
Submitted:
29 September 2024
Posted:
30 September 2024
You are already at the latest version
Abstract
Background: Narcolepsy is characterized by excessive daytime sleepiness (EDS) and episodes of cataplexy, frequently triggered by psychological stress, significant disturbances in sleep-wake cycles, pregnancy, or trauma. Modafinil is widely used as the preferred treatment due to its effectiveness in alleviating EDS, improving disease outcomes, and enhancing overall quality of life. Nonetheless, long-term safety and efficacy data are still lacking, underscoring the importance of future research to advance treatment options for narcolepsy. Aim: In our systematic review and meta-analysis, we aim to assess the effectiveness of Modafinil in the treatment of Narcolepsy. Methods: We searched in electronic databases (PubMed, Embase, Google Scholar, Scopus, Science Direct, Web of Science) was performed to identify cohort studies and randomized controlled trials (RCTs) up to 8th July 2024. Data extraction focused on baseline characteristics of the included studies and efficacy outcomes, including scores on the Maintenance of Wakefulness Test (MWT) and Epworth Sleepiness Scale (ESS) . We performed the meta-analysis utilizing the Review Manager software, version 5.4. To assess the outcomes, we compared the Modafinil-treated group with the placebo group, employing the mean difference (MD) and a 95% confidence interval (CI) for statistical analysis. Result: In total, 3833 articles were identified for screening, with nine studies included in the systematic review and five in the meta-analysis. These studies involved 997 adult patients with Narcolepsy treated with Modafinil. MWT revealed a significant increase in total scores (MD= 3.56, 95% CI [2.25 to 4.86], p < 0.00001) and ESS revealed a significant decrease in scores (MD= -3.34, 95% CI [-4.13 to -2.56], p < 0.00001). Conclusion: The research emphasizes the potential of Modafinil in alleviating EDS associated with Narcolepsy. While the results are promising, they are based on short term scale studies. It is crucial to undertake larger-scale, extended-duration, placebo-controlled studies that include a broad range of demographic populations. These trials are essential to confirm the efficacy, verify the safety profile, and fine-tune dosing strategies to maximize the long-term therapeutic benefits.
Keywords:
Modafinil
; Narcolepsy
; Daytime sleepiness
; CNS stimulant
Introduction
Narcolepsy is a chronic neurological disorder that disrupts the sleep-wake cycle. It has a prevalence of approximately 0.05% and typically manifests within the first two decades of life [2], persisting throughout the patient’s lifetime. The condition significantly affects the patient’s quality of life, motor function, social interactions, occupational performance, mental health, and overall well-being, consequently impacting economic productivity, employment, daily functioning, and healthcare utilization [3]. Patients with narcolepsy have an increased mortality rate across all age groups compared to the general population. However, this mortality difference is less pronounced in older age groups, where the death rate rises in both narcoleptic and non-narcoleptic individuals [4].
The onset of narcolepsy symptoms has been linked to significant psychological stress, major alterations in sleep-wake patterns, pregnancy, and trauma [1]. Narcolepsy is primarily characterized by excessive daytime sleepiness (EDS) and cataplexy. EDS manifests as recurrent, irresistible episodes of daytime sleep, typically every 2 hours, particularly during periods of physical inactivity, such as watching television or driving [1]. It is marked by the premature onset of rapid eye movement (REM) sleep. In contrast, cataplexy, a hallmark of narcolepsy, is the sudden, involuntary onset of skeletal muscle weakness or paralysis during wakefulness, triggered by emotional stimuli, especially positive emotions like joy or laughter, and less commonly by anger or frustration [1]. The disorder has a strong genetic association with the HLA DQB1*0602 allele [5]. Its pathogenesis is linked to a reduction in catecholamines such as norepinephrine, dopamine, and serotonin in the brain, along with hypersensitivity of cholinergic receptors [7].
Narcolepsy is diagnosed using the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), and the International Classification of Sleep Disorders, Third Edition (ICSD-3) [6]. According to DSM-5 criteria, patients must experience EDS at least three times per week for the past three months, in addition to one of the following: 1) cataplexy; 2) cerebrospinal fluid (CSF) hypocretin deficiency; 3) REM sleep latency of ≤15 minutes on nocturnal polysomnography (PSG); or 4) a mean sleep latency of ≤8 minutes with ≥2 sleep-onset REM periods (SOREMPs) on multiple sleep latency testing (MSLT). ICSD-3 categorizes narcolepsy into type 1 and type 2. Narcolepsy type 1 requires daily EDS for ≥3 months and one or both of the following: 1) cataplexy with mean sleep latency ≤8 minutes and ≥2 SOREMPs on MSLT; or SOREMP (≤15 minutes after sleep onset) on preceding PSG, which may replace one of the SOREMPs on MSLT; 2) low or absent CSF hypocretin-1 levels. Narcolepsy type 2 requires EDS and MSLT findings as described above, but without cataplexy, and CSF hypocretin-1 levels are either unknown or above the threshold for type 1. The hypersomnolence and MSLT findings must not be attributable to other conditions, such as insufficient sleep, obstructive sleep apnea (OSA), delayed sleep phase disorder, or the effects of medications or substance use or withdrawal.
The treatment of narcolepsy includes both pharmacologic and non-pharmacologic approaches. Non-pharmacologic measures include maintaining good sleep hygiene and scheduling naps, which can help reduce unscheduled daytime sleep episodes [8,9,10]. However, most patients continue to rely on central nervous system (CNS) stimulants [10,11], and the evidence supporting naps alone for managing daytime sleepiness is limited [12]. A significant advancement in the pharmacotherapy of narcolepsy occurred in the 1930s when CNS stimulants, particularly amphetamines, were introduced to manage symptoms [13,14]. Over time, several drug classes, including stimulants, antidepressants, and hypnosedatives, have been explored for narcolepsy treatment. Currently, the American Academy of Sleep Medicine (AASM) strongly recommends the use of modafinil, pitolisant, sodium oxybate, and solriamfetol, with conditional recommendations for armodafinil, methylphenidate, and dextroamphetamine [15]. While all these agents reduce daytime sleepiness, only pitolisant, sodium oxybate, and dextroamphetamine have shown notable improvements in cataplexy [15].
Modafinil (2-[(diphenylmethyl)sulfinyl]acetamide) is a distinctive non-amphetamine CNS stimulant, first introduced in France in the 1980s for the treatment of central hypersomnias, including narcolepsy [16]. Its mechanism of action has been debated; it was initially thought to function as a central alpha-adrenergic agonist [16]. However, further studies revealed that modafinil does not bind to adrenergic or serotonergic receptors even at high concentrations [17]. In vitro studies in rat and canine brains demonstrated that modafinil binds to dopamine transporters (DAT), inhibiting reuptake and increasing dopamine levels in the striatum [18]. These findings were supported by positron emission tomography (PET) studies in humans, showing that modafinil decreases the binding of [11C] cocaine (a DAT radioligand) and [11C] raclopride (a D2/D3 radioligand) to endogenous receptors [19]. Prior to modafinil, amphetamines were the primary treatment for narcolepsy, but modafinil became preferred due to its lower risk of tolerance, abuse, and disruption of nocturnal sleep compared to amphetamines [20]. Common side effects of modafinil include insomnia, nausea, diarrhea, headache, and dry mouth [16]. Modafinil is used as a racemic mixture of R- and S-enantiomers. The R-enantiomer has a half-life three to four times longer than the S-enantiomer [21]. The R-enantiomer is marketed separately as armodafinil, which has a higher plasma concentration at the end of the day compared to modafinil, allowing for once-daily dosing, whereas modafinil typically requires twice-daily administration [21].
Modafinil is preferred as a primary treatment for narcolepsy due to its significant impact on reducing excessive daytime sleepiness, improving disease severity, and enhancing quality of life [16]. However, its effects on cataplexy remain inconclusive [8]. New alternatives to modafinil, such as flmodafinil/lauflumide and novel dopamine transporter inhibitor CE-123, are currently under investigation [22,23].
The existing evidence suggests that Modafinil is a viable treatment option for effectively managing narcolepsy with favorable tolerability. This systematic review and meta-analysis aim to provide a comprehensive evaluation of Modafinil’s effectiveness in reducing daytime sleepiness in individuals with narcolepsy.
Methods
This review focuses on clinical studies concerning the use of Modafinil in patients with Narcolepsy . We excluded animal studies and publications that only discussed the pathophysiology of Modafinil without presenting clinical data. The review follows the guidelines for Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) for 2020 in Figure 1, and only uses data collected from published papers, eliminating the need for ethical approval.
Systematic Literature Search and Study Selection
We conducted a thorough search for relevant publications by using PubMed (including Medline), Embase, Google Scholar, Scopus, Web of Science and Science Direct: We searched for studies mentioned in review papers, editorials, and commentaries on PubMed. Nevertheless, we continued searching for additional studies that satisfied our inclusion criteria.
We had a list of abstracts that we independently reviewed for inclusion using specific criteria. The criteria included the use of Modafinil, focusing on Narcolepsy. We excluded review papers and animal studies. Four reviewers conducted a dual review, and disagreements were resolved through discussion.
Inclusion and Exclusion Criteria
To meet the objectives of our study, we defined particular inclusion and exclusion criteria for participant selection. Our focus was solely on clinical trials and cohort studies. The PICOS framework (Population, Intervention, Comparison, and Outcome) guiding our selection was structured as follows:
- Population: adult patients diagnosed with Narcolepsy.
- Intervention: treatment with Modafinil.
- Comparison: placebo or no intervention.
- Outcome: excessive daytime sleepiness symptoms were measured by the Maintenance of Wakefulness Test (MWT) and Epworth Sleepiness Scale (ESS).
Other criterias can be summarized in Table 1.
Search Strategy
The population, intervention/condition, control/comparison, and outcome (PICO) criteria were utilized to conduct a thorough literature review. The search was conducted on databases such as PubMed (including Medline), Embase, Google Scholar, Scopus, Web of Science and Science Direct using relevant keywords, such as Modafinil, Narcolepsy and Wakefulness. The medical subject heading (MeSH) approach for PubMed (including Medline), Embase, Google Scholar, Scopus, Web of Science and Science Direct as detailed in Supplementary Table 1, was employed to develop a comprehensive search strategy.
Quality Appraisal
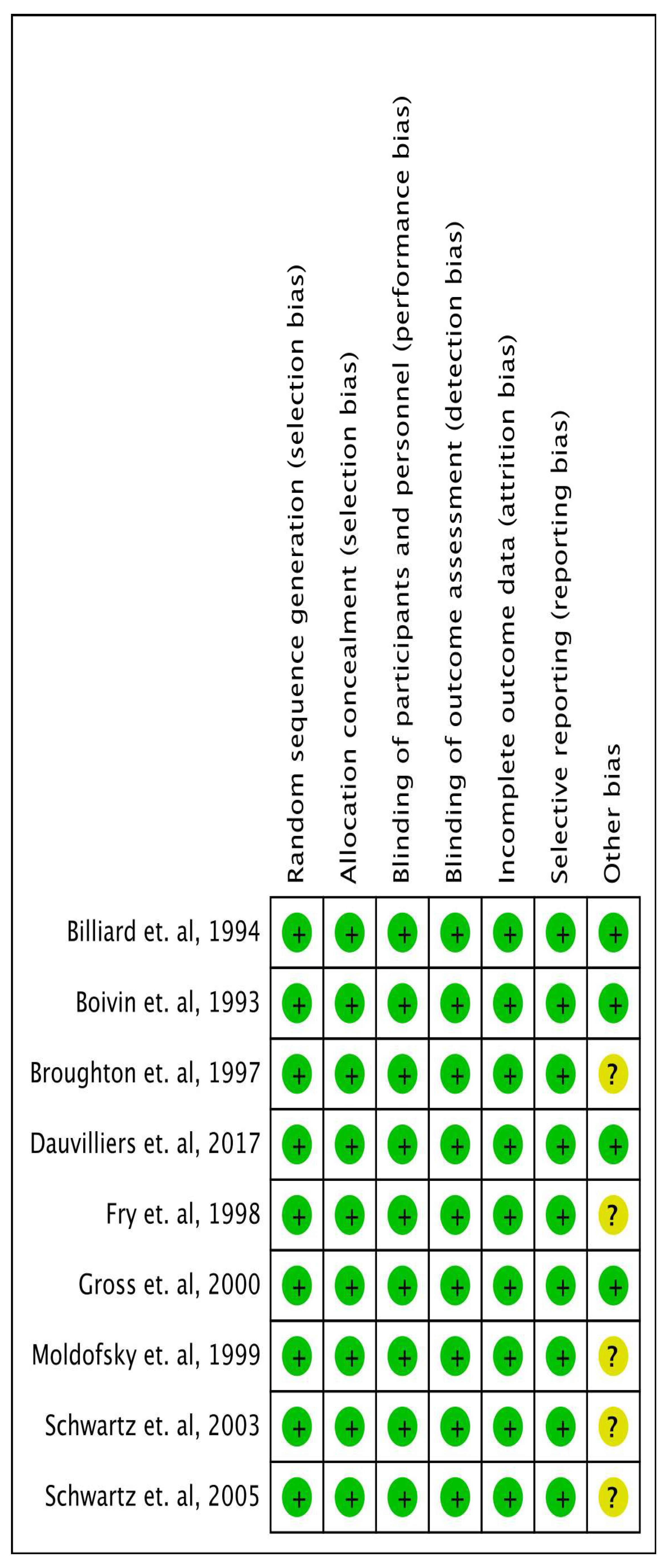
To ensure the reliability of our chosen papers, we utilized various quality assessment tools. For the chosen papers we employed the PRISMA checklist and Cochrane bias tool assessment for randomised clinical trials for systematic reviews and meta-analyses, as shown in Figure. 2.
Figure 2.
Risk of bias assessment of included studies.
Data Extraction and Outcome Measures
After the initial screening process, we gathered pertinent data using custom-designed extraction forms. Data extraction was carried out by three authors, with any discrepancies being resolved by two other authors. The collected information encompassed various aspects, including the study’s methodology, design, Modafinil dosage, participant demographics, levels of daytime sleepiness, and key findings ( Supplementary Table 2). The primary efficacy outcomes were evaluated using the MWT and ESS scores.
Meta-Analysis
For data analysis, we utilized Review Manager (RevMan) software, version 5.4. Continuous data were expressed as the mean difference between the Modafinil-treated group and the placebo, accompanied by a 95% confidence interval (CI). Statistical significance was defined by a p-value of ≤ 0.05. We assessed heterogeneity using the I-square statistic and its corresponding p-value. In accordance with the Cochrane Handbook’s guidelines for meta-analysis, we interpreted the I-square test as follows: 0–30% suggests low or no heterogeneity, 30–60% indicates moderate heterogeneity, 60–90% reflects substantial heterogeneity, and 75–100% signifies considerable heterogeneity, with a p-value < 0.05 considered statistically significant [26,27]. Given that some outcomes exhibited heterogeneity, we applied a random effects model to obtain a broader and more realistic confidence interval.
Results
After searching through six selected databases, PubMed (including Medline), Embase, Google Scholar, Scopus, Web of Science and Science Direct, we extracted 12,253 articles. We then carefully reviewed each paper and applied specific criteria, which led to excluding 1,311 articles. From the remaining 10,942 papers, we chose not to utilize 10,828 of them due to duplicates or unsatisfactory titles and abstracts. We closely examined the remaining 114 papers and excluded 105 more as their content did not meet our inclusion criteria.
Finally, we conducted a thorough quality check on the remaining nine papers, which all met our criteria. These nine articles are included in our final systematic review and five articles are included in meta-analysis. Table 2 provides a detailed description of each.

Table 2.
Summary of studies characteristics.
| Author, year | Country | Study Design | Number of patients | Intervention | Follow up duration | Conclusion |
|---|---|---|---|---|---|---|
| Moldofsky et. al, 2000 [35] | Canada | Randomised Double Blind Crossover study |
63 | Modafinil 500 mg daily dose during open label and were continued with either Modafinil or Placebo during double blind period. | 24 weeks | This study demonstrated that modafinil is effective and well-tolerated in the long-term treatment of EDS in narcoleptic patients. Over a 16-week open-label period, followed by a 2-week randomized, double-blind phase, patients on modafinil (mean dose 330 mg) showed a significant reduction in EDS. The MWT revealed a 70% longer sleep latency in the modafinil group compared to placebo. Similarly, the ESS scores were lower in the modafinil group, and episodes of severe somnolence and sleep were reduced. Importantly, no significant effects on nocturnal sleep, blood pressure, heart rate, ECG, or mood were observed, confirming the continued efficacy and safety of modafinil over the treatment period. |
| Billiard et. al, 1994 [28] | France | Randomized controlled, double blinded | 50 | Administration of Modafinil 300 mg | 12 weeks | The results showed no significant change in nighttime sleep duration, wake time, or number of awakenings. However, daytime sleepiness episodes significantly decreased, and total daytime sleep time reduced. No changes were noted in cataplexy or feelings upon awakening. Modafinil improved excessive daytime sleepiness as measured by the MWT. Side effects were lower with Modafinil compared to placebo. |
| Boivin et. al, 1993 [29] | France | Randomized Double blind crossover study | 10 | 4 weeks of either Modafinil 200 mg morning + 100 mg noon or Placebo | 12 weeks | The clinical evaluation by the sleep-disorder physician indicated that modafinil produced nonsignificant alerting effects. There was no change in the daily number of cataplectic attacks after modafinil treatment compared to placebo. However, modafinil significantly reduced the number of gaps and the percentage of errors on the Four-Choice Reaction Time Test (FCRTT) compared to placebo. Although a reduction in mean reaction time was observed during modafinil treatment, this change did not reach statistical significance. Modafinil did not produce any changes in nocturnal sleep parameters. Eight out of 10 narcoleptic patients had a pathological Periodic Limb Movement (PLM) index (>5). A nonsignificant reduction in both the number and index of PLMs was observed with modafinil compared to placebo. |
| Schwartz et. al, 2003 [31] | USA | Randomised Double Blind Crossover study | 32 | Modafinil 400 mg once daily / 400 mg split in split doses / 200 mg once daily. | 3 weeks | The study showed that split-dose regimens (400 mg and 600 mg) were significantly more effective in maintaining wakefulness in the late afternoon/evening compared to the 200 mg once-daily regimen. After 3 weeks, 60% of patients on the 400 mg split-dose regimen and 58% on the 600 mg split-dose regimen could stay awake for at least 20 minutes in the evening, compared to just 9% of patients on the 200 mg once-daily regimen. All regimens were well tolerated, with mild or moderate adverse events reported in 18% of participants. |
| Broughton et. al, 1997 [30] | Canada | Randomised Double Blind Crossover study | 75 | Placebo vs Modafinil 200 mg vs Modafinil 400 mg divided dose. | 6 weeks | The study found that modafinil effectively reduces EDS in patients with narcolepsy. Compared to placebo, the 200 mg and 400 mg doses increased sleep latency by 40% and 54%, respectively, on the MWT. Both doses significantly reduced the likelihood of falling asleep during daily activities, as measured by the ESS, with a reduction of 24% for 200 mg and 26% for 400 mg in involuntary sleep episodes and severe somnolence. Patients preferred modafinil over placebo, with 84% choosing modafinil as their best treatment, and side effects were more frequent with the 400 mg dose. The 200 mg dose was equally effective with fewer side effects, making it a well-tolerated option. |
| Fry et. al, 1997 [34] | USA | Randomized controlled, double blinded | 285 | Modafinil (400 mg) 100 mg×4 tablets daily or a placebo were given to participants during the double-blind phase. | 9 weeks | The study showed that Modafinil significantly improved subjective and objective measures of sleepiness, including the ESS and the Multiple Sleep Latency Test (MSLT). The mean sleep latency increased by up to 4 minutes in modafinil groups compared to placebo, and Clinical Global Impression scores also improved significantly in modafinil groups. Adverse effects were dose-dependent but mostly mild to moderate, with headache being the most common. The study demonstrated that modafinil is an effective and well-tolerated treatment for EDS in narcolepsy, with sustained efficacy over long-term use. |
| Gross et. al, 2000 [36] | USA | Randomized controlled, double blinded | 271 | Modafinil 200 mg once daily / modafinil 400 mg once daily / placebo | 9 weeks | The study showed that both dosages of modafinil significantly improved objective measures of EDS, as indicated by the MSLT and MWT. Specifically, the modafinil 400 mg group showed a mean MSLT sleep latency increase to 5.1 minutes compared to 3.5 minutes in the placebo group, and the MWT sleep latency was significantly extended at every follow-up visit. Subjective sleepiness also improved as reflected by the ESS. The treatment was well tolerated, with headache being the most common adverse effect, but its incidence was not significantly higher than that in the placebo group. The study concluded that modafinil is an effective and safe treatment option for managing EDS in narcolepsy, with no evidence of dependence or withdrawal symptoms over the treatment duration. |
| Schwartz et. al, 2005 [32] | USA | Randomized controlled, double blinded | 56 | Varying doses of modafinil (200 mg, 400 mg, 600 mg) in either once-daily or split-dose regimens. | 3 weeks | The study showed that split-dose regimens (400 mg and 600 mg) were significantly more effective in maintaining wakefulness in the late afternoon/evening compared to the 200 mg once-daily regimen. After 3 weeks, 60% of patients on the 400 mg split-dose regimen and 58% on the 600 mg split-dose regimen could stay awake for at least 20 minutes in the evening, compared to just 9% of patients on the 200 mg once-daily regimen. All regimens were well tolerated, with mild or moderate adverse events reported in 18% of participants. |
| Dauvilliers et. al, 2017 [33] | USA | Randomized controlled, double blinded | 155 | Sodium Oxybate 9 g nightly / Modafinil 200-600 mg once daily / their combination | 8 weeks | The post hoc analysis of polysomnography data from 155 patients revealed that SXB, alone or with modafinil, significantly reduced shifts from deep sleep stages (N2/3/REM) to light sleep or wakefulness. Sleep quality, measured using the Pittsburgh Sleep Quality Index, also improved significantly with SXB and SXB+modafinil, but not with modafinil alone. These results suggest that SXB has a specific effect on consolidating sleep and improving sleep quality, while modafinil alone had minimal impact on Distrupted nightime sleep (DNS). |
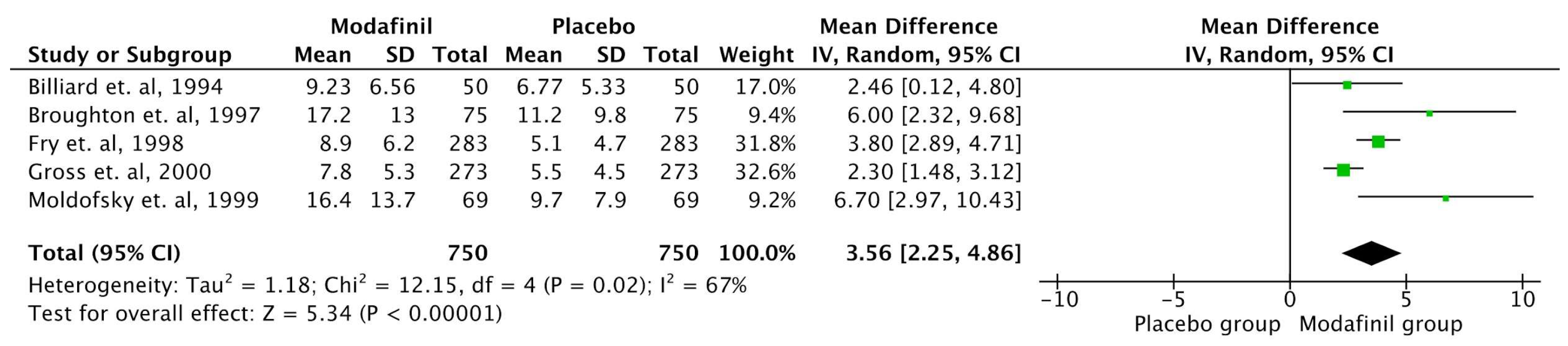
MWT
Five studies involving 750 patients utilized the MWT scale for outcome measurement. There was a significant increase in the MWT scale in the Modafinil treated group compared to placebo (MD= 3.56, 95% CI [2.25 to 4.86], p < 0.00001). Substantial heterogeneity was found across the outcome (Figure. 3). Sensitivity analysis was employed to address this heterogeneity in the MWT score outcome. There was a reduction in heterogeneity after removing the studies by Gross et al., [36] and Moldofsky et al. [35] (Supplementary Figure. 1). The reported heterogeneity was (p = 0.27, I-square = 23%). However, heterogeneity is not statistically significant (p > 0.05) [27].
Figure 3.
Analysis of the mean difference of MWT score between Modafinil group and Placebo group. (MWT = Maintenance of Wakefulness Test).
Figure 3.
Analysis of the mean difference of MWT score between Modafinil group and Placebo group. (MWT = Maintenance of Wakefulness Test).
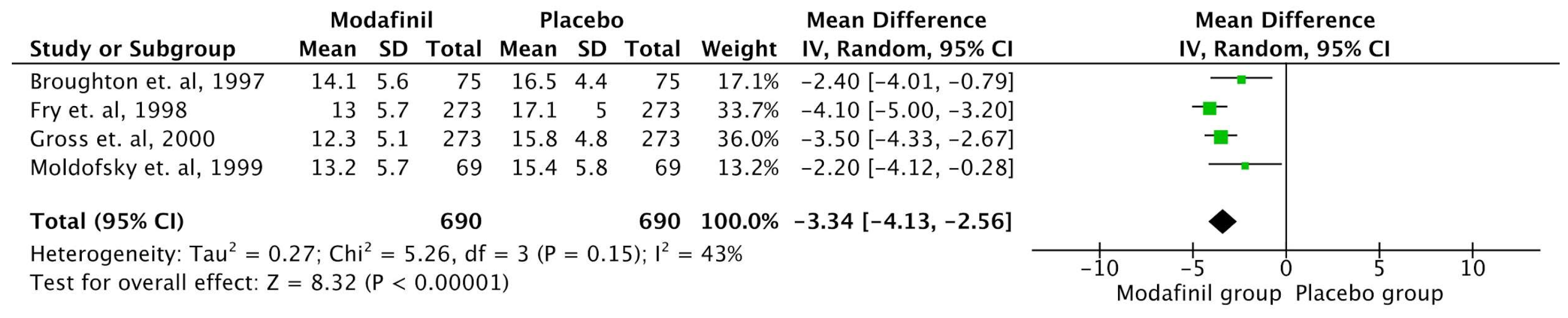
ESS
Four studies involving 690 patients utilized the ESS scale for outcome measurement. There was a significant reduction in the ESS scale in the Modafinil treated group compared to placebo (MD= -3.34, 95% CI [-4.13 to -2.56], p < 0.00001). Moderate heterogeneity was found across the outcome (Figure. 4). Sensitivity analysis was employed to address this heterogeneity in the ESS score outcome. There was a reduction in heterogeneity after removing the study by Fry et al. [34] (Supplementary Figure. 2). The reported heterogeneity was (p = 0.29, I-square = 18%). However, heterogeneity is not statistically significant (p > 0.05) [27].
Figure 4.
Analysis of the mean difference of ESS score between Modafinil group and Placebo group. (ESS = Epworth Sleepiness Scale).
Figure 4.
Analysis of the mean difference of ESS score between Modafinil group and Placebo group. (ESS = Epworth Sleepiness Scale).
Discussion
Narcolepsy is a chronic neurological disorder with profound social, economic, and health impacts [25]. The condition significantly impairs daily functioning, with excessive daytime sleepiness (EDS) and cataplexy leading to difficulties in maintaining employment, education, and personal relationships [37]. Individuals often face social isolation, stigma, and reduced quality of life due to their inability to control sleep episodes. Narcolepsy also places a substantial burden on healthcare systems, increasing costs associated with frequent medical visits and treatments. Effective management and increased public awareness are crucial to improving both social integration and clinical outcomes for affected individuals [38].
Modafinil, a non-amphetamine central nervous system (CNS) stimulant, plays a pivotal role in managing excessive daytime sleepiness (EDS) in narcolepsy. It enhances wakefulness by inhibiting dopamine reuptake through binding to dopamine transporters, leading to increased dopamine levels in the brain [39]. Compared to traditional stimulants like amphetamines, modafinil has a lower risk of tolerance, abuse, and disruption of nocturnal sleep [40]. It is well-tolerated, with common side effects including headache, nausea, and insomnia [41]. Modafinil’s efficacy in improving EDS has made it a first-line treatment for narcolepsy, significantly improving patients’ quality of life, though its effects on cataplexy remain inconclusive [42]. Its once-daily formulation, armodafinil, offers similar benefits with longer-lasting effects [43].
In our systematic review and meta-analysis, we assessed the efficacy of Modafinil in treating Narcolepsy, focusing on EDS. We analyzed data from nine studies encompassing 997 patients with Narcolepsy, with five studies included in our quantitative synthesis involving 750 patients. Our analysis revealed significant reductions in EDS, as measured by the MWT and ESS.
Multiple studies, including systematic reviews and meta-analyses, have consistently demonstrated the efficacy of modafinil in treating excessive daytime sleepiness (EDS) in narcolepsy. A meta-analysis reported significant improvements in wakefulness, attention, and overall functioning compared to placebo, with modafinil being well-tolerated in most patients [44]. Additionally, systematic reviews highlight modafinil’s superiority over traditional stimulants, such as amphetamines, due to its lower abuse potential and fewer side effects [41]. However, while modafinil effectively reduces EDS, its impact on cataplexy remains limited, necessitating adjunct therapies for comprehensive symptom management [45]. Overall, modafinil remains a cornerstone in narcolepsy treatment, improving patients’ quality of life and daily functioning [43].Meta-analyses indicate that Modafinil may confer benefits; however, further extensive, well-controlled studies are essential to ascertain the long-term safety and efficacy of this medication.
Our pooled analysis of the included studies showed significant increase in the MWT score in the Modafinil treated group compared to placebo. The study also demonstrated a decrease in ESS score among the group treated with modafinil compared to the placebo group. Notably, significant heterogeneity was observed among studies, which was mitigated by sensitivity analysis. The variability in study methodologies and designs, as well as the dosage of Modafinil, may contribute to the observed heterogeneity and complicate comparative studies.
Strengths and Limitations
The study employs a comprehensive search strategy across multiple databases, including PubMed, Embase, and Scopus, ensuring a broad inclusion of relevant studies. The use of standardized tools like PRISMA and the Cochrane bias tool for quality assessment enhances the reliability and rigor of the findings. Additionally, the study addresses heterogeneity through sensitivity analyses, allowing for more accurate conclusions despite variations in study methodologies and modafinil dosages.
Many clinical trials have relatively small sample sizes, which limit the generalizability of their findings. Additionally, most studies primarily focus on EDS without adequately addressing other critical symptoms such as cataplexy, which is less responsive to Modafinil. Long-term data on safety and efficacy remain sparse, with limited studies assessing outcomes beyond 12 months.The lack of comparative studies between modafinil and armodafinil in the treatment of narcolepsy significantly limits our understanding of their relative efficacy, side effects, and optimal therapeutic applications. Furthermore, systematic reviews often face heterogeneity in study designs, dosing regimens, and outcome measures, complicating direct comparisons and synthesis of results.
Conclusion
This study reaffirms Modafinil’s efficacy as a primary treatment for EDS in Narcolepsy. Across multiple studies, Modafinil significantly improved objective measures of wakefulness, such as the MWT, and reduced subjective sleepiness, as reflected in lower ESS scores, when compared to placebo. Modafinil’s favorable safety profile and lower risk of abuse compared to traditional stimulants further support its use. However, its limited efficacy in addressing cataplexy underscores the need for adjunct therapies in comprehensive narcolepsy management. The absence of comparative studies between modafinil and armodafinil in treating narcolepsy restricts our understanding of their relative efficacy and side effects. This gap hinders clinicians’ ability to make informed decisions, potentially impacting treatment outcomes for patients with narcolepsy. Overall, modafinil remains a well-tolerated and effective treatment, improving both daytime function and quality of life in narcoleptic patients. Further long-term studies are warranted to explore its extended safety and efficacy.
Ethical Approval
Not applicable.
Competing interests
The authors declare no competing interests.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
References
- Dauvilliers Y, Billiard M, Montplaisir J. Clinical aspects and pathophysiology of narcolepsy. Clin Neurophysiol. 2003 Nov;114(11):2000-17. [CrossRef] [PubMed]
- Thorpy MJ, Hiller G. The medical and economic burden of narcolepsy: Implications for managed care. Am Health Drug Benefits. 2017;10(5):233-41. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5620503/.
- Black J, Reaven NL, Funk SE, McGaughey K, Ohayon M, Guilleminault C, et al. The Burden of Narcolepsy Disease (BOND) study: Health-care utilization and cost findings. Sleep Med. 2014;15(5):522-9. [CrossRef]
- Ohayon MM, Black J, Lai C, Eller M, Guinta D, Bhattacharyya A. Increased mortality in narcolepsy. Sleep. 2014;37(3):439-44. [CrossRef]
- Longstreth WT Jr, Koepsell TD, Ton TG, Hendrickson AF, van Belle G. The epidemiology of narcolepsy. Sleep. 2007 Jan;30(1):13-26. [CrossRef] [PubMed]
- Ruoff C, Rye D. The ICSD-3 and DSM-5 guidelines for diagnosing narcolepsy: Clinical relevance and practicality. Curr Med Res Opin. 2016;32(10):1611-22. [CrossRef]
- . [CrossRef] [PubMed]
- Roehrs T, Zorick F, Wittig R, Paxton C, Sicklesteel J, Roth T. Alerting effects of naps in patients with narcolepsy. Sleep. 1986;9(1 Pt 2):194-9. [CrossRef] [PubMed]
- Rogers AE, Aldrich MS, Lin X. A comparison of three different sleep schedules for reducing daytime sleepiness in narcolepsy. Sleep. 2001 Jun 15;24(4):385-91. [CrossRef] [PubMed]
- Garma L, Marchand F. Non-pharmacological approaches to the treatment of narcolepsy. Sleep. 1994 Dec;17(8 Suppl):S97-102. [CrossRef] [PubMed]
- Rogers AE. Problems and coping strategies identified by narcoleptic patients. J Neurosurg Nurs. 1984 Dec;16(6):326-34. [CrossRef] [PubMed]
- Maski K, Trotti LM, Kotagal S, Robert Auger R, Swick TJ, Rowley JA, Hashmi SD, Watson NF. Treatment of central disorders of hypersomnolence: an American Academy of Sleep Medicine systematic review, meta-analysis, and GRADE assessment. J Clin Sleep Med. 2021 Sep 1;17(9):1895-1945. [CrossRef] [PubMed] [PubMed Central]
- DOYLE JB, DANIELS LE. SYMPTOMATIC TREATMENT FOR NARCOLEPSY. JAMA. 1931;96(17):1370–1372. [CrossRef]
- PRINZMETAL M, BLOOMBERG W. THE USE OF BENZEDRINE FOR THE TREATMENT OF NARCOLEPSY. JAMA. 1935;105(25):2051–2054. [CrossRef]
- Maski K, Trotti LM, Kotagal S, Robert Auger R, Rowley JA, Hashmi SD, Watson NF. Treatment of central disorders of hypersomnolence: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2021 Sep 1;17(9):1881-1893. [CrossRef] [PubMed] [PubMed Central]
- Bastuji H, Jouvet M. Successful treatment of idiopathic hypersomnia and narcolepsy with modafinil. Prog Neuropsychopharmacol Biol Psychiatry. 1988;12(5):695-700. [CrossRef] [PubMed]
- Mignot E, Nishino S, Guilleminault C, Dement WC. Modafinil binds to the dopamine uptake carrier site with low affinity. Sleep. 1994 Aug;17(5):436-7. [CrossRef] [PubMed]
- Wisor JP, Nishino S, Sora I, Uhl GH, Mignot E, Edgar DM. Dopaminergic role in stimulant-induced wakefulness. J Neurosci. 2001 Mar 1;21(5):1787-94. [CrossRef] [PubMed] [PubMed Central]
- Volkow ND, Fowler JS, Logan J, Alexoff D, Zhu W, Telang F, Wang GJ, Jayne M, Hooker JM, Wong C, Hubbard B, Carter P, Warner D, King P, Shea C, Xu Y, Muench L, Apelskog-Torres K. Effects of modafinil on dopamine and dopamine transporters in the male human brain: clinical implications. JAMA. 2009 Mar 18;301(11):1148-54. [CrossRef] [PubMed] [PubMed Central]
- Mitler MM, Aldrich MS, Koob GF, Zarcone VP. Narcolepsy and its treatment with stimulants. ASDA standards of practice. Sleep. 1994 Jun;17(4):352-71. [PubMed]
- Darwish M, Kirby M, Hellriegel ET, Robertson P Jr. Armodafinil and modafinil have substantially different pharmacokinetic profiles despite having the same terminal half-lives: analysis of data from three randomized, single-dose, pharmacokinetic studies. Clin Drug Investig. 2009;29(9):613-23. [CrossRef] [PubMed]
- Luca G, Bandarabadi M, Konofal E, Lecendreux M, Ferrié L, Figadère B, Tafti M. Lauflumide (NLS-4) Is a New Potent Wake-Promoting Compound. Front Neurosci. 2018 Aug 15;12:519. [CrossRef] [PubMed] [PubMed Central]
- Spreitzer I, Keife J, Strasser T, Kalaba P, Lubec J, Neuhaus W, Lubec G, Langer T, Wackerlig J, Loryan I. Pharmacokinetics of Novel Dopamine Transporter Inhibitor CE-123 and Modafinil with a Focus on Central Nervous System Distribution. Int J Mol Sci. 2023 Nov 29;24(23):16956. [CrossRef] [PubMed] [PubMed Central]
- 24. Erman M, Emsellem H, Black J, Mori F, Mayer G. Correlation between the Epworth Sleepiness Scale and the Maintenance of Wakefulness Test in patients with narcolepsy participating in two clinical trials of sodium oxybate. Sleep medicine. 2017 Oct 1;38:92-5.
- Johns MW. A new method for measuring daytime sleepiness: the Epworth Sleepiness Scale. Sleep. 1991 Dec;14(6):540-5.
- 26. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane Handbook for Systematic Reviews of Interventions. 2nd ed. Chichester (UK): John Wiley & Sons; 2019.
- Deeks JJ, Higgins JP, Altman DG, Cochrane Statistical Methods Group. Analysing data and undertaking meta-analyses. Cochrane Handbook for Systematic Reviews of Interventions. 2019 Sep 23:241–84.
- Billiard M, Besset A, Montplaisir J, Laffont F, Goldenberg F, Weill JS, Lubin S. Modafinil: a double-blind multicentric study. Sleep. 1994 Dec 1;17(suppl_8):S107-12.
- Boivin DB, Montplaisir J, Petit D, Lambert C, Lubin S. Effects of modafinil on symptomatology of human narcolepsy. Clinical neuropharmacology. 1993 Feb 1;16(1):46-53.
- Moldofsky H, Morehouse RL. Randomized, double-blind, placebo-controlled crossover trial of rnodafinil in the treatment of excessive daytime sleepiness in narcolepsy. Neurology. 1997;49:444451.
- Schwartz JR, Feldman NT, Bogan RK, Nelson MT, Hughes RJ. Dosing regimen effects of modafinil for improving daytime wakefulness in patients with narcolepsy. Clinical neuropharmacology. 2003 Sep 1;26(5):252-7.
- Schwartz JR, Feldman NT, Bogan RK. Dose effects of modafinil in sustaining wakefulness in narcolepsy patients with residual evening sleepiness. The Journal of neuropsychiatry and clinical neurosciences. 2005 Aug;17(3):405-12.
- Dauvilliers Y, Roth T, Guinta D, Alvarez-Horine S, Dynin E, Black J. Effect of sodium oxybate, modafinil, and their combination on disrupted nighttime sleep in narcolepsy. Sleep medicine. 2017 Dec 1;40:53-7.
- Fry, US Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil for the treatment of pathological somnolence in narcolepsy. Annals of Neurology. 1998 Jan;43(1):88-97.
- Moldofsky H, Broughton RJ, Hill JD. A randomized trial of the long-term, continued efficacy and safety of modafinil in narcolepsy. Sleep medicine. 2000 Apr 1;1(2):109-16.
- US Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil as a treatment for the excessive daytime somnolence of narcolepsy. Neurology. 2000 Mar 14;54(5):1166-75.
- Bassetti CL, Adamantidis A, Burdakov D, Han F, Gay S, Kallweit U, et al. Narcolepsy—clinical spectrum, aetiopathophysiology, diagnosis and treatment. Lancet Neurol. 2019 Oct;18(10):999-1012.
- Thorpy MJ, Dauvilliers Y. Narcolepsy in the modern era: Advances in pathophysiology, diagnosis, and treatment. Nat Rev Dis Primers. 2017 Mar 23;3:16100.
- Minzenberg MJ, Carter CS. Modafinil: A review of neurochemical actions and effects on cognition. Neuropsychopharmacology. 2008 Jun;33(7):1477-502.
- Thorpy MJ, Westbrook PR, Ferber R, et al. The clinical use of modafinil in treatment of narcolepsy: Implications for the clinician. Sleep Med Rev. 2001 Dec;5(6):483-509.
- Ballon JS, Feifel D. A systematic review of modafinil: Potential clinical uses and mechanisms of action. CNS Drug Rev. 2006;12(3-4):207-38.
- Morgenthaler TI, Kapur VK, Brown T, et al. Practice parameters for the treatment of narcolepsy and other hypersomnias of central origin. Sleep. 2007 Dec;30(12):1705-11.
- Schwartz JR, Feldman NT, Bogan RK, et al. Armodafinil for excessive sleepiness associated with shift work disorder or obstructive sleep apnea: A 12-month, open-label extension study. Clin Pharmacol Drug Dev. 2013 Oct;2(4):281-90.
- Veatch OJ, Goldman SE, Adkins KW, Malow BA. Efficacy of modafinil in the treatment of narcolepsy: A meta-analysis. J Clin Sleep Med. 2005 Dec;1(4):331-6.
- Morgenthaler TI, Kapur VK, Brown T, et al. Practice parameters for the treatment of narcolepsy and other hypersomnias of central origin. Sleep. 2007 Dec;30(12):1705-11.
Figure 1.
PRISMA 2020 flow chart representing the screening and selection of studies. (PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analysis).
Figure 1.
PRISMA 2020 flow chart representing the screening and selection of studies. (PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analysis).
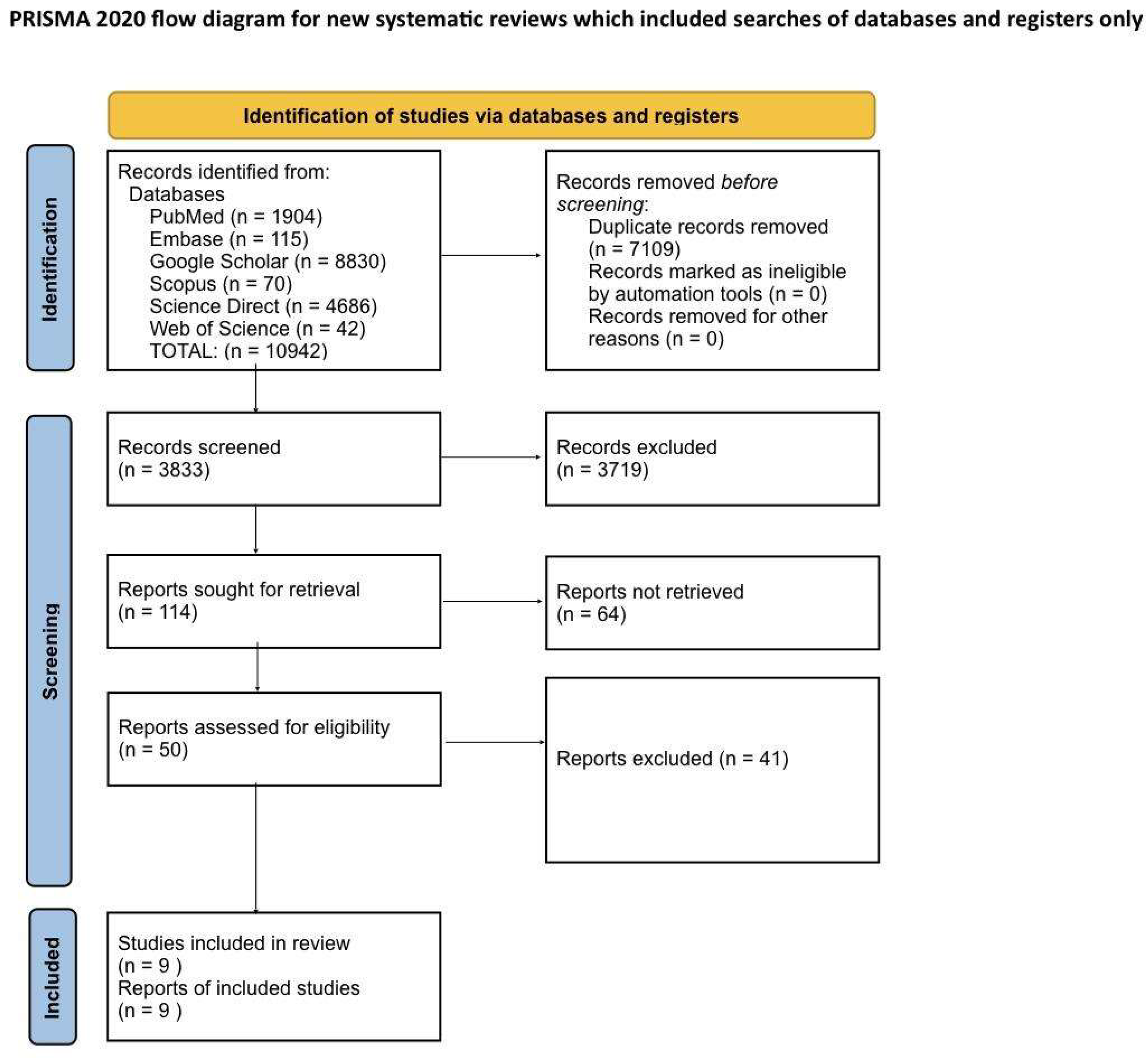
Table 1.
Inclusion and Exclusion criteria.
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Human Studies | Animal Studies |
| From 1990 to 2024 | Only pathophysiology /methodological studies with no outcome data |
| English text | Non-English text |
| Gender: All | Age: <18 years of age |
| Age: >18 years of age | Papers that needed to be purchased |
| Free papers | Studies involving clinical data other than Narcolepsy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



