
Submitted:
20 September 2024
Posted:
23 September 2024
You are already at the latest version
Abstract
Pomegranate juice possesses therapeutic properties against metabolic syndrome. Microencapsulation of pomegranate juice (MPJ) may extend its shelf life; however, further research is necessary to ascertain its comparative efficacy with fresh juice. This work evaluated the effect of (MPJ) in an animal model with induced metabolic syndrome (MetS). Male Wistar rats were induced-MetS by administering 30% sucrose orally for 22 weeks. Once MetS was verified in the animals, 7 groups were formed as follows: control (Ctrl); MetS, MetS+Placebo; Ctrl+MPJ; MetS+MPJ1 600, MetS+MPJ2 1800, and MetS+MPJ3 2900 mg/kg. Systolic and diastolic blood pressure, glucose, triglycerides, and total HDL-c levels in the MetS+MPJ groups improved significantly (p < 0.05) vs. the MetS group at the end of the study. Microencapsulation maintained the anti-metabolic syndrome properties of pomegranate juice and could be used to control metabolic syndrome.

Keywords:
Metabolic syndrome
; Microencapsulated pomegranate juice
; Cardiovascular diseases
; Punica granatum
; Biochemical markers
1. Introduction
Cardiovascular diseases (CVD) are a group of heart and blood vessel disorders and a leading cause of death worldwide. However, many early deaths could be avoided by improving some lifestyles, such as improving food choices, decreasing smoking, and increasing physical activity [1]. Metabolic syndrome (MetS) is an accumulation of several disorders such as abdominal obesity, hypertension, dyslipidemia, and hyperglycemia, all involved in the development of CVD and Type 2 diabetes [2]. The worldwide prevalence of MetS is estimated to range from 7.9% to 43% in men and 7% to 56% in women [3]. The National Cholesterol Education Program Adult Treatment Panel III (NCEP/ATP III) is a global health organization with established criteria for diagnosing MetS [4]. According to ATP III, a patient diagnosed with MetS must have three or more of the following criteria: (1) abdominal obesity with large waist circumference (>102 cm in men and >88 cm in women) (2) hypertriglyceridemia (>150 mg/dl or 1.7 mmol / l) (3) low levels of high-density lipoprotein cholesterol (HDLc) (<40 mg/dl or 1 mmol/l in men and <50 mg/dl or 1.3 mmol/l in women) (4) elevated blood pressure (≥130-85 mmHg), and (5) glucose intolerance (≥100 mg/dl or 5.5 mmol/l) or type 2 diabetes [5,6]. Patients with MetS are characterized by marked oxidative stress favoring inflammation; these patients tend to have lower antioxidant enzymes and high levels of oxidative markers such as lipoperoxidation [7]. Therefore, a pro-oxidant/antioxidant imbalance may play an important role in MetS by over-generating reactive oxygen and nitrogen species [8]. The consumption of antioxidant-rich foods, e.g., fruits, may contribute to MetS treatment by preventing and ameliorating the inflammatory process and complications such as atherosclerosis [9]. The pomegranate (Punica granatum L.) has been used to effectively treat various diseases in traditional medicine [10] and its value has been confirmed by preclinical and clinical studies [11,12]. Pomegranate fruit, especially peel and juice, has many bioactive compounds [13,14,15]. The juice is especially rich in antioxidant polyphenols [16] such as ellagitannins, anthocyanins, flavonoids, proanthocyanidins and significant amounts of chlorogenic acid, caffeic acid, coumaric acid, and ferulic acid [13,17]. While it has been reported that up to 124 different phytochemicals could be found in a pomegranate, the punicalagins are responsible for over 50% of the antioxidant potential of pomegranate juice [18]. In addition, pomegranate juice contains minerals, vitamins C and E, lipoic acid, steroids, and triterpenes, among others [19]. Many preclinical and clinical studies have demonstrated that pomegranate has anti-metabolic syndrome properties [13,20,21,22]. However, pomegranate consumption is limited because it only can be found in certain times of the year. To investigate a potential solution to this problem, we tested microencapsulated pomegranate juice (MPJ) to evaluate the effect of MPJ in an animal model with metabolic syndrome induced with 30% sucrose. MPJ has already been shown to improve endothelial dysfunction and biochemical parameters in women’s acute coronary syndrome [23].
2. Materials and Methods
2.1. Pomegranate and Microencapsulation
The pomegranate producer society “El Oasis de Tasquillo” (located in the Mezquital Valley, Hidalgo, Mexico) provided pomegranates for study in September 2018. A voucher specimen (U10) was deposited at the Herbarium of the Botany Department of the Autonomous University of the State of Hidalgo (UAEH), Mexico. We previously described the microencapsulation process of pomegranate juice compounds, which was done by spray drying [23].
2.2. Animals
The Animal Care Committee of the UAEH approved this project (approval number CIECUAL20145).
Fifty-six 4-week-old male Wistar rats were obtained and the sample size (n=6) per group was calculated using G-Power 3.0.1 software (HHU, Düsseldorf, Germany) considering the effect size, standard deviation and significance level (p = 0.05), power, and statistical tests. Rats weighing 45 ± 5 g were obtained from the UAEH animal facility. All animals were acclimatized for 14 days and housed in standard cages under controlled conditions with a 12 h light / 12 h dark cycle, constant temperature (26 ± 2 °C), and 50% relative humidity. Animals were fed commercial food (Formulab 5008, Lab diet, Framingham, MA, USA), and water was provided ad libitum. The number of animals per group was minimized.
2.3. Induction of MetS by 30% Sucrose
After two weeks of acclimatization of the animals, we followed the methodology described by Hafidi et al. to induce MetS [24]. Forty randomly selected rats received ad libitum 30% (w/v) commercially refined sucrose in their drinking water for 20 weeks to develop hyperglycemia and other MetS parameters. The other sixteen animals considered controls received sterile water ad libitum for the same period. At the end of the period, we confirmed that the 40 sucrose-fed animals, developed MetS by determining that their blood pressure; glucose levels; and lipid profile of total cholesterol, LDL-c, HDL-c, and triglycerides met the parameters according to ATP III diagnostic criteria [4]. Rats without confirmed MetS were excluded.
2.4. Measurement of Body Weight, Blood Pressure, and Biochemical Parameters
Animals were weighed using a compact scale (ADAM AQT-250, USA). Systolic and diastolic blood pressure was measured with a non-invasive method [25].
After an overnight fast, blood was drawn from the tail vein and allowed to stand for 30 minutes at 4°C, then centrifuged to obtain serum. A kit was used to measure biochemical levels of glucose (Wiener Lab®test kit Lab, Germany), triglycerides, total cholesterol, and HDL-c (Randox Lab, UK). The LDL-c level was calculated using the Friedewald method [26].
2.5. MPJ Supplementation
After the 20-week MetS induction, animals were randomly divided into 7 groups of 8 rats as follows: (1) Control (Ctrl) received water (no MetS induced); (2) Metabolic syndrome (MetS) received 30% sucrose in water; (3) placebo (MetS+Placebo) received 30% sucrose in water + maltodextrin-gum Arabic encapsulating matrix without pomegranate juice; (4) MPJ control (Ctrl+MPJ) received water + MPJ dose 1800 mg/kg, no MetS induced; (5) MetS+MPJ1, received 30% sucrose + MPJ dose 600 mg/kg; (6) MetS+MPJ2, received 30% sucrose + 1800 mg/kg MPJ and (7) MetS+MPJ3, received 30% sucrose + 2900 mg/kg MPJ. The groups that received 30% sucrose in water during the induction period consuming it during the study.
We established the doses of MPJ considering the mean therapeutic doses of juice reported in the literature for humans and animals, percent moisture, yield, and drying loss. We prepared MPJ daily by dissolving it in sterile water (administration volume 4 ml/kg). Administration was intragastric (i.g.). Treatments were continued biweekly for eight weeks, taking measurements of body weight, blood pressure, and biochemical parameters at the beginning and every seven days (in triplicate).
2.6. Statistical Analysis
The results were expressed as mean ± SD of each variable. For the diagnosis of MetS a Student’s t-test for independent samples was performed (Ctrl vs. MetS). The difference between the means for each variable was estimated by a two-way analysis of variance (ANOVA) with a Bonferroni post hoc to compare replicate means by row, with the treatment after induction being the independent variable, and the dependent variables: blood pressure, glucose, total cholesterol, HDL-c, LDL-c, triglycerides, and body weight. The ANOVA of the study was MetS versus control group, treated groups, and placebo. Statistical analyses were performed using GraphPad Prism 8 for Windows (GraphPad, CA, USA) with a p < 0.05.
3. Results
3.1. MetS Induction
To verify the development of MetS, we measured the indicators of blood pressure, glucose, total cholesterol, HDL-c, LDL-c, triglycerides, and body weight involved according to ATP III. We found that all, except HDL-c, showed statistically significant differences (p<0.05) between the Ctrl group and the MetS group, at least by the 6th week, which corroborated the induction of MetS for some indicators as shown in the Figure 1.
3.2. Body Weight
Figure 2 shows the body weight data of the rats expressed as mean ± SD in the different treatment groups. No significant differences (p <0.05) were found between the groups. Natural weight gain was constant and progressive for all groups over time. However, Ctrl+MPJ rats were observed to have less weight than the other groups. It is observed that the MetS group had a mean weight similar to other groups (except the Ctrl+MPJ group).
3.3. Blood Pressure
Figure 3 shows the groups’ systolic blood pressure (SBP) and diastolic blood pressure (DBP). Statistical analysis of systolic pressure revealed that, from week 2, the systolic pressure of the MetS+MPJ1 group decreased significantly (p<0.05) compared to the MetS group. At week 4, MetS+MPJ2 also decreased significantly. At weeks 6 and 8, the MetS+MPJ3 group also obtained significant differences compared to the MetS group.
MPJ also positively affected the diastolic pressure, where significant differences (p<0.05) were observed compared to the MetS group in all MPJ-treated groups from week 2, finding that for MetS+MPJ3, there were significant differences from week 4 onwards. These results suggest that MPJ, both in the three doses evaluated and in the Ctrl+MPJ group, had an antihypertensive effect. The placebo group did not present significant differences versus the MetS group; on the contrary, the data were similar (not shown in the figure).
3.4. Biochemical Analysis
Glucose
The Ctrl+MPJ group was observed to be statistically different (p<0.05) versus the MetS group. The result suggests a preventive role in the development of MetS by MPJ. In the treated groups, MetS+MPJ1, MetS+MPJ2, and MetS+MPJ3 showed a trend of decreasing glucose levels (Figure 4) although the lowest level of MPJ (MetS+MPJ1) was not consistently low.
Total Cholesterol
MPJ reduced total cholesterol levels relative to MetS (Figure 5).
LDL-c and HDL-c
Triglycerides
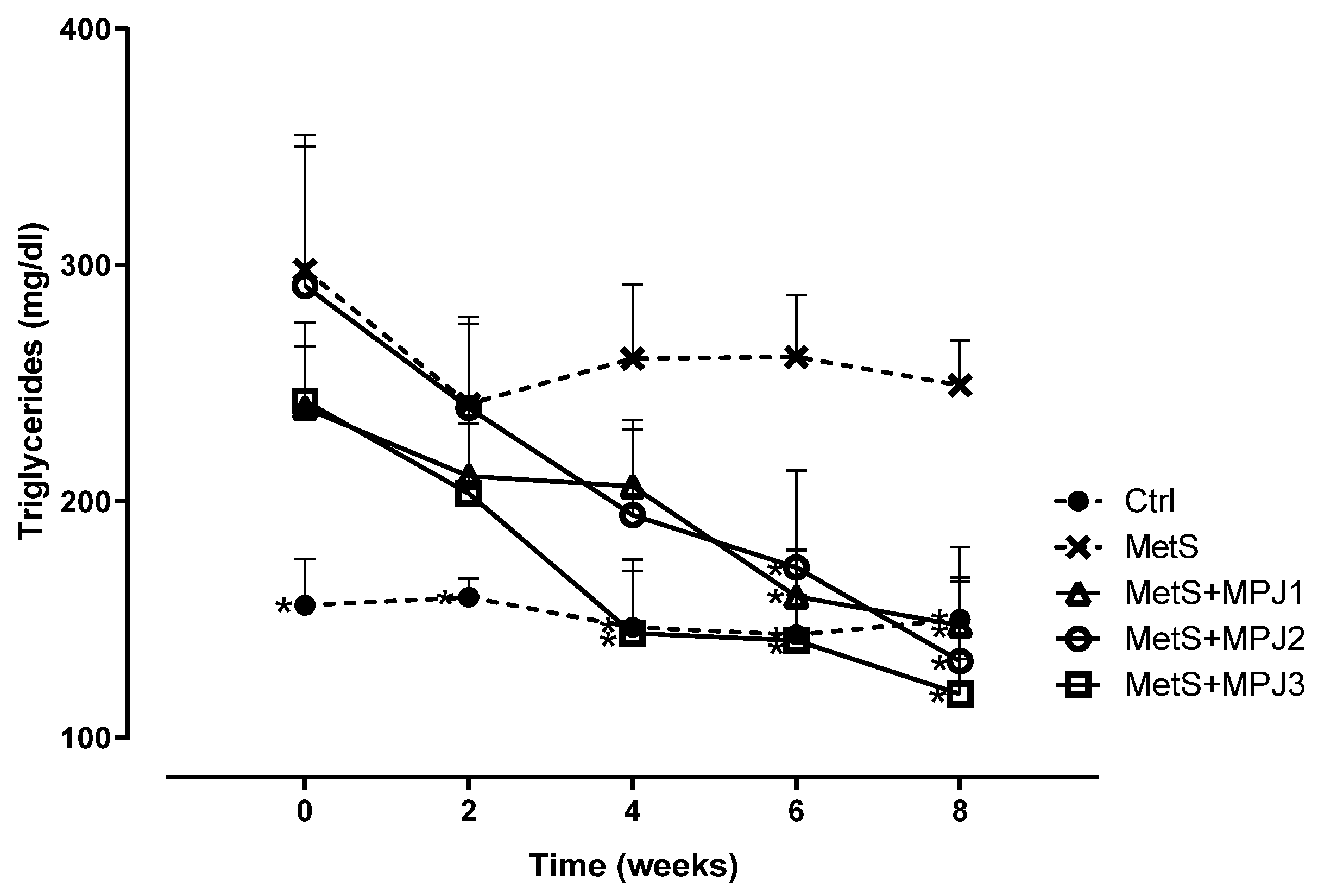
MPJ was increasingly effective over time in decreasing triglyceride levels (Figure 7). The MetS+Placebo group had no differences from the MetS group (data not shown), so the encapsulating matrix does not alter triglyceride levels.
4. Discussion
This study used the administration of 30% sucrose from week 4 of the rats’ life during 20 weeks to provide a model of MetS, plus 8 weeks of treatment study [24] to provide a model of MetS. We used MPJ as a natural treatment of this induced MetS. We chose to use male Wistar rats because of the evidence that males have a higher risk of cardiovascular disease [27]. We previously reported that MPJ consumption is safe in doses of up to 5000 mg/kg bw and did not cause subacute or subchronic toxicity [28].
While MPJ alone reduced weight gain relative to control, the MetS + MPJ treatments did not lower weight gain (Figure 2). The MetS+ MPJ did lower systolic and diastolic blood pressures (Figure 3), glucose (except MPJ1, Figure 4), total cholesterol (Figure 5), and HDL-c (Figure 6). MPJ did not consistently affect LDL-c (Figure 6). This work confirmed that a storage form of pomegranate juice, microencapsulated pomegranate juice (MPJ), has anti-metabolic syndrome effects.
Obesity is a chronic non-communicable disease that develops from a complex combination of nutritional, genetic, and environmental factors [29]. In this study, all rats increased their body mass because they were still growing while 30% sucrose increased the caloric content and caused weight gain. Interestingly, no significant differences in body mass were found in either group versus the MetS group or between them. At time zero (after 20 weeks drinking 30 % sucrose), it was observed that the MetS group had even less weight than the Ctrl group, which was unexpected due to the high sucrose intake and lack of treatment but which agrees with a study in which free fatty acids, adipocyte size, and systemic blood pressure were measured in Wistar rats with MetS induced with 30% sucrose administered with glycine for four weeks. When measuring fluid intake, diet, and body mass during four weeks of treatment, the researchers found no significant differences among the groups [24]. In another study [30], the effect of a water daily intake of 30% sucrose on food intake and weight was evaluated in male Wistar rats. At the end of the treatment, food intake and biochemical indicators showed that sugar water reduced the balanced food intake by more than 90%; therefore, sugar water consumption could cause malnutrition in the long term, as it causes a reduction in the nutrient-rich food intake. This result agrees with a previous study in rats [31], which showed that sugar water intake with 12% sucrose decreased balanced food intake by 47.54%, suggesting a sucrose concentration-dependent effect. Another explanation is that the elevated insulin levels in the brain cause a decrease in the intake of food [32]. Pomegranate extracts have been reported to decrease body mass in animal models fed a high-fat, high-calorie diet [33,34,35]. Possible mechanisms of action could be the inhibition of pancreatic lipase, thereby increasing the excretion of fats in feces [36], improving mitochondrial function [37], control of AMP-activated protein kinase (AMPK), lipolysis in adipose tissue, and stimulating fatty acid oxidation in the liver [38]. In this study the Ctrl+MPJ group had a minor increase in body mass. While MPJ reduced weight gain in control rats (Figure 2), probably due to the mechanisms mentioned, more research is required to determine why MPJ did not reduce body mass in the 30% sucrose-treated groups.
Cardiovascular disorders are among the leading causes of death and disability globally and hypertension, has a high worldwide prevalence and is the leading risk factor for developing cardio- and cerebrovascular disorders [39]. In this study, all groups receiving 30% sucrose water developed diastolic and systolic hypertension. MPJ treatment significantly (p < 0.05) decreased systolic and diastolic pressures (Figure 3) in the treated groups. Pomegranate juice compounds have an antihypertensive effect [16,40] so MPJ may have an inhibitory effect on angiotensin-converting enzyme [41,42] may reduce oxidative stress, improve mitochondrial function, and reduce chronic sympathetic nervous system activation in the paraventricular nucleus [43] and/or enhance nitric oxide/cGMP pathway signaling, as well as increase nitric oxide synthase bioactivity [44].
Pomegranate juice has been generally shown to have a hypoglycemic effect in human and rodents [45,46,47]. However, other studies in humans show no effect [48]. In this study, a trend of decreasing serum glucose levels was observed in the two higher MPJ-treated groups (Figure 4, MetS+MPJ2 and MetS+MPJ3) as time progressed. As MPJ is a pomegranate juice-based product, the action mechanisms should be similar to those previously found for fresh PJ, such as enhancing insulin secretion (without changing fasting glucose) [49] and increasing insulin sensitivity [50,51]. Ellagic acid (an essential component of pomegranate juice) is also known to up-regulate Glut-4 and PPAR-γ and increase insulin sensitivity conferred by pioglitazone [52]. Punicalagin has improved hyperglycemia, insulin, glutathione, and catalase activity levels in the streptozotocin-induced diabetic murine heart [53]. Pomegranate juice inhibits the action of resistin (a cytokine implicated in insulin resistance in obese subjects) [50,51], decreases inflammation, inhibits α-glucosidase and α-amylase, and maintains β-cell integrity [46].
Carotid atherosclerosis is a growing health problem; it is calculated that by 2020, 27.6% of adults aged 30-79 years will have carotid intima-media thickening worldwide, equivalent to 1,066.70 million people [54]. Diabetes, smoking, and hypertension are the most frequent risk factors for increased carotid intima-media thickness and carotid plaque [54], so this problem is closely related to MetS. In this study, serum triglyceride levels (Figure 7) significantly differed between the groups that did not receive 30% sucrose and those that did. Our results showed an excellent hypotriglyceridemic effect. Reports on the impact of pomegranate on triglycerides vary depending on the fraction or part of the pomegranate studied. For example, researchers reported increased triglyceride levels after administering pomegranate seed oil [55] while pomegranate seeds did not affect plasma triglyceride levels in other study [56]. In a study conducted by our research group, pomegranate juice diluted in water administered to diabetized CD-1 mice fed a high-fat diet had a hypotriglyceridemic effect [57]. It was also observed that MPJ administered orally in women with acute coronary syndrome for 30 days decreased triglyceride levels [23]. These results agree with those of Mirmiran et al. [58]; they supplemented subjects with hypertriglyceridemia with pomegranate seed oil capsules for four weeks, and a significant decrease in triglyceride levels, triglyceride/HDL ratio, and HDL cholesterol was found. In the last week, the MetS+ MPJ treatment had lower total cholesterol than MetS alone (Figure 5). Previous reports suggest that pomegranate may have a hypocholesterolemic effect during continuous and prolonged administration, as confirmed by a study in mice fed a high-fat diet and supplemented with pomegranate juice (300 µl/day) for 24 weeks. At week 12, a significant difference (p<0.05) was observed versus the group fed a high-fat diet and not supplemented with pomegranate [59]. Similarly, a study with commercial pomegranate juice for 14 weeks demonstrated a significant (p<0.05) reduction in total cholesterol in CD-1 mice [56]. The MPJ-treated groups had no discernable trend for HDL-c levels (Figure 6). Low HDL-c levels correlate with an elevated risk of coronary atherosclerosis [60]. The LDL-c levels were different from what was expected (due to sucrose, elevated levels were expected). The Ctrl group had higher LDL-c levels than the other groups, when hypothetically the groups with induced MetS should have higher levels. There are reports on the beneficial effect of pomegranate flower, seed and peel on these lipoproteins (increase of HDL-c and reduction of the total cholesterol/HDL-c ratio). In addition, a concentrated product based on pomegranate juice reduced LDL-c [61]. Pomegranate appears to regulate lipid metabolism by reducing oxidative damage, particularly lipid peroxidation. This effect is closely tied to enhancing cellular antioxidant capacity, including boosting levels of reduced glutathione (GSH) and total antioxidant capacity (TAC), as well as the activities of various antioxidant enzymes like glutathione peroxidase (GPx), glutathione reductase (GR), glutathione-S-transferase (GST), superoxide dismutase (SOD), and catalase (CAT). When cells face oxidative stress, they trigger the expression of genes for phase II detoxifying enzymes, largely through activating the Nrf2 transcription factor. Nrf2 moves into the nucleus, binding to response element promoters and prompting the transcription of phase II detoxifying enzymes such as SOD, HO-1, NQO-1, and γ-GCL. Research indicates that punicalagin and pomegranate extracts containing 40% punicalagin can activate Nrf2 and its downstream antioxidant enzymes. Therefore, pomegranate extracts have the potential to activate phase 2 enzymes, mitigating oxidative damage [21].
5. Conclusions
Daily MPJ supplementation in an animal model with MetS induced with 30% sucrose, had a palliative effect, as it was able to reduce systolic and diastolic blood pressure, glucose, triglycerides and cholesterol, preventing development of chronic diseases associated to MetS.
Author Contributions
José Antonio Guerrero-Solano: Conceptualization, Investigation, Visualization, Formal analysis, Software & Writing original draft. Juan Carlos Cancino: Validation, Methodology & Formal analysis. Osmar Antonio Jaramillo-Morales: Data curation, Analysis. Mirandeli Bautista and Juan Pablo Hernández-Uribe: Data curation & Validation. José Moisés Talamantes-Gómez & Carmen Valadez-Vega: Formal analysis. Helen Belefant-Miller: Formal analysis, Writing – review & editing. Gabriel Betanzos-Cabrera: Conceptualization, Methodology, Writing–review & editing, Supervision, Project administration & Funding acquisition.
Funding
This research received no external funding.
Institutional Review Board Statement
A veterinarian supervised the handling of the animals following the principles outlined in the National Institutes of Health Guide for the Care and Use of Laboratory Animals from the National Research Council Committee for the Update of the Guide for the and Use of Laboratory. The regulations of the “Norma Oficial Mexicana NOM-062-ZOO-1999”, for the technical specifications for the production, care, and use of laboratory animals were also followed.
Data Availability Statement
No Data Availability.
Acknowledgments
We thank Pedro Flores and José Morán-León for their technical assistance.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. Cardiovascular diseases (cvds). Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 5 March 2023).
- Ambroselli, D.; Masciulli, F.; Romano, E.; Catanzaro, G.; Besharat, Z.M.; Massari, M.C.; Ferretti, E.; Migliaccio, S.; Izzo, L.; Ritieni, A.; et al. New Advances in Metabolic Syndrome, from Prevention to Treatment: The Role of Diet and Food. Nutrients 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- James, M.; Varghese, T.P.; Sharma, R.; Chand, S. Association Between Metabolic Syndrome and Diabetes Mellitus According to International Diabetic Federation and National Cholesterol Education Program Adult Treatment Panel III Criteria: a Cross-sectional Study. J Diabetes Met Dis 2020, 19, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Yao, F.; Bo, Y.; Zhao, L.; Li, Y.; Ju, L.; Fang, H.; Piao, W.; Yu, D.; Lao, X. Prevalence and Influencing Factors of Metabolic Syndrome among Adults in China from 2015 to 2017. Nutrients 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Dayi, T.; Ozgoren, M. Effects of the Mediterranean diet on the components of metabolic syndrome. J Prevent Med Hygiene 2022, 63, E56–E64. [Google Scholar] [CrossRef]
- Zafar, U.; Khaliq, S.; Ahmad, H.U.; Manzoor, S.; Lone, K.P. Metabolic syndrome: an update on diagnostic criteria, pathogenesis, and genetic links. Hormones 2018, 17, 299–313. [Google Scholar] [CrossRef]
- Maslov, L.N.; Naryzhnaya, N.V.; Boshchenko, A.A.; Popov, S.V.; Ivanov, V.V.; Oeltgen, P.R. Is oxidative stress of adipocytes a cause or a consequence of the metabolic syndrome? J Clin Transl Endocrinol 2019, 15, 1–5. [Google Scholar] [CrossRef]
- Monserrat-Mesquida, M.; Quetglas-Llabrés, M.; Capó, X.; Bouzas, C.; Mateos, D.; Pons, A.; Tur, J.A.; Sureda, A. Metabolic Syndrome is Associated with Oxidative Stress and Proinflammatory State. Antioxidants 2020, 9. [Google Scholar] [CrossRef]
- Laurindo, L.F.; Barbalho, S.M.; Marquess, A.R.; Grecco, A.I.S.; Goulart, R.A.; Tofano, R.J.; Bishayee, A. Pomegranate (Punica granatum L.) and Metabolic Syndrome Risk Factors and Outcomes: A Systematic Review of Clinical Studies. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Ge, S.; Duo, L.; Wang, J.; GegenZhula; Yang, J.; Li, Z.; Tu, Y. A unique understanding of traditional medicine of pomegranate, Punica granatum L. and its current research status. J Ethnopharmacol 2021, 271, 113877. [Google Scholar] [CrossRef]
- Morvaridzadeh, M.; Sepidarkish, M.; Daneshzad, E.; Akbari, A.; Mobini, G.R.; Heshmati, J. The effect of pomegranate on oxidative stress parameters: A systematic review and meta-analysis. Compl Ther Med 2020, 48, 102252. [Google Scholar] [CrossRef]
- Pirzadeh, M.; Caporaso, N.; Rauf, A.; Shariati, M.A.; Yessimbekov, Z.; Khan, M.U.; Imran, M.; Mubarak, M.S. Pomegranate as a source of bioactive constituents: a review on their characterization, properties and applications. Crit Rev Food Sci Nut 2021, 61, 982–999. [Google Scholar] [CrossRef] [PubMed]
- Fahmy, H.; Hegazi, N.; El-Shamy, S.; Farag, M.A. Pomegranate juice as a functional food: a comprehensive review of its polyphenols, therapeutic merits, and recent patents. Food Funct 2020, 11, 5768–5781. [Google Scholar] [CrossRef] [PubMed]
- Hegazi, N.M.; El-Shamy, S.; Fahmy, H.; Farag, M.A. Pomegranate juice as a super-food: A comprehensive review of its extraction, analysis, and quality assessment approaches. J Food Comp Anal 2021, 97, 103773. [Google Scholar] [CrossRef]
- Singh, B.; Singh, J.P.; Kaur, A.; Singh, N. Phenolic compounds as beneficial phytochemicals in pomegranate (Punica granatum L.) peel: A review. Food Chem 2018, 261, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Ghaemi, F.; Emadzadeh, M.; Atkin, S.L.; Jamialahmadi, T.; Zengin, G.; Sahebkar, A. Impact of pomegranate juice on blood pressure: A systematic review and meta-analysis. Phytother Res 2023, 37, 4429–4441. [Google Scholar] [CrossRef]
- Gil, M.I.; Tomás-Barberán, F.A.; Hess-Pierce, B.; Holcroft, D.M.; Kader, A.A. Antioxidant activity of pomegranate juice and its relationship with phenolic composition and processing. J Agric Food Chem 2000, 48, 4581–4589. [Google Scholar] [CrossRef]
- Akhtar, S.; Ismail, T.; Fraternale, D.; Sestili, P. Pomegranate peel and peel extracts: chemistry and food features. Food Chem 2015, 174, 417–425. [Google Scholar] [CrossRef]
- Vučić, V.; Grabež, M.; Trchounian, A.; Arsić, A. Composition and Potential Health Benefits of Pomegranate: A Review. Curr Pharm Design 2019, 25, 1817–1827. [Google Scholar] [CrossRef]
- AlMatar, M.; Islam, M.R.; Albarri, O.; Var, I.; Koksal, F. Pomegranate as a Possible Treatment in Reducing Risk of Developing Wound Healing, Obesity, Neurodegenerative Disorders, and Diabetes Mellitus. Mini Rev Med Chem 2018, 18, 507–526. [Google Scholar] [CrossRef]
- Hou, C.; Zhang, W.; Li, J.; Du, L.; Lv, O.; Zhao, S.; Li, J. Beneficial Effects of Pomegranate on Lipid Metabolism in Metabolic Disorders. Mol Nut Food Res 2019, 63, e1800773. [Google Scholar] [CrossRef]
- Medjakovic, S.; Jungbauer, A. Pomegranate: a fruit that ameliorates metabolic syndrome. Food Funct 2013, 4, 19–39. [Google Scholar] [CrossRef] [PubMed]
- Estrada-Luna, D.; Carreón-Torres, E.; Bautista-Pérez, R.; Betanzos-Cabrera, G.; Dorantes-Morales, A.; Luna-Luna, M.; Vargas-Barrón, J.; Mejía, A.M.; Fragoso, J.M.; Carvajal-Aguilera, K.; et al. Microencapsulated Pomegranate Reverts High-Density Lipoprotein (HDL)-Induced Endothelial Dysfunction and Reduces Postprandial Triglyceridemia in Women with Acute Coronary Syndrome. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- El Hafidi, M.; Pérez, I.; Zamora, J.; Soto, V.; Carvajal-Sandoval, G.; Baños, G. Glycine intake decreases plasma free fatty acids, adipose cell size, and blood pressure in sucrose-fed rats. Am J Physiol. Reg Int Comp Physiol 2004, 287, R1387–1393. [Google Scholar] [CrossRef] [PubMed]
- Ventura-Clapier, R.; Piquereau, J.; Garnier, A.; Mericskay, M.; Lemaire, C.; Crozatier, B. Gender issues in cardiovascular diseases. Focus on energy metabolism. Bioch Biophys Acta 2020, 1866, 165722. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Cervantes, P.; Izquierdo-Vega, J.A.; Morán-León, J.; Guerrero-Solano, J.A.; García-Pérez, B.E.; Cancino-Díaz, J.C.; Belefant-Miller, H.; Betanzos-Cabrera, G. Subacute and subchronic toxicity of microencapsulated pomegranate juice in rats and mice. Toxicol Res 2021, 10, 312–324. [Google Scholar] [CrossRef]
- Preda, A.; Carbone, F.; Tirandi, A.; Montecucco, F.; Liberale, L. Obesity phenotypes and cardiovascular risk: From pathophysiology to clinical management. Rev Endocr Met Dis 2023, 24, 901–919. [Google Scholar] [CrossRef]
- Méndez-Gaspar, V.; Sánchez-Meza, K.; López-Alcaraz, F.; Palacios-Fonseca, A.J.; del Toro-Equihua, M.; Montero-Cruz, S.A.; Hummel, J.; Cerna-Cortés, J.F.; Cerna-Cortés, J. Reducción de la ingesta de alimento balanceado por consumo de agua endulzada con sacarosa en ratas Wistar. Acta Bioquím Clín Latinoam 2020, 54, 279–284. [Google Scholar]
- Villanueva-Gutiérrez, S.; Villegas Sepúlveda, N.; Olmedo-Buenrostro, B.; Virgen-Ortiz, A.; Palacios Fonseca, A.; López Alcaraz, F. Análisis comparativo del consumo crónico de agua endulzada con sacarosa o stevia con respecto al peso corporal, la cantidad de alimento consumido y el desarrollo de diabetes y dislipidemias en ratas Wistar. Temas Cienc Tecnol 2017, 21, 30–38. [Google Scholar]
- Chapman, I.M.; Goble, E.A.; Wittert, G.A.; Morley, J.E.; Horowitz, M. Effect of intravenous glucose and euglycemic insulin infusions on short-term appetite and food intake. Am J Physiol 1998, 274, R596–603. [Google Scholar] [CrossRef]
- Ahmed, M.M.; Samir el, S.A.; El-Shehawi, A.M.; Alkafafy, M.E. Anti-obesity effects of Taif and Egyptian pomegranates: molecular study. Biosci Biotechnol Biochem 2015, 79, 598–609. [Google Scholar] [CrossRef]
- Hassan, N.F.; Soliman, G.M.; Okasha, E.F.; Shalaby, A.M. Histological, Immunohistochemical, and Biochemical Study of Experimentally Induced Fatty Liver in Adult Male Albino Rat and the Possible Protective Role of Pomegranate. J Micros Ultrastruct 2018, 6, 44–55. [Google Scholar] [CrossRef]
- Les, F.; Carpéné, C.; Arbonés-Mainar, J.M.; Decaunes, P.; Valero, M.S.; López, V. Pomegranate juice and its main polyphenols exhibit direct effects on amine oxidases from human adipose tissue and inhibit lipid metabolism in adipocytes. J Funct Foods 2017, 33, 323–331. [Google Scholar] [CrossRef]
- Lei, F.; Zhang, X.N.; Wang, W.; Xing, D.M.; Xie, W.D.; Su, H.; Du, L.J. Evidence of anti-obesity effects of the pomegranate leaf extract in high-fat diet induced obese mice. Int J Obesity (2005) 2007, 31, 1023–1029. [Google Scholar] [CrossRef]
- Zou, X.; Yan, C.; Shi, Y.; Cao, K.; Xu, J.; Wang, X.; Chen, C.; Luo, C.; Li, Y.; Gao, J.; et al. Mitochondrial dysfunction in obesity-associated nonalcoholic fatty liver disease: the protective effects of pomegranate with its active component punicalagin. Antiox Redox Sign 2014, 21, 1557–1570. [Google Scholar] [CrossRef]
- Ok, E.; Do, G.M.; Lim, Y.; Park, J.E.; Park, Y.J.; Kwon, O. Pomegranate vinegar attenuates adiposity in obese rats through coordinated control of AMPK signaling in the liver and adipose tissue. Lip Health Dis 2013, 12, 163. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol 2021, 20, 795–820. [Google Scholar] [CrossRef]
- Bahari, H.; Omidian, K.; Goudarzi, K.; Rafiei, H.; Asbaghi, O.; Hosseini Kolbadi, K.S.; Naderian, M.; Hosseini, A. The effects of pomegranate consumption on blood pressure in adults: A systematic review and meta-analysis. Phytother Res 2024. [Google Scholar] [CrossRef]
- Mohan, M.; Waghulde, H.; Kasture, S. Effect of pomegranate juice on Angiotensin II-induced hypertension in diabetic Wistar rats. Phytother Res 2010, 24 Suppl 2, S196–203. [Google Scholar] [CrossRef]
- Wang, J.; Rong, X.; Um, I.S.; Yamahara, J.; Li, Y. 55-week treatment of mice with the unani and ayurvedic medicine pomegranate flower ameliorates ageing-associated insulin resistance and skin abnormalities. Evid Based Comp Altern Med 2012, 2012, 350125. [Google Scholar] [CrossRef]
- Sun, W.; Yan, C.; Frost, B.; Wang, X.; Hou, C.; Zeng, M.; Gao, H.; Kang, Y.; Liu, J. Pomegranate extract decreases oxidative stress and alleviates mitochondrial impairment by activating AMPK-Nrf2 in hypothalamic paraventricular nucleus of spontaneously hypertensive rats. Sci Rep 2016, 6, 34246. [Google Scholar] [CrossRef]
- Shao, J.; Wang, P.; Liu, A.; Du, X.; Bai, J.; Chen, M. Punicalagin Prevents Hypoxic Pulmonary Hypertension via Anti-Oxidant Effects in Rats. Am J Chin Med 2016, 44, 785–801. [Google Scholar] [CrossRef]
- Chakraborty, M.; Ahmed, M.G.; Bhattacharjee, A. The potential for interaction of tolbutamide with pomegranate juice against diabetic induced complications in rats. Integr Med Res 2017, 6, 354–360. [Google Scholar] [CrossRef]
- Olvera-Sandoval, C.; Fabela-Illescas, H.E.; Fernández-Martínez, E.; Ortiz-Rodríguez, M.A.; Cariño-Cortés, R.; Ariza-Ortega, J.A.; Hernández-González, J.C.; Olivo, D.; Valadez-Vega, C.; Belefant-Miller, H.; et al. Potential Mechanisms of the Improvement of Glucose Homeostasis in Type 2 Diabetes by Pomegranate Juice. Antioxidants 2022, 11. [Google Scholar] [CrossRef]
- Virgen-Carrillo, C.A.; Martínez Moreno, A.G.; Valdés Miramontes, E.H. Potential Hypoglycemic Effect of Pomegranate Juice and Its Mechanism of Action: A Systematic Review. J Med Food 2020, 23, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sohrab, G.; Roshan, H.; Ebrahimof, S.; Nikpayam, O.; Sotoudeh, G.; Siasi, F. Effects of pomegranate juice consumption on blood pressure and lipid profile in patients with type 2 diabetes: A single-blind randomized clinical trial. Clin Nutr 2019, 29, 30–35. [Google Scholar] [CrossRef]
- Nekooeian, A.A.; Eftekhari, M.H.; Adibi, S.; Rajaeifard, A. Effects of pomegranate seed oil on insulin release in rats with type 2 diabetes. Iran J Med Sci 2014, 39, 130–135. [Google Scholar]
- Huang, T.H.; Peng, G.; Kota, B.P.; Li, G.Q.; Yamahara, J.; Roufogalis, B.D.; Li, Y. Anti-diabetic action of Punica granatum flower extract: activation of PPAR-gamma and identification of an active component. Toxicol Appl Pharmacol 2005, 207, 160–169. [Google Scholar] [CrossRef]
- Huang, T.H.; Yang, Q.; Harada, M.; Li, G.Q.; Yamahara, J.; Roufogalis, B.D.; Li, Y. Pomegranate flower extract diminishes cardiac fibrosis in Zucker diabetic fatty rats: modulation of cardiac endothelin-1 and nuclear factor-kappaB pathways. J Cardiovasc Pharmacol 2005, 46, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Nankar, R.P.; Doble, M. Ellagic acid potentiates insulin sensitising activity of pioglitazone in L6 myotubes. J Funct Foods 2015, 15, 1–10. [Google Scholar] [CrossRef]
- El-Missiry, M.A.; Amer, M.A.; Hemieda, F.A.E.; Othman, A.I.; Sakr, D.A.; Abdulhadi, H.L. Cardioameliorative effect of punicalagin against streptozotocin-induced apoptosis, redox imbalance, metabolic changes and inflammation. Egyp J Basic Appl Sci 2015, 2, 247–260. [Google Scholar] [CrossRef]
- Song, P.; Fang, Z.; Wang, H.; Cai, Y.; Rahimi, K.; Zhu, Y.; Fowkes, F.G.R.; Fowkes, F.J.I.; Rudan, I. Global and regional prevalence, burden, and risk factors for carotid atherosclerosis: a systematic review, meta-analysis, and modelling study. Lancet Glob Health 2020, 8, e721–e729. [Google Scholar] [CrossRef]
- Yamasaki, M.; Kitagawa, T.; Koyanagi, N.; Chujo, H.; Maeda, H.; Kohno-Murase, J.; Imamura, J.; Tachibana, H.; Yamada, K. Dietary effect of pomegranate seed oil on immune function and lipid metabolism in mice. Nutrition 2006, 22, 54–59. [Google Scholar] [CrossRef]
- McFarlin, B.K.; Strohacker, K.A.; Kueht, M.L. Pomegranate seed oil consumption during a period of high-fat feeding reduces weight gain and reduces type 2 diabetes risk in CD-1 mice. Brit J Nutr 2009, 102, 54–59. [Google Scholar] [CrossRef]
- Betanzos-Cabrera, G.; Guerrero-Solano, J.A.; Martínez-Pérez, M.M.; Calderón-Ramos, Z.G.; Belefant-Miller, H.; Cancino-Diaz, J.C. Pomegranate juice increases levels of paraoxonase1 (PON1) expression and enzymatic activity in streptozotocin-induced diabetic mice fed with a high-fat diet. Food Res Int 2011, 44, 1381–1385. [Google Scholar] [CrossRef]
- Mirmiran, P.; Fazeli, M.R.; Asghari, G.; Shafiee, A.; Azizi, F. Effect of pomegranate seed oil on hyperlipidaemic subjects: a double-blind placebo-controlled clinical trial. Brit J Nutr 2010, 104, 402–406. [Google Scholar] [CrossRef]
- Estrada-Luna, D.; Martínez-Hinojosa, E.; Cancino-Diaz, J.C.; Belefant-Miller, H.; López-Rodríguez, G.; Betanzos-Cabrera, G. Daily supplementation with fresh pomegranate juice increases paraoxonase 1 expression and activity in mice fed a high-fat diet. Eur J Nutr 2018, 57, 383–389. [Google Scholar] [CrossRef]
- Casula, M.; Colpani, O.; Xie, S.; Catapano, A.L.; Baragetti, A. HDL in Atherosclerotic Cardiovascular Disease: In Search of a Role. Cells 2021, 10. [Google Scholar] [CrossRef]
- Esmaillzadeh, A.; Tahbaz, F.; Gaieni, I.; Alavi-Majd, H.; Azadbakht, L. Concentrated pomegranate juice improves lipid profiles in diabetic patients with hyperlipidemia. J Med Food 2004, 7, 305–308. [Google Scholar] [CrossRef]
- Flores-Chávez, P.; Infante-Vázquez, O.; Sánchez-Torres, G.; Martínez-Memije, R.; Rodríguez-Rossini, G. A non-invasive methods to record vital signs in rats. Vet Mex 2002, 22, 179–187. [Google Scholar]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 1972, 18, 499–502. [Google Scholar] [CrossRef]
Figure 1.
Confirmed criteria for the metabolic syndrome diagnosis in Wistar rats after twenty weeks of 30% sucrose-induced metabolic syndrome. Panel: a) Triglycerides; b) Glucose, and c) HDL-c. Statistically significant differences between Ctrl and MetS groups for the variables (p<0.05) after 20 weeks of metabolic syndrome induction.
Figure 1.
Confirmed criteria for the metabolic syndrome diagnosis in Wistar rats after twenty weeks of 30% sucrose-induced metabolic syndrome. Panel: a) Triglycerides; b) Glucose, and c) HDL-c. Statistically significant differences between Ctrl and MetS groups for the variables (p<0.05) after 20 weeks of metabolic syndrome induction.
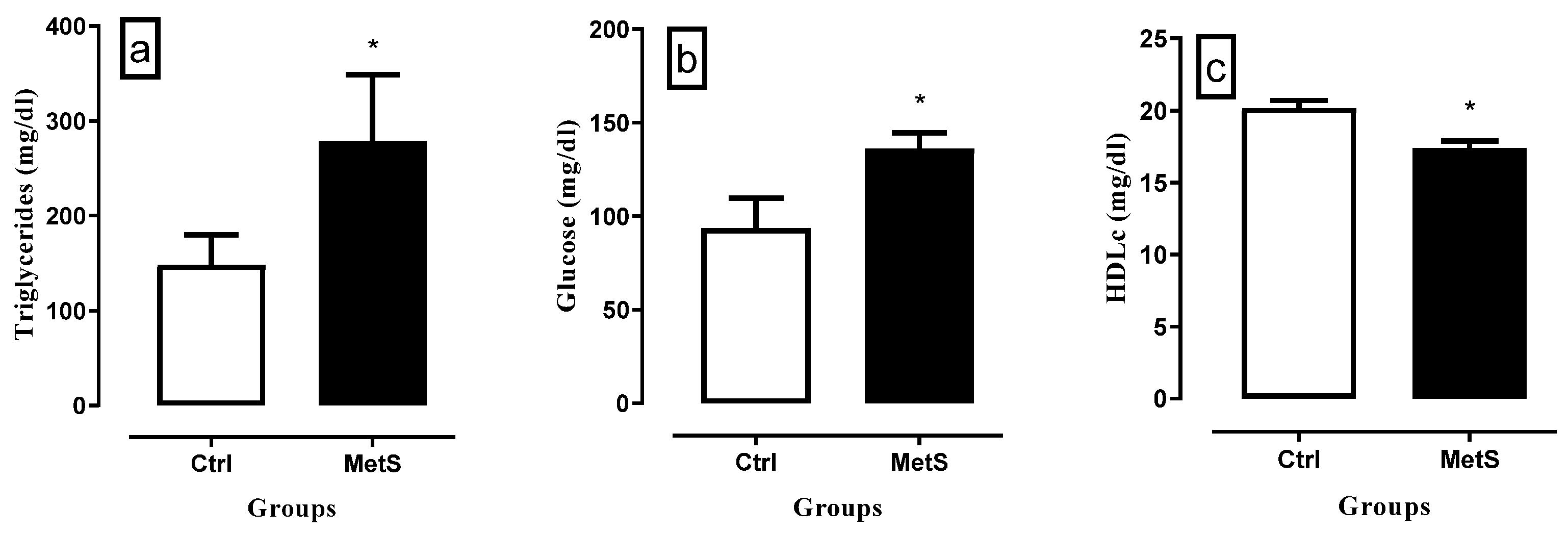
Figure 2.
Body weight of Wistar rats with MetS after being treated with MPJ. Mean ± SD of the bodyweight of the different treatment groups. No statistically significant difference was found between groups (p < 0.05). Ctrl = Control; MetS = Metabolic syndrome; Placebo = 30% sucrose + maltodextrin-gum arabic encapsulating matrix without pomegranate juice; Ctrl+MPJ = MPJ control (water + MPJ 1800 mg/kg); MetS+MPJ1 = 30% sucrose + MPJ 600 mg/kg; MetS+MPJ2 = 30% sucrose + MPJ 1800 mg/kg; MetS+MPJ3= 30% sucrose + MPJ 2900 mg/kg.
Figure 2.
Body weight of Wistar rats with MetS after being treated with MPJ. Mean ± SD of the bodyweight of the different treatment groups. No statistically significant difference was found between groups (p < 0.05). Ctrl = Control; MetS = Metabolic syndrome; Placebo = 30% sucrose + maltodextrin-gum arabic encapsulating matrix without pomegranate juice; Ctrl+MPJ = MPJ control (water + MPJ 1800 mg/kg); MetS+MPJ1 = 30% sucrose + MPJ 600 mg/kg; MetS+MPJ2 = 30% sucrose + MPJ 1800 mg/kg; MetS+MPJ3= 30% sucrose + MPJ 2900 mg/kg.
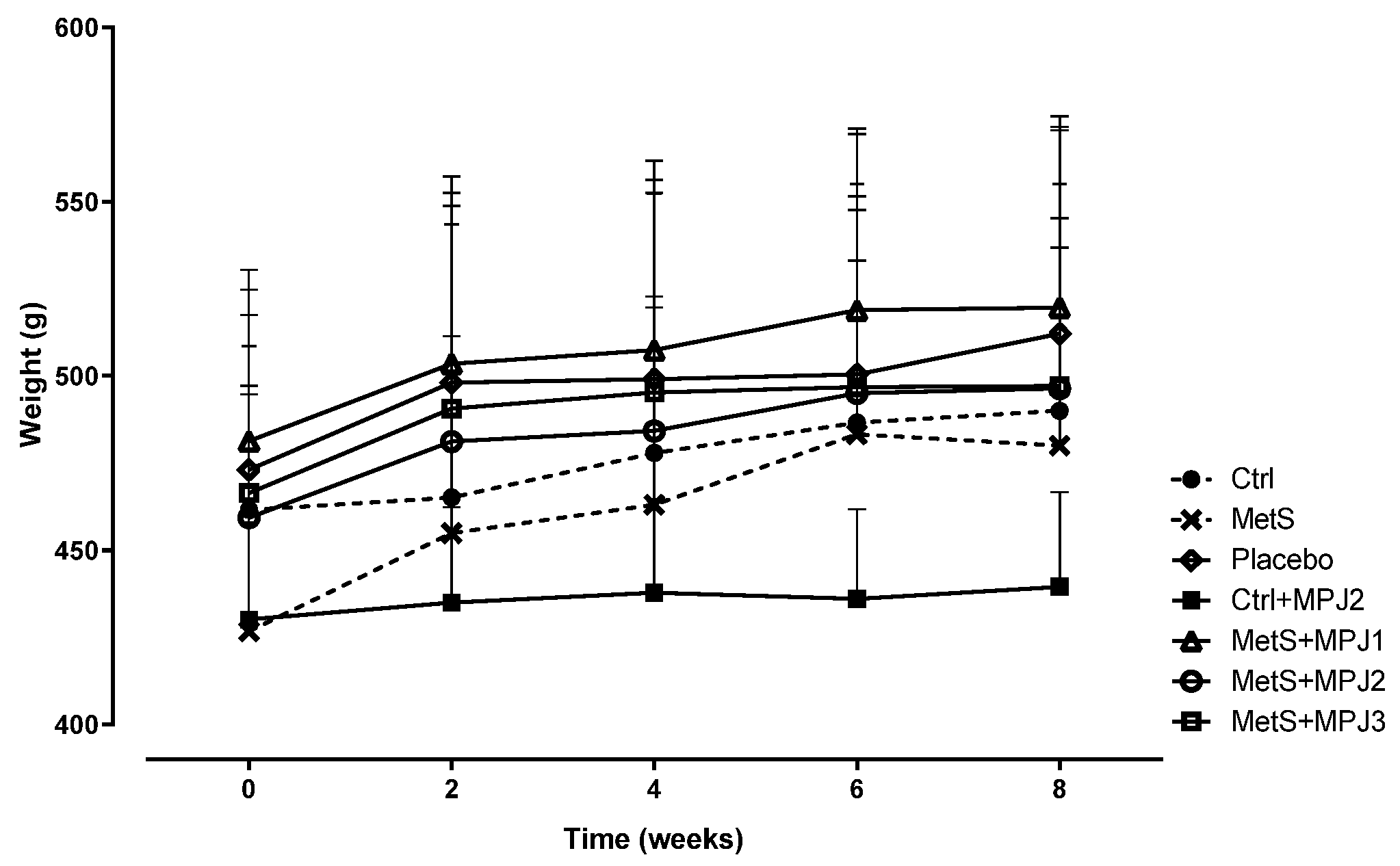
Figure 3.
Systolic (SBP) and diastolic blood pressure (DBP) of Wistar rats with MetS after being treated with MPJ. Mean ± SD of the systolic and diastolic blood pressure of groups. *= statistically significant difference versus MetS group (p<0.05). Ctrl = Control; MetS = Metabolic syndrome; MetS+MPJ1 = 30% sucrose + MPJ 600 mg/kg; MetS+MPJ2 = 30% sucrose + MPJ 1800 mg/kg; MetS+MPJ3= 30% sucrose + MPJ 2900 mg/kg.
Figure 3.
Systolic (SBP) and diastolic blood pressure (DBP) of Wistar rats with MetS after being treated with MPJ. Mean ± SD of the systolic and diastolic blood pressure of groups. *= statistically significant difference versus MetS group (p<0.05). Ctrl = Control; MetS = Metabolic syndrome; MetS+MPJ1 = 30% sucrose + MPJ 600 mg/kg; MetS+MPJ2 = 30% sucrose + MPJ 1800 mg/kg; MetS+MPJ3= 30% sucrose + MPJ 2900 mg/kg.
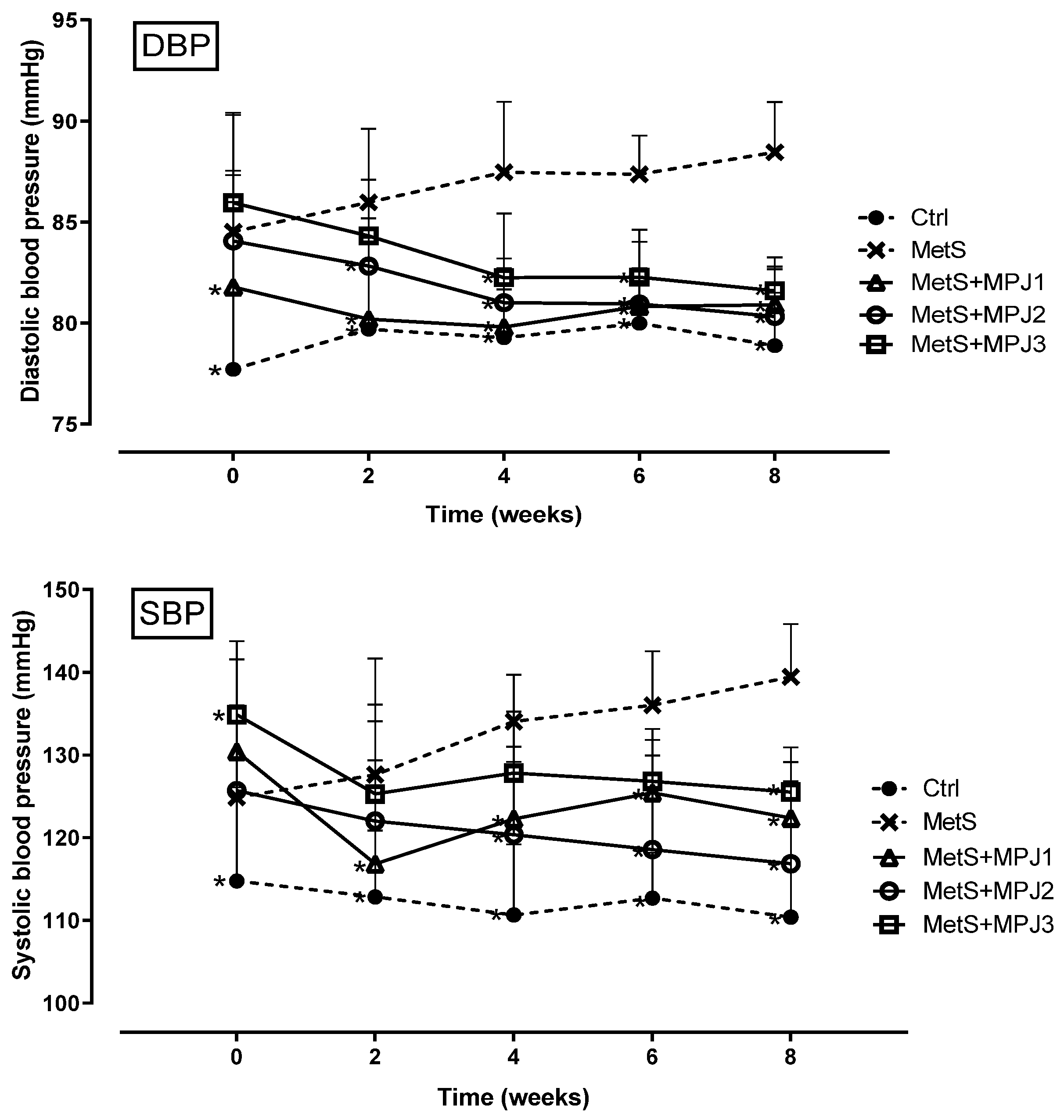
Figure 4.
Glucose of Wistar rats with MetS after being treated with MPJ. Mean ± SD of the glucose of the different treatment groups. *= statistically significant difference versus MetS group (p<0.05). Ctrl = Control; MetS = Metabolic syndrome; MetS+MPJ1 = 30% sucrose + MPJ 600 mg/kg; MetS+MPJ2 = 30% sucrose + MPJ 1800 mg/kg; MetS+MPJ3= 30% sucrose + MPJ 2900 mg/kg.
Figure 4.
Glucose of Wistar rats with MetS after being treated with MPJ. Mean ± SD of the glucose of the different treatment groups. *= statistically significant difference versus MetS group (p<0.05). Ctrl = Control; MetS = Metabolic syndrome; MetS+MPJ1 = 30% sucrose + MPJ 600 mg/kg; MetS+MPJ2 = 30% sucrose + MPJ 1800 mg/kg; MetS+MPJ3= 30% sucrose + MPJ 2900 mg/kg.
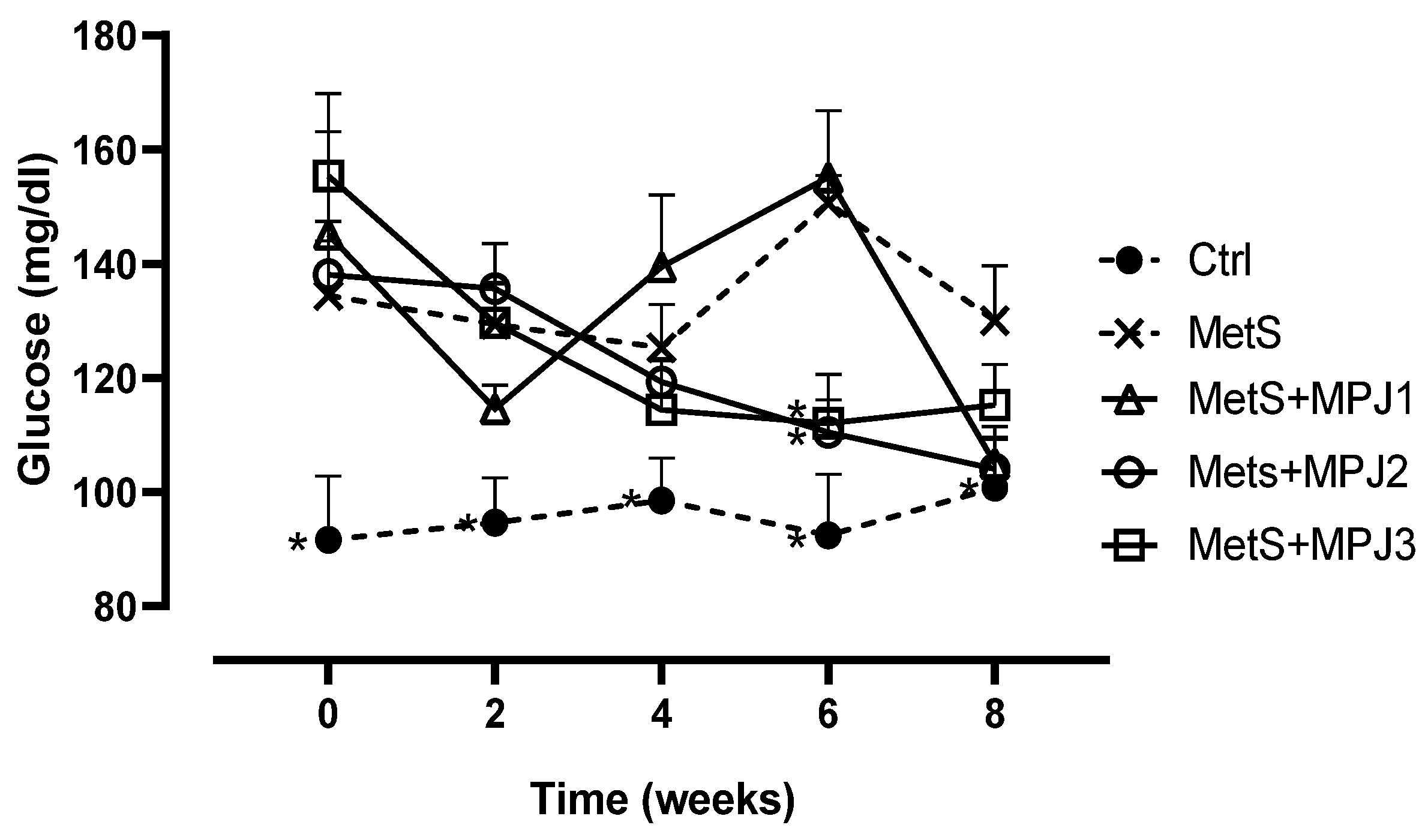
Figure 5.
Total cholesterol of Wistar rats with MetS after being treated with MPJ. Mean ± SD of the total cholesterol of the different treatment groups. *= statistically significant difference versus MetS group (p<0.05). Ctrl = Control; MetS = Metabolic syndrome; MetS+MPJ1 = 30% sucrose + MPJ 600 mg/kg; MetS+MPJ2 = 30% sucrose + MPJ 1800 mg/kg; MetS+MPJ3= 30% sucrose + MPJ 2900 mg/kg.
Figure 5.
Total cholesterol of Wistar rats with MetS after being treated with MPJ. Mean ± SD of the total cholesterol of the different treatment groups. *= statistically significant difference versus MetS group (p<0.05). Ctrl = Control; MetS = Metabolic syndrome; MetS+MPJ1 = 30% sucrose + MPJ 600 mg/kg; MetS+MPJ2 = 30% sucrose + MPJ 1800 mg/kg; MetS+MPJ3= 30% sucrose + MPJ 2900 mg/kg.
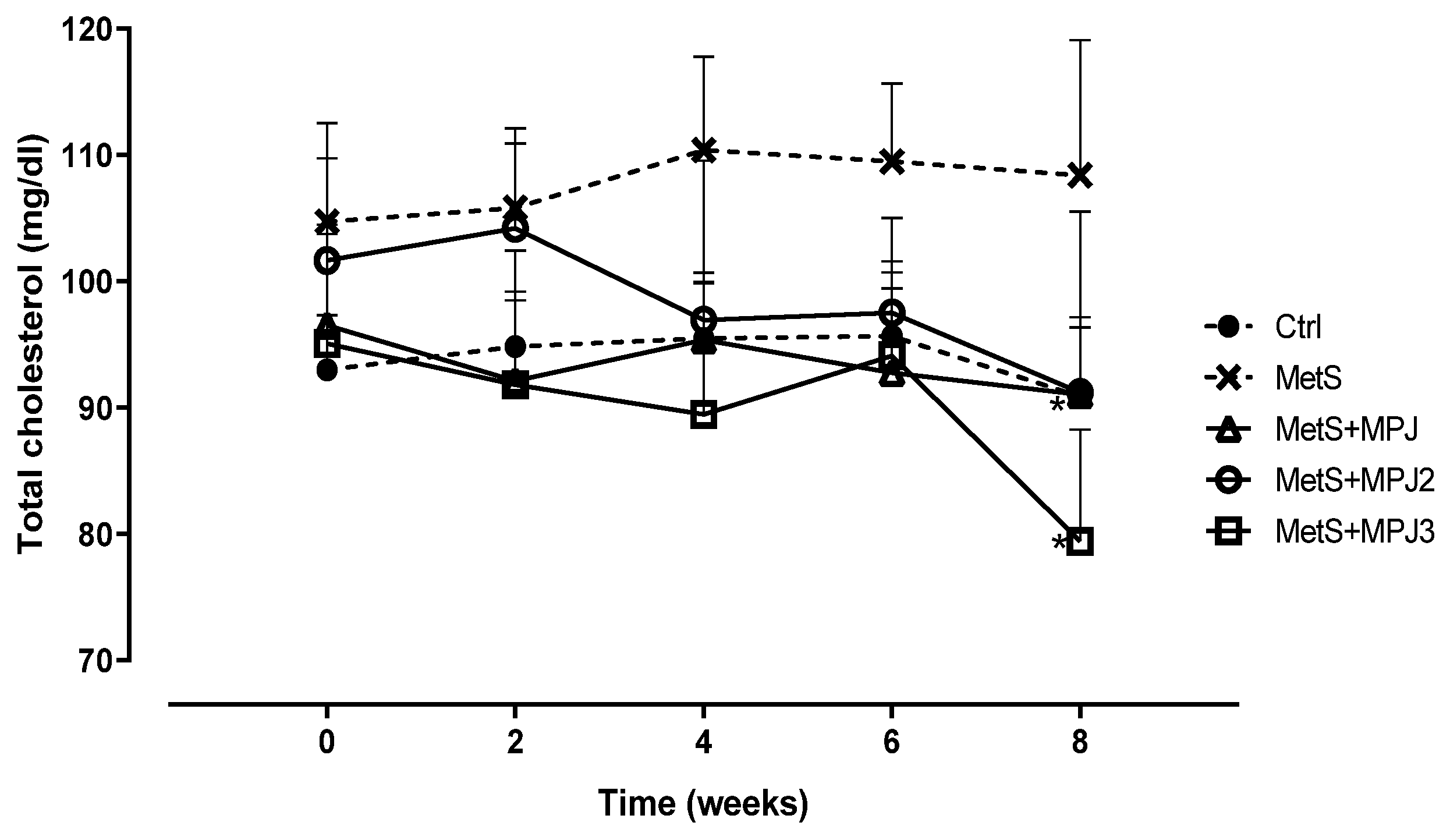
Figure 6.
LDL-c and HDL-c of Wistar rats with MetS after being treated with MPJ. Mean ± SD of LDL-c and HDL-c. *= statistically significant difference versus MetS group (p < 0.05). Ctrl = Control; MetS = Metabolic syndrome; MetS+MPJ1 = 30% sucrose + MPJ 600 mg/kg; MetS+MPJ2 = 30% sucrose + MPJ 1800 mg/kg; MetS+MPJ3= 30% sucrose + MPJ 2900 mg/kg. Week 8 tests were lost.
Figure 6.
LDL-c and HDL-c of Wistar rats with MetS after being treated with MPJ. Mean ± SD of LDL-c and HDL-c. *= statistically significant difference versus MetS group (p < 0.05). Ctrl = Control; MetS = Metabolic syndrome; MetS+MPJ1 = 30% sucrose + MPJ 600 mg/kg; MetS+MPJ2 = 30% sucrose + MPJ 1800 mg/kg; MetS+MPJ3= 30% sucrose + MPJ 2900 mg/kg. Week 8 tests were lost.

Figure 7.
Triglycerides of Wistar rats with MetS after being treated with MPJ. Mean ± SD of Triglycerides *= statistically significant difference versus MetS group (p < 0.05). Ctrl = Control; MetS = Metabolic syndrome; MetS+MPJ1 = 30% sucrose + MPJ 600 mg/kg; MetS+MPJ2 = 30% sucrose + MPJ 1800 mg/kg; MetS+MPJ3= 30% sucrose + MPJ 2900 mg/kg.
Figure 7.
Triglycerides of Wistar rats with MetS after being treated with MPJ. Mean ± SD of Triglycerides *= statistically significant difference versus MetS group (p < 0.05). Ctrl = Control; MetS = Metabolic syndrome; MetS+MPJ1 = 30% sucrose + MPJ 600 mg/kg; MetS+MPJ2 = 30% sucrose + MPJ 1800 mg/kg; MetS+MPJ3= 30% sucrose + MPJ 2900 mg/kg.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



