
Submitted:
02 August 2024
Posted:
02 August 2024
You are already at the latest version
Abstract
Minimally invasive surgery for adult spinal deformities (MIS deformity surgery) utilizes MIS lumbar interbody fusion and percutaneous pedicle screw fixation (PPSF) without posterior corrective osteotomy. While MIS reduces issues associated with open deformity surgery, it has limitations in correcting sagittal imbalance. This review discusses the limitations and solutions of lateral lumbar interbody fusion (LLIF) and introduces our experience in addressing marked sagittal deformities. We reviewed the literature and incorporated our clinical experience to evaluate the efficacy of recent MIS techniques, particularly focusing on oblique lumbar interbody fusion (OLIF) at L1-5 and L5-S1. The use of higher profile and greater angle cages and the application of PPSF with curved rods and percutaneous rod compression were discussed. Advances in MIS techniques, such as OLIF, have enabled significant improvements in increasing disc height and angle. Combining these new techniques and concepts, we successfully corrected marked sagittal deformities using MIS deformity surgery. Early onset of proximal junctional kyphosis was identified as a notable complication. Although recent advancements in MIS deformity surgery have shown promise in correcting sagittal deformities, further clinical experience and data are necessary to enhance outcomes and mitigate complications such as proximal junctional kyphosis.
Keywords:
adult spinal deformity
; minimally invasive surgery
; lateral lumbar interbody fusion
; percutaneous pedicle screw fixation
; marked sagittal deformity
1. Introduction
Minimally invasive surgery (MIS) for the spine began in 1991 with laparoscopic lumbar discectomy, a simple and low-risk surgery [1]. Currently, MIS can successfully replace nearly all types of spinal surgeries except those for spinal deformities, which require fusion and fixation across multiple spinal levels and represent the last challenge for MIS [2,3]. Since the first report of MIS surgery for adult spinal deformity (ASD) in 2008 [4], numerous studies have documented the outcomes of MIS surgery for degenerative spinal deformity [5,6,7,8,9,10].
There are three types of deformity surgeries: open deformity surgery using classical open techniques, hybrid deformity surgery combining MIS and open techniques, and MIS deformity surgery employing only MIS techniques [6]. Circumferential MIS (cMIS) deformity surgery involves MIS procedures on both the anterior and posterior sides, aligning with the definition of MIS deformity surgery [11], which combines MIS interbody fusion and posterior percutaneous screw fixation (PPSF) without corrective osteotomies or posterior bone fusion [4].
Open deformity surgery, the standard approach, has limitations [12], particularly for older patients with multiple comorbidities, leading to higher perioperative complication and mortality rates [12,13,14,15]. Studies indicate that MIS deformity surgery mitigates many issues associated with open surgery [4,5,13,16], making it a favorable option for ASD [17]. However, MIS deformity surgery still faces challenges in correcting rigid adult deformities [18,19] and sagittal imbalance in ASD [9,16,20].
This review examines the limitations of MIS deformity surgery, recent advancements in MIS techniques for deformity correction, solutions to overcome these limitations, and approaches to correcting marked sagittal deformities.
2. Techniques for MIS Deformity Surgery
The MIS techniques used for deformity surgery include MIS lumbar interbody fusion and PPSF.
2.1. MIS Lumbar Interbody Fusion
MIS lumbar interbody fusion techniques include anterior lumbar interbody fusion (ALIF), MIS transforaminal lumbar interbody fusion (TLIF), and lateral lumbar interbody fusion (LLIF) [19]. All these techniques—anterior, lateral, and posterior—are effective in correcting scoliosis [20,24,26,27,28]. However, their effectiveness in sagittal correction varies when a posterior corrective osteotomy is not performed. ALIF without osteotomy corrects the sagittal angle by approximately 5.3°–8.3° per level, outperforming posterior lumbar interbody fusion techniques [29,30]. In contrast, TLIF is less effective, achieving only -0.1° to 2° per level [29,31,32].
LLIF is divided into direct lateral lumbar interbody fusion (DLIF) [33], extreme lateral interbody fusion (XLIF) [34], oblique lumbar interbody fusion at L1-5 (OLIF25), and OLIF at L5-S1 level (OLIF51) [35,36]. DLIF and XLIF are retroperitoneal approaches to the lateral surface of the lumbar disc [33,34]. OLIF25 uses a retroperitoneal extrapsoas approach to the anterolateral lumbar disc [35,36]. OLIF51, distinct from DLIF and OLIF25, approaches the anterolateral L5-S1 disc through a pathway between the ureter and the common iliac artery [35,36].
For DLIF, either a right- or left-sided approach is used, with the patient in the right or left lateral decubitus position and the hip flexed, facilitating access at L4-5. In OLIF25 and OLIF51, the patient is positioned in a right lateral decubitus position without hip flexion, enabling interbody fusions from L1 to S1 in a single position [35,36].
2.2. Effectiveness of LLIF in Sagittal Correction
LLIF techniques show distinctive factors in creating lordotic angles compared to other methods [37,38,39]. DLIF with the cage placed in the middle or posterior part of the disc space is ineffective for sagittal correction, achieving only -1.2° to 3.8° per level [40,41]. However, DLIF with the cage positioned in the anterior disc space achieves sagittal correction similar to ALIF (7.4° per level) [42]. High-angle, high-profile cages placed in the anterior disc space during LLIF create more posterior space, increasing lumbar lordotic angle by posterior shortening [37,43]. OLIF25 allows for consistent anterior disc space placement due to the exposed anterior disc margin, which serves as a reference point for cage positioning. This improves the postoperative disc angle compared to DLIF [37]. OLIF51 uses cages with lordotic angles up to 24°, effectively increasing the lordotic angle at L5-S1 [44]. Mun et al. reported that the OLIF51 could achieve disc angles significantly greater than the cage angle by posterior rod compression (mean cage angle = 11.2 ± 1.6° vs. mean postoperative disc angle = 22.6 ± 4.7°), over 10° greater than TLIF [44]. The amount of angle correction at L5-S1 depends on the fusion technique and cage angle. OLIF51 with a 12° cage produces a greater angle than TLIF, and OLIF51 with a 24° cage achieves an even greater angle than OLIF51 with a 12° cage [Figure 1].
2.3. Percutaneous Pedicle Screw Fixation
PPSF is an essential technique in MIS deformity surgery for minimally invasive spinal stabilization. Compared to open pedicle screw fixation, PPSF offers several advantages, including higher accuracy, fewer injuries to spinal muscles and the medial branch of the dorsal ramus, less blood loss, shorter operation time, and reduced hospital stays [45,46,47,48,49,50,51]. Multilevel PPSF is effective for deformity correction, with rods bent to match the sagittal angle and rod compression resulting in greater lordotic angles [4]. The rods are then inserted into the iliac screws. The screw extender must have a large slot to pass the bent rod, as its curve elevates the rod tip at the thoracolumbar junction. Extender reduction starts from the caudal levels and continues proximally, similar to the cantilever maneuver in open deformity surgery [4,52]. Minimally invasive iliac screws or subcrestal iliac screws, when connected to the long-level thoracolumbar PPSF, provide strong mechanical support and protect the L5-S1 joint [13,52,53,54]. An illustrative case demonstrates the successful connection of a subcrestal iliac screw to the PPSF, as shown in Figure 2.
2.4. Avoiding Posterior Corrective Osteotomy
Corrective osteotomy techniques, such as Smith–Petersen osteotomy (SPO) for 10°–20°/level [55,56], pedicle subtraction osteotomy (PSO) for 30°–40°/level [57,58], and vertebral column resection (VCR) for >40°/level [59,60], can create additional lordotic angles. However, these osteotomies are associated with complications, including vascular [61,62], neural [60,63,64,65], increased intraoperative bleeding [66], and pseudoarthrosis [67,68]. Therefore, MIS deformity surgery should avoid corrective osteotomy whenever possible. Posterior corrective osteotomy can be avoided if the preoperative estimated angle correction via MIS deformity surgery is sufficient for successful sagittal correction.
Before surgery, it is essential to calculate the correctable lumbar angle using MIS techniques. Maximum lordotic angles can be achieved with LLIF and PPSF without corrective osteotomy by using higher-profile, greater lordotic angle cages inserted at the anterior disc space, allowing for additional rod compression for posterior shortening [Figure 3] [37,43]. A case illustrated in Figure 4 demonstrates the preoperative estimation of sagittal correction. The patient’s preoperative spinopelvic parameters were: SVA = 95.8 mm, PI = 54.2°; LL = +9.6°; and PI-LL = 63.8°. These parameters suggested that the patient should undergo open deformity surgery with posterior corrective osteotomies as recommended previously [7]. Setting the target LL between the PI and PI + 10° according to the SRS-Schwab criteria [69], the target LL would be ≥54.2°.
Angle correction must consider pre-existing angle losses due to kyphotic vertebral bodies or previous fusion operations. In this case, the total pre-existing angle loss was +7.5°, calculated from the kyphotic vertebra bodies of L1 (+17.9°) and L2 (+1.9°) with compensated lordotic angles at L3 body (-2.3°) and Cobb angle of L4-5 level (-10.0°). Thus, the minimum required angle correction was 54.2° + 7.5° = 61.7°. Postoperative disc angles can be estimated using cage angles, as data shows the postoperative disc angle is greater than the cage angle after LLIF and PPSF [37,43,44,52].
There were four lumbosacral disc levels (L1-2, L2-3, L3-4, and L5-S1) where OLIF and PPSF could produce lordotic angles. The estimated disc angles were ≥36° at the L1-2-3-4 levels using three 12° cages and ≥24° at the L5-S1 level using a 24° cage. The total estimated angle correction was ≥60°, and the corrected LL was ≥52.5° (60°–7.5°). According to the SRS-Schwab criteria or global alignment and proportion (GAP) score [67,68], this estimated LL was acceptable, allowing us to avoid posterior corrective osteotomy. The final postoperative lumbar angles were 62.3° and 56.5°, better than the preoperative estimates. Postoperative sagittal balance was satisfactory, with SVA = 25.3 mm and PI-LL = 2.3° [Figure 4].
3. Discussion
3.1. Limitations of MIS Deformity Surgery
Several studies have reported various limitations of MIS for deformity surgery in patients with ASD. While MIS deformity surgery is satisfactory for coronal correction, it is deficient in sagittal correction [20,21]. Patients with ASD often require multiple anterior and posterior releases due to their rigid deformities, unlike adolescent idiopathic scoliosis [18,22]. Severe fixed ASD must be corrected using open posterior surgery rather than MIS techniques [19,23]. The MIS approach to the L4-5 level in patients with a high iliac crest involves a long operation time and shows a high complication rate [24]. Mummaneni et al. suggested that open deformity surgery with posterior corrective osteotomies is needed for patients with preoperative SVA ≥60 mm and PI-LL ≥30 [7]. Wang et al. reported a maximum corrected lumbar lordosis (LL) of only 47.5° [16] and a ceiling effect of 23° for sagittal curve correction and 34° for coronal correction [23]. Yen et al. concluded that MIS deformity surgery remains in its early stages [8].
Combining the results of previous studies, the major concerns are twofold. First, MIS deformity surgery is effective only for coronal correction, not for sagittal correction, due to technical limitations. Second, MIS deformity surgery is suitable only for mild sagittal imbalance because of the limited sagittal angle correction. Since restoring sagittal balance is more critical than coronal balance [25], MIS deformity surgery presents significant challenges in managing ASD, with sagittal imbalance being the main issue.
To overcome these limitations, solutions must address technical constraints and achieve satisfactory correction of marked sagittal imbalance. Solutions include the effective use of LLIF and PPSF to increase disc angles and avoid posterior corrective osteotomies. The key lies in the optimal combination and application of MIS techniques for maximum angle correction.
3.2. Correction of Marked Sagittal Deformity
When deformity surgery is insufficient for correcting high-grade sagittal imbalance, it may not considered an appropriate surgical option for ASD. Most patients requiring surgery for ASD exhibit marked sagittal deformity, necessitating effective correction through MIS. Marked sagittal deformity is defined as having two or more significant sagittal modifiers: SVA >9.5 cm, PI-LL >20°, and PT >30° [69,70]. Unfortunately, no studies have focused on correcting marked sagittal deformities using MIS.
Based on our previous report [52], ASD patients with marked sagittal deformity underwent MIS deformity surgery with LLIF and PPSF and were followed for over 2 years post-surgery. The patients were divided into the OLIF51 and TLIF51 groups, with all patients undergoing LLIF at the lumbar level. The OLIF51 group underwent OLIF51, and the TLIF51 group underwent TLIF at L5-S1. Blood loss was significantly lower in the OLIF51 group compared to the TLIF51 group (260.7 ± 83.5 ml vs. 423.0 ± 59.3 ml). Preoperative SVA and PI-LL were 125.9 ± 21.3 mm and 36.5 ± 8.5° in the OLIF51 group, and 125.5 ± 22.1 mm and 34.1 ± 10.6° in the TLIF51 group. Postoperative SVA and PI-LL improved to 27.1 ± 11.4 mm and 3.6 ± 3.0° in the OLIF51 group, and 32.7 ± 18.4 mm and 7.5 ± 3.2° in the TLIF51 group. The corrected LL and LL corrections were 55.5 ± 2.8° and 38.7 ± 10.2° in the OLIF51 group, and 46.9 ± 5.2° and 26.6 ± 9.8° in the TLIF51 group, outperforming previous MIS deformity surgery reports with LL corrections up to 47.5° and 23° [16,23]. The OLIF51 group achieved better sagittal correction due to the greater corrected disc angle at L5-S1, with mean postoperative L5-S1 disc angles of 18.4 ± 3.7° and 6.9 ± 2.8°, respectively. An illustrative case of ASD with marked sagittal imbalance demonstrated successful sagittal correction after MIS deformity surgery [Figure 5].
3.3. Concerns of MIS Deformity Surgery
Our previous study indicated that MIS deformity surgery can result in various complications such as psoas symptoms, ileus, vascular injury, and proximal junctional kyphosis (PJK) [52]. No major complications were observed. The incidence of PKJ (30–31%) was similar to other reports of open deformity surgeries (26–41%) [71,72,73,74]. However, the onset of PJK in the OLIF51 group was significantly earlier (8.6±1.9 months post-surgery) than in the TLIF51 group (26.3 ± 4.7 months) and previous studies (18.6–34.8 months) [75,76]. The earliest onset of PJK in the OLIF51 group was 7 months post-surgery [Figure 6].
Several risk factors for PJK have been suggested, including age, bone quality, higher lumbar angle correction, higher PI, and smaller PI-LL [71,74,77,78]. Among these factors, we focused on achieving a harmonious lumbar curve with greater lower lumbar lordosis (LLL) at L4-5-S1 [79,80,81]. An exaggerated upper lumbar angle, indicating a smaller LLL proportion, increases stress at the proximal junction, leading to junctional failure [80]. The ideal LLL proportion is proposed to be 50–80% of the total LL [82,83,84]. We suspect that the persistent lordotic rod angle at the lower thoracic and thoracolumbar junction levels, along with a greater angle correction in the OLIF51 group, contributed to early PJK. Therefore, a solution is needed to decrease upper lumbar lordosis and increase LLL proportion to prevent early PJK after MIS deformity surgery.
Rigid lumbar joints, associated with degenerated stiff facet joints, can hinder the release of disc space without posterior corrective osteotomy [4,7,10,18,19,85]. In our experience, we encountered only one lumbar disc level that failed to release via LLIF due to rigid facet joints; however, almost all lumbar disc levels were successfully released during MIS deformity surgery (data not presented). A solution for releasing severely rigid joints without an osteotomy has yet to be established.
4. Conclusions
MIS has proven effective in correcting ASD using LLIF, including the correction of marked sagittal deformities. Among the techniques studied, oblique lumbar interbody fusion at the L5-S1 level (OLIF51) demonstrated superior angle correction compared to TLIF. Percutaneous fixation is crucial for achieving the desired lumbar angle through posterior shortening with rod compression. However, early onset of PJK remains a notable complication, potentially linked to exaggerated upper lumbar lordosis and a decreased proportion of LLL. The findings underscore the potential of MIS techniques in managing ASD effectively, yet also highlight the need for strategies to mitigate complications such as early PJK.
5. Future Directions
Future studies should explore optimized surgical protocols to enhance sagittal balance correction and investigate long-term outcomes to validate the sustainability of MIS benefits. Additionally, developing techniques to improve LLL proportion and reduce the incidence of PJK will be critical in advancing MIS deformity surgery.
Author Contributions
All authors made substantial contributions to the conception and design of the manuscript and performed a literature search and review.
Funding
Not applicable.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable
Conflicts of Interest
The author declared no conflicts of interest.
References
- Obenchain, T.G. Laparoscopic lumbar discectomy: Case report. Journal of Laparoendoscopic Surgery 1991, 1, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Momin, A.A.; Steinmetz, M.P. Evolution of minimally invasive lumbar spine surgery. World Neurosurg 2020, 140, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.D.; Canseco, J.A.; Houlihan, N.; Gabay, A.; Grasso, G.; Vaccaro, A.R. Overview of Minimally invasive spine surgery. World Neurosurg 2020, 142, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Anand, N.; Baron, E.M.; Thaiyananthan, G.; Khalsa, K.; Goldstein, T.B. Minimally invasive multilevel percutaneous correction and fusion for adult lumbar degenerative scoliosis: a technique and feasibility study. J Spinal Disord Tech 2008, 21, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Mundis, G.M.; Akbarnia, B.A.; Phillips, F.M. Adult deformity correction through minimally invasive lateral approach techniques. Spine (Phila Pa 1976) 2010, 35, S312–S321. [Google Scholar] [CrossRef] [PubMed]
- Haque, R.M.; Mundis, G.M.; Jr Ahmed, Y.; et al. Comparison of radiographic results after minimally invasive, hybrid, and open surgery for adult spinal deformity: a multicenter study of 184 patients. Neurosurg Focus 2014, 36, E13–E19. [Google Scholar] [CrossRef] [PubMed]
- Mummaneni, P.V.; Shaffrey, C.I.; Lenke, L.G.; et al. The minimally invasive spinal deformity surgery algorithm: a reproducible rational framework for decision making in minimally invasive spinal deformity surgery. Neurosurg Focus 2014, 36, E6–E12. [Google Scholar] [CrossRef] [PubMed]
- Yen, C.P.; Mosley, Y.I.; Uribe, J.S. Role of minimally invasive surgery for adult spinal deformity in preventing complications. Curr Rev Musculoskelet Med 2016, 9, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Theologis, A.A.; Mundis, G.M.; Jr Nguyen, S.; et al. Utility of multilevel lateral interbody fusion of the thoracolumbar coronal curve apex in adult deformity surgery in combination with open posterior instrumentation and L5-S1 interbody fusion: a case-matched evaluation of 32 patients. J Neurosurg Spine 2017, 26, 208–219. [Google Scholar] [CrossRef]
- Anand, N.; Kong, C.; Fessler, R.G. A Staged protocol for circumferential minimally invasive surgical correction of adult spinal deformity. Neurosurgery 2017, 81, 733–739. [Google Scholar] [CrossRef]
- Anand, N.; Cohen, J.E.; Cohen, R.B.; Khandehroo, B.; Kahwaty, S.; Baron, E. Comparison of a newer versus older protocol for circumferential minimally invasive surgical (CMIS) correction of adult spinal deformity (ASD)-Evolution over a 10-year experience. Spine Deform 2017, 5, 213–223. [Google Scholar] [CrossRef] [PubMed]
- Daubs, M.D.; Lenke, L.G.; Cheh, G.; Stobbs, G.; Bridwell, K.H. Adult spinal deformity surgery: complications and outcomes in patients over age 60. Spine (Phila Pa 1976) 2007, 32, 2238–2244. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.Y. Percutaneous iliac screws for minimally invasive spinal deformity surgery. Minim Invasive Surg 2012, 2012, 173685. [Google Scholar] [CrossRef] [PubMed]
- Pateder, D.B.; Gonzales, R.A.; Kebaish, K.M.; Cohen, D.B.; Chang, J.Y.; Kostuik, J.P. Short-term mortality and its association with independent risk factors in adult spinal deformity surgery. Spine (Phila Pa 1976) 2008, 33, 1224–1228. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.S.; Shaffrey, C.I.; Glassman, S.D.; et al. Risk-benefit assessment of surgery for adult scoliosis: an analysis based on patient age. Spine (Phila Pa 1976) 2011, 36, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.Y.; Mummaneni, P.V. Minimally invasive surgery for thoracolumbar spinal deformity: initial clinical experience with clinical and radiographic outcomes. Neurosurg Focus 2010, 28, E9–E16. [Google Scholar] [CrossRef] [PubMed]
- Scheufler, K.M.; Cyron, D.; Dohmen, H.; Eckardt, A. Less invasive surgical correction of adult degenerative scoliosis, part I: technique and radiographic results. Neurosurgery 2010, 67, 696–710. [Google Scholar] [CrossRef] [PubMed]
- Bradford, D.S.; Tay, B.K.; Hu, S.S. Adult scoliosis: surgical indications, operative management, complications, and outcomes. Spine (Phila Pa 1976) 1999, 24, 2617–2629. [Google Scholar] [CrossRef] [PubMed]
- Kanter, A.S.; Tempel, Z.J.; Ozpinar, A.; Okonkwo, D.O. A Review of Minimally Invasive Procedures for the Treatment of Adult Spinal Deformity. Spine (Phila Pa 1976) 2016, 41 Suppl 8, S59–S65. [Google Scholar] [CrossRef]
- Acosta, F.L.; Liu, J.; Slimack, N.; Moller, D.; Fessler, R.; Koski, T. Changes in coronal and sagittal plane alignment following minimally invasive direct lateral interbody fusion for the treatment of degenerative lumbar disease in adults: a radiographic study. J Neurosurg Spine 2011, 15, 92–96. [Google Scholar] [CrossRef]
- Hiyama, A.; Katoh, H.; Sakai, D.; et al. Changes in Spinal Alignment following eXtreme Lateral Interbody Fusion Alone in Patients with Adult Spinal Deformity using Computed Tomography. Sci Rep 2019, 9, 12039–12046. [Google Scholar] [CrossRef] [PubMed]
- Heary, R.F.; Kumar, S.; Bono, C.M. Decision making in adult deformity. Neurosurgery 2008, 63, 69–77. [Google Scholar] [CrossRef]
- Wang, M.Y.; Mummaneni, P.V.; Fu, K.M.; et al. Less invasive surgery for treating adult spinal deformities: ceiling effects for deformity correction with 3 different techniques. Neurosurg Focus 2014, 36, E12–E19. [Google Scholar] [CrossRef] [PubMed]
- Dakwar, E.; Cardona, R.F.; Smith, D.A.; Uribe, J.S. Early outcomes and safety of the minimally invasive, lateral retroperitoneal transpsoas approach for adult degenerative scoliosis. Neurosurg Focus 2010, 28, E8–E14. [Google Scholar] [CrossRef] [PubMed]
- Glassman, S.D.; Berven, S.; Bridwell, K.; Horton, W.; Dimar, J.R. Correlation of radiographic parameters and clinical symptoms in adult scoliosis. Spine (Phila Pa 1976) 2005, 30, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.H.; Wong, C.B.; Chen, L.H.; Niu, C.C.; Tsai, T.T.; Chen, W.J. Instrumented posterior lumbar interbody fusion for patients with degenerative lumbar scoliosis. J Spinal Disord Tech 2008, 21, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Crandall, D.G.; Revella, J. Transforaminal lumbar interbody fusion versus anterior lumbar interbody fusion as an adjunct to posterior instrumented correction of degenerative lumbar scoliosis: three year clinical and radiographic outcomes. Spine (Phila Pa 1976) 2009, 34, 2126–2133. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.K.; Kepler, C.K.; Girardi, F.P.; Cammisa, F.P.; Huang, R.C.; Sama, A.A. Lateral lumbar interbody fusion: clinical and radiographic outcomes at 1 year: a preliminary report. J Spinal Disord Tech 2011, 24, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, P.C.; Koski, T.R.; O’Shaughnessy, B.A.; et al. Anterior lumbar interbody fusion in comparison with transforaminal lumbar interbody fusion: implications for the restoration of foraminal height, local disc angle, lumbar lordosis, and sagittal balance. J Neurosurg Spine 2007, 7, 379–386. [Google Scholar] [CrossRef]
- Schwender, J.D.; Holly, L.T.; Rouben, D.P.; Foley, K.T. Minimally invasive transforaminal lumbar interbody fusion (TLIF): technical feasibility and initial results. J Spinal Disord Tech 2005, 18 Suppl, S1–S6. [Google Scholar] [CrossRef]
- Lee, D.Y.; Jung, T.G.; Lee, S.H. Single-level instrumented mini-open transforaminal lumbar interbody fusion in elderly patients. J Neurosurg Spine 2008, 9, 137–144. [Google Scholar] [CrossRef]
- Kim, S.B.; Jeon, T.S.; Heo, Y.M.; et al. Radiographic results of single level transforaminal lumbar interbody fusion in degenerative lumbar spine disease: focusing on changes of segmental lordosis in fusion segment. Clin Orthop Surg 2009, 1, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Knight, R.Q.; Schwaegler, P.; Hanscom, D.; Roh, J. Direct lateral lumbar interbody fusion for degenerative conditions: early complication profile. J Spinal Disord Tech 2009, 22, 34–37. [Google Scholar] [CrossRef]
- Ozgur, B.M.; Aryan, H.E.; Pimenta, L.; Taylor, W.R. Extreme Lateral Interbody Fusion (XLIF): a novel surgical technique for anterior lumbar interbody fusion. Spine J 2006, 6, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Davis, T.T.; Hynes, R.A.; Fung, D.A.; et al. Retroperitoneal oblique corridor to the L2-S1 intervertebral discs in the lateral position: an anatomic study. J Neurosurg Spine 2014, 21, 785–793. [Google Scholar] [CrossRef]
- Woods, K.R.; Billys, J.B.; Hynes, R.A. Technical description of oblique lateral interbody fusion at L1-L5 (OLIF25) and at L5-S1 (OLIF51) and evaluation of complication and fusion rates. Spine J 2017, 17, 545–553. [Google Scholar] [CrossRef]
- Ko, M.J.; Park, S.W.; Kim, Y.B. Effect of cage in radiological differences between direct and oblique lateral interbody fusion techniques. J Korean Neurosurg Soc 2019, 62, 432–441. [Google Scholar] [CrossRef]
- Ko, M.J.; Park, S.W.; Kim, Y.B. Correction of spondylolisthesis by lateral lumbar interbody fusion compared with transforaminal lumbar interbody fusion at L4-5. J Korean Neurosurg Soc 2019, 62, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.S.; Park, S.W.; Kim, Y.B. Direct lateral lumbar interbody fusion: clinical and radiological outcomes. J Korean Neurosurg Soc 2014, 55, 248–254. [Google Scholar] [CrossRef]
- Johnson, R.D.; Valore, A.; Villaminar, A.; Comisso, M.; Balsano, M. Pelvic parameters of sagittal balance in extreme lateral interbody fusion for degenerative lumbar disc disease. J Clin Neurosci 2013, 20, 576–581. [Google Scholar] [CrossRef]
- Ha, K.Y.; Kim, Y.H.; Seo, J.Y.; Bae, S.H. Percutaneous posterior instrumentation followed by direct lateral interbody fusion for lumbar infectious spondylitis. J Spinal Disord Tech 2013, 26, E95–E100. [Google Scholar] [CrossRef]
- Kepler, C.K.; Huang, R.C.; Sharma, A.K.; et al. Factors influencing segmental lumbar lordosis after lateral transpsoas interbody fusion. Orthop Surg 2012, 4, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Lee, Y.S.; Kim, Y.B.; Park, S.W.; Hung, V.T. Clinical and radiological outcomes of a new cage for direct lateral lumbar interbody fusion. Korean J Spine 2014, 11, 145–151. [Google Scholar] [CrossRef]
- Mun, H.Y.; Ko, M.J.; Kim, Y.B.; Park, S.W. Usefulness of oblique lateral interbody fusion at L5-S1 level compared to transforaminal lumbar interbody fusion. J Korean Neurosurg Soc 2020, 63, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.J.; Zhang, J.F.; Xu, W.B.; et al. Effect of pure muscle retraction on multifidus injury and atrophy after posterior lumbar spine surgery with 24 weeks observation in a rabbit model. Eur Spine J 2017, 26, 210–220. [Google Scholar] [CrossRef]
- Regev, G.J.; Lee, Y.P.; Taylor, W.R.; Garfin, S.R.; Kim, C.W. Nerve injury to the posterior rami medial branch during the insertion of pedicle screws: comparison of mini-open versus percutaneous pedicle screw insertion techniques. Spine (Phila Pa 1976) 2009, 34, 1239–1242. [Google Scholar] [CrossRef]
- Cimatti, M.; Forcato, S.; Polli, F.; Miscusi, M.; Frati, A.; Raco, A. Pure percutaneous pedicle screw fixation without arthrodesis of 32 thoraco-lumbar fractures: clinical and radiological outcome with 36-month follow-up. Eur Spine J 2013, 22, S925–S932. [Google Scholar] [CrossRef]
- Merom, L.; Raz, N.; Hamud, C.; Weisz, I.; Hanani, A. Minimally invasive burst fracture fixation in the thoracolumbar region. Orthopedics 2009, 32, 273–275. [Google Scholar] [CrossRef]
- Ni, W.F.; Huang, Y.X.; Chi, Y.L.; et al. Percutaneous pedicle screw fixation for neurologic intact thoracolumbar burst fractures. J Spinal Disord Tech 2010, 23, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Korovessis, P.; Repantis, T.; Petsinis, G.; Iliopoulos, P.; Hadjipavlou, A. Direct reduction of thoracolumbar burst fractures by means of balloon kyphoplasty with calcium phosphate and stabilization with pedicle-screw instrumentation and fusion. Spine (Phila Pa 1976) 2008, 33, E100–E108. [Google Scholar] [CrossRef]
- Kosmopoulos, V.; Schizas, C. Pedicle screw placement accuracy: a meta-analysis. Spine (Phila Pa 1976) 2007, 32, E111–E120. [Google Scholar] [CrossRef]
- Park, S.W.; Ko, M.J.; Kim, Y.B.; Le Huec, J.C. Correction of marked sagittal deformity with circumferential minimally invasive surgery using oblique lateral interbody fusion in adult spinal deformity. J Orthop Surg Res 2020, 15, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.Y.; Williams, S.; Mummaneni, P.V.; Sherman, J.D. Minimally invasive percutaneous iliac screws: Initial 24 case experiences with CT confirmation. Clin Spine Surg 2016, 29, E222–E225. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Hasan, M.Y.; Wong, H.K. Subcrestal Iliac-Screw: A technical note describing a free hand, in-line, low profile iliac screw insertion technique to avoid side-connector use and reduce implant complications. Spine (Phila Pa 1976) 2018, 43, E68–E74. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.J.; Bridwell, K.H.; Lenke, L.G.; Berra, A.; Baldus, C. Comparison of Smith-Petersen versus pedicle subtraction osteotomy for the correction of fixed sagittal imbalance. Spine (Phila Pa 1976) 2005, 30, 2030–2037. [Google Scholar] [CrossRef] [PubMed]
- Geck, M.J.; Macagno, A.; Ponte, A.; Shufflebarger, H.L. The Ponte procedure: posterior only treatment of Scheuermann’s kyphosis using segmental posterior shortening and pedicle screw instrumentation. J Spinal Disord Tech 2007, 20, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Lazennec, J.Y.; Neves, N.; Rousseau, M.A.; Boyer, P.; Pascal-Mousselard, H.; Saillant, G. Wedge osteotomy for treating post-traumatic kyphosis at thoracolumbar and lumbar levels. J Spinal Disord Tech 2006, 19, 487–494. [Google Scholar] [CrossRef] [PubMed]
- van Loon, P.J.; van Stralen, G.; van Loon, C.J.; van Susante, J.L. A pedicle subtraction osteotomy as an adjunctive tool in the surgical treatment of a rigid thoracolumbar hyperkyphosis; a preliminary report. Spine J 2006, 6, 195–200. [Google Scholar] [CrossRef]
- Saifi, C.; Laratta, J.L.; Petridis, P.; Shillingford, J.N.; Lehman, R.A.; Lenke, L.G. Vertebral column resection for rigid spinal deformity. Global Spine J 2017, 7, 280–290. [Google Scholar] [CrossRef]
- Enercan, M.; Ozturk, C.; Kahraman, S.; Sarıer, M.; Hamzaoglu, A.; Alanay, A. Osteotomies/spinal column resections in adult deformity. Eur Spine J 2013, 22 Suppl 2, S254–S264. [Google Scholar] [CrossRef]
- Camargo, F.P.; Cordeiro, E.N.; Napoli, M.M. Corrective osteotomy of the spine in ankylosing spondylitis. Experience with 66 cases. Clin Orthop Relat Res 1986, 157–167. [Google Scholar]
- Gill, J.B.; Levin, A.; Burd, T.; Longley, M. Corrective osteotomies in spine surgery. J Bone Joint Surg Am 2008, 90, 2509–2520. [Google Scholar] [CrossRef]
- Buchowski, J.M.; Bridwell, K.H.; Lenke, L.G.; et al. Neurologic complications of lumbar pedicle subtraction osteotomy: a 10-year assessment. Spine (Phila Pa 1976) 2007, 32, 2245–2252. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.P.; Ondra, S.L.; Chen, L.A.; Jung, H.S.; Koski, T.R.; Salehi, S.A. Clinical and radiographic outcomes of thoracic and lumbar pedicle subtraction osteotomy for fixed sagittal imbalance. J Neurosurg Spine 2006, 5, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Ahn, U.M.; Ahn, N.U.; Buchowski, J.M.; et al. Functional outcome and radiographic correction after spinal osteotomy. Spine (Phila Pa 1976) 2002, 27, 1303–1311. [Google Scholar] [CrossRef]
- Suk, S.I.; Kim, J.H.; Kim, W.J.; Lee, S.M.; Chung, E.R.; Nah, K.H. Posterior vertebral column resection for severe spinal deformities. Spine (Phila Pa 1976) 2002, 27, 2374–2382. [Google Scholar] [CrossRef] [PubMed]
- Dickson, D.D.; Lenke, L.G.; Bridwell, K.H.; Koester, L.A. Risk factors for and assessment of symptomatic pseudarthrosis after lumbar pedicle subtraction osteotomy in adult spinal deformity. Spine (Phila Pa 1976) 2014, 39, 1190–1195. [Google Scholar] [CrossRef] [PubMed]
- Kavadi, N.; Tallarico, R.A.; Lavelle, W.F. Analysis of instrumentation failures after three column osteotomies of the spine. Scoliosis Spinal Disord 2017, 12, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Schwab, F.; Ungar, B.; Blondel, B.; et al. Scoliosis Research Society-Schwab adult spinal deformity classification: a validation study. Spine (Phila Pa 1976) 2012, 37, 1077–1082. [Google Scholar] [CrossRef]
- Kyrola, K.; Repo, J.; Mecklin, J.P.; Ylinen, J.; Kautiainen, H.; Hakkinen, A. Spinopelvic changes based on the simplified SRS-Schwab adult spinal deformity classification: Relationships with disability and health-related quality of life in adult patients with prolonged degenerative spinal disorders. Spine (Phila Pa 1976) 2018, 43, 497–502. [Google Scholar] [CrossRef]
- Mendoza-Lattes, S.; Ries, Z.; Gao, Y.; Weinstein, S.L. Proximal junctional kyphosis in adult reconstructive spine surgery results from incomplete restoration of the lumbar lordosis relative to the magnitude of the thoracic kyphosis. Iowa Orthop J 2011, 31, 199–206. [Google Scholar] [PubMed] [PubMed Central]
- Bridwell, K.H.; Lenke, L.G.; Cho, S.K.; et al. Proximal junctional kyphosis in primary adult deformity surgery: evaluation of 20 degrees as a critical angle. Neurosurgery 2013, 72, 899–906. [Google Scholar] [CrossRef] [PubMed]
- Glattes, R.C.; Bridwell, K.H.; Lenke, L.G.; Kim, Y.J.; Rinella, A.; Edwards, C., 2nd. Proximal junctional kyphosis in adult spinal deformity following long instrumented posterior spinal fusion: incidence, outcomes, and risk factor analysis. Spine (Phila Pa 1976) 2005, 30, 1643–1649. [Google Scholar] [CrossRef] [PubMed]
- Maruo, K.; Ha, Y.; Inoue, S.; et al. Predictive factors for proximal junctional kyphosis in long fusions to the sacrum in adult spinal deformity. Spine (Phila Pa 1976) 2013, 38, E1469–E1476. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.S.; Shaffrey, E.; Klineberg, E.; et al. Prospective multicenter assessment of risk factors for rod fracture following surgery for adult spinal deformity. J Neurosurg Spine 2014, 21, 994–1003. [Google Scholar] [CrossRef]
- Akazawa, T.; Kotani, T.; Sakuma, T.; Nemoto, T.; Minami, S. Rod fracture after long construct fusion for spinal deformity: clinical and radiographic risk factors. J Orthop Sci 2013, 18, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Lafage, R.; Bess, S.; Glassman, S.; et al. Virtual Modeling of Postoperative Alignment after adult spinal deformity surgery helps predict associations between compensatory spinopelvic alignment changes, overcorrection, and proximal junctional kyphosis. Spine (Phila Pa 1976) 2017, 42, E1119–E1125. [Google Scholar] [CrossRef]
- Kim, Y.J.; Bridwell, K.H.; Lenke, L.G.; Kim, J.; Cho, S.K. Proximal junctional kyphosis in adolescent idiopathic scoliosis following segmental posterior spinal instrumentation and fusion: minimum 5-year follow-up. Spine (Phila Pa 1976) 2005, 30, 2045–2050. [Google Scholar] [CrossRef]
- Le Huec, J.C.; Hasegawa, K. Normative values for the spine shape parameters using 3D standing analysis from a database of 268 asymptomatic Caucasian and Japanese subjects. Eur Spine J 2016, 25, 3630–3637. [Google Scholar] [CrossRef] [PubMed]
- Faundez, A.A.; Richards, J.; Maxy, P.; Price, R.; Leglise, A.; Le Huec, J.C. The mechanism in junctional failure of thoraco-lumbar fusions. Part II: Analysis of a series of PJK after thoraco-lumbar fusion to determine parameters allowing to predict the risk of junctional breakdown. Eur Spine J 2018, 27, 139–148. [Google Scholar] [CrossRef]
- Bae, J.; Theologis, A.A.; Strom, R.; et al. Comparative analysis of 3 surgical strategies for adult spinal deformity with mild to moderate sagittal imbalance. J Neurosurg Spine 2018, 28, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Janik, T.J.; Harrison, D.D.; Cailliet, R.; Troyanovich, S.J.; Harrison, D.E. Can the sagittal lumbar curvature be closely approximated by an ellipse? J Orthop Res 1998, 16, 766–770. [Google Scholar] [CrossRef] [PubMed]
- Roussouly, P.; Gollogly, S.; Berthonnaud, E.; Dimnet, J. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine (Phila Pa 1976) 2005, 30, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Yilgor, C.; Sogunmez, N.; Boissiere, L.; et al. Global Alignment and Proportion (GAP) score: Development and validation of a new method of analyzing spinopelvic alignment to predict mechanical complications after adult spinal deformity surgery. J Bone Joint Surg Am 2017, 99, 1661–1672. [Google Scholar] [CrossRef] [PubMed]
- Savage, J.W.; Patel, A.A. Fixed sagittal plane imbalance. Global Spine J 2014, 4, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Tannoury, T.; Kempegowda, H.; Haddadi, K.; Tannoury, C. Complications associated with minimally invasive anterior to the psoas (ATP) fusion of the lumbosacral spine. Spine (Phila Pa 1976) 2019, 44, E1122–e9. [Google Scholar] [CrossRef] [PubMed]
- Abed Rabbo, F.; Wang, Z.; Sunna, T.; et al. Long-term complications of minimally-open anterolateral interbody fusion for L5-S1. Neurochirurgie 2020, 66, 85–90. [Google Scholar] [CrossRef]
- Xi, Z.; Burch, S.; Mummaneni, P.V.; Mayer, R.R.; Eichler, C.; Chou, D. The effect of obesity on perioperative morbidity in oblique lumbar interbody fusion. J Neurosurg Spine 2020, 27, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Abe, K.; Orita, S.; Mannoji, C.; et al. Perioperative complications in 155 patients who underwent oblique lateral interbody fusion surgery: Perspectives and indications from a retrospective, multicenter survey. Spine (Phila Pa 1976) 2017, 42, 55–62. [Google Scholar] [CrossRef]
- Liu, C.; Wang, J. Learning Curve of Minimally invasive surgery oblique lumbar interbody fusion for degenerative lumbar diseases. World Neurosurg 2018, 120, e88–e93. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Differences of postoperative disc angle at L5-S1 according to the types of lumbar interbody fusion (LIF) and cage angles. (a) Transforaminal LIF (TLIF) using a bullet-shaped cage; the postoperative disc angle was 7.8°. (b) Oblique LIF at L5-S1 (OLIF51) using a 12° cage; the postoperative disc angle was 18.9°. (c) OLIF51 using a 24° cage; the postoperative disc angle at L5-S1 was 24.5°. We performed posterior rod compression for posterior shortening without corrective osteotomy in all three cases.
Figure 1.
Differences of postoperative disc angle at L5-S1 according to the types of lumbar interbody fusion (LIF) and cage angles. (a) Transforaminal LIF (TLIF) using a bullet-shaped cage; the postoperative disc angle was 7.8°. (b) Oblique LIF at L5-S1 (OLIF51) using a 12° cage; the postoperative disc angle was 18.9°. (c) OLIF51 using a 24° cage; the postoperative disc angle at L5-S1 was 24.5°. We performed posterior rod compression for posterior shortening without corrective osteotomy in all three cases.
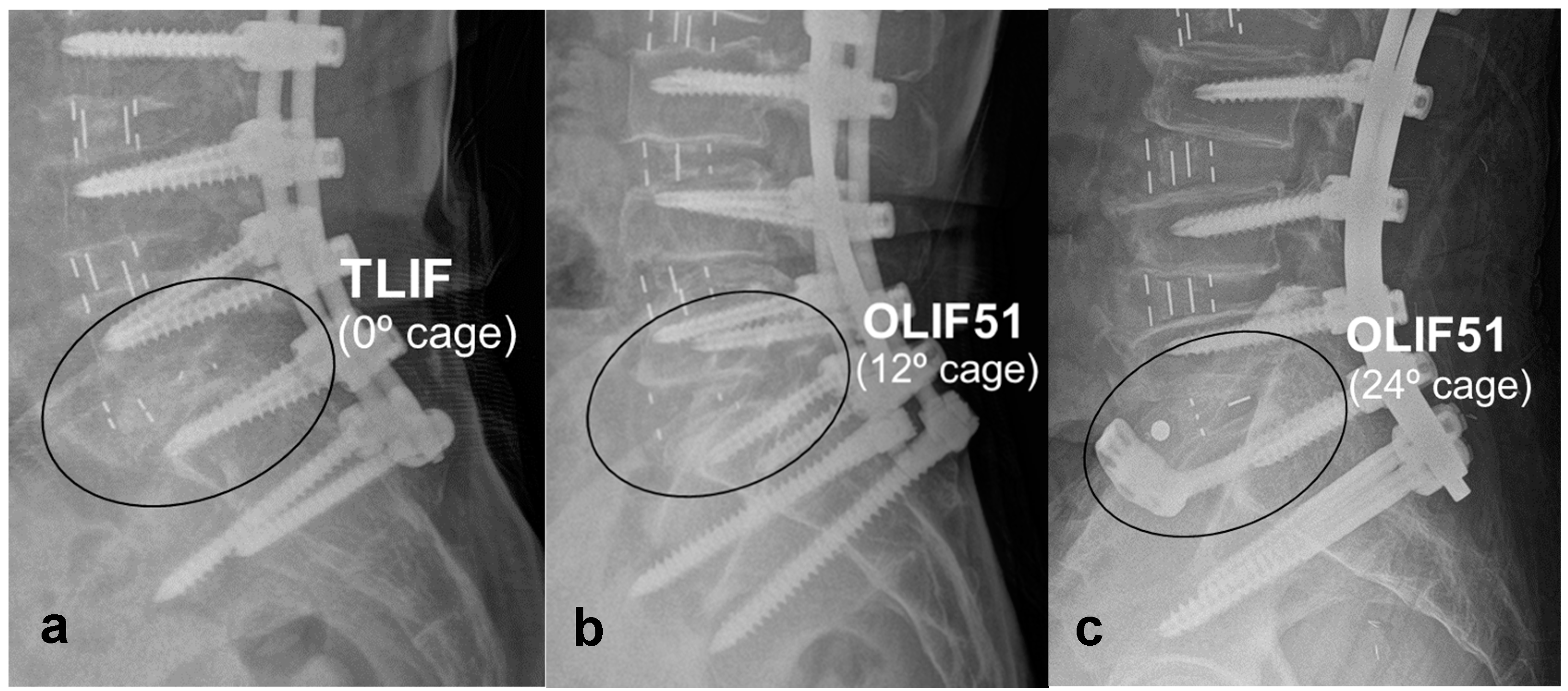
Figure 2.
A case of MIS deformity surgery with a long-level posterior percutaneous pedicle screw fixation connection to the subcrestal iliac screws (circles).
Figure 2.
A case of MIS deformity surgery with a long-level posterior percutaneous pedicle screw fixation connection to the subcrestal iliac screws (circles).
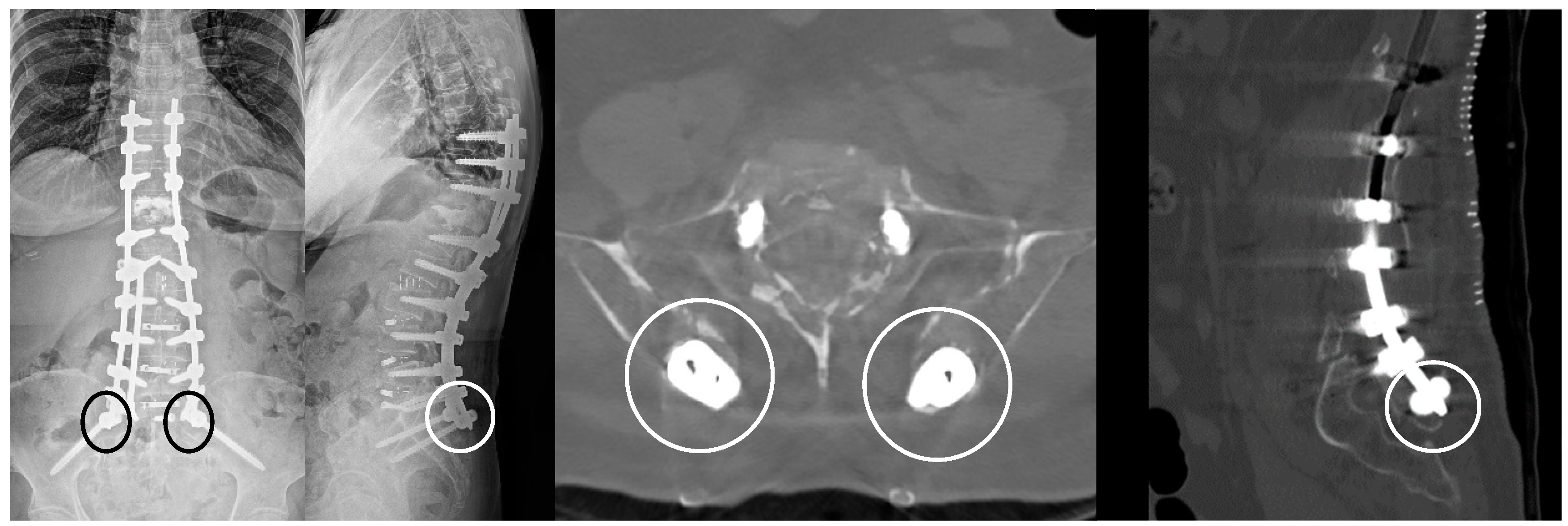
Figure 3.
A high-angle and high-profile cage, placed at the anterior disc space, can make more space posteriorly, providing an increased allowance for making lumbar angle by posterior shortening.
Figure 3.
A high-angle and high-profile cage, placed at the anterior disc space, can make more space posteriorly, providing an increased allowance for making lumbar angle by posterior shortening.
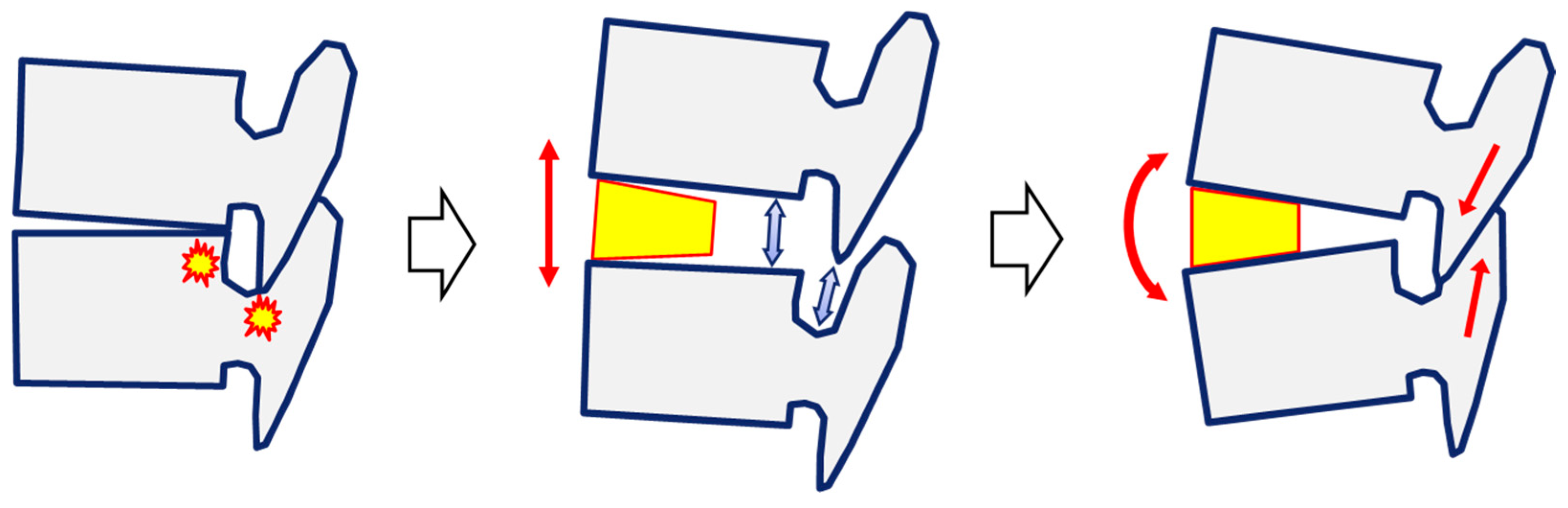
Figure 4.
An illustrative case of MIS deformity surgery showing how to calculate lumbar angle correction preoperatively. (a, b) Preoperative radiographs; SVA = 95.8 mm, PI = 54.2°, LL = +9.6°, and PI-LL = 63.8°. If we set the minimum target LL as ≥PI [69], the target LL would be ≥54.2°. A pre-existing angle loss was +7.5°: by summation of +17.9° (kyphotic L1 body), +1.9° (kyphotic L2 body), -2.3° (lordotic L3 body), and -10.0° (Cobb angle of L4-5). The minimum required angle correction was calculated as 54.2° + 7.5° = 61.7°. (c) Based on the data that the lateral lumbar interbody fusion could make disc angle greater than or equal to the cage angle [37,43,44,52], the estimated disc angle correction would be ≥36° at L1-2-3-4 with three 12° cages and ≥24° at L5-S1 with a 24° cage. Finally, the estimated angle correction and the estimated postoperative LL were ≥60° (36° + 24°) and ≥52.5°, respectively. According to the SRS-Schwab criteria or GAP score [66,81], the estimated LL was acceptable, and we could avoid the corrective osteotomy. (d, e) The final postoperative radiographs; lumbar angle correction = 62.3° and corrected lumbar angle = 56.5°, better than the preoperative estimations. Postoperative sagittal balance was satisfactory with SVA = 25.3 mm and PI-LL = 2.3°.
Figure 4.
An illustrative case of MIS deformity surgery showing how to calculate lumbar angle correction preoperatively. (a, b) Preoperative radiographs; SVA = 95.8 mm, PI = 54.2°, LL = +9.6°, and PI-LL = 63.8°. If we set the minimum target LL as ≥PI [69], the target LL would be ≥54.2°. A pre-existing angle loss was +7.5°: by summation of +17.9° (kyphotic L1 body), +1.9° (kyphotic L2 body), -2.3° (lordotic L3 body), and -10.0° (Cobb angle of L4-5). The minimum required angle correction was calculated as 54.2° + 7.5° = 61.7°. (c) Based on the data that the lateral lumbar interbody fusion could make disc angle greater than or equal to the cage angle [37,43,44,52], the estimated disc angle correction would be ≥36° at L1-2-3-4 with three 12° cages and ≥24° at L5-S1 with a 24° cage. Finally, the estimated angle correction and the estimated postoperative LL were ≥60° (36° + 24°) and ≥52.5°, respectively. According to the SRS-Schwab criteria or GAP score [66,81], the estimated LL was acceptable, and we could avoid the corrective osteotomy. (d, e) The final postoperative radiographs; lumbar angle correction = 62.3° and corrected lumbar angle = 56.5°, better than the preoperative estimations. Postoperative sagittal balance was satisfactory with SVA = 25.3 mm and PI-LL = 2.3°.
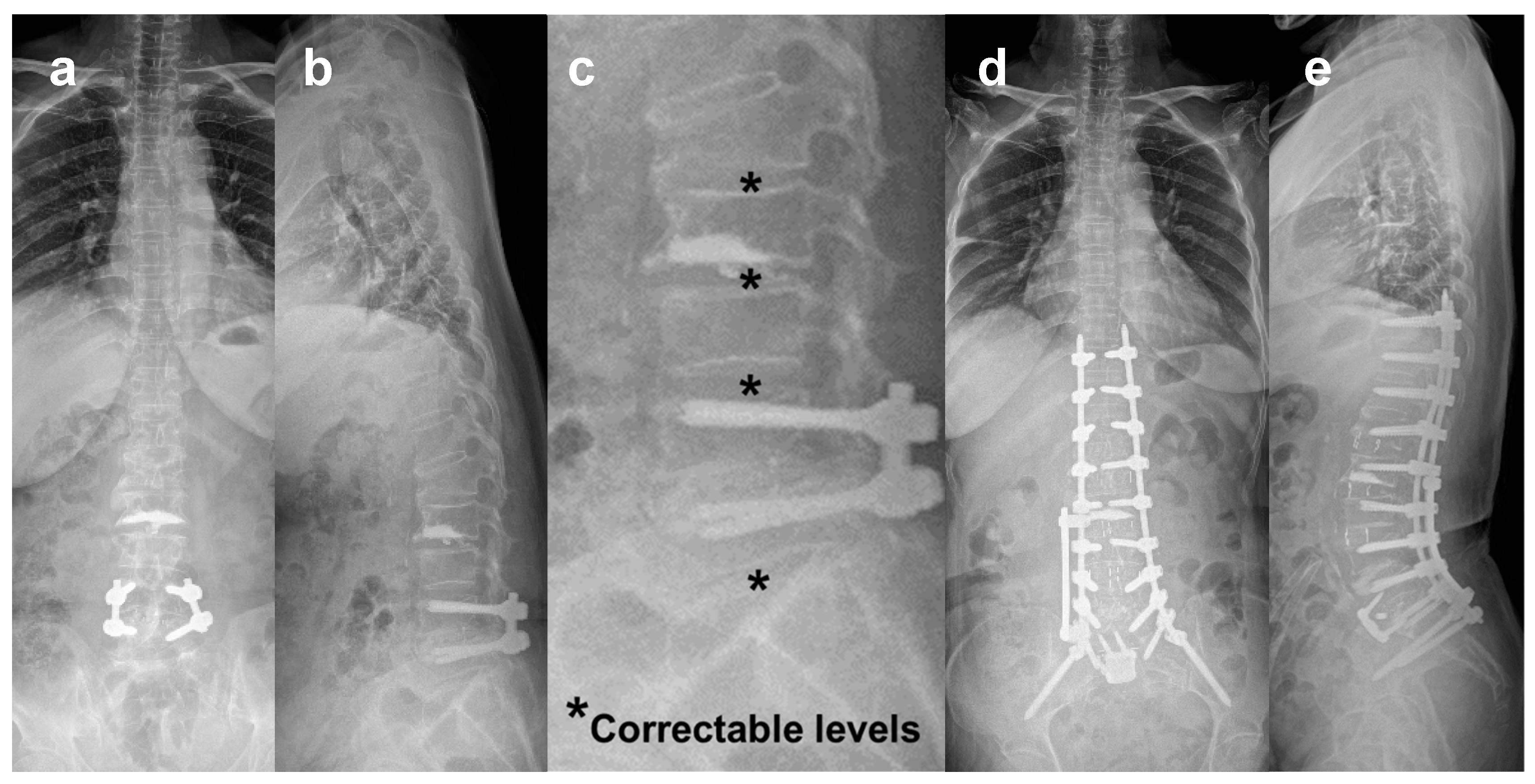
Figure 5.
Correction of marked sagittal imbalance by MIS deformity surgery using lateral lumbar interbody fusion at L2-3-4-5-S1 and posterior percutaneous pedicle screw fixation without corrective osteotomy. (a, b) Preoperative radiographs; PI = 50.7°. SVA = 147 mm, LL = +7.8°, PI-LL = 58.5°, and PT = 44.2°. (c, d) Postoperative radiographs; the SVA = -27.0 mm, LL = -53.9°, PI-LL = 3.1°, and PT = 23.9°.
Figure 5.
Correction of marked sagittal imbalance by MIS deformity surgery using lateral lumbar interbody fusion at L2-3-4-5-S1 and posterior percutaneous pedicle screw fixation without corrective osteotomy. (a, b) Preoperative radiographs; PI = 50.7°. SVA = 147 mm, LL = +7.8°, PI-LL = 58.5°, and PT = 44.2°. (c, d) Postoperative radiographs; the SVA = -27.0 mm, LL = -53.9°, PI-LL = 3.1°, and PT = 23.9°.
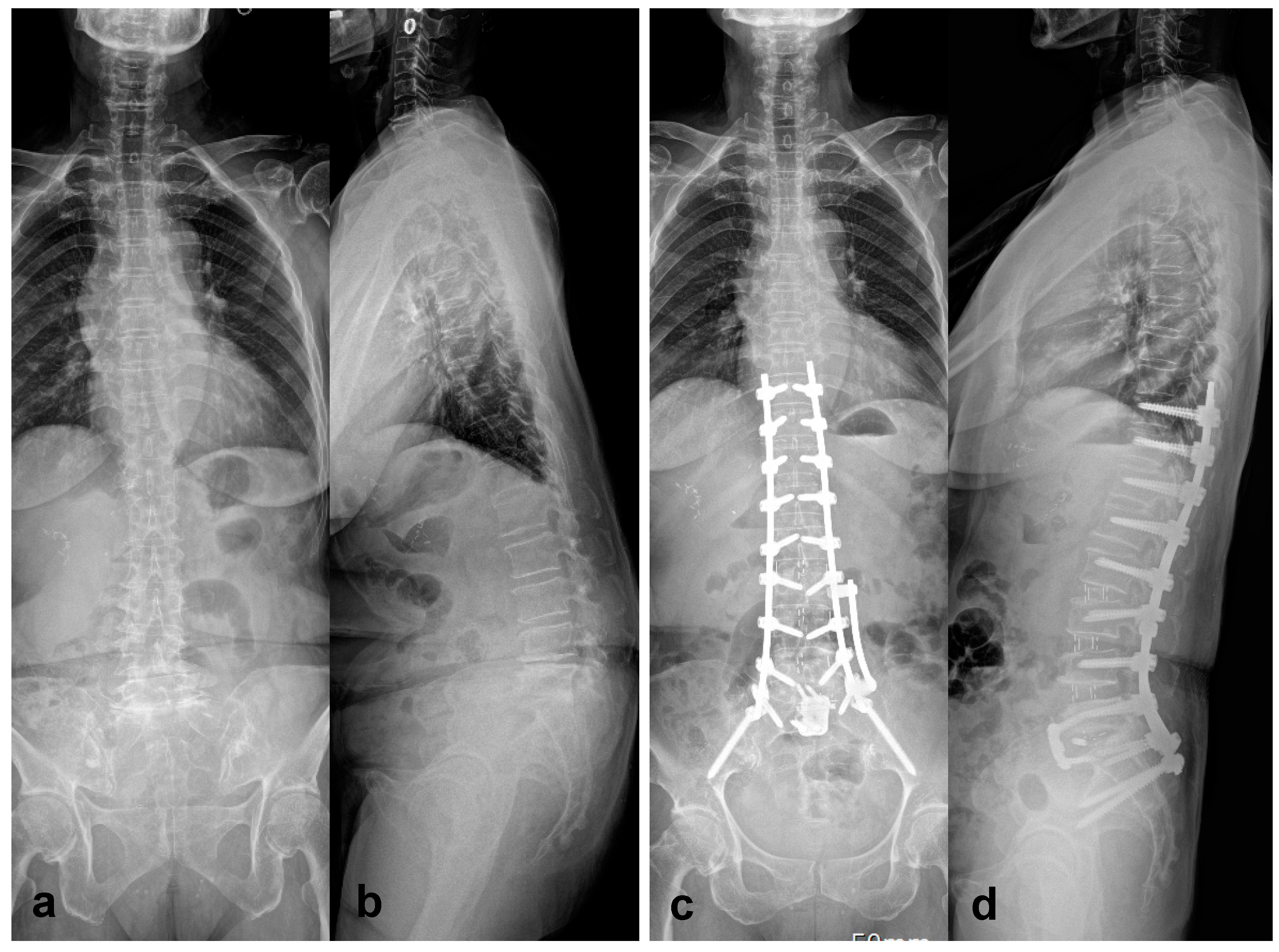
Figure 6.
Two cases underwent MIS deformity surgery with postoperative follow-up radiographs. Case 1 (a, b, and c): Preoperative (a), immediate postoperative (b), and postoperative 7 months (c) radiographs. Early PJK started 7 months after surgery due to exaggerated upper lumbar lordosis with a decreased lower lumbar lordosis (LLL) proportion (38.7%) caused by the lordotic rod curve at the thoracolumbar junction. Case 2 (d, e, and f): Preoperative (d), immediate postoperative (e), and postoperative 2 years (f) radiographs. The patient showed a well-preserved proximal junctional level 2 years after surgery. Compared to Case 1, the kyphotic rod angle at the thoracolumbar junction reduced upper lumbar lordosis and increased the LLL proportion (71.5%).
Figure 6.
Two cases underwent MIS deformity surgery with postoperative follow-up radiographs. Case 1 (a, b, and c): Preoperative (a), immediate postoperative (b), and postoperative 7 months (c) radiographs. Early PJK started 7 months after surgery due to exaggerated upper lumbar lordosis with a decreased lower lumbar lordosis (LLL) proportion (38.7%) caused by the lordotic rod curve at the thoracolumbar junction. Case 2 (d, e, and f): Preoperative (d), immediate postoperative (e), and postoperative 2 years (f) radiographs. The patient showed a well-preserved proximal junctional level 2 years after surgery. Compared to Case 1, the kyphotic rod angle at the thoracolumbar junction reduced upper lumbar lordosis and increased the LLL proportion (71.5%).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



