
Submitted:
02 October 2024
Posted:
03 October 2024
You are already at the latest version
Abstract
Gastric pH seems to be a key factor for the development of Equine Gastric Ulcer Syndrome (EGUS). It is influenced by the amount and duration of roughage uptake, as chewing increases the production of alkaline saliva. The protone-pump-inhibitor omeprazole is currently recommended by the American College of Veterinary Internal Medicine/European College of Equine Internal Medicine (ACVIM/ECEIM) consensus statement for therapy of both Equine Squamous Gastric Disease (ESGD) and Equine Glandular Gastric Disease (EGGD). We hypothesized that dental disorders decrease saliva production due to altered chewing and in consequence gastric pH, therefore predisposing horses to EGUS. In 54 horses, a gastroscopy with measurement of the intragastric pH after 12 hours of fasting and an examination of the oral cavity were carried out. Omeprazole therapy was recommended (n=32), dental disorders were corrected (n=22) and gastroscopy was repeated 4 weeks later (n=9). No influence of moderate-severe dental disorders on ESGD (grade ≥2/4) (p = 0.394) and EGGD (grade ≥2/3) (p = 0.857) could be determined. Nevertheless, there was a trend that moderate- severe dental disorders were associated with a low gastric pH (1-4) (p = 0.100). In conclusion, we found no evidence that gastroscopy should be recommend in horses with dental disorders and vice versa.
Keywords:
equine gastric ulcer syndrome
; omeprazole
; dental disorders
; horse
; pH
1. Introduction
Gastric ulcers in horses (equine gastric ulcer syndrome - EGUS) include disease of the squamous (equine squamous gastric disease - ESGD) and glandular mucosa (equine glandular gastric disease - EGGD) [1].
Gastroscopy is the only method to definitively identify gastric ulcers ante mortem [4]. Scoring systems have been developed to evaluate changes in the gastric mucosa. According to international consensus, a system from 0 (intact epithelium and no hyperkeratosis) to 4 (extensive lesions with deep ulcerating areas) exists for the cutaneous mucosa [1].
Even though the Consensus Statement [1] deliberately refrained from using a scoring system for EGGD, as visual findings correlate significantly less well with clinical signs and prognosis, scoring systems can be useful in the context of scientific studies and for assessing the course of treatment. Scoring systems with various subgrades were therefore also designed to assess the glandular mucosa [3,5,6]. EGGD and ESGD can occur simultaneously, but there is currently no clear association between the presence of the two diseases [4].
Pathophysiological responsibility for ESGD lies in management factors that increase the acid exposure of the squamous mucosa. The sensitivity of the squamous mucosa to hydrochloric acid and volatile fatty acids is pH-, time- and dose-dependent. After the initial damage caused by the acid, diffusion into the stratum spinosum leads to ulceration. By-products of bacterial fermentation of carbohydrates exacerbate the damage caused by hydrochloric acid. Dietary fiber probably has a dual role in the pathogenesis of ESGD, firstly by increasing saliva production during chewing, which has a buffering effect on gastric acid, and secondly by allowing a “roughage ball” to form in the stomach, which limits the distribution of acid [7].
In contrast to the squamous mucosa, the glandular mucosa has a number of protective factors as it is constantly exposed to hydrochloric acid [8]. The pathophysiology of glandular gastritis is not yet sufficiently understood. Factors that presumably contribute to EGGD are the breakdown of mucosal defenses, bacterial colonization, stress and inflammation [8], so that the mucosa is then no longer sufficiently protected against acid exposure. A low pH can therefore have a negative effect on both the squamous and glandular gastric mucosa and is therefore a very central factor in the pathogenesis of ESGD and EGGD.
Oral omeprazole (buffered or enteric-coated) is licensed for the treatment of gastric ulceration in many countries and is an effective agent for the management of ESGD [9,10]. A long-acting intramuscular formulation administered at a dose of 4 mg/kg every 5-7 days has been shown to be highly effective in the treatment of ESGD [11], but it does not hold a veterinary license. One study showed that 97% of horses treated with this intramuscular formulation were cured within four weeks, compared to 67% of horses treated with oral omeprazole paste [12]. In the case of EGGD, there were also better cure rates in one study after four weeks with injection (82%) compared to oral omeprazole therapy (50%) [13]. For the treatment of EGGD, a combination therapy of omeprazole at a dosage of 4 mg/kg PO SID and sucralfate at a dosage of 12 mg/kg PO BID is a valid first-line treatment [14], although the effect has not been clearly proven [15].
The prevalence of ESGD varies greatly depending on exercise, training condition, breed, sex and age and can range from 11% to 100% [16]. The prevalence of EGGD varies between 6% and 72% depending on the population in the publication [7].
The pH in the ventral stomach of adult horses is around 2.9 due to the constant secretion of acid. In contrast, the pH in the dorsal stomach is less acidic (mean pH: 6.8), but is subject to strong fluctuations, presumably due to feeding behavior. During the day, horses have a significantly higher pH in the dorsal stomach. In newborn foals, the pH is very variable (mean pH: 5.5). The squamous mucosa is thin at birth and presumably becomes thicker as an adaptation to the increased acid exposure [4].
The literature shows that slow and prolonged feed intake leads to a continuous flow of saliva and thus to a better buffering capacity in the stomach [17]. If horses are fasted, the pH in the stomach decreases [18]. One study showed that fasted horses had low-grade lesions in the cutaneous mucosa near the margo plicatus at the small and large curvature of the stomach [19].
Dental problems are the third or fourth most common reason owners present their horses for veterinary treatment in the USA [20]. Dental lesions are thought to lead to inefficient mastication resulting in reduced feed conversion and weight loss, increased risk of intraluminal oesophageal obstruction and intestinal obstruction and occasionally diarrhea [21].
Some studies have shown high levels of clinically significant, non-diagnosed dental disorders in horses [22,23]. Due to oral pain, some horses may also chew very slowly and may be reluctant to eat hay or silage (haylage). In extreme cases, feed intake is reduced, but most horses with dental-related pain will just spend longer eating, including re-eating “quidded” food (small boluses of partially masticated food falling from the mouth during chewing). The most common equine dental (and oral) disease is the development of sharp dental overgrowths and may cause lacerations of the cheeks and tongue during chewing [24].
Floating (rasping or filing) of the teeth is still the most frequently performed dental procedure. Dental floatation in horses is often performed to maintain symmetry and balance of the dental arcades and allow a free elliptical chewing motion that improves feed efficiency. It is further intended to relieve discomfort associated with soft tissue injuries caused by dental lesions and to avoid discomfort associated with the presence of a bit in the mouth [21].
Removing mechanical impediments to lateral chewing movements and painful dental overgrowth promotes normal chewing movements and helps restore normal oral food and saliva flow. The aim of routine dental care should be to prevent the development of such end-stages by regular dental inspections every 6-12 months [24]However, some authors are critical of excessive smoothing of the molar occlusal surface, as this ‘overcorrection’ could restrict the ability to chew hay [25].Food packing in diastemata should be cleaned out. Smaller diastemata can tightly trap food, which can lead to painful periodontitis and gingival retraction and cause chewing problems. If there is very extensive food pocketing these diastemata can be mechanically widened [24].
Localised cement caries is very common within the infundibula and is generally innocuous. As horses’ infundibula have no nerve supply, caries affecting only the infundibular cementum does not cause pain. However, if the caries process penetrates the enamel and reaches the dentin, it is very likely that the disease will cause some pain or discomfort and the tooth can fracture [26]. Peripheral cemental caries is usually of little significance but it can involve deeper dental structures [24].
Despite the many studies that have been published on the subject of gastric ulcers in horses, none have so far investigated a connection with disorders of the oral cavity. In this orientation study, we investigated whether disorders in the oral cavity have an influence on the gastric pH and the gastroscopic findings.
2. Materials and Methods
2.1. Animals
This observational study included 54 horses of various age (2-28 years), sex (mares: 27, stallions: 1 and geldings: 26) and breed, which were presented for gastroscopy at the Equine Clinic Hochmoor, Germany, and had an oral cavity examination under the same sedation between September 2023 and April 2024. The horses had a history of recurrent colic, weight loss, loss of appetite, fecal water, exercise insufficiency or typical gastric discomfort behavior (bruxism, groaning and hypersensitivity/aggressive behavior to grooming, the rider’s leg or fastening the girth). Horses were fasted overnight for approximately 12 h feed and 3 h water withdrawl. Most of the patients were stabled in the clinic the day before the examination and were given standardized hay or were already in the clinic due to colic therapy. Some horses were presented as ambulatory patients and fasted at home. Nine of the horses with obvious findings in the stomach were presented again for a control gastroscopy after treatment with omeprazole and two of them with additional dental treatment.
2.2. Gastroscopic Examination
The horses were sedated intravenously with 0.012 mg/kg bw detomidine (Domidine™ 10 mg/ml, Dechra Veterinary Products Deutschland GmbH) and 0.025 mg/kg bw butorphanol 0.025 mg/kg (Torbugesic™ VET 10 mg/ml, Zoetis Deutschland GmbH). For the gastroscopy a flexible endoscope of 330cm length and 1,3cm diameter (Karl Storz GmbH, Germany) was used and the stomach was insufflated with air for complete visualization of relevant structures (margo plicatus, small curvature and pylorus). During gastroscopy, a few milliliters of the gastric fluid in the ventral stomach were aspirated through the working channel and the pH value was measured using pH test strips (pH-indicator strips, MColorpHastTM). Food material adhering to the stomach was flushed away with water afterwards. The gastric findings were recorded by two veterinarians (diplomate and resident ECEIM) and divided into grades using scoring systems (Table 1 and Table 2).
2.3. Oral Cavity Examination
After the gastroscopy, the oral cavity was examined by a veterinarian under the same sedation. The findings were documented and categorized into 4 grades depending on the degree of severity, summation and influence on the occlusion (Table 3 and supplementary material). Examples of high-grade abnormalities are a very smooth geriatric or rasped occlusal tooth surface or several missing teeth. In contrast, for example, a cribbing bite is only a low-grade finding, as it generally has no negative influence on the occlusion. Hooks, edges and other pathologies are subjectively categorized as low-, medium- or high-grade depending on the degree of severity.
2.4. Owner Questionnaire
The owners were given a questionnaire (the original questionnaire was prepared in German and is available in English in the supplements). In addition to general information about the horse, questions were asked about its keeping, feeding and use, as well as its medical history, behavioral problems and stress factors and of course, its dental treatment status, gastric health and any previous treatments.
In order to analyse the influence of confounders, in particular the previous gastric treatment with omeprazole and the previous dental treatments, these variables were recorded in the questionnaire. The aim of these surveys was to identify possible distortions in the results and to analyse their effects on the horses’ gastric pH.
2.5. Treatment
In the case of ESGD ≥ 2/4 and/or EGGD ≥ 2/3, omeprazole treatment according to the recommendations of the consensus statement (buffered formulation, Gastrogard™, Boehringer Ingelheim Germany, 4mg/kg PO SID or 2mg/kg enteric coated granules, Equizol™, CP Pharma Germany, PO SID, both over 4 weeks) was recommended to the owners (overview of gastric/dental findings and recommended treatment for each horse in supplementary material). In addition, teeth were floated and diastases were cleaned. The patient owners were given management recommendations, such as avoiding long periods of food withdrawel and feeding concentrates after roughage. In order to monitor the success of the treatment, a control gastroscopy was recommended at the end of the therapy (about 4 weeks later).
2.6. Statistical Analysis
Clinical data were recorded in a digital patient documentation system (easyVET™, VetZ Gmbh, Isernhagen, Germany) and Microsoft Excel™. The statistical analysis included patients who also underwent an oral cavity examination following the gastroscopy. The IBM SPSS Statistics 29.0.1.0 program was used for the descriptive evaluation of the data, as well as statistical analyses and chart creation. A value of p < 0.05 was considered significant. The ESGD, EGGD and oral cavity score, as well as the gastric pH value, were combined into larger supergroups in order to increase the number of cases per group. The relationship between findings in the oral cavity and ESGD, EGGD and gastric pH was evaluated using a Chi square test. Logistic regression was applied to test whether higher grades of gastric disease (ESGD ≥ 2/4 and/or EGGD ≥ 2/3) was associated with low gastric pH values (≤4) and moderate to severe dental disorders (≥ 2/3). In addition, the confounders: pretreatment of the stomach with omeprazole within the week prior to gastroscopy (known from 6/48 participants) and time since last dental treatment (categorized as < 6 months (21/38), 6-12 months (12/38), > 12 months (5/38) known from 38 participants) were investigated.
3. Results
A majority of 55.6% (n = 30/54) of the horses had an ESGD grade ≥2/4 in the first examination and 17.0% (9/53) fully visible stomachs had an EGGD grade ≥2/3. The exact distribution is shown in Table 4. Therapy with omeprazole (Gastrogard™ or Equizol™) was recommended in 59.3% (32/54) of patients (supplementary material).
Moderate or severe findings in the oral cavity were initially seen in 48.1% (26/54). Of these, 19 and additionally the teeth of 3 horses with low grade findings were treated (table with individual findings in supplementary material). The gastric pH ranged between 1 and 9, with 40.4% (21/52) horses categorized in groups 1-4 and 59.6% (31/52) in groups 5-9 (Table 4). Gastric pH was not measured in 2/54 horses, as they had gastric lavage prior to gastroscopy. ESGD Scoring was performed in all horses (n=54), in one horse EGGD scoring was not possible, as the glandular mucosa was not suffiently visible (n=53).
34 out of 54 (63%) patient questionnaires were answered and could be used to find confounders.
The logistic regression showed that horses with moderate to severe dental disorders tend to have a gastric pH of ≤4 (p = 0.104; odds ratio [OR] = 2.571; 95% confidence interval [CI] 0.824-8.065) (Table 5). Including the confounder omeprazole pretreatment, the odds ratio increased (OR = 4.717; 95% CI 1.292-17.241) and it became significant (p = 0.019) (Figure 1). An association between dental disorders (moderate to severe) and ESGD (≥2/4) (p = 0.395; OR = 1.600, 95% Cl 0.542-4.726) was not clearly shown (Table 5). Including the confounders, the odds ratio increases and the p-value decreased, but there was still no significance (last dental treatment: OR = 2.513; 95% CI 0.552-11.432; p = 0.233; omeprazole pretreatment: OR = 2.671; CI 0.748-9.534; p = 0.130). No association was found for dental disorders (moderate to severe) and EGGD (≥2/3) (p = 0.857) (Table 5).
9 patients treated with omeprazole and 2 of those with correction of the dental disorders were presented for a control gastroscopy after approximately 4 weeks. ESGD was improved by at least 2 subgrades or achieved the grade 0 in 5/9 horses. Of patients with EGGD, 3 out of 8 fully visible stomachs showed a reduction of at least one subgrade (Table 6).
4. Discussion
To our knowledge, this study is the first to investigate a possible relation between oral cavity and gastric disease.
The majority horses showed at least grade 1/4 ESGD and at least grade 1/3 EGGD. Depending on breed and performance, EGUS prevalence between 37-100% for ESGD and from 6% to 72% for EGGD has been described [7]. Due to the wide range our results of 83% for ESGD and 59% for EGGD are consistent with this. As the horses in our study were examined after presenting typical clinical signs, these high prevalences are to be expected, although a former study in horses with a history of comparable clinical signs showed a lower ESGD and higher EGGD case rate [3].
A possible explanation might be that our study period from September to April excluded the summer season, which can lead to gastric ulcers in competition horses due to increased training and participation in competitions [27]. On the other hand, horses spend longer periods on pasture during the summer months, which can potentially lead to shorter feeding pauses.
In our study, ESGD was graded from 0 to 4 as previously recommended [1,2]. EGGD was graded from 0 to 3, modified from the Consensus Statement [1] and already used by Barton et al. [3]. The oral cavity score was developed based on the findings and the potential influence on function as described in the literature. In order to obtain a larger number of horses per group and therefore to increase the statistical power, the ESGD, EGGD and oral cavity score, as well as the fasted gastric pH, were combined into two supergroups and the statistical calculations were carried out with these. The division of the ESGD score into ≤ 1/4 and ≥ 2/4 was chosen because a score of 2/4 or higher can be considered clinically significant [28]. In case of EGGD, studies reported spontaneous healing of low grades [29], which is why the grades 0-1/3 and grades 2-3/3 framework was chosen. The classification of the gastric pH into 1-4 and 5-9 was chosen, as in various other studies the limit was also set at > 4 [30,31]. Furthermore, ESGD and/or EGGD ulcers have been shown to heal faster with an intragastric pH > 4[32]. The chosen group categorisation of the oral cavity resulted in a homogeneous distribution and divides the horses into those with unlikely influence (grades 0-1/3) and those with a likely influence on the chewing process (grades 2-3/3). We also assumed an impairment in case of multiple low-grade findings. However, as the categorisation was subjectively determined and moderate interobserver agreement may have occurred as formerly shown [3], this effect remained insignificant.
ESGD treatment was recommended starting at grade 2, as hyperkeratosis (grade 1) in the horse’s stomach may be considered as a “normal” reaction to acid exposure and as ESGD has also found in feral horses that are not exposed to any recognized risk factors [4,33]. In addition, many horses show no clinical signs despite ESGD findings and mild lesions can heal spontaneously [34,35].
Gastrogard™ is a buffered formulation which, according to the manufacturer’s instructions, is to be administered at a dosage of 4 mg/kg, while Equizol™ is available as enteric-coated granules and is recommended by the manufacturer at a dosage of 2 mg/kg due to its increased bioavailability [3].
There are variable study results on the healing and improvement rates of ESGD and EGGD with 4 weeks of omeprazole therapy, although the trend is the same. ESGD shows a better healing tendency than EGGD. We included horses treated with Equizol™ 2mg/kg and Gastrogard™ 4mg/kg, as former studies have shown no difference [3,15]. The Consensus Statement reports cure rates for Gastrogard™ of 78% for ESGD and 25% for EGGD. More recent studies [12,13,36] show, depending on the definition used, cure rates for omeprazole therapy of between 59% and 67% for ESGD and between 25% and 50% for EGGD. The patients who underwent gastroscopic follow-up in our study showed comparable cure rates, with 55.6% for ESGD and 37.5% for EGGD. The influence of dental treatment on the patients who were presented for repeat gastroscopy cannot be assessed due to the small number of cases.
According to Jenkins et al. [37], gastric acid secretion is significantly inhibited by omeprazole for 27 hours. In our study, we found that horses with poor oral cavity health and no recent omeprazole treatment (within one week prior to gastroscopy) had statistically lower gastric pH. Although oral cavity health showed a trend to have an influence on stomach pH, a relationship between oral cavity health and ESGD could not be clearly demonstrated. Similarly, omeprazole pretreatment had no significant effect on the correlation between oral cavity health and ESGD. No connection was seen between the oral cavity health and the EGGD-Score. Despite statistical evidence suggesting that the administration of omeprazole in the week prior to gastroscopy, combined with good oral cavity health, increases gastric pH, it seems more plausible that the observed significant results could be attributed to the implementation of a gastric-optimized stable management and feeding regime, rather than the administration of the relatively short-acting omeprazole.
A previous study showed that severe ESGD can be improved or even cured within 4 weeks without drug therapy by providing horses with roughage ad libitum and a small amount of a low-starch supplement. A predictable daily routine with a limited number of good care taking persons can contribute to lower stress levels and thus improve gastric health [38]. Another study has shown that periods of feeding breaks over 6 hours increase the risk of ESGD [28], as well as high starch intakes, because starch leads to an increased production of volatile fatty acids (VFAs), which reduce the integrity of the mucous membrane [39].
Additionally, the teeth of 22 horses (19 horses with medium to high grade findings and 3 with low grade findings at request of the patient’s owners) were treated. No treatment was carried out on the remaining patients with moderate to severe dental findings, as in the case of two horses with too smooth chewing surfaces or in the case of horses with only missing teeth. In addition, some owners decided to have the already planned dental treatments carried out by their own equine dentist.
In our study, the mean pH in stomach fluid was 4.81, which is higher than in other studies [40]. Especially when horses are fasting the pH should be lower, in one study it was 1.55 in fasting compared to 3.1 in fed horses [18]. A possible reason for high pH values measured in this study could be contamination with water or previous treatment with omeprazole. Some patients were starved at home, where implementation was not monitored, but a completely emptied stomach could be considered successfully fasted at gastroscopy.
The questionnaire was designed in a similar way to comparable studies [16] and was returned by 34/54 owners. Some questions were answered incompletely, sometimes because the horse had not been owned for long or because it was not known better. The reliability of other statements should also be treated with caution, as they were not checked further. For example, the indication of the last oral cavity examination, which was divided into the usual intervals [24], should not be given too much weight, as it does not necessarily mean that dental treatment was also carried out.
5. Conclusions
In conclusion, this study showed no influence of moderate to severe dental disorders on ESGD (≥2/4) and EGGD (≥2/3), although moderate to severe dental disorders tended to be associated with a low gastric pH (≤ 4). There is an increased chance for horses with no dental problems to have higher gastric pH. This is statistically significant in horses who have received previous administration of omeprazole (within the last week) is taken into account. However, this effect is more likely to be due to stomach-adapted stable management and feeding and not the shorter-acting omeprazole. There is no evidence that gastroscopy should be recommend in horses with dental disorders and vice versa. Further studies with a larger number of cases and a longer study period are required.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, A.B. and R.L.; methodology A.B. and R.L.; software IBM SPSS Statistics 29.0.1.0; formal analysis R.L. and R.M.; investigation R.L., C.W., F.T. and R.L.; data curation, R.L.; writing—original draft preparation, R.L.; writing—review and editing, A.B.; visualization, R.L.; supervision, A.B. and R.M.; project administration A.B. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Institutional Review Board Statement
Sampling of horses affected by gastric disease was not classified as animal experiments by the German State Office (Landesamt für Natur, Umwelt und Verbraucherschutz Nordrhein-Westfalen (LANUV), Az 2023-0030540). The owners gave written informed consent to involve their horses in the study
Informed Consent Statement
Not applicable
Data Availability Statement
Data is contained within the article or supplementary material, further inquiries can be directed to the corresponding author/s.
Conflicts of Interest
The authors declare no conflicts of interest
References
- Sykes, B.W.; Hewetson, M.; Hepburn, R.J.; Luthersson, N.; Tamzali, Y. European College of Equine Internal Medicine Consensus Statement--Equine Gastric Ulcer Syndrome in Adult Horses. J Vet Intern Med 2015, 29, 1288–1299. [Google Scholar] [CrossRef]
- Andrews, F.; Bernard, W.; Byars, D.; Cohen, N.; Divers, T.; MacAllister, C.; McGladdery, A.; Merritt, A.; Murray, M.; Orsini, J.; et al. Recommendations for the diagnosis and treatment of equine gastric ulcer syndrome (EGUS): The Equine Gastric Ulcer Council. Equine Veterinary Education 1999, 11, 262–272. [Google Scholar] [CrossRef]
- Barton, A.K.; Trachsel, D.; Merle, R.; Gehlen, H. Vergleich des Therapieerfolgs zweier Omeprazolpräparate und Übereinstimmung zwischen zwei Untersuchern beim Equinen Gastric Ulcer Syndrome (EGUS). Pferdeheilkunde 2022, 38, 118–126. [Google Scholar] [CrossRef]
- Hewetson, M.; Tallon, R. Equine Squamous Gastric Disease: Prevalence, Impact and Management. Vet Med (Auckl) 2021, 12, 381–399. [Google Scholar] [CrossRef]
- Tallon, R.; Hewetson, M. Inter-observer variability of two grading systems for equine glandular gastric disease. Equine Vet J 2021, 53, 495–502. [Google Scholar] [CrossRef]
- Vondran, S.; Venner, M.; Vervuert, I. Effects of two alfalfa preparations with different particle sizes on the gastric mucosa in weanlings: alfalfa chaff versus alfalfa pellets. BMC Vet Res 2016, 12, 110. [Google Scholar] [CrossRef]
- Vokes, J.; Lovett, A.; Sykes, B. Equine Gastric Ulcer Syndrome: An Update on Current Knowledge. Animals (Basel) 2023, 13. [Google Scholar] [CrossRef]
- Banse, H.E.; Andrews, F.M. Equine glandular gastric disease: prevalence, impact and management strategies. Vet Med (Auckl) 2019, 10, 69–76. [Google Scholar] [CrossRef]
- Sykes, B.W.; Underwood, C.; McGowan, C.M.; Mills, P.C. The effect of feeding on the pharmacokinetic variables of two commercially available formulations of omeprazole. J Vet Pharmacol Ther 2015, 38, 500–503. [Google Scholar] [CrossRef]
- Varley, G.; Bowen, I.M.; Habershon-Butcher, J.L.; Nicholls, V.; Hallowell, G.D. Misoprostol is superior to combined omeprazole-sucralfate for the treatment of equine gastric glandular disease. Equine Vet J 2019, 51, 575–580. [Google Scholar] [CrossRef]
- Sykes, B.W.; Kathawala, K.; Song, Y.; Garg, S.; Page, S.W.; Underwood, C.; Mills, P.C. Preliminary investigations into a novel, long-acting, injectable, intramuscular formulation of omeprazole in the horse. Equine Vet J 2017, 49, 795–801. [Google Scholar] [CrossRef]
- Gough, S.; Hallowell, G.; Rendle, D. A study investigating the treatment of equine squamous gastric disease with long-acting injectable or oral omeprazole. Vet Med Sci 2020, 6, 235–241. [Google Scholar] [CrossRef]
- Gough, S.; Hallowell, G.; Rendle, D. Evaluation of the treatment of equine glandular gastric disease with either long-acting-injectable or oral omeprazole. Vet Med Sci 2022, 8, 561–567. [Google Scholar] [CrossRef]
- Rendle, D.; Bowen, M.; Brazil, T.; Conwell, R.; Hallowell, G.; Hepburn, R.; Hewetson, M.; Sykes, B. Recommendations for the management of equine glandular gastric disease. UK-Vet Equine 2018, 2, 2–11. [Google Scholar] [CrossRef]
- Jung, F.B., R. Mäßige Therapieerfolge sowohl bei einer hochdosierten Therapie mit Omeprazol-Granulat (Equizol®) als auch bei der Kombinationstherapie aus Omeprazol-Paste (Gastrogard®) und Sucralfat (Sucrabest®) bei Pferden mit Equine Glandular Gastric Disease (EGGD). Pferdeheilkunde 2023, 39, 417–426. [Google Scholar] [CrossRef]
- Gehlen, H.; Prieß, A.; Doherr, M. Deutschlandweite multizentrische Untersuchung zur Ätiologie von Magenschleimhautläsionen beim Pferd. Pferdeheilkunde 2021, 37, 395–407. [Google Scholar]
- Andrews, F.M.; Buchanan, B.R.; Elliot, S.B.; Clariday, N.A.; Edwards, L.H. Gastric ulcers in horses. Journal of Animal Science 2005. [Google Scholar] [CrossRef]
- Murray, M.; Schusser, G. Measurement of 24-h gastric pH using an indwelling pH electrode in horses unfed, fed and treated with ranitidine. Equine veterinary journal 1993, 25, 417–421. [Google Scholar] [CrossRef]
- Husted, L.; Sanchez, L.C.; Baptiste, K.E.; Olsen, S.N. Effect of a feed/fast protocol on pH in the proximal equine stomach. Equine Vet J 2009, 41, 658–662. [Google Scholar] [CrossRef]
- Traub-Dargatz, J.; Salman, M.; Voss, J. Medical problems of adult horses, as ranked by equine practitioners. Journal of the American Veterinary Medical Association 1991, 198, 1745–1747. [Google Scholar] [CrossRef]
- Carmalt, J.L.; Townsend, H.G.G.; Allen, A.L. Effect of dental floating on the rostrocaudal mobility of the mandible of horses. Journal of the American Veterinary Medical Association 2003, 223, 666–669. [Google Scholar] [CrossRef]
- Brigham, E.J.; Duncanson, G.R. An equine postmortem dental study: 50 cases. Equine Veterinary Education 2000, 12, 59–62. [Google Scholar] [CrossRef]
- Kirkland, K.; Maretta, S.; Inoue, O.; Baker, G. Survey of equine dental disease and associated oral pathology. In Proceedings of the Proceedings of the 40th annual convention of the American Association of Equine Practitioners, 1994; pp. 119–120.
- Dixon, P.M.; Dacre, I. A review of equine dental disorders. The Veterinary Journal 2005, 169, 165–187. [Google Scholar] [CrossRef]
- Ralston, S.L.; Foster, D.L.; Divers, T.; Hintz, H.F. Effect of dental correction on feed digestibility in horses. Equine Veterinary Journal 2001, 33, 390–393. [Google Scholar] [CrossRef]
- du Toit, N. Clinical significance of equine cheek teeth infundibular caries. Veterinary Record 2017, 181, 233–234. [Google Scholar] [CrossRef]
- Pedersen, S.K.; Cribb, A.E.; Windeyer, M.C.; Read, E.K.; French, D.; Banse, H.E. Risk factors for equine glandular and squamous gastric disease in show jumping Warmbloods. Equine Vet J 2018, 50, 747–751. [Google Scholar] [CrossRef]
- Luthersson, N.; Nielsen, K.H.; Harris, P.; Parkin, T.D. Risk factors associated with equine gastric ulceration syndrome (EGUS) in 201 horses in Denmark. Equine Vet J 2009, 41, 625–630. [Google Scholar] [CrossRef]
- Sundra, T.; Kelty, E.; Rendle, D. Five- versus seven-day dosing intervals of extended-release injectable omeprazole in the treatment of equine squamous and glandular gastric disease. Equine Vet J 2024, 56, 51–58. [Google Scholar] [CrossRef]
- Merritt, A.M.; Sanchez, L.C.; Burrow, J.A.; Church, M.; Ludzia, S. Effect of GastroGard and three compounded oral omeprazole preparations on 24 h intragastric pH in gastrically cannulated mature horses. Equine Vet J 2003, 35, 691–695. [Google Scholar] [CrossRef]
- Sykes, B.W.; Underwood, C.; Mills, P.C. The effects of dose and diet on the pharmacodynamics of esomeprazole in the horse. Equine Vet J 2017, 49, 637–642. [Google Scholar] [CrossRef]
- Recknagel, S.; Abraham, G.; Regenthal, R.; Friebel, L.; Schusser, G.F. Intragastrale pH-Metrie während der Omeprazolbehandlung bei nüchternen und gefütterten Pferden. Pferdeheilkunde 2020, 36, 205–209. [Google Scholar] [CrossRef]
- Ward, S.; Sykes, B.W.; Brown, H.; Bishop, A.; Penaluna, L.A. A comparison of the prevalence of gastric ulceration in feral and domesticated horses in the UK. Equine Veterinary Education 2015, 27, 655–657. [Google Scholar] [CrossRef]
- Murray, M.J.; Grodinsky, C.; Anderson, C.W.; Radue, P.F.; Schmidt, G.R. Gastric ulcers in horses: a comparison of endoscopic findings in horses with and without clinical signs. Equine Vet J Suppl 1989, 68–72. [Google Scholar] [CrossRef]
- Murray, M.J.; Eichorn, E.S.; Jeffrey, S.C. Histological characteristics of induced acute peptic injury in equine gastric squamous epithelium. Equine Vet J 2001, 33, 554–560. [Google Scholar] [CrossRef]
- Sundra, T.; Gough, S.; Rossi, G.; Kelty, E.; Rendle, D. Comparison of oral esomeprazole and oral omeprazole in the treatment of equine squamous gastric disease. Equine Vet J 2023. [Google Scholar] [CrossRef]
- Jenkins, C.C.; Blackford, J.T.; Andrews, F.; Frazier, D.L.; Mattsson, H.; Olovsson, S.-G.; Peterson, A. Duration of antisecretory effects of oral omeprazole in horses with chronic gastric cannulae. Equine Veterinary Journal 1992, 24, 89–92. [Google Scholar] [CrossRef]
- Kranenburg, L.C.; van der Poel, S.H.; Warmelink, T.S.; van Doorn, D.A.; van den Boom, R. Changes in Management Lead to Improvement and Healing of Equine Squamous Gastric Disease. Animals (Basel) 2023, 13. [Google Scholar] [CrossRef]
- Andrews, F.M.; Buchanan, B.R.; Elliott, S.B.; Al Jassim, R.A.; McGowan, C.M.; Saxton, A.M. In vitro effects of hydrochloric and lactic acids on bioelectric properties of equine gastric squamous mucosa. Equine Vet J 2008, 40, 301–305. [Google Scholar] [CrossRef]
- Husted, L.; Sanchez, L.C.; Olsen, S.N.; Baptiste, K.E.; Merritt, A.M. Effect of paddock vs. stall housing on 24 hour gastric pH within the proximal and ventral equine stomach. Equine Vet J 2008, 40, 337–341. [Google Scholar] [CrossRef]
Figure 1.
Oral cavity findings in relation to gastric pH. The red marking indicates the division into the two groups for the statistical analysis. (A + B) Subdivision of oral cavity findings in horses that were pretreated with omeprazole within the week prior to the study (red) (B).
Figure 1.
Oral cavity findings in relation to gastric pH. The red marking indicates the division into the two groups for the statistical analysis. (A + B) Subdivision of oral cavity findings in horses that were pretreated with omeprazole within the week prior to the study (red) (B).
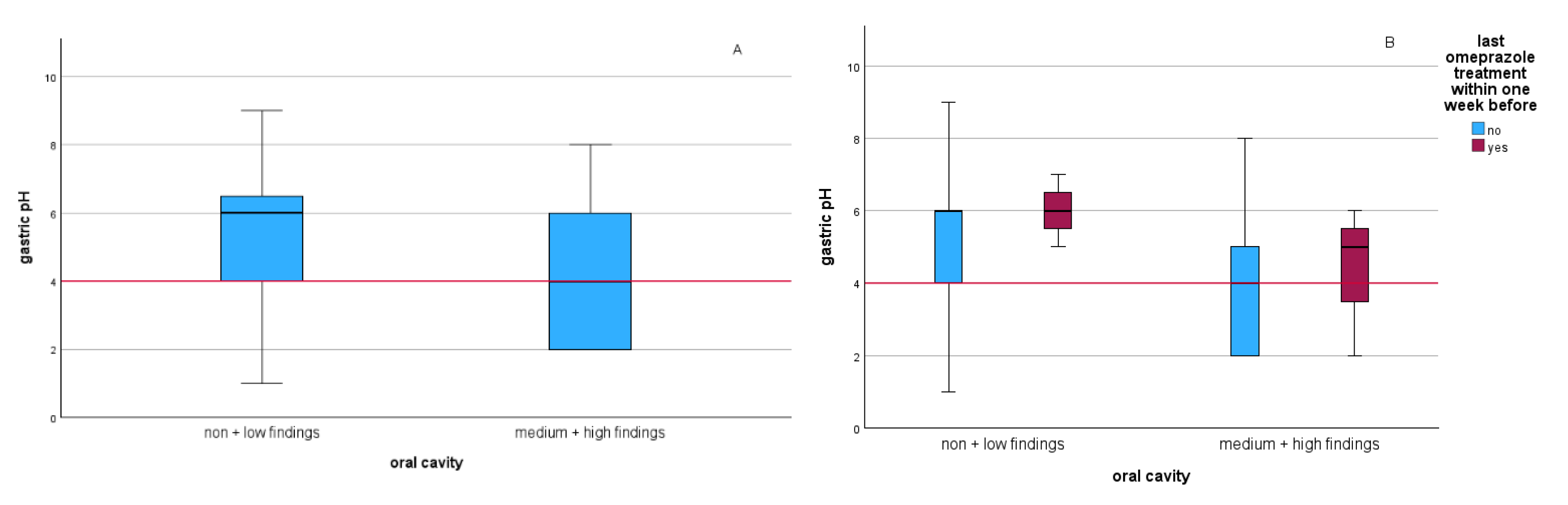

Table 1.
Grading system for equine squamous gastric disease (ESGD) from the ECEIM Consensus Statement (Skyes et al. 2015, adapted from Andrews et al. 1999a) [1,2]. The dotted line indicates the further division into supergroups.
| Grade | Squamous Mucosa |
|---|---|
| 0 | Intact epithelium and no appearance of hyperkeratosis |
| 1 | Intact mucosa, but areas of hyperkeratosis |
| 2 | Small, single or multifocal lesions |
| 3 | Large single or extensive superficial lesions |
| 4 | Extensive lesions with areas of apparent deep ulceration |
Table 2.
Grading system for equine glandular gastric disease (EGGD), modified from the ECEIM Consensus Statement (Sykes et al. 2015) [1] and Barton et al. 2022 [3]. The dotted line indicates the further division into supergroups.
| Grade | Glandular Mucosa |
|---|---|
| 0 | Intact mucosa |
| 1 | Intact mucosa, patchy or streaky yellowish or reddish lesions |
| 2 | Small, isolated or multifocal lesions |
| 3 | Large single or extensive superficial lesions, possibly bleeding |
Table 3.
Grading system for oral cavity health. The dotted line indicates the further division into supergroups. A score of grade ≥ 2/3 is labelled as moderate to severe dental/oral cavity disorders.
Table 3.
Grading system for oral cavity health. The dotted line indicates the further division into supergroups. A score of grade ≥ 2/3 is labelled as moderate to severe dental/oral cavity disorders.
| Grade | Oral Cavity |
|---|---|
| 0 (no findings) | No special findings |
| 1 (low findings) | ≤ 2 low-grade abnormalities |
| 2 (medium findings) | Medium-grade abnormalities or ≤ 4 low-grade abnormalities |
| 3 (high findings) | High-grade abnormalities or > 4 low-grade abnormalities |
Table 4.
Frequency of occurrence of the oral cavity and ESGD/EGGD scoring and gastric pH.
| Oral cavity Score | No. Horses (%, of 54) |
ESGD Score (0-4) |
No. Horses (%, of 54) |
EGGD Score (0-3) |
No. Horses (%, of 53) |
Gastric pH | No. Horses (%, of 52) |
|---|---|---|---|---|---|---|---|
| 1 | 1 (1.9) | ||||||
| 2 | 11 (21.2) | ||||||
| 0 | 8 (14.8) | 0 | 9 (16.7) | 0 | 22 (41.5) | 3 | 3 (5.8) |
| 1 | 20 (37.0) | 1 | 15 (27.8) | 1 | 22 (41.5) | 4 | 6 (11.5) |
| 2 | 17 (31.5) | 2 | 10 (18.5) | 2 | 8 (15.1) | 5 | 9 (17.3) |
| 3 | 9 (16.7) | 3 | 16 (29.6) | 3 | 1 (1.9) | 6 | 12 (23.1) |
| 4 | 4 (7.4) | 7 | 4 (7.7) | ||||
| 8 | 5 (9.6) | ||||||
| 9 | 1 (1.9) |
Table 5.
Relationship between oral cavity findings (non specific – low or moderate – severe) and gastric pH, ESGD and EGGD score with significance value determined by Chi² test.
Table 5.
Relationship between oral cavity findings (non specific – low or moderate – severe) and gastric pH, ESGD and EGGD score with significance value determined by Chi² test.
| Non specific – mild dental disorders | Moderate – severe dental disorders | p value (Chi² test) | |
|---|---|---|---|
| pH 1-4 | 8/21 (38.1%) | 13/21 (61.9%) | 0.100 |
| pH 5-9 | 19/31 (61.3%) | 12/31 (38.7%) | |
| ESGD ≤ 1/4 | 14/24 (58.3%) | 10/24 (41.7%) | 0.394 |
| ESGD ≥ 2/4 | 14/30 (46.7%) | 16/30 (53.3%) | |
| EGGD ≤ 1/3 | 23/44 (52.3%) | 21/44 (47.7%) | 0.857 |
| EGGD ≥ 2/3 | 5/9 (55.6%) | 4/9 (44.4%) |
Table 6.
ESGD and EGGD Scores before (first examination) and after omeprazol treatment (second (third) examination) in the 9 horses, presented for follow-up examination.
Table 6.
ESGD and EGGD Scores before (first examination) and after omeprazol treatment (second (third) examination) in the 9 horses, presented for follow-up examination.
| First Examination | Second (Third) Examination | |||
|---|---|---|---|---|
| Horse ID | ESGD (0-4) | EGGD (0-3) | ESGD (0-4) | EGGD (0-3) |
| 2* g | 4 | 2 | 1** | n.a. |
| 5 g | 3 | 3 | 2 | 1*** |
| 15 g | 3 | 1 | 0** | 0*** |
| 25 e | 3 | 1 | 0** | 1 |
| 32 g | 4 | 0 | 4 (2**) | 0 (0) |
| 34 e | 4 | 1 | 2** | 1 |
| 35* e | 3 | 1 | 2 | 1 |
| 39 g | 3 | 1 | 0** | 1 |
| 50 e | 3 | 2 | 3 | 1*** |
In 2 patients, the teeth were treated in addition to the omeprazole therapy (*). The stomachs were treated with Gastrogard™ (g) or Equizol™ (e). ESGD was improved ≥2 subgrades or achieving grade 0 in 5/9 horses (**) and EGGD was improved ≥1 subgrade in 3/8 horses (***). In one patient, the glandular mucosa of the stomach could not be fully visualized in the follow-up examination (?).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



