Submitted:
06 September 2024
Posted:
09 September 2024
You are already at the latest version
Abstract
Migraine is a neurological disorder characterized by severe disabling headaches with a substantial global burden and elevated morbidity rates. Extensive research has established a clear association between migraine and sex/gender, with a notably higher incidence reported in females, reaching up to 18%, which is three times greater compared to males. Additionally, women commonly experience more intense pain and greater frequency of migraine symptoms, both with and without aura, highlighting the differential impact of sex/gender on migraine presentation. This review comprehensively examines the pathophysiology of migraine, with a particular focus on the effects of sex hormones in migraine pathophysiology and the central nervous system. Furthermore, we explore various treatment modalities tailored to gender differences, including pharmacological interventions and emerging therapeutic approaches. Furthermore, we explored alternative treatment strategies such as nutraceuticals and behavioural techniques, including mindfulness and cognitive behavioural therapy. This review aims to provide a comprehensive overview of the multifaceted nature of migraine and the diverse therapeutic approaches available for their management.
Keywords:
Migraine
; sex hormones
; pathology
; treatment
Introduction
Migraine is an episodic neurological disorder, which can become chronic in later stages, characterized by severe disabling headaches with a strong genetic predisposition [1,2]. According to the Global Burden of Disease Study 2019, migraine ranked second in disability across all ages and genders, maintaining the highest rank among young women since 2019 [3]. Typical attacks involve unilateral moderate to severe headaches accompanied by nausea, vomiting, and sensitivity to light and sound [4,5]. Migraine is more prevalent in females, affecting them three times more than males, with an incidence rate as high as 18% [6,7,8]. The prevalence of migraine in women increases from puberty, affecting up to 55% during menstrual age, and varies with pregnancy and menopause [9,10,11]. This gender disparity is attributed to differences in sex hormone receptor binding, genetics, and environmental stressors [12,13,14]. While attack frequency is similar across genders, averaging 1 to 4 headache days per month, significant age-related differences are observed among women [15,16]. Studies suggest that women experience higher pain intensity due to longer attack durations and social constraints limiting men from expressing pain [17]. Additionally, women report higher frequencies of symptoms such as nausea, phonophobia, and photophobia [18]. Migraine recurrence is influenced by hormonal changes, including menarche, menstruation, pregnancy, menopause, and the use of contraceptives or hormone replacement therapy (HRT) [1,2,3].
The pathophysiology of migraine has advanced with functional neuroimaging and animal models yet remains incompletely defined. Migraine is characterized by recurrent unilateral throbbing headaches, often accompanied by nausea, photophobia, and phonophobia, leading to significant daily activity restriction [19] and pathophysiology is shown in Figure 1. Genetic, metabolic, environmental, and vascular factors contribute to migraine pathogenesis [20]. Historically, migraine has been recognized as a predominantly female condition. An episode of migraine may include four phases: premonitory, aura, headache, and postdrome, which can occur sequentially or overlap [21]. Initial theories by Thomas Willis in the 17th century proposed a neurovascular hypothesis, attributing migraine to carotid artery dilatation [22,23]. This shifted in the 18th century towards a neural hypothesis supported by neurologists like Edward Living and William Gowers [24]. The 20th century saw systematic research into migraine pathophysiology by neurologists such as Harold Wolff [24]. According to the International Classification of Headache Disorders, 3rd edition (ICHD-3), migraine with aura involves recurrent attacks of unilateral, fully reversible visual, sensory, or other CNS symptoms, usually followed by headache and other migraine symptoms [25,26,27]. The patterns of aura in migraine resemble cortical spreading depression (CSD), characterized by the progression of visual aura from the central visual field to the periphery, transient focal hyperemia followed by oligemia, and the effectiveness of ketamine in reducing aura intensity [28,29,30,31,32]. Moskowitz’s hypothesis links the aura and headache phases, emphasizing the role of the ophthalmic division of the trigeminal ganglion, which surrounds large blood vessels and dural venous sinuses [33,34,35,36]. Stimulation of these fibres releases substance P and calcitonin gene-related peptide (CGRP), causing vasodilation and contributing to migraine pathogenesis [35,36]. Trigeminal ganglion stimulation also induces mast cell degranulation and release of inflammatory mediators, highlighting the interplay between vascular and neuronal factors in migraine [35,36].
In summary, vascular changes are not sufficient alone to explain migraine; instead, increased neuronal sensitization to sterile inflammatory stimuli appears to be responsible for clinical features. The exact neural mechanisms and genetic predispositions remain unclear [33,34,35,36]. This review aims to explore the relationship of migraine with female gender and gender-specific treatments, including non-pharmacological approaches.
Impact of Sex Hormones in the Pathophysiology of Migraine
Migraines are often triggered by sensory and environmental stimuli such as bright lights, loud sounds, stress, exertion, irregular sleep, alcohol, or hormonal fluctuations [37,38]. This sensory sensitivity is due to dysfunctions in monoaminergic sensory control systems in the brainstem and hypothalamus, amplified in women during hormonal fluctuations of the menstrual cycle [37,38]. Estrogen and progesterone significantly impact brain function. In female migraineurs, migraines often begin at menarche, improve during pregnancy, and worsen during perimenopausal years, but generally improve after natural menopause [37,38,39]. Sixty per cent of female migraineurs report increased frequency during the perimenstrual period, correlated with abrupt falls in estrogen and progesterone levels [38,39]. Pavlović et al. compared sex hormone levels and rates of change between females with and without a history of migraine and reported that females with a history of migraine demonstrated a faster late luteal phase estrogen decline compared to controls. Migraine attacks increase during the perimenstrual period in approximately half of females who experience migraine. There are notable differences in the pathogenesis and clinical features of menstrually-related migraines compared to non-menstrual migraines [40]. Güven et al. reported that menstrually-related migraines last longer, and accompanying symptoms reported nausea, vomiting, phonophobia, headache aggravation with physical activity, premonitory symptoms, and allodynia are more frequent and diverse in patients with menstrually related migraine without aura, suggesting increased brain excitability or susceptibility in these patients [41].
Estrogen and progesterone also exert widespread effects on various neurotransmitter systems. In the central serotonergic system, estrogen enhances serotonin synthesis and receptor sensitivity, potentially stabilizing mood and mitigating pain [42,43]. Estrogen’s influence extends to the opioid system by increasing endogenous opioid activity, which helps modulate pain. It also impacts substance P receptor expression, a neuropeptide involved in pain pathways, potentially altering pain perception [44,45,46]. Estrogen boosts norepinephrine (NE) synthesis and release, which affects mood and alertness, while it enhances dopamine synthesis and receptor sensitivity, influencing mood and reward pathways [47,48].
Additionally, estrogen promotes endorphin release, contributing to pain relief and mood improvement [49]. It increases prolactin release, particularly during pregnancy and postpartum [49]. Estrogen also plays a crucial role in modulating calcitonin gene-related peptide (CGRP), a key player in migraine pathophysiology, by influencing its expression and release, which can promote vasodilation and neurogenic inflammation, potentially triggering migraines [50]. The International Classification of Headache Disorders, 2nd edition (ICHD-II), defines menstrual-related migraines as those occurring between -2 to +3 days of the menstrual cycle, whereas pure menstrual migraines occur only during these days [35]. Menstrual migraines are associated with estrogen withdrawal during the late luteal phase. Early studies demonstrated that estradiol supplementation delayed migraines until estrogen levels dropped to pretreatment levels [32]. Progesterone supplementation delayed bleeding but did not affect migraines, indicating that sudden estrogen withdrawal precipitates migraines [32]. Recent studies have shown faster declines in conjugated urinary estrogens (E1c) in female migraineurs compared to controls during the late luteal phase, supporting the role of estrogen withdrawal in migraine in the luteal phase [15,36]. During pregnancy, sustained high levels of estrogen and progesterone are maintained by the corpus luteum and placenta, leading to decreased migraine frequency [37,38]. However, most women report a return of migraines post-delivery. Conditions associated with declining estrogen levels, such as the late luteal phase, post-delivery, and hormone-free periods in contraceptive or HRT users, correlate with worsening migraines [50,51]. Conversely, natural menopause with gradual estrogen declines or sustained high estrogen levels during pregnancy significantly improves migraine attacks. Perimenopause, characterized by fluctuating ovarian hormones, often worsens migraine patterns [52,53,54].
The variability in migraine patterns due to hormonal changes remains unexplained for some women. Ovarian hormones influence migraine pathophysiology through activational effects on brain neurotransmitters [55,56,57]. Estrogen affects the brainstem and hypothalamus monoaminergic sensory control system, impacting serotonin and norepinephrine and impairing antinociceptive regulation. Estrogen also affects vasculature via increased nitric oxide activity, enhances neuronal excitability through glutaminergic system facilitation, and suppresses the GABAergic system. Cortical spreading depression (CSD), implicated in aura, relies heavily on glutaminergic transmission [58,59,60]. Combined oral contraceptives (COCs) stabilize hormonal fluctuations by providing consistent levels of estrogen and progestin. However, COCs have only demonstrated minor changes in the course of perimenstrual migraine in menstruating women with migraine [61]. Estro-progestin drugs in patients who use them may induce hyperinsulinism and hypoglycemia, thereby increasing the severity of migraines [62]. A systematic review reported that COC users with a history of migraine were 2-4 times more prone to an ischemic stroke than nonusers with a history of migraine [63]. Hormonal imbalances, including elevated androgens and irregular estrogen and progesterone levels, characterize polycystic ovary syndrome (PCOS). Hyperandrogenemia associated with PCOS may have a protective effect on migraine headaches; however, other manifestations and complications can exacerbate hormonal imbalances, thus inducing migraines. The association between PCOS and migraines may be partly explained by poor sleep quality in women with PCOS due to reduced REM sleep time [64]. There is conflicting evidence regarding the frequency of migraines after menopause. A meta-analysis reported that there may be an improvement in migraine after menopause, although there may be an increase in migraine frequency during perimenopause. Conversely, studies conducted on patients at headache centres often report no improvement or even worsening of migraines after menopause. The aetiology of menopause appears to influence the evolution of migraines during this period, with spontaneous menopause more likely to result in migraine improvement compared to surgical menopause [65]. Perimenopause is always marked by an increased prevalence of migraines in women, many of whom also experience vasomotor symptoms. Fluctuating estrogen levels influence migraines during this time, as estrogen withdrawal can trigger menstrual attacks of migraine without aura, and high estrogen levels can trigger migraine with aura [65]. Maintaining a stable estrogen environment through hormone replacement therapy can benefit women suffering from estrogen-withdrawal migraines and provide relief from vasomotor symptoms. For women with migraines, whether with or without aura, using the lowest effective doses of transdermal estrogen to control vasomotor symptoms helps minimize the risk of side effects. Cyclical progestogens can adversely affect migraines, so continuous progestogens, as provided by the levonorgestrel intrauterine system or continuous combined transdermal preparations, are preferred [66]. Vascular and neuronal effect is shown in Figure 2.
Physiology of the Female Hormonal Life Cycle
Estrogen and progesterone are crucial hormones for female health, influencing various organ systems, including the brain, throughout a woman’s life, from menarche to menopause [67]. They regulate the menstrual cycle, support pregnancy, and contribute to the development of secondary sexual characteristics. While estrogen and progesterone levels are high at birth, they decrease within months and remain low until puberty [68]. Puberty marks a significant increase in circulating sex hormones, primarily estrogen, which drives physical changes such as breast, vagina, uterus, and ovary development, as well as the onset of menstruation [69]. During the reproductive period, hormone levels fluctuate in a cyclical pattern over an average 28-day menstrual cycle, comprising the follicular and luteal phases, with each cycle starting on the first day of menstrual bleeding [70]. During menstruation, estrogen and progesterone levels are low. Estrogen gradually rises, peaking at the end of the follicular phase before a rapid decline just before ovulation due to luteinizing hormone (LH) surge. In the luteal phase, progesterone levels rise and plateau due to corpus luteum secretion, accompanied by a second rise in estrogen levels. In the absence of pregnancy, the corpus luteum degenerates, leading to decreased hormone levels and menstrual initiation [71]. This cycle repeats throughout the fertile period.
During pregnancy, estrogen and progesterone levels remain high and increase significantly, with the placenta maintaining their levels. They peak during the third trimester, around 32 weeks of gestation [72]. Postpartum delivery of the placenta reduces the levels of all placenta-produced hormones, leading to extremely low sex hormone levels comparable to menopause [73]. Perimenopause typically starts in the late forties, during which menstrual cycles become irregular due to a gradual decline in sex hormone levels [74]. Menopause is reached when a year passes after a woman’s last menstrual period, with low hormone levels causing physical, mental, and emotional issues [75]. These hormonal fluctuations throughout a woman’s life lead to significant physical and mental changes, increasing susceptibility to certain conditions, particularly affecting the brain and nervous system [76].
Effects of Sex Hormones on the Central Nervous System
In the brain, the effects of female sex hormones are broadly classified into organizational and activational categories. Organizational effects are long-lasting changes in brain structure, such as myelination and synapse strengthening, that permanently alter the brain’s architecture. Activational effects involve temporary changes in brain activity through modulation of neurotransmitters, significantly impacting brain function on a short-term basis. [36,39]. Estrogen and progesterone improve the brain’s resilience by upregulating enzymes that reduce free radicals, thereby minimizing oxidative stress. They also activate anti-apoptotic pathways that prevent cell death and promote the proliferation of neural cells, contributing to brain health and function. Progesterone specifically plays a crucial role in regulating neuronal myelination and glial cell activity, which is essential for maintaining the integrity and efficiency of neural networks. While estrogen and progesterone do not work synergistically, their combined effects are achieved during the natural hormonal fluctuations of the menstrual cycle. These fluctuations ensure that the protective and regulatory actions of these hormones are balanced, thus supporting both the structural and functional health of the brain throughout a woman’s reproductive years [36]
Effects on Neurotransmitter Systems
1. Effect on Nitric Oxide: Disturbances in nitric oxide (NO) signaling have been implicated in the initiation and progression of migraine attacks. Abnormalities in NO levels have been observed in various stages of migraine, including during the prodromal phase, aura, and headache phase. The vasodilatory effects of NO can lead to cerebral blood flow dysregulation, potentially contributing to migraine aura and headache [77]. Endogenous estrogen enhances NO production and bioavailability within the vasculature via upregulation and increased activity of endothelial Nitric Oxide Synthase (eNOS), an enzyme critical for NO synthesis. When combined with estrogen, progesterone or synthetic progestins help maintain high levels of eNOS. NO plays an important role in regulating the neuroplasticity of synapses, which contributes significantly to the neuroprotective functions of estrogen. By promoting NO production, estrogen supports vascular health and facilitates the adaptability and resilience of neural connections in the brain. [38,52].
2. Effect on Norepinephrine and Alpha Receptors: Estrogen’s influence on norepinephrine synthesis and breakdown is not fully defined. Estrogen infusion in ovariectomized rhesus macaques increased norepinephrine activity in the hypothalamus. The mechanism may involve estrogen’s influence on genes, enhancing norepinephrine activity. Estrogen treatment in rats upregulated alpha one receptors in the nucleus tractus solitaries (NTS), but mestranol treatment decreased alpha two receptors in the NTS and frontal cortex and both alpha one and alpha two receptors in the locus coeruleus. NE is involved in pain processing and modulation, and alterations in NE levels or receptor expression can influence migraine susceptibility and severity. Estrogen’s ability to increase NE activity in certain brain regions, such as the hypothalamus, may contribute to the onset or exacerbation of migraine. [40,51]
3. Effect on GABA: Estrogen and progesterone have complementary roles in modulating neurotransmission. Estrogen decreases GABA neurotransmission by inhibiting L-type calcium channels, leading to increased synaptic activity of glutamate and dopamine. This promotes excitatory neurotransmission, which can contribute to the onset and severity of migraines by enhancing neuronal excitability and cortical spreading depression, a wave of neuronal and glial depolarization associated with migraine aura. In contrast, progesterone promotes GABA activity by enhancing the activation of GABA-A receptors and increasing the function of GABA-mediated chloride channels, hyperpolarizing the cell membrane and inhibiting synaptic impulse transmission. The inhibitory effects of progesterone help stabilize neural activity, counterbalancing the excitatory effects of estrogen. During the menstrual cycle, the drop in estrogen levels just before menstruation can reduce its inhibitory effect on GABA neurotransmission, leading to increased neuronal excitability and the potential for migraine attacks. Conversely, the stabilizing effects of progesterone on GABA neurotransmission may offer some protective benefits against migraine triggers. [52,53].
4. Effect on Glutamate: Migraine pain-relay centres, such as the trigeminal ganglion, trigeminal nucleus caudalis, and thalamus, contain neurons that express glutamate that plays a key role in activating the trigeminal nucleus caudalis, a critical relay station involved in pain processing. Furthermore, glutamate is implicated in several migraine-related processes, including cortical spreading depression, trigeminovascular activation, and central sensitization, all of which contribute to the generation and propagation of migraine pain [78]. Estrogen increases glutamate release, upregulates NMDA receptor expression, and enhances receptor sensitivity, promoting neuron excitability, learning and memory. Progesterone inhibits glutamate transmission, release, and receptor sensitivity. Allopregnanolone inhibits glutamate release via L-type calcium channel inhibition on presynaptic neurons [52,53,54].
5. Effect on Dopamine: Estrogen upregulates dopaminergic receptors, increases dopamine synthesis, and reduces its breakdown and reuptake in synapses, influencing addiction, pleasure, rewards, motivation, and learning. Dopamine also plays a role in migraine pathophysiology, with most migraine features being inducible by dopaminergic stimulation. Migraineurs exhibit hypersensitivity to dopamine receptor agonists, experiencing migraine symptoms at doses ineffective in non-migraineurs. Dopamine receptor antagonists are effective in migraine treatment, particularly when combined with other anti-migraine agents [58,59].
6. Effect on Serotonin: Serotonin regulates mood, sleep, sexual behaviour, and cognitive functions, playing a role in psychiatric and neurological disorders, including migraine. Estrogen activates estrogen receptors in the trigeminovascular system, upregulating enzymes in serotonin production pathways like Tryptophan hydroxylase and downregulating enzymes in serotonin breakdown like Monoamine oxidase (MAO). Estrogen also increases the expression of 5HT1A, 1B, and 2A receptors and inhibits serotonin reuptake by presynaptic neurons. This leads to increased serotonin levels and activity in the trigeminovascular system, contributing to migraine pathogenesis. Serotonin and its receptors decrease following a fall in serum estrogen levels, leading to sensory control system dysfunction in the hypothalamus and brainstem (including the trigeminal nucleus), predisposing females to migraines [79].
7. Effect on CGRP: Calcitonin Gene-Related Peptide (CGRP) is a potent vasodilator primarily stored and secreted in sensory neurons, contributing to the pain pathway, particularly in migraine pathophysiology. Studies show that women in estrogen-deprived states (perimenopausal/post-late luteal estrogen peak) have higher plasma and urine CGRP concentrations. Conversely, replenishing estrogen in ovariectomized animals reduces plasma CGRP levels and CGRP receptor expression in the trigeminovascular system. The exact mechanism by which estrogen modulates CGRP levels remains unclear, but it is a basis for increased susceptibility to migraines and hot flashes, especially during perimenopause and the late luteal period. Notably, while many migraine patients experience reduced attacks post-menopause, those who have undergone surgical ovariectomy, often experience worsened migraine attacks due to the sudden fall in serum estradiol levels, unlike the gradual decline post-physiological menopause [34,35,36]. These activational effects of sex hormones on the central nervous system demonstrate the intricate modulation of neurotransmitter systems, highlighting the significant influence of estrogen and progesterone on brain function and behavior throughout a woman’s life cycle.
Management of Migraine
Migraine is characterized by sudden, severe headaches that occur recurrently, significantly impacting an individual’s quality of life and imposing a substantial socioeconomic burden on society [80]. Diagnosis relies heavily on the accuracy of history taking, which is subjective. Therefore, research focuses on identifying biological markers or specific changes in brain structure or function to improve diagnosis and treatment [81]. Migraine is three times more common in women than in men, leading to a negligible representation of men in migraine studies [82].
Migraine management is typically categorized into two types: episodic (less than 15 headache days per month) and chronic (15 or more headache days per month) [83]. Treatment usually involves a two-pronged approach: abortive therapy, which aims to relieve symptoms during an attack, and preventative therapy, which aims to reduce the frequency and severity of attacks [84,85,86,87,88]. Approximately 30-50% of cases find relief with abortive therapy, while around 40% require both approaches for effective management of severe, recurring episodes. Preventative measures are especially important for chronic cases and about a third of acute migraine patients [89]. Chronic migraine significantly impairs quality of life and is associated with increased incidence of comorbidities such as mood disorders, medication overuse, and obesity [87,88]. However, minimal compliance with treatment remains a major challenge, often due to issues of tolerance and safety [90,91]. The primary goal of migraine management is to avoid the overuse of over-the-counter headache medications, ensure timely and effective abortive medication during acute attacks, minimize headache intensity and frequency, and ensure an economical approach to management [92,93,94]. Pharmacological options for migraine management include calcium channel blockers, beta-blockers, tricyclic antidepressants, and anticonvulsants, with varying evidence regarding tolerance and efficacy [95,96]. Understanding gender-based differences in response to migraine medication can lead to more effective and targeted treatment strategies. Pharmacokinetics and pharmacodynamics differences between males and females is shown in Figure 3.
Abortive Therapy For the Management of Migraine
Abortive therapy for managing migraines involves a range of medications such as triptans, ergot derivatives, NSAIDs, paracetamol, opioids, and other derivatives. However, studies focusing on understanding gender-based differences in the response to therapy are very limited [97]. An overall pattern of compliance to prescribed medications is observed in women with triptans or ergot derivatives, while men mainly use over-the-counter medications for such acute attacks (NSAIDs, ibuprofen, acetylsalicylic acid, etc.) [98,99]. Moreover, women have a higher report of remission at 2 hours and 24 hours after medication and show higher relapse rates [99].
- Triptans: Triptans comprise a class of medications approved by the US Food and Drug Administration (FDA) as the first-line agent for treating acute migraine episodes with or without aura [101,102]. In the United States, seven triptans are available in diverse dosage formulations, including Sumatriptan, Naratriptan, Zolmitriptan, Rizatriptan, Almotriptan, frovatriptan, and Eletriptan [103]. Triptans bind to the vascular 5-HT1B receptors, leading to vasoconstriction of the cranial arteries, which dilate during a migraine attack. Triptans bind to the neurogenic and central 5-HT1D receptors and prevent the release of vasoactive neuropeptides by inhibiting trigeminal nerve activation and blocking the transmission of pain signals to the central nervous system [104]. Triptans are available in multiple dosage forms, including oral tablets, orally disintegrating tablets, nasal sprays, and SQ injections to accommodate patient preferences [103]. Patients are instructed to administer triptans at the first onset of the headache phase of a migraine attack, as their efficacy diminishes if taken during the aura phase before the onset of the headache [104]. If a patient has no response to one of the triptans after III trials, increasing the dose, switching to a different dosage of the same agent, or another triptan should be considered [105]. Triptans may cause nausea, dizziness, coronary vasoconstriction, flushing and paresthesia [106].
- Sumatriptan: Sumatriptan acts as an agonist on 5-HT1B/1D receptors by inducing vasoconstriction in the basilar artery and blood vessels within the dura mater. The drug reduces peripheral nociception either by selective cranial vasoconstriction or by affecting trigeminovascular nerves [107].
- Frovatriptan: It is the most potent triptan for its selective action on the 5HT1B receptor. It has a high affinity for 5HT1B and 5HT1D, like other triptans, and also a moderate affinity for 5HT1A and 5HT1F [108,109]. Studies have revealed the role of estrogen in mediating serotonin levels in the raphe nucleus by regulating the function of the tyrosine hydroxylase enzyme involved in the synthesis of 5HT and reducing the reuptake of this neurotransmitter. Estrogen also lowers the vasoconstriction effect of 5HT [110,111]. Frovatriptan attains twice the higher plasma levels in females as compared to males due to higher bioavailability in females [111,112,113]. It has a longer half-life and also a lower recurrence rate in the next 24 hours [114]. Naratriptan, Rizatriptan, and Zolmitriptan also exhibit similar efficacy in migraine management; however, they do not exhibit a sexually dimorphic response [115]. Frovatriptan is chiefly metabolized by CYP1A2 and is cleared by the kidney and liver making moderate failure of either organ not a limiting factor in treatment. Frovatriptan has a low risk of interactions with other drugs [116].
- Lasmiditan—Lasmiditan is a high-affinity, highly selective 5-HT1F receptor agonist that acts on the trigeminal system, where it hyperpolarizes nerve endings and reduces the release of CGRP to provide pain relief [117]. Because it is selective to 5-HT1F receptors, lasmiditan has no action on 5-HT1B/1D receptors located on cerebral blood vessels and does not involve vasoconstrictive mechanisms [118]. Lasmiditan can be used as an acute therapy for migraine in patients for whom triptans may be ineffective or contraindicated [119]. It is less likely to produce other side effects common to triptans, such as chest, neck, and throat tightness, and, therefore, may be a useful option for patients who experience these undesired phenomena [120]. The most common adverse effects associated with Lasmiditan use include dizziness, nausea, fatigue and paresthesias, which are dose-dependent [121].
- NSAIDs: Non-steroidal anti-inflammatory Drugs (NSAIDs) function by inhibiting the enzyme cyclooxygenase, which is responsible for the conversion of arachidonic acid into prostaglandins, especially E1, F2⍺, I (prostacyclin). These prostaglandins alter the excitability of afferent neurons and the sensitivity of the trigeminal nerve [122].
- CGRP Antagonist: CGRP antagonists reduce neuronal inflammation and thereby provide relief from migraine headaches [123]. Some of the CGRP antagonists that have the potential for abortive management of migraine episodes are Rimegepant, Olcegepant, and Telcagepant. Studies in healthy human beings have revealed that CGRP levels are higher in plasma in females than in males [123]. Animal experiments have revealed that in ovariectomized rats, administration of estrogen increases the level of CGRP in the arterioles. This establishes the fact that CGRP levels are higher in males than females and are particularly raised at higher levels by the intake of estrogen-containing birth control pills [124]
- Hormone Therapy: Fluctuating levels of sex steroids, both estrogen and androgen, have been found to be associated with frequent attacks of migraine. Menstrual migraine is one such condition where the fluctuation of plasma estrogen level is more drastic than in non-migraineurs [125]. This was proved in a study where intramuscular administration of estrogen during the perimenstrual period led to the postponement of migraine attacks. However, the same effect was not seen in the administration of progesterone during migraine attacks [126,127]. HRT, which is used for the management of postmenopausal symptoms, can also lead to the onset of migraine de novo or worsening of the preexisting condition. These conditions can be managed by minimizing the degree of fluctuation of the level of estrogen. This can be done by administration of gels and patch forms of sex steroids rather than their oral variants [128,129]. The association of migraine attacks is higher in surgically induced menopause than in naturally induced conditions. Furthermore, studies have shown that in male-to-female transsexuals, the use of anti-androgens to suppress male characteristics has led to an increased frequency of migraine attacks [130].
- GnRH Agonist: Recent studies have shown the role of GnRH agonists in the management of severe treatment-resistant menstrual migraine. Administration of GnRH agonists with a specific dose of estrogen and progesterone has shown relief in menstrual migraine. The role of GnRH agonists in migraine of males has not been studied yet [131].
- Prophylactic Therapy for Migraine: The main aim of prophylactic therapy is to reduce the frequency and severity of the episodes in chronic cases. There is a wide range of therapeutic options available like calcium channel blockers, antiepileptic drugs, botulinum neurotoxin, and antibodies against CGRP. Sexually dimorphic response to prophylactic management has not been identified yet. However, it is noted that women are more likely to use prescribed medications for prophylactic therapy than males [132].
Drugs commonly used for prophylactic management: Focused on Sex-based differences
1. Propranolol: Propranolol is a non-selective beta-blocker often used in the prophylactic treatment of migraine. The clearance of propranolol from plasma is lower in females compared to males. Thus, women may have higher plasma concentrations of the drug for a longer period, potentially increasing both its efficacy and the risk of side effects [133].
2. Atenolol: Atenolol, another beta-blocker, is also used for migraine prevention. Females exhibit lower clearance and a lower volume of distribution for atenolol, leading to higher plasma concentrations compared to males. This higher concentration could enhance the drug’s effectiveness in preventing migraines in women but might also increase the likelihood of side effects. Therefore, careful monitoring and possible dose adjustments are important when prescribing atenolol to females [133].
3. Verapamil: Verapamil is a calcium channel blocker used for migraine prevention. The bioavailability of verapamil is higher in females than in males, resulting in increased plasma concentrations of the drug. Thus, women may experience more pronounced effects, both therapeutic and adverse [133].
4. CYP45A—The cytochrome P450 enzyme system (CYP450) and P-glycoprotein play crucial roles in drug metabolism and clearance. There are various sex-based differences in the activity of these enzymes, making the pharmacokinetics of many drugs, including those used for migraine prevention, more complex in males and females. These differences can affect the metabolism and clearance rates of various medications, necessitating sex-specific considerations in drug dosing and management [133].
5. SSRIs: SSRIs are sometimes used off-label for migraine prevention. Females tend to have increased bioavailability of SSRIs due to reduced hepatic metabolism, thus more likely to achieve therapeutic plasma concentrations at lower doses than men [133].
6. Anti-epileptics: The primary role of antiepileptics in migraine prevention is to suppress the CSD (cortical spreading depression) and thus prevent neural inflammation and trigeminal sensitization [134]. They act by stabilizing the voltage-gated ion channels and preventing neuronal stimulation [135]. Topiramate and sodium valproate are the only two AEDs that are FDA-approved for the prevention of migraine. The most striking sex-based pharmacokinetic difference in antiepileptics is the increased rate of elimination and hepatic clearance associated with increased activity of CYP enzymes and increased protein binding capacity during pregnancy and intake of OC pills [136].
Alternative treatment approach for migraine
Alternative treatment approaches for migraine encompass a range of methods, including nutraceuticals, behavioral techniques, and surgical interventions. These approaches provide potential alternatives or complements to traditional migraine treatments, especially for cases resistant to pharmacologic interventions.
Nutraceuticals
- 1.1
- Riboflavin (Vitamin B12)—Riboflavin is a precursor of flavin mononucleotide and flavin adenine dinucleotide. All these coenzymes are important for energy production inside mitochondria and energy-related cellular functions. During magnetic resonance spectroscopy use of Riboflavin in migraine emerged, and studies suggest that there can be mitochondrial dysfunction in the migraine brain. In Belgium the first randomized controlled trial to assess the use of Riboflavin was done in which 400 mg of the daily dose was tested in 55 adult migraine patients (with or without aura). Riboflavin showed positive results by reducing headache and attack frequency with only minor or rare adverse effects compared to placebo. AAN/AHS guidelines have given evidence B for the treatment of migraine. The recommended dose is 400 mg daily for at least three months, during which adverse effects like diarrhoea, polyuria and yellowish discolouration of urine are noticed. Still, research is needed on Riboflavin. Riboflavin Coenzyme Q10 plays a vital role in energy metabolism. In one randomized control trial, 50 migraine children and adolescents were given a dose of CoQ10 100 mg per day and compared to a placebo, and no difference or effect was seen. Further studies are needed to support the use of CoQ10 for migraine. CoQ10 is available in the market in the US, and AAN/AHS guidelines consider CoQ10 for the prevention of migraine. The recommended dose is 1-3mg/kg/day [137,138].
- 1.2
- 1.3
- Petasites hybridus or butterbur—Butterbur root is an herbal extract. Petadolex is a tablet made of butterbur root extract manufactured in Germany, and safety concerns there due to its liver toxicity issues. To date, two placebo-controlled trials have been conducted for the first time by Lipton et al., in which 50 mg and 75 mg doses reduced migraine attacks with no adverse effects. Another study conducted by Diener in which 100mg butterbur was given for 12 weeks showed promising results by reducing migraine attacks compared to placebo [137,138].
- 1.4
- 1.5
- OnabotulinumtoxinA- Botulinum toxin is used as a muscle relaxant for pain. In 2010 FDA approved botulinum toxin (Brand name –Botox) for migraine prevention based on two large trials [137].
2. Behavioural Techniques
- 2.1
- Relaxation Technique—Relaxation techniques (RT) include meditation, autogenic training and muscle relaxation. RT does not only help in relaxing muscles but also reduces stress. It also enhances self-efficacy, self-esteem and self-control. RT includes deep breathing, intense progressive muscular RT, guided imagery RT, etc. Studies suggest that RT can reduce migraine attack frequency to 41% and 43% [139].
- 2.2
- Cognitive Behavior Therapy- Cognitive behaviour therapy (CBT) is mainly used for managing stress, anxiety, depression, sleep disorders, migraine pain, etc. CBT is mainly used when medication does not positively affect patients, such as during pregnancy, history of allergy to a specific medicine or medical comorbidities. CBT showed positive results with proper pharmacological therapies. CBT helps in the self-management of migraine pain; in a recent randomized trial, 135 children and adolescents were compared based on CBT plus amitriptyline with headache education plus amitriptyline. The CBT shows a positive result by reducing headaches to 11.5 in comparison to 20 weeks. In one study, CBT reduces stress; in another study, CBT reduces stress by 4% to 12%, and one CBT study helped reduce medication frequency by 20% to 25% [141,142].
- 2.3
- Mindfulness- Mindfulness is becoming popular in the United States, but MF has a long relation with Buddhism, Hinduism and Daoism. Langer and colleagues were the first US researchers to examine the effect of MF on patients. MF-based stress reduction (MBSR) was developed by Kabat –Linn which is effective in chronic pain. Standard MBSR is an eight week two hours groups with a mindfulness retreat as a conclusive session of 6 hours. Well et al. conducted the first randomized controlled trial on 25 people with episodic migraine. After one month of MBSR, there was a reduced headache with enhanced self-efficacy. Acceptance and Commitment is the newest member of MF-based interventions. ACT is based on psychological flexibility in which the patient, day-to-day life obstacles and other life circumstances are addressed. ACT is divided into six core processes, i.e., acceptance, cognitive delusion, contact with the present, self-values and Commitment to action. In one study, patients receiving MF reduced the frequency of headaches to 50%. MF-based intervention reduces the symptoms of chronic pain, and still, further studies need to be done [140,141].
- 3.
- Surgical Techniques for Migraine- Surgical management for migraine was first attempted by Dr. Harvey Cushing, but his attempt was unsuccessful. Migraine surgery became famous in 1999 when two patients got relief from headaches after forehead rejuvenation. In this surgery, part of the globular muscles is removed around the supraorbital and supratrochlear nerves with an incision on the eyelid or endoscopically and skeletonizing the nerves. Still, research needed to be done on surgery as it is not only a brain disorder. It also involves functional and structural plasticity of both the central and peripheral nervous systems [140,141].
- 3.1
-
Complementary Alternative Medicine (CAM)Complementary Alternative Medicine (CAM) for migraine includes a variety of non‐conventional therapies, such as acupuncture, herbal supplements, chiropractic care, and relaxation techniques. While these treatments are not universally recommended, many people turn to CAM approaches to complement traditional medical treatments, seeking to reduce the frequency and severity of migraine attacks and improve their overall quality of life.
- 3.2
- Acupuncture—Acupuncture is an ancient Chinese therapy based on the theory of disease causation secondary to an energy imbalance in the body. In acupuncture, needles are interested in acupoints (specific points along the energy meridians) in the body, which releases obstructed energy, which helps bring the body to balance and disease. A meta-analysis reported that acupuncture led to a 5% reduction in headache frequency. Acupuncture needs 6-8 sessions to manage symptoms of migraine. However, Acupuncture has adverse effects ranging from minimal effects like therapy failure or change in pain intensity to severe issues like bleeding, pneumothorax, infection, and nerve injury. Patients in whom pharmacological therapies are not effective are seen opting for acupuncture [137,138,139].
- 3.3
- Homoeopathic medicine—Several individuals frequently use homoeopathic medicine for migraine attacks. Damiana is the most popular homoeopathic medicine for migraine. Ceanothus is used when a patient has a migraine due to acidity. When a patient has a frontal headache with nausea, Iris V is effective. A few more homoeopathic medicines are available for migraine treatment and management: Onosmodium, Ptelea, Robin, etc. Evidence for their use is still lacking and further research is required to understand their role in the management of migraine [139,140,141].
- 3.4
- Chiropractors- Chiropractors are the most common complementary and alternative medicine (CAM) for treating and managing migraine. Roland et al. conducted an evidence-based chiropractic study that needs to be done based on guidelines even considering type, frequency, dosage, and duration of treatment [142]. Adverse effects of chiropractic study were seen in a controlled trial conducted by Aleksander et al. in which tenderness was seen [143]. Craig et al. highlighted important questions about the therapeutic approach to chiropractic migraine management that warrant further investigation. They reported that more primary research is needed to evaluate how chiropractors approach headache and migraine management, as well as to understand the prevalence, burden, and comorbidities of migraine within chiropractic patient populations [144].
Future Directions and Conclusion
Migraine is an episodic headache disorder that is more prevalent in women than men, with both male and female sex hormones playing significant roles in its pathophysiology. The estrogen withdrawal hypothesis is crucial in understanding hormonal therapy for migraine in females, although authentic evidence supporting this is lacking. Treatment for migraine includes abortive and preventive therapies, with triptans and NSAIDs falling under abortive therapy, and preventive therapies like SSRIs and propranolol mainly used for chronic cases. A recent meta-analysis of seven randomized clinical trials found that greater occipital nerve (GON) block significantly reduced the severity of pain in migraineurs compared to a control intervention. GON block is primarily used for prophylaxis in chronic migraine and in acute attacks of pediatric migraine, although its use in acute attacks of migraine is still limited.
Additionally, a non-hormonal correlation has been proposed as an alternative explanation for menstrual migraine, with studies showing lower ferritin levels in women with chronic recurrent migraine and a strong association between iron deficiency anaemia and menstrual migraine. Clinical evidence and genetic findings suggest a role for dopamine in migraine pathophysiology, with dopaminergic systems being correlated with multiple phases of migraine. Dopamine may modulate nociception pathways or alter cerebral blood flow, and dopaminergic hypersensitivity has been observed in the interictal state via neuroendocrine tests. Dopaminergic neural stimulation is influenced by sex steroids, particularly estrogen, which increases striatal dopamine synthesis and release. The correlation between the fall in estrogen levels and the risk of migraine attacks has been well-established. Apart from pharmacotherapy, nutritional supplements like vitamin B12 and behavioural techniques like CBT and mindfulness have shown positive results in migraine management. While migraine surgery, acupuncture, and homoeopathic medicine have also shown promise, further research is needed in these areas. Migraine treatment is not solely based on sex hormones, and all therapeutic interventions can be used for both male and female patients.
In conclusion, there is a significant gender-based difference in the manifestation pattern and response to therapy of migraine. Further studies are necessary to deepen our understanding of this aspect and enable more efficient management. Future research areas could include animal studies to elucidate the role of sex steroids in migraine pathophysiology, clinical studies on pharmacokinetics, and epidemiological studies to establish improved diagnostic criteria for faster and more effective treatment.
Acknowledgments
All authors contributed to writing, reviewing and editing. Figures are drawn by Mr. Faizan Ahmad and final proof reading and editing by Dr Rabeet Tariq
Data Availability Statement
Data can be made available on request.
Conflicts of Interest
The authors declare that they have no conflict of interest.
Consent for Publication: All authors have given consent for publication.
Abbreviations
| TMC | Trigeminal Nucleus Caudalis |
| EAAT1 | Excitatory Amino acid transport |
| CSD | Cortical Spreading Depression |
| NE | Norepinephrine |
| CGRP | Calcitonin Gene Related Peptide |
| HRT | Hormone Replacement Therapy |
| COCs | Combined Oral Contraceptives |
| PCOS | Polycystic Ovary Syndrome |
| REM | Sleep Rapid Eye Movement Sleep |
| eNOS | endothelial Nitric Oxide Synthase |
| MAO | Monoamine Oxidase |
| NSAIDs | Non Steroidal Anti-inflammatory Drugs |
| SSRIs | Selective Serotonin Reuptake Inhibitors |
| RT | Relaxation Techniques |
| CBT | Cognitive Behaviour Therapy |
| MBSR | Mindfulness based Stress reduction |
| GON | Greater Occipital Nerve |
References
- Critchley M. Migraine: from Cappadocia to Queen Square. London: Heinemann, 1967.
- GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459-480. [CrossRef]
- Gori S, Lucchesi C, Baldacci F, Bonuccelli U. Preferential occurrence of attacks during night sleep and/or upon awakening negatively affects migraine clinical presentation. Funct Neurol. 2015;30(2):119-123. [CrossRef]
- Kelman L, Rains JC. Headache and sleep: examination of sleep patterns and complaints in a large clinical sample of migraineurs. Headache. 2005;45(7):904-910. [CrossRef]
- Silberstein SD. Migraine symptoms: results of a survey of self-reported migraineurs. Headache. 1995;35(7):387-396. [CrossRef]
- Goadsby PJ, Holland PR, Martins-Oliveira M, Hoffmann J, Schankin C, Akerman S. Pathophysiology of Migraine: A Disorder of Sensory Processing. Physiol Rev. 2017;97(2):553-622. [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1-211. [CrossRef]
- Weitzel KW, Strickland JM, Smith KM, Goode JV. Gender-specific issues in the treatment of migraine. J Gend Specif Med. 2001;4(1):64-74.
- Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41(7):646-657. [CrossRef]
- Couturier EG, Bomhof MA, Neven AK, van Duijn NP. Menstrual migraine in a representative Dutch population sample: prevalence, disability and treatment. Cephalalgia. 2003;23(4):302-308. [CrossRef]
- Granella F, Sances G, Zanferrari C, Costa A, Martignoni E, Manzoni GC. Migraine without aura and reproductive life events: a clinical epidemiological study in 1300 women. Headache. 1993;33(7):385-389. [CrossRef]
- Fillingim RB, Hastie BA, Ness TJ, Glover TL, Campbell CM, Staud R. Sex-related psychological predictors of baseline pain perception and analgesic responses to pentazocine. Biol Psychol. 2005;69(1):97-112. [CrossRef]
- Gasbarri A, Arnone B, Pompili A, et al. Emotional memory and migraine: effects of amitriptyline and sex related difference. Behav Brain Res. 2008;189(1):220-225. [CrossRef]
- Wang XP, Liu JM, Zhao YB. Migraine: sex-influenced trait model?. Med Hypotheses. 2008;71(1):14-21. [CrossRef]
- Delaruelle Z, Ivanova TA, Khan S, et al. Male and female sex hormones in primary headaches. J Headache Pain. 2018;19(1):117. Published 2018 Nov 29. [CrossRef]
- Buse DC, Loder EW, Gorman JA, et al. Sex differences in the prevalence, symptoms, and associated features of migraine, probable migraine and other severe headache: results of the American Migraine Prevalence and Prevention (AMPP) Study. Headache. 2013;53(8):1278-1299. [CrossRef]
- Robinson ME, Riley JL 3rd, Myers CD, et al. Gender role expectations of pain: relationship to sex differences in pain. J Pain. 2001;2(5):251-257. [CrossRef]
- Bolay H, Ozge A, Saginc P, et al. Gender influences headache characteristics with increasing age in migraine patients. Cephalalgia. 2015;35(9):792-800. [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition (beta version). Cephalalgia. 2013;33:629-808.
- 20. https://www.scienceofmigraine.com/pathophysiology/phases-of-migraine.
- Andersen AR, Friberg L, Olsen TS, Olesen J. Delayed Hyperemia Following Hypoperfusion in Classic Migraine: Single Photon Emission Computed Tomographic Demonstration. Arch Neurol. 1988;45(2):154–159. [CrossRef]
- Olsen, T.S. (1990), Migraine With and Without Aura: The Same Disease Due to Cerebral Vasospasm of Different Intensity. A hypothesis based on CBF studies during migraine.. Headache: The Journal of Head and Face Pain, 30: 269-272. [CrossRef]
- Ferrari MD, Haan J, Blokland JAK, et al. Cerebral Blood Flow During Migraine Attacks Without Aura and Effect of Sumatriptan. Arch Neurol. 1995;52(2):135–139. [CrossRef]
- Gazerani P, Cairns BE. Dysautonomia in the pathogenesis of migraine. Expert Rev Neurother. 2018;18:153-165.
- Lashley KS. Patterns of cerebral integration indicated by the scotomas of migraine. Arch Neurol Psychiatry. 1941;46:331–9.
- Olesen J. Cerebral and extracranial circulatory disturbances in migraine: Pathophysiological implications. Cerebrovasc Brain Metab Rev. 1991;3:1–28.
- Goadsby PJ, Giffin N, Kaube H, Afridi S. Ketamine reduces the severity of prolonged migraine aura: Support for the glutamate hypothesis of aura. Neurology. 2011;76(Suppl 4):A443.
- Moskowitz MA, Macfarlane R. Neurovascular and molecular mechanisms in migraine headaches. Cerebrovasc Brain Metab Rev. 1993 Fall;5(3):159-77. [PubMed]
- Petersen KA, Nilsson E, Olesen J, Edvinsson L. Presence and function of the calcitonin gene-related peptide receptor on rat pial arteries investigated in vitro and in vivo. Cephalalgia. 2005;25:424–32.
- Moskowitz MA, Cutrer FM. SUMATRIPTAN: A receptor-targeted treatment for migraine. Ann Rev Med. 1993;44:145–54.
- Dimitriadou V, Buzzi MG, Moskowitz MA, Theoharides TC. Trigeminal sensory fiber stimulation induces morphological changes reflecting secretion in rat dura mater mast cells. Neuroscience. 1991;44:97–112.
- Schytz HW, Birk S, Wienecke T, Kruuse C, Olesen J, Ashina M. PACAP38 induces migraine-like attacks in patients with migraine without aura. Brain. 2009 Jan;132(Pt 1):16-25. Epub 2008 Dec 3. [CrossRef] [PubMed]
- Pavlović JM, Allshouse AA, Santoro NF, Crawford SL, Thurston RC, Neal-Perry GS, Lipton RB, Derby CA. Sex hormones in women with and without migraine: Evidence of migraine-specific hormone profiles. Neurology. 2016 Jul 5;87(1):49-56. Epub 2016 Jun 1. [CrossRef] [PubMed] [PubMed Central]
- Aggarwal M, Puri V, Puri S. Effects of estrogen on the serotonergic system and calcitonin gene-related peptide in trigeminal ganglia of rats. Ann Neurosci. 2012 Oct;19(4):151-7. [CrossRef] [PubMed] [PubMed Central]
- I: de Vries Lentsch, Eloísa Rubio-Beltrán, Antoinette MaassenVanDenBrink, Changing levels of sex hormones and calcitonin gene-related peptide (CGRP) during a woman’s life, 2021; -77, 35. Simone de Vries Lentsch, Eloísa Rubio-Beltrán, Antoinette MaassenVanDenBrink, Changing levels of sex hormones and calcitonin gene-related peptide (CGRP) during a woman’s life: Implications for the efficacy and safety of novel antimigraine medications, Maturitas, Volume 145, 2021, Pages 73-77, ISSN 0378-5122. [CrossRef]
- Durham PL. Calcitonin gene-related peptide (CGRP) and migraine. Headache. 2006 Jun;46 Suppl 1(Suppl 1):S3-8. [CrossRef] [PubMed] [PubMed Central]
- 37. https://www.factsaboutfertility.org/hormonal-balance-and-the-female-brain-a-review/.
- Stephania Paredes, Santiago Cantillo, Kenneth D. Candido, Nebojsa Nick Knezevic. “An Association of Serotonin with Pain Disorders and Its Modulation by Estrogens”, International Journal of Molecular Science, 2019.
- Herbison AE, Simonian SX, Thanky NR, Bicknell RJ. Oestrogen modulation of noradrenaline neurotransmission. Novartis Found Symp. 2000;230:74-85; discussion 85-93. [CrossRef] [PubMed]
- Pavlović JM, Allshouse AA, Santoro NF, Crawford SL, Thurston RC, Neal-Perry GS, Lipton RB, Derby CA. Sex hormones in women with and without migraine: evidence of migraine-specific hormone profiles. Neurology. 2016 Jul 5;87(1):49-56.
- Güven B, Güven H, Çomoğlu S. Clinical characteristics of menstrually related and non-menstrual migraine. Acta Neurologica Belgica. 2017 Sep;117:671-6.
- Wharton W, E Gleason C, Sandra O, M Carlsson C, Asthana S. Neurobiological underpinnings of the estrogen-mood relationship. Current psychiatry reviews. 2012 Aug 1;8(3):247-56.
- Craft RM. Modulation of pain by estrogens. Pain. 2007 Nov 1;132:S3-12.
- SHOUPE D, MONTZ FJ, LOBO RA. The effects of estrogen and progestin on endogenous opioid activity in oophorectomized women. The Journal of Clinical Endocrinology & Metabolism. 1985 Jan 1;60(1):178-83.
- Villablanca AC, Hanley MR. 17β-estradiol stimulates substance P receptor gene expression. Molecular and cellular endocrinology. 1997 Dec 12;135(2):109-17.
- Iversen L. Substance P equals pain substance?. Nature. 1998 Mar 26;392(6674):334-5.
- Zhang J, Bai W, Wang W, Jiang H, Jin B, Liu Y, Liu S, Wang K, Jia J, Qin L. Mechanisms underlying alterations in norepinephrine levels in the locus coeruleus of ovariectomized rats: Modulation by estradiol valerate and black cohosh. Neuroscience. 2017 Jun 23;354:110-21.
- Stahl SM. Effects of estrogen on the central nervous system. Journal of Clinical Psychiatry. 2001 May 1;62(5):317-8.
- Kelly MJ, Qiu J, Rønnekleiv OK. Estrogen signaling in the hypothalamus. Vitamins & Hormones. 2005 Jan 1;71:123-45.
- Raffaelli B, Storch E, Overeem LH, Terhart M, Fitzek MP, Lange KS, Reuter U. Sex hormones and calcitonin gene–related peptide in women with migraine: a cross-sectional, matched cohort study. Neurology. 2023 Apr 25;100(17):e1825-35.
- Pau KY, Hess DL, Kohama S, Bao J, Pau CY, Spies HG. Oestrogen upregulates noradrenaline release in the mediobasal hypothalamus and tyrosine hydroxylase gene expression in the brainstem of ovariectomized rhesus macaques. J Neuroendocrinol. 2000 Sep;12(9):899-909. [CrossRef] [PubMed]
- Krolick KN, Zhu Q, Shi H. Effects of Estrogens on Central Nervous System Neurotransmission: Implications for Sex Differences in Mental Disorders. Prog Mol Biol Transl Sci. 2018;160:105-171. Epub 2018 Aug 28. [CrossRef] [PubMed] [PubMed Central]
- Del Rà o Juan Pablo, Alliende Marà a I., Molina Natalia, Serrano Felipe G., Molina Santiago, Vigil Pilar, TITLE=Steroid Hormones and Their Action in Women’s Brains: The Importance of Hormonal Balance , JOURNAL=Frontiers in Public Health, VOLUME=6,2018,URL=https://www.frontiersin.org/articles/10.3389/fpubh.2018.00141 ISSN=2296-2565. [CrossRef]
- Al-Hassany Linda, Haas Jennifer, Piccininni Marco, Kurth Tobias, Maassen Van Den Brink Antoinette, Rohmann Jessica L., TITLE=Giving Researchers a Headache – Sex and Gender Differences in Migraine, JOURNAL=Frontiers in Neurology, VOLUME=11, 2020, URL=https://www.frontiersin.org/articles/10.3389/fneur.2020.549038 DOI=10.3389/fneur.2020.549038, ISSN=1664-2295.
- Hehui Zhang, Xiaokai Yang, Yijun Lin, Linglong Chen, Hua Ye, The efficacy of greater occipital nerve block for the treatment of migraine: A systematic review and meta-analysis, Clinical Neurology and Neurosurgery, Volume 165, 2018, Pages 129-133, ISSN 0303-8467. [CrossRef]
- Calhoun, A.H.; Gill, N. Presenting a New, Non-Hormonally Mediated Cyclic Headache in Women: End-Menstrual Migraine. Headache 2017, 57, 17–20.
- MacGregor, E.A.; Frith, A.; Ellis, J.; Aspinall, L.; Hackshaw, A. Incidence of migraine relative to menstrual cycle phases of rising and falling estrogen. Neurology 2006, 67, 2154–2158.
- Fanciullacci M, Alessandri M, Del Rosso A. Dopamine involvement in the migraine attack. Funct Neurol. 2000;15 Suppl 3:171-81. PMID: 11200788.
- Lammers, C.-H., D’Souza, U., Qin, Z.-H., Lee, S.-H., Yajima, S. and Mouradian, M.M. (1999), regulation of striatal dopamine receptors by estrogen. Synapse, 34: 222-227. [CrossRef]
- Sarchielli P, Tognoloni M, Russo S, Vulcano MR, Feleppa M, Mala` M, Sartori M, Gallai V (1996) Variations in the platelet arginine nitric oxide pathway during the ovarian cycle in females affected by menstrual migraine. Cephalalgia 16:468–475.
- Kim C, Siscovick DS, Sidney S, Lewis CE, Kiefe CI, Koepsell TD. Oral contraceptive use and association with glucose, insulin, and diabetes in young adult women: the CARDIA study. Diabetes Care. 2002 Jun 1;25(6):1027-32.
- Lieba-Samal D, Wöber C, Frantal S, Brannath W, Schmidt K, Schrolnberger C, Wöber-Bingöl Ç, PAMINA Study Group. Headache, menstruation and combined oral contraceptives: a diary study in 184 women with migraine. European Journal of Pain. 2011 Sep 1;15(8):852-7.
- Curtis KM, Mohllajee AP, Peterson HB. Use of combined oral contraceptives among women with migraine and nonmigrainous headaches: a systematic review. Contraception. 2006 Feb 1;73(2):189-94.
- Sarahian N, Noroozzadeh M, Saei Ghare Naz M, Eskandari-Roozbahani N, Mahboobifard F, Ramezani Tehrani F. Is there any association between migraine headache and polycystic ovary syndrome (PCOS)? A review article. Molecular biology reports. 2022 Jan 1:1-9.
- Ripa P, Ornello R, Degan D, Tiseo C, Stewart J, Pistoia F, Carolei A, Sacco S. Migraine in menopausal women: a systematic review. International journal of women’s health. 2015 Aug 20:773-82.
- MacGregor EA. Migraine, menopause and hormone replacement therapy. Post reproductive health. 2018 Mar;24(1):11-8.
- Somerville BW (1972) The role of estradiol withdrawal in the etiology of menstrual migraine. Neurology 22:355–365.
- D.P. Shackelford, M.M. McConnaughey, S.G. Iams; The effects of estradiol and mestranol on alpha-adrenoceptors in select regions of the rat brain; Brain Research Bulletin; Volume 21, Issue 2, 1988; Pages 329-333,ISSN 0361-9230.
- Nattero G, Allais G, De Lorenzo C, et al. Menstrual migraine: new biochemical and psychological aspects. Headache. 1988;28(2):103-107.
- Calhoun, A.H. (2018), Understanding Menstrual Migraine. Headache: The Journal of Head and Face Pain, 58: 626-630. https://doi.org/10.1111/head.13291.
- Silberstein SD, Merriam GR. Estrogens, progestins,and headache. Neurology. 1991;41(6):786-793.
- Akcali D, Sayin A, Sara Y, Bolay H (2010) Does single cortical spreading depression elicit pain behaviour in freely moving rats? Cephalalgia 30:1195–1206.
- Granella F, Sances G, Pucci E, Nappi RE, Ghiotto N, Nappi G (2000) Migraine with aura and reproductive life events: a case control study. Cephalalgia 20:701–707.
- Aegidius K, Zwart JA, Hagen K, Stovner L (2009) The effect of pregnancy and parity on headache prevalence: the Head-HUNT study. Headache 49:851–859.
- Kvisvik EV, Stovner LJ, Helde G, Bovim G, Linde M (2011) Headache and migraine during pregnancy and puerperium: the MIGRA-study. J Headache Pain 12:443–451.
- Nattero G, Allais G, De Lorenzo C, et al. Menstrual migraine: new biochemical and psychological aspects. Headache. 1988;28(2):103-107.
- Gruber HJ, Bernecker C, Lechner A, Weiss S, Wallner-Blazek M, Meinitzer A, Höbarth G, Renner W, Fauler G, Horejsi R, Fazekas F. Increased nitric oxide stress is associated with migraine. Cephalalgia. 2010 Apr;30(4):486-92.
- Ramadan NM. The link between glutamate and migraine. CNS spectrums. 2003 Jun;8(6):446-9.
- Paredes S, Cantillo S, Candido KD, Knezevic NN. An association of serotonin with pain disorders and its modulation by estrogens. International journal of molecular sciences. 2019 Nov 15;20(22):5729.
- Vos T, Abajobir A, Abate K, Abbafati C, Abbas K, Abd-Allah F et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. The Lancet. 2017;390(10100):1211-1259.
- Gazerani P. Current Evidence on Potential Uses of MicroRNA Biomarkers for Migraine: From Diagnosis to Treatment. Molecular Diagnosis & Therapy. 2019;23(6):681-694.
- Vetvik K, MacGregor E. Sex differences in the epidemiology, clinical features, and pathophysiology of migraine. The Lancet Neurology. 2017;16(1):76-87.
- The International Classification of Headache Disorders—ICHD-3 [Internet]. ICHD-3. 2022 [cited 21 July 2022]. Available from: https://ichd-3.org.
- Buse D, Scher A, Dodick D, Reed M, Fanning K, Manack Adams A et al. Impact of Migraine on the Family: Perspectives of People With Migraine and Their Spouse/Domestic Partner in the CaMEO Study. Mayo Clinic Proceedings. 2016;91(5):596-611.
- Correction to Lancet Respir Med 2021; published online April 9. https://doi. org/10.1016/S2213-2600(21)00160-0. The Lancet Respiratory Medicine. 2021;9(6):e55.
- Announcements. Cephalalgia. 1999;19(10):913-913.
- Buse D, Manack A, Serrano D, Turkel C, Lipton R. Sociodemographic and comorbidity profiles of chronic migraine and episodic migraine sufferers. 2022.
- Lipton R, Bigal M, Diamond M, Freitag F, Reed M, Stewart W. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology. 2007;68(5):343-349.
- Evans R, Linde M. Expert Opinion: Adherence to Prophylactic Migraine Medication. Headache: The Journal of Head and Face Pain. 2009;49(7):1054-1058.
- Gracia Naya M, Santos Lasaosa S, Ríos Gómez C, Sánchez Valiente S, García Gomara M, Latorre Jiménez A et al. Factores predisponentes al abandono del tratamiento preventivo en una serie de pacientes con migraña. Revista de Neurología. 2011;53(04):201.
- Silberstein S, Holland S, Freitag F, Dodick D, Argoff C, Ashman E. Evidence-based guideline update: Pharmacologic treatment for episodic migraine prevention in adults: Table 1. Neurology. 2012;78(17):1337-1345.
- Silberstein S, Winner P, Chmiel J. Migraine Preventive Medication Reduces Resource Utilization. Headache: The Journal of Head and Face Pain. 2003;43(3):171-178.
- Loder E, Burch R, Rizzoli P. The 2012 AHS/AAN Guidelines for Prevention of Episodic Migraine: A Summary and Comparison With Other Recent Clinical Practice Guidelines. Headache: The Journal of Head and Face Pain. 2012;52(6):930-945.
- Shamliyan T, Choi J, Ramakrishnan R, Miller J, Wang S, Taylor F et al. Preventive Pharmacologic Treatments for Episodic Migraine in Adults. Journal of General Internal Medicine. 2013;28(9):1225-1237.
- Goadsby P, Sprenger T. Current practice and future directions in the prevention and acute management of migraine. The Lancet Neurology. 2010;9(3):285-298.
- van Casteren D, Couturier E, van den Brink A. Sex- and Gender-Specific Aspects of Migraine Treatment. Gender and Migraine. 2019;:31-43.
- Buse D, Loder E, Gorman J, Stewart W, Reed M, Fanning K et al. Sex Differences in the Prevalence, Symptoms, and Associated Features of Migraine, Probable Migraine and Other Severe Headache: Results of the American Migraine Prevalence and Prevention (AMPP) Study. Headache: The Journal of Head and Face Pain. 2013;53(8):1278-1299.
- Lipton R, Manack Adams A, Buse D, Fanning K, Reed M. A Comparison of the Chronic Migraine Epidemiology and Outcomes (CaMEO) Study and American Migraine Prevalence and Prevention (AMPP) Study: Demographics and Headache-Related Disability. Headache: The Journal of Head and Face Pain. 2016;56(8):1280-1289.
- Dodick D, Lipton R, Goadsby P, Tfelt-Hansen P, Ferrari M, Diener H et al. Predictors of Migraine Headache Recurrence: A Pooled Analysis From the Eletriptan Database. Headache: The Journal of Head and Face Pain. 2007;0(0):070629211050002.
- Cady R, Schreiber C. Sumatriptan: update and review. Expert Opin Pharmacother. 2006 Aug;7(11):1503-14. [CrossRef] [PubMed]
- Negro A, Koverech A, Martelletti P. Serotonin receptor agonists in the acute treatment of migraine: a review on their therapeutic potential. J Pain Res. 2018 Mar 8;11:515-526. [CrossRef] [PubMed] [PubMed Central]
- Antonaci F, Ghiotto N, Wu S, Pucci E, Costa A. Recent advances in migraine therapy. Springerplus. 2016 May 17;5:637. [CrossRef] [PubMed] [PubMed Central]
- Tepper SJ, Rapoport AM, Sheftell FD. Mechanisms of action of the 5-HT1B/1D receptor agonists. Arch Neurol. 2002 Jul;59(7):1084-8. [CrossRef] [PubMed]
- Olesen J, Diener HC, Schoenen J, Hettiarachchi J. No effect of eletriptan administration during the aura phase of migraine. Eur J Neurol. 2004 Oct;11(10):671-7. [CrossRef] [PubMed]
- Sinclair AJ, Sturrock A, Davies B, Matharu M. Headache management: pharmacological approaches. Pract Neurol. 2015 Dec;15(6):411-23. Epub 2015 Jul 3. [CrossRef] [PubMed] [PubMed Central]
- González-Hernández A, Marichal-Cancino BA, MaassenVanDenBrink A, Villalón CM. Side effects associated with current and prospective antimigraine pharmacotherapies. Expert Opin Drug Metab Toxicol. 2018 Jan;14(1):25-41. Epub 2017 Dec 15. [CrossRef] [PubMed]
- Brar Y, Hosseini SA, Saadabadi A. Sumatriptan. [Updated 2023 Nov 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470206/.
- Brown AM, Ho M, Thomas DR, Parsons AA. Functional effects of frovatriptan (VML 251), sumatriptan and naratriptan on human recombinant 5-HT1 and 5-HT7 receptors. Headache. 1998;38:376.
- Stewart M. The binding affinity and functional activity of eletriptan and other 5-HT_< 1B/1D> agonists at the human recombinant 5-HT_< 1B> and 5-HT_< 1D> receptors. Br J Pharmacol. 1999;127:93P.
- Gupta S, McCarson KE, Welch KM, Berman NE. Mechanisms of pain modulation by sex hormones in migraine. Headache: The Journal of Head and Face Pain. 2011 Jun;51(6):905-22.
- Aggarwal M, Puri V, Puri S. Effects of estrogen on the serotonergic system and calcitonin gene-related peptide in trigeminal ganglia of rats. Annals of neurosciences. 2012 Oct;19(4):151.
- Jhee SS, Shiovitz T, Crawford AW, Cutler NR. Pharmacokinetics and pharmacodynamics of the triptan antimigraine agents. Clinical pharmacokinetics. 2001 Mar;40(3):189-205.
- Elkind AH, Wade A, Ishkanian G. Pharmacokinetics of frovatriptan in adolescent migraineurs. The Journal of Clinical Pharmacology. 2004 Oct;44(10):1158-65.
- Negro A, Lionetto L, Casolla B, Lala N, Simmaco M, Martelletti P. Pharmacokinetic evaluation of frovatriptan. Expert Opinion on Drug Metabolism & Toxicology. 2011 Nov 1;7(11):1449-58.
- Franconi F, Finocchi C, Allais G, Omboni S, Tullo V, Campesi I, Reggiardo G, Benedetto C, Bussone G. Gender and triptan efficacy: a pooled analysis of three double-masked, randomized, crossover, multicenter, Italian studies comparing frovatriptan vs. other triptans. Neurological Sciences. 2014 May;35(1):99-105.
- Buchan P, Wade A, Ward C, Oliver SD, Stewart AJ, Freestone S. Frovatriptan: a review of drug-drug interactions. Headache. 2002 Apr;42 Suppl 2:S63-73. [CrossRef] [PubMed]
- Clemow DB, Johnson KW, Hochstetler HM, Ossipov MH, Hake AM, Blumenfeld AM. Lasmiditan mechanism of action—review of a selective 5-HT1F agonist. J Headache Pain. 2020 Jun 10;21(1):71. [CrossRef] [PubMed] [PubMed Central]
- Hou M, Xing H, Li C, Wang X, Deng D, Li J, Zhang P, Chen J. Short-term efficacy and safety of lasmiditan, a novel 5-HT1F receptor agonist, for the acute treatment of migraine: a systematic review and meta-analysis. J Headache Pain. 2020 Jun 5;21(1):66. [CrossRef] [PubMed] [PubMed Central]
- Chan C, Goadsby PJ. Recent Advances in Pharmacotherapy for Episodic Migraine. CNS Drugs. 2019 Nov;33(11):1053-1071. doi: 10.1007/s40263-019-00665-9. PMID: 31556018.
- Lupi C, Benemei S, Guerzoni S, Pellesi L, Negro A. Pharmacokinetics and pharmacodynamics of new acute treatments for migraine. Expert Opin Drug Metab Toxicol. 2019 Mar;15(3):189-198. Epub 2019 Feb 12. [CrossRef] [PubMed]
- Rizzoli PB. Emerging therapeutic options for acute migraine: focus on the potential of lasmiditan. Neuropsychiatr Dis Treat. 2014 Mar 31;10:547-52. [CrossRef] [PubMed] [PubMed Central]
- Dong XD, Svensson P, Cairns BE. The analgesic action of topical diclofenac may be mediated through peripheral NMDA receptor antagonism. PAIN®. 2009 Dec 15;147(1-3):36-45.
- Edvinsson L, Haanes KA, Warfvinge K, Krause DN. CGRP as the target of new migraine therapies—successful translation from bench to clinic. Nature Reviews Neurology. 2018 Jun;14(6):338-50.
- Valdemarsson S, Edvinsson L, Hedner P, Ekman R. Hormonal influence on calcitonin gene-related peptide in man: effects of sex difference and contraceptive pills. Scandinavian Journal of Clinical and Laboratory Investigation. 1990 Jan 1;50(4):385-8.
- Gupta S, McCarson KE, Welch KM, Berman NE. Mechanisms of pain modulation by sex hormones in migraine. Headache: The Journal of Head and Face Pain. 2011 Jun;51(6):905-22.
- Pavlović JM, Allshouse AA, Santoro NF, Crawford SL, Thurston RC, Neal-Perry GS, Lipton RB, Derby CA. Sex hormones in women with and without migraine: evidence of migraine-specific hormone profiles. Neurology. 2016 Jul 5;87(1):49-56.
- MacGregor EA. Estrogen replacement and migraine. Maturitas. 2009 May 20;63(1):51-5.
- Nappi RE, Cagnacci A, Granella F et al. (2001) Course of primary headaches during hormone replacement therapy. Maturitas 38:157–163.
- Macgregor A (1999) Effects of oral and transdermal estrogen replacement on migraine. Cephalalgia 19:124–125.
- Pringsheim T, Gooren L. Migraine prevalence in male to female transsexuals on hormone therapy. Neurology. 2004 Aug 10;63(3):593-4.
- Murray SC, Muse KN. Effective treatment of severe menstrual migraine headaches with gonadotropin-releasing hormone agonist and “add-back” therapy. Fertility and sterility. 1997 Feb 1;67(2):390-3.
- Vetvik KG, MacGregor EA. Sex differences in the epidemiology, clinical features, and pathophysiology of migraine. The Lancet Neurology. 2017 Jan 1;16(1):76-87.
- Soldin OP, Chung SH, Mattison DR. Sex differences in drug disposition. Journal of Biomedicine and Biotechnology. 2011 Oct;2011.
- Costa C, Tozzi A, Rainero I, Cupini LM, Calabresi P, Ayata C, Sarchielli P. Cortical spreading depression as a target for anti-migraine agents. The journal of headache and pain. 2013 Dec;14(1):1-8.
- White HS. Molecular pharmacology of topiramate: managing seizures and preventing migraine. Headache: The Journal of Head and Face Pain. 2005 Apr;45:S48-56.
- Yerby MS, Friel PN, McCormick K, Koerner M, Van Allen M, Leavitt AM, Sells CJ, Yerby JA. Pharmacokinetics of anticonvulsants in pregnancy: alterations in plasma protein binding. Epilepsy research. 1990 Apr 1;5(3):223-8.
- Francesca Puledda and Kevin Shields Non-Pharmacological Approaches for Migraine Neurotherapeutics. 2018 Apr; 15(2): 336–345.
- .Licia Grazzi, Claudia Toppo, Domenico D’Amico Non-Pharmacological Approaches to Headaches: Non-Invasive Neuromodulation, Nutraceuticals, and Behavioral Approaches Int J Environ Res Public Health. 2021 Feb; 18(4): 1503.
- Andrea Pérez-Muñoz , Dawn C Buse , Frank Andrasik Behavioral Interventions for Migraine Neurol Clin2019 Nov;37(4):789-813. doi: 10.1016/j.ncl.2019.07.003. Epub 2019 Aug 22.
- Palak S Patel , Mia T Minen Complementary and Integrative Health Treatments for Migraine J Neuroophthalmol 2019 Sep;39(3):360-369. [CrossRef]
- A: Totonchi, Bahman Guyuron, Hossein Ansari Surgical Options for Migraine, 2021; 141. Ali Totonchi , Bahman Guyuron, Hossein Ansari Surgical Options for Migraine: An Overview Neurology India (2021) 105-109. [CrossRef]
- Bryans R, Descarreaux M, Duranleau M, Marcoux H, Potter B, Ruegg R, Shaw L, Watkin R, White E. Evidence-based guidelines for the chiropractic treatment of adults with headache. J Manipulative Physiol Ther. 2011 Jun;34(5):274-89. [CrossRef] [PubMed]
- Chaibi A, Benth JŠ, Tuchin PJ, Russell MB. Adverse events in a chiropractic spinal manipulative therapy single-blinded, placebo, randomized controlled trial for migraineurs. Musculoskelet Sci Pract. 2017 Jun;29:66-71. Epub 2017 Mar 14. Erratum in: Musculoskelet Sci Pract. 2017 Oct;31:21. [CrossRef] [PubMed]
- Craig Moore, Jon Adams, Andrew Leaver, Romy Lauche, and David Sibbritt The treatment of migraine patients within chiropractic: analysis of a nationally representative survey of 1869 chiropractors BMC Complement Altern Med. 2017; 17: 519.
Figure 1.
Pathophysiology of Migraine: Migraine begins with dysregulation in the hypothalamus, which activates the trigeminovascular system involving the trigeminal nucleus caudalis (TNC). The TNC becomes hyperactive, processing nociceptive signals from the meninges and cervical structures and transmitting pain signals to higher brain centres. Concurrently, overactive excitatory neurons utilizing glutamate lead to cortical spreading depression (CSD), a wave of neuronal depolarization followed by suppression. Genetic factors, such as mutations in CACNA1A (FHM1), SCN1A (FHM3), and dysfunctions in the Na+-HCO3- cotransporter 1 (NBCE1) and the excitatory amino acid transporter 1 (EAAT1), exacerbate this hyperexcitability by disrupting ion homeostasis and neurotransmitter regulation. This cascade results in the characteristic headache and sensory disturbances of a migraine.
Figure 1.
Pathophysiology of Migraine: Migraine begins with dysregulation in the hypothalamus, which activates the trigeminovascular system involving the trigeminal nucleus caudalis (TNC). The TNC becomes hyperactive, processing nociceptive signals from the meninges and cervical structures and transmitting pain signals to higher brain centres. Concurrently, overactive excitatory neurons utilizing glutamate lead to cortical spreading depression (CSD), a wave of neuronal depolarization followed by suppression. Genetic factors, such as mutations in CACNA1A (FHM1), SCN1A (FHM3), and dysfunctions in the Na+-HCO3- cotransporter 1 (NBCE1) and the excitatory amino acid transporter 1 (EAAT1), exacerbate this hyperexcitability by disrupting ion homeostasis and neurotransmitter regulation. This cascade results in the characteristic headache and sensory disturbances of a migraine.
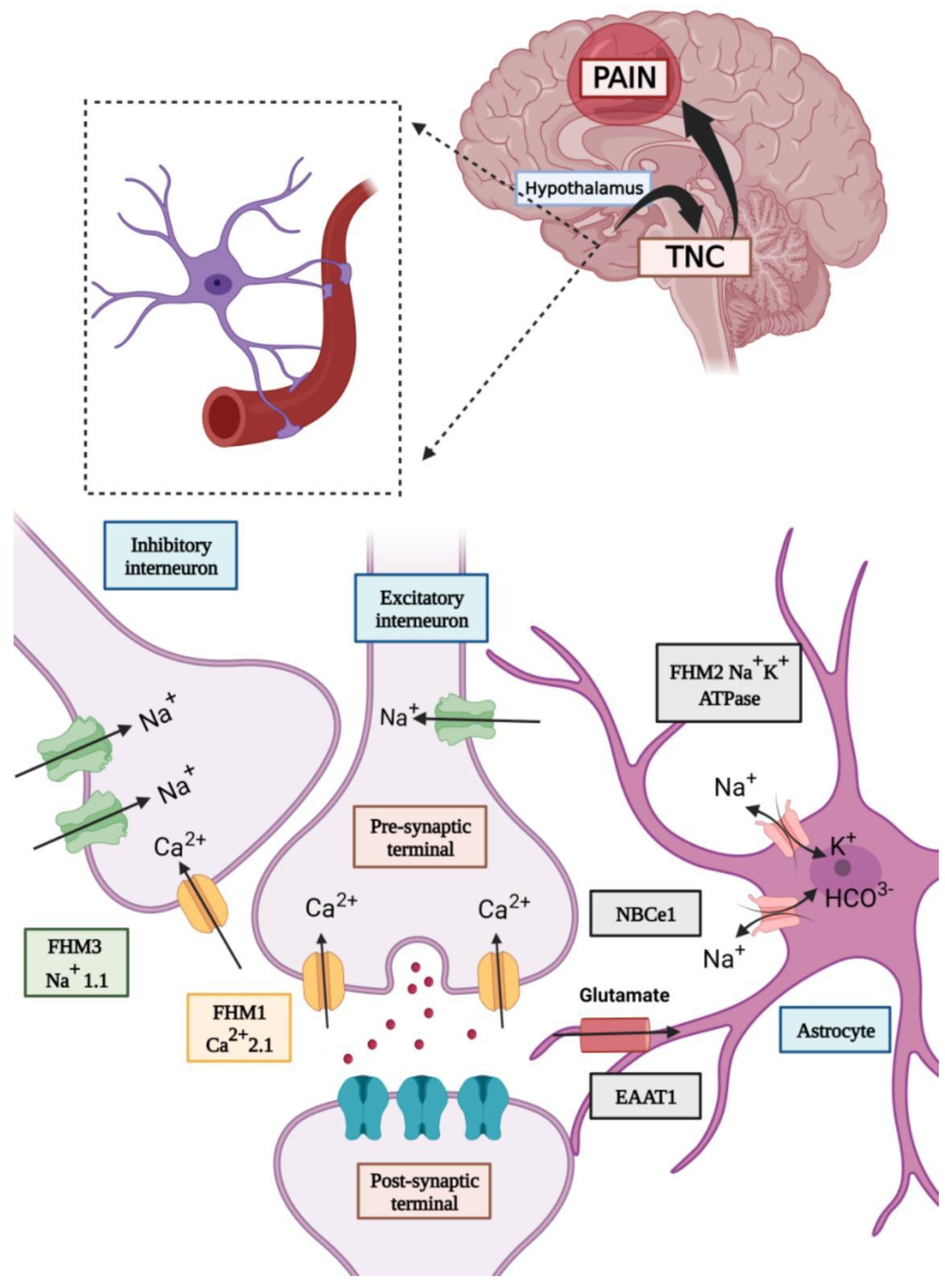
Figure 2.
Estrogen-mediated activation of alpha-1 receptors promotes vasoconstriction, while activation of alpha-2 receptors induces vasodilation. Additionally, estrogen enhances the serotonergic system, increasing serotonin levels, which can affect vascular tone and pain perception. These conflicting effects can lead to fluctuations in blood vessel diameter, contributing to the vascular component of migraines. Estrogen also stimulates the synthesis and release of nitric oxide (NO) and calcitonin gene-related peptide (CGRP), both potent vasodilators that play critical roles in migraine pathogenesis by promoting neurogenic inflammation and vasodilation, exacerbating pain. Furthermore, estrogen increases intracellular calcium levels and decreases magnesium levels, which heightens neuronal excitability and susceptibility to cortical spreading depression (CSD) associated with migraine aura and headache. Elevated estrogen levels also upregulate the expression of immediate early genes like cFos and pro-inflammatory transcription factors like NF-κB, which are involved in pain signalling pathways. The increased neuronal activity and inflammation due to these factors amplify pain perception during a migraine attack.
Figure 2.
Estrogen-mediated activation of alpha-1 receptors promotes vasoconstriction, while activation of alpha-2 receptors induces vasodilation. Additionally, estrogen enhances the serotonergic system, increasing serotonin levels, which can affect vascular tone and pain perception. These conflicting effects can lead to fluctuations in blood vessel diameter, contributing to the vascular component of migraines. Estrogen also stimulates the synthesis and release of nitric oxide (NO) and calcitonin gene-related peptide (CGRP), both potent vasodilators that play critical roles in migraine pathogenesis by promoting neurogenic inflammation and vasodilation, exacerbating pain. Furthermore, estrogen increases intracellular calcium levels and decreases magnesium levels, which heightens neuronal excitability and susceptibility to cortical spreading depression (CSD) associated with migraine aura and headache. Elevated estrogen levels also upregulate the expression of immediate early genes like cFos and pro-inflammatory transcription factors like NF-κB, which are involved in pain signalling pathways. The increased neuronal activity and inflammation due to these factors amplify pain perception during a migraine attack.
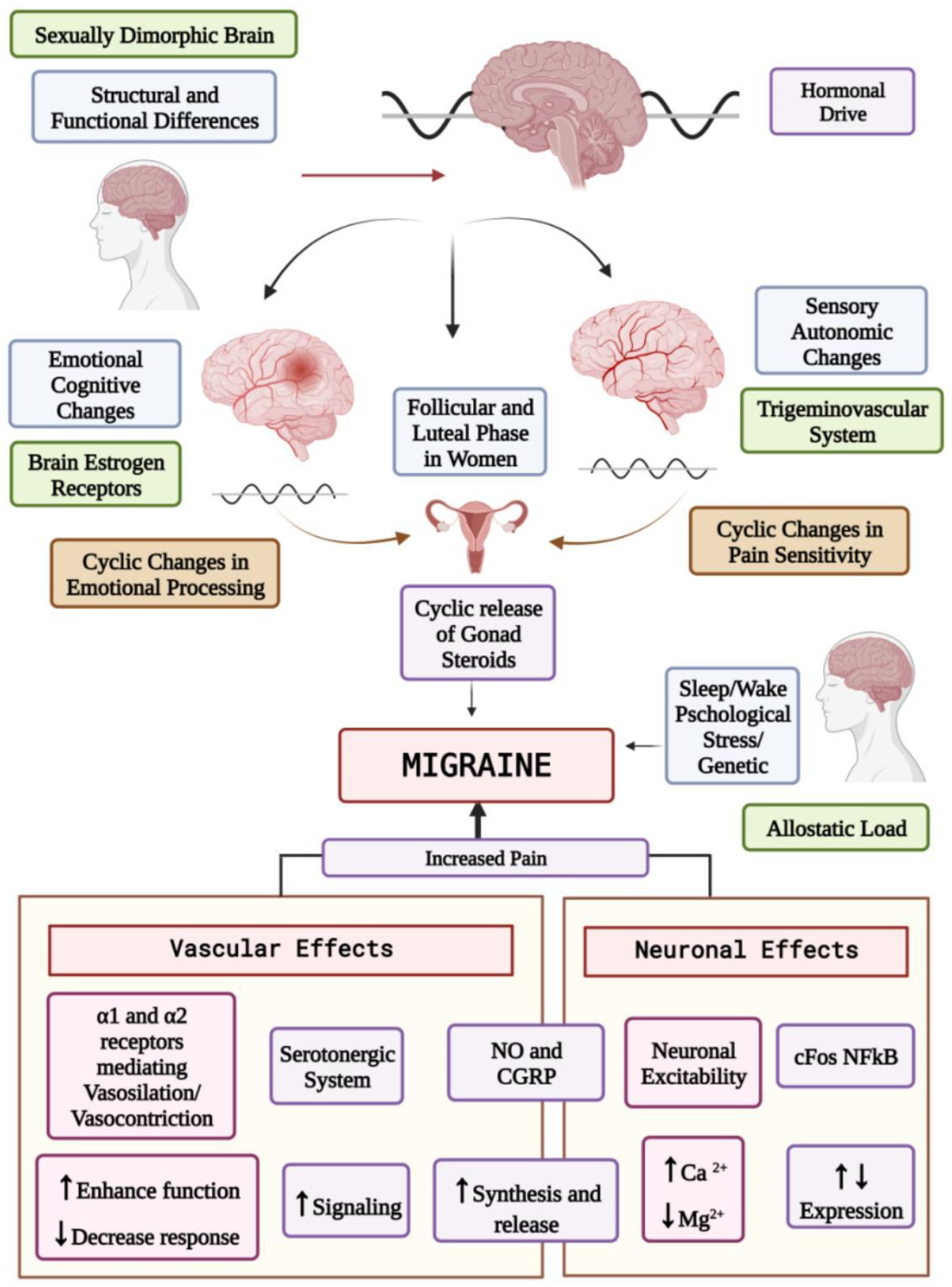
Figure 3.
Pharmacokinetic and pharmacodynamic differences between males and females. This figure illustrates the processes involved in pharmacokinetics and pharmacodynamics, emphasizing the differences between males and females in drug absorption, distribution, metabolism, excretion, and response. The figure emphasizes that males and females may differ in these pharmacokinetic and pharmacodynamic processes due to variations in physiology, enzyme activity, hormonal levels, and body composition, impacting drug effectiveness and safety.
Figure 3.
Pharmacokinetic and pharmacodynamic differences between males and females. This figure illustrates the processes involved in pharmacokinetics and pharmacodynamics, emphasizing the differences between males and females in drug absorption, distribution, metabolism, excretion, and response. The figure emphasizes that males and females may differ in these pharmacokinetic and pharmacodynamic processes due to variations in physiology, enzyme activity, hormonal levels, and body composition, impacting drug effectiveness and safety.
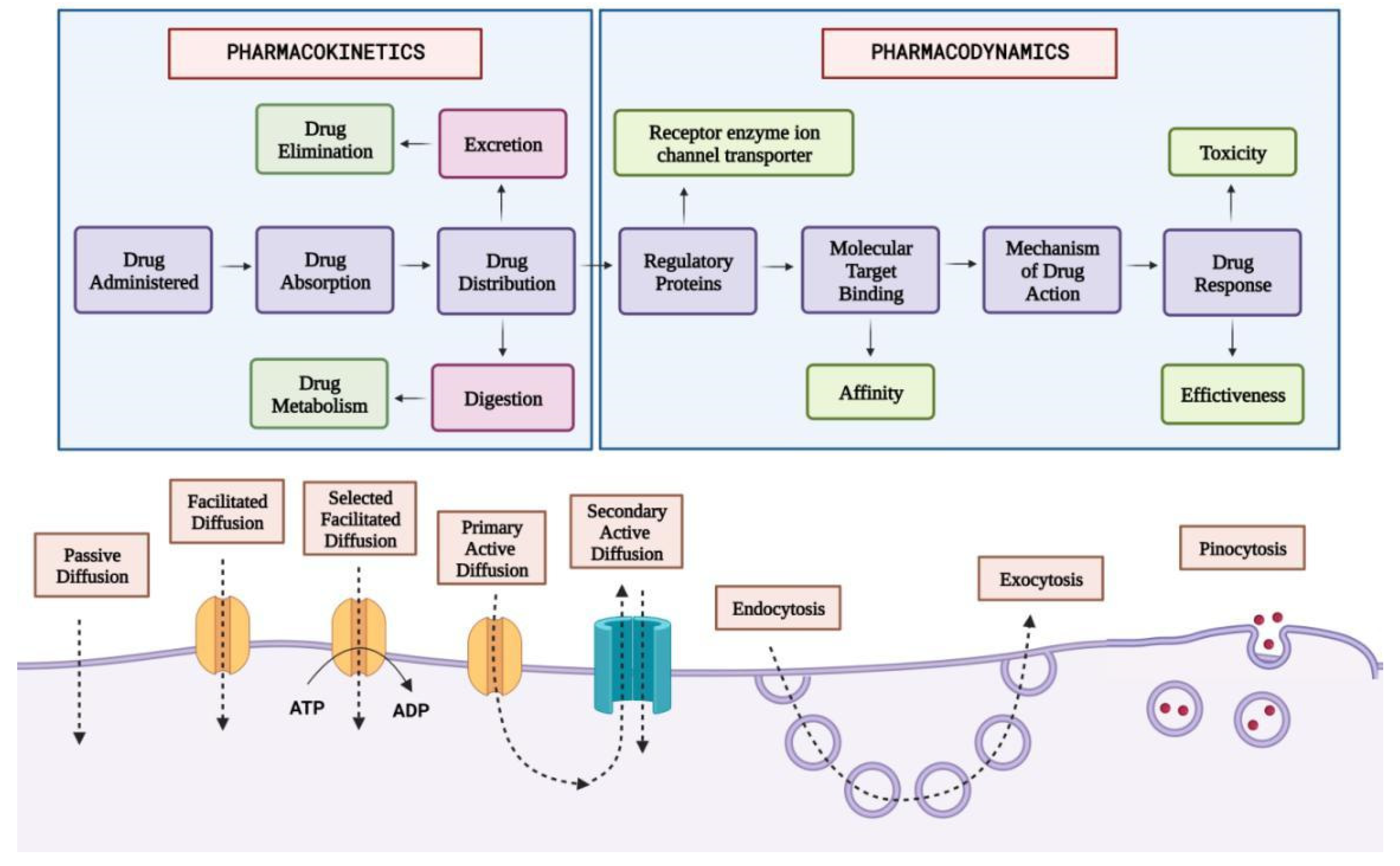
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



