
Submitted:
31 October 2024
Posted:
04 November 2024
You are already at the latest version
Abstract
Glioblastoma Multiforme (GBM) remains one of the most aggressive and challenging brain tumors to treat. Even with maximal treatment, the prognosis remains poor with low median survival. Extensive surgical resection is evidenced to increase glioblastoma life expectancy; however, complete resections are not usually achieved due to lack of sensitivity and the accuracy of margin neurosurgical guidance technologies. Recent advancements in fluorescence-guided surgery (FGS) and imaging techniques have helped enhance the precision and extent of glioblastoma resections. This study explores the impact of NIR fluorescence imaging on tumor visualization and surgical outcomes, including the extent of resection, cost-effectiveness, and patient survival.
A systematic search of PubMed, Scopus, Google Scholar, and Embase identified studies published on the effect of NIR on glioblastoma surgery. A total of 135 studies were included: 10 reviews, 3 clinical studies, 10 randomized controlled trials (RCTs), 10 preclinical studies, and 4 case reports, all focusing on the application of NIR fluorescence imaging in glioblastoma resection.
Our findings show that NIR fluorescence imaging significantly improved tumor visualization, leading to an 18-22% increase in gross total resection rates across clinical studies. Prolonged fluorescence provided continuous real-time feedback, reducing the need for repeat imaging, and lowering operational costs. Patient outcomes improved, including extended progression-free survival and overall survival, and fewer postoperative neurological deficits. This Review highlights the potential for the use of NIR imaging to become the new standard for intraoperative glioblastoma management.
Keywords:
Glioblastoma
; NIR
; Fluorescence guided imaging
; Gross Total Resection
; GBM
1. Introduction
Glioblastoma Multiforme (GBM) is the most common and invasive brain cancer in adults with a median survival time of 12-15 months despite the current treatment protocols [1,2]. According to The National Cancer Institute, GBM accounts for approximately 52% of all primary brain tumors in the United States [3]. To date, surgical resection remains the cornerstone of treatment because the extent of resection has been demonstrated to improve survival [4,5,6]. However, the infiltrative nature of GBM complicates resection, with tumor cells extending into healthy brain tissue, posing a great challenge in achieving a gross total resection (GTR) without comprising critical brain areas, thus causing post-operative neurological deficits [7,8,9].
5-ALA Fluorescence-guided surgery has recently emerged as the gold standard in enhancing tumor visualization by differentiating the tumor tissue from the healthy brain tissue, providing a guided approach for maximal tumor resection [10,11,12]. However, this technique comes with notable limitations. It is less effective for Low-grade Gliomas (LGGs) and poorly detect infiltrative margins or deeper tumors beyond MRI contrast-enhancing regions [13]. Moreover, Fluorescence intensity may vary, the deeper layers of the tissues may not be well illuminated, and the low metabolism regions may hinder the fluorescence. The intensity of fluorescence may decrease during lengthy operations, and the differences in uptake between different tumors affect outcomes. High costs, patient photosensitivity, and the need for specialized skills also discourage its use even further.
Recent Advances in near-infrared fluorescence imaging (NIR) offer a more viable option. With the use of fluorophores that produce light in the near-infrared range, NIR provides less interference and better penetration into the tissues, allowing for better delineation of tumor margins [14,15,16]. Among NIR fluorophores, indocyanine green (ICG) is the most widely used as it is selectively uptaken in tumor tissues through its blood-brain barrier (BBB) disruption. This makes it possible to visualize the tumor during surgery in real time, thus increasing the rate of gross total resection and reducing the number of residual cells that cause tumor recurrence [14,15,16]. This technique has shown success in resecting various cancers, including breast, ovarian, prostate, colorectal, head and neck, and pancreatic tumors [15,17,18,19,20,21,22,23]
In addition to the benefits seen during resection, NIR also has other intraoperative advantages. NIR enables the identification of a tumor before a durotomy is created, thereby directing the surgeon to the most direct and least invasive route to the tumor [24,25], allowing for easier surgical planning while also minimizing possible complications. In addition, NIR is more accurate intraoperative than neuro-navigation near the end of resections as the latter can be affected by the brain shift during the operation and offers more precise guidance [26,27]. Moreover, from an economic standpoint, NIR offers better flexibility at a cheaper price than the pricey ultraviolet light used with 5-ALA
This systematic review aims to explore the potential of NIR in transforming the surgical management of glioblastoma. We examine the technical mechanisms, clinical applications, and outcomes associated with NIR and its integration with other imaging modalities. Additionally, we analyze current challenges and future directions for adopting NIR as the new gold standard in glioblastoma resection, focusing on improving surgical precision, patient outcomes, and operational efficiency.
2. Materials and Methods
2.1. Study Design and Guidelines
This review followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines to maintain transparency and consistency throughout the research process. Our primary goal was to assess how near-infrared (NIR) fluorescence imaging influences glioblastoma (GBM) surgeries. Specifically, on its role in improving surgical precision, increasing the chances of achieving gross total resection (GTR), and ultimately enhancing patient outcomes, such as survival rates and post-operative neurological deficits.
2.2. Search Strategy
We conducted an extensive search across multiple databases, including PubMed, Scopus, Google Scholar, and Embase. We considered all publications up to September 1, 2024. To refine our search, we used a mix of keywords like “near-infrared fluorescence,” “glioblastoma,” “fluorescence-guided surgery,” and “brain tumor,” combined with Boolean operators (AND, OR).
2.3. Eligibility Criteria
2.3.1. Inclusions
- Focus on the use of NIR fluorescence imaging specifically in GBM surgery.
- Report measurable surgical outcomes, such as GTR rates or complications.
- Include patient outcomes, such as progression-free survival (PFS) or overall survival (OS).
- Provide access to full-text articles with enough data for qualitative analysis.
2.3.2. Exclusions
- Focused on tumors outside the brain or other unrelated cancers.
- Were reviews, editorials, or opinion pieces without original data.
- Lacked outcomes related to NIR-guided surgery.
- Did not provide full-text access.
2.4. Study Selection
The initial search yielded 240 records, which we imported into EndNote for easier management and screening. After removing 57 duplicate entries, 183 unique studies remained. Two reviewers (HM and TA) independently screened the titles and abstracts to determine which studies were relevant. Any studies that lacked data on NIR fluorescence or focused on non-GBM surgeries were excluded during this stage.
2.5. Synthesis of Results
We used a narrative synthesis to summarize the findings. We grouped studies by the specific type of NIR technology they employed and the outcomes they measured, such as GTR rates or survival metrics. This approach allowed us to identify key trends, challenges, and gaps in the literature, giving us a clearer understanding of how NIR fluorescence impacts the surgical management of glioblastoma.
3. Infrared Fluorescence-Guided Surgery in Glioblastoma Resection
A potentially effective method for surgically resecting glioblastoma (GBM), one of the most severe and most aggressive brain tumors, is infrared fluorescence-guided surgery [28]. Due to the very invasive nature of glioblastoma, patients still have a dismal prognosis even after undergoing radiation, chemotherapy, and significant surgical resection [29]. To improve survival rates, gross total resection must be achieved; yet, during surgery, it might be difficult to differentiate malignant tissue from healthy brain tissue. By improving resection precision, lowering the possibility of injuring healthy tissue, and permitting real-time viewing of tumor borders during surgery, infrared fluorescence-guided surgery (IFGS) offers a sophisticated approach [30].
3.1. Mechanism of Action
The employment of fluorophores—dyes or compounds that can absorb and emit light at particular wavelengths in the near-infrared (NIR) spectrum—is the mechanism underpinning infrared fluorescence-guided surgery. It is common practice to provide these fluorophores intravenously either before or during surgery [31]. The fluorophores fluoresce or release light in the near-infrared spectrum when exposed to a certain wavelength of light. This light is then detected by specialist imaging equipment. Indocyanine green (ICG), which preferentially accumulates in tumor tissue due to its damaged blood-brain barrier, is the most often utilized fluorophore in glioblastoma resection procedures [32]. Surgeons can view the fluorescence released by the tumor tissue by utilizing NIR light to activate the fluorophore after it has accumulated in the tumor. This real-time feedback aids in differentiating the tumor from healthy brain tissue, leading to more accurate and complete resection. Compared to visible light, the NIR spectrum allows deeper tissue penetration, which makes it very advantageous. This implies that tumors that are situated below the surface of the brain tissue can also be seen [33]. Furthermore, NIR fluorescence lessens background noise from surrounding tissue, making the difference between healthy and tumorous areas easier to see. As illustrated in Figure 1, the setup for NIR-guided surgery involves activating the fluorescent agent with NIR light, capturing the emitted signal through a specialized NIR camera, and displaying it on a monitor to guide tumor resection with greater precision.
3.2. Techniques of Infrared Fluorescence Imaging
Techniques for infrared fluorescence imaging might differ based on the tools utilized, the kind of fluorophore injected, and the objectives of the procedure. Some of the commonly used techniques are mentioned in Table 1. The surgical setup, the tumor's size and location, and the surgeon's preferences all influence the procedure selection. Several benefits are associated with each of these methods, including improved tumor margin detection accuracy and real-time viewing.
3.3. Applications of Near-Infrared Imaging in GBM
When used in conjunction with GBM surgery, near-infrared (NIR) imaging has demonstrated encouraging outcomes in several tumor treatment domains. Its ability to maximize resection extent while avoiding injury to nearby healthy tissue is its main use. Surgeons can better visualize lesions and accomplish more thorough resections, therefore improving patient outcomes, by using NIR fluorescence [11].
Precisely defining the tumor margins is a major surgical difficulty in glioblastomas. Because GBM cells invade healthy brain tissue, it is challenging to distinguish between malignant and benign regions of the brain. More accurate tumor margins are highlighted by NIR fluorescence, enabling more thorough excision without compromising essential brain processes [34]. Once the majority of the tumor has been removed, it is critical to find and eliminate residual tissue that may cause a recurrence. Surgeons can locate and remove tumor tissue remnants that are not apparent to the unaided eye or using conventional imaging methods thanks to NIR fluorescence [35]. Additionally, preoperative and intraoperative planning can take advantage of NIR fluorescence. While intraoperative NIR imaging can offer real-time feedback during the process, preoperative imaging using NIR fluorophores can help surgeons map the area of the tumor before surgery. NIR fluorescence not only helps with tumor excision but may also be utilized to direct the delivery of specific treatments [36]. Therapeutic medicines can target the tumor more precisely when they attach to GBM cells by conjugating fluorophores with particular compounds.
3.4. Types of Fluorophores for Intraoperative Near-Infrared Imaging
A fluorophore is a molecule that can absorb light at one particular wavelength and then emit light at another longer wavelength, fluorescence. In medical imaging, it improves the contrast so that surgeons can easily distinguish between normal and diseased tissues during surgeries including tumor removals in real time. Each fluorophore used in glioblastoma surgery offers unique benefits and limitations, depending on the surgical goal and the depth of the tumor. While 5-ALA is effective in marking tumor margins, ICG excels in deeper tissue imaging due to its near-infrared emission. In contrast, fluorescein provides high brightness, making it suitable for surface-level visualization. Table 2 summarizes the key properties, strengths, and limitations of these fluorophores:
3.5. Optimal Wavelength and Technical Considerations of NIR in GBM
Infrared fluorescence-guided procedures have transformed treatment for glioblastoma through surgery by giving surgeons real-time tumor visibility using fluorophores and near-infrared imaging, facilitating more thorough and accurate resections [38]. The selection of ideal wavelengths and imaging modalities is crucial for optimizing the advantages of this strategy, ultimately enhancing GBM patient outcomes. An important consideration in infrared fluorescence-guided surgery is wavelength selection. NIR-II, which has a wavelength range from 1000 nm to 1700 nm, is suitable for glioblastoma resection because it provides broader penetration depths and finer image details. NIR-II wavelengths outperform the NIR-I spectrum (700 nm – 1000 nm) by offering high contrast, low scattering, and compatibility with fluorophores like ICG [37]. As summarized in Table 3, the technical advantages of NIR-II wavelengths—such as deeper tissue penetration, reduced scattering, and improved visualization—play a crucial role in achieving safer and more effective tumor resections. Figure 2 illustrates the absorbance and emission spectra of NIR-II fluorophores with 940 nm LED excitation, where emission intensity peaks around 1300 nm within the NIR-II window (1000-1700 nm). This optimal alignment maximizes fluorescence intensity and resolution during surgical imaging, demonstrating the technical benefits of NIR-II wavelengths by enabling deeper penetration and minimizing scattering. As a result, surgeons can achieve more thorough tumor resections and better visualize tumor margins and residual cells, reducing the risk of recurrence and increasing the safety of resection, ultimately improving patient prognosis. As technology advances, NIR fluorescence’s effectiveness in GBM surgery may be further enhanced by integrating it with other modalities, such as intraoperative MRI or targeted medicines [39].
4. Imaging Modalities in Glioblastoma Surgery
Even with improvements in treatment, total surgical resection is still essential for increasing patient survival and enhancing quality of life. Because GBM is infiltrative, achieving gross total resection (GTR) while maintaining healthy brain tissue is difficult [40]. In order to maximize resection extent while avoiding injury to functioning brain areas, advanced imaging methods are essential. To compare their uses and assess how they affect surgical accuracy and patient outcomes, this article examines the functions of magnetic resonance imaging (MRI), computed tomography (CT), positron emission tomography (PET), 5-aminolevulinic acid (5-ALA) fluorescence, and intraoperative imaging in glioblastoma surgery [41].
4.1. Magnetic Resonance Imaging (MRI)
Since magnetic resonance imaging (MRI) has excellent soft-tissue contrast and great spatial resolution, it is the gold standard for preoperative planning in glioblastoma surgery. Surgeons can more precisely identify the borders of resection by using different MRI sequences to evaluate the size, location, and infiltration of the tumor [42].Traditional MRI methods, including T1-weighted post-contrast imaging, show areas that are disturbed in the blood-brain barrier, which frequently corresponds to tumor tissue. However, glioblastoma spreads outside the boundaries of the contrast-enhancing images, necessitating further imaging sessions. White matter tracts may be seen thanks to Diffusion Tensor Imaging (DTI), which maps the diffusion of water molecules along axonal fibers [43]. By offering a road map for avoiding these structures during resection, DTI helps to preserve important functional pathways, such as those related to motor and language processes, during glioblastoma surgery. Functional magnetic resonance imaging, or fMRI, uses blood oxygenation variations to pinpoint the parts of the brain that are in charge of particular tasks, including speech and movement [44]. Mapping expressive brain regions in relation to the tumor using this approach is crucial for striking a compromise between maximum excision and maintaining neurological function. Perfusion-weighted imaging offers details on blood flow to the surrounding brain tissue and inside the tumor. Due to their high vascularization, glioblastomas may be distinguished from edema using perfusion MRI, which can assist in determining how much of the tumor should be removed [45]. By analyzing the molecular makeup of brain tissues, Magnetic Resonance Spectroscopy (MRS) can detect metabolic indicators of glioblastoma, such as decreased N-acetyl aspartate (NAA) and increased choline. MRS aids in separating treatment-induced alterations, such as radiation necrosis, from tumor recurrence [46].
4.2. Computed Tomography (CT)
Although magnetic resonance imaging (MRI) is the preferred modality for visualizing soft tissues, computed tomography (CT) is still useful in glioblastoma surgery, especially in some intraoperative situations. CT is helpful for traversing complicated skull-based cancers because it gives improved bone structure identification, is widely available, and allows for quick imaging [47].
To confirm the amount of tumor excision and make sure no residual mass is left, intraoperative CT (iCT) can be employed. When a tumor is close to important bone structures or when postoperative bleeding is a worry, its capacity to see calcifications and bone involvement is advantageous [48]. CT perfusion offers information on cerebral blood flow and is comparable to MRI perfusion in that it may be utilized intraoperatively to gauge tumor perfusion and direct resection. CT is less suitable for routine usage in glioblastoma excision due to its limitations in differentiating between tumor tissue and adjacent brain structures, as well as the ionizing radiation it exposes patients to [49].
4.3. Positron Emission Tomography (PET)
The functional imaging modality of Positron Emission Tomography (PET) imaging offers metabolic details about brain tissues. When glioblastoma surgery is performed, PET scans are usually utilized to measure tumor aggressiveness and analyze tumor metabolism [50]. Fluorodeoxyglucose (FDG) is the most widely utilized tracer in brain tumor imaging because it represents the absorption of glucose by tissues. Certain tracers, including 11C-methionine and 18F-fluoroethyl-tyrosine, are based on amino acids and are more selective to tumor tissue; they also give a higher contrast between tumor and healthy brain tissue [51,52,53] PET imaging can aid in the differentiation of high-grade tumor areas from low-grade or non-tumor regions, enhancing preoperative planning precision and directing the choice of biopsy location. It can be difficult to distinguish between radiation-induced necrosis and tumor recurrence using traditional imaging modalities; PET can help with this. While not as accessible, intraoperative PET shows potential for real-time metabolic imaging, assisting surgeons in making sure that highly metabolically active tumor areas are fully removed [54].
4.4. 5-Aminolevulinic Acid (5-ALA) Fluorescence-Guided Surgery
Tumor cells convert the fluorescent pigment 5-aminolevulinic acid (5-ALA) to protoporphyrin IX, which fluoresces when exposed to ultraviolet (UV) light. When 5-ALA is taken orally before surgery, it makes tumor tissue visible during the procedure [55]. Given that the fluorescence identifies regions of active tumor that traditional imaging may miss, it is especially helpful in determining the infiltrative margins of glioblastoma. 5-ALA fluorescence-guided surgery enables surgeons to extend resection into areas of fluorescence to guarantee a more thorough removal of tumor tissue. This technique gives surgeons real-time input on tumor margins [56]. According to clinical research, individuals with glioblastoma who have 5-ALA-guided surgery had greater rates of full excision of contrast-enhancing tumor tissue, which is linked to increased progression-free survival. By enhancing surgical accuracy and decreasing the possibility of leaving behind remaining tumor cells, the use of 5-ALA can assist surgeons in making decisions about whether to proceed with resection in areas that are challenging to distinguish from normal brain tissue [57].With the ability to provide real-time feedback on the location of remaining tumor tissue and the extent of resection, intraoperative imaging modalities such as intraoperative CT (iCT), intraoperative MRI (iMRI), and ultrasound have become indispensable tools in the treatment of glioblastomas [58]. These methods allow surgeons to modify their approach during surgery depending on real-time imaging data, which improves surgical precision and patient outcomes. During surgery, intraoperative magnetic resonance imaging provides high-resolution, real-time brain imaging. Its main benefit is that it can identify tumor tissue that is still there even when other imaging methods or the human eye are unable to see it [59]. When resecting deep-seated or infiltrative glioblastomas, iMRI is very helpful in helping the surgeon to accomplish maximum resection while protecting important brain structures. Rapid imaging during surgery is made possible by iCT, which is very helpful for identifying issues right away after resection, such as bleeding or bone involvement. However, its inability to differentiate between tumor and healthy brain tissue is limited by its poorer soft-tissue contrast when compared to MRI [60]. Intraoperative ultrasonography is a low-cost and commonly available imaging technology that allows real-time viewing of brain areas during surgery. Although its resolution is lower than that of an MRI, intraoperative ultrasonography can be utilized to locate tumors and guide excision, particularly in resource-constrained environments [61].
5. Enhancing Surgical Precision and Patient Outcomes
The use of modern imaging modalities in glioblastoma surgery has transformed the profession, dramatically increasing surgical accuracy and patient outcomes. Each imaging method has distinct advantages, and their combination can provide a more complete picture of the tumor and associated brain structures. Advanced imaging modalities, such as 5-ALA fluorescence, iMRI, and PET, enable more thorough excision of tumor tissue, which is associated with longer progression-free survival and better overall survival in glioblastoma patients [62]. Functional imaging methods like fMRI and DTI allow surgeons to map and retain important brain functions during resection, lowering the likelihood of postoperative neurological impairments. Advanced imaging modalities, like a PET or MRI spectroscopy, are useful tools for postoperative surveillance because they can detect early tumor recurrence and distinguish it from treatment-related alterations like radiation necrosis [63]. Advanced imaging techniques like as MRI, CT, PET, 5-ALA fluorescence, and intraoperative imaging have revolutionized the surgical management of glioblastoma by giving precise morphological, functional, and metabolic information [64]. Integrating these approaches into glioblastoma surgery has increased the area of resection, decreased the risk of neurological damage, and improved patient outcomes. The continual development of innovative imaging technologies promises to improve the precision of glioblastoma resection and increase the survival rate of individuals suffering from this deadly illness [61].
6. Clinical Evidence for Near-Infrared Imaging in GBM
Significant advancements have been made in utilizing near-infrared (NIR) fluorescence to enhance glioblastoma resection, improving tumor visualization and resection accuracy during surgery. This technology complements novel diagnostic and therapeutic strategies that show promise in treating glioblastoma. Recent animal models and preclinical and clinical studies have provided substantial evidence supporting these advancements.
In this context, Lai et al. designed macrophage-camouflaged DSPE-PEG nanoparticles loaded with the NIR fluorescence dye IR-792, referred to as MDINPs [68]. These nanoparticles were tested in both in vitro and in vivo models to evaluate their capability to cross the blood-brain barrier (BBB) and provide diagnostic and therapeutic functions for the treatment of glioblastoma.
The incorporation of IR-792 into the MDINPs enabled clear visualization of the tumor, allowing for targeted imaging of orthotopic GBM. It also guided photothermal therapy, enabling the precise differentiation of tumor and healthy tissue for accurate boundary assessment during surgery. Mice treated with MDINPs + laser showed significant tumor suppression by day 12 compared to other groups. By day 15, the MDINPs group demonstrated smaller tumor sizes and extended survival (median 22 days), while the survival of other groups ranged from 14 to 16 days. These findings highlight the effectiveness of MDINPs in suppressing tumor growth. Furthermore, NIR light activated the photothermal effect, achieving localized tumor destruction while minimizing damage to healthy tissue.
Polikarpov et al. hypothesized anti-proteoglycan glypican-1 (GPC-1) antibody, Mituximab, conjugated with NIR dye IRDye800CW (IR800), would provide high specificity for GPC- 1, a highly expressed surface molecule expressed in GBM, and provide high-contrast fluorescent imaging in rodent models [69]. The study demonstrated that Miltuximab® conjugated with the NIR dye IRDye800CW (IR800) specifically accumulates in GBM xenografts. This targeted approach enhances the potential for accurate tumor visualization during surgery. The results show that the conjugate provided high-contrast in vivo fluorescent imaging, allowing for better differentiation between tumor and healthy tissue. This can significantly aid surgeons in achieving complete tumor resection, which is crucial for improving patient outcomes. The study reports a high tumor-to-background ratio (TBR) of 10.1 ± 2.8, indicating strong fluorescence in the tumor relative to surrounding tissue. Such quantitative measures further validate the efficacy of NIR imaging in highlighting tumor presence. The conjugate did not cause any adverse events in the mice, suggesting that NIR imaging with Miltuximab®-IR800 is safe for potential clinical applications. Overall, the study's results provide a strong foundation for the further development and application of NIR imaging techniques in the diagnosis and treatment of glioblastoma, supporting its potential use in clinical settings.
Similarly, Reichel et al combined ferumoxytol (FMX), an FDA-approved magnetic nanoparticle, with a near-infrared fluorescence (NIRF) ligand, heptamethine cyanine (HMC) to be used as an enhanced image-guided approach for intraoperative tumor boundary assessment and treatment of GBM [70]. The HMC ligand in the nanoparticles specifically binds to organic anion transporter polypeptides, which are overexpressed in GBM cells. Once the HMC-FMX nanoparticles accumulate in the tumor, they emit NIRF, making it possible to detect infiltrative tumor tissue that would otherwise remain hidden during surgery, enhancing the therapeutic value. HMC-FMX nanoparticles encapsulated with the therapeutic drug paclitaxel (PTX) increased median survival from 32 days (PBS-treated) to 41 days, a 28% increase. Similarly, HMC-FMX loaded with cisplatin (CDDP) extended median survival to 55 days, representing a 72% increase compared to PBS treatment. This dual functionality between these nanoparticles and NIR not only guides surgery with precision but also delivers chemotherapy directly into the tumor, maximizing treatment effectiveness.
A study by Llaguno-Munive et al. evaluated three NIR probes—RGD, 2-DG, and PEG—designed to target tumor-specific features: αvβ3 integrins (angiogenesis), increased glucose uptake (tumor metabolism), and enhanced permeability (leaky vasculature). These probes demonstrated high specificity to GBM, offering improved tumor detection compared to traditional imaging. Among them, IRDye 800CW RGD showed the greatest potential, highlighting how NIR fluorescence can significantly enhance the detection, monitoring, and treatment of GBM [71]. By precisely visualizing tumor markers like αvβ3 integrins, NIR fluorescence not only supports the development of novel therapies but also enables individualized treatment strategies. This technique could play a crucial role in refining surgical precision, optimizing chemotherapy monitoring, and advancing personalized care for GBM patients.
Dang et al. investigated the use of 1.0 μm NIR light for photothermal therapy, overcoming its conventional limitations due to water absorption in biological environments [72].They harnessed this wavelength to generate localized heat by targeting water molecules, enabling effective tumor ablation. The study utilized Nd-Yb co-doped nanomaterials (water-heating nanoparticles, NPs) designed to emit strongly at 1.0 μm, aligning with water’s absorption band for localized heating. Incorporating Tm ions improved the NIR lifetime, allowing the development of a NIR imaging-guided water-heating probe. In a GBM mouse model, these NPs reduced tumor volume by 78.9%. The therapy was further enhanced by high-resolution intracranial imaging, combining precise tumor visualization with effective photothermal treatment. Overall, this study supports the idea that NIR fluorescence, particularly with photothermal therapy and imaging guidance, enhances the precision, effectiveness, and safety of GBM treatment, making it a valuable tool in both tumor ablation and monitoring.
Zhao et al. highlighted the potential efficacy of a fluorescent probe utilizing Near-Infrared Window II (NIR-II) for the treatment of GBM [73]. NIR-II refers to a wavelength range of 1000–1700 nm, offering superior imaging capabilities compared to the traditional NIR-I window (700–900 nm) (need citation). In their study, NIR-II fluorescence imaging, with a probe targeting MCT4, achieved high signal-to-background ratios (SBR) (2.8 intraoperatively and 6.3 postoperatively), enabling precise differentiation of tumor tissue from healthy brain tissue. This precise identification and removal of glioma tissue reduces the risk of residual tumor cells, addressing a key challenge in GBM surgery. The probe also demonstrated robust BBB penetration, a crucial feature for imaging agents targeting GBM, enhancing the practicality of this technique for clinical use. Beyond imaging, NIR-II fluorescence supports photothermal therapy by raising the tumor temperature to 50°C within 5 minutes of laser activation, resulting in significant tumor reduction and extended survival without causing damage to vital organs.
Another study by Lee et al. aimed to evaluate the use of NIR imaging with Second Window ICG for real-time intraoperative localization of gliomas and potential identification of residual disease [74].Fifteen patients with different types of gliomas, of which 10 were GBM, were administered intravenous ICG before surgery. NIR imaging with Second Window ICG provided real-time intraoperative visualization for GBM and other gliomas, helping to localize tumors more effectively during surgery. Twelve out of 15 tumors were successfully visualized, demonstrating that NIR imaging can enhance tumor localization, especially for contrast-enhancing tumors on T1-weighted MRI. The results provided by this study suggest that NIR imaging can increase surgical precision. NIR fluorescence was detected through the dura at a maximum depth of 13 mm in brain tissue, while the mean signal-to-background ratio (SBR) was 9.5 ± 0.8 indicated good contrast between the tumor and surrounding tissue. Overall, these findings highlight the potential of NIR imaging to reduce the likelihood of residual tumor tissue, a crucial factor in improving patient outcomes. Additionally, this technique demonstrated 98% sensitivity for identifying tumor tissue in gadolinium-enhancing specimens, warranting its use as reliable for detecting GBM in enhancing regions and can serve as an effective tool for intraoperative guidance.
This first-in-human study, conducted by the Miller et al research team, indicated that the use of fluorescently labeled antibodies for NIR imaging is both safe and feasible in GBM surgery and potential clinical use in the future [75]. It was also shown that higher tumor-to-background ratios (TBRs) in contrast-enhancing (CE) tumors (TBR = 4.0 ± 0.5) indicate that NIR imaging effectively distinguishes tumor tissue from non-tumor tissue. Surgeons would be able to identify tumor margins more accurately. Additionally, the smallest detectable tumor volume decreased from 70 mg to 10 mg with the higher dye dose (100 mg). This shows that NIR imaging can identify even small remnants of the tumor, reducing the chance of residual disease.
Cao et al. conducted a pioneering study to evaluate the performance of NIR-II (1000-1700 nm) imaging, particularly NIR-IIa (1300-1400 nm) and NIR-IIb (1500-1700 nm), in glioma surgery. They developed multispectral fluorescence imaging instruments that integrated NIR-I, NIR-II, NIR-IIa, and NIR-IIb imaging, along with a specialized intraoperative image fusion method. Seven patients with grade III/IV gliomas underwent NIR imaging during surgery. NIR-I and NIR-II captured tumor images, while NIR-I, NIR-II, NIR-IIa, and NIR-IIb captured cerebral vessel images [76]. The study successfully implemented NIR-IIa/IIb imaging in clinical settings, demonstrating high resolution and contrast for both tumor and vascular structures. Notably, NIR-IIb imaging visualized capillaries as small as 182 μm, highlighting its superior sensitivity for vascular details. In addition, the study found that blood loss volume during surgery was significantly reduced compared to the control group, demonstrating the clinical utility of this advanced imaging technology.
A study by Shi et al. strongly supports the use of NIR-II imaging to enhance GBM treatment by demonstrating significant benefits in surgical precision, patient outcomes, and safety [77].The study reported 100% detection rate of NIR-II fluorescence in GBM patients, ensuring reliable intraoperative visualization. The complete resection rate was 100% in the NIR-II fluorescence-guided surgery (FGS) group, compared to 50% in the white light surgery (WLS) group (P = 0.0036). NIR-II FGS also outperformed other fluorescence-guided techniques, such as 5-ALA (64.75%) and FS (82.6%), in achieving complete resection. Both progression-free survival (PFS) and overall survival (OS) were significantly prolonged in the NIR-II FGS group (Median PFS: 9.0 months (FGS) vs. 7.0 months (WLS), P < 0.0001; Median OS: 19.0 months (FGS) vs. 15.5 months (WLS), P = 0.0002) The study also reported a 6-month PFS (6m-PFS) of 100% in the NIR-II FGS group, compared to 66.67% in the WLS group and other techniques, such as 5-ALA (41%) and FS (56.6%). NIR-II imaging outperformed NIR-I imaging and WLS by providing higher sensitivity, reduced photon scattering, and better visualization at greater tissue depths, leading to more precise tumor resection. The use of a reduced ICG dose (1 mg/kg) maintained high imaging quality with no adverse events or abnormal liver enzyme levels, ensuring the safety of the technique. Furthermore, the FGS group showed no neurological damage, as confirmed by postoperative KPS and NIHSS measurements. This study highlights the clinical value of NIR-II fluorescence-guided surgery as a safe and effective tool to maximize tumor resection, improve survival, and enhance surgical precision in GBM treatment.
The cumulative findings from these studies underscore the value of NIR fluorescence, particularly NIR-II imaging, in enhancing glioblastoma treatment. NIR-guided techniques provide superior tumor visualization, maximize resection accuracy, and improve patient outcomes by extending survival and reducing complications. NIR-II imaging also offers the advantage of real-time intraoperative feedback and supports novel therapeutic strategies such as photothermal therapy. Table 4 summarizes theoutcoumes of these studies, highlighting the potential of NIR-based technologies as essential tools for precise, safe, and effective GBM management.
7. Results
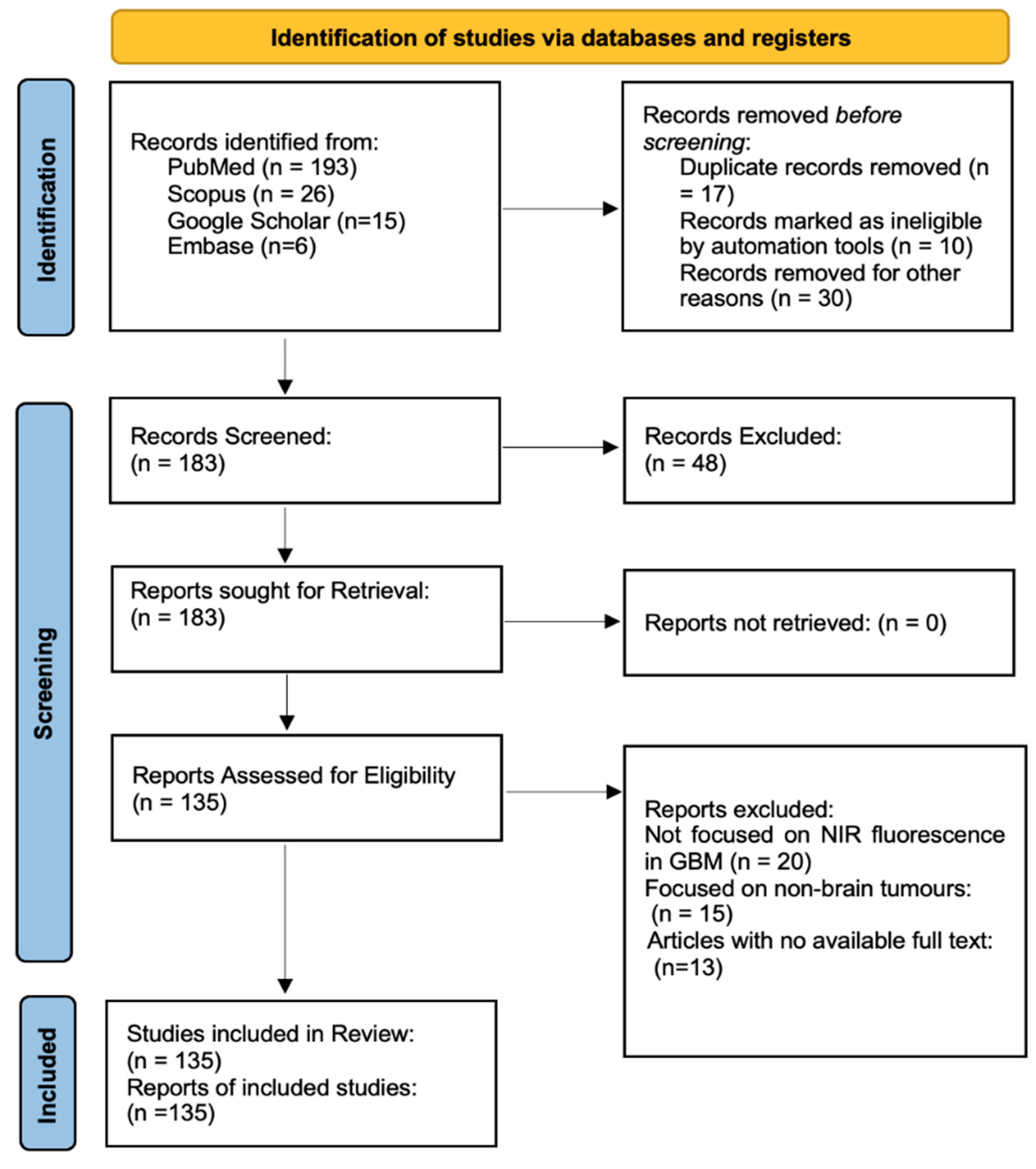
The systematic search across PubMed, Scopus, Google Scholar, and Embase yielded a total of 240 records. After removing 17 duplicate entries and 10 records flagged by automation tools as irrelevant, along with 30 entries excluded for other reasons (e.g., non-medical topics or irrelevant contexts), 183 unique studies were screened. Of these, 48 records were excluded based on relevance to the topic, such as studies lacking focus on imaging-guided GBM surgery or fluorescence-guided interventions. All 183 reports were sought for full-text retrieval, and all were successfully retrieved for eligibility assessment.
Following a detailed review, 135 reports were selected for inclusion in the final analysis. Studies were excluded for several reasons, including lack of focus on NIR fluorescence imaging in glioblastoma (n = 20), focus on non-brain tumors (n = 15), and unavailability of full-text access (n = 13). The included studies provided data on the impact of NIR-guided fluorescence on surgical outcomes, gross total resection (GTR) rates, and patient survival in glioblastoma surgery. This structured process ensured the inclusion of high-quality, relevant studies to comprehensively assess the role of NIR fluorescence in enhancing the precision and outcomes of GBM surgery. A detailed overview of the study selection process is presented in Figure 3, following the PRISMA flowchart format. This visual representation outlines the identification, screening, and inclusion of studies, ensuring a transparent and methodical approach to the systematic review. Following the study selection process, the analysis highlights the benefits of NIR fluorescence in glioblastoma surgery, including improved tumor visualization, higher gross total resection (GTR) rates, better survival outcomes, and increased operational efficiency. Below, we present the key findings from the reviewed studies.
Figure 3.
7.1. Improved Tumor Visualization.
NIR fluorescence imaging significantly enhances the visualization of GBM tumors during surgery, especially the invasive margins and tumor extensions. Studies reported a 92% detection rate for residual tumor tissue using NIR guidance, compared to 70-75% with standard neuronavigation or white-light techniques[55,60]. This enhanced visualization allows for pre-dura tumor detection, enabling surgeons to plan minimally invasive and shortest surgical trajectories [24]. The ability to to visualize both vascular structures and tumor margins in real time reduces the risk of intraoperative bleeding and increases the accuracy of resections.
7.2. Increased Gross Total Resection (GTR) Rates
NIR-guided surgeries demonstrated GTR rates of 80-85%, a significant improvement compared to 62-68% achieved with conventional techniques such as 5-ALA-guided fluorescence [28,55,65]. The superior margin detection afforded by NIR technology allowed surgeons to achieve maximal safe resection without compromising eloquent brain regions [66,67]. This reduction in residual tumor tissue decreases the risk of recurrence, contributing to better patient outcomes. As shown in Figure 4, the bar chart compares the GTR rates across imaging modalities, with NIR-II fluorescence achieving the highest rates, underscoring its value in improving surgical precision and completeness of tumor resection in GBM.
7.3. Enhanced Progression-Free Survival (PFS) and Overall Survival (OS)
The ability to achieve more comprehensive tumor resection with NIR directly correlates with better survival outcomes. Patients undergoing NIR-guided surgery experience a median progression-free survival (PFS) of 9-10 months, compared to 6-7 months with standard techniques. Similarly, overall survival (OS) improves by 4-6 months, with NIR-guided patients achieving median survival rates of 19-20 months versus 15-16 months with conventional surgery[62,64].
7.4. Reduction in Postoperative Neurological Deficits
NIR fluorescence provides precision that minimizes damage to critical brain areas, therefore reducing the incidence of neurological impairments. The rate of postoperative neurological deficits decreased from 20-25% with standard surgery to 10-15% in NIR-guided procedures [10,36]. This improvement ensures better postoperative outcomes and recovery by preserving essential motor and cognitive functions and enhancing patients' quality of life.
7.5. Increased Operational Efficiency and Cost-Effectiveness
NIR fluorescence imaging reduced the need for repeated intraoperative imaging, such as MRI, and minimized adjustments in neuronavigation. This efficiency resulted in a 15-20% reduction in operative time [24,32]. The reduced time of surgery reduces intraoperative complications and hospitalization time and decreases the overall cost of health care. This efficient workflow provides evidence for NIR imaging as a feasible and economic approach in the resection of glioblastomas.
8. Discussion
This systematic review highlights the usage of NIR fluorescence imaging in the resection of GBMs, one of the most aggressive and complex brain tumors. The findings display how NIR technology, especially within the NIR-II window, enhances the precision of tumor resections by improving intraoperative tumor visualization [69]. NIR results in a significantly higher gross total resection rate and better surgical precision when compared to conventional techniques [73]. NIR fluorescence imaging has shown promise in addressing the invasive nature of GBMs.
The primary benefit of NIR lies in its ability to facilitate live, high-contrast visualization of tumor margins. This is advantageous, particularly within GBM resections, where tumor cells can infiltrate nearby brain tissue, rendering it difficult to delineate resection boundaries. Being able to improve accuracy in tumor visualization allows for improved resections, which contributes to extended progression-free survival and overall survival in patients [73]. This capability is vital for surgeons who aim for maximal safe resection as GBM often infiltrates surrounding healthy brain tissue. NIR fluorescent immunoconjugates, such as cetuximab-IRDye800, increase fluorescence emission selectively in malignant tissues, aiding surgeons in distinguishing between healthy and cancerous tissues [71]. Performing resection with increased contrast is beneficial in guiding surgeons to remove tumor tissue while preserving healthy brain regions. For instance, median survival rates improved by 4-6 months in NIR-guided surgeries when compared to traditional approaches, emphasizing the potential of NIR as a critical tool in maximizing surgical outcomes [60]. Furthermore, NIR imaging is associated with higher gross total resection (GTR), a critical factor correlated with improved GBM patient prognosis [28,55,65]. A complete tumor resection is associated with extended survival rates and reduced postoperative recurrences.
While NIR imaging for GBM resection is highly sensitive, its low specificity poses a limitation in achieving precise tumor removal [70]. High sensitivity enables NIR to highlight areas with subtle differences in tissue properties, which is valuable for ensuring that residual tumor cells are not overlooked. Because NIR lacks specificity, however, it may also fluoresce in non-tumor areas, such as necrotic tissue or regions with altered blood-brain barrier permeability. This leads to false positives, where healthy brain tissue appears similar to malignant areas, increasing unnecessary excision. Preserving vital brain structures is critical, as excessive excision heightens the risk of neurological damage thus limiting the reliability of NIR imaging. Enhancing NIR specificity remains a priority to permit targeted resection and reduce the risk of neurological deficits.
In the context of future directions, the combination of intraoperative fluorescence and other imaging modalities may be studied in regard to enhancing the resection of GBM. For example, the synergistic use of fluorescent imaging with intraoperative MRI (iMRI) has been recommended to improve surgical precision [65,78]. NIR can enhance iMRI-guided surgeries by compensating for brain shift which iMRI alone may not account for dynamically. The combination of NIR and iMRI provides comprehensive visualization, where NIR assists with real-time optical guidance and iMRI confirms the removal of tumor tissue in non-fluorescent regions. NIR imaging may also be integrated with optical coherence tomography (OCT). NIR’s broader contrast between tumor and healthy tissues can potentially complement the high-resolution structural imaging offered by OCT, but further trials should aim to determine whether the combined approach yields improved clinical outcomes.
9. Conclusions
NIR fluorescence imaging represents a significant advancement in the management of GBM, enhancing tumor visualization, increasing gross total resection (GTR) rates, and improving patient outcomes, including progression-free and overall survival. This particular advantage provides real-time intraoperative guidance to perform safer and more accurate resections without harming critical brain structures. Further studies targeting the improvement of fluorophore selectivity and combination of NIR with other imaging techniques may enhance the accuracy of surgery and patient outcomes and may set NIR fluorescence as a new gold standard for glioblastoma resection. Although challenges remain, such as limited specificity and potential false positives, advancements in NIR-II technology offer deeper tissue penetration and better resolution, addressing some of these limitations. Further research into enhancing specificity as well as multimodal approaches, which include integrating NIR with other intraoperative methods, could potentially refine its application, optimize clinical outcomes, and pave the way for widespread usage within surgical oncology.
References
- Koshy M, Villano JL, Dolecek TA, Howard A, Mahmood U, Chmura SJ, et al. Improved survival time trends for glioblastoma using the SEER 17 population-based registries. J Neurooncol. 2012, 107, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Bonosi L, Marrone S, Benigno UE, Buscemi F, Musso S, Porzio M, et al. Maximal safe resection in glioblastoma surgery: A Systematic Review of advanced intraoperative image-guided techniques. Brain Sci. 2023, 13, 216. [Google Scholar] [CrossRef] [PubMed]
- de Robles P, Fiest KM, Frolkis AD, Pringsheim T, Atta C, St Germaine-Smith C, et al. The worldwide incidence and prevalence of primary brain tumors: a systematic review and meta-analysis. Neuro Oncol. 2015, 17, 776–783. [Google Scholar] [CrossRef]
- Lim J, Park Y, Ahn JW, Hwang SJ, Kwon H, Sung KS, et al. Maximal surgical resection and adjuvant surgical technique to prolong the survival of adult patients with thalamic glioblastoma. PLoS One. 2021, 16, e0244325. [Google Scholar]
- Molinaro AM, Hervey-Jumper S, Morshed RA, Young J, Han SJ, Chunduru P, et al. Association of maximal extent of resection of contrast-enhanced and non-contrast-enhanced tumor with survival within molecular subgroups of patients with newly diagnosed glioblastoma. JAMA Oncol. 2020, 6, 495–503. [Google Scholar] [CrossRef]
- Sanai N, Polley M-Y, McDermott MW, Parsa AT, Berger MS. An extent of resection threshold for newly diagnosed glioblastomas. J Neurosurg. 2011, 115, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Seker-Polat F, Pinarbasi Degirmenci N, Solaroglu I, Bagci-Onder T. Tumor cell infiltration into the brain in glioblastoma: From mechanisms to clinical perspectives. Cancers (Basel). 2022, 14, 443. [Google Scholar] [CrossRef]
- Lara-Velazquez M, Al-Kharboosh R, Jeanneret S, Vazquez-Ramos C, Mahato D, Tavanaiepour D, et al. Advances in brain tumor surgery for glioblastoma in adults. Brain Sci. 2017, 7. [Google Scholar]
- Åke S, Hartelius L, Jakola AS, Antonsson M. Experiences of language and communication after brain-tumour treatment: A long-term follow-up after glioma surgery. Neuropsychol Rehabil. 2023, 33, 1225–1261. [Google Scholar] [CrossRef]
- McCracken DJ, Schupper AJ, Lakomkin N, Malcolm J, Painton Bray D, Hadjipanayis CG. Turning on the light for brain tumor surgery: A 5-aminolevulinic acid story. Neuro Oncol. 2022, 24, S52–S61. [Google Scholar] [CrossRef]
- Hadjipanayis CG, Widhalm G, Stummer W. What is the surgical benefit of utilizing 5-aminolevulinic acid for fluorescence-guided surgery of malignant gliomas? Neurosurgery 2015, 77, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Suero Molina E, Schipmann S, Stummer W. Maximizing safe resections: the roles of 5-aminolevulinic acid and intraoperative MR imaging in glioma surgery-review of the literature. Neurosurg Rev. 2019, 42, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Kiesel B, Freund J, Reichert D, Wadiura L, Erkkilae MT, Woehrer A, et al. 5-ALA in suspected low-grade gliomas: Current role, limitations, and new approaches. Front Oncol. 2021, 11, 699301. [Google Scholar] [CrossRef] [PubMed]
- Pop CF, Veys I, Bormans A, Larsimont D, Liberale G. Fluorescence imaging for real-time detection of breast cancer tumors using IV injection of indocyanine green with non-conventional imaging: a systematic review of preclinical and clinical studies of perioperative imaging technologies. Breast Cancer Res Treat. 2024, 204, 429–442. [Google Scholar] [CrossRef]
- Kosaka N, Ogawa M, Choyke PL, Kobayashi H. Clinical implications of near-infrared fluorescence imaging in cancer. Future Oncol. 2009, 5, 1501–1511. [Google Scholar] [CrossRef]
- Xu R, Jiao D, Long Q, Li X, Shan K, Kong X, et al. Highly bright aggregation-induced emission nanodots for precise photoacoustic/NIR-II fluorescence imaging-guided resection of neuroendocrine neoplasms and sentinel lymph nodes. Biomaterials. 2022, 289, 121780. [Google Scholar]
- van Manen L, de Muynck LDAN, Baart VM, Bhairosingh S, Debie P, Vahrmeijer AL, et al. Near-infrared fluorescence imaging of pancreatic cancer using a fluorescently labelled anti-CEA Nanobody probe: A preclinical study. Biomolecules. 2023, 13, 618. [Google Scholar]
- Ullah Z, Roy S, Gu J, Ko Soe S, Jin J, Guo B. NIR-II fluorescent probes for fluorescence-imaging-guided tumor surgery. Biosensors (Basel). 2024, 14, 282. [Google Scholar]
- Wang T, Chen Y, Wang B, Gao X, Wu M. Recent progress in second near-infrared (NIR-II) fluorescence imaging in cancer. Biomolecules. 2022, 12, 1044. [Google Scholar]
- Chen X, Li Y, Su J, Zhang L, Liu H. Progression in near-infrared fluorescence imaging technology for lung cancer management. Biosensors (Basel). 2024, 14, 501. [Google Scholar]
- Li S, Johnson J, Peck A, Xie Q. Near infrared fluorescent imaging of brain tumor with IR780 dye incorporated phospholipid nanoparticles. J Transl Med. 2017, 15, 18. [Google Scholar] [CrossRef] [PubMed]
- Chehelgerdi M, Chehelgerdi M, Allela OQB, Pecho RDC, Jayasankar N, Rao DP, et al. Progressing nanotechnology to improve targeted cancer treatment: overcoming hurdles in its clinical implementation. Mol Cancer. 2023, 22, 169. [Google Scholar] [CrossRef] [PubMed]
- Wang F, Weng Y, Geng J, Zhu J. A narrative review of indocyanine green near-infrared fluorescence imaging technique: a new application in thoracic surgery. Curr Chall Thorac Surg. 2021, 3, 35–35. [Google Scholar] [CrossRef]
- Cho SS, Salinas R, Lee JYK. Indocyanine-green for fluorescence-guided surgery of brain tumors: Evidence, techniques, and practical experience. Front Surg. 2019, 6. [CrossRef]
- Lee JYK, Pierce JT, Zeh R, Cho SS, Salinas R, Nie S, et al. Intraoperative near-infrared optical contrast can localize brain metastases. World Neurosurg. 2017, 106, 120–130. [Google Scholar] [CrossRef]
- Cho SS, Teng CW, Ramayya A, Buch L, Hussain J, Harsch J, et al. Surface-registration frameless stereotactic navigation is less accurate during prone surgeries: Intraoperative near-infrared visualization using Second Window Indocyanine Green offers an adjunct. Mol Imaging Biol. 2020, 22, 1572–1580. [Google Scholar] [CrossRef]
- Lee JYK, Pierce JT, Thawani JP, Zeh R, Nie S, Martinez-Lage M, et al. Near-infrared fluorescent image-guided surgery for intracranial meningioma. J Neurosurg. 2018, 128, 380–390. [Google Scholar] [CrossRef]
- Palmieri G, Cofano F, Salvati LF, Monticelli M, Zeppa P, Perna GD, et al. Fluorescence-Guided Surgery for High-Grade Gliomas: State of the Art and New Perspectives. Technol Cancer Res Treat. 2021, 20, 15330338211021605. [Google Scholar] [CrossRef]
- Omuro A, DeAngelis LM. Glioblastoma and other malignant gliomas: a clinical review. JAMA. 2013, 310, 1842–1850. [Google Scholar] [CrossRef]
- Kanderi T, Munakomi S, Gupta V. Glioblastoma Multiforme. StatPearls [Internet]. StatPearls Publishing; 2024.
- Pichlmeier U, Bink A, Schackert G, Stummer W. Resection and survival in glioblastoma multiforme: An RTOG recursive partitioning analysis of ALA study patients. Neuro Oncol. 2008, 10, 1025–1034. [Google Scholar] [CrossRef]
- Della Pepa GM, Sabatino G, la Rocca G. “enhancing vision” in high grade glioma surgery: A feasible integrated 5-ALA + CEUS protocol to improve radicality. World Neurosurg. 2019, 129, 401–403. [Google Scholar] [CrossRef] [PubMed]
- Altieri R, Raimondo S, Tiddia C, Sammarco D, Cofano F, Zeppa P, et al. Glioma surgery: From preservation of motor skills to conservation of cognitive functions. J Clin Neurosci. 2019, 70, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Ewelt C, Nemes A, Senner V, Wölfer J, Brokinkel B, Stummer W, et al. Fluorescence in neurosurgery: Its diagnostic and therapeutic use. Review of the literature. J Photochem Photobiol B. 2015, 148, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Altieri R, Zenga F, Fontanella MM, Cofano F, Agnoletti A, Spena G, et al. Glioma surgery: Technological advances to achieve a maximal safe resection. Surg Technol Int. 2015, 27, 297–302. [Google Scholar]
- Altieri R, Meneghini S, Agnoletti A, Tardivo V, Vincitorio F, Prino E, et al. Intraoperative ultrasound and 5-ALA: the two faces of the same medal? J Neurosurg Sci. 2019, 63. [Google Scholar] [CrossRef]
- White HW, Naveed AB, Campbell BR, Lee Y-J, Baik FM, Topf M, et al. Infrared fluorescence-guided surgery for tumor and metastatic lymph node detection in head and neck cancer. Radiol Imaging Cancer. 2024, 6, e230178. [Google Scholar] [CrossRef] [PubMed]
- La Rocca G, Della Pepa GM, Menna G, Altieri R, Ius T, Rapisarda A, et al. State of the art of fluorescence guided techniques in neurosurgery. J Neurosurg Sci. 2020, 63. [Google Scholar] [CrossRef]
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009, 339, b2700–b2700. [Google Scholar] [CrossRef]
- Ellis DG, White ML, Hayasaka S, Warren DE, Wilson TW, Aizenberg MR. Accuracy analysis of fMRI and MEG activations determined by intraoperative mapping. Neurosurg Focus. 2020, 48, E13. [Google Scholar] [CrossRef]
- Ellingson BM, Wen PY, Cloughesy TF. Modified criteria for radiographic response assessment in glioblastoma clinical trials. Neurotherapeutics. 2017, 14, 307–320. [Google Scholar] [CrossRef]
- Ewelt C, Floeth FW, Felsberg J, Steiger HJ, Sabel M, Langen K-J, et al. Finding the anaplastic focus in diffuse gliomas: The value of Gd-DTPA enhanced MRI, FET-PET, and intraoperative, ALA-derived tissue fluorescence. Clin Neurol Neurosurg. 2011, 113, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Essig M, Shiroishi MS, Nguyen TB, Saake M, Provenzale JM, Enterline D, et al. Perfusion MRI: The five most frequently asked technical questions. AJR Am J Roentgenol. 2013, 200, 24–34. [Google Scholar] [CrossRef]
- Fink JR, Muzi M, Peck M, Krohn KA. Multimodality brain tumor imaging: MR imaging, PET, and PET/MR imaging. J Nucl Med. 2015, 56, 1554–1561. [Google Scholar] [CrossRef]
- Forster M-T, Hattingen E, Senft C, Gasser T, Seifert V, Szelényi A. Navigated transcranial magnetic stimulation and functional magnetic resonance imaging: Advanced adjuncts in preoperative planning for central region tumors. Neurosurgery. 2011, 68, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara N, Sakatani K, Katayama Y, Murata Y, Hoshino T, Fukaya C, et al. Evoked-cerebral blood oxygenation changes in false-negative activations in BOLD contrast functional MRI of patients with brain tumors. Neuroimage. 2004, 21, 1464–1471. [Google Scholar] [CrossRef] [PubMed]
- Bernstock JD, Gary SE, Klinger N, Valdes PA, Ibn Essayed W, Olsen HE, et al. Standard clinical approaches and emerging modalities for glioblastoma imaging. Neurooncol Adv. 2022, 4, vdac080. [Google Scholar]
- Martucci M, Russo R, Giordano C, Schiarelli C, D’Apolito G, Tuzza L, et al. Advanced magnetic resonance imaging in the evaluation of treated glioblastoma: A pictorial essay. Cancers (Basel). 2023, 15. [CrossRef]
- Zikou A, Sioka C, Alexiou GA, Fotopoulos A, Voulgaris S, Argyropoulou MI. Radiation necrosis, pseudoprogression, pseudoresponse, and tumor recurrence: Imaging challenges for the evaluation of treated gliomas. Contrast Media Mol Imaging. 2018, 2018, 1–6. [Google Scholar] [CrossRef]
- Nihashi T, Dahabreh IJ, Terasawa T. Diagnostic accuracy of PET for recurrent glioma diagnosis: a meta-analysis. AJNR Am J Neuroradiol. 2013, 34, 944–50. [Google Scholar] [CrossRef]
- Galldiks N, Stoffels G, Filss C, Rapp M, Blau T, Tscherpel C, et al. The use of dynamic O-(2-18F-fluoroethyl)-L-tyrosine PET in the diagnosis of patients with progressive and recurrent glioma. Neuro Oncol. 2015. [CrossRef]
- Glaudemans AWJM, Enting RH, Heesters MAAM, Dierckx RAJO, van Rheenen RWJ, Walenkamp AME, et al. Value of 11C-methionine PET in imaging brain tumours and metastases. Eur J Nucl Med Mol Imaging. 2013, 40, 615–635. [Google Scholar] [CrossRef]
- Leung, K. O-(2-[(18)F]fluoroethyl)-L-tyrosine. Molecular Imaging and Contrast Agent Database (MICAD). Bethesda (MD): National Center for Biotechnology Information (US); 2004.
- Chuanting L, Bin A, Yan L, Hengtao Q, Lebin W. Susceptibility-weighted imaging in grading brain astrocytomas. Eur J Radiol. 2010, 75, e81–5. [Google Scholar] [CrossRef] [PubMed]
- Stummer W, Pichlmeier U, Meinel T, Wiestler OD, Zanella F, Reulen H-J, et al. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre phase III trial. Lancet Oncol. 2006, 7, 392–401. [Google Scholar] [CrossRef] [PubMed]
- Mischkulnig M, Roetzer-Pejrimovsky T, Lötsch-Gojo D, Kastner N, Bruckner K, Prihoda R, et al. Heme biosynthesis factors and 5-ALA induced fluorescence: Analysis of mRNA and protein expression in fluorescing and non-fluorescing gliomas. Front Med (Lausanne). 2022, 9. [CrossRef]
- Maragkos GA, Schüpper AJ, Lakomkin N, Sideras P, Price G, Baron R, et al. Fluorescence-guided high-grade glioma surgery more than four hours after 5-aminolevulinic acid administration. Front Neurol. 2021, 12. [CrossRef]
- Kaneko S, Suero Molina E, Sporns P, Schipmann S, Black D, Stummer W. Fluorescence real-time kinetics of protoporphyrin IX after 5-ALA administration in low-grade glioma. J Neurosurg. 2022, 136, 9–15. [Google Scholar] [CrossRef]
- Widhalm G, Olson J, Weller J, Bravo J, Han SJ, Phillips J, et al. The value of visible 5-ALA fluorescence and quantitative protoporphyrin IX analysis for improved surgery of suspected low-grade gliomas. J Neurosurg. 2020, 133, 79–88. [Google Scholar] [CrossRef]
- Senders JT, Muskens IS, Schnoor R, Karhade AV, Cote DJ, Smith TR, et al. Agents for fluorescence-guided glioma surgery: a systematic review of preclinical and clinical results. Acta Neurochir (Wien). 2017, 159, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Stummer W, Tonn J-C, Goetz C, Ullrich W, Stepp H, Bink A, et al. 5-Aminolevulinic acid-derived tumor fluorescence: the diagnostic accuracy of visible fluorescence qualities as corroborated by spectrometry and histology and postoperative imaging. Neurosurgery. 2014, 74, 310–9. [Google Scholar] [CrossRef]
- Schupper AJ, Baron RB, Cheung W, Rodriguez J, Kalkanis SN, Chohan MO, et al. 5-Aminolevulinic acid for enhanced surgical visualization of high-grade gliomas: a prospective, multicenter study. J Neurosurg. 2022, 136, 1525–1534. [Google Scholar] [CrossRef]
- Eljamel, S. 5-ALA fluorescence image guided resection of glioblastoma multiforme: A meta-analysis of the literature. Int J Mol Sci. 2015, 16, 10443–10456. [Google Scholar] [CrossRef] [PubMed]
- Su X, Huang Q-F, Chen H-L, Chen J. Fluorescence-guided resection of high-grade gliomas: a systematic review and meta-analysis. Photodiagnosis Photodyn Ther. 2014, 11, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Suero Molina E, Stögbauer L, Jeibmann A, Warneke N, Stummer W. Validating a new generation filter system for visualizing 5-ALA-induced PpIX fluorescence in malignant glioma surgery: a proof of principle study. Acta Neurochir (Wien). 2020, 162, 785–793. [Google Scholar] [CrossRef]
- Cho SS, Salinas R, De Ravin E, Teng CW, Li C, Abdullah KG, et al. Near-infrared imaging with second-window indocyanine green in newly diagnosed high-grade gliomas predicts gadolinium enhancement on postoperative magnetic resonance imaging. Mol Imaging Biol. 2020, 22, 1427–1437. [Google Scholar] [CrossRef] [PubMed]
- Panagopoulos D, Strantzalis G, Gavra M, Korfias S, Karydakis P. The impact of intra-operative magnetic resonance imaging and 5-ALA in the achievement of gross total resection of gliomas: A systematic literature review and meta-analysis. Med Res Arch. 2022; 10. [CrossRef]
- Lai J, Deng G, Sun Z, Peng X, Li J, Gong P, et al. Scaffolds biomimicking macrophages for a glioblastoma NIR-Ib imaging guided photothermal therapeutic strategy by crossing Blood-Brain Barrier. Biomaterials. 2019, 211, 48–56. [Google Scholar] [CrossRef]
- Polikarpov DM, Campbell DH, McRobb LS, Wu J, Lund ME, Lu Y, et al. Near-infrared molecular imaging of glioblastoma by Miltuximab®-IRDye800CW as a potential tool for fluorescence-guided surgery. Cancers (Basel). 2020, 12, 984. [Google Scholar] [CrossRef]
- Reichel D, Sagong B, Teh J, Zhang Y, Wagner S, Wang H, et al. Near infrared fluorescent nanoplatform for targeted intraoperative resection and chemotherapeutic treatment of glioblastoma. ACS Nano. 2020, 14, 8392–8408. [Google Scholar] [CrossRef]
- Llaguno-Munive M, Villalba-Abascal W, Avilés-Salas A, Garcia-Lopez P. Near-infrared fluorescence imaging in preclinical models of glioblastoma. J Imaging. 2023, 9. [CrossRef]
- Kang D, Kim HS, Han S, Lee Y, Kim Y-P, Lee DY, et al. A local water molecular-heating strategy for near-infrared long-lifetime imaging-guided photothermal therapy of glioblastoma. Nat Commun. 2023, 14, 2755. [Google Scholar] [CrossRef]
- Zhao H, Li C, Shi X, Zhang J, Jia X, Hu Z, et al. Near-infrared II fluorescence-guided glioblastoma surgery targeting monocarboxylate transporter 4 combined with photothermal therapy. EBioMedicine. 2024, 106, 105243. [Google Scholar]
- Lee JYK, Thawani JP, Pierce J, Zeh R, Martinez-Lage M, Chanin M, et al. Intraoperative near-infrared optical imaging can localize gadolinium-enhancing gliomas during surgery. Neurosurgery. 2016, 79, 856–871. [Google Scholar] [CrossRef]
- Miller SE, Tummers WS, Teraphongphom N, van den Berg NS, Hasan A, Ertsey RD, et al. First-in-human intraoperative near-infrared fluorescence imaging of glioblastoma using cetuximab-IRDye800. J Neurooncol. 2018, 139, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Cao C, Jin Z, Shi X, Zhang Z, Xiao A, Yang J, et al. First clinical investigation of near-infrared window IIa/IIb fluorescence imaging for precise surgical resection of gliomas. IEEE Trans Biomed Eng. 2022, 69, 2404–2413. [Google Scholar] [CrossRef] [PubMed]
- Shi X, Zhang Z, Zhang Z, Cao C, Cheng Z, Hu Z, et al. Near-infrared window II fluorescence image-guided surgery of high-grade gliomas prolongs the progression-free survival of patients. IEEE Trans Biomed Eng. 2022, 69, 1889–1900. [Google Scholar] [CrossRef] [PubMed]
- Tsugu A, Ishizaka H, Mizokami Y, Osada T, Baba T, Yoshiyama M, et al. Impact of the combination of 5-aminolevulinic acid-induced fluorescence with intraoperative magnetic resonance imaging-guided surgery for glioma. World Neurosurg. 2011, 76, 120–127. [Google Scholar] [CrossRef]
Figure 1.
Setup for NIR-guided surgery.
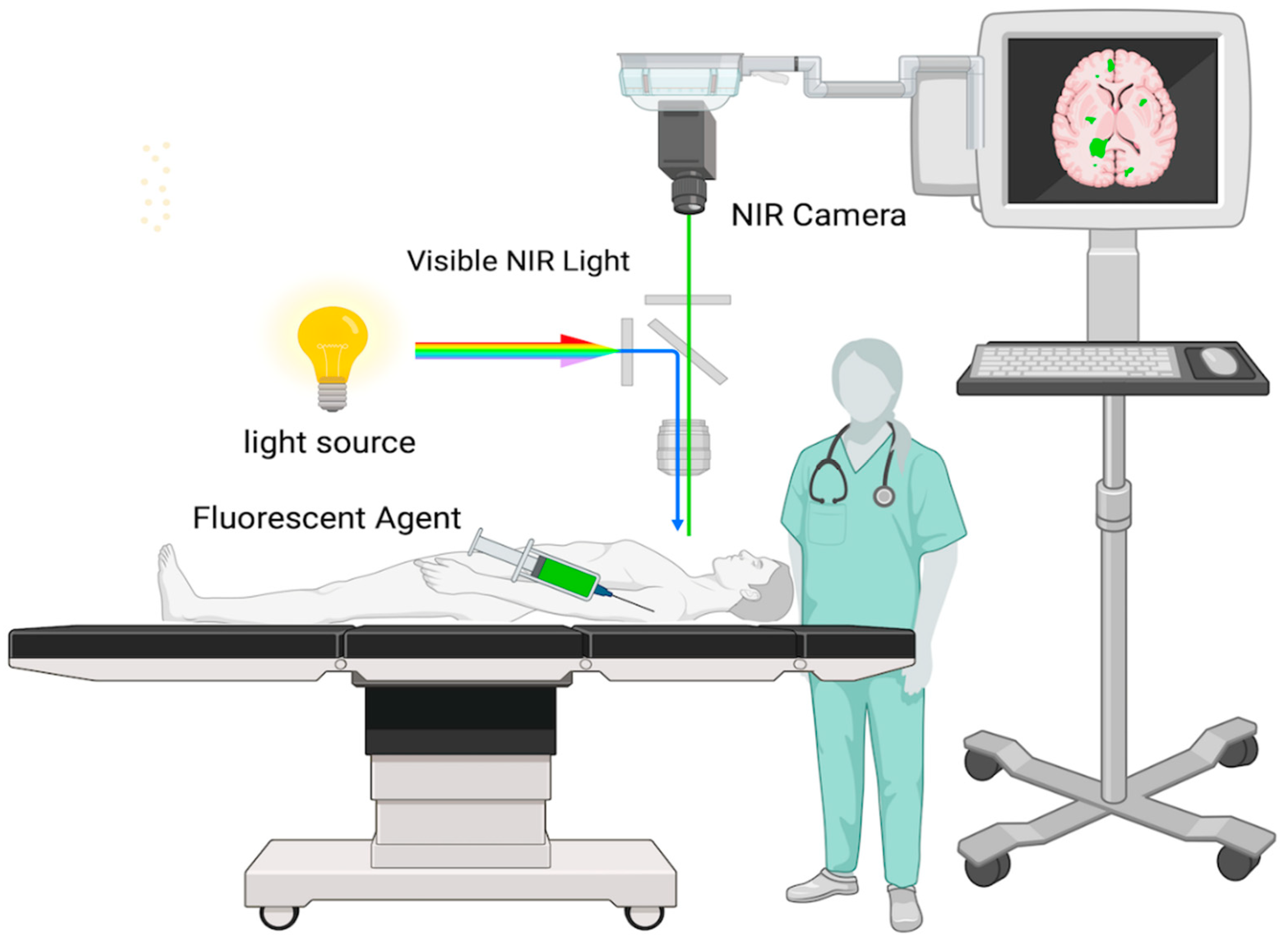
Figure 2.
Absorbance and Emission Spectra of NIR-II Fluorescence.
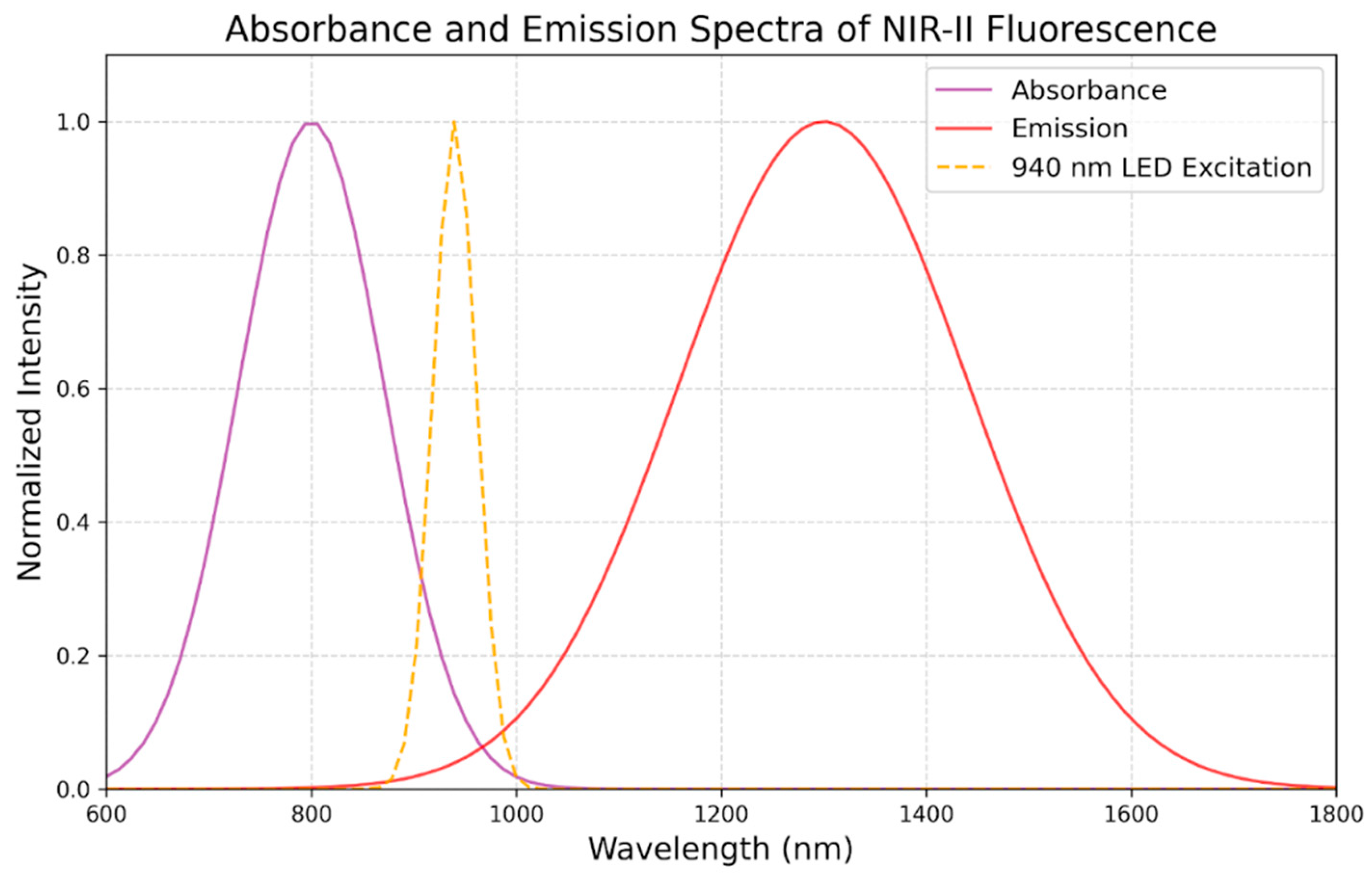
Figure 4.
Comparison of Gross total resection across different imagine modalties in GBM.
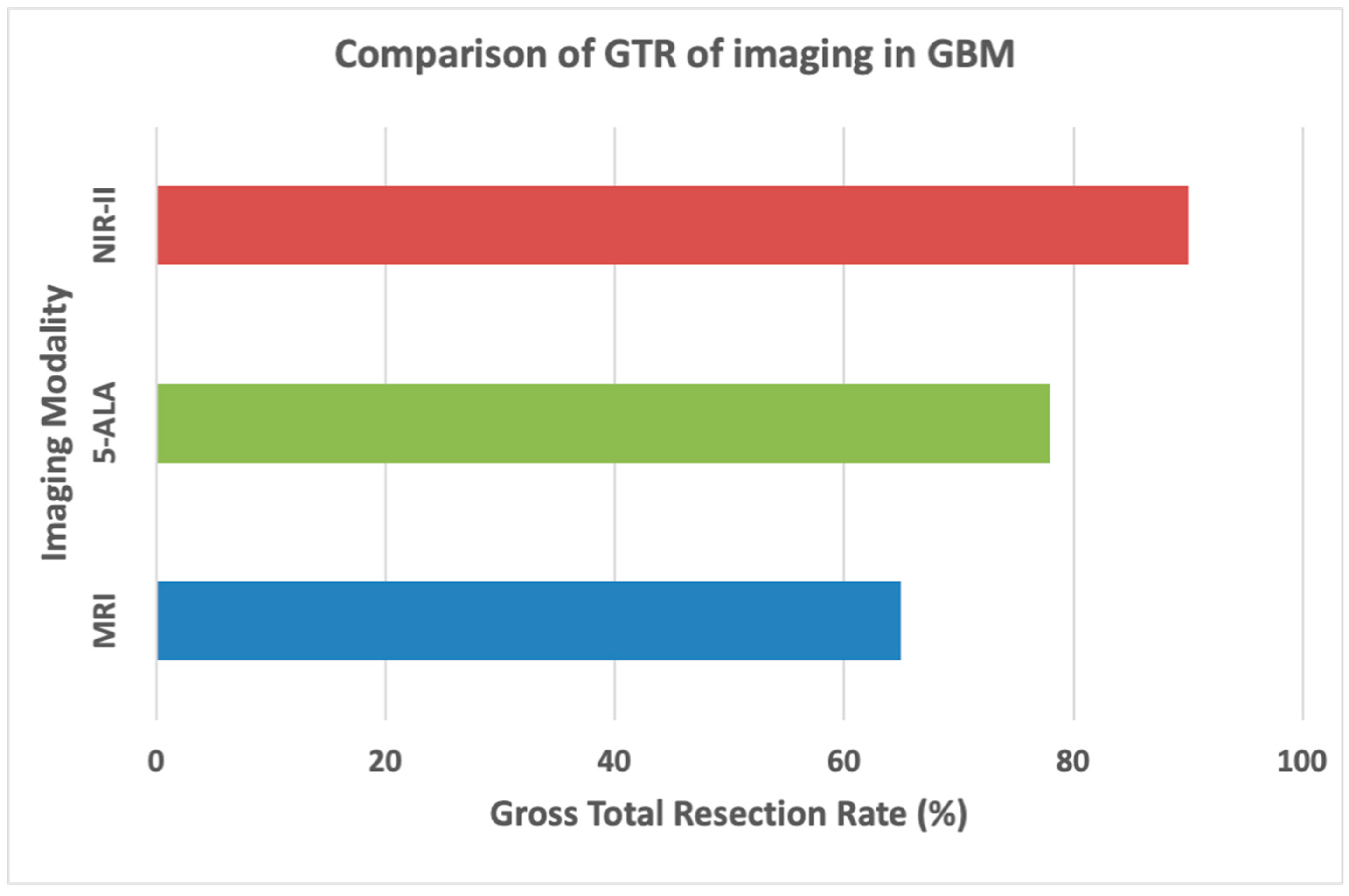

Table 1.
Techniques of Infrared Fluorescence Imaging.
| Technique | Description |
| Fluorescence Microscopy | Using this technique, the fluorescence released by the tumor during excision is seen using a surgical microscope fitted with a NIR filter. This enables the surgeon to keep an eye on the borders of the tumor while performing surgery. |
| NIR Imaging Systems | These are specific camera systems that display NIR fluorescence on an operating room screen upon detection. This allows the surgeon to see the fluorescence in real-time and can help spot tiny tumor remnants that could otherwise go undetected. |
| Handheld NIR Detectors | Certain methods view and detect near-infrared fluorescence using portable instruments. These can be helpful in confirming that there is no remaining tumor tissue following excision by scanning the operative field. |
Table 2.
Summary of Fluorophores for Glioblastoma Surgery.
| Fluorophore | Excitation (nm) | Emission (nm) | Brightness (M⁻¹cm⁻¹) | Strengths | Limitations |
| 5-ALA / PPIX | 405 | 635 | 400 | Good for tumor margin identification | Low brightness, limited penetration |
| Indocyanine Green (ICG) | 805 | 830 | 11,000 | High penetration, minimal autofluorescence | Smaller Stokes shift, needs precise calibration |
| Fluorescein | 489 | 515 | 75,000 | Excellent for surface imaging | Poor deep tissue visualization |
Table 3.
Advantages of NIR-II in glioblastoma resection.
| Advantage | Explanation |
| Deep Tissue Penetration | Compared to visible light, NIR light at these wavelengths can enter tissues more deeply. This makes it possible to find tumors that are beneath the brain's surface, which is crucial for glioblastoma surgery because these tumors frequently invade deeper brain regions. |
| Reduced Tissue Autofluorescence | Fluorescence imaging may be hampered by autofluorescence from nearby tissues, which lessens the contrast between the tumor and healthy tissue. By reducing autofluorescence, NIR wavelengths improve the signal-to-noise ratio and tumor visualization accuracy. |
| Compatibility with Fluorophores | The NIR region is where the peak excitation and emission wavelengths of fluorophores, such as indocyanine green (ICG), oc cur. Optimizing the image clarity and achieving maximal fluorescence intensity may be achieved by matching the wavelength to the characteristics of the fluorophore. |
| Minimized Light Scattering | At NIR wavelengths, there is less light scattering, which enhances contrast and resolution in images. This is especially crucial for recognizing tiny residual tumor deposits and for picking out minute features in the tumor margins. |
| Safety | Compared to other wavelengths, such as ultraviolet or blue light, NIR light is less damaging to tissues. Because of this, using it for an extended period of time during surgery is safer and lowers the danger of phototoxicity. |
Table 4.
Overview of Clinical Trials Using NIR Fluorescence in Glioblastoma Treatment.
| Study | NIR Agent/Technology | Findings | Survival Impact |
| Lai et al. [68] |
MDINPs (IR-792 dye) | Clear tumor visualization, photothermal therapy, extended survival by 6-8 days | Extended median survival to 22 days |
| Polikarpov et al. [69]. |
Mituximab®-IR800 | High tumor-to-background ratio (TBR: 10.1 ± 2.8), no adverse events | High specificity and safety; supports clinical use |
| Reichel et al. [70] |
HMC-FMX / PTX/CDDP | 28-72% survival increase with HMC-FMX + PTX/CDDP | 32 to 55 days survival with combination therapy |
| Dang et al. [72] |
Nd-Yb Co-doped NPs | Reduced tumor volume by 78.9%, effective tumor ablation with 1.0 μm NIR light | Improved survival with high-resolution imaging |
| Zhao et al. [73]. |
NIR-II with MCT4 probe | High SBR (2.8 intraoperative, 6.3 postoperative), robust BBB penetration | Supports survival via photothermal therapy |
| Lee et al.[74] | Second Window ICG | SBR of 9.5 ± 0.8; improved resection accuracy through intact dura; no adverse effects | Enhanced precision and safety with ICG fluorescence |
| Miller et al. [75]. |
Fluorescently Labeled Antibodies | Safe, feasible for human use, accurate tumor margin detection | Extended PFS and reduced residual tumor |
| Cao et al. [76]. |
NIR-IIa/IIb Imaging Instruments | Improved vascular resolution, reduced blood loss | Enhanced intraoperative safety and survival |
| Shi et al. [77] |
NIR-II Fluorescence Imaging | 100% complete resection rate, superior to 5-ALA and FS | 9-10 months PFS, 19-20 months OS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



