
Submitted:
18 September 2024
Posted:
19 September 2024
You are already at the latest version
Abstract
Introduction. The management of anemia in chronic kidney disease (CKD-An) presents significant challenges for nephrologists due to variable responsiveness to erythropoietin-stimulating agents (ESA), hemoglobin (Hb) cycling, and multiple clinical factors affecting erythropoiesis. The Anemia Control Model (ACM) is a decision support system designed to personalize anemia treatment, which has shown improvements in achieving Hb targets, reducing ESA doses, and maintaining Hb stability. This study aimed at evaluating the association between ACM-guided anemia management with hospitalizations and survival in a large cohort of hemodialysis patients. Methods. This mul-ti-center, retrospective cohort study evaluated adult hemodialysis patients within the European Fresenius Medical Care NephroCare network from 2014 to 2019. Patients treated according to ACM recommendations were compared to those from centers without ACM. Data on demographics, comorbidities, and dialysis treatment were used to compute a propensity score estimating the like-lihood of receiving ACM-guided care. The primary endpoint was hospitalizations during follow-up; the secondary endpoint was survival. A 1:1 propensity score-matched design was used to minimize confounding bias. Results. A total of 20,209 eligible patients were considered (reference group: 17,101; ACM adherent group: 3,108). Before matching, the mean age was 65.3±14.5 years, with 59.2% men. Propensity score matching resulted in two groups of 1,950 patients each. Matched ACM adherent and non-ACM patients showed negligible differences in baseline characteristics. Hospi-talization rates were lower in the ACM group both before matching (71.3 vs. 82.6 per 100 per-son-years, p<0.001) and after matching (74.3 vs. 86.7 per 100 person-years, p<0.001). During fol-low-up, 385 patients died, showing no significant survival benefit for ACM-guided care (hazard ratio = 0.93; p=0.51). Conclusions: ACM-guided anemia management was associated with a sig-nificant reduction in hospitalization risk among hemodialysis patients. These results further support the utility of ACM as a decision support tool enhancing anemia management in clinical practice.
Keywords:
End Stage Renal Disease (ESRD)
; anemia management
; erythropoiesis stimulating agent (ESA)
; Artificial Intelligence (AI)
; Personalized Medicine
1. Introduction
Anemia of chronic kidney disease (CKD-An) is common among individuals undergoing kidney dialysis. Uncontrolled CKD-An associates to risk for low Health-Related Quality of Life, as well as for mortality and hospitalization. [1,2] Consequently, clinical guidelines recommend the correction of CKD-An in most dialysis patients. [3,4,5,6,7,8,9] The established protocol entails the administration of iron supplements and erythropoiesis-stimulating agents (ESAs) [10] to maintain hemoglobin (Hb) serum levels within the recommended target range. [1,11] Nevertheless, the effective management of renal anemia presents distinct challenges for nephrologists, with recent findings indicating that only 45-65% of hemodialysis patients consistently achieve hemoglobin concentrations within the target range. [12,13,14,15]
Anemia management is a complex clinical task requiring a challenging trade-off negotiation between anemia correction and minimization of potential side effects of ESA and Iron therapy. Both hemoglobin fluctuations [16,17], and excessive ESA usage are associated with higher risk of morbidity and mortality [18,19,20,21,22,23,24,25,26]. A meta-regression analysis found significant associations between high ESA dose and development of hypertension, stroke, and thrombotic events as well as with all-cause mortality, irrespective of the achieved hemoglobin levels [27]. High doses of these compounds were likewise associated with increased rate of arteriovenous fistula failure [28], higher risk of cardiovascular complications [27,29] and hospitalizations [30], and enhanced mortality [31,32], also among ESA hypo-responders [33]. On the other hand, hemoglobin cycling above and below the target range are associated with increased all cause hospitalization [29,34] and cardiovascular risk [29,35], as well as higher mortality [21,35,36,37]. Hemoglobin cycling is a common condition depending on fluctuations in ESA bioavailability and bone marrow responsiveness due to transient inflammation, hydration, iron deficiency, and malnutrition [38,39].
Hence, tailoring anemia management to accommodate individual patient variances and temporal fluctuations in erythropoiesis presents a challenging yet fundamental clinical task, aimed at minimizing hemoglobin fluctuations while optimizing erythropoiesis-stimulating agent (ESA) dosages. In order to provide support and standardization for medical decision-making, we have developed the Anemia Control Model (ACM) [40], an artificial intelligence (AI) decision support system designed to assist physicians in selecting personalized anemia therapies for their patients. Initial investigations have demonstrated that the implementation of the ACM into routine clinical practice has led to an increase in the proportion of patients achieving target hemoglobin values, a reduction in ESA dosages, and a mitigation of individual hemoglobin fluctuations [41,42]. Moreover, a recent large-scale cohort study, utilizing propensity-score matching, has further underscored the real-world effectiveness of the ACM. This study revealed that compared to standard care approaches, ACM-guided care was associated with higher rates of hemoglobin target-achievement, as well as lower incidences of severe anemia and ESA utilization for patients with hemoglobin level above 12 g/dL [43].
In the present study we sought to investigate the association between ACM-guided anemia care and patient-centered outcomes such as hospitalization and survival among hemodialysis patients treated in the European Fresenius Medical Care Nephrocare network.
2. Materials and Methods
2.1. The Anemia Control Model (ACM)
The Anemia Control Model (ACM) is an Artificial Neural Network Algorithm which personalizes ESA and Iron dosage based on estimated individual, dose-response relationship. The ACM suggests the optimal dose of ESA and iron monthly [40,44,45,46,47]. ACM first simulates how future hemoglobin values would vary for different possible ESA and Iron dosage and secondly, the ACM policy extractor assigns a utility score to each simulated ESA dosages based on a reward function anchored at pre-specified clinical targets. The simulated action achieving the highest utility score is suggested. The ACM integrates a comprehensive dataset, including current Hb levels and all Hb values within the 120 days prior to the algorithm’s execution, ferritin levels, and additional laboratory data such as albumin, calcium, C-reactive protein, leukocytes, mean corpuscular hemoglobin (MCH), mean corpuscular volume (MCV), potassium, phosphate, sodium, transferrin saturation (TSat), and overhydration status. Hemodialysis (HD) treatment data, including pre-dialysis weight, dry body weight, Kt/V, ESA and iron administration details (dose quantities, units, routes, and codes) within 140 days, are also considered. Basic patient demographics (age, gender, height, admission date) and transfusion records within the past 120 days further contribute to the model.
The architecture of the ACM involves a cloud-based suggestion engine that processes pseudonymized patient data from hospital information systems, ensuring secure data handling. The ACM operates as a decision support tool, where recommendations are presented to nephrologists via an integrated application within the hospital’s IT environment. Nephrologists can review and either accept or reject the suggested dosages, allowing for clinical discretion and personalized patient management. This integration facilitates the seamless application of ACM’s data-driven, evidence-based recommendations into routine clinical practice, supporting the optimization of anemia management in patients with end-stage renal disease (ESRD)
The ACM was certified as a medical device within the European Community under MDR 2017/745. We further corroborated ACM effectiveness in improving hemoglobin target achievement rate and reducing Erythropoietin Stimulating Agents consumption in a recent multicenter real-world evidence study [48].
2.2. Study Design & Participants
In this multi-center, matched, retrospective, historical cohort, observational study we screened for eligibility all incident adult patients on chronic hemodialysis receiving care for at least 180 days in the European Fresenius Medical Care NephroCare network of Bosnia and Herzegovina, Czech Republic, France, Hungary, Italy, Poland, Portugal, Romania, Slovakia and Spain from January 1st, 2014 to December 31st, 2019. Study design is displayed in Figure 1. We included patients with complete information regarding biological sex, Fresenius Medical Care Nephrocare admission date, renal replacement therapy onset date, and patient’s age. A Continuous Quality Improvement program called Medical Patient Review (CQI-MPR) operates in all FMC-Nephrocare clinics since 2014. The Medical Patient Review program associates extensive medical training and guidance with key performance indicator targets across the network. Under Medical Patient Review, physicians are required to test hemoglobin monthly and ferritin at least quarterly in all patients. Additionally, participating centers are required to reach pre-specified hemoglobin targets achievement rates every month. Characteristics and outcomes of the Medical Patient Review program have been described elsewhere [49]. We used the first 180 days of dialysis after the date of first hemoglobin assessment/ACM suggestion (index date) as the ascertainment period. Finally, we excluded patients with cancer and transfusions in the ascertainment period. Study endpoints have been evaluated over 365 days of follow up since the end of the ascertainment period (Figure 1).
2.3. Definition of Exposure Groups
2.3.1. ACM Adherent Patients
patients who were consistently treated according to ACM recommendations were allocated in the ACM adherent group. ACM does not produce any suggestions in case of errors in reporting ESA or Iron dosage (i.e., wrong measurement unit of dosage, wrong route of administration, etc), elevated frequency of missed treatment in the 4 months prior to the index hemoglobin measurement, and never for patients with a diagnosis of porphyria. Therefore, we excluded patients with less than 3 ACM suggestions during the ascertainment period. Patients in the ACM group were further classified as ACM compliant if more than 65% of suggestions have been accepted by the physician and ACM non-compliant otherwise. The threshold is consistent with previous clinical research concerning the use of ACM [42,47].
2.3.2. Reference group
Patients treated in centers where ACM was not activated were included in the reference group. All patients included in this group were managed according to established clinical standards [40]. For patients in the reference group, we required that patients received 3 or more hemoglobin assessments in the ascertainment period.
2.4. Covariates
We abstracted demographic (age, biologic sex, ethnicity) and anthropometric information (BMI) from patients’ clinical records. Relevant comorbidities were ascertained based on the occurrence of suggestive ICD10 codes during the ascertainment period. The full list of ICD10 code used to classify patients’ comorbidities is reported in supplementary Table 1. All biochemical assessment occurring during the ascertainment period have been averaged and abstracted from patients’ clinical chart.
2.5. Outcome Definition
The primary endpoint was the number of hospitalizations occurring for each patient during the study follow-up period. The secondary endpoint was patients’ survival after the ascertainment period. We censored at the end of follow up period, and patients’ leaving the FMC-Nephrocare network.
2.6. Statistical Analysis
We computed mean and standard deviation or median and interquartile range for continuous variables as appropriate and absolute and relative frequency for categorical variables. 1-way ANOVA, Mann-Whitney test and χ2 test were used to assess differences in covariate distribution across groups as appropriate.
2.6.1. Primary Analysis
In order to simulate a randomized controlled trial and account for potential indication bias we constructed a 1:1 matched cohort to compare ACM adherent patients with a reference group of patients without any exposure to ACM.
Propensity Score (PM) Estimation
Since the decision whether to accept or not the ACM monthly suggestion may depend on patients’ characteristics, we estimated a propensity score (PS) representing the likelihood that the attending physicians would consistently accept ACM suggestions for each patient treated in ACM centers included in the study. A patient was considered consistently treated in accordance with ACM, if the attending physicians accepted more than 65% of software recommendations for that patient during the ascertainment period. The PM was estimated by a logistic regression model assessing the likelihood of consistent ACM acceptance (ACM adherent patient, i.e., >65% of suggestions were accepted) versus inconsistent acceptance (ACM non-adherent patient; <65% of accepted suggestions) given the full set of baseline covariates described above.
Matching Strategy
In order to mitigate the indication bias, we matched each ACM adherent patient to 1 corresponding patient in the reference group (i.e., patients treated in clinics where ACM was never activated). We applied an optimal matching algorithm to obtain a 1:1 matched sample. The maximum caliper allowed for matching was 0.05 and we limited to control matches with an index date and dialysis vintage difference compared to ACM cases smaller than 180 days.
Outcomes estimation
We estimated the event rate ratio per 100 patient-month of hospitalization and hazard ratio of mortality using a zero inflated negative binomial regression and Proportional Hazard regression, respectively. We accounted for the matched design of the study by adding a random intercept representing dependency within pairs.
2.6.2. Secondary Analysis
Since we observed residual imbalance in Kt/V after propensity score matching, we further added Kt/V as a covariate in the model.
3. Results
3.1. Study Sample before Matching
We included 20209 patients meeting the eligibility criteria (Reference group: 17101; ACM Adherent group: 3108; Figure 2). Patients were 59.2% male (n=11962) with mean age of 65.3±14.5 years. Distribution of each variable included in the PS model by exposure group before matching are reported in Table 1.
3.2. Propensity Score Estimation
We estimated a propensity score (PS) representing the likelihood that the attending physicians would consistently accept ACM suggestions for each patient treated in ACM centers included in the study. We included in the model patients’ characteristics potentially affecting Hb target achievement based on our previous studies [50]. The distribution of propensity scores before matching is displayed in Figure 3.
The distribution of propensity scores across groups shows a wide common support region. However, a non-negligible share of ACM patients with extremely high propensity scores have only few available matches among patients in the reference group. After matching, the propensity score in the ACM group was not significantly different compared to the reference group (ACM: 0.593±0.102; Reference: 0.592±0.102). Among unmatched ACM patients the propensity score was slightly higher (ACMU=0.62±114).
3.3. Study Sample after Matching
After PS matching, both exposure groups included 1942 patients whereas 1167 ACM adherent patients could not be matched. Unmatched ACM patients had longer dialysis vintage, more likely had peripheral artery disease and were more likely to have an arteriovenous fistula as vascular access. Differences in baseline characteristics between matched ACM adherent and non-ACM patients were negligible or very small in magnitude (Table 2). Of note, after matching, 19.5% (n=323) in the reference group and of the ACM group (n=74.6%) were treated with online hemodiafiltration (OL-HDF). Given that we observed a strong overlap between ACM activation in centers were HDF was more prevalent, we could not include this variable in the statistical model.
3.4. Hospitalization and Mortality Rate
The incidence of hospitalization in the whole sample before matching was 80.9/100 person-years (95% CI: 79.6-82.3/100 person-years). Hospital admission rate was lower in the ACM group compared to the reference group (ACM group: 71.3/100 person-years, 95% CI: 68.0-74.6/100 person-years; Reference group: 82.6/100 person-years, 95% CI: 81.2-84.2/100 person-years; Incidence Rate Difference: 11.4, 95% CI: 7.6-15.2/100 person-years, p<0.001).
After propensity score matching, we observed 80.9 admissions/100 person-years (95% CI: 77.8-84.1/100 person-years). Hospital admission rate was statistically lower in the ACM group compared to the reference group after matching (ACM group: 74.3/100 person-years, 95% CI: 70.2-78.7/100 person-years; Reference group: 86.7/100 person-years, 95% CI: 82.4-91.6/100 person-years; Incidence Rate Difference: 12.6/100 person-years, 95% CI: 6.3-18.9/100 person-years, p<0.001). During the follow-up period, 385 patients died (incidence rate: 9.89%; 95% CI: 8.93–10.91%). We observed no evidence of survival benefit for patients treated with ACM guidance during the follow up period of 1 year (hazard ratio = 0.93; p-value=0.51).
3.5. Secondary Analysis
Since we observed residual imbalance in Kt/V after propensity score matching, we included this variable as a confounder in a zero-inflated negative binomial model. Lower Kt/V was significantly associated with increased hospitalization risk (RR=0.96 per each 0.1 increase in Kt/V; p<0.01). The estimated risk of hospitalization in the ACM group was still 12% lower compared to the reference group (adjusted rates: ACM group, 83.6/100 person-years; Reference group, 95.0/100 person-years; adjusted Risk Ratio: 0.88, p<0.001).
4. Discussion
In this propensity-score matched, real-world, historical cohort study we observed that anemia management based on the Anemia Control Model (ACM) recommendations compared to standard of care was associated with a significant reduction in all cause hospitalizations among hemodialysis patients. Mechanisms leading to reduced hospitalization associated with optimization of anemia management may include reduced likelihood of cardiovascular complications associated with Hb variability [29,34,35] and optimization of ESA and supplemental iron dosing [20,27,51,52,53,54,55]. While previous clinical studies have consistently shown that usage of ACM in clinical practice is associated with large ESA savings as well as improved clinical outcomes, including hemoglobin target achievement, reduced risk of severe anemia, and reduced hemoglobin cycling [42,46,48], this study further showed that improved anemia management by the use of AI-supported decision making is associated with reduced hospitalization rates.
ACM is a decision support system providing personalized drug dosage suggestions considering a set of commonly available clinical information such as hemoglobin and ferritin values, markers of inflammation, hydration status, and demographic variables [40]. The software is based on an artificial neural network which first simulates patient-specific dose-response relationship and then uses a reward function to select the optimal dosage minimizing drug utilization while maximizing the likelihood of hemoglobin target achievement [40,44,45]. Usage of predictive algorithms such as ACM or other AI-assisted anemia management systems [56,57,58] may help overcome known clinical challenges, including non-linearity of ESA dose-response relationships [58,59], the temporal discrepancy between the ESA half-life and RBCs’ lifespan (months) [60], differences in ESA responsiveness between patients [24,61] and temporal variations in bone marrow responsiveness [60,62,63].
Despite improvement in hospitalization rate, the reduction in mortality rate associated with ACM was not statistically significant. Previous studies have shown that patients exposed to higher dosage of ESA may be at higher mortality risk [64,65,66,67,68]. Conversely, studies concerning the association between hemoglobin variability, hemoglobin levels and mortality risk obtained mixed results [29,35,61,69,70,71,72,73]. Failure to observe a statistically significant reduction in mortality rate in our study may be due insufficient power, short follow up time or insufficient improvement in anemia management to translate in sizeable survival benefits.
This study has several strengths. Our large multinational sample allowed extensive adjustment for potential confounding factors and extends the generizability of results to different populations and clinical settings. Additionally, the use of Propensity Score Matching offers several advantages in observational studies by addressing confounding bias and approximating the conditions of a randomized controlled trial. By matching participants with similar propensity scores, it balances the distribution of observed covariates between treated and reference groups, enhancing the comparability of these groups. Despite ACM activation does not depend on clinical considerations but it is a policy decision adopted at clinic level, acceptance of ACM suggestions may be related to patients’ clinical characteristics. In our study, the distribution of propensity scores of the two groups largely overlapped, suggesting that activation and usage of ACM was poorly related to patients’ medical parameters. Nevertheless, this study is also subject to few limitations. Observational studies cannot provide definitive proof of causality. Despite extensive adjustment by propensity score matching, residual confounding from unmeasured clinical parameters cannot be completely ruled out. Additionally, we could not match a non-trivial proportion of patients in the ACM arm. Unmatched ACM patients had longer dialysis vintage, more likely had peripheral artery disease and were more likely to have an arteriovenous fistula as vascular access. Hospitalization rate among unmatched ACM patients was lower than either the reference group, and the matched ACM patients. Even though our stringent matching criteria may have led to underestimation of ACM benefit, it may also have ensured the generalizability of results to the broader dialysis population. Finally, we could not rule out the possibility that the unequal distribution of online hemodiafiltration (OL-HDF) treatment across exposure groups may have affected our results. In fact, there was a strong overlap between ACM activation in centers were HDF was more prevalent, a condition that prevented including this variable in the model. Even though the Convince Study, the FRENCHIE study and the Turkish OL-HDF study did not show a statistically significant hospitalization risk reduction in the OL-HDF group [74,75,76], this benefit has been reported in previous studies [77], thus leaving the possibility that our results are confounded by imbalance in treatment modality distribution across exposure groups. Therefore, further studies should analyze the interplay between ACM and dialysis modality in detail.
5. Conclusion
We observed a statistically significant association between the adoption of ACM-assisted anemia management and reduced hospitalization among hemodialysis patients. The results from this study extend on previous research showing that ACM usage improved hemoglobin target achievement, reduced the likelihood of severe anemia and hemoglobin variability while reducing ESA usage. Overall, the evidence generated in this article further supports the utility of the ACM as a decision support tool for anemia management in clinical practice and provides the rational to assess the potential for incremental benefits of ACM among OL-HDF patients. Further studies should assess the cost-effectiveness of ACM for anemia management compared to standard of care.
Author Contributions
Mario Garbelli designed the study, conducted statistical analyses, contributed to interpretation of the results, wrote the first draft of the paper, and approved the final version of the manuscript. Luca Fumagalli contributed to statistical analysis, contributed to interpretation of results, contributed to manuscript drafting and approved the final version of the manuscript. Luca Neri designed the study, contributed to statistical analysis, contributed to interpretation of the results, and approved the final version of the manuscript. Stefano Stuard designed the study, contributed to interpretation of the results, and approved the final version of the manuscript. Maria Eva Baro Salvador, Abraham Rincon Bello, Diana Samaniego Toro Francesco Bellocchio, Luca Fumagalli, Milena Chermisi, Christian Apel, Jovana Petrovic, Dana Kendzia, Jasmine Jon Titapiccolo, Julianna Yeung, Carlo Barbieri, Flavio Mari, Len Usvyat, and John Larkin contributed to the study design and interpretation of the results and approved the final version of the manuscript. All authors discussed the results, revised the first version of the manuscript, and approved the submitted version of the article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
All subjects consented in writing that their data could be used for secondary analysis. Each patient was informed of their right to withdraw their consent at any time. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Hospital Clínic, Barcelona (HCB/2022/1141).
Informed Consent Statement
All subjects consented in writing that their data could be used for secondary research and analysis. Each patient was informed of their right to withdraw their consent at any time. Given the retrospective, registry-based nature of the research, a study-specific informed consent was waived by the Ethical Committee.
Data Availability Statement
The data that support the findings of this study are not publicly available due to privacy reasons, but they can be obtained from the corresponding author, Luca Neri, upon reasonable request.
Conflicts of Interest
Mario Garbelli, Maria Eva Baro Salvador, Abraham Rincon Bello, Diana Samaniego Toro, Francesco Bellocchio, Luca Fumagalli, Milena Chermisi, Christian Apel, Jovana Petrovic, Dana Kendzia, Jasmine Jon Titapiccolo, Julianna Yeung, Carlo Barbieri, Flavio Mari, Len Usvyat, John Larkin, Stefano Stuard, Luca Neri are full time employees at Fresenius Medical Care. Len Usvyat, John Larkin report share options/ownership in Fresenius Medical Care and being an inventor on patents in the field of dialysis. Len Usvyat reports being an advisory board member for Privacy Analytics Inc. John Larkin reports receipt of honorarium from The Lancet, being on the Editorial Board of Frontiers in Physiology and Frontiers in Medicine, Nephrology, and being a chairperson for the MONitoring Dialysis Outcomes (MONDO) Initiative study group and serving on the MONDO Steering Committee.
References
- Kidney Disease: Improving Global Outcomes (KDIGO) Anemia Work Group. KDIGO Clinical Practice Guideline for Anemia in Chronic Kidney Disease. Kidney Int Suppl. Published online 2012. [CrossRef]
- Hanna RM, Streja E, Kalantar-Zadeh K. Burden of Anemia in Chronic Kidney Disease: Beyond Erythropoietin. Adv Ther. 2021;38(1):52-75. [CrossRef]
- KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for Anemia in Chronic Kidney Disease. Am J Kidney Dis. 2006;47(5 Suppl 3).
- Toft G, Heide-Jørgensen U, van Haalen H, et al. Anemia and clinical outcomes in patients with non-dialysis dependent or dialysis dependent severe chronic kidney disease: a Danish population-based study. J Nephrol. 2020;33(1):147-156. [CrossRef]
- Quon P, Gitlin M, Isitt JJ, et al. Cost-effectiveness of treating chronic anemia with epoetin alfa among hemodialysis patients in the United States. Health Outcomes Res Med. 2012;3(2):e79-e89. [CrossRef]
- Toida T, Iwakiri T, Sato Y, Komatsu H, Kitamura K, Fujimoto S. Relationship between hemoglobin levels corrected by interdialytic weight gain and mortality in japanese hemodialysis patients: Miyazaki dialysis cohort study. PLoS One. 2017;12(1):1-15. [CrossRef]
- KIDGO Anaemia work group. KDIGO Clinical Practice Guideline for Anemia in Chronic Kidney Disease. Kidney Int Suppl. 2012;2(4).
- McMurray JJV, Parfrey PS, Adamson JW, et al. Kidney disease: Improving global outcomes (KDIGO) anemia work group. KDIGO clinical practice guideline for anemia in chronic kidney disease. Kidney Int Suppl. 2012;2(4). [CrossRef]
- Locatelli F, Nissenson AR, Barrett BJ, et al. Clinical practice guidelines for anemia in chronic kidney disease: Problems and solutions. A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). In: Kidney International. Vol 74. ; 2008. [CrossRef]
- Borawski B, Malyszko JS, Kwiatkowska M, Malyszko J. Current status of renal anemia pharmacotherapy—what can we offer today. J Clin Med. 2021;10(18). [CrossRef]
- Drüeke TB, Parfrey PS. Summary of the KDIGO guideline on anemia and comment: Reading between the (guide)line(s). Kidney Int. 2012;82(9):952-960. [CrossRef]
- UK Renal Registry (UKRR). Adults on In-Centre Haemodialysis ( ICHD ) in the UK at the End of 2020.; 2020. https://ukkidney.org/sites/renal.org/files/24th_UKRR_ANNUAL_REPORT_ICHD_Ch5.pdf.
- Zhao X, Niu Q, Gan L, et al. Baseline data report of the China Dialysis Outcomes and Practice Patterns Study (DOPPS). Sci Rep. 2021;11(1):1-10. [CrossRef]
- Chait Y, Nathanson BH, Germain MJ. Individualized anemia management enhanced by ferric pyrophosphate citrate protocol. Sci Rep. 2022;12(1):1-7. [CrossRef]
- United States Renal Data System. Clinical indicators & preventive care. In: 2022 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2022. https://usrds-adr.niddk.nih.gov/2022/end-stage-renal-disease/3-clinical-indicators-and-preventive-care.
- Gilbertson DT, Ebben JP, Foley RN, Weinhandl ED, Bradbury BD, Collins AJ. Hemoglobin level variability: Associations with mortality. Clin J Am Soc Nephrol. 2008;3(1):133-138. [CrossRef]
- Ishani A, Solid CA, Weinhandl ED, Gilbertson DT, Foley RN, Collins AJ. Association between number of months below K/DOQI haemoglobin target and risk of hospitalization and death. Nephrol Dial Transplant. 2008;23(5):1682-1689. [CrossRef]
- Phrommintikul A, Haas SJ, Elsik M, Krum H. Mortality and target haemoglobin concentrations in anaemic patients with chronic kidney disease treated with erythropoietin: a meta-analysis. Lancet. 2007;369(9559):381-388. [CrossRef]
- Parfrey PS, Foley RN, Wittreich BH, Sullivan DJ, Zagari MJ, Frei D. Double-blind comparison of full and partial anemia correction in incident hemodialysis patients without symptomatic heart disease. J Am Soc Nephrol. 2005;16(7):2180-2189. [CrossRef]
- Singh AK, Szczech L, Tang KL, et al. Correction of Anemia with Epoetin Alfa in Chronic Kidney Disease. N Engl J Med. 2006;355(20):2085-2098. [CrossRef]
- Lau JH, Gangji AS, Rabbat CG, Brimble KS. Impact of haemoglobin and erythropoietin dose changes on mortality: A secondary analysis of results from a randomized anaemia management trial. Nephrol Dial Transplant. 2010;25(12):4002-4009. [CrossRef]
- Besarab A, Bolton WK, Browne JK, et al. The Effects of Normal as Compared with Low Hematocrit Values in Patients with Cardiac Disease Who Are Receiving Hemodialysis and Epoetin. N Engl J Med. 1998;339(9):584-590. Accessed May 6, 2024. [CrossRef]
- Pfeffer MA, Burdmann EA, Chen CY, et al. A Trial of Darbepoetin Alfa in Type 2 Diabetes and Chronic Kidney Disease. N Engl J Med. 2009;361(21):2019-2032. [CrossRef]
- Solomon SD, Uno H, Lewis EF, et al. Erythropoietic Response and Outcomes in Kidney Disease and Type 2 Diabetes. N Engl J Med. 2010;363(12):1146-1155. [CrossRef]
- Szczech LA, Barnhart HX, Inrig JK, et al. Secondary analysis of the CHOIR trial epoetin-a dose and achieved hemoglobin outcomes. Kidney Int. 2008;74(6):791-798. [CrossRef]
- Food and Drug Administration. FDA Drug Safety Communication: Modified Dosing Recommendations to Improve the Safe Use of Erythropoiesis-Stimulating Agents in Chronic Kidney Disease.; 2011.
- Koulouridis I, Alfayez M, Trikalinos TA, Balk EM, Jaber BL. Dose of Erythropoiesis-Stimulating Agents and Adverse Outcomes in CKD: a metaregression analysis. Am J Kidney Dis. 2013;61(1):44-56. [CrossRef]
- Jeong HY, Ko EJ, Kim SH, et al. Administration of a high-dose erythropoietin-stimulating agent in hemodialysis patients is associated with late arteriovenous fistula failure. Yonsei Med J. 2017;58(4):793-799. [CrossRef]
- Kuragano T, Matsumura O, Matsuda A, et al. Association between hemoglobin variability, serum ferritin levels, and adverse events/mortality in maintenance hemodialysis patients. Kidney Int. 2014;86(4):845-854. [CrossRef]
- Pérez-García R, Varas J, Cives A, et al. Increased mortality in haemodialysis patients administered high doses of erythropoiesis-stimulating agents: a propensity score-matched analysis. Nephrol Dial Transplant. 2018;33(1). [CrossRef]
- Filho NS, Lages JS, de Araújo Brito DJ, et al. Variability in hemoglobin levels and the factors associated with mortality in hemodialysis patients: A 78-month follow-up study. Int J Environ Res Public Health. 2021;18(3):1-11. [CrossRef]
- Streja E, Park J, Chan TY, et al. Erythropoietin Dose and Mortality in Hemodialysis Patients: Marginal Structural Model to Examine Causality. Int J Nephrol. 2016;2016. [CrossRef]
- Cizman B, Smith HT, Camejo RR, et al. Clinical and Economic Outcomes of Erythropoiesis-Stimulating Agent Hyporesponsiveness in the Post-Bundling Era. Kidney Med. 2020;2(5):589-599.e1. [CrossRef]
- Ebben JP, Gilbertson DT, Foley RN, Collins AJ. Hemoglobin level variability: associations with comorbidity, intercurrent events, and hospitalizations. Clin J Am Soc Nephrol. 2006;1(6):1205-1210. [CrossRef]
- Lin FJ, Zhang X, Huang LS, et al. Impact of hemoglobin variability on cardiovascular mortality in maintenance hemodialysis patients. Int Urol Nephrol. 2018;50(9):1703-1712. [CrossRef]
- Zhao L, Hu C, Cheng J, Zhang P, Jiang H, Chen J. Haemoglobin variability and all-cause mortality in haemodialysis patients: A systematic review and meta-analysis. Nephrology. 2019;24(12):1265-1272. [CrossRef]
- Yang W, Israni RK, Brunelli SM, Joffe MM, Fishbane S, Feldman HI. Hemoglobin variability and mortality in ESRD. J Am Soc Nephrol. 2007;18(12):3164-3170. [CrossRef]
- Fishbane S, Berns JS. Evidence and implications of haemoglobin cycling in anaemia management. Nephrol Dial Transplant. 2007;22(8):2129-2132. [CrossRef]
- Schneider A, Asmus G, Biggar P, et al. Hemoglobin Cycling in Hemodialysis Patients. Nephrol Res Rev. 2010;2(1):1-5. [CrossRef]
- Barbieri C, Mari F, Stopper A, et al. A new machine learning approach for predicting the response to anemia treatment in a large cohort of End Stage Renal Disease patients undergoing dialysis. Comput Biol Med. 2015;61:56-61. [CrossRef]
- Barbieri C, Molina M, Ponce P, et al. An international observational study suggests that artificial intelligence for clinical decision support optimizes anemia management in hemodialysis patients. Kidney Int. 2016;90(2). [CrossRef]
- Bucalo ML, Barbieri C, Roca S, et al. The anaemia control model: Does it help nephrologists in therapeutic decision-making in the management of anaemia? Nefrologia. 2018;38(5). [CrossRef]
- Garbelli M, Bellocchio F, Baro Salvador ME, et al. The use of Anemia Control Model is Associated with Improved Hemoglobin Target Achievement, Lower Rates of Inappropriate Erythropoietin Stimulating Agents and Severe Anemia Among Dialysis Patients. Blood Purif. Published online February 21, 2024. [CrossRef]
- Barbieri C, Bolzoni E, Mari F, et al. Performance of a predictive model for long-Term hemoglobin response to darbepoetin and iron administration in a large cohort of hemodialysis patients. PLoS One. 2016;11(3). [CrossRef]
- Escandell-Montero P, Chermisi M, Martínez-Martínez JM, et al. Optimization of anemia treatment in hemodialysis patients via reinforcement learning. Artif Intell Med. 2014;62(1):47-60. [CrossRef]
- Barbieri C, Molina M, Ponce P, et al. An international observational study suggests that artificial intelligence for clinical decision support optimizes anemia management in hemodialysis patients. Kidney Int. 2016;90(2):422-429. [CrossRef]
- Barbieri C, Molina M, Ponce P, et al. An international observational study suggests that artificial intelligence for clinical decision support optimizes anemia management in hemodialysis patients. Kidney Int. 2016;90(2):422-429. [CrossRef]
- Garbelli M, Bellocchio F, Salvador MEB, et al. The Use of Anemia Control Model Is Associated with Improved Hemoglobin Target Achievement, Lower Rates of Inappropriate Erythropoietin Stimulating Agents, and Severe Anemia among Dialysis Patients. Blood Purif. 2024;53(5):310-322. [CrossRef]
- Garbelli M, Ion Titapiccolo J, Bellocchio F, Stuard S, Brancaccio D, Neri L. Prolonged patient survival after implementation of a continuous quality improvement programme empowered by digital transformation in a large dialysis network. Nephrol Dial Transplant. 2022;37(3):469-476. [CrossRef]
- Pellicer-Valero OJ, Cattinelli I, Neri L, Mari F, Martín-Guerrero JD, Barbieri C. Enhanced prediction of hemoglobin concentration in a very large cohort of hemodialysis patients by means of deep recurrent neural networks. Artif Intell Med. 2020;107:101898. [CrossRef]
- Palmer SC, Navaneethan SD, Craig JC, et al. Meta-analysis: Erythropoiesis-stimulating agents in patients with chronic kidney disease. Ann Intern Med. 2010;153(1):23-33. [CrossRef]
- Solomon SD, Uno H, Lewis EF, et al. Erythropoietic Response and Outcomes in Kidney Disease and Type 2 Diabetes. N Engl J Med. 2010;363(12):1146-1155. [CrossRef]
- Besarab A, Bolton WK, Browne JK, et al. The Effects of Normal as Compared with Low Hematocrit Values in Patients with Cardiac Disease Who Are Receiving Hemodialysis and Epoetin. N Engl J Med. 1998;339(9):584-590. [CrossRef]
- Pfeffer MA, Burdmann EA, Chen CY, et al. A Trial of Darbepoetin Alfa in Type 2 Diabetes and Chronic Kidney Disease. N Engl J Med. 2009;361(21):2019-2032. [CrossRef]
- Szczech LA, Barnhart HX, Inrig JK, et al. Secondary analysis of the CHOIR trial epoetin-.alpha dose and achieved hemoglobin outcomes. Kidney Int. 2008;74(6):791-798. [CrossRef]
- Bachmann F, Koch G, Pfister M, Szinnai G, Schropp J. OptiDose: Computing the Individualized Optimal Drug Dosing Regimen Using Optimal Control. J Optim Theory Appl. 2021;189(1):46-65. [CrossRef]
- Yang JY, Lee TC, Liao WT, Hsu CC. Multi-head self-attention mechanism enabled individualized hemoglobin prediction and treatment recommendation systems in anemia management for hemodialysis patients. Heliyon. 2023;9(2):e12613. [CrossRef]
- Rogg S, Fuertinger DH, Volkwein S, Kappel F, Kotanko P. Optimal EPO dosing in hemodialysis patients using a non-linear model predictive control approach. J Math Biol. 2019;79(6-7):2281-2313. [CrossRef]
- Jörg DJ, Fuertinger DH, Kotanko P. Mechanisms of hemoglobin cycling in anemia patients treated with erythropoiesisstimulating agents. PLoS Comput Biol. 2023;19(1). [CrossRef]
- Kalicki RM, Uehlinger DE. Red Cell Survival in Relation to Changes in the Hematocrit: More Important than You Think. Blood Purif. 2008;26(4):355-360. [CrossRef]
- Gilbertson DT, Hu Y, Peng Y, Maroni BJ, Wetmore JB. Variability in hemoglobin levels in hemodialysis patients in the current era: A retrospective cohort study. Clin Nephrol. 2017;88(5):254-263. [CrossRef]
- Portolés J, Martín L, Broseta JJ, Cases A. Anemia in Chronic Kidney Disease: From Pathophysiology and Current Treatments, to Future Agents. Front Med. 2021;8(March):1-14. [CrossRef]
- Gaweda AE, Goldsmith LJ, Brier ME, Aronoff GR. Iron, inflammation, dialysis adequacy, nutritional status, and hyperparathyroidism modify erythropoietic response. Clin J Am Soc Nephrol. 2010;5(4):576-581. [CrossRef]
- Karimi Z, Raeisi Shahraki H, Mohammadian-Hafshejani A. Erythropoiesis-stimulating agents and cardiovascular mortality: A systematic review and meta-analysis of 17 studies and 372,156 hemodialysis patients. Int J Cardiol Cardiovasc risk Prev. 2023;19:200220. [CrossRef]
- Suttorp MM, Hoekstra T, Mittelman M, et al. Treatment with high dose of erythropoiesis-stimulating agents and mortality: Analysis with a sequential Cox approach and a marginal structural model. Pharmacoepidemiol Drug Saf. 2015;24(10):1068-1075. [CrossRef]
- Weinhandl ED, Gilbertson DT, Collins AJ. Association of mean weekly epoetin alfa dose with mortality risk in a retrospective cohort study of medicare hemodialysis patients. Am J Nephrol. 2011;34(4):298-308. [CrossRef]
- Streja E, Park J, Chan TY, et al. Erythropoietin Dose and Mortality in Hemodialysis Patients: Marginal Structural Model to Examine Causality. Int J Nephrol. 2016;2016. [CrossRef]
- Pérez-García R, Varas J, Cives A, et al. Increased mortality in haemodialysis patients administered high doses of erythropoiesis-stimulating agents: a propensity score-matched analysis. Nephrol Dial Transplant. 2018;33(1):690-699. [CrossRef]
- Handelman GJ, Kotanko P, Cisternas MG, et al. Hospitalization and mortality in hemodialysis patients: Association with hemoglobin variability. Blood Purif. 2013;35(4):247-257. [CrossRef]
- Eckardt KU, Kim J, Kronenberg F, et al. Hemoglobin variability does not predict mortality in european hemodialysis patients. J Am Soc Nephrol. 2010;21(10):1765-1775. [CrossRef]
- Goodkin DA, Fuller DS, Robinson BM, et al. Naturally occurring higher hemoglobin concentration does not increase mortality among hemodialysis patients. J Am Soc Nephrol. 2011;22(2):358-365. [CrossRef]
- Ofsthun N, LaBrecque J, Lacson E, Keen M, Lazarus JM. The effects of higher hemoglobin levels on mortality and hospitalization in hemodialysis patients. Kidney Int. 2003;63(5):1908-1914. [CrossRef]
- Weinhandl ED, Peng Y, Gilbertson DT, Bradbury BD, Collins AJ. Hemoglobin variability and mortality: Confounding by disease severity. Am J Kidney Dis. 2011;57(2):255-265. [CrossRef]
- Morena M, Jaussent A, Chalabi L, et al. Treatment tolerance and patient-reported outcomes favor online hemodiafiltration compared to high-flux hemodialysis in the elderly. Kidney Int. 2017;91(6):1495-1509. [CrossRef]
- Ok E, Asci G, Toz H, et al. Mortality and cardiovascular events in online haemodiafiltration (OL-HDF) compared with high-flux dialysis: results from the Turkish OL-HDF Study. Nephrol Dial Transplant. 2013;28(1):192-202. [CrossRef]
- Blankestijn PJ, Vernooij RWM, Hockham C, et al. Effect of Hemodiafiltration or Hemodialysis on Mortality in Kidney Failure. N Engl J Med. 2023;389(8):700-709. [CrossRef]
- Mitchell CR, Hornig C, Canaud B. Systematic review to compare the outcomes associated with the modalities of expanded hemodialysis (HDx) versus high-flux hemodialysis and/or hemodiafiltration (HDF) in patients with end-stage kidney disease (ESKD). Semin Dial. 2023;36(2):86-106. [CrossRef]
Figure 1.
Study Design Diagram. This diagram illustrates the timeline and structure of the study, detailing the ascertainment period, follow-up period, exposure groups (ACM users and standard of care), potential confounders, and primary study endpoints (hospital admissions and mortality).
Figure 1.
Study Design Diagram. This diagram illustrates the timeline and structure of the study, detailing the ascertainment period, follow-up period, exposure groups (ACM users and standard of care), potential confounders, and primary study endpoints (hospital admissions and mortality).
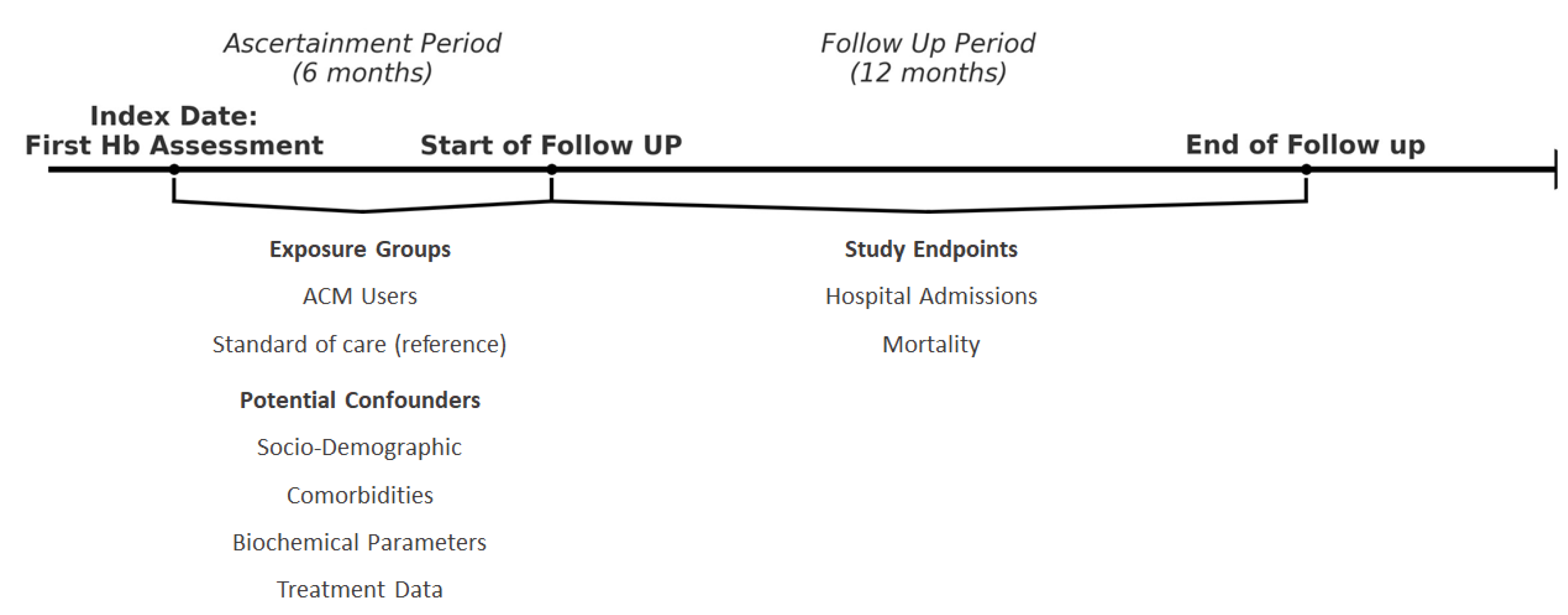
Figure 2.
Study Flowchart Diagram. Flowchart depicting the selection process for the ACM and Reference groups from the initial sample (N=37,009). The ACM group (N=5,273) was refined through multiple exclusion criteria, resulting in a final sample size of N=3,108. The Reference group (N=31,736) was similarly refined to a final sample size of N=17,101.
Figure 2.
Study Flowchart Diagram. Flowchart depicting the selection process for the ACM and Reference groups from the initial sample (N=37,009). The ACM group (N=5,273) was refined through multiple exclusion criteria, resulting in a final sample size of N=3,108. The Reference group (N=31,736) was similarly refined to a final sample size of N=17,101.
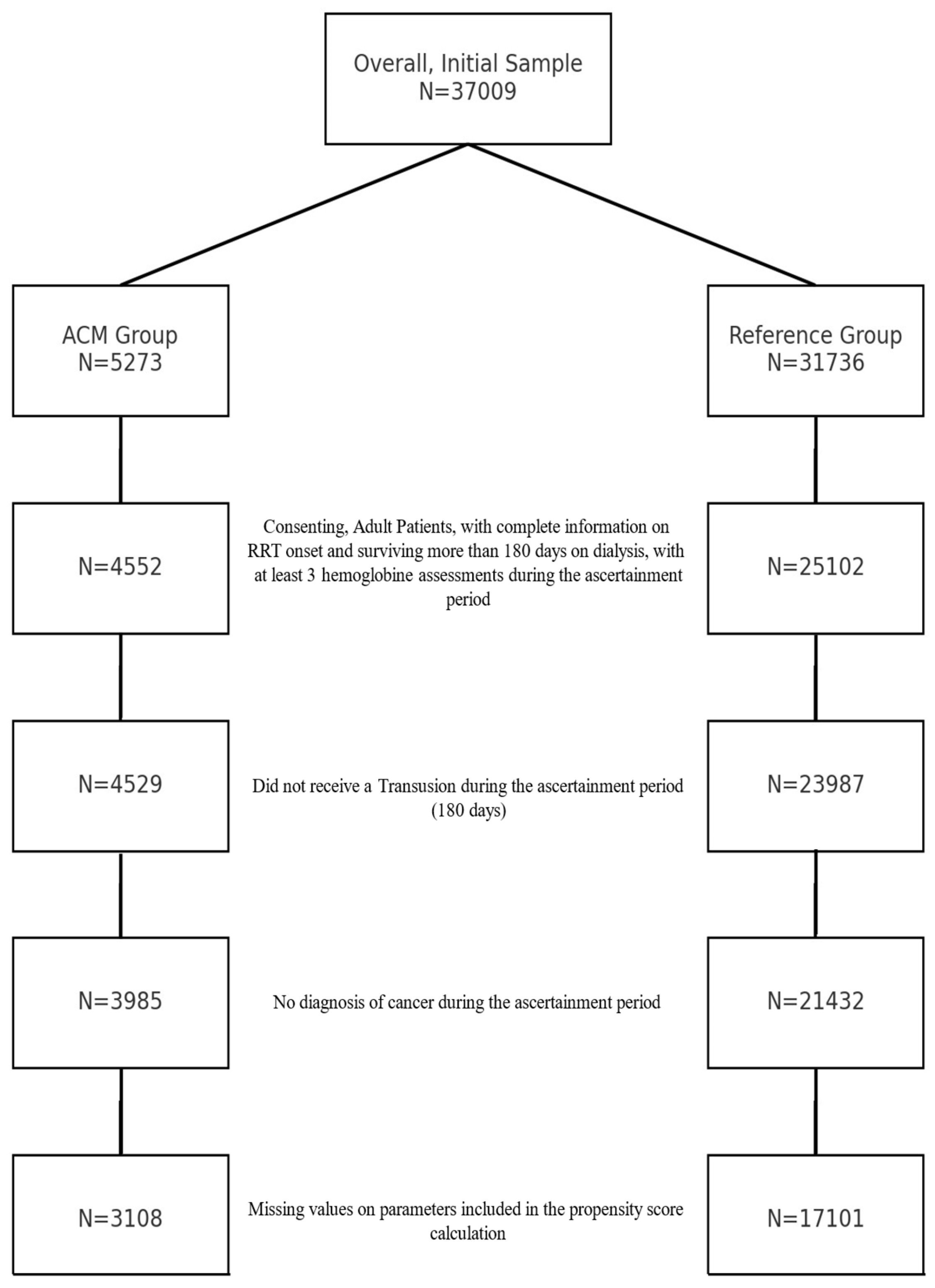
Figure 3.
Distribution of Propensity Scores in the ACM and Reference Group before matching. Distribution of propensity scores for the ACM group (red) and the Reference group (black). The histogram demonstrates the overlap and divergence in propensity scores between the two groups, indicating the relative frequency of individuals across the range of propensity scores.
Figure 3.
Distribution of Propensity Scores in the ACM and Reference Group before matching. Distribution of propensity scores for the ACM group (red) and the Reference group (black). The histogram demonstrates the overlap and divergence in propensity scores between the two groups, indicating the relative frequency of individuals across the range of propensity scores.
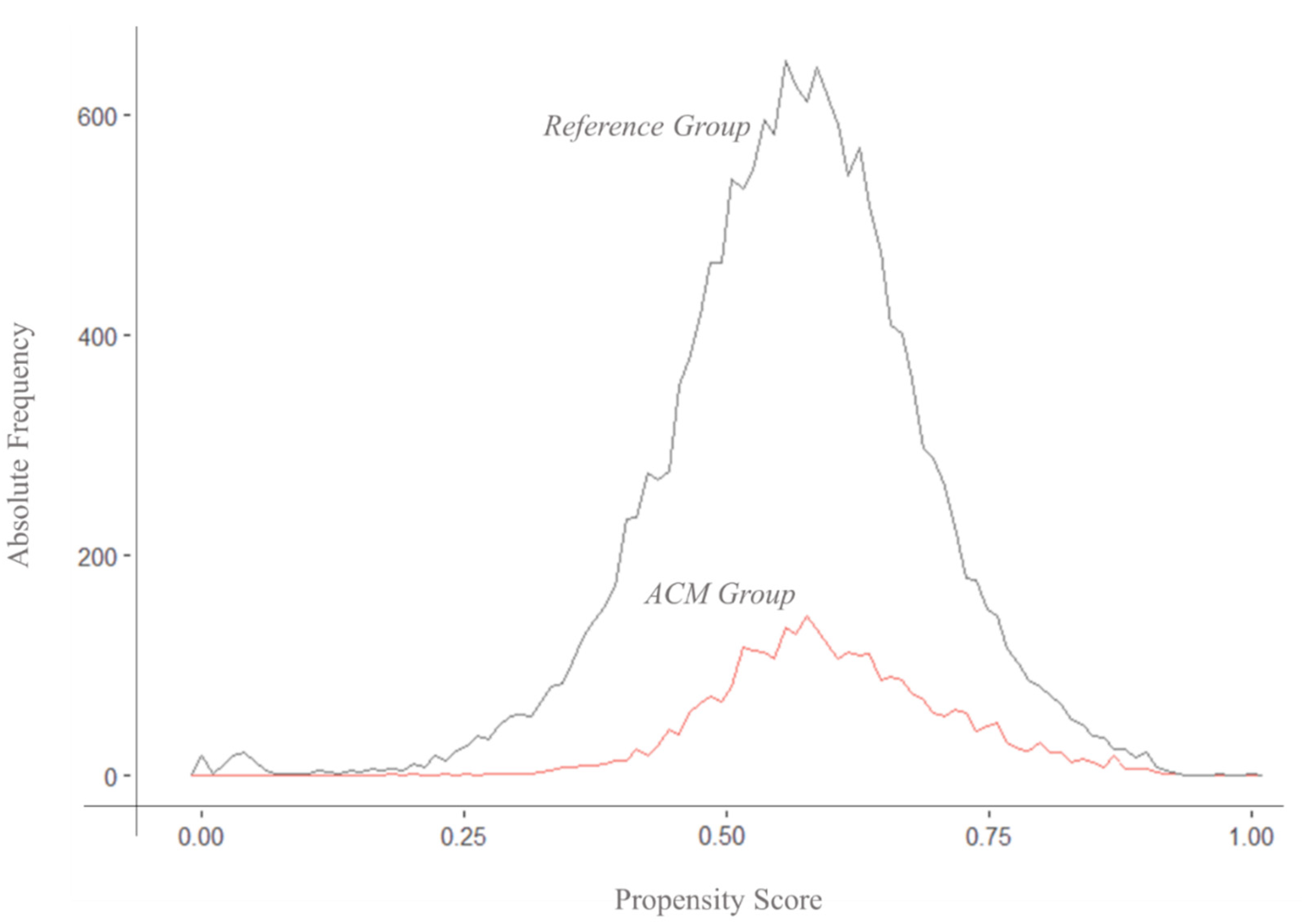

Table 1.
Sample Characteristics.
| Exposure Groups | Significance* | ||||
|---|---|---|---|---|---|
| Characteristics |
Whole Sample (n= 20209) |
ACM Group (n=3108) |
Reference Group (n= 17101) |
p-value | Effect Size |
| N (%), mean (St.D), or Median (IQR) | |||||
| Age | 65.3 (14.5) | 67.8 (14.4) | 64.8 (14.4) | <0.001 | 0.0107 |
| Men | 11962 (59.2) | 1945 (62.6) | 10017 (58.6) | <0.001 | 0.0234 |
| BMI | 26.8 (6.5) | 26.4 (5.4) | 26.9 (6.7) | <0.001 | 0.0015 |
| Dialysis Vintage (years) | 2,03 (4,7) | 2,8 (5,26) | 1,87 (4,59) | <0.001 | 0,2672 |
| Vascular Access | <0.001 | 0.1280 | |||
| Arteriovenous Fistula | 5578 (28.2) | 592 (19.0) | 4986 (29.9) | ||
| Catheter or Graft | 14188 (71.8) | 2517 (81.0) | 11671 (70.1) | ||
| Missing | 419 (2.1) | 0 (0) | 419 (2.5) | ||
| Kt/V | 1.6 (0.4) | 1.9 (0.4) | 1.6 (0.4) | <0.001 | 0.2554 |
| Treatment Time (minutes) | 241.8 (13.1) | 243.7 (13.1) | 241.5 (13.1) | <0.001 | 0.0169 |
| Hemoglobin (g/dL) | 11.1 (1.2) | 11.4 (1.1) | 11.0 (1.2) | <0.001 | 0.0188 |
| Albumin (g/dL) | 3.9 (0.4) | 4.0 (0.5) | 3.9 (0.4) | <0.001 | 0.0075 |
| Ferritin (ng/mL) | 558.8 (436.5) | 567.0 (349.7) | 557.3 (450.8) | 0.176 | 0.0037 |
| Phosphate (mg/dL) | 4.7 (1.4) | 4.3 (1.1) | 4.8 (1.4) | <0.001 | 0.0269 |
| Leukocytes (10^3/µL) | 7883.2 (41545.4) | 6582.5 (1824.9) | 8123.0 (45203.6) | <0.001 | 0.0286 |
| C-Reactive Protein (mg/L) | 13.6 (22.3) | 12.1 (17.0) | 13.8 (23.1) | <0.001 | 0.0030 |
| Transferrin Saturation (%) | 29.9 (12.8) | 32.2 (11.9) | 29.5 (12.9) | <0.001 | 0.0007 |
| MCV (fL) | 94.3 (6.5) | 95.1 (5.9) | 94.1 (6.6) | <0.001 | 0.0288 |
| MCH (pg/cell) | 32.9 (43.1) | 32.9 (0.8) | 32.9 (46.9) | 0.874 | 0.0044 |
| Serum Sodium (mmol/L) | 138.1 (4.0) | 138.3 (2.6) | 138.1 (4.1) | 0.0042 | 0.0042 |
| Serum Potassium (meq/L) | 4.9 (0.9) | 5.0 (0.6) | 4.9 (0.9) | 0.0066 | 0.0066 |
| Serum Calcium (mg/dL) | 8.8 (1.3) | 9.0 (0.6) | 8.8 (1.4) | 0.0060 | 0.0059 |
| Cerebrovascular disease | 2750 (13.6) | 486 (15.6) | 2264 (13.2) | <0.001 | 0.0401 |
| Chronic pulmonary disease | 2197 (10.9) | 398 (12.8) | 1799 (10.5) | <0.001 | 0.0417 |
| Congestive heart failure | 4376 (21.7) | 696 (22.4) | 3680 (21.5) | 0.287 | 0.0075 |
| Connective tissue disorder | 332 (1.6) | 43 (1.4) | 289 (1.7) | 0.246 | 0.0105 |
| Coronary artery disease | 4199 (20.8) | 621 (20.0) | 3578 (20.9) | 0.243 | 0.0152 |
| Dementia | 313 (1.5) | 53 (1.7) | 260 (1.5) | 0.491 | 0.0115 |
| Diabetes without complication | 6155 (30,5) | 214 (6.9) | 871 (5.1) | <0.001 | 0.0052 |
| Diabetes with organ damage | 5070 (25.1) | 921 (29.6) | 4149 (24.3) | <0.001 | 0.0560 |
| Hemiplegia | 157 (0.8) | 20 (0.6) | 137 (0.8) | 0.418 | 0.0157 |
| Mild liver disease | 2002 (9.9) | 385 (12.4) | 1617 (9.5) | <0.001 | 0.0419 |
| Moderate/severe liver disease | 111 (0.5) | 16 (0.5) | 95 (0.6) | 0.880 | 0.0179 |
| Peptic ulcer disease | 1026 (5.1) | 152 (4.9) | 874 (5.1) | 0.638 | 0.0125 |
| Peripheral Vascular Disease | 3769 (18.7) | 740 (23.8) | 3029 (17.7) | <0.001 | 0.0506 |
Table 1. Sample Characteristics before propensity score matching. Notes: ACM = Anemia Control Model; BMI = Body Mass Index; Kt/V = Dialysis Dose (a measure of dialysis adequacy); MCV = Mean Corpuscular Volume; MCH = Mean Corpuscular Hemoglobin. The table includes mean (standard deviation) for continuous variables and count (percentage) for categorical variables. Statistical significance was assessed using p-values, with effect sizes reported as Cramer’s V for categorical variables and η2 for continuous variables.
Table 2.
Sample Characteristics after Propensity Score Matching.
| Exposure Groups | Significance* | |||||
|---|---|---|---|---|---|---|
| Characteristics | Whole Sample (n= 5051) |
ACM Group (n=1952) |
ACM unmatched (n=1167) |
Reference Group (n= 1952) |
p-value | Effect Size |
| N (%) or mean (St.D) | ||||||
| Age | 66,1 (14,7) | 67,6 (14,5) | 68,3 (14,3) | 63,3 (14,8) | <0.001 | 0.0413 |
| Men | 3165 (62.7) | 1243 (64.0) | 701 (60.1) | 1221 (62.9) | 0.09 | 0.0111 |
| BMI | 26.7 (5.6) | 26.4 (5.3) | 26.3 (5.5) | 27.2 (6.0) | <0.001 | 0.0010 |
| Dialysis Vintage | 2.03 (4.59) | 1.25 (2.98) | 5.29 (5.51) | 1.05 (3.28) | <0.001 | 0.0004 |
| Vascular Access | <0.001 | 0.1410 | ||||
| Catheter or Graft | 1241 (24.8) | 420 (21.6) | 172 (14.7) | 649 (34.2) | ||
| Arteriovenous Fistula | 3766 (75.2) | 1522 (78.4) | 995 (85.3) | 1249 (65.8) | ||
| Missing | 44 (0.9) | 0 (0) | 0 (0) | 44 (2.3) | ||
| Kt/V | 1.8 (0.4) | 1.9 (0.4) | 1.9 (0.4) | 1.5 (0.4) | <0.001 | 0.3300 |
| Treatment Time (minutes) | 242.2 (13.3) | 243.9 (11.8) | 243.2 (15.0) | 239.8 (13.2) | <0.001 | 0.0170 |
| Hemoglobin (g/dL) | 11.3 (1.0) | 11.3 (0.9) | 11.6 (1.2) | 11.2 (0.9) | <0.001 | 0.0061 |
| Albumin (g/dL) | 3.9 (0.4) | 3.9 (0.5) | 4.0 (0.4) | 3.9 (0.4) | <0.001 | 0.0000 |
| Ferritin (ng/mL) | 520.5 (371.9) | 561.0 (362.0) | 577.0 (328.2) | 443.4 (394.3) | <0.001 | 0.0460 |
| Phosphate (mg/dL) | 4.4 (1.1) | 4.3 (1.1) | 4.2 (1.1) | 4.6 (1.1) | <0.001 | 0.0358 |
| Leukocytes (10^3/µL) | 6738.9 (2148.4) | 6685.2 (1833.5) | 6411.6 (1798.3) | 6992.9 (2569.3) | <0.001 | 0.0094 |
| C-Reactive Protein (mg/L) | 11.8 (16.6) | 12.4 (18.0) | 11.8 (15.2) | 11.3 (16.1) | 0.213 | 0.0020 |
| Transferrin Saturation (%) | 30.3 (11.8) | 31.8 (11.6) | 32.9 (12.3) | 27.6 (11.1) | <0.001 | 0.0641 |
| MCV (fL) | 94.3 (6.1) | 95.2 (5.9) | 94.9 (5.9) | 92.9 (6.3) | <0.001 | 0.0663 |
| MCH (pg/cell) | 32.8 (1.0) | 32.9 (0.9) | 32.9 (0.8) | 32.8 (1.1) | <0.001 | 0.0049 |
| Serum Sodium (mmol/L) | 138.1 (3.1) | 138.2 (2.6) | 138.4 (2.7) | 137.9 (3.7) | <0.001 | 0.0044 |
| Serum Potassium (meq/L) | 4.9 (0.6) | 4.9 (0.6) | 5.0 (0.6) | 4.8 (0.6) | <0.001 | 0.0137 |
| Serum Calcium (mg/dL) | 8.9 (0.6) | 8.9 (0.6) | 9.0 (0.7) | 8.8 (0.6) | <0.001 | 0.0137 |
| Cerebrovascular disease | 736 (14.6) | 296 (15.2) | 192 (16.5) | 248 (12.8) | 0.011 | 0.0348 |
| Chronic pulmonary disease | 594 (11.8) | 261 (13.4) | 140 (12.0) | 193 (9.9) | 0.003 | 0.0535 |
| Congestive heart failure | 1117 (22.1) | 425 (21.9) | 275 (23.6) | 417 (21.5) | 0.377 | 0.0043 |
| Connective tissue disorder | 74 (1.5) | 25 (1.3) | 18 (1.5) | 31 (1.6) | 0.703 | 0.0108 |
| Coronary artery disease | 964 (19.1) | 362 (18.6) | 260 (22.3) | 342 (17.6) | 0.005 | 0.0127 |
| Dementia | 84 (1.7) | 37 (1.9) | 16 (1.4) | 31 (1.6) | 0.507 | 0.0098 |
| Diabetes without complication | 332 (6.6) | 141 (7.3) | 73 (6.3) | 118 (6.1) | 0.291 | 0.0226 |
| Diabetes with organ damage | 1454 (28.8) | 612 (31.5) | 311 (26.6) | 531 (27.3) | 0.003 | 0.0450 |
| Hemiplegia | 31 (0.6) | 9 (0.5) | 11 (0.9) | 11 (0.6) | 0.239 | 0.0036 |
| Mild liver disease | 549 (10.9) | 204 (10.5) | 179 (15.3) | 166 (8.5) | <0.001 | 0.0324 |
| Moderate/severe liver disease | 30 (0.6) | 11 (0.6) | 5 (0.4) | 14 (0.7) | 0.578 | 0.0064 |
| Peptic ulcer disease | 239 (4.7) | 88 (4.5) | 66 (5.7) | 85 (4.4) | 0.232 | 0.0025 |
| Peripheral Vascular Disease | 1087 (21.5) | 424 (21.8) | 318 (27.2) | 345 (17.8) | <0.001 | 0.0502 |
Table 2. Sample Characteristics after Propensity Score Matching. Notes: ACM = Anemia Control Model; BMI = Body Mass Index; Kt/V = Dialysis Dose (a measure of dialysis adequacy); MCV = Mean Corpuscular Volume; MCH = Mean Corpuscular Hemoglobin. The table includes mean (standard deviation) for continuous variables and count (percentage) for categorical variables. *Statistical significance refers to the comparison between ACM matched group and the reference group. It was assessed using χ2 or T-test where appropriate, with effect sizes reported as Cramer’s V for categorical variables and η2 for continuous variables.
Table 3.
Incidence Rate of Hospitalization.
| Group | Incidence Rate (events/100 person-years) |
Incidence Rate Difference (events/100 person-years) |
p-value |
|---|---|---|---|
| Before Matching | |||
| Whole Sample | 80.9 (95% CI: 79.6–82.3) | - | - |
| ACM Group | 71.3 (95% CI: 68.0–74.6) | - | - |
| Reference Group | 82.6 (95% CI: 81.2–84.2) | 11.4 (95% CI: 7.6–15.2) | <0.001 |
| After Matching | |||
| Matched Sample | 80.9 (95% CI: 77.8–84.1) | - | - |
| ACM Group | 74.3 (95% CI: 70.2–78.7) | - | - |
| Reference Group | 86.7 (95% CI: 82.4–91.6) | 12.6 (95% CI: 6.3–18.9) | <0.001 |
Table 3. Incidence Rate of Hospitalization. Comparison of hospitalization incidence rates and rate differences between ACM and reference groups before and after matching, with 95% confidence intervals and p-values based on zero-inflated negative binomial regression.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



