
Submitted:
17 October 2024
Posted:
18 October 2024
You are already at the latest version
Abstract
Seafood is a vital source of nutrients, and its consumption has grown globally. Shellfish is a major cause of food allergy and anaphylaxis worldwide, affecting an estimated 0.5-2.5% of the general population. Most basic and clinical research has traditionally focused on crustaceans, leaving the characteristics of mollusk allergy poorly understood. In the Canary Islands, limpets (sea gastropod) are commonly consumed as part of the local cuisine. While some cases of limpet allergy have been reported, there are no published studies featuring large series or detailed clinical analyses of this specific food allergy. A cohort of patients with sensitization to limpet were studied: 66 were monosensitized to limpets (group A), while 64 were also sensitized to other shellfish (group B). Limpet ingestion caused delayed and severe symptoms. In group A, only 11,5% of patients showed positive shellfish allergen detection, compared to 67,9% in group B. The presence of protein bands in the 25-40 and 50-200 kDa range in monosensitized patients distinguishes our study from another researchs. Our study presents the largest reported series of patients with limpet allergy to date. The aim is to analyze the clinical and immunological characteristics of a local sample of limpet-allergic patients, contributing to a better understanding of this emerging condition.
Keywords:
Limpet allergy
; Gastropod allergy
; Mollusk allergy
; Anaphylaxis
; Food allergy
; shellfish allergy
; seafood allergy
; allergens
1. Introduction
Seafood, including both fish and shellfish, is a rich source of essential nutrients such as high-quality proteins and antioxidants, making it an important role in human nutrition. Its significance is particularly notable in countries where seafood is a staple due to dietary habits [1,2]. In recent years, global consumption of seafood has increased significantly, leading to a corresponding rise in allergic reactions [1,2].
The term “shellfish” typically refers to both crustaceans and mollusks, recognized for their nutritional significance. Shellfish belong to the group of Invertebrates, within the Animal Kingdom Eumatozoa, which is divided into four phyla: Mollusca, Arthropoda, Nematoda y Echinodermata. The phyla Arthropoda contains the subphylum Crustacea and includes the large group of crustacean foods, as well as another classes -Arachnida class and Insecta class- with arthropods with known allergy relevance (mites, parasites). Mollusca represent the largest marine phyla, with around 85000 described species [3], which are classified into eight classes, but only three are significant for human consumption: Cephalopoda (cuttlefish, squid, octopus), Bivalvia (clams, cockles, mussels, blue mussels, scallop, oyster), and Gastropoda classes (limpets, conchs, periwinkles, sea slugs, whelks, snails, and abalone) [4].
Food allergy (FA) refers to an adverse immune system reaction to certain foods [5]. The actual prevalence of FA is difficult to determine, but some reviews estimate that food allergies affect approximately 3.5%-4% of the global population [3,4]. Shellfish is one of the leading causes of FA and anaphylaxis worldwide, with prevalence estimated at around 0.5-2.5% of the general population, and varies based on geographical location and consumption habits [3]. For instance, in Spain, shellfish is the third most common cause of FA in adults, with a prevalence of around 14.8% and around 8.1% in Canary Islands [6], although, cases are increasingly reported at younger ages, after than milk, egg, fruit, and fish allergies [6]. Moreover, shellfish allergy is one of the leading causes of FA at any ages in many Asian countries, such as Thailand, Taiwan, Hong Kong, Vietnam, and Singapore, where shellfish is more frequently consumed [7,8].
Coastal regions of Asia are prominent consumers of crustaceans and mollusks, while Southern Europe, particularly Spain, favors cephalopods (octopus, squid) and other shellfish. Japanese diets feature higher quantities of squid, whereas Italians, French, Portuguese, and Spaniards consume significant amounts of terrestrial gastropod (snail) [3,7]. Consequently, although the importance of mollusk allergies is increasingly recognized, their prevalence remains unclear [9], due to research predominantly focusing on crustaceans, resulting in notably sparse studies on mollusk, particularly gastropod, allergies [7].
The probability of cross-reactivity between different shellfish and mollusk classes is not well established, with only a few proteins, such as tropomyosin—long considered the major allergen involved in shellfish and mite cross-reactivity—appearing to be shared by crustaceans and mollusks [10]. The described homology in the protein sequence between tropomyosin of different families of crustaceans (prawn, shrimp, lobster, etc.) is high, however, the homology between mollusk tropomyosin is lower [4,9,10,11,12]. Recent evidence suggests that other proteins may contribute to the immunological cross-reactivity of shellfish; however, these proteins have yet to be clearly identified [10].
In the Canary Islands, regional gastronomy includes the regular consumption of limpets (sea gastropod) as a local dish. In our area, we commonly consume two species of limpets mainly: Patella crenata (black limpet) and Patella aspera (white limpet). Some cases of limpet allergy had been reported, however, there are no published studies that include large series of this specific food allergy with in-depth clinical analysis, nor analyses of the allergenic composition of these two species.
The aim of this paper is to analyze the clinical and immunological characteristics of a sample of local limpet allergic patients, providing better knowledge of this emerging pathology.
2. Materials and Methods
2.1. Subjects
Patients (children and adult) with suggestive symptoms after ingestion of limpet were recruited from the Outpatient Allergy Clinic at Hospital Universitario de Canarias (Tenerife, Spain) from February 2022 to February 2023. This open longitudinal prospective study was previously authorized by the domestic Ethical Committee of Hospital Universitario de Canarias, Tenerife, Spain (CHUC_2022_10 (ECCIAALT). Written informed consent was obtained and signed by each patient, as well as parents or guardians for participants under 18 years old, upon inclusion in the current investigation.
2.2. Clinical History
The following clinical data were recorded: both sociodemographic information (gender, age, allergic comorbidities) and characteristics of food reactions, such as clinical and grade of symptoms (anaphylaxis, severe asthma, urticaria, angioedema, oral allergy syndrome, etc.), latency after consumption, emergency room visits, and prescribed treatment. Patients were also evaluated for tolerance or allergy to other shellfish, recording clinical symptoms after ingestion of any crustaceans, cephalopods, bivalves, or any other gastropods. The severity of allergic reactions was also evaluated by trained allergists according to specific guidelines [13].
The inclusion criteria involved a suggestive clinical history of allergy symptoms with a confirmed allergic sensitization -demonstrated either by skin tests and/or serum specific IgE (sIgE)- against gastropods (limpets and/or terrestrial snails).
Patients were excluded if they lacked a suggestive history following limpet ingestion, had no positive sIgE results against gastropods, were pregnant or were undergoing treatment with immunomodulatory agents, including biological therapies or immunosuppressants.
2.3. Skin Tests
The SPT was carried out according to European standards [14], attaching a 2 common commercial batteries (Laboratorios Inmunotek®, Spain): local aeroallergens (Dermatophagoides pteronyssinnus, Dermatophagoides farinae, Blomia tropicalis, Lepidoglyphus destructor, Tyrophagus putrescentiae, Alternaria alternata, cat and dog epithelium, grass mix- Poa pratensis, Dactilis glomerata, Lolium perenne, Phleum pratense and Festuca pratensis-, Parietaria judaica and Artemisia vulgaris) and shellfish extracts (shrimp, mussel, clam, squid, and oyster ). Any skin test was considered positive if the wheal was equal to or larger than 3 mm, with a negative control (saline solution) and positive control (histamine 10 mg/ml) [14]. Wheal diameters were measured after 20 minutes.
Due to the absence of commercial extract of limpet, we performed a prick-by-prick skin test with natural food on the volar side of each subject’s arm, using both raw and cooked presentations of limpet [5].
2.4. Limpet Extracts
Four limpet extracts were prepared based on the most frequent consumed species of limpet in our region: raw and cooked black limpet (Patella crenata) and raw and cooked white limpet (Patella aspera). The extracts were prepared extracting this material in 1/10 wt/vol 0.01 M phosphate buffered saline buffer (PBS, pH 7.2) for 16 hours at 5±3°C under magnetic starring. Then, the extracts were centrifugated at 15,000xg for 10 minutes at 4°C. Afterwards, the supernatant was recollected, clarified by filtration and dialyzed. Finally, the native extracts were frozen and lyophilized. The protein content was measured by Bradford method.
2.5. Serological Analysis
The RAST technique (Radio Allergo Sorbent Test, Pharmacia®, Sweden) was used to determinate the presence of seric sIgE (range 0.1kUA/L - 100kUA/L) against common aeroallergens, shellfish allergens and against terrestrial snail, the only gastropod sIgE available at this moment.
Levels of seric total IgE and sIgE were also measured by a multiplex array (ALEX® MacroArray Diagnostics, Vienna, Austria) according to the manufacturer’s instructions in all included subjects [15]. ALEX test performed contain 295 reagents -178 molecules and 117 extracts of airborne allergens and cross-reactive food allergens- with the ability of simultaneously measuring the concentration of seric sIgE (test range 0.3-50 kUA/L) and total IgE (test range 1-2500 kU/L). The different allergens and components are coupled onto polystyrene nano-beads, and then the allergen beads are deposited onto a nitrocellulose membrane, as formerly published [16]. A total of 5 shellfish molecular allergens were included in ALEX test: Pen m 1, Pen m 2, Pen m 3, Pen m 4 and Cra c 6.
2.6. SDS-PAGE and IgE Western Blot
Proteins from limpet extracts were separated by mini-PROTEAN TGX Stain-Free precast gels (Bio-Rad, Hercules, CA, USA) with sodium dodecylsulfate (SDS-PAGE) under reducing conditions according to Laemmli´s method [17]. Proteins were visualized by GelCode Blue stain reagent (Life Technologies, Carlsbad, CA, USA).
For Western Blot, proteins from the gel electrophoresis were electrotransferred to nitrocellulose membranes 0,45 µm (Bio-Rad Laboratories, Hercules, CA, USA). Ponceau Red 5% was added to previsualize the bands and, after washing with distilled water, the membrane was blocked with PBS 0.25%-Tween 20 0.5% (blocking solution) for 1 hour at room temperature. Then, the membrane was incubating with the corresponding serum overnight at 4ºC.
We performed two steps assay by Western blot with the aim of analyze the specific binding of IgE antibodies to allergens. First time Western Blot was carried out using pooled sera from randomly selected patients (16 from group A and another 16 from group B) to raw and cooked extract of both types of limpets: black limpet (Patella crenata) and white limpet (Patella aspera), followed by individual testing of N patients to same types of limpets and also shrimp extract.
2.7. Use of AI Assisted Tools
OpenAI´s ChatGPT (GPT4, OpenAI, San Francisco, CA, USA) was exclusively used to assist with text refinement and improving clarity. All content was reviewed and edited by the authors to ensure accuracy, and the final manuscript reflects the authors´original research and conclusions.
3. Results
3.1. Classification of the Study Population
Over a 12-months period from February 2022 to February 2023, we enrolled a total of 130 patients with sensitization to limpet or with a suggestive history of allergic reactions following to limpet ingestion or. Subsequently, individuals were categorized based on shellfish sensitization into two groups: group A (n=66) comprising exclusively limpet-sensitized individuals, and group B (n=64) consisting of those sensitized to limpet as well as other shellfish (cephalopods, bivalves, and/or crustaceans).
3.2. Demographic and Clinical Characteristics of Investigated Patients
After classifying patients into two groups the analysis of clinical presentations and demographic data was conducted separately for each group. We found no statistically significant differences (p > 0.05) in demographic and clinical characteristics between both groups (Table 1): they were mostly young adults (median age < 30 y.o.; p value 0.4433) but with a wide age range (4-62 y.o.), and there were not significant gender differences (p value= 0.3003).
3.2.1. Personal History: Respiratory Disease
Additionally, all patients presented a previous medical history of allergic rhinoconjunctivitis (92.5% group A, 84.4% group B) and/or asthma (39.4% group A, 42.2% group B). We can highlight that the 100% of our sample was sensitized to mites, being the animal epitheliums the second aeroallergen more frequent. The completed results were summarized in Table 2, as previous described in our area [18].
3.2.2. Food Allergy
Clinical symptoms following limpet ingestion manifested later than expected, with a mean value onset time of 120 minutes (range: 5 to 360 minutes in both groups) and were typically severe. The incidence of anaphylaxis was significantly (p=0.0027) higher in group A (66.7%) compared to group B (41.2%). This is reflected in the frequency of urgent medical assistance required (more than 50%) in both groups (Table 1).
In our cohort of patients with limpet allergy, severe bronchospasm following limpet ingestion ocurred independently of a prior asthma diagnosis. In group A, 40 out of 66 patients (60.6%) had no pre-existing asthma diagnosis, while in group B, 37 out of 64 patients (57.8%) similarly lacked such a diagnosis, however, respiratory symptoms were observed in both groups. In fact, in group A up to 29 out of 40 patients (72.5%) without a previous asthma diagnosis experienced respiratory symptoms after ingesting limpets: 7 cases of exclusive severe bronchospasm and 22 cases of anaphylaxis (including bronchospasm); and in group B up to 14 out of 37 patients (37.8%) without a previous asthma diagnosis presented respiratory symptoms: 5 cases of isolated severe asthma and 9 cases of anaphylaxis (Figure 3).
With respect to the tolerance of other shellfish groups, all patients in group A strictly avoided limpets after their allergic reaction. Among these, 48 out of 66 individuals (72.7%) demonstrated confirmed clinical tolerance to cephalopods, bivalves, and crustaceans. Conversely, 18 out of 66 individuals (27.3%) abstained from consuming any shellfish post-reaction, primarily due to fear of re-experiencing the sensation of impending doom. In group B, 34 out of 64 patients (53%) developed symptoms following the ingestion of limpets. The remaining 30 patients in group B (47%) exhibited symptoms after consuming other types of shellfish and were incidentally found to be sensitized to limpets, though they had never consumed them, as they had intentionally avoided limpet consumption. Furthermore, 14 out of the 34 patients (41.2%) who exhibited symptoms after limpet ingestion were able to tolerate cephalopods without further complications post-reaction.
3.3. Skin Tests, Total IgE and sIgE Reactivity
Regarding the prick-by-prick test with natural limpet, we did not find statistically significant differences between the results for raw or cooked limpet in both groups (p = 0.9644 in group A; p = 0.5894 in group B), nor between results of group A and group B (Table 3). The sensitivity as a diagnostic method obtained by this cutaneous test varies from 61% to 71%.
We found that the levels of total IgE were higher in group B than group A, but the difference was not statistically significant (p = 0.0525). Additionally, there was a greater recognition of sIgE to terrestrial gastropods (snail) in group B (91%) compared to group A (51%) (Table 3).
3.4. Molecular Profile According to Clinical Phenotypes
We then performed a specific molecular analysis using the multiplex platform ALEX® technique on an aleatory sample of 105 patients (52 from group A and 53 from group B): in both groups we have obtained a different pattern of positive results for at least one of the 6 shellfish allergens included in this technique, mostly tropomyosin, arginine kinase, and troponin C (Table 4).
In group A, only 6 out of 52 patients (11.5%) had a positive detection of tested shellfish allergens by ALEX® (Table 5). It is stricking that the most frequently recognized allergen was Cra c 6 (Troponin C), identified by 5 out of 52 patients (9.6%) (Table 5). Interestingly, one of these individuals recognized four allergens simultaneously: Pen m 1, Pen m 3, Pen m 4 and Cra c 6 (Table 5).

Table 5.
1 Selected patients (6 out 52) with positive results of shellfish allergens sensitization analysis by ALEX® (KU/L) in monosensitized to limpet group (group A).
Table 5.
1 Selected patients (6 out 52) with positive results of shellfish allergens sensitization analysis by ALEX® (KU/L) in monosensitized to limpet group (group A).
| Monosensitized selected patients |
Pen m 1 | Pen m 2 | Pen m 3 | Pen m 4 | Cra c 6 |
|---|---|---|---|---|---|
| 1 | <0.10 | <0.10 | <0.10 | <0.10 | 0.6 |
| 2 | 0.19 | <0.10 | <0.10 | <0.10 | 0.34 |
| 3 | <0.10 | <0.10 | <0.10 | <0.10 | 1.26 |
| 4 | 39.83 | <0.10 | 17.54 | 4.02 | >50 |
| 5 | 0.10 | 1.53 | <0.10 | <0.10 | <0.10 |
| 6 | 4.25 | <0.10 | <010 | <0.10 | 6.52 |
Table 5.
2. Specific IgE profiles aggregated into selected shellfish allergens (6 out 52 subjects) tested via microarray ALEX (KU/L). Profiles are ordered by the number of recognized molecules. (*) indicate sIgE sensitization to a single shellfish molecular allergen.
Table 5.
2. Specific IgE profiles aggregated into selected shellfish allergens (6 out 52 subjects) tested via microarray ALEX (KU/L). Profiles are ordered by the number of recognized molecules. (*) indicate sIgE sensitization to a single shellfish molecular allergen.
| n=6 | % | Number of molecules | Pen m 1 | Pen m 2 | Pen m 3 | Pen m 4 | Cra c 6 | |
|---|---|---|---|---|---|---|---|---|
| 3 | 50 | 1 | * | |||||
| 1 | 16.7 | 1 | * | |||||
| 1 | 16.7 | 2 | * | * | ||||
| 1 | 16.7 | 4 | * | * | * | * |
In group B, 36 out of 53 patients (67.9%) had a positive detection of tested shellfish allergens by ALEX® (Table 6). The most commonly identified allergen was Pen m 1 (tropomyosin), which was recognized by 25 out of 53 patients, constituting 47.17% (Table 6). Cra c 6 (Troponin C) was identified by 17 out of 53 patients (32.08%), while Pen m 2 (Arginine kinase) was recognized by 11 out of 53 patients, making up 20.75% (Table 6). The majority of patients identified one or two shellfish allergens. Only 4 out of 53 patients recognized three allergens simultaneously: one of them recognized Pen m 1, Pen m 2, and Pen m 3, and three recognized Pen m 1, Pen m 2, and Cra c 6 (Table 6).
Table 6.
1. Selected patients (36 out 53) with positive results of shellfish allergens sensitization by ALEX® (KU/L) in allergy to limpet and other shellfish group (group B). Results <0.1 are represented by (-).
Table 6.
1. Selected patients (36 out 53) with positive results of shellfish allergens sensitization by ALEX® (KU/L) in allergy to limpet and other shellfish group (group B). Results <0.1 are represented by (-).
| Patients group B | Pen m 1 | Pen m 2 | Pen m 3 | Pen m 4 | Cra c 6 |
|---|---|---|---|---|---|
| 1 | - | 4.03 | - | - | - |
| 2 | - | - | - | - | - |
| 3 | - | - | 0.13 | - | 0.67 |
| 4 | 0.67 | - | - | - | - |
| 5 | - | - | - | - | 0.59 |
| 6 | - | - | - | - | 1.94 |
| 7 | 45.17 | - | - | - | 0.17 |
| 8 | 42.12 | - | 0.18 | - | 1.36 |
| 9 | 31.01 | - | - | - | - |
| 10 | 44.99 | 12,95 | 2,23 | - | - |
| 11 | 0.54 | 1.60 | - | - | 0.60 |
| 12 | 37.49 | - | - | - | 10.32 |
| 13 | - | - | - | - | 8.99 |
| 14 | 22.89 | - | - | 0.27 | - |
| 15 | 43.42 | - | - | - | 0.73 |
| 16 | 11.49 | 0.33 | - | - | 3.48 |
| 17 | 0.43 | - | - | - | - |
| 18 | 112 | 3.03 | - | - | - |
| 19 | - | - | - | 10.04 | - |
| 20 | - | 0.87 | - | - | - |
| 21 | 27.21 | - | - | - | 6.95 |
| 22 | 5.92 | - | - | - | - |
| 23 | - | 2.16 | - | - | - |
| 24 | 2.40 | - | - | - | - |
| 25 | 30.31 | - | 0,15 | - | 1.17 |
| 26 | 1.02 | - | - | - | - |
| 27 | 30.37 | - | - | - | - |
| 28 | - | - | - | - | 6.76 |
| 29 | - | 5.57 | - | - | 4.53 |
| 30 | 0.62 | - | - | - | - |
| 31 | 42.04 | - | - | - | 3.79 |
| 32 | 9.08 | 2.43 | - | - | 2.8 |
| 33 | 0.62 | 0.36 | - | - | - |
| 34 | 9.87 | - | - | - | 9.21 |
| 35 | - | 0.86 | - | - | - |
| 36 | 40 | 0.59 | - | - | 1.03 |
Table 6.
2. Specific IgE profiles aggregated into selected shellfish allergens (6 out of 53 subjects) tested via microarray ALEX® (KU/L) . Profiles are ordered by the number of recognized molecules. (*) indicate positive sIgE to a single shellfish molecular allergen.
Table 6.
2. Specific IgE profiles aggregated into selected shellfish allergens (6 out of 53 subjects) tested via microarray ALEX® (KU/L) . Profiles are ordered by the number of recognized molecules. (*) indicate positive sIgE to a single shellfish molecular allergen.
| n=36 | % | Number of molecules | Pen m 1 | Pen m 2 | Pen m 3 | Pen m 4 | Cra c 6 | |
|---|---|---|---|---|---|---|---|---|
| 11 | 30.6 | 1 | * | |||||
| 4 | 11.1 | 1 | * | |||||
| 1 | 2.8 | 1 | * | |||||
| 5 | 13.9 | 1 | * | |||||
| 8 | 22.2 | 2 | * | * | ||||
| 2 | 5.6 | 2 | * | * | ||||
| 1 | 2.8 | 2 | * | * | ||||
| 1 | 2.8 | 3 | * | * | * | |||
| 3 | 8.3 | 3 | * | * | * |
3.5. SDS PAGE and IgE Western Blot
Subsequently, Western Blot was carried out in a first assay using pooled sera from both groups, followed by individual testing using sera from randomly selected patients: 16 monosensitized to limpets (group A) and another 16 sensitized to limpets and other shellfish (group B) (Figure 5). The first Western Blot analysis revealed a distinctive band recognition pattern among monosensitized patients (group A) for each analyzed sample.
Specifically, a band between 36 and 40 kDa was consistently recognized in both raw and cooked limpet extracts, along with weaker bands between 50 and 75 kDa. On the other hand, in the individual assay of selected 6 patients, western blot displayed several band recognitions between 50 and 200 kDa, and pattern band being more pronounced in raw extracts (contrasting with previous observations in shrimp extracts, where band recognition is typically more prominent in cooked extracts).
In cooked shrimp extract, while several bands were recognized with pooled sera, on an individual analysis bands were only observed in one patient. Notably, there was a patient who exhibited recognition of a mixture of bands across all extracts, a phenomenon challenging to interpret due to clinical tolerance (Figure 5).
Additionally, the Western blot analysis conducted with pooled sera from group B (patients sensitized to limpets and other shellfish) revealed a band recognition pattern similar to group A, albeit with greater intensity in group B. Furthermore, individually, the allergenic profile of the 16 patients sensitized to limpets and other shellfish exhibited recognition of approximately 4 bands between 15 and 40 kDa in both raw and cooked limpet extracts. Additionally, only 5 patients recognized bands between 50-200 kDa, with this recognition being more pronounced in the raw limpet extracts.
In the case of cooked shrimp extract, it was observed that 7 patients recognized some bands between 50-200 kDa, though quantification proved challenging (Figure 5).
4. Limitations
Currently, the lack of both a specific molecular diagnosis and commercial extract to this type of gastropod (limpet) restricts the diagnostic procedure, particularly in geographical areas where this consumption is more prevalent compared to others.
Additionally, in mild cases, many patients may opt out of undergoing the oral tolerance test, even in some cases they reported more than one episode after isolated consumption of limpets. It is essential to note that our study, conducted in a single center with a limited population, primarily the restricted scope of our sample and results.
5. Discussion
Allergy to gastropods is poorly documented in scientific literature, with only a limited number of reported cases. This lack of documentation could be attributed to the localized consumption of this type of shellfish, particularly limpets [7], with only a handful of published studies featuring concise case series focused on patients monosensitized to limpet [9,19,20,21,22,23].
The first two reported cases of limpet allergy surfaced in 1991, documented by Carrillo et al. in the Canary Islands [19]. The study featured two patients monosensitized to limpets, both experiencing anaphylaxis following isolated limpet ingestion. Subsequently, in 1994, Carrillo et al. expanded their study to include six patients, concluding that limpets could pose a potentially serious allergen for individuals previously sensitized to mites [20]. Conversely, in 2003, Azofra and coworkers described a short series of five patients with history of limpet allergy, and they identified a 75 kDa protein in their cases that could be related to Der p 4 amylase (60 kDa) [21]. In 2017, Azofra also pinpointed actin (45 KDa) in limpets, suggesting its involvement in the cross-reactivity between dust mites and gastropods [9]. However, the precise mechanisms of this cross-reactivity remain unclear. In populations like ours, it is conceivable that proteins shared between dust mites and gastropods may exist, suggesting the possibility of co-sensitization both. Notably, our study contributes the most extensive series of patients with limpet allergy to date.
In our current study, we enrolled 130 outpatients with a clinically-documented history of limpet allergy. Our patient cohort primarily consists of young adults, although with a wide range of age, with patients as young as four years old to elderly, and no significant differences in gender distribution. Notably, patients commonly reported experiencing a severe reaction upon limpet ingestion, from severe bronchospasm to anaphylaxis, with a significant proportion requiring urgent medical intervention. Consequently, strict avoidance of limpet consumption was recommended thereafter.
Unlike other shellfish allergies, where symptoms typically manifest quickly [22], the clinical symptoms in our study appeared later than expected, up to 120 minutes post-ingestion, but the range of reactions varies from immediate responses (within 30 minutes) to later responses occurring up to 6-8 hours. This contrasts with findings by Azofra et al. [9,21], who described a series of 5 patients, where symptoms were reported to occur within the first hour after ingestion in all cases. Similar to findings in other series, a significant percentage of our patients exhibited severe respiratory symptoms, including cases of anaphylaxis [19,24,25], especially in monosensitized to limpets (group A), as well as instances involving only severe bronchospasm, regardless of a pre-existing asthma diagnosis. Further studies are needed to determine whether O-glycosylation of proteins might be involved in this delayed mechanism, similar to what occurs in IgE-mediated reactions to alpha-gal in meat-allergic patients, where symptoms typically appear in a delayed manner [26,27,28].
While the gold standard for diagnosing food allergies remains the oral tolerance test, in many cases, due to the severity of symptoms and the heightened concern among patients, our diagnostic approach -like that in other published series- relied on a suggestive clinical history combined with the detection of sIgE, either through serum or cutaneous methods, which may provide sufficient evidence to confirm the diagnosis [5].
Despite previous studies suggesting that patients exhibited positive results only for prick-by-prick skin tests with cooked limpet extract [19], our study indicates variations in both extracts (from 61 to 71%). Discrepancies between our findings and those of other studies may stem from the limited statistical power inherent in smaller series.
The unavailability of serum sIgE laboratory tests against limpets led us to conduct tests against the only available gastropod, the terrestrial snail. Unfortunately, this approach did not consistently contribute to confirming sensitization according to our results, possibly due to the unknown cross-reactivity between limpets and terrestrial snails. The high percentage of negative results to terrestrial snail sIgE in the monosensitized group (49%) may be attributed to this unknown cross-reactivity, compounded by the limited consumption of terrestrial snails in our region, complicating the study of cross-reactivity between these gastropods.
Additionally, we have access to the ALEX® technique, which includes a panel of five well described shellfish allergens (Pen m 1, Pen m 2, Pen m 3, Pen m 4 y Cra c 6). In Group A, although they were monosensitive to limpet, up to 6 patients exhibited positive detection of several tested shellfish allergens. It is notable the low recognition of the allergens tested in this group, being more recognized the Cra c 6 (Troponin C) by 5 out of 6 patients. Intriguingly, only one patient recognized up to 3 allergens, Pen m 1, Pen m 3, and Pen m 4 simultaneously.
In contrast, Group B displayed a higher percentage of patients recognizing Pen m 1, Pen m 2, and Cra c 6. Further analysis revealed that 8 out of 53 patients in Group B recognized several allergens at the same time: 4 recognized Pen m 1, Pen m 2, and Cra c 6, 2 recognized Pen m 1 and Pen m 2, and 1 recognized Pen m 1, Pen m 2, and Pen m 3. This difference between both groups can be explained by the fact that in group B, the associated allergy to crustaceans and cephalopods. These proteins may play a role in the potential cross-reactivity between limpets and other mollusks or crustaceans, but polysensitization condition may be considered. Additionally, there may be cross-reactivity that accounts for the different foods involved in the seafood group.
A noteworthy distinction from other studies lies in the observation that a substantial number of our patients were not only monosensitized to limpets but also presented allergies to other classes of mollusks and crustaceans. This phenomenon may be attributed to either co-sensitization or cross-reactivity. Published studies have explored protein sequence homology, revealing ranges of 68% to 88% between different classes of mollusks and 56% to 68% between mollusks and crustaceans. Notably, these figures are lower than the protein sequence homology observed between different classes of crustaceans, which stands at 98% [4,9,10,11,12]. This underscores the complexity of allergic responses within and across different marine species and warrants further investigation to delineate the specific mechanisms underlying these sensitivities. However, comprehensive studies are required to elucidate and clarify these relationships further.
Conversely, there is a prevailing belief in the shared allergens between gastropods and dust mites, evidenced by the manifestation of allergic symptoms triggered by gastropods in patients always sensitized previously to dust mites, preceding the onset of food allergy [3,9,12,24,25,29,30,31,32]. In our selected patients, all presented mite allergic rhinoconjunctivitis and/or asthma, indicating a very close relationship between both allergies, aligning with prior observations [3,9,12,24,25,29,30,31,32]. The cross-reactivity between house dust mites and snails, specifically terrestrial gastropods, had been related to several mite allergens, including Der p 4, Der p 5, Der p 7, and hemocyanin [33]. Unlike crustaceans, tropomyosin does not appear to play a significant role in gastropod allergy [21]. In a minority of our patients (3.8% in Group A and 47.17% in Group B), we observed the recognition of tropomyosin (Pen m 1) as an allergenic protein. However, it is noteworthy that there have been reports of mollusk allergy in patients who tolerate crustaceans, and in those cases, tropomyosin was not implicated [9].
Nevertheless, comprehensive series and molecular studies are required to fully elucidate this complex matter and provide a better understanding of the mechanisms underlying cross-reactivity between dust mites and gastropods. Cross-reactivity among different gastropods or between gastropods and other shellfish remains understudied. Additionally, recent research suggests that O-glycosylation may play a role in patients experiencing anaphylaxis due to snails and allergy to Artemisia vulgaris [34]. This finding highlights the complexity of allergenic mechanisms and underscores the importance of further investigation into the role of glycosylation and its implications for shellfish allergy management and diagnosis [7,26,27,28].
Molecular-level identification of allergens in mollusks has been limited, with myosin (100 KDa) emerging as the sole allergen identified thus far, notably as the major allergen in abalone [4,35,36]. Additionally, Azofra et al., in northern Spain, described three new allergens in mollusks: actin (45 KDa) identified as the major allergen in razor fish and limpet, enolase (50 KDa) in razor fish, and a putative C1q domain-containing protein of 42 KDa in mussel [9]. These findings highlight the intricate nature of allergens in mollusks, underscoring the need for further research to comprehensively understand the molecular basis of allergic reactions in these marine species.
Nevertheless, a majority of our patients exhibited recognition of protein bands within the 25-40 kDa and 50-200 kDa range, a phenomenon not extensively described in other series focusing on limpet allergy. Bands exceeding 200 kDa suggest potential involvement of protein domains related to the three-dimensional structure of the heavy chain of myosin [9]. Interestingly, these high molecular weight bands have been previously identified in Helix aspersa as a major allergen [24]. While Lourenço Martins et al. ruled out the role of this high-molecular-weight protein in potential cross-reaction between gastropods and meat, they acknowledged its potential implication in cross-reactivity among mollusks, crustaceans, and arachnids [24].
Intriguingly, one out of the 16 patients recognized protein bands across all the extracts, a finding consistent with the observations of Misnan R et. al [31]. However, the underlying cause of this pattern remains unclear in our study. Further investigation is needed to elucidate the significance of this recognition and its potential implications for limpet and related allergen sensitivities. This observation underscores the highly heterogeneous profile of patients allergic to limpets.
6. Unmet Needs and Future Direction
At present, our diagnostic capabilities for gastropod allergy are limited. We rely on commercial snail extract available for conducting skin prick tests and sIgE testing against snail allergens. Unfortunately, there are no commercial extracts or specific seric IgE test available for limpet, necessitating the use of fresh raw and cooked food for skin prick tests to confirm allergic sensitization to gastropod [7].
Currently, the lack of both a specific molecular diagnosis and commercial extract to this type of gastropod restricts the diagnostic procedure, particularly in geographical areas where this consumption is more prevalent compared to others. There is an urgent need to optimize the diagnosis procedures of limpet allergy to enhance the performance of allergy studies and improve the accuracy of precision diagnosis. By doing so, we aim to reduce the unnecessary avoidance of limpets and related mollusks, to achieve a better and secure management options for our patient [7].
Additionally, efforts should focus on identifying allergenic proteins from various consumable gastropods to incorporate them into diagnostic tools. This approach aims to ascertain whether the coexistence of dust mite allergy and gastropod shellfish allergy, as well as allergy to other shellfish groups, arises from common proteins (cross-reactivity) or mere co-sensitization, thus providing insight into the actual probability of cross-reactivity between these groups. Allergic reactions to gastropods tend to be severe, posing potential life-threatening risks to affected individuals. Consequently, it is crucial to offer comprehensive health education, prescribe, and provide guidance on the use of epinephrine auto-injectors and other necessary medications. However, addressing these challenges consumes significant time and resources.
7. Conclusion
In conclusion, limpet, a commonly consumed sea mollusk in the Canary Islands, has led to a notable local prevalence of limpet allergies. Our study, to the best of our knowledge, presents the most extensive series of patients with limpet allergy reported to date. The identification of protein bands within the 25-40 and 50-200 kDa range in monosensitized patients distinguishes our findings from other series on limpet allergy. However, further studies are imperative to ascertain the specific allergens recognized by our patients and to elucidate their functions. These advancements not only facilitate the development of accurate diagnostic methods but also contribute to a deeper understanding of this condition, thereby improving overall knowledge, management and therapeutic interventions in the future of limpet allergies.
Author Contributions
Conceptualization and methodology, S.M.I., P.G.P and M.L.E.; software, M.L.E.; validation and formal analysis, G.P.R, S.M.I and P.G.P.; investigation and resources, G.T, M.MJ, P.F. and M.L.E.; data curation, M.L.E.; writing—original draft preparation, S.M.I. and M.L.E. writing—review and editing, P.F., G.P.R. and P.G.P.; visualization and supervision, S.M.I. and G.P.R.; project administration, M.L.E and P.G.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Hospital Universitario de Canarias (CHUC_2022_10 (ECCIAALT), February 2022), for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
the correnponding author have the data that belonging to SCS.
Acknowledgments
To the AAVV “Por la defensa del Caletón” (La Matanza of Tenerife, Spain) for their invaluable collaboration in the development of the project, and all nurses of Allergy Department of HUC for her implicated job and dedication. The authors acknowledge to OpenAI´s ChatGPT (GPT4, OpenAI, San Francisco, CA, USA) for assistance in refining the manuscript text. However, all interpretations, analyses and conclusions are the responsibility of the authors.
Conflicts of Interest
The authors declare no conflicts of interest. Specifically, G.T., M.MJ. and P.F. are full-time employees of Inmunotek SL Laboratories with no competing conflicts of interest that could influence the outcomes of research.
References
- Giovannini, M.; Beken, B.; Buyuktiryaki, B.; Barni, S.; Liccioli, G.; Sarti, L.; Lodi, L.; Pontone, M.; Bartha, I.; Mori, F.; et al. IgE-Mediated Shellfish Allergy in Children. Nutrients 2023, 15, 2714. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Cai, J.; Gao, T.; Ma, A. Shellfish consumption and health: a comprehensive review of human studies and recommendations for enhanced public policy. Crit Rev Food Sci Nutr. 2022, 62, 4656–4668. [Google Scholar] [CrossRef] [PubMed]
- Khora, S.S. Seafood-Associated Shellfish Allergy: A Comprehensive Review. Immunol Invest. 2016, 45, 504–30. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.L. Molluscan Shellfish Allergy. Advances in food and nutrition research. 2008, 54, 139–177. [Google Scholar] [CrossRef]
- Santos, A.F.; Riggioni, C.; Agache, I.; Akdis, C.A.; Akdis, M.; Álvarez-Perea, A.; Alvaro-Lozano, M.; Ballmer-Weber, B.; et al. EAACI guidelines on the diagnosis of IgEmediated food allergy. Allergy First Published, 10 October. [CrossRef]
- Alergológica 2015, SEAIC. Available online: https://www.seaic.org/inicio/noticias-general/alergologica-2015.
- Mederos-Luis, E.; Poza-Guedes, P.; Pineda, F.; Sánchez-Machín, I.; González-Pérez, R. Gastropod Allergy: A Comprehensive Narrative Review. Curr. Issues Mol. Biol. 2024, 46, 5950–5964. [Google Scholar] [CrossRef]
- Wai, C.Y.; Leung, N.Y.; Leung, A.S.; Wong, G.W.; Leung, T.F. Seafood allergy in Asia: geographical specificity and beyond. Frontiers in Allergy 2021, 2, 676903. [Google Scholar] [CrossRef]
- Azofra, J.; Echechipia, S.; Irazábal, B.; Muñoz, D.; Bernedo, N.; Gacía, B.E.; Gastaminza, G.; Goikoetxea, M.J.; Joral, A.; Lasa, E.; Gamboa, P.; Díaz, C.; Beristain, A.; Quiñones, D.; Bernaloa, G.; Echenagusia, M.A.; Liarte, I.; García, E.; Cuesta, J.; Martínez, M.D.; Velasco, M.; Longo, N.; Pastro-Vargas, C. Heterogenecity in allergy to mollusks: a clinicalimmunological study in a population from the north of Spain. J Investig Allergol Clin Immunol 2017, 27, 252–260. [Google Scholar] [CrossRef]
- Gelis, S.; Rueda, M.; Valero, A.; Fernández, E.A.; Moran, M.; Fernández-Caldas, E. Shellfish allergy: unmet needs in diagnosis and treatment. J Investig Allergol Clin Immunol 2020, 30, 409–420. [Google Scholar] [CrossRef]
- Ayuso, R. Update on diagnosis and treatment of shellfish allergy. Curr Allergy Asthma Rep. 2011, 11, 309–16. [Google Scholar] [CrossRef]
- Pedrosa, M.; Boyano-Martínez, T.; García-Ara, C.; Quirce, S. Shellfish Allergy: a comprehensive Review. Clin Rev Allergy Immunol. 2015, 49, 203–16. [Google Scholar] [CrossRef]
- Arasi, S.; Nurmatov, U.; Dunn-Galvin, A.; Daher, S. ; Roberts, G.; Turner, P.J.; Shinder, S.B.; Gupta, R.; Eigenmann, P.; et al. Consensus on Definition of food allergy severity (DEFASE) an integrated mixed methods systematic review. World Allergy Organization Journal 2021, 14, 100503. [Google Scholar] [CrossRef] [PubMed]
- Heinzerling, L.; Mari, A.; Bergmann, K.C.; Bresciani, M.; Burbach, G.; Darsow, U.; Durham, S.; Fokkens, W.; Gjomarkaj, M.; Haahtela, T.; et al. The skin prick test-European standards. Clin. Transl. Allergy 2013, 3, 3. [Google Scholar] [CrossRef] [PubMed]
- Bojcukova, J.; Vlas, T.; Forstenlechner, P.; Panzner, P. Comparison of two multiplex arrays in the diagnostics of allergy. Clin. Transl Allergy 2019, 9, 31. [Google Scholar] [CrossRef]
- Lis, K.; Bartuzi, Z. Selected Technical Aspects of Molecular Allergy Diagnostics. Curr Issues Mol Biol. 2023, 45, 5481–5493. [Google Scholar] [CrossRef]
- Laemmli, U.K. Cleavage of structural proteins during the Assembly of the head of bacteriophage T4. Nature 1970, 227, 680–685. [Google Scholar] [CrossRef]
- González-Pérez, R.; Poza-Guedes, P.; Pineda, F.; Galán, T.; Mederos-Luis, E.; Abel-Fernández, E.; Martínez, M.J.; Sánchez-Machín, I. Molecular Mapping of allergen exposome among different atopic phenotypes. Int. J. Mol. Sci. 2023, 24, 10467. [Google Scholar] [CrossRef]
- Carrillo, T.; De Castro, F.R.; Cuevas, M.; Caminero, J.; Cabrera, P. Allergy to limpet. Allergy 1991, 46, 515–519. [Google Scholar] [CrossRef]
- Carrillo, T.; Rodríguez de Castro, F.; Blanco, C.; Castillo, R.; Quiralte, J.; Cuevas, M. Anaphylaxis due to limpet ingestión. Ann Allergy 1994, 73, 504–8. [Google Scholar]
- Azofra, J.; Lombardero, M. Limpet Anaphylaxis: cross-reactivity between limpet and house-dust mite Dermatophagoides pteronyssinus. Allergy 2003, 58, 146–149. [Google Scholar] [CrossRef]
- Gutiérrez-Fernández, D.; Fuentes-Vallejo, M.S.; Bartolomé-Zavala, B.; Foncubierta-Fernández, A.; Lucas-Velarde, J.; León-Jiménez, A. Urticaria-angioedema due to limpet ingestión. J Allergol Clin Immunol 2009, 19, 64–79. [Google Scholar]
- Mederos-Luis, E.; Poza-Guedes, P.; Martínez, M.J.; González-Pérez, R.; Galán, T.; Sánchez-Machín, I. Limpet molecular profile: tropomyosin or not tropomyosin, that is the question. Thematic poster session (TPS). Allergy 2023, 78, 283–682. [Google Scholar] [CrossRef]
- Lourenço-Martins, L.M.; Peltre, G.; Fialho da Costa-Faro, C.J.; Vieira-Pires, E.M.; Da Cruz-Inacio, F.F. The Helix aspersa (brown garden snail) allergens repertoire. Int Arch Allergy Immunol 2005, 136, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Lopata, A.L.; Zinn, C.; Potter, P.C. Characteristics of hypersensitivity reactions and identification of a unique 49 kd IgE-binding protein (Hal-m-1) in abalone (Haliotis midae). J Allergy Clin Immunol 1997, 100, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.H.; Mirakhur, B.; Chan, E.; Le, Q.-T.; Berlin, J.; Morse, M.; Murphy, B.A.; Satinover, S.M.; Hosen, J.; Mauro, D.; et al. Cetuximab induced anaphylaxis and IgE specific for galactose-a-1,3-galactose. N. Engl. J. Med. 2008, 358, 1109–1117. [Google Scholar] [CrossRef]
- Commins, S.P.; Satinover, S.M.; Hosen, J.; Mozena, J.; Borish, L.; Lewis, B.; Woodfolk, J.A.; Platts-Mills, T.A. Delayed anaphylaxis, angioedema, or urticaria after consumption of red meat in patients with IgE antibodies specific for galactose-a-1,3-galactose. J. Allergy Clin. Immunol. 2009, 123, 426–433. [Google Scholar] [CrossRef]
- Homann, A.; Schramm, G.; Jappe, U. Glycans andglycan-specific IgE in clinical and molecular allergology: Sensitization, diagnostics and clinical symptoms. J. Allergy Clin. Immunol. 2017, 140, 356–368. [Google Scholar] [CrossRef]
- Van Ree, R.; Antonicelli, L.; Akkerdaas, J.H.; Pajno, G.B.; Barberio, G.; Corbetta, L.; Ferro, G.; Zambito, M.; Garritani, M.S.; Aalberse, R.C.; Bonifazi, F. Asthma after consumption of snails in house-dust-mite-allergic patients: a case of IgE cross-reactivity. Allergy 1996, 51, 387–393. [Google Scholar]
- Vidal, C.; Bartolome, B.; Rodríguez, V.; Armisén, M.; Linneberg, A.; González-Quintela, A. Sensitization pattern of crustacea-allergic individuals can indicate allergy to mollusks. Allergy 2015, 70, 1493–1496. [Google Scholar] [CrossRef]
- Misnan, R.; Abd Aziz, N.S.; Yadzir, Z.H.M.; Bakhtiar, F.; Abdullah, N.; Murad, S. Impact of thermal treatments on major and minor allergens of sea snail, Cerithidea obtuse (obtuse horn shell). Ira J Allergy Asthma Immunol. 2016, 15, 309–316. [Google Scholar]
- Klaewsongkram. High prevalence of shellfish and house dust mite allergies in Asia-Pacific: probably not just a coincidence. Asian Pac J Allergy Immunol 2012, 30, 247–248. [Google Scholar]
- Guilloux, L.; Vuitton, D.A.; Delbourg, M.; et al. Cross-reactivity between terrestial snails (Helix species) and house-dust mite (Dermatophagoides pteronyssinus). II. In vitro study. Allergy 1998, 53, 151–158. [Google Scholar]
- Prados-Castaño, M.; Cimbollek, S.; Bartolomé, B.; Castillo, M.; Quiralte, J. Snailinduced anaphylaxis in patients with underlying Artemisia vulgaris pollinosis: the role of carbohydrates. Allergol Immunopathol (Madr). 2024, 52, 60–64. [Google Scholar] [CrossRef] [PubMed]
- López-Matas, M.A.; de Larramendi, C.H.; Moya, R.; Sánchez-Guerrero, I.; Ferrer, A.; Huertas, A.J.; Flores, I.; Navarro, L.A.; García-Abujeta, J.L.; Vicario, S.; Andreu, C.; Peña, M.; Carnés, J. In vivo diagnosis with purified tropomyosin in mite and shellfish allergic patients. Ann Allergy Asthma Immunol 2016, 116, 538–543. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Kobayashi, Y.; Hiraki, Y.; et al. Paramyosin of the disc abalone Haliotis discus discos: identification as a new allergen and cross-reactivity with tropomyosin. Food Chemestry 2011, 124, 921–926. [Google Scholar] [CrossRef]
Figure 3.
Summary of respiratory symptoms following ingestion of limpets in patients without previous diagnosis of asthma. SBE: severe bronchospasm; others: urticaria, angioedema, rinoconjuncthivitis, etc.
Figure 3.
Summary of respiratory symptoms following ingestion of limpets in patients without previous diagnosis of asthma. SBE: severe bronchospasm; others: urticaria, angioedema, rinoconjuncthivitis, etc.
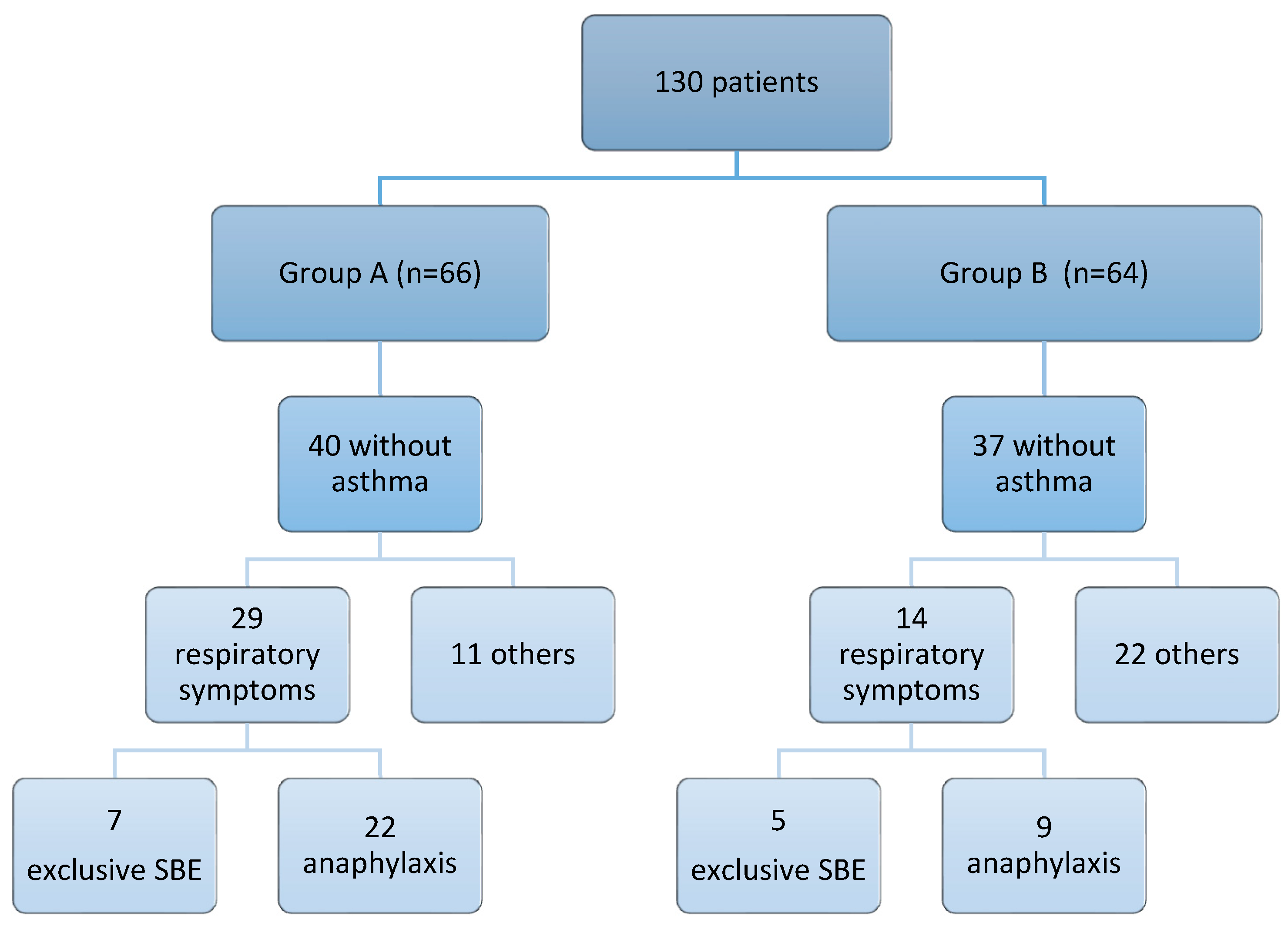
Figure 5.
SDS-PAGE (1) and IgE Western blot (2) under reducing conditions with pool of sera of all patients from group A and B to limpet extract, and with individual sera (3) of 16 random patients from group A and B to allergens of raw and cooked black limpet (Patella crenata), raw and cooked white limpet (Patella aspera) and cooked shrimp extract.
Figure 5.
SDS-PAGE (1) and IgE Western blot (2) under reducing conditions with pool of sera of all patients from group A and B to limpet extract, and with individual sera (3) of 16 random patients from group A and B to allergens of raw and cooked black limpet (Patella crenata), raw and cooked white limpet (Patella aspera) and cooked shrimp extract.
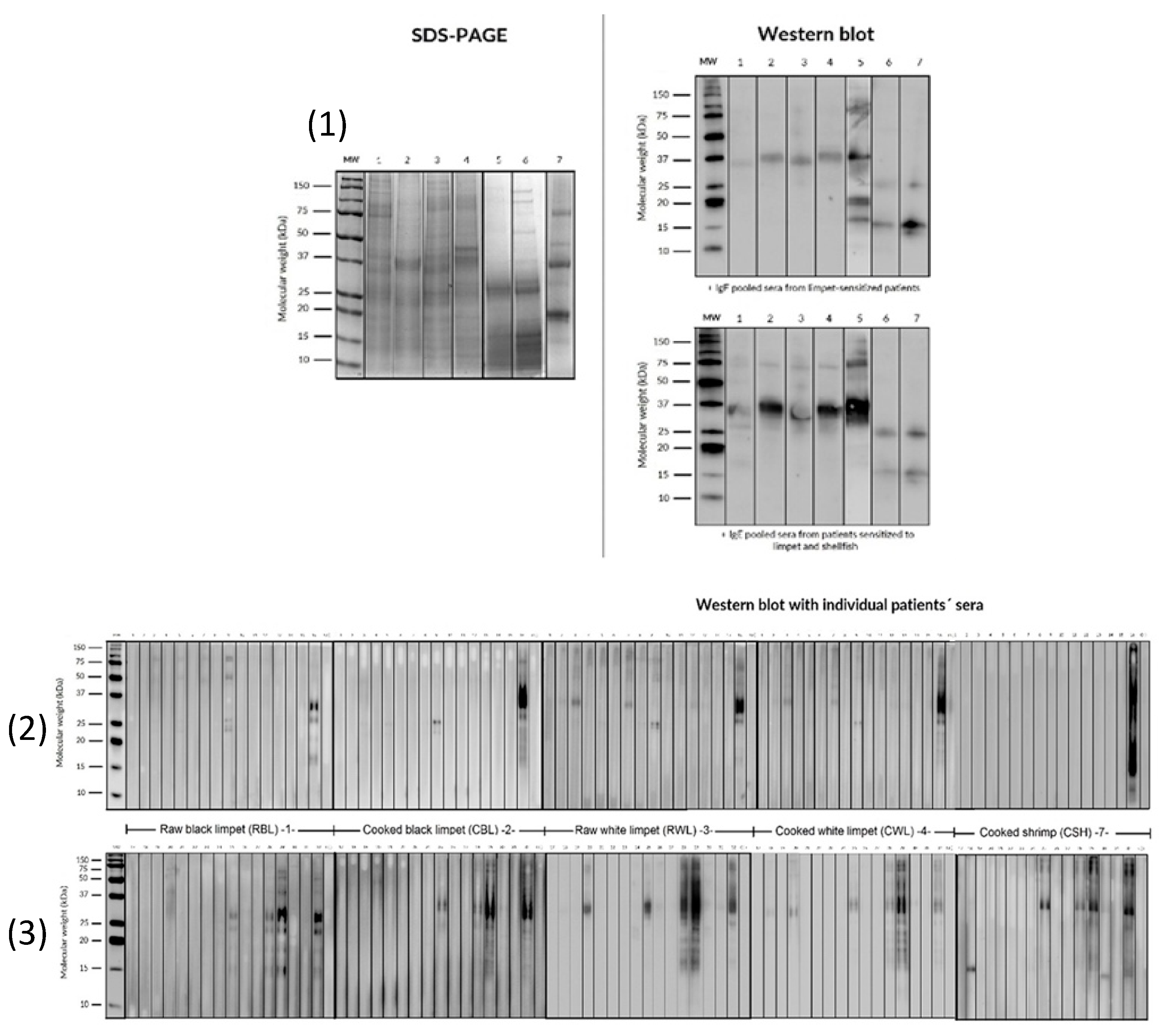
Table 1.
Clinical and demographical characteristics between 2 groups: monosensitized limpet patients (group A), and patients with limpet and other shellfish allergies (group B).
Table 1.
Clinical and demographical characteristics between 2 groups: monosensitized limpet patients (group A), and patients with limpet and other shellfish allergies (group B).
| Group A (n=66) | Group B (n=64) | |
|---|---|---|
| Gender (% Female) | 57.6 | 48.4 |
| Median age [range] | 27 y.o. [10–53] | 25.23 y.o. [4–62] |
| Personal History | ||
| RC (%) | 92.5 | 84.4 |
| Asthma (%) | 39.4 | 42.2 |
| Clinical Manifestation | ||
| Anaphylaxis (%) | 66.7 | 41.2 |
| Exclusive severe asthma (%) | 21.2 | 38.2 |
| Urticaria, angioedema (%) | 6.1 | 8.8 |
| Median of latency (minutes) | 120 [5–360] | 120 [5–360] |
| Urgent assistance (%) | 77 | 54 |
Table 2.
Results of sensitization to local aeroallergens by skin prick test (SPT) (n=130).
| Positive SPT | Group A [N(%)] | Group B [N(%)] |
|---|---|---|
|
Mites Dermatophagoides spp. |
66 (100) |
64 (100) |
| Blomia tropicalis | 48 (72.7) | 49 (76.6) |
| Storage mites | 42 (63.6) | 51 (79.7) |
| Pet epithelium (cat and dog) | 41 (62.1) | 33 (51.6) |
| Alternaria alternata | 1 (1.5) | 3 (4.7) |
| Pollen | 14 (21.2) | 8 (12.5) |
Table 3.
Immunological characteristics: Total IgE levels, skin test results, and sIgE measurements were compared between group A and group B. The prick-by-prick test (P-P) and sIgE levels were assessed with `+´indicating a positive result.
Table 3.
Immunological characteristics: Total IgE levels, skin test results, and sIgE measurements were compared between group A and group B. The prick-by-prick test (P-P) and sIgE levels were assessed with `+´indicating a positive result.
| Group A (n=66) | Group B (n=64) | |
|---|---|---|
| Medium total IgE (UI/L) [range] | 491.97 [15.8-4302] | 759.16 [51.2-4557] |
| + P-P raw limpet (%) | 61 | 66 |
| + P-P cooked limpet (%) | 61 | 71 |
| Median sIgE snail (kU/L) [range] | 0.375 [0.11-5.34] | 0,63 [0.10-87.5] |
| sIgE to snail >0,10 KU/L (%) | 51% | 91% |
Table 4.
Comparison of allergen recognition between the monosensitized limpet group (group A) and the group with allergy to limpet and other shellfish (group B).
Table 4.
Comparison of allergen recognition between the monosensitized limpet group (group A) and the group with allergy to limpet and other shellfish (group B).
| Allergen (kU/L) | Group A (n=52/66) | Group B (n=53/64) |
|---|---|---|
| Pen m 1 | 2/52 (3.8%) | 25/53 (47.17%) |
| Pen m 2 | 1/52 (1.9%) | 11/53 (20.75%) |
| Pen m 3 | 1/52 (1.9%) | 1/53 (1.87%) |
| Pen m 4 | 1/52 (1.9%) | 1/53 (1.87%) |
| Cra c 6 | 5/52 (9.6%) | 17/53 (32.08%) |
Pen m 1 (tropomyosin), Pen m 2 (Arginin-kinasa), Pen m 3 (Myosin light chain), Pen m 4 (Calcium binding protein), Cra c 6 (Troponin C).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



