
Submitted:
01 October 2024
Posted:
02 October 2024
You are already at the latest version
Abstract
Background and Objectives: Kidney transplantation is the preferred treatment for children with end-stage renal disease (ESRD), but its outcome can be affected by urological complications, with incidence rates of 1%-27%. The aim of this study was to evaluate the occurrence of urological complications and their management in a cohort of pediatric kidney transplant recipients. Materials and Methods: A retrospective analysis on 178 patients undergone to renal transplantation at our Pediatric Kidney Transplant Center between 2011 and 2023 was conducted. Demographic and clinical data were analyzed. Urological complications were categorized as early, intermediate, or late based on their onset time. Results: Out of 178 patients, 28 (15.7%) experienced urological complications. Most patients (61%) had a pre-existing uropathy. Early complications (7-30 days) were all obstructive, namely ureterovesical junction obstruction and perirenal collections. Intermediate complications (1-3 months) comprised ureteral stenosis, symptomatic vesicoureteral reflux (VUR), and obstructive lymphocele. Late complications (>3 months) included symptomatic VUR and ureteral stenosis, with one case leading to ureteral rupture. Early complications were often detected due to acute graft dysfunction, while late ones were mainly identified during routine clinical, laboratory, or ultrasound follow-up. Urological complications requiring surgical or endoscopic therapy were 13.4%. Most ureteral stenoses were treated with initial endoscopic stents, followed by definitive surgery. VUR was treated with endoscopic correction with a high success rate (75%), while open surgery was reserved for cases where initial treatments failed, or complications recurred. No clear correlations were found between patient characteristics and risk of urological complication. Urological complications required multiple diagnostic procedures and therapeutic interventions (+2.5 admissions in mean and approximately +24,000 euros) compared to an uncomplicated post-transplant course. However, they did not significantly impact transplant outcomes, with a graft survival rate comparable to the control group. Conclusions: Regular post-transplant follow-up is crucial, especially for patients with known risk factors, to allow timely detection and treatment of urological complications, avoiding detrimental effects on graft function and improving transplantation outcomes.
Keywords:
kidney transplantation
; pediatric
; urological complication
; ureteral stricture
; vesicoureteral reflux
; endoscopic surgery
1. Introduction
Kidney transplantation has emerged as the leading treatment for children with end-stage renal disease (ESRD) due to its superior outcomes, cost-effectiveness, and lower mortality rates compared to dialysis [1]. Over the years, advancements in immunosuppressive therapy and transplant surgical techniques have improved graft survival rates. However, long-term success can be hindered by several complications arising from episodes of rejection, severe infections, or relapsing underlying disease. Additionally, urological complications can have adverse effects on the function, survival, and general well-being of both the patient and the graft.
The most common urological complications reported in the literature include ureteral obstruction, vesicoureteral reflux (VUR), either asymptomatic or complicated by urinary tract infections (UTI), anastomotic leakage and/or urinary extravasation, and lymphocele [2]. Urological complications can be immediate (as urine leaks or lymphoceles) or delayed (as ureteral strictures, symptomatic VUR, urolithiasis, or recurrent UTI), and may often require surgical intervention or multiple procedures. Therefore, promptly identifying and diagnosing urological complications is essential for optimizing graft function [3].
Ureteral stenosis represents the most common post-transplant complication and can be intrinsic (nephrolithiasis, recurrent urinary tract infections, BK virus infection) or extrinsic (lymphocele, hematoma). It should be suspected in patients with newly onset hydronephrosis not otherwise explained, with or without worsening of renal function, and requires surgical correction (such as ureteral stenting, endoscopic dilation/incision, ureterovesical re-anastomosis, ureteroureterostomy, pyeloureterostomy or ureteral replacement) in most cases [4].
VUR is among the most frequent late complications and is primarily characterized by recurrent urinary infections, which can lead to a decline in graft function [5]. It may be suspected in symptomatic patients with ultrasound findings of hydronephrosis, but confirmation diagnosis is obtained through voiding cystourethrography. Current management of VUR is based on endoscopic injecting of bulking agents, such as dextranomer-hyaluronic acid (DX-HA, Deflux®) or polydimethylsiloxane (Macroplastique®) and secondarily on a surgical approach [6].
Fluid collections, such as urinomas, seromas, and lymphoceles, may be paucisymptomatic or may compress the graft with potential kidney dysfunction. Therefore, if smaller collections can be monitored, larger symptomatic ones require surgical drainage [7].
Urolithiasis is a rare, delayed complication following kidney transplantation and can clinically manifest with non-specific abdominal pain, macroscopic hematuria, impaired renal function, urinary infections, or hydronephrosis [8]. Several risk factors have been recognized, such as urinary stasis due to ureteral obstruction or metabolic abnormalities including secondary hyperparathyroidism, recurrent urinary infections, cyclosporine-induced hyperuricemia, or calcineurin-inhibitors induced hyperoxaluria or hypocitraturia [9]. Generally, the conventional techniques employed for native stone disease (such as extracorporeal shock wave lithotripsy, retrograde ureteroscopy, and antegrade percutaneous endoscopy) can be safely applied to graft urolithiasis [10].
Data regarding urological complications in pediatric kidney transplant recipients are very limited compared to the adult population, therefore it is hard to obtain definitive incidence rates for each complication and to define risk factors [11]. Several studies on adults identified male gender, delayed graft function, abnormal pre-transplant voiding cystourethrogram (VCUG), repeat transplantation, obesity, multiple donor arteries, and atrophic bladder as predisposing conditions for urological complications after transplantation [12,13]. Posterior urethral valves appeared to be a risk factor for ureteral obstruction, possibly due to pre-transplant bladder ischemia, thickness, and collagen remodeling [14]. Additionally, atrophic bladder has been linked to a heightened risk of urological complications. [13]. In a retrospective study on pediatric kidney transplant recipients, a weight at the time of transplantation of less than 15 kg and a history of previous abdominal surgery emerged as risk factors for the development of intra-abdominal collections after transplantation [7].
The objective of this study was to evaluate the occurrence of urological complications and their management in a cohort of pediatric patients who underwent renal transplantation at our Center from 2011 to 2023. The secondary endpoint was to identify potential risk factors in order to develop a clinical-instrumental approach for early diagnosis and treatment.
2. Patients and Methods
We conducted a retrospective analysis of 178 patients who underwent renal transplantation at our Paediatric Kidney Transplant Center between January 2011 and April 2023. Post-operative urological complications included in the evaluation comprised ureteral or ureterovesical obstruction (both intrinsic and extrinsic) and VUR complicated by UTI, lymphocele, nephrolithiasis, new-onset bladder dysfunction, vesical lesions, and ureteral rupture. (Figure 1).
Based on the time of onset, urological complications were classified as early (occurring between 7 days and 1-month post-transplantation), intermediate (occurring between 1 and 3 months post-transplantation), and late (occurring more than 3 months post-transplantation).
Demographic data, including age, gender, cause of ESRD, donor source (deceased or living), history of previous kidney transplants, type and duration of previous renal replacement therapy, previous abdominal surgery, and surgical details (such as mean ureteral tube dwell time) were recorded. The mean follow-up was 65 months (range 4-150 months). Follow-up was considered concluded upon the resumption of renal replacement therapy in case of graft failure.
According to our practice, a trans-anastomotic external stent is inserted up to the renal pelvis, and a urinary catheter is placed during transplantation intervention. In a functioning graft, the ureteral tube is removed on day 7th and the vesical catheter on day 8th after transplantation. Dwelling time is prolonged until functional recovery in case of delayed graft function or upon specific clinical indications (e.g., the vesical catheter is maintained if vesical re-cycling is indicated by the Pediatric Urologist). Post-transplant suspected urological complications are initially assessed using conventional ultrasonography. Depending on the clinical and ultrasound findings, additional diagnostic investigations are employed as appropriate, including sequential renal scintigraphy with 99mTc-MAG3 in case of suspected obstruction, and VCUG for the evaluation of possible VUR. Further investigations, such as antegrade pyelography following percutaneous nephrostomy, retrograde ureteropyelography post-cystoscopy, abdominal computed tomography (CT), and magnetic resonance urography (MR urography) are performed according to the indications of the Pediatric Urologist. In cases of obstructive perirenal fluid collections, fluid analysis is performed as needed. Furthermore, patients who develop ureteral or ureterovesical stenosis are investigated for BK virus infection by BK virus-DNA testing in urine, blood, and renal and/or ureteral biopsy. UTI diagnosis is defined based on fever and/or abdominal pain accompanied by the presence of more than 10^5 colonies per ml of a single microorganism from a midstream clean-catch urine sample, or more than 10^3 colonies per ml from a urine sample obtained by catheterization. In case of clinically suspected pyelonephritis but a negative urine culture, acute DMSA scintigraphy is performed during the febrile episode. Suspected cases of bladder dysfunction are further investigated using video urodynamics testing.
2.1. Statistical Analysis
Group comparisons for continuous variables were performed using the independent t-test or the Mann-Whitney test, as appropriate. Categorical variables were analyzed using the Chi-squared test and Fisher’s exact test. Statistical significance was defined as a p-value < 0.05. Continuous variables are presented as mean (standard deviation), while categorical variables are shown as counts and percentages.
We also compared the Kaplan-Meier survival time and graft survival time of the study group to the control group. In addition, a log-rank test statistic was used to highlight possible statistical differences between these two groups.
3. Results
3.1. Characteristics of the Population
Among 178 pediatric recipients transplanted at our Centre between January 2011 and April 2023, 28 patients (15.7%) developed post-transplant urological complications. Children with urological complications did not differ from those without complications (150 patients, 84.3%) for demographic and clinical characteristics (gender, age, donor type, cause of ESRD, previous renal replacement therapy, number of transplants) (Table 1).
In detail, most of the subjects with urological complications were male (17 patients, 60.7%). In the study group (28 patients), the median age at transplantation was 12 years (range 3-21 years). The main cause of ESRD was represented by CAKUT (17 patients, 60.7%), followed by congenital nephrotic syndrome (4 cases, 14.2%), cystic diseases (4 children, 14.2%), corticosteroid-resistant nephrotic syndrome (2 patients, 7.1%), and chronic renal damage resulting from perinatal asphyxia (1 case, 3.5%). The source of the transplant was non-living donors in most cases (20 patients, 71.4%) and most children (13, 46.4%) had undergone renal replacement therapy before transplantation, with an average duration of dialysis of 33 months (7-98 months). Six patients (21.4%) had undergone a previous kidney transplant and 15 (53.6%) had had prior abdominal surgery, but no bladder augmentation. Pre-existing bladder dysfunction (bladder outlet stenosis and/or poor bladder capacity) was known in 8 cases (28.5%). Follow-up was discontinued due to graft failure in 2 patients and death in 1 case, but not related to the urological complications.
3.2. Classification and management of urological complications
Among the children with urological complications (28 patients, 15.7%), 12 (6.7%) were symptomatic VUR whereas 16 patients (9%) presented with ureteral or ureterovesical junction (UVJ) obstruction, also including obstruction due to extrinsic compression (2 cases of symptomatic lymphocele and 1 case of symptomatic hematoma). Detailed characteristics of patients with obstructive complications and VUR are summarized in Table 2.
Most children with urological complications (26 subjects, 92.8% of the study group) needed elective and/or emergency open, endoscopic, and/or minimally invasive surgery, yielding an incidence of complications needing surgery of 14.6% in the overall transplant population. Drainage tube dwell time was available in 19 cases: ureteral stent mean dwell time was 10 days (range 7-27 days) in patients with obstruction/urinary stenosis and 9.8 days in patients with VUR (range 7-13 days) without a statistically significant difference between the two groups (p 0.93).
As regards the time of occurrence of complications, 7 (25%) were early, 9 (32%) intermediate, and 12 cases (43%) were late complications. The type of surgical complications, time of occurrence, diagnostic studies conducted, and treatment performed are detailed in Table 3, Table 4 and Table 5.
Among early complications, 5 (71.4%) were UVJ obstructions presenting with acute renal failure and/or progressive hydroureteronephrosis detected during screening ultrasound performed after the removal of the ureteral stent (8-11 days post-transplant in mean). Three of these patients developed renal failure and/or urinary output abnormalities severe enough to require urgent invasive diagnostic investigations (cystoscopy and retrograde pyelourethrography in one case, and urgent percutaneous nephrostomy tube insertion with anterograde pyelourethrography in the other two cases). As for treatment, the first patient received a retrograde endoscopic mono-J (MJ) ureteral stent, and the second an antegrade placement of a double-J (DJ) ureteral stent after the urgent nephrostomy insertion. In the third case, no initial ureteral stent was placed, but later ureterovesical reimplantation and DJ ureteral stent placement were performed. The other 2 cases of UVJ obstructions presented with progressive worsening of hydronephrosis at ultrasound and increasing serum creatinine between the 21st and 26th day post-transplantation. Upon confirmation of obstruction by sequential MAG3 scintigraphy, one patient underwent ureterovesical reimplantation while the other was treated with percutaneous nephrostomy placement and anterograde pyelourethrography, followed by DJ ureteral stent placement.
The remaining two additional early complications were represented by perirenal fluid collections due to a lymphocele and an organized hematoma, respectively, both occurring with ultrasound evidence of worsening hydronephrosis between the 21st and 27th day post-surgery. Immediate surgical intervention was performed: lymphocele drainage via peritoneal fenestration and DJ ureteral stent placement for the hematoma, which was removed upon hydronephrosis recovery.
Among the 9 intermediate complications, 5 cases (55.5%) of UVJ stenosis or obstruction were documented. These included one middle-third ureteral stricture, one pyeloureteral junction (PUJ) stricture associated with urolithiasis, one upper-third ureteral stricture, and two UVJ strictures. Three of these patients developed acute kidney injury (AKI) and required urgent intervention. One patient, experiencing obstruction at the middle third of the ureter, was initially treated with a DJ stent, which was later replaced with a MJ stent due to contamination from C. Glabrata. This was followed by an end-to-side uretero-ureteral anastomosis between the transplanted ureter and the native ureter. In another case, AKI was due to urolithiasis with a wedged stone at the PUJ, which was treated with an urgent percutaneous nephrostomy and subsequent anterograde pyeloureterography, with a DJ ureteral stent placed anterograde. The third patient, presenting with a UVJ obstruction, received endoscopic balloon dilatation and DJ stent placement. Upon removal of the stent, however, the patient experienced a recurrence of UVJ obstruction with associated AKI and was treated with nephrostomy and antegrade pyeloureterography, followed by end-to-side ureteroureterostomy on the native ureter.
The last case together with another patient showed a significant increase in blood BK virus-DNA, suggesting BK virus infection as a potential cause of stenosis. The other case was managed with DJ stent placement.
The fifth case had UVJ stenosis associated with urethral outlet obstruction, requiring vesicostomy placement. Later, DJ stent placement and, due to persistent obstructive symptoms and bladder dysfunction, ureteral reimplantation and continent enterocystoplasty were performed.
All 3 cases of late-onset stenosis involved UVJ strictures. The first one, associated with an abscessed urinoma, was treated with percutaneous drainage and MJ stent insertion, and then with nephrostomy and ureter replacement using the native ureter. The second patient presented with UVJ stenosis secondary to a bladder lithiasic lesion, which was managed with two endoscopic removal procedures and the placement of a DJ stent. The third patient presented recurrent UVJ stenosis and was initially treated with endoscopic balloon dilatation and DJ stent placement, followed by ureteral reimplantation.
Overall, most intermediate and late ureteral obstructions were initially managed with endoscopic ureteral stent placement (DJ or MJ) (6 out of 8 cases, 75%), but subsequent open surgeries, including two ureteral reimplantations, two end-to-side anastomoses, and one native ureter replacement, was required in 4 of these 6 cases (66.6%).
All 12 cases of VUR presented as intermediate or late complications occurring 23 months post-transplant. Symptoms were represented by UTI, with most patients (66.6%) presenting two or more UTIs. Table 6 shows all the bacteria identified in urine cultures: E. Coli and K. Pneumoniae, accounting respectively for 8 (44%) and 3 cases (17%) out of 18, were prevalent.
Diagnostic methods included contrast-enhanced voiding cystourethrography (ceVUS) (performed in one case at another hospital for unavailability of standard voiding cystography) and DMSA scintigraphy. First-line treatment was endoscopic correction with Deflux injection in 8 out of 12 cases (67%). Two cases required repeated Deflux injections because of recurrent UTIs and VUR. Two children with low-grade reflux were managed conservatively with antibiotic prophylaxis. Circumcision was performed during the endoscopic procedure in two cases.
Bladder outlet obstruction and/or low bladder capacity were identified as the main causes of VUR in two children, who underwent percutaneous suprapubic cystostomy and bladder augmentation surgery with catheterizable stoma creation (Monti procedure).
3.3. Costs of Urological Complications
Children who experienced urological complications required an average of 2.5 additional hospital admissions compared to those who did not. The median cost per admission at our Centre was 9,574 euros. Therefore, the average cost per patient increased by approximately 23,935 euros in the presence of urological complications.
3.4. Patient and Graft Survival
We compared overall patient and graft survival between the group of children with urological complications and the control group. Survival curves are comparable between the two groups, with no statistically significant differences (Figure 2).
4. Discussion
Urinary complications are relatively common in renal transplant recipients and can lead to significant morbidity and mortality [15,16].
Early diagnosis and appropriate management are thus essential for preserving graft function [17]. Children are particularly at risk for these complications, which are often due to urinary tract dysfunction as the primary cause of ESRD. Additionally, their smaller anatomical structures present unique surgical challenges.
In our study, urological complications were observed in 28 children (15.7%) out of the 178 pediatric kidney transplants performed between January 2011 and April 2023. Our results are consistent with previous data, reporting urological complications in approximately 10-20% of pediatric kidney transplant recipients, even if a broad range of overall urological complication rates, varying from 1% to 27%, is reported in most studies [15; 17-22]. More in detail, obstructive complications occurred in 9% (7.3% ab intrinseco and 1.7% ureteral compression by fluid collections) and symptomatic VUR in 6.7% of our population. In several recent pediatric series, ureteral stenosis ranged from 5% to 8% [18,19,20,21,22], and in a very large case series of 526 pediatric kidney transplants from a single tertiary center, ureteral obstruction occurred in 8% of cases [23], a rate that is consistent with our finding of 7.3% of patients experiencing post-transplant ureteral strictures ab intrinseco. Therefore, ureteral stenosis emerges as the most common urological complication following kidney transplantation, predominantly occurring within the first year post-surgery, as confirmed by our series, in which all the ureteral or UVJ strictures were detected within 8 months from the transplant, with over 80% occurring within the first 3 months, and a median time to diagnosis of approximately 2 months (58 days) post-transplantation.
Endourological techniques, such as balloon dilation and stenting, are now the standard procedure for managing ureteral obstructions, thanks to their minimally invasive nature and high success rates. These methods are particularly effective for stenoses under 1.5 cm and for treatment within 3 months of onset [10]. In our study, the initial approach to ureteral stenosis involved ureteral stenting, which successfully resolved the issue in 5 cases (38.5%). Success rates reported in the literature are generally higher [24], but the difference may be attributed to the length of the stenosis and to the timing of intervention. In 61.5% of our cases, a definitive surgical correction, such as ureteral reimplantation or ureteroureterostomy, was required. This is consistent with other studies, which highlight that more complex stenoses or failures of endoscopic treatment often necessitate surgical intervention [25].
VUR, although less common than other complications, significantly increases the risk of recurrent UTIs and graft pyelonephritis in transplant recipients. VUR can arise from surgical techniques, such as a short submucosal tunnel in neo cystostomy, or from bladder issues as a non-compliant bladder, leading to retrograde urine flow and complex infections [26]. Several studies have documented post-transplant symptomatic VUR rates between 2% and 13%. [15; 17-20; 27]. In our study, 6.7% of patients developed symptomatic VUR, with 83.3% requiring endoscopic or surgical intervention. Diagnosis typically occurred within two years post-transplantation, though some patients developed infections up to eight years later. VUR was diagnosed by voiding VCUG in all our patients, except for one. VCUG is the gold standard for VUR evaluation, even if it involves radiation exposure, and literature data suggest that ceVUS performed by experienced operators may serve as a viable alternative to traditional VCUG if the latter is unavailable [26].
Most of our patients with VUR (8 out of 12, 4.5% of the overall population) were treated with endoscopic Deflux injections at the bladder level. Six patients had no recurrence of infection after the initial treatment, while two needed a second injection, with a 75% success rate of the first endoscopic treatment in preventing infection recurrence. Literature reports a 50% success rate with Deflux for VUR management and suggests that endoscopic treatment is more effective in patients without lower urinary tract dysfunction while it shows higher failure rates in those with such issues [17; 28].
Recent studies have identified CAKUT, BK virus infection, posterior urethral valves, and a history of prior ureteral surgery as risk factors for urological complications in pediatric kidney transplant recipients [15; 19; 20-21]. Comparing the patients who experienced urological complications with control recipients who did not, no significant differences in terms of sex, age at transplantation, donor source, cause of ESRD, or history of dialysis and previous transplants emerged in our study. Previous research also reported no notable differences in obstruction rates based on age or gender. Some authors attributed this to the relative rarity of these complications, which may limit the ability to detect statistically significant differences [19; 23]. Conversely, 28% of our patients had pre-existing bladder dysfunction, with 25% having both lower urinary tract dysfunction (LUTD) and CAKUT as the underlying cause of ESRD. LUTD has already been demonstrated to be a significant risk factor for developing post-transplant urological complications [15; 18]. These data emphasize the importance of a comprehensive urological evaluation during pre-transplant assessment, especially in children with such risk factors. Optimal evaluation and management strategies for these patients remain uncertain, however, recommendations include abdominal ultrasound, voiding cystourethrography for patients with a history of UTIs or prior urological interventions, and invasive urodynamic studies for bladder dysfunction [29,30]. Management of lower urinary tract issues may involve bladder rehabilitation therapy, pharmacological treatments, intermittent catheterization, and surgical reconstruction. Conservative treatments to improve native bladder function should be prioritized before reconstructive procedures such as urinary diversion or bladder augmentation. Reconstructive surgery is generally recommended before transplantation, but caution is advised in children with severe chronic kidney disease [30,31,32,33].
In a recent retrospective analysis of 136 pediatric patients undergoing kidney transplantation, the incidence of urological complications requiring surgical or endoscopic therapy for stenosis or VUR was 13% [14]. Taher et al. reported that nearly 20% of 146 pediatric patients undergoing kidney transplantation experienced intra-abdominal complications, and about 6.2% required surgical drainage for fluid collections [7]. In our population, urological complications requiring surgical or endoscopic therapy were 13.4%. Importantly, these complications required multiple diagnostic procedures and therapeutic interventions with an overall increase in hospitalization episodes (+2.5 admissions in mean) and cost approximately 24,000 euros compared to an uncomplicated post-transplant course. However, urological complications did not significantly impact transplant outcomes, with a graft survival rate comparable to the control group. This could be attributed to a careful screening for post-transplant urological complications, which allowed timely detection and treatment, contributing to preserving graft function. Additionally, the advancement of minimally invasive techniques facilitates more effective management of these complications, further contributing to the preservation of graft function. Previous studies have already demonstrated that urological complications do not significantly impact graft survival [34,35]. In a study by van Roijen et al., involving 695 kidney transplant recipients, 10.8% developed urological complications. However, the graft failure rates at 5 and 10 years were comparable between patients with and without these complications, suggesting that early identification and treatment of urological complications do not compromise graft function [34].
5. Conclusions
Urological complications are common after pediatric kidney transplantation, with an incidence of 15.7% in our study, consistent with previous reports. Most patients had pre-existing urological malformations, as previously reported [19,20]. Furthermore, our findings confirm existing data on the timing of onset of urological complications, as ureteral stenosis and leakage typically occur within a month post-transplantation, while VUR often requires treatment years later. While early complications are often detected due to acute clinical manifestations (usually AKI), late ones are mainly identified during routine clinical, laboratory, or ultrasound follow-up. Regular post-transplant ultrasound follow-up is therefore crucial, especially for patients with known risk factors. Endoscopic surgery is usually the first line of treatment, with open surgery reserved for cases where initial treatments failed, or complications recurred. Pre-transplant comprehensive urological assessment can help in minimizing post-transplant complications and can guide patient-tailored surgical techniques. Meticulous post-transplantation follow-up and collaboration with a well-coordinated multidisciplinary team may allow timely detection and treatment of complications, avoiding detrimental effects on graft function and improving transplantation outcomes.
Author Contributions
Conceptualization, M.S. and E.M.; methodology, M.S., E.M. and A.M; formal analysis, M.S. and E.M.; investigation, E.M, M.S., S.V., M.M. and N.B.P.; data curation: E.M, M.S., S.V. and N.B.P.; writing—original draft preparation, M.S., E.M. and A.M.; writing—review and editing, E.B.; visualization, M.M.; supervision, E.B.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are contained within the article, further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Saran, R.; Robinson, B.; Abbott, K.C.; Agodoa, L.Y.C.; Bragg-Gresham, J.; Balkrishnan, R.; et al. US Renal Data System 2018 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2019, 73 (Suppl 1), A7–A8. [Google Scholar] [CrossRef] [PubMed]
- Bonthuis, M.; Vidal, E.; Bjerre, A.; Aydoğ, Ö.; Baiko, S.; Garneata, L.; et al. Ten-Year Trends in Epidemiology and Outcomes of Pediatric Kidney Replacement Therapy in Europe: Data from the ESPN/ERA-EDTA Registry. Pediatr. Nephrol. 2021, 36, 2337–2348. [Google Scholar] [CrossRef]
- Choate, H.R.; Mihalko, L.A.; Choate, B.T. Urologic Complications in Renal Transplants. Transl. Androl. Urol. 2019, 8, 14147–14147. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.S.; Kim, K.S.; Choi, S.W.; Bae, W.J.; Hong, S.H.; Lee, J.Y.; et al. Ureteral Complications in Kidney Transplantation: Analysis and Management of 853 Consecutive Laparoscopic Living-Donor Nephrectomies in a Single Center. Transplant Proc. 2016, 48, 2684–2688. [Google Scholar] [CrossRef] [PubMed]
- Ranchin, B.; Chapuis, F.; Dawhara, M.; Canterino, I.; Hadj-Aïssa, A.; Saïd, M.H.; et al. Vesicoureteral Reflux after Kidney Transplantation in Children. Nephrol. Dial. Transplant. 2000, 15, 1852–1858. [Google Scholar] [CrossRef]
- Williams, M.A.; Giel, D.W.; Hastings, M.C. Endoscopic Deflux Injection for Pediatric Transplant Reflux: A Feasible Alternative to Open Ureteral Reimplant. J. Pediatr. Urol. 2008, 4, 341–344. [Google Scholar] [CrossRef] [PubMed]
- Taher, A.; Zhu, B.; Ma, S.; Shun, A.; Durkan, A.M. Intra-Abdominal Complications after Pediatric Kidney Transplantation: Incidence and Risk Factors. Transplantation 2019, 103, 1234–1239. [Google Scholar] [CrossRef] [PubMed]
- Mamarelis, G.; Vernadakis, S.; Moris, D.; Altanis, N.; Perdikouli, M.; Stravodimos, K.; et al. Lithiasis of the Renal Allograft, a Rare Urological Complication Following Renal Transplantation: A Single-Center Experience of 2,045 Renal Transplantations. Transplant Proc. 2014, 46, 3203–3205. [Google Scholar] [CrossRef]
- Stapenhorst, L.; Sassen, R.; Beck, B.; Laube, N.; Hesse, A.; Hoppe, B. Hypocitraturia as a Risk Factor for Nephrocalcinosis after Kidney Transplantation. Pediatr. Nephrol. 2005, 20, 652–656. [Google Scholar] [CrossRef]
- Caamiña, L.; Pietropaolo, A.; Prudhomme, T.; et al. Endourological Management of Ureteral Stricture in Patients with Renal Transplant: A Systematic Review of Literature. J. Endourol. 2024, 38, 290–300. [Google Scholar] [CrossRef]
- Oomen, L.; De Wall, L.L.; Krupka, K.; Tönshoff, B.; Wlodkowski, T.; Van Der Zanden, L.F.; et al. The Strengths and Complexities of European Registries Concerning Paediatric Kidney Transplantation Health Care. Front. Pediatr. 2023, 11, 1121282. [Google Scholar] [CrossRef] [PubMed]
- Bessede, T.; Hammoudi, Y.; Bedretdinova, D.; Parier, B.; Francois, H.; Durrbach, A.; et al. Preoperative Risk Factors Associated with Urinary Complications after Kidney Transplantation. Transplant Proc. 2017, 49, 2018–2024. [Google Scholar] [CrossRef] [PubMed]
- Hotta, K.; Miura, M.; Wada, Y.; Fukuzawa, N.; Iwami, D.; Sasaki, H.; et al. Atrophic Bladder in Long-Term Dialysis Patients Increases the Risk for Urological Complications after Kidney Transplantation. Int. J. Urol. 2017, 24, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.M.; Windsperger, A.; Alanee, S.; Humar, A.; Kashtan, C.; Shukla, A.R. Risk Factors and Treatment Success for Ureteral Obstruction after Pediatric Renal Transplantation. J. Urol. 2010, 183, 317–322. [Google Scholar] [CrossRef]
- Irtan, S.; Maisin, A.; Baudouin, V.; Nivoche, Y.; Azoulay, R.; Jacqz-Aigrain, E.; et al. Renal Transplantation in Children: Critical Analysis of Age-Related Surgical Complications. Pediatr. Transplant. 2010, 14, 512–519. [Google Scholar] [CrossRef]
- Torricelli, F.C.M.; Watanabe, A.; Piovesan, A.C.; Antonopoulos, I.M.; David-Neto, E.; Nahas, W.C. Urological Complications, Vesicoureteral Reflux, and Long-Term Graft Survival Rate after Pediatric Kidney Transplantation. Pediatr. Transplant. 2015, 19, 844–848. [Google Scholar] [CrossRef]
- Castagnetti, M.; Angelini, L.; Ghirardo, G.; Zucchetta, P.; Gamba, P.; Zanon, G.; et al. Ureteral Complications after Renal Transplant in Children: Timing of Presentation, and Their Open and Endoscopic Management. Pediatr. Transplant. 2014, 18, 150–154. [Google Scholar] [CrossRef]
- Rossi, V.; Torino, G.; Gerocarni Nappo, S.; Mele, E.; Innocenzi, M.; Mattioli, G.; et al. Urological Complications Following Kidney Transplantation in Pediatric Age: A Single-Center Experience. Pediatr. Transplant. 2016, 20, 485–491. [Google Scholar] [CrossRef]
- Routh, J.C.; Yu, R.N.; Kozinn, S.I.; Nguyen, H.T.; Borer, J.G. Urological Complications and Vesicoureteral Reflux Following Pediatric Kidney Transplantation. J. Urol. 2013, 189, 1071–1076. [Google Scholar] [CrossRef]
- Morrison, C.D.; Shannon, R.; Rosoklija, I.; Nettey, O.S.; Superina, R.; Cheng, E.Y.; et al. Ureteral Complications of Pediatric Renal Transplantation. J. Urol. 2019, 201, 810–814. [Google Scholar] [CrossRef]
- Englesbe, M.J.; Lynch, R.J.; Heidt, D.G.; Thomas, S.E.; Brooks, M.; Dubay, D.A.; et al. Early Urologic Complications after Pediatric Renal Transplant: A Single-Center Experience. Transplantation 2008, 86, 1560–1564. [Google Scholar] [CrossRef] [PubMed]
- Shokeir, A.A.; Ali-El-Dein, B.; Osman, Y.; Zahran, M.; Eldiasty, I. Surgical Complications in Live-Donor Paediatric and Adolescent Renal Transplantation: Study of Risk Factors – Mansoura Experience 1976–2017. Arab J. Urol. 2018, 16, S23–S24. [Google Scholar] [CrossRef]
- Serrell, E.C.; Su, R.; O’Kelly, F.; Semanik, M.; Farhat, W.A. The Utility of Native Ureter in the Management of Ureteral Complications in Children after Renal Transplantation. Pediatr. Transplant. 2021, 25, e14051. [Google Scholar] [CrossRef] [PubMed]
- Territo, A.; Bravo-Balado, A.; Andras, I.; et al. Effectiveness of Endourological Management of Ureteral Stenosis in Kidney Transplant Patients: EAU-YAU Kidney Transplantation Working Group Collaboration. World J. Urol. 2023, 41, 1951–1957. [Google Scholar] [CrossRef] [PubMed]
- Rahnemai-Azar, A.A.; Gilchrist, B.F.; Kayler, L.K. Independent Risk Factors for Early Urologic Complications after Kidney Transplantation. Clin. Transplant. 2015, 29, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Paltiel, H.J.; Barnewolt, C.E.; Chow, J.S.; Bauer, S.B.; Diamond, D.A.; Stamoulis, C. Accuracy of Contrast-Enhanced Voiding Urosonography Using Optison™ for Diagnosis of Vesicoureteral Reflux in Children. J. Pediatr. Urol. 2023, 19, 135.e1–135.e8. [Google Scholar] [CrossRef]
- Kasiske, B.L.; Vazquez, M.A.; Harmon, W.E.; Brown, R.S.; Danovitch, G.M.; Gaston, R.S.; et al. Recommendations for the Outpatient Surveillance of Renal Transplant Recipients. J. Am. Soc. Nephrol. 2000, 11 Suppl 15, S1–86. [Google Scholar] [CrossRef]
- Sharma, A.; Ramanathan; Posner, M. ; Fisher. Pediatric Kidney Transplantation: A Review. Transpl. Res. Risk Manag. 2013, 5, 21–29. [Google Scholar]
- Riley, P.; Marks, S.D.; Desai, D.Y.; Mushtaq, I.; Koffman, G.; Mamode, N. Challenges Facing Renal Transplantation in Pediatric Patients with Lower Urinary Tract Dysfunction. Transplantation 2010, 89, 1299–1307. [Google Scholar] [CrossRef]
- Husmann, D.A. Lessons Learned from the Management of Adults Who Have Undergone Augmentation for Spina Bifida and Bladder Exstrophy: Incidence and Management of the Non-Lethal Complications of Bladder Augmentation. Int. J. Urol. 2018, 25, 94–101. [Google Scholar] [CrossRef]
- Rajpoot, D.K.; Gomez, A.; Tsang, W.; Shanberg, A. Ureteric and Urethral Stenosis: A Complication of BK Virus Infection in a Pediatric Renal Transplant Patient. Pediatr. Transplant. 2007, 11, 433–435. [Google Scholar] [CrossRef] [PubMed]
- Hart, A.; Smith, J.M.; Skeans, M.A.; Gustafson, S.K.; Wilk, A.R.; Castro, S.; et al. OPTN/SRTR 2018 Annual Data Report: Kidney. Am. J. Transplant. 2020, 20 (Suppl. S1), 20–130. [Google Scholar] [CrossRef]
- Van Roijen, J.H.; Kirkels, W.J.; Zietse, R.; Roodnat, J.I.; Weimar, W.; Ijzermans, J.N. Long-Term Graft Survival after Urological Complications of 695 Kidney Transplantations. J. Urol. 2001, 165 Pt 1, 1884–1887. [Google Scholar] [CrossRef] [PubMed]
- Di Carlo, H.N.; Darras, F.S. Urologic Considerations and Complications in Kidney Transplant Recipients. Adv. Chronic Kidney Dis. 2015, 22, 306–311. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Design of the study.
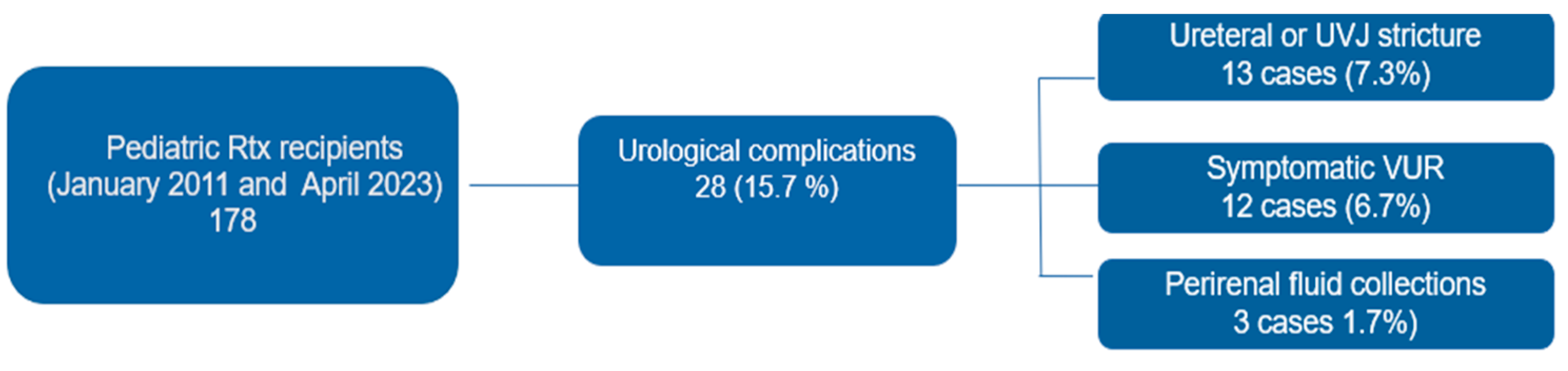
Figure 2.
Overall patient (up) and graft survival (down) curves in recipients with urological complications (blue line) and in control group (red line).
Figure 2.
Overall patient (up) and graft survival (down) curves in recipients with urological complications (blue line) and in control group (red line).
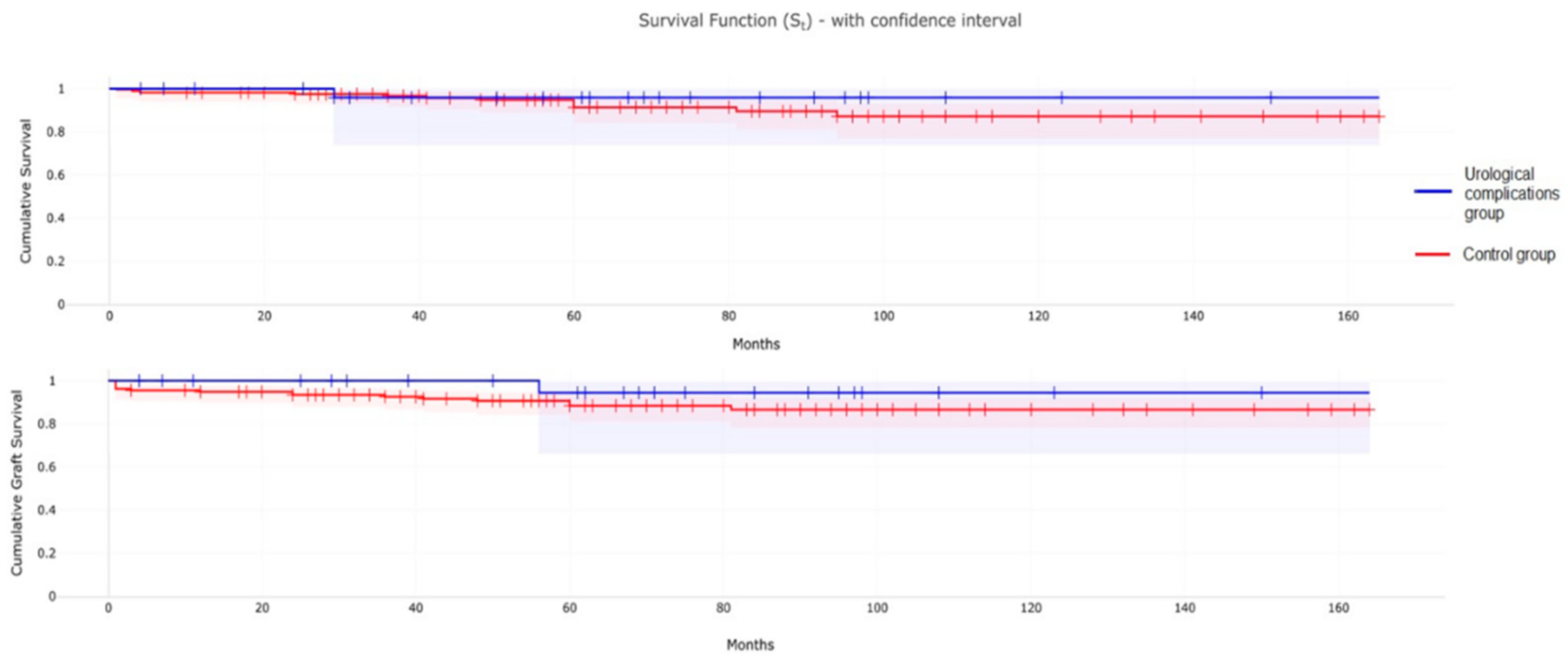

Table 1.
Characteristics of the patients.
| Variable | Study group | Control group | P value |
| Number of patients | 28 | 150 | |
| Gender | 0.589951 | ||
| Male | 17 (60%) | 99 (66%) | |
| Female | 11 (40%) | 51 (34%) | |
| Source | 0.164926 | ||
| Living donor | 8 (29%) | 26 (17.3%) | |
| Deceased donor | 20 (71%) | 124 (82.7%) | |
| Mean age at RTx, y (SD) | 11 (5) | 9.61 (5.57) | 0.4456 |
| Cause of ESRD | |||
| CAKUT | 17 (61%) | 73 (48.6%) | 0.24 |
| Other causes* | 11 (39%) | 77 (51.4%) | |
| Renal replacement therapy | 0.240508 | ||
| Previous RTx and dialysis | 6 (21%) | 17 (11.3%) | |
| Dialysis pre RTx | 13 (46%) | 106 (70.7%) | |
| Pre-emptive RTx | 9 (32%) | 27 (18%) |
CAKUT, Congenital Anomalies of Kidney and Urinary Tract. ESRD, End Stage Renal Disease. RTx renal transplantation. SD standard deviation. * Detailed in Table 2
Table 2.
Characteristics of the study group and comparison among ureteral obstruction and VUR subgroups.
Table 2.
Characteristics of the study group and comparison among ureteral obstruction and VUR subgroups.
| Variable | Study patients | Ureteral obstruction subgroup * | VUR subgroup |
| Number of patients | 28 | 16 (57%) | 12 (43%) |
| Gender | |||
| Male | 17 (60%) | 9 (56%) | 8 (67%) |
| Female | 11 (40%) | 7 (44%) | 4 (33%) |
| Cause of ESRD | |||
| CAKUT | 17 (61%) | 11 (69%) | 6 (50%) |
| Renal hypoplasia/dysplasia/ agenesis +/- VUR | 15 |
10 |
5 |
| PUV | 1 | 1 | 0 |
| Urogenital sinus malformation | 1 | 0 | 1 |
| Other causes | 11 (39%) | 5 (31%) | 6 (50%) |
| Congenital nephrotic syndrome | 4 | 2 | 2 |
| SRNS | 2 | 2 | 0 |
| Cystic disease | 4 | 1 | 3 |
| Renal impairment after neonatal asphyxia | 1 | 0 | 1 |
| Age at RTx, mean years (SD) | 11 (5) | 12 (5) | 8 (5) |
| Source | |||
| Living donor | 8 (29%) | 4 (25%) | 4 (33%) |
| Deceased donor | 20 (71%) | 12 (75%) | 8 (67%) |
| Renal replacement therapy | |||
| Previous RTx and dialysis | 6 (21%) | 6 (37,5%) | 0 (%) |
| Dialysis pre RTx [mean months, SD] | 13 (46%) [38.6, 27] | 6 (37,5%) [37.7, 25.7] | 7 (58%) [43.6, 30.6] |
| Pre-emptive RTx | 9 (32%) | 4 (25%) | 5 (42%) |
| Pre-existing bladder dysfunction | 8 (28%) | 5 (31%) | 3 (25%) |
| Abdominal surgery pre-RTx | 15 (53%) | 8 (50%) | 7 (58%) |
| Follow-up, mean months (SD) | 65 (36) | 60 (32) | 73 (41) |
| Graft failure | 2 | 1 | 1 |
CAKUT, Congenital Anomalies of Kidney and Urinary Tract. ESRD, End Stage Renal Disease. PUV, posterior urethral valves. RTx renal transplantation. SD standard deviation. SRNS, steroid resistant nephrotic syndrome. VUR, vesicoureteral reflux. *Including extrinsic causes of stenosis (i.e., obstructive lymphocele and hematoma).
Table 3.
Early urological complications (occurring between 7 and 30 days after transplantation).
| Complications | N | Post-RTx onset day | Diagnostic studies | First Treatment | Subsequent treatments |
|---|---|---|---|---|---|
|
UVJ obstruction (AKI) + Urinary leakage |
3 | 8th (2), 11th, | Ultrasound (3), Anterograde pyelography (2); Cystoscopy + retrograde pyelography (1), | Emergency nephrostomy and DJ stent placement (2); MJ ureteral stent placement (1) | DJ replacement (1), Ureteroneocystostomy (3) |
| Obstructive lymphocele | 1 | 21st | Ultrasound, Drained fluid analysis | Surgical drainage into peritoneal cavity | |
| UVJ obstruction (AKI) + Urinary leakage | 2 | 21st, 26th |
Ultrasound (2), MAG3 scintigraphy (2), Anterograde pyelography (1) | Ureteroneocystostomy and DJ stent placement (1), Emergency nephrostomy (1), | DJ stent placement (1) |
| Obstructive perirenal hematoma | 1 | 27Th | Ultrasound | DJ stent placement | |
| Total | 7 |
AKI, acute kidney injury. DJ stent, double-J stent. MJ stent, mono-J stent. RTx renal transplantation. UVJ, ureterovesical junction.
Table 4.
Intermediate urological complications (occurring between 30 and 90 days after renal transplantation).
Table 4.
Intermediate urological complications (occurring between 30 and 90 days after renal transplantation).
| Complications | N | Post-RTx day of onset | Diagnostic studies | First treatment | Subsequent treatments |
|---|---|---|---|---|---|
| VUR complicated by UTI (3) | 3 | 35th, 59th and 63rd | VCUG(3), DMSA scintigraphy (3) | Endoscopic injection of a bulking agent (Deflux) (2) + Circumcision (1), Conservative (antibiotic prophylaxis) (1) | 2nd Endoscopic injection of a bulking agent (Deflux) (2) |
| Obstructive lymphocele | 1 | 42nd | Ultrasound, Drained fluid analysis | Ultrasound-guided percutaneous drainage | |
| Middle 1/3 ureteral stricture (AKI) | 1 | 48th | Ultrasound, MAG3 Scintigraphy. | DJ ureteral stent placement | End-to-side anastomosis of the transplant to the native ureter |
| Ureteral (1) and UVJ (AKI) (1) stricture in suspected BK virus infection/ reactivation | 2 | 65th and 79th | Ultrasound (2), MAG3 Scintigraphy (2), Magnetic Resonance Urography + Cystoscopy and retrograde pyelography (1) | DJ ureteral stent placement (2) + Balloon dilatation (1); | Nephrostomy and subsequent End-to-side anastomosis of the transplant to the native ureter (1); |
| Urolithiasis and pyeloureteral junction stricture (AKI) | 1 | 58th | Ultrasound; Anterograde pyelography; MAG3 Scintigraphy; Abdominal CT + Transnephrostomic contrastographic study under CT guidance; | Emergency nephrostomy | DJ ureteral stent placement |
| Bladder outlet obstruction and UVJ stricture | 1 | 69th | Ultrasound, MAG3 Scintrigraphy | Vesicostomy | DJ stent placement and subsequent continent enterocystoplasty and catheterizable stoma (Monti Procedure). |
| Total | 9 |
AKI, acute kidney injury. CT, computed tomography. DJ stent, double-J stent. RTx renal transplantation. UTI Urinary tract infection. UVJ, ureterovesical junction. VCUG, Voiding cystourethrogram. VUR, vesicoureteral reflux. .
Table 5.
Late urological complications (occurring more than 90 days after renal transplantation).
| Complications | N | Post-RTx day of onset | Diagnostic studies | First Treatment | Subsequent treatments |
|---|---|---|---|---|---|
| Bladder dysfunction and VUR complicated by UTI | 1 | 110th | Ultrasound, MAG3 scintigraphy, Video urodynamic tests | Suprapubic percutaneous cystostomy | Stimulation of the posterior tibial-pudendal nerve |
| VUR complicated by UTI in pre-existing poor bladder capacity | 1 | 117th | Ultrasound (1), ceVUS (1), | Bladder augmentation | |
|
UVJ obstruction with ureteral rupture and abscessed urinoma. Recurrent UVJ obstruction after ureteral stent removal |
1 | 157th | Abdominal CT, Drained fluid analysis, Retrograde endoscopic urethrography. Anterograde pyelography and retrograde endoscopic urethrography. |
Ultrasound-guided percutaneous drainage, MJ ureteral stent placement. Emergency nephrostomy |
Replacement of ureteral MJ stent with DJ stent. Subsequent replacement of a transplanted ureter with a native ureter and ureteral stent placement. |
| Exophytic amorphous vesical lesion and UVJ stricture | 1 | 199th | Ultrasound, MAG3 scintigraphy, cystoscopy. | Endoscopic removal of bladder exophytic lesion and placement of a DJ ureteral stent | 2° Endoscopic removal of bladder exophytic lesion and placement of a DJ ureteral stent |
| Ureteral stricture | 1 | 219th | Sonography, MAG3 scintigraphy | DJ ureteral stent placement | Uretero-neocystostomy, DJ stent placement and circumcision |
|
VUR complicated by UTI (6), Urethral stricture (1) |
7 | 270th, 545th, 567th, 771st, 1168th, 1764th, 3121st |
DMSA scintigraphy (5), VCUG (5), Video urodynamic tests (1) | Endoscopic injection of a bulking agent (Deflux) (5), Conservative (antibiotic prophylaxis) (1), Endoscopic urethral dilatation (1) | Circumcision (1) |
| Total | 12 |
ceVUS, contrast-enhanced voiding urosonography. CT, computed tomography. DJ stent, double-J stent. MJ stent, mono-J stent. RTx renal transplantation. UTI Urinary tract infection. VCUG, Voiding cystourethrogram. VUR, vesicoureteral reflux. .
Table 6.
Bacteria identified as the cause of UTI affecting the transplanted kidney through urine culture in patients with VUR. .
Table 6.
Bacteria identified as the cause of UTI affecting the transplanted kidney through urine culture in patients with VUR. .
| Patient number | 1st UTI | 2nd UTI | 3rd UTI |
|---|---|---|---|
| Patient n.1 | Klebsiella Pneumoniae | Escherichia coli | Escherichia coli |
| Patient n.2 | K. Ornithinolytica | K. Ornithinolytica | Escherichia coli |
| Patient n.3 | Klebsiella Pneumoniae and Escherichia coli | Klebsiella Oxytoca | |
| Patient n.4 | Enterococcus faecium | P. Aeruginosa | P. Aeruginosa |
| Patient n.5 | Escherichia coli | ||
| Patient n.6 | Enterococcus faecalis | ||
| Patient n.7 | Escherichia coli | ||
| Patient n.8 | Klebsiella Pneumoniae | Escherichia coli | |
| Patient n.9 | Escherichia coli |
UTI Urinary tract infection.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



