
Submitted:
03 September 2024
Posted:
04 September 2024
You are already at the latest version
Abstract
Nurses continue to experience intense psychological repercussions despite the official conclusion of the COVID-19 pandemic. In this cross-sectional study conducted after the end of the pandemic crisis, in nurses, we evaluated the levels and explored the associations between anger, insomnia and resilience. A total of 442 nurses participated in an online survey and were invited to state their work experience, gender and age and complete the self-report measures of the Dimensions of Anger Reactions-5 (DAR-5), the Athens Insomnia Scale (AIS) and the Brief Resilience Scale (BRS). 62.1% of participants presented with positive scores on the AIS, 41.5% displayed positive values on the DAR-5 scale, whereas 24.9% of nurses demonstrated scores indicative of low resilience on the BRS scale. Regression analysis revealed that 23.5% of the variance in the AIS scores can be attributed to the DAR-5 scores and 3% to the BRS scores. Mediation analysis confirmed the protective role of resilience contributing as a negative mediator in the DAR-5 and the AIS relationship. Screening for insomnia symptoms and anger issues among nurses after the end of the pandemic and implementing appropriate interventions is considered imperative to avoid long-term health consequences.
Keywords:
insomnia
; anger
; resilience
; post-pandemic
; nursing workforce
1. Introduction
The American Psychological Association defines resilience as “the process of adapting effectively in the face of adversity, trauma, tragedy, threats or even significant sources of stress” [1]. Essentially, psychological resilience is the ability to endure, recover and thrive when confronted with stressors and challenging demands. It is a dynamic process that is influenced by various factors including biological, psychological, social and environmental inputs [2]. The pandemic period was particularly stressful [3,4], especially for healthcare workers who have experienced additional pressures [5].
Despite past warnings about impending pandemics [6], the coronavirus pandemic took the health systems by surprise, with shortages of personal protective equipment, ventilators and intensive care beds [7,8]. Public health facilities were often deemed inadequate for the magnitude of the crisis, hospitals in many areas were rapidly overwhelmed, especially during the surge in COVID-19 cases [9,10]. These strains were further intensified for health workers as many of them became sick or were quarantined, leading to increased staff shortages [11,12]. Misinformation and conflicting messages often further complicated the public health response [13,14]. Among health workers, nurses manifested more stress than doctors, making them particularly vulnerable at times when they were most needed [15,16].
The adverse effects of the pressure exerted by the pandemic on health personnel and especially on nurses were evidenced in numerous studies from the beginning to the end of the pandemic, as the psychological and physical burden on nurses was immense [17]. Sleep disorders, nightmares and especially insomnia appeared to be a major problem for healthcare workers and especially for nurses [18,19,20]. It should be emphasized here that sleep is a biological necessity for the maintenance of human life comparable to the need for air, water and food [19,21]. Sleep disturbances are associated with serious physical diseases such as myocardial infarction, hypertension, diabetes [22,23] and major mental disorders such as depression [24,25]. At the same time adequate eight hours of sleep at night is associated with a reduced risk of fatigue-related injuries and errors [20].
In the context of adversity during the pandemic prolonged stress and the perceived threat of COVID-19 triggered feelings of anger among nurses [26]. Anger is one of the basic human emotions [27] that involves a complex set of psychological and physiological reactions to injustice, perceived threats, frustration or even stress [26]. Basic emotions are characterized by the fact that their functioning is essential for adaptation and evolution [28]. Moreover, basic emotions have universal behavioral patterns and most likely an inherent neural substrate [29]. Throughout evolution the adaptive role of anger in human survival has been related to its involvement in the fight-or-flight response [30]. Although anger has an adaptive role, exaggerated expression of anger may be maladaptive [31]. Expressions of anger can manifest as early as at six months of age [32,33] and exhibit cross-cultural homogeneity in their basic characteristics [34]. Anger reactions usually peak in early childhood and remit as children socialize and become more capable of regulating emotions [31].
High levels of anger and insomnia were observed in health care workers [35] and especially in nurses during the pandemic [26]. The relationship between anger and sleep disorders has been highlighted in several studies, which have suggested that high levels of anger are associated with symptoms of disturbed sleep in adults [36] and with insomnia in adolescents [37]. Recent research evidences an association between sleep quality and the anger expression in nurses [38]. The relationship between the two constructs, namely anger and insomnia is complex and possibly bidirectional [39,40]. Although it is difficult to disentangle the direction of causation and excluding studies on sleep quality, few studies have examined the effect of insomnia on anger [41,42,43], but research investigating the effect of anger on insomnia is even more limited [44,45,46] and in conjunction with resilience and their interrelations, in our opinion nonexistent.
The COVID-19 pandemic that first emerged in early 2020 has become a chronic stressor for healthcare workers and nurses in particular. On 5 May 2023, the World Health Organization announced the “conclusion of the global health emergency caused by the coronavirus disease 2019 (COVID-19)”, effectively putting an end to the pandemic crisis [47,48]. However, experience from previous epidemics has shown that the psychological impact on health professionals lasted from several months up to three years after their onset [49]. Four years after the outbreak of the pandemic and with the announcement of its end, one hypothesis that should be explored is whether rates of anger and insomnia have decreased in nursing staff. However, the main purpose of this study was to investigate the protective role of resilience on the relationship between anger and insomnia at the end of the pandemic crisis. The basic assumption was that increased resilience might mitigate the adverse effect of anger on insomnia.
More specifically, the objectives of the present study are to:
- Evaluate the levels of insomnia, anger and resilience three and a half years after the onset of the pandemic and one month after its official conclusion.
- Explore the relationships among anger, insomnia, and resilience.
- Investigate if resilience would negatively mediate the effect of anger on insomnia.
2. Subjects and Methods
2.1. Research Design and Ethical Considerations
To answer the above objectives we conducted a cross-sectional correlational study. From June 1, 2023 to June 31, 2023, we sent 600 invitations, via email, to registered nurses inviting them to participate in the study by answering the self-report questionnaires. The emails were acquired from professional nurses’ associations. The survey employed a convenience sampling methodology, since no statistical randomized method was used for the selection of the invited participants. The invitation message stated the purpose of the study and included an anonymous link to access the online survey platform in Google Forms. We also clarified that participation in the survey was voluntary and that we ensured the anonymity of responses. The study sample included 441 individuals who agreed to participate (73% response rate). This sample was deemed satisfactory as we had more participants than an adequate sample. Given that the total number of employed nurses in Greece was 27,103 [50], a margin of error of 5%, a confidence level of 95%, and a 50% confidence rate, the minimum size was calculated to be 379 employees.
Upon accessing the online survey platform, participants were required to grant online informed consent by answering positively to the question “I agree to participate in this study”, and only with a positive answer they could have access to the questionnaires. This study has been approved by the Clinical Research Ethics Committee of “Sotiria” General Hospital (Number 20649/23). The study adhered to the European Union General Data Protection Regulation (GDPR-2016/679) and was conducted in accordance with the ethical principles as defined by the Declaration of Helsinki.
2.2. Measurement Tools
After providing informed consent, participants were asked to state their work experience, gender and age and subsequently complete the following questionnaires:
a) The Athens Insomnia Scale (AIS)
To evaluate insomnia we used the Athens Insomnia Scale (AIS), a self-assessment tool designed to quantify sleep disturbances in the last month. The designers used the ICD-10 (International Classification of Diseases 10th revision) criteria for insomnia to generate the scale [51,52]. The AIS is a widely used questionnaire consisting of eight items. Each item can be answered on a 4-point Likert scale where 0 is rated as no problem up to 3 indicating severe difficulties. Thus the score can range from 0-32, where higher scores indicate increased sleep problems [53]. A value of 6 is used as a cut-off point to distinguish healthy individuals from those with insomnia. The internal consistency of the scale is high (Cronbach’s α = 0.89) according to the scale’s authors [51], and in the present study Cronbach’s alpha was equal to 0.86.
b) Dimensions of Anger Reactions-5 (DAR-5)
The Dimensions of Anger Reactions-5 (DAR-5) scale [54,55] was used to record anger over the past four weeks. The scale consists of five items, measuring individuals’ anger frequency, intensity, duration, antagonism toward others, and interference with social functioning. Each item can be rated by the respondent on a 5-point Likert scale ranging from 5 = always or almost always to 1 = never or almost never. Thus, the total score of the questionnaire can range from 5 to 25. High scores indicate a severe experience of anger while low scores indicate a low experience of anger. The cut-off point is considered to be 12 while internal consistency is usually satisfactory (Cronbach’s α = 0.81) [26,50].
c) The Brief Resilience Scale (BRS)
We administered the Brief Resilience Scale (BRS) to measure a nurse’s perceived competence in overcoming stress and adversity. The BRS includes six items to which the participant is asked to respond on a five-point Likert scale ranging from strongly disagree (1) to strongly agree (5). The sum of the scale can yield values from 6 to 30, where low values indicate low resilience. To obtain the final score of the scale it is required to divide the sum by the number of items answered by the respondent. Values lower than 2.99 indicate low resilience and values higher than 4.30 indicate high resilience [56,57]. The internal consistency of the BRS is considered high as reported from previous studies (Cronbach’s α = 0.86) [58]. The Cronbach’s alpha coefficient in this study was α = 083.
2.3. Statistical Analysis
Since the study employed a convenience sampling method it was necessary to examine with the use of chi-square (χ2) and t-test if this sample was representative in terms of gender, age and years of work as to the general population of nurses in Greece [50,59]. Descriptive statistics served so that continuous variables could be expressed in means and standard deviations. We performed t-test to compare the values of the variables in the present study with values of the same variables during the pandemic from previous studies in the same population. We compared the means of the continuous variables of the present study as to gender by t-test. In order to estimate the effect size of the t-test results we used Hedges’ g, since in all cases the group sizes we compared were not equal. Values of g close to 0.2 indicate a small effect size, values close to 0.5 a moderate effect size and values close to 0.8 a high effect size. We tested for correlations between continuous variables with Pearson’s correlation analysis. We verified whether the linear regression assumptions (normality, homoscedasticity, independence, and linear relationship) were satisfied. We constructed a regression model to investigate whether the correlated variables were significant predictors of insomnia. Simple mediation analysis was performed using Hayes SPSS Process Macro v4.0 (model 4) [60,61]. In all analyses, statistical significance was set at p<0.05 (two-tailed). IBM SPSS Statistics 23 software was utilized for all statistical analyses (IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp).
3. Results
Initially, to ensure the representativeness of the sample we compared the characteristics of the sample of this study with the target population i.e., the total number of working nurses in Greece [59]. No statistical difference was found as to gender (χ2 p>0.05). No statistical difference was found regarding age (sample t-test p>0.05) or years of work (sample t-test p>0.05). In the Athens Insomnia Scale, 62.1% of the sample scored above ≥ 6. In the Dimensions of Anger Reactions-5 a percentage of 41.5% displayed values ≥12. In the Brief Resilience Scale a percentage of 11.1% exhibited high resilience with values >4.30 while a rate of 24.9% demonstrated low resilience with values <2.99.
In the present study nurse participants scored a mean of 7.32±4.15 in the insomnia scale (Table 1). This value was significantly higher (sample t-test p<0.01) than the value of 5.98±4.24 (Hedges’ g: 0.32) recorded at the beginning of the pandemic in Greek nurses [19] and did not differ from the value of 7.15±4.34 (sample t-test p>0.05) presented in a similar study conducted in the second year of the pandemic at the end of 2021 [62].
Also, nurse participants from this study evidenced higher scores on the DAR-5 scale 11.24±3.85 (Table 1), (sample t-test p<0.01, Hedges’ g: 0.25) compared with the values of 10.31±3.53 recorded in another study at the beginning of the pandemic in Greek nurses using the DAR-5 scale [26].
Meanwhile, the mean resilience score in this study was 3.40±0.78 (Table 1) significantly lower (sample t-test p<0.01, Hedges’ g: 0.28) compared to the value of 3.61±0.80 observed in a study from the initial phase of the pandemic [58].
Investigating the correlations among continuous variables, the expected association between age and work experience was observed, but at the same time age displayed a negative correlation with scores on the Athens Insomnia Scale and a positive correlation with scores on the Brief Resilience Scale (Table 2). Scores on the Athens Insomnia Scale exhibited negative correlations with scores on the Brief Resilience Scale and positive correlations with the Dimensions of Anger Reactions-5 scale. Negative correlations were evidenced between scores on the Dimensions of Anger Reactions-5 scale and scores on the Brief Resilience Scale.
Before performing multiple regression analysis we examined whether the necessary assumptions were satisfied. We checked normality, by visual inspection of the predicted probability plots (PP). We examined homoscedasticity through visual inspection of the scatter plot of predicted values standardized by regression and standardized regression residuals. The value of 1.94 (Table 3) in the Durbin-Watson test supports the independence of the residuals while the values in the Variance Inflation Factor Analysis (VIF) declared the absence of multicollinearity (Table 3).
To determine which variables best explained the variance in the Athens Insomnia Scale scores we conducted a multiple regression analysis with the Stepwise method. Insomnia was defined as the dependent variable while we set gender, work experience, age, anger as expressed by the Dimensions of Anger Reactions-5 and resilience as recorded by the Brief Resilience Scale as independent variables. The anger scale explained 23.5% of the insomnia scale’s variance and an additional 5.8% was explained by the resilience scale (Table 3). The remaining variables were not statistically involved in explaining insomnia.
To investigate whether resilience mediates the anger-insomnia relationship we used Hayes SPSS Process Macro model 4, based on an analysis of 5000 bootstrap samples. For this purpose, the Brief Resilience Scale was set as the mediator variable, the Athens Insomnia Scale as the outcome variable and the Dimensions of Anger Reactions-5 as a predictor variable. In addition, age and work experience were entered as covariates.
Mediation analysis confirmed our hypothesis that the Brief Resilience Scale negatively mediated the relationship between the Dimensions of Anger Reactions-5 and the Athens Insomnia Scale (Figure 1 and Table 4). Brief Resilience Scale had a statistically significant but indirect effect [b = 0.1154, 95% CI (0.0712, 0.1669), p ≤ 0.01], as in the presence of the mediator (the Brief Resilience Scale) the direct effect of the Dimensions of Anger Reactions-5 on the Athens Insomnia Scale was still statistically significant [b = 0.4074, 95% CI (0.3144, 0.5004), p ≤ 0.001). The model explained 22% of the variance in the outcome variable, the Athens Insomnia Scale (Table 4). The variables used as covariates did not display statistically significant relationships.
4. Discussion
The psychological burden placed on nurses had been documented prior to the COVID-19 pandemic [63,64]; however, the unique circumstances of the pandemic dramatically compromised the mental health of nurses. The increased levels of insomnia observed in this study are likely to reflect this deterioration in nurses’ overall mental health. In this study, at the end of the pandemic crisis, a percentage of 62% of participants were symptomatic of insomnia, compared to a rate of 49.7% who were symptomatic in the first year of the pandemic, and not significantly different from the 61.4% in the second year of the pandemic. Studies from around the world confirm that sleep disorders in nurses were a significant problem during the pandemic crisis. In countries where we have comparable data it seems that in the second year of the pandemic we have a peak in sleep disorders in nurses. A study in China, using the Athens Insomnia Scale in the first year of the pandemic (March 2020), reports a rate of 41.5% [65] while in a similar study conducted in the second year (March 2021) of the pandemic in China, insomnia symptoms in nurses escalated to 57.3% [66]. In Greece, high rates of insomnia symptoms remained almost invariable until the end of the pandemic crisis [20,62].
The factors responsible for this increase in insomnia rates between the first and the following years of the pandemic could be numerous; first the course of the pandemic itself and the fatigue it progressively induced to the nursing staff [17], or even the gradual emergence of posttraumatic stress disorder (PTSD) symptoms associated with sleep disorders [66,67]. From a different perspective, we can focus on the protective factors that are beneficial to sleep, such as resilience. Resilience in Greek nurses was reduced at the end of the pandemic crisis compared to measurements in the first year of the pandemic [58]. Another study examining an additional positive factor, family support in Greek nurses, found a similar decline in family support after the first year of the pandemic [19]. It is possible that positive factors were increased in the first year of the pandemic among nurses because of the popularity and even heroism that the profession experienced at the beginning of the pandemic crisis [26,68] that began to fade in the following months. We cannot prove this, but we can assume that the sense of heroism significantly curtailed the sense of anger during the first year of the pandemic.
During the first year of the pandemic the extremely unfavourable conditions, which have been highlighted in many studies, fully justified the high level of anger experienced by the health personnel. However, we would expect that the normalization of living conditions would reduce the sense of anger rather than increase it. We cannot rule out factors such as trauma or PTSD, also prevalent in veteran soldiers, being responsible for the high sense of anger observed in this study’s sample [44,69,70,71]. Research suggests that problematic anger is increased and remained stable across time in repeat military combat recruits compared to first-time service members, as the protective effect of resilience on anger prior to enlistment in the military campaigns is weakened over time [72]. An analogue is viewed in repeated waves of the COVID-19 that probably have a cumulative impact and inflict similar deleterious effects on nurses, undermining resilience and resulting in signs of burnout [73,74,75]. Nurses experienced the COVID-19 pandemic as an ongoing stressor of uncertain duration and overactivation of the stress system could lower the threshold for problematic anger, effectuating more chronically elevated anger levels [72,76,77]. Whereas in military settings anger may be more acceptable than other negative emotions [78], in the context of nursing anger expression may severely compromise the performance and quality of work and adversely impact upon sleep quality [38,79,80]. Existing evidence implicates anger in sleep disorders especially the anger-control deficits [45].
From a neural perspective insomnia and anger share the same neurobiological substrate associated with abnormal functioning of the amygdale, the ventral anterior cingulate cortex and the medial prefrontal cortex [42]. As previously stated, anger and sleep probably have a bidirectional relationship, yet in this study we argued that anger predicts insomnia and, specifically the study claims that over 23% of the variance in insomnia can be explained by anger. A plausible explanation of how anger contributes to insomnia relies on the cognitive process of rumination of hostile thoughts that are responsible for both maintaining and increasing anger prior to the sleep process [45,81,82,83]. Thus, feelings of anger before sleep onset along with pre-sleep cognitive rumination on an anger provoking stimulus result in physiological and cognitive arousal compromising sleep initiation and maintenance [84,85,86]. However, we should point out that in the literature there is also the opposite view that insomnia and poor sleep are responsible for increased feelings of anger. Studies suggest that the quality of sleep the previous night predicted the frequency of anger the next day [87,88] and that the frequency of anger on the current day had no effect on sleep quality [87]. It should be emphasized, though, that the majority of the literature supporting that disturbed sleep is a predictor of anger derives from observations in forensic studies and in studies of psychiatric patients, specifically suggesting that disrupted sleep is a risk factor for impulsive or reactive aggression [89,90].
Hyperarousal and stress dysregulation are implicated in insomnia aetiology [91,92]. Exposure to similar amounts of stress which acts as a precipitating insomnia factor has diverse sleep disturbance consequences among individuals, due to differences in sleep reactivity, which functions both as predisposing and as a perpetuating factor of insomnia [93,94]. Other specific perpetuating factors significantly involved in maintaining persistent insomnia symptoms are sleep effort and pre-sleep cognitive arousal [95]. Insomnia and anger are intimately linked to stress, in the way that the impact of stress on sleep also depends on emotion regulation [96,97]. Research suggests that insomnia after stressful life events is more common among individuals with higher state anger than those without insomnia even after stressful experiences [43]. In this sense, stress-related insomnia is an indicator of sleep reactivity [98] and higher sleep reactivity is related to anger [43]. Sleep reactivity and cognitive-emotional reactivity in response to stress and emotional distress has been associated with the high comorbidity between insomnia and depression [93]. Importantly, REM sleep interferes with emotion regulation through the overnight resolution of emotional distress, a process that is disrupted in insomnia indirectly giving rise to hyperarousal, which further perpetuates insomnia [99].
In the present study resilience displayed a negative association with both anger and insomnia and even mediated their relationship, reducing the adverse effects of anger on sleep. We cannot, however, argue with certainty about the mechanism through which resilience interferes with this relationship and future studies may be able to provide more evidence. One possible speculation, supported by a recent study, is that resilience acts as a moderator in the relationship between rumination and sleep quality [100]. The study suggests that at high levels of resilience the impact from daily stressful life events and rumination on sleep quality is expected to be reduced, whereas at low levels of resilience it is expected to be increased [100].
Studies confirm that resilience is compromised among individuals with insomnia compared to good sleepers [101,102,103], reflecting their low capacity to overcome stress which may influence their ability to regulate emotions and arousal, in turn contributing to the maintenance of insomnia [102,103,104]. Differently, emotion dysregulation may impact the relationship between limited capacity to adapt to stress and pre-sleep hyperarousal, creating a vicious cycle that contributes to the chronicity of insomnia [103,105]. Recent research supports that maladaptive emotion regulation strategies undermine the favourable effect of resilience on sleep [106]. In our study resilience successfully counteracted the effects of anger on insomnia. In accordance, previous studies suggest that resilience has the ability to attenuate feelings of anger and effectively suppresses insomnia [20,58].
Aforementioned considerable findings hold clinical implications [107,108] and underscore the importance of screening for sleep problems and anger issues in nursing personnel after the end of the pandemic. Available effective interventions include evidence-based cognitive behavioural therapies for insomnia [109,110], mindfulness based cognitive behavioural therapy for anger [111] and educational programs to enhance resilience [112].
This study has several limitations. The shortcomings of self–report measures employed, specifically concerning the retrospective assessment of the variables, could have introduced a more subjective dimension and/or bias. The cross-sectional design of the study would not permit causal inferences and in this way results from the study could be interpreted as indicating that insomnia predicts anger and not vice-versa. Future longitudinal investigations could clarify this discrepancy, considering additional reciprocal associations between insomnia and anger. The convenience sampling methodology of the study might have affected the sample’s representativity and the collected data accuracy. Moreover, we did not evaluate stress, other mental health problems, specific sleep-related constructs (i.e., sleep reactivity, chronotypes), personal life-stressors, or other work related factors, personality traits and/or emotion regulation strategies [19,113,114]. Additionally, this study did not include important positive factors such as sense of coherence [115,116], social [117] and family support [19,118] or even the sense of religiosity [119] that could act protectively. Also, gender disproportionality prohibited the generalizabiliy of the results to other populations. Finally, excluding nurses without internet access was an important drawback, as was the lack of information about nurses’ working department, shifts at work, rotation and staff shortages.
5. Conclusions
Persistently elevated rates of insomnia and anger are recorded among nursing professionals after the end of the pandemic, whereas self-reported resilience seems to diminish over time. More than six out of ten nurses admit insomnia symptoms; four out of ten nurses experience anger emotions and one in four nurses exhibits low resilience. Anger exacerbates insomnia and resilience counteracts anger and insomnia. The protective role of resilience is confirmed as it mediates the relationship between anger and insomnia and successfully ameliorates anger and suppresses insomnia. Elevated anger emotions and compromised resilience may contribute to insomnia symptoms perpetuation. In the post-pandemic era urgent screening for insomnia symptoms among nurses and implementing the necessary interventions is of outmost importance.
Author Contributions
Conceptualization, Ar.P., C.S. and A.T.; methodology, As.P., E.K. and A.T.; software, N.S., M.I., M.M. and C.S.; validation, Ar.P., N.S., M.I and C.S.; formal analysis, Ar.P., I.I and A.T.; investigation, As.P, C.S. and A.T.; resources, Ar.P. and I.I.; data curation, N.S., M.I., C.S. and A.T.; writing—original draft preparation, Ar.P., M.M. and A.T.; writing—review and editing, Ar.P., As.P., M.M. and C.S.; supervision, Ar.P. and A.T.; project administration, A.P. and A.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Clinical Research Ethics Committee of “Sotiria” General Hospital (Number 20649/23).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, [A.T.], upon reasonable request.
Acknowledgments
We would like to thank all participants in our study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Denckla, C. A., Cicchetti, D., Kubzansky, L. D., Seedat, S., Teicher, M. H., Williams, D. R., & Koenen, K. C. (2020). Psychological resilience: An update on definitions, a critical appraisal, and research recommendations. European Journal of Psychotraumatology, 11(1), 1822064.
- Ungar, M., & Theron, L. (2020). Resilience and mental health: How multisystemic processes contribute to positive outcomes. The Lancet Psychiatry, 7(5), 441-448.
- Tselebis, A.; Pachi, A. Primary Mental Health Care in a New Era. Healthcare 2022, 10, 2025. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, A., & Ghosh, T. (2022). COVID-19 pandemic and stress: coping with the new normal. Journal of Prevention and Health Promotion, 3(1), 30-52.
- ittzen-Brown C, Dolan H, Norton A, Bethel C, May J, Rainbow J. Unbearable suffering while working as a nurse during the COVID-19 pandemic: A qualitative descriptive study. Int J Nurs Stud Adv. 2023 Dec;5:100127. doi: 10.1016/j.ijnsa.2023.100127. Epub 2023 Apr 12. [CrossRef] [PubMed]
- Mahroum, N., Seida, I., Esirgün, S. N., & Bragazzi, N. L. (2022). The COVID-19 pandemic–How many times were we warned before? European Journal of Internal Medicine, 105, 8-14.
- Cohen, J., & van der Meulen Rodgers, Y. (2020). Contributing factors to personal protective equipment shortages during the COVID-19 pandemic. Preventive medicine, 141, 106263.
- World Health Organization, 2. (2020). Rational use of personal protective equipment for coronavirus disease (COVID-19) and considerations during severe shortages: interim guidance, 6 April 2020 (No. WHO/2019-nCov/IPC_PPE_use/2020.3). World Health Organization.
- Sen-Crowe, B., Sutherland, M., McKenney, M., & Elkbuli, A. (2021). A closer look into global hospital beds capacity and resource shortages during the COVID-19 pandemic. Journal of Surgical Research, 260, 56-63.
- McCabe, R., Schmit, N., Christen, P., D’Aeth, J. C., Løchen, A., Rizmie, D., … & Hauck, K. (2020). Adapting hospital capacity to meet changing demands during the COVID-19 pandemic. BMC medicine, 18, 1-12.
- Khubchandani, J.; Bustos, E.; Chowdhury, S.; Biswas, N.; Keller, T. COVID-19 Vaccine Refusal among Nurses Worldwide: Review of Trends and Predictors. Vaccines 2022, 10, 230. [Google Scholar] [CrossRef] [PubMed]
- Ferland, L.; Carvalho, C.; Dias, J.G.; Lamb, F.; Adlhoch, C.; Suetens, C.; Beauté, J.; Kinross, P.; Plachouras, D.; Hannila-Handelberg, T.; et al. Risk of hospitalization and death for healthcare workers with COVID-19 in nine European countries, January 2020–January 2021. J. Hosp. Infect. 2022. [Google Scholar] [CrossRef] [PubMed]
- Roozenbeek, J., Schneider, C. R., Dryhurst, S., Kerr, J., Freeman, A. L., Recchia, G., … & Van Der Linden, S. (2020). Susceptibility to misinformation about COVID-19 around the world. Royal Society open science, 7(10), 201199.
- Milionis, C.; Ilias, I.; Tselebis, A.; Pachi, A. Psychological and Social Aspects of Vaccination Hesitancy—Implications for Travel Medicine in the Aftermath of the COVID-19 Crisis: A Narrative Review. Medicina 2023, 59, 1744. [Google Scholar] [CrossRef] [PubMed]
- Couarraze S, Delamarre L, Marhar F, Quach B, Jiao J, Avilés Dorlhiac R, Saadaoui F, Liu AS, Dubuis B, Antunes S, Andant N, Pereira B, Ugbolue UC, Baker JS; COVISTRESS network; Clinchamps M, Dutheil F. The major worldwide stress of healthcare professionals during the first wave of the COVID-19 pandemic - the international COVISTRESS survey. PLoS One. 2021 Oct 6;16(10):e0257840. [CrossRef] [PubMed] [PubMed Central]
- Wang, H., Liu, Y., Hu, K., Zhang, M., Du, M., Huang, H., & Yue, X. (2020). Healthcare workers’ stress when caring for COVID-19 patients: An altruistic perspective. Nurs Ethics. 2020 Nov;27(7):1490-1500. Epub 2020 Jul 14. [CrossRef] [PubMed]
- Sikaras C, Ilias I, Tselebis A, Pachi A, Zyga S, Tsironi M, Gil APR, Panagiotou A. Nursing staff fatigue and burnout during the COVID-19 pandemic in Greece. AIMS Public Health. 2021 Nov 23;9(1):94-105. [CrossRef]
- Pappa, S., Ntella, V., Giannakas, T., Giannakoulis, V. G., Papoutsi, E., & Katsaounou, P. (2020). Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain, behavior, and immunity, 88, 901-907.
- Tselebis A, Lekka D, Sikaras C, Tsomaka E, Tassopoulos A, Ilias I, Bratis D, Pachi A. Insomnia, Perceived Stress, and Family Support among Nursing Staff during the Pandemic Crisis. Healthcare. 2020; 8(4):434. [CrossRef]
- Pachi, A., Tselebis, A., Sikaras, C., Sideri, E. P., Ivanidou, M., Baras, S., … & Ilias, I. (2024). Nightmare distress, insomnia and resilience of nursing staff in the post-pandemic era. AIMS Public Health, 11(1), 36-57.
- Tucker, M. A. (2020). The value of sleep for optimizing health. Nutrition, Fitness, and Mindfulness: An Evidence-Based Guide for Clinicians, 203-215.
- Chaput, J.-P.; McNeil, J.; Després, J.-P.; Bouchard, C.; Tremblay, A. Seven to Eight Hours of Sleep a Night Is Associated with a Lower Prevalence of the Metabolic Syndrome and Reduced Overall Cardiometabolic Risk in Adults. PLoS ONE 2013, 8, e72832. [Google Scholar] [CrossRef]
- Puri, S., Herrick, J. E., Collins, J. P., Aldhahi, M., & Baattaiah, B. (2017). Physical functioning and risk for sleep disorders in US adults: results from the National Health and Nutrition Examination Survey 2005–2014. Public Health, 152, 123-128.
- Berk, M. Sleep and depression—theory and practice. Aust Fam Physician. 2009;38: 302–304. [PubMed]
- Faulkner, S., & Bee, P. (2016). Perspectives on sleep, sleep problems, and their treatment, in people with serious mental illnesses: a systematic review. PLoS One, 11(9), e0163486.
- Pachi A, Anagnostopoulou M, Antoniou A, Papageorgiou SM, Tsomaka E, Sikaras C, Ilias I, Tselebis A. Family support, anger and aggression in health workers during the first wave of the pandemic. AIMS Public Health. 2023 Jun 15;10(3):524-537. [CrossRef]
- Williams, R. Anger as a Basic Emotion and Its Role in Personality Building and Pathological Growth: The Neuroscientific, Developmental and Clinical Perspectives. Front Psychol. 2017 Nov 7;8:1950. [CrossRef] [PubMed]
- Ekman, P. (1992). An argument for basic emotions. Cognition & emotion, 6(3-4), 169-200.
- Ekman, P. (1999). Basic emotions. Handbook of cognition and emotion, 98(45-60), 16.
- Berkowitz, L., & Harmon-Jones, E. (2004). Toward an understanding of the determinants of anger. Emotion, 4(2), 107–130. [CrossRef]
- Liu C, Moore GA, Beekman C, Pérez-Edgar KE, Leve LD, Shaw DS, Ganiban JM, Natsuaki MN, Reiss D, Neiderhiser JM. Developmental patterns of anger from infancy to middle childhood predict problem behaviors at age 8. Dev Psychol. 2018 Nov;54(11):2090-2100. Epub 2018 Sep 27. [CrossRef] [PubMed] [PubMed Central]
- Izard, C. E., Fantauzzo, C. A., Castle, J. M., Haynes, O. M., Rayias, M. F., & Putnam, P. H. (1995). The ontogeny and significance of infants’ facial expressions in the first 9 months of life. Developmental psychology, 31(6), 997 –1013.
- Lewis, M., Ramsay, D. S., & Sullivan, M. W. (2006). The relation of ANS and HPA activation to infant anger and sadness response to goal blockage. Developmental Psychobiology: The Journal of the International Society for Developmental Psychobiology, 48(5), 397-405.
- Matsumoto, D., Yoo, S. H., & Chung, J. (2010). The expression of anger across cultures. In M. Potegal, G. Stemmler, & C. Spielberger (Eds.), International handbook of anger: Constituent and concomitant biological, psychological, and social processes (pp. 125–137). Springer Science + Business Media. [CrossRef]
- Söğütlü, Y., Söğütlü, L., & Göktaş, S. Ş. (2021). Relationship of COVID-19 pandemic with anxiety, anger, sleep and emotion regulation in healthcare professionals. Journal of Contemporary Medicine, 11(1), 41-49.
- Shin, C., Kim, J., Yi, H., Lee, H., Lee, J., & Shin, K. (2005). Relationship between trait-anger and sleep disturbances in middle-aged men and women. Journal of Psychosomatic Research, 58(2), 183-189.
- Sisman, F. N., Basakci, D., & Ergun, A. (2021). The relationship between insomnia and trait anger and anger expression among adolescents. Journal of child and adolescent psychiatric nursing, 34(1), 50-56.
- Sevgi Aldemir & Gülay Taşdemır Yiğitoğlu. The Relation Between Sleep Quality and Anger Expression That Occur in Nurses: A Cross-Sectional Study. Journal of Radiology Nursing 43 (2024) 60-67.
- Kahn M, Sheppes G, Sadeh A. Sleep and emotions: bidirectional links and underlying mechanisms. Int J Psychophysiol. 2013 Aug;89(2):218-28. Epub 2013 May 24. [CrossRef] [PubMed]
- Ten Brink M, Dietch JR, Tutek J, Suh SA, Gross JJ, Manber R. Sleep and affect: A conceptual review. Sleep Med Rev. 2022 Oct;65:101670. Epub 2022 Aug 18. [CrossRef] [PubMed]
- Z Krizan, A Miller, G Hisler, 0276 Does Losing Sleep Unleash Anger?, Sleep, Volume 43, Issue Supplement_1, April 2020, Page A105. [CrossRef]
- Saghir Z, Syeda JN, Muhammad AS, Balla Abdalla TH. The Amygdala, Sleep Debt, Sleep Deprivation, and the Emotion of Anger: A Possible Connection? Cureus. 2018 Jul 2;10(7):e2912. [CrossRef] [PubMed]
- Jichul Kim, Chang Woo Lee, Sehyun Jeon, Bum Joon Seok, and Seog Ju Kim. Anger Associated with Insomnia and Recent Stressful Life Events in Community-Dwelling Adults. Chronobiol Med 2019;1(4):163-167.
- Miles SR, Pruiksma KE, Slavish D, Dietch JR, Wardle-Pinkston S, Litz BT, Rodgers M, Nicholson KL, Young-McCaughan S, Dondanville KA, Nakase-Richardson R, Mintz J, Keane TM, Peterson AL, Resick PA, Taylor DJ; Consortium to Alleviate PTSD. Sleep disorder symptoms are associated with greater posttraumatic stress and anger symptoms in US Army service members seeking treatment for posttraumatic stress disorder. J Clin Sleep Med. 2022 Jun 1;18(6):1617-1627. [CrossRef] [PubMed]
- Hisler, G., & Krizan, Z. (2017). Anger tendencies and sleep: Poor anger control is associated with objectively measured sleep disruption. Journal of Research in Personality, 71, 17–26. [CrossRef]
- Krizan Z, Hisler G. Sleepy anger: Restricted sleep amplifies angry feelings. J Exp Psychol Gen. 2019 Jul;148(7):1239-1250. Epub 2018 Oct 25. [CrossRef] [PubMed]
- Wise J (2023) Covid-19: WHO declares end of global health emergency. BMJ 2023;381:p1041. [CrossRef]
- Harris E (2023) WHO declares end of COVID-19 global health emergency. JAMA 329: 1817. [CrossRef]
- Preti E, Di Mattei V, Perego G, et al. The Psychological Impact of Epidemic and Pandemic Outbreaks on Healthcare Workers: Rapid Review of the Evidence. Curr Psychiatry Rep. 2020;22:43.
- Tselebis A, Sikaras C, Milionis C, Sideri EP, Fytsilis K, Papageorgiou SM, Ilias I, Pachi A. A Moderated Mediation Model of the Influence of Cynical Distrust, Medical Distrust, and Anger on Vaccination Hesitancy in Nursing Staff. European Journal of Investigation in Health, Psychology and Education. 2023; 13(11):2373-2387. [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: Validation of an instrument based on ICD-10 criteria. J. Psychosom. Res. 2000, 48, 555–600. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. The diagnostic validity of the Athens Insomnia Scale. J. Psychosom. Res. 2002, 55, 263–267. [Google Scholar] [CrossRef]
- Eleftheriou, A., Rokou, A., Arvaniti, A., Nena, E., & Steiropoulos, P. (2021). Sleep quality and mental health of medical students in Greece during the COVID-19 pandemic. Frontiers in public health, 9, 775374.
- Kim, H.J.; Lee, D.H.; Kim, J.H.; Kang, S.-E. Validation of the Dimensions of Anger Reactions Scale (the DAR-5) in non-clinical South Korean adults. BMC Psychol 11, 74 (2023). [CrossRef]
- Forbes, D.; Alkemade, N.; Hopcraft, D.; Hawthorne, G.; O’halloran, P.; Elhai, J.D.; McHugh, T.; Bates, G.; Novaco, R.W.; Bryant, R.; et al. Evaluation of the Dimensions of Anger Reactions-5 (DAR-5) Scale in combat veterans with posttraumatic stress disorder. J. Anxiety Disord. 2014, 28, 830–835. [Google Scholar] [CrossRef]
- Smith, B. W., Dalen, J., Wiggins, K., Tooley, E., Christopher, P., & Bernard, J. (2008). The brief resilience scale: assessing the ability to bounce back. International journal of behavioral medicine, 15, 194-200.
- Kyriazos TA, Stalikas A, Prassa K, et al. (2018) Psychometric evidence of the Brief Resilience Scale (BRS) and modeling distinctiveness of resilience from depression and stress. Psychology 9: 1828-1857.
- Pachi, A.; Kavourgia, E.; Bratis, D.; Fytsilis, K.; Papageorgiou, S.M.; Lekka, D.; Sikaras, C.; Tselebis, A. Anger and Aggression in Relation to Psychological Resilience and Alcohol Abuse among Health Professionals during the First Pandemic Wave. Healthcare 2023, 11, 2031. [Google Scholar] [CrossRef]
- Tziallas D, Goutzias E, Konstantinidou E, et al. Quantitative and qualitative assessment of nurse staffing indicators across NHS public hospitals in Greece. Hell J Nurs. 2018;57:420–449.
- Hayes A F, Rockwood N J (2020) Conditional process analysis: Concepts, computation, and advances in the modeling of the contingencies of mechanisms. Am Behav Sci 64: 19-54. [CrossRef]
- Hayes AF (2015) An index and test of linear moderated mediation. Multivariate Behav Res 50: 1-22. [CrossRef]
- Sikaras, C., Tsironi, M., Zyga, S., & Panagiotou, A. (2023). Anxiety, insomnia and family support in nurses, two years after the onset of the pandemic crisis. AIMS Public Health, 10(2), 252.
- Cheung, T., & Yip, P. S. (2015). Depression, anxiety and symptoms of stress among Hong Kong nurses: a cross-sectional study. International journal of environmental research and public health, 12(9), 11072-11100.
- Tselebis, A., Gournas, G., Tzitzanidou, G., Panagiotou, A., & Ilias, I. (2006). Anxiety and depression in Greek nursing and medical personnel. Psychological Reports, 99(1), 93-96.
- Shen, Y., Zhan, Y., Zheng, H., Liu, H., Wan, Y., & Zhou, W. (2021). Anxiety and its association with perceived stress and insomnia among nurses fighting against COVID-19 in Wuhan: a cross-sectional survey. Journal of Clinical Nursing, 30(17-18), 2654-2664.
- Lu, M. Y., Ahorsu, D. K., Kukreti, S., Strong, C., Lin, Y. H., Kuo, Y. J., … & Ko, W. C. (2021). The prevalence of post-traumatic stress disorder symptoms, sleep problems, and psychological distress among COVID-19 frontline healthcare workers in Taiwan. Frontiers in psychiatry, 12, 705657.
- McLay RN, Klam WP, Volkert SL. Insomnia is the most commonly reported symptom and predicts other symptoms of post-traumatic stress disorder in U.S. service members returning from military deployments. Mil Med. 2010 Oct;175(10):759-62. [CrossRef] [PubMed]
- Cox CL. ‘Healthcare Heroes’: problems with media focus on heroism from healthcare workers during the COVID-19 pandemic. J Med Ethics Aug. 2020;46:510–513. [CrossRef]
- Zhan, N., Zhang, L., Gong, M., & Geng, F. (2024). Clinical correlates of irritability, anger, hostility, and aggression in posttraumatic stress disorder. Psychological Trauma: Theory, Research, Practice, and Policy, 16(6), 1055–1062. [CrossRef]
- McFall ME, Wright PW, Donovan DM, Raskind M. Multidimensional assessment of anger in Vietnam veterans with posttraumatic stress disorder. Compr Psychiatry. 1999 May-Jun;40(3):216-20. [CrossRef] [PubMed]
- Forbes, D. Forbes, D., Metcalf, O., Lawrence-Wood, E. et al. Problematic Anger in the Military: Focusing on the Forgotten Emotion. Curr Psychiatry Rep 24, 789–797 (2022). [CrossRef]
- Campbell-Sills L, Kautz JD, Choi KW, et al. Effects of prior deployments and perceived resilience on anger trajectories of combat-deployed soldiers. Psychological Medicine. 2023;53(5):2031-2040. [CrossRef]
- Marey-Sarwan I, Hamama-Raz Y, Asadi A, Nakad B, Hamama L. “It’s like we’re at war”: Nurses’ resilience and coping strategies during the COVID-19 pandemic. Nurs Inq. 2022 Jul;29(3):e12472. doi: 10.1111/nin.12472. Epub 2021 Nov 1. [CrossRef] [PubMed]
- Manchia M, Gathier AW, Yapici-Eser H, Schmidt MV, de Quervain D, van Amelsvoort T, Bisson JI, Cryan JF, Howes OD, Pinto L, van der Wee NJ, Domschke K, Branchi I, Vinkers CH. The impact of the prolonged COVID-19 pandemic on stress resilience and mental health: A critical review across waves. Eur Neuropsychopharmacol. 2022 Feb;55:22-83. Epub 2021 Oct 29. [CrossRef] [PubMed]
- Wolotira EA. Trauma, Compassion Fatigue, and Burnout in Nurses: The Nurse Leader’s Response. Nurse Lead. 2023 Apr;21(2):202-206. Epub 2022 May 13. [CrossRef] [PubMed]
- Smid, G. E., Kleber, R. J., Rademaker, A. R., van Zuiden, M., & Vermetten, E. (2013). The role of stress sensitization in progression of posttraumatic distress following deployment. Social Psychiatry and Psychiatric Epidemiology, 48(11), 1743–1754. [CrossRef]
- Russo JE, Dhruve DM, Oliveros AD. Coping with COVID-19: Testing the stress sensitization hypothesis among adults with and without a history of adverse childhood experiences. J Affect Disord Rep. 2022 Dec;10:100379. Epub 2022 Jul 3. [CrossRef] [PubMed]
- Adler, A. B., Brossart, D. F., & Toblin, R. L. (2017). Can anger be helpful?: Soldier perceptions of the utility of anger. The Journal of Nervous and Mental Disease, 205(9), 692–698. [CrossRef]
- Lee HY, Jang MH, Jeong YM, Sok SR, Kim AS. Mediating Effects of Anger Expression in the Relationship of Work Stress with Burnout among Hospital Nurses Depending on Career Experience. J Nurs Scholarsh. 2021 Mar;53(2):227-236. Epub 2021 Feb 1. [CrossRef] [PubMed]
- La IS, Yun EK. Effects of Trait Anger and Anger Expression on Job Satisfaction and Burnout in Preceptor Nurses and Newly Graduated Nurses: A Dyadic Analysis. Asian Nurs Res (Korean Soc Nurs Sci). 2019 Oct;13(4):242-248. Epub 2019 Sep 26. [CrossRef] [PubMed]
- Wilkowski BM, Robinson MD. The anatomy of anger: an integrative cognitive model of trait anger and reactive aggression. J Pers. 2010 Feb;78(1):9-38. [CrossRef] [PubMed]
- Palagini L, Moretto U, Dell’Osso L, Carney C, Sleep-related cognitive processes, arousal, and emotion dysregulation in insomnia disorder: the role of insomnia-specific rumination, Sleep Medicine, Volume 30, 2017, Pages 97-104, ISSN 1389-9457. [CrossRef]
- Kalmbach DA, Buysse DJ, Cheng P, Roth T, Yang A, Drake CL. Nocturnal cognitive arousal is associated with objective sleep disturbance and indicators of physiologic hyperarousal in good sleepers and individuals with insomnia disorder. Sleep Med. 2020 Jul;71:151-160. Epub 2019 Nov 14. [CrossRef] [PubMed]
- Vandekerckhove M, Weiss R, Schotte C, Exadaktylos V, Haex B, Verbraecken J, Cluydts R. The role of presleep negative emotion in sleep physiology. Psychophysiology. 2011 Dec;48(12):1738-44. Epub 2011 Sep 6. [CrossRef] [PubMed]
- Norell-Clarke A, Hagström M and Jansson-Fröjmark M (2021) Sleep-Related Cognitive Processes and the Incidence of Insomnia Over Time: Does Anxiety and Depression Impact the Relationship? Front. Psychol. 12:677538. [CrossRef]
- Ham EM, You MJ. Role of Irrational Beliefs and Anger Rumination on Nurses’ Anger Expression Styles. Workplace Health Saf. 2018 May;66(5):223-232. Epub 2017 Nov 9. [CrossRef] [PubMed]
- Metcalf O, Little J, Cowlishaw S, Varker T, Arjmand HA, O’Donnell M, Phelps A, Hinton M, Bryant R, Hopwood M, McFarlane A, Forbes D. Modelling the relationship between poor sleep and problem anger in veterans: A dynamic structural equation modelling approach. J Psychosom Res. 2021 Nov;150:110615. Epub 2021 Sep 8. [CrossRef] [PubMed]
- Hruska B, Anderson L, Barduhn MS. Multilevel analysis of sleep quality and anger in emergency medical service workers. Sleep Health. 2022 Jun;8(3):303-310. Epub 2022 Apr 19. [CrossRef] [PubMed]
- Krizan, Z., & Herlache, A. D. (2016). Sleep disruption and aggression: Implications for violence and its prevention. Psychology of Violence, 6, 542-552.
- Kamphuis, J., Meerlo, P., Koolhaas, J. M., & Lancel, M. (2012). Poor sleep as a potential causal factor in aggression and violence. Sleep Medicine, 13, 327-334.
- Dressle RJ, Riemann D. Hyperarousal in insomnia disorder: Current evidence and potential mechanisms. J Sleep Res. 2023 Dec;32(6):e13928. Epub 2023 May 14. [CrossRef] [PubMed]
- Tselebis A, Zoumakis E, Ilias I. Dream Recall/Affect and the Hypothalamic–Pituitary–Adrenal Axis. Clocks & Sleep. 2021; 3(3):403-408.
- Kalmbach DA, Cuamatzi-Castelan AS, Tonnu CV, Tran KM, Anderson JR, Roth T, Drake CL. Hyperarousal and sleep reactivity in insomnia: current insights. Nat Sci Sleep. 2018 Jul 17;10:193-201. [CrossRef] [PubMed]
- Altena E, Chen IY, Daviaux Y, Ivers H, Philip P, Morin CM. How Hyperarousal and Sleep Reactivity Are Represented in Different Adult Age Groups: Results from a Large Cohort Study on Insomnia. Brain Sci. 2017 Apr 14;7(4):41. 4. [CrossRef] [PubMed]
- Hailey Meaklim, Flora Le, Sean P A Drummond, Sukhjit K Bains, Prerna Varma, Moira F Junge, Melinda L Jackson, Insomnia is more likely to persist than remit after a time of stress and uncertainty: a longitudinal cohort study examining trajectories and predictors of insomnia symptoms, Sleep, Volume 47, Issue 4, April 2024, zsae028. [CrossRef]
- Demichelis OP, Grainger SA, Burr L, Henry JD. Emotion regulation mediates the effects of sleep on stress and aggression. J Sleep Res. 2023 Jun;32(3):e13787. Epub 2022 Nov 16. [CrossRef] [PubMed]
- Larsson J, Bjureberg J, Zhao X, Hesser H. The inner workings of anger: A network analysis of anger and emotion regulation. J Clin Psychol. 2024 Feb;80(2):437-455. Epub 2023 Nov 17. [CrossRef] [PubMed]
- Reffi AN, Kalmbach DA, Cheng P, Drake CL. The sleep response to stress: how sleep reactivity can help us prevent insomnia and promote resilience to trauma. J Sleep Res. 2023 Dec;32(6):e13892. Epub 2023 Apr 5. [CrossRef] [PubMed]
- Wassing R, Benjamins JS, Dekker K, Moens S, Spiegelhalder K, Feige B, Riemann D, van der Sluis S, Van Der Werf YD, Talamini LM, Walker MP, Schalkwijk F, Van Someren EJ. Slow dissolving of emotional distress contributes to hyperarousal. Proc Natl Acad Sci USA. 2016 Mar 1;113(9):2538-43. Epub 2016 Feb 8. [CrossRef] [PubMed]
- Li Y, Gu S, Wang Z, Li H, Xu X, Zhu H, Deng S, Ma X, Feng G, Wang F, Huang JH. Relationship Between Stressful Life Events and Sleep Quality: Rumination as a Mediator and Resilience as a Moderator. Front Psychiatry. 2019 May 27;10:348. [CrossRef] [PubMed]
- Lo Martire, V., Berteotti, C., Zoccoli, G. et al. Improving Sleep to Improve Stress Resilience. Curr Sleep Medicine Rep 10, 23–33 (2024). [CrossRef]
- L Palagini, B Olivia, E Petri, G Cipollone, U Moretto, G Perugi, 0294 Resilience, Emotion and Arousal Regulation in Insomnia Disorder, Sleep, Volume 40, Issue suppl_1, 28 April 2017, Pages A108–A109. [CrossRef]
- Palagini L, Moretto U, Novi M, Masci I, Caruso D, Drake CL, Riemann D. Lack of resilience is related to stress-related sleep reactivity, hyperarousal, and emotion dysregulation in insomnia disorder. J Clin Sleep Med. 2018;14(5):759–766.
- Zhan N, Xu Y, Pu J, Wang W, Xie Zand Huang H (2024). The interaction between mental resilience and insomnia disorder on negative emotions in nurses in Guangdong Province, China. Front. Psychiatry 15:1396417. [CrossRef]
- Basta M, Chrousos GP, Vela-Bueno A, Vgontzas AN. CHRONIC INSOMNIA AND STRESS SYSTEM. Sleep Med Clin. 2007 Jun;2(2):279-291. [CrossRef] [PubMed]
- Meng-Yin Cheng, Meng-Jia Wang, Ming-Yu Chang, Rui-Xing Zhang, Chao-Fan Gu & Yu-Hua Zhao (2020): Relationship between resilience and insomnia among the middleaged and elderly: mediating role of maladaptive emotion regulation strategies, Psychology, Health & Medicine. [CrossRef]
- de Almondes KM, Marín Agudelo HA, Jiménez-Correa U. Impact of Sleep Deprivation on Emotional Regulation and the Immune System of Healthcare Workers as a Risk Factor for COVID 19: Practical Recommendations From a Task Force of the Latin American Association of Sleep Psychology. Front Psychol. 2021 May 20;12:564227. [CrossRef] [PubMed]
- Demir G, Karadag G. The Relationship Between Nurses’ Sleep Quality and Their Tendency to Commit Medical Errors. Sleep Sci. 2023 Nov 30;17(1):e7-e15. [CrossRef] [PubMed]
- Cheng P, Kalmbach DA, Hsieh H-F, Castelan AC, Sagong C, Drake CL. Improved resilience following digital cognitive behavioral therapy for insomnia protects against insomnia and depression one year later. Psychological Medicine. 2023;53(9):3826-3836. [CrossRef]
- Philip Cheng, Melynda D Casement, David A Kalmbach, Andrea Cuamatzi Castelan, Christopher L Drake, Digital cognitive behavioral therapy for insomnia promotes later health resilience during the coronavirus disease 19 (COVID-19) pandemic, Sleep, Volume 44, Issue 4, April 2021, zsaa258. [CrossRef]
- Landry CA, McCall HC, Beahm JD, Titov N, Dear B, Carleton RN, Hadjistavropoulos HD. Web-Based Mindfulness Meditation as an Adjunct to Internet-Delivered Cognitive Behavioral Therapy for Public Safety Personnel: Mixed Methods Feasibility Evaluation Study. JMIR Form Res. 2024 Jan 30;8:e54132. [CrossRef] [PubMed]
- Rosen B, Preisman M, Read H, Chaukos D, Greenberg RA, Jeffs L, Maunder R, Wiesenfeld L. Resilience coaching for healthcare workers: Experiences of receiving collegial support during the COVID-19 pandemic. Gen Hosp Psychiatry. 2022 Mar-Apr;75:83-87. Epub 2022 Feb 22. [CrossRef] [PubMed]
- Lee, C. Y., Chen, H. C., Tseng, M. C. M., Lee, H. C., & Huang, L. H. (2015). The relationships among sleep quality and chronotype, emotional disturbance, and insomnia vulnerability in shift nurses. Journal of Nursing Research, 23(3), 225-235.
- Chan, M. F. (2009). Factors associated with perceived sleep quality of nurses working on rotating shifts. Journal of Clinical Nursing, 18(2), 285-293.
- Pachi A, Tselebis A, Ilias I, Tsomaka E, Papageorgiou SM, Baras S, Kavouria E, Giotakis K. Aggression, Alexithymia and Sense of Coherence in a Sample of Schizophrenic Outpatients. Healthcare. 2022; 10(6):1078. [CrossRef]
- Tselebis, A.; Bratis, D.; Pachi, A.; Moussas, G.; Karkanias, A.; Harikiopoulou, M.; Theodorakopoulou, E.; Kosmas, E.; Ilias, I.; Siafakas, N.; et al. Chronic Obstructive Pulmonary Disease: Sense of Coherence and Family Support Versus Anxiety and Depression. Psychiatriki 2013, 24, 109–116. [Google Scholar] [PubMed]
- Jarrin, D. C., Chen, I. Y., Ivers, H., & Morin, C. M. (2014). The role of vulnerability in stress-related insomnia, social support and coping styles on incidence and persistence of insomnia. Journal of sleep research, 23(6), 681-688.
- Tselebis, A., Anagnostopoulou, T., Bratis, D., Moulou, A., Maria, A., Sikaras, C., … & Tzanakis, N. (2011). The 13 item Family Support Scale: Reliability and validity of the Greek translation in a sample of Greek health care professionals. Asia Pacific family medicine, 10, 1-4.
- Ellison, C. G., Deangelis, R. T., Hill, T. D., & Froese, P. (2019). Sleep quality and the stress-buffering role of religious involvement: a mediated moderation analysis. Journal for the scientific study of religion, 58(1), 251-268.
Figure 1.
Mediation analysis of Brief Resilience Scale (BRS) on Dimensions of Anger (DAR-5) - Athens Insomnia Scale (AIS) relationship.
Figure 1.
Mediation analysis of Brief Resilience Scale (BRS) on Dimensions of Anger (DAR-5) - Athens Insomnia Scale (AIS) relationship.
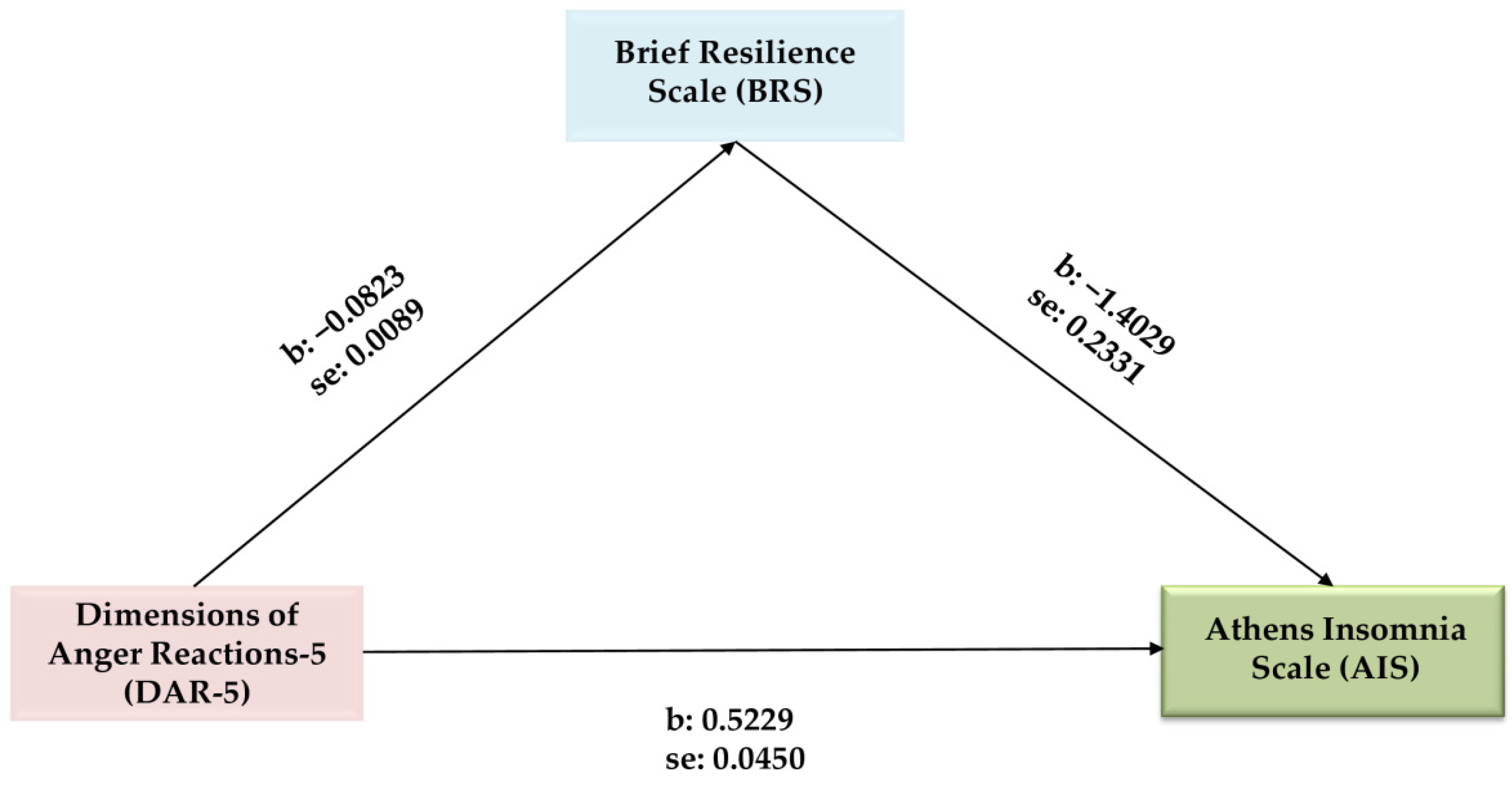

Table 1.
Descriptive statistics of participants.
| Age | Work Experience (in Years) | Dimensions of Anger Reactions-5 (DAR-5) |
Athens Insomnia Scale (AIS) |
Brief Resilience Scale (BRS) | ||
|---|---|---|---|---|---|---|
| Male | Mean | 46.620* | 20.063 | 9.848** | 6.051** | 3.599* |
| N | 79 | 79 | 79 | 79 | 79 | |
| Std. Deviation | 10.564 | 11.613 | 3.146 | 3.958 | 0.779 | |
| Female | Mean | 43.149* | 17.845 | 11.541** | 7.602** | 3.357* |
| N | 362 | 362 | 362 | 362 | 362 | |
| Std. Deviation | 10.838 | 11.916 | 3.923 | 4.139 | 0.776 | |
| Hedges’ g | 0.322 | 0.446 | 0.378 | 0.312 | ||
| Total | Mean | 43.771 | 18.243 | 11.238 | 7.324 | 3.400 |
| N | 441 | 441 | 441 | 441 | 441 | |
| Std. Deviation | 10.859 | 11.880 | 3.848 | 4.146 | 0.781 | |
* t-test p < 0.05; ** t-test p < 0.01.
Table 2.
Correlations among age, work experience (in years), AIS, DAR-5 & BRS.
| Age | Work Experience (in Years) | AIS | DAR-5 | ||
|
Athens Insomnia Scale (AIS) |
r | -0.105* | -0.077 | ||
| p | 0.028 | 0.108 | |||
| N | 441 | 441 | |||
| Dimensions of Anger Reactions-5 (DAR-5) | r | -0.056 | -0.040 | 0.485** | |
| p | 0.238 | 0.406 | 0.001 | ||
| N | 441 | 441 | 441 | ||
| The Brief Resilience Scale (BRS) | r | 0.217** | 0.185** | -0.418** | -0.405** |
| p | 0.001 | 0.001 | 0.001 | 0.001 | |
| N | 441 | 441 | 441 | 441 | |
* Pearson Correlations p < 0.05, ** Pearson Correlations p < 0.01.
Table 3.
Stepwise multiple regression.
| Dependent Variable: Athens Insomnia Scale (AIS) |
R Square | R Square Change | Beta | t | p | VIF | Durbin- Watson |
|---|---|---|---|---|---|---|---|
| Dimensions of Anger Reactions (DAR-5) |
0.235 | 0.235 | 0.378 | 8.609 | 0.001* | 1.197 | 1.937 |
| Brief Resilience Scale (BRS) | 0.294 | 0.058 | −0.264 | −6.019 | 0.001* | 1.197 |
Notes: Only statistically significant variables are included Beta = standardized regression coefficient; *Correlations are statistically significant at the p < 0.001 level.
Table 4.
Mediation analysis of the Brief Resilience Scale (BRS) on the Dimensions of Anger Reactions (DAR-5) and the Athens Insomnia Scale (AIS) relationship*.
Table 4.
Mediation analysis of the Brief Resilience Scale (BRS) on the Dimensions of Anger Reactions (DAR-5) and the Athens Insomnia Scale (AIS) relationship*.
| Variables | b | SE | t | p | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| LLCI | ULCI | |||||
| DAR-5 → BRS | −0.0823 | 0.0089 | −9.2896 | 0.001 | −0. 0997 | −0.0649 |
| DAR-5 → AIS | 0.5229 | 0.0450 | 11.6283 | 0.001 | 0.4345 | 0.6112 |
| DAR-5 → BRS → AIS | −1.4029 | 0.2331 | −6.0185 | 0.001 | −1.8610 | −0.9448 |
| Effects | ||||||
| Direct | 0.4074 | 0.0473 | 8.6092 | 0.001 | 0.3144 | 0.5004 |
| Indirect * | 0.1154 | 0.0244 | 0.0712 | 0.1669 | ||
| Total | 0.5229 | 0.0450 | 11.6283 | 0.001 | 0.4345 | 0.6112 |
Notes: 1. * Based on 5000 bootstrap samples; 2. Work experience and age were included in the analysis as covariates. They are not shown in the table as they did not give significant results (p > 0.05).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



