
Submitted:
29 September 2024
Posted:
30 September 2024
You are already at the latest version
Abstract
(1) Background: Eosinophils importance as T2 inflammation markers is known to be fundamental in asthma, chronic sinusitis, vasculitis. In cancer, despite their potential antiproliferative effect, their role remains unclear. Our purpose was to describe the relation between baseline blood eosinophil count (EOS) and overall survival in pancreatic ductal adenocarcinoma (PDAC) patients. (2) Methods: We have analyzed retrospectively the data of 137 adult patients, who underwent surgical treatment of PDAC between years 2012-2019 with no history of systemic steroid use directly before surgical treatment and no metastases found intraoperatively. (3) Results: EOS<0,1 G/l (vs. ≥0,1 G/l) was an independent prognostic factor for OS both the uni- and multivariate Cox regression (respectively: HR=1,48, p=0,035 and HR=1,57, p=0,021). According to EOS and PDAC stage, median OS were: in stage I-III, EOS ≥0,1 G/l group: 14,5 months, in stage I-III, EOS <0,1 G/l group: 8,0 months, in stage IV, EOS ≥0,1 G/l group: 7,0 months, in stage IV, EOS <0,1 G/l group: 5,0 months. (4) Conclusions: Peripheral eosinophilia seems to be a potential independent prognostic factor. Further studies are necessary to confirm this hypothesis, since our findings suggest that T2 inflammation may be the factor directly or indirectly lengthening survival of PDAC patients.
Keywords:
cancer biology
; clinical observations
; immunology
; pancreatic ductal adenocarcinoma
; pancreatic cancer
1. Introduction
The outcomes of pancreatic ductal adenocarcinoma cancer (PDAC) surgical treatment did not increase substantially in the last decades. 5-year survival time median still does not exceed 20 – 30% with median overall survival (OS) up to 20 months [1]. Well-known predictive factors improving these outcomes are administration of chemotherapy, pN0 nodal status and R0 resection with negative resection margin [2]. Despite this, researchers try to find preoperative factors in peripheral blood, other than tumor markers (carbohydrate an-tigens), affecting the OS in PDAC patients such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), eosinophil-lymphocyte ratio (ELR), FT3 to FT4 conversion ratio or gender-specific coagulation profile [3,4,5,6,7]. Current research commonly aims to find the mechanisms underlying the systemic inflammation caused by PDAC, which is probably related to the microenvironment of the tumor causing immunologic disorder. This knowledge could lead to better understanding of pathogenesis of the disease and development of patient-dedicated immunotherapies improving the outcomes [8].
The human immune system is the guardian of our well-being – it recognizes pathogens and initiates a suitable response. Eosinophil is one of the elements of its arsenal. Eosinophils are leukocytes taking a role in immunological responses of the organism by receptors for cytokines, chemokines and adhesion molecules. It is involved in parasitic, bacterial, fungal and viral infections as well as response to tissue damage and metabolic disorders, and as their involvement is promoted by Th2 lymphocytes, eosinophilic inflammation is also named a T2 inflammation.. In recent years its role in pathogenesis of various diseases has gained interest from researchers.
Eosinophils are regulated by adaptive immunity and treated as effector cells [9]. Under physiological conditions there is high concentration of eosinophils in the gastrointestinal (GI) tract, where they regulate mucosal immunoglobulin A (IgA) secretion by producing interleukin 1 (IL-1), regulate the number of Th17 lymphocytes by expressing an antagonist for receptor of interleukin 1 (IL-1R) and regulate Treg differ-entiation through tumor growth factor β (TGF-β) and retinoic acid [10,11,12]. These processes take a role in maintaining the homeostasis between suppression and promotion of cell proliferation. CCL11 (eotaxin-1) is one of the most important and effective eosinophil-specific chemokine targeting eosinophils – it promotes its maturation in bone marrow, triggers release of eosinophils into the blood and causes directed trafficking of eosinophils into tissue [13]. Following this biological pathway Simson et al. in 2007 found out that eosinophils could have a potential antiproliferative effect in in vivo studies in mice as an effector cell in cancer immune surveillance – it is suppressing in vivo and in vitro carcinogenesis and/or the development of chemically induced cancers [13]. Clear relationship between peripheral eosinophil count and cancer development is not well known but blood eosinophilia has been already described as a prognostic factor for OS or progression-free survival in some cases of solid cancer tumors such as melanoma, colon cancer, neuroendocrine tumors, urothelial carcinoma, renal cell carcinoma, glioblastoma, xanthoastrocytoma, ovarian cancer, prostate cancer, leiomyosarcoma, non-small cell lung cancer and breast cancer [14,15,16,17]. Hypereosinophilia has also been described to be an early sign of the disease in hematological cancer patients [18]. Knowledge about eosinophilia in and its relationship with OS in PDAC patients undergoing surgical treatment is lacking, thus our aim was to determine prognostic value of blood eosinophilia (EOS) in this group of patients.
2. Material and Methods
We have analyzed retrospectively the data from electronic medical record system of 137 adult patients, who consecutively underwent surgical treatment of PDAC in General and Transplant Surgery Department (Medical University of Lodz, Poland) between years 2012-2019 and fulfilled inclusion (no history of systemic steroid use at least 1 month before surgical treatment, available: age, sex, blood morphology baseline with white blood cell differential, tumor localization, grade, stage: localized or regional, PDAC confirmation in post-operational histopathological examination, survival time) and exclusion criteria (distant metastases found intraoperatively; neoadjuvant chemotherapy; diagnosis or being under diagnostic process of: fungal or parasitic infection, eosinophilic asthma, hypereosinophilic syndrome or EGPA, use of systemic steroids treatment at least 1 month before surgery). All the patients were qualified to surgical procedure treatment without preoperative diagnosis (due to the tumor size or diagnostic failure of preoperative percutaneous biopsies) – including locally advanced stages where priority was to obtain a tissue sample.
Samples of peripheral blood for blood morphology test were collected on the admission to the hospital (up to 24 hours before surgery). Eosinophil counts were obtained as part of routine preoperative blood tests performed up to 24 hours before surgery. Blood samples were processed using an automated hematology analyzer (Sysmex XN-2000), which provided a complete blood count (CBC) with differential, including the absolute eosinophil count. The results were reported as absolute eosinophils per liter (G/l), and patients were categorized based on eosinophil levels into two groups: EOS ≥ 0.1 G/l and EOS < 0.1 G/l.
The patients were classified according to the American Joint Committee on Cancer (AJCC) 8th edition TNM staging system, which is commonly used to assess the extent of pancreatic cancer. This staging system is based on three key factors:
- T (Tumor): The size and extent of the primary tumor.
- N (Nodes): The involvement of regional lymph nodes.
- M (Metastasis): The presence of distant metastasis.
We categorized patients into two major groups:
- Stage I-III: This group included patients with resectable or borderline resectable disease. These patients were eligible for curative surgical resection, either through pancreaticoduodenectomy (for tumors located in the head of the pancreas) or distal pancreatectomy with splenectomy (for tumors located in the body or tail of the pancreas).
- Stage IV: This group comprised patients with unresectable, locally advanced, or metastatic disease. These patients either underwent palliative surgery or biopsy depending on the extent of the disease at the time of surgery.
Extreme values of baseline peripheral eosinophils count >0,4 G/l constituted 3,6% of all observations (Figure 1). They were excluded from the analyses sensitive to the outliers (correlations); but as this group was not statistically different from the rest of the study group (supplementary material), in terms of tested clinical data, these patients were analysed along others in U tests and survival analysis. We have decided not to involve PDAC patients undergoing surgical treatment after 2019 to ensure a sufficiently long follow-up as well as in purpose to avoid the influence of possible COVID-19 on the calculations.
Statistical analyses were performed using Statistica 13.1 software. Nominal variables were compared using the chi-square test, while continuous variables were analyzed with the Mann-Whitney U test and Spearman’s rank correlation. Survival medians were estimated through the Kaplan-Meier method. In the analysis of subgroups, differences in survival curves were evaluated with the log-rank test or its equivalent for multiple group comparisons. Cox proportional hazards regression was applied for survival analysis. Statistical significance was defined as p < 0.05 for all tests.
3. Results
The study group consisted of 58 subjects presenting baseline EOS<0,1 G/l (42,3%), 74 with EOS between 0,1 and 0,4 G/l (54,0%) and 5 patients with extremely high EOS>0,4 G/l (general characteristics of the study group is presented in Table 1). PDAC’s grade, localization, as well as patients’ sex, age, EOS and relative eosinophilia levels did not differ statistically significantly between the groups of stage I-III and IV (resectable vs. not resectable disease) while 6-, 12- and 24-months survival percentages were longer in stage I-III group, as expected (Table 2). There was no correlation between EOS vs. overall survival values in the stage IV group; while in the stage I-III group a weak but clearly visible correlation (R=0,24 and p= 0,060) was detectable (Figure 2). Subgroups according to EOS (<0,1 G/l vs. ≥0,1 G/l) also did not differ statistically significantly in the main clinical features terms (Table 3), but OS was longer in EOS ≥0,1 G/l group (respectively: 6-months survival: n=27; 46,6% vs. n=50; 63,29%, p=0,051; 12-months survival: n=16; 27,6% vs. 35; 44,30%, p=0,045; 24-months survival: n=2; 3,45% vs. n=14; 17,72%, p=0,011; Table 3). EOS status was also a statistically significant OS predictor both in univariate (HR=1,48; p=0,035; Table 4) and multivariate (HR=1,57; p=0,021; Table 5) Cox proportional hazard regression, along with the stage (respectively, HR=1,88; p=0,001 and HR=1,73; p=0,003). Dividing the whole study population according to stage and EOS status led to distinguishing Kaplan-Meier curves with p=0,024 (Table 6 and Figure 3) with median survival times: stage I-III, EOS≥0,1 G/l equal 14,5 months, for stage I-III, EOS <0,1 G/l - 8,0 months; for stage IV, EOS ≥0,1 G/l 7,0 months and stage IV, EOS <0,1 G/l - 5,0 months..
4. Discussion
4.1. Eosinophilia and Malignancies
The interpretation of blood eosinophilia causes problems, both in terms of normal range definition and its prognostic value for the risk of developing malignancies. Curran&Bertics in their publication regarding gliomas made some interesting observations: firstly, immunity of atopic conditions – high total IgE, IL-4 activation and in consequence eosinophil action may promote anticancer processes, thus, secondly, that there were some data published that are in line with that hypothesis; allergy, asthma and eczema diagnoses were associated with lower HR for glioma development (OR=0,34-0,96, dependent on the study) [19]. Andersen et al. performed a research of eosinophilia predictive value for solid cancer development in the Danish population. The researchers used The Copenhagen Primary Care Differential Count (CopDIFF) Data-base containing morphology test results from 626 157 adults from 2000 to 2010 and randomly chose 356 196 for statistical analysis. They investigated 3-year incidence of any solid tumor, which revealed that patients with eosinophils count between 0,5 – 1,0 G/l (mild eosinophilia) had 1,93 times higher risk of developing bladder cancer in comparison to no (<0,5 x 109/l) or severe (≥ 1,0 x 109/l) eosinophilia [18]. In another study they assessed the risk of 4-year all-cause mortality based on blood eosinophilia, revealing that it is the highest for eosinopenia, the lowest for individuals with EOS about 0,15 G/l and for higher values it increases proportionally to EOS level [19]. We have compared our results with the Andersen team’s findings (Figure 4). At the EOS level 0-0,1 G/l the two OR trend lines seem identical but with higher values a reverse trend is visible for PDAC patients.
The association between eosinophils concentration and OS was examined in several types of cancers. Alves et al. described eosinophilia >0,5 G/l to be a positive predictive factor for better outcomes (non-progression) in non-small cell lung cancer patients undergoing immunotherapy. Hypereosinophilia was also associated with higher risk of immune-related adverse effects such as asthenia, hypothyroidism, pneumonia and pruritus [16]. In a group of patients with various cancers (including PDAC), it was shown that survival (OS) is higher in the group of patients with eosinophilia. The occurrence of eosinophilia was associated with better disease control - each increase of 0,1 × 109/l in the number of eosinophils was associated with a 28% increase in the chance of better disease control. Additionally, eosinophilia was associated with a higher risk of treatment toxicity [20].
Ghebeh et al. investigated the association of eosinophil count with response to chemoimmunotherapy in advanced triple-negative breast cancer. Higher eosinophil count and increase in peripheral blood eosinophil count >0,3 G/l during the treatment was associated with better OS in this group of patients [17]. Meta-analysis authored by Hu et al. [21] summarized and proved the tumor-associated tissue eosinophilia (TATE) link to favorable clinical outcome, which was described as protective in: oral cancer [22,23], laryngeal cancer [24], nasopharyngeal cancer [25], colorectal cancer [26,27,28,29], esophageal cancer [30,31], Hodgkin’s lymphoma [32], gastric cancer [33], penile cancer [34], cervical cancer [35]; without prognostic significance in oral cancer [36] and bladder cancer [37] and as predictor of shorter OS in tongue cancer [38], head and neck cancer [39], laryngeal cancer [40,41], Hodgkin’s lymphoma [42,43] and cervical cancer [44]. Although the relation between TATE and tumor-associated blood eosinophilia (TABE) is not yet determined in patients with solid malignancies, it seems reasonable to assume that as it is adopted in eosinophilic asthma, TATE and TABE represent each other.
4.2. Eosinophilia in PDAC Patients
Despite the increasing number of reports on the role of eosinophilia in the development of cancer disease, pancreatic cancer is almost a blank page in this topic. The available literature is limited to some case reports [45,46,47,48,49] and retrospective studies by Holub [14], Abu-Shawer [49], Ohkuma [50] (Table 7).
Holub et al. analyzed the records of patients who had undergone External Beam Radiotherapy; the information about qualification to this regiment is lacking. The cuf-off point adopted was EOS 0,5 G/l with <0,5 subgroup of n=63 (95,5%) vs. >= 0,5 G/l n=3 (4,5%) and applying this division lead to no statistically important results in Cox proportional hazard regression for OS; while in progression free survival univariate Cox analysis EOS >=0,5 corresponded to good prognosis and the result was statistically significant (HR=0,25, p=0,024). Nevertheless, ELR (eosinophil to lymphocyte ratio), also analyzed by Holub et al. revealed to be a predictor for OS: with shorter survival associated with ELR <0,04 (univariate HR=3,33 p=0,001). This group constituted 13,6% of the whole study group and was characterized by EOS median=0,0 G/l (range= 0,0-0,1 G/l); which de facto corresponds to eosinopenia, and its poor prognosis is consistent with our study findings [14]. The study of Abu-Shawer et al. concentrated on detecting metastases; the cut-off point was chosen to predict their presence; despite this fact the results also seem to be in line with ours (worse prognosis for low EOS values) [49].
Ohkuma et al. reported that higher eosinophil counts and eosinophil-to-lymphocyte ratios were associated with improved survival in patients with stage II resectable PDAC. In contrast, our study examined the prognostic value of eosinophils across a broader range of stages (I-IV) and found that while eosinophilia (defined as EOS ≥ 0.1 G/l) was associated with better survival outcomes, the overall median survival times were shorter than those reported by Ohkuma et al. Several factors may account for this discrepancy:
- Patient Population: Our cohort included patients with both resectable (Stage I-III) and unresectable (Stage IV) PDAC, while Ohkuma et al. focused solely on resectable stage II patients. The inclusion of patients with advanced-stage disease in our study likely contributed to the overall shorter survival outcomes.
- Follow-up and treatment protocols: The duration of follow-up and the therapeutic approaches, such as adjuvant chemotherapy and radiation, varied between studies. In our cohort, patients with stage IV disease were more likely to have received palliative care, which could explain the shorter survival times observed. The specific treatment protocols followed by patients in the Ohkuma study were also not explicitly comparable to ours, potentially contributing to the differences in outcomes.
- Methodology: Differences in the statistical methodologies used may also explain the variation in survival data. While both studies used Cox proportional hazard models, the cutoff points for eosinophil levels and the variables included in the multivariate analyses differed. Ohkuma et al. used a cutoff of EOS < 0.126 G/l, while we used EOS < 0.1 G/l. Additionally, our study did not focus specifically on the eosinophil-to-lymphocyte ratio, which may further explain the differences in our results.
Despite these discrepancies, both studies reinforce the hypothesis that eosinophils may play a protective role in the immune response against pancreatic cancer. Our findings suggest that eosinophilia is associated with longer survival, particularly in earlier stages of PDAC, but further investigation is needed to fully understand the biological mechanisms underlying these observations [50].
Despite the shortcomings in methodology, all the papers report similar distribution of EOS values as well as matching direction of low EOS prognosis; also, hypereosinofilic patients’ status seems to be unclear (Holub et al. & current study). None of the previous studies proposed a hypothesis explaining the observations.
4.3. Anti-Eosinophil Treatment and the Risk of Developing Malignancy
The exact definitions of eosinopenia and hypereosinophilia vary between the laboratories and publications; in general eosinopenia is defined by no eosinophils detected in peripheral blood morphology test or low count near to 0 G/l, e.g.; 0 - 0,05 G/l or 0,01 G/l, while hypereosinophilia, a state of too high blood eosinophilia is defined as mild (0,5 - 0,15 G/l), moderate (0,15 - 5,0 G/l) or severe (>5,0 G/l) [50,51]. Normal range should be located in between, but as the knowledge about eosinophilic diseases evolves and the criteria for treatment follow, “the norm” conception becomes elusive and uncertain. Authors discuss whether the optimum criterium for anti-eosinophil treatment is EOS >0,3 G/l or 0,15 G/l; this should certainly be interpreted as an indication that the interpretation of blood counts will change in the near future and blood eosinophilia “the normal range” needs to be reestablished. Nevertheless, it is indisputable that in a state of eosinophilic inflammation (T2 inflammatory diseases like eosinophilic asthma, chronic rhinosinusitis etc.), even theoretically normal levels of eosinophils speak in favor of benefit from anti-eosinophil treatment, so in its essence it is the symptom of disease.
Conclusions from the studies investigating safety of anti-eosinophil therapies are also interesting. Benralizumab - a monoclonal antibody directed against the interleukin 5 α receptor, which causes a rapid, almost complete reduction in the number of eosinophils as a result of increased antibody-dependent cellular cytotoxicity and consequently causes eosinopenia in treated people. SIROCCO, CALIMA, ZONDA, BORA and MELTEMI studies on benralizumab use in patients with severe, uncontrolled eosinophilic asthma proved it was generally well-tolerated, with no apparent association between treatment and increased risks of infections or malignancies [51,52]. Mepolizumab as a humanized IgG1 kappa monoclonal antibody, directly binds to circulating IL-5 and reduces the number of eosinophils by inhibiting IL-5 signaling [53]; patients present substantially reduced blood eosinophilia. To analyze the long-term effects and safety of mepolizumab, a randomized, double-blind, placebo-controlled study was conducted with mepolizumab in adults with FIP1L1/PDGFRA-negative hypereosinophilic syndrome which also confirmed safety of anti-eosinophil therapy in the context of carcinogenesis; similarly in tests on subject with eosinophilic asthma [54]. These results, together with Andersen et al. studies strongly suggest that not blood eosinophilia per se, but the mechanism underneath it shall be blamed for the dismal prognosis of eosinopenia.
4.4. Therapeutic Potential
Until the mechanism laying underneath the favorable T2 inflammation-like immune response in PC cancer remains a mystery, there is room for exploring potential uses of this phenomenon. The results of PDAC treatment are poor. The 5-year survival rate is only 5%. This is due to the high aggressiveness of the cancer and its diagnosis at an advanced stage [55]. Neoadjuvant chemotherapy theoretically ensures tumor shrinkage, making it resectable, especially in initially borderline tumors, and affects micrometastases, sterilizing the area of surgery and improving surgical results [56]. However, the role of neoadjuvant chemotherapy in daily clinical practice remains undefined. A meta-analysis of articles covering a large group of patients revealed that neoadjuvant chemotherapy of resectable and borderline resectable PDAC prolongs OS (18 vs. 14,8 months), even though it reduces the percentage of resec-table tumors (66% vs. 81.3%). The study of Ghebeh et al. on triple-negative breast cancer revealed that high pretreatment eosinophilia and increase in peripheral blood eosinophil count >0,3 G/l during chemoimmunotheraphy was associated with better OS [17]. This phenomenon is worth exploring in the case of PC, as it has a potential to be a useful stratifier of the risk of neoadjuvant chemotherapy. Complete surgical treatment of PC is the most successful method of treatment. However, it is only possible in patients with the early stage of advancement [57]. In the light of our results, it seems that even after resection, determining the status of preoperative eosinophilia may be potentially useful in planning further chemotherapy, at least – also - to stratify the risk of short survival. Attempts to use immunotherapy in patients with PDAC have been unsuccessful. Studies of monoclonal antibodies used to treat other malignancies – ipilimumab, pembrolizumab, durvulumab, tremelimumab - have not given any positive results [58,59,60,61,62,63,64]. Probably in the case of PDAC the success of immunotherapy will lie in taking a different path of influencing immune reactions.
4.5. Curative versus Palliative Treatment
The extent of the surgical procedure varies between the curative (Stage I-III) and palliative (Stage IV) groups, making direct comparisons between them challenging. Indeed, patients undergoing curative surgery (e.g.; pancreaticoduodenectomy or distal pancreatectomy) have fundamentally different outcomes compared to those receiving palliative procedures aimed at symptom relief or biopsy.
The aim of the study is not intended to directly compare surgical outcomes, but rather to explore the prognostic value of peripheral eosinophil counts within each treatment cohort. We acknowledge that survival differences between these groups are significantly influenced by the nature of the surgery itself, as well as by disease stage and the patient’s overall health status.
The relatively small number of curative patients (n=72) over the 8-year period reflects the reality of PDAC, where only a minority of patients present with resectable disease at diagnosis. We understand that the small sample size limits the statistical power of our analysis, particularly when stratifying patients into further subgroups (stages I, II, and III). However, this study aims to offer preliminary insights into the potential role of eosinophils as a prognostic factor in pancreatic cancer, with the hope that future studies, potentially involving multicenter collaborations, can validate these findings with larger cohorts.
4.6. Study Limitations
Main weakness of this study is its retrospective character and following ambiguities which surely influence the results; nevertheless, its results seem to correspond with available literature data.
Another limitation of our study is the lack of detailed data regarding important prognostic factors such as adjuvant therapy. Adjuvant chemotherapy is well-established as a critical component of post-operative management in PDAC, often contributing to improved survival outcomes. Unfortunately, due to the retrospective nature of the study and the lack of uniform documentation in patient records, we were unable to include information on adjuvant therapies in our analysis.
As such, we recommend that future studies integrate both surgical and adjuvant therapy data to provide a more comprehensive analysis of survival outcomes and prognostic factors in PDAC patients. While retrospective analyses are often used as hypothesis-generating studies, we recognize that a prospective design would provide more reliable and controlled data. However, given the aggressive nature of PDAC and the relatively short survival time of many patients, conducting large-scale, long-term prospective studies remains a significant challenge.
5. Conclusions
Our results suggest that EOS >0,1 G/l or in other words, lack of eosinopenia in PDAC patients may be the prognostic factor for longer survival, but only in these individuals who undergo surgical resection. However, this is definitely the moment to discuss the type of immune response not only in inflammatory diseases but also in the case of solid cancers. Is type 2 inflammation a kind of double-edged sword, acting protectively but only until some decisive event occurs? Further studies are needed to shed light to this hypothesis.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Medical University of Lodz, Poland (protocol code: KE/826/23, 10.10.2023).
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
Data will be shared after a reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kolbeinsson, H.M.; Chandana, S.; Wright, G.P.; Chung, M. Pancreatic Cancer: A Review of Current Treatment and Novel Therapies. J. Investig. Surg. 2023, 36, 2129884. [Google Scholar] [CrossRef]
- Weyhe, D.; Obonyo, D.; Uslar, V.N.; Stricker, I.; Tannapfel, A. Predictive factors for long-term survival after surgery for pancreatic ductal adenocarcinoma: Making a case for standardized reporting of the resection margin using certified cancer center data. PLOS ONE 2021, 16, e0248633. [Google Scholar] [CrossRef]
- Yang, J.-J.; Hu, Z.-G.; Shi, W.-X.; Deng, T.; He, S.-Q.; Yuan, S.-G. Prognostic significance of neutrophil to lymphocyte ratio in pancreatic cancer: A meta-analysis. World J. Gastroenterol. 2015, 21, 2807–15. [Google Scholar] [CrossRef]
- Zhou, Y.; Cheng, S.; Fathy, A.H.; Qian, H.; Zhao, Y. Prognostic value of platelet-to-lymphocyte ratio in pancreatic cancer: a comprehensive meta-analysis of 17 cohort studies. OncoTargets Ther. 2018, 11, 1899–1908. [Google Scholar] [CrossRef]
- Andersen, C.L.; Siersma, V.D.; Hasselbalch, H.C.; Vestergaard, H.; Mesa, R.; Felding, P.; Olivarius, N.D.; Bjerrum, O.W. Association of the blood eosinophil count with hematological malignancies and mortality. Am. J. Hematol. 2014, 90, 225–229. [Google Scholar] [CrossRef]
- Majos, A.; Sewerynek, E.; Grząsiak, O.; Ciesielski, W.; Hogendorf, P.; Hołyński, J.; Strzelczyk, J.; Durczyński, A. FT3 to FT4 Conversion Ratio May Be an Independent Prognostic Factor in Pancreatic Cancer Patients. Biomedicines 2022, 11, 77. [Google Scholar] [CrossRef]
- Szmiel, A.; Majos, A.; Ciesielski, W.; Kumor, A.; Strzelczyk, J.; Szwedziak, K.; Hogendorf, P.; Durczyński, A. Gender-Specific Coagulation Profiles of Peripheral and Portal Blood May Help to Differentiate Malignant from Benign Pancreatic Tumour—Pilot Study. J. Clin. Med. 2022, 11, 1573. [Google Scholar] [CrossRef]
- Upparahalli Venkateshaiah, S.; Manohar, M.; Kandikattu, H.K.; Mishra, A. Experimental Modeling of Eosinophil-Associated Diseases. Methods Mol Biol. 2021; 2241, 275–291. [Google Scholar]
- Fettrelet, T.; Gigon, L.; Karaulov, A.; Yousefi, S.; Simon, H.U. The Enigma of Eosinophil Degranulation. International journal of molecular sciences 2021, 22, 7091. [Google Scholar] [CrossRef]
- Gurtner, A.; Gonzalez-Perez, I.; Arnold, I.C. Intestinal eosinophils, homeostasis and response to bacterial intrusion. Semin. Immunopathol. 2021, 43, 295–306. [Google Scholar] [CrossRef]
- Rodrigo-Muñoz, J.M.; Gil-Martínez, M.; Sastre, B.; del Pozo, V. Emerging Evidence for Pleiotropism of Eosinophils. Int. J. Mol. Sci. 2021, 22, 7075. [Google Scholar] [CrossRef]
- Jacobsen, E.A.; Jackson, D.J.; Heffler, E.; Mathur, S.K.; Bredenoord, A.J.; Pavord, I.D.; Akuthota, P.; Roufosse, F.; Rothenberg, M.E. Eosinophil Knockout Humans: Uncovering the Role of Eosinophils Through Eosinophil-Directed Biological Therapies. Annu. Rev. Immunol. 2021, 39, 719–757. [Google Scholar] [CrossRef] [PubMed]
- Simson, L.; Ellyard, J.I.; Dent, L.A.; Matthaei, K.I.; Rothenberg, M.E.; Foster, P.S.; Smyth, M.J.; Parish, C.R. Regulation of Carcinogenesis by IL-5 and CCL11: A Potential Role for Eosinophils in Tumor Immune Surveillance. J. Immunol. 2007, 178, 4222–4229. [Google Scholar] [CrossRef] [PubMed]
- Holub, K.; Conill, C. Unveiling the mechanisms of immune evasion in pancreatic cancer: may it be a systemic inflammation responsible for dismal survival? Clin Transl Oncol. 2020, 22, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Moreira, A.; Erdmann, M.; Uslu, U.; Vass, V.; Schuler, G.; Schuler-Thurner, B. Blood Eosinophilia Is an on-Treatment Biomarker in Patients with Solid Tumors Undergoing Dendritic Cell Vaccination with Autologous Tumor-RNA. Pharmaceutics 2020, 12, 210. [Google Scholar] [CrossRef] [PubMed]
- Alves, A.; Dias, M.; Campainha, S.; Barroso, A. Peripheral blood eosinophilia may be a prognostic biomarker in non-small cell lung cancer patients treated with immunotherapy. J. Thorac. Dis. 2021, 13, 2716–2727. [Google Scholar] [CrossRef]
- Ghebeh, H.; A Elshenawy, M.; AlSayed, A.D.; Al-Tweigeri, T. Peripheral Blood Eosinophil Count is Associated with Response to Chemoimmunotherapy in Metastatic Triple-Negative Breast Cancer. Immunotherapy 2022, 14, 189–199. [Google Scholar] [CrossRef]
- Andersen, C.L.; Siersma, V.D.; Hasselbalch, H.C.; Lindegaard, H.; Vestergaard, H.; Felding, P.; Olivarius, N.d.F.; Bjerrum, O.W. Eosinophilia in routine blood samples as a biomarker for solid tumor development – A study based on The Copenhagen Primary Care Differential Count (CopDiff) Database. Acta Oncol. 2014, 53, 1245–1250. [Google Scholar] [CrossRef]
- Curran, C.S.; Bertics, P.J. Eosinophils in glioblastoma biology. J. Neuroinflammation 2012, 9, 11. [Google Scholar] [CrossRef]
- Krishnan, T.; Tomita, Y.; Roberts-Thomson, R. A retrospective analysis of eosinophilia as a predictive marker of response and toxicity to cancer immunotherapy. Future Sci. OA, 2020; 6, FSO608. [Google Scholar]
- Hu, G.; Wang, S.; Zhong, K.; Xu, F.; Huang, L.; Chen, W.; Cheng, P. Tumor-associated tissue eosinophilia predicts favorable clinical outcome in solid tumors: a meta-analysis. BMC Cancer 2020, 20, 454. [Google Scholar] [CrossRef]
- Peurala, E.; Tuominen, M.; Löyttyniemi, E.; Syrjänen, S.; Rautava, J. Eosinophilia is a favorable prognostic marker for oral cavity and lip squamous cell carcinoma. APMIS 2018, 126, 201–207. [Google Scholar] [CrossRef]
- Dorta, R.G.; Landman, G.; Kowalski, L.P.; Lauris, J.R.P.; O Latorre, M.R.D.; Oliveira, D.T. Tumour-associated tissue eosinophilia as a prognostic factor in oral squamous cell carcinomas. Histopathology 2002, 41, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.C.; Bradley, P.J.; Griffin, N.R. Tumor-associated tissue eosinophilia and long-term prognosis for carcinoma of the larynx. Am. J. Surg. 1994, 168, 469–471. [Google Scholar] [CrossRef] [PubMed]
- Leighton, S.E.J.; Teo, J.G.C.; Leung, S.F.; Cheung, A.Y.K.; Lee, J.C.K.; van Hasselt, C.A. Prevalence and prognostic significance of tumor-associated tissue eosinophilia in nasopharyngeal carcinoma. Cancer 1996, 77, 436–440. [Google Scholar] [CrossRef]
- Harbaum, L.; Pollheimer, M.J.; Kornprat, P.; A Lindtner, R.; Bokemeyer, C.; Langner, C. Peritumoral eosinophils predict recurrence in colorectal cancer. Mod. Pathol. 2015, 28, 403–413. [Google Scholar] [CrossRef]
- Fernández-Aceñero, M.J.; Galindo-Gallego, M.; Sanz, J.; Aljama, A. Prognostic influence of tumor-associated eosinophilic infiltrate in colorectal carcinoma. Cancer 2000, 88, 1544–1548. [Google Scholar] [CrossRef]
- Nielsen HJ, Hansen U, Christensen IJ, Reimert CM, Brunner, N.; Moesgaard, F. Independent prognostic value of eosinophil and mast cell infiltration in colorectal cancer tissue. J Pathol. 1999, 189, 487–495. [CrossRef]
- Prizment, A.E.; Vierkant, R.A.; Smyrk, T.C.; Tillmans, L.S.; Lee, J.J.; Sriramarao, P.; Nelson, H.H.; Lynch, C.F.; Thibodeau, S.N.; Church, T.R.; et al. Tumor eosinophil infiltration and improved survival of colorectal cancer patients: Iowa Women’s Health Study. Mod. Pathol. 2016, 29, 516–527. [Google Scholar] [CrossRef]
- Zhang, Y.; Ren, H.; Wang, L.; Ning, Z.; Zhuang, Y.; Gan, J.; Chen, S.; Zhou, D.; Zhu, H.; Tan, D.; et al. Clinical Impact of Tumor-Infiltrating Inflammatory Cells in Primary Small Cell Esophageal Carcinoma. Int. J. Mol. Sci. 2014, 15, 9718–9734. [Google Scholar] [CrossRef]
- Ishibashi, S.; Ohashi, Y.; Suzuki, T.; Miyazaki, S.; Moriya, T.; Satomi, S.; Sasano, H. Tumor-associated tissue eosinophilia in human esophageal squamous cell carcinoma. Anticancer Res. 2006, 26, 1419–24. [Google Scholar] [PubMed]
- Hollander, P.; Rostgaard, K.; Smedby, K.E.; Molin, D.; Loskog, A.; de Nully Brown, P.; Enblad, G.; Amini, R.-M.; Hjalgrim, H.; Glimelius, I. An anergic immune signature in the tumor microenvironment of classical Hodgkin lymphoma is associated with inferior outcome. Eur. J. Haematol. 2018, 100, 88–97. [Google Scholar] [CrossRef]
- Iwasaki, K.; Torisu, M.; Fujimura, T. Malignant tumor and eosinophils: I. Prognostic significance in gastric cancer. Cancer 1986, 58, 1321–1327. [Google Scholar] [CrossRef] [PubMed]
- Ono, Y.; Ozawa, M.; Tamura, Y.; Suzuki, T.; Suzuki, K.; Kurokawa, K.; Fukabori, Y.; Yamanaka, H. Tumor-associated tissue eosinophilia of penile cancer. Int. J. Urol. Off. J. Jpn. Urol. Assoc. 2002, 9, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Bethwaite, P.B.; Holloway, L.J.; Yeong, M.L.; Thornton, A. Effect of tumour associated tissue eosinophilia on survival of women with stage IB carcinoma of the uterine cervix. . J. Clin. Pathol. 1993, 46, 1016–1020. [Google Scholar] [CrossRef] [PubMed]
- Tostes Oliveira D, Tjioe KC, Assao A, Sita Faustino SE, Lopes Carvalho A, Landman G, Kowalski LP. Tissue eosinophilia and its association with tumoral invasion of oral cancer. Int J Surg Pathol. 2009, 17, 244–249. [Google Scholar] [CrossRef]
- Flamm, J. Tumor-associated tissue inflammatory reaction and eosinophilia in primary superficial bladder cancer. Urology 1992, 40, 180–185. [Google Scholar] [CrossRef]
- Paz D, Chang KP, Kao HK, Lao WWK, Huang YC, Chang YL, Huang, Y. Clinical implications of tumor-associated tissue eosinophilia in tongue squamous cell carcinoma. Laryngoscope. 2018, 129, 1123–1129. [Google Scholar]
- Alrawi SJ, Tan D, Stoler DL, Dayton M, Anderson GR, Mojica P, Douglas W, Hicks W, Jr, Rigual, N, Loree, T. Tissue eosinophilic infiltration: a useful marker for assessing stromal invasion, survival and locoregional recurrence in head and neck squamous neoplasia. Cancer J. 2005, 11, 217–225.
- Ercan I, Cakir B, Basak T, Ozdemir, T, Sayin, I, Turgut, S. Prognostic significance of stromal eosinophilic infiltration in cancer of the larynx. Prognostic significance of stromal eosinophilic infiltration in cancer of the larynx. Otolaryngol Head Neck Surg. 2005, 132, 869–873.
- Sassier, A.M.; Mcclatchey, K.D.; Wolf, G.T.; Fisher, S.G. Eosinophilic infiltration in advanced laryngeal squamous cell carcinoma. Laryngoscope 1995, 105, 413–416. [Google Scholar] [CrossRef]
- Keresztes, K.; Szollosi, Z.; Simon, Z.; Tarkanyi, I.; Nemes, Z.; Illes, A. Retrospective analysis of the prognostic role of tissue eosinophil and mast cells in Hodgkin’s lymphoma. Pathol. Oncol. Res. 2007, 13, 237–242. [Google Scholar] [CrossRef]
- von Wasielewski R, Seth S, Franklin J, Fischer R, Hubner K, Hansmann ML, Diehl, V, Georgii, A. Tissue eosinophilia correlates strongly with poor prognosis in nodular sclerosing Hodgkin’s disease, allowing for known prognostic factors. Blood. 2000, 95, 1207–1213. [CrossRef]
- van Driel, W.J.; Hogendoorn, P.C.; Jansen, F.-W.; Zwinderman, A.H.; Trimbos, J.; Fleuren, G.J. Tumor-associated eosinophilic infiltrate of cervical cancer is indicative for a less effective immune response. Hum. Pathol. 1996, 27, 904–911. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, U.; Asti, D.; Saqib, A.; Mudduluru, B.M.; Ayaz, S.; Odaimi, M. Eosinophilia as the presenting sign in pancreatic cancer: an extremely rare occurrence. Postgrad. Med. 2017, 129, 399–401. [Google Scholar] [CrossRef] [PubMed]
- Haldane, J.H.; Kapoor, H.; Morris, J. Severe eosinophilia associated with a malignant islet cell tumour. CMAJ 1989, 140, 1061–1063. [Google Scholar]
- Hirata, J.; Koga, T.; Nishimura, J.; Ibayashi, H. Pancreatic carcinoma associated with marked eosinophilia: A case report. Eur. J. Haematol. 1987, 39, 462–466. [Google Scholar] [CrossRef]
- Checinska, Z. [A CASE OF SEVERE EOSINOPHILIA IN A CASE OF CANCER OF THE HEAD OF THE PANCREAS]. Pol Arch Med Wewn. 1964, 34, 1373–1376. [Google Scholar]
- Abu-Shawer, O.; Abu-Shawer, M.; Shurman, A.; Lattouf, A.; Haimour, A.; Hamdan, O.; Mansour, R.; Altamimi, T.; Al-Hussaini, M. The clinical value of peripheral immune cell counts in pancreatic cancer. PLOS ONE 2020, 15, e0232043. [Google Scholar] [CrossRef]
- Ohkuma, R.; Kubota, Y.; Horiike, A.; Ishiguro, T.; Hirasawa, Y.; Ariizumi, H.; Watanabe, M.B.; Onoue, R.B.; Ando, K.; Tsurutani, J.; et al. The Prognostic Impact of Eosinophils and the Eosinophil-to-Lymphocyte Ratio on Survival Outcomes in Stage II Resectable Pancreatic Cancer. Pancreas 2021, 50, 167–175. [Google Scholar] [CrossRef]
- FitzGerald, J.M.; Bleecker, E.R.; Bourdin, A.; Busse, W.W.; Ferguson, G.T.; Brooks, L.; Barker, P.; Martin, U.J. Two-Year Integrated Efficacy And Safety Analysis Of Benralizumab In Severe Asthma. J. Asthma Allergy 2019, ume 12, 401–413. [Google Scholar] [CrossRef]
- Jackson, D.J.; Korn, S.; Mathur, S.K.; Barker, P.; Meka, V.G.; Martin, U.J.; Zangrilli, J.G. Safety of Eosinophil-Depleting Therapy for Severe, Eosinophilic Asthma: Focus on Benralizumab. Drug Saf. 2020, 43, 409–425. [Google Scholar] [CrossRef]
- Ortega, H.G.; Liu, M.C.; Pavord, I.D.; Brusselle, G.G.; Fitzgerald, J.M.; Chetta, A.; Humbert, M.; Katz, L.E.; Keene, O.N.; Yancey, S.W.; et al. Mepolizumab Treatment in Patients with Severe Eosinophilic Asthma. N. Engl. J. Med. 2014, 371, 1198–1207. [Google Scholar] [CrossRef] [PubMed]
- Pavord, I.D.; Korn, S.; Howarth, P.; Bleecker, E.R.; Buhl, R.; Keene, O.N.; Ortega, H.; Chanez, P. Mepolizumab for severe eosinophilic asthma (DREAM): a multicentre, double-blind, placebo-controlled trial. Lancet 2012, 380, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Yeo, C.J.; Cameron, J.L.; Lillemoe, K.D. i wsp. Pancreaticoduodenectomy with or without distal gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma, part 2: randomized controlled trial evaluating survival, morbidity, and mortality. Ann. Surg. 2002, 236, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Versteijne, E.; Suker, M.; Groothuis, K.; Akkermans-Vogelaar, J.M.; Besselink, M.G.; Bonsing, B.A.; Buijsen, J.; Busch, O.R.; Creemers, G.-J.M.; van Dam, R.M.; et al. Preoperative Chemoradiotherapy Versus Immediate Surgery for Resectable and Borderline Resectable Pancreatic Cancer: Results of the Dutch Randomized Phase III PREOPANC Trial. J. Clin. Oncol. 2020, 38, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Kamisawa T, Wood LD, Itoi T, Takaori, K. Pancreatic cancer. Lancet 2016, 388, 73–85. [Google Scholar] [CrossRef]
- Royal, R.E.; Levy, C.; Turner, K.; Mathur, A.; Hughes, M.; Kammula, U.S.; Sherry, R.M.; Topalian, S.L.; Yang, J.C.; Lowy, I.; et al. Phase 2 Trial of Single Agent Ipilimumab (Anti-CTLA-4) for Locally Advanced or Metastatic Pancreatic Adenocarcinoma. J. Immunother. 2010, 33, 828–833. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Tykodi, S.S.; Chow, L.Q.M.; Hwu, W.-J.; Topalian, S.L.; Hwu, P.; Drake, C.G.; Camacho, L.H.; Kauh, J.; Odunsi, K.; et al. Safety and Activity of Anti-PD-L1 Antibody in Patients with Advanced Cancer. N. Engl. J. Med. 2012, 366, 2455–2465. [Google Scholar] [CrossRef]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; De Jesus-Acosta, A.; Delord, J.-P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of Pembrolizumab in Patients With Noncolorectal High Microsatellite Instability/Mismatch Repair–Deficient Cancer: Results From the Phase II KEYNOTE-158 Study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef]
- O’Reilly, E.M.; Oh, D.-Y.; Dhani, N.; Renouf, D.J.; Lee, M.A.; Sun, W.; Fisher, G.; Hezel, A.; Chang, S.-C.; Vlahovic, G.; et al. Durvalumab With or Without Tremelimumab for Patients With Metastatic Pancreatic Ductal Adenocarcinoma: A Phase 2 Randomized Clinical Trial. JAMA Oncol. 2019, 5, 1431–1438. [Google Scholar] [CrossRef]
- Aglietta, M.; Barone, C.; Sawyer, M.B.; Moore, M.J.; Miller, W.H., Jr.; Bagalà, C.; Colombi, F.; Cagnazzo, C.; Gioeni, L.; Wang, E.; et al. A phase I dose escalation trial of tremelimumab (CP-675,206) in combination with gemcitabine in chemotherapy-naive patients with metastatic pancreatic cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2014, 25, 1750–1755. [Google Scholar] [CrossRef]
- Renouf, D.J.; Knox, J.J.; Kavan, P.; Jonker, D.; Welch, S.; Couture, F.; Lemay, F.; Tehfe, M.; Harb, M.; Aucoin, N.; et al. LBA65 The Canadian Cancer Trials Group PA.7 trial: Results of a randomized phase II study of gemcitabine (GEM) and nab-paclitaxel (Nab-P) vs GEM, nab-P, durvalumab (D) and tremelimumab (T) as first line therapy in metastatic pancreatic ductal adenocarcinoma (mPDAC). Ann. Oncol. 2020, 31, S1195. [Google Scholar]
- Renouf, D.J.; Knox, J.J.; Kavan, P.; Jonker, D.; Welch, S.; Couture, F.; Lemay, F.; Tehfe, M.; Harb, M.; Aucoin, N.; et al. LBA65 The Canadian Cancer Trials Group PA.7 trial: Results of a randomized phase II study of gemcitabine (GEM) and nab-paclitaxel (Nab-P) vs GEM, nab-P, durvalumab (D) and tremelimumab (T) as first line therapy in metastatic pancreatic ductal adenocarcinoma (mPDAC). Ann. Oncol. 2020, 31, S1195. [Google Scholar]
Figure 1.
Baseline eosinophils count in peripheral blood distribution in the whole group (n=137).
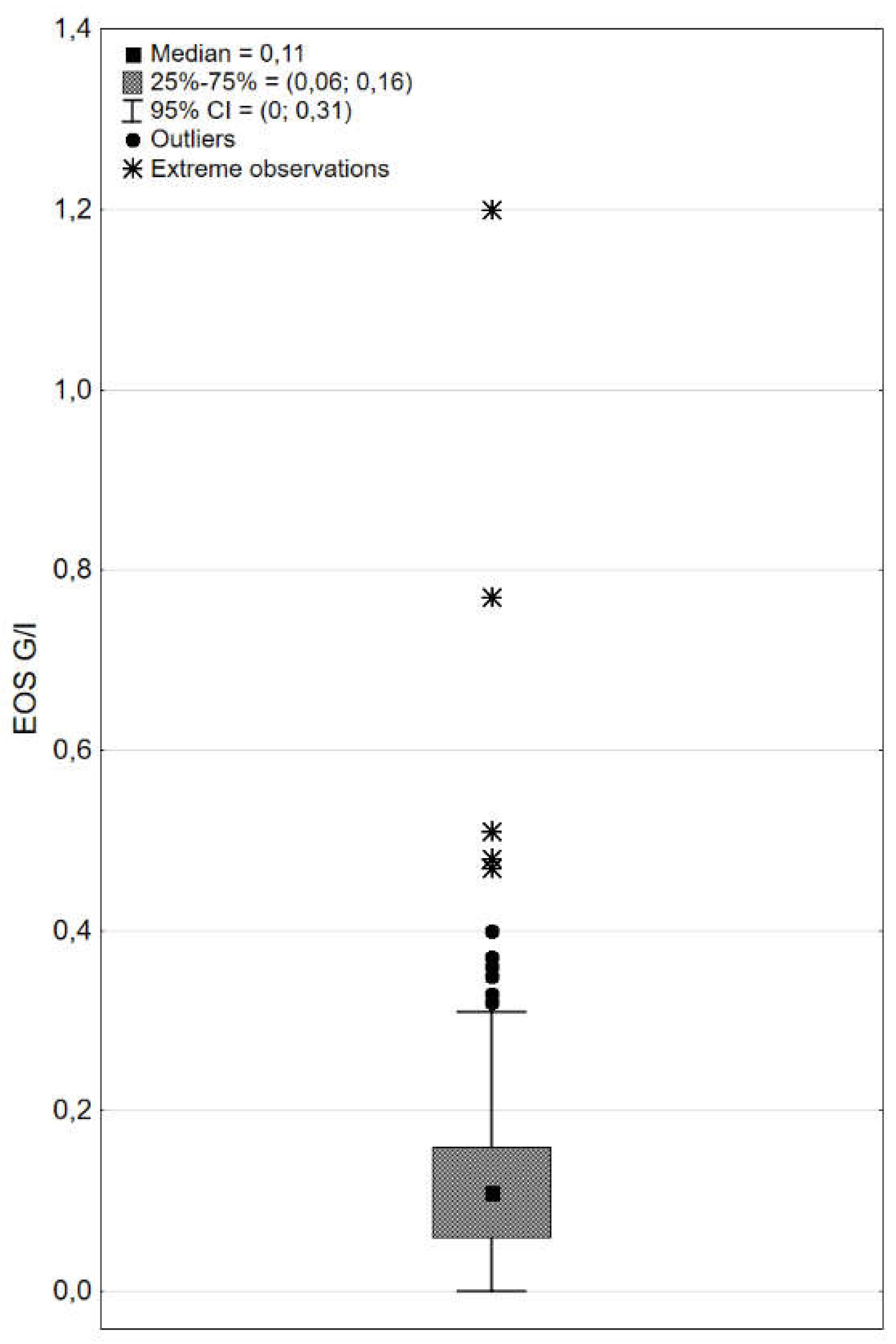
Figure 2.
Baseline peripheral eosinophils count vs. overall survival distribution, according to the stage. (a) stage I-III: Spearman’s R =0,24; p=0,060. (b) stage IV: Spearman’s R=0,07; p=0,578.
Figure 2.
Baseline peripheral eosinophils count vs. overall survival distribution, according to the stage. (a) stage I-III: Spearman’s R =0,24; p=0,060. (b) stage IV: Spearman’s R=0,07; p=0,578.
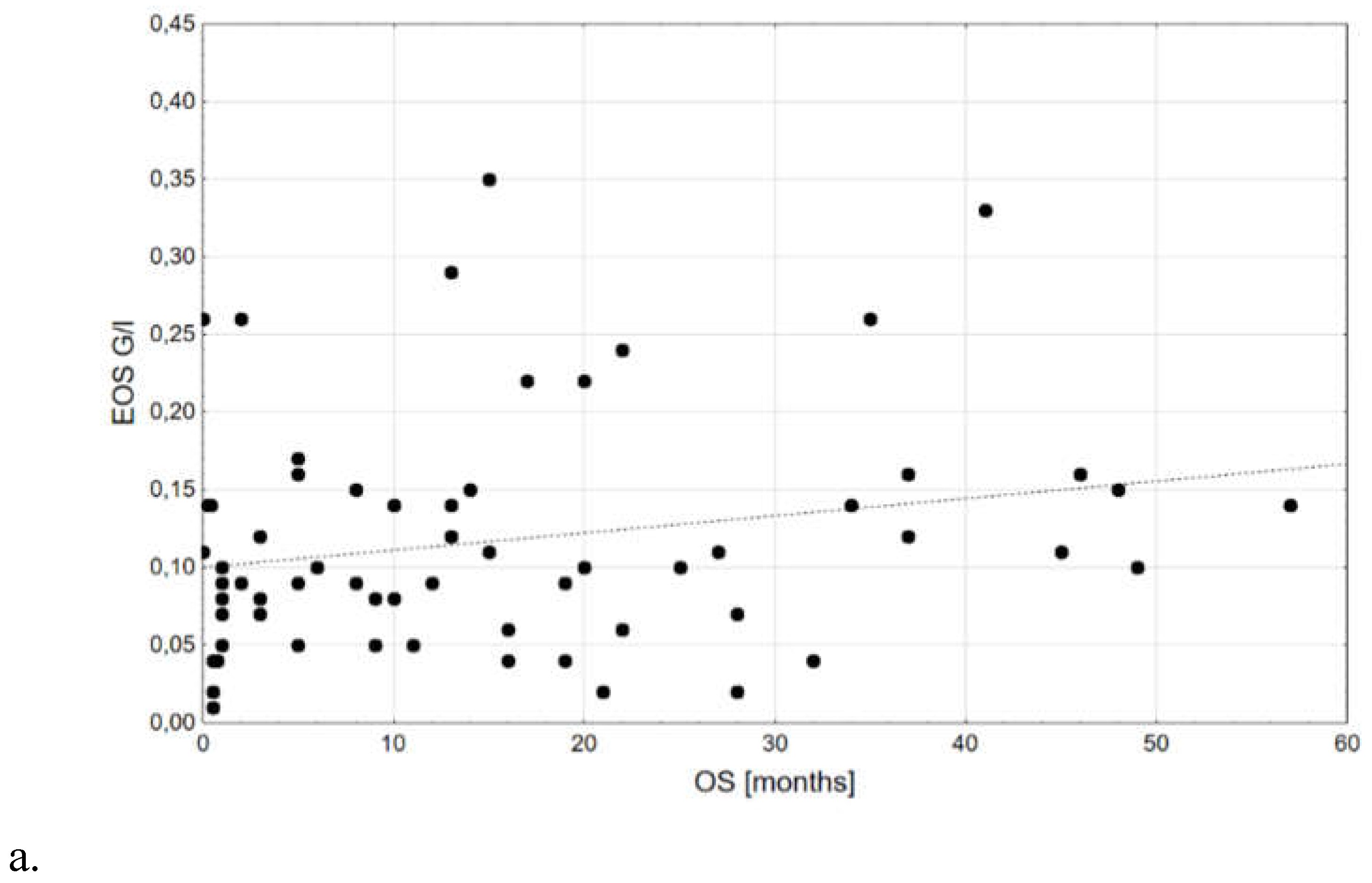
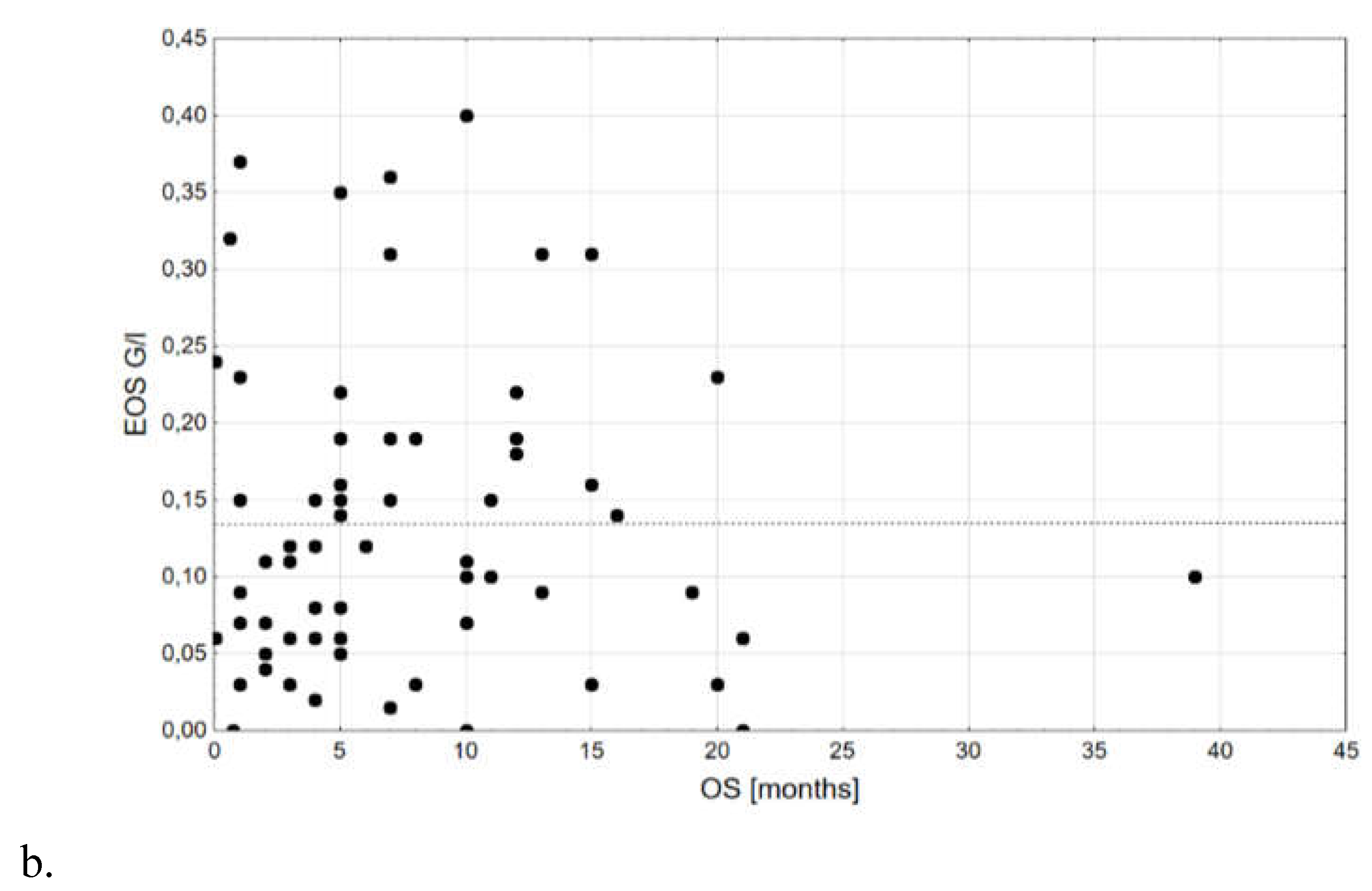
Figure 3.
Kaplan-Meyer curves for subgroups according to the stage and baseline peripheral eosinophils count [G/l]; p=0,024.
Figure 3.
Kaplan-Meyer curves for subgroups according to the stage and baseline peripheral eosinophils count [G/l]; p=0,024.
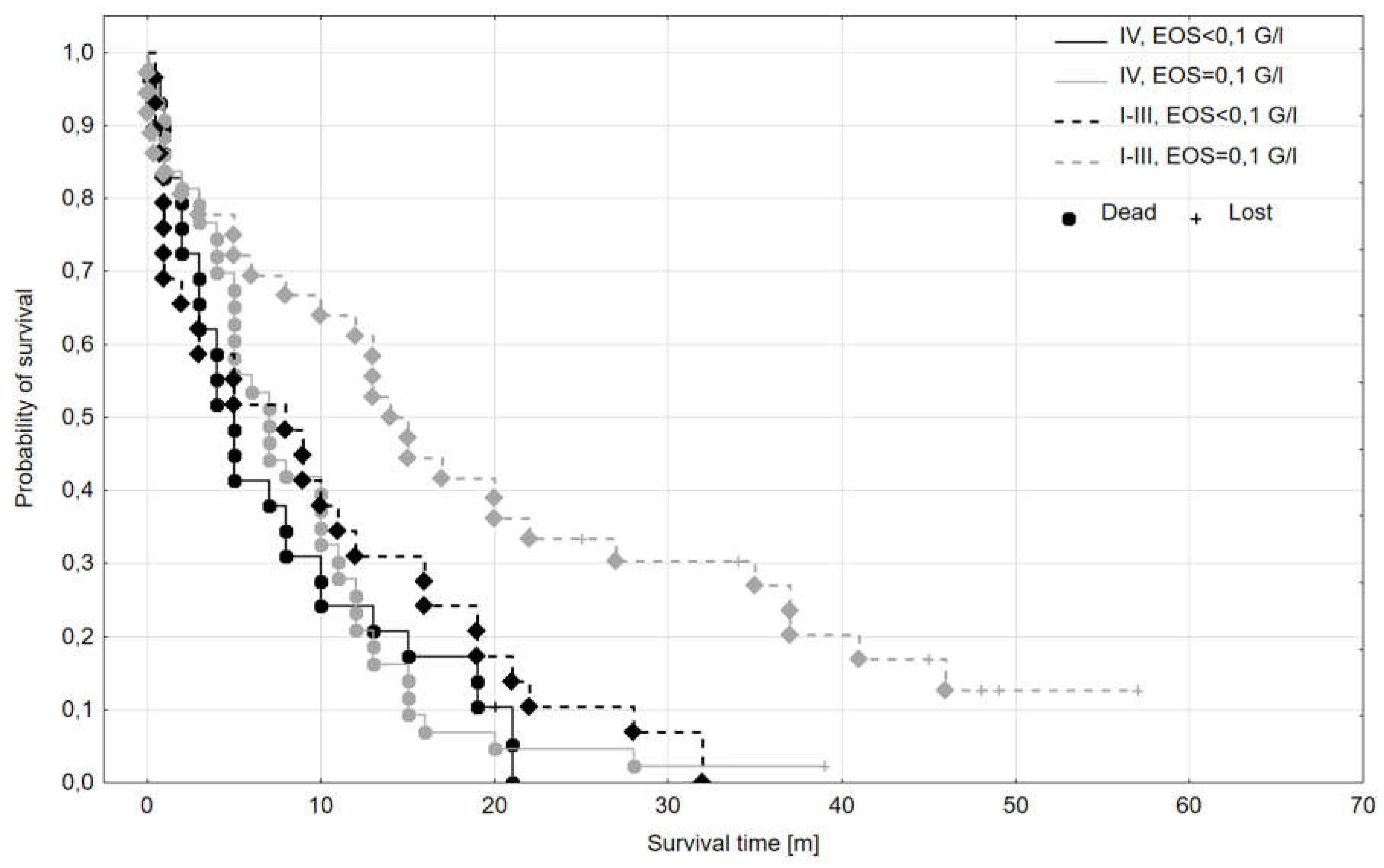
Figure 4.
Odds ratios for all-cause mortality: black line - 1-year all-cause mortality, current study; black histogram – blood eosinophilia values dispersion in current study; grey lines - 4-year all-cause mortality, Andersen et al.; grey histogram – blood eosinophilia values dispersion in Andersen et al. study; the histograms of blood eosinophilia are included for illustrative purposes - black for the current study, grey from Andersen et al. study [19].
Figure 4.
Odds ratios for all-cause mortality: black line - 1-year all-cause mortality, current study; black histogram – blood eosinophilia values dispersion in current study; grey lines - 4-year all-cause mortality, Andersen et al.; grey histogram – blood eosinophilia values dispersion in Andersen et al. study; the histograms of blood eosinophilia are included for illustrative purposes - black for the current study, grey from Andersen et al. study [19].
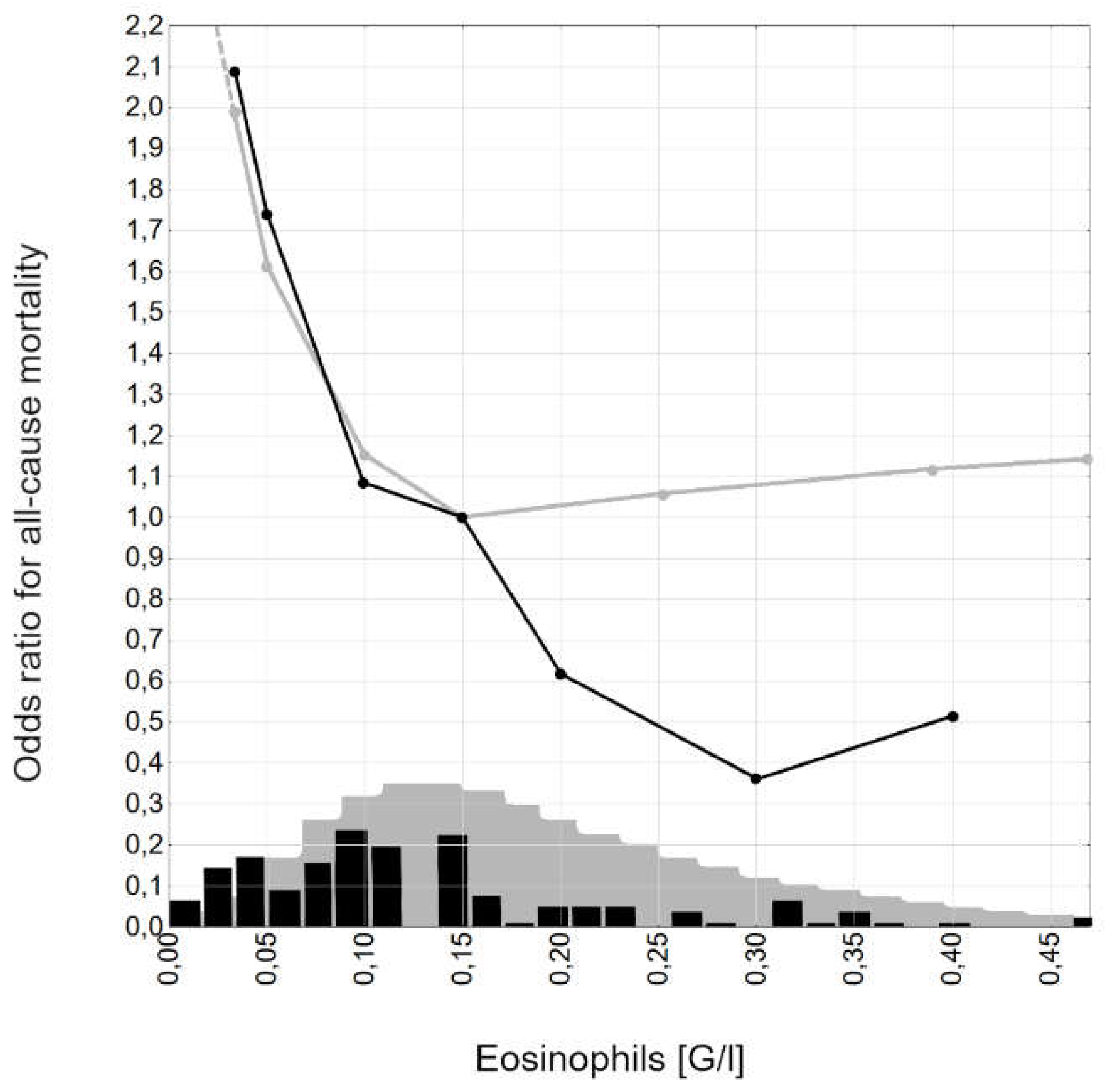

Table 1.
General characteristics of the study group.
| Parameter - nominal | N, % |
| Grade: 1 2 3 |
26; 19,0% 93; 67,9% 18; 13,1% |
| Tumor localization Head Body/tail |
98; 71,5% 39; 28,5% |
| Stage I-III IV |
65; 47,4% 72; 52,6% |
| Sex Female Male |
79; 57,7% 58; 42,3% |
| Survival 6-months 12-months 24-months |
58; 42,3% 74; 54,0% 5; 3,7% |
| Parameter – linear |
Mean ±SD; median; IQR; minimum; maximum |
| Age, years | 64,2±7,7; 65,0; 59,0-70,0; 46,0; 82,0 |
| EOS, G/l | 0,15±0,15; 0,11; 0,06-0,16; 0,00; 1,2 |
| Relative eosinophilia, % | 2,0±1,9; 1,6; 0,8-2,5; 0,0; 13,8 |
Table 2.
Characteristics of the subgroups according to the stage.
| Parameter - nominal |
Stage I-III N, % |
Stage IV N, % |
p |
| Grade: 1 2 3 |
11; 17,46% 45; 71,43% 7; 11,11% |
15; 21,74% 45; 65,22% 9; 13,04% |
0,743 |
| Tumor localization Head Body/tail |
46; 73,02% 17; 26,98% |
47; 68,12% 22; 31,88% |
0,537 |
| Sex Female Male |
29; 46,03% 34; 53,97% |
29; 42,03% 40; 57,97% |
0,644 |
| Survival 6-months 12-months 24-months |
40; 63,49% 31; 49,21% 14; 22,22% |
34; 49,28% 17; 24,64% 1; 1,45% |
0,100 0,003 0,000 |
| Parameter – linear |
Mean ±SD; median; IQR; minimum; maximum |
p | |
| Age, years | 64,0±7,8; 66,0; 58,0-70,0; 47,0; 82,0 | 54,6±7,4; 65,0; 61,0-71,0; 46,0; 78,0 | 0,149 |
| EOS, G/l | 0,18±0,08; 0,10; 0,06-0,15; 0,01; 0,35 | 0,13±0,10; 0,11; 0,06-0,19; 0,00; 0,40 | 0,773 |
| Relative eosinophilia, % | 1,69±1,14; 1,57; 0,94-2,19; 0,24; 5,77 | 1,89±1,42; 1,62; 0,72-2,53; 0,00; 7,67 | 0,773 |
Table 3.
Characteristics of the subgroups according to baseline peripheral eosinophils count.
| Parameter - nominal |
< 0,1 G/l N, % |
≥ 0,1 G/l N, % |
p |
| Grade: 1 2 3 |
9; 15,52% 44; 75,86% 5; 8,62% |
17; 21,52% 49; 62,03% 13; 16,46% |
0,207 |
| Tumor localization Head Body/tail |
40; 68,97% 18; 31,03% |
58; 73,42% 21; 26,58% |
0,568 |
| Stage I-III IV |
29; 50,00% 29; 50,00% |
36; 45,57% 43; 54,45% |
0,607 |
| Sex Female Male |
30; 51,72% 28; 48,28% |
49; 62,03% 30; 37,97% |
0,227 |
| Survival 6-months 12-months 24-months |
27; 46,6% 16; 27,6% 2; 3,45% |
50; 63,29% 35; 44,30% 14; 17,72% |
0,051 0,045 0,011 |
| Parameter – linear | Mean ±SD; median; IQR; minimum; maximum | ||
| Age, years | 63,8±8,6; 63,5; 58,0-70,0; 46,0; 81,0 | 64,5±7,0; 66,0; 59,0-70,0; 49,0; 82,0 | 0,663 |
| EOS, G/l | 0,05±0,03; 0,06 0,03-0,08; 0,0; 0,09 | 0,21±0,16; 0,15; 0,12-0,26; 0,10; 1,20 | 0,000 |
| Relative eosinophilia, % | 0,86±0,53; 0,76; 0,48-1,17; 0,00; 2,28 | 2,92±2,03; 2,35; 1,67-3,28; 0,97; 13,79 | 0,000 |
Table 4.
Univariate Cox regression parameters.
| Parameter | Effect level -reference level | p | HR | HR 95%CI |
|---|---|---|---|---|
| Grade | 1 - 3 | 0,177 | 0,53 | 0,28-1,00 |
| 2 - 3 | 0,134 | 0,54 | 0,12-0,93 | |
| Localization | Head – body/tail | 0,508 | 0,88 | 0,59-1,30 |
| Stage | IV - I-III | 0,001 | 1,88 | 1,29-2,75 |
| Sex | Female - male | 0,747 | 1,06 | 0,74-1,25 |
| Age>65 years | No - yes | 0,414 | 0,86 | 0,60-1,23 |
| EOS | <0,1 G/l - ≥0,1 G/l | 0,035 | 1,48 | 1,03-2,13 |
Table 5.
Multivariate Cox regression parameters.
| Parameter | Effect level -reference level | p | HR | HR 95%CI |
|---|---|---|---|---|
| Grade | 1 - 3 | 0,422 | 0,62 | 0,33-1,15 |
| 2 - 3 | 0,126 | 0,57 | 0,32-0,99 | |
| Localization | Head – body/tail | 0,427 | 1,18 | 0,79-1,76 |
| Stage | IV - I-III | 0,003 | 1,73 | 1,19-2,50 |
| Sex | Female - male | 0,933 | 1,01 | 0,71-1,45 |
| Age>65 years | No - yes | 0,360 | 0,84 | 0,59-1,21 |
| EOS | <0,1 G/l - ≥0,1 G/l | 0,021 | 1,57 | 1,07-2,31 |
Table 6.
Survival time parameters according to stage and EOS.
| Subgroup | Median OS [m] | Mean OS [m] | OS SD [m] | No. of complete observations | No. of lost observations | n total |
|---|---|---|---|---|---|---|
| I-III, EOS ≥0,1 G/l | 14,50 | 19,33 | 16,85 | 30 | 6 | 36 |
| I-III, EOS <0,1 G/l | 8,00 | 9,84 | 9,66 | 28 | 1 | 29 |
| IV, EOS ≥0,1 G/l | 7,00 | 8,57 | 7,56 | 42 | 1 | 43 |
| IV, EOS <0,1 G/l | 5,00 | 7,48 | 6,87 | 28 | 1 | 29 |
Table 7.
Characteristics of studies regarding EOS predictive value for OS in PDAC patients. N/A - not available.
Table 7.
Characteristics of studies regarding EOS predictive value for OS in PDAC patients. N/A - not available.
| Parameter | Holub | Abu-Shawer | Ohkuma | Current study |
|---|---|---|---|---|
| Year | 2020 | 2020 | 2021 | 2023 |
| Protocol | retrospective | retrospective | retrospective | retrospective |
| n | 66 | 355 | 67 | 137 |
| Subjects with distant meta included? | No | Yes | No | No |
| Resection status known | Yes | No | Yes | Yes |
| Chemotherapy | Yes | N/A | N/A | N/A |
| Radiotherapy | Yes | N/A | N/A | N/A |
| EOS: median; mean [G/l] | 0,1; 0,189 | 0,140; 0,190 | N/A | 0,11; 0,15 |
| Cut-off point | 0,5 | 0,143 | 0,126 | 0,1 |
| Result from univariate Cox regression | ≥0,5; HR 1,9 p=0,300 | ≥0,143 HR=0,9 p=0,54 | ≥0,126 HR=0,51 p=0,042 | <0,1: HR 1,48 p=0,035 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



