 11 |
| Pigmented Lesions | Presence of pigmentation resembling other benign or even malignant pigmented lesions | Delayed accurate diagnosis due to misclassification as benign nevi or melanoma | 19,26 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



