Submitted:
16 August 2024
Posted:
16 August 2024
Read the latest preprint version here
Abstract
Background/Objectives: Advancements in surgical stapling devices play a crucial role in improving outcomes for bariatric procedures. This study evaluates the performance and safety of a new endoscopic stapler (EnDrive®BelugaTM) regarding perioperative results across multiple bariatric surgery types.
Methods: A retrospective analysis was conducted on 112 patients who underwent bariatric procedures using the Beluga stapler at two centres in the UAE and Kenya over 6-month period (June-December 2023). Procedures included laparoscopic sleeve gastrectomy (LSG), Roux-en-Y gastric bypass (LRYGB), mini gastric bypass (OAGB-MGB), and revisions. Perioperative outcomes, complications, and haemoglobin changes were assessed.
Results: The cohort included 29 males and 83 females, with a mean age of 32.8 years and preoperative BMI of 41.1 kg/m². Procedures performed were 88 primary LSG, three primary LRYGB, 12 primary OAGB-MGB, and nine revision surgeries. No conversions, deaths, bleeding, or leaks occurred. Minor complications were observed in 4 patients. One patient required reoperation for intestinal obstruction. The mean hospital stay was 1.5 days. Haemoglobin levels showed minimal change from preoperative (12.8 g/dL) to postoperative day 1 (12.3 g/dL).
Conclusions: The new Beluga endoscopic stapler demonstrated safe and effective performance across various bariatric procedures, with low complication rates and minimal blood loss. Its enhanced articulation capabilities may offer advantages in specific cases. Further studies are warranted to compare long-term outcomes with established stapling devices.
Keywords:
bariatric
; metabolic
; surgery
; endoscopic stapler
; bleeding
; leak
1. Introduction
Bariatric surgery has emerged as the most effective treatment for severe obesity and its associated comorbidities [1]. As the prevalence of obesity continues to rise globally, the demand for bariatric procedures has increased substantially [2]. This trend has driven innovations in surgical techniques and technologies aimed at improving outcomes, reducing complications, and enhancing the efficiency of these operations [3].
Among the technological advancements in bariatric surgery, surgical staplers play a pivotal role [4]. These devices are crucial for creating anastomoses and resecting tissues, particularly in laparoscopic procedures where manual suturing can be challenging [5]. The evolution of stapling devices has focused on improving tissue compression, staple formation, and ease of use in confined spaces. They have a capital balancing role allowing perfusion and hemostasis of tissue while making the anastomosis.
Recent innovations in endoscopic staplers have aimed to address earlier models’ limitations, such as inadequate articulation, suboptimal tissue compression, and inconsistent staple formation [6]. These factors can contribute to complications like bleeding, leaks, and strictures, which remain significant concerns in bariatric surgery [7]. Therefore, introducing new stapling devices with enhanced features warrants careful evaluation to assess their performance and safety in clinical practice.
The Beluga endoscopic linear cutting powered stapler (David® EnDrive®Beluga™, Ningbo Verykind Medical Device Co., Ltd) represents a new generation of stapling devices designed to offer improved articulation and tissue compression. However, limited data exist on its performance in bariatric procedures across different techniques and patient populations. The EnDrive®BelugaTM reloads use the same height in the three staple rows.
This study aims to evaluate the perioperative outcomes of using the EnDrive®BelugaTM stapler in a diverse range of bariatric procedures performed at two international centres. By assessing complication rates, hemostasis, and technical performance, we seek to provide insights into this new stapling device’s safety and efficacy in bariatric surgery.
2. Material and Methods
2.1. Study Design and Patient Selection
This retrospective study analyzed data from patients who underwent bariatric surgery using the EnDrive®BelugaTM powered endoscopic stapler at two specialized centers in the United Arab Emirates and Kenya between June and December 2023. The institutional review boards of both participating centres approved the study protocol, and informed consent was obtained from all patients.
Inclusion criteria encompassed adult patients (age ≥18 years) with morbid obesity who underwent primary or revision bariatric procedures during the study period. Exclusion criteria included patients with open surgery or incomplete perioperative data.
2.2. Surgical Procedures
All surgeries were performed laparoscopically by experienced bariatric surgeons. The procedures included:
- Laparoscopic Sleeve Gastrectomy (LSG)
- Laparoscopic Roux-en-Y Gastric Bypass (LRYGB)
- One Anastomosis Gastric Bypass - Mini Gastric Bypass (OAGB-MGB)
- Revision surgeries (conversion of sleeve to mini bypass, revision of gastric band to bypass)
LSG employed tow techniques: a 3-port approach (n=37) and a 5-port approach (n=51). Gastrectomy started at 2-4 cm from pylorus. Stapling was performed using 2 green and 2-3-4 yellow reloads of the Beluga stapler (Table 1). In 5 cases, concomitant hiatal hernia repair with posterior hiatoplasty was performed, and in 1 case, cholecystectomy was associated.
OAGB-MGB procedures utilized a 5-port technique, with green and yellow reloads. In revision cases, three patients underwent hiatal repair with a re-sleeve.
LRYGB procedures employed a 5-port technique, using green and yellow reloads for the stomach and white reloads for the jejunojejunal anastomosis.
All surgeries were performed with 36 Fr calibration bougie.
All procedures were performed in conjunction with the Viper™ Ultrasonic Surgical System (Viper™, Ningbo Verykind Medical Device Co., Ltd) for energy-based tissue dissection and vessel sealing. No Staple Line Reinforcement (SLR) by oversewing or buttressing material was used in this series.
2.3. Data Collection and Outcome Measures
Demographic and clinical data were collected, including age, gender, preoperative weight, height, and body mass index (BMI). Operative details such as procedure type, technique variations, and use of additional interventions (e.g., hiatal hernia repair) were recorded.
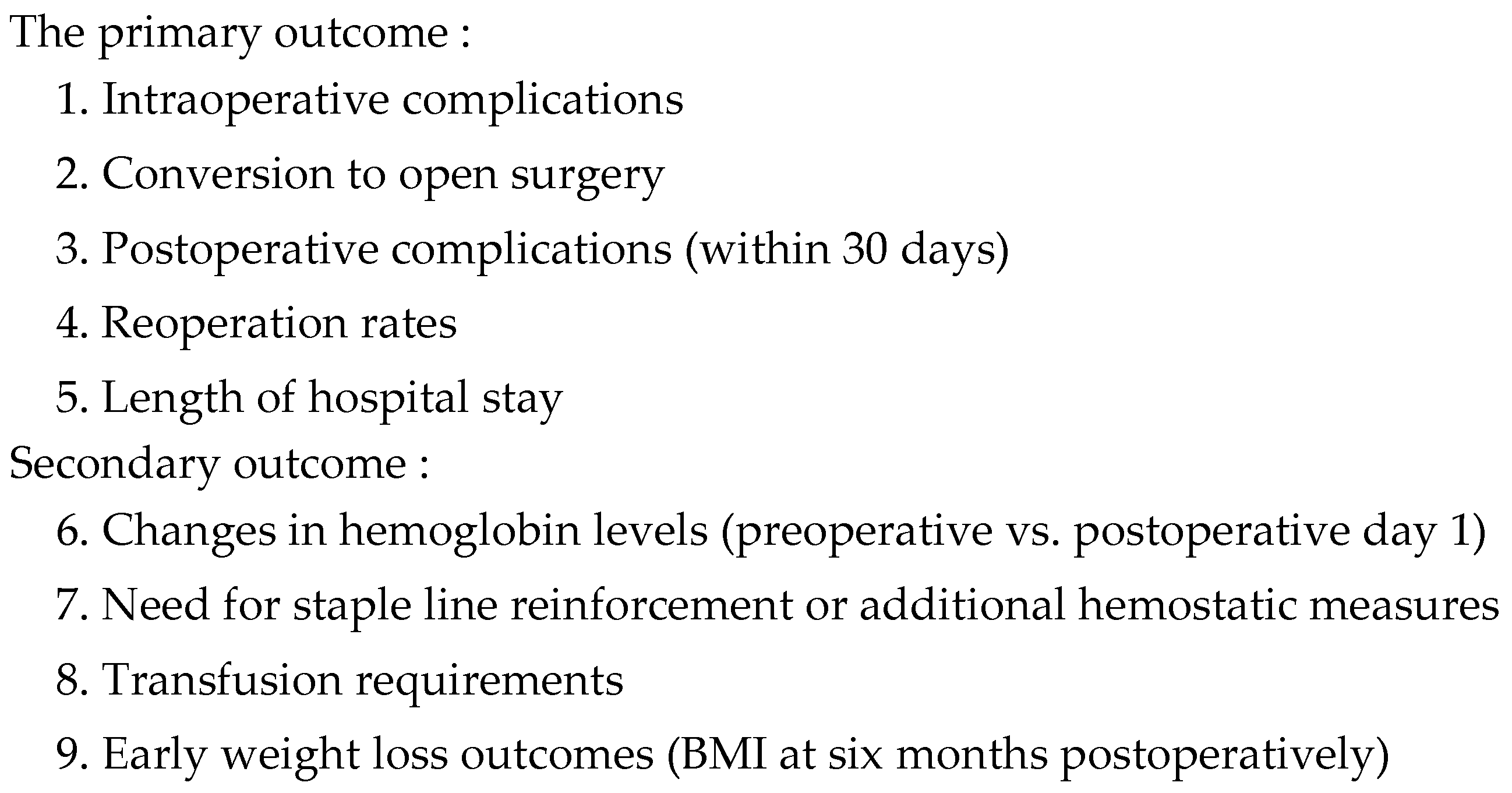
The primary and secondary outcome measures are summarized in Table 2.
2.4. Statistical Analysis
Descriptive statistics were used to summarize patient characteristics and outcomes. Continuous variables are presented as means with ranges, while categorical variables are expressed as frequencies and percentages. Paired t-tests were used to compare preoperative and postoperative hemoglobin levels. All statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). A p-value <0.05 was considered statistically significant.
3. Results
3.1. Patient Characteristics
A total of 112 patients (29 male, 83 female) were included in the study. The mean age was 32.8 years (range: 19-59 years). Preoperative anthropometric measurements were as follows:
- Mean BMI: 41.1 kg/m2 (range: 30.8-73 kg/m2)
- Mean weight: 107 kg (range: 61-234 kg)
- Mean height: 163 cm (range: 144-187 cm)
3.2. Surgical Procedures
The distribution of procedures was as follows:
Primary LSG: 88 cases (78.6%)
Primary OAGB-MGB: 12 cases (10.7%)
Primary LRYGB: 3 cases (2.7%)
Revision sleeve to mini bypass: 7 cases (6.3%)
Revision gastric band to bypass: 1 case (0.9%)
Distalization of gastric bypass: 1 case (0.9%)
3.3. Intraoperative Outcomes
All procedures were completed laparoscopically, with no conversions to open surgery. The EnDrive®BelugaTM stapler was used successfully for tissue transection and anastomosis creation. Surgeons reported that the device allowed for effective tissue compression and offered enhanced articulation capabilities, which was particularly beneficial in challenging anatomical situations.
No intraoperative complications directly related to stapler use were reported. Additional interventions performed during the primary procedures included:
Hiatal hernia repair: 5 cases
Cholecystectomy: 1 case
Ventral hernia repair: 1 case (during OAGB-MGB)
3.4. Postoperative Outcomes
No mortality occurred in the study cohort. The mean hospital stay was 1.5 days (range: 1-12 days). Early postoperative complications (within 30 days) were observed in 5 patients (4.5%):
- Elevated blood pressure (190/110 mmHg) in one patient, managed medically
- Vomiting until postoperative day 3 in one LSG patient, resolved with conservative management
- Upper abdominal pain on day 3 in one LRYGB patient, with normal CT scan findings and managed successfully medically
- Abdominal pain with excessive gas in one patient treated medically
- Intestinal obstruction on day four after LRYGB, requiring reoperation
The single reoperation (0.9%) was performed for intestinal obstruction due to a twist at the jejunojejunal anastomosis. The patient underwent laparoscopic revision of the distal anastomosis with favourable outcomes.
3.5. Hemostasis and Blood Loss
Preoperative mean hemoglobin level was 12.8 g/dL (range: 9.1-14.8 g/dL) in 95 patients with available data. Postoperative day one haemoglobin levels were available for 45 patients, with a mean of 12.3 g/dL (range: 9.2-14.1 g/dL). The difference was insignificant (p=0.09), indicating minimal blood loss.
Additional hemostatic measures were minimal:
Endoclips applied in 1 patient
Bipolar coagulation was used in 5 patients
Monopolar coagulation was used in 6 patients
No patients required blood transfusion or iron supplementation.
3.6. Weight Loss Outcomes
At six months postoperatively, the mean BMI decreased to 28.5 kg/m2 (range: 20.7-53 kg/m2), representing a significant reduction from the preoperative values.
4. Discussion
This multicenter study provides valuable insights into the perioperative outcomes of using a new endoscopic powered stapler (EnDrive®BelugaTM) in various bariatric procedures. The results demonstrate favorable safety and efficacy profiles across different surgical techniques and patient populations, warranting a comprehensive discussion of their implications for bariatric surgical practice.
4.1. Stapler Performance and Safety
The absence of stapler-related intraoperative complications, such as misfiring or tissue damage, suggests that the Beluga stapler performed reliably across various tissue thicknesses encountered in bariatric procedures. This is particularly noteworthy given the heterogeneous nature of the study cohort, which included both primary and revision surgeries [8]. The ability to handle different tissue types and thicknesses is crucial in bariatric surgery, where variations in gastric wall thickness and the presence of scar tissue in revision cases can pose significant challenges [1].
The low rate of postoperative complications (4.5%) and single reoperation (0.9%) in our series compares favorably with published literature on bariatric surgery outcomes [9,10]. While direct comparisons with other stapler types were not performed in this study, these results suggest that the Beluga stapler does not introduce additional risks and may contribute to the overall safety profile of the procedures. It is important to note that complication rates in bariatric surgery can vary widely depending on factors such as surgeon experience, patient characteristics, and institutional protocols [2]. Therefore, the low complication rate observed in this study should be interpreted within the context of the participating centers' expertise and patient selection criteria.
4.2. Hemostasis and Blood Loss
One of the key findings of this study was the minimal change in haemoglobin levels from preoperative to postoperative day 1, indicating effective hemostasis. The low requirement for additional hemostatic measures (10.7% of cases) further supports the stapler's ability to achieve reliable tissue approximation and seal [11]. This is particularly important in bariatric surgery, where bleeding from staple lines remains a concern and can lead to significant morbidity [12].
Whether staple lines should be routinely reinforced in bariatric surgery remains controversial [3]. Some studies have shown that SLR can reduce bleeding and leak rates [4,11], while others have found no significant benefit [5]. Our results suggest that the EnDrive®BelugaTM powered stapler may provide adequate hemostasis without routine reinforcement, potentially streamlining the surgical procedure and reducing costs associated with reinforcement materials.
However, more extensive comparative studies are needed to confirm this observation and evaluate its long-term implications.
4.3. Technical Advantages and Learning Curve
The enhanced articulation capabilities of the EnDrive®BelugaTM stapler, as reported by the surgeons, may offer advantages in technically challenging cases or confined spaces. This feature could be particularly beneficial in revision surgeries or patients with complex anatomy, potentially reducing operative times and improving precision. The importance of stapler articulation in laparoscopic bariatric surgery cannot be overstated, as it allows for better access to difficult angles and may contribute to more precise tissue transection [6].
It is worth noting that the introduction of any new surgical device is associated with a learning curve. While our study did not specifically assess the learning curve for the EnDrive®BelugaTM stapler, the low complication rates suggest that experienced bariatric surgeons can safely adopt this device. Future studies should consider evaluating the learning curve associated with the Beluga stapler, as this information would be valuable for surgeons and institutions considering its adoption.
4.4. Procedure-Specific Considerations
The majority of procedures in our study were laparoscopic sleeve gastrectomies (LSG), reflecting the global trend towards this procedure [3,7]. The Beluga stapler performed well in LSG, with no reported leaks or bleeding complications. This is particularly important given that staple line leaks and bleeding are among the most feared complications of LSG [7].
While our cohort had fewer gastric bypass procedures (both LRYGB and OAGB-MGB), the results were equally encouraging. The single case of intestinal obstruction requiring reoperation was likely related to technical aspects of the anastomosis rather than stapler performance. Nonetheless, this case highlights the importance of meticulous technique in creating jejunojejunal anastomosis in RYGB procedures [8].
Including revision surgeries in our cohort is noteworthy, as these procedures are generally associated with higher complication rates [9]. The successful use of the Beluga stapler in revision cases, particularly in sleeve to mini-bypass conversions, suggests that it may be suitable for these more challenging scenarios. However, more extensive studies on revision procedures must confirm these preliminary observations.
4.5. Weight Loss Outcomes
The early weight loss outcomes observed six months postoperatively are consistent with expected results following bariatric procedures [13]. While longer-term follow-up is necessary to assess the durability of these outcomes, the initial results suggest using the Beluga stapler does not negatively impact the effectiveness of the bariatric interventions. It is important to note that weight loss outcomes are influenced by numerous factors beyond the choice of stapling device, including patient compliance with dietary recommendations, hormonal changes, and variations in surgical technique [10].
4.6. Cost Considerations
While our study did not perform a cost analysis, the potential economic implications of adopting a new stapling device should be considered. The initial cost of new technology must be weighed against potential benefits such as reduced complication rates, shorter operative times, and decreased need for SLR. Future studies should include comprehensive cost-effectiveness analyses to provide a more complete picture of the value proposition the Beluga stapler offers.
4.7. Limitations and Future Directions
This study has several limitations that should be acknowledged. First, its retrospective nature and lack of a control group limit our ability to draw definitive conclusions about the superiority of the Beluga stapler compared to other devices. Second, the relatively short follow-up period precludes assessment of long-term outcomes, such as staple line integrity and sustained weight loss. Third, while diverse, the study population may only partially represent some bariatric patient populations, potentially limiting generalizability.
Despite these limitations, this study provides valuable initial data on the Beluga stapler’s performance in a real-world bariatric surgery setting. The low complication rates and favorable hemostasis outcomes observed across multiple procedure types and two international centres suggest that this new stapling device can be safely and effectively incorporated into bariatric surgical practice.
Future research directions should include:
- Prospective, randomized controlled trials comparing the Beluga stapler to other established devices across various bariatric procedures.
- Long-term follow-up studies to assess staple line integrity, sustained weight loss, and resolution of obesity-related comorbidities.
- Evaluation of the learning curve associated with adopting the Beluga stapler.
- Cost-effectiveness analyses to determine the economic impact of this new technology.
- Studies focusing on using the Beluga stapler in challenging cases like super-obese patients or complex revision surgeries.
5. Conclusions
The EnDrive®BelugaTM endoscopic powered stapler demonstrated safe and effective performance across various bariatric procedures, with low complication rates and minimal blood loss. Its enhanced articulation capabilities may offer advantages in specific cases, particularly those with challenging anatomy. While these results are promising, further prospective studies with larger cohorts and extended follow-up periods are warranted to fully evaluate this new stapling device’s long-term outcomes and potential advantages in bariatric surgery.
Institutional Review Board Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinkideclaration and its later amendments or comparable ethical standards.
Informed Consent Statement
Informed consent was obtained from all individual participants included in the study.
Conflicts of Interest
Dr Layani has been a speaker for Ningbo Verykind Medical Device Co. and has received honorariums. Dr Noel has been speaker for Ningbo Verykind Medical Device Co. and has received honorariums.This study was not sponsored by a research grant from Ningbo Verykind Medical Device Co. The other authors declare no conflict of interest.
References
- Sjöström, L. Review of the key results from the Swedish Obese Subjects (SOS) trial - a prospective controlled intervention study of bariatric surgery. J Intern Med. 2013;273(3):219-234.
- Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384(9945):766-781.
- Angrisani L, Santonicola A, Iovino P, et al. IFSO Worldwide Survey 2020-2021: Current Trends for Bariatric and Metabolic Procedures. Obes Surg. 2024;34(4):1075-1085.
- Chekan E, Whelan RL. Surgical stapling device-tissue interactions: what surgeons need to know to improve patient outcomes. Med Devices (Auckl). 2014;7:305-318.
- Baker RS, Foote J, Kemmeter P, et al. The science of stapling and leaks. Obes Surg. 2004;14(10):1290-1298.
- Ito E, Ohdaira H, Nakashima H, et al. Endoscopic surgical stapler for gastrojejunostomy: a comparative study. Surg Endosc. 2008;22(2):436-440.
- Aurora AR, Khaitan L, Saber AA. Sleeve gastrectomy and the risk of leak: a systematic analysis of 4,888 patients. Surg Endosc. 2012;26(6):1509-1515.
- Higa K, Boone K, Arteaga I, Lopez-Tomassetti E. Mesenteric closure in laparoscopic gastric bypass: surgical technique and literature review. Surg Laparosc Endosc Percutan Tech. 2007;17(6):452-457.
- Chang SH, Stoll CR, Song J, et al. The effectiveness and risks of bariatric surgery: an updated systematic review and meta-analysis, 2003-2012. JAMA Surg. 2014;149(3):275-287.
- Berger ER, Clements RH, Morton JM, et al. The Impact of Different Surgical Techniques on Outcomes in Laparoscopic Sleeve Gastrectomies: The First Report from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP). Ann Surg. 2016;264(3):464-473.
- Shikora SA, Mahoney CB. Clinical Benefit of Gastric Staple Line Reinforcement (SLR) in Gastrointestinal Surgery: a Meta-analysis. Obes Surg. 2015;25(7):1133-1141.
- Trastulli S, Desiderio J, Guarino S, et al. Laparoscopic sleeve gastrectomy compared with other bariatric surgical procedures: a systematic review of randomized trials. Surg Obes Relat Dis. 2013;9(5):816-829.
- Golomb I, Ben David M, Glass A, Kolitz T, Keidar A. Long-term Metabolic Effects of Laparoscopic Sleeve Gastrectomy. JAMA Surg. 2015;150(11):1051-1057.
- Raftopoulos Y, Rajkumar S, Davidson E, Papasavas P. Prospective randomized comparaison of linear endostaplers during laparoscopic sleeve gastrectomy. Obes Surg. 2022;32:3472-3480.

Table 1.
EnDrive®BelugaTM Reloads.
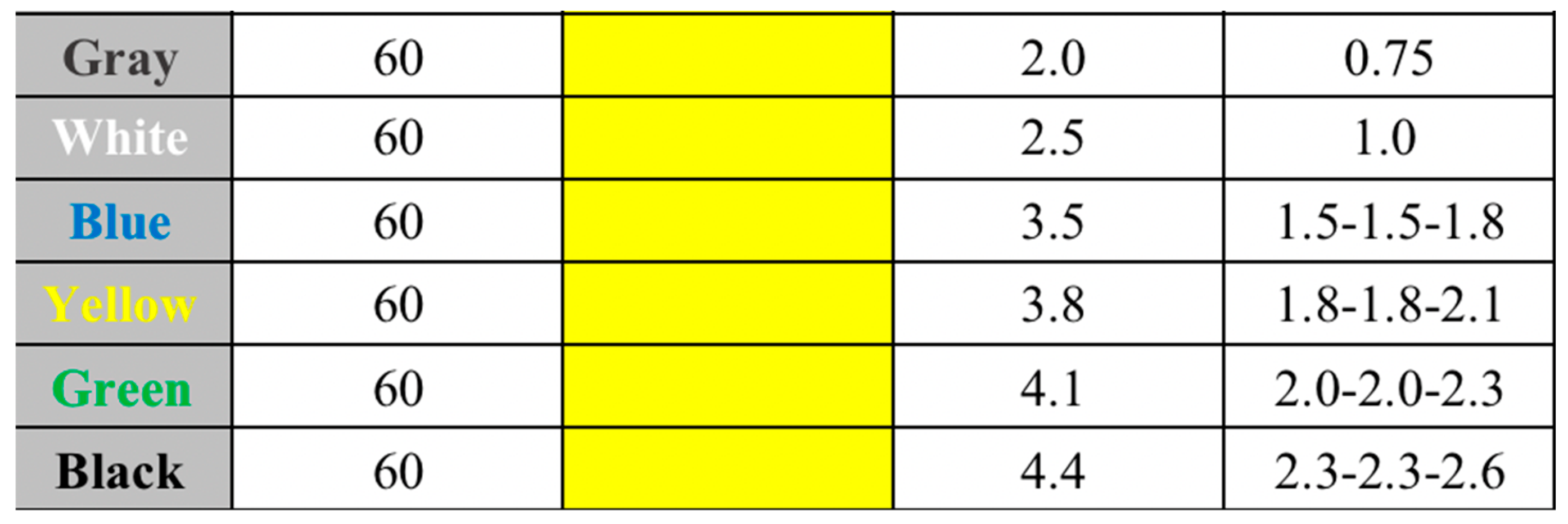
Table 2.
Primary and secondary outcome measures.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



