Submitted:
08 October 2024
Posted:
10 October 2024
You are already at the latest version
Abstract
Background: Bone metastases (BM) have a detrimental effect on survival for patients with solid cancers. Materials and methods: This systematic review respected the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Results: When investigating OP as a risk factor for BM development, for breast cancer patients, some articles do not differentiate between intrinsic breast cancer subtypes. BMD does not seem to contribute in a significant manner when investigating Luminal A breast cancer. While researching breast cancer regardless of intrinsic subtype, untreated OP increases the risk of bone metastasis when compared to no OP group or treated OP group. In urological cancer cases, OP seems to predispose the patients to BM, especially early after diagnosis. Investigating risk factors for OP development in cancer patients resulted in the identification of 32 articles. Most articles identified risk factors for osteoporosis development in the context of breast cancer patients. Other commonly investigated solid cancers were prostate, other urological cancers, gynecological malignancies, and other less common subtypes of solid tumors. Discussion: While investigating OP as a risk factor for BM, it becomes clear that there is a high grade of heterogeneity in the behavior of each type of cancer in its dynamic concerning bone metastasis, and thus, OP might have different behaviors as a risk factor depending on the situation. Conclusion: There is a need for data regarding cancer subtypes that have not been explored concerning their interaction with the skeletal system in a low bone mineral density scenario.
Keywords:
bone metastasis
; osteoporosis
; cancer
; risk factors
; solid cancers
; low bone mineral density
1. Introduction
Bone metastases (BM) have a detrimental effect on survival for patients with solid cancers. Characteristics such as number of bone metastases, time from diagnostic to bone metastasis development [1], alkaline phosphatase levels [2], and others can be used as prognostic factors in survival estimation for patients with bone metastatic disease. The estimated time to develop bone metastasis is around 400 days [3] with a cumulative incidence of 5.6% at two years, 6.9% at five years, and 8,4% at ten years [3]. The tendency to develop bone metastasis varies widely between the cancer subtype and stage at diagnosis. Prostate cancer patients have the highest risk of developing bone disease followed by lung, renal, and breast [3]. While some cancers have a high tendency to develop bone metastasis in time, a combination of high survival with a high risk of developing bone metastasis leads to high prevalence rates, some cancers have a very high risk of bone disease at diagnosis. At diagnosis lung – 18.05%, liver-6.63%, nasopharyngeal carcinoma – 6.33%, and renal cancer -5.45% had the highest rates of presenting themselves with bone metastasis [4]. The presence of BM increased the risk of mortality and decreased survival compared to previous stages, especially for patients with prostate cancer (aHR: 18,24) [4].
While survival rates for cancer patients have been improving, due to advancements in therapeutic options, the prevalence of metastatic bone disease has been on the rise. Due to the increased prevalence of BM, the complications of this bone disease are experienced by an increasing number of patients. Reports from 2004 from NIH estimated that in the US 1.5 million people suffer a fracture due to metastatic bone disease [5]. Other skeletal complications that impede the quality of life of patients with BM are hypercalcemia, bone pain, spinal cord compression due to BM, and cachexia [6]. All these complications require complex interventions such as surgical interventions, radiotherapy, systemic treatments, pain management, nutritional management, etc. Management of skeletal-related events (SREs) also imposes a significant economic burden on medical systems. The estimated lifetime SRE-related cost per lung cancer patient with bone metastatic disease was 11,979 USD (95% CI 10,193-13,766 USD) in a retrospective analysis performed on a large US health insurance claims database published in 2005 [7]. Radiotherapy accounted for the highest proportion of the cost. High costs of SRE management are also reported in Europe, with regards to costs involved in treating a prostate cancer patient with bone metastasis, a study from The Netherlands published in 2003 [8], reported an average cost of treatment per patient of €13,051 over 24 months with an average cost of €6973 per patient to treat SREs [8]. A systematic review of relevant economic analyses regarding the management of bone metastasis concluded that bisphosphonate treatments are cost-effective options, and denosumab has a less advantageous value proposition. Evidence concerning EBR and Sr89 is limited and less definitive [9].
Osteoporosis (OP) is a pathological state of the skeletal system in which bone mineral density and bone mass decrease, many studies identify cancer patients as being at major risk for developing this bone disease [10]. Having certain kinds of cancer, such as cervical cancer [11], and cancer-specific treatments can predispose patients to osteoporosis [12]. Many modern treatments such as androgen deprivation therapy (ADT), aromatase inhibitors (AIs), selective estrogen receptor modulators (SERMs), chemotherapy regimens, high doses of corticosteroids usage over long periods, and other treatments used in cancer patient treatment can lead to early development of osteoporosis [12].
While an undeniable relationship exists between cancer patients during treatment and an increased risk of osteopenia and osteoporosis development, some argue that an inverse relationship also exists between patients with osteoporosis and an increased risk of developing bone metastases. The idea that metastatic cancer cells don’t develop in random patterns dates to 1889 with the “seed and soil” hypothesis. Recent studies refined our understanding of specific microenvironment traits that can lead to the development of cancer cell colonies from a micro-metastasis state to macro-metastasis [13]. Some studies suggest the existence of a so-called “pre-metastatic niche” characterized by the presence of abnormal immune cells and a specific configuration of the extracellular matrix proteins [13]. This niche seems to be created by a combination of soluble factors produced by the primary tumor and other non-tumor-dependent factors such as endocrine or metabolic factors.
The endocrine system plays a key role in the development of osteoporosis and, some authors argue, in developing the premetastatic niches needed to develop bone metastases in certain subtypes of cancers [14]. Bone homeostasis is maintained by a fine-tuned balance between bone formation promoted by osteoblast activity, a cellular subset derived from mesenchymal stem cells, and bone removal performed by the osteoclasts, a cellular subset derived from hematopoietic stem cells [15]. The major endocrine promoters of high bone turnover found in malignant pathologies are PTH and PTH-like substances, which also have a key role in calcium-level regulation, high glucocorticoid levels, low progesterone, androgen, and estrogen levels. The osteoblasts and osteoclasts present on their surface estrogen receptors thus making estrogen levels especially important in osteoporosis pathogenesis and bone metastasis formation [16]. Antiresorptive agents such as bisphosphonates and anti-RANKL monoclonal antibodies are widely used in patients with metastatic bone disease treatment regimens. These agents have a beneficial effect on bone density and reduce the fracture risk of these patients. While bone density increases predict a risk reduction for subsequent fractures, BMD increases and reductions do not fully explain fracture risk [17]. Bone architecture plays a major role alongside bone mass density (BMD) in the physical characteristics of the bone, for example, lumbar vertebrae murine models showed that two of the strongest correlations that predict the compressive strength of the bone are BMD and trabecular bone volume [18]. Some studies report that antiresorptive agents, such as risendronate and others, have a beneficial effect on bone architecture as well as BMD [19]. Due to the intertwined relationship between osteoporosis and bone metastasis development, we designed a systematic literature review with two main goals. Firstly, we investigated osteoporosis as a risk factor for bone metastasis development, and secondly, we investigated the risk factors for osteoporosis development in oncological patients.
2. Materials and Methods
2.1. Search Strategy and Study Selection
The systematic review respected the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [20]. The identification of relevant studies was done by searching multiple online bibliographic databases such as Google Scholar, Cochrane Library, Embase, International Clinical Trials Registry Platform (ICTRP), and Cumulative Index to Nursing and Allied Health Literature (CINAHL) database. ClinicalTrials.gov was also included in the research to identify any ongoing trials concerning osteoporosis and bone metastases. The search was performed from inception until the date of the search, August 2024. Citations of the retrieved articles were also analyzed using a forward-backward search method. The publications selected this way were chosen using the same selection criteria as the rest of the articles. The search query included combinations of the terms: “osteoporosis”, “cancer patients”, “bone metastases/metastasis”, “risk factors”, and “solid cancers”. The selection process involved screening the title and abstract of the retrieved articles and extended reading of selected articles, any conflicts of selection between the first two authors were resolved by the third author. Two selection processes were performed, one in which the focus was on identifying OP as a risk factor for bone metastases development, and, for the secondary objective of the study a second selection was performed in which all risk factors for osteoporosis development in the context of cancer patients were identified.
2.2. Data Extraction
Data was extracted from the articles by the authors and two databases were created in Microsoft Excel spreadsheet application. In the first database studies that investigated OP as a risk factor for BM were selected. An ID was attributed to each study with an appropriate identification tied to the study reference, year of publication, country of publication, study type, number of patients included, controls, groups that were compared, and statistical analysis measures were extracted from the main text and summarized in the database. In the second database, data from studies that investigated risk factors for OP development in cancer patients was selected. An ID was attributed to each study with an appropriate identification tied to the study reference, year of publication, country of publication, number of patients investigated, cancer subtype investigated, specified risk or protective factor, type of effect of the said factor, and statistical analysis measures of the effect.
2.3. Inclusion and Exclusion Criteria
Studies that were peer-reviewed with available texts in English were included. Types of studies evaluated for inclusion have consisted of randomized controlled trials, cross-sectional, cohort studies, case-control, systematic analyses, and meta-analyses. When analyzing studies exploring OP as a risk factor for BM the following inclusion criteria were used: (1) Randomised control trials, cross-sectional, cohort studies, and case-controls; (2) Studies that explored OP as a risk factor for BM; (3) Studies that included adult patients, defined as above 18 years of age. Exclusion criteria (1) Language of publication – not English; (2) Studies that included pediatric patients; (3) Articles that explored only animal models/cell lines. When exploring the risk and protective factors involved in OP development in oncological contexts, the same inclusion and exclusion criteria were applied with the mention that the included study types were extended to include systematic analyses and meta-analyses.
2.4. Quality Assessment
Quality assessment for the studies that analyzed the main objective of the study was performed using the NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies [21]. This tool includes a 14-item questionnaire in which a total score of 14 points can be obtained. Each question can be answered in one of 3 ways: Yes (1 point); No (0 points); or CD, cannot be determined (0 points)/NA, not applicable (0 points)/NR, not reported (0 points). The questions evaluate how the research was done; study population; groups recruited from the same population and uniform eligibility criteria; sample size justification; exposure assessed before outcome measurement; sufficient timeframe to see an effect; different levels of the exposure of interest; exposure measures and assessment; repeated exposure assessment; outcome measures; blinding of outcome assessors; follow up rate and, lastly statistical analyses. A quality rating of good, fair, or poor can be attributed to each evaluated study as a conclusion to the assessment.
3. Results
3.1. Search Results
The online database searches, with multiple search combinations of the keywords, as mentioned earlier led to the identification of 382 articles of interest and 4 articles identified through citation research. The databases were searched from the date of inception until June 2024. For the main objective of this review only studies that reported a statistical analysis of the risk OP represents for BM development were selected, the selection process is detailed in Figure 1. Only 3 studies respected the inclusion criteria and were included in the final analysis.
For the second objective of the study, investigating risk factors reported in studies as being risk factors for OP development in the context of cancer patients, to the 382 articles found through databases research 10 more articles were added through citation research. A total of 61 articles were assessed in full text, which led to the identification of 32 articles that met the inclusion criteria as detailed in Figure 2. For the secondary objective, the inclusion criteria have been expanded to include not only studies that reported a statistical analysis of the identified risk factor for OP development but also systematic reviews and meta-analyses that concluded concerning said risk factor. The reasoning behind this decision was supported by the intent of the secondary objective, which is the identification of said risk factors. A meta-analysis of the data reported in this systematic analysis was excluded as the lack of uniformity of data reporting and the lack of data with regards to specific subgroup analyses such as cancer types, cancer stages, pre-postmenopausal female patients, and others, led to a high heterogeneity of data which in turn made a meta-analysis of this statistical data undue at the time of analysis.
3.2. Characteristics of the Studies and Participants – OP a Risk Factor for BM Development?
Only limited data regarding this topic is available. All 3 studies identified were large retrospective studies, the first two studies [22,23], one from Taiwan and the other from South Korea, investigated breast cancer patients. In the first study, data was extracted from a nationwide database, the intrinsic subtype of breast cancer was not specified. This study concluded that even if precancer osteoporosis was not associated with a difference in BM incidence, in the context of breast cancer patients, those who had precancer osteoporosis had a shorter time for BM development. This predisposition was mitigated by treating OP as seen in Table 1. To sum up, OP does not increase the incidence of de novo BM, but it leads to accelerated BM progression when it occurs if left untreated.
In the second study [23], 348 patients with Luminal A breast cancer subtype were investigated. In this retrospective study, the patients were grouped into 2 categories, normal BMD vs low BMD (the authors included osteoporosis and osteopenia in this category). No statistically significant link between BMD and BM was found. Based on the trend of BMD after surgery, the subgroup analysis showed that upward trends, downward trends, and stable BMD did not show any significant differences either.
The last articles explored the relationship between OP and BM in the context of urologic cancers. Published in 2024 in the USA [24], it investigated a large, matched control cohort from a pool of 685066 urological cancer patients, as seen in Table 1. The article concluded that there is a strong correlation between precancer deficit of bone mineral density and BM apparition, especially in the first week after diagnosis for all investigated cancer subtypes. Bisphosphonate administration reduces the risk of BM for kidney, bladder, and prostate cancers.
To sum up the findings, for breast cancer a better investigation of OP as a risk factor for BM is required as many articles do not differentiate between intrinsic breast cancer subtypes [22]. Up to this point, BMD does not seem to contribute in a significant manner when investigating Luminal A breast cancer [23] - defined as estrogenic receptor (ER) and progesterone receptor (PR) positive, HER 2 negative, ki67 low [25]. When investigating breast cancer regardless of intrinsic subtype, untreated OP seems to increase the risk of bone metastasis after diagnosis when compared to no OP group or treated OP group. In contrast to breast cancer, which appears to be a heterogeneous group due to the different behavior that it has due to the intrinsic subtypes of cancer that it encompasses, in all urological cancer cases, OP seems to predispose the patients to BM, especially early after diagnosis.
3.3. Characteristics of the Studies and Participants – Risk Factors for OP Development in Cancer Patients
Out of the 32 articles identified, as seen in Figure 2, most articles identified risk factors for osteoporosis development in the context of breast cancer patients. 19 articles contained data regarding breast cancer patients [26,27,28,29,30,31,32,33,34,35,36,37,38,44,47,49,51,52,54,57], most common deleterious factors for bone mass density identified were treatments that led to ovarian failure and a low estrogenic bone environment. The most notable examples are chemotherapy that resulted in ovarian insufficiency/ovarian failure, an analog of luteinizing hormone-releasing hormone usage, aromatase inhibitors usage, steroidal inhibitor- exemestane, SERM usage when used in the pre-menopausal setting, oophorectomy, high dose glucocorticoids and lastly but not least breast cancer in of itself can serve as a risk factor for OP, articles findings summarized in Figure 2. Protective factors identified in this setting include weight/high BMI (body mass index), high levels of gonadal inhibin of the transforming (TGF)-B superfamily levels, SERM usage in the postmenopausal/low estrogen context, statin usage, melatonin supplementation, and mixed-mode exercises.
Prostate cancer patients are also explored in large meta-analyses [41], large propensity score-matched retrospective studies [43], and other studies, Table 2. The most frequent detrimental effects identified are the presence of bone metastasis, the presence of prostate cancer, low BMI, advanced age, high dose glucocorticoids, inactivity, bilateral orchiectomy, and most notably ADT (androgen deprivation therapy) usage, which is the backbone of prostate cancer treatment in both metastatic and neo/adjuvant treatment [58]. One of the most cited protective factors is physical activity with many regimens being studied now [47] to determine the most effective regimen for this scenario. Other urological malignancies that imply a raised risk of OP development are renal cancers. For most non-metastatic cases of renal cancer, the routine treatment involves either radical nephrectomy or nephron-sparing surgery. Compared to the more radical surgical approaches nephron-sparing surgery has a protective effect on BMD [53].
Another cluster of studied cancers is gynecological malignancies. While most authors agree that cervical and ovarian cancers have a detrimental effect on BMD [39,45,55,56] even in the pretreatment setting, the same thing cannot be concluded for endometrial cancer [39; 45]. Treating all 3 types of malignancies has a deleterious effect on BMD. Changes in BMD are lowest after surgical treatment. The highest detrimental effect on BMD is observed when multimodal treatment involving chemoradiotherapy after surgery is used [45].
Other, more scarcely researched risk factors, like melatonin supplementation [54], statins administration [49], or post-operative thyroid-stimulating hormone suppression after surgery for papillary or follicular thyroid carcinoma surgery [46] have also been included in this review, summaries available in Table 2. Melatonin supplementation seems to have a protective effect on bone density, but notable changes in BMD have been observed only in prolonged administration regimens [54]. Statins appear to have a favorable impact on BMD, with multiple articles observing an inverse correlation between LDL cholesterol levels and BMD at multiple sites such as the spine and hip while HDL cholesterol levels have conflicting correlations with BMD, mostly measured at the femoral neck level in this scenario [49]. Postoperative thyroid–stimulating hormone suppression has also been explored, but no statistically significant difference has been observed [46].
3.4. Quality Assessment
As mentioned before, Quality assessment for the studies that analyzed the study's main objective, as seen in Table 1, was performed using the NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies [21]. Scoring between 0-5 points was interpreted as being Poor, 6-10 as being Fair, and 11-14 as being Good. The first two authors evaluated the studies, and the third author mediated any conflicts. All three studies were graded as being Fair.
4. Discussion
While investigating OP as a risk factor for BM, from the studies included in Table 1, it becomes clear that there is a high grade of heterogeneity in the behavior of each type of cancer in its dynamic concerning bone metastasis, and thus, OP might have different behaviors as a risk factor depending on the situation. When investigating breast cancer, regardless of intrinsic subtype, untreated OP seems to increase the incidence of BM when compared to the normal BMD group or the treated subgroup after it has been diagnosed [22]. The same things cannot be said about the risk of BM in the OP group vs. the normal BMD group at diagnosis [22]. Also, breast cancer needs to be investigated in this regard considering the intrinsic subtype investigated, because, for example, lower BMD does not seem to impact Luminal A breast cancer patients in the same way [23]. Recent ESMO breast cancer guidelines have included adjuvant bisphosphonates as part of the standard therapy in early breast cancer, with the mention that bisphosphonate therapy is approved for treating bone metastases and osteoporosis and not for the prevention of relapse, with a level of evidence of [I, A] [59].
By contrast, urological cancers seem to exhibit a more homogenous behavior. The strongest association between OP and BM is observed 1 week after diagnosis, with adjusted odds ratios for bladder: 2.37; kidney: 2.37; and prostate: 2.84 being similar and statistically significant (all P<.001) [24]. The only outlier is testicular cancer in which the adjusted odds ratio was reported to be 4.45 with a P<.001 [24]. Still, this result only supports the trend presented by the other urological malignancies. Data regarding low bone mineral density and its effect on the risk of bone metastasis in other cancers is lacking. More studies are needed to understand and adjust treatment intensity with antiresorptive agents. Data thus far points towards a necessity in screening oncological patients for osteoporosis and osteopenia and treating it accordingly as it may also impact the oncological outcomes.
The need for implementing a coherent screening of bone mineral density in all oncological patients is also backed by the plethora of risk factors that oncological patients who receive treatment are subjected to. Multiple solid cancers present an increased risk of osteoporosis development, such as prostate cancer [41], cervical cancer [45,55,56], ovarian cancer [45], and BM presence [43]. Also, most treatments used that induce ovarian failure, testicular failure, complex multimodal treatments, and high doses of corticosteroid usage also seem to create a context favorable for BMD degradation, Table 2.
5. Conclusions
In conclusion, it has been found that oncological patients with low bone mineral density have an increased tendency to develop bone metastases. The importance of osteoporosis as a risk factor for developing bone metastases varies depending on the type of cancer that it interacts with. A good example in this regard is a heterogeneity of behavior in this regard can be observed when investigating different types of breast cancer. Also, there are a myriad of cancer-related risk factors and cancer treatment-related risk factors that predispose oncological patients to bone loss. There is a need for data regarding cancer subtypes that have not been explored concerning their interaction with the skeletal system in a low bone mineral density scenario. These results can lead to the development of a coherent strategy and an intensive osteoporosis treatment can lead to improved quality of life due to a decrease in bone metastasis incidence.
Author Contributions
A.D.A.S. contributed to the literature search, figures, data collection, data analysis, data interpretation, and writing; R.V.S. was involved in data interpretation and writing; G.D.M. was involved in data collection, data interpretation, and writing; T.T. was involved in data collection, and writing; D.S. was involved in data interpretation and writing; G.T. contributed to literature search, figures, data collection, data analysis, data interpretation, and writing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
A.D.A.S. reports personal fees from Egis and Astra Zeneca outside the submitted work. No other conflicts of interest have been declared by the other authors.
References
- Sugiura H, Yamada K, Sugiura T, Hida T, Mitsudomi T. Predictors of survival in patients with bone metastasis of lung cancer. Clinical orthopaedics and related research. 2008 Mar;466:729-36.
- Yang Y, Wang Y, Li X, Xie X. Clinical role of pretreatment albumin-to-alkaline phosphatase ratio in lung cancer: a meta-analysis. Scientific Reports. 2024 Jan 12;14(1):1166.
- Hernandez RK, Wade SW, Reich A, Pirolli M, Liede A, Lyman GH. Incidence of bone metastases in patients with solid tumors: analysis of oncology electronic medical records in the United States. BMC cancer. 2018 Dec;18:1-1.
- Zhang J, Cai D, Hong S. Prevalence and prognosis of bone metastases in common solid cancers at initial diagnosis: a population-based study. BMJ open. 2023 Oct 1;13(10):e069908.
- Office of the Surgeon General (US. Bone health and osteoporosis: a report of the surgeon general.
- Tsuzuki S, Park SH, Eber MR, Peters CM, Shiozawa Y. Skeletal complications in cancer patients with bone metastases. International Journal of Urology. 2016 Oct;23(10):825-32.
- Delea T, Langer C, McKiernan J, Liss M, Edelsberg J, Brandman J, Sung J, Raut M, Oster G. The cost of treatment of skeletal-related events in patients with bone metastases from lung cancer. Oncology. 2005 Jan 1;67(5-6):390-6.
- Groot MT, Kruger CB, Pelger RC, Uyl-de Groot CA. Costs of prostate cancer, metastatic to the bone, in the Netherlands. European urology. 2003 Mar 1;43(3):226-32.
- Andronis L, Goranitis I, Bayliss S, Duarte R. Cost-effectiveness of treatments for the management of bone metastases: a systematic literature review. Pharmacoeconomics. 2018 Mar;36:301-22.
- Drake, MT. Osteoporosis and cancer. Current osteoporosis reports. 2013 Sep;11:163-70.
- Choi HG, Lee JW, Min CY, Yoo DM, Lee SW. Analyses of the association between cervical cancer and osteoporosis/osteoporotic fracture: a cross-sectional study using KoGES HEXA data. International Journal of Clinical Oncology. 2021 Sep;26:1752-8.
- Pfeilschifter J, Diel IJ. Osteoporosis due to cancer treatment: pathogenesis and management. Journal of Clinical Oncology. 2000 Apr 7;18(7):1570-93.
- Akhtar M, Haider A, Rashid S, Al-Nabet AD. Paget’s “seed and soil” theory of cancer metastasis: an idea whose time has come. Advances in anatomic pathology. 2019 Jan 1;26(1):69-74.
- Salamanna F, Borsari V, Contartese D, Aldini NN, Fini M. Link between estrogen deficiency osteoporosis and susceptibility to bone metastases: a way towards precision medicine in cancer patients. The Breast. 2018 Oct 1;41:42-50.
- Choi IA, Umemoto A, Mizuno M, Park-Min KH. Bone metabolism–an underappreciated player. npj Metabolic Health and Disease. 2024 Jul 1;2(1):12.
- Long, F. Building strong bones: molecular regulation of the osteoblast lineage. Nature reviews Molecular cell biology. 2012 Jan;13(1):27-38.
- Wasnich RD, Miller PD. Antifracture efficacy of antiresorptive agents are related to changes in bone density. The Journal of Clinical Endocrinology & Metabolism. 2000 Jan 1;85(1):231-6.
- Borah B, Dufresne TE, Chmielewski PA, Gross GJ, Gross MC, Phipps RJ. Architecture is one of the determinants of bone strength. Journal of Bone and Mineral Research. 2003 Feb 1;18(2):38. [CrossRef]
- Dufresne TE, Chmielewski PA, Manhart MD, Johnson TD, Borah B. Risedronate preserves bone architecture in early postmenopausal women in 1 year as measured by three-dimensional microcomputed tomography. Calcified tissue international. 2003 Oct;73:423-32.
- Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. Bmj. 2015 Jan 2;349.
- National Heart, Lung, and Blood Institute. Quality assessment tool for observational cohort and cross-sectional studies.
- Chen HM, Chen FP, Yang KC, Yuan SS. Association of bone metastasis with early-stage breast cancer in women with and without precancer osteoporosis according to osteoporosis therapy status. JAMA network open. 2019 Mar 1;2(3):e190429-.
- Lee S, Kim HY, Jung YJ, Kang SK, Kim JY, Yun MS. Is bone mineral density a prognostic factor in postmenopausal women with luminal A breast cancer?. Korean Journal of Clinical Oncology. 2023 Jun;19(1):27.
- Bowling GC, Albright JA, Maloney TJ, Quinn MS, Daniels AH, Chesnut GT. Poor Bone Mineral Density Is Associated With Increased Risk of Urological Bone Metastases. Urology. 2024 May 6. [CrossRef]
- Orrantia-Borunda E, Anchondo-Nuñez P, Acuña-Aguilar LE, Gómez-Valles FO, Ramírez-Valdespino CA. Subtypes of breast cancer. Breast Cancer [Internet]. 2022 Aug 6.
- Twiss JJ, Waltman N, Ott CD, Gross GJ, Lindsey AM, Moore TE. Bone mineral density in postmenopausal breast cancer survivors. Journal of the American Academy of Nurse Practitioners. 2001 Jun;13(6):276-84.
- Nicks KM, Fowler TW, Akel NS, Perrien DS, Suva LJ, Gaddy D. Bone turnover across the menopause transition: the role of gonadal inhibins. Annals of the New York Academy of Sciences. 2010 Apr;1192(1):153-60.
- Vehmanen L, Saarto T, Elomaa I, Mäkelä P, Välimäki M, Blomqvist C. Long-term impact of chemotherapy-induced ovarian failure on bone mineral density (BMD) in premenopausal breast cancer patients. The effect of adjuvant clodronate treatment. European Journal of Cancer. 2001 Dec 1;37(18):2373-8.
- Coleman RE, Rathbone E, Brown JE. Management of cancer treatment-induced bone loss. Nature Reviews Rheumatology. 2013 Jun;9(6):365-74.
- Saarto T, Blomqvist C, Välimäki M, Mäkelä P, Sarna S, Elomaa I. Chemical castration induced by adjuvant cyclophosphamide, methotrexate, and fluorouracil chemotherapy causes rapid bone loss that is reduced by clodronate: a randomized study in premenopausal breast cancer patients. Journal of Clinical Oncology. 1997 Apr;15(4):1341-7.
- Delmas PD, Balena R, Confravreux E, Hardouin C, Hardy P, Bremond A. Bisphosphonate risedronate prevents bone loss in women with artificial menopause due to chemotherapy of breast cancer: a double-blind, placebo-controlled study. Journal of Clinical Oncology. 1997 Mar;15(3):955-62.
- Gnant M, Mlineritsch B, Luschin-Ebengreuth G, Kainberger F, Kässmann H, Piswanger-Sölkner JC, Seifert M, Ploner F, Menzel C, Dubsky P, Fitzal F. Adjuvant endocrine therapy plus zoledronic acid in premenopausal women with early-stage breast cancer: 5-year follow-up of the ABCSG-12 bone-mineral density substudy. The Lancet oncology. 2008 Sep 1;9(9):840-9.
- Fogelman I, Blake GM, Blamey R, Palmer M, Sauerbrei W, Schumacher M, Serin D, Stewart A, Wilpshaar W. Bone mineral density in premenopausal women treated for node-positive early breast cancer with 2 years of goserelin or 6 months of cyclophosphamide, methotrexate and 5-fluorouracil (CMF). Osteoporosis international. 2003 Dec; 14:1001-6.
- Sverrisdottir A, Fornander T, Jacobsson H, Von Schoultz E, Rutqvist L. Bone mineral density among premenopausal women with early breast cancer in a randomized trial of adjuvant endocrine therapy. Journal of Clinical Oncology. 2004 Sep 15;22(18):3694-9.
- Powles TJ, Hickish T, Kanis JA, Tidy A, Ashley S. Effect of tamoxifen on bone mineral density measured by dual-energy x-ray absorptiometry in healthy premenopausal and postmenopausal women. Journal of Clinical Oncology. 1996 Jan;14(1):78-84.
- Fisher B, Costantino JP, Wickerham DL, Cecchini RS, Cronin WM, Robidoux A, Bevers TB, Kavanah MT, Atkins JN, Margolese RG, Runowicz CD. Tamoxifen for the prevention of breast cancer: current status of the National Surgical Adjuvant Breast and Bowel Project P-1 study. Journal of the National Cancer Institute. 2005 Nov 16;97(22):1652-62.
- Eastell R, Adams J, Clack G, Howell A, Cuzick J, Mackey J, Beckmann MW, Coleman RE. Long-term effects of anastrozole on bone mineral density: 7-year results from the ATAC trial. Annals of Oncology. 2011 Apr 1;22(4):857-62.
- Coleman RE, Banks LM, Girgis SI, Vrdoljak E, Fox J, Cawthorn SJ, Patel A, Bliss JM, Coombes RC, Kilburn LS. Reversal of skeletal effects of endocrine treatments in the Intergroup Exemestane Study. Breast cancer research and treatment. 2010 Nov;124:153-61.
- Kim HY, Choi H. Bone density in patients with cervical cancer or endometrial cancer in comparison with healthy control, according to the stages. Maturitas. 2015 May 1;81(1):171.
- Altieri B, Di Dato C, Modica R, Bottiglieri F, Di Sarno A, Pittaway JF, Martini C, Faggiano A, Colao A. Bone metabolism and vitamin D implication in gastroenteropancreatic neuroendocrine tumors. Nutrients. 2020 Apr 8;12(4):1021.
- Lassemillante AC, Doi SA, Hooper JD, Prins JB, Wright OR. Prevalence of osteoporosis in prostate cancer survivors II: a meta-analysis of men not on androgen deprivation therapy. Endocrine. 2015 Nov; 50:344-54.
- Baldessari C, Pipitone S, Molinaro E, Cerma K, Fanelli M, Nasso C, Oltrecolli M, Pirola M, D’Agostino E, Pugliese G, Cerri S. Bone metastases and health in prostate cancer: from pathophysiology to clinical implications. Cancers. 2023 Feb 28;15(5):1518.
- Kwon T, Jeong IG, Park M, You D, Lee J, Kim HK, Hong S, Hong JH, Ahn H, Kim CS. Bone mineral density in prostate cancer: a comparative study of patients with prostate cancer and healthy controls using propensity score matching. Urology. 2014 Feb 1;83(2):385-92.
- Brown SA, Guise TA. Cancer treatment-related bone disease. Critical Reviews™ in Eukaryotic Gene Expression. 2009;19(1).
- Lee JE, Park CY, Lee E, Ji YI. Effect of gynecological cancer and its treatment on bone mineral density and the risk of osteoporosis and osteoporotic fracture. Obstetrics & Gynecology Science. 2020 Jul 8;63(4):470-9.
- Zhang P, Xi H, Yan R. Effects of thyrotropin suppression on lumbar bone mineral density in postmenopausal women with differentiated thyroid carcinoma. OncoTargets and therapy. 2018 Oct 9:6687-92.
- Singh B, Toohey K. The effect of exercise for improving bone health in cancer survivors—A systematic review and meta-analysis. Journal of science and medicine in sport. 2022 Jan 1;25(1):31-40.
- Melton LJ, Alothman KI, Khosla S, Achenbach SJ, Oberg AL, Zincke H. Fracture risk following bilateral orchiectomy. The Journal of urology. 2003 May;169(5):1747-50.
- Mandal, CC. High cholesterol deteriorates bone health: new insights into molecular mechanisms. Frontiers in endocrinology. 2015 Oct 23;6:165.
- Hatano T, Oishi Y, Furuta A, Iwamuro S, Tashiro K. Incidence of bone fracture in patients receiving luteinizing hormone-releasing hormone agonists for prostate cancer. BJU international. 2000 Sep;86(4):449-52.
- Salamanna F, Borsari V, Contartese D, Aldini NN, Fini M. Link between estrogen deficiency osteoporosis and susceptibility to bone metastases: a way towards precision medicine in cancer patients. The Breast. 2018 Oct 1;41:42-50.
- Ferreira Poloni P, Vespoli HD, Almeida-Filho BD, Bueloni-Dias F, Nahas-Neto J, Nahas EA. Low bone mineral density is associated with breast cancer in postmenopausal women: a case–control study. Climacteric. 2017 Sep 3;20(5):491-7.
- Ballon-Landa E, Panian J, Derweesh IH, McKay RR. Management of bone complications in patients with genitourinary malignancies. InUrologic Oncology: Seminars and Original Investigations 2020 Mar 1 (Vol. 38, No. 3, pp. 94-104). Elsevier.
- MacDonald IJ, Tsai HC, Chang AC, Huang CC, Yang SF, Tang CH. Melatonin inhibits osteoclastogenesis and osteolytic bone metastasis: implications for osteoporosis. International journal of molecular sciences. 2021 Aug 30;22(17):9435.
- Hung YC, Yeh LS, Chang WC, Lin CC, Kao CH. Prospective study of decreased bone mineral density in patients with cervical cancer without bone metastases: a preliminary report. Japanese journal of clinical oncology. 2002 Oct 1;32(10):422-4.
- CHO SH, CHO SH, LEE JA, MOON H, KIM DS. Reduced spinal bone mass in patients with uterine cervical cancer. Obstetrics & Gynecology. 1991 Oct 1;78(4):689-92.
- Nunes FA, Farias ML, Oliveira FP, Vieira L, Lima LF, Paranhos FD, Mendonça LM, Madeira M. Use of aromatase inhibitors in patients with breast cancer is associated with deterioration of bone microarchitecture and density. Archives of Endocrinology and Metabolism. 2021 Jul 28;65(4):505-11.
- Parker C, Castro E, Fizazi K, Heidenreich A, Ost P, Procopio G, Tombal B, Gillessen S. Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology. 2020 Sep 1;31(9):1119-34.
- Loibl S, André F, Bachelot T, Barrios CH, Bergh J, Burstein HJ, Cardoso MJ, Carey LA, Dawood S, Del Mastro L, Denkert C. Early breast cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up☆. Annals of Oncology. 2024 Feb 1;35(2):159-82.
Figure 1.
PRISMA flow diagram of the study selection process for the main objective – osteoporosis as a risk factor for bone metastasis development.
Figure 1.
PRISMA flow diagram of the study selection process for the main objective – osteoporosis as a risk factor for bone metastasis development.
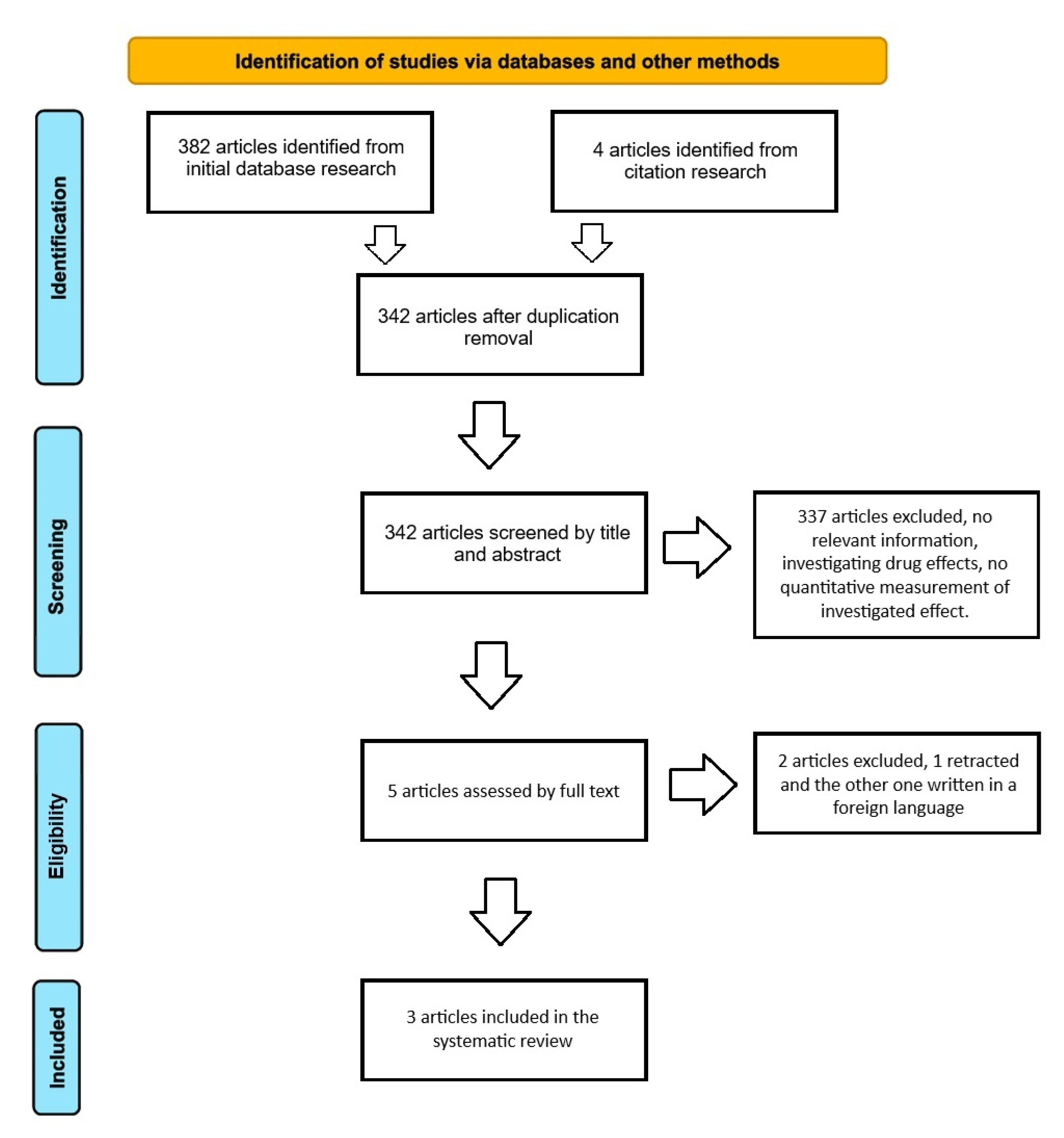
Figure 2.
PRISMA flow diagram of the study selection process for the secondary objective – risk factors for osteoporosis development in cancer patients.
Figure 2.
PRISMA flow diagram of the study selection process for the secondary objective – risk factors for osteoporosis development in cancer patients.
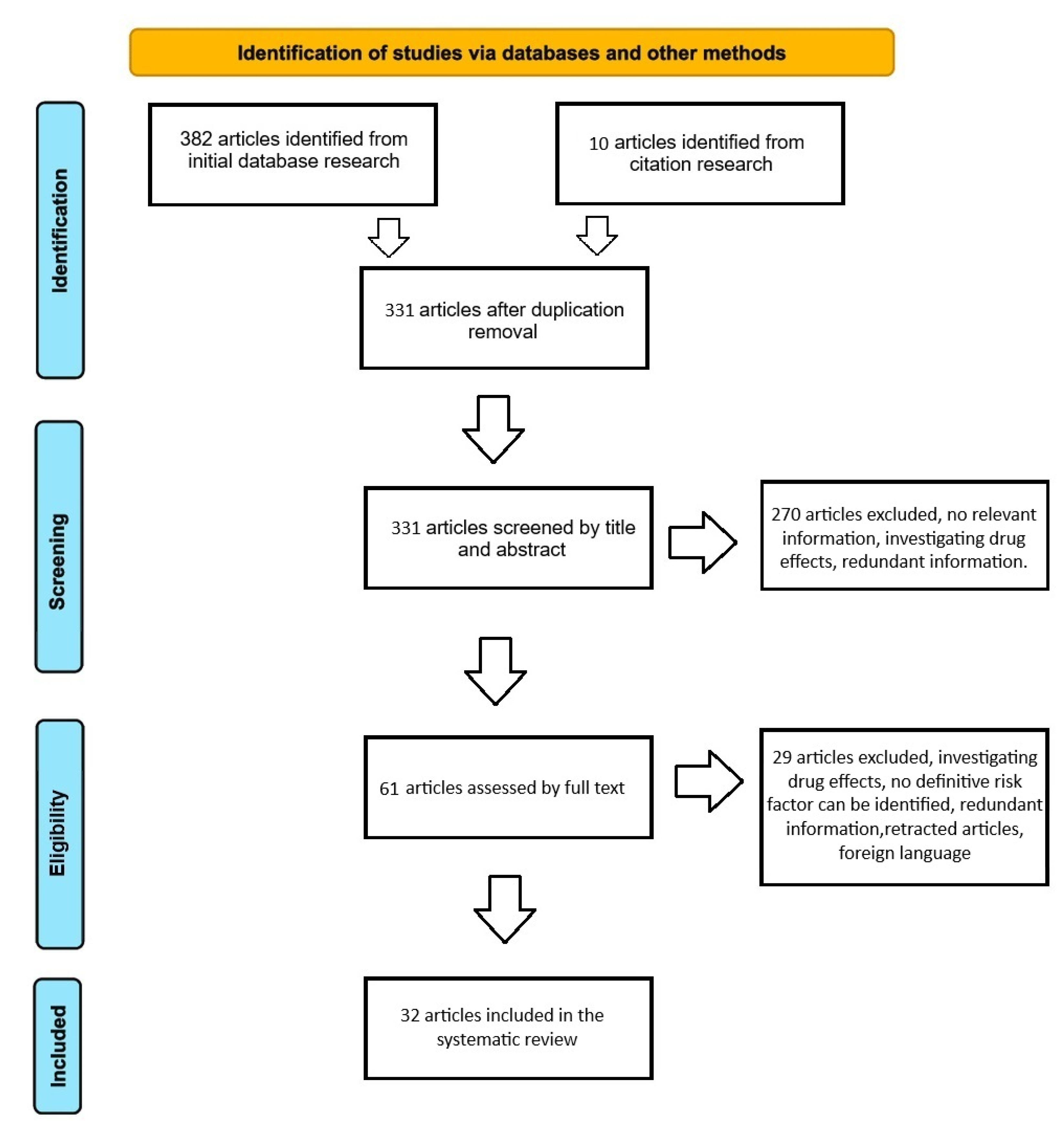

Table 1.
Studies that investigate osteoporosis as a risk factor for bone metastasis. PBMD (precancer-poor bone mineral density) - defined as osteopenia or osteoporosis.
Table 1.
Studies that investigate osteoporosis as a risk factor for bone metastasis. PBMD (precancer-poor bone mineral density) - defined as osteopenia or osteoporosis.
| ID | Year | Country | No. of Patients | No. of Controls | Study type | Cancer subtype | Comparison | Reported value |
|---|---|---|---|---|---|---|---|---|
| Hsiu-Man Chen [22] | 2019 | Taiwan | 9104 - breast cancer 14 020 - precancer osteoporosis | NA | Nationwide retrospective cohort study | Breast cancer - subtype not specified | Breast cancer group – precancer osteoporosis vs without | No additional risk of bone metastasis (aHR, 0.87; 95% CI, 0.58-1.30; P = .49) |
| Precancer osteoporosis group – osteoporosis therapy vs NUL | No association with risk of bone metastasis (bisphosphonates: aHR, 1.47; 95% CI, 1.00-2.17; P = .05; non-bisphosphonate drugs: aHR, 1.00; 95% CI, 0.72-1.39; P > .99) | |||||||
| Breast cancer group – no precancer osteoporosis vs untreated osteoporosis vs treated osteoporosis | Median time to develop bone metastasis was shorter in the untreated group vs the other two groups. (no precancer osteoporosis 2.87 years; IQR, 1.34-4.86 years) vs (untreated 1.74 years; IQR, 0.58-3.60 years; P < .001) vs (bisphosphonates: 2.34 years; IQR, 1.23-3.13 years; non-bisphosphonate drugs: 2.08 years; IQR, 0.92-4.95 years) |
|||||||
| Seungju Lee [23] | 2023 | South Korea | 348 - breast cancer | 129 – normal bone density | Retrospective study | Breast cancer – Luminal A | Breast cancer – low BMD vs normal BMD | BMD not statistically significant on five-year DFS (98.2% - low BMD group vs 95.0% - normal BMD group, P=0.33), metastases (5 y - 4 in the normal BMD group vs 2 in the low BMD group) or incidence of contralateral breast cancer |
| Breast cancer – no change in BMD over time vs improvement vs worsening BMD | DFS at 5 y was 97.0% for - no change in the BMD group, 94.6% for the BMD improvement group, and 98.4% for the BMD degradation group (P=0.79). | |||||||
| Gartrell C. Bowling [24] | 2024 | USA | 69,721 - kidney cancer, 84,755 - bladder cancer, 184,855 – prostate cancer, 3202 -testicular cancer. | Matched control cohort from a total pool of 685,066 patients with urological cancers. | PearlDiver Database - retrospective, propensity-matched cohort analysis | Kidney, bladder, prostate, and testicular cancer. | Kidney, bladder, prostate, and testicular cancer groups – PBMD vs matched control group | Strong assoiation at 1 week of cancer diagnosis (kidney: adjusted odds ratio [aOR], 2.37, P <.001; bladder: [aOR], 2.37, P <.001; prostate: [aOR], 2.84, P <.001; testicular: [aOR], 4.45, P <.001). Bisphosphonates use associated with reduced risk of kidney ([aOR], 0.46, P <.001), bladder ([aOR], 0.61, P <.001), and prostate ([aOR], 0.66, P <.001) cancer bone metastasis. |
Table 2.
Studies that investigate risk factors for bone loss, defined as osteoporosis and osteopenia, for oncological patients .
Table 2.
Studies that investigate risk factors for bone loss, defined as osteoporosis and osteopenia, for oncological patients .
| Year | Country | No. of patients | Study type | Cancer subtype | Risk factor | Type of effect | Reported value or conclusion | |
|---|---|---|---|---|---|---|---|---|
| Janice J. Twiss [26] | 2005 | USA | 30 | Longitudinal | Breast | Weight Age Months since diagnosis Months since menopause Daily calcium intake Cigarettes per day Daily caffeine intake |
Protective NUL NUL NUL NUL NUL NUL |
Weight and BMD gm/cm2 score at the spine (r=.417, p=.022), and at the hip (r=.458, p=.011). The subjects were all postmenopausal women. |
| Kristy M. Nicks [27] | 2010 | USA | - | Review | Breast | Gonadal inhibin of the transforming growth factor (TGF)-B superfamily levels | Protective | Bone loss in pre-menopausal women due to anti-cancer treatment – leads to low levels of inhibins |
| L Vehmanen [28] | 2001 | Finland | 73 | RCT | Breast | Adjuvant chemotherapy -CMF: cyclophosphamide, methotrexate, 5-fluorouracil | Deleterious | Chemotherapy-induced ovarian failure induced accelerated bone loss (p<0.001 in both spine and femoral neck; changes in BMD -0,3% in the menstruating group and -5,8% in the amenorrhea group) |
| Robert E. Coleman [29] | 2013 | UK | - | Review | Breast Prostate |
ADT Ovarian failure High dose glucocorticoids Fatigue-related immobility |
Deleterious Deleterious Deleterious Deleterious |
Early chemotherapy-induced bone loss might not be caused by the direct action of the chemotherapy agent but due to induced menopause, corticoid use, and immobility |
| T. Saarto [30] | 1997 | Finland | 148 | RCT | Breast | Adjuvant chemotherapy -CMF: cyclophosphamide, methotrexate, 5-fluorouracil Ovarian failure |
Deleterious Deleterious |
The mean difference at 2 years -4.6 CI (-6.9 to -2.3) in the amenorrhea group vs regular menses group at 2 years 0.0 CI (-3.9 to +3.9) |
| P. D. Delmas [31] | 1997 | France | 53 | RCT | Breast | Chemotherapy-induced ovarian failure | Deleterious | 2-y mean difference 2.5% +/- 1.2% (95% CI, 0.2 to 4.9) – (P=.041) lumbar spine, 2.6%+/-1.1% (95% CI,0.3 to 4.8) – (P=.029) femoral neck |
| Michael Gnant [32] | 2011 | Austria | 404 | RCT | Breast | OFS Anastrozole + OFS Tamoxifen + OFS |
Deleterious Deleterious |
GnRH analogs in pre-menopausal women – BMD after 3y reduced by 11.3% and 7.3% lumbar spine and trochanter – over the next 2y for the 75% of women who regained menses BMD at both sites recovered. Anastrozole + OFS – had higher bone loss than the tamoxifen + OFS – 13.6% vs -9% at 3y |
| I. Fogelman [33] | 2003 | UK | 1640 – sub-study involved 96 patients (53 in the goserelin group vs 43 in the CMF group) | RCT | Breast | OFS Adjuvant chemotherapy – CMF protocol |
Deleterious Deleterious |
Premenopausal subjects – GnRH analog adjuvant vs adjuvant CMF chemotherapy – at 2y, lumbar spine -10.5% OFS group vs -6.5% CMF group (p=.0005). Femoral neck OFS group -6.4% and -4.5% CMF group (p=.04). At 3 y partial recovery was observed in the OFS group (ovarian function regain). By contrast the BMD loss in the CMF group was persistent thus at 3y no difference was observed between the groups. |
| Á. Sverrisdóttir [34] | 2004 | Sweden | 89 | RCT | Breast | OFS vs OFS + Tamoxifen vs Tamoxifen alone |
Deleterious Deleterious Deleterious |
Mean change at 2y: -5%, P=.001 vs mean changes -1.4%, P=.02 vs -1.5%, P=.001. OFS group only showed partial recovery after 1y of cessation 1.5%, P=.02 Tamoxifen seems to counteract the effect of OFS on BMD. Different effects are based on baseline hormonal status. |
| T J Powles [35] | 1996 | UK | 179 | RCT | Breast | Tamoxifen | Deleterious in the premenopausal context Protective in the postmenopausal context |
BMD decreased progressively in the spine (P=.001) and hip(P<.05). Annual loss of BMD under Tamoxifen for premenopausal women was 1.44 Opposite effect on postmenopausal women with an annual increase in BMD of 1.17% in the spine (P=.005) and 1.71% in the hip (P<.001). |
| Bernard Fisher [36] | 2005 | USA | 13388 | RCT | Breast prevention | Tamoxifen | Protective in the postmenopausal context | 32% reduction in osteoporotic fractures at 7y follow up (RR=.68, 95%CI= .51 to .92). |
| R. Eastell [37] | 2011 | UK | 71 | RCT | Breast | Tamoxifen Anastrozole |
Detrimental even after treatment cessation Detrimental effect fades after treatment cessation |
Lumbar and total hip median BMD after 1 and 2 years of treatment cessation: -0.79% (P=.2), -0.30%(P=.9) respectively total Hip median BMD at 1 year and 2 years: -2.09%(P=.0003) respectively -2.52%(P=.0002) Lumbar spine increase: +2.35%(P=.04), at 1y +4.02%(P=.0004) at 2years Total hip median BMD: +0.71% (P=.3) at 1 year +0.5%(P=.8) at 2 years |
| Robert E. Coleman [38] | 2010 | UK | 4724 patients in the main study 206 patients in the bone sub-study |
RCT | Breast | Tamoxifen vs Exemestane |
The trend of persistence of the detrimental effect Detrimental effect fades |
At 2 years from the end of treatment with Exemestane spine BMD increased by +1.53% (P=.001) and decreased by -1.93% (P=.0002) after cessation of Tamoxifen. Changes at 2y in the two groups were similar with both treatment strategies. |
| HY Kim [39] | 2015 | Korea | 218 cervical cancer patients 85 endometrial cancer patients 259 healthy controls |
RCT | Cervical cancer Endometrial cancer |
Cervical cancer in postmenopausal status - pretreatment Endometrial cancer in postmenopausal status – pretreatment |
Detrimental No statistically relevant difference |
Osteoporosis was more frequent in the cervical cancer group 18.81% vs 10.81% in the control group and osteopenia was 38.99% vs 36.29% in the control group The endometrial cancer group also showed a higher incidence of osteoporosis (16.47%) while osteopenia was lower (28.24%) but no statistical difference (P=.228) |
| Barbara Altieri [40] | 2020 | Germany | - | Review | GEP-NET | GEP-NET Supplementation with vitamin D |
Detrimental Potentially protective |
Up to 76% of cases of GEP-NET patients present osteoporosis or osteopenia. Potential benefits of Vit. D supplementation in cases of insufficient or deficient Vit. D levels |
| Annie-Claude M. Lassemillante [41] | 2015 | Australia | 5812 studies initial search 15 articles for final review |
Meta-analysis |
Prostate cancer | Prostate cancer | Detrimental | Up to 37.8% of PC hormone naïve patients show osteoporosis, thus PC through bone resorption promotion might be a risk factor |
| Cinzia Baldessari [42] | 2023 | Italy | - | Review | Prostate cancer | LHRH analogs Older age Lower body mass index Bilateral orchiectomy |
Detrimental Detrimental Detrimental Detrimental |
The usual rate of bone loss in men varies between 0,5% and 1%. In patients with metastatic PC in the first year of ADT, bone loss varies between 2-8% at the lumbar spine level, and between 1,5-6.5% at the hip. At the end of ADT, BMD may increase in the lumbar spine while remaining low at other sites. |
| Taekmin Kwon [43] | 2014 | Korea | 3122: 502 PC group matched with 502 control group |
Retrospective propensity score matched | Prostate cancer | Prostate cancer Bone metastasis BMI |
Detrimental Detrimental Low - detrimental |
Higher osteoporosis incidence in the PC group (P=.0001) Independent predictor of osteoporosis (OR 3.45, P=.002) Continuous, OR 0.75, P<.001) |
| Sue A. Brown [44] | 2009 | USA | - | Review | Breast cancer | Tamoxifen Anastrozole Oophorectomy Chemotherapy OFS |
Detrimental/Protective Detrimental Detrimental Detrimental Detrimental |
Tamoxifen’s effect varies based on estrogen levels in premenopausal women More tissue level estrogen deprivation thus BMD losses |
| Jeong Eun Lee [45] | 2020 | Korea | 243 gynecological cancer patients: 105 cervical; 63 endometrial 75 ovarian 240 controls |
Retrospective | Cervical cancer Endometrial cancer Ovarian cancer |
Cervical cancer Endometrial cancer Ovarian cancer |
Detrimental No statistically relevant difference Detrimental |
Lower BMD for cervical cancer group -1st, 2nd lumbar and femoral neck – average score and SD, -0.9 +/- 1.4, P=.013; -0.8+/-1.5, P=.029; -0.9+/-1.0, P=.029 No statistical difference for the endometrial group Lower BMD from the 1st to the 4th lumbar at each level: -1.2+/- 1.4, P=.00; -1.1+/- 1.5, P=.001; -0.9+/- 1.5, P=.007; -0.7+/-1.5, P=.004; |
| Cervical cancer post-treatment 1y Endometrial cancer post-treatment 1y Ovarian cancer post-treatment 1y |
Detrimental Detrimental Detrimental |
Differences in BMD ofL3, L4 and femoral neck (P=.043; P=.022; P=.026) BMD of the endometrial group decreased significantly after the treatment Changes in BMD are lowest in patients who only underwent surgical treatment Highest bone loss in patients who underwent chemoradiotherapy after surgery |
||||||
| Pei Zhang [46] | 2018 | China | 225 postmenopausal women with DTC thyroid residual ablation or metastasis treatment | RCT | Differentiated thyroid carcinoma – papillary and follicular carcinoma | Postoperative thyroid–stimulating hormone suppression | No statistically relevant difference | Reduction of 1.9% in BMD in lumbar spine at 2y, but not statistically different |
| Benjamin Singh [47] | 2021 | Australia | 26 trials, interventions ranging from 12 weeks to 2 years | Meta-analysis | Cancer survivors – mostly breast cancer | Mixed-mode exercises: aerobic, resistance, mixed-mode and others | Protective | Whole body BMD, trochanter BMD, femoral neck BMD, and hip BMD were positively impacted, SMD range: .19-0.39, all p<.05) vs controls |
| L. Joseph Melton [48] | 2003 | USA | 429 | Retrospective | Prostate cancer | Bilateral orchiectomy Age Inactivity |
Detrimental Detrimental Detrimental |
Cumulative incidence of fractures after 15 years of 40% vs 19% expected (P=<.001) |
| Chandi C. Mandal [49] | 2015 | India | - | Review | Breast cancer, multiple myeloma | Statins | Protective | Levels of cellular cholesterol of cells occupying the bone microenvironment e.g. osteoblasts, osteoclasts, and metastasized cancer cells, might be a good predictor for bone health, thus agents that modulate the levels of intracellular cholesterol might improve bone health. |
| T. Hatano [50] | 2002 | Japan | 218 | RCT | Prostate cancer | ADT | Deleterious | The bone density in the fracture group was significantly lower than in the non-fracture group. There is a need to evaluate and treat secondary osteoporosis in patients receiving long-term ADT. |
| F. Salamanna [51] | 2018 | Italy | - | Review | Breast cancer Prostate cancer Lung cancer Others |
17 beta-estradiol levels | Low – deleterious | Low levels of 17 beta-estradiol due to menopause will lead to accelerated bone loss, and microarchitectural deterioration which in turn can lead to increased risk of fractures and uncoupling in the remodeling unit. |
| P. Ferreira Poloni [52] | 2017 | Brazil | 112 breast cancer survivors 224 controls |
Prospective case-control study | Breast cancer survivors | Breast cancer Chemotherapy history Regular physical activity High BMI (≥30) |
Deleterious Deleterious Protective Protective |
Higher incidence of osteopenia and osteoporosis in the femoral neck vs controls (39.3% vs 9%, P=.0005). Lumbar spine BMD did not differ between groups. OR 6.90, 95% CI 5.57-9.77 OR 0.24, 95% CI 0.06-0.98 OR 0.09, 95% CI 0.02-0.37 |
| Eric Ballon-Landa [53] | 2019 | USA | - | Review | Prostate cancer Renal cell carcinoma |
Long term ADT Nephron sparing surgery |
Deleterious Protective |
Average BMD decreased between 1.4 to 2.6% per year between 3 to 8 years of ADT treatment Significantly less osteoporosis between NSS 3.7 vs RN 7.0, P<.0001 |
| Ioana J. McDonald [54] | 2021 | Taiwan | - | Review | Breast, prostate, lung, bladder, and others (e.g. osteosarcoma | Melatonin supplementation | Protective | After 1y of treatment, femoral neck BMD increased by 0.5% with 1mg/ day supplementation and 2.3% with 3mg/day. 6 months of supplementation showed only a trend of bone resorption decrease Over 1y of treatment improved lumbar spine BMD by 4.3%. |
| Yao-Ching Hung [55] | 2002 | Taiwan | 50 cervical cancer patients 50 controls |
Prospective | Non-metastatic cervical cancer | Cervical cancer | Deleterious | Significantly lower BMD in the cervical cancer group P<.05 |
| Sooh Cho [56] | 1991 | Korea | 85 cervical cancer patients 148 controls |
Prospective | Cervical cancer patients | Cervical cancer | Deleterious | Age-adjusted and mean menopause duration-adjusted, cervical cancer group presented 12.8% lower spinal BMD, P=.0003 |
| Nunes FA [57] | 2021 | Brazil | 34 postmenopausal women with breast cancer 17 AI group 17 non-AI group |
Cross-sectional study | Breast cancer | AI exposure vs post-chemotherapy patients |
Deleterious | AI group had lower areal bone mineral density and T-scores at the hip. There is a higher incidence of osteoporosis on DXA scan, 47% in the AI group vs 17.6% in the non-AI group. |
Table 3.
Quality assessment of studies investigating the main objective using the NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies.
Table 3.
Quality assessment of studies investigating the main objective using the NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies.
| Hsiu-Man Chen [1] | Seungju Lee [2] | Gartrell C. Bowling [3] | |
|---|---|---|---|
| Was the research question or objective in this paper clearly stated? | 1 | 1 | 1 |
| Was the study population clearly specified and defined? | 1 | 1 | 1 |
| Was the participation rate of eligible persons at least 50%? | 0 | NA | 1 |
| Were all the subjects selected or recruited from the same or similar populations (including the same time period)? Were inclusion and exclusion criteria for being in the study prespecified and applied uniformly to all participants? | 0 | 1 | 1 |
| Was a sample size justification, power description, or variance and effect estimates provided? | 0 | 0 | 0 |
| For the analyses in this paper, were the exposure(s) of interest measured prior to the outcome(s) being measured? | 1 | 1 | 1 |
| Was the timeframe sufficient so that one could reasonably expect to see an association between exposure and outcome if it existed? | 1 | 1 | 1 |
| For exposures that can vary in amount or level, did the study examine different levels of the exposure as related to the outcome (e.g., categories of exposure, or exposure measured as a continuous variable)? | 0 | 0 | 0 |
| Were the exposure measures (independent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? | 1 | 1 | 1 |
| Was the exposure(s) assessed more than once over time? | 1 | 1 | 1 |
| Were the outcome measures (dependent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? | 1 | 0 | 1 |
| Were the outcome assessors blinded to the exposure status of participants? | 0 | 0 | 0 |
| Was loss to follow-up after baseline 20% or less? | 0 | NA | NA |
| Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)? | 1 | 0 | 1 |
| Score | 8 | 7 | 10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



