
Submitted:
11 June 2025
Posted:
13 June 2025
You are already at the latest version
Abstract
Mysticism has been an integral part of human society for ages. It involves both spirituality and religiosity. The former is associated with attaining higher states of consciousness without an essential belief in a supernatural power (or God), while the latter does. While there is plenty of speculative literature available on these topics, we instead focus on peer-reviewed scientific literature that is evidence-based. First, we briefly review technologies that can measure brain function. We make the case that concepts such as emotions and subjective experiences, which have long been considered outside the scope of objective scientific inquiry, are in fact amenable to objective scientific inquiry with technologies available today. To substantiate this point, we showcase scientific studies on spiritual aspects of mysticism such as meditation, mantra/chanting, and breath modulation. While we recognize that much of the research on these topics deal with their health benefits, we argue that associated brain changes are also conducive for attaining higher states of consciousness related to spirituality. Next, we present limited scientific literature on religiosity, dealing with its neural correlates, evolutionary biological origin, and usefulness for mental health. We close by arguing that the brain basis of mysticism cannot be seen in isolation from the body since these entities are intimately connected. We propose that future research should look at brain-body interactions and associated markers of mysticism using latest technologies.
Keywords:
meditation
; Yoga
; spiritual
; religiosity
; mantra and chanting
; functional MRI
; medical imaging
1. Introduction
Mysticism can be defined as the practice of certain spiritual or religious prescriptions that leads to sensory or extrasensory experiences. Mysticism has been associated with both religiosity and spirituality for thousands of years. Mysticism associated with religiosity involves experiences during altered states of consciousness whilst acknowledging the presence of the Absolute God as a fundamental belief. Two popular theories still afloat are the ‘push’ and ‘pull’ theories [1]. According to the ‘push’ theory, there is a single ‘God spot’ which when activated prompts individuals to mystical experiences (and in some cases, associated with higher states of consciousness). Based on this conjecture, injury to this particular region decreases the chances of mysticism. On the contrary, the ‘pull’ theory suggests that to have mystical experiences, the inhibitory functions need to be suppressed, which would lead to increased mysticism in case of injury in those regions. In contrast, mysticism associated with spirituality focuses on techniques such as meditation to attain higher states of consciousness without the necessity to believe in anything, including an absolute God.
A large amount of information is available on the internet and is popularized on social media (Facebook, Twitter, WhatsApp, etc.) on the topic of ‘brain and mysticism’. However, much of that information is speculative in nature, with a substantial proportion of outright misinformation. They are not grounded on either historical or empirical evidence. The relatively small portion of the literature based on well-defined experimental evidence, with about 1500 peer-reviewed journal articles, has sufficient methodological details and testable results to be termed as ‘hard science’. Such research investigations conform to the scientific method of hypothesis-experiment-observation-inference, and their reported results are testable/verifiable by a third person. This scientific literature forms the basis for the topic of this article. The results reported in peer-reviewed journals are generally reproducible and replicable, leading the world to trust the conclusions. As such, investigating mysticism is considered today as a valid scientific enterprise. The focus here is to highlight these findings in particular. We will mostly avoid speculative literature and explicitly mention speculation when relevant.
Meditation, a spiritual practice endorsed for millennia, has long been hypothesized to affect our brains. To ascertain the depth and scope of this topic Lauricella et al. [2] showed a graph (Figure 1, top) that portrays increasing research interest in this topic during 1979–2014. An exponentially growing number of scientific articles on this topic can be observed post 2000. The geographical distribution of the articles (Figure 1, bottom) indicates a heavy concentration in North America, Australia, New Zealand, Asia, the UK, Ireland, and France. Although the interest in the scientific community can be recognized, the fact that there is much skepticism as well cannot be denied. The skepticism is a product of multiple factors. First, the amount of speculation and misinformation on this topic (as discussed before) raises the level of skepticism. Next, the study of states of mind and psychology, in general, were considered to be subjective science not amenable to objective inquiry. This is no longer the case. Recent technological advancements allow us to measure neural correlates of mental states objectively. In fact, government funding for brain research, in general, increased in the United States, first during the “decade of the brain” in the 1990s during the Bush administration and then during the “brain initiative” starting with the Obama administration in 2013. Similar projects in Europe (Human Brain Project) and Asia have provided an impetus for objective measurements of neural processes in the brain during subjective experiences. Also, interest in the beneficial effects of Yogic practices such as meditation on mental health is increasingly being studied [3], which has increased funding in this area. Consequently, the scientific enterprise is receptive today to investigating the brain basis of mysticism. In fact, neuroscientists welcomed the Dalai Lama to the Society for Neuroscience annual meeting in Washington D.C. to recognize that this is now a valid scientific enterprise [4].
The purpose of this article is to present studies that scientifically investigate the brain basis of mysticism. To start with, it is essential to have an idea about the brain, the mind, and the dichotomy between them, and how the latest technologies can be utilized to investigate them. This is dealt with in the next section. Section-3 describes how brain function can be measured objectively using these technologies. Section 4, Section 5 and Section 6 discuss the scientific literature on spirituality associated with meditation, mantra/chanting, and breath modulation, respectively. Section-7 presents scientific studies on religiosity, and section-8 describes the importance of brain-body relationships in understanding the physiological basis of mysticism. Section-9 provides concluding remarks.
2. Brain and Mind
The brain is a complex organ responsible for controlling thoughts, emotions, actions, sensations (such as vision and hearing), coordination, and all other functions for body regulation. The 3-pound weighing organ (2% of body weight) is comprised of 100 billion neurons, the basic building block to receive and transmit information, that is connected with each other via one quadrillion (a million billion) connections. The proper functioning of the brain requires 20-25% of the body’s energy budget [5,6]. A deficiency in glucose supply to the brain disrupts brain metabolism leading to impaired function and growth [7]. Thus, with a drop in glucose level, termed hypoglycemia, individuals suffer from blurred vision, drowsiness, inability to concentrate, experience confused thinking, and slurred speech [8]. A prolonged period of low glucose levels can affect the brain severely, leading to seizures, coma, or even death in a few cases. The brain has traditionally been considered a physical entity enclosed in the skull and one that sustains based on physical metabolites such as oxygen and glucose. On the contrary, historically, the mind has been hypothesized to underlie thoughts, feelings, and emotions, which were considered by some as non-physical entities. The field of "consciousness studies", dealing with origin or basis of conscious thought, is a vast subject and beyond the scope of the current article. The relationship between the brain and the mind has been a topic of philosophical debate about whether they are the same or different or interdependent (known as the mind-body problem or mind-body dualism [9]). However, in the neuroscience field, the mind is referred to as the outcome of conscious and unconscious self when awake and unconscious when asleep [10].
Here we argue that the philosophical discussion about the mind-body problem and whether the mind is a physical entity or not are unimportant for a scientific study of the brain basis of mysticism. This is because we can measure brain function with today’s technologies, and irrespective of whether the brain is the mind or the brain is modulated by the mind, we are able to directly or indirectly infer the correlates of the mind. What matters is that today it is possible to measure and modulate attributes of the mind such as emotions and intentions, which were hitherto considered subjective and experiential. For example, research shows that electrical stimulation of the brain can determine whether one feels happy or sad [11]. Deep brain stimulation is a technology that can cure individuals suffering from treatment-resistant depression (i.e., those who cannot be cured with any other medication or therapy). It is a device with electrodes implanted in the brain like a pacemaker [11]. The device is placed under the collar bone and the electrodes are placed in Brodmann Area 25 (the sadness center), the junction box of brain circuits that regulates our moods. Each electrode has four contact points that could be regulated (switched ON or OFF) from outside to initiate the stimulation. After turning on and stimulating certain electrodes, one of the participants in the study reportedly smiled after decades. Although the treatment procedure and its results are fascinating, it is crucial to understand that every individual is different and requires personalized brain stimulation [12]. A wide range of similar procedures have been carried out to bring respite to many lives [13,14,15]. The underlying science to determine the stimulation target was itself developed through extensive neuroimaging research. Furthermore, today deep brain stimulation is FDA-approved to treat not only depression and insomnia [16] but also other neurological disorders such as obsessive-compulsive disorder (OCD) [17], Parkinson's [18,19], epilepsy [20], essential tremor [21], dystonia [22,23], and many more. The takeaway is that emotions such as happiness or sadness can be physically measured and manipulated. It is also possible to measure and manipulate perception (five senses), cognition (decision making, attention, etc.) and other emotions, indicating that the ability to measure/change brain faculties is quite ubiquitous and not limited to the example of depression/happiness presented above. Thus, current technologies provide an unprecedented opportunity to investigate the brain basis of phenomena historically considered outside the purview of objective investigation. We believe the same logic can be extended to the study of the brain basis of mysticism, which is commonly associated with altered states of mind or, more specifically, altered states of consciousness. Before the 1980s, the mind was considered a nonphysical entity and the brain as a physical entity; thereby, there was a debate about the brain basis for the mind. Whether the mind has physical existence is a philosophical topic of discussion, which we will not elaborate on. However, as argued before, it is certain that the mind has a physical basis in the brain, which can be physically manipulated. Thereby it is possible to investigate the basis of hitherto abstract notions such as mysticism within a sound scientific framework.
3. Measurement of Brain Function
A range of techniques are available to measure brain function, as shown in Figure 2. The objective is to capture as much spatial detail as possible (spatial resolution), as quickly as possible (temporal resolution). The modalities low on both the spatial and temporal scale, i.e., those with high spatial and temporal resolutions, are all invasive technologies such as multi-unit activity (MUA)/local field potential (LFP), and single-unit activity (SUA), which are mostly feasible only in animals (requires opening the skull for direct brain contact). For humans, it is difficult to always rely on invasive techniques for all investigations except in rare situations where a human subject undergoing brain surgery provides consent for research experiments [24]. Thereby, non-invasive technologies such as electroencephalogram (EEG) and MEG (magnetoencephalography) are popular, with EEG existing for almost a century and MEG for half of that time. Even though their temporal resolution is satisfactory, their spatial resolution is coarse, and it is difficult to pinpoint precisely where the signal is generated due to poor spatial specificity. Thereby, a higher spatio-temporal resolution modality with impressive sensitivity and specificity is more desirable. Observing the graph in Figure 2, functional magnetic resonance imaging (fMRI) fits this requirement and has a unique place in the spatio-temporal space amongst the range of imaging modalities. Its spatial resolution (0.5–2 cubic mm) is impressive and its temporal resolution (0.5–2 s) is acceptable. In addition, fMRI also simultaneously optimizes spatial coverage (image the entire brain area as much as possible) and signal-to-noise ratio (data quality), apart from being sensitive to small changes in brain function. FMRI images are relatively easy to acquire and are not associated with risks of ionizing radiation. The discovery of fMRI in the early 1990s has seen an explosion in research due to its suitability and reliability.
In order to scan and take pictures of the brain, the human body is placed inside an MRI scanner with a strong magnetic field. The machine captures pictures of the brain across multiple time instances (akin to a video of brain function). MRI as an imaging technology has made an immense contribution to the scientific world and has two Nobel prizes as well, one in physics for nuclear magnetic resonance (NMR) to Felix Bloch and Edward Purcell (1946: atomic nuclei absorb and re-emit radio frequency energy) [26,27] and the other in medicine for MRI to Paul Lauterbur and Sir Peter Mansfield (1970s: spatial frequency encoding of NMR to produce images) [28]. FMRI was invented by Seiji Ogawa, Kenneth Kwong, and their colleagues in the year 1992 to show how MRI can be used to measure brain function non-invasively [29,30,31].
MRI is of two types - structural and functional. The most common one used clinically is structural MRI, which provides 3D anatomical information (picture) of the brain. The time component is absent in these kinds of images. The other type is fMRI. As the name suggests, it gives an idea of how the function of the brain evolves over time. FMRI is widely used to understand which brain regions are responsible for various tasks. For example, when an individual taps their finger, the primary motor cortex gets activated, suggesting its involvement in that particular task [32]. Activation in fMRI is the brain region that consumes the most oxygen and glucose (energy driving factor), time-locked to an external sensory stimulus or a motor/cognitive task being performed by the subject. The inference that tapping finger task activates the primary motor cortex is typically known as forward inference. To give an idea of the neurological map, Figure 3 shows the cortical homunculus, representing the brain location dedicated to specific sensory and motor functions of different body parts.
Conversely, identifying the task being performed by the subject based on the regions of brain activation from fMRI is termed reverse inference. For example, one study done at MIT looked at fMRI signals in the visual cortex to decode the letter that the participant was viewing (which was the letter ‘M’) [35]. Another study predicted movie scenes being viewed (from the movie “The Good, The Bad, and The Ugly”) based on the fMRI data [36]. Thereby, it is evident that by training a machine learning model or an artificial neural network, emotion, task, and/or behavior of participants can be predicted. In other words, ‘mind reading’ is within the realm of possibility. An important application of this field of research can be seen in brain-machine interfaces and lie detection (instead of age-old polygraph tests that could be inaccurate). In brain-machine interface, paralyzed individuals or those with artificial limbs can move their limbs just by thinking to do so [37]. Likewise, fMRI in lie detection can identify if the person is testifying false evidence. The idea is not only perceivable in today’s world but is even admissible as evidence in court [38]. Furthermore, a similar technique was used in a murder case in Mumbai, India, in 2007, where the results showed that the accused had to be the killer [38]. It was accepted in court as well.
The takeaway message is that it is possible to detect, measure, and objectively characterize one’s feelings, perceptions, and thoughts with physical measurements. Thereby, as an extension, the brain basis of mysticism is a valid scientific pursuit. In the following sections, we elaborate on the neural basis of both the spiritual and religious aspects of mysticism. First, we consider the spiritual aspects with scientific studies on meditation, mantra and chanting, as well as breathing modulation, followed by a scientific take on religiosity and a holistic view of the brain and body.
4. Meditation
4.1. Meditation and the Brain
Meditation has long been a southern and eastern Asian tradition, primarily rooted in India. In recent years, western society has equally accepted and adopted this tradition since the scientific world has begun to investigate the neural basis and effects of meditation on the human brain, ultimately improving human lives. Specifically, the effects of meditation on both brain structure and function have been probed. The causality between the two (effects on structure and function) assists in identifying the associated mechanistic underpinnings [39]. Research highlights the alterations in gray and white matter due to meditation, along with changes in brain functional networks (responsible for cognition, emotion, and executive functions) [40]. Brain networks are an ensemble of different brain regions that communicate among themselves to accomplish essential functions. It is an embodiment of distributed information processing, similar to the internet or wireless communication networks, which is a network of computational units whose capabilities are derived by the communication among them. With techniques such as fMRI at our disposal, it is feasible to observe brain networks during meditation (meditation state, i.e., ‘altered sensory, cognitive, and self-referential awareness’) and after meditation (meditation trait or the lasting changes) [41]. The prevalence of a varied range of meditation practices and research findings on the same indicate distinct functional outcomes where both activation (engaging) and de-activation (disengaging) are equally important for meditative benefits [42]. Fox et al. presented the results of a meta-analysis on the activations and de-activations in the brain for focused attention, open monitoring, mantra recitation, and loving-kindness/compassion meditation (Figure 4). The diversity in meditative practices and their outcomes is fascinating. In attention meditation, the focus is on an external object or a quality of one’s self, whereas a few other practices (loving-kindness, and compassion meditation) are about meta-awareness [43,44,45,46]. However, the desired outcome across methods is attaining a deep sense of relaxation on the one hand, and integral attentiveness on the other. In the following paragraphs, we highlight some key findings and research on the effects of meditation on the human brain.
Studies investigating structural changes brought about by meditation have looked at the brain's cortical thickness. The outer layer of the brain or cortex, constituting the gray matter, consists of billions of neuronal cell bodies. The inner layer comprises the white matter or the connections between neurons consisting of axons. Increased gray matter thickness is generally associated with higher cognitive ability or intelligence and better brain health [47,48,49]. A few studies have found a positive correlation between grey matter thickness and intelligence in particular brain regions [50]. With age, cortical thickness gradually declines [51,52], which is an entirely natural phenomenon. A study done at Harvard Medical School by Lazar et al. found that people who practiced long-term mindfulness meditation exhibited reverse cognitive aging [53] (Vipassana meditation is usually termed as mindfulness in academic literature). Characteristically these individuals did not show a decline of cortical thickness with age (Figure 5); that is, their brains remained young even in old age.
Another collaborative study between Dalian University, China, and the National Institutes of Health (NIH), USA, showed increased neuronal fiber density for short-term meditation practice [54]. Individuals underwent integrative body–mind training, a mixture of Zen and other similar Buddhist methods based on mindfulness, wherein they performed meditation for 30 minutes each day for a stretch of one month (a total of 11 hours). The duration is short and thereby can be termed as short-term meditation practice. Neuronal fiber density was assessed before and after meditation training (i.e., in a gap of one month). White matter density increased in the anterior cingulate cortex leading to efficient transfer of information during cognitive processes. This study was important because the prior belief was that only long-term meditation has a measurable impact (as in [53]), and such notions were turned around with this study. A similar study that extended the idea and investigated the implications of short-term mindfulness meditation found increased gray matter volume in the ventral posterior cingulate cortex, which is known to underlie age-related cognition, emotion, and self-awareness [55].
We next focus on changes in brain function due to meditation. Functional changes are the ones in which we observe changes due to meditation in activation of brain regions or connectivity between different regions of brain networks. Here, we find two categories of studies in the literature. First is case studies, where the number of individuals is less (usually N<3 and in most cases N=1). The other category is population studies that identify changes in a large set of people representative of the population. Generally speaking, the results of case studies are not necessarily generalizable to the larger population. However, in neuroscience and medicine, since the adverse conditions expressed in the population are very low, case studies are well recognized not as conclusive results but to form hypotheses and as a basis for further investigation. In this spirit, we present a few case studies as well.
An un-named 65 year old male Indian Yoga master claimed that he does not feel pain while meditating. To understand and verify his claim, Kakigi et al. carried out an experiment at the National Institute for Physiological Sciences, Japan, where the Yoga master was subjected to pain while inside the MRI scanner during both meditating and non-meditating conditions [56]. Surprisingly enough, the brain regions that got activated when the individual was subjected to pain whilst not meditating did not get activated while meditating (these regions were the thalamus, SII, insula, and cingulate cortex, which are known to be part of the brain’s pain circuit). This confirms the claim by the Yoga master that he does not experience pain while meditating. It is well known that the perception of pain can be blocked by silencing regions along the pain pathway either in peripheral or central nervous systems (which painkiller medications do effectively). In fact, mindfulness meditation has been shown to provide pain relief [57]. Interestingly, a similar effect can be obtained by voluntary control over the activation of certain brain regions using meditative techniques [58,59]. This is not outside the realm of possibility since neurofeedback also seems to allow subjects to gain voluntary control over pain regions such as the anterior cingulate, thereby reducing pain in patients experiencing chronic pain [60]. Overall, changes in brain structure and function have been established in both short-term and long-term meditators, and exciting claims such as pain tolerance in meditators have been verified. The improvement in brain structure/function due to meditation align with brain patterns of improved mental health, and thus meditation is also being explored as a therapy to ameliorate psychiatric conditions such as depression and anxiety.
4.2. Meditation as a Tool to Achieve Mystical Experiences
Above, we presented the broader landscape of meditation as a tool that changes the brain and has health benefits. Here, we review literature that shows the utilization of this effective tool to enable mystical experiences. In a case study performed at Boston University, researchers tested the claim of an individual experiencing ecstatic ‘Kundalini’ meditative experiences [61]. The study found activation in the anterior prefrontal cortex, a part of the brain uniquely evolved in humans. Parts of this unique brain area are not even present in the last common ancestor of humans, the chimpanzees. The function of the anterior prefrontal cortex is enigmatic, however, and it is believed to promote higher cognitive functions [62,63]. These results corroborate with shifts in breathing and EEG patterns obtained during Kundalini meditation in a Yoga master, which was reported in 2001 [64].
Another form of active meditative correspondence is believed to be telepathy or mind reading sans physical or sensory interaction. A group of researchers at NIMHANS (National Institute of Mental Health and Neurosciences), Bangalore, India, investigated the neural basis of telepathy [65]. By establishing a telepathic link (Figure 6), a mentalist could draw a very close representation of what another person drew, devoid of any prior knowledge of that representation. The experiment was validated with a control subject (non-mentalist), to exclude trivial explanations, who failed to draw something nearly close to the actual image. FMRI data were acquired from both the mentalist and non-mentalist during the experiment. There was activation in the right parahippocampal gyrus (responsible for spatial memory and navigation) for the mentalist and in the left inferior frontal gyrus (responsible for language comprehension and production) in the case of the non-mentalist. This case study shows that it is possible to investigate the neural basis of phenomena that have been traditionally considered to be “extra-sensory perception”.
A few other studies of physiological measurements obtained from individuals in higher states of consciousness are noteworthy. These include investigations on Sri Ramanand Yogi during his stay in an air-tight box [66], voluntary control over visceral functions during meditation by Yogis [67,68], and observance of alpha EEG activity during meditation (showing a relaxed state of mind) in four Yogis even when their hand was immersed in ice cold water for 45–50 minutes during meditation [69]. These case studies demonstrate that meditation can be used as a tool to achieve mystical experiences and that such experiences leave physiological imprints on the brain and body, which can be measured to infer the characteristics of such experiences.
Due to the low sample size of case studies discussed above, the probability of the outcome being obtained by chance is higher. Therefore, in order to advance generalizable scientific knowledge, we need population studies wherein the sample size is large and the data acquired is representative of the population, or we need deep phenotyping of a single individual wherein the person is scanned (experimented upon) multiple times (>10) and statistical inferences are drawn. While we recognize that case studies are essential for studying phenomena that are unique to individuals (such as a Yogi attaining the highest state of consciousness) and can sometimes be well-powered if the effect sizes are large, population studies or deep phenotyping are important for making broader inferences. Although there have been no deep phenotyping studies on meditation, many population studies have investigated mind wandering and meditation. A scientist from Denmark analyzed Patanjali’s definition of meditation and put it into a neuroscientific framework [70] by linking meditation with the control of mind wandering. This allows the design of experimental paradigms around known concepts such as mind wandering. According to Patanjali, the Indian author of one of the most authoritative texts on meditation called ‘Yoga Sutra’, to attain the optimum stable state through meditation, one must overcome mind wandering (which he refers to as mental noises or waves of thoughts) [71]. Many researchers have followed this framework. One such study using EEG observed the effects of meditation on mind wandering and sleepiness for both expert and non-expert meditators [72]. For expert meditators, meditation depth increased with time, and mind wandering decreased with time more than for non-expert meditators. Figure 7 illustrates their results. It is noteworthy that the reduction of mind wandering is an outcome of any active task. But in meditation, the active task is itself to modulate attention in a way that is oriented towards the self, and this distinguishes it from other active tasks that may be oriented towards the outside world.
Another fascinating study is where subjects with brain injuries in certain brain regions suddenly had spontaneous spiritual experiences and altered states of consciousness, also known as Geschwind syndrome [73]. Brain injuries in the temporal lobe, the same region activated during telepathy, are hypothesized to lead to hyper synchronization or information influx between various regions, resulting in a heightened state of consciousness. The reason behind this is yet to be uncovered.
Next, we glance at studies that investigated the effects of specific prevailing meditative techniques such as ‘Samyama’, ‘Sahaja Yoga’, ‘Raja Yoga’, etc. ‘Samyama’ is a collective meditation practice commencing with attention followed by Dhāraṇā (concentration), Dhyāna (meditation or unbroken concentration), and Samaadhi (an exalted state of consciousness), the three limbs of the eight limbs of the astanga yoga. Researchers observed increased fMRI resting-state connectivity between the salience network and the default mode network (DMN) after execution of ‘Samyama’ (an intense technique that requires one to be silent for a period of 8 days) in the case of meditators [74]. A correlation was observed between the data (increment in the intra-network connection) and the self-reported mindfulness score. The result is in agreement with increased connectivity and mindfulness reported in earlier research [75]. On the contrary, during focused breathing, the intra-network connections exhibited a decrease in connectivity that signifies the controlling ability of ‘Samyama’ meditators for regulating mind wandering (DMN is the responsible network) with increased focus and attention. Likewise, a systematic review and meta-analysis on focused attention meditation identified the default mode, salience, and executive control networks [76] as important brain networks modulated by meditation.
Another similar meditation practice that has been scientifically investigated is the ‘Sahaja’ Yoga technique. This technique trains one’s mind to eliminate or reduce thoughts significantly and attain a state of mental silence. Barrós-Loscertales et al. studied the functional connectivity changes among brain regions that showed an increase in gray matter volume from a previous study with the same population (‘Sahaja’ Yoga meditator and non-meditator) [77,78]. Connectivity changes were observed in these regions responsible for cognitive control, attention, and executive function [77].
The Brahma Kumaris (Prajapita Brahma Kumaris World Spiritual University), a spiritual movement initiated in the 1930s in Hyderabad (India), follow a meditation technique termed ‘Rajyoga’ wherein individuals perceive themselves through the area between the eyebrows while focusing on a meaningful external symbol (representation of a supreme God) keeping their eyes-open (an exception to other forms of meditation where eyes remain closed as in samyama/astanga yoga or where eyes are half closed as in Zen technique) and reiterating positives around peace, love, bliss, etc. [79,80]. Ramesh Babu et al., for the first time, attempted to identify neural plasticity due to ‘Rajyoga’ meditation on the reward processing centers of the brain (right superior frontal gyrus, left inferior orbitofrontal cortex and bilateral precuneus) [81]. They observed an increase in gray matter volume in the reward processing center related to happiness and a positive correlation with individual happiness scores (Oxford happiness questionnaire) with longer meditative hours.
Transcendental meditation is a meditation technique that involves silent chanting (of mantras) until the attainment of relaxation and peace. Like other meditation techniques, long-term transcendental meditators exhibit higher activation in the anterior cingulate and dorsolateral prefrontal cortices responsible for attention and executive function (like thinking, planning, monitoring, etc.) [82]. In contrast to prior research [83,84], the study also revealed lower activation in the pons and cerebellum that are responsible for arousal [82]. Owing to these findings and the fact that transcendental meditation requires the least effort (of course, for expert meditators, that comes with practice), it could be inferred that training in this type of technique can lead to peace and bliss effortlessly (the concept of transcending to that feeling).
As described earlier, not only long-term but short-term meditation practice also affects the white and gray matter of our brain (structural changes) [54,55]. Here, we present the effects of intensive short-term meditation practices. Kwak et al. carried out a study as part of the Templestay project, wherein the participants underwent three days and four nights of intensive meditation practice. They were scanned twice (fMRI scans 2-3 days before and after the course) [85]. The format was quite similar to the Templestay in Buddhist culture, where individuals experience staying in a temple and practicing mindfulness, eating healthy food, walking, exercising, etc. Participants showed enhanced executive function (e.g., attention) and neural activity in areas responsible for alertness and attention as compared to the control group (who stayed in the temple in a vacation style). Furthermore, a functional near-infrared spectroscopy (fNIRS) study found that loving-kindness meditation, also known as compassion meditation, results in cognitive benefits in novice meditators after a short meditation session [86].
In summary, modern technologies have been utilized to study several meditation-based spiritual practices. We now have a better understanding of the brain mechanisms that underlie these practices. Lifestyle benefits and mystical experiences associated with these practices have been well-documented for a long time, and these research investigations provide empirical evidence for these practices and also help us better understand these phenomena.
4.3. Focused Research Initiatives on Meditation by Organizations
Alongside the studies discussed above, focused research initiatives by certain organizations have helped uncover the effects of long and short-term meditation and Yoga. On the one hand, there are organizations such as Ashtanga Yoga Vijnana Mandiram (AYVM; https://www.ayvm.in/), the Isha Foundation (https://isha.sadhguru.org/us-en/isha-research-center), and Art of Living (http://www.aolresearch.org/index.html) that have carried out research on the effects of their specific Yoga and meditation practices on the brain and body. On the other hand, organizations such as Swami Vivekananda Yoga Anusandhana Samsthana (S-VYASA; https://svyasa.edu.in/research_publications.html), Patanjali Research Institute (https://patanjali.res.in/research-paper.php) and Center for the Healthy Minds at the University of Wisconsin Madison (https://centerhealthyminds.org/science/publications) have advanced research on multiple meditation techniques currently in vogue. Below, we provide a glimpse of published research by such organized efforts. It is noteworthy that many more organizations have contributed to this endeavor, but it is outside our scope here to document that work fully. Instead, we aim to provide only a glimpse of such efforts, and this is in no way comprehensive or complete. We only include those studies that deal with meditation or mind control in some form. We substantiate the concepts and ideas with peer-reviewed scientific studies.
AYVM (originating from Hedathale, Karnataka, India) was one of the pioneers in the application of scientific methods for understanding the physiological correlates of higher states of consciousness induced by meditation. In one of the first experiments conducted way back in 1955, physiological measurements were made from a subject in the highest state of consciousness (also referred to as Samaadhi). Markers of subdued metabolism such as decreased body temperature, feeble heart sounds, and imperceptible pulse at the radial artery were observed [87,88]. Interestingly, the state was characterized by a strange combination of subdued metabolism, increased muscle tone and sensory withdrawal (for example, even when the subject had opened her eyes, there was no behavioral manifestation of visual perception). A series of experiments were conducted by researchers between 1985 and 1995 with support from AYVM using more advanced instrumentation. In these experiments, EEG, electromyogram (EMG), electrocardiogram (ECG), and breathing were measured from subjects while they attained higher states of consciousness through meditation. One such case study showed increased dimensional complexity of EEG during meditative states [89].
Following early pioneering work by AYVM, recent efforts by other organizations have gathered pace since 2000. The 3-month long Anaadhi retreat program of Isha Foundation (Coimbatore, Tamil Nadu, India), where participants underwent rigorous in-house meditation and Yoga practices, indicated a positive effect on several biomarkers, an increase of the anti-inflammatory marker Interleukin-10 (IL-10) and a decrease of the pro-inflammatory marker Interleukin-12 (IL-12). It confirms a reduction in inflammation and a strengthening of the immune response [90]. The same meditation practice also showed enhanced attention and neuroplasticity [91].
Correspondingly, practitioners of the Sudarshan Kriya Yoga (SKY), a program by the Art of Living Foundation (Bangalore, Karnataka, India) involving a rhythmic and cyclical pattern of breathing, demonstrated an increase in EEG beta activity, indicating greater mental focus [92]. Thereafter, a one-week trial using the technique on Iraq and Afghanistan war veterans exhibited a significant decrease in post-traumatic stress disorder (PTSD) symptoms, which persisted for a year without follow-up sessions [94]. Other studies by the Art of Living (on SKY) showed evidence of improved brain functionality [92,94,95,96], with improved relapse response from stressful situations [97].
At S-VYASA (Jigani, Karnataka, India), an institute dedicated to understanding the implications of Yoga in humankind, researchers have published articles on this topic from as early as 1995. One fMRI study emphasized the three stages of Yogic meditation: focused attention, object-centric focused attention, and effortless focused attention [97]. Results suggested an association with sustained attention, memory, semantic cognition, and creativity, in addition to an increased ability to mentally detach for effortless focused meditation. Researchers from the Patanjali Research Institute (Haridwar, Uttarakhand, India) have investigated neurophysiological changes due to Yogic breathing techniques using EEG [98]. Dr. Richard Davidson from the Center for the Healthy Minds (Madison, Wisconsin, USA) was an early pioneer in meditation research [99]. His collaborations with the Dalai Lama have produced interesting scientific literature on meditation. We are unable to review that literature here, but readers can find information at: https://centerhealthyminds.org/science/publications/list?s=228
5. Mantra and Pranayama
Mantra and chanting are also prevalent in many cultures in the form of a single word, multiple words, songs, or unique sounds. Chanting is integral to some forms of meditation (such as Transcendental Meditation). However, this section focuses exclusively on studies that investigated chanting without coupling it with meditative practices. These practices have been present in various cultures and religions for ages, with notions that it helps to heal, feel “close to the supreme power”, and reduce stress. South Asian religions (Hinduism, Buddhism, Sikhism and Jainism) use the word ‘Om’ or ‘Aum’. Buddhism has other sets of chants as well based on various schools. Chanting is also widespread among the Aboriginals of Australia, African and Native American cultures, Judaism, Islam (Dhikr) [100], and Christianity (Gregorian chants) via ancient songs and tales [101]. In the following section, a couple of studies are presented that specifically focus on the effects of various mantras and chanting practices on brain function.
A scientific study that gathered public attention compared Vedic priests (experienced in mantra chanting) with a matched control group (did not chant mantras) and showed increased cortical thickness among Vedic priests in the frontal (involved in higher cognition) and temporal lobes (which is known to be important for spirituality) [102]. More rigorous and extensive experiments are required to identify the mechanistic underpinning of this outcome. Another famous study done in Israel, involving Jews undertaking chanting using repetitive speech, induced large-scale deactivation in the brain [103]. This is important because this deactivation calms down the over-activated limbic regions responsible for emotional over-reactivity. Another study investigated the effects and benefits of ‘OM’ chanting on brain function [104]. A popular treatment to induce limbic deactivation in psychiatric disorders is via Vagal nerve stimulation, an invasive procedure that reduces stress and anxiety [105]. The study found that chanting ‘OM’ had similar limbic deactivation effects. The experiment had four blocks of chanting ‘OM’ or ‘SSSS’ (control) or silence (REST), each lasting for 15 seconds (REST, OM, REST, SSSS). In order to identify the brain response specific to the ‘OM’ chant, which is a nasal sound, the non-nasal chant of ‘SSSS’ was administered as a control condition. Connectivity strength between various brain regions of the limbic system decreased [106] (the regions interacted with each other less) during “OM” chanting as compared to chanting “SSSS” or silence, which induces calming and de-stressing effects during ‘OM’ chanting.
Besides meditation, mantra, and chanting, the other important aspect investigated is the effect of various breathing techniques on the brain. Voluntary control of breathing is referred to as “Pranayama”, an integral part of the Yogic traditions of India. However, it is important to note here that a full review of neural correlates of mantra and chanting mentioned above and pranayama in the upcoming section are out of the scope of this article. We intend to give an overview on the topics with peer-reviewed scientific studies.
Breathing is essentially used as a tool to modulate attention; hence, it is organically intertwined with meditation. In fact, many of the meditation techniques discussed in this article involve voluntary breath modulation as an essential step. Therefore, the neural mechanisms underlying such meditative practices cannot be easily separated from the neural substrates of voluntary control of breathing. That said, here we present a few studies focusing exclusively on the voluntary modulation of breathing without connotations to meditation. For example, a systematic review synthesized the available literature on the link between nasal airflow and brain activity, and proposed that asymmetrical brain activity and nasal flow influence one another throughout the day [107]. They suggested that asymmetry of brain activity (an ultradian rhythm) induces asymmetry in breathing, i.e., how much one breathes through each nostril (relative airflow). This process happens involuntarily. It follows that it should then be possible to voluntarily modulate breathing to affect brain activity. For example, one can voluntarily close their nose to perform uni-nostril breathing. Then the trigeminal nerve endings in the open nostril get activated with the airflow, and in turn, the stimulus travels all the way to the cortex via the spinal trigeminal nucleus and brainstem reticular formation, affecting cognitive functioning and processing speed [108,109]. Studies also show that uni-nostril nasal airflow has greater effects on the contralateral cortex [109,110,111,112]. These mechanisms form the basis of the effects of Pranayama.
An fNIRS study reported a surprising finding about breathing and brain activity [13]. Individuals performed either right or left nostril breathing, and data were collected before and during the process. Results showed a higher oxyHb (oxygenated hemoglobin) level in the left pre-frontal cortex with right nostril Yoga breathing and a lower oxyHb level with left nostril Yoga breathing. This could be due to the fact that airflow affects the contralateral cortex. The researchers substantiated the results with arguments from both Ayurveda and modern science. In Ayurveda, a traditional ancient Yogic view is that left nostril Yoga breathing (also termed ‘Chandra anuloma-viloma’) produces a calming and relaxing effect, possibly brought out by lower activity in the left hemisphere. In contrast, right nostril Yoga breathing (also termed ‘Surya anulom-aviloma’) is more activating and energizing, possibly caused by higher activity in the left hemisphere [110]. The simile here to “Chandra” or moon for calming and “Surya” or sun for energizing is interesting. The studies presented above show that even in the absence of explicit meditation or focusing of attention, voluntary control of breathing is a powerful technique for modulating brain activity. It is conceivable that specific patterns of breathing can be designed that modulate brain activity in particular ways, sometimes in ways that are beneficial for attention modulation, and hence meditation. We speculate that this has led to synergy and intertwining of breathing and meditative practices.
6. Religiosity
As mentioned in this article’s introduction, both spirituality and religiosity may involve experiencing higher states of consciousness. However, in contrast to spirituality, religiosity is associated with beliefs, related practices, and philosophical principles of specific religions. Many civilizations that developed in isolation, such as the Aboriginals of Australia, also have the concept of God and aspects of religiosity. Since they had limited connection (if any) with the rest of the world, the possibility that religious ideas propagated from elsewhere could generally be ruled out. Thus, the question arises whether there is any biological or evolutionary basis for religion that allows it to evolve spontaneously in a given society. To answer this, one might ponder the possibility that our brains are wired in a way that drives us toward believing in the existence of God or a supernatural power to continue our survival. This is a new field of active research called neurotheology [114,115]. One study that provides some insight into this concept performed fMRI scans on two groups of people who identified themselves as highly religious or highly non-religious [116]. The data was acquired at NIH, Baltimore, USA, and analyzed at Auburn University, Alabama, USA.
The question probed was how religious beliefs shape one’s brain. The research group focused not only on the brain regions that were activated during the processing of religious information but also on the connections between those regions. Religious people showed a stronger connection between the right medial frontal gyrus and the left inferior frontal gyrus in the frontal cortex (a region specialized in humans) compared to non-religious people. This connection is known to be involved in decoding the intentions of others [116]. This makes sense since one would have to attribute intentions to a supernatural power or God to believe in a religion. It also raises the possibility that the spontaneous evolution of religion in societies is a likely byproduct of the evolution of Theory of Mind (ToM) abilities in humans (which are used to decode the intentions of others). Another research group reported that the brain region (caudate) associated with the feeling of bliss is also activated during religious prayers [117].
If religiosity has a neural basis, the question arises whether religiosity is useful to us as a living organism. The theory of evolution suggests that traits that are useful for the long-term survival of the organism are retained and passed on, whilst the rest are discarded slowly over generations (survival of the fittest). If religiosity does have an evolutionary basis, then it must have some beneficial effects that increase the survival of the human race. A few studies have addressed this question. For example, McGowan et al. showed that having a higher purpose in life has an influence on higher happiness and reduced stress [118]. A vast number of people find meaning in religion. Hence, the reduced stress level arising from that can have health benefits. In another notable study, Schoenthaler et al. investigated the effect of religiosity on relapse and remission rates of addiction [119]. The findings suggested that the remission rates are higher for religious people, whereas the relapse rates are higher for non-religious people. This is merely an empirical observation and does not suggest causation. However, it is noteworthy that religious people showing higher remission rates exhibited higher cognitive control, which may improve the organism's survival. Thus, it is reasonable to hypothesize that religiosity may have an evolutionary basis by playing an essential role in the survival of our species. Further large-scale studies are needed to test these hypotheses conclusively.
7. Brain and the Body
Until the previous section, the focus was solely on the brain. However, the brain cannot be seen in isolation. The body plays a vital role in how our brain responds and vice-versa. The brain is connected with the rest of the body via various neural pathways through the spinal cord and the peripheral nervous system. The central nervous system is neurally connected to the periphery via bundles of axons, and neurotransmitters, chemicals, and hormones additionally regulate these links. These pathways enable the brain to send signals through an electric impulse or via chemical signaling to the body and vice-versa to control and maintain everyday functions (breathing, digestion, sensory feelings, motor actions, etc.). One of the most critical pathways that connects the brain and the body is the ‘gut-brain axis’, through which the brain and the enteric nervous system (related to the intestine) communicate bidirectionally, bridging between the emotional and cognitive centers of the brain and the intestine and its outlying areas [120]. Recent research has shown that gut microbiota (organisms thriving in our enteric system) influences the interaction between the brain and the enteric nervous system, and the brain can significantly influence it and be influenced by it [121]. The other signaling pathway known as the hypothalamic pituitary adrenal axis, as shown in Figure 8, regulates the neuroendocrine mechanisms (response to stress that in turn modulates body processes such as digestion) [122]. The intrinsic relation between the brain and the body can be understood within the framework of the somatic marker hypothesis that explains how feedback from the body affects decision-making in the brain [123]. For instance, food intake, stress response, and emotional state affect the neuroendocrine responses [124].
Besides the body, genetics can also be influenced by brain states. For example, Ravnik-Glavač et al. showed significant differential gene expression associated with higher states of consciousness [125]. Mindfulness meditation also has epigenetic effects, likely affecting physiological processes throughout the body, including in the brain [126]. There are immense possibilities for further research on the bidirectional interplay between higher states of consciousness (and mysticism in general) and various bodily systems via multiple pathways that exist between the brain and the body [127].
8. Conclusions
This article addresses the longstanding question of the brain basis of mysticism. We trace this question's historical and philosophical context and prevailing skepticism on this topic in the current society. We offer a prescription in terms of rigorous scientific research on this question to address the skepticism. Consequently, we showcased peer-reviewed literature on various aspects of the brain basis of mysticism. This includes both spirituality and religiosity, with the former covering practices such as meditation, mantra/chanting, and breathing. In the end, we concluded by espousing that the intricate relationships between the brain and body must be considered in future research endeavors regarding the brain basis of mysticism.
Our review of the peer-reviewed scientific literature clearly suggested that research on the brain basis of mysticism has explicit benefits to society. First, many practices that are part of mysticism also have direct health benefits. Therefore, it has the potential to improve human health. Understanding their mechanistic basis would be essential for their benefits to be realizable in the clinic. Next, understanding the brain basis of mysticism will likely answer some fundamental questions that humans have been wrestling with for ages. It is essential for the scientific enterprise to shape the narrative on this topic with hard facts. Else, others will do so with misinformation. Science should address them because these questions will not go away from the inquisitive human mind. We feel that now is the right time to do so.
Acknowledgments
We (G.D. and D.R.) express gratitude to Sri Sriranga Mahaguru (1913–1969), who contributed to and inspired our thought process through his life and work. One of the aspects of his multidimensional life was that [87,88] he conducted experimental research on topics of Yoga, meditation and Samaadhi using naaDi measurements (a traditional Indian system of diagnosis and subjective biophysical measurement based on the time-varying spatiotemporal patterns of blood flow at the wrist’s radial artery). He also conducted experiments using contemporary instruments with limited facilities available during his time. Additionally, he investigated extraneous and lifestyle factors that favorably or unfavorably affected the mind/body in pursuing higher states of consciousness such as Samaadhi. His ideas and work predated even the first evidence-based journal publication on Yogic meditation. He argued that the concepts of ancient Indian literature can be investigated objectively. At a time when traditional scholars and scientists generally disagreed with each other, he showed a way forward to bridge the two, which were way ahead of his times. While conducting the investigations presented in this report, we adopted many of his ideas. We also express gratitude to Smt. Vijayalakshmi Srimataji (1919–2022), who carried this spirit forward and provided us with the necessary encouragement and nourishment. We thank Ashtanga Yoga Vijnana Mandiram (AYVM), Karnataka, India (an organization founded by Sriranga Mahaguru in 1947) for maintaining the ideas of Sriranga Mahaguru and educating us about the same. We are grateful to Dr. D. Narayana Dutt for inspiring and educating us through his life and work, and for valuable discussions during the course of this investigation.
Disclosures
The authors report no competing financial interests related to the contents of this manuscript.
References
- C. Q. Choi. (February 09, 2016) Mystical Experiences Open a ‘Door of Perception’ in the Brain. Accessed on December 26, 2022. [Online]. Available: https://www.livescience.com/53652-brain-origins-of-mysticism-found.html.
- S. Lauricella, “The ancient-turned-new concept of “spiritual hygiene”: an investigation of media coverage of meditation from 1979 to 2014,” Journal of religion and health, vol. 55, no. 5, pp. 1748–1762, 2016.
- C. Gururaja, D. Rangaprakash, and G. Deshpande, “Research Trends in the Application of Yoga to Human Health: A Data Science Approach,” International journal of public mental health and neurosciences, vol. 7, no. 1, p. 8, 2020.
- Y. Bhattacharjee, “Neuroscientists welcome Dalai Lama with mostly open arms,” Science, vol. 310, no. 5751, pp. 1104–1104, 2005.
- P. Mergenthaler, U. Lindauer, G. A. Dienel, and A. Meisel, “Sugar for the brain: the role of glucose in physiological and pathological brain function,” Trends in neurosciences, vol. 36, no. 10, pp. 587–597, 2013.
- M. S. Goyal and M. E. Raichle, “Glucose requirements of the developing human brain,” Journal of pediatric gastroenterology and nutrition, vol. 66, no. Suppl 3, p. S46, 2018.
- K. Rehni and K. R. Dave, “Impact of hypoglycemia on brain metabolism during diabetes,” Molecular neurobiology, vol. 55, no. 12, pp. 9075–9088, 2018.
- J. M. Rosenthal, S. A. Amiel, L. Yaguez, E. Bullmore, D. Hopkins, M. Evans, A. Pernet, H. Reid, V. Giampietro, C. M. Andrew et al., “The effect of acute hypoglycemia on brain function and activation: a functional magnetic resonance imaging study,” Diabetes, vol. 50, no. 7, pp. 1618–1626, 2001.
- G. N. Cantor, J. R. Christie, M. J. S. Hodge, and R. C. Olby, Companion to the history of modern science. Routledge, 2006.
- J. Shaffer, “Neuroplasticity and clinical practice: building brain power for health,” Frontiers in psychology, vol. 7, p. 1118, 2016.
- H. S. Mayberg, A. M. Lozano, V. Voon, H. E. McNeely, D. Seminowicz, C. Hamani, J. M. Schwalb, and S. H. Kennedy, “Deep brain stimulation for treatment-resistant depression,” Neuron, vol. 45, no. 5, pp. 651–660, 2005.
- K. W. Scangos, A. N. Khambhati, P. M. Daly, G. S. Makhoul, L. P. Sugrue, H. Zamanian, T. X. Liu, V. R. Rao, K. K. Sellers, H. E. Dawes et al., “Closed-loop neuromodulation in an individual with treatment-resistant depression,” Nature Medicine, vol. 27, no. 10, pp. 1696–1700, 2021.
- V. R. Rao, K. K. Sellers, D. L. Wallace, M. B. Lee, M. Bijanzadeh, O. G. Sani, Y. Yang, M. M. Shanechi, H. E. Dawes, and E. F. Chang, “Direct electrical stimulation of lateral orbitofrontal cortex acutely improves mood in individuals with symptoms of depression,” Current Biology, vol. 28, no. 24, pp. 3893–3902, 2018.
- N. Phillips. (April 04, 2018) Brain-stimulation trials get personal to lift depression. Accessed on December 14, 2022. [Online]. Available: https://www.nature.com/articles/d41586-018-03864-4.
- J. Kingsland. (January 21, 2021) Personalized brain stimulation lifts a patient’s depression. Accessed on December 20, 2022. [Online]. Available: https://www.medicalnewstoday.com/articles/personalized-brain-stimulation-lifts-a-patients-depression.
- D. N. Phillips, K. S. Bonat, N. F. Olumide, and S. Medavarapu, “Importance and effectiveness of brain stimulation in the treatment of depression and insomnia,” Archives of Medicine, vol. 9, no. 1:4, 2017.
- B. Greenberg, L. Gabriels, D. Malone, A. Rezai, G. Friehs, M. Okun, N. Shapira, K. Foote, P. Cosyns, C. Kubu et al., “Deep brain stimulation of the ventral internal capsule/ventral striatum for obsessive-compulsive disorder: worldwide experience,” Molecular Psychiatry, vol. 15, no. 1, pp. 64–79, 2010.
- G. Deuschl, C. Schade-Brittinger, P. Krack, J. Volkmann, H. Schafer, K. Botzel, C. Daniels, A. Deutschlander, U. Dillmann, W. Eisner et al., “A randomized trial of deep-brain stimulation for Parkinson’s disease,” New England Journal of Medicine, vol. 355, no. 9, pp. 896–908, 2006.
- D.-B. S. for Parkinson’s Disease Study Group, “Deep-brain stimulation of the subthalamic nucleus or the pars interna of the globus pallidus in Parkinson’s disease,” New England Journal of Medicine, vol. 345, no. 13, pp. 956–963, 2001.
- R. Fisher, V. Salanova, T. Witt, R. Worth, T. Henry, R. Gross, K. Oommen, I. Osorio, J. Nazzaro, D. Labar et al., “Electrical stimulation of the anterior nucleus of thalamus for treatment of refractory epilepsy,” Epilepsia, vol. 51, no. 5, pp. 899–908, 2010.
- P. R. Schuurman, D. A. Bosch, P. M. Bossuyt, G. J. Bonsel, E. J. Van Someren, R. M. De Bie, M. P. Merkus, and J. D. Speelman, “A comparison of continuous thalamic stimulation and thalamotomy for suppression of severe tremor,” New England Journal of Medicine, vol. 342, no. 7, pp. 461–468, 2000.
- M. Vidailhet, L. Vercueil, J.-L. Houeto, P. Krystkowiak, A.-L. Benabid, P. Cornu, C. Lagrange, S. Tezenas du Montcel, D. Dormont, S. Grand et al., “Bilateral deep-brain stimulation of the globus pallidus in primary generalized dystonia,” New England Journal of Medicine, vol. 352, no. 5, pp. 459–467, 2005.
- Kupsch, S. Klaffke, A. Ku¨hn, W. Meissner, G. Arnold, G. Schneider, K. Maier-Hauff, and T. Trottenberg, “The effects of frequency in pallidal deep brain stimulation for primary dystonia,” Journal of Neurology, vol. 250, pp. 1201–1205, 2003.
- M. J. Nelson, I. El Karoui, K. Giber, X. Yang, L. Cohen, H. Koopman, S. S. Cash, L. Naccache, J. T. Hale, C. Pallier et al., “Neurophysiological dynamics of phrase-structure building during sentence processing,” Proceedings of the National Academy of Sciences, vol. 114, no. 18, pp. E3669–E3678, 2017.
- B. He and Z. Liu, “Multimodal functional neuroimaging: integrating functional MRI and EEG/MEG,” IEEE reviews in biomedical engineering, vol. 1, pp. 23–40, 2008.
- M. A. Shampo and R. A. Kyle, “Felix Bloch—developer of magnetic resonance imaging,” in Mayo Clinic Proceedings, vol. 70, no. 9. Elsevier, 1995, p. 889.
- M. A. Shampo and R. A. Kyle, “Edward M. Purcell—Nobel Prize for Magnetic Resonance Imaging,” in Mayo Clinic Proceedings, vol. 72, no. 6. Elsevier, 1997, p. 585.
- J. Gore, “Out of the shadows—MRI and the Nobel Prize,” New England Journal of Medicine, vol. 349, no. 24, pp. 2290–2292, 2003.
- S. Ogawa, T.-M. Lee, A. R. Kay, and D. W. Tank, “Brain magnetic resonance imaging with contrast dependent on blood oxygenation.” Proceedings of the National Academy of Sciences, vol. 87, no. 24, pp. 9868–9872, 1990.
- S. Ogawa, T.-M. Lee, A. S. Nayak, and P. Glynn, “Oxygenation-sensitive contrast in magnetic resonance image of rodent brain at high magnetic fields,” Magnetic resonance in medicine, vol. 14, no. 1, pp. 68–78, 1990.
- K. K. Kwong, J. W. Belliveau, D. A. Chesler, I. E. Goldberg, R. M. Weisskoff, B. P. Poncelet, D. N. Kennedy, B. E. Hoppel, M. S. Cohen, R. Turner, and et al., “Dynamic magnetic resonance imaging of human brain activity during primary sensory stimulation.” Proceedings of the National Academy of Sciences, vol. 89, no. 12, p. 5675–5679, 1992.
- P. A. Bandettini, E. C. Wong, R. S. Hinks, R. S. Tikofsky, and J. S. Hyde, “Time course EPI of human brain function during task activation,” Magnetic resonance in medicine, vol. 25, no. 2, pp. 390–397, 1992.
- B. Cummings, “Chapter 12: Functional Areas of the Cerebral Cortex,” Austin Peay State University [Online]. Available: http://www.apsu.edu/ [Accessed 10 January 2013].
- G. Queiros, “Computational methods for fMRI image processing and analysis,” Master’s thesis, University of Porto, 2013.
- J. R. Polimeni, B. Fischl, D. N. Greve, and L. L. Wald, “Laminar analysis of 7 T BOLD using an imposed spatial activation pattern in human V1,” Neuroimage, vol. 52, no. 4, pp. 1334–1346, 2010.
- U. Hasson, Y. Nir, I. Levy, G. Fuhrmann, and R. Malach, “Intersubject synchronization of cortical activity during natural vision,” Science, vol. 303, no. 5664, pp. 1634–1640, 2004.
- D. Orenstein. (May 16, 2012) People with paralysis control robotic arms using brain-computer interface. Accessed on February 14, 2023. [Online]. Available: https://news.brown.edu/articles/2012/05/braingate2.
- Saini. (May 27, 2009) The brain police: judging murder with an MRI. Accessed on December 12, 2022. [Online]. Available: https://www.wired.co.uk/article/guilty.
- E. De Filippi, A. Escrichs, E. Camara, C. Garrido, T. Marins, M. Sanchez-Fibla, M. Gilson, and G. Deco, “Meditation-induced effects on whole-brain structural and effective connectivity,” Brain Structure and Function, vol. 227, no. 6, pp. 2087–2102, 2022.
- R. F. Afonso, I. Kraft, M. A. Aratanha, and E. H. Kozasa, “Neural correlates of meditation: a review of structural and functional MRI studies,” Frontiers in Bioscience-Scholar, vol. 12, no. 1, pp. 92–115, 2020.
- B. R. Cahn and J. Polich, “Meditation states and traits: EEG, ERP, and neuroimaging studies.” Psychological Bulletin, vol. 132, no. 2, p. 180, 2006.
- K. C. Fox, M. L. Dixon, S. Nijeboer, M. Girn, J. L. Floman, M. Lifshitz, M. Ellamil, P. Sedlmeier, and K. Christoff, “Functional neuroanatomy of meditation: A review and meta-analysis of 78 functional neuroimaging investigations,” Neuroscience & Biobehavioral Reviews, vol. 65, pp. 208–228, 2016.
- C. J. Dahl, A. Lutz, and R. J. Davidson, “Reconstructing and deconstructing the self: cognitive mechanisms in meditation practice,” Trends in cognitive sciences, vol. 19, no. 9, pp. 515–523, 2015.
- Lutz, H. A. Slagter, J. D. Dunne, and R. J. Davidson, “Attention regulation and monitoring in meditation,” Trends in cognitive sciences, vol. 12, no. 4, pp. 163–169, 2008.
- Y.-Y. Tang, B. K. Holzel, and M. I. Posner, “The neuroscience of mindfulness meditation,” Nature Reviews Neuroscience, vol. 16, no. 4, pp. 213–225, 2015.
- C. Conversano, R. Ciacchini, G. Orru`, M. Di Giuseppe, A. Gemignani, and A. Poli, “Mindfulness, compassion, and self-compassion among health care professionals: what’s new? A systematic review,” Frontiers in Psychology, vol. 11, p. 1683, 2020.
- S. Karama, M. E. Bastin, C. Murray, N. A. Royle, L. Penke, S. Munoz Maniega, A. J. Gow, J. Corley, M. Valdes Hernandez, J. D. Lewis et al., “Childhood cognitive ability accounts for associations between cognitive ability and brain cortical thickness in old age,” Molecular Psychiatry, vol. 19, no. 5, pp. 555–559, 2014.
- S. R. Cox, S. J. Ritchie, C. Fawns-Ritchie, E. M. Tucker-Drob, and I. J. Deary, “Structural brain imaging correlates of general intelligence in UK Biobank,” Intelligence, vol. 76, p. 101376, 2019.
- S. J. Ritchie, T. Booth, M. d. C. V. Hernandez, J. Corley, S. M. Maniega, A. J. Gow, N. A. Royle, A. Pattie, S. Karama, J. M. Starr et al., “Beyond a bigger brain: Multivariable structural brain imaging and intelligence,” Intelligence, vol. 51, pp. 47–56, 2015.
- K. L. Narr, R. P. Woods, P. M. Thompson, P. Szeszko, D. Robinson, T. Dimtcheva, M. Gurbani, A. W. Toga, and R. M. Bilder, “Relationships between IQ and regional cortical gray matter thickness in healthy adults,” Cerebral cortex, vol. 17, no. 9, pp. 2163–2171, 2007.
- M. Thambisetty, J. Wan, A. Carass, Y. An, J. L. Prince, and S. M. Resnick, “Longitudinal changes in cortical thickness associated with normal aging,” Neuroimage, vol. 52, no. 4, pp. 1215–1223, 2010.
- S. Ramanoe l, E. Hoyau, L. Kauffmann, F. Renard, C. Pichat, N. Boudiaf, A. Krainik, A. Jaillard, and M. Baciu, “Gray matter volume and cognitive performance during normal aging. A voxel-based morphometry study,” Frontiers in Aging Neuroscience, vol. 10, p. 235, 2018.
- S. W. Lazar, C. E. Kerr, R. H. Wasserman, J. R. Gray, D. N. Greve, M. T. Treadway, M. McGarvey, B. T. Quinn, J. A. Dusek, H. Benson et al., “Meditation experience is associated with increased cortical thickness,” Neuroreport, vol. 16, no. 17, p. 1893, 2005.
- E. A. Zimmermann, E. Schaible, H. Bale, H. D. Barth, S. Y. Tang, P. Reichert, B. Busse, T. Alliston, J. W. Ager III, and R. O. Ritchie, “Age-related changes in the plasticity and toughness of human cortical bone at multiple length scales,” Proceedings of the National Academy of Sciences, vol. 108, no. 35, pp. 14416–14421, 2011.
- R. Tang, K. J. Friston, and Y.-Y. Tang, “Brief mindfulness meditation induces gray matter changes in a brain hub,” Neural plasticity, vol. 2020, pp. 8830005. 2020.
- R. Kakigi, H. Nakata, K. Inui, N. Hiroe, O. Nagata, M. Honda, S. Tanaka, N. Sadato, and M. Kawakami, “Intracerebral pain processing in a Yoga Master who claims not to feel pain during meditation,” European Journal of Pain, vol. 9, no. 5, pp. 581–589, 2005.
- F. Zeidan and D. R. Vago, “Mindfulness meditation–based pain relief: a mechanistic account,” Annals of the New York Academy of Sciences, vol. 1373, no. 1, pp. 114–127, 2016.
- G. Riegner, G. Posey, V. Oliva, Y. Jung, W. Mobley, and F. Zeidan, “Disentangling self from pain: mindfulness meditation-induced pain relief is driven by thalamic-default mode network decoupling,” Pain, vol. 164, no. 2, pp. 280–291, 2023.
- D. Zhou, Y. Kang, D. Cosme, M. Jovanova, X. He, A. Mahadevan, J. Ahn, O. Stanoi, J. K. Brynildsen, N. Cooper et al., “Mindful attention promotes control of brain network dynamics for self-regulation and discontinues the past from the present,” Proceedings of the National Academy of Sciences, vol. 120, no. 2, p. e2201074119, 2023.
- R. C. DeCharms, F. Maeda, G. H. Glover, D. Ludlow, J. M. Pauly, D. Soneji, J. D. Gabrieli, and S. C. Mackey, “Control over brain activation and pain learned by using real-time functional MRI,” Proceedings of the National Academy of Sciences, vol. 102, no. 51, pp. 18626–18631, 2005.
- E. J. Modestino, “Neurophenomenology of an altered state of consciousness: An fMRI case study,” Explore, vol. 12, no. 2, pp. 128–135, 2016.
- E. Koechlin, G. Corrado, P. Pietrini, and J. Grafman, “Dissociating the role of the medial and lateral anterior prefrontal cortex in human planning,” Proceedings of the National Academy of Sciences, vol. 97, no. 13, pp. 7651–7656, 2000.
- C. K. Kovach, N. D. Daw, D. Rudrauf, D. Tranel, J. P. O’Doherty, and R. Adolphs, “Anterior prefrontal cortex contributes to action selection through tracking of recent reward trends,” Journal of Neuroscience, vol. 32, no. 25, pp. 8434–8442, 2012.
- P. Arambula, E. Peper, M. Kawakami, and K. H. Gibney, “The physiological correlates of Kundalini Yoga meditation: a study of a yoga master,” Applied Psychophysiology and Biofeedback, vol. 26, pp. 147–153, 2001.
- G. Venkatasubramanian, P. N. Jayakumar, H. R. Nagendra, D. Nagaraja, R. Deeptha, and B. N. Gangadhar, “Investigating paranormal phenomena: Functional brain imaging of telepathy,” International Journal of Yoga, vol. 1, no. 2, p. 66, 2008.
- B. Anand, G. Chhina, and B. Singh, “Studies on Shri Ramanand Yogi during his stay in an air-tight box. 1961,” The Indian journal of medical research, vol. 136, no. 4, pp. 691–698, 2012.
- M. A. Wenger, B. Bagchi, and B. Anand, “Experiments in India on “voluntary” control of the heart and pulse,” Circulation, vol. 24, no. 6, pp. 1319–1325, 1961.
- M. A. Wenger and B. Bagchi, “Studies of autonomic functions in practitioners of yoga in India,” Behavioral Science, vol. 6, no. 4, pp. 312–323, 1961.
- B. Anand, G. Chhina, and B. Singh, “Some aspects of electroencephalographic studies in yogis,” Electroencephalography and Clinical Neurophysiology, vol. 13, no. 3, pp. 452–456, 1961.
- K. B. Baerentsen, “Patanjali and neuroscientific research on meditation,” Frontiers in Psychology, vol. 6, p. 915, 2015.
- S. V. Bharati, Yoga sutras of Patanjali. Motilal Banarsidass Publications, 2002.
- T. Brandmeyer and A. Delorme, “Reduced mind wandering in experienced meditators and associated EEG correlates,” Experimental brain research, vol. 236, no. 9, pp. 2519–2528, 2018.
- K. Dewhurst and A. Beard, “Sudden religious conversions in temporal lobe epilepsy,” The British Journal of Psychiatry, vol. 117, no. 540, pp. 497–507, 1970.
- R. V. Vishnubhotla, R. Radhakrishnan, K. Kveraga, R. Deardorff, C. Ram, D. Pawale, Y.-C. Wu, J. Renschler, B. Subramaniam, and S. Sadhasivam, “Advanced meditation alters resting-state brain network connectivity correlating with improved mindfulness,” Frontiers in Psychology, vol. 12, pp. 745344. 2021.
- Doll, B. K. Holzel, C. C. Boucard, A. M. Wohlschlager, and C. Sorg, “Mindfulness is associated with intrinsic functional connectivity between default mode and salience networks,” Frontiers in human neuroscience, vol. 9, p. 461, 2015.
- S. Ganesan, E. Beyer, B. Moffat, N. T. Van Dam, V. Lorenzetti, and A. Zalesky, “Focused attention meditation in healthy adults: A systematic review and meta-analysis of cross-sectional functional MRI studies,” Neuroscience & Biobehavioral Reviews, vol. 141, p. 104846, 2022.
- Barros-Loscertales, S. E. Hernandez, Y. Xiao, J. L. Gonzalez-Mora, and K. Rubia, “Resting state functional connectivity associated with Sahaja Yoga Meditation,” Frontiers in Human Neuroscience, vol. 15, p. 614882, 2021.
- S. E. Hernandez, J. Suero, A. Barros, J. L. Gonzalez-Mora, and K. Rubia, “Increased grey matter associated with long-term Sahaja Yoga meditation: a voxel-based morphometry study,” PloS one, vol. 11, no. 3, p. e0150757, 2016.
- T. Ramsay, L. Manderson, and W. Smith, “Changing a mountain into a mustard seed: Spiritual practices and responses to disaster among New York Brahma Kumaris,” Journal of Contemporary Religion, vol. 25, no. 1, pp. 89–105, 2010.
- K. Sharma, S. Chandra, and A. K. Dubey, “Exploration of lower frequency EEG dynamics and cortical alpha asymmetry in long-term Rajyoga meditators,” International journal of yoga, vol. 11, no. 1, p. 30, 2018.
- M. Babu, R. Kadavigere, P. Koteshwara, B. Sathian, and K. S. Rai, “Rajyoga meditation induces grey matter volume changes in regions that process reward and happiness,” Scientific Reports, vol. 10, no. 1, pp. 1–11, 2020.
- M. C. Mahone, F. Travis, R. Gevirtz, and D. Hubbard, “fMRI during Transcendental Meditation practice,” Brain and Cognition, vol. 123, pp. 30–33, 2018.
- Manna, A. Raffone, M. G. Perrucci, D. Nardo, A. Ferretti, A. Tartaro, A. Londei, C. Del Gratta, M. O. Belardinelli, and G. L. Romani, “Neural correlates of focused attention and cognitive monitoring in meditation,” Brain Research Bulletin, vol. 82, no. 1-2, pp. 46–56, 2010.
- J. A. Grant, J. Courtemanche, and P. Rainville, “A non-elaborative mental stance and decoupling of executive and pain-related cortices predicts low pain sensitivity in Zen meditators,” Pain, vol. 152, no. 1, pp. 150–156, 2011.
- S. Kwak, S.-Y. Kim, D. Bae, W.-J. Hwang, K. I. K. Cho, K.-O. Lim, H.-Y. Park, T. Y. Lee, and J. S. Kwon, “Enhanced attentional network by short-term intensive meditation,” Frontiers in Psychology, vol. 10, p. 3073, 2020.
- M. Izzetoglu, P. A. Shewokis, K. Tsai, P. Dantoin, K. Sparango, and K. Min, “Short-term effects of meditation on sustained attention as measured by fNIRS,” Brain Sciences, vol. 10, no. 9, p. 608, 2020.
- S. Chamu, “Sri Ranga Mahaguru” (in Kannada language). Mysore, India: Ashtanga Yoga Vijnana Mandiram, 1972.
- S. Chamu, “Sri Ranga Sadguru: A Short Biography of a Yogi”. Mysore, India: Ashtanga Yoga Vijnana Mandiram, 1992.
- N. Pradhan and D. Narayana Dutt, “An analysis of dimensional complexity of brain electrical activity during meditation,” in Proceedings of the First Regional Conference of IEEE Engineering in Medicine and Biology Society and 14th Conference of the Biomedical Engineering Society of India. New Delhi, India, pp. 92-93, 1995.
- B. R. Cahn, M. S. Goodman, C. T. Peterson, R. Maturi, and P. J. Mills, “Yoga, meditation and mind-body health: increased BDNF, cortisol awakening response, and altered inflammatory marker expression after a 3-month yoga and meditation retreat,” Frontiers in Human Neuroscience, vol. 11, p. 315, 2017.
- C. Braboszcz, B. R. Cahn, B. Balakrishnan, R. K. Maturi, R. Grandchamp, and A. Delorme, “Plasticity of visual attention in Isha yoga meditation practitioners before and after a 3-month retreat,” Frontiers in psychology, vol. 4, p. 914, 2013.
- M. Bhatia, A. Kumar, N. Kumar, R. Pandey, and V. Kochupillai, “Electrophysiologic evaluation of Sudarshan Kriya: an EEG, BAER, P300 study.” Indian Journal of Physiology and Pharmacology, vol. 47, no. 2, pp. 157–163, 2003.
- E. M. Seppala, J. B. Nitschke, D. L. Tudorascu, A. Hayes, M. R. Goldstein, D. T. Nguyen, D. Perlman, and R. J. Davidson, “Breathing-based meditation decreases posttraumatic stress disorder symptoms in US Military veterans: A randomized controlled longitudinal study,” Journal of Traumatic Stress, vol. 27, no. 4, pp. 397–405, 2014.
- P. N. V. Murthy, B. Gangadhar, N. Janakiramaiah, and D. Subbakrishna, “Normalization of P300 amplitude following treatment in dysthymia,” Biological Psychiatry, vol. 42, no. 8, pp. 740–743, 1997.
- P. N. V. Murthy, N. Janakiramaiah, B. Gangadhar, and D. Subbakrishna, “P300 amplitude and antidepressant response to Sudarshan Kriya Yoga (SKY),” Journal of Affective Disorders, vol. 50, no. 1, pp. 45–48, 1998.
- S. Chandra, A. K. Jaiswal, R. Singh, D. Jha, and A. P. Mittal, “Mental stress: Neurophysiology and its regulation by Sudarshan Kriya Yoga,” International Journal of Yoga, vol. 10, no. 2, p. 67, 2017.
- S. Telles, N. Singh, K. Naveen, S. Deepeshwar, S. Pailoor, N. Manjunath, L. George, R. Dawn, and A. Balkrishna, “A fMRI study of stages of yoga meditation described in traditional texts,” Journal of Psychology and Psychotherapy, vol. 5, no. 3, pp. 185, 2015.
- S. Pal, N. Kala, S. Telles, and A. Balkrishna, “Neurophysiological changes determined by the EEG with yoga breathing practices: A mini review,” Psychology, pp. 845–847, 2018.
- R. J. Davidson, J. Kabat-Zinn, J. Schumacher, M. Rosenkranz, D. Muller, S. F. Santorelli, F. Urbanowski, A. Harrington, K. Bonus, and J. F. Sheridan, “Alterations in brain and immune function produced by mindfulness meditation,” Psychosomatic Medicine, vol. 65, no. 4, pp. 564–570, 2003.
- Schimmel, Mystical dimensions of Islam. University of North Carolina Press, 1975.
- S. S. Yoga. (October 08, 2021) Sounding off on spirituality: Exploring chanting in different cultures. Accessed on January 10, 2023. [Online]. Available: https://www.soundoflife.com/blogs/places/sounding-off-on-spirituality-exploring-chanting-different-cultures.
- G. P. Kalamangalam and T. M. Ellmore, “Focal cortical thickness correlates of exceptional memory training in Vedic priests,” Frontiers in Human Neuroscience, vol. 8, p. 833, 2014.
- Berkovich-Ohana, M. Wilf, R. Kahana, A. Arieli, and R. Malach, “Repetitive speech elicits widespread deactivation in the human cortex: the “Mantra” effect?” Brain and Behavior, vol. 5, no. 7, p. e00346, 2015.
- G. Kalyani, G. Venkatasubramanian, R. Arasappa, N. P. Rao, S. V. Kalmady, R. V. Behere, H. Rao, M. K. Vasudev, and B. N. Gangadhar, “Neurohemodynamic correlates of ‘OM’ chanting: a pilot functional magnetic resonance imaging study,” International Journal of Yoga, vol. 4, no. 1, p. 3, 2011.
- J. D. Bremner, N. Z. Gurel, M. T. Wittbrodt, M. H. Shandhi, M. H. Rapaport, J. A. Nye, B. D. Pearce, V. Vaccarino, A. J. Shah, J. Park et al., “Application of noninvasive vagal nerve stimulation to stress-related psychiatric disorders,” Journal of Personalized Medicine, vol. 10, no. 3, p. 119, 2020.
- N. P. Rao, G. Deshpande, K. B. Gangadhar, R. Arasappa, S. Varambally, G. Venkatasubramanian, and B. N. Ganagadhar, “Directional brain networks underlying OM chanting,” Asian Journal of Psychiatry, vol. 37, pp. 20–25, 2018.
- Price and R. Eccles, “Nasal airflow and brain activity: is there a link?” The Journal of Laryngology & Otology, vol. 130, no. 9, pp. 794–799, 2016.
- S. Telles, P. Raghuraj, S. Maharana, and H. Nagendra, “Immediate effect of three yoga breathing techniques on performance on a letter-cancellation task,” Perceptual and Motor Skills, vol. 104, no. 3 suppl, pp. 1289–1296, 2007.
- M. Joshi and S. Telles, “Short communication immediate effects of right and left nostril breathing on verbal and spatial scores,” Indian Journal of Physiology and Pharmacology, vol. 52, no. 2, pp. 197–200, 2008.
- S. Telles, M. Joshi, and P. Somvanshi, “Yoga breathing through a particular nostril is associated with contralateral event-related potential changes,” International Journal of Yoga, vol. 5, no. 2, p. 102, 2012.
- D. Werntz, R. Bickford, and D. Shannahoff-Khalsa, “Selective hemispheric stimulation by unilateral forced nostril breathing.” Human Neurobiology, vol. 6, no. 3, pp. 165–171, 1987.
- D. S. Shannahoff-Khalsa, M. R. Boyle, and M. E. Buebel, “The effects of unilateral forced nostril breathing on cognition,” International Journal of Neuroscience, vol. 57, no. 3-4, pp. 239–249, 1991.
- K. Singh, H. Bhargav, and T. Srinivasan, “Effect of uninostril yoga breathing on brain hemodynamics: A functional near-infrared spectroscopy study,” International Journal of Yoga, vol. 9, no. 1, p. 12, 2016.
- Sayadmansour, “Neurotheology: The relationship between brain and religion,” Iranian Journal of Neurology, vol. 13, no. 1, p. 52, 2014.
- U. Schjoedt, “The religious brain: A general introduction to the experimental neuroscience of religion,” Method & Theory in the Study of Religion, vol. 21, no. 3, pp. 310–339, 2009.
- D. Kapogiannis, G. Deshpande, F. Krueger, M. P. Thornburg, and J. H. Graf- man, “Brain networks shaping religious belief,” Brain Connectivity, vol. 4, no. 1, pp. 70–79, 2014.
- U. Schjødt, H. Stødkilde-Jørgensen, A. W. Geertz, and A. Roepstorff, “Rewarding prayers,” Neuroscience Letters, vol. 443, no. 3, pp. 165–168, 2008.
- P. McGowan, Amanda L, Z. M. Boyd, Y. Kang, L. Bennett, P. Mucha, K. Ochsner, D. S. Bassett, E. B. Falk, and D. M. Lydon-Staley, “Network analysis of within-person temporal associations among physical activity, sleep, and wellbeing in situ,” Apr 2022. [Online]. Available: psyarxiv.com/q4jn3.
- S. J. Schoenthaler, K. Blum, E. R. Braverman, J. Giordano, B. Thompson, M. Oscar-Berman, R. D. Badgaiyan, M. A. Madigan, K. Dushaj, M. Li et al., “NIDA-Drug Addiction Treatment Outcome Study (DATOS) relapse as a function of spirituality/religiosity,” Journal of Reward Deficiency Syndrome, vol. 1, no. 1, p. 36, 2015.
- M. Carabotti, A. Scirocco, M. A. Maselli, and C. Severi, “The gut-brain axis: interactions between enteric microbiota, central and enteric nervous systems,” Annals of Gastroenterology, vol. 28, no. 2, p. 203, 2015.
- S. H. Rhee, C. Pothoulakis, and E. A. Mayer, “Principles and clinical implications of the brain–gut–enteric microbiota axis,” Nature reviews Gastroenterology & hepatology, vol. 6, no. 5, pp. 306–314, 2009.
- D. Muehsam, S. Lutgendorf, P. J. Mills, B. Rickhi, G. Chevalier, N. Bat, D. Chopra, and B. Gurfein, “The embodied mind: a review on functional genomic and neurological correlates of mind-body therapies,” Neuroscience & Biobehavioral Reviews, vol. 73, pp. 165–181, 2017.
- Bechara, D. Tranel, H. Damasio, and A. R. Damasio, “Failure to respond autonomically to anticipated future outcomes following damage to prefrontal cortex,” Cerebral Cortex, vol. 6, no. 2, pp. 215–225, 1996.
- Y. M. Ulrich-Lai, S. Fulton, M. Wilson, G. Petrovich, and L. Rinaman, “Stress exposure, food intake and emotional state,” Stress, vol. 18, no. 4, pp. 381–399, 2015.
- M. Ravnik-Glavac, S. Hrasovec, J. Bon, J. Dreu, and D. Glavac, “Genome-wide expression changes in a higher state of consciousness,” Consciousness and Cognition, vol. 21, no. 3, pp. 1322–1344, 2012.
- S. Venditti, L. Verdone, A. Reale, V. Vetriani, M. Caserta, and M. Zampieri, “Molecules of silence: Effects of meditation on gene expression and epigenetics,” Frontiers in Psychology, vol. 11, p. 1767, 2020.
- H. Niles, D. H. Mehta, A. A. Corrigan, M. K. Bhasin, and J. W. Denninger, “Functional genomics in the study of mind-body therapies,” Ochsner Journal, vol. 14, no. 4, pp. 681–695, 2014.
Figure 1.
Number of articles related to meditation published by year (top). Geographical distribution of articles, 1979–2014 (bottom) [2].
Figure 1.
Number of articles related to meditation published by year (top). Geographical distribution of articles, 1979–2014 (bottom) [2].
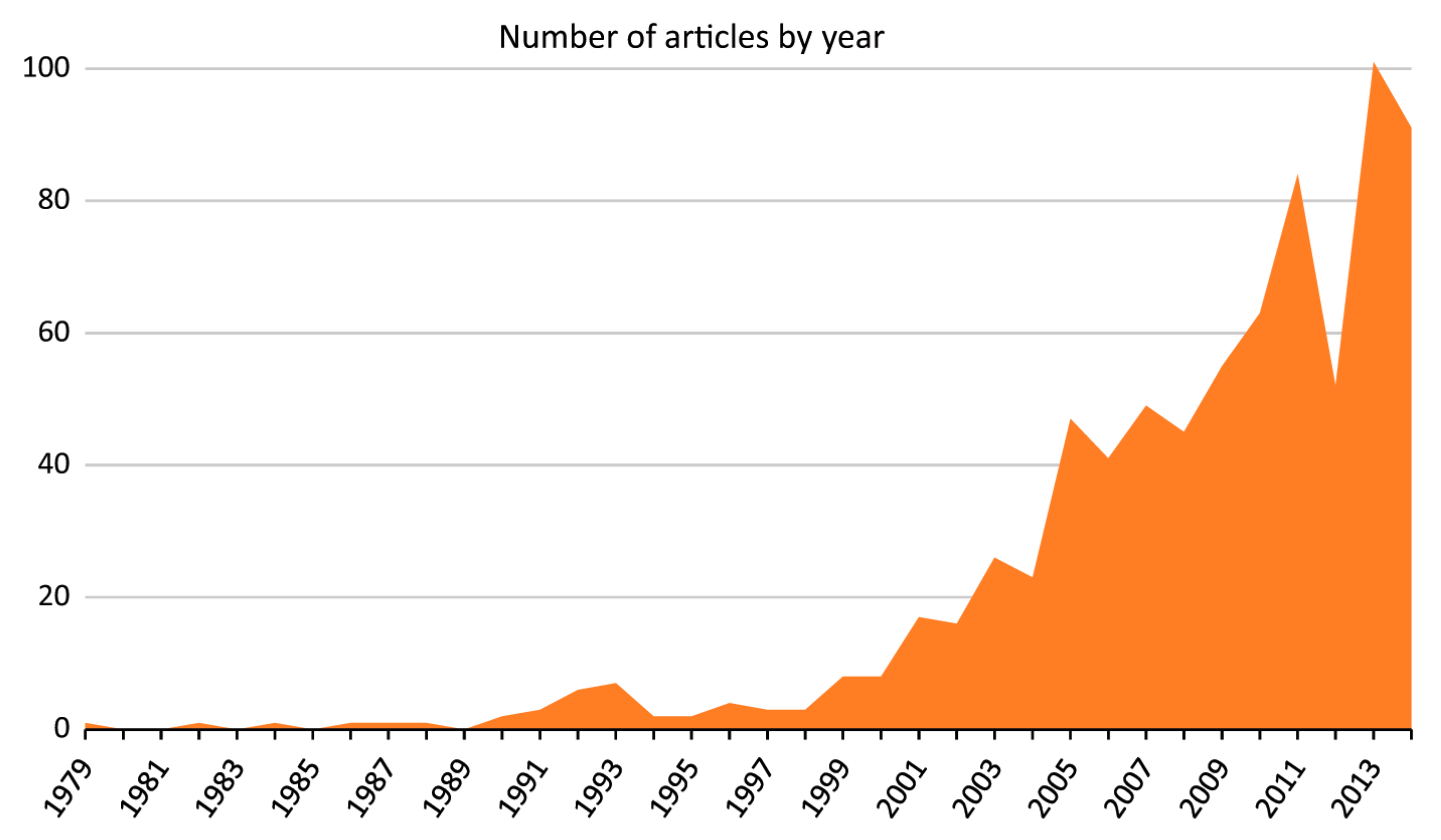
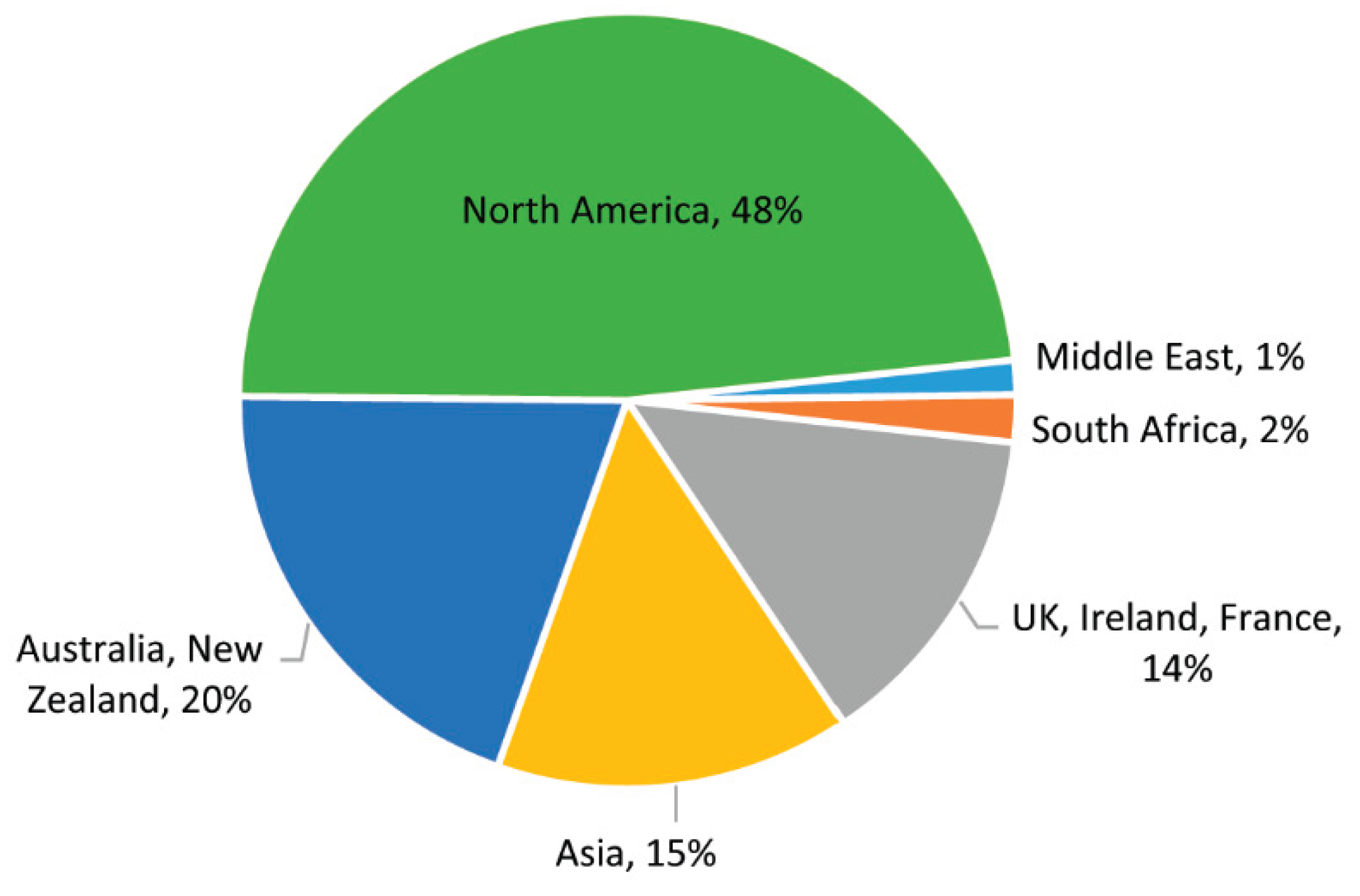
Figure 2.
Spatial and temporal resolution of various modalities to observe brain function. It should be noted that this figure is almost a decade old, and the temporal resolution of fMRI today is approaching that of EEG/MEG, which makes it an even better modality than it was previously [25].
Figure 2.
Spatial and temporal resolution of various modalities to observe brain function. It should be noted that this figure is almost a decade old, and the temporal resolution of fMRI today is approaching that of EEG/MEG, which makes it an even better modality than it was previously [25].
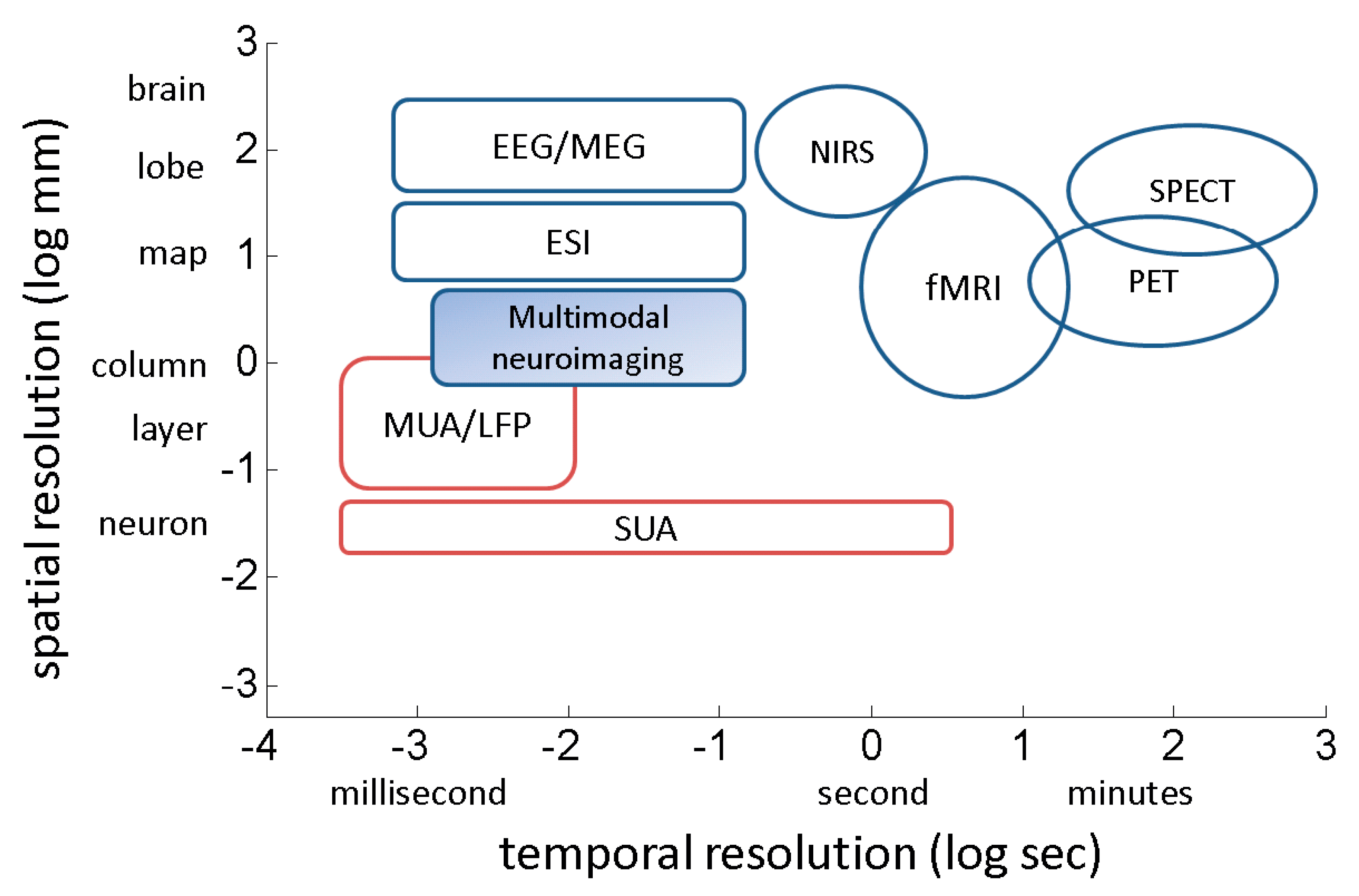
Figure 3.
Topographic organization of the primary motor (left) and sensory (right) cortex on representational coronal slices of the brain [33,34].
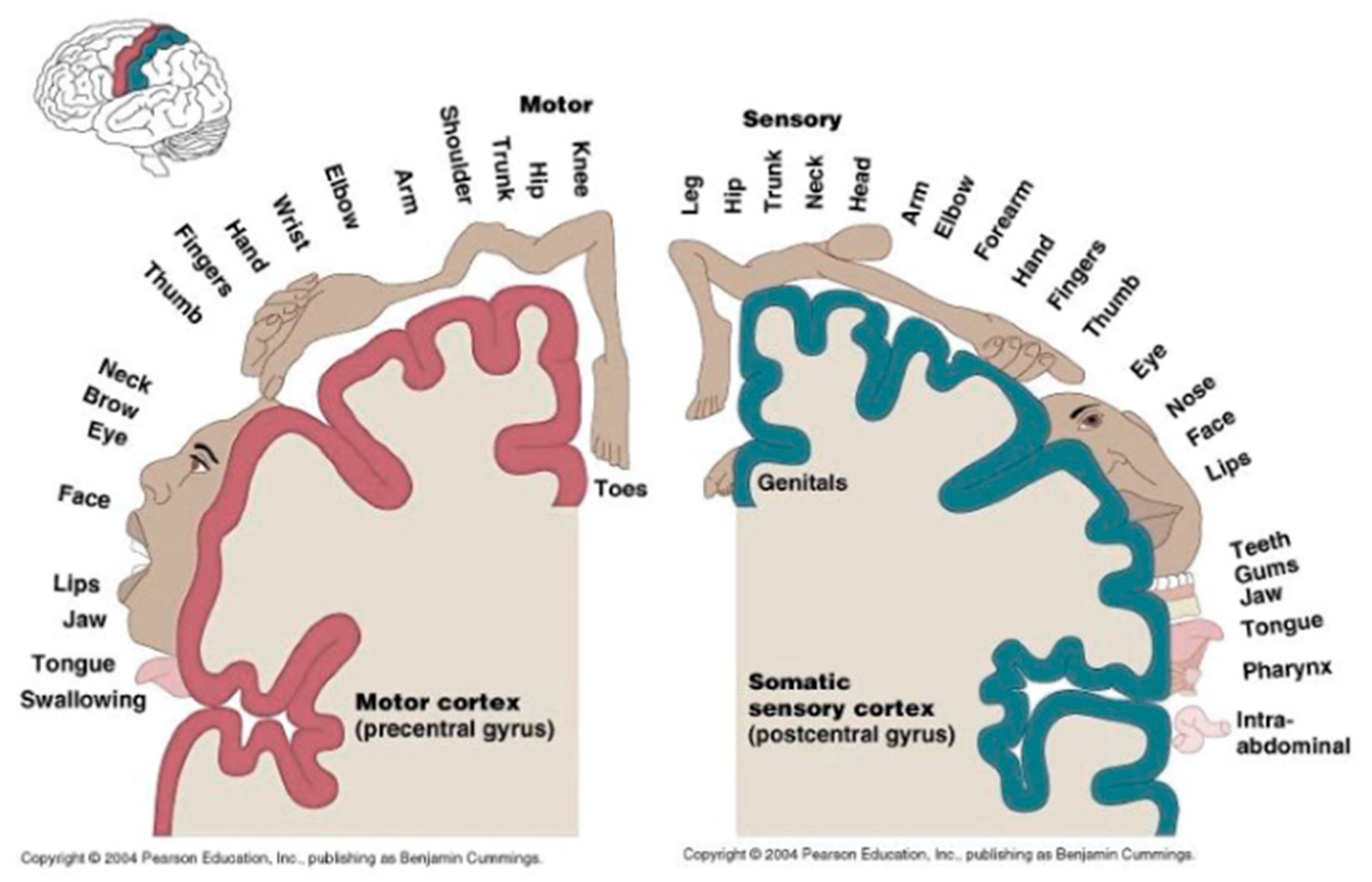
Figure 4.
The results of a meta-analysis depicting the activations and de-activations for specific meditation techniques; the colors refer to different meditation techniques. Red: focused attention; blue: open monitoring; green: mantra recitation; yellow: loving-kindness/compassion. The filled colored circles denote activations and those with a downward arrow denote de-activations. The region of interest (ROI) names abbreviated in the figure are as follows. DLPFC (dorsolateral prefrontal cortex), RLPFC (rostrolateral prefrontal cortex), PMC (premotor cortex), IPL (inferior parietal lobule), IFG (inferior frontal gyrus), Broca (Broca’s area), RMPFC (rostromedial prefrontal cortex), ACC (anterior cingulate cortex), dACC (dorsal ACC), SMA (supplementary motor area), PCC (posterior cingulate cortex), BG (basal ganglia), SII (secondary somatosensory cortices), aIns (anterior insula), mIns (mid-insula) [42].
Figure 4.
The results of a meta-analysis depicting the activations and de-activations for specific meditation techniques; the colors refer to different meditation techniques. Red: focused attention; blue: open monitoring; green: mantra recitation; yellow: loving-kindness/compassion. The filled colored circles denote activations and those with a downward arrow denote de-activations. The region of interest (ROI) names abbreviated in the figure are as follows. DLPFC (dorsolateral prefrontal cortex), RLPFC (rostrolateral prefrontal cortex), PMC (premotor cortex), IPL (inferior parietal lobule), IFG (inferior frontal gyrus), Broca (Broca’s area), RMPFC (rostromedial prefrontal cortex), ACC (anterior cingulate cortex), dACC (dorsal ACC), SMA (supplementary motor area), PCC (posterior cingulate cortex), BG (basal ganglia), SII (secondary somatosensory cortices), aIns (anterior insula), mIns (mid-insula) [42].
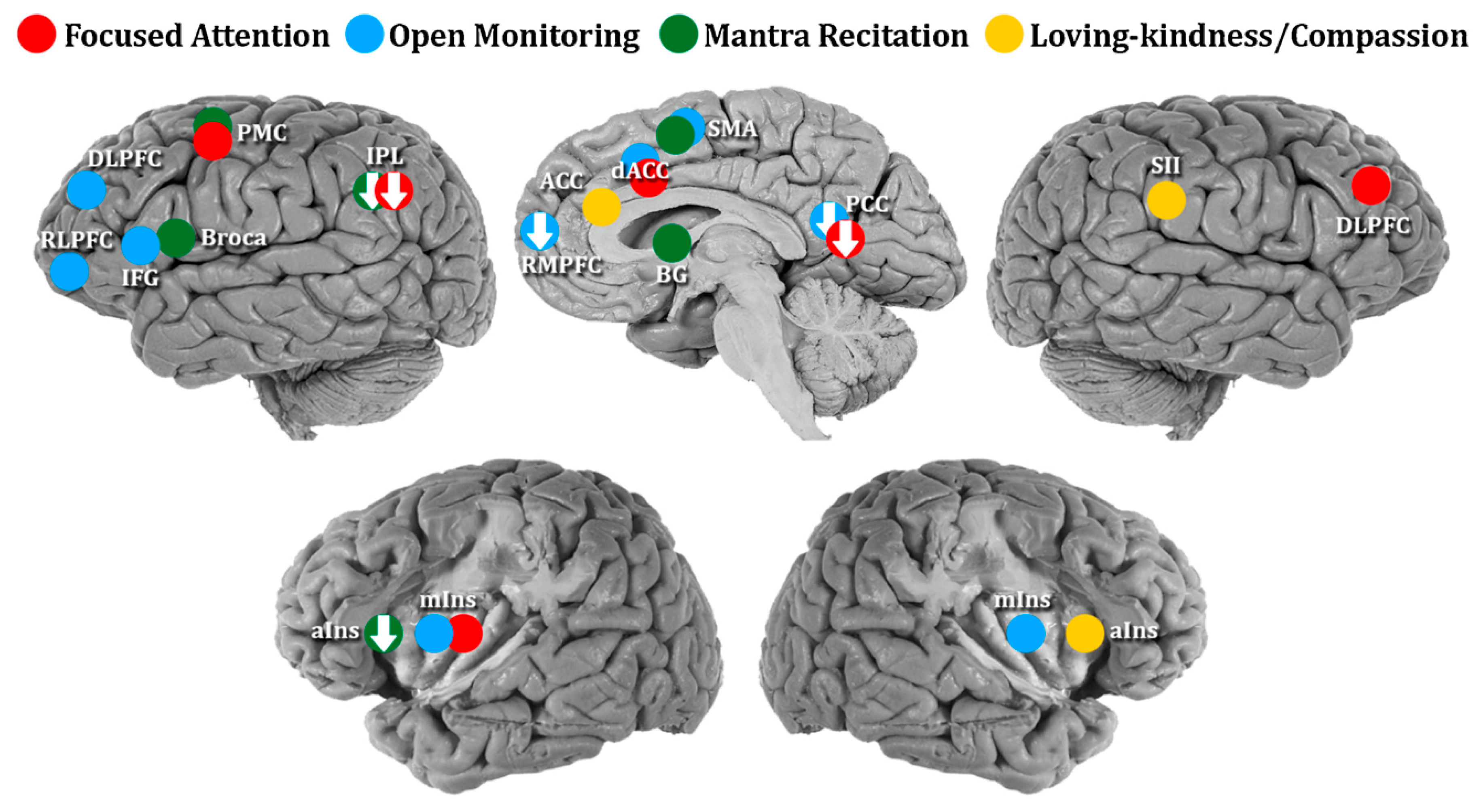
Figure 5.
Relationship between cortical gray matter thickness of the insula (a brain region) and the age of participants [53]. Meditation participants: blue circles; control participants: red squares.
Figure 5.
Relationship between cortical gray matter thickness of the insula (a brain region) and the age of participants [53]. Meditation participants: blue circles; control participants: red squares.
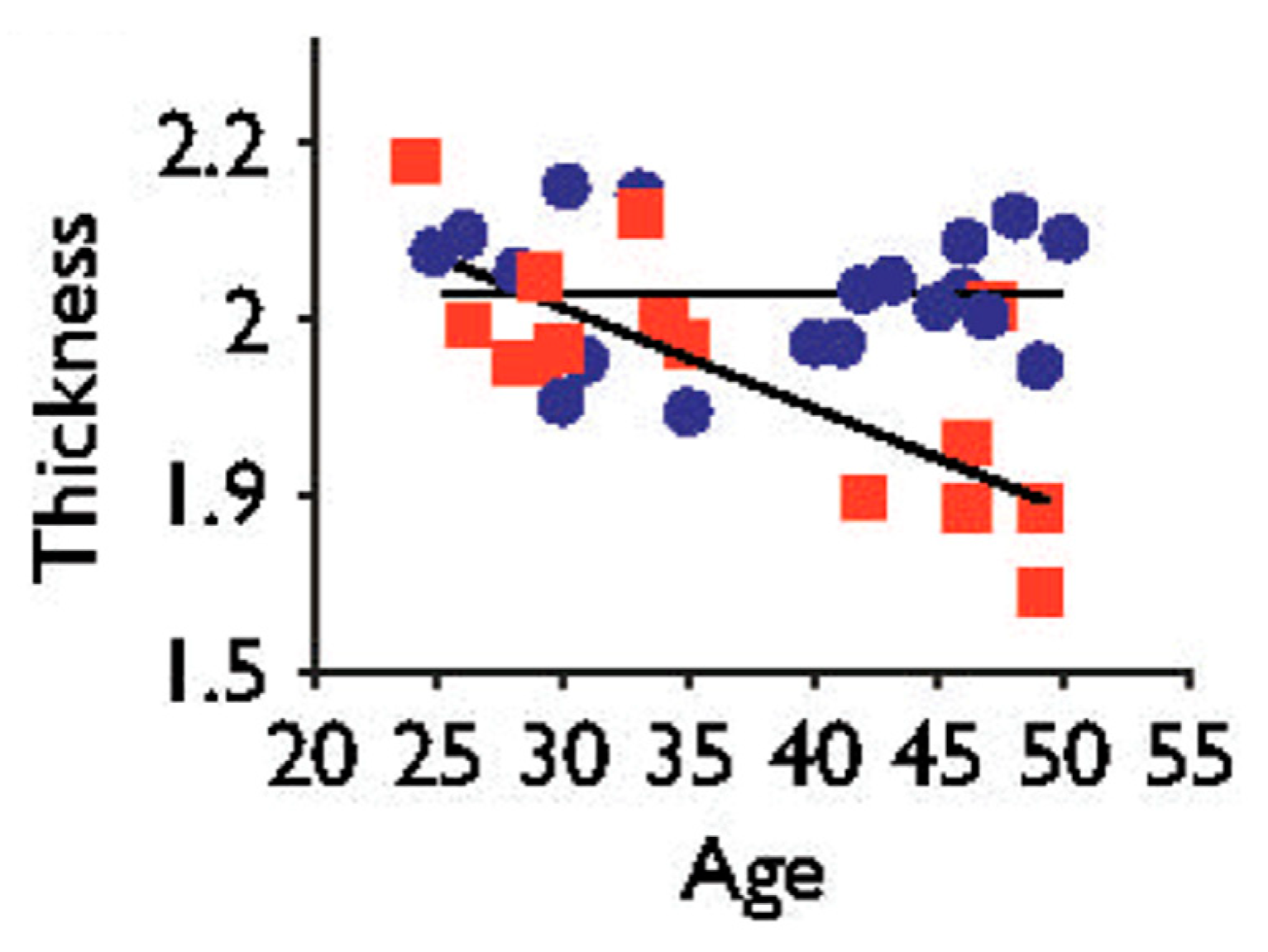
Figure 6.
Comparing an image drawn secretly by the investigator (top row) and those drawn after that by the mentalist (bottom-left) and a control subject (bottom-right) [65]. (A) Image drawn secretly for the mentalist; (B) image drawn secretly for the control subject; (C) image drawn by the mentalist; (D) image drawn by the control subject.
Figure 6.
Comparing an image drawn secretly by the investigator (top row) and those drawn after that by the mentalist (bottom-left) and a control subject (bottom-right) [65]. (A) Image drawn secretly for the mentalist; (B) image drawn secretly for the control subject; (C) image drawn by the mentalist; (D) image drawn by the control subject.
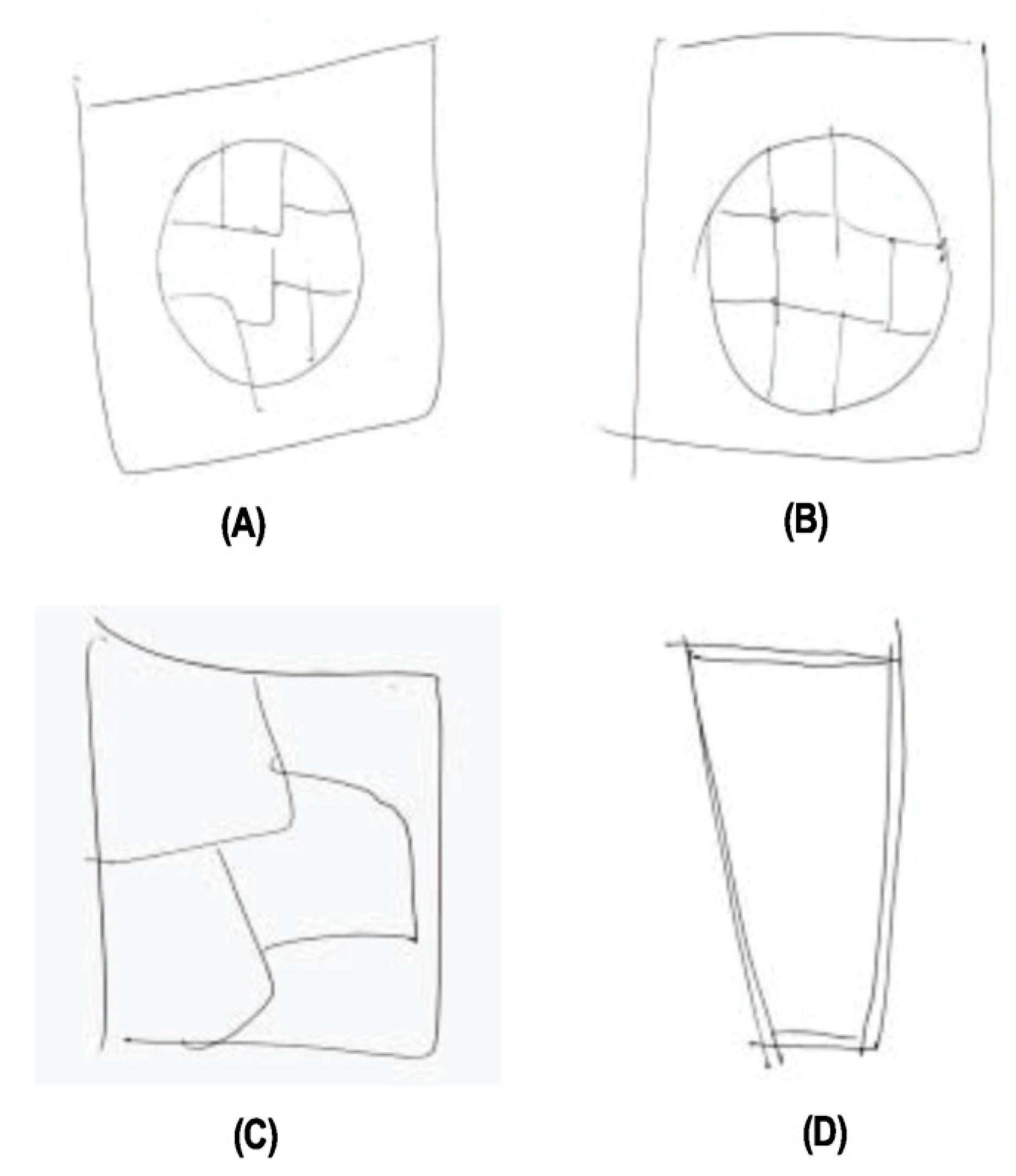
Figure 7.
The variation in responses to experiential probes for meditation depth, mind wandering, and sleepiness scores for expert and non-expert meditators [72].
Figure 7.
The variation in responses to experiential probes for meditation depth, mind wandering, and sleepiness scores for expert and non-expert meditators [72].
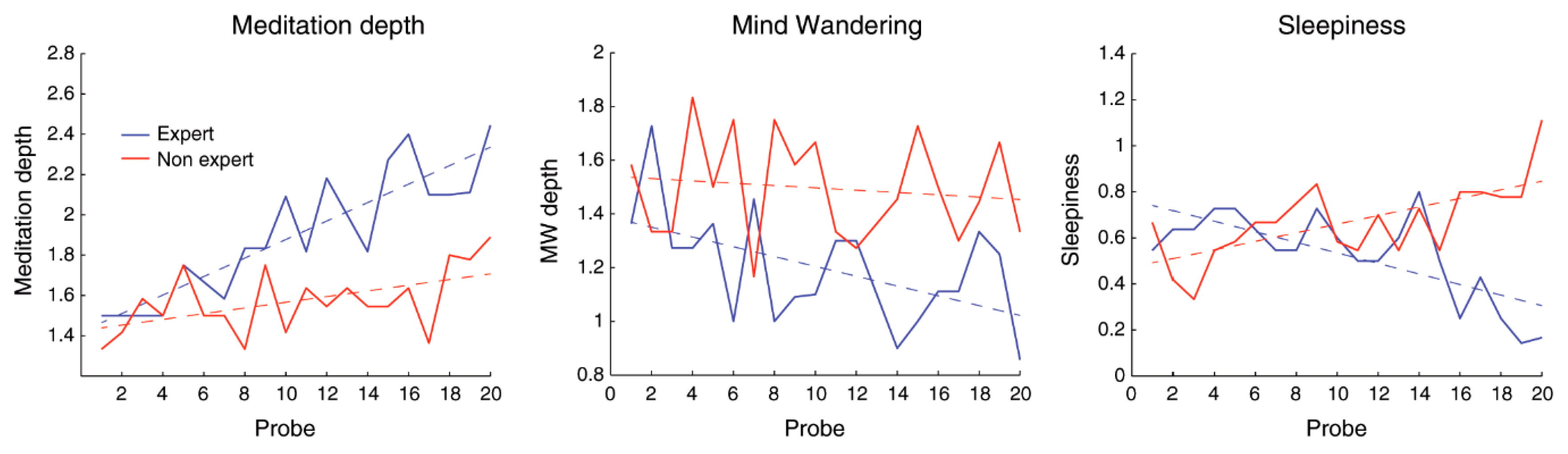
Figure 8.
Biological methods of mind-body therapies [122].
Figure 8.
Biological methods of mind-body therapies [122].
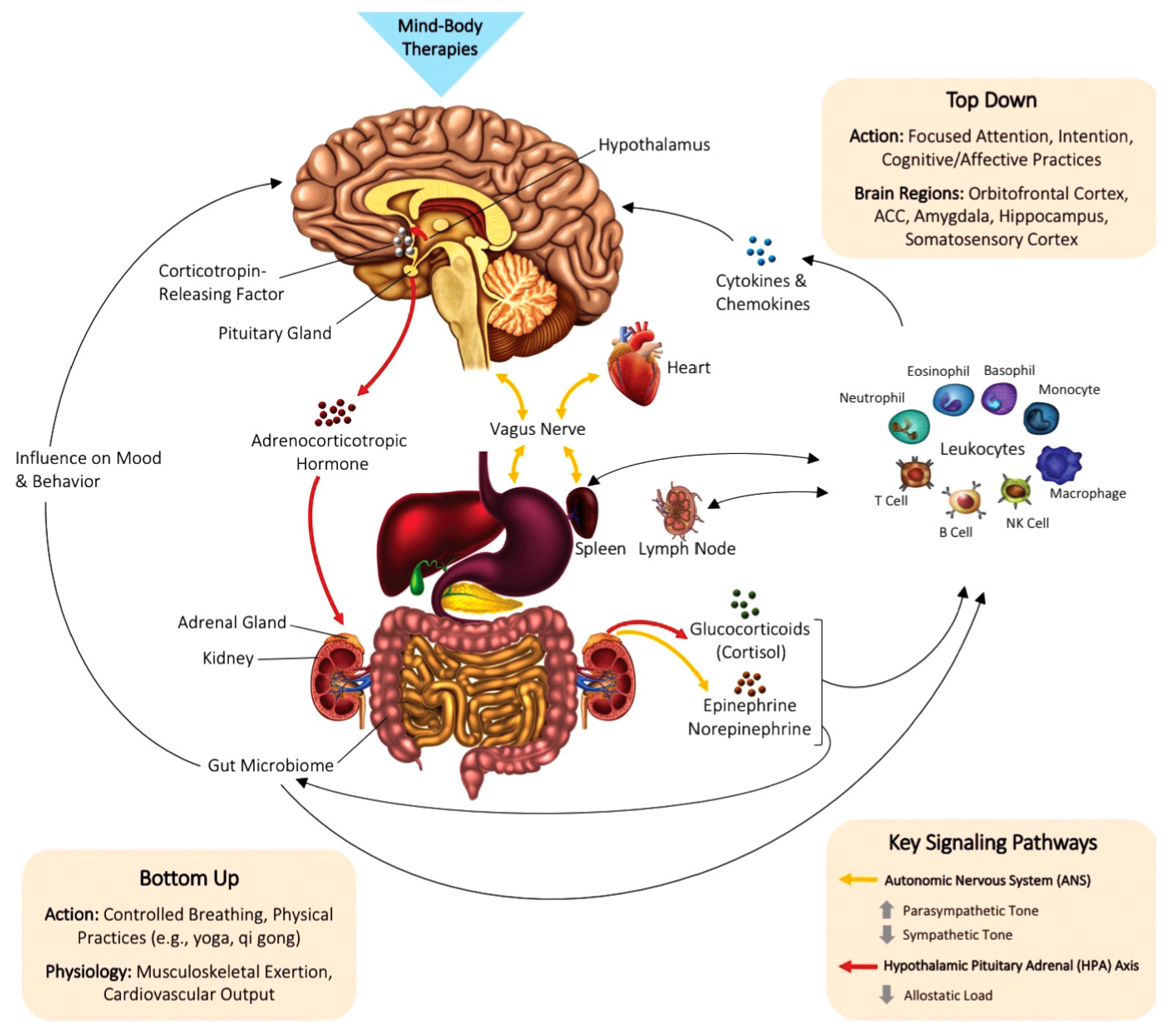
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



