
Submitted:
21 October 2024
Posted:
22 October 2024
You are already at the latest version
Abstract
Adolescent eating disorders pose a significant public health challenge, deeply affecting both physical and emotional well-being. Early diagnosis is important for improving treatment outcomes, though it remains complex due to multiple influencing factors. The family perspective is essential in this process, as it provides valuable insights into changes in adolescents’ habits and emotional health. Methods: A descriptive qualitative study was conducted in Madrid, Spain, between January and February 2023, using a phenomenological approach to explore the experiences and perspectives of family members of adolescents with eating disorders. Results: Four thematic blocks with their categories were identified: (T1) Diagnosis, (T2) Family (T3) Resources, and (T4) Treatment. Participants emphasized the need for early intervention and a multidisciplinary approach to the treatment of eating disorders. Family therapy was recognized as vital in treatment, and common dissatisfaction in the public health structure underscored the need for greater investment in research and access to specialists. Mental health nurse practitioners have an important role in providing comprehensive care and support as well as mental health literacy. Conclusions: A holistic patient-centered approach, including family involvement and appropriate support systems, is key to improving outcomes and quality of life of adolescents undergoing treatment for eating disorders. Improving healthcare resources and addressing the challenges faced by families is essential. In addition, mental health literacy is critical, as it enables families to understand the disease better, make informed decisions, and actively participate in the recovery process, contributing to improved therapeutic outcomes and quality of life for patients.
Keywords:
Family Therapy
; Nursing
; Eating Disorders
; Qualitative Research
; Mental Health Literacy
1. Introduction
Eating disorders (EDs) are serious mental disorders that affect people's relationship with eating patterns, self-perception [1], and distortion of body image [2] and represent the third leading cause of chronic disease in adolescents behind obesity and asthma [3]. According to the latest update of Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR) published in 2022 [4], the main eating disorders include anorexia nervosa (AN), bulimia nervosa (BN) and binge eating disorder (BED). AN is defined by extreme restriction of energy intake, resulting in a significantly low body weight, an intense fear of weight gain, and a distorted perception of one's body image. As for BN, diagnostic criteria include recurrent episodes of binge eating, where the person consumes an excessive amount of food in a short period, followed by inappropriate compensatory behaviors, such as self-induced vomiting, laxative use or excessive exercise, occurring at least once a week for three months. For its part, BED is characterized by recurrent episodes of uncontrolled food intake, accompanied by significant emotional distress, without the presence of compensatory behaviors, and must also occur at least once a week for a minimum period of three months [4].
Although they can appear at any age, EDs are particularly prevalent in adolescents and young adults [5], a vulnerable group due to the physical, emotional, and social changes they experience during this stage of personal and family development [2]. The impact of EDs is not limited to physical health; it also profoundly affects mental health, personal relationships, and family environment [6]. The prevalence of EDs has increased significantly in recent decades [7] with the COVID-19 pandemic exacerbating eating disorders [2]. In addition, during COVID-19, an increased incidence of restrictive eating behaviors, binge eating, and increased exercise was reported in patients with eating disorders [8]. A recent review of epidemiological studies confirmed that the incidence of AN is increasing in young individuals worldwide, especially in those under 15 years of age, with a peak age of onset between 13 [9] and 18 years [10]. These disorders present differences in onset [11], with AN manifesting at younger ages than BN [12]. The lifetime prevalence of AN is 4% in the female population and 0.3% in the male population. The lifetime prevalence of BN is up to 3% in the female population and more than 1% in the male population, with symptoms increasing among girls aged 14 to 16 years and among boys aged 16 years and older [9,10].
The etiopathogenesis of EDs is multifactorial, involving both genetic and environmental factors [2]. Sociocultural influences, such as social pressure to conform to beauty standards, the impact of social media, and the overvaluation of thinness, exacerbate these disorders, making adolescents more vulnerable to dysfunctional eating behaviors [2,13]. Early diagnosis and appropriate intervention are necessary to improve prognosis and reduce associated risks, such as severe malnutrition, physical complications, and chronic emotional problems. Given their prevalence, severity, and tendency to become chronic, EDs represent a serious public health issue, requiring specialized treatment [14]. In this context, mental health literacy (MHL) is essential for effective EDs management. This concept is defined as the ability to obtain, process, and understand the knowledge and skills necessary to promote mental health [15]. For EDs patients and their families [16,17] an adequate MHL is essential for understanding the nature of the disorder, the importance of timely treatment, and how to meet the challenges of recovery, ultimately improving both physical and psychological outcomes [18,19,20].
Equally important is the role of the family, which serves as a fundamental pillar of care by observing early signs of EDs and offering support throughout diagnosis, treatment, and recovery [21]. A supportive family environment and active involvement positively influence treatment outcomes[22], but for families to provide effective support, they require information, emotional assistance, and tools to manage these complex conditions. Nursing professionals play a pivotal role in this process, acting as intermediaries in symptom identification, offering continuous support, and educating families about EDs [23,24]. As part of multidisciplinary teams, they implement therapeutic strategies, provide follow-up to prevent relapses, and facilitate communication between adolescents, their families, and others healthcare providers, ensuring a comprehensive approach to treatment [23,25].
This article seeks to explore family perspectives on the diagnosis of adolescent EDs, offering a qualitative approach to deep understanding the experiences, challenges, and emotional needs of families in this process. In doing so, it aims to highlight the importance of a holistic approach, where families and nursing professionals work together to improve outcomes in the treatment of adolescent EDs.
2. Methods
2.1. Study Design
A descriptive qualitative study based on the theoretical-methodological orientation of phenomenology was conducted to explore the experiences of family members of adolescent patients diagnosed with ED [26]. Phenomenology, which aims to understand the essence of a phenomenon through first-person narrated experiences, provides the framework for a detailed description of the family's lived experiences [27]. This study was conducted by the Consolidated Criteria for Reporting Qualitative Studies (COREQ) and the Standards for Reporting Qualitative Research [28]. (See Supplementary File 1)
2.2. Experience or Role of Researchers
The research team consisted of 4 women and 3 men, including 4 nurses with experience in qualitative research design (E.G.C.-B, E.M-M, A.T-R, C.G-M) and two researchers with clinical and research experience in mental health (P.D.-H; C-G.-N). Data were triangulated by two external researchers (E.V-V; C.G.-N). None of the research team members had a prior relationship with the participants. Commencing the study, the researchers’ position was determined based on their beliefs, previous experiences, theoretical framework, and motivation for the study.
2.3. Participants and Setting
A snowball-completed purposive sampling approach [29] was employed to recruit relatives of adolescents aged 12 to 19 years diagnosed with EDs. Participants who had not lived with the patient since diagnosis and those with a diagnosis less than one year ago were excluded. Data saturation was reached at participant number twelve when additional new information was attained, and further coding was no longer feasible [30]. Therefore, the researchers did not seek to recruit more participants. No dropouts occurred during the study. Table 1 shows the demographic data.
2.4. Data Collection Instrument
Data was collected between January and February 2023 through in-depth interviews and field notes. These interviews were conducted in a semi-structured manner, following a question guide designed to explore specific topics of interest (Table 2).
Semi-structured in-depth interviews were used as the primary data collection method. A question guide based on existing literature (Table 2) facilitated an in-depth exploration of participants' thoughts and experiences of the phenomenon [29]. Its flexible nature allows participants to express themselves freely while the researcher probes into areas of interest [31]. The interviews were conducted both face-to-face at the place and time preferred and via video call, based on the participant’s preferences by two researchers (E.G.C-B, C.G-M). Due to the topic´s sensitive nature, family members were informed that they could stop the interview at any time if they found it emotionally distressing. On average, each interview lasted approximately 57 minutes. Field notes were also collected by the researchers, providing additional insights into participants' personal experiences and behaviors during data collection, as well as the researchers' reflections on methodological aspects [32]. The transcripts were returned to the participants for additional comments, and all transcripts and field notes were securely stored in a digital location with restricted access.
2.5. Data Analysis
A qualitative analysis of each interview and the researchers' field notes was performed using an inductive thematic approach [33]. Codes were generated to identify the most descriptive content, which was then reduced and grouped to identify common categories representing significant content units. This process led to the emergence of thematic areas describing the experiences of the study participants. Double and independent coding was carried out by five researchers (E.G.C-B, C.G-M, A.T-R, E.M-M, P.D.-H) on each interview and each field note. They then met to discuss, compare, and refine their findings. Subsequently, the same process was carried out with the themes. In addition, joint meetings were held to consolidate the analysis results and represent the parents' experiences, as well as an external audit with an independent researcher to ensure confirmability. All codings were discussed by the research team until a consensus was reached on the main categories and themes, creating a final matrix of categories. The computer program ATLAS-TI-24 was used for the analysis.
2.6. Quality and Rigor Criteria
The studio was commissioned to develop comprehensive standards for providing information on current surveys [34] by the norms for the presentation of information on current investments [35]. To ensure the accuracy and reliability of the data, the Cuban and Lincoln standards must be taken into account [39]. (See Table 3)
2.7. Ethical Considerations
The study was conducted according to the Declaration of Helsinki and received ethical approval from the Research Ethics Committee of the University Hospital (PIC015-23FJD). All participants were informed of the objectives of the study and signed a written informed consent before the interviews, assuring them the right to withdraw at any time without consequences. The interviews were conducted anonymously, voluntarily, and confidentially, without collecting personal data or devices that could identify the informants, and were recorded with the permission of the participants and then transcribed verbatim. The information obtained was treated anonymously and confidentially, complying with the General Data Protection Regulation (EU) 2016/679 of the European Parliament and Organic Law 3/2018. The researchers did not report ethical, moral, or legal conflicts, nor did they receive financial compensation, just as the participants did not receive compensation for their collaboration in the study.
3. Results
Twelve individual interviews were conducted with family members of patients with eating disorders. More than half (58.33%) were female interviewees with a average age of 44.7 years. 75% were diagnosed with AN while 25% were diagnosed with BN with a mean average age at diagnosis of 17.4 years.
3.1. Themes
Four thematic blocks with their categories were identified: (T1) Diagnosis, (T2) Family (T3) Resources, and (T4) Treatment (See Table 4).
3.2. Theme 1. Diagnosis
During the interviews, participants shared their perspectives on possible triggers for EDs development in their family members and circumstances surrounding the onset of the disorder. Some mentioned the influence of social media and comparisons with peers as influential factors.
"My relative compared herself to girls her age, questioning why they could eat without gaining weight, while she felt that she gained weight even when eating minimal amounts of food "E6.
Additionally, traumatic events such as the death of a loved one were highlighted as possible triggers for ED:
"My relative faced a difficult emotional circumstance after her father´s death. She had a significant bereavement problem, which led her to self-harm and injure her wrists” E2.
Regarding the confinement due to the COVID-19 pandemic, it is not considered a triggering or aggravating reason, but it did complicate the situation experienced, and in some cases, this led many families to realize that their adolescents have an ED.
"Well, of course, you see yourself locked up at home without being able to go out, without being able to do sport, locked up like a family therapy beast everything. We all eat lunch, breakfast, and dinner at the same time and there is no way to escape.... So, yes, it was very traumatic then because she didn't want to leave the room, she cried...". E2
Participants also identified personality traits such as high levels of control and low self-esteem as influential factors in ED-related behaviors.
"She exercised, she went to the gym a lot, she is a very active person, very controlling, if she leaves something somewhere she wants to see it there, she has everything very controlled" E10.
Some agreed that low self-esteem was an underlying cause of their relatives' illness. According to their opinions, ED could manifest as a problem related to self-acceptance and self-esteem, including perfectionism. For them, the ED represents a more profound problem beyond the simple relationship with food.
"(...) but it is not about being fat or thin; it is a deeper problem of accepting yourself as you are, that is to say, that the manifestation is food, but the origin is something else" E11.
On the other hand, they noticed significant changes in the behavior of their loved ones :
"She used to be a cheerful and outgoing adolescent, but as a result of this whole process, she became defensive, bad-tempered, overreacting to any comment and even crying. The situation became complicated for everyone." E6
The situation became complex for everyone involved, as these emotional and behavioral changes profoundly impacted family dynamics. Furthermore, family members noted that their affected loved ones exhibited emotions and behaviors characterized by isolation, avoidance, and frequent bouts of bad moods. They described a shift in the individual's responses, becoming more defensive:
"I have always kept joking, and she has always played along with me... but I remember once I made a comment about her and her reaction was to start crying inconsolably. Apart from that, she was continually defensive." E7
When asked about their initial reaction to receiving their relative's diagnosis and its impact, it was found that more than half of the participants did not experience any significant change in their emotions. This lack of surprise was attributed to their pre-existing suspicions about the condition. One family member expressed this sentiment by saying:
"Mmm, I did not feel any special way because I already suspected it." E9
They had noticed certain signs and symptoms that led them to anticipate the possibility of an eating disorder.
However, there were others who, despite having some suspicions, still expressed surprise at the formal diagnosis. They acknowledged that they were expecting the news, but the severity of their relative's health situation surpassed their expectations. One participant explained:
"Well, the truth is that I was surprised because we were waiting to be told that, but I did not think it was or she was in such a serious moment." E4
This unexpected seriousness added an extra layer of complexity and concern to their emotions.
Furthermore, some family members admitted feeling confused in response to the diagnosis. They were unsure about how to handle the situation and what steps to take. The gravity of the situation and the unfamiliarity of dealing with an eating disorder led to a sense of uncertainty and unease. One participant shared their experience, saying:
I felt confused at the time of diagnosis because I did not know what to do..."E7.
The lack of clarity in understanding the disorder and its implications added to their emotional challenge in coping with the diagnosis.
Overall, the reactions to the diagnosis varied among family members, with some confirming their suspicions, others being surprised by the severity, and a few feeling unsure and confused about how to proceed. These emotions reflected the complexity of facing an eating disorder diagnosis within the family unit.
3.3. Theme 2. Family
Firstly, we explored the family structure and relationship, finding cases of both structured nuclei and contrasting situations. One participant described their family as a structured nucleus with parents and a sibling, while another mentioned experiencing problems at home after the death of the father, leading to a desire to leave home.
"We are family, the family nucleus in this case is structured, his father and I are together, and we have another son... "E1
"His father had died [...], he began to have a lot of problems at home, with his mother, he did not want to be with her, he wanted to leave home" E8.
Regarding the pre-existing relationship with their relative before the illness, all participants reported having a good relationship characterized by trust and open communication. There were no instances of a problematic relationship before the disorder emerged, as most participants described it as a typical and healthy family dynamic.
"A normal relationship, of trust, of asking for your opinion, advice... I mean, each adolescent is different, but it was a normal relationship" E12.
Interestingly, in one case, the illness seemed to have strengthened the family bond, making them feel more united and resilient:
"No, it didn't change, it hasn't changed. Not at all, it has strengthened; on the contrary, it has made us stronger" E1.
However, for most participants, the illness had a negative impact, leading to a breakdown in trust and a less intimate relationship. They attributed this change to the necessity of lying that often accompanies the development of the disorder.
"To act on the illness you need to lie, don't you? And then, of course, everything changed." E9
The impact of the illness extended beyond family relationships and permeated various aspects of daily life. Family members shared experiences of adjusting their routines and habits to accommodate the challenges posed by the illness. For some, holidays became stressful as they had to navigate unfamiliar territories and disrupted routines. Additionally, the marital relationship was heavily affected, causing disagreements and conflicts over the best approach to support their loved one's recovery:
"I had to change my daily life " E4 "The first year of holidays I remember it as a nightmare, we took her out of her comfort zone and it was chaotic." E6
"It worsened my relationship with my wife." E7
"We had many problems within the family nucleus, as my wife and I did not agree on the best way for her to be cured. We argued every day, we cried out of helplessness and although our aim was the same, we could not agree" E7.
"Above all, we saw that it was fundamental to be well in the marriage. That was paramount. And then, if you are well, you can help your children, but if not, you can't" E3.
In several cases, family members took on new roles, with siblings becoming caregivers. This change in roles brought about feelings of being overwhelmed, hopeless, and unsure of how to handle the situation. Some expressed frustration when their relative refused help, leaving them feeling powerless and desperate to assist.
"He changed with his siblings, because also siblings at the beginning tend to.... to watch over... and the role of siblings is not that" E4.
"You see that a person is drowning and you throw them a float, and they don't catch it" E4.
Furthermore, the slow progress of the illness added to the uncertainty and anxiety experienced by family caregivers. Eating disorders are often unpredictable, and not knowing what to expect or how to effectively support their loved one further compounds the burden they carry.
In addition, they reported that it was difficult to see the progress as it was slow; this generated uncertainty for them as it was not a predictable disease, and they did not know what was going to happen or how it was going to develop.
"Feeling hopeless... hopeless, I didn't see myself as capable" E7.
Despite the challenges, family involvement in the treatment process was highly valued and considered vital for the patient's recovery. Family members expressed a genuine interest in actively participating in their relative's treatment, often suggesting joint sessions or seeking educational resources to enhance their support, emphasizing the importance of family therapy and support in the recovery journey:
" (…) there were courses for families on how to deal with Christmas, meetings… and, believe me, that was fundamental to me and I truly believe, it was very important for her also" E2.
Most participants felt deeply involved in the treatment and considered their contribution highly valuable. Some expressed satisfaction with their involvement, while others expressed a strong sense of commitment.
3.4. Theme 3. Resources
All participants unanimously agreed that the public health system has scarce resources to effectively address the complexities of this type of pathology. Although they initially sought help from public services, none of their relatives received treatment there. They attributed this issue to the overwhelming number of patients and the lack of adequately trained staff, resulting in a saturated system and the experience of what is known as scarce public resources.
"The public health system, in my opinion, has very few resources for this type of patient" E7.
Participants highlighted the sluggishness of the services, including long waiting times for appointments and consultations, which hindered effective follow-up and continuity of care:
"Because of social security, they offered us a psychologist almost for the following year" E12.
Although they expressed satisfaction with the treatment and resources available during hospitalization, they emphasized that such care was only temporary, at the hospital level, and did not extend to outpatient settings, creating a gap in the long-term management of the disorder:
"(…) Yes, during her hospitalization, yes… she was very grateful because all the professionals in the hospital helped her a lot, they were great, but after that... mmm... I think it was not enough, she did not have a proper follow-up" E5.
Moreover, they raised concerns about the lack of resources and support available for patients who transitioned to adulthood and were no longer eligible for pediatric treatments. According to their perception, resources for adults were less comprehensive than those available for adolescents, and searching for appropriate resources was challenging upon reaching adulthood.
When seeking therapies or consultations with specialists in the field, they discovered that the options were predominantly in private health, leaving them to navigate this situation on their own, which incurred additional costs:
"She has been managing it privately, she has had to struggle and look for help on her own" E4
Based on their experiences, participants agreed that an effective treatment approach should involve a multidisciplinary team comprising psychologists, psychiatrists, nutritionists, mental health nurse practitioner, and other professionals. However, this comprehensive approach is hindered by the high cost of such services, making them inaccessible to many individuals and families:
"I was shocked at the prices charged by each one, there are few of them, and on top of that, they are very expensive privately" E7.
The role of nursing in the treatment process was highly regarded by those who had direct contact with mental health nurse practitioner, especially during hospitalization, where they had more contact with them, as well as in outpatient follow-ups:
"Nursing professionals have an essential role in the approach" E4.
However, some participants admitted that they were not fully aware of the specific role of mental health nurse practitioner in this area, as they had not had direct contact with nursing professionals during the disease:
"Honestly, I don't know because... surely yes, it is possible that nursing plays an important role, but so far we have not had the opportunity to learn about it" (E7).
Others recognized the significance of nurses working in parallel with doctors, emphasizing the importance of continuous and individualized care, which includes regular follow-up through calls or consultations, complementing medical treatment:
"It is very important that the doctor sees you, but the follow-up by the nurse…" E1.
3.5. Theme 4. Treatment
The vast majority of family members currently acknowledge that they would approach the situation differently based on their learning and experiences. As one participant aptly stated:
"Experience is the mother of science" E2.
They unanimously agreed on the importance of timely intervention in treating the illness, emphasizing the need to act swiftly without dismissing the possibility of the disorder, even in seemingly idyllic situations:
"Act quickly and don't keep thinking that it can't be because your daughter is idyllic... because you think that it can't happen to her and it does happen, and that ends up prejudicing the diagnosis of her illness" E6.
Over time, they gradually became more aware of the challenges they were facing and had to confront, prompting them to seek assistance and cope through various channels, ranging from primary care to the hospitalization of their relative. To address the complexities of the illness, family members embraced a multidisciplinary approach, seeking assistance from various professionals. They acknowledged the significance of incorporating family members into the therapeutic process, recognizing their role as essential caregivers:
"I think this help could be improved by doing family therapy, group therapy, or including family members in some kind of consultation or information session... to include them in the treatment as they are going to be the main caregivers" E4.
Despite this recognition, it was noted that none of the participants had received family-based therapy.
When asked about potential improvements to the healthcare resources for EDs, the responses varied. However, they unanimously agreed on the necessity of increasing the number of professionals to lower the doctor/nurse-patient ratio and ensure quality care with adequate time allocation for each individual's needs.
"I would like everything to be easier and quicker" E6.
They emphasized the importance of personalized attention, akin to treating other medical conditions where tailored treatment is provided.
"Like when you have a cold and they prescribe paracetamol, just the same” E1.
Moreover, given the significant impact on many individuals, they underscored the need for increased investment and research in EDs. They acknowledged the scarcity of information about these disorders and believed that further research could lead to the development of alternative and more effective treatment methods.
"I've read that it's what we know the least about; maybe they need to do more research" E5.
These results illustrate the complexity of families' perceptions and experiences of adolescent eating disorders. Figure 1 shows a map of agents and interactions and allows us to establish the following themes: 1. Diagnosis (Triggers, Personality traits, Behavioral changes, impact). The second theme deals with the family (Family relationship, marriage, change of role, role of the primary caregiver, and involvement). The third theme deals with resources (scarce public resources, and private costs, multidisciplinary teams, and nursing care) and the fourth theme deals with treatment (approaching the situation, seeking assistance and coping, and needs for improvement). All of these are interrelated with each other and with eating disorders through the ATLAS-TI program used to code and synthesize the data, and a graphic designer prepared the results in Figure 1 in the form of a map of agents and interactions.
4. Discussion
Eating disorders are complex diseases influenced by a combination of biological, environmental, social, psychological, and cultural factors [36,37]. The present study revealed family members' recognition of similarities between their loved ones' risk factors and the characteristics associated with EDs. Notably, low self-esteem emerged as a triggering factor, although no evidence of a pre-existing depressive state was found. The impact of social networks promoting certain beauty ideals and the exacerbating effects of the pandemic were also noted [38,39]. The pandemic, in particular, shed light on the eating disorders suffered by their family members
Family members play an important role as primary caregivers, assuming significant responsibilities and burdens that can negatively impact their well-being and quality of life [40,41]. In line with previous research, participants in our study expressed feelings of overwhelm, hopelessness, and powerlessness in their caregiving roles. Studies have shown that specific interventions targeted at families can significantly reduce the emotional burden, alleviate distress and anxiety, and enhance caregivers' general well-being and interpersonal skills [41]. In this context, nurses have a responsibility to provide clear and accessible information to both the patient and their family environment. Since EDs often involve a distorted understanding of body image and unhealthy eating patterns, those affected must receive ongoing education about the risks and consequences of their behavior. This is where MHL becomes vital, as a greater understanding of the disease allows patients and their families to recognize the severity of the disorder and the need to adhere to medical and nutritional recommendations [16,18,19,20]. Nurses not only impart knowledge but also encourage informed decision-making [42]. A person with a good level of MHL will be able to actively participate in their recovery process, which is essential in ED, where the patient will have a key role [19,24]. In addition, nurses help patients develop skills to recognize harmful behaviors and thoughts, teaching them how to make healthier food and self-care choices, such as identifying hunger and satiety cues, which is important to restoring balanced eating patterns [17,18,20,24,42].
The NICE clinical practice guideline emphasizes the importance of supporting adult caregivers through appropriate programs, information, and psychosocial support [43]. However, our results indicate that several participants felt excluded, lacked sufficient information, and were not adequately considered. To address this issue, it is essential to adopt a comprehensive approach that recognizes the multifaceted nature of eating disorders and includes aspects beyond nutrition, such as family relationships [44]. Through MHL, patients and their families can better understand how their emotions affect their eating behavior and how to address them as part of treatment [16,18,19]. By providing this understanding, nurses help patients come to terms with their disorder and engage more fully with recommended psychological and nutritional therapies, which is necessary for effective disease management [17,20,24].
Several studies have highlighted widespread dissatisfaction among family members regarding available care and resources for EDs [40,45]. The transition from adolescent to adult care poses challenges, resulting in a significant decrease in available resources upon reaching adulthood [46]. To ensure continuity of care, a multidisciplinary and individualized approach is essential, meeting the demands expressed by interviewed relatives who seek comprehensive care with diverse perspectives [40,44].
The significance of nursing in treating eating disorders is emphasized in various sources, highlighting the role of mental health nurse practitioners. These patients often present complex challenges, requiring personnel with specific expertise. Moreover, nursing is essential in health education, emphasizing self-care, patient autonomy, and the promotion of healthy eating habits [47]. Our study findings affected must receive participants who highlighted nurses’ essential role in caring for their relatives. Nurses were perceived as spending considerable time with the patients, fostering a close patient-professional relationship. This close bond proved valuable in providing effective care and support throughout the treatment process.
The involvement of specialized nurses in the management of eating disorders can contribute significantly to improved patient outcomes [17]. Their expertise in mental health and dedication to patient care makes them invaluable multidisciplinary team members. Moreover, their focus on health education empowers patients to take charge of their well-being, promoting positive lifestyle changes [48] and enhancing their overall treatment experience [18,19,49].
In conclusion, collaborative efforts among multidisciplinary teams and continuity of care during the transition from adolescent to adult care are important in improving outcomes for ED patients. Additionally, family members´ inclusion and consideration throughout the treatment process are vital for an effective and comprehensive approach to managing these complex diseases. Addressing the challenges faced by family caregivers is essential in providing comprehensive care and improving patient outcomes [16,20]. Moreover, increasing investment in research and public healthcare resources for EDs is imperative to meet the growing demand for specialized treatment.
4.1. Strengths and Limitations
The study provides valuable insight into the experiences and perceptions of family caregivers of individuals with eating disorders. Through its qualitative approach, a comprehensive and in-depth understanding of the challenges and needs faced by these families is achieved. By considering the views of diverse family members and health professionals, the study provides a multidisciplinary perspective on the treatment of eating disorders, enriching the overall understanding of the topic. In addition, the study provides practical recommendations, such as the importance of family therapy and the key role of nursing in treatment. These suggestions may inform future treatment protocols and interventions for eating disorders.
The study has limitations in that further research with larger and more diverse samples is needed to validate the results in different populations. The small sample size and possible lack of diversity among participants may limit the generalizability of the findings. Because the study relies on family members' accounts of their experiences, there is the potential for recall bias. Family members may not accurately recall all events or may perceive them differently from how they occurred. In addition, the qualitative nature of the data collected may introduce subjectivity into the interpretation of participants' responses. It is essential to ensure rigor in the analysis and interpretation of the data to minimize possible biases.
4.2. Nursing Implications
The study highlights the importance of adopting a personalized therapeutic approach for patients with eating disorders, emphasizing the need for healthcare professionals, such as psychologists, psychiatrists, nutritionists, and nurses, to work in a multidisciplinary team to address the multifactorial causes of these disorders. This approach will ensure that patients receive comprehensive and individualized care, promoting improved treatment outcomes. In addition, the research highlights the critical role of family members in the treatment process, noting that healthcare professionals should actively involve families in therapy sessions, support groups, and educational programs to improve patient care. Recognizing and addressing family dynamics can contribute significantly to the patient's recovery and overall well-being.
Likewise, the dissatisfaction expressed by family members about the insufficiency of public resources for the treatment of eating disorders requires urgent attention and health authorities should invest in increasing the availability of resources and specialized personnel to provide timely and quality care. Mental health nurse practitioners have a relevant role in the treatment of eating disorders, building strong therapeutic relationships, and promoting self-discipline and healthy eating habits. Patient empowerment is another area where MHL and nursing intertwine; nurses teach self-care skills that enable patients to take control of their recovery, including recognizing relapse symptoms and planning healthy meals.
In addition, they have a central role in the coordination of multidisciplinary care, ensuring that medical indications are translated into understandable terms for patients and families, which facilitates greater adherence to treatment. Finally, nurses are key in the prevention and early detection of eating disorders, intervening in community or school settings to promote MHL from early stages, enabling people to recognize the initial signs of an ED in themselves or others, which contributes to early diagnoses and more effective treatment.
5. Conclusions
In conclusion, our findings demonstrate that eating disorders do not have a singular trigger, highlighting the importance of personalized and tailored care to achieve effective treatment outcomes. The effects of these disorders go beyond the individual, affecting family dynamics and underscoring the need to involve families in the treatment process. Family members who assume the role of caregivers experience significant psychological implications, emphasizing the need to provide them with support and care as well. Dissatisfaction with public resources highlights the urgency of increasing the availability of specialized personnel and resources in the public health system.
In this context, MHL becomes an essential component, and nurses play a crucial role in raising this level of understanding. Through education, emotional support, promotion of self-care, and multidisciplinary coordination, they help patients better understand their disorder and make informed decisions about their recovery. This not only improves patients' prognosis but also contributes to relapsing prevention and better long-term quality of life. For future research, we recommend evaluating the efficacy of family therapy in the treatment of eating disorders, and exploring the impact of increasing public health investment and recruitment of specialized professionals to improve accessibility and quality of care. Involving patients in research will provide valuable insights and encourage more patient-centered care, leading to progress toward more holistic and effective treatment that benefits both patients and their families.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. The following supporting information can be reviewed in the COREQ Checklist document.
Author Contributions
Conceptualization, E.G.C; A.T.R and P.P.H.; methodology, A.T.R, E.G.C.; formal analysis, C.G.M.; investigation, E.C.S.; resources, P.P.H.; data curation, C.G.M.; writing—original draft preparation, E.G.C. and P.P.H.; writing—review and editing, E.V.V and E.M.M.; visualization,C.G.N; supervision, P.P.H.; project administration, E.G.C.; funding acquisition, P.P.H. All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted by the Declaration of Helsinki and received ethical approval from the Research Ethics Committee of the University Hospital (PIC015-23FJD).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data are available upon request of the first author.
Public Involvement Statement
There was no public involvement in any aspect of this research.
Guidelines and Standards Statement
this manuscript was written following the COREQ guideline for qualitative research.
Use of Artificial Intelligence
AI or AI-assisted tools were not used in drafting any aspect of this manuscript.
Acknowledgments
We would like to thank all the participants who contributed to this research.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Alfoukha, M.M.; Hamdan-Mansour, A.M.; Banihani, M.A. Social and psychological factors related to risk of eating disorders among high school girls. J. Sch. Nurs. 2019, 35, 169–177. [CrossRef]
- Gómez-Romero, M.R.; Montoro-Pérez, N.; Martín-Baena, D.; Talavera-Ortega, M.; Montejano-Lozoya, R. A descriptive cross-sectional study on eating disorders, suicidal thoughts, and behaviors among adolescents in the Valencian Community (Spain). The pivotal role of school nurses. J. Pediatr. Nurs. 2024, 75, 1–7. [CrossRef]
- Jowik, K.; Dutkiewicz, A.; Słopień, A.; Tyszkiewicz-Nwafor, M. A multi-perspective analysis of dissemination, etiology, clinical view and therapeutic approach for binge eating disorder (BED). Psychiatr. Pol. 2020, 54, 223-238. [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; DSM-V-TR; American Psychiatric Association: Washington, DC, USA, 2022.
- Yu, Z.; Muehleman, V. Eating disorders and metabolic diseases. Int. J. Environ. Res. Public Health 2023, 20, 2446. [CrossRef]
- Mora, F.; Alvarez-Mon, M.A.; Fernandez-Rojo, S.; Ortega, M.A.; Felix-Alcantara, M.P.; Morales-Gil, I.; Quintero, J. Psychosocial factors in adolescence and risk of development of eating disorders. Nutrients 2022, 14, 1481. [CrossRef]
- Wilksch, S.M.; O'Shea, A.; Ho, P.; Byrne, S.; Wade, T.D. The relationship between social media use and disordered eating in young adolescents. Int. J. Eat. Disord. 2020, 53, 96–106. [CrossRef]
- Phillipou, A.; Meyer, D.; Neill, E.; Tan, E.J.; Toh, W.L.; Van Rheenen, T.E.; Rossell, S.L. Eating and exercise behaviors in eating disorders and the general population during the COVID-19 pandemic in Australia: Initial results from the COLLATE project. Int. J. Eat. Disord. 2020, 53, 1158–1165. [CrossRef]
- Alsheweir, A.; Goyder, E.; Alnooh, G.; Caton, S.J. Prevalence of eating disorders and disordered eating behaviours amongst adolescents and young adults in Saudi Arabia: A systematic review. Nutrients 2023, 15, 4643. [CrossRef]
- Van Eeden, A.E.; Van Hoeken, D.; Hoek, H.W. Incidence, prevalence and mortality of anorexia nervosa and bulimia nervosa. Curr. Opin. Psychiatry 2021, 34, 515–524.
- Lozano, N.; Borrallo, Á.; Guerra, M.D. Anales del sistema sanitario de Navarra. An. Sist. San. Navarra 2022, 45, e1009.
- Lindvall Dahlgren, C.; Wisting, L.; Rø, Ø. Feeding and eating disorders in the DSM-5 era: A systematic review of prevalence rates in non-clinical male and female samples. J. Eat. Disord. 2017, 5, 56. [CrossRef]
- Smith, A.R.; Zuromski, K.L.; Dodd, D.R. Eating disorders and suicidality: What we know, what we don’t know, and suggestions for future research. Curr. Opin. Psychol. 2018, 22, 63–67. [CrossRef]
- Sattler, F.A.; Eickmeyer, S.; Eisenkolb, J. Body image disturbance in children and adolescents with anorexia nervosa and bulimia nervosa: A systematic review. Eur. Eat. Disord. Rev. 2020, 25, 857–865. [CrossRef]
- Jorm, A.F. Mental health literacy: Empowering the community to take action for better mental health. Am. Psychol. 2012, 67, 231–243. [CrossRef]
- Brooks, H.; Prawira, B.; Windfuhr, K.; Irmansyah, I.; Lovell, K.; Syarif, A.K.; Dewi, S.Y.; Pahlevi, S.W.; Rahayu, A.P.; Syachroni; Afrilia.; et al. Mental health literacy amongst children with common mental health problems and their parents in Java, Indonesia: A qualitative study. Glob. Ment. Health (Camb.)2022, 9, 72–83. [CrossRef]
- Özer, D.; Şahin Altun, Ö. Nursing students' mental health literacy and resilience levels: A cross-sectional study. Arch. Psychiatr. Nurs. 2024, 51, 222–227.
- Nobre, J.; Oliveira, A.P.; Monteiro, F.; Sequeira, C.; Ferré-Grau, C. Promotion of mental health literacy in adolescents: A scoping review. Int. J. Environ. Res. Public Health 2021, 18, 9500. [CrossRef]
- Cormier, E.; Park, H.; Schluck, G. College students' eMental health literacy and risk of diagnosis with mental health disorders. Healthcare (Basel) 2022, 10, 2406. [CrossRef]
- Carvalho, D.; Sequeira, C.; Querido, A.; Tomás, C.; Morgado, T.; Valentim, O.; Moutinho, L.; Gomes, J.; Laranjeira, C. Positive mental health literacy: A concept analysis. Front. Psychol. 2022, 13, 877611. [CrossRef]
- Flütsch, N.; Hilti, N.; Schräer, C.; Soumana, M.; Probst, F.; Häberling, I.; Berger, G.; Pauli, D. Feasibility and acceptability of home treatment as an add-on to family-based therapy for adolescents with anorexia nervosa: A case series. Int. J. Eat. Disord. 2021, 54, 1707–1710. [CrossRef]
- Holtom-Viesel, A.; Allan, S. A systematic review of the literature on family functioning across all eating disorder diagnoses in comparison to control families. Clin. Psychol. Rev. 2014, 34, 29–43. [CrossRef]
- Dezutti, J.E. Eating disorders and equine therapy: A nurse's perspective on connecting through the recovery process. J. Psychosoc. Nurs. Ment. Health Serv. 2013, 51(9), 24–31. [CrossRef]
- Navas-Echazarreta, N.; Satústegui-Dordá, P.J.; Rodríguez-Velasco, F.J.; García-Perea, M.E.; Martínez-Sabater, A.; Chover-Sierra, E.; Ballestar-Tarín, M.L.; Del Pozo-Herce, P.; González-Fernández, S.; de Viñaspre-Hernández, R.R.; et al. Media Health Literacy in Spanish Nursing Students: A Multicenter Cross-Sectional Study. Nurs. Rep. 2024, 14, 2565–2579. [CrossRef]
- Cole, B. Understanding eating disorders and the nurse's role in diagnosis, treatment, and support. J. Christ. Nurs. 2024, 41(2), 80–87.
- Giorgi, A. Concerning the application of phenomenology to caring research. Scand. J. Caring Sci. 2000, 14(1), 11–15. [CrossRef]
- Norlyk, A.; Harder, I. What makes a phenomenological study phenomenological? An analysis of peer-reviewed empirical nursing studies. Qual. Health Res. 2010, 20(3), 420–431. [CrossRef]
- Van Hout, M.C.; Crowley, D.; O'Dea, S.; Clarke, S. Chasing the rainbow: Pleasure, sex-based sociality and consumerism in navigating and exiting the Irish Chemsex scene. Cult. Health Sex. 2019, 21(9), 1074–1086. [CrossRef]
- Creswell, J.; Poth, C. Qualitative inquiry and research design: Choosing among five approaches. Los Angeles: SAGE Publications; 2018.
- Glaser, B.; Strauss, A.L. Discovery of grounded theory: Strategies for qualitative research. Routledge, 2017.
- Kusi, G.; Boamah Mensah, A.B.; Boamah Mensah, K.; Dzomeku, V.M.; Apiribu, F.; Duodu, P.A.; Adamu, B.; Agbadi, P.; Bonsu, K.O. The experiences of family caregivers living with breast cancer patients in low and middle-income countries: A systematic review. Syst. Rev. 2020, 9(1), 165. [CrossRef]
- Moser, A.; Korstjens, I. Series: Practical guidance to qualitative research. Part 3: Sampling, data collection, and analysis. Eur. J. Gen. Pract. 2018, 24(1), 9–18. [CrossRef]
- Braun, V.; Clarke, V. Is thematic analysis used well in health psychology? A critical review of published research, with recommendations for quality practice and reporting. Health Psychol. Rev. 2023, 17(4), 695–718. [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Criterios consolidados para informar investigaciones cualitativas (COREQ): Una lista de verificación de 32 elementos para entrevistas y grupos focales. Int. J. Qual. Health Care 2007, 19, 349–357.
- O'Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89(9), 1245–1251.
- Canals, J.; Arija, V. Risk factors and prevention strategies in eating disorders [Factores de riesgo y estrategias de prevención en los trastornos de la conducta alimentaria]. Nutr. Hosp. 2022, 39(Spec No2), 16–26.
- Mora, F.; Álvarez-Mon, M.A.; Fernández-Rojo, S.; Ortega, M.A.; Félix-Alcantara, M.P.; Morales-Gil, I.; Rodríguez-Quiroga, A.; Álvarez-Mon, M.; Quintero, J. Psychosocial factors in adolescence and risk of development of eating disorders. Nutrients 2022, 14(7), 1481. [CrossRef]
- Batista, M.; Žigić Antić, L.; Žaja, O.; Jakovina, T.; Begovac, I. Predictor of eating disorder risk in anorexia nervosa adolescents. Acta Clin. Croat. 2018, 57(3), 399-410.
- Mento, C.; Silvestri, M. C.; Muscatello, M. R. A.; Rizzo, A.; Celebre, L.; Praticò, M.; Zoccali, R. A.; Bruno, A. Psychological impact of pro-anorexia and pro-eating disorder websites on adolescent females: A systematic review. Int J Environ Res and Public Health 2021, 18(4), 2186. [CrossRef]
- Joy, E. A.; Wilson, C.; Varechok, S. The multidisciplinary team approach to the outpatient treatment of disordered eating. Curr. Sports Med. Rep. 2003, 2(6), 331-336. [CrossRef]
- Guillén, V.; Arnal, A.; Pérez, S.; Garcia-Alandete, J.; Fernandez-Felipe, I.; Grau, A.; Botella, C.; Marco, J. H. Family connections in the treatment of relatives of people with eating disorders and personality disorders: Study protocol of a randomized control trial. BMC Psychol 2023, 11(1), 88. [CrossRef]
- Tay, J.; Tay, Y.; Klainin-Yobas, P. Mental health literacy levels. Arch. Psychiatr. Nurs. 2018, 32, 757–763. [CrossRef]
- Pelone, F., Jacklin, P., Francis, J. M., & Purchase, B. Health economic evaluations of interventions for supporting adult carers in the UK: A systematic review from the NICE Guideline. Int. Psychogeriatr. 2022, 34(9), 839-852. [CrossRef]
- Alonso, M., Corral, I., González, J., Fernández, S., Becerro, R., & Losa, M. Anales del sistema sanitario de Navarra. An. sist. Sanit. 2021, 44(1), 41-49.
- Johns, G., Taylor, B., John, A., & Tan, J. Current eating disorder healthcare services: The perspectives and experiences of individuals with eating disorders, their families, and health professionals. BJPsych Open 2019, 5(4), e59.
- Figueroa, L. M., & Soto, M. Transitional care from adolescence to adulthood. Rev. de Salud Pública (Bogotá, Colombia) 2018, 20(6), 784-786.
- Corral, I., Alonso, M., González, J., Fernández, S., Becerro, R., & Losa, M. Holistic nursing care for people diagnosed with an eating disorder: A qualitative study based on patients and nursing professionals' experience. Perspect. Psychiatr. Care 2022, 58(2), 840-849.
- Morgado, T., & Botelho, M. R. Intervenções promotoras da literacia em saúde mental dos adolescentes: Uma revisão sistemática da literatura. Revista Portuguesa de Enfermagem e Saúde Mental 2014, 1, 90–96.
- Kieling, C., Baker-Henningham, H., Belfer, M., Conti, G., Ertem, I., Omigbodun, O., Rohde, L. A., Srinath, S., Ulkuer, N., & Rahman, A. Child and adolescent mental health worldwide: Evidence for action. The Lancet 2011, 378, 1515–1525. [CrossRef]
Figure 1.
Map of agents and interactions.
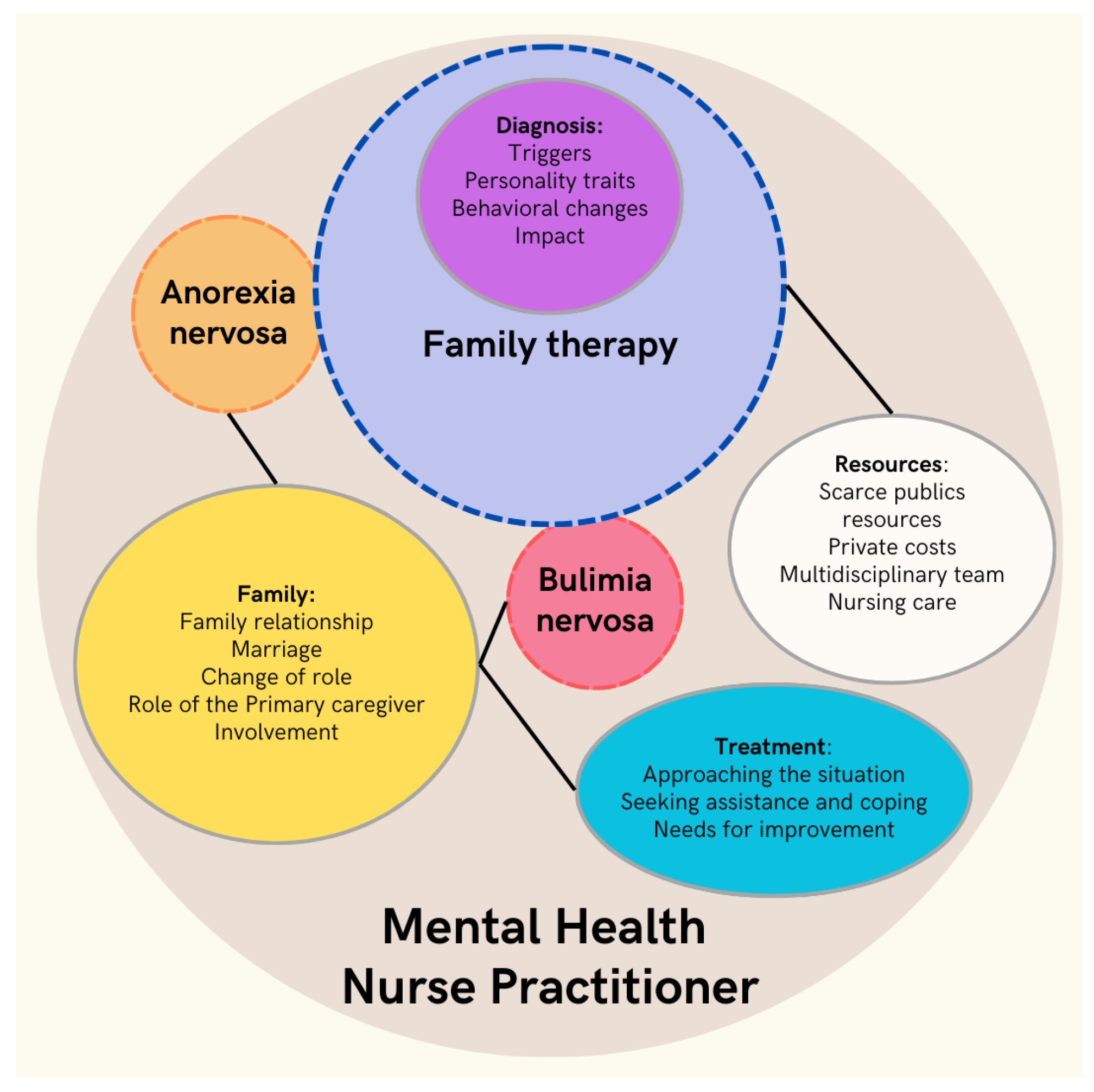

Table 1.
Participants characteristics (n = 12).
| Participants | Sex of interviewee | Age of interviewee | Relationship | EDs diagnosis | Age at diagnosis |
|---|---|---|---|---|---|
| E 1 | Woman | 56 | Mother | Anorexia nervosa | 19 |
| E 2 | Woman | 51 | Mother | Anorexia nervosa | 17 |
| E 3 | Man | 54 | Father | Anorexia nervosa | 17 |
| E 4 | Woman | 21 | Sister | Anorexia nervosa | 18 |
| E 5 | Man | 75 | Grandfather | Bulimia nervosa | 17 |
| E 6 | Woman | 49 | Mother | Anorexia nervosa | 17 |
| E 7 | Man | 50 | Father | Anorexia nervosa | 17 |
| E 8 | Woman | 25 | Sister | Bulimia nervosa | 18 |
| E 9 | Woman | 54 | Mother | Anorexia nervosa | 17 |
| E 10 | Man | 51 | Father | Anorexia nervosa | 17 |
| E 11 | Woman | 57 | Mother | Anorexia nervosa | 18 |
| E 12 | Man | 52 | Father | Bulimia nervosa | 17 |
E: interview.
Table 2.
Semi-structured question script.
| Research area | Interview Questions |
| Diagnostic feeling |
|
| Family relations |
|
| Assistance |
|
| Treatment |
|
Table 3.
Rigor criteria.
| Criteria | Techniques and procedures used |
| Credibility | - Researcher triangulation: each interview was analyzed by five researchers (E.G.C-B, C.G-M, A. T-R, E.M-M, P.D.-H) and two researchers with clinical and research experience in mental health (P.D.-H; C.G.-N). Team meetings were held to compare analyses and identify categories and themes with the rest of the team. - The analysis was carried out by five researchers and an external auditor (E.V-V). - Triangulation of data collection methods: Semi-structured interviews were conducted and field notes were taken by the researchers. - Participant validation (member-checking): Participants were offered the opportunity to review the audio recordings to confirm their experience. No additional comments were made by any of the participants. |
| Transferability | - Detailed descriptions of the study conducted, detailing the characteristics of the researchers, participants, settings, sampling strategies, and data collection and analysis procedures. |
| Reliability / Trustworthiness | - External researcher audit: An external researcher (E.V-V) assessed the research protocol, focusing on the methods applied and the study design. |
| Confirmability | - Researcher triangulation, member checking, and data collection triangulation. |
Table 4.
Themes and categories.
| Themes (T) | Categories | |
|---|---|---|
| T1 | Diagnosis | Triggers Personality traits Behavioral changes Impact |
| T2 | Family | Family relationship Marriage Change of role Role of the primary caregiver Involvement |
| T3 | Resources | Scarce publics resources Private costs Multidisciplinary team Nursing care |
| T4 | Treatment | Approaching the situation Seeking assistance and coping Needs for improvement |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



