
Submitted:
20 September 2024
Posted:
23 September 2024
You are already at the latest version
Abstract
Background: Skin- (SSM) and nipple-sparing (NSM) mastectomies are frequently performed surgeries with a considerable risk for post-operative hematoma or seroma. Tranexamic acid (TXA) is a potent antifibrinolytic drug commonly used in many surgical fields but rather novel in plastic and specifically breast surgery. This study investigates the influence of TXA in patients undergoing SSM or NSM with expander-based reconstruction (EbR) on post-operative outcomes. Methodology: A retrospective study was conducted on 132 patients undergoing uni- or bilateral SSM or NSM with EbR between May 2015 and March 2022. Patients receiving systemic TXA treatment for 48 hours following a standardized protocol were compared to those who received no treatment. Multivariable linear regression was performed to identify influencing factors and quantify their effect on drainage volume, duration of drain placement, length of hospital stay, post-operative bleeding, and seroma formation. Results: 132 patients underwent a total of 155 mastectomies (72 in the TXA group, 83 in the control group). TXA significantly reduced drainage volume (-22.3ml, P=0.011). Duration of drain placement and length of hospital stay were significantly shorter in the TXA group (P<0.001 and P=0.001). No significant side effects were reported. Conclusion: TXA is a safe drug if administered respecting the well-defined contraindications. Systemic TXA administration significantly reduces drainage volume in patients undergoing SSM or NSM and should encourage surgeons to reconsider using drains in post-operative protocols. Duration of drain placement and length of hospital stay were significantly reduced in the TXA group but other factors like resection weight might have a more substantial impact.
Keywords:
tranexamic acid
; systemic tranexamic acid
; mastectomy
; complications
; drainage
; expander
1. Introduction
Tranexamic acid (TXA) is one of the most widely used and studied antifibrinolytic drugs in medical practice today. It acts as a lysine analogue blocking lysine receptors on plasminogen, thereby decreasing its conversion to plasmin [1]. Furthermore, it acts directly as an anti-plasmin agent [2]. Plasmin in turn is an important enzyme active in the degradation of many blood plasma proteins, including fibrin which is present in blood clots, but also part of inflammatory processes [3,4]. Through this mechanism of action, it can be used to treat blood loss in many situations, first and foremost massive hemorrhage after trauma [5] or post-partum[6]. In recent years its use in perioperative blood loss prevention has been increasing and studies have shown decreased mortality and need for blood transfusions post-operatively when TXA was administered[7]. Therefore, it is now considered a standard in many fields such as orthopedic and cardiothoracic surgery.
Other studies have further investigated its effect on inflammatory pathways and have found that TXA reduces several inflammatory cytokines[8] including IL-10[9], IL-6[10,11,12], TNFα[10,11,13], and CRP[12], and reduces the transvasal migration of leukocytes after reperfusion[14]. Furthermore, studies have shown that TXA normalizes vascular permeability after pathological situations, therefore decreasing extravasal fluid accumulation[8,15].
Plastic surgery, including reconstructive and aesthetic procedures, presents a wide range of possible applications of TXA since many operations are associated with extended tissue undermining, respectively a large wound surface. More recently, some evidence has also emerged from both aesthetic and non-aesthetic breast surgery. Literature shows that the application of TXA significantly reduces the incidence of post-operative hematoma in patients undergoing breast surgery, particularly in aesthetic procedures[16]. Furthermore, studies have shown a significant reduction in post-operative drainage volume and length of hospital stay after surgery for breast cancer including axillary lymph node dissection, lumpectomy, and mastectomy[17,18]. However, the available literature is scarce, especially on the use of TXA in patients undergoing mastectomy.
Mastectomies are associated with a high risk of post-operative complications like hematoma and seroma with an incidence of 2.3-3.3%[19,20,21] and 6.9-51%[21,22,23] respectively. These complications can lead to surgical revision, increased patient comorbidity, higher infection risk, prolonged hospitalization, and eventually delay of further oncological treatment[24,25,26,27]. Many mastectomy techniques have been developed over the years, from the radical mastectomy by Halsted[28], through the modified radical[29] and simple mastectomy[30] up to techniques that preserve the skin envelope, including skin-sparing (SSM)[31], nipple-sparing (NSM)[32], and skin reducing mastectomy (SRM)[33,34], common nowadays. These techniques have different indications and present with different complications and although previous studies have not shown any significant variance in drainage volume between these mastectomy techniques[35,36], the differentiation between skin-sparing (including SSM, NSM, and SRM), and simple/radical mastectomy seems inherent due to the difference in pocket size and thus wound surface.
Although the exact formation process has not yet been fully elucidated, it is known that drainage fluid is composed of both blood and serous fluid which in turn consist of inflammatory exudates produced as a physiological reaction to surgical trauma through ultrafiltration of the blood. Several studies have identified risk factors for excessive fluid production or seroma formation which include the type of surgery (breast-conserving vs. mastectomy)[37,38], number and extent of axillar lymph node involvement[39], and extent of dissection[40]. Furthermore, lymphatic leakage following axillar lymph node surgery was identified as a contributing factor to seroma formation[26,41].
In June 2019 we implemented a change in regimen wherein all patients undergoing mastectomy received a 48-hour systemic administration of TXA perioperatively given there are no contraindications. This study aims to evaluate the effect of systemic TXA administration on drainage volume, duration of drain placement, length of hospital stay, and incidence of post-operative complications, namely hematoma and seroma in patients undergoing mastectomy with immediate expander-based reconstruction (EbR).
2. Materials and Methods
2.1. Study Design
After approval by the local ethics committee (BASEC number 2021-01918), a retrospective study was performed according to the STROBE guidelines of 132 patients undergoing immediate EbR at a single institution between 2015 and 2022. Inclusion criteria included all female patients over 18 who gave informed consent and who underwent SSM, NSM, or SRM for breast cancer or as a prophylactic intervention in gene carriers or high-risk patients. The exclusion criteria were: TXA-administration other than the mentioned 48-hour protocol, previous surgery on the breast of interest, alterations in preoperative coagulation lab, and pregnancy.
Data was collected from patient files, including operations reports and drainage volume measurements conducted by ward nurses and checked by resident doctors throughout the hospital stay.
Patients were divided into two groups: The case group (patients operated on after June 2019) including 83 breasts receiving the 48-hour TXA protocol (1g i.v. at the beginning of surgery, followed by 1g i.v. every eight hours for the first 24 hours and 1g p.o. every eight hours for the following 24 hours post-operatively) and 72 breasts in the control group (patients operated on before June 2019) who did not receive TXA.
The primary outcome measure was drainage volume, and the two secondary outcome measures included duration of drain placement and respectively length of hospital stay. The mastectomy was performed by one of two senior breast surgeons, while expander implantation was performed in a pre- or sub-pectoral manner by one of two senior plastic surgeons.
Age was calculated as the difference between date of birth and date of surgery. Body mass index (BMI) was calculated using height and weight before surgery. Comorbidities were extracted from previous medical history and included: hypertension, diabetes mellitus (type 1 and 2), heart disease including arrhythmias, conduction problems, atrial fibrillation, and cardiomyopathies as well as kidney disease including chronic renal insufficiency and chronic kidney disease. Current smoking, chronic NSAID use, antiaggregation and anticoagulation therapy, previous thromboembolic events, previous radiotherapy, and neoadjuvant chemotherapy were further extracted from previous medical history. The biochemical variables thrombocytes, QUICK, and international normalized ratio (INR) were also recorded within one year previous to the operation if no confounding factors such as neoadjuvant chemotherapy were present. The side of the operated breast (right or left), resection weight, type of mastectomy (skin sparing, nipple sparing, skin reducing), sentinel lymph node biopsy, axillar lymph node dissection, additional axillar access, expander placement (prepectoral/subpectoral), expander type (Allergan Natrelle 133 (AbbVie Inc., North Chicago, Illinois, USA), Mentor CPX4 (Johnson & Johnson Services, Inc., New Brunswick, New Jersey, USA), Motiva Flora (Establishment Labs® S.A, Alajuela, Costa Rica)), synthetic mesh application, and biologic mesh (acellular dermal matrix) application were extracted from surgical reports. Axillar lymph node dissection ad continuitatem was defined as patients with axillar lymph node dissection but no additional axillar access.
The complications hematoma and seroma were recorded within the first month after surgery. Drainage volume was measured from the first post-operative day until its removal. To best standardize the time-point of drain removal for the duration of drain placement, the total days until measured fluid production was less than 30ml/24 hours were calculated. 30ml was chosen as a common cut-off value for drainage after breast reconstruction with expanders[42]. Length of hospital stay was defined as days from surgery until discharge.
2.2. Statistical Analysis
Quantitative data were presented as mean with standard deviation or as median with the corresponding 25th and 75th percentiles. Qualitative data were presented as percentages with absolute numbers. Variables were compared between subjects receiving TXA and subjects not receiving TXA using Student t-test, Mann-Whitney test, chi-squared test, or Fisher exact test as appropriate.
For our primary outcome, a linear mixed-effects regression model was used due to its ability to account for correlated data (daily measurement of fluid drainage) and the different number of days with drain among subjects. This regression model with random effects on the intercept accounting for subjects permits to obtain adjusted regression coefficients and to identify predictors independently associated with the outcome of interest. It returns the change in drainage per day for each variable.
For our two secondary outcome measures, normal linear regression models were used.
We performed univariable analysis on all variables for our primary and two secondary outcome measures. A fully adjusted model was then built based on the results of univariable regression analysis (cut-off p-value < 0.15) and a priori knowledge. The variables included in the full model are age, BMI, current smoking, type of mastectomy, biologic mesh (acellular dermal matrix) application, expander type used, axillar lymph node dissection ad continuitatem, resection weight, hematoma, and TXA.
All statistical tests were performed two-sided, and p-value < 0.05 was considered statistically significant. Statistical analysis was performed using Stata version 17.0 software (StataCorp LP, College Station, TX, USA) and R version 4.3.2.
3. Results
A total of 141 patients undergoing EbR between 2015-2022 were included. 9 were excluded resulting in a final patient cohort of 132 patients accounting for 155 breasts. Of those, 83 breasts were in the TXA-group and 72 breasts in the control group. Besides common symptoms like headache and nausea, no significant side effects requiring discontinuation of TXA-administration have been described by the patients receiving TXA.
Hematoma and Seroma rates did not differ between the two groups with an incidence of 6% in the TXA-group and 5.6% in the control group for hematoma and 6% in the TXA-group and 4.2% in the control group for seroma. Neither reaching statistical significance.
For total drainage volume, after full adjustment, TXA was associated with an average reduction in drainage volume of 19 ml per day (-19, 95%CI -34.96-(-3.02), P= Resection weight was associated with an increased average drainage volume of 0.04ml per resected gram per day (0.04, 95%CI 0.01-0.06, P=. Axillar lymph node dissection ad continuitatem with the mastectomy pocket was significantly associated with an average increase in drainage of 18ml per day (18.3, 95%CI 6.90-29.69, P=. Furthermore, hematoma significantly impacted drainage volume with an average increase of 24ml per day (23.7, 95%CI -10.58-36.82, P<0.001 while skin-reducing mastectomy was associated with an average reduction of 11ml per day (-10.8, 95%CI -20.76-(-0.79), P= compared to skin-sparing mastectomy. The use of Allergan (Natrelle 133) and Motiva (Flora) expanders were associated with a reduced average drainage volume of 18ml per day (-18.4, 95%CI -34.27-(-2.52), P= and 24ml per day (-23.5, 95%CI -33.30-(-13.79), P<0.001 respectively compared to the Mentor (CPX4) expander (Table 4).
The difference in drainage volume between TXA-group and control group was observed to be stronger during the first 4 days, specifically throughout the 48-hour period of administration (Figure 1).
Drain removal occurred after a mean of 3.3 days (3.33, 95%CI -2.91-3.76) in the TXA-group compared to 4.6 days (4.63, 95%CI 4.24-5.01) in the control group (P<0.001 (Table 3). Factors associated with an increase in the duration of drain placement were resection weight with an increase of 0.003 days per gram (0.003, 95%CI 0.001-0.005, P=, and hematoma with an increase of 1.2 days (1.17, 95%CI 0.005-2.33, P=. Motiva (Flora) expanders were associated with a decrease in duration of drain placement of 1.3 days (-1.31, 95%CI -2.20-(-0.42), P= compared to the Mentor (CPX4) expander (Table 5).
Mean length of hospital stay was 5.3 days (5.28, 95%CI 4.88-5.67) in the TXA-group compared to 6.2 days (6.17, 95%CI 5.82-6.51) in the control group (P=0.001 (Table 3). Administration of TXA was not associated with a significant influence on length of hospital stay (-0.61, 95%CI -1.90-0.67, P=. The two factors significantly associated with an increase in length of hospital stay were BMI with an increase of 0.1 days per kg/m2 (0.10, 95%CI 0.003-0.19, P=resection weight with an increase of 0.002 days per gram (0.002, 95%CI 0.000-0.004, P=. The Motiva (Flora) expander was associated with a reduction in length of hospital stay of 1.2 days (-1.24, 95%CI -2.01-(-0.46), P= compared to the Mentor (CPX4) expander (Table 6).
4. Discussion
TXA is a potent antifibrinolytic drug commonly used in surgical fields like traumatology, gynecology, and cardiothoracic surgery where it has been shown to significantly reduce major hemorrhage[5,6,7]. By decreasing the conversion of plasminogen to plasmin, it reduces fibrin degradation but also has an inhibitory effect on several inflammatory processes.
Though, the use of TXA in breast surgery is rather novel, and albeit first reports date back to 1994[17], the majority of studies were published from 2018 onwards[16,43,44], where it has been used both topically[45,46,47] and systemically[17,43,48] with a significant reduction in hematoma and seroma rates but also drainage volume. However, the current literature provides no data for mastectomies with immediate EbR using a standardized systemic TXA protocol.
Systemic administration of TXA using a standardized 48-hour protocol significantly reduces drainage volume in patients undergoing NSM, SSM, or SRM with immediate EbR. It was shown that specifically throughout the 48-hour period of administration the difference in drainage volume was markedly reduced in the TXA-group (Figure 1) which raises the question, of whether patients could benefit from TXA-administration beyond 48 hours.
While other studies demonstrated a reduction in drainage volume with a systemic 5-day protocol[17,18,49], they are not specific to mastectomy with EbR.
Both duration of drain placement and length of hospital stay were significantly reduced in the TXA-group with a mean decrease of 1.3 and 0.9 days respectively, potentially greatly impacting patient comfort and health care costs.
Factors associated with an increased drainage volume included hematoma, resection weight of the mammary gland, axillar lymph node dissection ad continuitatem, i.e., when performed from the same surgical approach as the mastectomy. Increased resection weight is associated with a larger wound surface and axillar lymph node dissection is associated with transection of lymph vessels discharging into the mastectomy pocket, resulting in increased drainage volume, prolonged drain placement, and eventually longer hospital stay.
Seroma and hematoma rates did not differ between the two groups. With an incidence of hematoma of 6% in the TXA-group and 5.5% in the control group, our results are comparable to the literature where an incidence of 2.3-3.3% is reported[19,20,21]. However, our seroma rates of 6% in the TXA-group and 4% in the control group are significantly below the incidence reported in the current literature ranging from 12% to 44%[17,46,49]. Recent data from 2023 reports a seroma incidence of 1.9% in both TXA and control groups undergoing mastectomy with immediate implant-based reconstruction[47]. As the diagnosis “seroma” is not clearly defined, its diagnosis is somewhat subjective and leads to inconsistent descriptions making comparability difficult.
As mentioned, other studies have investigated different aspects of TXA-administration in breast surgery. Three studies investigated the topical application of TXA after mastectomy without immediate reconstruction[46,47,50]. Eldesouky et al. and Ausen et al. have shown decreased drainage volume in patients receiving TXA locally[46,50], however, only Safran et al. describe immediate reconstructive efforts following the mastectomy, as demonstrated in a randomized control trial on patients undergoing bilateral NSM with immediate implant-based reconstruction, where one breast served as control and the other was treated with 3g of TXA diluted in 100cc of saline. They have shown that topical TXA-application would significantly lower drainage volume[47]. However, their study protocol and that of Eldesouky et al. relied on data collected by patients themselves after prompt discharge following surgery[46,47] and therefore represents a risk of bias.
Five studies have investigated systemic administration of TXA in patients undergoing breast surgery[17,18,48,49,51], however, only two were specific to mastectomy[49,51] and of these only Gogna et al. have measured drainage volume[49].
Oertli et al. investigated the effects of a systemic 5-day regimen of 3x1g TXA daily in patients undergoing both lumpectomies and mastectomies. This resulted in a significant reduction in drainage volume and length of hospital stay[17]. However, this data is not specific to mastectomies and no subsequent immediate reconstructive procedures are mentioned[17].
Weissler et al. have investigated the effect of TXA on complication rates in patients undergoing SSM or NSM, followed by immediate expander-to-implant reconstruction. While administration of 1g of TXA systemically once prior and once immediately after surgery reduced the risk of hematoma, drainage volume was not assessed. [48].
Gogna et al. conducted a prospective randomized study on patients undergoing modified radical mastectomy without reconstruction. They applied a 5-day protocol of 1g TXA systemically every 8 hours and demonstrated a reduction in drainage volume and duration of drain remaining in situ, but an increase in post-operative seroma rates[49]. Furthermore, the total time of drains remaining was relatively long with a mean of 10 days for the TXA-group and 13 days for the control group, associated with large amounts of total drainage volume (means of 781ml and 1023ml respectively). Another limitation of this study might be the rather small cohort of 25 patients per group.
The herein presented results not only address this gap but directly translate into clinical practice where a reduction in drainage volume and consequently duration of drains remaining in situ minimizes the risk of further complications like surgical site infections[52,53,54] and allows the patient to return to their normal life sooner. Furthermore, these results show that in patients with minimal risk factors for increased drainage volume (small mastectomy weight and no axillar lymph node dissection ad continuitatem), TXA-administration resulted in early drain removal which is known to further reduce drainage volume, healing time, and experienced pain[55] or might even question the need of drain placement in the first place.
The limitations of this study lie in its retrospective nature. There is a significant difference between case and control groups regarding expander type and expander pocket used. This is due to a change in regimen after June 2019 to not only include TXA after mastectomy but also prefer the prepectoral approach and the use of an MR-compatible expander[56]. This is particularly significant in the context of postmastectomy radiation therapy[57] and radiological follow-up using the hybrid approach where repeated injection of autologous fat graft before exchanging the expander with a definitive implant requires the expander to be in place for a much longer period[58]. The majority of the patients in the control group received a macrotextured expander using a subpectoral placement, whereas the majority of patients in the TXA-group received a nanotextured expander mainly placed prepectorally. Although this limits the informative value of the exact estimates, it does not have any negative impact on the finding that TXA reduces drainage volume. Macrotexturization is associated with reduced fluid production in the surgical site due to quicker adhesion to the surrounding tissues while nanotexturization could lead to less adhesion to the surrounding tissue since they are associated with a longer period of residual fluid staying between the expander and the mastectomy flap resulting in increased or prolonged drainage[59,60]. This may lead to an underestimation of the reduction in drainage volume in the TXA-group. The role of the placement is another possible bias, however, current literature, albeit not very extensive, shows no significant difference in drainage volume between pre- and subpectoral placement[61,62].
Nevertheless, the fact that TXA still showed to be significant in reducing drainage volume despite other counteracting factors is a strong argument in its favor.
Nanotextured expanders were a significant reducing factor throughout all outcome variables which however cannot be ignored and poses the question of the underlying cause which should be investigated in future studies.
5. Conclusions
This study shows that even with factors like low surface texturization of the device, which is associated with increased and prolonged fluid production, TXA still significantly reduces drainage volume. Furthermore, duration of drain placement and length of hospital stay were reduced in the TXA-group, representing the positive impact of TXA on both patient comfort and potentially socioeconomic burden. Finally, resection weight of breast tissue and axillar lymph node dissection ad continuitatem with the mastectomy pocket have an important increasing effect on the duration of drain placement and length of hospital stay and could be taken into account when considering drain removal.
This study further supports the systemic use of TXA in reconstructive breast surgery but should also encourage surgeons to reconsider using surgical drains in post-operative protocols for selected surgical indications and patients. Future studies are warranted with health care cost analysis to further promote and bring forward TXA administration in the field of reconstructive breast surgery.
Author Contributions
Conceptualization, L.G., S.M, Y.H. and D.S.; methodology, L.G., S.M., Y.H, and D.S.; validation, L.G., S.M., Y.H. and D.S.; formal analysis, L.G. and A.P.; investigation, L.G., S.M., A.C., Y.H., and D.S.; resources, S.M., A.C., and Y.H.; data curation, L.G., S.M., A.C., and A.P.; writing—original draft preparation, L.G. and D.S.; writing—review and editing, L.G., S.M., A.C., Y.H., and D.S.; visualization, L.G.; supervision, D.S. and Y.H.; project administration, L.G., S.M., Y.H. and D.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Local Ethics Committee of Ticino (BASEC number 2021-01918).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to privacy reasons.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Okamoto S, Hijikata-Okunomiya A, Wanaka K, Okada Y, Okamoto U. Enzyme-Controlling Medicines: Introduction. Semin Thromb Hemost. 1997;23(06):493-501. [CrossRef]
- Lee JH. Effect of Topical Tranexamic Acid on Seroma Formation in a Rat Mastectomy Model. Published online 2022.
- Baker SK, Strickland S. A critical role for plasminogen in inflammation. Journal of Experimental Medicine. 2020;217(4):e20191865. [CrossRef]
- Draxler DF, Medcalf RL. The Fibrinolytic System—More Than Fibrinolysis? Transfusion Medicine Reviews. 2015;29(2):102-109. [CrossRef]
- Roberts I, Shakur H, Coats T, et al. The CRASH-2 trial: a randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Health Technol Assess. 2013;17(10). [CrossRef]
- Shakur H, Roberts I, Fawole B, et al. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. The Lancet. 2017;389(10084):2105-2116. [CrossRef]
- Ker K, Edwards P, Perel P, Shakur H, Roberts I. Effect of tranexamic acid on surgical bleeding: systematic review and cumulative meta-analysis. BMJ. 2012;344(may17 1):e3054-e3054. [CrossRef]
- Prudovsky I, Kacer D, Zucco VV, et al. Tranexamic acid: Beyond antifibrinolysis. Transfusion. 2022;62(S1). [CrossRef]
- Walker PF, Foster AD, Rothberg PA, Davis TA, Bradley MJ. Tranexamic acid decreases rodent hemorrhagic shock-induced inflammation with mixed end-organ effects. PLoS One. 2018;13(11):e0208249. [CrossRef]
- Teng Y, Feng C, Liu Y, Jin H, Gao Y, Li T. Anti-inflammatory effect of tranexamic acid against trauma-hemorrhagic shock-induced acute lung injury in rats. Exp Anim. 2018;67(3):313-320. [CrossRef]
- Jimenez JJ, Iribarren JL, Lorente L, et al. Tranexamic acid attenuates inflammatory response in cardiopulmonary bypass surgery through blockade of fibrinolysis: a case control study followed by a randomized double-blind controlled trial. Crit Care. 2007;11(6):R117. [CrossRef]
- Lei Y, Xie J, Huang Q, Huang W, Pei F. Additional benefits of multiple-dose tranexamic acid to anti-fibrinolysis and anti-inflammation in total knee arthroplasty: a randomized controlled trial. Arch Orthop Trauma Surg. 2020;140(8):1087-1095. [CrossRef]
- Peng Z, Ban K, LeBlanc A, Kozar RA. Intraluminal Tranexamic Acid Inhibits Intestinal Sheddases and Mitigates Gut and Lung Injury and Inflammation in a Rodent Model of Hemorrhagic Shock. J Trauma Acute Care Surg. 2016;81(2):358-365. [CrossRef]
- Reichel CA, Lerchenberger M, Uhl B, et al. Plasmin Inhibitors Prevent Leukocyte Accumulation and Remodeling Events in the Postischemic Microvasculature. PLoS One. 2011;6(2):e17229. [CrossRef]
- Hyman YG, Vischer TL. Protease inhibitors reduce the reverse passive arthus reaction. Agents and Actions. 1978;8(5):532-535. [CrossRef]
- Calpin GG, McAnena PF, Davey MG, et al. The role of tranexamic acid in reducing post-operative bleeding and seroma formation in breast surgery: A meta-analysis. The Surgeon. 2023;21(4):e183-e194. [CrossRef]
- Oertli D, Laffer U, Haberthuer F, Kreuter U, Harder F. Perioperative and postoperative tranexamic acid reduces the local wound complication rate after surgery for breast cancer. British Journal of Surgery. 2005;81(6):856-859. [CrossRef]
- Lohani KR, Kumar C, Kataria K, Srivastava A, Ranjan P, Dhar A. Role of tranexamic acid in axillary lymph node dissection in breast cancer patients. Breast J. 2020;26(7):1316-1320. [CrossRef]
- Seth AK, Hirsch EM, Kim JYS, et al. Hematoma After Mastectomy With Immediate Reconstruction An Analysis of Risk Factors in 883 Patients. Annals of Plastic Surgery. 2013;71(1):20-23. [CrossRef]
- Bloom JA, Foroutanjazi S, Erlichman Z, et al. The Use of Hemostatic Agents to Decrease Bleeding Complications in Breast Cancer Surgery. The American Surgeon. 2023;89(3):395-400. [CrossRef]
- Marinescu SA, Bejinariu LG, Marina MC, Giuglea C. Complications related to breast reconstruction after mastectomy using multiple surgical techniques – a national and international comparative analysis.
- Adrien C, Katia M, Marie-Lucile B, Alice R, Claire B, Roman R. Prevention of lymphocele or seroma after mastectomy and axillary lymphadenectomy for breast cancer: systematic review and meta-analysis. Sci Rep. 2022;12(1):10016. [CrossRef]
- Barwell J, Campbell L, Watkins RM, Teasdale C. How long should suction drains stay in after breast surgery with axillary dissection? Ann R Coll Surg Engl. 1997;79(6):435-437.
- Srivastava V, Basu S, Shukla VK. Seroma Formation after Breast Cancer Surgery: What We Have Learned in the Last Two Decades. J Breast Cancer. 2012;15(4):373. [CrossRef]
- Kumar S, Lal B, Misra MC. Post-mastectomy seroma: a new look into the aetiology of an old problem. J R Coll Surg Edinb. 1995;40(5):292-294.
- Sampathraju S, Rodrigues G. Seroma Formation after Mastectomy: Pathogenesis and Prevention. Indian J Surg Oncol. 2010;1(4):328-333. [CrossRef]
- Pogson CJ, Adwani A, Ebbs SR. Seroma following breast cancer surgery. European Journal of Surgical Oncology (EJSO). 2003;29(9):711-717. [CrossRef]
- Halsted WS. I. The Results of Operations for the Cure of Cancer of the Breast Performed at the Johns Hopkins Hospital from June, 1889, to January, 1894. Ann Surg. 1894;20(5):497-555.
- Patey DH, Dyson WH. The Prognosis of Carcinoma of the Breast in Relation to the Type of Operation Performed. Br J Cancer. 1948;2(1):7-13.
- McWHIRTER R. The value of simple mastectomy and radiotherapy in the treatment of cancer of the breast. Br J Radiol. 1948;21(252):599-610. [CrossRef]
- Toth BA, Lappert P. Modified skin incisions for mastectomy: the need for plastic surgical input in preoperative planning. Plast Reconstr Surg. 1991;87(6):1048-1053.
- Crowe J Joseph P, Kim JA, Yetman R, Banbury J, Patrick RJ, Baynes D. Nipple-Sparing Mastectomy: Technique and Results of 54 Procedures. Archives of Surgery. 2004;139(2):148-150. [CrossRef]
- Bostwick J. Total mastectomy with breast skin and volume reduction using an inverted T incision. Plastic and reconstructive breast surgery. 1990;2:1048-1054.
- Querci della Rovere G, Nava M, Bonomi R, Catanuto G, Benson JR. Skin-reducing mastectomy with breast reconstruction and sub-pectoral implants. Journal of Plastic, Reconstructive & Aesthetic Surgery. 2008;61(11):1303-1308. [CrossRef]
- Suga H, Shiraishi T, Shibasaki Y, Takushima A, Harii K. Predictive Factors for Drainage Volume after Expander-based Breast Reconstruction. Plastic and Reconstructive Surgery - Global Open. 2016;4(6):e727. [CrossRef]
- Lim YM, Lew DH, Roh TS, Song SY. Analysis of factors that affect drainage volume after expander-based breast reconstruction. Arch Plast Surg. 2020;47(01):33-41. [CrossRef]
- Gonzalez EA, Saltzstein EC, Riedner CS, Nelson BK. Seroma Formation Following Breast Cancer Surgery. Breast Journal. 2003;9(5):385-388. [CrossRef]
- Hashemi E, Kaviani A, Najafi M, Ebrahimi M, Hooshmand H, Montazeri A. Seroma formation after surgery for breast cancer. World J Surg Onc. 2004;2(1):44. [CrossRef]
- Petrek JA. Axillary Lymphadenectomy: A Prospective, Randomized Trial of 13 Factors Influencing Drainage, Including Early or Delayed Arm Mobilization. Arch Surg. 1990;125(3):378. [CrossRef]
- Loo W, Chow L. Factors predicting seroma formation after mastectomy for Chinese breast cancer patients. Indian J Cancer. 2007;44(3):99. [CrossRef]
- Kuroi K, Shimozuma K, Taguchi T, et al. Pathophysiology of seroma in breast cancer. Breast Cancer. 2005;12(4):288-293. [CrossRef]
- Khansa I, Hendrick RGJ, Shore A, Meyerson J, Yang M, Boehmler JHI. Breast Reconstruction with Tissue Expanders: Implementation of a Standardized Best-Practices Protocol to Reduce Infection Rates. Plastic and Reconstructive Surgery. 2014;134(1):11. [CrossRef]
- Lardi AM, Dreier K, Junge K, Farhadi J. The use of tranexamic acid in microsurgery—is it safe? Gland Surg. 2018;7(S1):S59-S63. [CrossRef]
- Liechti R, Van De Wall BJM, Hug U, Fritsche E, Franchi A. Tranexamic Acid Use in Breast Surgery: A Systematic Review and Meta-Analysis. Plastic & Reconstructive Surgery. 2023;151(5):949-957. [CrossRef]
- Ausen K, Fossmark R, Spigset O, Pleym H. Randomized clinical trial of topical tranexamic acid after reduction mammoplasty. British Journal of Surgery. 2015;102(11):1348-1353. [CrossRef]
- Eldesouky MS, Ashour HSA, Shahin MA. Effect of topical application of tranexamic acid on reduction of wound drainage and seroma formation after mastectomy.
- Safran T, Vorstenbosch J, Viezel-Mathieu A, Davison P, Dionisopoulos T. Topical Tranexamic Acid in Breast Reconstruction: A Double-Blind Randomized Controlled Trial. Plastic & Reconstructive Surgery. 2023;152(4):699-706. [CrossRef]
- Weissler JM, Banuelos J, Jacobson SR, et al. Intravenous Tranexamic Acid in Implant-Based Breast Reconstruction Safely Reduces Hematoma without Thromboembolic Events. Plastic & Reconstructive Surgery. 2020;146(2):238-245. [CrossRef]
- Gogna S, Goyal P. Prospective randomized study on effect of tranexamic acid on wound drainage following modified radical mastectomy for cancer breast. Int J Cur Res. 2015;7:16192-16194.
- Ausen K, Hagen AI, Østbyhaug HS, et al. Topical moistening of mastectomy wounds with diluted tranexamic acid to reduce bleeding: randomized clinical trial. BJS Open. 2020;4(2):216-224. [CrossRef]
- Wolter A, Scholz T, Pluto N, Diedrichson J, Arens-Landwehr A, Liebau J. Subcutaneous mastectomy in female-to-male transsexuals: Optimizing perioperative and operative management in 8 years clinical experience. Journal of Plastic, Reconstructive & Aesthetic Surgery. 2018;71(3):344-352. [CrossRef]
- Xue DQ, Qian C, Yang L, Wang XF. Risk factors for surgical site infections after breast surgery: a systematic review and meta-analysis. Eur J Surg Oncol. 2012;38(5):375-381. [CrossRef]
- Murray JD, Elwood ET, Jones GE, Barrick R, Feng J. Decreasing expander breast infection: A new drain care protocol. Can J Plast Surg. 2009;17(1):17-21.
- Hanna KR, Tilt A, Holland M, et al. Reducing Infectious Complications in Implant Based Breast Reconstruction: Impact of Early Expansion and Prolonged Drain Use. Ann Plast Surg. 2016;76 Suppl 4:S312-315. [CrossRef]
- Lembo F, Cecchino LR, Parisi D, Portincasa A. Reduction of seroma and improvement of quality of life after early drain removal in immediate breast reconstruction with tissue expander. Preliminary report from a randomized controlled study. J Plast Reconstr Aesthet Surg. 2021;74(10):2565-2572. [CrossRef]
- Bayasgalan M, Munhoz AM, Shellock FG. Breast Tissue Expander With Radiofrequency Identification Port: Assessment of MRI Issues. American Journal of Roentgenology. 2020;215(1):159-164. [CrossRef]
- Matsubayashi F, Takahashi T, Miyauchi H, Ito Y, Harada A, Yoshioka Y. Modeling of a tissue expander with a radiofrequency identification port in postmastectomy radiation therapy planning. J Radiat Res. 2024;65(3):360-368. [CrossRef]
- Stillaert FBJL, Lannau B, Landuyt KV, Blondeel PN. The Prepectoral, Hybrid Breast Reconstruction: The Synergy of Lipofilling and Breast Implants. Plastic and Reconstructive Surgery Global Open. 2020;8(7). [CrossRef]
- Chiu WK, Fracol M, Feld LN, Qiu CS, Kim JYS. Judging an Expander by Its Cover: A Propensity-Matched Analysis of the Impact of Tissue Expander Surface Texture on First-Stage Breast Reconstruction Outcomes. Plast Reconstr Surg. 2021;147(1):1e-6e. [CrossRef]
- Lee KT, Park HY, Jeon BJ, Mun GH, Bang SI, Pyon JK. Does the Textured-Type Tissue Expander Affect the Outcomes of Two-Stage Prosthetic Breast Reconstruction? A Propensity Score Matching Analysis between Macrotextured and Microtextured Expanders. Plast Reconstr Surg. 2021;147(3):545-555. [CrossRef]
- Suh YC, Kim JK, Kim NR, et al. A comparative study of pre- or subpectoral expander position with the fenestrated Acellular dermal matrix anterior coverage, on drainage volume and Seroma Formation after Non-Nipple-Sparing Mastectomy. J Plast Reconstr Aesthet Surg. 2021;74(9):2237-2243. [CrossRef]
- Ozturk CN, Ozturk C, Magner WJ, Ali A, Diehl J, Sigurdson SL. Seroma After Breast Reconstruction With Tissue Expanders: Outcomes and Management. Ann Plast Surg. 2023;91(3):331-336. [CrossRef]
Figure 1.
Average drainage volume per day.
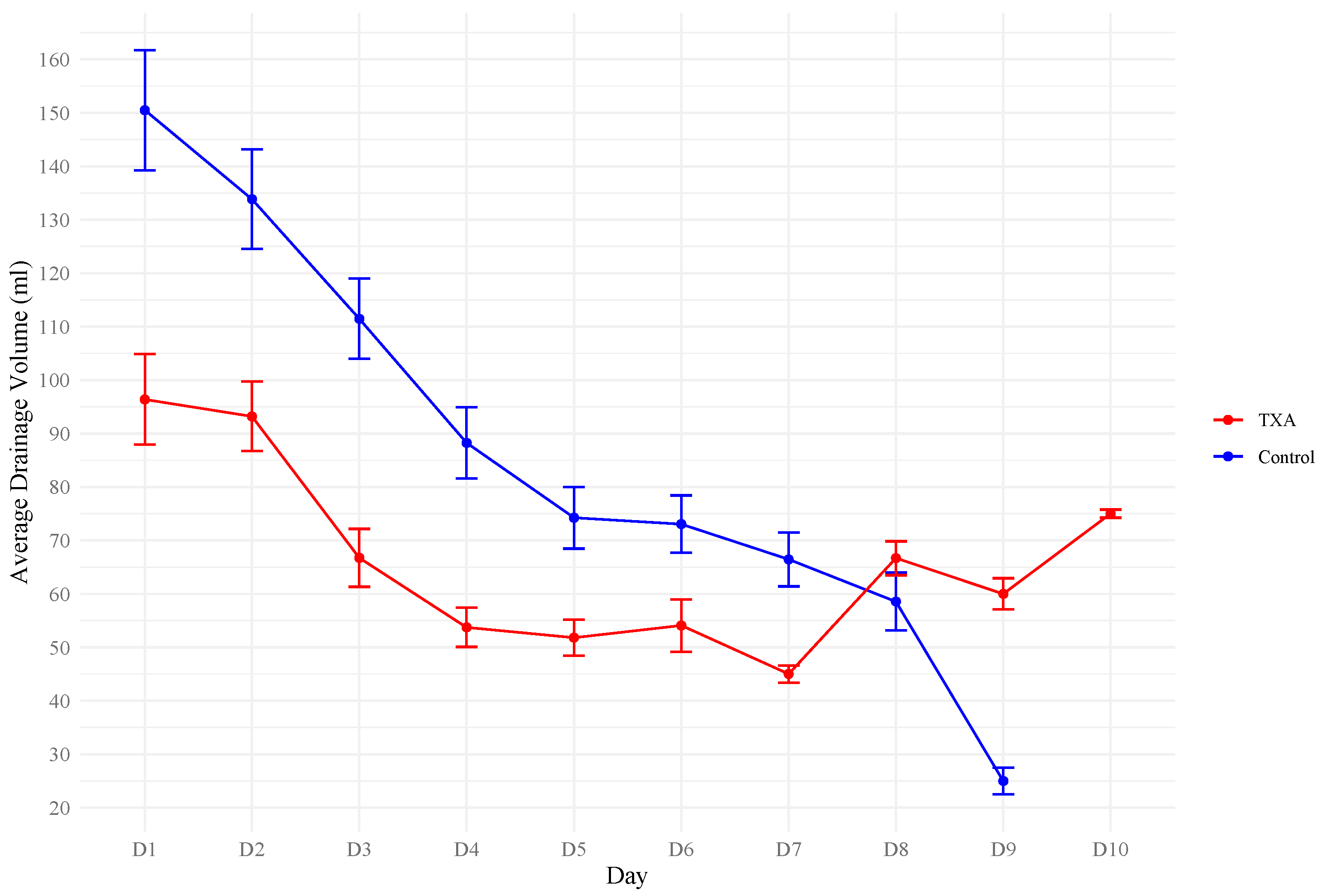

Table 1.
Baseline patient demographics
| Variable | TXA N = 83 | Controls N = 72 | P-Value |
|---|---|---|---|
| Age a | 50 (46, 58) | 48 (42, 62) | 0.722 d |
| BMI a | 22.0 (20.8, 26.0) | 22.3 (20.3, 25.3) | 0.380 d |
| DM b | 1 (1.4) | 0 (0) | 0.281 c |
| Hypertension b | 10 (12.1) | 6 (8.3) | 0.448 c |
| Heart disease b | 7 (8.4) | 5 (6.9) | 0.729 c |
| Kidney disease b | 4 (4.8) | 0 (0) | 0.059 c |
| Active smoking b | 27 (32.5) | 17 (23.6) | 0.219 c |
| Chronic NSAID b | 2 (2.8) | 1 (1.2) | 0.478 c |
| Antiaggregation b | 1 (1.2) | 4 (5.6) | 0.126 c |
| Anticoagulation b | 2 (2.4) | 1 (1.4) | 0.645 c |
| Previous thromboembolic event b | 0 (0) | 4 (5.6) | 0.030 c |
| Previous radiotherapy b | 7 (8.4) | 0 (0) | 0.012 c |
| Neoadjuvant chemotherapy b | 21 (25.3) | 11 (15.3) | 0.124 c |
| Thrombocytes a | 253 (220, 312) | 269 (219, 331) | 0.236 d |
| Quick a | 103 (96, 113) | 98.5 (90, 106) | 0.012 d |
| INR a | 1 (0.9, 1) | 1 (1, 1) | 0.002 d |
a Median (25th percentile, 75th percentile), b N (%), c Chi2-test, d t-test, BMI = body mass index, DM = diabetes mellitus, NSAID = non-steroidal anti-inflammatory drugs, INR = international normalized ratio
Table 2.
Surgical parameters.
| Variable | TXA N = 83 | Controls N = 72 | P-Value |
|---|---|---|---|
| Breast | |||
| Rightb | 41 (49.4) | 30 (41.7) | 0.335 c |
| Leftb | 42 (50.6) | 42 (58.3) | 0.335 c |
| Resection weight (g) a | 332 (228, 550) | 316.5 (218.5, 485.5) | 0.588 d |
| Type of mastectomy | <0.001 c | ||
| Skin-sparingb | 14 (16.9) | 23 (31.9) | |
| Nipple-sparingb | 36 (43.4) | 45 (62.5) | |
| Skin-reducingb | 33 (39.8) | 4 (5.6) | |
| Expander placement | <0.001 c | ||
| Prepectoralb | 71 (85.5) | 29 (40.3) | |
| Subpectoralb | 12 (14.5) | 43 (59.7) | |
| Expander | <0.001 c | ||
| Allergan (Natrelle 133)b | 0 (0) | 65 (90.3) | |
| Mentor (CPX4)b | 18 (21.7) | 5 (6.9) | |
| Motiva (Flora)b | 65 (78.3) | 2 (2.8) | |
| Sentinel lymph node biopsy b | 49 (59.0) | 49 (68.1) | 0.245 c |
| Axillar lymph node dissection ad continuitatemb | 6 (7.2) | 6 (8.3) | 0.797 c |
| Axillar access b | 39 (47.0) | 41 (56.9) | 0.216 c |
| Use of synthetic mesh b | 10 (12.1) | 14 (19.4) | 0.204 c |
| Use of biological mesh (acellular dermal matrix) b | 11 (13.3) | 0 (0) | 0.001 c |
a Median (25th percentile, 75th percentile), b N (%), c Chi2-test, d t-test
Table 3.
Surgical complications and secondary outcome measures.
| Variable | TXA N = 83 | Controls N = 72 | P-Value |
|---|---|---|---|
| Hematoma b | 5 (6.0) | 4 (5.6) | 0.901 c |
| Seroma b | 5 (6.0) | 3 (4.2) | 0.602 c |
| Duration of drain placement (days) a | 3.3 (1.8) | 4.6 (1.6) | <0.001 d |
| Length of hospital stay (days) a | 5.3 (1.8) | 6.2 (1.5) | 0.001 d |
a Mean (SD), b N (%), c Chi2-test, d t-test
Table 4.
Full Model – Drainage volume.
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Variable | Estimate (SE) | P-Value | 95% CI | Estimate (SE) | P-Value | 95% CI |
| Age (per year) | 0.1 (0.2) | 0.520 | -0.2 - 0.5 | 0.1 (0.1) | 0.401 | -0.2 - 0.4 |
| BMI (per kg/m2) | 0.9 (0.5) | 0.098 | -0.2 - 2.0 | 0.3 (0.6) | 0.607 | -0.9 - 1.5 |
| Current smoking | -7.1 (4.6) | 0.118 | -16.1 - 1.8 | -4.4 (3.7) | 0.234 | -11.5 - 2.8 |
| Type of mastectomy (Skin-sparing as reference) | ||||||
| Nipple-sparing | -9.0 (5.0) | 0.069 | -18.8 - 0.7 | -3.6 (4.1) | 0.387 | -11.7 - 4.5 |
| Skin-reducing | -17.0 (5.8) | 0.004 | -28.4 - (-5.5) | -10.8 (5.1) | 0.034 | -20.8 - (-0.8) |
| Biologic mesh (acellular dermal matrix) | -18.6 (7.9) | 0.018 | -34.1 - (-3.2) | -2.7 (6.6) | 0.690 | -15.7 - 10.4 |
| Type of expander (Mentor (CPX4) as reference) | ||||||
| Allergan (Natrelle 133) | 1.9 (5.4) | 0.729 | -8.8 - 12.5 | -18.4 (8.1) | 0.023 | -34.3 - (-2.5) |
| Motiva (Flora) | -25.0 (5.4) | <0.001 | -35.6 - (-14.4) | -23.5 (5.0) | <0.001 | -33.3 - (-13.8) |
| Axillar lymph node dissection ad continuitatem | 20.3 (7.7) | 0.009 | 5.2 - 35.4 | 18.3 (5.8) | 0.002 | 6.9 - 29.7 |
| Resection weight (per gram) | 0.03 (0.01) | 0.002 | 0.01 - 0.05 | 0.04 (0.01) | 0.001 | 0.01 - 0.06 |
| Hematoma | 20.2 (8.7) | 0.020 | 3.2 - 37.3 | 23.7 (6.7) | <0.001 | 10.6 - 36.8 |
| Tranexamic acid | -23.3 (3.7) | <0.001 | -30.6 - (-16.1) | -19.0 (8.1) | 0.020 | -35.0 - (-3.0) |
BMI = Body mass index
Table 5.
Full Model – Duration of drain placement
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Variable | Estimate (SE) | P-Value | 95% CI | Estimate (SE) | P-Value | 95% CI | |
| Age (per year) | -0.004 (0.01) | 0.759 | -0.03 - 0.02 | -0.01 (0.01) | 0.468 | -0.03 - 0.02 | |
| BMI (per kg/m2) | 0.1 (0.04) | 0.033 | 0.007 - 0.2 | 0.0 (0.1) | 0.995 | -0.1 - 0.1 | |
| Current smoking | -0.7 (0.3) | 0.050 | -1.3 - (-0.001) | -0.5 (0.3) | 0.148 | -1.1 - 0.2 | |
| Type of mastectomy (Skin-sparing as reference) | |||||||
| Nipple-sparing | -0.7 (0.4) | 0.062 | -1.5 - 0.04 | -0.3 (0.4) | 0.360 | -1.0 - 0.4 | |
| Skin-reducing | -0.9 (0.4) | 0.042 | -1.8 - (-0.04) | -0.5 (0.4) | 0.236 | -1.4 - 0.3 | |
| Biologic mesh (acellular dermal matrix) | -1.3 (0.6) | 0.021 | -2.5 - (-0.2) | -0.5 (0.6) | 0.399 | -1.6 - 0.6 | |
| Type of expander (Mentor (CPX4) as reference) | |||||||
| Allergan (Natrelle 133) | 0.1 (0.5) | 0.753 | -0.7 - 1.0 | -0.7 (0.7) | 0.313 | -2.0 - 0.7 | |
| Motiva (Flora) | -1.3 (0.5) | 0.004 | -2.2 - (-0.4) | -1.3 (0.5) | 0.004 | -2.2 - (-0.4) | |
| Axillar lymph node dissection ad continuitatem | 1.2 (0.6) | 0.036 | 0.08 - 2.3 | 1.0 (0.5) | 0.055 | -0.02 - 2.0 | |
| Resection weight (per gram) | 0.003 (0.001) | <0.001 | 0.002 - 0.004 | 0.003 (0.001) | 0.001 | 0.001 - 0.005 | |
| Hematoma | 1.1 (0.7) | 0.105 | -0.2 - 2.4 | 1.2 (0.6) | 0.049 | 0.005 - 2.3 | |
| Tranexamic acid | -1.3 (0.3) | <0.001 | -1.9 - (-0.7) | -0.7 (0.7) | 0.341 | -2.0 - 0.7 | |
BMI = Body mass index
Table 6.
Full Model – Length of hospital stay
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Variable | Estimate (SE) | P-Value | 95% CI | Estimate (SE) | P-Value | 95% CI | |
| Age (per year) | 0.005 (0.01) | 0.720 | -0.02 - 0.03 | -0.003 (0.01) | 0.819 | -0.03 - 0.02 | |
| BMI (per kg/m2) | 0.1 (0.03) | <0.001 | 0.1 - 0.2 | 0.095 (0.047) | 0.043 | 0.003 - 0.2 | |
| Current smoking | -0.5 (0.3) | 0.110 | -1.1 - 0.1 | -0.286 (0.290) | 0.326 | -0.9 - 0.3 | |
| Type of mastectomy (Skin-sparing as reference) | |||||||
| Nipple-sparing | -0.7 (0.3) | 0.045 | -1.3 - (-0.02) | -0.267 (0.330) | 0.419 | -0.9 - 0.4 | |
| Skin-reducing | -0.6 (0.4) | 0.134 | -1.4 - 0.2 | -0.513 (0.405) | 0.207 | -1.3 - 0.3 | |
| Biologic mesh (acellular dermal matrix) | -0.8 (0.5) | 0.117 | -1.9 - 0.2 | 0.097 (0.533) | 0.855 | -1.0 - 1.2 | |
| Type of expander (Mentor (CPX4) as reference) | |||||||
| Allergan (Natrelle 133) | -0.005 (0.4) | 0.991 | -0.8 - 0.8 | -0.782 (0.649) | 0.230 | -2.1 - 0.5 | |
| Motiva (Flora) | -1.1 (0.4) | 0.005 | -1.9 - (-0.3) | -1.236 (0.391) | 0.002 | -2.0 - (-0.5) | |
| Axillar lymph node dissection ad continuitatem | 0.4 (0.5) | 0.409 | -0.6 - 1.4 | 0.248 (0.461) | 0.591 | -0.7 - 1.2 | |
| Resection weight (per gram) | 0.003 (0.001) | <0.001 | 0.002 - 0.004 | 0.002 (0.001) | 0.025 | 0.0 - 0.004 | |
| Hematoma | 0.6 (0.6) | 0.338 | -0.6 - 1.7 | 0.965 (0.535) | 0.073 | -0.1 - 2.0 | |
| Tranexamic acid | -0.9 (0.3) | 0.001 | -1.4 - (-0.4) | -0.611 (0.650) | 0.349 | -1.9 - 0.7 | |
BMI = Body mass index
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



