Submitted:
01 November 2024
Posted:
01 November 2024
You are already at the latest version
Abstract
Objective: To investigate the effects of sevoflurane combined with propofol continuous anaesthesia on anaesthesia and postoperative analgesia and recovery in elderly patients undergoing lower limb fracture surgery.Methods: In this study, 344 elderly patients who underwent surgical treatment for lower limb fractures in our hospital between June 2020 and May 2022 were enrolled for prospective analysis, and the patients were equally divided into a control group and an experimental group by the random number table method, with 172 patients in each group.In the control group, continuous anaesthesia with propofol was used, while in the experimental group, continuous anaesthesia with sevoflurane and propofol was used. The anesthetic effect, postoperative analgesic effect, recovery effect and adverse reactions of the patients in the two groups were compared.Results: The excellent anesthesia rate in the experimental group was significantly higher than that in the control group (P<0.05); VAS scores at T1, T2, T3 and T4 were significantly lower in the experimental group than in the control group (P>0.05); Time to awaken, time to extubation and time to leave the anesthesia recovery room were all significantly lower in the experimental group than in the control group (P<0.05); The difference in the incidence of postoperative adverse reactions between the two groups was not statistically significant (P>0.05).Conclusion: Sevoflurane combined with propofol continuous anaesthesia is ideal for anaesthesia in elderly patients undergoing lower limb fracture surgery. This protocol is effective in suppressing postoperative pain and facilitating recovery from anaesthesia and does not increase the risk of postoperative adverse effects in patients.
Keywords:
Sevoflurane
; Propofol
; Continuous anaesthesia
; Elderly
; Lower limb fractures
; Surgery
; Anaesthetic outcome
; Postoperative analgesia and recovery
1. Introduction
Lower limb fractures are a frequent orthopaedic disorder in the elderly [1]. Due to the age of the elderly, the bone density of the body gradually decreases with age and the fragility of the bones gradually increases, which makes the elderly population vulnerable to fractures when they are hit by external forces [2]. Studies have demonstrated that patients with lower limb fractures should be treated immediately and effectively to minimise further deterioration of the fracture [3], as lower limb fractures may have serious physical and psychological consequences, and some patients with severe fractures may suffer from permanent disability.At present, the treatment of lower limb fractures is mainly surgical [4], but due to the relatively low tolerance of surgery and anaesthesia in the elderly population, and the possible combination of coronary heart disease, diabetes and other serious underlying diseases, the risk of surgery in this group is greatly increased compared to that of young adults [5]. Therefore, when dealing with elderly patients, a safe and efficient anaesthetic plan should be developed according to the patient's condition and their actual situation, thus helping to reduce the risk of surgery and further improve the effectiveness of surgical treatment [6].
Propofol is a commonly used anesthetic drug in clinical practice. It has the characteristics of rapid onset of action and ideal recovery from anesthesia, and it has been used in clinical practice for many years and its safety has been widely recognized [7]. Sevoflurane, a new type of inhaled general anaesthetic, is characterised by its lack of taste irritation and low blood gas distribution coefficient, which makes it suitable for rapid induction of anaesthesia under the mask during surgery in elderly patients due to its weak irritation of the patient's airways [8].Studies have shown that sevoflurane can effectively maintain haemodynamic stability during surgical anaesthesia in elderly patients,which could open up a new clinical approach to anaesthesia [9]. Based on the above reasons, 344 elderly patients undergoing surgical treatment for lower limb fractures in our hospital between June 2020 and May 2022 were selected for prospective analysis in this study, with the aim of analyzing the effects of sevoflurane combined with propofol continuous anesthesia on anesthesia and postoperative analgesia and recovery in elderly patients undergoing lower limb fracture surgery.
2. Materials and Methods
2.1. General Information
In this study, 344 elderly patients who underwent surgical treatment for lower limb fractures in our hospital between June 2020 and May 2022 were enrolled for the seventh anniversary extension analysis.General information on the patients including gender, age, body mass (BMI), anesthesia classification and surgical site were collected. The patients were equally divided into a control group and an experimental group by the random number table method, with 172 cases in each group.The study was approved by the ethics committee of Handan Central Hospital, No.19297593.
2.2. Inclusion and Exclusion Criteria
2.2.1. Inclusion Criteria
- (1)
- All patients were >60 years of age.
- (2)
- Patients who were diagnosed with the presence of a lower limb fracture by relevant orthopaedic diagnostic findings.
- (3)
- Patients who recived treatement in our hospital for the relevant surgery.
- (4)
- Patients who were graded as grade I-II in anaesthesia.
- (5)
- Patients and their families were informed and voluntarily signed the relevant informed consent forms for this study.
2.2.2. Exclusion Criteria
- (1)
- Patients with contraindications related to surgery or anaesthesia.
- (2)
- Patients with abnormalities in coagulation and metabolic function.
- (3)
- Patients with combined malignancy.
- (4)
- Patients with immune disorders of the organism.
- (5)
- Patients with combined psychiatric disorders or communication disorders.
- (6)
- Patients and family members who were unable to cooperate fully with this study for various reasons.
2.3. Methods
Patients in both groups underwent routine pre-operative fasting and were given mask oxygenation, as well as routine pre-operative measures such as establishing intravenous access and cardiac monitoring of blood pressure, heart rate and oxygen saturation.
- (1) Control group: In the control group, the patient is first given preoperative intravenous dexmedetomidine hydrochloride (Jiangsu Hengrui Medicine Co., Ltd., Nation Drug Administration NO.H20090248) at a dose of 0.5 ug/kg, requiring slow sedation for 10 minutes; Then patients were administered an intravenous drip of 1.5mg of midazolam (Jiangsu Enhua Pharmaceutical Co., Ltd., Nation Drug Administration NO.H20143222) for induction of anaesthesia; After the patient's muscles had relaxed, tracheal intubation was performed and respiratory parameters were set with a tidal volume of 8 ml/kg and intraoperative oxygen saturation maintained at >98%, moreover, dexmedetomidine is continuously pumped at 0.5 ug/(kg·h); Subsequently, patients were offered propofol (Hebei Yipin Pharmaceutical Co., Ltd., Nation Drug Administration NO.H20093542) as a continuous pump anaesthetic with a maintenance anaesthetic of 2 mg/kg.
- (2) Experimental group: In the experimental group, sevoflurane (Shandong New Age Pharmaceutical Co., Ltd., Nation Drug Administration NO.H20080680) was combined with anaesthesia protocol in the control group, and the concentration of sevoflurane was adjusted to 5% and inhaled continuously through an airtight mask by patients.
2.4. Observed Indicators
- (1) Anaesthetic outcome. Excellent: no adverse stress reactions in the patient, ideal intraoperative muscle relaxation, stable intraoperative haemodynamics, overall smooth procedure. Good: patients with controllable adverse stress reactions, fair degree of intraoperative muscle relaxation, relatively stable intraoperative haemodynamics, overall smooth procedure; General: patients with uncontrollable adverse stress reactions, fair intraoperative muscle relaxation, significant intraoperative haemodynamic fluctuations and an overall uneventful procedure; Poor: patients with uncontrollable adverse stress reactions requiring adjunctive pharmacological interventions.
- (2) Postoperative analgesic effects. Patients' analgesia was assessed using the Visual Analogue Pain Scale (VAS) at 3h (T1), 6h (T2), 12h (T3) and 1d (T4) postoperatively. The scale is scored out of 10, with a higher score indicating a more severe pain condition.
- (3) Recovery from anaesthesia. The indicators of recovery from anaesthesia were (time to awaken, time to extubation and time to leave the recovery room), all of which were recorded by the relevant medical and nursing staff in our hospital.
- (4) Adverse reactions. Adverse reactions to anaesthetic drugs in patients include nausea and vomiting, bradycardia, respiratory depression, pruritus and drowsiness.
2.5. Statistical Analysis
The data of this study were collated and analysed using SPSS 22.0. The measurement data were expressed as mean ± standard deviation (±s) and compared using t-test; the count data were expressed as number of cases (%) and tested using x². P<0.05 indicates that the comparison is statistically significant. GraphPad Prism 8 was used as the graphing software.
3. Results
3.1. General Information
In the control group, there were 94 male and 78 female patients; age 61-84 years, mean age (71.19±4.36); BMI range was 19-26 kg/m², mean BMI (22.37±1.82) kg/m²; anaesthetic classification was grade I in 77 cases and grade II in 95 cases; surgical sites were femoral neck in 64 cases, femoral trochanter in 71 cases and tibiofibular in 37 cases. In the experimental group, there were 97 male and 75 female patients; age 62-85 years, mean age (71.26±4.41) years; BMI range was 19-27 kg/m², mean BMI (22.46±1.93) kg/m²; anaesthetic classification was grade I in 79 cases and grade II in 93 cases; surgical sites were femoral neck in 61 cases, femoral trochanter in 76 cases and tibiofibular in 35 cases. The general information of the two groups of patients was comparable and there was no significant difference in their comparison (P>0.05) see Table 1.
3.2. Comparison of Anesthesia Effect
The excellent anesthesia rate of patients in the control group was 84.9% (146/172), of which 68 cases were excellent, 78 cases were good, 21 cases were general and 5 cases were poor; the excellent anesthesia rate of patients in the experimental group was 97.1% (167/172), of which 75 cases were excellent, 92 cases were good, 4 cases were general and 1 case was poor. The excellent anesthesia rate of the experimental group was significantly higher than that of the control group (P<0.05), as detailed in Table 2.
3.3. Comparison of Analgesic Effects at Individual Postoperative Time Points
As shown in Figure 1, the VAS scores at T1, T2, T3 and T4 in the control group were (3.29±0.62, 3.48±0.61, 3.73±0.71, 4.33±0.75); the VAS scores at T1, T2, T3 and T4 in the experimental group were (2.72±0.54, 2.83±0.54, 3.12±0.61, 3.63± 0.66). The VAS scores at T1, T2, T3 and T4 were significantly lower in the experimental group than in the control group (P>0.05).
3.4. Comparison of Anesthesia Recovery Effects
As shown in Figure 2, the awakening time, extubation time and time to leave the recovery room were (12.84±5.16, 16.23±6.38 and 53.69±10.28) in the control group and (11.32±4.65, 13.41±5.26 and 48.67±9.06) in the experimental group respectively. The time to awaken, time to extubation and time to leave the recovery room were all significantly lower in the experimental group than in the control group (P<0.05).
3.5. Comparison of Adverse Reactions
The incidence of adverse reactions in the control group was 16.9% (29/172), including 9 cases of nausea and vomiting, 6 cases of bradycardia, 2 cases of respiratory depression, 7 cases of skin pruritus and 5 cases of drowsiness. The difference in the incidence of postoperative adverse reactions between the two groups was not statistically significant (P > 0.05), see Table 3 for details.
4. Discussion
Due to the increasing ageing of our population, the incidence of lower limb fractures in the elderly is also showing a trend of increasing year by year. The occurrence of this disease can lead to severe pain, thus seriously affecting the daily life of patients [10]. Surgery is the most common clinical treatment for lower limb fractures, but due to the degeneration of the organs of the body and the combination of various underlying chronic diseases in elderly patients, it is difficult for them to tolerate the trauma caused by surgery and anaesthesia, especially in patients with combined cardiovascular and cerebrovascular diseases, who are prone to adverse stress reactions during surgical anaesthesia, which makes the risk of surgery significantly higher [11]. The choice of anaesthetic drug is a major factor in determining the outcome of the operation and the patient's prognosis for recovery. Different intraoperative anaesthetic drugs have different effects on the patient's organism, so the choice of anaesthetic drugs and doses needs to be more careful in elderly patients undergoing surgery for lower limb fractures [12]. Propofol is widely recognized as a short-acting intravenous anesthetic induction and maintenance drug of the alkylate class. Propofol can effectively reduce cortisol concentrations and sympathetic nervous system activity in patients, but it may also lead to disturbances in oxygen metabolism in the human brain [13]. Sevoflurane is a new inhalation-induced anaesthetic drug that is gently dosed, smoothly acting and well suited to deep anaesthetic regulation, and has the advantages of rapid recovery from anaesthesia and less tracheal irritation [14]. It has also been shown that the use of sevoflurane can further enhance the muscle relaxation effect caused by non-depolarising muscle relaxants, thus helping to improve the puncture success rate and anaesthetic effect of compound anaesthesia in patients [15]. To investigate the effects of sevoflurane combined with propofol continuous anaesthesia on anaesthesia and postoperative analgesia and recovery in elderly patients undergoing lower limb fracture surgery, 344 elderly patients undergoing lower limb fracture surgery in our hospital were selected for this study and analysed.
The results of this study showed that the excellent anesthesia rate of patients in the experimental group was significantly higher than that of patients in the control group, which was similar to the results of previous studies [16,17], confirming that the combination of sevoflurane application on top of continuous anesthesia with propofol can further improve the anesthetic effect of patients. Postoperative pain is always a major clinical and patient concern. Postoperative pain is a major factor in negative emotional and physiological-psychological changes, and severe pain can have a serious negative impact on the patient's postoperative recovery [18]. Dong [19] et al. (2021) indicated in their study of anaesthesia in 267 elderly patients with lower limb fractures that whether or not sevoflurane combined with continuous propofol anaesthesia was used did not have a significant effect on patients' pain at various postoperative time points, whereas the results of the current study showed that the VAS scores at 3h, 6h, 12h and 1d postoperatively were significantly lower in the experimental group than in the control group, which was not consistent with the findings of Dong et al. The reasons for this discrepant result may be related to the sample size of the study, the different determination criteria used, etc. Studies have shown that combining inhalation induction techniques with tissue anaesthesia is more effective than tissue anaesthesia alone, with advantages such as higher bioavailability and ease of administration [20]. At the same time, the patient's voluntary breathing is preserved after sevoflurane anaesthesia, which shortens the recovery time after surgery [21]. With regard to the postoperative recovery of the patients in this study, the time to awaken, time to extubation and time to leave the recovery room were significantly lower in the experimental group than in the control group, confirming once again the role of sevoflurane anaesthesia in facilitating the recovery of the patients. In the final comparison regarding adverse reactions, the results of this study showed no statistically significant difference in the incidence of postoperative adverse reactions between the two groups, a result that provides more evidence-based medical evidence for the clinical safety of sevoflurane.
There are still a number of shortcomings in this study, such as the lack of assessment of patients' cognitive function and the lack of regular follow-up, which prevented this study from assessing patients' post-operative cognitive function and subsequent quality of life, and further clinical studies are expected to supplement this analysis.
5. Conclusions
Sevoflurane combined with propofol continuous anaesthesia is ideal for anaesthesia in elderly patients undergoing lower limb fracture surgery. The protocol can effectively suppress patients' postoperative pain and facilitate their recovery from anaesthesia, and it does not increase the risk of postoperative adverse effects in patients.
References
- Costa, M.L., et al., Effect of Negative Pressure Wound Therapy vs Standard Wound Management on 12-Month Disability Among Adults With Severe Open Fracture of the Lower Limb: The WOLLF Randomized Clinical Trial. Jama, 2018. 319(22): p. 2280-2288.
- Aloraibi, S., et al., Optimal management of older people with frailty non-weight bearing after lower limb fracture: a scoping review. Age Ageing, 2021. 50(4): p. 1129-1136. [CrossRef]
- Costa, M.L., et al., Effect of Incisional Negative Pressure Wound Therapy vs Standard Wound Dressing on Deep Surgical Site Infection After Surgery for Lower Limb Fractures Associated With Major Trauma: The WHIST Randomized Clinical Trial. Jama, 2020. 323(6): p. 519-526.
- Keene, D.J., et al., Exercise for people with a fragility fracture of the pelvis or lower limb: a systematic review of interventions evaluated in clinical trials and reporting quality. BMC Musculoskelet Disord, 2020. 21(1): p. 435. [CrossRef]
- Aloraibi, S., et al., Optimal care for the management of older people non-weight bearing after lower limb fracture: a consensus study. BMC Geriatr, 2021. 21(1): p. 332. [CrossRef]
- Yeh, H.W., et al., Risk of Cardiovascular Disease Due to General Anesthesia and Neuraxial Anesthesia in Lower-Limb Fracture Patients: A Retrospective Population-Based Cohort Study. Int J Environ Res Public Health, 2019. 17(1). [CrossRef]
- Sahinovic, M.M., M. Struys, and A.R. Absalom, Clinical Pharmacokinetics and Pharmacodynamics of Propofol. Clin Pharmacokinet, 2018. 57(12): p. 1539-1558. [CrossRef]
- Zhang, Y., et al., Propofol compared with sevoflurane general anaesthesia is associated with decreased delayed neurocognitive recovery in older adults. Br J Anaesth, 2018. 121(3): p. 595-604. [CrossRef]
- Palanca, B.J.A., M.S. Avidan, and G.A. Mashour, Human neural correlates of sevoflurane-induced unconsciousness. Br J Anaesth, 2017. 119(4): p. 573-582. [CrossRef]
- Matsumura, T., et al., Clinical outcome of conversion from external fixation to definitive internal fixation for open fracture of the lower limb. J Orthop Sci, 2019. 24(5): p. 888-893. [CrossRef]
- Friedl, W. and G. Gradl, Nailing of lower extremity fractures. Injury, 2019. 50 Suppl 3: p. 1-3. [CrossRef]
- Griffioen, M.A. and G. OʼBrien, Analgesics Administered for Pain During Hospitalization Following Lower Extremity Fracture: A Review of the Literature. J Trauma Nurs, 2018. 25(6): p. 360-365. [CrossRef]
- Wang, N., et al., Effects of Sevoflurane versus Propofol on Endogenous Nitric Oxide Metabolism during Laparoscopic Surgery. J Healthc Eng, 2021. 2021: p. 6691943. [CrossRef]
- Sondekoppam, R.V., et al., The impact of sevoflurane anesthesia on postoperative renal function: a systematic review and meta-analysis of randomized-controlled trials. Can J Anaesth, 2020. 67(11): p. 1595-1623. [CrossRef]
- Kangralkar, G. and P.B. Jamale, Sevoflurane versus halothane for induction of anesthesia in pediatric and adult patients. Med Gas Res, 2021. 11(2): p. 53-57. [CrossRef]
- Suo, L. and M. Wang, Dexmedetomidine alleviates sevoflurane-induced neurotoxicity via mitophagy signaling. Mol Biol Rep, 2020. 47(10): p. 7893-7901. [CrossRef]
- Ao, C.B., et al., Clinical effect of ultrasound-guided nerve block and dexmedetomidine anesthesia on lower extremity operative fracture reduction. World J Clin Cases, 2022. 10(13): p. 4064-4071. [CrossRef]
- Sumitani, M., et al., Perioperative factors affecting the occurrence of acute complex regional pain syndrome following limb bone fracture surgery: data from the Japanese Diagnosis Procedure Combination database. Rheumatology (Oxford), 2014. 53(7): p. 1186-93. [CrossRef]
- Dong, J., et al., Ultrasound-guided anterior iliopsoas muscle space block versus posterior lumbar plexus block in hip surgery in the elderly: A randomised controlled trial. Eur J Anaesthesiol, 2021. 38(4): p. 366-373.
- Brovman, E.Y., et al., Anesthesia Type Is Not Associated With Postoperative Complications in the Care of Patients With Lower Extremity Traumatic Fractures. Anesth Analg, 2019. 129(4): p. 1034-1042. [CrossRef]
- Moro, E.T., et al., Quality of recovery from anesthesia of patients undergoing balanced or total intravenous general anesthesia. Prospective randomized clinical trial. J Clin Anesth, 2016. 35: p. 369-375. [CrossRef]
Figure 1.
Comparison of analgesic effects at various
postoperative time points (±s).
Note: * indicates P<0.05 for comparison.
Figure 1.
Comparison of analgesic effects at various
postoperative time points (±s).
Note: * indicates P<0.05 for comparison.
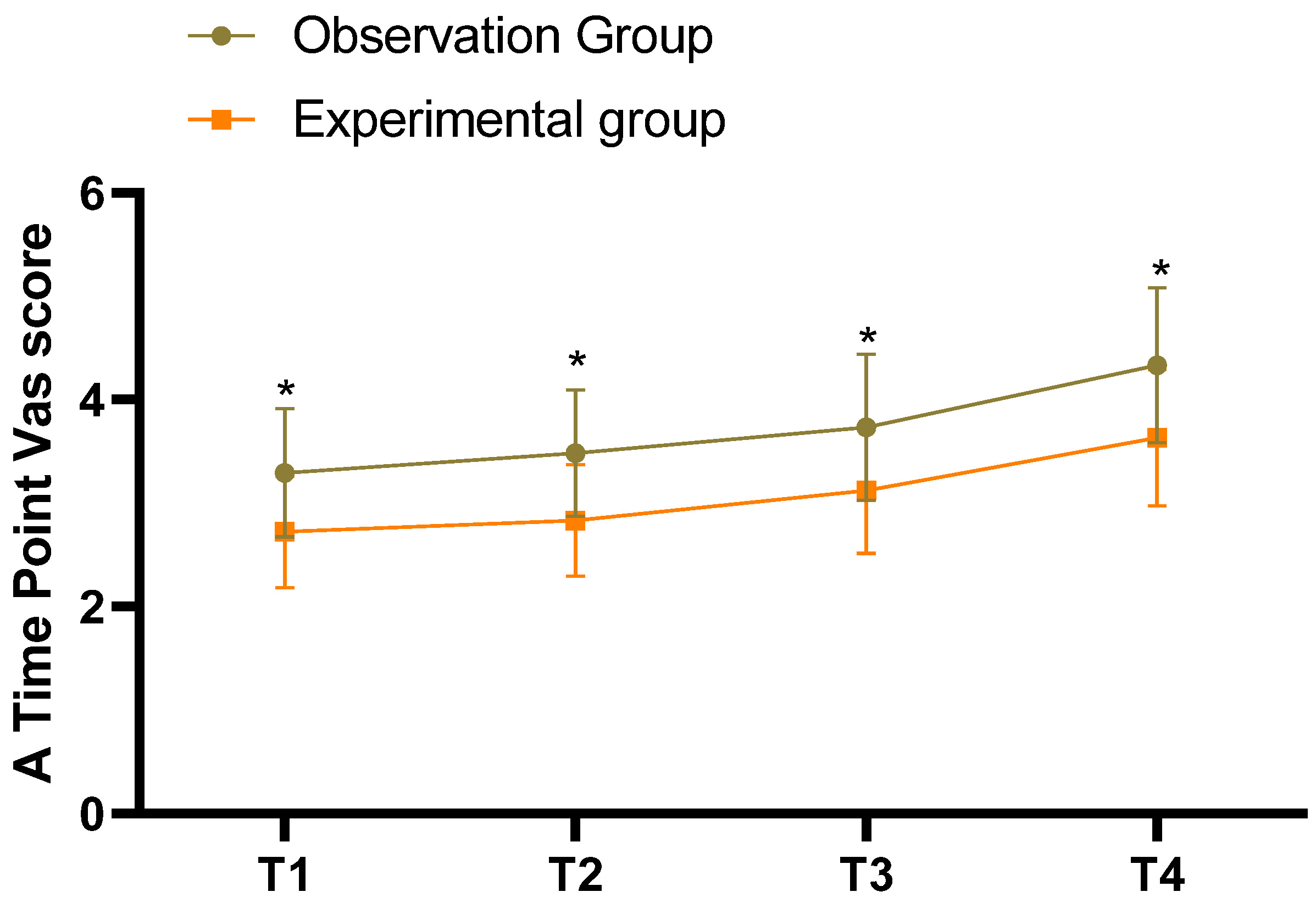
Figure 2.
Comparison of recovery from anaesthesia (±s). Note: * indicates P<0.05 for comparison.
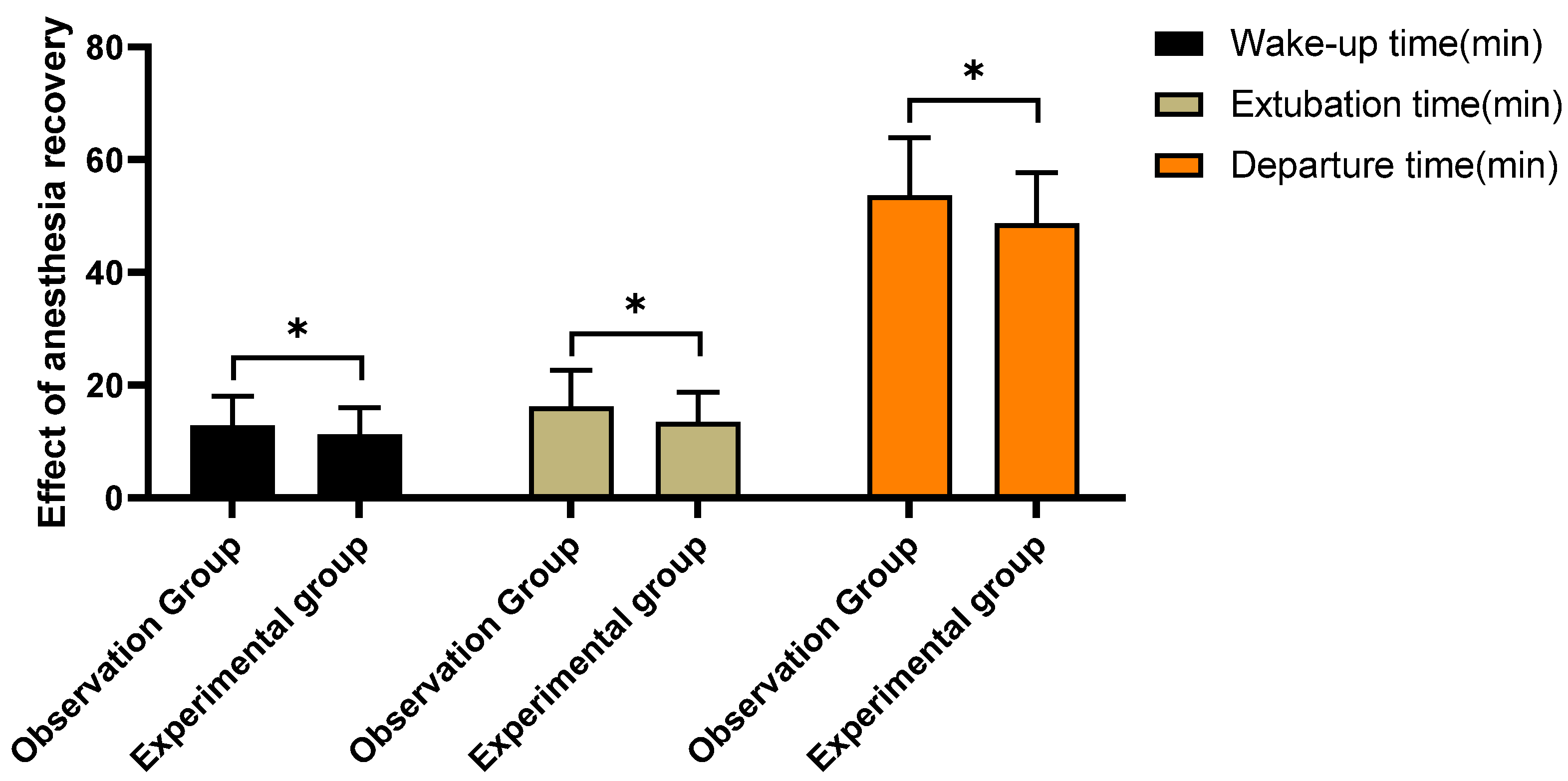

Table 1.
General data comparison [±s, n(%)].
| Control group(n=172) | Experimental group(n=172) | t/x² | P | |
| Gender | 0.106 | 0.745 | ||
| Male | 94 | 97 | ||
| Female | 78 | 75 | ||
| Age (years) | 61-84 | 62-85 | ||
| Average age (years) | 71.19±4.36 | 71.26±4.41 | -0.148 | 0.882 |
| BMI(kg/m²) | 19-26 | 19-27 | ||
| Average BMI (kg/m²) | 22.37±1.82 | 22.46±1.93 | -0.445 | 0.657 |
| Grading of anaesthesia | 0.047 | 0.829 | ||
| Level I | 77 | 79 | ||
| Level II | 95 | 93 | ||
| Surgical site | ||||
| Femoral neck | 64 | 61 | 0.113 | 0.737 |
| Femoral ridge | 71 | 76 | 0.297 | 0.586 |
| Tibiofibular | 37 | 35 | 0.07 | 0.791 |
Table 2.
Comparison of anesthetic effects [n (%)].
| Group | Cases | Excellent | Good | General | Poor | Excellent and good Rate (%) |
| Control group | 172 | 68 | 78 | 21 | 5 | 84.9%(146/172) |
| Experimental group | 172 | 75 | 92 | 4 | 1 | 97.1%(167/172) |
| x² | - | - | - | - | - | 15.635 |
| P | - | - | - | - | - | <0.001 |
Table 3.
Comparison of adverse reactions [n (%)].
| Adverse reactions | Control group(n=172) | Experimental group(n=172) | x² | P |
| Nausea and vomiting | 9 | 11 | - | - |
| Bradycardia | 6 | 7 | - | - |
| Respiratory depression | 2 | 2 | - | - |
| Itchy skin | 7 | 6 | - | - |
| Drowsiness | 5 | 6 | - | - |
| Total incidence (%) | 16.9%(29/172) | 18.6%(32/172) | 0.179 | 0.672 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



