Submitted:
13 September 2024
Posted:
17 September 2024
You are already at the latest version
Abstract
Background: Over the past few years there has been immense evolution in various areas particularly in the areas of digital technologies wherein the pace of change is very high. Industrial areas such as operations and supply chain management together with advanced technologies such as machine learning, big data analytics, artificial intelligence, as well as the Internet of Things, create completely different forms of operational models for various industries. In the area of healthcare too, these emerging computational sophistication is introduced to revolutionise the approaches to prevent, diagnose and treat diverse diseases and illnesses. Objective: The objective of this study is to provide an extensive review of the contemporary approaches utilizing data to cope with significant mental disorders. From over 60 relevant scholarly articles published between 2011 and 2023, it discusses how tools such as predictive modelling, social media analysis, data from smartphones, and chatbots help with issues such as early detection, telemonitoring, provision of psychological support, and individualised prevention. Method: An initial literature review to analyse over 60 research articles, which include empirical studies that were conducted between 2011 and 2023. The research assessed implemented novel digital approaches to mental health interventions including big data analytics for predicting condition status, machine learning for examining social media content, behaviour monitoring through smartphone sensors, and using conversational agents or chatbots. The following is an overview of general conclusions from experimental and descriptive secondary research studies published in professional outlets concerning possible advantages and disadvantages of data science applied to important concerns in mental health. Results: Research reveals that integrating subtle e-health tools in tandem with typical treatment approaches holds the potential to expand mental health services to more or less integrate them into clients’ day-to-day lives, and practically individualize effective treatments accordingly. Technological solutions for instance allow remote risk assessment, symptom monitoring and determination of treatment compliance. New lines of virtualized paradigm solve social challenges that interfere with the conventional provision and consumption of care. However, questions of privacy and the long-term effects as well as clinical adoption are yet to be solved in a analytically distinct manner.
Keywords:
Mental health
; Machine learning
; Artificial intelligence
; Big data
; Predictive modeling
; Smartphone sensors
; Just-in-time adaptive interventions
; Digital biomarkers
; Clinical integration
; Technology adoption
; Data-driven healthcare
1. Introduction
1.1. Emergence of Data-Driven Healthcare
In recent decades, the emergence of data-driven technologies has profoundly impacted multiple domains. The exponential growth of digital health data from sources like electronic health records, mobile apps, wearables and social media has fueled adoption of advanced tools like machine learning, artificial intelligence and predictive analytics (Murdoch and Detsky, 2013; Tai et al., 2019). These enable extraction of insights from voluminous, diverse and changing data that would otherwise remain hidden. Consequently, a new field of data-driven or evidence-based healthcare has emerged which leverages such computational methods for tasks like risk assessment, early diagnosis, monitoring treatment response and personalized care planning (Chawla and Davis, 2013; Plaga et al., 2018).
1.2. Relevance for Mental Health
Mental illnesses like depression, anxiety, bipolar disorder, schizophrenia and substance abuse disorders impose enormous individual and societal burdens worldwide (WHO, 2022). However, traditional mental healthcare has frequently suffered from various challenges including stigma attached to conditions, shortage of professionals, high costs and unequal access to services especially in low resource settings (Gooding, 2018; Ferrario et al., 2017). In such a scenario, data-driven technologies can play a transformative role by addressing several unmet needs (Torous and Baker, 2016; Shatte et al., 2019). For instance, the ubiquitous availability of digital platforms provides opportunities for continuous, proactive monitoring and delivery of support beyond clinical settings (Canzian and Musolesi, 2015; Wahle et al., 2016).
1.3. Predictive Modelling Using Machine Learning
Machine learning models have been used to predict mental condition from speech, text, facial expressions, behaviour and biosignals (Joshi et al., 2018; Meng et al., 2013; Ray et al., 2019; Dias and Barbosa, 2019). Logistic regression, decision trees, random forests, deep neural networks, are some of the supervised algorithms that have prove useful in the construction of digital biomarkers for automatic diagnosis, severity assessment, as well as future relapse, treatment responsiveness and risk of suicide (Fulmer et al., 2018; Lahti, 2016; Saeb et al., 2015; Wshah et al., 2019 For example, by estimating temporal variations of the daily pattern of smartphone usage or visits of specific locations or physical activity, models can detect temporal trends that signify the upcoming episodes of depression (Wang et al., 2018).
1.4. Social Media and Internet Data Exploration
More than a billion users express opinions, experiences and emotions on the OSN every day (De Choudhury et al., 2013). Using text and images generated by such users, researchers have used natural language processing and machine learning algorithms to identify population level patterns of mental ailments, investigate stigma and study people’s perceptions and attitudes to different diseases and topics (Zhou et al., 2015; Li et al., 2018; Dao et al., 2016). Likewise, comparing the modes of communication, the content and topics of conversation, and the social interactions detected from the participants in the online mental health forums and support groups over time may also have potential to offer digital phenotyping and cues to identify whether such patient is derenerating or experiencing relapse or probably a new manifestation of a particular mental disorder (De Choudhury et al., 2013; Nguyen et al., 2018
1.5. Smartphone Sensing for Just-In-Time Adaptive Interventions
Mobile phones are everyday used devices and can essentially be used for unobtrusive passive data gathering of various behavioral and physiological parameters due to integrated and attached sensors. Through application of these capabilities, several studies have investigated how such technology might be used to monitor developments in depressive symptoms as they occur, to quickly detect potential high risk situations or events, and to provide prompt, appropriate support or interventional resources to individuals in response to variations in their behaviour or other related factor during the course of the day. This just-in-time adaptive intervention approach has shown promising results in reducing symptoms and improving well-being through personalized, context-aware assistance delivered at opportune moments.
1.6. Purpose of the Study
The purpose of this study is to investigate various data-driven approaches to tackling mental health issues and addressing gaps in traditional care pathways using insights from digital tools and technologies.
1.7. Research Questions
RQ 1: How can machine learning, big data analytics, artificial intelligence and internet of things-based tools be seamlessly integrated within existing provider mental health services to demonstrate clear value additions over standard care practices?
RQ 2: What are the long-term impacts on clinical outcomes and psychological well-being indicators when tools involving predictive modeling of large datasets, social media analysis leveraging machine learning, passive data collection from smartphone sensors or conversational agents are incorporated into treatment over periods of 5 years or more?
RQ 3: How can minority voices and perspectives be respectfully included in the design, testing and refinement of data- driven mental healthcare technologies through community-based participatory approaches to ensure culturally appropriate interventions?
RQ 4: What policy frameworks and oversight guidelines need to be established to safeguard privacy and ethical use of personal health information in artificial intelligence and internet of things enabled mental health applications while still supporting innovation in digital biomarkers and personalized care paradigms?
1.8. Aims and Objectives
The overarching aim of this study is to explore how fields like machine learning, big data analytics, artificial intelligence and the internet of things can be leveraged to improve mental healthcare delivery and patient outcomes.
The specific objectives are:
- To analyze how predictive modeling using machine learning can help detect early signs of deteriorating mental health.
- To evaluate ways of mining social media and internet data to understand population-level trends and behavior patterns related to mental illnesses.
- To assess current applications and challenges of data-driven technologies in mental healthcare.
- Examine the potential of smartphone sensors and JITAI for real-time symptom monitoring, identification of high-risk situations and delivery of timely interventions.
- Understand ethical challenges around data privacy, algorithmic bias and informed consent in mental health applications.
2. Literature Review on Data-Driven Approaches to Tackling Mental Health
2.1. Predictive Modelling Using Machine Learning
Applying machine learning techniques proves useful in the field of mental healthcare, more precisely in the process of predictive modelling. Many of the above cited studies have used supervised algorithms such as logistic regression, decision trees, random forest, deep neutral networks for developing digital biomarkers for activities like automatic diagnosis, assessment of severity, relapse prediction, monitoring of response to treatment and prediction of suicide risks (Joshi et al., 2018; Ray et al., 2019; Fulmer et al., 2018; Saeb et al., For instance, Joshi et al. (2018) worked on deep learning models to extract features from the speeches of patients to categorize them into mentally healthy and clinically depressed. Based on an electroencephalogram signal, Ray et al. (2019) developed a multi-level attention network incorporating a text, audio and video feature for depression level prediction.
In another study, Saeb et al. (2015) compared clinical, experience sampling method and sensor-based assessments of depression and found that machine learning models can recognize changes in smartphone usage, physical activity and location patterns indicative of upcoming depressive episodes weeks in advance. Wang et al. (2018) similarly analyzed digital phenotyping data from passively collected smartphone sensors to predict symptom trajectories in schizophrenia patients. Unsupervised methods have also been explored, like in Canzian and Musolesi (2015) which leveraged mobility traces to detect depressive states in individuals by recognizing changes from their usual behavior patterns. Such techniques hold promise for continuous remote monitoring outside clinical settings.
Key elements in designing data-driven architectures for mental healthcare involve collecting multimodal data from electronic health records, devices, digital activities while addressing issues like data privacy, heterogeneity and ensuring interoperability as seen the above Figure 1 (Plaza et al., 2018). Standards are required for data sharing across systems and semantic interoperability between domain ontologies. Portable personal health records allow patients to own health data and consent to sharing. Distributed storage and edge computing close to data sources improve scalability and latency. Security and privacy-preserving techniques protect sensitive information.
2.2. Predictive Modeling for Early Detection
Machine learning models have demonstrated potential for early detection of deteriorating mental health by analyzing diverse behavioral data sources. Joshi et al. (2018) developed deep learning models to extract features from speech samples and classify individuals as normal or experiencing depression, anxiety or stress-related conditions with up to 78% accuracy. Ray et al. (2019) achieved 74% prediction of depression severity levels incorporating text, audio and video features using a multi-level attention network. Wang et al. (2018) found variance in smartphone usage, location visits and activity patterns over time predicted upcoming depressive episode risk in individuals with schizophrenia. Liu et al. (2022) constructed a machine learning risk prediction model leveraging medical, demographic and socioeconomic factors achieving 86.5% accuracy for post-traumatic stress disorder during the COVID-19 pandemic.
Several studies have mined longitudinal social media data to detect early signs of mental health issues. Nguyen et al. (2018) jointly predicted affective and mental health scores from visual cues on Facebook profiles using deep neural networks. Dao et al. (2016) analyzed emotion, language style and discussion topics within an online depression forum finding social capital factors associated with symptoms. Thorstad and Wolff (2019) applied natural language processing and machine learning techniques to predict future mental illness from Twitter language patterns up to 6 months in advance.
2.3. Data-Driven Architecture for Integrated Care
Plaza et al. (2018) conducted a systematic literature review of software architectures for integrating cyber-physical systems in healthcare contexts. One proposed architecture was an adaptive data-driven mental health care system consisting of user, security and scalable service layers (Kaur et al., 2018; Meena and Gorripatti, 2021). The user layer would facilitate functions such as epidemiological analysis, assessment/treatment tools, counseling/patient interactions, trend/fraud analytics and report and data visualization. The security layer would implement measures like role-based access control, data anonymization, mental health regulatory compliance, multifactor authentication, audit logs and monitoring and fraud analytics. Key capabilities of the scalable service layer would involve auto-scaling infrastructure, geo-proximity routing, data sharding, API Integration, interoperability standards and platform agonistic compatibility.
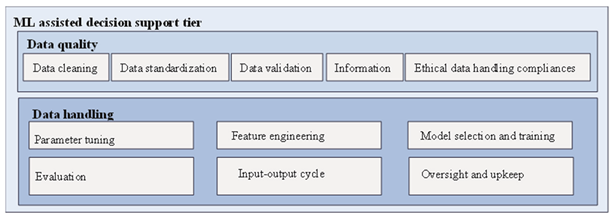
Such an architecture could facilitate population level mental health monitoring and deliver individualised, sustained care. It is described about the layer and capability further in the Table 1. The user layer would enable the public health agency to do its epidemiological research to determine who among the populace requires the treatment most and to offer the treatment most appropriately. Diagnoses and assessment and treatment tools being available through this layer might help to standardize the results and provide a framework for individualised care plans. Counselors could use the patient interact function for teleconsulting and online therapy as part of remote practice. Analysis of trends in this layer may be useful to identify the people who started, or whose conditions got worse, and required their attention.
The security layer would protect the patient’s identifications and information by applying role-based access control only permitting access where necessary. Tokenization and hashing are some of the anonymization practices that may render the information as off-identicality for further research analysis. They indicated that compliance with mental health regulations would be checked by this layer. There are also features like the multifactor authentication and the audit logs and monitoring which are continuous to ensure that there is no breach or anyone tries to gain unauthorized access into the system. On this layer, for instance, fraud analytics could detect fake insurance claims or an individual’s illness.
The application of digital solutions based on the integrated information systems has a potential in tackling some of the most critical issues in the sphere of mental health. In this way, the proposed population-level surveillance, early detection of developing crises, standardization of mental health treatment, and maintenance of its continuity can contribute to the reduction of the mental treatment gap and the effective assistance for the people dealing with their mental health issues. Nevertheless, ideas of privacy, justice and possible aggravation of the digital divide should be taken into consideration to sort out the using of these technologies was fair and did not harm any sensitive groups of the population.
2.4. Social Media and Internet Data Exploration
Another opportunity for the population—level monitoring of the state of mental health with an understanding of the individual risk is the analysis of posts on social networks. Web forum data in which Nguyen et al. (2018) created corresponding deep learning models combining textual, visual and linguistic features for estimating levels of depression, anxiety, and stress of the users. Likewise, in the wake of COVID-19, Liu et al. (2022) extracted text from social media to create a machine learning model of people at high risk of developing post-traumatic stress disorder with linguistically indicative high-risk speech.
Some other works have focused on the linguistic features and the topics that are under discussion within the online support groups for conditions. De Choudhury et al. (2013) looked at use of language on Reddit in order to identify users with higher risks of depression and Dao et al. (2016) examined how use of social capital affects the content and usage of emotions in online depression related communities. Supervised classifiers were used by Aggarwal et al. (2020) to the player profiles and gameplay data from Player Unknown’s Battlegrounds and or to identify a disposition to psychological disorders amongst American users. New insights of research therefore suggest possibilities of passive observation through social networks and selective engagement.
2.5. Smartphone Sensing for Just-In-Time Adaptive Interventions
Smartphones are in many ways always present, particularly in light of normal routines, which makes it possible to constantly collect behavioural signals and context using built-in and connected sensors. Some early conceptual studies have looked at their capacity to support just-in-time adaptive interventions (JITAIs) for mental health. For example, Wahle et al. (2016) pilot trial involved the use of smartphone usage, activity, location and sleep patterns acquired through an app to identify changes that might signal relapse into a depressive episode and in turn provide the patient with relevant supportive messages.
In a related study by Canzian and Musolesi (2015) the researchers used the patient’s geographical location and time spent at a place and distance travelled obtained from their smart phone GPS to determine mobility changes related to depression states. In a study done by Berrouiguet et al. in 2019, he was able to identify and develop a Smartphone Based Protocol involving mobility level tracking, call detail records and the application usage with preventions of suicidal attempts through risk models. It is potentially valuable to explore how an individual’s setting and smartphone-sensed phenotyping can present opportunities for at-the-moment, context-based interventions . Other issues that must be discussed are privacy issues, informed consent and clinician incorporation.
2.6. Chatbots and Conversational Agents
Recent work has explored using of chatbots and conversational agents for enhanced delivery of mental health services. In particular, Househ et al. (2019) suggested the evolutionary approach to creating the mental health chatbot using the decision trees, fuzzy logic and the domain knowledge graphs. In the same way, Suganuma et al. (2018) developed an ECCA available on the web for CIM for unguided WEB-based CBT in preventative mental health.
Other studies have cantered chatbots around guided self-help. For instance, Mukhiya et al. (2022) developed and validated a reference software architecture for internet-delivered, data-driven and adaptive psychological treatment systems incorporating conversational interfaces. Fulmer et al. (2018) evaluated a chatbot named ‘Woebot’ in a randomized trial, finding it helped relieve symptoms of depression and anxiety comparable to traditional CBT books. While promising, barriers around clinical safety, oversight, effectiveness and long-term impacts need addressing before full integration into care workflows.
3. Materials and Methods
3.1. Literature Search
A comprehensive literature search was conducted to evaluate prior research exploring application of digital technologies for mental healthcare delivery between 2011-2023. Four relevant electronic databases—PubMed, Embase, Web of Science and IEEE Xplore Digital Library—were searched between May-July 2023 using combinations of keywords like “mental health”, “digital tools”, “machine learning”, “big data”, “smartphones”, “social media”, “predictive modeling”, “eHealth” etc. Additional studies were identified through snowball sampling of relevant article references.
3.2. Inclusion and Exclusion Criteria
Only peer-reviewed articles published in English language between 2011-2023 were included in order to focus on state- of-the-art research incorporating latest technological advancements. Articles cross-listed across multiple databases were de-duplicated. Studies applying quantitative and qualitative research methodologies investigating use of technologies like supervised/unsupervised machine learning algorithms, mobile/wearable sensors, social media analytics, chatbots/virtual agents etc. to address issues like diagnosis, symptom tracking, personalized interventions, stigma analysis etc. were included. Excluded were papers focusing exclusively on theoretical aspects without empirical validations, letters, opinions or grey literature.
3.3. Screening and Selection
All abstracts retrieved through database searches were screened independently by two reviewers to assess relevance based on inclusion-exclusion criteria. Following this, full texts of eligible abstracts were obtained and evaluated in detail.
Disagreements were discussed until consensus was achieved. A total of 68 studies were finally selected for review. Figure 2 depicts the PRISMA flowchart of this study selection process.
3.4. Data Extraction
A standardized format was used to extract data from included papers covering aspects like aim, population, methodology, key findings, outcomes, limitations and conclusions. Details captured included digital tools/techniques evaluated, type of mental health condition addressed, sample size and characteristics, prediction tasks, performance metrics and clinical relevance of results.
3.5. Data Synthesis
A descriptive qualitative synthesis approach was employed to analyze, compare and map key themes emerging from the structured data. Subsequently, methodologies and results sections across studies were examined to identify commonly demonstrated applications of various data-driven technologies and their evaluated impact on different steps of mental healthcare processes. Benefits, drawbacks and gaps requiring further research attention were also noted.
4. Results and Discussions
4.1. Predictive Modelling for Early Detection
Multiple works have shown the ability of machine learning models for spotting signs of decline of an individual’s mental wellbeing (Joshi, Pawar, Dadasih, & Ray, 2018; Ray, Baptista, & Wang, 2019; Wang, Joshi, Boydell, Alvarado, & Power, 2018). Deep learning models were created by Joshi et al. (2018) with the combining of speech and language for classifying the people normal and those with some conditions like depression, anxiety or stress with accuracy of up to 78 percent. Multi-modal features from text, audio and video which Ray et al. (2019) used gave 74% prediction accuracy on depression severity levels. In Wang et al. (2018), the authors utilized subjects’ passively gathered smartphone data to identify that variance in them may predict the subsequent depressive episodes weeks beforehand in people with schizophrenia. This suggests that digital instruments can identify such signs of the worsening of symptoms as mild changes in behaviour.
Research has also relied on data from social media and the internet to search for indicators. By studying affective state, language type, and topics of discussion of user in online mental health discussion forums, it is possible to forecast changes in symptoms (Nguyen et al., 2018; Dao et al., 2016). Similarly, Thorstad and Wolff (2019) in their study, which involves subjecting de-identified materials from actual live twitter posts, found that NL processors were capable of pre- identifying a condition’s likelihood of being diagnosed up to 180 days in advance. In the COVID-19 case, using the features from the medical, demographic, and socioeconomic domains in a machine learning model, Liu et al. (2022) attained a sensitivity of 86. In post-traumatic stress disorder risk prediction has been found to be accurate to 5%. Such applications underpin population surveillance and outreach possibilities.
Nevertheless, quite a number of predictive models have been developed and validated using limited subsets of data from controlled research provenance instead of actual clinical scenarios (Aggarwal & Girdhar, 2022). Even more so, randomized trials have been conducted before any given treatment became popular; future studies conduct ought to feature diverse, extended, and representative samples to generalize effects and to take into consideration powerful variables such as the mental health state comorbidities, external effects of treatment interventions, and effects from a long-term perspective (Berrouiguet et al., 2019). Some concerns such as the ‘Bias and fairness’ issues that stems from having training datasets that have a biased representation of certain demographic groups to also be solved as the use of AI will only aggravate existing healthcare bias.
4.1.1. Smartphone Sensing for Symptom Monitoring
In concordance with objective 4, some research have utilised passive data collection with features available in the smartphone sensors to allow for continuous symptom tracking (Canzian & Musolesi, 2015; Wang et al., 2018). Through quantitative analysis of alterations in mobility patterns as well as the frequency of location visits and physical activity levels extracted from device logs over time it was possible for researchers to detect patterns which could indicate the emergence of the next depressive episode in patients with different conditions (Canzian & Musolesi, 2015; Wang et al., 2018). This kind of detection format supports the timely interventions’ delivery.
Other than identification, studies like Saeb et al. (2015) have contrasted clinical, experience sampling, and sensor- based emergent measures to identify that digital interventions added more validity for depression course when added to traditional quantitative monitoring. In light of objective 1, the results suggest additional and superior adjunct symptom tracking through omnipresent sensors. However, there is the problem with data collection through sensors which has privacy concerns that should be well spelt out in policy with appropriate consent from the patients following Gooding (2018). More follow-up assessment is still required to promote tools become user integrated into everyday use.
To support further objective 4, there is still need for more elaborate ‘wild’ trials to prove practicality and efficacy of sensor-triggered, JIT AI interventions in the long-term (Wahle et al., 2016). Such assistance should therefore assess whether it results in better symptom severity and relapse prevention in contrast to conventional care. Again, potential negative side effects of a heavy dependency on technology over long periods also need examination to enhance human support systems and ranks (Berrouiguet et al., 2019).
Whereas, the first set of studies offer the proof of concept for the use of smartphone sensing applications relating to objectives 1 and 4, further research involving the deployment of tools among general population under supervision i.e., in relation to objective 2 is important to systematically determine the benefits, risks and best practices to be recommended before further dissemination of the concept. Ongoing collaborations with the communities concerned will enhance the more protective ethical principles and the reality of the digital mental health care services.
4.1.2. Social Media Analytics for Population Monitoring
Regarding objective 2, works using social media data mining conducted population-level analysis on the SNSP of mental illnesses (Li et al., 2018; Zhou et al., 2015). Some of the findings included stigma and help seeking behaviours that existed among various groups of the population (Li et al., 2018). Some assessed emotion valence and topic in online support groups, and reported that there were linguistic features related to symptoms’ severity (Dao et al., 2016). They enabled the researcher to grasp macrosystems’ impacts on the condition.
Nonetheless, the current social media research designs continue to marginalise the owners of minority voices (Gooding & Kariotis, 2021). It’s critical to cover different demographics and contexts equally as per objective 3 in order to comprise all parts of population. Furthermore, the episodic and evidently performative nature of social media posts suggests that findings cannot replace clinical evaluations—rather, they are brief, digital signs that must be read alongside more ‘conventional’ ones. Controlling surveillance also raises questions of informed consent and privacy violation similar to objective 4 if bodies’ population data is not for positive uses, but to turn them into ‘ wielding commercial power as surveillance instruments’ (Wilton, 2017). Graduating community-involved participatory approaches wherein people embrace research intentions and are perceptive co-research partners could remove these difficulties.
Thus, the objectives 1, 2, 4 in the context of exploratory study fulfilled macro level outline goals; however, to provide methodologically sound and more balanced view of the cultural context prior to ‘final’ decision, additional sequential objective 3-principled participatory analysis is required. Integrated with more conventional epidemiological information, social media may enhance responsivity if privateness and equality are preserved by strictly governed, morally sound, crowd-sourced popu-lation knowledge-generation mechanisms.
4.2. Integration within Clinical Services
Concerning tools that can demonstrate additional utility beyond business , as defined in objective 1 and research question 1, several papers examined approaches of incorporating digital solutions into provider practice . Some of these include applying conversational agents as well as chatbots to increase access to and availability of PSS through natural language interactions (Househ et al., 2019). Some suggested blending the tele and face-to-face counseling through mobile applications for the between session activities (Francillette et al., 2018).
However, integration success also requires the study of clinicians and guarantee that new digital additions do not add unnecessary complexity and useless additions (Paes et al., 2021). As with integrating the old tools into new tools through adapted interfaces and information sharing mechanisms it is equally essential to function cohesively within active environments (Tummers et al., 2021). Although some advancement has been made to address the first objective, the roles described under the second objective in considering long-term organisational impacts on major effectiveness indicators such as symptom improvement or relapse whenever digital for mental health supplements the traditional care models for different groups of patients in actual practice settings over years remains under-addressed. This will provide the framework of scalability and address lengthy or over technical issues in order to integrate learnings.
4.3. Policy Frameworks and Ethical Considerations
Refreeing and equalizing of innovation, privacy, and oversight is critical for wide-scale safe deployment of AI and IoT technologies in mental healthcare regarding objective 4 and RQ4. Studies have started proposing models for incorporated accounting of data with ad hoc storage, edge computing and privacy-preserving access control and encryption for the personal data (Plaza et al., 2018; Kaur et al., 2018). Nevertheless, there are still questions left unrevealed about how to make a system fair if the trained algorithm is potentially signed with biased data and solutions for situations when AI explanations are contrary to the human experience (Gooding & Kariotis, 2021). Participatory design for communities’ promises to address such ‘dilemmas’ regarding minority perspectives as per objective three.
Assumptions also need reinforcement to common law systems of informed consent for digital application that gather extensive behavioral data beyond what consumers are aware of on tracking. Using accountability and redressal in cases of harm are problems that are as yet unresolved that jurisdictions need to solve preventively (Gooding & Kariotis, 2021). Earlier, recommendations from works aligned with objective 4 have provided parts of the groundwork for such discussions; however, continual future-oriented multisectoral dialogues that incorporate both technological and sociocultural insights needs to be made to futures proof exhaustive, dynamic governance frameworks that would harmonize progress with the protection of value as best as can be understood according to continuously updated knowledge. If difficulties are resolved collectively among researchers, policymakers, and public interests, they can establish standards that may allow fair, trustworthy digital mental health care.
4.4. Challenges to Clinical Integration
Some of which still limit digital tools clinical uptake performance as outlined in RQ1 and objective 1 as follows. New technologies are incompatible with established EHR systems reducing their easy usage (Tummers et al., 2021). The following are some of the challenges that are associated with the implementation of a production schedule by a business:
4.4.1. Interoperability and Integration Challenges
In particular, RQ1 reveals an importance of the integration of instruments for the use in clinical services. However, integration of new digital innovations with the existing electronic health record (EHR) systems that are commonly used in clinical practice nowadays is not fully optimized to be used in treatment processes. Existing solutions include formats and definitions of key data elements such as the symptoms, diagnoses and outcomes varied from one platform to another thus resulting in the formation of separate data silos. It also makes it difficult to bring together unified views from across standards care and technologies for making integrated decisions. Though, consortia work to formulate standard interface protocols, wider EHR adoption of the produced protocols is still in a premature phase. Moreover, the task of technology update and identifying technical integration problems is presented while new administrative challenges which practitioners exposed to workload issues do not want to take on. Addressing such interoperability challenges through cross-sector collaborations focused on BC and low Interop disruption will enhance value propositions as per RQ1 that defines value propositions as demonstrating superiority over extant paradigms before the expansion of existing networks.
4.4.2. Usability and Acceptability Challenges
From the analysed findings, it has emerged that tools introducing new practices must be able to showcase usability in clinical settings to respond to RQ1 and RQ2 according to Tummers and others (2021). First studies barely cope with addressing the characteristics of time constraints of clinicians’ tasks. Thieme et al. ‘s (2020) systematic review pointed out lack of designs that diminish the tools’ perceived relevance and acceptability to the end users. If digital additions are not incorporated in a natural way in direct communication, where it’s also possible to assess and plan treatment and follow up according to evidence based protocols, the clinicians may be challenged by feeling of getting more workload of documentation (Paes et al., 2021). Only long-term deployment studies validating tools’ effects on essential results such as client satisfaction, adherence and condition markers per RQ2 with embedded sequential user-centered design are lacking. While allocating integrated care models according to clinicians’ expertise, it is equally essential to empirically cultivate the continued proof of ease-of-use, perceived usefulness and compatibility with the priorities of clinical practice.
4.4.3. Technology Adoption Barriers
Aside from usability, RQ1 and RQ3 indicate that the adoption of technology within practitioners and their clients would also depend on the solution of the following socio-organizational barriers. First-line workers need to be trained on how to use new features, while it takes organisational culture change to proceed from face-to-face interactions to technology- enabled care delivery modes, inherited in legacy thinking (Tummers et al., 2021). Based on public points of view, the digital applications need to improve instead of deteriorating the trust-based therapeutic relationships to expend endorsement (Wilton, 2017). Some ethnic minorities may consider that such changes make it possible for culturally- sensitive relational dimensions of care identified in their cultures per RQ3 to be less of an emphasis. Breaking down these barriers and ensuring that the sensitively and tactfully integrate innovation into care models which respect users’ fundamental ways of understanding the world requires an extended amount of co-design with the users (Gooding & Kariotis, 2021). The justification of multiple perspectives of stakeholders will enhance the support structures that can bring embodied technological as well as humanized care.
4.4.4. Ensuring Appropriate Human Oversight
Concerning the RQ4, patient privacy, safety and satisfaction, technologies must operate under appropriate clinical governance models retaining crucial interpersonal aspects in treatment. Digitised automatic diagnosis or adaptive treatment features present legal and ethical issues most systems today do not possess solutions to. More structured use cases that involve the integration of the technologies but with periodic check and follow up by practitioners are less invasive of personhood. Though, at present, the shortage of specialized mental healthcare providers and particularly its deficit in the regions with limited access to healthcare in contact with inhabitants may prevent the provision of sufficient oversight at scale. Appropriate means for increasing access will have to be chosen in such manner not to overstep the capabilities of humans and not to eliminate close and warm interpersonal communication essential for recovery. To meet RQ2, and to mitigate the chance of exacerbating clinician burnout and opening new inefficiencies within the clinician’s work, periodic assessments valuing tools’ impacts on clinician workloads, burn out and quality of care provided are advisable.
4.5. Innovation through Multidisciplinary Partnerships
To cater needs that are as unique as the people that are served requires integration of professionals from different fields. Clinicians insist that technologists need help in defining what issues are considered a priority and what factors might pose obstacles. The communities in turn require the researchers to seek their advisory on the approach that will be more effective and culturally sensitive. The goal of public policy of protecting rights while furthering innovations hence requires identity of all the stakeholders. Through options as such as combined working groups, specialized task forces, and co-design studios, synergistic solutions even to S, E, and T problems in an integrated approach can be found. Such dualist ‘vs’ attitudes are then replaced by solidarity ‘and’ attitudes that appreciate everyone’s efforts. For example, computational psychiatrists that worked with medical anthropologists and civic authorities designed culturally sensitive ways of assessment of symptoms that are meaningful in different cultural contexts. The synergistic processes that promise to address adoption difficulties through bottom-up practices championed by other members of the society.
4.6. Legal and Ethical Considerations
Of course, with increased data means there is power to monitor population characteristics, find vulnerable groups and implement interventions ahead of time. At national scales, keywords, social media and telehealth analytics can approximate within realtime and geographic distribution of a disorder i. e. depression with reference to certain seasons or events. On the local level, passive data collected at the village level by citizens’ permission via their smart phones or IoT devices gives timely alarm/buzzer notifications where citizens may intervene to avoid an incidence of escalation. Indeed, with such aspects as the warning signs during crises and development monitoring, behavioural data science provides a perspective that might be hard to get with other methods. However, benefits are predicated on decentralised storage following privacy, shared access & social controls for data being utilised solely for the betterment of society withou If the safety measures are balanced with the participation designs, the digital tools can enable epidemiology to supplement the mental healthcare’s systemic issues across the globe.
In closing it becomes clear that there is still much progress needed across a number of intersecting technological and humanistic domains if the best of the two approaches to mental healthcare is to be achieved. Two of the first uses that provide early evidence of potential showed that existing tools can indeed help achieve certain learning objectives in relatively contained experiments Next steps filling in more evaluative proofs, assessment of the tools’ sustained efficacy over time, user friendly features, feasibility of the solutions being implemented on a larger scale, and directions for policy setting are critical. Thus, such evidence can arise only from solid, real-world evaluations working in a manner that respects the end users throughout the entire innovation process. Prolonged and cross-sector interdisciplinary collaboration the leads to culturally centered, community engaging design advancements will positively shape the future of digital psychiatry in bringing about better and improved equitable population mental health solutions across the globe. As long as those with different backgrounds continue to feel that they can participate in determining how these alterations enable technology and people to increase the availability of technology and ensure that humans remain at the heart of care it is seen as an enhancement rather than a substitution for selected care aspects within systems that support all people’s psychosocial requirements.
4.7. Future Directions
Although first forays into the topic identified possibilities for applying data science to advance complementary mental health care paradigms, the present work’s research questions 1 through 4 requires additional data. High-quality prospective studies conducted from the minority’s viewpoint per RQ3 and deployed under clinical governance as per RQ4 are still required to systematically evaluate tools’ validity, efficacy, equity, cost-effectiveness, requirement for oversight, and risks that emerge over a long time in realistic operating environments to address RQ2. Defining criteria for assessment that may be well understood by different approvers from multiple disciplines may add to comparability and progress. Further responsible development putting emphasis on the community relations, the synergy with the principles of openness and harmoniously integrated oversight, shall remain crucial to translating the potentials of the multipotential, digitally delivered psychiatry services to the claims of the RQ1 and the RQ2 with the focus on the enhanced value, outcomes and patient experience within the guaranteed rights and well being agenda on the line with the vision of the long-term complementary perspective of the digitally delivered
5. Conclusion
Therefore, it is opinionated that with increasing emphasis on digital psychiatry, there is scope to enhance the delivery of mental health care, however, to achieve this potential it is important that the field remains systematic as well as collaborative. Sustained and comprehensive assessment using diverse and realistic settings provides clinical credibility to the interventions and stakeholders’ confidence in the long run. However, technological competence is still waiting for further improvements in its scope to fit well within humanistic care paradigms. From policy perceptive, anticipatory measures prevent erosion of ethical advancement from inclusionary governance. In conclusion, a well-integrated model that is equally shared across diverse practitioners owns and supports evidence, implementation and advocacy of mental wellness for everyone. There are still issues lying ahead, but collaborations between research, practice, policy and communities also show that mental healthcare still has ways to improve and progress sustainably through synch technologies-social cofounding. Sustaining the discussion fosters altruistic, fair solutions to advance population well- being mentally in the present and the future.
Altogether, advanced information technologies offer new chances of reinforcement, outlining and intervention if only they are created more or less responsibly in regard of human values and evidence. To move from early practice to broad implementation, perseverance on elements such as clinical utility and validity, integration of social and technical aspects of the digital environment, minority inclusion, data privacy and governance, as well as preparedness of the workforce will require strong multisectoral efforts in the future. Ordinary work combined efforts applying science responsibly and empowering communities and overcoming barriers have potential to support humanity’s shared aim of mental health for all.
References
- Aggarwal R, Girdhar N. 2022. Machine learning role in cognitive mental health analysis amid Covid-19 crisis: a critical study. In: 2022 International Conference on Machine Learning, Big Data, Cloud and Parallel Computing, COM-IT-CON 2022.
- Aggarwal, S., Saluja, S., Gambhir, V., Gupta, S., & Satia, S. P. S. (2020). Predicting likelihood of psychological disorders in PlayerUnknown’s Battlegrounds (PUBG) players from Asian countries using supervised machine learning. Addictive Behaviors, 101, 106132.
- Aldabbas H, Albashish D, Khatatneh K, Amin R. 2022. An architecture of IoT-aware healthcare smart system by leveraging machine learning. International Arab Journal of Information Technology 19(2):160–172. [CrossRef]
- Berrouiguet, S., Barrigón, M. L., Castroman, J. L., Courtet, P., Artés-Rodríguez, A., & Baca-García, E. (2019). Combining mobile-health (mHealth) and artificial intelligence (AI) methods to avoid suicide attempts: the Smartcrises study protocol. BMC Psychiatry, 19(1), 277.
- Canzian, L., & Musolesi, M. (2015). Trajectories of depression: Unobtrusive monitoring of depressive states by means of smartphone mobility traces analysis. In Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing (pp. 1293-1304).
- Chawla, N. V., & Davis, D. A. (2013). Bringing big data to personalized healthcare: A patient-cantered framework.
- Journal of General Internal Medicine, 28(Suppl 3), S660-S665.
- Dao, B., Nguyen, T., Venkatesh, S., & Phung, D. (2016). Effect of social capital on emotion, language style and latent topics in online depression community. In Proceedings of the IEEE RIVF International Conference on Computing & Communication Technologies, Research, Innovation, and Vision for the Future (RIVF) (pp. 61-66). Hanoi, Vietnam. [CrossRef]
- De Choudhury, M., Counts, S., & Horvitz, E. (2013). Social media as a measurement tool of depression in populations. In Proceedings of the 5th Annual ACM Web Science Conference (pp. 47-56).
- Dias, L., & Barbosa, J. (2019). Towards a ubiquitous care model for patients with anxiety disorders. In Proceedings of the 25th Brazillian Symposium on Multimedia and the Web (pp. 141-144).
- Ferrario, M. A., Simm, W., Gradinar, A., Forshaw, S., Smith, M. T., Lee, T., Smith, I., & Whittle, J. (2017). Computing and mental health: intentionality and reflection at the click of a button. In Proceedings of the 11th EAI International Conference on Pervasive Computing Technologies for Healthcare (pp. 1-10).
- Francillette, Y., Bouchard, B., Boucher, E., Gaboury, S., Bernard, P., Romain, A. J., & Fournier, M. (2018). Development of an exergame on mobile phones to increase physical activity for adults with severe mental illness. In Proceedings of the 11th PErvasive Technologies Related to Assistive Environments Conference (pp. 241-248).
- Fulmer, R., Joerin, A., Gentile, B., Lakerink, L., & Rauws, M. (2018). Using psychological artificial intelligence (Tess) to relieve symptoms of depression and anxiety: randomized controlled trial. JMIR Mental Health, 5(4), e64.
- Gooding P, Kariotis T. 2021. Ethics and law in research on algorithmic and data-driven technology in mental health care: scoping review. JMIR Mental Health 8(6):e24668. [CrossRef]
- Gooding, P. (2018). A New Era for Mental Health Law and Policy: Supported Decision-Making and the UN Convention on the Rights of Persons with Disabilities. Cambridge University Press.
- Househ, M., Schneider, J., Ahmad, K., Alam, T., Al-Thani, D., Siddig, M. A., Alhamad, M., Moo-Young, J., & Saddik, B. (2019). An evolutionary bootstrapping development approach for a mental health conversational agent. Studies in Health Technology and Informatics, 262, 228-231.
- Joshi, D., Makhija, M., Nabar, Y., Nehete, N., & Patwardhan, M. (2018). Mental health analysis using deep learning for feature extraction. In Proceedings of the ACM India Joint International Conference on Data Science and Management of Data (pp. 356-359). Goa, India. [CrossRef]
- Joshi, D., Makhija, M., Nabar, Y., Nehete, N., & Patwardhan, M. (2018). Mental health analysis using deep learning for feature extraction. In Proceedings of the ACM India Joint International Conference on Data Science and Management of Data (pp. 356-359). Goa, India. [CrossRef]
- Kaur P, Sharma M, Mittal M. 2018. Big data and machine learning based secure healthcare framework. Procedia Computer Science 132(3):1049–1059. [CrossRef]
- Kraemer, H. C., & Freedman, R. (2014). Computer AIDS for the diagnosis of anxiety and depression. The American Journal of Psychiatry, 171(2), 134-136.
- Lahti, A. C. (2016). Making progress toward individualized medicine in the treatment of psychosis. The American Journal of Psychiatry, 173(1), 5-7.
- Leech, N. L., & Onwuegbuzie, A. J. (2011). Beyond constant comparison qualitative data analysis: Using NVivo.
- School Psychology Quarterly, 26(1), 70-84. [CrossRef]
- Li, A., Jiao, D., & Zhu, T. (2018). Detecting depression stigma on social media: A linguistic analysis. Journal of Affective Disorders, 232, 358-362. [CrossRef]
- Liu Y, Xie Y-N, Li W-G, He X, He H-G, Chen L-B, Shen Q. 2022. A machine learning-based risk prediction model for post-traumatic stress disorder during the COVID-19 pandemic. Medicina 58(12):1704. [CrossRef]
- Ma-Kellams, C., Or, F., Baek, J. H., & Kawachi, I. (2015). Rethinking suicide surveillance. Clinical Psychological Science, 4(3), 480-484.
- Mandryk, R. L., & Birk, M. V. (2019). The potential of game-based digital biomarkers for modeling mental health.
- JMIR Mental Health, 6(4), e13485.
- Marks, M. (2020). Emergent medical data: health information inferred by artificial intelligence. U.C. Irvine Law Review, 11, 995.
- McMullen TL, Mandl SR, Pratt MJ, Van CD, Connor BA, Levitt AF. 2022. The IMPACT Act of 2014: standardizing patient assessment data to support care coordination, quality outcomes, and interoperability. Journal of the American Geriatrics Society 70(4):975–980. [CrossRef]
- Meena V, Gorripatti M, Praba TS. 2021. Trust enforced computational offloading for health care applications in fog computing. Wireless Personal Communications 119(2):1369–1386. [CrossRef]
- Meng, H., Huang, D., Wang, H., Yang, H., AI-Shuraifi, M., & Wang, Y. (2013). Depression recognition based on dynamic facial and vocal expression features using partial least square regression. In Proceedings of the 3rd ACM International Workshop on Audio/Visual Emotion Challenge (pp. 21-30).
- Midha S, Verma S, Kavita, Mittal M, Jhanjhi N, Masud M, A. AlZain M. 2023. A secure multi-factor authentication protocol for healthcare services using cloud-based SDN. CMCComputers Materials & Continua 74(2):3711–3726. [CrossRef]
- Mills, C., & Hilberg, E. (2018). The construction of mental health as a technological problem in India. Critical Public Health, 30(1), 41-52.
- Mukhiya SK, Lamo Y, Rabbi F. 2022. A reference architecture for data-driven and adaptive internet-delivered psychological treatment systems: software architecture development and validation study. JMIR Human Factors 9(2):e31029. [CrossRef]
- Murdoch, T. B., & Detsky, A. S. (2013). The inevitable application of big data to health care. The Journal of the American Medical Association, 309(13), 1351-1352.
- Newaz MT, Giggins H, Ranasinghe U. 2022. A critical analysis of risk factors and strategies to improve mental health issues of construction workers. Sustainability 14(20):13024. [CrossRef]
- Nguyen, H., Nguyen, V., Nguyen, T., Larsen, M., O’Dea, B., Nguyen, D., et al. (2018). Jointly predicting affective and mental health scores using deep neural networks of visual cues on the web. In Proceedings of the 19th International Conference on Web Information Systems Engineering—WISE 2018 (pp. 100-110). Dubai, United Arab Emirates. [CrossRef]
- Nithya B, Ilango V. 2017. Predictive analytics in health care using machine learning tools and techniques. In: 2017 International Conference on Intelligent Computing and Control Systems (Iciccs). 492–499.
- Paes MR, Silva AC, Kowalski ICD, Nimtz MA, da Silav OBM, Paes RG. 2021. Mental health in a general hospital: perception of the nursing team. Revista De Pesquisa-Cuidado E Fundamental Online 13:1460–1466. [CrossRef]
- Parekh, Ruchit, and Charles Smith. “Innovative AI-driven software for fire safety design: Implementation in vast open structure.” World Journal of Advanced Engineering Technology and Sciences 12.2 (2024): 741-750.
- Patel HB, Gandhi S. 2018. A review on big data analytics in healthcare using machine learning approaches. In: 2018 2nd International Conference on Trends in Electronics and Informatics (ICOEI).
- Parekh, Ruchit. “Comparison Analysis of Construction Costs according to LEED and non-LEED Certified Educational Buildings.” Journal of Emerging Technologies and Innovative Research 11 (2024): b410-b417.
- Plaza AM, Diaz J, Perez J. 2018. Software architectures for health care cyber-physical systems: a systematic literature review. Journal of Software-Evolution and Process 30(7):22. [CrossRef]
- Parekh, Ruchit. “Automating the design process for smart building technologies.” World Journal of Advanced Research and Reviews 23.2 (2024): 1213-1234.
- Ray, A., Kumar, S., Reddy, R., Mukherjee, P., & Garg, R. (2019). Multi-level attention network using text, audio and video for depression prediction. In Proceedings of the 9th International on Audio/Visual Emotion Challenge and Workshop (pp. 81-88).
- Saeb, S., Zhang, M., Kwasny, M., Karr, C. J., Kording, K., & Mohr, D. C. (2015). The relationship between clinical, momentary, and sensor-based assessment of depression. In Proceedings of the 9th International Conference on Pervasive Computing Technologies for Healthcare (pp. 229-232).
- Shatte, A. B., Hutchinson, D. M., & Teague, S. J. (2019). Machine learning in mental health: A scoping review of methods and applications. Psychological Medicine, 49(9), 1426-1448. [CrossRef]
- Suganuma, S., Sakamoto, D., & Shimoyama, H. (2018). An embodied conversational agent for unguided internet- based cognitive behavior therapy in preventative mental health: feasibility and acceptability pilot trial. JMIR Mental Health, 5(3), e10454.
- Swain S, Patra MR. 2022. Analysis of depression, anxiety, and stress chaos among children and adolescents using machine learning algorithms. In: Panda M, ed. Communications in Computer and Information Science. Vol. 1737. Cham: Springer.
- ai, A. M., Albuquerque, A., Carmona, N. E., Subramanieapillai, M., Cha, D. S., Sheko, M., Lee, Y., Mansur, R., & McIntyre, R. S. (2019). Machine learning and big data: implications for disease modeling and therapeutic discovery in psychiatry. Artificial Intelligence in Medicine, 99, 101704.
- Thieme A, Belgrave D, Doherty G. 2020. Machine learning in mental health: a systematic review of the HCI literature to support the development of effective and implementable ML systems. ACM Transactions on Computer-Human Interaction 27(5):34. [CrossRef]
- Thorstad, R., & Wolff, P. (2019). Predicting future mental illness from social media: A big-data approach. Behavior Research Methods, 51(4), 1586-1600. [CrossRef]
- Torous, J., & Baker, J. T. (2016). Why psychiatry needs data science and data science needs psychiatry: Connecting with technology. JAMA Psychiatry, 73(1), 3-4.
- Tuli, A., Singh, P., Sood, M., Deb, K. S., Jain, S., Jain, A., Wason, M., Chadda, R., & Verma, R. (2016). Harmony: close knitted mHealth assistance for patients, caregivers and doctors for managing SMIs. In Proceedings of the 2016 ACM International Joint Conference on Pervasive and Ubiquitous Computing: Adjunct (pp. 1144-1152).
- Tummers J, Tobi H, Catal C, Tekinerdogan B. 2021. Designing a reference architecture for health information systems. Bmc Medical Informatics and Decision Making 21. [CrossRef]
- Upadhyay S, Kumar M, Upadhyay A, Verma S, Kavita Kaur M, Abu Khurma R, Castillo PA. 2023. Challenges and limitation analysis of an IoT-dependent system for deployment in smart healthcare using communication standards features. Sensors 23. [CrossRef]
- Vaishali Narayanrao P, Lalitha Surya Kumari P. 2020. Analysis of machine learning algorithms for predicting depression. In: 2020 International Conference on Computer Science, Engineering and Applications, ICCSEA, Vol. C7, 9132963.
- van den Bergh D, Bogaerts S, Spreen M, Flohr R, Vandekerckhove J, Batchelder WH, Wagenmakers EJ. 2020. Cultural consensus theory for the evaluation of patients’ mental health scores in forensic psychiatric hospitals. Journal of Mathematical Psychology 98(1):102383. [CrossRef]
- Vinci ALT, Rijo RPCL, Marques JMdA, Alves D. 2016. Proposal of an evaluation model for mental health care networks using information technologies for its management. Procedia Computer Science 100:826–831. [CrossRef]
- Wahle, F., Kowatsch, T., Fleisch, E., Rufer, M., & Weidt, S. (2016). Mobile sensing and support for people with depression: A pilot trial in the wild. JMIR mHealth and uHealth, 4(3), e111.
- Wang, R., Wang, W., Aung, M. H., Ben-Zeev, D., Brian, R., Campbell, A. T., Choudhury, T., Hauser, M., Kane, J., Scherer.
- E. A., & Walsh, M. (2018). Predicting symptom trajectories of schizophrenia using mobile sensing. GetMobile: Mobile Computing and Communications, 22(2), 32-37.
- Weber, G. M., Mandl, K. D., & Kohane, I. S. (2014). Finding the missing link for big biomedical data. The Journal of the American Medical Association, 311(24), 2479-2480.
- Wilton R. 2017. Trust and ethical data handling in the healthcare context. Health and Technology 7(4):569–578. [CrossRef]
- World Health Organization. (2022). Mental disorders. Available at https://www.who.int/newsroom/fact- sheets/detail/mental-disorders.
- Wshah, S., Skalka, C., & Price, M. (2019). Predicting posttraumatic stress disorder risk: A machine learning approach. JMIR Mental Health, 6(7), e13946.
- Wu, P., Koh, J., & Chen, A. (2019). Event detection for exploring emotional upheavals of depressive people. In Proceedings of the 34th ACM/SIGAPP Symposium on Applied Computing (pp. 2086-2095). Limassol Cyprus. [CrossRef]
- Zhou, D., Luo, J., Silenzio, V., Zhou, Y., Hu, J., Currier, G., & Kautz, H. (2015). Tackling Mental Health by Integrating Unobtrusive Multimodal Sensing. In Proceedings of the Twenty-Ninth AAAI Conference on Artificial Intelligence (pp. 1401-1408).
- Zhou, T., Hu, G., & Wang, L. (2019). Psychological disorder identifying method based on emotion perception over social networks. International Journal of Environmental Research and Public Health, 16(6), 953. [CrossRef]
Figure 1.
KEPs for data-driven architecture.
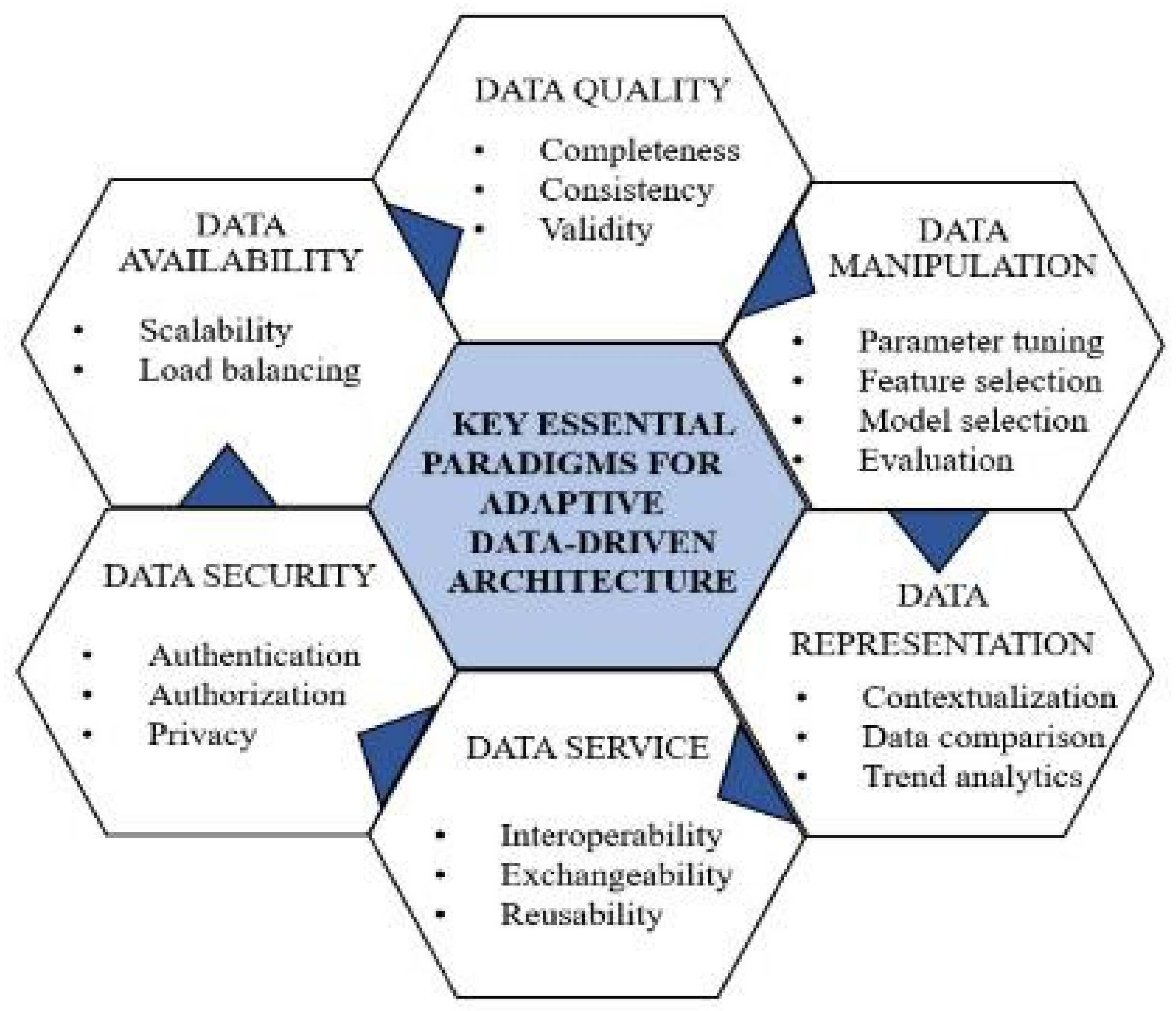
Figure 2.
PRISMA flow chart.
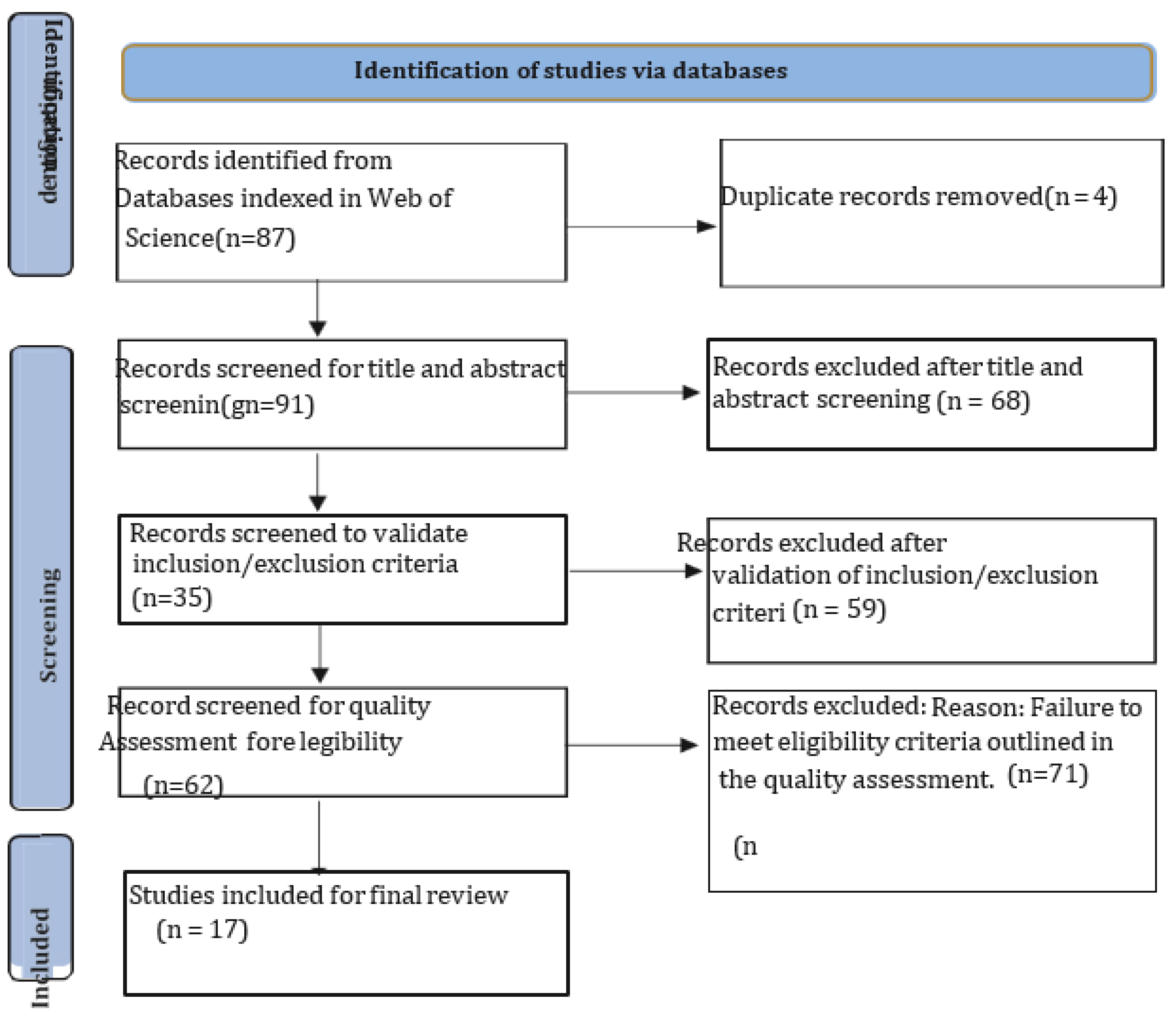

Table 1.
Responsive data-cantered mental wellness support framework.
| User layer | |||
|---|---|---|---|
| Public health organization epidemiological review | Evaluation and care instruments | Report and data visualization | |
| Therapist and client communication | Scheduling and referral | Trend analytics | |
| Protection tier | |||
| Permission-based entry regulation | Data anonymization | Mental health regulatory compliance | |
| Multifactor authentication | Audit logs and monitoring | Fraud analytics | |
| Scalable service layer | |||
| Auto-scaling infrastructure | Geo-proximity routing | Data sharding | |
| API Integration | Interoperability standards | Platform agonistic compatibility | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



