
Submitted:
27 September 2024
Posted:
30 September 2024
You are already at the latest version
Abstract
Delirium and agitation are common and challenging issues in the intensive care unit (ICU), leading to longer hospital length of stay, prolonged need of mechanical ventilation, and higher costs. These conditions also increase the risk of complications and mortality. In the ICU setting it is common to observe an inappropriate use of sedatives and antipsychotics to manage agitation without an accurate diagnosis. Although the Richmond Agitation-Sedation Scale (RASS) has improved the reliability, accuracy, and specificity of delirium diagnosis, it is important to consider that delirium may be a symptom caused by a variety of diseases and medical conditions like sepsis rather than just a neurological problem. Antipsychotics, such as quetiapine, are often used in the ICU to manage these symptoms effectively. Quetiapine is a particularly valuable therapeutic option because of its capability to reduce agitation and delirium without significantly affecting the respiratory function, making it a safer choice for critically ill patients. This review explores quetiapine’s pharmacodynamics, side effects, efficacy, and recently described uses in the ICU. A comprehensive search was conducted across six major databases, and articles were assessed based on their relevance and quality. Our findings aim to provide a clear understanding of the application of quetiapine and its potential value in critical care settings.
Keywords:
delirium
; quetiapine
; ICU
1. Introduction
Delirium and agitation are common conditions in intensive care unit (ICU) patients, posing significant challenges to patient care and his outcome. These conditions often lead to extended hospital stays, prolonged dependence on mechanical ventilation, and subsequently higher healthcare costs [1,2,3,4]. More critically, they contribute to higher rates of morbidity and mortality among this vulnerable population [5].
Over the years, the diagnosis of delirium in the ICU has become more standardized and reliable, thanks to the implementation of universally accepted assessment tools such as the Richmond Agitation-Sedation Scale (RASS) [6,7]. The RASS has been integrated into hospital guidelines and protocols, allowing for consistent and accurate evaluation of patients’ level of agitation and sedation [8,9,10]. Based on this evaluation, proper therapeutic interventions can therefore be evaluated and administered. However, it is fundamental to consider that in some cases, delirium may be an epiphenomenon of underlying conditions such as sepsis or other organ dysfunctions, which are not always directly related to cerebral pathology per se [11,12]. Hence before considering pharmacological therapy, which carries its own costs and potential side effects, it is essential to carefully explore and address any possible underlying causes of delirium. Effective assessment and treatment of these primary conditions can often alleviate delirium without the need for additional medication [13]. With the aim to mitigate the possible pathological consequences related to delirium, antipsychotic drugs are frequently employed in the ICU [14,15]. They serve a multifaceted role, addressing acute psychosis, substance withdrawal, treatment-resistant agitation, and delirium [16].
Compared to traditional sedatives, antipsychotics are often preferred because they can effectively manage acute agitation without significantly impairing respiratory function. This makes them a potentially safer choice for patients already struggling with critical illness. The use of antipsychotic medications in the ICU, however, is not free to challenges including choosing the correct posology, related adverse drug reactions, monitoring, and possibility of discontinuation before discharge [17]. A wide array of these drugs has been studied for their efficacy in treating ICU delirium, leading to diverse prescribing practices across different medical institutions. Among these medications, quetiapine stands out for its off-label use in managing ICU delirium and agitation [18,19]. Its popularity in this context is largely due to its sedative properties and a side effect profile that is generally more favorable compared to older, first-generation antipsychotics [20,21,22,23].
In addition to antipsychotics, several classes of medications are available for managing ICU delirium and agitation, offering clinicians a range of options to tailor the treatment to individual patient needs. Quetiapine has relatively mild side effects which make it an attractive option for clinicians aiming to balance efficacy with patient safety. However, its off-label status underscores the need for ongoing research and clinical trials to better understand its best use and long-term impact on ICU patients. The goal remains to refine treatment protocols that not only alleviate the immediate symptoms of delirium and agitation, but also enhance overall patient outcomes in critical settings.
In this literature review, we aim to briefly describe the mechanisms of action of quetiapine, the potential benefits and adverse effects, and its most recent indications in the ICU described in the most recent and important medical researches. To evaluate the use of quetiapine in the ICU setting and its clinical outcomes, a comprehensive review of the literature was conducted (Figure 1). We searched six major databases: PubMed (1996–present), Embase (1974–present), Scopus (2004–present), SpringerLink (1950–present), Ovid Emcare (1995–present), and Google Scholar (2004–present). The search strategy involved using keywords such as “quetiapine,” “delirium,” “quetiapine and delirium,” and “quetiapine in ICU” to identify relevant studies. Two authors, AM and PF, were responsible for retrieving and reviewing the full texts of articles that met the search criteria. They carefully examined titles and abstracts to determine relevance and obtained full-text versions for detailed evaluation. Studies were excluded if they involved policy statements, or guidelines, ensuring a focus on relevant clinical research. The quality of the selected articles was assessed by evaluating their method, sample size, study design, and relevance to the topic of quetiapine use in the ICU. To ensure a consistent and reliable selection process, inter-rater agreement between AM and PF was measured using Cohen’s Kappa coefficient, which was calculated at 0.88, indicating a high level of agreement. In cases where there was a disagreement between the two reviewers, a third author, MU, was consulted to resolve the differences and achieve consensus.
2. Definition and Characteristics of Delirium
Delirium is defined as an acute syndrome which includes multiple features such as disturbance in attention (i.e., reduced ability to direct, focus, sustain, and shift attention), and awareness (reduced orientation to the environment) [1]. It is paramount to underline that it represents an acute change from baseline attention and awareness and tends to fluctuate in severity during the course of a day [24]. It may also present as an additional disturbance in cognition, like memory impairment, disorientation, language, visuospatial ability, or perception [25].
Patients with delirium often struggle with disorientation and find it difficult to perform complex tasks. Considering its fluctuating nature, the patients may experience periods of lucidity interspersed with episodes of significant confusion. Importantly, delirium is distinct from coma, as it does not involve - even in its hypoactive form - a severely reduced level of arousal [26]. Moreover, delirium results from an underlying medical condition and cannot be better explained by any other preexisting, evolving, or established neurocognitive disorder [25].
It is now widely recognized that the etiology of delirium is likely multifactorial, with factors such as older age and cognitive impairment contributing to its development. Other predictive factors include the presence of multiple conditions associated with coma, use of sedative medications (e.g., benzodiazepines), analgesics (e.g., opioids and ketamine), increased severity of illness, emergency type of admission as opposed to planned, admission diagnoses (such as neurological, neurosurgical, and trauma cases), presence of infection, dehydration, malnutrition, renal failure, and the use of hemofiltration [2,27,28]. The pathophysiological mechanisms underlying delirium may vary depending on the cause and likely involve multiple pathways. including the GABAergic and cholinergic neurotransmitter systems. This is supported by the increased risk associated with the use of GABA agonists and anticholinergic drugs [29]. Medication side effects account for up to 39% of delirium cases, therefore, great care should be taken in selecting the most appropriate drug [30].
The most described neurotransmitter disorders involved in delirium are a deficit in acetylcholine and/or melatonin availability, an excess in dopamine, norepinephrine, and/or glutamate release, and variable alterations in serotonin, histamine, and/or γ-aminobutyric acid (GABA) activity, which can either decrease or increase depending on the delirium presentation and cause [31]. To conclude, it is unlikely that any single theory can fully explain the etiology or phenomenological manifestations of delirium [32]. Instead, it is more likely that two or more of these factors, if not all, interact to cause the biochemical disturbances that lead to the complex cognitive and behavioral changes involved in delirium [33].
2.1. Clinical Features of Delirium
Delirium can manifest in different forms, which are generally categorized based on the predominant behavioral aspects in a hyperactive and a hypoactive form. Hyperactive delirium is characterized by agitation and restlessness, making it relatively easy to recognize due to the overt behavior changes [34]. In contrast, hypoactive delirium is often more subtle; patients may appear withdrawn, mute, and drowsy, which can sometimes cause it to go unnoticed as it does not present as immediately problematic [35]. Mixed delirium includes features of both hyperactive and hypoactive delirium, with patients fluctuating between the two states.
The symptoms of delirium extend beyond cognitive impairment [36]. Patients may experience psychotic symptoms such as hallucinations, delusions, and paranoia. Emotional disturbances are also common, including feelings of fear, anxiety, irritability, and anger. Some patients exhibit a phenomenon known as sundowning, where they become more confused and hyperactive at night. Additionally, delirium can lead to increased sympathetic activity, resulting in physical symptoms such as hypertension and tachycardia [37].
In ICU, delirium frequently emerges as an epiphenomenon of underlying conditions rather than as a direct result of primary neurological disorders [11]. Sepsis, for instance, is a common precipitating factor, where systemic infection triggers a cascade of inflammatory responses leading to delirious states [12]. Similarly, cardiopulmonary abnormalities, such as acute respiratory failure or cardiac dysfunction, can significantly disrupt cerebral homeostasis, manifesting as delirium. Thus, the occurrence of delirium in ICU patients often stems from critical systemic disturbances rather than organic neurological pathologies, challenging the initial assumption that it primarily originates from direct brain injury.
Lastly, it is important to consider that the same symptoms may also be triggered by other physical and environmental factors strictly related to the ICU stay, like mechanical ventilation, difficulty or impossibility to speak due to orotracheal intubation, low sleep hygiene, inappropriate pain management and prolonged immobilization.
3. Quetiapine in ICU Care: Applications, Dosage, and Key Considerations
Quetiapine, an atypical antipsychotic, is commonly used in ICU settings to address a range of conditions including insomnia, agitation, and delirium [48]. Available only in enteral forms, it is administered either orally or through feeding tubes. Once administered, quetiapine is absorbed rapidly, reaching peak plasma levels in about an hour. Its primary half-life is approximately seven hours, but its effects are prolonged by its active metabolite, N-desalkyl quetiapine, which has a half-life of around twelve hours [49]. This extended duration of action helps ensure continued symptom management. Quetiapine is metabolized in the liver by the enzyme CYP3A4, which means that liver function plays a crucial role in determining the appropriate dosage and ensuring the drug’s effectiveness [50].
At lower doses, quetiapine primarily acts as a sedative by blocking histamine H1 and muscarinic acetylcholine receptors [51]. This action helps induce sleep and reduce anxiety with minimal risk of exacerbating delirium. It also partially activates 5-HT1A receptors, contributing to its calming effects. At higher doses, quetiapine has a more significant impact on dopamine D2 and serotonin 5-HT2A receptors, aligning it more closely with the action of other atypical antipsychotics [52]. This shift is particularly useful in managing more severe forms of agitation and delirium.
In the ICU, quetiapine is often considered for its ability to provide effective sedation while maintaining a relatively mild side-effect profile compared to other antipsychotics. Its versatility in dosing allows for individualized treatment, which is essential in managing the complex needs of critically ill patients. Overall, quetiapine proves to be a valuable tool in critical care, offering effective management for insomnia, agitation, and delirium while contributing to an integrated approach to the patient care. The main findings of the literature report are summarized in Table 1.
In addition to its role in treating insomnia, quetiapine proves to be a valuable long-term agent for managing agitation, especially in patients undergoing mechanical ventilation [23]. Effective sedation is critical in this context as it helps to reduce patient distress and facilitates better synchronization with the ventilator, which can be challenging in agitated or restless patients [53]. In a randomized double blinded pilot study, treatment with quetiapine did not improve the number of days alive without delirium or coma, nor did it increase adverse outcomes [54]. Overall, quetiapine’s adaptability in addressing both short-term and long-term needs in the ICU underscores its importance in critical care pharmacotherapy. Its ability to manage insomnia without causing prolonged sedation, coupled with its effectiveness in controlling agitation and delirium, reinforces its role as a key component in the comprehensive care of critically ill patients.
Quetiapine is often prescribed to address insomnia, with typical doses ranging from 25 to 50 mg taken at bedtime [55]. This range of dosage is designed to help patients achieve a more restful sleep, which can significantly impact their overall well-being and recovery process in the high-stress environment of the ICU. Effective sleep management is not just about comfort; it is about supporting the body’s healing processes and enhancing the patient’s ability to cope with the physical and emotional demands of critical care. When it comes to managing agitated delirium, quetiapine is usually started at 50 mg every 12 hours [56]. This approach provides an initial level of sedation and symptom control, which can be adjusted based on how the patient responds. The dose can be gradually increased by 50 mg per day, allowing for a tailored approach to each patient’s needs. While many patients benefit from a maximum dose of around 200 mg twice daily, some may require higher doses to effectively manage their symptoms [57]. In such cases, the total daily dose might be adjusted up to approximately 800 mg. It’s important to monitor patients closely during these adjustments to ensure that the medication is both safe and effective.
For patients whose agitation and insomnia are primarily nocturnal, a single bedtime dose might be sufficient, providing relief without unnecessary medication throughout the day. For patients with liver impairment, quetiapine dosing needs careful consideration due to its metabolism in the liver [58]. Hepatic dysfunction can alter how the drug is processed, potentially requiring dose adjustments to prevent adverse effects and ensure optimal efficacy. Therefore, it is essential to monitor liver function closely and adjust the dosage as needed. On the other hand, renal dysfunction does not necessitate changes in quetiapine dosing, as the drug’s elimination is not significantly affected by kidney function. This makes dosing adjustments for patients with renal issues less complex compared to those with liver problems.
4.2. Quetiapine in the Pediatric ICU Setting
Delirium in the pediatric population is a prevalent condition and, akin to adults, poses significant diagnostic and therapeutic challenges. The limitations of existing tools for assessing delirium in the pediatric ICU (PICU) population, such as the Delirium Rating Scale (DRS), Pediatric Confusion Assessment Method for the ICU (pCAM-ICU), and Pediatric Anesthesia Emergence Delirium (PAED) scale, have been noted[59,60,61,62,63,64]. Briefly, the DRS was developed for use by psychiatrists and is time-consuming. The pCAM-ICU, even if is a really sophisticated cognitive assessment tool, requires patient cooperation and is only applicable to children over 5 years old, is less effective in those with developmental delays, and necessitates extensive nurse training. The PAED scale, designed for anesthesiologists to use immediately postoperatively, primarily identifies the hyperactive subtype of delirium. An ideal screening tool would be capable of detecting all forms of delirium—hyperactive, hypoactive, and mixed—in patients of all ages and developmental stages. The Cornell Assessment of Pediatric Delirium (CAPD) may be a useful tool for the diagnosis of delirium in PICU. In a study by Traube et al CAPD has shown high accuracy with a sensitivity of 94.1% (95% CI, 83.8–98.8%) and specificity of 79.2% (95% CI, 73.5–84.9%) and notably 31% of the diagnosis were in children less than 2 years old, and 27% of the diagnosis assessments were in children who were developmentally delayed; this data need to be confirmed by other evidences, but CAPD appears to be really promising in this population [65]. A study by Tapia et al. also demonstrated the effective performance of the RASS in this cohort for monitoring sedation in the PICU, particularly for categorizing patients into deep sedation, moderate-light sedation, and agitation. However, it may not be as useful for diagnosing delirium [66].
Similarly to diagnosis, the treatment of delirium in the PICU also poses several challenges. The use of benzodiazepines may be linked to an increased risk of delirium in critically ill children. Despite this association, benzodiazepines continue to be the first-line sedative in pediatric intensive care units (PICU) [67].Strong evidences in this respect are still lacking, but some researchers explored the use of antipsychotics to treat delirium in PICU.
Cronin et al. showed that patients treated with haloperidol or quetiapine did not exhibit short-term improvement in delirium screening scores after initiating treatment compared to untreated, propensity score-matched patients and, additionally, clinical outcomes were either not improved or were worse among the treated patients [21].
Similar findings were reported by Caballero et al., who observed that quetiapine did not have a statistically significant impact on the dosing of other deliriogenic medications used to manage the agitation; they also noted minimal changes in QTc intervals and no detection of dysrhythmias [68].
Joyce et al., addressing the lack of specific data on the use of quetiapine for managing delirium in critically ill children, extrapolated a potential dosing regimen from available adult data [69]. They proposed initiating therapy in the PICU at a dose of 1.5 mg/kg/day, divided into three doses. For breakthrough agitation, additional doses of 0.5 mg/kg were administered on top of the regular every-8-hour schedule with a usual maximum dosage limit of 6 mg/kg/day in their PICU. Dose escalation was guided by ongoing reassessment of the patient’s condition. The authors showed that short-term use of quetiapine as treatment for delirium appears to be safe, without serious adverse events; in fact, they reported only three episodes of QTc prolongation that were clinically nonsignificant with no associated dysrhythmia.
John et al in a study including 139 patients included in the PICU also found that QTc interval did not have a statistically significant change after the administration of antipsychotics, while there was improvement in the CAPD score. [70].
A meta-analysis including 32 RCTs showed no association between quetiapine and antipsychotic-induced hypo- and hyperprolactinemia in children and adolescents, whereas risperidone, paliperidone, and olanzapine were associated with significant prolactin increase, and aripiprazole was associated with significant decrease [71].
Although there are no established guidelines in this area to clarify dosages and first-line medications, and while it is essential to exercise caution and maintain close monitoring, quetiapine may be administered safely in the PICU.
5. Contraindications, Toxicity, and Cautions
Quetiapine is generally well-tolerated by patients, but its safety profile requires careful consideration of several key aspects. One notable concern is its potential to prolong the QTc interval [72]. While quetiapine can cause a slight prolongation of this interval, the actual risk of inducing a serious arrhythmia known as torsade de pointes is very low. A comprehensive review identified only four cases of torsade de pointes associated with quetiapine, all of which involved additional significant risk factors [73]. Thus, although caution is necessary for patients with pre-existing QT prolongation, quetiapine alone poses minimal risk in this regard [74].
Another important aspect of quetiapine’s safety profile is its low incidence of extrapyramidal side effects [75]. These movement disorders are common with many antipsychotic medications but are notably less frequent with quetiapine. This characteristic makes it particularly advantageous for patients with Parkinson’s disease, as it does not exacerbate their motor symptoms [76]. The studies by Mistraletti et al [77] and Tomichek et al [78] report low incidences of extrapyramidal symptoms and no significant differences in mortality rates between quetiapine and placebo groups. The reduced risk of extrapyramidal symptoms is a significant benefit, contributing to quetiapine’s suitability for a broad range of patients in critical care settings.
However, quetiapine does have potential to cause hypotension, particularly orthostatic hypotension, which is a drop in blood pressure upon standing. This effect results from its antagonism of alpha-adrenergic receptors. While hypotension is more pronounced compared to some other antipsychotics, such as olanzapine, it typically manifests as mild dizziness or lightheadedness. This side effect is manageable with proper monitoring and adjustments, ensuring that patients remain stable while receiving treatment. Additionally, a consideration for quetiapine use in the ICU is its potential continuation after patients transition to less critical care settings, including following hospital discharge. The ongoing administration of quetiapine in such contexts highlights the need for careful management and monitoring even as patients move towards recovery [17,79,80].
Overall, while quetiapine is associated with certain safety considerations, its benefits in managing symptoms and its relatively favorable side-effect profile make it a valuable option in critical care and beyond. Several studies have shown that quetiapine is effective in reducing the duration and severity of delirium in ICU patients. Devlin et al [81] conducted a double-blind, placebo-controlled trial demonstrating that quetiapine significantly shortened the duration of delirium compared to placebo. Similar findings were reported by Girard et al [54] who observed a faster resolution of delirium symptoms with quetiapine compared to placebo. Quetiapine has been shown to effectively manage agitation in ICU patients. Studies such as those by Devlin et al [82] suggest that quetiapine, when added to standard care, reduces agitation levels and the need for additional sedative medications. The impact of quetiapine on ICU length of stay remains inconsistent [19]. Some studies suggest a reduction in ICU stay with quetiapine use [81] attributed to the quicker resolution of delirium. However, others have found no significant difference in ICU or hospital length of stay when compared to placebo or other antipsychotics [83].
6. Clinical Practical Algorithm
The initial step in evaluating a patient exhibiting the characteristic clinical signs of delirium is to conduct the CAM-ICU assessment. If delirium is confirmed, it is essential to identify and rule out all potential underlying factors or conditions that may contribute to its onset, including fever, sepsis, and primary neurological disorders. Once the diagnosis of delirium is established, it is crucial to optimize environmental factors. This includes implementing effective pain management, minimizing noise and light to promote good sleep hygiene, and initiating mobilization as soon as feasible.
After optimizing all these factors, it is advisable to assess the level of sedation and agitation using the RASS scale, allowing for the differentiation of delirium based on behavioral characteristics into hypoactive and hyperactive subtypes. If the patient has no contraindications (such as allergy, prolonged QTc interval, or concurrent use of contraindicated medications like azole antifungals, erythromycin, or clarithromycin), the initiation of treatment with quetiapine may be considered.
For a patient with hypoactive delirium, treatment should be initiated with 25-50 mg once daily, with the possibility of increasing the dose to a maximum of 200 mg once daily. For a patient with hyperactive delirium, the starting dose should be 50 mg twice daily, which can be escalated to a maximum of 400 mg twice daily. If the treatment is ineffective, a change in antipsychotic should be considered. Conversely, if the therapy is effective, it is advisable to maintain the dosage until complete resolution is achieved. Once the delirium has fully resolved, it is crucial to consider a gradual reduction of the dosage and, if feasible, the discontinuation of the medication prior to discharge. This therapeutic algorithm is summarized in Figure 2.
7. Conclusions
Quetiapine appears to be a viable option for managing delirium and agitation in ICU patients, with evidence supporting its efficacy in reducing delirium duration and agitation. The safety profile of quetiapine is acceptable, with manageable side effects. However, its impact on ICU length of stay is less clear, necessitating further research. The heterogeneity of study designs, patient populations, and outcome measures in the existing literature underscores the need for larger, well-designed RCTs to provide more definitive conclusions. While there is promising evidence regarding its benefits, further research is required to fully understand its impact on ICU length of stay and long-term outcomes.
Author Contributions
Conceptualization, A.M. and P.F..; methodology, G.S. and P.F. resources, A.M. and M.U.; writing—original draft preparation, A.M, G.M. M.E.A. and P.F.; writing—review and editing, A.G, G.M.,A.P. and P.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ali, M.; Cascella, M. ICU Delirium. In StatPearls; StatPearls Publishing: Treasure Island, FL, 2024. [Google Scholar]
- Fiest, K.M.; Soo, A.; Hee Lee, C.; Niven, D.J.; Ely, E.W.; Doig, C.J.; Stelfox, H.T. Long-Term Outcomes in ICU Patients with Delirium: A Population-Based Cohort Study. Am J Respir Crit Care Med 2021, 204, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Ramírez Echeverría, M.d.L.; Schoo, C.; Paul, M. Delirium. In StatPearls; StatPearls Publishing: Treasure Island, FL, 2024. [Google Scholar]
- Mart, M.F.; Boehm, L.M.; Kiehl, A.L.; Gong, M.N.; Malhotra, A.; Owens, R.L.; Khan, B.A.; Pisani, M.A.; Schmidt, G.A.; Hite, R.D.; et al. Long-Term Outcomes after Treatment of Delirium during Critical Illness with Antipsychotics (MIND-USA): A Randomised, Placebo-Controlled, Phase 3 Trial. The Lancet Respiratory Medicine 2024, 12, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Li, H.-C.; Yeh, T.Y.-C.; Wei, Y.-C.; Ku, S.-C.; Xu, Y.-J.; Chen, C.C.-H.; Inouye, S.; Boehm, L.M. Association of Incident Delirium With Short-Term Mortality in Adults With Critical Illness Receiving Mechanical Ventilation. JAMA Netw Open 2022, 5, e2235339. [Google Scholar] [CrossRef] [PubMed]
- Sessler, C.N.; Gosnell, M.S.; Grap, M.J.; Brophy, G.M.; O’Neal, P.V.; Keane, K.A.; Tesoro, E.P.; Elswick, R.K. The Richmond Agitation-Sedation Scale: Validity and Reliability in Adult Intensive Care Unit Patients. Am J Respir Crit Care Med 2002, 166, 1338–1344. [Google Scholar] [CrossRef] [PubMed]
- Ely, E.W.; Truman, B.; Shintani, A.; Thomason, J.W.W.; Wheeler, A.P.; Gordon, S.; Francis, J.; Speroff, T.; Gautam, S.; Margolin, R.; et al. Monitoring Sedation Status over Time in ICU Patients: Reliability and Validity of the Richmond Agitation-Sedation Scale (RASS). JAMA 2003, 289, 2983–2991. [Google Scholar] [CrossRef] [PubMed]
- Martinez, F.E.; Tee, R.; Poulter, A.-L.; Jordan, L.; Bell, L.; Balogh, Z.J. Delirium Screening and Pharmacotherapy in the ICU: The Patients Are Not the Only Ones Confused. J Clin Med 2023, 12, 5671. [Google Scholar] [CrossRef]
- Su, J.-Y.; Lockwood, C.; Tsou, Y.-C.; Mu, P.-F.; Liao, S.-C.; Chen, W.-C. Implementing the Richmond Agitation-Sedation Scale in a Respiratory Critical Care Unit: A Best Practice Implementation Project. JBI Database System Rev Implement Rep 2019, 17, 1717–1726. [Google Scholar] [CrossRef] [PubMed]
- Rashidi, M.; Molavynejad, S.; Javadi, N.; Adineh, M.; Sharhani, A.; Poursangbur, T. The Effect of Using Richmond Agitation and Sedation Scale on Hospital Stay, Ventilator Dependence, and Mortality Rate in ICU Inpatients: A Randomised Clinical Trial. J Res Nurs 2020, 25, 734–746. [Google Scholar] [CrossRef]
- Gunther, M.L.; Morandi, A.; Ely, E.W. Pathophysiology of Delirium in the Intensive Care Unit. Crit Care Clin 2008, 24, 45–65. [Google Scholar] [CrossRef]
- Tokuda, R.; Nakamura, K.; Takatani, Y.; Tanaka, C.; Kondo, Y.; Ohbe, H.; Kamijo, H.; Otake, K.; Nakamura, A.; Ishikura, H.; et al. Sepsis-Associated Delirium: A Narrative Review. J Clin Med 2023, 12, 1273. [Google Scholar] [CrossRef]
- Kim, M.S.; Rhim, H.C.; Park, A.; Kim, H.; Han, K.-M.; Patkar, A.A.; Pae, C.-U.; Han, C. Comparative Efficacy and Acceptability of Pharmacological Interventions for the Treatment and Prevention of Delirium: A Systematic Review and Network Meta-Analysis. J Psychiatr Res 2020, 125, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.; Herzig, S.J.; Howell, M.D.; Le, S.H.; Mathew, C.; Kats, J.S.; Stevens, J.P. Antipsychotic Utilization in the Intensive Care Unit and in Transitions of Care. J Crit Care 2016, 33, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Devlin, J.W.; Skrobik, Y. Antipsychotics for the Prevention and Treatment of Delirium in the Intensive Care Unit: What Is Their Role? Harv Rev Psychiatry 2011, 19, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Swan, J.T.; Fitousis, K.; Hall, J.B.; Todd, S.R.; Turner, K.L. Antipsychotic Use and Diagnosis of Delirium in the Intensive Care Unit. Crit Care 2012, 16, R84. [Google Scholar] [CrossRef] [PubMed]
- Kram, B.L.; Kram, S.J.; Brooks, K.R. Implications of Atypical Antipsychotic Prescribing in the Intensive Care Unit. J Crit Care 2015, 30, 814–818. [Google Scholar] [CrossRef] [PubMed]
- Devlin, J.W.; Michaud, C.J.; Bullard, H.M.; Harris, S.A.; Thomas, W.L. Quetiapine for Intensive Care Unit Delirium: The Evidence Remains Weak. Pharmacotherapy 2016, 36, e12–e13, discussion e13–e14. [Google Scholar] [CrossRef]
- Alghadeer, S.; Almesned, R.S.; Alshehri, E.A.; Alwhaibi, A. Evaluation of the Efficacy and Safety of Quetiapine in the Treatment of Delirium in Adult ICU Patients: A Retrospective Comparative Study. J Clin Med 2024, 13, 802. [Google Scholar] [CrossRef]
- Hanna, M.P.; Adie, S.K.; Ketcham, S.W.; Deshmukh, A.; Gondi, K.; Abdul-Aziz, A.A.; Prescott, H.C.; Thomas, M.P.; Konerman, M.C. Atypical Antipsychotic Safety in the CICU. Am J Cardiol 2022, 163, 117–123. [Google Scholar] [CrossRef]
- Cronin, M.T.; Di Gennaro, J.L.; Watson, R.S.; Dervan, L.A. Haloperidol and Quetiapine for the Treatment of ICU-Associated Delirium in a Tertiary Pediatric ICU: A Propensity Score-Matched Cohort Study. Paediatr Drugs 2021, 23, 159–169. [Google Scholar] [CrossRef]
- Zakhary, T.; Ahmed, I.; Luttfi, I.; Montasser, M. Quetiapine Versus Haloperidol in the Management of Hyperactive Delirium: Randomized Controlled Trial. Neurocrit Care 2024. [Google Scholar] [CrossRef]
- Mo, Y.; Yam, F.K. Rational Use of Second-Generation Antipsychotics for the Treatment of ICU Delirium. J Pharm Pract 2017, 30, 121–129. [Google Scholar] [CrossRef]
- Arumugam, S.; El-Menyar, A.; Al-Hassani, A.; Strandvik, G.; Asim, M.; Mekkodithal, A.; Mudali, I.; Al-Thani, H. Delirium in the Intensive Care Unit. J Emerg Trauma Shock 2017, 10, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Diagnostic and Statistical Manual of Mental Disorders | Psychiatry Online. Available online: https://psychiatryonline.org/doi/book/10.1176/appi.books.9780890425596 (accessed on 10 July 2024).
- Stevens, R.D.; Nyquist, P.A. Coma, Delirium, and Cognitive Dysfunction in Critical Illness. Crit Care Clin 2006, 22, 787–804. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.B. Which Medications to Avoid in People at Risk of Delirium: A Systematic Review. Age Ageing 2011, 40, 23–29. [Google Scholar] [CrossRef]
- Reisinger, M.; Reininghaus, E.Z.; Biasi, J.D.; Fellendorf, F.T.; Schoberer, D. Delirium-associated Medication in People at Risk: A Systematic Update Review, Meta-analyses, and GRADE-profiles. Acta Psychiatr Scand 2023, 147, 16–42. [Google Scholar] [CrossRef] [PubMed]
- Zaal, I.J.; Devlin, J.W.; Hazelbag, M.; Klein Klouwenberg, P.M.C.; van der Kooi, A.W.; Ong, D.S.Y.; Cremer, O.L.; Groenwold, R.H.; Slooter, A.J.C. Benzodiazepine-Associated Delirium in Critically Ill Adults. Intensive Care Med 2015, 41, 2130–2137. [Google Scholar] [CrossRef] [PubMed]
- Alagiakrishnan, K.; Wiens, C.A. An Approach to Drug Induced Delirium in the Elderly. Postgrad Med J 2004, 80, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, J.R. Neuropathogenesis of Delirium: Review of Current Etiologic Theories and Common Pathways. Am J Geriatr Psychiatry 2013, 21, 1190–1222. [Google Scholar] [CrossRef]
- Flacker, J.M.; Lipsitz, L.A. Neural Mechanisms of Delirium: Current Hypotheses and Evolving Concepts. J Gerontol A Biol Sci Med Sci 1999, 54, B239–B246. [Google Scholar] [CrossRef]
- Yu, M.; Li, Y.; Li, B.; Ge, Q. Inflammatory Biomarkers and Delirium: A Mendelian Randomization Study. Front Aging Neurosci 2023, 15, 1221272. [Google Scholar] [CrossRef]
- Springer, B. Hyperactive Delirium with Severe Agitation. Emerg Med Clin North Am 2024, 42, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Rosen, J.H.; Bieber, E.; Matta, S.E.; Sayde, G.E.; Fedotova, N.O.; deVries, J.; Rafferty, M.; Stern, T.A. Hypoactive Delirium: Differential Diagnosis, Evaluation, and Treatment. Prim Care Companion CNS Disord 2024, 26, 23f03602. [Google Scholar] [CrossRef] [PubMed]
- Cole, M.G.; McCusker, J.; Dendukuri, N.; Han, L. Symptoms of Delirium among Elderly Medical Inpatients with or without Dementia. J Neuropsychiatry Clin Neurosci 2002, 14, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Alexander, S.K.; Needham, E. Diagnosis of Delirium: A Practical Approach. Pract Neurol 2023, 23, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, V.; O’Neill, P.J.; Cotton, B.A.; Pun, B.T.; Haney, S.; Thompson, J.; Kassebaum, N.; Shintani, A.; Guy, J.; Ely, E.W.; et al. Prevalence and Risk Factors for Development of Delirium in Burn Intensive Care Unit Patients. J Burn Care Res 2010, 31, 706–715. [Google Scholar] [CrossRef] [PubMed]
- Salluh, J.I.; Soares, M.; Teles, J.M.; Ceraso, D.; Raimondi, N.; Nava, V.S.; Blasquez, P.; Ugarte, S.; Ibanez-Guzman, C.; Centeno, J.V.; et al. Delirium Epidemiology in Critical Care (DECCA): An International Study. Crit Care 2010, 14, R210. [Google Scholar] [CrossRef] [PubMed]
- Rosgen, B.K.; Krewulak, K.D.; Stelfox, H.T.; Ely, E.W.; Davidson, J.E.; Fiest, K.M. The Association of Delirium Severity with Patient and Health System Outcomes in Hospitalised Patients: A Systematic Review. Age Ageing 2020, 49, 549–557. [Google Scholar] [CrossRef]
- Salluh, J.I.F.; Wang, H.; Schneider, E.B.; Nagaraja, N.; Yenokyan, G.; Damluji, A.; Serafim, R.B.; Stevens, R.D. Outcome of Delirium in Critically Ill Patients: Systematic Review and Meta-Analysis. BMJ 2015, 350, h2538. [Google Scholar] [CrossRef]
- Miranda, F.; Gonzalez, F.; Plana, M.N.; Zamora, J.; Quinn, T.J.; Seron, P. Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) for the Diagnosis of Delirium in Adults in Critical Care Settings. Cochrane Database Syst Rev 2023, 11, CD013126. [Google Scholar] [CrossRef]
- Devlin, J.W.; Skrobik, Y.; Gélinas, C.; Needham, D.M.; Slooter, A.J.C.; Pandharipande, P.P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit Care Med 2018, 46, e825–e873. [Google Scholar] [CrossRef]
- Lees, R.; Corbet, S.; Johnston, C.; Moffitt, E.; Shaw, G.; Quinn, T.J. Test Accuracy of Short Screening Tests for Diagnosis of Delirium or Cognitive Impairment in an Acute Stroke Unit Setting. Stroke 2013, 44, 3078–3083. [Google Scholar] [CrossRef] [PubMed]
- Bellelli, G.; Morandi, A.; Davis, D.H.J.; Mazzola, P.; Turco, R.; Gentile, S.; Ryan, T.; Cash, H.; Guerini, F.; Torpilliesi, T.; et al. Validation of the 4AT, a New Instrument for Rapid Delirium Screening: A Study in 234 Hospitalised Older People. Age Ageing 2014, 43, 496–502. [Google Scholar] [CrossRef]
- De, J.; Wand, A.P.F.; Smerdely, P.I.; Hunt, G.E. Validating the 4A’s Test in Screening for Delirium in a Culturally Diverse Geriatric Inpatient Population. Int J Geriatr Psychiatry 2017, 32, 1322–1329. [Google Scholar] [CrossRef] [PubMed]
- Palakshappa, J.A.; Hough, C.L. How We Prevent and Treat Delirium in the ICU. Chest 2021, 160, 1326–1334. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, J.M. Quetiapine Fumarate (Seroquel): A New Atypical Antipsychotic. Drugs Today (Barc) 1999, 35, 193–210. [Google Scholar] [CrossRef] [PubMed]
- DeVane, C.L.; Nemeroff, C.B. Clinical Pharmacokinetics of Quetiapine: An Atypical Antipsychotic. Clin Pharmacokinet 2001, 40, 509–522. [Google Scholar] [CrossRef] [PubMed]
- Bakken, G.V.; Rudberg, I.; Christensen, H.; Molden, E.; Refsum, H.; Hermann, M. Metabolism of Quetiapine by CYP3A4 and CYP3A5 in Presence or Absence of Cytochrome B5. Drug Metab Dispos 2009, 37, 254–258. [Google Scholar] [CrossRef]
- Seeman, P. Atypical Antipsychotics: Mechanism of Action. Can J Psychiatry 2002, 47, 27–38. [Google Scholar] [CrossRef]
- Gefvert, O.; Lundberg, T.; Wieselgren, I.M.; Bergström, M.; Långström, B.; Wiesel, F.; Lindström, L. D(2) and 5HT(2A) Receptor Occupancy of Different Doses of Quetiapine in Schizophrenia: A PET Study. Eur Neuropsychopharmacol 2001, 11, 105–110. [Google Scholar] [CrossRef]
- Ritchie, H.R.; Hodle, T.J.; Spinner, H.E. Antipsychotic Initiation in Mechanically Ventilated Patients in a Medical Intensive Care Unit. Am J Pharmacother Pharm Sci 2024, 3. [Google Scholar] [CrossRef]
- Girard, T.D.; Pandharipande, P.P.; Carson, S.S.; Schmidt, G.A.; Wright, P.E.; Canonico, A.E.; Pun, B.T.; Thompson, J.L.; Shintani, A.K.; Meltzer, H.Y.; et al. Feasibility, Efficacy, and Safety of Antipsychotics for Intensive Care Unit Delirium: The MIND Randomized, Placebo-Controlled Trial. Crit Care Med 2010, 38, 428–437. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-Y.; Chiang, C.-H.; Tseng, M.-C.M.; Tam, K.-W.; Loh, E.-W. Effects of Quetiapine on Sleep: A Systematic Review and Meta-Analysis of Clinical Trials. Eur Neuropsychopharmacol 2023, 67, 22–36. [Google Scholar] [CrossRef] [PubMed]
- Abraham, M.P.; Hinds, M.; Tayidi, I.; Jeffcoach, D.R.; Corder, J.M.; Hamilton, L.A.; Lawson, C.M.; Bollig, R.W.; Heidel, R.E.; Daley, B.J.; et al. Quetiapine for Delirium Prophylaxis in High-Risk Critically Ill Patients. Surgeon 2021, 19, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Hawthorne, A.; Delgado, E.; Battle, A.; Norton, C. Quetiapine Twice Daily Versus Bedtime Dosing in the Treatment of ICU Delirium. J Pharm Pract 2023, 8971900231193545. [Google Scholar] [CrossRef] [PubMed]
- Gunther, M.; Dopheide, J.A. Antipsychotic Safety in Liver Disease: A Narrative Review and Practical Guide for the Clinician. J Acad Consult Liaison Psychiatry 2023, 64, 73–82. [Google Scholar] [CrossRef]
- Schieveld, J.N.M.; van der Valk, J.A.; Smeets, I.; Berghmans, E.; Wassenberg, R.; Leroy, P.L.M.N.; Vos, G.D.; van Os, J. Diagnostic Considerations Regarding Pediatric Delirium: A Review and a Proposal for an Algorithm for Pediatric Intensive Care Units. Intensive Care Med 2009, 35, 1843–1849. [Google Scholar] [CrossRef]
- Schieveld, J.N.M. On Pediatric Delirium and the Use of the Pediatric Confusion Assessment Method for the Intensive Care Unit. Crit Care Med 2011, 39, 220–221. [Google Scholar] [CrossRef] [PubMed]
- Blankespoor, R.J.; Janssen, N.J.J.F.; Wolters, A.M.H.; Van Os, J.; Schieveld, J.N.M. Post-Hoc Revision of the Pediatric Anesthesia Emergence Delirium Rating Scale: Clinical Improvement of a Bedside-Tool? Minerva Anestesiol 2012, 78, 896–900. [Google Scholar]
- Silver, G.; Traube, C.; Kearney, J.; Kelly, D.; Yoon, M.J.; Nash Moyal, W.; Gangopadhyay, M.; Shao, H.; Ward, M.J. Detecting Pediatric Delirium: Development of a Rapid Observational Assessment Tool. Intensive Care Med 2012, 38, 1025–1031. [Google Scholar] [CrossRef]
- Smith, M.J.; Breitbart, W.S.; Platt, M.M. A Critique of Instruments and Methods to Detect, Diagnose, and Rate Delirium. J Pain Symptom Manage 1995, 10, 35–77. [Google Scholar] [CrossRef]
- On the Utility of Diagnostic Instruments for Pediatric Delirium in Critical Illness: An Evaluation of the Pediatric Anesthesia Emergence Delirium Scale, the Delirium Rating Scale 88, and the Delirium Rating Scale-Revised R-98 – PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/21567109/ (accessed on 4 August 2024).
- Traube, C.; Silver, G.; Kearney, J.; Patel, A.; Atkinson, T.M.; Yoon, M.J.; Halpert, S.; Augenstein, J.; Sickles, L.E.; Li, C.; et al. Cornell Assessment of Pediatric Delirium: A Valid, Rapid, Observational Tool for Screening Delirium in the PICU*. Crit Care Med 2014, 42, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Tapia, R.; López-Herce, J.; Arias, Á.; Del Castillo, J.; Mencía, S. Validity and Reliability of the Richmond Agitation-Sedation Scale in Pediatric Intensive Care Patients: A Multicenter Study. Front Pediatr 2021, 9, 795487. [Google Scholar] [CrossRef]
- Mody, K.; Kaur, S.; Mauer, E.A.; Gerber, L.M.; Greenwald, B.M.; Silver, G.; Traube, C. BENZODIAZEPINES AND DEVELOPMENT OF DELIRIUM IN CRITICALLY ILL CHILDREN: ESTIMATING THE CAUSAL EFFECT. Crit Care Med 2018, 46, 1486–1491. [Google Scholar] [CrossRef] [PubMed]
- Caballero, A.; Bashqoy, F.; Santos, L.; Herbsman, J.; Papadopoulos, J.; Saad, A. Quetiapine for the Treatment of Pediatric Delirium. Ann Pharmacother 2023, 57, 1172–1177. [Google Scholar] [CrossRef] [PubMed]
- Joyce, C.; Witcher, R.; Herrup, E.; Kaur, S.; Mendez-Rico, E.; Silver, G.; Greenwald, B.M.; Traube, C. Evaluation of the Safety of Quetiapine in Treating Delirium in Critically Ill Children: A Retrospective Review. J Child Adolesc Psychopharmacol 2015, 25, 666–670. [Google Scholar] [CrossRef]
- John, C.J.; Engler, M.; Zaki, H.; Crooker, A.; Cabrera, M.; Golden, C.; Whitehill, R.; Xiang, Y.; Liu, K.; Fundora, M.P. The Effect of Antipsychotic Medications on QTc and Delirium in Paediatric Cardiac Patients with ICU Delirium. Cardiol Young 2024, 1–5. [Google Scholar] [CrossRef]
- Krøigaard, S.M.; Clemmensen, L.; Tarp, S.; Pagsberg, A.K. A Meta-Analysis of Antipsychotic-Induced Hypo- and Hyperprolactinemia in Children and Adolescents. J Child Adolesc Psychopharmacol 2022, 32, 374–389. [Google Scholar] [CrossRef]
- Wang, C.-L.; Wu, V.C.-C.; Lee, C.H.; Wu, C.-L.; Chen, H.-M.; Huang, Y.-T.; Chang, S.-H. Incidences, Risk Factors, and Clinical Correlates of Severe QT Prolongation after the Use of Quetiapine or Haloperidol. Heart Rhythm 2024, 21, 321–328. [Google Scholar] [CrossRef]
- Hasnain, M.; Vieweg, W.V.R.; Howland, R.H.; Kogut, C.; Breden Crouse, E.L.; Koneru, J.N.; Hancox, J.C.; Digby, G.C.; Baranchuk, A.; Deshmukh, A.; et al. Quetiapine, QTc Interval Prolongation, and Torsade de Pointes: A Review of Case Reports. Ther Adv Psychopharmacol 2014, 4, 130–138. [Google Scholar] [CrossRef]
- Dube, K.M.; DeGrado, J.; Hohlfelder, B.; Szumita, P.M. Evaluation of the Effects of Quetiapine on QTc Prolongation in Critically Ill Patients. J Pharm Pract 2018, 31, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.S. Extrapyramidal Symptoms Associated with Quetiapine. Aust N Z J Psychiatry 2003, 37, 773. [Google Scholar] [CrossRef] [PubMed]
- Leucht, S.; Pitschel-Walz, G.; Abraham, D.; Kissling, W. Efficacy and Extrapyramidal Side-Effects of the New Antipsychotics Olanzapine, Quetiapine, Risperidone, and Sertindole Compared to Conventional Antipsychotics and Placebo. A Meta-Analysis of Randomized Controlled Trials. Schizophr Res 1999, 35, 51–68. [Google Scholar] [CrossRef] [PubMed]
- Mistraletti, G.; Mantovani, E.S.; Cadringher, P.; Cerri, B.; Corbella, D.; Umbrello, M.; Anania, S.; Andrighi, E.; Barello, S.; Di Carlo, A.; et al. Enteral vs. Intravenous ICU Sedation Management: Study Protocol for a Randomized Controlled Trial. Trials 2013, 14, 92. [Google Scholar] [CrossRef]
- Tomichek, J.E.; Stollings, J.L.; Pandharipande, P.P.; Chandrasekhar, R.; Ely, E.W.; Girard, T.D. Antipsychotic Prescribing Patterns during and after Critical Illness: A Prospective Cohort Study. Crit Care 2016, 20, 378. [Google Scholar] [CrossRef]
- Lambert, J.; Vermassen, J.; Fierens, J.; Peperstraete, H.; Petrovic, M.; Colpaert, K. Discharge from Hospital with Newly Administered Antipsychotics after Intensive Care Unit Delirium - Incidence and Contributing Factors. J Crit Care 2021, 61, 162–167. [Google Scholar] [CrossRef]
- Marshall, J.; Herzig, S.J.; Howell, M.D.; Le, S.H.; Mathew, C.; Kats, J.S.; Stevens, J.P. Antipsychotic Utilization in the Intensive Care Unit and in Transitions of Care. J Crit Care 2016, 33, 119–124. [Google Scholar] [CrossRef]
- Devlin, J.W.; Roberts, R.J.; Fong, J.J.; Skrobik, Y.; Riker, R.R.; Hill, N.S.; Robbins, T.; Garpestad, E. Efficacy and Safety of Quetiapine in Critically Ill Patients with Delirium: A Prospective, Multicenter, Randomized, Double-Blind, Placebo-Controlled Pilot Study. Crit Care Med 2010, 38, 419–427. [Google Scholar] [CrossRef]
- Devlin, J.W.; Bhat, S.; Roberts, R.J.; Skrobik, Y. Current Perceptions and Practices Surrounding the Recognition and Treatment of Delirium in the Intensive Care Unit: A Survey of 250 Critical Care Pharmacists from Eight States. Ann Pharmacother 2011, 45, 1217–1229. [Google Scholar] [CrossRef]
- Maneeton, B.; Maneeton, N.; Srisurapanont, M.; Chittawatanarat, K. Quetiapine versus Haloperidol in the Treatment of Delirium: A Double-Blind, Randomized, Controlled Trial. Drug Des Devel Ther 2013, 7, 657–667. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of search strategy.
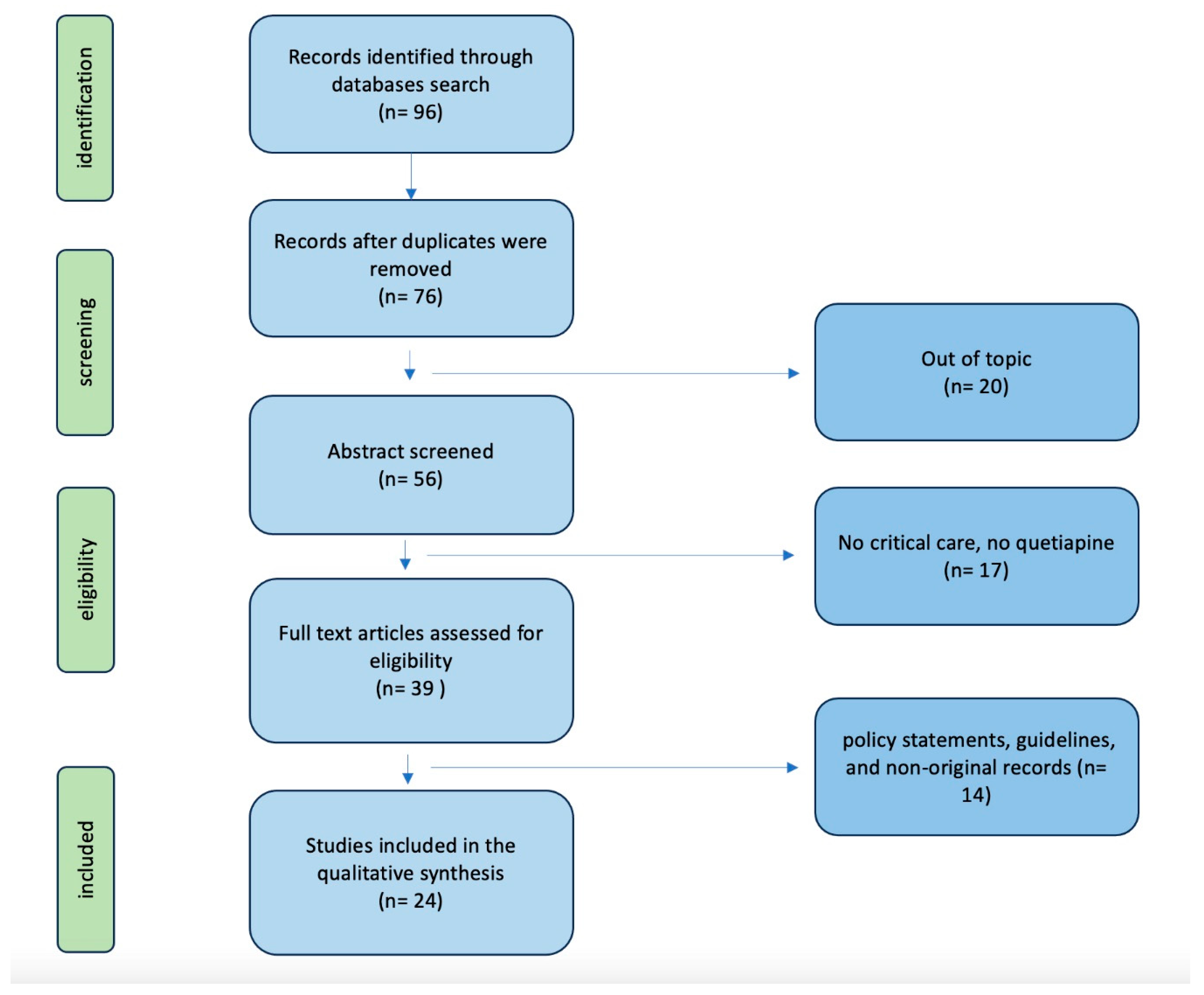
Figure 2.
Schematic clinical approach in ICU patients with suspect delirium.
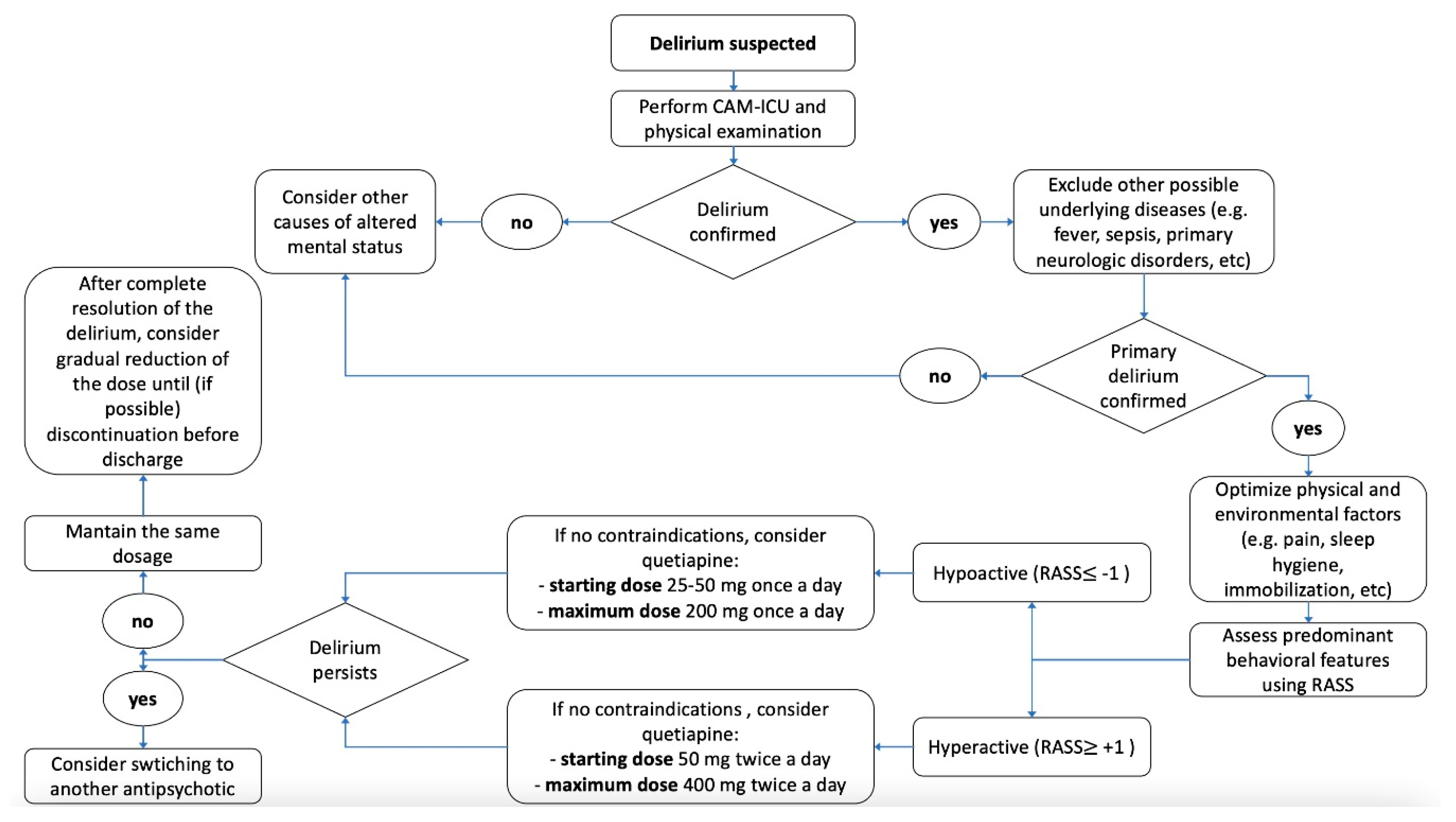

Table 1.
Principal investigation on Quetiapine in critical care setting.
| Study | Patients | Design | Main Findings |
|---|---|---|---|
| Martinez et al.[8] | 665 ICU patients | Retrospective observational study | The screening rates for RASS and CAM-ICU were below the recommended levels. The administration of antipsychotic medications – mostly quetiapine in this cohort - occurs more frequently than the diagnosis of delirium |
| Sessler et al.[6] | 192 ICU patients | Comparative study | RASS showed a high inter-rater reliability among the entire adult ICU population. Robust correlations between the investigator-assigned RASS and the visual analog scale scores validated the use of RASS across all subgroups within the ICU. The RASS scores documented by individual physicians, nurses, and pharmacists exhibited a strong correlation with the principal investigator’s visual analog scale score. |
| Ely et al.[7] | 290 ICU patients | Prospective cohort study | The RASS represents the first sedation scale validated for its capacity to identify variations in sedation levels over successive days of ICU treatment, in relation to constructs such as consciousness levels and delirium, and it showed a correlation with the dosages of sedative and analgesic medications administered. This study confirmed the reliability and validity of RASS for monitoring sedation status over time. |
| Miranda et al.[42] | 2817 ICU | Cochrane review | This study evaluated CAM-ICU for diagnosing delirium in critical care settings. The test is primarily beneficial for ruling out delirium. However, it may fail to identify a subset of patients with newly developed delirium. Consequently, in scenarios where comprehensive detection of all delirium cases is essential, it may be advisable to either retest or to use the CAM-ICU in conjunction with an additional assessment. |
| Marshall et al.[80] | 164’996 ICU patients | Retrospective observational cohort study | Antipsychotic medications are prescribed to 1 in every 10 patients in the ICU, and their use is correlated with prolonged lengths of stay in both the ICU and the hospital. Patients receiving antipsychotics without any recorded diagnosis of a mental disorder exhibit longer ICU stays, extended hospitalizations, and higher mortality rates in comparison to those with a documented mental disorder. |
| Girard et al.[54] | 101 ICU patients mechanically ventilated | Randomized, double-blind, placebo-controlled | Neither haloperidol nor ziprasidone significantly shortened the duration of delirium when compared to placebo. Patients across the three treatment groups had a comparable number of days alive without experiencing delirium or coma. |
| Mart et al.[4] | 566 ICU patients | Randomized, double-blind, placebo-controlled | In critically ill patients experiencing delirium, neither haloperidol nor ziprasidone demonstrated a significant impact on cognitive, functional, psychological, or quality-of-life outcomes in survivors. |
| Devlin et al.[81] | 36 ICU patients with delirium | Prospective, randomized, double-blind, placebo-controlled | The inclusion of quetiapine with as-needed haloperidol is associated with a more rapid resolution of delirium, decreased levels of agitation, and a higher rate of discharge to home or rehabilitation. Patients receiving quetiapine needed fewer days of as-needed haloperidol. Furthermore, the occurrence of QTc prolongation and extrapyramidal symptoms was comparable between the groups. |
| Zakhary et al.[22] | 100 ICU patients | Randomized controlled | Quetiapine has been shown to be as effective as haloperidol in alleviating the symptoms of hyperactive delirium in critically ill patients, although it does not confer any benefit in terms of mortality. |
| Maneeton et al.[83] | 52 ICU patients with delirium | Prospective, double-blind, randomized controlled | Low doses of quetiapine and haloperidol demonstrate comparable efficacy and safety for managing behavioral disturbances (efficacy, tolerability, total sleep time) in patients with delirium, particularly when combined with environmental modifications. |
| Alghadeer et al.[19] | 47 ICU patients | Retrospective comparative study | The authors found no significant differences in efficacy or adverse effects when comparing the treatment of delirium with quetiapine, haloperidol, risperidone, and olanzapine |
| Wang et al.[72] | 11173 patients, quetiapine vs haloperidol | Multicenter retrospective cohort study | The authors showed that severe QT prolongation was prevalent among patients undergoing treatment with quetiapine or haloperidol. A considerable proportion of these patients were exposed to risk factors associated with QT prolongation, including older age, heart failure, hypokalemia, and the concurrent administration of medications recognized to elevate the risk of torsades des pointes. |
| Dube et al.[74] | 103 ICU patients | Single-center, prospective cohort analysis | There were no reported occurrences of torsades de pointes. QTc prolongation was relatively rare among critically ill patients receiving quetiapine. Patients who were prescribed concomitant medications known to prolong the QTc interval may be at a heightened risk. |
| Tomichek et al.[78] | 500 ICU patients | Single-centre prospective cohort study | The administration of an atypical antipsychotic markedly increased the probability of receiving an antipsychotic prescription at discharge, a practice that should be carefully evaluated during medication reconciliation |
| Lambert et al.[79] | 196 ICU patients | Retrospective observational study | About 20% of patients were released from the hospital while still on antipsychotic medications. Hospital discharge protocols should incorporate strategies for the systematic reduction of antipsychotic dosages and improved monitoring of antipsychotic use during transitions of care. |
| Traube et al.[65] | 111 PICU patients | Validation study | Cornell Assessment of Pediatric Delirium (CAPD) has shown high accuracy in diagnosing delirium, and notably 31% of the diagnosis were in children less than 2 years old, and 27% of the diagnosis assessments were in children who were developmentally delayed. |
| Cronin et al.[21] | 846 PICU patients | A single-center retrospective cohort study | Patients administered haloperidol or quetiapine did not demonstrate any short-term improvement in delirium screening scores following the initiation of treatment, relative to untreated patients matched by propensity scores. Additionally, clinical outcomes for those receiving treatment were either not improved or were worse. |
| Caballero et al.[68] | 37 PICU patients | Single-center observational study | Quetiapine did not produce a statistically significant effect on the dosages of deliriogenic medications. There were negligible alterations in the QTc interval, and no dysrhythmias were detected. |
| John et al.[70] | 139 PICU patients | Retrospective observational study | The QTc interval did not exhibit a statistically significant alteration following the administration of antipsychotics, whereas an improvement in the CAPD score was observed. Atypical antipsychotic medications can be used safely without causing substantial QTc prolongation and are effective in treating delirium. |
| Joyce et al.[69] | 50 PICU patients | Retrospective observational study | Authors proposed a potential dosing regimen initiating therapy at a dose of 1.5 mg/kg/day, divided into three doses. For breakthrough agitation, additional doses of 0.5 mg/kg were administered on top of the regular every-8-hour schedule with a usual maximum dosage limit of 6 mg/kg/day. In this cohort, the short-term administration of quetiapine for the management of delirium seems to be safe, with no significant adverse events reported. |
* PICU: pediatric intensive care unit.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



